
Submitted:
29 June 2023
Posted:
29 June 2023
You are already at the latest version
Abstract
Respiratory infections are usually characterized by mucus hypersecretion. This condition may worsen and prolong symptoms and signs. Mucoactive agents include different molecules with different mechanisms of action. Sobrerol is a monoterpene able to fluidify mucus, increase mucociliary clearance, and exert antioxidant activity. Sobrerol is available in various formulations (granules, syrup, nebulized, and suppository). Sobrerol has been on the market for over 50 years. Several studies investigated its efficacy and safety in acute and chronic respiratory diseases characterized by mucus hyperproduction. Seven pediatric studies have been conducted with favorable outcomes. Recently, regulatory agencies reduced the treatment duration to three days. Therefore, a future study will test the hypothesis that a combination of oral and topical sobrerol could benefit children and adults with frequent respiratory infections. The rationale considers that mucus accumulation could be a risk factor for increased susceptibility to have infections.
Keywords:
sobrerol
; mucolytic agent
; respiratory infections
1. Background on respiratory infections
Respiratory infections are extremely frequent diseases and constitute among the most frequent causes of access to primary care doctors, as recently reported by a systematic review including data from 12 countries across five continents [1]. Acute upper respiratory infections (AURIs) are prevalent and usually recognize a bacterial or viral cause, although viral forms are the most common [2]. Many viral agents may cause AURIs, but rhinovirus, coronavirus, syncytial, influenza, parainfluenza, adenovirus, coxsackievirus, echovirus, paramyxovirus, and enterovirus are the most common [3,4,5,6,7,8]. Moreover, viral respiratory infections are typically seasonal, such as increased infectivity during cold seasons [9]. Namely, exposure to cold exerts different mechanisms to promote respiratory infections, including impaired mucociliary clearance, deficient nasal defense, and reduced immune function [10].
Clinically, we have to consider that all respiratory viruses may induce an influenza-like illness (ILI), also named flu-like syndrome [11]. Indeed, ILI represents a typical acute viral illness and mimics the clinical feature of influenza [12]. Also, ILI is an acute medical condition characterized by general and respiratory symptoms. In particular, the definition of ILI (common throughout Europe) includes "any person who presents a sudden and rapid onset of at least one of the following general symptoms: fever or feverishness, malaise/exhaustion, headache, myalgia, and at least one of the following respiratory symptoms: cough, sore throat, and wheezing" [13]. However, if milder manifestations occur, the typical common cold has to be considered [14]. Even if AURI may be associated with lower respiratory tract involvement, a healthy and immunocompetent subject usually presents only symptoms concerning the upper respiratory tract. In addition, we must remember that common cold and ILI are umbrella terms that include different conditions, including rhinitis, sinusitis, pharyngitis, laryngitis, otitis, and tonsillitis [15].
These respiratory infections, mainly in children and adolescents, significantly burden the family and society from a social and economic perspective.
1. Practical management
From a clinical point of view, AURI management is generally grounded in a quick treatment that presumes a diagnosis usually based on clinical and epidemiological criteria [16]. The most common symptoms include sneezing, rhinorrhea, nasal congestion, hypo/anosmia, hypo/ageusia, facial pressure, sore throat, cough, headache, discomfort, myalgias, and low-grade fever [17]. Notably, these symptoms usually last less than ten days, apart from the cough, which tends to last longer [18]. Therefore, the treatment should be timely and appropriate for every single patient. However, if symptoms persist longer or worsen, a trivial common cold may evolve into rhinosinusitis, needing an appropriate work-up [19]. As mentioned above, it has to be underlined that the cough may last even for more than a month in some subjects [20]. Another aspect that has to be considered is that even if these symptoms commonly are self-resolving, they are still particularly annoying. The parents want to solve them immediately, mainly if a fever is present. Namely, fever often instills fear in parents, even unmotivated fear, so a real fever-phobia is generated [21].
Consequently, doctors prescribe symptomatic relievers as a first-line treatment [22]. The main goal of treatment is, in fact, the prompt reduction of symptom intensity and duration. It is vital to recommend to patients and parents that antibiotics should not be used unless a bacterial complication occurs [23]. Usually, NSAIDs, nasal lavage, and non-pharmacologic remedies are sufficient to cure rapidly the most acute viral infections [24]. Another aspect that we still need to consider has been further emphasized by the recent COVID-19 pandemic [25]. Indeed, we have to believe that facing an infection is always accompanied by inflammation [26]. As a result, inflammation dampening represents a leading therapeutical target in managing infections. The second lesson provided by COVID-19 infection concerns the dramatic outbreak of other respiratory infections that occurred successively. The explanation of this infections epidemy depends on the restrictive measure (lockdown, mask use, and social distancing) that significantly diminished the incidence of respiratory infections. The paradigmatic example was the negligible prevalence of bronchiolitis during the early COVID-19 pandemic [27]. However, since the slackening of restrictive measures, there has been a surge in cases of bronchiolitis that has put a strain on the pediatric hospital network [28]. Consistently, the 2022/2023 seasonal influenza epidemic had an early onset, extraordinary incidence, clinical severity, and persistent duration of the epidemic plateau [29]. Also, other respiratory infections spread at the same time [30]. Therefore, respiratory infections have become increasingly impactful in daily life. In this regard, a poorly trained immune system contributed significantly to this increased infection susceptibility. Consequently, careful management of respiratory infections is required today, considering all factors that could contribute to worsening the infection evolution.
1. The relevance of mucus hyperproduction in respiratory infections
The respiratory mucus secretion is a complex mixture produced by different structures, including submucosal glands and secreting epithelial cells (goblet cells and Clara cells) [31,32]. The submucosal glands are tubular/tubulacinar formations producing mucous, serous, or seromucous secretions. The goblets cells are mucous-secreting cells intercalated in the cylindrical ciliated epithelium lining, disappearing in the terminal bronchioles. The Clara cells are intercalated with the low or cubic cylindrical epithelium, ciliated or not, which extends in a single layer along the peripheral airways. These cells produce both a mucous secretion (like goblet cells) and a lipoprotein secretion (like type B pneumocytes), which can be identified as an alveolar surfactant.
The amount of mucus produced depends on the number of mucus-secreting cells present at that level, which in turn is related to the total surface area of the airways; thus, mucus production occurs more in the peripheral airways than in the central airways [33]. Physiologically, an adult produces about 10-100 mL of mucus per day, and the amount of mucus that reaches the trachea is approximately 10-20 mL/day [31,32]. The superficial layer constitutes the 'sol' phase of the mucus, very rich in water, about 3 microns thick, and occupies almost the entire length of the cilia of the epithelial cells [34]. Above, there is a dense layer: the 'gel' phase. It mainly contains glycoproteins (mucins), characterized by a central protein structure anchored to lateral polysaccharide chains formed by sialic acid (sialomucins) or fucose (fucosomucins). In the gel layer, molecules with anti-infective activity exist, such as secretory IgA (S-IgA), lactoferrin, and lysozyme. In addition, it has been hypothesized that a third layer consisting of surfactant exists between the sol and gel layers [33]. Usually, only the gel layer is transported, but the sol layer seems essential for mucus transport because it allows the cilia to beat effectively [35]. Mucus transport is governed by the mechanical forces of ciliary beating and airflow, counteracted by the friction and inertia of the mucus itself [36]. Mucociliary clearance is prevalent in the peripheral airways. Each ciliary cell has about 200 cilia, and the cilia are equipped with 'claws' that reach into the gel layer and push it toward the oropharynx [33,34]. The mucociliary clearance efficacy depends on the airflow velocity, which is a function of the airway diameter and the pressure the expiratory muscles create [32]. Moreover, in the first years of life, the small airways tend to collapse during normal breathing, and the ciliary machinery develops progressively [37].
Mucus hypersecretion is a common manifestation shared by many pathological conditions of both the upper airways (rhinitis, rhinosinusitis, pharyngitis, laryngitis) and the lower airways (acute and chronic bronchitis, bronchiectasis, and pneumonia) [37].
Initially, the hypersecretion of mucus represents a defense system: the increased thickness of the secretion promotes the clearance and dilution of soluble particles. The inflammatory vasodilatation increases the secretory activity of mucous cells and the production of immunoglobulin and complement fractions, enhancing the function of S-IgA. The quantitative increase in mucous secretion may be associated with changed viscoelastic characteristics of the mucus, resulting from the prevalence of neutral mucins (fucosomucins) over acidic mucins (sialomucins and sulphomucins). From a rheological point of view, neutral mucins are denser and more adhesive. Later, when hypersecretion becomes excessive, the defensive role diminishes and can worsen respiratory infection because of impaired mucociliary clearance, wall edema, and bronchial obstruction [38].
In chronic inflammation, the abundant secretions are only partially reabsorbed in the airways. Also, hypertrophy and hyperplasia of the secretory structures contribute to maintaining hypersecretion. In addition, vasodilatation and mucosal edema cause fluid supply into mucous glands, worsening hypersecretion [39]. In other words, a vicious circle starts and self-maintains: mucus hypersecretion fosters further hypersecretion. As a result, to stop this negative loop, "mucoactive" drugs may be helpful in clinical practice.
1. Muco-active drugs
Muco-active drugs are molecules able to modify viscous-elastic characteristics of mucus, promoting its clearance. This definition disregards the specific mechanism of action. In particular, mucolytic medications can reduce mucus viscosity by depolymerizing mucin glycoproteins. Mucolytics may be classified into two main groups: mucolytics with direct action and indirect action. Table 1 summarizes the classification of mucolytic agents based on the mechanism of action.
In clinical practice, mucoactive drugs may be a therapeutic option in medical conditions characterized by mucus hypersecretion [40]. In particular, mucolytics facilitate airway clearance in specific diseases, including bronchiectasis, bronchitis, cystic fibrosis, and rhinosinusitis, with abundant mucus production [41]. Also, mucolytics may relieve acute productive (wet) cough [41]. Several clinical studies investigated the usefulness of mucolytics in clinical practice. However, the evidence level generally was weak, mainly for methodological issues. Anyway, mucolytics are used, usually preferring consolidated molecules, including sobrerol.
1. Sobrerol
Sobrerol has been on the market in many European countries for over 50 years since its launch in the early 1970s. Sobrerol (5-hydroxy-α, α, 4-trimethyl-3-cyclohexene-1-methanol) is a monocyclic monoterpene with two hydroxyl functions. Various effects characterize it (Figure 1).
In particular, sobrerol in vivo increased mucus production and ciliary motility, thus improving mucociliary clearance [42]. In addition, sobrerol reduced the viscosity of tracheobronchial mucus without causing any alterations of the alveolar surfactants [43]. Radical scavenging activities have also been reported [44]. Finally, sobrerol may increase the production of secretory IgAs. Sobrerol is available in different formulations, including syrup, water-soluble sachets, nebulization, intramuscular (or intravenous) vials, and suppositories. The main indication is the treatment of respiratory disorders characterized by thick, viscous hypersecretion. The recommended oral dose in adults is 600 mg (equivalent to the contents of two sachets) per day for up to three days. In children, this dosage is halved. The dose administered by the aerosol route is one vial for nebulization, containing 40 mg of sobrerol, one to two times daily. Clinical studies in the literature have used a treatment duration of up to three months or a maximum daily dosage of 900 mg for ten consecutive days [40]. The only contraindication is used in children under 30 months of age or with a history of epilepsy or febrile convulsions, as well as hypersensitivity to the active ingredient or any of the excipients used in the various formulations. Particular precaution must, however, be observed in subjects with severe respiratory insufficiency, asthmatics, and debilitated patients, as the increased fluidity of secretions requires effective expectoration.
As sobrerol has been prescribed for over 50 years, numerous clinical studies have been conducted, especially in the 1970s and 1980s [45]. A recent review updated and synthetically reported some of them [40]. Globally, 25 studies were published, including 10 double-blind, randomized, and controlled trials and 15 open studies (controlled or non-controlled) concerning acute and chronic respiratory diseases in children and adults [46-70].
In particular, the published pediatric studies are seven, regarding different medical conditions; three were RCT, and four were open studies [46,55,57,65,68,70].
The first pediatric RCT study evaluated the efficacy and safety of oral sobrerol compared to oral N-acetylcysteine in 40 children with acute respiratory diseases (bronchitis or pharyngo-tracheobronchitis) [46]. For three days, Sobrerol was administered as granules in one-dose sachets at 100 mg/3 times a day. N-acetylcysteine granules were used at 300 mg/day for three days. Clinical parameters and biological data, including rheological examination of expectorate, were considered at baseline and the end of the course. The two treatments were effective without significant differences. However, sobrerol induced a better reduction of expectorate viscosity and was better tolerated than N-acetylcysteine. The second RCT study was conducted as double-blind, randomized, and placebo-controlled in 100 patients aged between 12 and 74 years with acute or chronic upper or lower respiratory infections [55]. Sobrerol syrup (260 mg) was administered with carbocysteine capsules (375 mg) four times a day for 21 days. This combination significantly improved objective and subjective clinical parameters and lung function compared to a placebo. In addition, the treatment was well tolerated. Unfortunately, pediatric outcomes could not be deduced. A third RCT study was conducted as double-blind, randomized, and placebo-controlled in 30 children with pertussis aged between 10 months and 12 years [56]. The measured outcomes included clinical and functional parameters. The treatment consisted of an oral combination of clofedanol (central antitussive agent) 1.62 mg/Kg/ daily with sobrerol 3.6 mg/Kg/day for 15 days. The active treatment was safe and significantly improved signs and lung function compared to placebo. The first open study included 40 children under five years old with acute and recurrent bronchitis [57]. This study randomly compared oral sobrerol (50-100 mg/twice daily) with oral bromhexine (2-4 mg/three times daily) for two weeks. The outcome was an improvement rate. The results showed that both drugs were effective, but no significant differences occurred. The second open study retrospectively recruited 59 children with acute upper respiratory infections and wet cough aged between 3 and 14 years [65]. This study compared children treated with oral antibiotics (amoxicillin or a macrolide) with children treated with nebulized mucoactive drugs (sobrerol or N-acetylcysteine) used in standard practice. The children treated with mucolytics significantly improved clinical parameters compared with children treated with antibiotics. A third open study considered a group of 30 children (5-10 years old) with secretory otitis media and treated with nebulized sobrerol (one 40mg vial/day) alone for ten consecutive days [68]. The treatment improved clinical outcomes (nasal obstruction, deafness, and earache) and impedance values. The improvement depended on mucus fluidification in the upper airways. The last observational study included 20 children (6 months-2 years old) with pertussis [70]. The primary outcome was the time course to symptom resolution. Children were treated with oral or rectal sobrerol (four times daily), oral salbutamol, and oral erythromycin (40 mg/kg/day) until clinical resolution. This treatment was considered better than historical controls (antibiotics alone or associated with hyperimmune gamma globulins and/or cough sedatives).
Notably, all these studies were conducted in Italy. The global outcomes were positive; however, the records were heterogeneous concerning the medical conditions and treatments. Anyway, the clinical judgment was always favorable, as confirmed by the consolidated use in clinical practice. However, regulatory agencies recently restricted the treatment duration to only three days for all formulations. This limitation may prompt new possible strategies for using sobrerol.
1. Future perspectives
Acute respiratory infections significantly burden the healthcare system and single subjects, mainly in childhood. In particular, a relevant quote about toddlers having frequent respiratory infections. Children frequently contract respiratory infections because their immune systems are still partially immature. As a result, respiratory infections significantly impact morbidity, healthcare costs, overmedication (mainly concerning antibiotics), and family quality of life. In addition, the susceptibility to frequent respiratory infections recognizes some risk factors in children, including age (the smaller they are, the sicker they get), preschool attendance, indoor and outdoor pollution, passive smoking, poor socioeconomic status, and allergic diseases. Antipyretic and antibiotic treatment is common, but their use is often empiric and not based on critical reasoning.
Moreover, overuse of antibiotics accounts for the overwhelming problem of bacterial resistance, and abuse of antipyretics also exposes the risk of adverse events. As a consequence, managing children with frequent respiratory infections represents a crucial task in clinical practice. In this regard, an attractive idea could be to use a combination of two sobrerol formulations, such as oral (syrup) and nebulization (vial), during respiratory infections. The rationale of this combination is to achieve an optimal effect respecting the short duration (three days). Usually, the use of mucolytics lasts for 1-2 weeks or at least until clinical resolution. The combined use of topical and systemic routes could assure an ideal fluidification of secretions that could theoretically reduce some factors involved in the frequency of infections. Clean airways and restored mucociliary clearance could prevent pathogens colonization.
1. Conclusive remarks
Respiratory infections are a common medical condition affecting virtually the entire population. In addition, respiratory infections significantly affect the healthcare system and patients' quality of life. Mucus hypersecretion is a typical consequence of infection and could promote recurrence or prolong infection duration. Therefore, mucus fluidification could represent a therapeutical option currently used in clinical practice. In this regard, using a mucolytic (sobrerol), using two administration routes, could define an innovative strategy, respecting the requested posology.
Author Contributions
G.C. conceptualization and writing and review; A.V. review and editing.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are present in literature.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Finley, C.R.; Chan, D.S.; Garrison, S.; Korownyk, C.; Kolber, M.R.; Campbell, S. What are the most common conditions in primary care? Systematic review. Can Fam Physician 2018, 64(11), 832–840. [Google Scholar]
- Murgia, V.; Manti, S.; Licari, A.; De Filippo, M.; Ciprandi, G.; Marseglia, G.L. Upper Respiratory Tract Infection-Associated Acute Cough and the Urge to Cough: New Insights for Clinical Practice. Pediatr Allergy Immunol Pulmonol 2020, 33(1), 3–11. [Google Scholar] [CrossRef]
- Esneau, C.; Duff, A.C.; Bartlett, N.W. Understanding Rhinovirus Circulation and Impact on Illness. Viruses 2022, 14(1), 141. [Google Scholar] [CrossRef]
- Li, G.; Fan, Y.; Lai, Y.; Han, T.; Li, Z.; Zhou, P.; Pan, P.; Wang, W.; Hu, D.; Liu, X.; et al. Coronavirus infections and immune responses. J Med Virol 2020, 92(4), 424–432. [Google Scholar] [CrossRef]
- Hutchinson, E.C. Influenza Virus. Trends Microbiol 2018, 26(9), 809–810. [Google Scholar] [CrossRef] [PubMed]
- Branche, A.R.; Falsey, A.R. Parainfluenza Virus Infection. Semin Respir Crit Care Med 2016, 37(4), 538–54. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, A.; Ferrara, T.; Maglione, M.; Capasso, L.; Raimondi, F. New perspectives in Respiratory Syncitial Virus infection. J Matern Fetal Neonatal Med 2013, 26 Suppl 2, 55–9. [Google Scholar] [CrossRef]
- Schuster, J.E.; Williams, J.V. Emerging Respiratory Viruses in Children. Infect Dis Clin North Am 2018, 32(1), 65–74. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, M.; Hugentobler, W.J.; Iwasaki, A. Seasonality of Respiratory Viral Infections. Annu Rev Virol 2020, 7(1), 83–101. [Google Scholar] [CrossRef]
- Eccles, R.; Wilkinson, J.E. Exposure to cold and acute upper respiratory tract infection. Rhinology 2015, 53, 99–106. [Google Scholar] [CrossRef]
- Humiston, S.G.; Pham, T.N. Influenza-Like Illness Diagnosis and Management in the Acute Care Setting. Pediatr Emerg Care 2016, 32(12), 875–882. [Google Scholar] [CrossRef] [PubMed]
- Spencer, J.A.; Shutt, D.P.; Moser, S.K.; Clegg, H.; Wearing, H.J.; Mukundan, H.; Manore, C.A. Distinguishing viruses responsible for influenza-like illness. J Theor Biol 2022, 545, 111145. [Google Scholar] [CrossRef] [PubMed]
- Fitzner, J.; Qasmieh, S.; Mounts, A.W.; Alexander, B.; Besselaar, T.; Briand, S.; Brown, C.; Clark, S.; Dueger, E.; Gross, D.; et al. Revision of clinical case definitions: influenza-like illness and severe acute respiratory infection. Bull World Health Organ 2018, 96(2), 122–128. [Google Scholar] [CrossRef]
- Heikkinen, T.; Järvinen, A. The common cold. Lancet 2003, 361(9351), 51–9. [Google Scholar] [CrossRef] [PubMed]
- Kardos, P.; Malek, F.A. Common Cold - an Umbrella Term for Acute Infections of Nose, Throat, Larynx and Bronchi. Pneumologie 2017, 71(4), 221–226. [Google Scholar] [CrossRef] [PubMed]
- Passioti, M.; Maggina, P.; Megremis, S.; Papadopoulos, N.G. The common cold: potential for future prevention or cure. Curr Allergy Asthma Rep 2014, 14(2), 413. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Common cold. https://www.cdc.gov/dotw/common- cold/index.html.
- DeGeorge, K.C.; Ring, D.J.; Dalrymple, S.N. Treatment of the common cold. Am Fam Physic 2019, 100, 281–9. [Google Scholar]
- Fokkens, W.; Lund, V.; Hopkins, C.; Hellings, P.; Kern, R.; Reitsma, S.; Toppila-salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology 2020, 58 (Suppl S29), 1–464. [Google Scholar] [CrossRef]
- Degeorge, K.C.; Ring, D.J.; Dalrymple, S.N. Treatment of the common cold. Am Fam Physician 2019, 100, 281–9. [Google Scholar]
- Chiappini, E.; Parretti, A.; Becherucci, P.; Pierattelli, M.; Bonsignori, F.; Galli, L.; de Martino, M. Parental and medical knowledge and management of fever in Italian pre-school children. BMC Pediatrics 2012, 12, 97. [Google Scholar] [CrossRef]
- Ciprandi, G.; Tosca, M.A. Non-pharmacological remedies for post-viral acute cough. Monaldi Arch Chest Dis. 2021, 9(1). [Google Scholar]
- Centers for Disease Control and Prevention. Antibiotic use in the United States, 2023: progress and opportunities. Accessed June, 22, 2023.
- Jaume, F.; Valls-Mateus, M.; Mullol, J. Common Cold and Acute Rhinosinusitis: Up-to-Date Management in 2020. Curr Allergy Asthma Rep 2020, 20(7), 28. [Google Scholar] [CrossRef]
- Forchette, L.; Sebastian, W. , Liu T. A Comprehensive Review of COVID-19 Virology, Vaccines, Variants, and Therapeutics. Curr Med Sci. 2021, 41(6), 1037–1051. [Google Scholar]
- Anka, A.U; Tahir, M.I.; Abubakar, S.D.; Alsabbagh, M.; Zian, Z.; Hamedifar, H.; Sabzevari, A. , Azizi, G. Coronavirus disease 2019 (COVID-19): An overview of the immunopathology, serological diagnosis and management. Scand J Immunol. 2021, 93(4), e12998. [Google Scholar]
- Van Brusselen, D.; De Troeyer, K.; Ter Haar, E.; Vander Auwera, A.; Poschet, K.; Van Nuijs, S.; Bael, A.; Stobbelaar, K.; Verhulst, S. , Van Herendael, B. , et al. Bronchiolitis in COVID-19 times: a nearly absent disease? Eur J Pediatr 2021, 180(6), 1969–1973. [Google Scholar]
- Cardenas, J.; Pringle, C.; Filipp, S.L.; Gurka, M.J.; Ryan, K.A.; Avery, K.L. Changes in Critical Bronchiolitis After COVID-19 Lockdown. Cureus 2022, 14(5), e25064. [Google Scholar] [CrossRef] [PubMed]
- Krumbein, H.; Kümmel, L.S.; Fragkou, P.C.; Thölken, C.; Hünerbein, B.L.; Reiter, R.; Papathanasiou, K.A.; Renz, H. , Skevaki, C. Respiratory viral co-infections in patients with COVID-19 and associated outcomes: A systematic review and meta-analysis. Rev Med Virol. 2023, 33(1), e2365. [Google Scholar]
- Moore, N.; Bosco-Levy, P.; Thurin, N.; Blin, P.; Droz-Perroteau, C. NSAIDs and COVID-19: A Systematic Review and Meta-analysis. Drug Saf 2021, 44(9), 929–938. [Google Scholar] [CrossRef] [PubMed]
- Fahy, J.V.; Dickey, B.F. Airway mucus function and dysfunction. N Engl J Med 2010, 363(23), 2233–47. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Rubin, B.K.; Voynow, J.A. Mucins, Mucus, and Goblet Cells. Chest 2018, 154(1), 169–176. [Google Scholar] [CrossRef]
- Van der Schans, C.P. Bronchial mucus transport. Respir Care 2007, 52, 1150–6. [Google Scholar]
- Widdicombe, J. H. Regulation of the depth and composition of airways surface liquid. J Anat 2002, 201, 313–18. [Google Scholar] [CrossRef]
- Bansil, R.; Turner, B.S. The biology of mucus: Composition, synthesis and organization. Adv Drug Deliv Rev 2018, 124, 3–15. [Google Scholar] [CrossRef]
- Carlson, T.L.; Lock, J.Y.; Carrier, R.L. Engineering the Mucus Barrier. Annu Rev Biomed Eng 2018, 20, 197–220. [Google Scholar] [CrossRef]
- Francis, R.J.; Chatterjee, B.; Loges, N.T.; Zentgraf, H.; Omran, H.; Lo, C.W. Initiation and maturation of cilia-generated flow in newborn and postnatal mouse airway. Am J Physiol Lung Cell Mol Physiol 2009, 296, 1067–75. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.M.; Koo, J.S. Airway mucus: the good, the bad, the sticky. Pharmacol Ther 2009, 121, 32–48. [Google Scholar] [CrossRef]
- Randell, S.H.; Boucher, R.C. Effective mucus clearance is essential for respiratory health. Am J Respir Cell Mol Biol 2006, 35, 20–8. [Google Scholar] [CrossRef] [PubMed]
- Scaglione, F.; Petrini, O. Mucoactive Agents in the Therapy of Upper Respiratory Airways Infections: Fair to Describe Them Just as Mucoactive? Clin Med Insights Ear Nose Throat 2019, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rogers, D.F. Mucoactive agents for airway mucus hypersecretory diseases. Respir Care 2007, 52, 1176–1193. [Google Scholar]
- Braga, P.C.; Allegra, L.; Bossi, R.; Scuri, R.; Castiglioni, C.L.; Romandini, S. Review on sobrerol as a muco-modifying drug: experimental data and clinical findings in hypersecretory bronchopulmonary diseases. Int J Clin Pharmacol Res 1987, 7, 381–400. [Google Scholar]
- Dalla Valle, V. L’impiego in terapie del dl-sobrerolo. Boll Chim Farm 1970, 109, 761–765. [Google Scholar]
- Braga, P.C.; Culici, M. Dal Sasso, M.; Falch, M.; Spallino, A. Antiradical activity of sobrerol investigated by electron paramagnetic resonance (EPR). Giorn It Mal Tor, 2009; 63, 263–267. [Google Scholar]
- Braga, P.C.; Allegra, L.; Bossi, R.; Scuri, R.; Castiglioni, C.L.; Romandini, S. Review on sobrerol as a muco-modifying drug: experimental data and clinical findings in hypersecretory bronchopulmonary diseases. Int J Clin Pharmacol Res 1987, 7, 381–400. [Google Scholar]
- Seidita, F.; Deiana, M.; Careddu, P. Acute bronchial diseases in paediatrics: therapeutic approach with sobrerol granules. G Ital Mal Torace 1984, 38, 191–194. [Google Scholar]
- Finiguerra, M.; De Martini, S.; Negri, L.; Simonelli, A. Clinical and functional effects of domiodol and sobrerol in hypersecretory bronchopneumonias. Minerva Med 1981, 72, 1353–1360. [Google Scholar]
- Medici, T.C.; Shang, H.; Grosgurin, P.; Berg, P.; Achermann, R.; Wehrli, R. No demonstrable effect of sobrerol as an expectorant in patients with stable chronic bronchial diseases. Bull Eur Physiopathol Respir 1985, 21, 477–483. [Google Scholar] [PubMed]
- Meyer-Shang, H.; Grosgurin, P.; Medici, T.C. Sobrerol as an expectorant in patients with stable chronic airway diseases: a controlled study. Prax Klin Pneumol 1983, 37, 936–938. [Google Scholar] [PubMed]
- Shang, H.; Grosgurin, P.; Medici, T.C. Sobrerol as expectorant in patients with stable chronic respiratory tract infections. A controlled study. Schweiz Med Wochenschr 1982, 112, 1846–1848. [Google Scholar]
- Pulerà, N.; Santolicandro, A.; Bernard, P. , Solfanelli, S.; Giuntini, C. Monodisperse labeled aerosol to visualize airflow redistribution in the lung after a mucokinetic drug. J Nucl Med Allied Sci 1989, 33, 258–263. [Google Scholar] [PubMed]
- Castiglioni, C.L.; Gramolini, C. Effect of long-term treatment with sobrerol on the exacerbations of chronic bronchitis. Respiration 1986, 50, 202–217. [Google Scholar] [CrossRef]
- Bellussi, L.; Manini, G.; Buccella, M.G.; Cacchi, R. Evaluation of the efficacy and safety of sobrerol granules in patients suffering from chronic rhinosinusitis. J Int Med Res 1990, 18, 454–459. [Google Scholar] [CrossRef]
- Distefano, S.M.; Palermo, F.; Crimi, N.; Mistretta, A.; Pamparana, F.; Messa, A. Evaluation of the activity of the carbocysteine-sobrerol combination on mucus spinnability. Int J Clin Pharmacol Res 1988, 8, 31–35. [Google Scholar]
- Milvio, C.; Di Tommaso, G.; Mader, R. Traitement des hypersécretions bronchiques dans les bronchopneumopathies aiguës et chroniques—étude contrôlée d’un nouveau composé à action mucolytique. Acta Ther 1981, 7, 243–260. [Google Scholar]
- Miraglia del Giudice, M.; Capristo, A.F.; Mirra, G.; Maiello, N.; Coppola, T. Controlled double-blind study on the efficacy of clofedanol-sobrerol in the treatment of pediatric pertussis. Minerva Pediatr 1984, 36, 1199–1206. [Google Scholar]
- Azzollini, E.; Bosi, M.; Mantegazza, M.; Piceci, E.; Careddu, P. Sobrerol (Sobrepim) administered dropwise to children with acute hypersecretory bronchopulmonary disease — a controlled trial v bromhexine. Clin Trials J 1990, 27, 241–249. [Google Scholar]
- Balzano, E.; De Gaetani, G. D1-sobrerol in the treatment of acute and chronic bronchopulmonary phlogoses. Minerva Med 1973, 64, 1995–2002. [Google Scholar] [PubMed]
- Monzali, G.; Marchioni, C.F. Utilità di una nuova sostanza, il sobrerolo, nella terapia delle sequele della tubercolosi polmonare. Riv Pat Clin Tuberc 1970, 43, 562–563. [Google Scholar]
- Dotta, F.; Bianchi, A. Sobrerol for the treatment of chronic obstructive bronchopneumopathies (clinical and functional observations). Policlin Med 1971, 78, 82–90. [Google Scholar]
- Morandini, G.; Finiguerra, M.; Conti, P.; Bernocchi, D.; Manini, G. Treatment of chronic bronchitis—combined therapy with sustained-release theophylline (Teonova) and a mucoactive drug sobrerol (Sobrepin). Clin Trials J 1989, 26, 163–174. [Google Scholar]
- Morandini, G.C.; Finiguerra, M.; Messa, A.; Pamparana, F. L’associazione carbocisteina-sobrerolo nel trattamento della patologia cronico-ostruttiva dell’apparato respiratorio. Min Pneum 1986, 25, 127–133. [Google Scholar]
- Catena, E.; Marcatili, S.; Ciaccia, A. L’associazione carbocisteina-sobrerolo — studio clinico long-term nella profilassi delle riacutizzazioni da bronchite cronica. Med Toracica 1989, 11, 83–100. [Google Scholar]
- Gramiccioni, E.; Pamparana, F.; Messa, A. Mucolytic agents. Polycentric study of a carbocysteine-sobrerol combination. Arch Monaldi Mal Torace, 1989; 44, 791–793. [Google Scholar]
- Zanasi, A.; Cazzato, S.; Aprile, A.; Mazzolini, M.; Zenezini, C.; Pandolfi, P. Are antibiotics effective in treating children with acute moist cough? a retrospective study vs symptomatic therapy. Multidiscip Respir Med 2012, 7, 1–5. [Google Scholar]
- Zanasi, A.; Lecchi, M.; Mazzolini, M.; Mastroroberto, M.; Nardi, E.; Morselli-Labate, A. Observational prospective study comparing mucoactive and antibiotic treatment in the management of acute cough from upper respiratory tract infections. Minerva Med 2015, 106, 239–246. [Google Scholar]
- Fadda, G. Oral neltenexine in patients with obstructive airways diseases: an open, randomised, controlled comparison versus sobrerol. Minerva Med 2001, 92, 269–275. [Google Scholar]
- Bellussi, L.; Bernocchi, D.; Ciferri, G.; Manini, G.; Passali, D. Sobrerol in the treatment of secretory otitis media in childhood. J Int Med Res 1989, 17, 277–286. [Google Scholar] [CrossRef]
- Milder, H.; Massari, M. Étude clinique d’un nouveau composé à activité mucolytique dans les bronchopneumopathies aiguës et chroniques. Acta Ther 1981, 7, 391–408. [Google Scholar]
- Crosca, V.; Ajello, A.; Crosca, C.; Minniti, A. Salbutamol combined with erythromycin and sobrerol in the therapy of pertussis. Arch Sci Med (Torino) 1982, 139, 247–250. [Google Scholar] [PubMed]
Figure 1.
Mechanisms of action of sobrerol.
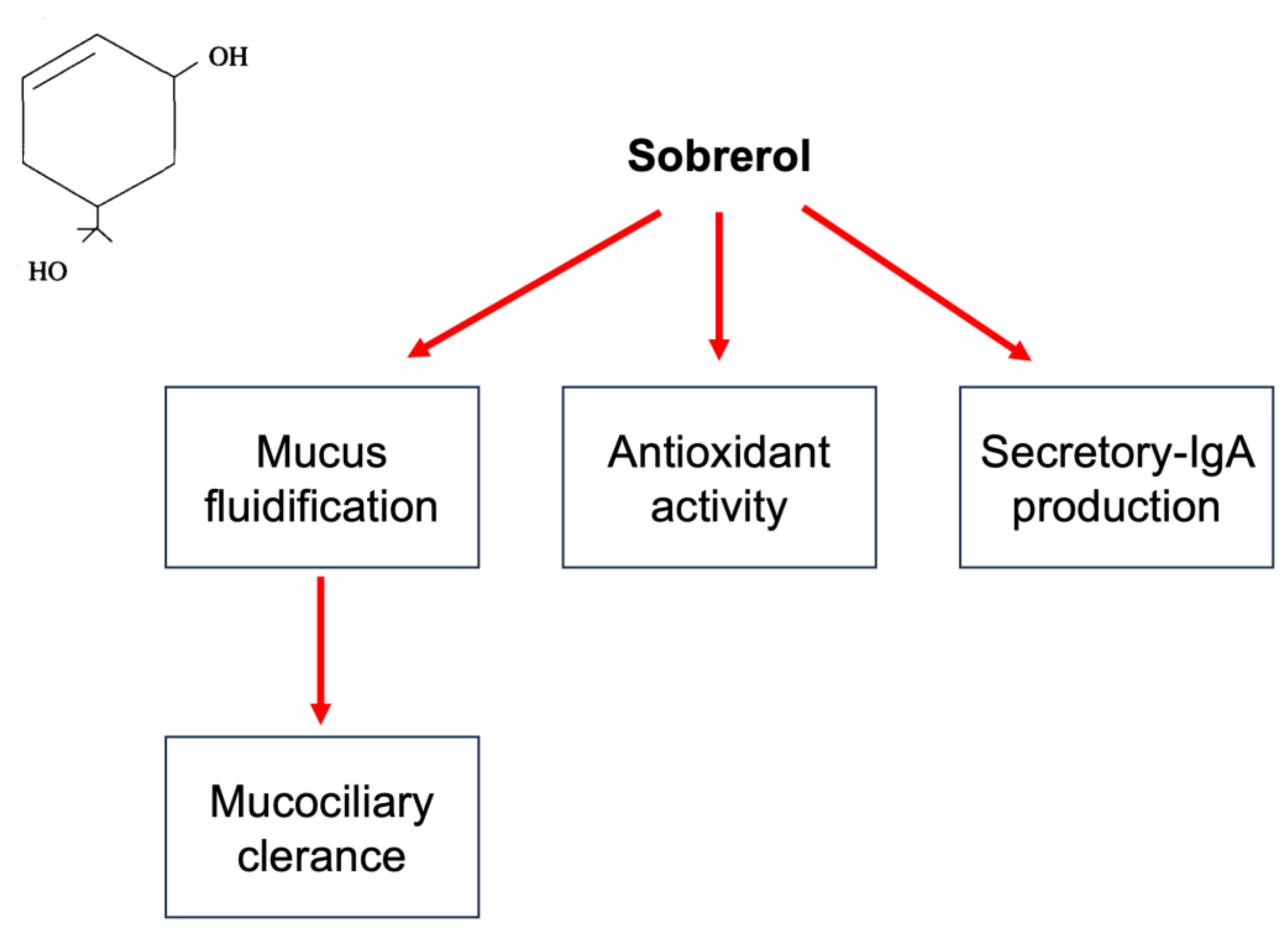

Table 1.
Classification of mucolytic agents based on specific mechanisms of action.
| Direct action |
Drugs depolymerizing mucins | - Thiolics - Enzymes - Other molecules |
- Cysteine - Methylciytein - Ethylciytein - Acetylcysteine - Erdostein - Ludostein - Stepronin - Thipronin - Mesna - Trypsin - Streptokinase - Serratiopeptidase - Stericase - Urea - Ascorbic acid - Hypertonic saline - Inorganic iodures |
| Indirect action |
Drugs modifying mucus secretion Drugs modifying adhesivity of gel layer Drugs modifying the sol layer Volatile and balsamic agents Drugs stimulating gastric reflex (cough inducing) Drugs modifying secretion |
• S-carbossimethylcystein • Sobrerol • Domiodol • Hydropropylidenglycerol • Ambroxol • Bromexine • Propylene-glycol • Etasulphate sodic • Bicarbonate sodic • H2O • Potassium salts • Sodium salts • Pinanes - Terpenes - Methanes - Phenol derivates - Ammonium chloride - Sodium citrate - Guaifenesin - Ipecap • -adrenergic agents - cholinergic agents - corticosteroids • - antihistamines |
Table 2.
Pediatric studies using sobrerol.
| Authors (ref) | Study design | Disease | Patients number (age) | Primary outcomes | Treatments (dosage and duration) |
Results |
|---|---|---|---|---|---|---|
| Seidita et al. (46) | RCT | Acute respiratory infections | 20/20 (3-12 years) |
Clinical signs Expectorate Biological data |
Oral sobrerol (100mgx3/day) Oral N-Acteylcysteine (100mgx3/day) One week |
Sobrerol significantly reduced mucus viscosity |
| Milvio et al. (55) | RCT | Acute and chronic infections | 50/50 (12-74 years) |
Lung function Expectorate |
Oral sobrerol (260mg) + carbocysteine (375mg)x4/day Placebo 14-21 days |
Active treatment significantly improved all outcomes |
| Miraglia del Giudice et al. (56) | RCT | Pertussis | 15/15 (10 months-12 years) |
Clinical signs Lung function |
Clofedanol (1.62mg/kg/d)+oral sobrerol (6mg/kg/d) Placebo 15 days |
Active treatment improved parameters more quickly |
| Azzolini et al. (57) | Open | Acute and recurrent bronchitis | 40 (< 5 years) |
Improvement rate | Oral sobrerol (50-100mgx2/d) Oral brohexine (2-4x3/d) 2 weeks |
No difference |
| Zanasi et al. (65) | Open | Acute upper respiratory infections with wet cough | 59 (3-14 years) |
Severity, frequency, and duration of cough | Antibiotics (amoxicillin or erythromycic) Nebulized sobrerol or N-Acetylcysteine. |
Mucolytics improved cough |
| Bellussi et al. (68) | Open | Secretory otitis media | 30 (5-10 years) |
Nasal obstruction, earache, deafness | Nbulized sobrerol (40mg/d) 10 days |
Significant reduction of all outcomes |
| Crosca et al. (70) | Open | Pertussis | 20 (6 months-2 years) |
Time to resolution | Oral or rectal sobrerol Salbutamol Erythromycin Until resolution |
Better outcomes in comparison with historical records |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



