
Submitted:
30 June 2023
Posted:
03 July 2023
You are already at the latest version
Abstract
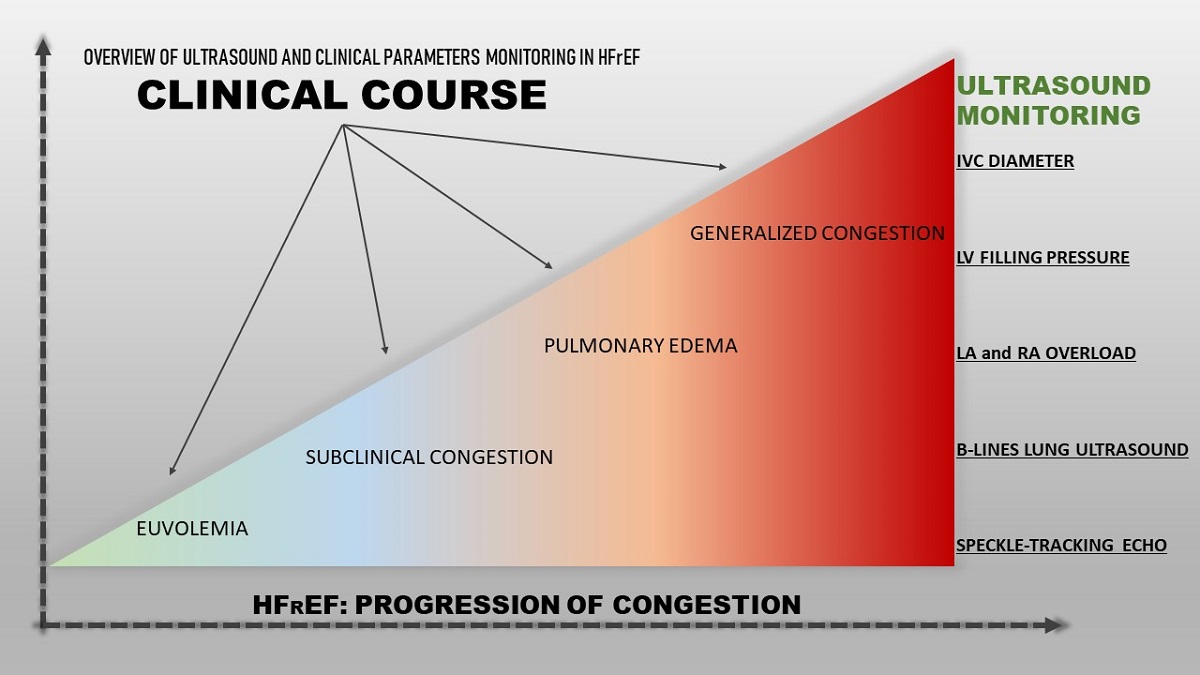
Heart failure with reduced ejection fraction (HFrEF) is considered a major healthcare problem with frequent decompensations, high hospitalization and mortality rates. In severe heart failure (HF), the symptoms are refractory to medical treatment and require advanced therapeutic strategies. Early recognition of HF sub- and decompensation is the cornerstone of the timely treatment intensification and, therefore, improvement of the prognosis. Echocardiography is the gold standard for the assessment of systolic and diastolic functions. It allows to obtain accurate and non-invasive measurements of the ventricular function in HF. In severely compromised HF patients, advanced cardiovascular ultrasound modalities may provide a better assessment of intracardiac hemodynamic changes and subclinical congestion. Particularly, cardiovascular and lung ultrasound allow to make a more accurate diagnosis of subclinical congestion in HFrEF. The aim of this review is to summarize the advantages and limitations of currently available ultrasound modalities in the ambulatory monitoring of patients with HFrEF.
Keywords:
heart failure with reduced ejection fraction
; echocardiography
; outpatient monitoring
; left ventricular filling pressure
; lung ultrasound
; inferior vena cava
1. Introduction
Heart failure (HF) is considered a major healthcare problem with more than a million new cases every year [1]. During the last decades, guideline-recommended treatment has considerably improved the outcomes of heart failure with reduced ejection fraction (HFrEF) [2,3]. Despite that, the mortality and rehospitalization rates remain high [1,2,4,5]. Moreover, the number of hospitalizations for HF is expected to increase significantly in the future and may double by 2045 due to the aging and growth of the population [6,7].
HF decompensation may be provoked by trigger factors, such as infection, myocardial ischemia, acute renal injury, or anaemia. In case of disease deterioration due to an increasing fluid retention, subclinical congestion precedes the clinical manifestation of HF symptoms and hospitalizations for an acute HF decompensation by several days or weeks. Therefore, the identification of vulnerable period before the symptomatic HF decompensation allows for a prompt increase of diuretic doses and treatment modification, which may prevent the upcoming hospital admission [8]. Physical examination, particularly identification of crackles on auscultation, is the main strategy routinely used for the prediction and diagnosis of left-sided HF decompensation in outpatients [9]. However, while it allows the identification of symptomatic patients, the asymptomatic phase of HF decompensation is usually missed.
Hospitalizations negatively affect the prognosis and quality of life [10]. Moreover, they are strongly associated with a risk of cardiovascular and all-cause mortality, which increases progressively with every subsequent hospitalization [11]. Thus, the prevention of rehospitalizations is one of the main goals of HF management. For an effective reduction of unexpected hospital visits, early prediction of HF decompensation and prompt treatment modification are of paramount importance. Effective ambulatory monitoring and timely treatment modification are the key strategies for the reduction of cardiovascular events and improvement of the prognosis [12]. Numerous data suggest, that those HF patients, who have undergone an echocardiographic examination, have better survival rates due to a more intensive medical treatment and interventions [13].
The aim of this review is to summarize the current knowledge regarding echocardiographic and ultrasound features of subclinical congestion among a broad range of HFrEF patients.
2. Left ventricular decompensation: natriuretic peptides and basic echocardiography
It is evident, that hemodynamic deterioration precedes the development of clinical signs and symptoms by days or weeks, thus, symptomatic clinical congestion may be seen as a “tip of an iceberg” of the hemodynamic compromise [14]. Due to the delay between symptom manifestation and the progressive left ventricular (LV) filling pressure increase, physical examination alone may be insufficient for the identification of patients in vulnerable phase of asymptomatic decompensation and for the prediction of upcoming hospital readmissions in outpatients [15,16].
It is well established, that an increased venous pressure can be detected by cardiovascular ultrasound, particularly by the assessment of inferior vena cava (IVC) characteristics and the detection of interstitial pulmonary oedema through B-line identification. On the other hand, intracardiac hemodynamic changes and LV filling pressure increase precede the manifestation of HF symptoms and can be diagnosed by echocardiography [12,17]. Comprehensive cardiovascular ultrasound with Tissue Doppler imaging (TDI) and lung ultrasound overcome the limitations of physical examination and clinical picture-based strategies for the prediction of HF decompensation.
During the last decade it has become apparent, that natriuretic peptide-guided management of ambulatory chronic HF patients may optimize the treatment. Natriuretic peptides are important components of HF diagnostic work-up due to their high negative predictive value. However, the data on utility of natriuretic peptides in the prevention of HF decompensations are relatively scarce. In PARADIGM-HF trial low levels of natriuretic peptides were associated with lower risks of cardiovascular events [18]. In GUIDE-IT study involving 894 high risk patients with HFrEF, the most important predictor of cardiovascular death and HF hospitalizations was the baseline natriuretic peptide level [19]. The data suggest, that natriuretic peptides also correlate with the risk of hospitalization and the duration of hospital stay [6]. However, with the introduction of neprilysin inhibitor in the treatment of HFrEF, the accuracy and reliability of natriuretic peptides as prognostic markers have been questioned. By inhibiting neprilysin, sacubitril leads to increase of B-type natriuretic peptide (BNP) and reduction of N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentrations [20]. Thus, the role of natriuretic peptides in the prediction of hospital admissions in outpatients has to be further investigated.
Another concern regarding the diagnostic role of natriuretic peptides is related to morbidly obese patients, who have consistently lower natriuretic peptide levels [21,22,23]. Other limitations of natriuretic peptides include their level changes in atrial fibrillation and renal dysfunction. Given the limitations of natriuretic peptides, along with the complex physiology of HF, it is reasonable to consider implementation of other parameters and markers for the improvement of HF management and prevention of decompensations.
Basic echocardiographic assessment is an important tool for the diagnosis, classification and treatment of HF. Some authors recommend using LV ejection fraction (EF) for the assessment of prognosis in ambulatory HFrEF patients, based on the role of EF dynamic increase as a predictor marker of an improved survival and hospitalization risk in this patient population [24]. However, EF loses its prognostic role at later stages of the disease and when the values are close to the threshold [25]. As a prognostic marker for HF decompensations, EF has other important limitations. Among them, technical pitfalls, preload dependence, possible measurement errors in the presence of severe mitral regurgitation, atrial fibrillation or heart rate variations, and a weak association with functional class and exercise capacity [26,27,28]. The abovementioned limitations advocate for the use of additional parameters and methods for the assessment of LV function, such as TDI, longitudinal strain quantification by speckle tracking, 3-dimensional echocardiography and cardiac magnetic resonance imaging (MRI).
An increase in left atrial (LA) volume and LV filling pressure contribute to LA remodelling and HF decompensation leading to frequent hospitalizations due to the lung congestion. In clinical practice, the LA volume index is widely used to assess LA overload. A clinically significant increase is considered an LA volume index > 34 ml/m2 [29]. LA volume index is an independent predictor of cardiovascular events, including atrial fibrillation, as well as cardiovascular mortality [26,30]. Moreover, the LA volume index is a marker of diastolic dysfunction and, unlike EF, correlates well with the patient's functional class and overall exercise capacity [27,31]. The LA volume index correlates with the E/e' ratio and can serve as a useful predictor of increased LV filling pressure during exercise [32].
Echocardiography with intracardiac hemodynamic assessment provides a semiquantitative analysis of decompensation and identifies filling pressure abnormalities. LV filling pressure measurements are of special interest in patients with HFrEF, because the increase in filling pressure underlines the pathophysiological mechanisms of HF deterioration and precedes the manifestation HF signs and symptoms [12].
Currently, echocardiographic doppler and TDI are widely used in clinical practice for the evaluation of LV systolic and diastolic functions. As a marker of diastolic dysfunction, LV filling pressure can be assessed by calculating E/e’ ratio, where E wave is the peak velocity of the early diastolic flow across the mitral valve as measured by pulsed-wave doppler, and e’ is the early diastolic velocity of the septal or lateral mitral annulus obtained by TDI (Figure 1). The accepted threshold for the normal LV end-diastolic pressure is E/e’ < 8, while E/e’ > 14 and peak tricuspid regurgitation (TR) velocity > 2.8 m/s indicate high LV end-diastolic pressure [33]. Recent studies emphasize the importance of the routine measurements of E/e’ for the assessment of LV filling pressure, risk stratification and prognostication in HF patient population [33,34]. Benfari G. et al. suggested E/e’ ratio > 14 as a cut-off for the identification of high-risk patients [35]. The Authors reported increased short and long-term mortality in individuals with E/e’ > 14, with a considerable worsening of prognosis in E/e’ > 20 [35]. Therefore, in HFrEF additional parameters should be considered for the assessment of LV filling pressures and atrial hypertension to predict intracardiac volume overload and subclinical deterioration.
In summary, mean E/e' ratio > 14 and LA volume index > 34 mL/m2 are important markers for the assessment of LV diastolic dysfunction and correlate with invasively measured LV filling pressure [36,37,38]. Moreover, unlike EF, LA volume index, E/e’ and TR velocity have better correlation with overall physical capacity in patients with HFrEF [33].
The systemic review and meta-analysis of echocardiographic quantification of LV filling pressure found, that non-invasive echocardiographic estimation of filling pressure correlates with invasive right heart catheterization results and its use is feasible in both HF with reduced and preserved EF [39]. Although in patients with HFrEF the pooled correlation coefficient was stronger for clinical translation, the application of E/e’ along with LA volume and TR velocity showed increased correlation with the invasive assessment [40,41].
HF patients with LVEF below 40% may demonstrate different echocardiographic patterns of congestion based on LV filling pressure, LA volume index and lung ultrasound. The implementation of these parameters in routine clinical practice may provide important information and be of value in predicting HF decompensations [42,43].
Ballo R. and co-authors investigated the prognostic role of longitudinal LV systolic function assessed by TDI. The Authors evaluated the average value of lateral and septal peak systolic annular velocities (Sm) and reported the Sm threshold of ≤ 6.5 cm/sec as a statistically significant prognostic value in dilated cardiomyopathy of non-ischemic origin [44]. However, the patients with ischemic aetiology of HF were not included in the study, thus, the possible influence of local asynergies on the value of the peak systolic velocity of the mitral ring was not investigated.
Despite several limitations of single E/e’ ratio measurements in the prediction of elevated LV filling pressure, the complex assessment of LV filling pressure, pulmonary artery systolic pressure and LA volume index has a significant diagnostic value. When combined these parameters allow for risk stratification and are associated with outcomes in patients with heterogeneous EF within HFrEF population.
3. Speckle tracking
During the last decades, speckle tracking echocardiography (STE) has emerged as a relatively new technique for the assessment of HF individuals. STE provides information about the ventricular function by identifying and analysing movement of dots or “speckles” in the ventricular wall image and by tracing length and thickness changes in any given segment of the myocardium. Evaluation of the myocardial displacement is performed in 4-chamber, 2-chamber and apical long-axis views and is presented as a percentage. Speckle tracking imaging allows measurement of global longitudinal strain (GLS), radial and circumferential strains of the ventricles, as well as atrial longitudinal strain.
To date the LV GLS is the most widely investigated and implemented parameter among speckle tracking strains. Numerous data suggest, that GLS may be a useful marker for the clinical risk stratification and prognostication of HFrEF [45,46,47]. As a prognostic marker GLS is superior to LV EF in predicting reduced exercise capacity, poor prognosis and mortality in patient with HFrEF [48,49,50]. Compared to LV EF, GLS allows for a more accurate quantification of the extent of systolic dysfunction. Other significant disadvantages of LV EF include inability to quantify regional myocardial function and geometric assumptions [51].
Carluccio E. and co-authors analyzed the role of LA longitudinal strain in HFrEF patients. Based on the results, peak LA longitudinal strain has a significant prognostic value in HFrEF independently of LA volume and LV longitudinal contraction [52]. Moreover, reduced peak LA longitudinal strain is associated with a higher LA and LV volumes, as well as more severe systolic and diastolic dysfunctions [52]. In HF patients, LA longitudinal strain can also be used as an alternative parameter for the assessment of LV filling pressure [53,54].
STE is superior to standard echocardiography in detecting impaired systolic function using longitudinal and circumferential deformation, particularly in the heterogeneous group of HF patients. Since its initial use over 15 years ago, STE has emerged as a method, that provides more robust, reproducible and sensitive parameters of regional dysfunction and myocardial dyssynchrony. An important advantage of STE imaging over TDI is the absence of the angle-dependency [27]. However, STE requires high quality images to obtain accurate measurements, it is a time-consuming technique with a high interobserver variability. Another limitation of STE is the need for high resolution images, which are not always possible to obtain during routine examination. Therefore, taking into consideration the number of limitations, STE is not always applicable for the assessment of ambulatory patients.
4. Lung ultrasound
Lung ultrasound (LUS) is a novel strategy for the assessment of pulmonary congestion in HF patients. During the last years it has been widely used for the differential diagnosis of acute onset dyspnoea in emergency situations and for the management of acute HF. Additionally, LUS has a prognostic value in the monitoring of chronic HF patients.
In healthy lungs, only horizontal parallel A-lines can be observed. In case of extravascular fluid accumulation in the lungs, B-lines can be detected, which are vertical white artefacts arising from the pleura and reaching the bottom of the screen (Figure 2) [55]. LUS can be performed in the supine position of the patient in 28 areas and the total number of B-lines is reported [55]. Progressive increase in B-lines is associated with the severity of pulmonary congestion, total number of B-lines > 5 in 28 zones is considered abnormal, while B-lines > 30 suggests severe congestion [55,56].
LUS has a high prognostic value for the prediction of hospitalizations. Among the patients hospitalized for acute HF, presence of residual B-lines at discharge is associated with a higher risk of rehospitalizations [57,58]. LUS can also be effectively used as a prognostic marker of hospital readmissions in ambulatory patients with chronic HF. There is a strong association between the presence of B-lines (greater than 15 in 28 zones) and an increased risk of hospitalizations for HF decompensation [59,60]. Moreover, LUS is superior and more sensitive in the detection of pulmonary congestion compared to physical examination. An important advantage of LUS over physical examination is the ability to detect asymptomatic patients with subclinical congestion both at discharge and in outpatient settings [55].
Use of LUS for the detection of residual congestion at discharge among the patients admitted for acute decompensated HF allows identification of undertreated patients who require more intensive diuretic regimens for the prevention of early rehospitalizations. Additionally, detection of asymptomatic pulmonary congestion before the symptom onset allows an early diagnosis of subclinical HF decompensation in outpatients. Thus, it may enable to make timely treatment modifications, particularly loop diuretic dose up-titration, for the prevention of HF decompensations in ambulatory settings.
In summary, the detection of B-lines by LUS plays an important role in the differential diagnosis of congestion and acute decompensated HF. Moreover, implementation of LUS in the ambulatory follow-up may enable HF specialists to identify the patients at high risk of an upcoming decompensation and may provide guidance in determining the optimal treatment strategy for the prevention of hospitalizations among patients with chronic HF.
5. Right ventricular HF decompensation
Both patients and healthcare providers can be involved in the clinical follow-up-based approach for the prevention of hospitalizations in ambulatory patients. Self-assessment of congestion by the patient requires daily weight checking and self-administration of an additional diuretic dose in case of body weight increase for ≥ 2 kilograms in 2 days or exacerbation of oedema [61,62]. Despite the improvement of the outcomes, self-control strategy highly depends on the compliance and psychological state of the individual [63]. Moreover, ambulatory weight change monitoring and self-assessment of the symptoms are unreliable and have low effectiveness in the prevention of HF hospitalizations [64]. This is due to the fact, that development of oedema and HF decompensation are driven not only by the circulating blood volume increase, but also largely depend on fluid redistribution in the body [65].
In patients with HF, echocardiographic measurements of right ventricular (RV) pump function and right atrial (RA) pressure provide important information about RV dysfunction, overload, pulmonary artery and central venous pressures. For the evaluation of RV systolic function EF and tricuspid annular plane systolic excursion (TAPSE) are used in clinical practice. However, both parameters have important limitations. Particularly, the assessment of RV EF is difficult due to RV geometry and suboptimal visualization of endocardial borders. Limitations of TAPSE include angle and load dependence, and extrapolation of single segment displacement amplitude to the overall RV ventricular function [66]. Therefore, implementation of additional parameters and advanced techniques for the evaluation of RV systolic function should be consider in the monitoring of HFrEF patients.
New parameters for the quantitative measurement of RV function have been widely investigated. Based on the available data they are reliable, have a good correlation with cardiac MRI findings and can be used for the prediction of RV remodelling and clinical deterioration of the patients [66,67]. TAPSE, RV shortening and peak systolic tricuspid annular velocity (S’) measured by TDI have an important role in the assessment of HF severity and identification of patients with high risk of frequent rehospitalizations and mortality [68].
The prognostic value of RA enlargement was analysed in the study conducted by Almodares Q. et al. [69]. Meanwhile, RV dysfunction and RA pressure increase were reported as poor outcome predictors and were associated with higher event risk among ambulatory patients with HF at 12 months after the discharge [70].
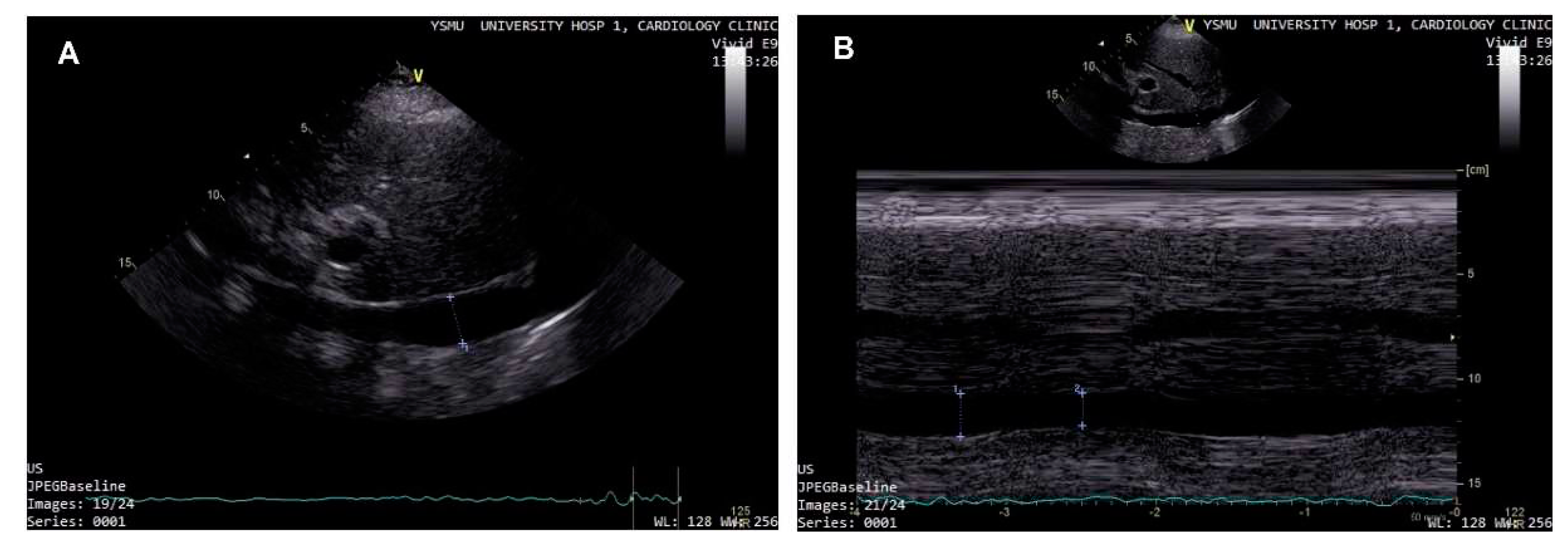
Studies have demonstrated, that patients with IVC diameter > 2.5cm and collapse of <50% on inspiration have RA pressure more than 10 mmHg (Figure 3) [71,72]. Evaluation of IVC can be easily performed and successfully used in outpatients with HF [73]. The examination can be reliably performed by the medical personal with a limited training and experience in echocardiography, particularly by point-of-care mobile ultrasound systems [74,75,76]. Assessment of IVC diameter and collapsibility in ambulatory patients may aid in the prediction of HF deterioration and hospitalization and may have an added prognostic value when combined with physical examination [77,78]. In HF population, IVC distension correlated with an increased risk of adverse events, furthermore, as a poor outcome predictor its value was comparable with NT-proBNP [45]. Among the individuals with HF, presence of dilated IVC was associated with higher risk of complications, particularly renal function decline [79]. However, IVC dilation develop after significant expansion of plasma volume and rise of RA pressure, thus, it cannot serve as an early sign of congestion. Moreover, limitations of IVC assessment include difficulty of measurement interpretation in case of intrathoracic pressure increase, intraabdominal hypertension, and positive pressure mechanical ventilation.
In this review we outline the gaps of LV EF evaluation by basic echocardiography and emphasize the importance of implementing other parameters beyond EF for the evaluation of HF patients in everyday clinical practice. This paper focuses on the heterogeneous group of HFrEF patients with high or normal LV filling pressure and RV congestion. We suggest to perform a risk stratification of HFrEF patients based on the echocardiographic evidence of LA hypertension for the prediction of decompensations and treatment optimization.
6. Conclusions
- Several important echocardiographic parameters beyond EF can be routinely used as part of an algorithm for prediction of decompensations in chronic HF patients.
- Integration of multiple parameters, which can be easily determined by lung ultrasound and cardiovascular ultrasound, including LV filling pressure, central venous pressure, left and right atrial remodelling, enables to move beyond considering only LV systolic function.
- Complex cardiovascular ultrasound assessment allows to obtain more precise parameters of HF deterioration and enables to identify patients, who require a personalized treatment approach.
Funding
No external funding.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; et al. American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA Guideline for the Management of Heart Failure. J Am Coll Cardiol. 2013, 62, 147–239. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; et al. ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology ( ESC ) Developed with the special contribution. Eur Heart J 2016, 128, 1–85. [Google Scholar]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; et al. American Heart Association Statistics Committee; Stroke Statistics Subcommittee. Heart disease and stroke statistics-2016 update a report from the American Heart Association. Circulation. 2016, 26, 38–360. [Google Scholar]
- Maggioni, A.P.; Dahlström, U.; Filippatos, G.; et al. Heart Failure Association of ESC (HFA). EURObservational research programme: The heart failure Pilot survey (ESC-HF Pilot). Eur J Heart Fail. 2010, 12, 1076–1084. [Google Scholar] [CrossRef]
- Orso, F.; Fabbri, G.; Maggioni A Pietro. Epidemiology of Heart Failure. Handb Exp Pharmacol 2017, 243, 15–33. [Google Scholar]
- Savarese, G.; Musella, F.; Amore, C.D.; et al. Changes of Natriuretic Peptides Predict Hospital Admissions in Patients With Chronic Heart Failure. JACC Hear Fail. 2014, 2, 148–58. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.; Metra, M.; Adamo, M.; et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Murphy, N.; Shanks, M.; Alderman, P. Management of Heart Failure With Outpatient Technology. J Nurse Pract. 2019, 15, 12–8. [Google Scholar] [CrossRef]
- Damy, T.; Kallvikbacka-Bennett, A.; Zhang, J.; et al. Does the physical examination still have a role in patients with suspected heart failure? Eur J Heart Fail. 2011, 13, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Čerlinskaitė, K.; Mebazaa, A.; Cinotti R, et al. Readmission following both cardiac and non-cardiac acute dyspnoea is associated with a striking risk of death. ESC Heart Fail. 2021, 8, 2473–2484. [Google Scholar] [CrossRef] [PubMed]
- Lindmark, K.; Boman, K.; Stålhammar, J.; et al. Recurrent heart failure hospitalizations increase the risk of cardiovascular and all-cause mortality in patients with heart failure in Sweden: a real-world study. ESC Heart Fail. 2021, 8, 2144–2153. [Google Scholar] [CrossRef] [PubMed]
- Mangi, M.A.; Rehman, H.; Rafique, M.; Illovsky, M. Ambulatory Heart Failure Monitoring : A Systemic Review Common methods for HF monitoring. Cureus. 2017, 9, 1174. [Google Scholar]
- Tribouilloy, C.; Rusinaru, D.; Mahjoub, H.; Goissen, T.; Lévy, F.; Peltier, M. Impact of echocardiography in patients hospitalized for heart failure: a prospective observational study. Arch Cardiovasc Dis. 2008, 101, 465–73. [Google Scholar] [CrossRef]
- Gheorghiade, M.; Follath, F.; Ponikowski, P. , et al, European Society of Cardiology; European Society of Intensive Care Medicine. Assessing and grading congestion in acute heart failure: a scientific statement from the acute heart failure committee of the heart failure association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur J Heart Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.B. Pathophysiology of the transition from chronic compensated and acute decompensated heart failure: New insights from continuous monitoring devices. Curr Heart Fail Rep. 2009, 6, 287–292. [Google Scholar] [CrossRef]
- Lampert, B.C.; Emani, S. Remote hemodynamic monitoring for ambulatory left ventricular assist device patients. J Thorac Dis. 2015, 7, 2165–2171. [Google Scholar] [CrossRef] [PubMed]
- Dokainish, H.; Nguyen, J.S.; Bobek, J.; Goswami, R.; Lakkis, N.M. Assessment of the American Society of Echocardiography-European Association of Echocardiography guidelines for diastolic function in patients with depressed ejection fraction: an echocardiographic and invasive haemodynamic study. Eur J Echocardiogr. 2011, 12, 857–64. [Google Scholar] [CrossRef]
- Zile, M.R.; Claggett, B.L.; Prescott, M.F.; et al. Prognostic Implications of Changes in N-Terminal Pro-B-Type Natriuretic Peptide in Patients With Heart Failure. J Am Coll Cardiol. 2016, 68, 2425–2436. [Google Scholar] [CrossRef]
- O’Connor, C.; Fiuzat, M.; Mulder, H.; et al. Clinical factors related to morbidity and mortality in high-risk heart failure patients: the GUIDE-IT predictive model and risk score. Eur J Heart Fail. 2019, 21, 770–8. [Google Scholar] [CrossRef]
- Rocca, H.B.; Wijk, S.S. Biomarkers Natriuretic Peptides in Chronic Heart Failure. Card Fail Rev. 2019, 5, 44–49. [Google Scholar] [CrossRef]
- Madamanchi, C.; Alhosaini, H.; Sumida, A.; Runge, M.S. Obesity and natriuretic peptides, BNP and NT-proBNP: mechanisms and diagnostic implications for heart failure. Int J Cardiol. 2014, 176, 611–7. [Google Scholar] [CrossRef]
- Horwich, T.B.; Hamilton, M.A.; Fonarow, G.C. B-type natriuretic peptide levels in obese patients with advanced heart failure. J Am Coll Cardiol. 2006, 47, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.R.; Uber, P.A.; Park, M.H.; et al. Obesity and suppressed B-type natriuretic peptide levels in heart failure. J Am Coll Cardiol. 2004, 43, 1590–5. [Google Scholar] [CrossRef] [PubMed]
- Breathett, K.; Allen, L.A.; Udelson, J.; Davis, G.; Bristow, M. Changes in Left Ventricular Ejection Fraction Predict Survival and Hospitalization in Heart Failure With Reduced Ejection Fraction. Circ Heart Fail. 2016, 9, e002962. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H. Methods used for the assessment of LV systolic function: common currency or tower of Babel? Heart. 2013, 99, 1078–1086. [Google Scholar] [CrossRef] [PubMed]
- Marwick, T.H. The role of echocardiography in heart failure. J Nucl Med. 2015, 56 (Suppl. 4), 31S–38S. [Google Scholar] [CrossRef]
- Pastore, M.C.; Mandoli, G.E.; Aboumarie, H.S.; et al. Basic and advanced echocardiography in advanced heart failure : an overview. Heart Fail Rev. 2019, 25, 937–948. [Google Scholar] [CrossRef]
- Savarese, G.; Lund, L. Global Public Health Burden of Heart Failure. Card Fail Rev. 2017, 3, 7–11. [Google Scholar] [CrossRef]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: An expert consensus document of the European Association of Cardiovascular Imag. Eur Heart J Cardiovasc Imaging. 2017, 18, 1301–1310. [Google Scholar] [CrossRef]
- Di Tullio, M.R.; Qian, M.; Thompson, J.L.P.; et al. Left atrial volume and cardiovascular outcomes in systolic heart failure: effect of antithrombotic treatment. ESC Hear Fail. 2018, 5, 800–808. [Google Scholar] [CrossRef]
- Romano, G.; Magro, S.; Agnese, V.; et al. Echocardiography to estimate high filling pressure in patients with heart failure and reduced ejection fraction. ESC Heart Fail. 2020, 7, 2268–2277. [Google Scholar] [CrossRef] [PubMed]
- Hammoudi, N.; Achkar, M.; Laveau, F.; et al. Left atrial volume predicts abnormal exercise left ventricular filling pressure. Eur J Heart Fail. 2014, 16, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography : An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Cameli, M.; Pastore, M.C.; Mandoli, G.E.; Nistor, D. Prognosis and Risk Stratification of Patients With Advanced Heart Failure (from PROBE). Am J Cardiol. 2019, 124, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Benfari, G.; Miller, W.L.; Antoine, C.; et al. Diastolic Determinants of Excess Mortality in Heart Failure With Reduced Ejection Fraction. JACC Hear Fail. 2019, 7, 808–17. [Google Scholar] [CrossRef]
- Ommen, S.R.; Nishimura, R.A.; Appleton, C.P.; et al. Clinical utility of Doppler echocardiography and tissue Doppler imaging in the estimation of left ventricular filling pressures: A comparative simultaneous Doppler-catheterization study. Circulation. 2000, 102, 1788–1794. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Marwick, T.H. Use and Limitations of E/e' to Assess Left Ventricular Filling Pressure by Echocardiography. J Cardiovasc Ultrasound. 2011, 19, 169–173. [Google Scholar] [CrossRef]
- Lancellotti, P.; Galderisi, M.; Edvardsen, T.; et al. Echo-Doppler estimation of left ventricular filling pressure: results of the multicentre EACVI Euro-Filling study. Eur Heart J Cardiovasc Imaging. 2017, 18, 961–968. [Google Scholar] [CrossRef]
- Jones, R.; Varian, F.; Alabed, S.; et al. Meta-analysis of echocardiographic quantification of left ventricular filling pressure. ESC Heart Fail. 2021, 8, 566–576. [Google Scholar] [CrossRef]
- Obokata, M.; Kane, G.C.; Reddy, Y.N.; Olson, T.P.; Melenovsky, V.; Borlaug, B.A. Role of Diastolic Stress Testing in the Evaluation for Heart Failure With Preserved Ejection Fraction: A Simultaneous Invasive-Echocardiographic Study. Circulation. 2017, 135, 825–838. [Google Scholar] [CrossRef]
- Hummel, Y.M.; Liu, L.C.Y.; Lam, C.S.P.; et al. Echocardiographic estimation of left ventricular and pulmonary pressures in patients with heart failure and preserved ejection fraction: a study utilizing simultaneous echocardiography and invasive measurements. Eur J Heart Fail. 2017, 19, 1651–1660. [Google Scholar] [CrossRef]
- Marini, C.; Fragasso, G.; Italia, L.; et al. Lung ultrasound-guided therapy reduces acute decompensation events in chronic heart failure. Heart. 2020, 106, 1934–1939. [Google Scholar] [CrossRef] [PubMed]
- Cuthbert, J.J.; Pellicori, P.; Flockton, R.; et al. The prevalence and clinical associations of ultrasound measures of congestion in patients at risk of developing heart failure. Eur J Heart Fail. 2021, 23, 1831–1840. [Google Scholar] [CrossRef]
- Ballo, P.; Guarini, G.; Simioniuc, A.; et al. Prognostic value of pulsed tissue Doppler imaging for the assessment of left ventricular systolic function in patients with nonischemic dilated cardiomyopathy. Echocardiography. 2012, 29, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Pellicori, P.; Carubelli, V.; Zhang, J.; et al. IVC Diameter in patients with chronic heart failure: relationships and prognostic significance. JACC Cardiovasc Imaging. 2013, 6, 16–28. [Google Scholar] [CrossRef]
- Jung, I.H.; Park, J.H.; Lee, J.; et al. Left Ventricular Global Longitudinal Strain as a Predictor for Left Ventricular Reverse Remodeling in Dilated Cardiomyopathy. J Cardiovasc Imaging. 2020, 28, 137–149. [Google Scholar] [CrossRef]
- Kaufmann, D.; Szwoch, M.; Kwiatkowska, J.; Raczak, G.; Daniłowicz-Szymanowicz, L. Global longitudinal strain can predict heart failure exacerbation in stable outpatients with ischemic left ventricular systolic dysfunction. PLoS One. 2019, 14, e0225829. [Google Scholar] [CrossRef]
- Nahum, J.; Bensaid, A.; Dussault, C.; et al. Impact of longitudinal myocardial deformation on the prognosis of chronic heart failure patients. Circ Cardiovasc Imaging. 2010, 3, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Sengeløv, M.; Jørgensen, P.G.; Jensen, J.S.; et al. Global Longitudinal Strain Is a Superior Predictor of All-Cause Mortality in Heart Failure with Reduced Ejection Fraction. JACC Cardiovasc Imaging. 2015, 8, 1351–1359. [Google Scholar] [CrossRef] [PubMed]
- Hasselberg, N.E.; Haugaa, K.H.; Sarvari, S.I.; et al. Left ventricular global longitudinal strain is associated with exercise capacity in failing hearts with preserved and reduced ejection fraction. Eur Heart J Cardiovasc Imaging. 2015, 16, 217–24. [Google Scholar] [CrossRef]
- Modin, D.; Andersen, D.M.; Biering-Sørensen, T. Echo and heart failure: when do people need an echo, and when do they need natriuretic peptides? Echo Res Pract. 2018, 5, R65–R79. [Google Scholar] [CrossRef]
- Carluccio, E.; Biagioli, P.; Mengoni, A.; et al. Left Atrial Reservoir Function and Outcome in Heart Failure With Reduced Ejection Fraction. Circ Cardiovasc Imaging. 2018, 11, e007696. [Google Scholar] [CrossRef]
- Guler, A.; Tigen, K.M.; Dundar, C.; et al. Left atrial deformation and nonischemic dilated cardiomyopathy. A 2D speckle-tracking imaging study. Herz. 2014, 39, 251–7. [Google Scholar] [CrossRef]
- Cameli, M.; Mandoli, G.E.; Loiacono, F.; Dini, F.L.; Henein, M.; Mondillo, S. Left atrial strain: a new parameter for assessment of left ventricular filling pressure. Heart Fail Rev. 2016, 21, 65–76. [Google Scholar] [CrossRef]
- Picano, E.; Pellikka, P.A. Clinical update Ultrasound of extravascular lung water : a new standard for pulmonary congestion. Eur Heart J. 2016, 37, 2097–104. [Google Scholar] [CrossRef]
- Volpicelli, G.; Lichtenstein, D.A.; Kirkpatrick, A.W.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–91. [Google Scholar] [CrossRef] [PubMed]
- Coiro, S.; Rossignol, P.; Ambrosio, G.; et al. Prognostic value of residual pulmonary congestion at discharge assessed by lung ultrasound imaging in heart failure. Eur J Heart Fail. 2015, 17, 1172–1181. [Google Scholar] [CrossRef] [PubMed]
- Gargani, L.; Pang, P.S.; Frassi, F.; et al. Persistent pulmonary congestion before discharge predicts rehospitalization in heart failure : a lung ultrasound study. Cardiovasc Ultrasound. 2015, 13, 40. [Google Scholar] [CrossRef]
- Miglioranza, M.H.; Picano, E.; Badano, L.P.; et al. Pulmonary congestion evaluated by lung ultrasound predicts decompensation in heart failure outpatients. Int J Cardiol. 2017, 240, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Platz, E.; Lewis, E.F.; Uno, H.; et al. Detection and prognostic value of pulmonary congestion by lung ultrasound in ambulatory heart failure patients. Eur Heart J. 2016, 37, 1244–1251. [Google Scholar] [CrossRef]
- Chaudhry, S.I.; Wang, Y.; Concato, J.; Concato, J.; Gill, T.M.; Krumholz, H.M. Patterns of weight change preceding hospitalization for heart failure. Circulation 2007, 116, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Bui, A.L.; Fonarow, G.C. Home monitoring for heart failure management. J Am Coll Cardiol. 2012, 59, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Riegel, B.; Moser, D.K.; Anker, S.D.; et al. State of the science: Promoting self-care in persons with heart failure: A scientific statement from the american heart association. Circulation 2009, 120, 1141–63. [Google Scholar] [CrossRef]
- Goldberg, L.R.; Piette, J.D.; Walsh, M.N.; et al. Randomized trial of a daily electronic home monitoring system in patients with advanced heart failure: the Weight Monitoring in Heart Failure (WHARF) trial. Am Heart J. 2003, 146, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Damman, K.; Harjola, V.-P.; et al. The use of diuretics in heart failure with congestion — a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2019, 21, 137–155. [Google Scholar] [CrossRef]
- Rudski, L.G.; Lai, W.W.; Afilalo, J.; et al. Guidelines for the Echocardiographic Assessment of the Right Heart in Adults: A Report from the American Society of Echocardiography Endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010, 23, 685–713. [Google Scholar] [CrossRef]
- Grant, A.D.M.; Smedira, N.G.; Starling, R.C.; Marwick, T.H. Independent and incremental role of quantitative right ventricular evaluation for the prediction of right ventricular failure after left ventricular assist device implantation. J Am Coll Cardiol. 2012, 60, 521–528. [Google Scholar] [CrossRef]
- Meluzín, J.; Špinarová, L.; Dušek, L.; Toman, J.; Hude, P.; Krejčí, J. Prognostic importance of the right ventricular function assessed by Doppler tissue imaging. Eur J Echocardiogr. 2003, 4, 262–271. [Google Scholar] [CrossRef]
- Almodares, Q.; Wallentin Guron, C.; Thurin, A.; et al. Larger right atrium than left atrium is associated with all-cause mortality in elderly patients with heart failure. Echocardiography. 2017, 34, 662–667. [Google Scholar] [CrossRef]
- Kato, T.S.; Stevens, G.R.; Jiang, J.; et al. Risk stratification of ambulatory patients with advanced heart failure undergoing evaluation for heart transplantation. J Hear Lung Transplant. 2013, 32, 333–340. [Google Scholar] [CrossRef]
- Kircher, B.J.; Himelman, R.B.; Schiller, N.B. Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol. 1990, 66, 493–6. [Google Scholar] [CrossRef] [PubMed]
- Nath, J.; Vacek, J.L.; Heidenreich, P.A. A dilated inferior vena cava is a marker of poor survival. Am Heart J. 2006, 151, 730–5. [Google Scholar] [CrossRef] [PubMed]
- Curbelo, J.; Rodriguez-Cortes, P.; Aguilera, M.; Gil-Martinez, P.; Martín, D.; Fernandez, C.S. Comparison between inferior vena cava ultrasound, lung ultrasound, bioelectric impedance analysis and natriuretic peptides in chronic heart failure. Curr Med Res Opin. 2019, 35, 705–713. [Google Scholar] [CrossRef] [PubMed]
- Razi, R.; Estrada, J.R.; Doll, J.; Spencer, K.T. Echocardiography At The “Point Of Care” Bedside Hand-Carried Ultrasound by Internal Medicine Residents Versus Traditional Clinical Assessment for the Identification of Systolic Dysfunction in Patients Admitted with Decompensated Heart Failure. J Am Soc Echocardiogr. 2011, 24, 1319–1324. [Google Scholar] [CrossRef] [PubMed]
- Dalen, H.; Gundersen, G.H.; Skjetne, K.; et al. Feasibility and reliability of pocket-size ultrasound examinations of the pleural cavities and vena cava inferior performed by nurses in an outpatient heart failure clinic. Eur J Cardiovasc Nurs. 2015, 14, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Gundersen, G.H.; Norekval, T.M.; Haug, H.H.; et al. Adding point of care ultrasound to assess volume status in heart failure patients in a nurse-led outpatient clinic. A randomised study. Heart. 2016, 102, 29–34. [Google Scholar] [CrossRef]
- Saha, N.M.; Barbat, J.J.; Fedson, S.; Anderson, A.; Rich, J.D.; Spencer, K.T. Outpatient Use of Focused Cardiac Ultrasound to Assess the Inferior Vena Cava in Patients With Heart Failure. Am J Cardiol. 2015, 116, 1224–1228. [Google Scholar] [CrossRef]
- Curbelo, J.; Aguilera, M.; Rodriguez-Cortes, P.; Gil-Martinez, P.; Fernandez, C.S. Usefulness of inferior vena cava ultrasonography in outpatients with chronic heart failure. Clin Cardiol. 2018, 41, 510–517. [Google Scholar] [CrossRef]
- Lee, H.F.; Hsu, L.A.; Chang, C.J.; et al. Prognostic significance of dilated inferior vena cava in advanced decompensated heart failure. Int J Cardiovasc Imaging. 2014, 30, 1289–1295. [Google Scholar] [CrossRef]
Figure 1.
(A) Peak velocity of the early diastolic flow across the mitral valve (E wave) measured by pulsed-wave Doppler; (B) Early diastolic velocity of the septal mitral annulus obtained by Tissue Doppler echocardiography.
Figure 1.
(A) Peak velocity of the early diastolic flow across the mitral valve (E wave) measured by pulsed-wave Doppler; (B) Early diastolic velocity of the septal mitral annulus obtained by Tissue Doppler echocardiography.
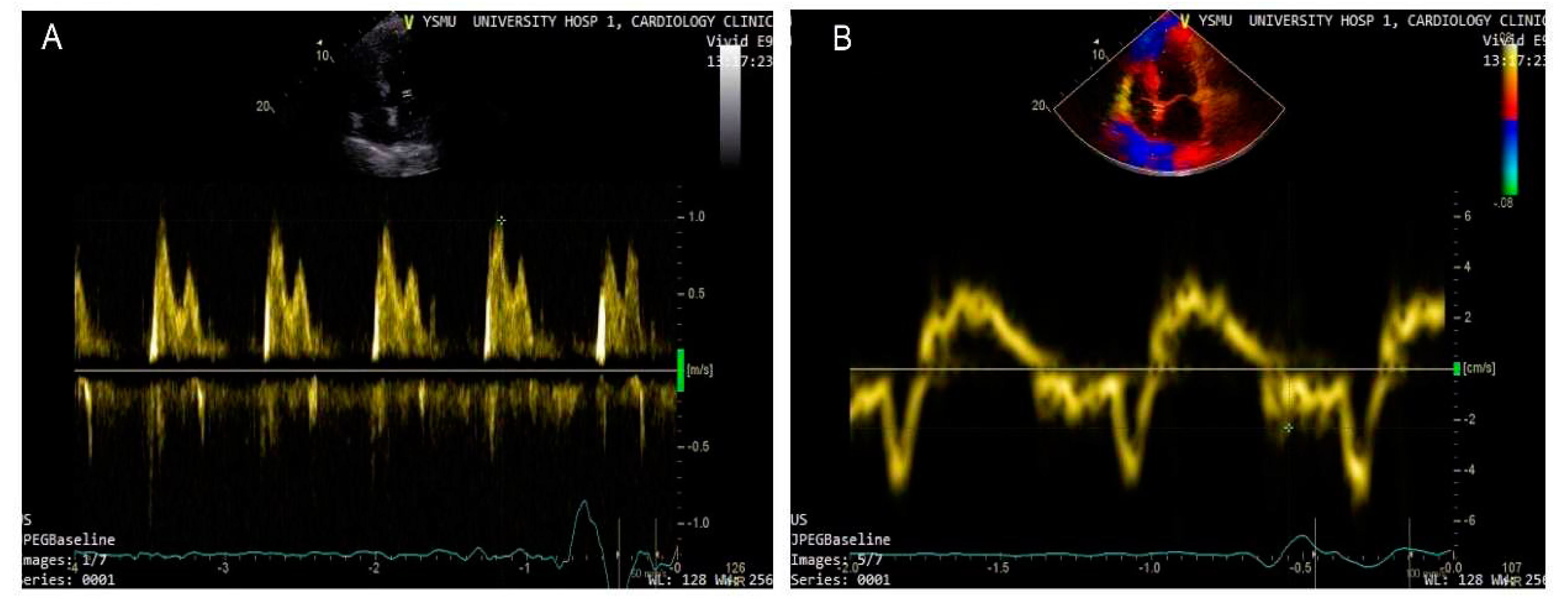
Figure 2.
(A) 2-3 moderate B-lines at lung ultrasound; (B) Wide B lines detected by bedside point-of-care ultrasound in a patient with acute decompensated HF in CCU. .
Figure 2.
(A) 2-3 moderate B-lines at lung ultrasound; (B) Wide B lines detected by bedside point-of-care ultrasound in a patient with acute decompensated HF in CCU. .
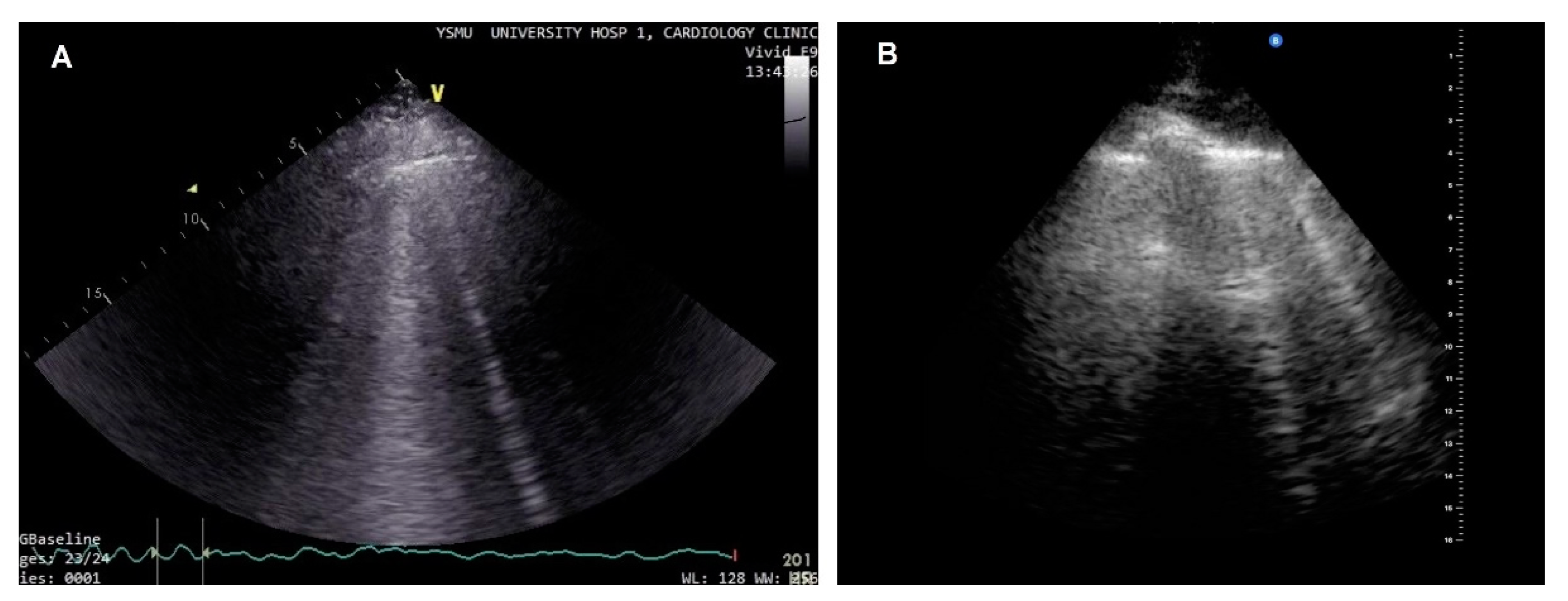
Figure 3.
(A) Increased IVC diameter in a patient with high right atrial pressure; (B) IVC with an impaired collapse (< 50%) on inspiration.
Figure 3.
(A) Increased IVC diameter in a patient with high right atrial pressure; (B) IVC with an impaired collapse (< 50%) on inspiration.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



