
Submitted:
28 June 2023
Posted:
29 June 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Data on immunogenicity, immune response persistency, and safety of COVID-19 boosters in patients with comorbidities are limited. Therefore, we aimed to evaluate and compare three different boosters in individuals who received two doses of the BBIBP-CorV vaccine including underlying diseases and healthy cases as control.
One hundred forty subjects including 63 ones with at least one of three underlying diseases (UD) (including obesity, hypertension, and diabetes mellitus) and 77 healthy ones (HC) who had received a booster dose (either PastoCovac Plus or PastoCovac or BBIBP-CorV) were enrolled. The presence of SARS-CoV-2 antibodies was assessed before the booster injection and 28, 60, 90, and 180 days after it. Moreover, the adverse events (AEs) were recorded on days 7 and 21 post-booster shot for evaluating safety outcomes.
Significantly increased titers of anti-spike, anti-RBD, and neutralizing antibodies were observed in both UD and HC groups 28 days after the booster dose, although the titer rise of anti-spike IgG and anti-RBD IgG was insignificantly inferior in the UD group compared to the HC group. All antibodies’ titers declined, with no significant differences between the two groups over time. Notably, all specific antibodies persisted up to 180 days; particularly the neutralizing antibody in both groups. Furthermore, no significant difference in antibody levels was observed between each UD subgroup and the HC group, except for neutralizing antibodies in the hypertension sub-group. PastoCovac Plus and PastoCovac boosters induced higher antibodies’ fold rise in UD individuals than BBIBP-CorV booster recipients. Safety outcomes did not show any serious AEs after the booster injection. The overall incidence of AEs post the booster injection was higher in the UD group than the HC group. Furthermore, the highest systemic AEs rate was reported in the UD group receiving the BBIBP-CorV booster.
In conclusion, administration of COVID-19 boosters can equally induce robust and persistent humoral immune responses in individuals with or without UD primarily vaccinated with 2-doses of the BBIBP-CorV. Protein-based boosters with higher antibodies' fold rise and lower AEs in individuals with comorbidities might be considered a better choice for these individuals.
Keywords:
COVID-19 vaccine
; booster
; underlying diseases
; antibody
1. Introduction
As of Jan 20, 2023, 663,640,386 confirmed cases of COVID-19 and 6,713,093 deaths have been globally reported by WHO [1]; 7,562,998 confirmed cases of COVID-19 and 144,728 deaths were in Iran [2]. On May 11, 2023, WHO declared the end of coronavirus disease 2019 (COVID-19) as a global public health emergency [3]. However, monitoring the impact of COVID-19 and the effectiveness of prevention and control strategies remains a public health priority [4]. Various types of studies have demonstrated that people with comorbidities are at a higher mortality risk when develop COVID-19 [5,6], which is a major concern for these individuals and a major challenge for the global health system. Considering the potential threat of COVID-19 morbidity and severity in this population, prevention of infection/reinfection is a crucial priority. There is no doubt that vaccination is one of the most successful and cost-effective ways to control SARS-CoV-2 spread [7]. Although several COVID-19 vaccines have been widely approved [8], the safety and immunogenicity of COVID-19 vaccines in specific groups such as those with chronic diseases remain unclear. Several studies have revealed lower immunogenicity of COVID-19 vaccines in populations with obesity [9,10,11,12], diabetes [13,14,15,16], and hypertension [9,17,18] compared to healthy subjects. Hence, there seems to be an association between comorbidities and lower antibody levels, especially regarding inactivated COVID-19 vaccines. However, the antibody persistency of COVID-19 boosters in these populations has not been determined, yet. Therefore, a booster dose might be essential in these patients in order to boost the immune response.
From another point of view, some studies have shown that protein subunit vaccines could be administrated as a better alternative booster following two doses of inactivated vaccine [19,20]. Two protein subunit COVID-19 vaccines, PastoCovac (Soberana 02) and PastoCovac Plus (Soberana Plus) have been manufactured at Pasteur Institute of Iran in collaboration with the Finlay Vaccine Institute in Cuba. Although recent studies have confirmed the safety and immunogenicity of both vaccines in healthy adults [21,22,23] and children [24,25], there is no efficient associated data of these vaccines among populations with comorbidities. Therefore, we retrospectively evaluated and compared the immunogenicity and safety of three COVID-19 boosters in people with underlying diseases who had received two doses of the BBIBP-CorV vaccine. Moreover, the durability of humoral immune response after COVID-19 booster vaccination in specific individuals was evaluated.
2. Materials and Methods
2.1. Study design and participants
We conducted a retrospective study to evaluate the safety, immunogenicity, and antibody persistency of different COVID-19 boosters in individuals with underlying diseases in comparison with healthy subjects after primary vaccination with the BBIBP-CorV.
This study was conducted on 140 participants who were referred to Pasteur Institute of Iran between February 2022 and August 2022 to be vaccinated and subsequently agreed to be followed in a 180-day follow-up schedule. Data on the demographic and clinical features of all participants were collected through face-to-face or phone interviews.
The participants aged ≥18 years who were primed with BBIP-CorV (SinoPharm, Beijing CNBG with an interval of 4-5 weeks) were investigated as below:
- 1)
- BBIP-CorV primed/ PastoCovac Plus boosted (BP)
- 2)
- BBIP-CorV primed / PastoCovac boosted (BPa)
- 3)
- BBIP-CorV primed / BBIP-CorV boosted (BB)
The booster shot was administrated 3-6 months post the second dose in all groups.
Participants were divided into two UD or HC groups according to the recorded medical history and profiles. UD group was defined as people with at least one of the three conditions including obesity, hypertension, and diabetes mellitus. The UD group was divided into three subgroups including obesity, hypertension, and multi.
People with a body mass index (BMI) ≥30 kg/m 2 have been considered obese people. Hypertension and diabetes mellitus were diagnosed by physicians’ screen based on the medical history and relevant medicine therapy. According to CDC guidelines, people with diabetes mellitus are diagnosed with high level of fasting blood sugar (≥ 126 mg/dL) [26]. Moreover, hypertensive patients were defined as having high blood pressure (with systolic blood pressure ≥ 130 mmHg and diastolic blood pressure ≥ 80 mmHg) [27]. People with more than one mentioned disease are categorized in multi subgroup. In addition, those with normal BMI and without any underlying diseases were considered the HC group.
Exclusion criteria were other comorbidities, pregnant women, and vaccinated participants who had been primed with other COVID-19 vaccines rather than BBIP-CorV or did not meet the standard interval time.
All study participants who met criteria of the study and agreed to participate were provided a consent form. The study was approved by the Ethics Committee of the Pasteur Institute Iran (reference number: IR.NREC.1400.020) and all the applied methods were in accordance with the Declaration of Helsinki.
2.2. Antibodies response
Blood sera samples were collected before booster administration and 28, 60, 90, and 180 days after it. The levels of anti-spike IgG antibody, anti-RBD IgG, and neutralizing antibody were measured by using Anti-SARS-CoV-2 Quantivac ELISA (IgG) (Euroimmun, Lübeck, Germany), anti-RBD IgG (Idealtashkhis, Iran), and SARS-CoV-2 Neutralizing Ab (Pishtazteb, Iran), respectively. Thresholds of ≥2.5, 5, and 11 IU/mL were considered positive for SARS-CoV-2 Neutralizing Ab, anti-RBD SARS-CoV-2, and Anti-spike SARS-CoV-2 IgG, respectively. The antibody concentration above the threshold was repeated by diluting the samples with diluent solution.
2.3. Safety Assessment
All participants were monitored for adverse reactions (AEs) for 30 minutes after receiving the booster shot. For evaluating late adverse events, all the local (pain at the injection site, soreness, induration, swelling, and warmness) and systemic adverse events (fever, chill, weakness, headache, fatigue, nausea, vomiting, diarrhea, and arthralgia) were recorded in the questionnaire via phone-calls on days 7 and 21 after the booster dose. The classification of adverse events was performed based on the related guidelines.
2.4. Statistical analysis
Statistical analysis was reported as geometric mean and 95%CI, median and interquartile range (IQR) for quantitative variables and frequency and percent for qualitative variables. For each antibody, fold rise was calculated using dividing the titer of the antibody on day 28, 60, 90, and 180 by day zero.
The distribution of each antibody between the two groups was assessed using the Mann-Whitney U test. Just in the UD group, the fold rise distribution of each antibody at each time point was compared in different subgroups using the Mann-Whitney U test and Kruskal Wallis test. The chi-square test was used for assessing categorical variables. All the tests were considered two-way and a p-value < 0.05 was reported as statistically significant. All statistical analyses and graphs were performed using SPSS statistics software (version 26.0) and GraphPad Prism (version 9.0.0).
3. Results
3.1. Study population
This study recruited 140 participants including 77 HC and 63 UD. The demographics are shown in Table 1. All participants were divided into age subgroups ≤40 years old and >40 years old.
Of all participants with UD, 57.14% and 25.40% had obesity and hypertension retrospectively, and 17.46% had more than one comorbidity. Patients with diabetes mellitus were included in the multi subgroup due to the coexistence of their disease with other comorbidities.
The COVID-19 history showed that 14.3% of the UD group and 23.4% of the HC ones had a history of COVID-19. In the UD group, 41.3%, 27%, and 31.7% of patients received PastoCovac Plus, PastoCovac, and BBIBP-CorV, as booster doses, respectively. In the HC group, 28, 27, and 22 participants belonged to BP, BPa, and BB groups, respectively.
3.2.Comparison of COVID 19 booster simmunogenicity and antibody persistency between UD and HC groups
To determine whether the underlying disease is associated with humoral immune responses, we examined post-booster antibody levels in UD and HC participants. In addition, the baseline of GMT values regarding anti-spike IgG, anti-RBD IgG, and neutralizing antibodies were compared to the antibodies level on days 28, 60, 90, and 180 to assess booster vaccines for both groups.
The titers of anti-spike IgG, anti-RBD IgG, and neutralizing antibodies were not significantly different in both UD and HC groups over time (Table 2). Significantly increased antibodies’ titers were found in both groups 28 days after the booster dose (Figure 1B–D), the titers rise of anti-spike IgG and anti-RBD IgG was inferior in the UD group compared to the HC group. A decline in the level of all antibodies’ titers was observed on days 60, 90, and 180 compared to day 28 (Table 2, Figure 1B–D). However, this trend was not significantly different between healthy and UD groups. Antibody persistence results indicated that neutralizing antibodies were the most persistent during 180 days post-booster shots (Figure 1B–D).
The titers and fold rise of specific antibodies between the HC and UD at different time points are shown in Table 2. Furthermore, the antibodies’ titers of each UD subgroup were compared with the HC group and the results showed no significant difference in antibody levels (Figure 2A–F,H,I). Nevertheless, neutralizing antibody level on day 28 was significantly lower in the hypertension subgroup (P = 0.000) compared to the HC group (Figure 2G).
3.2.1. Immunogenicity and antibody persistency of boosters among people with underlying diseases
In our study, we investigated to find whether there is a possible association between the fold rise of specific antibodies and demographic parameters such as age, sex, as well as COVID-19 history, types of UD, and boosters.
The median fold rise of anti-spike IgG on day 28 was more in UD participants aged > 40 years (7.69, IQR: 14.26), compared to younger participants (1.61, IQR: 6.07) (p=0.02). The fold rise of anti-RBD IgG on day 60 in men (9.70, IQR:46.30) was significantly higher than in women (p=0.03). Also, the fold rise distribution of neutralizing antibody on day 60 was significantly different between females (1.05, IQR: 0.13) and males (1.23, IQR:1.39) (p=0.03).
Fold rise of neutralizing antibody on day 28 was significantly different among sub-groups of UD (p=0.04), obesity (1.09, IQR:0.39), hypertension (1.6, IQR:2.03), and multigroup (1.5, IQR:8.13).
A significant difference in anti-Spike IgG fold rise on day 28 was observed among the booster groups of UD participants (p <0.001), the BB group (1.55, IQR: 1.19) showed lower fold rise of anti-Spike IgG in comparison to both BP (11.01, IQR:36.75) and BPa (11.34, IQR: 20.25) groups. Furthermore, the fold rise of neutralizing antibody on day 28 showed a significant difference between UD participants receiving PastoCovac Plus (1.66, IQR: 3.04) compared to BBIBP-CorV booster (1.03, IQR: 0.14).
In the UD group, a high rate of anti-RBD IgG fold rise was observed in the BP (15.26, IQR: 121.92) and BPa (13.85, IQR: 23.06) groups than the BB group (15.26, IQR: 121.92) on days 28 (p <0.001, p=0.03), while PastoCovac Plus injection had the greatest effects. Moreover, similar results were observed on day 90, with a greater increase in anti-RBD IgG fold rise in the BP group (11.57, IQR: 151.55) than in the BB group (11.57, IQR: 151.55).
On day 60, there was a significant difference in anti-RBD IgG fold rise among three booster groups (p=0.03), while BPa (9.38, IQR: 45.09) showed the highest fold rise in comparison to other indicated groups ([BB: 1.05, IQR: 0.94], [BP: 4.74, IQR: 20.33]) (Table 2). Other variables had no significant impact on the antibodies’ median fold rise on 28, 60, 90, and 180 days following the booster shot (Table 3).
3.3. Comparative safety outcomes of COVID-19 boosters between UD and HC groups
To investigate whether comorbidities were associated with the incidence of adverse events, we assessed the adverse events incidence after booster administration in participants with UD. No serious AEs were observed within 30 min after the booster injection. Fourteen people (8 healthy people and 6 UD people, p<0.99) reported local AEs within 7 days after receiving a booster dose. Fifteen out of all participants reported at least one systemic AE. Furthermore, systematic AEs were significantly higher in the UD group (17.5%) in comparison with healthy people (5.2%, (p=0.01). The most frequently reported local AE in the UD and HC groups was pain at the injection site (9.5%, 10.4%) (Figure 3A). Weakness was the most common systemic AE and which reported significantly more in the UD group (p=0.01) (Figure 3B). On day 21 after booster vaccination, six people reported local AEs, with injection-site pain being the most AE. Moreover, seven people reported at least one systemic AE, of which weakness was the most common. There was higher local and systemic AEs incidence within day 21 in the HC group compared to the UD group. However, the difference between the two groups was not statistically significant.
Among booster subtypes, more local AEs (13.6%) were observed in the BPa group compared with the BP (5.6%) and BB (11.9%) groups, but it was not significant (p=0.37). BBIBP-CorV injected people reported significantly more systemic AE (21.4%) than the BP (1.9%) and BPa (9.1%) groups (p=0.005).
Based on subgroup analysis, there were no reported differences in local AEs between the UD and HC groups, while those with UD who had injected BBIBP-CorV reported more systemic AEs (40%) than other booster groups (p=0.005) (Figure 3C,D).
4. Discussion
Based on the available scientific evidence, people with underlying diseases (e.g., obesity, hypertension, etc.), are at risk of increased rate of severe complications and mortality induced by COVID-19, due to the impaired and dysregulated immune response [5,6]. Therefore, vaccination is a top priority in these populations [7]. Inactivated vaccines are the most widely administered vaccine type in Iran, especially among the elderly. Many published results have reported a decline in antibodies’ titers after primary vaccination with the BBIBP-CorV vaccine and the positive effects of boosters to restore diminish antibodies [28,29]. Therefore, the identification of booster type that can induce stronger immunogenicity in BBIBP-CorV immunized UD people is important, as the data on this issue is limited. In the current study, for the first time, we assessed the presence of SARS-CoV-2 antibodies before and after booster vaccination during 6 months of follow-up in individuals with underlying diseases. Moreover, the safety, immunogenicity, and antibody persistency of protein-based and inactivated booster vaccines were compared in specific populations.
Our results revealed that anti-spike, anti-RBD, and neutralizing antibodies titers significantly increased on day 28 after the booster dose. This assessment indicates the good immunogenicity impact of protein subunit vaccines on BBIBP-CorV primed participants. Consistent with our study, no significant difference in antibody titers was observed between Chinese participants with and without underlying medical conditions after vaccination with Vero cell-derived inactivated COVID-19 vaccine [30]. Moreover, a previous study comparing the immunogenicity of CoronaVac vaccine between people with comorbidities and healthy controls showed that there was no significant difference in neutralizing antibody levels between both groups at different time points [31]. Conversely, some investigations reported lower antibody titers in patients with comorbidities post-vaccination in comparison with healthy people [13,14,15,16,32]. Although we observed that antibodies’ titers had declined by days 60, 90, and 180, they remained at an acceptable level over 180 days; neutralizing antibodies were the most persistent ones. In the same manner, two investigations confirmed the persistence of antibody titers several months after vaccination in hypertensive patients [17,33]. Moreover, the persistence of neutralizing antibody of the PastoCovac Plus booster was reported in Cubans eight months after primary vaccination with the PastoCovac vaccine [34]. These findings have noted the positive effects of booster vaccines on production and persistency of antibody response in immunized people living with UD.
In our study, we evaluated the association between the fold rise of specific antibodies and demographic parameters such as age, sex, as well as types of UD and boosters. We found that the antibodies’ fold rise was not different between age sub-groups. However, the anti-spike IgG fold rise on day 28 was different in the UD group aged >40 than younger people, which could be due to a higher baseline antibody level in this subgroup or/and more population of them compared to healthy people. In agreement with our results, A study revealed that the two doses of CoronaVac inactivated vaccines induced higher neutralizing antibody levels in senior people and cancer patients than in younger and healthy people [31]. In contrast, some studies reported lower SARS-CoV-2 antibody levels in older people [35,36,37,38]. Therefore, previous studies and the present results demonstrate antibody response to SARS-CoV-2 after booster dose in people with older age enhanced, emphasizing the excellent immunogenicity of booster dose in the population with comorbidities and older age.
Various types of studies established that patients with comorbidities showed different post-vaccination humoral immune responses [30,33,39]. We found that people with hypertension had lower levels of neutralizing antibodies on day 28 compared to the HC group. In agreement with our results, two recent studies revealed that anti-spike and anti-RBD antibodies after primary vaccination with the CoronaVac vaccine were significantly lower in the hypertension group than in the healthy group [17,33]. Therefore, designing and implementing the vaccination program with more efficiency in this subgroup seems necessary.
Several studies have shown that men experience more severe COVID-19 outcomes [40,41,42] and sex differences affect the immune responses to COVID-19 vaccines [43]; though, the exact cause of this gender-based difference is not clear. We found that antibodies’ titers did not discriminate by sex, except for anti-RBD and neutralizing antibodies fold rise on day 60. Similarly, a meta-analysis study showed greater efficacy of the COVID-19 vaccines in men than in women [44]. One study showed that antibody response to a COVID-19 vaccine at one and five months after primary vaccination was not affected by sex, while anti-spike IgG levels differed between women and men at 3 months post-vaccination [17]. In addition, another study has reported no significant difference in antibodies’ titers between men and women after the booster dose [45]. Differences regarding impact of sex on antibody levels may be due to the coexistence of other host factors such as age and other comorbidities, and further clinical trials are necessary to determine and evaluate the impact of sex differences on the effectiveness of the COVID-19 vaccine.
Good immunogenicity and safety of protein subunit COVID-19 vaccines have been reported in recent data [46,47]. We demonstrated that the antibodies’ fold rise in some follow-up days was significantly different among booster groups. The lowest antibodies’ fold rise was observed in UD people after receiving the BBIBP-CorV booster. In agreement with our findings, the higher rate of neutralizing antibody induced by NVSI-06-07 booster (protein-based vaccine) was detected in comparison with the BBIBP-CorV homologous regimen [48]. Our previous study also showed the better boosting effect of PastoCovac and PasctoCovac plus as a booster vaccine on humoral immune response in comparison to the inactivated vaccine in Iranian adults [49]. Overall, our research has revealed that the protein subunit vaccines appear to be able to induce a stronger humoral immune response than the inactivated COVID-19 vaccine.
Besides immunogenicity, we surveyed the safety outcome of inactivated and protein-based COVID-19 boosters in people with UD. In our study, no serious AEs were found after the booster injection. We observed that the overall incidence of adverse events within 7 days was higher in the UD group than in the HC group. The most common local AE in healthy and UD people was pain at the injection site. Weakness is the most common systemic AE in people with UD. Among booster sub-groups, the systemic AEs were significantly higher in UD individuals who received the BBIBP-CorV booster than in other groups. These results indicated that protein subunit vaccines could be proposed as a better alternative to booster doses with lower AEs in people with UD. Similarly, a study performed by Li et al. demonstrated that the incidence of injection-site pain, fatigue, and headache was higher in some disease groups than in healthy control after primary vaccination with CoronaVac vaccine [50]. Moreover, no AEs were observed in people with obesity and hypertension following inactivated COVID-19 vaccination [30]. Overall, booster vaccines, especially protein-based boosters, have good immunogenicity, good safety and are therefore recommended for people with underlying diseases.
There are some limitations in the current study. First, the sample size was small. Second, cellular immunity was not studied, which could determine whether participants with a low rate of antibody response could develop adequate T-cell response to prevent COVID-19. Further long-term studies are required to evaluate the persistence of cellular immune responses in participants with chronic diseases after booster vaccination. This may be important in determining the schedule of subsequent vaccinations.
5. Conclusion
In conclusion, our data provide the first comprehensive picture of the safety, immunogenicity, and antibody persistency of COVID-19 booster vaccination in Iranian cases with comorbidities. We found that different types of booster vaccines could elicit equally strong and persistent humoral immune responses in those vaccinated with BBIBP-CorV with or without UD. Among UD people, protein-based booster vaccines had higher antibodies' fold rise and lower AEs in comparison with inactivated booster vaccines. Because UD subjects are a high-risk group, we strongly recommend vaccinating this group with the protein-based vaccine. In addition, further research is needed to select the best booster vaccine for this population.
Author Contributions
A.R. and F.A. contributed to the study’s conceptualization and design. Analyses and interpretation of data were performed by F.B.A. A.B and M.Z. performed the assays and managed the laboratory tests. The first draft of the manuscript was written by F.A. M.S.L. revised the manuscript. A.R. revised and finalized the manuscript. All authors read and approved the final manuscript.
Funding
This study was supported by Pasteur Institute of Iran (Grant No. 2127).
Institutional Review Board Statement
The study was approved by the ethical board of the Pasteur Institute of Iran (Reference number: IR.NREC.1400.020). The study complied with the Declaration of Helsinki. All enrolled prticipants signed the informed consent.
Informed Consent Statement
Written informed consent was obtained from all participants involved in the study.
Data availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of interest
The authors declare that they have no competing interests.
References
- WHO. Coronavirus (COVID-19) Dashboard. 2023:https://covid19.who.int/.
- WHO. WHO Health Emergency Dashboard.https://covid19.who.int/region/emro/country/ir.
- 2023.
- CDC. End of the Federal COVID-19 Public Health Emergency (PHE) Declaration [Internet]. 2023.
- Yin T, Li Y, Ying Y, Luo Z. Prevalence of comorbidity in Chinese patients with COVID-19: systematic review and meta-analysis of risk factors. BMC infectious diseases. 2021;21:1-13. [CrossRef]
- Emami A, Javanmardi F, Pirbonyeh N, Akbari A. Prevalence of underlying diseases in hospitalized patients with COVID-19: a systematic review and meta-analysis. Archives of academic emergency medicine. 2020;8(1).
- Huynh G, Nguyen TV, Nguyen DD, Lam QM, Pham TN, Nguyen HTN. Knowledge about COVID-19, beliefs and vaccination acceptance against COVID-19 among high-risk people in Ho Chi Minh City, Vietnam. Infection and drug resistance. 2021:1773-80. [CrossRef]
- Wang H, Zhang Y, Huang B, Deng W, Quan Y, Wang W, et al. Development of an inactivated vaccine candidate, BBIBP-CorV, with potent protection against SARS-CoV-2. Cell. 2020;182(3):713-21. e9. [CrossRef]
- Watanabe M, Balena A, Tuccinardi D, Tozzi R, Risi R, Masi D, et al. Central obesity, smoking habit, and hypertension are associated with lower antibody titres in response to COVID-19 mRNA vaccine. Diabetes/metabolism research and reviews. 2022;38(1):e3465.
- Zhu Q, Zhang Y, Kang J, Chen Z, Peng M, Chen M, et al. Weakened humoral and cellular immune response to the inactivated COVID-19 vaccines in Chinese individuals with obesity/overweight. Genes & Diseases. 2022. [CrossRef]
- Malavazos AE, Basilico S, Iacobellis G, Milani V, Cardani R, Boniardi F, et al. Antibody responses to BNT162b2 mRNA vaccine: infection-naïve individuals with abdominal obesity warrant attention. Obesity. 2022;30(3):606-13. [CrossRef]
- Dicker D, Golan R, Baker JL, Busetto L, Frühbeck G, Goossens GH, et al. Vaccinating people with obesity for COVID-19: EASO call for action. Obesity Facts. 2021;14(3):334. [CrossRef]
- Sauré D, O'Ryan M, Torres JP, Zuniga M, Santelices E, Basso LJ. Dynamic IgG seropositivity after rollout of CoronaVac and BNT162b2 COVID-19 vaccines in Chile: a sentinel surveillance study. The Lancet Infectious Diseases. 2022;22(1):56-63. [CrossRef]
- Singh AK, Phatak SR, Singh R, Bhattacharjee K, Singh NK, Gupta A, et al. Antibody response after first and second-dose of ChAdOx1-nCOV (CovishieldTM®) and BBV-152 (CovaxinTM®) among health care workers in India: The final results of cross-sectional coronavirus vaccine-induced antibody titre (COVAT) study. Vaccine. 2021;39(44):6492-509. [CrossRef]
- Karamese M, Tutuncu EE. The effectiveness of inactivated SARS-CoV-2 vaccine (CoronaVac) on antibody response in participants aged 65 years and older. Journal of Medical Virology. 2022;94(1):173-7. [CrossRef]
- Ali H, Alterki A, Sindhu S, Alahmad B, Hammad M, Al-Sabah S, et al. Robust antibody levels in both diabetic and non-diabetic individuals after BNT162b2 mRNA COVID-19 vaccination. Frontiers in immunology. 2021:4909. [CrossRef]
- Soegiarto G, Wulandari L, Purnomosari D, Fahmita KD, Gautama HI, Hadmoko ST, et al. Hypertension is associated with antibody response and breakthrough infection in health care workers following vaccination with inactivated SARS-CoV-2. Vaccine. 2022;40(30):4046-56. [CrossRef]
- Pellini R, Venuti A, Pimpinelli F, Abril E, Blandino G, Campo F, et al. Initial observations on age, gender, BMI and hypertension in antibody responses to SARS-CoV-2 BNT162b2 vaccine. EClinicalMedicine. 2021;36:100928. [CrossRef]
- Ai J, Zhang H, Zhang Q, Zhang Y, Lin K, Fu Z, et al. Recombinant protein subunit vaccine booster following two-dose inactivated vaccines dramatically enhanced anti-RBD responses and neutralizing titers against SARS-CoV-2 and Variants of Concern. Cell research. 2022;32(1):103-6. [CrossRef]
- Cao Y, Hao X, Wang X, Wu Q, Song R, Zhao D, et al. Humoral immunogenicity and reactogenicity of CoronaVac or ZF2001 booster after two doses of inactivated vaccine. Cell research. 2022;32(1):107-9. [CrossRef]
- Toledo-Romaní ME, García-Carmenate M, Valenzuela-Silva C, Baldoquín-Rodríguez W, Martínez-Pérez M, Rodríguez-González M, et al. Safety and efficacy of the two doses conjugated protein-based SOBERANA-02 COVID-19 vaccine and of a heterologous three-dose combination with SOBERANA-Plus: a double-blind, randomised, placebo-controlled phase 3 clinical trial. The Lancet Regional Health–Americas. 2023;18. [CrossRef]
- Toledo-Romani ME, García-Carmenate M, Verdecia-Sánchez L, Pérez-Rodríguez S, Rodriguez-González M, Valenzuela-Silva C, et al. Safety and immunogenicity of anti-SARS CoV-2 conjugate vaccine SOBERANA 02 in a two-dose or three-dose heterologous scheme in adults: Phase IIb Clinical Trial. MedRxiv. 2022:2022.01. 01.21268271. [CrossRef]
- Sadat Larijani M, Sorouri R, Eybpoosh S, Doroud D, Moradi L, Ahmadinezhad M, et al. Assessment of long-term adverse events regarding different COVID-19 vaccine regimens within an 18-month follow-up study. Pathogens and Disease. 2023:ftad010. [CrossRef]
- Puga-Gómez R, Ricardo-Delgado Y, Rojas-Iriarte C, Céspedes-Henriquez L, Piedra-Bello M, Vega-Mendoza D, et al. Open label phase I/II clinical trial and predicted efficacy of SARS-CoV-2 RBD protein vaccines SOBERANA 02 and SOBERANA Plus in children. medRxiv. 2022:2022.03. 03.22271313. [CrossRef]
- Mafinezhad S, Bayani G, Ehteshammanesh H, Langari M, Shokrollahi N, Bozorgnia Y, et al. Evaluation of the side effects of Sinopharm and PastoCovac COVID-19 vaccines in children aged 5-12 years in Iran. International Journal of Pediatrics. 2023;11(4):17572-82.
- CDC. Diabetes Tests. 2023:https://www.cdc.gov/diabetes/basics/getting-tested.html#:~:text=A%20fasting%blood%sugar%level,higher%indicates%you%have%diabetes.
- CDC. High Blood Pressure Symptoms and Causes. 2021:https://www.cdc.gov/bloodpressure/about.htm.
- Muangnoicharoen S, Wiangcharoen R, Nanthapisal S, Kamolratakul S, Lawpoolsri Niyom S, Jongkaewwattana A, et al. Single Ad26. COV2. S Booster Dose Following Two Doses of BBIBP-CorV Vaccine Against SARS-CoV-2 Infection in Adults: Day 28 Results of a Phase 1/2 Open-Label Trial. 2023.
- Amellal H, Assaid N, Akarid K, Maaroufi A, Ezzikouri S, Sarih Mh. Mix-and-match COVID-19 vaccines trigger high antibody response after the third dose vaccine in Moroccan health care workers. Vaccine: X. 2023;14:100288. [CrossRef]
- Zhang Y, Chen H, Lv J, Huang T, Zhang R, Zhang D, et al. Evaluation of Immunogenicity and Safety of Vero Cell-Derived Inactivated COVID-19 Vaccine in Older Patients with Hypertension and Diabetes Mellitus. Vaccines. 2022;10(7):1020. [CrossRef]
- Li C, Bi H, Fu Z, Li A, Wan N, Hu J, et al. Retrospective study of the immunogenicity and safety of the CoronaVac SARS-CoV-2 vaccine in people with underlying medical conditions. Communications Medicine. 2022;2(1):151.
- Pellini R, Venuti A, Pimpinelli F, Abril E, Blandino G, Campo F, et al. Obesity may hamper SARS-CoV-2 vaccine immunogenicity. MedRXiv. 2021:2021.02. 24.21251664. [CrossRef]
- Rifai A, Wahono CS, Pratama MZ, Handono K, Susianti H, Iskandar A, et al. Association between the effectiveness and immunogenicity of inactivated SARS-CoV2 vaccine (CoronaVac) with the presence of hypertension among health care workers. Clinical and Experimental Hypertension. 2022;44(3):233-9. [CrossRef]
- Toledo-Romani ME, Garcia-Carmenate M, Silva CV, Baldoquin-Rodriguez W, Pérez MM, Gonzalez MR, et al. Efficacy and safety of SOBERANA 02, a COVID-19 conjugate vaccine in heterologous three-dose combination. MedRxiv. 2021. [CrossRef]
- Pellini R, Venuti A, Pimpinelli F, Abril E, Blandino G, Campo F, et al. Early onset of SARS-CoV-2 antibodies after first dose of BNT162b2: Correlation with age, gender and BMI. Vaccines. 2021;9(7):685. [CrossRef]
- Míguez HM, García IM, Gómez MO, Merino IMG, Cano EL, De La Torre A. Immunogenicity, effectiveness and safety of COVID-19 vaccine in older adults living in nursing homes: A real-life study. Revista Española de Geriatría y Gerontología. 2023. [CrossRef]
- Bruel T, Pinaud L, Tondeur L, Planas D, Staropoli I, Porrot F, et al. Neutralising antibody responses to SARS-CoV-2 omicron among elderly nursing home residents following a booster dose of BNT162b2 vaccine: A community-based, prospective, longitudinal cohort study. EClinicalMedicine. 2022;51:101576. [CrossRef]
- Shapiro JR, Sitaras I, Park HS, Aytenfisu TY, Caputo C, Li M, et al. Association of Frailty, Age, and Biological Sex With Severe Acute Respiratory Syndrome Coronavirus 2 Messenger RNA Vaccine–Induced Immunity in Older Adults. Clinical Infectious Diseases. 2022;75(Supplement_1):S61-S71. [CrossRef]
- Gaborit B, Fernandes S, Loubet P, Ninove L, Dutour A, Cariou B, et al. Early humoral response to COVID-19 vaccination in patients living with obesity and diabetes in France. The COVPOP OBEDIAB study with results from the ANRS0001S COV-POPART cohort. Metabolism. 2023;142:155412. [CrossRef]
- Fathi M, Vakili K, Sayehmiri F, Mohamadkhani A, Hajiesmaeili M, Rezaei-Tavirani M, et al. The prognostic value of comorbidity for the severity of COVID-19: A systematic review and meta-analysis study. PloS one. 2021;16(2):e0246190. [CrossRef]
- Channappanavar R, Fett C, Mack M, Ten Eyck PP, Meyerholz DK, Perlman S. Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection. The Journal of Immunology. 2017;198(10):4046-53. [CrossRef]
- Badawi A, Ryoo SG. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): a systematic review and meta-analysis. International Journal of Infectious Diseases. 2016;49:129-33. [CrossRef]
- Naaber P, Tserel L, Kangro K, Sepp E, Jürjenson V, Adamson A, et al. Declined antibody responses to COVID-19 mRNA vaccine within first three months. medRxiv. 2021:2021.04. 19.21255714. [CrossRef]
- Bignucolo A, Scarabel L, Mezzalira S, Polesel J, Cecchin E, Toffoli G. Sex disparities in efficacy in COVID-19 vaccines: a systematic review and meta-analysis. Vaccines. 2021;9(8):825. [CrossRef]
- Erdem MG, Unlu O, Buber S, Demirci M, Kocazeybek BS. Could Prior COVID-19 Affect the Neutralizing Antibody after the Third BNT162b2 Booster Dose: A Longitudinal Study. Vaccines. 2023;11(3):560. [CrossRef]
- Salimian J, Ahmadi A, Amani J, Olad G, Halabian R, Saffaei A, et al. Safety and immunogenicity of a recombinant receptor-binding domain-based protein subunit vaccine (Noora vaccine™) against COVID-19 in adults: A randomized, double-blind, placebo-controlled, Phase 1 trial. Journal of Medical Virology. 2023;95(2). [CrossRef]
- Heidary M, Kaviar VH, Shirani M, Ghanavati R, Motahar M, Sholeh M, et al. A comprehensive review of the protein subunit vaccines against COVID-19. Frontiers in microbiology. 2022;13:927306. [CrossRef]
- Kaabi NA, Yang YK, Zhang J, Xu K, Liang Y, Kang Y, et al. Immunogenicity and safety of NVSI-06-07 as a heterologous booster after priming with BBIBP-CorV: a phase 2 trial. Signal Transduction and Targeted Therapy. 2022;7(1):172. [CrossRef]
- Ramezani A, Sorouri R, Haji Maghsoudi S, Dahmardeh S, Doroud D, Sadat Larijani M, et al. PastoCovac and PastoCovac Plus as protein subunit COVID-19 vaccines led to great humoral immune responses in BBIP-CorV immunized individuals. Scientific Reports. 2023;13(1):8065. [CrossRef]
- Li C, Li A, Bi H, Hu J, Yang F, Zhou T, et al. Immunogenicity and safety of the CoronaVac inactivated SARS-CoV-2 vaccine in people with underlying medical conditions: a retrospective study. medRxiv. 2022:2022.04. 28.22274402. [CrossRef]
Figure 1.
Comparative time-course analysis of antibody response to CIVID-19 vaccination. (A) COVID-19 vaccination study design. (B) The titers of anti-spike IgG antibodies, (C) anti-RBD IgG, and (D) neutralizing antibodies in the healthy control and people with underlying diseases over time. HC: healthy control, UD: participants who had at least one comorbidity. P value < 0.05 was considered significant.
Figure 1.
Comparative time-course analysis of antibody response to CIVID-19 vaccination. (A) COVID-19 vaccination study design. (B) The titers of anti-spike IgG antibodies, (C) anti-RBD IgG, and (D) neutralizing antibodies in the healthy control and people with underlying diseases over time. HC: healthy control, UD: participants who had at least one comorbidity. P value < 0.05 was considered significant.
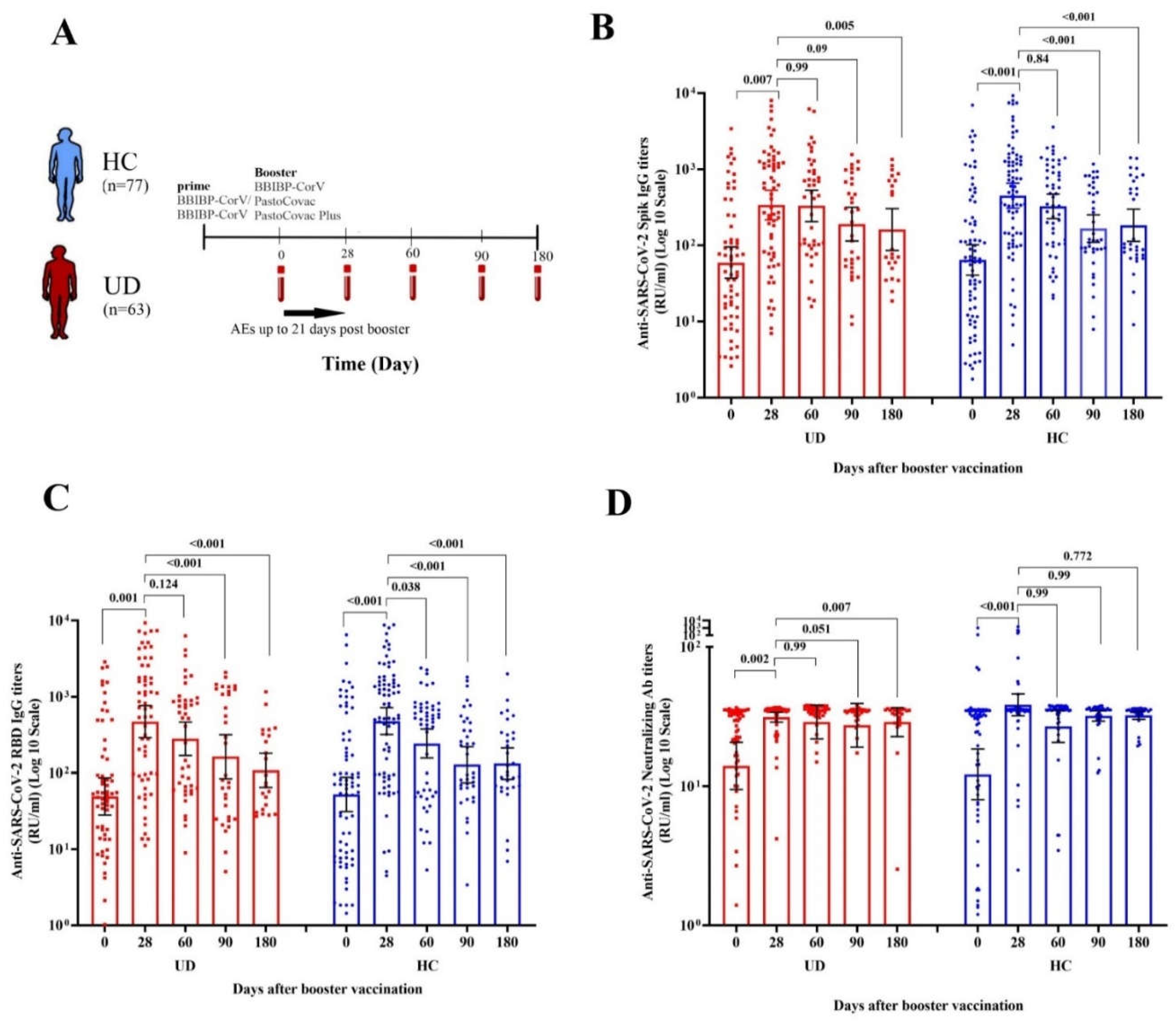
Figure 2.
Comparative analysis of specific antibodies response to COVID-19 vaccination stratified by the presence of underlying diseases. The antibodies’ titers before vaccination (baseline) up to 180-day follow-up demonstrated in participants with different comorbidities in comparison to the healthy control group (HC). Anti-SARS-CoV-2 Spike IgG titers in (A) hypertension, (B) obesity, and (C) multi subgroups. Anti-SARS-CoV-2 RBD IgG titers in (D) hypertension, (E) obesity, and (F) multi subgroups. Anti-SARS-CoV-2 Neutralizing antibody titers in (G) hypertension, (H) obesity, and (I) multi subgroups. *P<0.05 was considered statistically significant. The Mann-Whitney U test was used for comparison titers of each antibody at each time between HC and UD groups.
Figure 2.
Comparative analysis of specific antibodies response to COVID-19 vaccination stratified by the presence of underlying diseases. The antibodies’ titers before vaccination (baseline) up to 180-day follow-up demonstrated in participants with different comorbidities in comparison to the healthy control group (HC). Anti-SARS-CoV-2 Spike IgG titers in (A) hypertension, (B) obesity, and (C) multi subgroups. Anti-SARS-CoV-2 RBD IgG titers in (D) hypertension, (E) obesity, and (F) multi subgroups. Anti-SARS-CoV-2 Neutralizing antibody titers in (G) hypertension, (H) obesity, and (I) multi subgroups. *P<0.05 was considered statistically significant. The Mann-Whitney U test was used for comparison titers of each antibody at each time between HC and UD groups.
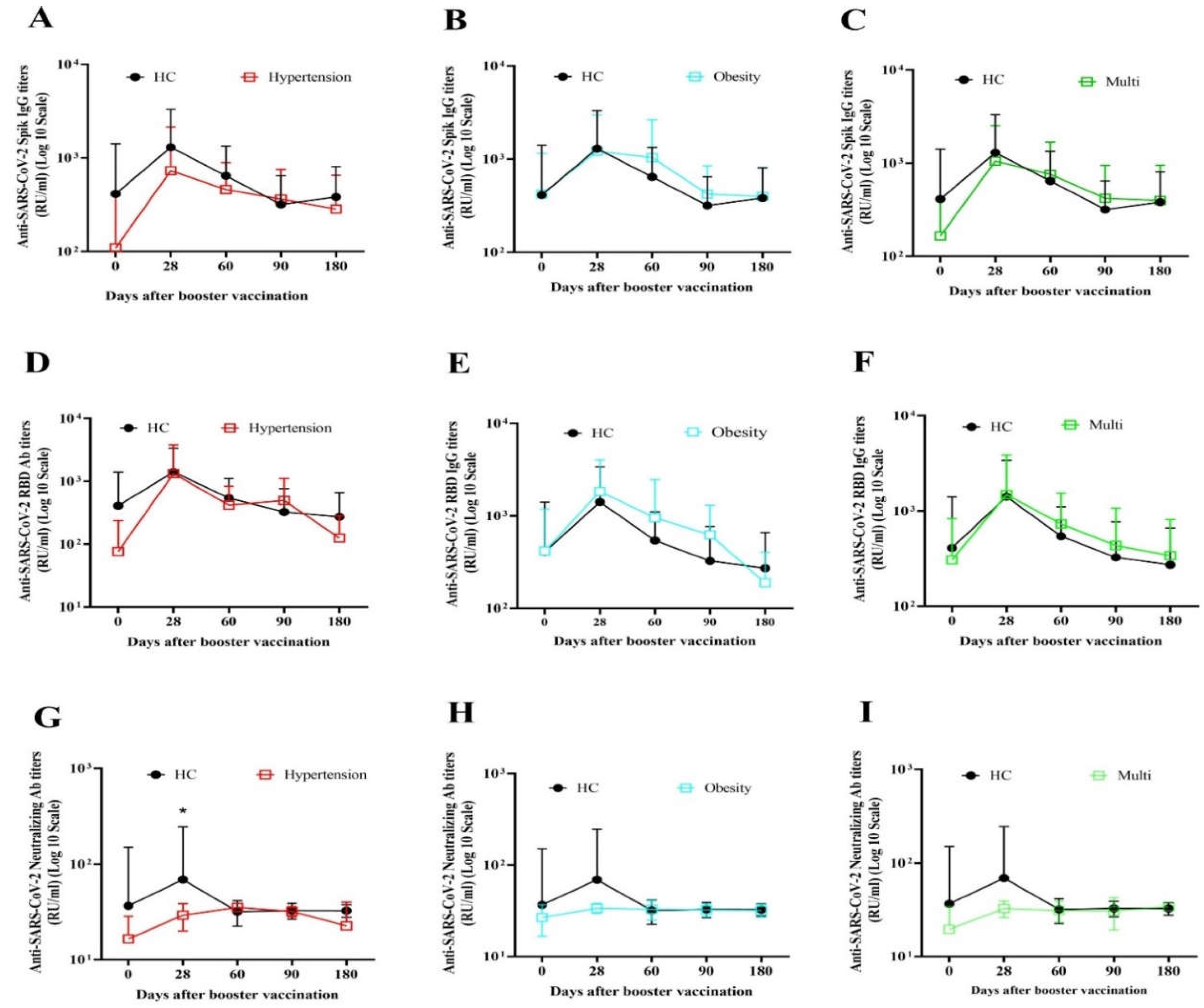
Figure 3.
Incidence of adverse events reported within 7 days after booster vaccination. Incidence of (A) local and (B) systemic AEs in healthy and UD participants. Incidence of (C) local and (D) systemic AEs between the HC and UD groups base on booster groups. HC: healthy control, UD: participants who had at least one comorbidity. *P<0.05 was considered statistically significant.
Figure 3.
Incidence of adverse events reported within 7 days after booster vaccination. Incidence of (A) local and (B) systemic AEs in healthy and UD participants. Incidence of (C) local and (D) systemic AEs between the HC and UD groups base on booster groups. HC: healthy control, UD: participants who had at least one comorbidity. *P<0.05 was considered statistically significant.
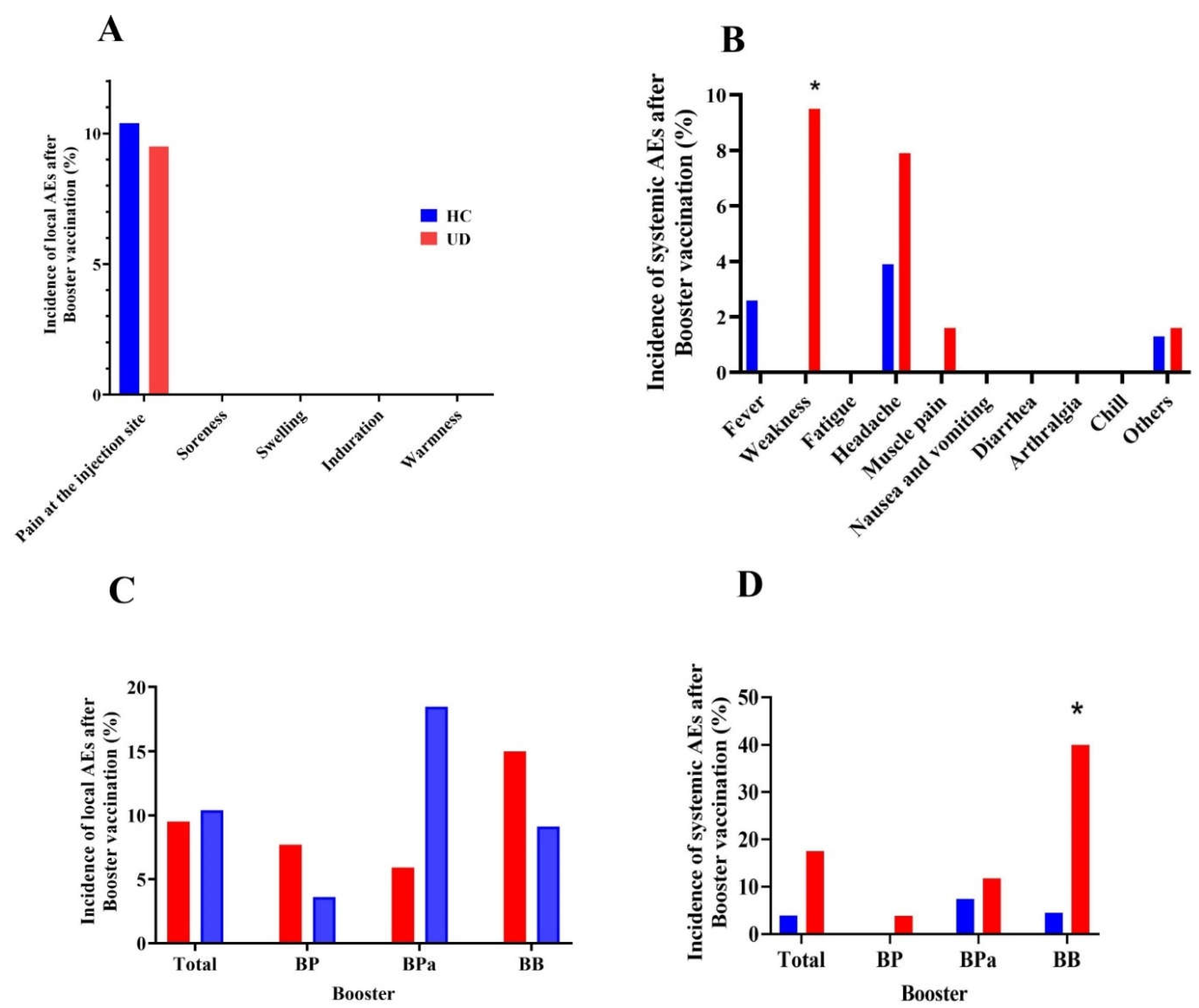

Table 1.
The baseline clinical characteristics of the study participants.
| Total N(%) |
HC N(%) |
UD N(%) |
|
|---|---|---|---|
| Gender | |||
| Female | 74 (52.9%) | 41 (53.2%) | 33 (52.4%) |
| Male | 66 (47.1%) | 36(46.8%) | 30 (47.6%) |
| Age | |||
| ≤ 40 | 57 (40.7%) | 38 (49.4%) | 19 (30.2%) |
| > 40 | 83 (59.3%) | 39 (50.6%) | 44 (69.8%) |
| COVID-19 History | |||
| No | 113 (80.7) | 59 (76.9) | 54 (85.7) |
| Yes | 27 (19.3) | 18 (23.4) | 9 (14.3) |
| Booster | |||
| BP | 54 (38.6%) | 28 (36.4%) | 26 (41.3%) |
| BPa | 44 (31.4%) | 27 (35.1%) | 17 (27.0) |
| BB | 42 (30.0) | 22 (28.6%) | 20 (31.7%) |
HC: healthy control, UD: participants who had at least one comorbidity (obesity, hypertension, and diabetes mellitus). BP: BBIBP-CorV /PastoCovac-Plus, BPa: BBIBP-CorV /PastoCovac, BB: BBIBP-CorV /BBIBP-CorV.
Table 2.
Anti-SARS-CoV-2 Spike, anti-SARS-CoV-2 RBD, and neutralizing antibody levels and fold rise between healthy and UD participants in different time points.
Table 2.
Anti-SARS-CoV-2 Spike, anti-SARS-CoV-2 RBD, and neutralizing antibody levels and fold rise between healthy and UD participants in different time points.
| HC | UD | P value | |
|---|---|---|---|
| Anti-SARS-CoV-2 Spike antibody (Geometric mean, 95% CI) | |||
| Antibodies titers | |||
| Day 0 | 64.26 (40.53-101.88) | 59.22 (36.87-95.12) | 0.86 |
| Day 28 | 449.52 (301.75-656.59) | 339.09 (216.83-530.28) | 0.38 |
| Day 60 | 325.87 (224.88-472.21) | 330.00 (205.34-530.34) | 0.97 |
| Day 90 | 166.11 (109.63-251.69) | 189.99 (113.92-316.86) | 0.79 |
| Day 180 | 183.41 (112.74-298.35) | 161.22 (85.65-303.49) | 0.39 |
| Mean Fold rise | |||
| Day 28 | 7.00 (5.01-9.76) | 5.72 (3.92-8.37) | 0.31 |
| Day 60 | 3.88 (2.33-6.46) | 4.27 (2.35-7.77) | 0.75 |
| Day 90 | 1.67 (0.95-2.94) | 2.88 (1.29-6.45) | 0.25 |
| Day 180 | 1.54 (0.69-3.41) | 1.61 (0.56-4.65) | 0.98 |
| Neutralizing antibody (Geometric mean, 95% CI) | |||
| Antibodies titers | |||
| Day 0 | 12.16 (8.01-18.47) | 13.97 (9.47-20.62) | 0.78 |
| Day 28 | 38.31 (31.95-45.95) | 31.27 (28.79-33.96) | 0.054 |
| Day 60 | 26.84 (20.61-34.96) | 28.85 (21.82-38.15) | 0.90 |
| Day 90 | 31.91 (29.31-34.74) | 27.32 (19.04-39.22) | 0.10 |
| Day 180 | 32.22 (30.14-34.45) | 28.79 (22.66-36.57) | 0.34 |
| Mean Fold rise | |||
| Day 28 | 9.14 (5.98- 13.96) | 9.52 (5.24-19.30) | 0.55 |
| Day 60 | 3.51 (2.01-6.12) | 4.10 (2.04-8.23) | 0.95 |
| Day 90 | 1.78 (1.22-2.60) | 1.55 (0.87-2.78) | 0.32 |
| Day 180 | 1.52 (1.17-1.97) | 1.66 (0.80-3.45) | 0.83 |
| Anti-SARS-CoV-2 RBD antibody (Geometric mean, 95% CI) | |||
| Antibodies titers | |||
| Day 0 | 52.38 (31.24-87.83) | 49.12 (28.07-85.95) | 0.88 |
| Day 28 | 478.74 (319.48-717.38) | 470.89 (290.65-762.90) | 0.98 |
| Day 60 | 242.97 (156.99-376.03) | 279.99 (169.23-463.24) | 0.34 |
| Day 90 | 128.02 (74.30-220.57) | 163.21 (84.18-316.43) | 0.77 |
| Day 180 | 132.60 (82.72-212.55) | 107.96 (64.67-180.24) | 0.34 |
| Mean Fold rise | |||
| Day 28 | 3.15 (2.13-4.66) | 2.23 (1.52-3.27) | 0.27 |
| Day 60 | 1.61 (1.03-2.49) | 1.78 (1.19-2.66) | 0.54 |
| Day 90 | 1.31 (0.66-2.61) | 3.70 (1.27-10.78) | 0.39 |
| Day 180 | 1.05 (0.44-2.54) | 1.29 (0.37-4.45) | 0.11 |
Fold rise was calculated using dividing the titer of the antibody on days 28, 60, 90, and 180 by day zero. HC: healthy control, UD: participants who had at least one comorbidity (obesity, hypertension, and diabetes mellitus). The distribution of GMT was assessed using the Mann-Whitney U test at each daytime point.
Table 3.
Median and IQR of anti-SARS-CoV-2 Spike, anti-SARS-CoV-2 RBD, and neutralizing antibody fold rise on days 28, 60, 90, and 180 in people with underlying disease.
Table 3.
Median and IQR of anti-SARS-CoV-2 Spike, anti-SARS-CoV-2 RBD, and neutralizing antibody fold rise on days 28, 60, 90, and 180 in people with underlying disease.
| Day 28 | Day 60 | Day 90 | Day 180 | |||||
|---|---|---|---|---|---|---|---|---|
| Median (IQR) | P | Median (IQR) | P | Median (IQR) | P | Median (IQR) | P | |
| Anti-SARS-CoV-2 Spike antibody median fold rise (IQR) | ||||||||
| Age | ||||||||
| ≤ 40 | 1.61 (6.07) | 0.02 | 2.73(9.32) | 0.55 | 1.37(4.77) | 0.22 | 0.92(3.30) | 0.36 |
| > 40 | 7.69 (14.26) | 4.12(25.18) | 3.90(14.19) | 2.77(17.39) | ||||
| Gender | ||||||||
| Female | 3.45(11.14) | 0.3 | 1.90(5.53) | 0.08 | 1.33(11.02) | 0.13 | 0.86(9.89) | 0.33 |
| Male | 5.80(18.23) | 6.84(30.94) | 5.02(11.19) | 3.49(14.48) | ||||
| COVID-19 History | ||||||||
| No | 4.58(12.96) | 0.62 | 4.04(17.82) | 0.19 | 3.86(11.04) | 0.63 | 1.86(14.40) | 0.66 |
| Yes | 4.30(11.63) | 1.14(25.51) | 2.37(12.60) | 0.75(18.53) | ||||
| Types of UD | ||||||||
| Hypertension | 9.39(34.58) | 0.21 | 4.12(19.25) | 0.91 | 5.26(86) | 0.54 | 19.53() | 0.25 |
| Obesity | 3.92(10.58) | 2.45(25.18) | 3.86(12.44) | 0.92(14.43) | ||||
| Multi | 4.48(14.03) | 3.56(6.34) | 1.55(4.73) | 0.98(2.28) | ||||
| Booster | ||||||||
| BP | 11.01 (36.75) | <0.001 | 6.07 (31.60) | 0.33 | 5.62 (110.79) | 0.53 | 1.43 (64.41) | 0.83 |
| BPa | 11.34 (20.25) | 6.05 (28.82) | 4.42 (11.83) | 3.50 (14.96) | ||||
| BB | 1.55 (1.19) | 2.18 (2.53) | 1.45 (2.86) | 1.14 (1.95) | ||||
| Anti-SARS-CoV-2 Neutralizing antibody median fold rise (IQR) | ||||||||
| Age | ||||||||
| ≤ 40 | 1.05(0.52) | 0.19 | 1.05(0.43) | 0.28 | 1(0.46) | 0.69 | 0.96(0.16) | 0.36 |
| > 40 | 1.18(1.81) | 1.11(0.85) | 1.12(0.69) | 1.03(0.67) | ||||
| Gender | ||||||||
| Female | 1.09(1.16) | 0.4 | 1.05 (0.13) | 0.03 | 1(0.19) | 0.17 | 0.99(0.20) | 0.92 |
| Male | 1.14(1.54) | 1.23 (1.39) | 1.46(0.68) | 1.01(11.86) | ||||
| COVID-19 History | ||||||||
| No | 1.12(1.38) | 0.11 | 1.10(0.96) | 0.61 | 1.10(0.71) | 0.30 | 0.98(0.58) | 0.84 |
| Yes | 1.02(0.15) | 1.08(0.16) | 0.99(0.15) | 1.10(0.23) | ||||
| Types of UD | ||||||||
| Hypertension | 1.60 (2.03) | 1.18(1.03) | 0.57 | 1.57(170.96) | 0.73 | 0.96() | 0.94 | |
| Obesity | 1.09 (0.39) | 0.04 | 1.08(0.19) | 1.10(0.54) | 1.01(0.37) | |||
| Multi | 1.50 (8.13) | 1.13(4.80) | 0.99(2.77) | 1.01(11.47) | ||||
| Booster | ||||||||
| BP | 1.61 (3.04) | 1.05(1.18) | 0.1 | 1.50(2.19) | 0.29 | 1.03(60.69) | 0.42 | |
| BPa | 1.11 (0.61) | 0.01 | 1.20(0.90) | 1.11(0.63) | 1.01(0.59) | |||
| BB | 1.03 (0.14) | 1.03(0.18) | 1(0.10) | 0.96(0.10) | ||||
| Anti-SARS-CoV-2 RBD antibody median fold rise (IQR) | ||||||||
| Age | ||||||||
| ≤ 40 | 2.28(32.18) | 0.73 | 1.36(11.32) | 0.35 | 0.35(9.53) | 0.05 | 0.35(0.17) | 0.12 |
| > 40 | 5.10(29.58) | 4.22(18.20) | 8.73(20.61) | 1.18(11.28) | ||||
| Gender | ||||||||
| Female | 2.29(30.07) | 0.07 | 1.28 (4.23) | 0.02 | 0.82(19.25) | 0.24 | 0.039(2.54) | 0.47 |
| Male | 10.75(36.62) | 9.70(46.30) | 9.39(21.23) | 0.72(20.92) | ||||
| COVID-19 History | ||||||||
| No | 4.69(34.15) | 0.78 | 3.19(17.45) | 0.35 | 1.43(22.66) | 0.53 | 0.52(4.61) | 0.96 |
| Yes | 6.38(27.27) | 0.98(15.66) | 1.10(19.35) | 0.66(5.26) | ||||
| Types of UD | ||||||||
| Hypertension | 6.38(38.46) | 0.66 | 2.17(21.07) | 0.92 | 11.56(192.97) | 0.32 | 37.53() | 0.18 |
| Obesity | 5.10(29.81) | 1.80(17.13) | 1.62(19.23) | 0.40(2.99) | ||||
| Multi | 4.63(17.70) | 1.95(9.35) | 0.65(13.25) | 0.38(2.58) | ||||
| Booster | ||||||||
| BP | 15.26 (121.92) | 4.74 (20.33) | 11.57 (151.55) | 0.54 (34.19) | 0.72 | |||
| BPa | 13.85 (23.06) | <0.001 | 9.83 (45.09) | 0.03 | 8.73 (19.05) | 0.03 | 0.95 (5.66) | |
| BB | 1.26 (0.57) | 1.05 (0.94) | 0.34 (0.67) | 0.39 (0.55) | ||||
HC: healthy control, UD: participants who had at least one comorbidity (obesity, hypertension, and diabetes mellitus). BP: BBIBP-CorV /PastoCovac-Plus, BPa: BBIBP-CorV /PastoCovac, BB: BBIBP-CorV /BBIBP-CorV. Bold P values are shown as significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



