
Submitted:
28 June 2023
Posted:
29 June 2023
You are already at the latest version
Abstract
Background: There is an exponential increase in caesarean sections with epidemic proportions worldwide, which is considered as a serious public health issue that influences negatively both maternal and childhood health. Aims: This study aimed to evaluate the associations between pre-dominant maternal risk factors and the prevalence of caesarean section in a representative sample of women from Greece. Methods: This is a cross-sectional study conducted on 5182 healthy, re-productive-aged women from 11 geographically diverse Greek areas after applying specific inclu-sion and exclusion criteria. Statistical analysis was applied to evaluate the impact of maternal so-ciodemographic, anthropometric, lifestyle and perinatal factors in the risk of caesarean section de-liveries. Results: A high prevalence of 56.4% of caesarean section deliveries was recorded in the study population. The incidence of caesarean sections reached to 51.5% in private hospitals in which an increasing rate of 47.5% for planned caesarean sections were noticed. Older maternal age, pre-pregnancy overweight and obesity, excess gestational weight gain, high rates of preterm birth, better economic status, smoking habits, and private type of birth hospital were significantly related with enhanced risk of caesarean section, independently of multiple confounding factors. Conclu-sions: Our study revealed that caesarean section rates are continuously increase, while several maternal risk factors, including especially pre-pregnancy overweight/obesity and excess gestational weight gain, cumulatively raise its prevalence which further increase the risk for postnatal adverse outcomes for both the mothers and their children. Emergent public health policies and strategies should be promoted to confront the predominant maternal risk factors-related with caesarean sec-tion and inform future mothers how to be prevented from them by applying healthier nutritional and lifestyle habits and to select caesarean section only due to emergency medical reasons. Alarmingly enough, targeted nutritional intervention strategies are strongly recommended to ef-fectively reduce the prevalence of maternal pre-pregnancy overweight/obesity and the excess gestational weight gain, which in turn may minimize the risk of childhood overweight/obesity.
Keywords:
caesarean section
; pre-pregnancy
; overweigh
; obesity
; gestational weight gain
; preterm birth
; pregnancy complications
; nutritional interventions
; maternal risk factors
1. Introduction
Caesarean section constitutes an important medical procedure for saving mothers’ and children’ lives in emergency obstetric conditions, contributing to reduction of their morbidity and mortality [1]. The World Health Organization (WHO) recommends a caesarean section rate close to 10%-15% of all births [2]. However, over the past two decades, there has been an exponential increase in caesarean section deliveries, reaching ‘epidemic proportions’ worldwide [3]. This is an important public health issue since while caesarean sections can be lifesaving, they can also negatively affect maternal and child health [1,2,3].
In Greece, this situation is even worse, since more than half of childbirths occur by caesarean section, rendering it one of the countries with the highest caesarean section rates in the world. Alarmingly enough, caesarean section rates in Greece elevated by approximately 50% from 1983 to 1996 [4]. Notably, a Greek study by Mossialos et al. documented a 41.6% caesarean section rate in 2 public hospitals and a 53% caesarean section rate in a private hospital [5]. Based on these results, the authors supported that obstetricians tend to perform a caesarean section for economic and convenience reasons [5,6]. In this aspect, a large-scale, population-based study clearly indicated that the rate of caesarean section, have continuously and more rapidly increased for women delivering in private health care units compared to those delivering in public hospitals [7].
WHO strongly supported that population caesarean section rates above 10% are not related with a decrease in mothers and matched children morbidity and mortality rates, while caesarean sections should ideally be applied merely when there are strong medical recommendations [8]. In addition, caesarean section, as any other major surgical operation, is related with several short and long-term adverse outcomes, such as greater risk of uterine rupture, ectopic pregnancy, fetal death, premature delivery, and psychiatric symptoms [9,10]. Importantly, there are several short-term risks of caesarean sections for neonates such as diminished immune development, greater probability of allergy, atopy, and asthma [9], as well as increased respiratory and obesity complications [11,12].
In the last few years, several epidemiological studies have supported that the rising rates of caesarean sections may be associated with specific maternal risk factors. In support of this view, pre-pregnancy maternal obesity has been considered as a significant risk factor for caesarean delivery, even if some studies were characterized by certain limitations [13,14]. Moreover, mothers’ age lower than 30 years was shown to decrease the risk of comorbidities related with caesarean section, whereas older maternal age, i.e., 35 years or more, was shown to considerably enhanced the rate of caesarean sections and their adverse outcomes [15]. Several previous studies also indicated that residency, women's education, wealth, and parity may considerably increase caesarean section rates; however, there are also studies which did not confirm these associations [16].
Furthermore, excess gestational weight gain above the Institute of Medicine (IOM) recommendations has been linked with elevated rates for caesarean section [17]. There are also certain studies supporting evidence that caesarean section might be a risk factor of preterm birth, but other studies did not confirm this finding [18,19], reinforcing the need for further investigation. Women developing gestational diabetes also have a greater likelihood of pre-eclampsia and delivering by caesarean section [20], which further leads postnatally to increasing rates of type 2 diabetes and hypertension-related disorders [21]. Several evidence has also shown that mothers who deliver by caesarean section may be less probable to breastfeed, and/or more probable to delay breastfeeding initiation which may lead to increased rates of maternal and childhood adverse outcomes [22]. Moreover, in parallel with the gradually increasing prevalence of caesarean sections worldwide, there is also a considerable rise in planned caesarean sections often without a clear medical reason, which may lead to rising rates of iatrogenic premature birth, and, in turn, potential adverse childhood outcomes [23]. In view of all the above, the present cross-sectional study aims to assess the potential associations of several maternal sociodemographic, anthropometric, lifestyle and perinatal maternal factors with the rates of caesarean section in a nationally representative population in Greece considering multiple potential confounding factors.
2. Materials and Methods
2.1. Study Population
In the present study, 7191 women were primarily enrolled from 11 geographically different Greek regions, rural, urban and islands (Athens, Thessaloniki, Larisa, Kavala, Alexandroupolis, Ioannina, Patra, Kalamata, Crete, South and North Aegean). The inclusion criteria for the primary enrollment were women with a singleton birth 2-5 years before enrollment, independently of parity, and who had no pregnancy at the interval between the time of this singleton birth and the time of study, i.e., 2-5 years postpartum. In multiparous women, merely the last pregnancy was considered. Recruitment to the study was between May 2016 and September 2020. All participants’ information was confidential. All participants were informed about the purpose of the study and signed a consent form in which they approved that their personal data may be published. Sample size estimation was established using PS: Power and Sample Size calculator program, while the randomization was conducted using a sequence of random binary numbers (i.e., 001110110 in which 0 represented enrolment and 1 not enrolment to the study). Among 7191 primarily enrolled women, 766 women (10.7%) were excluded due to lost or incomplete data, leading to a final response rate equal to 89.3%. Among the remaining 6425 women, 1243 (19.4%) of them were then excluded because of any history of disease. A total of 5182 healthy women were included in the final analysis, leading to a final response rate equal to 72.1%. The study was approved by the Ethics Committee of the University of the Aegean (ethics approval code: no 12/14.5.2016) and was in compliance with the World Health Organization (52nd WMA General Assembly, Edinburgh, Scotland, 2000). The exclusion criterion was any disease for the enrolled women except for gestational diabetes and pregnancy induced hypertension.
2.2. Study Design
At the time of study, i.e., 2-5 years postpartum, certified semi-quantitative questionnaires were applying for evaluating various sociodemographic and lifestyle factors of the study population [22,24]. Women weight at the first weeks of gestation and right before the delivery were recovered from their personal gynecologists’ or hospitals’ medical records in which measured weight data had been assessed during their visits to public or private health care units. Gestational weight gain was estimated by subtracting the recovered measured weight of the first weeks of gestation from the recovered measured weight right before the delivery. At the time of study, women weight and height were also measured by trained nutritionists, dietitians or physicians as per protocol, i.e., 2-5 years postpartum [22,24]. Weight was measured utilizing the same electronic scale, and height was measured utilizing a portable stadiometer [22,24].
Smoking habits, educational level, economic status, age, nationality, and parity status were recovered by the given questionnaires 2-5 years postpartum and were based on women memory recall. In fact, educational level was estimated based on the sum of years of education and financial status was categorized according to the yearly family income as: 0 ≤ 5000€, 1 ≤ 10000€, 2 ≤ 15000€, 3 ≤ 20000€, 4 ≤ 25000€ and 5 ˃ 25000€. Financial status was further categorized as low for yearly income ≤ 10000€, medium for yearly income ˃10000€ and ≤ 20000€, and high for yearly income ˃ 20000€. Additionally, the mode of delivery (vaginal or caesarean section) and maternal prenatal outcomes (gestational diabetes and gestational hypertension) were also recorded. The cohort was additional categorized based on the hospital type of delivery in women delivering in public hospitals and in those giving a birth in private hospitals. Among the women who delivered by caesarean section, the type of delivering was additional categorized as planned or emergency caesarean delivery.
Additionally, mothers were questioned whether they were exclusively breastfeeding for at least four months. To overcome recall bias, the women were answered for exclusive breastfeeding for at least four months because at this time point most of them were advised to progressively insert pulp foods to the nourishing practices of their children and they therefore recalled more accurately this time point, rendering their answers more consistent [22,24]. In contrast, mothers who breastfed for shorter periods, they were not able to respond with absolute certainty about the precise period of breastfeeding [22,24].
Mothers were also questioned to report if they had a preterm birth (< 37th week) and their answers were additional cross-checked by their medical files for more precise records for the exact week of preterm birth to be achieved. Nevertheless, we detected that there were several lost data regarding the precise week of preterm birth in the medical records and several of them did not come to an agreement with the mothers’ responses and thus preterm birth was treated as binary outcome as before and after of 37th week of pregnancy. Women history for gestational diabetes and gestational hypertension were also recovered from their personal medical documents.
Explaining directions were thoroughly given to the participants by registered nutritionists, dietitians and physicians concerning the completion of questionnaires, while a detailed demonstration of the questions to enable precise responses was rigorously accomplished.
2.3. Statistical Analysis
Statistical analysis was accomplished by Student’s t-test and one-way ANOVA for continuous variables found to follow normal distribution. Normality distribution was evaluated by Kolmogorov-Smirnov test. Chi-square test was utilized for categorical variables. Mann-Whitney non-parametric test was applied for non-normally distributed continuous variables between two groups, while Kruskal-Wallis non-parametric test was performed for non-normally distributed variables between three or more groups. The normally distributed quantitative variables are stated as mean value ± Standard Deviation (SD), the quantitative non-normally distributed continuous variables are given as median value (Interquartile Range, IQR), and the qualitative variables as absolute or relative frequencies. Multivariate logistic regression analysis was performed to evaluate whether the type of delivery (caesarean section vs vaginal) is independently related with mothers’ sociodemographic, anthropometric and lifestyle factors and maternal perinatal outcomes by adjusting for several possible confounding factors. Differences were considered significant at p < 0.05 and 95% Confidence Interval. The statistical analysis of the survey data was accomplished by Statistica 10.0 software, Europe (Informer Technologies, Inc., Hamburg, Germany).
3. Results
3.1. Descriptive Statistics of the Study Population
The present study finally enrolled 5182 healthy, reproductive-aged women with a mean age of 37.5 ± 4.8 years. Regarding their ethnicity, 95.7% of the women were Greek and the resting 4.3% were of other nationalities (Russian, Albanian, Ukrainian, Bulgarian, Romanian). Concerning educational level of the mothers, the mean years of education were 14.5 ± 2.8 years (range: 6-18 years). As far as the economic status as concern, 46.2% of the participant women stated low yearly income, 45.1% medium and 8.7% high yearly income. Additionally, 25.6% of the women were smokers, pre-pregnancy.
Caesarean section was performed in 56.4% of the mothers and vaginal delivery in the remaining 43.6%. Concerning the type of hospital where the deliveries were performed, 51.5% of them were completed in private hospitals and 48.5% in public hospitals. Among caesarean sections, 47.5% were planned and 52.5% were emergency caesarean section deliveries.
The mean Body Mass Index (BMI) of the women before pregnancy was 22.7±3.7 Kg/m2 (range: 15.9-37.6 Kg/m2). Pre-pregnancy, 17.5% of the women were affected by overweight, and 5.0% were affected by obesity, based on their BMI status, and therefore in total an incidence of 22.5% pre-pregnancy overweight/obesity was noted. The mean gestational weight gain was 13.8±6.1 Kg (range 4.0-45.0 Kg).
Almost half of women (49.7%) did breastfeed exclusively for at least 4 months (mean duration: 4.8±1.9 months), and 50.3% of them did not exclusively breastfeed for at least 4 months or did not breastfeed at all. An incidence of preterm birth (<37th week) equal to 30,1% of the study population was documented. Regarding parity, 64.2% of women stated that they were nulliparous (non-previous birth) and the remaining 35.8% were multiparous (at least one previous birth). Also, 4.3% of the women diagnosed with gestational diabetes mellitus during their pregnancy, and 4.1% of the women diagnosed with gestational hypertension.
3.2. Associations of the Mode of Delivery with Sociodemographic, Anthropometric and Lifestyle Characteristics of the Participant Women
Maternal age was significantly higher amongst the women giving a child by caesarean section than those delivered vaginally (Figure 1A, Table 1, 38.2±5.0 vs 36.6±4.4 years old, p=0.0001). Women who delivered by caesarean section had significantly higher pre-pregnancy BMI values compared to those who delivered vaginally (Figure 1B, Table 1, 23.1±3.8 vs 22.1±3.4 Kg/m2, p=0.0001). In crosstabulation, women performing caesarean section showed a significantly higher prevalence of pre-pregnancy overweight/obesity than those delivering vaginally (Table 1, p˂0.0001). Women delivered by caesarean section were significantly more frequently smokers compared to those delivered vaginally (Table 1, p=0.0004). Women with elevated educational level considerably more often delivered by caesarean section than those with lower educational level (Figure 1C, Table 1, p=0.0011). Women with higher economic status significantly more frequently performed caesarean section than those of lower economic status (Table 1, p=0.0117). Caesarean section was marginally but not significantly more frequently performed in multiparous women than nulliparous women (Table 1, p=0.0638). Women performing caesarean section had a significantly lower prevalence for exclusive breastfeeding compared to those performing vaginal delivery (Table 1, p˂0.0001). There was no significant difference between Greek women and those of other ethnicities as far as the mode of delivery is concerned (Table 1, p˃0.05).
3.3. Associations of Mode of Delivery with Maternal Perinatal Factors
Women performing caesarean section had significantly higher gestational weight gain compared to those delivering vaginally (Figure 1C, Table 1, p˂0.0001). Women performing caesarean section had a significantly greater prevalence of preterm birth than those performing vaginal delivery (Table 1. p˂0.0001). The rates of the caesarean sections were significantly higher in private hospitals than public hospitals (Table 1, p=0.0001). Private hospitals were associated with a significantly higher prevalence of planned caesarean sections (56.1%) than emergency ones (43.9%), whereas public hospitals were related with a considerably greater prevalence of emergency caesarean sections (63.4%) than planned ones (36.6%) (p = 0.0001, data not shown). Non-significant associations between mode of delivery and gestational diabetes and hypertension were noted (Table 1, p˃0.05).
3.4. Multivariate Regression Analysis for Mode of Delivery by Adjustment for Multiple Confounding Factors
In the multivariate logistic regression analysis, the type of delivery was independently related with maternal age, pre-pregnancy BMI, economic status, smoking habits, gestational weight gain, preterm birth, exclusive breastfeeding, and type of hospital delivery after adjustment for multiple confounders (Table 2). Women of older age (≥ 37.5 years) had a 58% higher probability to perform caesarean section compared to those of younger age (˂37.5 years) (Table 2, p=0.0048). Pre-pregnancy overweight and obese women had a 2-fold greater probability of performing caesarean section compared to underweight and normal weight women (Table 2, p=0.0008). Women of high economic status had a 31% greater risk of delivering by caesarean section than those of low or medium economic status (Table 2, p=0.0387). Smoker women showed a 72% higher probability of performing caesarean section than no smokers (Table 2, p=0.0412).
Women with higher rates of gestational weight gain (≥ 13.8 Kg) had a 26% increased risk of delivering by caesarean section than those with lower rates (˂13.8 Kg) (Table 2, p=0.0094). An 84% higher likelihood of preterm birth was recorded in women performing caesarean section than those delivering vaginally (Table 2, p=0.0012). Women delivered by caesarean section had a 56% higher risk of not breastfeeding exclusively than those delivering vaginally (Table 2, p=0.0002). Caesarean sections had a two-fold higher probability to be performed in a private hospital than in a public hospital (Table 2, p=0.0021). Maternal nationality, educational level, gestational diabetes, and pregnancy induced hypertension was not associated with the mode of delivery in multivariate analysis (Table 2, p˃0.05).
4. Discussion
In the last two decades, there is a continuously rise in caesarean section rates worldwide with considerable public attention and argument, on both the reasons and the adverse effects of this rise as the causes for this increase remain not fully understood [1,2,3]. More to the point, caesarean section rates have gradually risen to 19% worldwide with no notable difference on maternal and neonatal morbidity and mortality, while in the southeastern European countries, they have risen to or above 50% of total deliveries [25,26]. In Greece, in 2005, a 41.6% caesarean section rate in two public hospitals and an even higher at a 53% rate in a private hospital were previously reported; however, larger studies are recommended to confirm these rising rates [5].
In agreement with the above increasing trends, the current study revealed a 56.4% caesarean section rate during the period 2016-2020, in a nationally representative sample from 11 geographically diverse regions, rural, urban and islands, in Greece. Alarmingly enough, we found that private hospitals had a higher prevalence of caesarean sections than public hospitals and that the increasing rates of planned caesarean sections were more frequent in private hospitals than public hospitals. This association was sufficiently established in private hospitals where planned caesarean sections were clearly more frequent than emergency once. In this aspect, a systematic review of 17 studies suggested that several individual and social maternal reasons, involving fear of pain during childbirth and perceived inequality and inadequacy of care, contributed to the increased incidence of caesarean section delivery on maternal requests [27]. In accordance with our study, a greater incidence of caesarean section deliveries in private hospitals than public hospitals has been documented in several previous studies [28,29]. These growing caesarean sections rates in private health care centers may be ascribed to the economic benefits of caesarean delivery for private institutions because of decreased birthing time, the subsequent capability of the hospital to attend more deliveries, and the higher cost of caesarean delivery [28,29]. This fact may also explain the greater prevalence of planned caesarean sections in private hospitals than public hospitals. In view of the above, the significant relationship between increased rates of caesarean sections and better economic status found in the present study seems not to be random.
There is currently quite a lot of evidence that caesarean sections have been associated with multiple maternal risk factors. However, some of the existing findings seem inconsistent and inconclusive, providing rather contradictory results at least for certain maternal risk factors. Currently, there is substantial evidence that older maternal age, i.e., 35 years or more, considerably increases the rate of caesarean sections and their adverse outcomes [15,30]. In line with the above findings, we found a significantly higher age in women performing caesarean section compared to those delivering vaginally, independently of multiple confounding factors which are also linked with raised probability of caesarean section delivery. In this aspect, it should be noted that as maternal age increases, considerably over 35 years, the probability of prenatal and perinatal complications raises [31]. Usually observed adverse clinical outcomes amongst pregnant mothers over 35 years comprise of gestational diabetes, preeclampsia, placenta previa, placental abruption, preterm delivery, low birth weight, small-for-gestation-age infants, fetal distress, intrauterine fetal death, gestational hypertension, and increased perinatal morbidity and mortality [32].
Moreover, several studies in both developed and developing countries reported that women of greater socioeconomic backgrounds delay childbearing until they reach the age of 30 years or older to carry out their education, obtain a job, and become economically secure before giving children [33,34]. Certain studies also documented that residency, women's education, wealth, and parity may significantly be associated with caesarean section rates [16]. In support of this view, we found that women performing caesarean section had higher educational level and better economic status than those delivering vaginally; however, these associations were attenuated after adjusting for confounding factors. Multiparity also showed a marginal trend of correlation with caesarean section, at a non-significant level though.
There is strong evidence which suggests that maternal pre-pregnancy overweight and obesity increases the probability of caesarean delivery [14,34,35]. Moreover, overweight, and obese women who had a caesarean section experienced more adverse outcomes when compared to normal weight women with a caesarean section or obese women with a vaginal delivery [36]. In this aspect, the recommended strategies to reduce caesarean section have included measures to prevent maternal overweight and obesity [17]. In line with the above evidence, we found a greater prevalence of pre-pregnancy overweight and obesity in women delivering by caesarean section than those performing vaginal delivery, independently of multiple confounding factors.
There are also previous studies supporting evidence that excess gestational weight gain above the Institute of Medicine (IOM) guidelines may increase the rates of caesarean section delivery, and this proportion is expected to increase as the incidence of overweight and obesity rises [17]. In line with the existing knowledge, the present study demonstrated that women performing caesarean section had significantly higher rates of gestational weight gain than those delivering vaginally. In this aspect, it should be noted that only some women are usually advised about the IOM recommendations for gestational weight gain and even less are informed about the significance of supporting a healthy weight status before pregnancy [37]. This signifies a lost prospect for effective prevention of pregnancy complications, since it has been reported that only 12% of women were advised correctly by health care providers, which suggests an urgent demand for improved women education [38].
Caesarean section has also been considered as a probability factor for preterm birth in previous studies [18,19,39]. However, there are also studies that did not support this association, while it remains unknown whether the association between caesarean section and preterm birth is causal [18,19,39]. Compared with vaginal delivery, caesarean section in the second stage of labor was related with enhanced rates of subsequent spontaneous preterm birth at less than 37 weeks of pregnancy, and early spontaneous preterm birth at less than 34 weeks of pregnancy [19]. Alarmingly enough, preterm birth is the primary cause of mortality and morbidity in early childhood with a projected worldwide rate of 10,6% and about 15 million deliveries yearly [40]. In accordance with the above studies, we found a positive association between caesarean section prevalence and preterm birth, independently of multiple confounding factors such as maternal age, overweight/ obesity, excessive gestational weight gain, gestational diabetes, and hypertension.
Pregnant women developing gestational diabetes had a higher probability of delivering by caesarean section [20], which may further increase the probability of diabetes mellitus type 2 and hypertension disease in mothers at the next stages of their life [21]. Preterm delivery, macrosomia, abortion, pulmonary distress, stillbirth, and neonatal deaths have been considered among the most common outcomes of gestational diabetes [20,21]. However, in our study, we found non association between caesarean section prevalence and gestational diabetes. In this point of view, it should be noted that a significant percentage of women in our study had increased pre-pregnancy BMI as well as excessive gestational weight gain. These contributing factors cannot be excluded in the overall analysis of delivery mode, since both pre-pregnancy BMI and gestational weight gain were related with higher rates of caesarean section, and they may act as confounding factors ameliorating the association of gestational diabetes with caesarean section [41]. Moreover, an increase in caesarean deliveries has been associated with elevated incidence for maternal pregnancy-induced hypertension [42,43]. However, in our study, we found only a marginal non-significant trend of correlation between caesarean section and gestational hypertension which may be ascribed to the low number of women developing gestational hypertension included in our study population.
Caesarean section has previously been identified as an autonomous probability factor of the incompetence to begin and maintain breastfeeding, reducing the risk of any, predominant and exclusive breastfeeding from discharge to 6 months postpartum [44,45]. In a recent scoping review analyzing 16 demographic surveys, Sonedo et al. documented that caesarean deliveries were linked to a greater probability of postponed initiation of breastfeeding as well as early interruption of exclusive breastfeeding [46]. The above findings were further confirmed by our study highlighting the need to reduce caesarean section rate and give specific breastfeeding assistance during early postpartum period to the mothers.
The interpretation of the findings of the present study should be made with some limitations in mind. It should be noted that BMI was utilized to distinguish maternal overweight and obesity. Nevertheless, direct measures of body fat mass and distribution are required to extend and verify our results. Additionally, recall bias was inherent in our study since several potential risk factors were self-reported by women. Moreover, in spite of a careful approach to confounding adjustment, we recognize the probability of unmeasured confounding. Even though we have adjusted for maternal age, nationality education, economic status, smoking habits, parity and other maternal perinatal factors, it is still probable that residual confounding may affect our findings, while additional lifestyle or health-related factors, like maternal physical activity and mental health status, should be included in adjusted multivariate models. The study sample is enough adequate and representative since it includes women from 9 geographically diverse areas of Greece. However, large scale, population-based, epidemiologic surveys with sample from additional regions of the country, urban, rural and island areas are necessary for more reliable conclusions concerning the Greek population to be drawn. In addition, no conclusions about causality can be made because of the cross-sectional design of our study despite its nationally representative nature.
5. Conclusions
This is a cross-sectional, nationally representative study in women of reproductive age which supported evidence that advanced maternal age, pre-pregnancy overweight/obesity, excess gestational weight gain, higher rates of preterm birth, better economic status and smoking habits were considerably related with elevated probability of caesarean section, independently of multiple confounding factors. The incidence of the caesarean section deliveries recorded in the present cohort was far above the WHO recommendations and especially those performing in private health care units. However, the present findings should be confirmed by future large-scale, population-based clinical trials. Moreover, to address the excess of caesarean deliveries, particularly in private centers, future strategies, and policies for stricter diagnosis of the medical indications for caesarean delivery and for preventing incentives for caesarean delivery should be accomplished.
Emergent public health policies and strategies should also be promoted to confront the predominant maternal risk factors-related with caesarean section and inform future mothers how to be prevented from them by applying healthier nutritional and lifestyle habits and to select caesarean section only due to emergency medical reasons. Alarmingly enough, targeted nutritional intervention strategies are strongly recommended to effectively reduce the prevalence of maternal pre-pregnancy overweight/obesity and the excess gestational weight gain, which in turn may minimize the risk of childhood overweight/obesity. In this aspect, nutritional intervention studies applying healthy dietary patterns such as Mediterranean Diet may be proved very efficiently both before and during the gestation for controlling body weight of reproductive-aged women, minimizing the risk of perinatal complications and increasing the probability for healthier newborns with physiological birth body weight, and reducing risk of development of pathological states during childhood such as overweight/obesity childhood asthma, diabetes mellitus, e.t.c.
Author Contributions
Conceptualization, S.K.P.; D.P.; G.T.; and C.G.; methodology, E.P. (Eleni Pavlidou); M.S.; G.T.; and C.G.; validation, E.P. (Evmorfia Psara); M.M.; and M.S.; formal analysis, E.P. (Eleni Pavlidou); S.K.P.; D.P..; A.S.; investigation, E.P. (Eleni Pavlidou); O.A.; and C.G.; resources, S.K.P.; O.A.; M.S.; G.T.; G.V.; and E.T.; data curation, E.P. (Eleni Pavlidou); O.A.; E.P. (Evmorfia Psara); M.M.; A.S.; G.V.; and E.T.; writing—original draft preparation, E.P. (Eleni Pavlidou); and C.G.; writing—review and editing, E.P. (Eleni Pavlidou); D.P; and C.G.; visualization, S.K.P.; D.P.; G.T.; and C.G.; supervision, C.G.; project administration, C.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of the Aegean (ethics approval code: no 12/14.5.2016) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Research data is available upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Betran, A.; Torloni, M.R.; Zhang, J.J.; et al. WHO statement on caesarean section rates. BJOG 2016, 123, 667–670. [Google Scholar] [CrossRef] [PubMed]
- Betrán, A.P.; Ye, J.; Moller, A.B.; et al. The increasing trend in caesarean section rates: global, regional and national estimates: 1990-2014. PLoS One 2016, 11, e0148343. [Google Scholar] [CrossRef] [PubMed]
- Betran, A.P.; Ye, J.; Moller, A.B.; et al. Trends and projections of caesarean section rates: global and regional estimates. BMJ Glob Health 2021, 6, e005671. [Google Scholar] [CrossRef]
- Skalkidis. Y.; Petridou, E.; Papathoma, E.; et al. Are operative delivery procedures in Greece socially conditioned? Int J Qual Health Care 1996, 8, 159–165. [Google Scholar] [CrossRef]
- Mossialos, E.; Allin, S.; Karras, K.; et al. An investigation of Caesarean sections in three Greek hospitals: the impact of financial incentives and convenience. Eur J Public Health 2005, 15, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Giaxi, P.; Gourounti, K.; Vivilak,i V. G.; et al. Which classification system could empower the understanding of caesarean section rates in Greece? A review of systematic reviews. Eur J Midwifer. 2022, 6, 39. [Google Scholar] [CrossRef]
- Einarsdóttir, K.; Haggar, F.; Pereira, G.; et al. Role of public and private funding in the rising caesarean section rate: a cohort study. BMJ Open 2013, 3, e002789. [Google Scholar] [CrossRef]
- Visser, G.H.; Ayres-de-Campos, D.; Barnea, E.R.; et al. FIGO position paper: How to stop the caesarean section epidemic. Lancet 2018, 392, 1286–1287. [Google Scholar] [CrossRef]
- Sandall, J.; Tribe, R.M.; Avery, L.; et al. Short-term and long-term effects of caesarean section on the health of women and children. Lancet 2018, 392, 1349–1357. [Google Scholar] [CrossRef]
- Dekel, S.; Ein-Dor, T.; Berman, Z.; et al. Delivery mode is associated with maternal mental health following childbirth. Archiv Womens Ment Health 2019, 22, 817–824. [Google Scholar] [CrossRef]
- Blustein, J.; Liu, J. Time to consider the risks of caesarean delivery for long term child health. BMJ. 2015, 350, h2410. [Google Scholar] [CrossRef]
- Visser, G.H. Women are designed to deliver vaginally and not by cesarean section: An obstetrician's view. Neonatology 2015, 107, 8–13. [Google Scholar] [CrossRef]
- Brizan JB, Amabebe E. Maternal obesity as a risk factor for caesarean delivery in Sub-Saharan Africa: A systematic review. Life (Basel) 2022, 12, 906. [Google Scholar] [CrossRef]
- Dal' Maso, E.; Rodrigues, P.R.M.; Ferreira, M.G.; et al. Cesarean birth and risk of obesity from birth to adolescence: A cohort study. Birth 2022, 49, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Das, P.; Samad, N.; Sapkota, A.; et al. Prevalence and factors associated with caesarean delivery in Nepal: Evidence from a nationally representative sample. Cureus 2021, 13, e20326. [Google Scholar] [CrossRef]
- Bhandari, A,K. ; Dhungel, B.; Rahman, M. Trends and correlates of cesarean section rates over two decades in Nepal. BMC Pregnancy Childbirth 2020, 20, 763. [Google Scholar] [CrossRef]
- Dzakpasu, S.; Fahey, J.; Kirby, R.S.; et al. Contribution of prepregnancy body mass index and gestational weight gain to caesarean birth in Canada. BMC Pregnancy Childbirth 2014, 14, 106. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, D.M.; Larson, J.; Jacobsson, B.; et al. Cross-country individual participant analysis of 4.1 million singleton births in 5 countries with very high human development index confirms known associations but provides no biologic explanation for 2/3 of all preterm births. PLoS One 2016, 11, e0162506. [Google Scholar] [CrossRef]
- Williams, C.; Fong, R.; Murray, S.M.; et al. Caesarean birth and risk of subsequent preterm birth: a retrospective cohort study. BJOG. 2021, 128, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Fiolna, M.; Kostiv, V.; Anthoulakis, C.; et al. Prediction of adverse perinatal outcome by cerebroplacental ratio in women undergoing induction of labor. Ultrasound Obstet Gynecol. 2019, 53, 473–80. [Google Scholar] [CrossRef]
- Darbandi, M.; Rezaeian, S.; Dianatinasab, M.; et al. Prevalence of gestational diabetes and its association with stillbirth, preterm birth, macrosomia, abortion and cesarean delivery: a national prevalence study of 11 provinces in Iran. J Prev Med Hyg. 2022, 62, E885–E891. [Google Scholar] [CrossRef]
- Mantzorou, M.; Papandreou, D.; Vasios, G.K.; Pavlidou, E.; Antasouras, G.; Psara, E.; Taha, Z.; Poulios, E.; Giaginis, C. Exclusive breastfeeding for at least four months is associated with a higher prevalence of overweight and obesity in mothers and their children after 2-5 years from delivery. Nutrients 2022, 14, 3599. [Google Scholar] [CrossRef] [PubMed]
- Coates, D.; Homer, C.; Wilson, A.; et al. Indications for, and timing of, planned caesarean section: A systematic analysis of clinical guidelines. Women Birth 2020, 33, 22–34. [Google Scholar] [CrossRef]
- Koutelidakis, A.E.; Alexatou, O.; Kousaiti, S.; Gkretsi, E.; Vasios, G.; Sampani, A.; Tolia, M.; Kiortsis, D.N.; Giaginis, C. Higher adherence to Mediterranean diet prior to pregnancy is associated with decreased risk for deviation from the maternal recommended gestational weight gain. Int Food Sci Nutr. 2018, 69, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Molina G, Weiser TG, Lipsitz SR, et al. Relationship between caesarean delivery rate and maternal and neonatal mortality. JAMA. 2015, 314, 2263–2270. [Google Scholar] [CrossRef] [PubMed]
- Berman, Y.; Ibiebele, I.; Patterson, J.A.; et al. Rates of stillbirth by maternal region of birth and gestational age in New South Wales, Australia 2004-2015. Aust N Z J Obstet Gynaecol. 2020, 60, 425–432. [Google Scholar] [CrossRef]
- McCourt, C.; Weaver, J.; Statham, H.; et al. Elective caesarean section and decision making: a critical review of the literature. Birth 2007, 34, 65–79. [Google Scholar] [CrossRef] [PubMed]
- Béhague, D.P. Beyond the simple economics of cesarean section birthing: women’s resistance to social inequality. Cult Med Psychiatry 2002, 26, 473–507. [Google Scholar] [CrossRef]
- Jahnke, J.R.; Houck, K.M.; Bentley, M.E.; et al. Rising rates of cesarean delivery in Ecuador: Socioeconomic and institutional determinants over two decades. Birth 2019, 46, 335–343. [Google Scholar] [CrossRef]
- Attali, E.; Yogev, Y. The impact of advanced maternal age on pregnancy outcome. Best Pract Res Clin Obstet Gynaecol. 2021, 70, 2–9. [Google Scholar] [CrossRef]
- Genc, S.; Emeklioglu, C.N.; Cingillioglu, B.; et al. The effect of parity on obstetric and perinatal outcomes in pregnancies at the age of 40 and above: a retrospective study. Croat Med J. 2021, 62, 130–136. [Google Scholar] [CrossRef]
- Janoud. ; Kelly, S.; Yasseen, A.; et al. Factors associated with increased rates of caesarean section in women of advanced maternal age. J Obstet Gynaecol Can. 2015, 37, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Budds, K.; Locke, A.; Burr, V. “For some people it isn’t a choice, it’s just how it happens”: Accounts of ‘delayed’ motherhood among middle-class women in the UK. Fem Psychol. 2016, 26, 170–187. [Google Scholar] [CrossRef]
- Muhammad, T.; Srivastava, S.; Kumar, P.; et al. Prevalence and predictors of elective and emergency caesarean delivery among reproductive-aged women in Bangladesh: evidence from demographic and health survey, 2017-18. BMC Pregnancy Childbirth 2022, 22, 512. [Google Scholar] [CrossRef]
- Jatta, F.; Sundby, J.; Vangen, S.; et al. Association between Maternal Origin, Pre-Pregnancy Body Mass Index and Caesarean Section: A Nation-Wide Registry Study. Int J Environ Res Public Health. 2021, 18, 5938. [Google Scholar] [CrossRef]
- Santos, S.; Voerman, E.; Amiano, P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American, and Australian cohorts. BJOG Int J Obstet Gynaecol. 2019, 126, 984–995. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.D.; Pullenayegum, E.; Taylor, V.H.; et al. Despite 2009 guidelines, few women report being counseled correctly about weight gain during pregnancy. Am J Obstet Gynecol. 2011, 205, 333. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, B.; Dzakpasu, S.; Heaman, M.; et al. The Canadian maternity experiences survey: an overview of findings. J Obstet Gynaecol Can. 2008, 30, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Barros, F.C.; de Lyra Rabello Neto, D.; Villar, J.; et al. Caesarean sections and the prevalence of preterm and early-term births in Brazil: secondary analyses of national birth registration. BMJ Open 2018, 8, e021538. [Google Scholar] [CrossRef]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: a systematic review and modelling analysis. Lancet Glob Health 2019, 7, e37–e46. [Google Scholar] [CrossRef]
- Lackovic, M.; Milicic, B.; Mihajlovic, S.; et al. Gestational Diabetes and Risk Assessment of Adverse Perinatal Outcomes and Newborns Early Motoric Development. Medicina (Kaunas) 2021, 57, 741. [Google Scholar] [CrossRef] [PubMed]
- Renes, L.; Barka, N.; Gyurkovits, Z.; Paulik, E.; Nemeth. G.; Orvos, H. Predictors of caesarean section - a cross-sectional study in Hungary. J Maternal-Fetal Neonat Med. 2017, 31, 1–5. [Google Scholar] [CrossRef]
- Panda, S.; Begley, C.; Corcoran, P.; Daly, D. Factors associated with cesarean birth in nulliparous women: A multicenter prospective cohort study. Birth 2022, 49, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Wang, Y.; Huang. J.; et al. The association between caesarean delivery and the initiation and duration of breastfeeding: a prospective cohort study in China. Eur J Clin Nutr. 2018, 72, 1644–1654. [CrossRef]
- Hoang Nguyen, P.T.; Binns, C.W.; Vo, Van Ha A.; et al. Caesarean delivery associated with adverse breastfeeding practices: a prospective cohort study. J Obstet Gynaecol. 2020, 40, 644–648. [CrossRef]
- Sodeno, M.; Tappis, H.; Burnham, G.; Ververs, M. Associations between caesarean births and breastfeeding in the Middle East: a scoping review. East Mediterr Health J. 2021, 27, 931–940. [Google Scholar] [CrossRef]
Figure 1.
Associations of the mode of delivery with: A) Maternal age, B) Maternal pre-pregnancy BMI, C) Maternal educational level and D) Gestational weight gain.
Figure 1.
Associations of the mode of delivery with: A) Maternal age, B) Maternal pre-pregnancy BMI, C) Maternal educational level and D) Gestational weight gain.
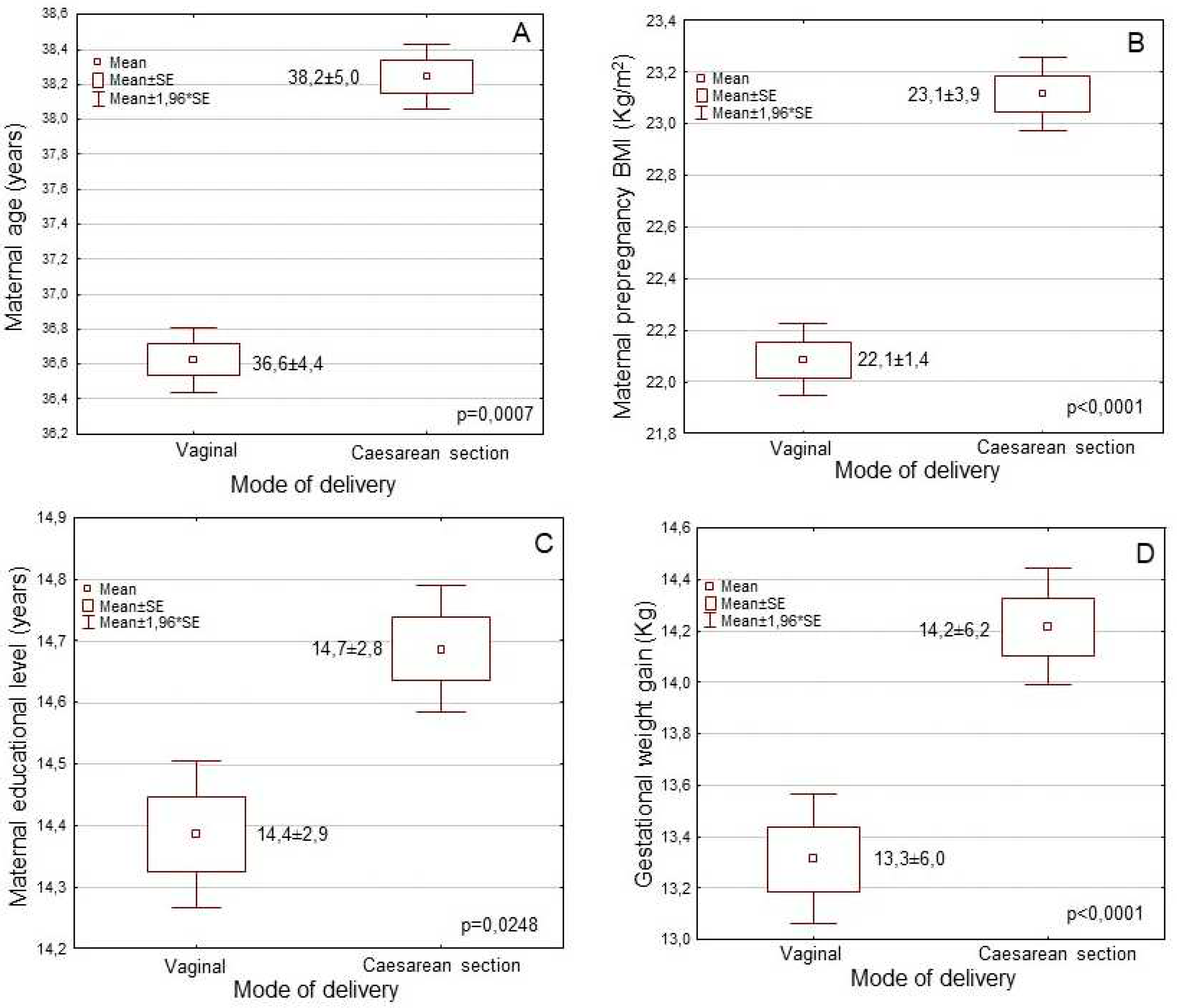

Table 1.
Associations of mode of delivery with maternal sociodemographic, anthropometric and lifestyle characteristics and maternal perinatal outcomes.
Table 1.
Associations of mode of delivery with maternal sociodemographic, anthropometric and lifestyle characteristics and maternal perinatal outcomes.
| Characteristics (n=5182) | Mode of delivery | ||
|---|---|---|---|
| Vaginal (43.6%) |
Caesarean (56.4%) |
p-value | |
| Mothers’ age (mean±SD; years) | 36.6±4.4 | 38.2±5.0 | p = 0.0001 |
| Mothers’ nationality (n, %) | p = 0.4735 | ||
| Greek | 2169 (95.9) | 2788 (95.5) | |
| Others | 93 (4.1) | 132 (4.5) | |
| Pre-pregnancy BMI (mean±SD;Kg/m2) | 22.1±3.4 | 23.1±3.8 | p = 0.0001 |
| Pre-pregnancy BMI status (n,%) | p < 0.0001 | ||
| Underweight | 98 (4.3) | 51 (1.8) | |
| Normal weight | 1751 (77.4) | 2118 (72.5) | |
| Overweight | 352 (15.6) | 553 (18.9) | |
| Obese | 61 (2.7) | 198 (6.6) | |
| Education level (mean±SD; years) | 14.3±2.9 | 14.7±2.8 | p = 0.0011 |
| Economic status (n, %) | p = 0.0117 | ||
| Low | 1082 (47.8) | 1315 (45.0) | |
| Medium | 1011 (44.7) | 1325 (45.4) | |
| High | 169 (7.5) | 280 (9.6) | |
| Smoking habits (n, %) | p = 0.0004 | ||
| No smokers | 1739 (76.9) | 2118 (72.5) | |
| Smokers | 523 (23.1) | 802 (275.) | |
| Parity (n, %) | p = 0.0638 | ||
| Nulliparity | 1484 (65.6) | 1843 (63.1) | |
| Multiparity | 778 (34.4) | 1077 (36.9) | |
| Gestational weigh gain (mean±SD; Kg) | 13.3±6.0 | 14.2±6.2 | p < 0.0001 |
| Preterm birth (<37th week, n, %) | p < 0.0001 | ||
| No | 1920 (84.9) | 1701 (58.3) | |
| Yes | 342 (15.1) | 1219 (41.7) | |
| Gestational diabetes (n, %) | p = 0.7019 | ||
| No | 2167 (95.8) | 2791 (95.6) | |
| Yes | 95 (4.2) | 129 (4.4) | |
| Pregnancy induced hypertension (n, %) | p = 0.1426 | ||
| No | 2179 (96.3) | 2789 (95.5) | |
| Yes | 83 (3.7) | 131 (4.5) | |
| Exclusive breastfeeding (n, %) | p < 0.0001 | ||
| No | 872 (38.6) | 1736 (59.5) | |
| Yes | 1390 (61.4) | 1184 (40.5) | |
| Hospital type of delivery (n, %) | p = 0.0001 | ||
| Public hospital | 1226 (54.2) | 1296 (44.4) | |
| Private hospital | 1036 (45.8) | 1624 (5.6) | |
Table 2.
Multivariate logistic regression analysis for caesarean section.
| Characteristics | Caesarean section | |
|---|---|---|
| HR* (95% CI**) | p-value | |
| Age (below / over mean value) | 1.58 (1.25-1.91) | p = 0.0048 |
| Nationality (Greek / other) | 0.97 (0.34-1.67) | p= 0.5503 |
| Pre-pregnancy BMI (underweight or normal / overweight or obese) | 2.14 (1.91-2.40) | p = 0.0008 |
| Education level (below / over mean value) | 1.43 (0.88-1.99) | p = 0.1705 |
| Economic status (low or medium / high) | 1.31 (0.92-1.76) | p = 0.0387 |
| Smoking habits (No / Yes) | 1.72 (1.28-2.38) | p = 0.0412 |
| Parity (Nulliparity / Multiparity) | 1.20 (0.83-1.73) | p = 0.1433 |
| Gestational weigh gain (below / over mean value) | 1.26 (0.96-1.62) | p = 0.0094 |
| Preterm birth (No / Yes) | 1.84 (1.59-2.09) | p=0.0012 |
| Gestational diabetes (No / Yes) | 1.07 (0.23-2.04) | p = 0.8498 |
| Pregnancy induced hypertension (No / Yes) | 1.18 (0.69-1.85) | p = 0.2085 |
| Exclusive breastfeeding (No / Yes) | 0.44 (0.19-0.68) | p = 0.0002 |
| Type of hospital of delivery (public / private) | 2.05 (1.78-2.41) | p = 0.0021 |
* Hazard Ratio: HR; ** CI: Confidence Interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



