
Submitted:
28 June 2023
Posted:
29 June 2023
You are already at the latest version
Abstract
Excretion of β2-microglobulin (β2M) above 300 µg/g creatinine, termed tubulopathy, was regarded as the critical effect of chronic exposure to the metal pollutant cadmium (Cd). However, current evidence suggests that Cd may induce nephron atrophy, resulting in a reduction in the estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m2. Herein, these pathologies were investigated in relation to Cd exposure, smoking, diabetes and hypertension. Data were from 448 residents of Cd-polluted and non-polluted regions of Thailand. The body burden of Cd, indicated by the mean Cd excretion (ECd) normalized to creatinine clearance (Ccr) as (ECd/Ccr) ×100 in women and men did not differ (3.21 vs. 3.12 µg/L filtrate). The prevalence odds ratio (POR) for tubulopathy and a reduced eGFR were increased by 1.9-fold and 3.2-fold for every 10-fold rise in Cd body burden. In women only, a dose-effect relationship was seen between β2M excretion (Eβ2M/Ccr) and ECd/Ccr (F = 3.431, η2 0.021). In men, Eβ2M/Ccr was associated with diabetes (β = 0.279). In both genders, eGFR was inversely associated with Eβ2M/Ccr. The respective covariate- adjusted mean eGFR values were 16.5 and 12.3 mL/min/1.73 m2 lower in women and men who had severe tubulopathy; (Eβ2M/Ccr) ×100 ≥ 1000 µg/L filtrate. These findings indicate that women were particularly susceptible to the nephrotoxicity of Cd, and that the increment of Eβ2M/Ccr could be attributable mostly to Cd-induced impairment in tubular reabsorption of the protein together with Cd-induced nephron loss, evident from an inverse relationship between Eβ2M/Ccr and the eGFR.
Keywords:
β2-microglobulin
; cadmium
; diabetes
; GFR
; hypertension
; smoking
; tubular proteinuria
1. Introduction
Cadmium (Cd) is a toxic metal pollutant that accumulates in the proximal tubule of kidneys, where it causes tubular cell injury, resulting in cell death, tubular and nephron atrophy, and eventually a reduction in the estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m2 [1,2,3,4]. Because diet is an inevitable Cd exposure source, Cd has become one of the environmental toxicants of increasing public health concern worldwide. The Japan total diet study undertaken from 2013 to 2018 reported that rice and its products, green vegetables, cereals, and seeds plus potatoes constituted 38%, 17%, and 11% of total dietary exposure, respectively [5].
To safeguard against excessive exposure to Cd in the human diet, exposure guidelines, referred to as a tolerable intake level of Cd, was derived by the Joint FAO/WHO Expert Committee on Food Additives and Contaminants (JECFA) [6]. Of note, the “tolerable” intake level derived was based on the risk assessment model that assumed tubular proteinuria, reflected by an increase in the excretion of the low-molecular-weight protein β2-microglubulin (β2M, Eβ2M) above 300 μg/g creatinine to be an early warning sign of the nephrotoxicity of Cd. Consequently, tubulopathy is the most frequently reported as an adverse effect of Cd exposure. Numerous studies, however, have cast considerable doubt on the utility of Eβ2M for such purposes.
This study aimed to examine if exposure to Cd adversely impacts kidney toxicity differently in men and women. To this end, tubular dysfunction and changes in the eGFR were quantified in residents of Cd-polluted and non-polluted regions of Thailand and analyzed in relation to Cd exposure levels. The confounding impact of smoking, diabetes and hypertension were also evaluated. Exposure to Cd was assessed by measurement of blood Cd concentration ([Cd]b), and urinary Cd excretion (ECd). Tubular dysfunction was assessed by Eβ2M. Equations developed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) were used to compute the estimated GFR (eGFR) [7].
2. Materials and Methods
2.1. Participants
To obtain a group with a wide range of environmental Cd exposure amenable to dose-effect relationship assessment, we assembled data from 334 women and 114 men who participated in the cross-sectional studies conducted in a high-exposure area of the Mae Sot District, Tak Province [8] and a low-exposure locality in Pakpoon Municipality of Nakhon-Si-Thammarat Province [9]. Based on the data from a nationwide survey of Cd levels in soils and food crops [10], environmental exposure to Cd in Nakhon Si Thammarat were low.
The study protocol for the Mae Sot group was approved by the Institutional Ethical Committees of Chiang Mai University and the Mae Sot Hospital [8]. The study protocol for the Nakhon Si Thammarat group was approved by the Office of the Human Research Ethics Committee of Walailak University in Thailand [9].
All participants gave informed consent prior to participation. They had lived at their current addresses for at least 30 years. Exclusion criteria were pregnancy, breast-feeding, a history of metal work, and a hospital record or physician’s diagnosis of an advanced chronic disease. Diabetes was defined as fasting plasma glucose levels ≥126 mg/dL (https://www.cdc.gov/diabetes/basics/getting-tested.html (accessed on 25 June 2023) or a physician’s prescription of anti-diabetic medications. Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg [11], a physician’s diagnosis, or prescription of anti-hypertensive medications.
2.2. Collection and Analysis of Blood and Urine Samples
Second morning urine samples were collected after overnight fast, and whole blood samples were obtained within 3 h after the urine sampling. Aliquots of urine, whole blood, and plasma were stored at −20 or −80 °C for later analysis. The assay for urine and plasma concentrations of creatinine ([cr]u and [cr]p) was based on the Jaffe reaction. The assay of urinary β2M concentration ([β2M]u) was based on the latex immunoagglutination method (LX test, Eiken 2MGII; Eiken and Shionogi Co., Tokyo, Japan) or the ELISA method (Sino Biological Inc., Wayne, PA, USA).
Urinary Cd concentration ([Cd]u) was determined using atomic absorption spectrophotometer. Urine standard reference material No. 2670 (National Institute of Standards, Washington, DC, USA) or the reference urine metal control levels 1, 2, and 3 (Lyphocheck, Bio-Rad, Hercules, CA, USA) were used for quality control, analytical accuracy, and precision assurance. was used for quality assurance and control purposes. The limit of detection (LOD) of Cd quantitation was defined as 3 times the standard deviation of blank measurements. When [Cd]u was below its detection limit (0.1 µg/L), the Cd concentration assigned was the LOD divided by the square root of 2 [12]
2.3. Estimated Glomerular Filtration Rates (eGFRs)
The GFR is the product of nephron number and mean single nephron GFR, and in theory, the GFR is indicative of nephron function [13,14,15]. In practice, the GFR is estimated from established chronic kidney disease–epidemiology collaboration (CKD-EPI) equations and is reported as eGFR [15].
Male eGFR = 141 × [plasma creatinine/0.9]Y × 0.993age, where Y = −0.411 if [cr]p ≤ 0.9 mg/dL, and Y = −1.209 if [cr]p > 0.9 mg/dL. Female eGFR = 144 × [plasma creatinine/0.7]Y × 0.993age, where Y = −0.329 if [cr]p ≤ 0.7 mg/dL, and Y = −1.209 if [cr]p > 0.7 mg/dL. CKD stages 1, 2, 3a, 3b, 4, and 5 corresponded to eGFR of 90–119, 60–89, 45–59, 30−44, 15–29, and <15 mL/min/1.73 m2, respectively.
2.4. Normalization of Excretion Rate
Ex was normalized to Ecr as [x]u/[cr]u, where x = Cd or β2M; [x]u = urine concentration of x (mass/volume); and [cr]u = urine creatinine concentration (mg/dL). The ratio [x]u/[cr]u was expressed in μg/g of creatinine.
Ex was normalized to Ccr as Ex/Ccr = [x]u[cr]p/[cr]u, where x = Cd or β2M; [x]u = urine concentration of x (mass/volume); [cr]p = plasma creatinine concentration (mg/dL); and [cr]u = urine creatinine concentration (mg/dL). Ex/Ccr was expressed as the excretion of x per volume of filtrate [7].
2.5. Statistical Analysis
Data were analyzed with IBM SPSS Statistics 21 (IBM Inc., New York, NY, USA). The Mann–Whitney U test was used to assess differences in mean values in women and men, and the Pearson chi-squared test was used to assess differences in percentages. The one-sample Kolmogorov–Smirnov test was used to identify departures of continuous variables from a normal distribution, and logarithmic transformation was applied to variables that showed rightward skewing before they were subjected to parametric statistical analysis.
The multivariable logistic regression analysis was used to determine the Prevalence Odds Ratio (POR) for categorical outcomes. Reduced eGFR was assigned when eGFR ≤ 60 mL/min/1.73 m2. For Ccr-normalized data, tubular dysfunction was defined as (Eβ2M/Ccr) × 100 ≥ 300 µg/L of filtrate. For Ecr-normalized data, tubular dysfunction was defined as Eβ2M/Ecr ≥ 300 µg/g creatinine [6]. Univariate analysis of covariance with Bonferroni correction in multiple comparisons was used to obtain covariate-adjusted mean ECd/Ccr and mean Eβ2M/Ccr. For all tests, p-values ≤ 0.05 were considered to indicate statistical significance.
3. Results
3.1. Descriptive Characteristics of Participants
This cohort consisted of 334 women (mean age 51.5 years) and 114 men (mean age 49.9 years) (Table 1).
Notes: n, number of subjects; BMI, body mass index; eGFR, estimated glomerular filtration rate; β2M, β2-microglobulin; Ex, excretion of x; cr, creatinine; Ccr, creatinine clearance; Cd, cadmium; a eGFR, was determined by established CKD-EPI equations [15]; b reduced eGFR corresponds to eGFR ≤60 mL/min/1.73m2; c Ex/Ecr = [x]u/[cr]u; d Ex/Ccr = [x]u[cr]p/[cr]u, where x = Cd or β2M [7]. Data for all continuous variables are arithmetic means ± standard deviation (SD). For all tests, p ≤ 0.05 identifies statistical significance, determined by Pearson chi-square test for % differences and by the Mann–Whitney U-test for mean differences between women and men. #p = 0.005; * p = 0.004; **p = 0.002.
The respective overall percentages of smoking, hypertension, diabetes and reduced eGFR were 31.3%, 48.7% 15.4% and 6.9%. More than half of men (68.4%) smoked cigarettes, while only 18.6% of women did. The % all other ill health conditions in men and women did not differ nor did their mean age.
With the exception for BMI, mean plasma creatinine, mean urine creatinine, and mean blood Cd all were lower in women than men. Mean eGFR, mean urine Cd and mean β2M concentrations in women and men were not statistically different.
For Ccr-normalized data, the mean ECd/Ccr and mean Eβ2M/Ccr in women and men both did not differ statistically. However, there were statistically significant differences in the % of women and men across three Eβ2M/Ccr groups.
For Ecr-normalized data, the mean ECd/Ecr and mean Eβ2M/Ecr were higher in women than men. The % of men across three Eβ2M/Ecr groups differed, but there was no difference in the % of women across Eβ2M/Ecr groups.
3.2. Cadmium Exposure Characterization
Figure 1 provides scatterplots relating two Cd exposure indicators, namely blood Cd concentration and excretion rate of Cd as ECd/Ccr.
A strong positive association between log([Cd]b×103) and [log[(ECd/Ccr)×105] was evident in both women and men (Figure 1a). After adjustment for covariates and interactions, Cd body burden ([log[(ECd/Ccr) ×105] explained a larger proportion of the variation in blood Cd concentrations (log([Cd]b×103) in men (η2 = 0.407) than in women (η2 = 0.105) (Figure 1b).
To further address the variables/factors that may influence blood Cd levels, we conducted multiple regression and univariate analyses of variance that incorporated age, BMI, log[(ECd/Ccr) ×105], smoking, diabetes and hypertension as independent variables. Table 2 provides results of these analyses.
β, standardized regression coefficient; adjusted R2, coefficient of determination; DM, diabetes; HTN, hypertension; SMK, smoking; n/a, not applicable. β indicates strength of association of log([Cd]b×103) with independent variables (first column). Adjusted R2 indicates a fractional variation of log([Cd]b×103) explained by all independent variables. Eta square (η2) indicates the fraction of the variability of each dependent variable explained by a corresponding independent variable. p-values ≤ 0.05 indicate a statistically significant contribution of variation of an independent variable to variation of a dependent variable.
In women, higher [Cd]b values were associated strongly with higher ECd/Ccr (β = 0.619), and moderately associated with smoking (β = 0.123), and younger age (β = −0.170). ECd/Ccr, age, and smoking explained respectively 36.7%, 5.7% and 2.8% of the variation of [Cd]b in women, while the interaction between diabetes and hypertension contributed to 1.6% of [Cd]b variability. In men, higher [Cd]b values were associated strongly with higher ECd/Ccr (β = 0.581), moderately with smoking (β = 0.184) and not having diabetes (β = −0.246). ECd/Ccr, smoking and diabetes accounted, respectively for 42%%, 5.5% and 9.5% of the variation of [Cd]b in men, while the interaction between smoking, diabetes and hypertension contributed to 4.2 % of [Cd]b variability.
3.3. Effects of Cadmium Exposure on β2M excretion
We assessed the effects of Cd exposure on Eβ2M with multiple linear regression and univariate/covariance analysis, where the indicators of Cd exposure ([Cd]b and ECd) were incorporated as the independent variables together with age, BMI, smoking, diabetes, and hypertension (Table 3).
β, standardized regression coefficient; adjusted R2, coefficient of determination; β indicates strength of association of log[(Eβ2M/Ccr) ×103] with independent variables (first column). Adjusted R2 indicates a fractional variation of log[(Eβ2M/Ccr)×103] explained by all independent variables. For each test, p-values ≤ 0.05 indicate a statistically significant contribution of an independent variable to log[(Eβ2M/Ccr)×103] variability.
In all subjects, Eβ2M/Ccr was associated age (β = 0.137), ECd/Ccr (β = 0.283) and diabetes (β = 0.323). In women, the associations of Eβ2M/Ccr with these three independent variables were evident. In men, Eβ2M/Ccr showed a significant association only with diabetes (β = 0.279).
We next examined the association between the ECd/Ccr and Eβ2M/Ccr with scatterplots and the covariate-adjusted mean Eβ2M in subjects grouped by ECd/Ccr tertiles (Figure 2).
The relationship between Eβ2M/Ccr and ECd/Ccr was weak and statistically insignificant in all subjects (Figure 1a), as were in women and men (Figure 2c). However, with adjustment for covariates that included age and BMI, diabetes, hypertension, and smoking (Figure 2b), a significant contribution of Cd body burden to the variability of Eβ2M became was evident when all subjects were included in an analysis (F = 4.473, η2 0.012, p = 0.021). The Eβ2M in subjects of the high ECd/Ccr tertile was higher, compared with those of middle and low ECd/Ccr tertiles (Figure 1b). In subgroup analysis (Figure 1d), a dose-effect relationship of ECd and Eβ2M was seen in women only (F = 3.431, η2 0.021, p = 0.034).
3.4. Effects of Cadmium Exposure on the Prevalenec Odds of Tubulopathy
Table 4 provides the results of the logistic regression analysis of abnormal Eβ2M that incorporated age, BMI, log[(ECd/Ccr)×105], gender, smoking, diabetes, and hypertension as independent variables.
POR, prevalence odds ratio; CI, confidence interval. The units of (Eβ2M/Ccr) × 100 and log[(ECd/Ccr)×105] are µg/L filtrate; Data were generated from logistic regression analyses relating POR for excessive β2M excretion to seven independent variables (first column). For all tests, p-values ≤ 0.05 indicate a statistically significant association of POR with a given independent variable.
Among seven independent variables, the prevalence odds ratios (POR) for (Eβ2M/Ccr) ×100 ≥ 300–999, and ≥ 1000 µg/L filtrate were increased with age, log[(ECd/Ccr)×105], and diabetes. All other 4 independent variables did not show a significant association with abnormal β2M excretion. For every 10-fold rise of ECd/Ccr the POR for (Eβ2M/Ccr) ×100 of ≥ 300 and ≥ 1000 µg/L were increased by 1.94-fold and 3.34-fold, respectively.
3.5. Effects of Cadmium Exposure on eGFR
Similarly, we assessed the effects of Cd exposure on the estimated glomerular filtration rate (eGFR) by multiple linear regression and logistic regression analyses, where [Cd]b and ECd were incorporated as the independent variables together with age, BMI, smoking, diabetes, and hypertension (Table 5).
eGFR, estimated glomerular filtration rate; β, standardized regression coefficient; adjusted R2, coefficient of determination; β indicates strength of association of eGFR with independent variables (first column). Adjusted R2 indicates a fractional variation of eGFR explained by all independent variables. For each test, p-values ≤ 0.05 indicate a statistically significant contribution of an independent variable to eGFR variability.
In all subjects, eGFR was inversely associated with age (β = −0.517), ECd (β = −0.148) and diabetes (β = −0.109). In subgroup analysis, inverse associations of eGFR with these three independent variables (age, ECd and diabetes) were seen only in the women group. In men, eGFR was not associated with ECd, but this parameter showed inverse associations with age (β = −0.506) and hypertension (β = −0.212).
In logistic regression of a reduced eGFR (eGFR ≤60 mL/min/1.73m2), age, BMI, log[(ECd/Ccr) ×105], gender, smoking, diabetes, and hypertension were incorporated as independent variables (Table 6).
The POR values for a reduced eGFR were increased with age, log[(ECd/Ccr)×105], and diabetes. For every 10-fold rise of ECd/Ccr, the POR for a reduced eGFR was increased by 3.2-fold. There was a 4.2-fold increase in the POR for a reduced eGFR among the diabetic.
3.6. Inverse Relationship of β2M Excretion and eGFR
Figure 3 provides scatterplots relating eGFR to Eβ2M among study subjects together with covariates-adjusted means of eGFR in women and men.
A statistically significant inverse relationship between eGFR and Eβ2M was seen in all subjects (Figure 3a), as well as in women and men (Figure 3c). In all subjects (Figure 3b), eGFR explained 5.7% of the variation in Eβ2M/Ccr (F =12.247, p < 0.001).
For simplicity, the degree of tubulopathy, assessed with Eβ2M, was graded into three levels where levels 1, 2 and 3 of tubulopathy corresponded to (Eβ2M/Ccr) ×100 <300, 300–999 and ≥ 1000 µg/L filtrate, respectively.
The covariates-adjusted mean eGFR was 14.0 and 10.5 mL/min/1.73m2 lower in subjects with level 3 tubulopathy, compared to those with tubular dysfunction levels 2 and 1, respectively (Figure 3b).
In subgroup analysis (Figure 3d), the η2 values indicated a nearly twice larger effect size of eGFR on Eβ2M in women (η2 = 0.114), compared to men (η2 = 0.066). In women, those with the tubulopathy of level 3 had the covariates-adjusted mean eGFR 16.5 and 12.0 mL/min/1.73 m2 lower, compared to those with tubulopathy levels 1 and 2, respectively. In men, those with tubulopathy of level 3, had the covariates-adjusted mean eGFR 12.3 mL/min/1.73 m2 lower, compared to those of tubulopathy level 1. The adjusted mean eGFR values in men of tubulopathy levels 3 and 2 did not differ statistically.
In another logistic regression, a relative contribution of Cd exposure and tubular dysfunction levels to the prevalence of a reduced eGFR was determined. ECd was entered as a continuous variable, while Eβ2M was categorized into levels 1, 2 and 3, as previously stated. Table 7 provides results of such analysis.
The POR values for a reduced eGFR rose with age (POR = 1.14), ECd/Ccr (POR = 2.25), tubulopathy level 2 (POR = 8.31), and tubulopathy level 3 (POR = 33.7). All other independent variables, such as diabetes and hypertension, did not show a significant association with the POR for reduced eGFR.
An equivalent logistic regression was conducted using Ecr-normalized ECd and Eβ2M data (Table 8).
The POR values for a reduced eGFR increased with age (POR = 1.10), and the levels of tubular dysfunction; Eβ2M/Ecr 300–999 µg/g creatinine (POR = 3.20) and Eβ2M/Ecr ≥100 µg/g creatinine (POR = 19.0). Associations of POR for a reduced eGFR with ECd/Ecr and all other variables were statistically insignificant.
4. Discussion
This study used a cross-sectional analysis of kidney dysfunction, tubular proteinuria and eGFR decline, to determine the differential impact of Cd exposure in men and women. Whereas many previous studies focused primarily on Cd-induced tubulopathy in women, we investigated these health outcomes in both men and women along with confounding risk factors, smoking, diabetes and hypertension. The excretion rate of Cd and β2M (ECd and Eβ2M) were normalized to the surrogate measure of GFR, creatinine clearance (Ccr). This Ccr-normalization of ECd and Eβ2M, as ECd/Ccr and Eβ2M/Ccr, depict excretion rates per functional nephron, thereby it corrects for differences in the number of functioning nephrons among study subjects [7]. This Ccr-normalized excretion rate also corrects for urine dilution, but it is unaffected by creatinine excretion (Ecr). Thus, ECd/Ccr and Eβ2M/Ccr provide an accurate quantification of the kidney burden of Cd and its toxicity to kidney tubular cells.
We selected subjects from two population-based studies, undertaken in an area with endemic Cd contamination in Mae Sot district, Tak province [8] and a control, non-contamination area in Nakhon-Si-Thammarat province of Thailand [9,10]. The Cd content of the paddy soil samples from the Mae Sot district exceeded the standard of 0.15 mg/kg, and rice samples collected from households contained 4 times the amount of the permissible Cd level of 0.1 mg/kg [16].
4.1. Exposure Levels of Cadmium in Women versus Men
Men and women in this cohort carry the same body burden of Cd, evident from a nearly identical mean (ECd/Ccr) ×100 values of 3.12 vs 3.21 µg/L filtrate. The sources of Cd could be differentiated through an analysis of blood-urine Cd relationships.
[Cd]b and ECd/Ccr correlated strongly with each other in women (R2 =0.624) and men (R2 = 0.661) (Figure 1a), and the covariate-adjusted means [Cd]b showed a stepwise increase through ECd/Ccr tertiles in both genders. Of note, ECd/Ccr explained a larger fraction of the variation in [Cd]b in men than it did in women (η2 0.407 vs. 0.105) (Figure 1b). The variability in [Cd]b was associated mostly with ECd/Ccr in both genders while smoking explained a larger fraction of the [Cd]b variability among men than among women (5.5% vs 2.8%). This result was expected, given the high % of smokers in the men group (68.4% vs. 18.6%) and the higher mean [Cd]b in men than that of women (3.25 vs. 4.36 µg/L) In men only, [Cd]b variation was associated with diabetes.
4.2. The Toxic Manifestation of Cadmium Exposure in Women versus Men
An independent health survey reported that the prevalence of chronic kidney disease (CKD), defined as the eGFR ≤ 60 mL/min/1.73 m2, among Mae Sot residents was 16.1%, while the prevalence of tubulopathy, referred to as tubular proteinuria was 36.1% [17]. This reported tubular proteinuria was based on the cut-off value of Eβ2M/Ecr at 300 µg/g creatinine [6], which equates Eβ2M/Ccr of 2–3 µg/ L filtrate or (Eβ2M/Ccr) ×100 of 200–300 µg/ L filtrate. Notably, the cut-off value for Eβ2M/Ecr at 300 µg/g creatinine was used as the critical effect of exposure to Cd in the human diet [6].
In this cohort, tubular proteinuria affected more than half of women (61.1%) and men (52.6%). One of four women had severe tubular impairment [(Eβ2M/Ccr) ×100 ≥ 1000 µg/L filtrate], whereas one of five men had this abnormality.
In women, Eβ2M/Ccr showed a moderate positive association with age (β = 0.131), and an equally strong association with ECd/Ccr (β = 0.306) and diabetes (β = 0.349) (Table 3). In men, Eβ2M/Ccr did not show a significant association with age or ECd/Ccr, but this tubular defect was associated with diabetes only (β = 0.279). In covariance analysis, the contribution of ECd/Ccr to the variability of Eβ2M/Ccr in women was demonstrable together with a dose-effect relationship after adjustment of covariates and interactions (Figure 2d). In contrast, the contribution of ECd/Ccr to the variation of Eβ2M/Ccr in men was statistically insignificant (Figure 2d). An association of the marker of tubular dysfunction (EβM) and diabetes seen in both men and women is in line with the current knowledge that diabetes adversely affects both glomerular (GFR) and tubular function, termed diabetic tubulopathy [18,19].
The overall mean eGFR was 90 mL/min/1.73 m2 and the overall prevalence of a reduced in eGFR in this cohort was 6.9% (Table 1). The difference in the % of a reduced eGFR in women and men (8.1% vs. 3.5%) did not reach a statistical significance level (p = 0.097) nor did the difference in mean eGFR in women and men (p = 0.145). The weaker effect of Cd exposure on eGFR in men, compared to women, remains to be confirmed with sufficiently large sample group of men. However, the regression analysis also indicated gender differences in susceptibility to the nephrotoxicity of Cd (Table 5). In women, the eGFR was inversely associated with age (β = −0.511), ECd/Ccr (β =−0.185) and diabetes (β = −0.128). In comparison, the eGFR in men was not associated with ECd/Ccr, while showing an inverse association with age (β = −0.506) and hypertension (β = −0.212). Adverse effects of hypertension and diabetes on the eGFR have been noted in a cross-sectional study of the U.S. general population, where Cd-induced GFR reduction was more pronounced in those who had diabetes and/or hypertension [20].
We speculate that gender differences in levels of some protective factors, notably body status of nutritionally essential metals such as iron and zinc may contribute to the increased susceptibility to Cd nephrotoxicity seen in women. Similarly, environmental Cd exposure has been linked to a reduction eGFR among participants in various cycles of the U.S. National Health and Nutrition Examination Survey (NHANES) undertaken over 18 years (1999 to 2016) [20,21,22]. Lin et al. (2014) reported that the risk for a reduced eGFR was higher in those with lower serum zinc (OR 3.38), compared to those with similar Cd exposure levels and serum zinc > 74 μg/dL (OR 2.04) [22].
4.3. Increment of β2M Excretion as GFR Falls
The protein β2M with the molecular weight of 11,800 Da is filtered freely by the glomeruli, and is reabsorbed almost completely by the kidney’s tubular epithelial cells [13]. Thus, defective tubular re-absorption of β2M will result in an enhanced excretion rate of β2M [23,24,25,26]. Loss of nephrons also raises the excretion β2M for the following reasons [23,26]. When the reabsorption rate of β2M per nephron remains constant, its excretion will vary directly with its production. If the production and reabsorption per nephron remain constant as nephrons are lost, the excretion of β2M will rise [27].
It can thus be expected that the excretion of β2M will increase, when GFR falls for any causes. Indeed, Eβ2M/Ccr was inversely associated with eGFR in both women and men (Figure 3c) although the causes of their eGFR decreases seemed to be different. In a quantitative analysis (Figure 3d), the η2 value describing the effect size of Eβ2M/Ccr on eGFR variability among women was 1.7-fold larger (0.114 vs. 0.066). In both women and men, eGFR was lowest in those who had (Eβ2M/Ccr) ×100 ≥1000 µg/L filtrate, indicative of severely impaired tubular function.
Of note, the POR for a reduced eGFR was increased by 8.3-fold and 33.7-fold those with (Eβ2M/Ccr) ×100 of 300–999, and ≥1000 µg/L filtrate, respectively (Table 7), compared to those with Eβ2M/Ccr) ×100 <300 µg/L filtrate. A substantial loss of functioning nephrons was a likely cause of massive increases in Eβ2M/Ccr seen in those who had eGFR below 60 mL/min/1.73 m2.
4.4. The Pitfall of Adjusting Excretion Rate to Ecr and Implication for Health Risk Estimation
The Ccr-normalized data indicate that women and men shared the same burden of Cd (Table 1). The data indicate also that the % of women and men across three categories of tubulopathy were all statistically different, thereby linking Cd exposure to the severity of tubulopathy in both genders. The logistic regression data (Table 7) show that the likelihood of having a reduced eGFR was increased by 8.3-fold and 33.7-fold in those who had (Eβ2M/Ccr) ×100 of 300–999 and ≥1000 µg/L filtrate, compared to those with (Eβ2M/Ccr) ×100 <300 µg/L filtrate.
The Ecr-normalized data indicated that the mean ECd/Ecr in women was statistically higher than that of men (4.26 vs. 3.30 µg/g creatinine). They also indicated that the difference in % of women across the three tubulopathy categories was minuscule, and that the % distribution of men across tubulopathy categories was statistically significant. These data suggest an association of Cd exposure and the severity of tubulopathy in men only. The logistic regression data (Table 8) show that the likelihood of having a reduced eGFR was increased by 3.2-fold and 19-fold in those who had Eβ2M/Ecr of 300–999 and ≥1000 µg/g creatinine, compared to those with Eβ2M/Ecr < Eβ2M/Ecr.
Previously, Eβ2M/Ecr of 100–299, 300–999, and ≥1000 μg/g creatinine were found to be associated with 4.7-, 6.2- and 10.5-fold increases in the prevalence odds of a reduced eGFR [28]. Similarly, a rise in Eβ2M/Ecr to levels not higher than 100 μg/g creatinine was associated with an increased risk of hypertension in the Japanese general population [29], while a prospective cohort data showed that Eβ2M/Ecr was associated with a 79% increase in the likelihood of having a large decline in eGFR (10 mL/min/1.73 m2) over a five-year period [30]. Thus, a cut-off value for Eβ2M/Ecr above 300 μg/g creatinine does not reflect an early warning sign of the nephrotoxicity of Cd. The utility of this Eβ2M/Ecr value as a toxicity criterion to derive a toxicity threshold level for Cd is inappropriate.
In summary, adjusting ECd and Eβ2M to Ecr produces an erroneous interpretation of the effect of Cd exposure on the eGFR, while underestimating the severity of Cd-induced tubulopathy. These data calls into question the utility of Eβ2M/Ecr of 300 µg/g creatinine to represent the critical effect of exposure to Cd in the human diet. New health guidance values need to be established for this toxic metal as well as public measures to minimize the Cd contamination of food chains.
5. Conclusions
Excretion of β2M above 300 µg/g creatinine (≈ 2–3 µg/L filtrate) and reduced glomerular function, indicated by eGFR below 60 mL/min/1.73 m2 are the manifestations of severe kidney toxicities of chronic exposure to Cd that are more prevalent and more severe in women than men of the same body burden.
Author Contributions
Conceptualization, S.S.; methodology, S.S. and S.Y.; formal analysis, S.S.; investigation, S.Y., P.P. and T.K.; resources, G.C.G. and D.A.V.; writing—original draft preparation, S.S.; writing—review and editing, G.C.G. and D.A.V.; project administration, S.S. and S.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Informed Consent Statement
Informed consent was obtained from all participants in the study prior to their participation.
Data Availability Statement
All data are contained within this article.
Acknowledgments
This work was supported with resources from the Centre for Kidney Disease Research, Translational Research Institute, and the Department of Kidney and Transplant Services, Princess Alexandra Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Satarug, S.; Baker, J.R.; Reilly, P.E.; Moore, M.R.; Williams, D.J. Cadmium levels in the lung, liver, kidney cortex, and urine samples from Australians without occupational exposure to metals. Arch. Environ. Health 2002, 57, 69–77. [Google Scholar] [CrossRef]
- Barregard, L.; Fabricius-Lagging, E.; Lundh, T.; Mölne, J.; Wallin, M.; Olausson, M.; Modigh, C.; Sallsten, G. Cadmium, mercury, and lead in kidney cortex of living kidney donors: Impact of different exposure sources. Environ. Res. 2010, 110, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Barregard, L.; Sallsten, G.; Lundh, T.; Mölne, J. Low-level exposure to lead, cadmium and mercury, and histopathological findings in kidney biopsies. Environ. Res. 2022, 211, 113119. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Kataoka, Y.; Hayashi, K.; Matsuda, R.; Uneyama, C. Dietary exposure of the Japanese general population to elements: Total diet study 2013–2018. Food Saf. 2022, 10, 83–101. [Google Scholar] [CrossRef]
- JECFA. In Proceedings of the Joint FAO/WHO Expert Committee on Food Additives and Contaminants, Seventy-Third Meeting, Geneva, Switzerland, 8–17 June 2010. In Summary and Conclusions; JECFA/73/SC.; Food and Agriculture Organization of the United Nations/World Health Organization: Geneva, Switzerland, 2011. Available online: https://apps.who.int/iris/handle/10665/44521 (accessed on 25 June 2023).
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling cadmium exposures in low- and high-exposure areas in Thailand. Environ. Health Perspect. 2013, 121, 531–536. [Google Scholar] [CrossRef]
- Yimthiang, S.; Pouyfung, P.; Khamphaya, T.; Kuraeiad, S.; Wongrith, P.; Vesey, D.A.; Gobe, G.C.; Satarug, S. Effects of environmental exposure to cadmium and lead on the risks of diabetes and kidney dysfunction. Int. J. Environ. Res. Public Health 2022, 19, 2259. [Google Scholar] [CrossRef]
- Zarcinas, B.A.; Pongsakul, P.; McLaughlin, M.J.; Cozens, G. Heavy metals in soils and crops in Southeast Asia. 2. Thailand. Environ. Geochem. Health 2004, 26, 359–371. [Google Scholar] [CrossRef]
- Bloch, M.J.; Basile, J.N. Review of recent literature in hypertension: Updated clinical practice guidelines for chronic kidney disease now include albuminuria in the classification system. J. Clin. Hypertens (Greenwich) 2013, 15, 865–867. [Google Scholar] [CrossRef]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
- Murton, M.; Goff-Leggett, D.; Bobrowska, A.; Garcia Sanchez, J.J.; James, G.; Wittbrodt, E.; Nolan, S.; Sörstadius, E.; Pe-coits-Filho, R.; Tuttle, K. Burden of chronic kidney disease by KDIGO categories of glomerular filtration rate and albuminuria: A Systematic review. Adv. Ther. 2021, 38, 180–200. [Google Scholar] [CrossRef] [PubMed]
- Soveri, I.; Berg, U.B.; Björk, J.; Elinder, C.G.; Grubb, A.; Mejare, I.; Sterner, G.; Bäck, S.E.; SBU GFR Review Group. Measuring GFR: A systematic review. Am. J. Kidney Dis. 2014, 64, 411–424. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Suwatvitayakorn, P.; Ko, M.S.; Kim, K.W.; Chanpiwat, P. Human health risk assessment of cadmium exposure through rice consumption in cadmium-contaminated areas of the Mae Tao sub-district, Tak, Thailand. Environ. Geochem. Health 2020, 42, 2331–2344. [Google Scholar] [CrossRef]
- Swaddiwudhipong, W.; Nguntra, P.; Kaewnate, Y.; Mahasakpan, P.; Limpatanachote, P.; Aunjai, T.; Jeekeeree, W.; Punta, B.; Funkhiew, T.; Phopueng, I. Human health effects from cadmium exposure: Comparison between persons living in cadmium-contaminated and non-contaminated areas in northwestern Thailand. Southeast Asian, J. Trop. Med. Publ. Health 2015, 46, 133–142. [Google Scholar]
- Zhou, X. ; Xu. C.; Dong, J.; Liao, L. Role of renal tubular programed cell death in diabetic kidney disease. Diabetes Metab. Res. Rev. 2023, 39, e3596. [Google Scholar]
- Yao, L.; Liang, X.; Qiao, Y.; Chen, B.; Wang, P.; Liu, Z. Mitochondrial dysfunction in diabetic tubulopathy. Metabolism 2022, 131, 155195. [Google Scholar] [CrossRef]
- Madrigal, J.M.; Ricardo, A.C.; Persky, V.; Turyk, M. Associations between blood cadmium concentration and kidney function in the U.S. population: Impact of sex, diabetes and hypertension. Environ. Res. 2018, 169, 180–188. [Google Scholar] [CrossRef]
- Navas-Acien, A.; Tellez-Plaza, M.; Guallar, E.; Muntner, P.; Silbergeld, E.; Jaar, B.; Weaver, V. Blood cadmium and lead and chronic kidney disease in US adults: A joint analysis. Am. J. Epidemiol. 2009, 170, 1156–1164. [Google Scholar] [CrossRef]
- Ferraro, P.M.; Costanzi, S.; Naticchia, A.; Sturniolo, A.; Gambaro, G. Low level exposure to cadmium increases the risk of chronic kidney disease: Analysis of the NHANES 1999–2006. BMC Public Health 2010, 10, 304. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.S.; Ho, W.C.; Caffrey, J.L.; Sonawane, B. Low serum zinc is associated with elevated risk of cadmium nephrotoxicity. Environ. Res. 2014, 134, 33–38. [Google Scholar] [CrossRef]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.H.; Roumelioti, M.E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering beta-2 microglobulin as a biomarker across the spectrum of kidney diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef] [PubMed]
- Portman, R.J.; Kissane, J.M.; Robson, A.M. Use of B2-microglobulin to diagnose tubulo-interstitial renal lesions in children. Kidney Int. 1986, 30, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Gauthier, C.; Nguyen-Simonnet, H.; Vincent, C.; Revillard, J.-P.; Pellet, M.V. Renal tubular absorption of beta 2 microglobulin. Kidney Int. 1984, 26, 170–175. [Google Scholar] [CrossRef]
- Peterson, P.A.; Evrin, P.-E.; Berggard, I. Differentiation of glomerular, tubular, and normal proteinuria: Determination of urinary excretion of B2-microglobulin, albumin, and total protein. J. Clin. Investig. 1969, 48, 1189–1198. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Đorđević, A.B. The validity of benchmark dose limit analysis for estimating permissible accumulation of cadmium. Int. J. Environ. Res. Public Health 2022, 19, 15697. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Nishijo, M.; Ruangyuttikarn, W.; Gobe, G.C. The inverse association of glomerular function and urinary β2-MG excretion and its implications for cadmium health risk assessment. Environ. Res. 2019, 173, 40–47. [Google Scholar] [CrossRef]
- Mashima, Y.; Konta, T.; Kudo, K.; Takasaki, S.; Ichikawa, K.; Suzuki, K.; Shibata, Y.; Watanabe, T.; Kato, T.; Kawata, S.; et al. Increases in urinary albumin and beta2-microglobulin are independently associated with blood pressure in the Japanese general population: The Takahata Study. Hypertens. Res. 2011, 34, 831–835. [Google Scholar] [CrossRef]
- Kudo, K.; Konta, T.; Mashima, Y.; Ichikawa, K.; Takasaki, S.; Ikeda, A.; Hoshikawa, M.; Suzuki, K.; Shibata, Y.; Watanabe, T.; et al. The association between renal tubular damage and rapid renal deterioration in the Japanese population: The Takahata study. Clin. Exp. Nephrol. 2011, 15, 235–241. [Google Scholar] [CrossRef]
Figure 1.
Blood cadmium and urinary cadmium excretion relationship. Scatterplots relate log([Cd]b × 103] to log[(ECd/Ccr) × 105] in women and men (a). Coefficients of determination (R2) and p-values are provided for all scatterplots. Bar graph (b) depicts means log([Cd]b × 103] values in women and men across ECd/Ccr tertiles. All means were obtained by univariate analysis with adjustment for covariates and interactions. For women, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles 1, 2 and 3 are 0.37 (0.47), 2.34 (0.52) and 6.84 (4.46) µg/L of filtrate. For men, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles quartiles 1, 2 and 3 are 0.36 (0.42), 2.14 (0.63) and 6.81 (3.78) µg/L of filtrate. For all tests, p-values ≤ 0.05 indicate statistically significant differences.
Figure 1.
Blood cadmium and urinary cadmium excretion relationship. Scatterplots relate log([Cd]b × 103] to log[(ECd/Ccr) × 105] in women and men (a). Coefficients of determination (R2) and p-values are provided for all scatterplots. Bar graph (b) depicts means log([Cd]b × 103] values in women and men across ECd/Ccr tertiles. All means were obtained by univariate analysis with adjustment for covariates and interactions. For women, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles 1, 2 and 3 are 0.37 (0.47), 2.34 (0.52) and 6.84 (4.46) µg/L of filtrate. For men, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles quartiles 1, 2 and 3 are 0.36 (0.42), 2.14 (0.63) and 6.81 (3.78) µg/L of filtrate. For all tests, p-values ≤ 0.05 indicate statistically significant differences.
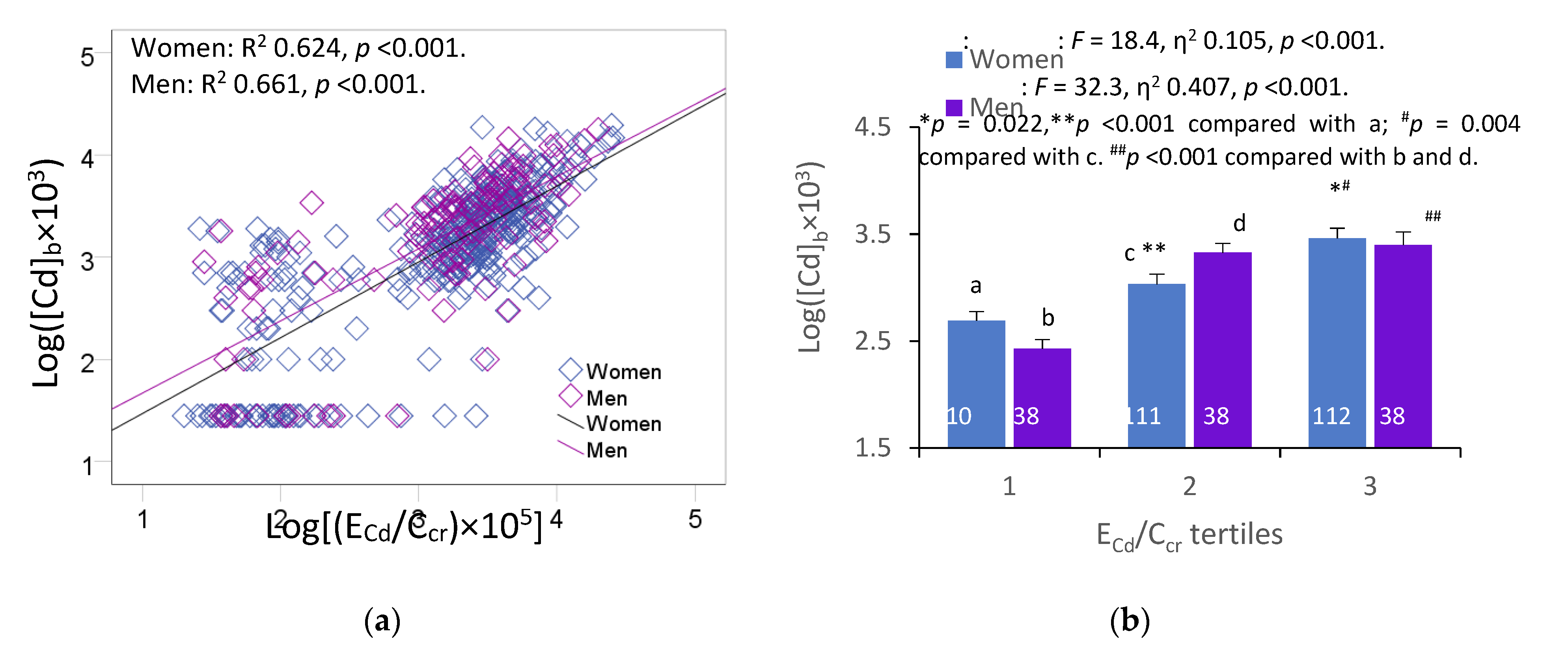
Figure 2.
Dose-effect relationship of β2-microgloubulin and cadmium excretion. Scatterplots relate log[(EβM/Ccr) × 103] to log[(ECd/Ccr) × 105] in all subjects (a), and women and men (c). Coefficients of determination (R2) and p-values are provided for all scatterplots. The color-coded area graph (b) depicts means of log[(Eβ2M/Ccr)×103] across ECd/Ccr tertiles. Shaded areas indicate variability of means. Bar graph (d) depicts mean log[(Eβ2M/Ccr) × 103] in women and men in each ECd/Ccr tertile. The respective numbers of subjects in ECd/Ccr tertiles 1, 2 and 3 are 149, 149 and 150. All means were obtained by univariate analysis with adjustment for covariates and interaction. For women, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles 1, 2 and 3 are 0.37 (0.47), 2.34 (0.52) and 6.84 (4.46) µg/L of filtrate. For men, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles quartiles 1, 2 and 3 are 0.36 (0.42), 2.14 (0.63) and 6.81 (3.78) µg/L of filtrate. For all tests, p-values ≤ 0.05 indicate statistically significant differences.
Figure 2.
Dose-effect relationship of β2-microgloubulin and cadmium excretion. Scatterplots relate log[(EβM/Ccr) × 103] to log[(ECd/Ccr) × 105] in all subjects (a), and women and men (c). Coefficients of determination (R2) and p-values are provided for all scatterplots. The color-coded area graph (b) depicts means of log[(Eβ2M/Ccr)×103] across ECd/Ccr tertiles. Shaded areas indicate variability of means. Bar graph (d) depicts mean log[(Eβ2M/Ccr) × 103] in women and men in each ECd/Ccr tertile. The respective numbers of subjects in ECd/Ccr tertiles 1, 2 and 3 are 149, 149 and 150. All means were obtained by univariate analysis with adjustment for covariates and interaction. For women, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles 1, 2 and 3 are 0.37 (0.47), 2.34 (0.52) and 6.84 (4.46) µg/L of filtrate. For men, respective arithmetic means and standard deviations (SD) for (ECd/Ccr)×100 tertiles quartiles 1, 2 and 3 are 0.36 (0.42), 2.14 (0.63) and 6.81 (3.78) µg/L of filtrate. For all tests, p-values ≤ 0.05 indicate statistically significant differences.
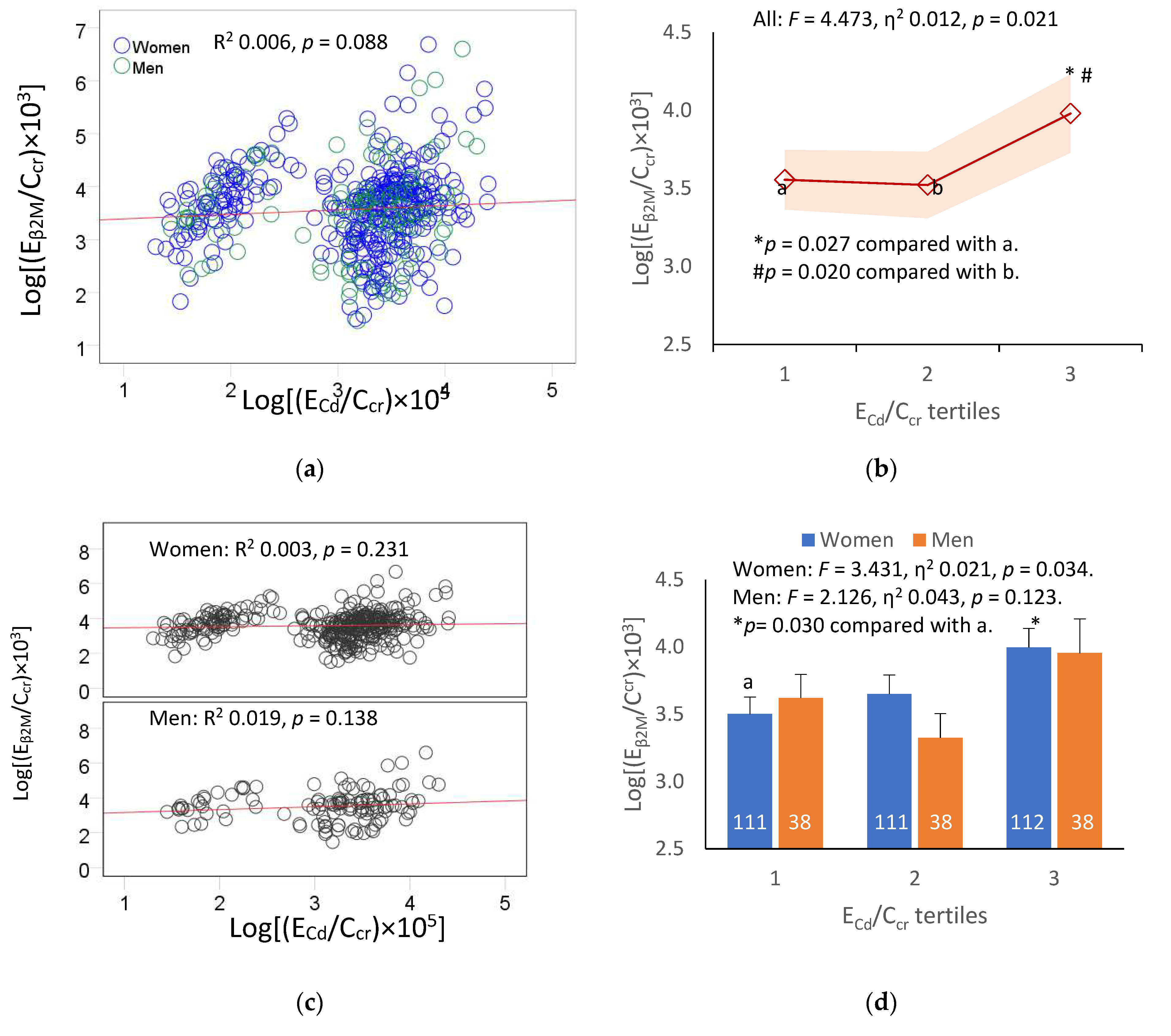
Figure 3.
An inverse relationship of eGFR with β2-microgloubulin excretion. Scatterplots relate eGFR to log[(EβM/Ccr) × 103] in all subjects (a), and women and men (c). Coefficients of determination (R2) and p-values are provided for all scatterplots. The color-coded area graph (b) depicts means of eGFR across three Eβ2M/Ccr ranges. Shaded areas indicate variability of means. Bar graph (d) depicts means of eGFR in women and men in each Eβ2M/Ccr range. The respective numbers of subjects in (Eβ2M/Ccr)×100 <300, 300−999 and ≥1000 µg/L of filtrate are 184, 156 and 109. All means were obtained by univariate analysis with adjustment for covariates and interaction. For all tests, p-values ≤ 0.05 indicate statistically significant differences.
Figure 3.
An inverse relationship of eGFR with β2-microgloubulin excretion. Scatterplots relate eGFR to log[(EβM/Ccr) × 103] in all subjects (a), and women and men (c). Coefficients of determination (R2) and p-values are provided for all scatterplots. The color-coded area graph (b) depicts means of eGFR across three Eβ2M/Ccr ranges. Shaded areas indicate variability of means. Bar graph (d) depicts means of eGFR in women and men in each Eβ2M/Ccr range. The respective numbers of subjects in (Eβ2M/Ccr)×100 <300, 300−999 and ≥1000 µg/L of filtrate are 184, 156 and 109. All means were obtained by univariate analysis with adjustment for covariates and interaction. For all tests, p-values ≤ 0.05 indicate statistically significant differences.
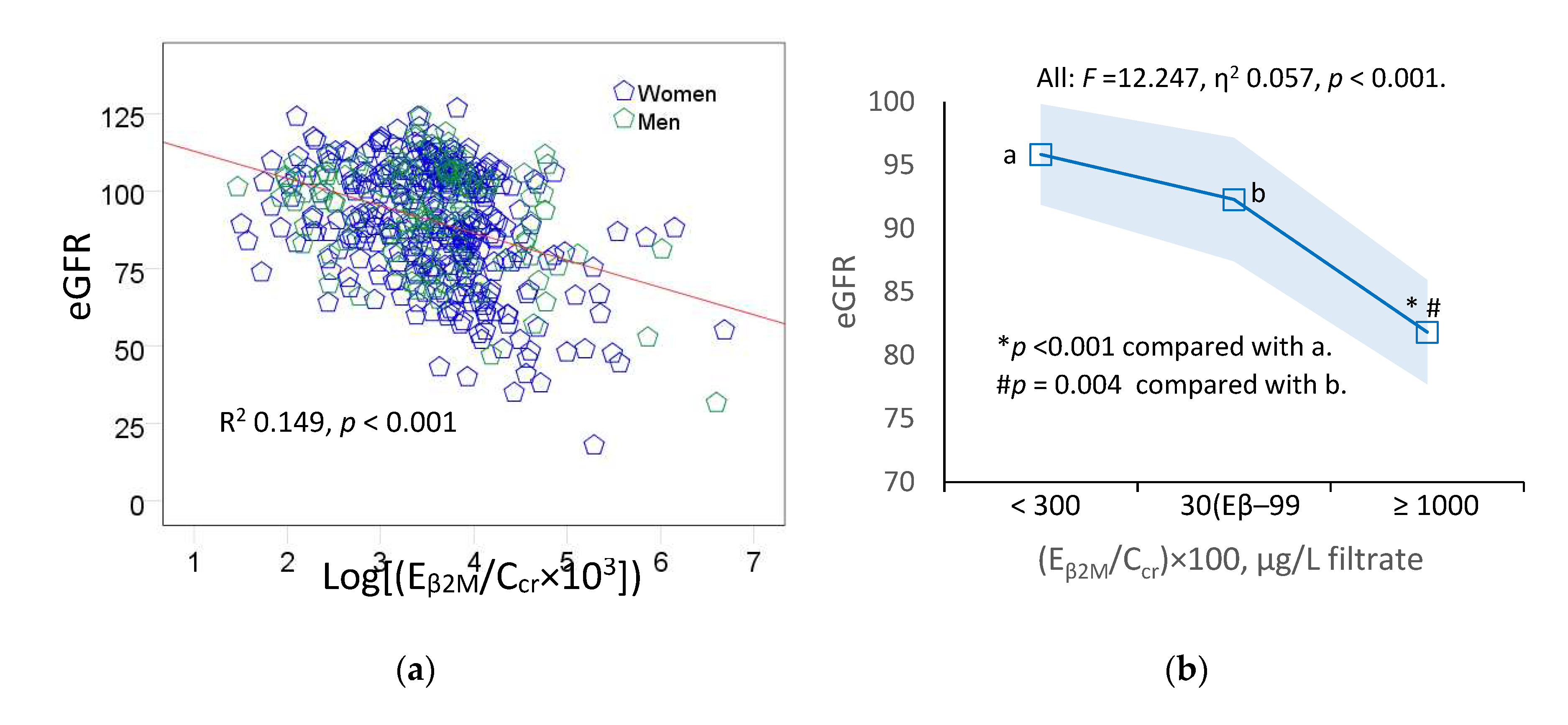
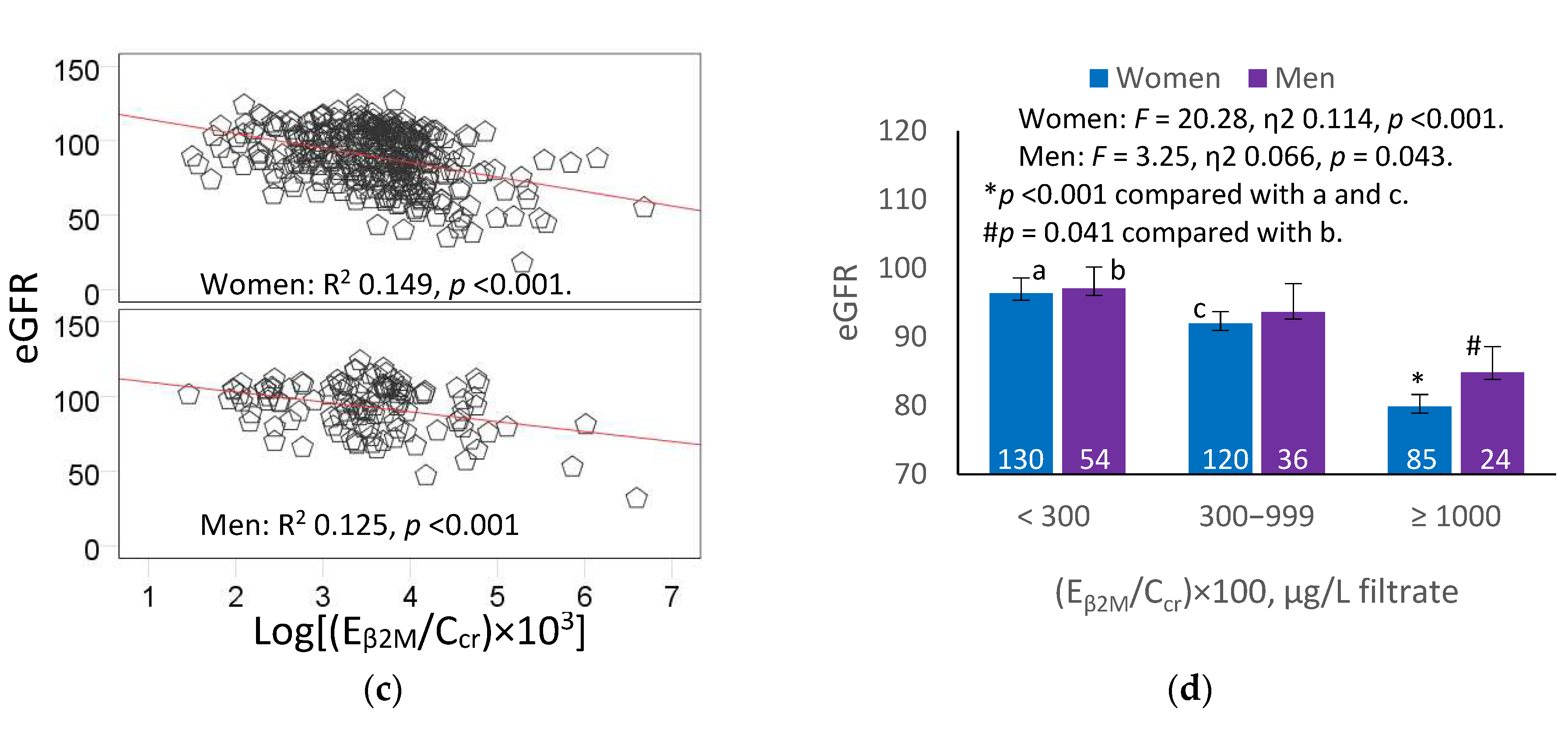

Table 1.
Characteristics of Study Subjects.
| Parameters | All Subjects, n = 448 | Women, n = 334 | Men, n = 114 | p |
|---|---|---|---|---|
| Age, years | 51.1 ± 8.6 | 51.5 ± 9.0 | 49.9 ± 7.2 | 0.344 |
| BMI, kg/m2 | 24.8 ± 4.0 | 25.2 ± 4.0 | 23.7 ± 3.6 | <0.001 |
| Smoking, % | 31.3 | 18.6 | 68.4 | <0.001 |
| Hypertension, % | 48.7 | 50.6 | 43.0 | 0.160 |
| Diabetes, % | 15.4 | 16.2 | 0.442 | 0.442 |
| eGFR a, mL/min/1.73 m2 | 90 ± 18 | 89 ± 19 | 93 ± 16 | 0.145 |
| Reduced eGFR b, % | 6.9 | 8.1 | 3.5 | 0.097 |
| Plasma creatinine, mg/dL | 0.82 ± 0.22 | 0.78 ± 0.21 | 0.95 ± 0.21 | <0.001 |
| Urine creatinine, mg/dL | 114 ± 74 | 108 ± 74 | 132 ± 72 | <0.001 |
| Blood Cd, µg/L | 2.75 ± 3.19 | 2.58 ± 3.10 | 3.25 ± 3.41 | 0.038 |
| Urine Cd, µg/L | 4.22 ± 5.67 | 4.36 ± 6.14 | 3.82 ± 4.01 | 0.875 |
| Urine β2M, µg/L | 3122 ± 18836 | 2596 ± 17238 | 4665 ± 22903 | 0.544 |
| Normalized to Ccr (Ex/Ccr) c | ||||
| (ECd/Ccr) ×100, µg/L filtrate | 3.19 ± 3.72 | 3.21 ± 3.79 | 3.12 ± 3.55 | 0.639 |
| (Eβ2M/Ccr) ×100, µg/L filtrate | 3839 ± 30422 | 3078 ± 26986 | 6072 ± 38837 | 0.212 |
| (Eβ2M/Ccr) ×100, µg/L filtrate, % | ||||
| < 300 | 41.1 | 38.9 | 47.4 | |
| 300−999 | 34.8 | 35.9 | 31.6 | |
| ≥ 1000 | 24.1 | 25.1 # | 21.1 ** | |
| Normalized to Ecr (Ex/Ecr) d | ||||
| ECd/Ecr, µg/g creatinine | 4.02 ± 4.41 | 4.26 ± 4.62 | 3.30 ± 3.68 | 0.028 |
| Eβ2M/Ecr, µg/g creatinine | 3220 ± 21847 | 3005 ± 22812 | 3850 ± 18815 | 0.017 |
| Eβ2M/Ecr, µg/g creatinine, % | ||||
| < 300 | 35.5 | 32.3 | 45.6 | |
| 300−999 | 34.6 | 34.7 | 34.2 | |
| ≥ 1000 | 29.7 | 32.9 | 20.2 * |
Table 2.
Determinants of blood cadmium concentration with cadmium excretion and other variables.
| Independent Variables/Factors |
Log([Cd]b ×103), µg/L | ||||||
|---|---|---|---|---|---|---|---|
| Women, n = 334 | Men, n = 114 | ||||||
| β | η2 | p | p | η2 | p | ||
| Age, years | −0.170 | 0.057 | <0.001 | −0.004 | 1×10−6 | 0.946 | |
| BMI, kg/m2 | −0.019 | 0.001 | 0.586 | −0.079 | 0.022 | 0.180 | |
| Log[(ECd/Ccr)×105], µg/L filtrate | 0.619 | 0.367 | <0.001 | 0.581 | 0.420 | <0.001 | |
| Smoking | 0.123 | 0.028 | 0.001 | 0.184 | 0.055 | 0.002 | |
| Diabetes | -0.053 | 0.010 | 0.182 | −0.246 | 0.095 | <0.001 | |
| Hypertension | 0.048 | 0.007 | 0.162 | −0.061 | 0.004 | 0.287 | |
| DM× HTN | n/a | 0.016 | 0.023 | n/a | n/a | n/a | |
| SMK × DM × HTN | n/a | n/a | n/a | n/a | 0.042 | 0.036 | |
| Adjusted R2 | 0.624 | n/a | <0.001 | 0.661 | n/a | <0.001 | |
Table 3.
Associations of β2-mcirogloubulin excretion with cadmium exposure measures.
| Independent Variables/Factors |
Log[(Eβ2M/Ccr) ×103], µg/ L filtrate | |||||||
|---|---|---|---|---|---|---|---|---|
| All subjects | Women | Men | ||||||
| β | p | β | p | β | p | |||
| Age, years | 0.137 | 0.013 | 0.131 | 0.041 | 0.128 | 0.238 | ||
| BMI, kg/m2 | −0.089 | 0.065 | −0.102 | 0.062 | −0.043 | 0.664 | ||
| Log([Cd]b×103), µg/L filtrate | −0.016 | 0.824 | −0.083 | 0.328 | 0.217 | 0.180 | ||
| Log[(ECd/Ccr)×105], µg/L filtrate | 0.283 | <0.001 | 0.306 | <0.001 | 0.175 | 0.247 | ||
| Gender (male) | 0.052 | 0.318 | − | − | − | − | ||
| Smoking | 0.063 | 0.255 | 0.093 | 0.094 | −0.065 | 0.526 | ||
| Diabetes | 0.323 | <0.001 | 0.349 | <0.001 | 0.279 | 0.017 | ||
| Hypertension | 0.015 | 0.745 | −0.023 | 0.660 | 0.142 | 0.139 | ||
| Adjusted R2 | 0.105 | <0.001 | 0.125 | <0.001 | 0.059 | 0.060 | ||
Table 4.
Prevalence odds for excessive excretion of β2M in relation to cadmium excretion and other variables.
Table 4.
Prevalence odds for excessive excretion of β2M in relation to cadmium excretion and other variables.
| Independent variables/factors | Number of Subjects | (Eβ2M/Ccr) ×100 ≥ 300 µg/L | (Eβ2M/Ccr) × 100 ≥ 1000 µg/L | ||
|---|---|---|---|---|---|
| POR (95% CI) | p | POR (95% CI) | p | ||
| Age, years | 448 | 1.036 (1.007, 1.067) | 0.016 | 1.062 (1.027, 1.098) | <0.001 |
| BMI, kg/m2 | 448 | 0.971 (0.919, 1.025) | 0.284 | 0.958 (0.896, 1.023) | 0.203 |
| Log[(ECd/Ccr)×105], µg/L filtrate | 448 | 1.940 (1.344, 2.802) | <0.001 | 3.343 (2.036, 5.488) | <0.001 |
| Gender (male) | 114 | 1.406 (0.835, 2.367) | 0.200 | 1.299 (0.687, 2.458) | 0.421 |
| Smoking | 140 | 1.067 (0.645, 1.765) | 0.801 | 1.388 (0.763, 2.522) | 0.282 |
| Diabetes | 69 | 5.294 (2.526, 11.09) | <0.001 | 11.52 (5.004, 26.50) | <0.001 |
| Hypertension | 218 | 1.066 (0.714, 1.592) | 0.753 | 1.535 (0.942, 2.501) | 0.085 |
Table 5.
Associations of eGFR with cadmium exposure measures and other variables.
| Independent. Variables/Factors |
eGFR, mL/min/1.73m2 | |||||||
|---|---|---|---|---|---|---|---|---|
| All subjects | Women | Men | ||||||
| β | p | β | p | β | p | |||
| Age, years | −0.517 | <0.001 | −0.511 | <0.001 | −0.506 | <0.001 | ||
| BMI, kg/m2 | −0.064 | 0.136 | −0.048 | 0.327 | −0.149 | 0.095 | ||
| Log([Cd]b×103), µg/L filtrate | 0.053 | 0.420 | 0.102 | 0.182 | −0.153 | 0.291 | ||
| Log[(ECd/Ccr)×105], µg/L filtrate | −0.148 | 0.026 | −0.185 | 0.018 | 0.011 | 0.933 | ||
| Gender (male) | −0.001 | 0.977 | − | − | − | − | ||
| Smoking | 0.025 | 0.610 | 0.018 | 0.717 | 0.071 | 0.438 | ||
| Diabetes | −0.109 | 0.023 | −0.128 | 0.021 | −0.055 | 0.593 | ||
| Hypertension | −0.079 | 0.055 | −0.050 | 0.295 | −0.212 | 0.014 | ||
| Adjusted R2 | 0.279 | <0.001 | 0.281 | <0.001 | 0.249 | <0.001 | ||
Table 6.
Prevalence odds for a reduced eGFR in relation to cadmium excretion and other variables.
| Independent Variables/ Factors |
Reduced eGFR a | ||||
|---|---|---|---|---|---|
| β Coefficients | POR | 95% CI | p | ||
| (SE) | Lower | Upper | |||
| Age, years | 0.136 (0.027) | 1.146 | 1.086 | 1.209 | <0.001 |
| BMI, kg/m2 | 0.020 (0.051) | 1.021 | 0.923 | 1.128 | 0.688 |
| Log[(ECd/Ccr)×105], µg/L filtrate | 1.154 (0.358) | 3.172 | 1.572 | 6.402 | 0.001 |
| Gender (male) | −0.542 (0.649) | 0.582 | 0.163 | 2.075 | 0.404 |
| Smoking | −0.228 (0.583) | 0.796 | 0.254 | 2.493 | 0.695 |
| Diabetes | 1.439 (0.524) | 4.217 | 1.510 | 11.78 | 0.006 |
| Hypertension | 0.115 (0.427) | 1.122 | 0.486 | 2.591 | 0.787 |
a Reduced eGFR is defined as the estimated glomerular filtration rate ≤ 60 mL/min/1.73m2; β, regression coefficient; POR, prevalence odds ratio; S.E., standard error of mean; CI, confidence interval. Data were generated from logistic regression relating POR for a reduced eGFR to seven independent variables (first column). For each test, p-values ≤ 0.05 indicate a statistically significant contribution of individual independent variables to the POR for a reduced eGFR.
Table 7.
Prevalence odds of a reduced eGFR in relation to cadmium and β2M excretion rates normalized to Ccr.
Table 7.
Prevalence odds of a reduced eGFR in relation to cadmium and β2M excretion rates normalized to Ccr.
| Independent Variables/ Factors |
Reduced eGFR a | ||||
|---|---|---|---|---|---|
| Number of subjects | POR | 95% CI | p | ||
| Lower | Upper | ||||
| Age, years | 448 | 1.140 | 1.072 | 1.211 | <0.001 |
| BMI, kg/m2 | 448 | 1.066 | 0.950 | 1.198 | 0.278 |
| Log[(ECd/Ccr) ×105], µg/L filtrate | 448 | 2.251 | 1.043 | 4.858 | 0.039 |
| Gender (male) | 114 | 0.674 | 0.176 | 2.583 | 0.565 |
| Smoking | 140 | 0.885 | 0.270 | 2.899 | 0.840 |
| Diabetes | 69 | 1.216 | 0.394 | 3.753 | 0.734 |
| Hypertension | 218 | 1.199 | 0.487 | 2.957 | 0.693 |
| (Eβ2M/Ccr) ×100, µg/L filtrate | |||||
| < 300 | 184 | Referent | |||
| 300–999 | 156 | 8.310 | 2.655 | 26.01 | <0.001 |
| ≥ 1000 | 108 | 33.731 | 4.193 | 271.3 | 0.001 |
a, Reduced eGFR is defined as the estimated glomerular filtration rate ≤ 60 mL/min/1.73m2; SE, POR, prevalence odds ratio; CI, confidence interval. Data were generated from multivariable logistic regression analyses relating the POR for a reduced eGFR to eight independent variables (first column). p-values < 0.05 indicate a statistically significant increase in the POR for a reduced eGFR.
Table 8.
Prevalence odds of a reduced eGFR in relation to cadmium and β2M excretion rates normalized to Ecr.
Table 8.
Prevalence odds of a reduced eGFR in relation to cadmium and β2M excretion rates normalized to Ecr.
| Independent Variables/ Factors |
Reduced eGFR a | ||||
|---|---|---|---|---|---|
| Number of subjects | POR | 95% CI | p | ||
| Lower | Upper | ||||
| Age, years | 448 | 1.101 | 1.045 | 1.160 | <0.001 |
| BMI, kg/m2 | 448 | 1.032 | 0.929 | 1.147 | 0.555 |
| Log[(ECd/Ecr) ×103], µg/g creatinine | 448 | 1.278 | 0.630 | 2.593 | 0.497 |
| Gender (male) | 114 | 0.671 | 0.181 | 2.484 | 0.550 |
| Smoking | 140 | 0.762 | 0.240 | 2.418 | 0.644 |
| Diabetes | 69 | 1.614 | 0.581 | 4.484 | 0.359 |
| Hypertension | 218 | 1.041 | 0.449 | 2.415 | 0.926 |
| (Eβ2M/Ccr)×100, µg/g creatinine | |||||
| <300 | 160 | ||||
| 300–999 | 155 | 3.204 | 1.226 | 8.375 | 0.018 |
| ≥1000 | 133 | 19.042 | 2.387 | 151.907 | 0.005 |
a, Reduced eGFR is defined as the estimated glomerular filtration rate ≤ 60 mL/min/1.73m2; SE, POR, prevalence odds ratio; CI, confidence interval. Data were generated from multivariable logistic regression analyses relating the POR for a reduced eGFR to eight independent variables (first column). p-values < 0.05 indicate a statistically significant increase in the POR for a reduced eGFR.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



