Submitted:
12 August 2023
Posted:
15 August 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Long Covid is a heterogeneous clinical condition in which Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and brain fog stand out among the different clinical symptoms and syndromes. The cerebral metabolic alterations and neuroendocrine disorders seem to constitute an important part of Long Covid. Given the substantial lack of drugs and effective therapeutic strategies, hypothalamic phospholipid liposomes which have been on the market for several years as adjuvant therapy of cerebral metabolic alterations resulting from neuroendocrine disorders, can be taken into consideration in an overall therapeutic strategy that aims to control the Long Covid associated symptoms and syndromes. Their pharmacological mechanisms and clinical effects strongly support their usefulness in Long Covid. Our initial clinical experience corroborates this rationale. Further research is imperative in order to obtain robust clinical evidence.
Keywords:
Covid-19
; post-COVID syndrome
; neuroendocrine disorders
; chronic fatigue
; brain fog
; phospholipids
; phospholipid liposome
; phosphatidylserine
1. Introduction
The COVID-19 pandemic caused in Italy, by April 2023, over 25 million of documented infection cases and about 190,000 deaths [1]. Beyond the devastating impact on hospital services which, in the first pandemic phase (2020–2021), were engaged almost exclusively in dealing with COVID-19, and a serious delay in taking care of other pathologies, despite having now the epidemic wave under control, thanks to vaccines and wise behavior, a new pathological entity has emerged that seems to be a direct consequence of the SARS-CoV-2 infection: Post COVID-19 condition (commonly known as Long COVID) [2,3,4,5]. We analyze the potential role of hypothalamic phospholipid liposomes as an adjuvant therapy for some important manifestations of Post COVID-19 condition, such as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome and brain fog, based on the current knowledge on Post COVID-19 condition and hypothalamic phospholipid liposomes’ pharmacology.
2. Definition and epidemiology of Post COVID-19 condition
Many definitions have been adopted to describe this complex of symptoms and syndromes that may follow the COVID-19 infection [2,3]. The term “Post COVID-19 condition” (PCC) has been adopted by the World Health Organization (WHO) and the Center for Disease Control (CDC) and it refers to a wide range of sequelae that compromise the physical and mental health of some patients and that occur after SARS-CoV-2 infection [3,6]. PCC is referred to by a wide range of names, including: Long COVID, Post-acute COVID-19, Long-term effects of COVID, Post-acute COVID syndrome, chronic COVID, long-lasting COVID, Late sequelae, Post-acute sequelae of SARS-COV-2 infection (PASC).
The CDC indicates that PCC is present if recovery does not occur within 4 weeks after the acute phase, although many patients may continue to improve within 12 weeks [6,7]. After 12 weeks persistent illness becomes more likely [7]. In fact, the WHO defines PCC as a condition occurring 3 months after acute infection, lasting for at least 2 months [3]. However, the 4-week threshold allows a rapid identification and treatment of PCC [8]. The CDC uses the 4-week period to define PCC and emphasizes the importance of initial clinical evaluation and supportive care during the initial 4–12 weeks after acute COVID-19 [7].
The prevalence of PCC is difficult to estimate, with studies reporting a range from 5 to 30% [7,9]. The variety of symptoms or conditions studied, the time criteria used (from three weeks to many months after SARS-CoV-2 infection), the population studied (outpatient vs. hospitalized patients), and the method used to evaluate symptoms and conditions (e.g., self-reporting vs. electronic health record database) are a few factors that contribute to these wide-ranging prevalence estimates [7,10,11,12]. Recent data have shown that up to 18% of SARS-CoV-2 infected individuals are affected by PCC two years after infection, even though a decrease in the severity of symptoms and health impairment may be seen over time [13]. CDC data demonstrate that women, bisexual and transgender adults, as well as adults with disabilities are more likely to have PCC [14].
3. Clinical Symptoms & Syndromes
The PCC manifestations comprise a long list of symptoms referred to different apparatus (Table 1). Core symptoms include fatigue, brain fog, breathlessness, anosmia and mental health problems among others [15].
The heterogeneity of this condition is further demonstrated by its different patterns of onset, such as [7]:
- persistent symptoms and conditions that begin at the time of acute COVID-19 illness,
- signs, symptoms or conditions of new onset following asymptomatic illness or a period of improvement or remission of acute symptoms,
- evolution of symptoms and conditions which include some persistent symptoms (e.g., shortness of breath) with the addition of new symptoms (e.g., cognitive difficulties),
- worsening of pre-existing symptoms or conditions.
Some manifestations may share similarities with other post-infectious syndromes, such as Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), Fibromyalgia (FM), post-treatment Lyme diseases syndrome (PTLDS), Postural Orthostatic Tachycardia Syndrome (POTS) and other forms of dysautonomia, or Mast Cell Activation Syndrome (MCAS). Some of these conditions have also been described in patients with Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS), two other life-threatening diseases resulting from coronavirus infections [7,16].
A wide range of other symptoms, new or already present, can occur in people who have suffered from SARS-CoV-2 acute disease of varying degrees, including mild asymptomatic form [10,12]. These symptoms may overlap with multiple organ complications or the effects of treatment or hospitalization. It can be difficult to distinguish the symptoms of PCC from those that have other causes. It is therefore always necessary to consider alternative diagnoses in order to avoid serious diagnostic errors, in cases of patients presenting with symptoms such as dyspnea, chest pain, neurological disorders, etc. [17].

| Post COVID syndrome | Clinical manifestations | Comment |
| Post COVID fatigue syndrome | Profound fatigue, post-exertion malaise and/or poor resistance | Rule out causes like anemia, electrolyte imbalance, hypothyroidism, |
| Post COVID cardio-respiratory Syndrome | Cough, dyspnea or increased fatigue, low grade fever, chest pain, orthostatic hypotension, palpitations, and tachycardia | Sudden worsening of dyspnea: Consider tension pneumothorax, pulmonary embolism, coronary artery disease or heart failure. |
| Post COVID neuro-psychiatric Syndrome | Headaches, anosmia or dysgeusia, cognitive impairment or “brain fog”, depression and other mood changes, paresthesia, insomnia and other sleep difficulties, dizziness | If acute onset neurological symptoms also consider vasculitis, thrombosis or demyelination. Properly evaluate post-COVID psychological problems. |
| Post COVID gastro-intestinal Syndrome | Abdominal discomfort, diarrhea, constipation, vomiting | GI symptoms can be a sequalae of the disease or therapy-related side effects |
| Post COVID hepato-biliary Syndrome | Nausea, jaundice, Liver Function Tests alterations | Drugs used in the treatment of COVID-19 can cause hepatic impairment. |
| Post COVID musculo-skeletal Syndrome | Arthralgia, myalgia, muscle weakness | Causes include: COVID-19 disease, prolonged ICU care, neurological problems, myopathy, or electrolyte imbalance. Usually subside during follow up. Inflammatory arthralgia must be differentiated from other causes like Systemic Lupus Erythematosus, Rheumatoid Arthritis. |
| Post COVID thromboembolic Syndrome | Depending upon the vascular territory of involvement dyspnea in Pulmonary Embolism, chest pain in Coronary Artery Disease and limb weakness and neurological deficit in stroke | Early diagnosis and treatment are lifesaving. Follow the standard treatment protocol. |
| Post COVID multisystem inflammatory syndrome/post COVID autoimmune syndrome | Fever, gastrointestinal symptoms, rash, chest pain, Palpitations | Elevated levels of markers of inflammation. |
| Post COVID genito-urinary Symptoms | Proteinuria, hematuria, development of kidney injury, menstrual cycle irregularities, erectile dysfunction | COVID-19 may predispose surviving patients to chronic kidney disease, independently of clinically apparent acute kidney injury (AKI). Therefore, post-acute COVID-19 care should include close attention to kidney function. |
| Post COVID dermatological Syndrome | Vesicular, maculopapular, urticarial, or chilblain-like lesions on the extremities (COVID toe) |
PCC has a substantial impact on ability to work and activities of daily living [7,15]. Patients suffering from PCC show high levels of functional impairment and low health-related quality of life. These results seem to be comparable to, or even worse than, those of patients suffering from diseases such as Parkinson’s disease, stroke or advanced/metastatic cancers [15]. Fatigue appears to be the symptom most strongly associated with functional impairment, causing significant impact on the patients’ ability to work and care for others [15].
3.1. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
This condition has been already described as a consequence of viral infections, (e.g., after infectious mononucleosis, especially in patients who present the prolonged persistence of anti-EBV IgM). Considered by many a pathological condition with a strong neuropsychiatric component, ME/CFS is one of the most prevalent and most disabling syndromes in PCC [19,20,21,22].
According to the National Academy of Medicine, the diagnosis of ME/CFS requires the concomitant presence of the following three symptoms [19]:
1. Substantial reduction or alteration of employment, educational, social, or personal capacities that persists for more than 6 months and is accompanied by asthenia, often profound, of new or recent onset (not pre-existing), is not the result of continuous excessive effort, and is not effectively alleviated by rest
2. Post-exertion malaise
3. Non-restorative sleep
The presence of cognitive impairment and/or orthostatic intolerance is also required for the diagnosis [19]. Symptoms of post-exertion malaise, non-restorative sleep and cognitive impairment should be of at least of moderate intensity and present at least 50% of the time during a 6-month period to make the diagnosis of ME/CFS [19].
The possible mechanisms that cause Post COVID-19 fatigue comprise a wide range of central, peripheral and psychological factors [20,21,22,23]. Chronic inflammation in the brain, as well as in the neuromuscular junctions, can result in chronic fatigue [23]. Damage and atrophy of skeletal muscle fibers have been proposed to play a role as well [22,23] (Figure 1).
3.2. Cognitive impairment
Cognitive symptoms are a major feature of PCC [16]. Often referred to by patients as “brain fog”, cognitive impairment in PCC affects different domains with memory problems and attention difficulties being its most notable manifestations [13,24]. Activities of daily living are frequently impacted by cognitive impairment in PCC and research suggests that it may be as debilitating as 10 years of cognitive ageing [16].
Several underlying mechanisms of cognitive impairment have been hypothesized in PCC: hypometabolic activity in various brain areas, a reduced inhibitory activity of GABA, but also neuroinflammatory phenomena with cerebral microstructural modifications and vascular disorders [21,23,25,26].
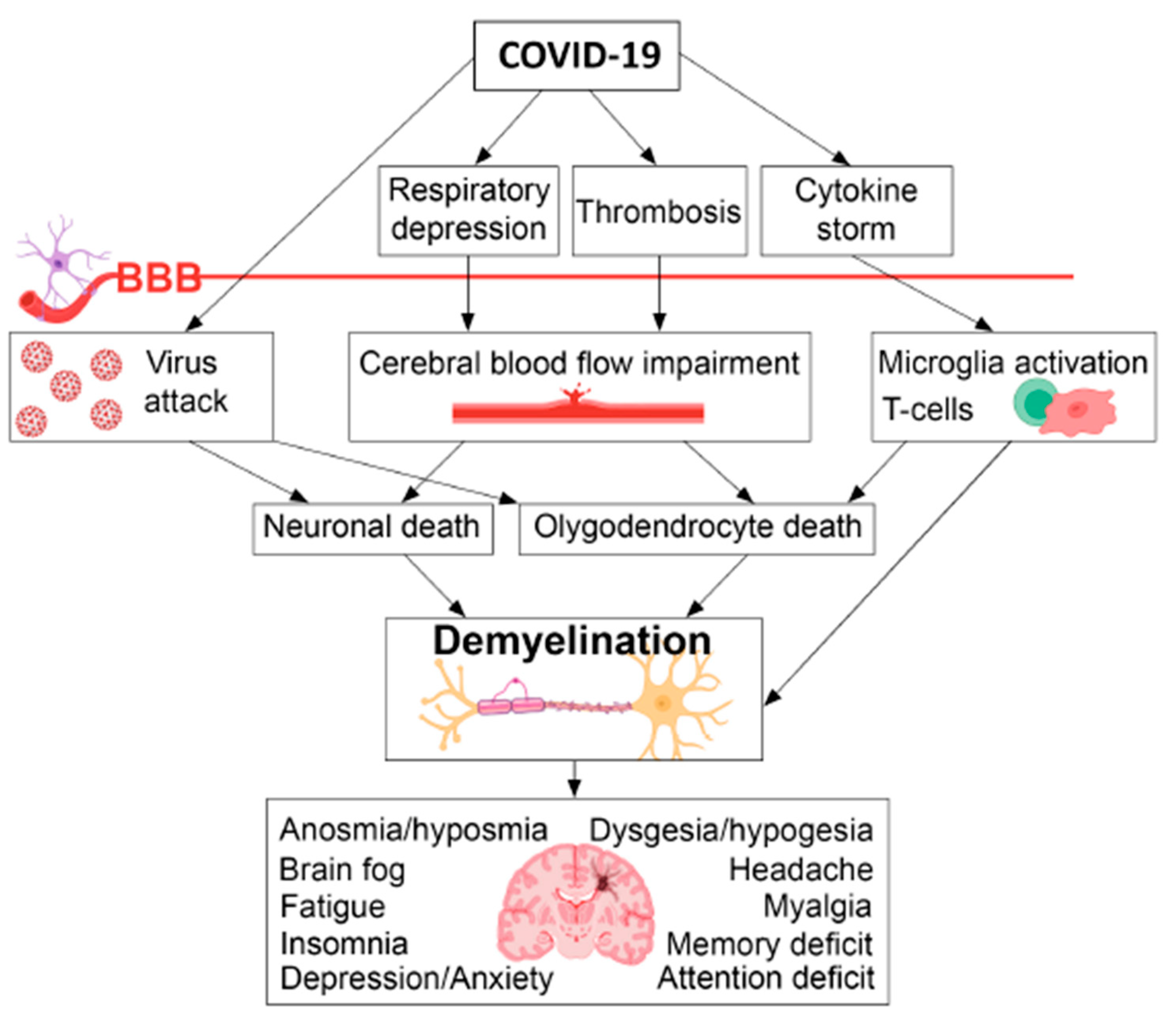
One explanation of the multiple neuro-cognitive symptoms of PCC may be demyelination generated by the concomitant action of viral replication, alterations of cerebral microcirculation and activation of microglia T cells (Figure 2) [27]. The neuroradiological findings are however modest and sporadic, because a very limited number of studies have used highly sensitive techniques for myelin quantification [27].
Another hypothesis that received attention because it might offer either a comprehensive pathophysiological understanding of the mechanism underlying several manifestations of PCC or some therapeutic perspectives, refers to the generation of amyloid fibrin micro-clots in the vascular system [28]. This hypothesis, supported by an elegant although isolated scientific report, has however generated the uncontrolled use of expensive treatments whose real effectiveness is at least doubtful: blood washing and triple anticoagulation therapy [29]. Many patients turn to private facilities in Europe to undergo apheresis procedures, spending a lot of money for a procedure without clear evidence of efficacy [29].
The National Institute of Health has committed more than 1 USD billion to post-COVID-19 research, and the WHO is coordinating global efforts [30]. Although it is challenging to fully understand and address the post-infectious sequelae of SARS-CoV-2, doing so will increase the likelihood of finding effective therapies [30].
In the meantime, several drugs and nutrients have been proposed and tested to control PCC clinical manifestations (e.g., low molecular weight heparin, vitamin D, etc.) [31,32,33]. Nevertheless, we are dealing with a substantial lack of specific drugs and effective therapeutic strategies [15]. It is therefore necessary to try to help every single patient by also considering the potential role of preparations that have been on the market for several years, with an excellent safety profile, which can be taken into consideration in an overall therapeutic strategy that aims to control the PCC associated symptoms and syndromes.
4. The potential role of hypothalamic phospholipid liposomes in Post COVID-19 condition
In COVID-19, important variations in sphingolipids and glycerophospholipids have been described: the increase in the blood level of specific compound seems to be correlated with the degree of disease severity [34,35,36,37]. In particular, elevated levels of phosphatidylcholine (PC) correlate with a less severe form of COVID-19 and this could be useful both as a prognostic marker and as a potential therapeutic intervention [37]. Furthermore, alterations of phospholipid metabolism as well as phospholipid composition of cellular structures (such as the mitochondria of microglia), have also been reported in the literature [38,39]. On the other hand, various complex mechanisms underly the pathophysiology of PCC including cerebral metabolism alterations and neuroendocrine disorders [40]. Indeed, recent findings that SARS-CoV-2 spike protein can bind to the receptors of the neuroendocrine system shed light on the neuroendocrine involvement in COVID-19 [41]. Additionally, the levels of copeptin, a neuroendocrine biomarker of the stress response by Hypothalamic-Pituitary axis, correlate with COVID-19 severity [42]. COVID-19 infection alters the Hypothalamic-Pituitary-Adrenal (HPA) axis due to direct viral infection of hypothalamic structures or the effect of pro-inflammatory cytokines [43,44]. Finally, among the heterogenous clinical manifestations of PCC, ME/CFS is a syndrome characterized by the presence of neuroendocrine disorders as part of its pathophysiological and clinical features [45,46].
In this view, taking into account the alterations of the phospholipid metabolism, as well as the importance of the neuroendocrine disorders in the pathophysiology and the clinical manifestations of PCC, a medicine containing a mixture of hypothalamic phospholipids (Liposom Forte®) indicated as “adjuvant therapy of cerebral metabolic alterations resulting from neuroendocrine disorders” elicits particular interest [47,48]. Liposom Forte® is a mixture of hypothalamic phospholipids in the form of liposomes. It is extracted from porcine brain and its major components are phosphatidylcholine (PC), phosphatidylethanolamine (PE) and phosphatidylserine (PS), representing all together about 90% of the total phospholipids of the mixture [47]. Hypothalamic phospholipid liposomes reach the central nervous system where they exert different effects by influencing the physicochemical and structural properties of the neural membrane, as well as by affecting its function and that of the related cellular structures [47,48]. Liposom Forte® has shown an excellent safety profile during its long-time presence on the market [47]. Its mechanism of action, as well as the clinical evidence on its efficacy, offer a strong rationale on the use of hypothalamic phospholipid liposomes in PCC.
4.1. Pathophysiological mechanisms in Post COVID-19 condition and the pharmacology of hypothalamic phospholipid liposomes
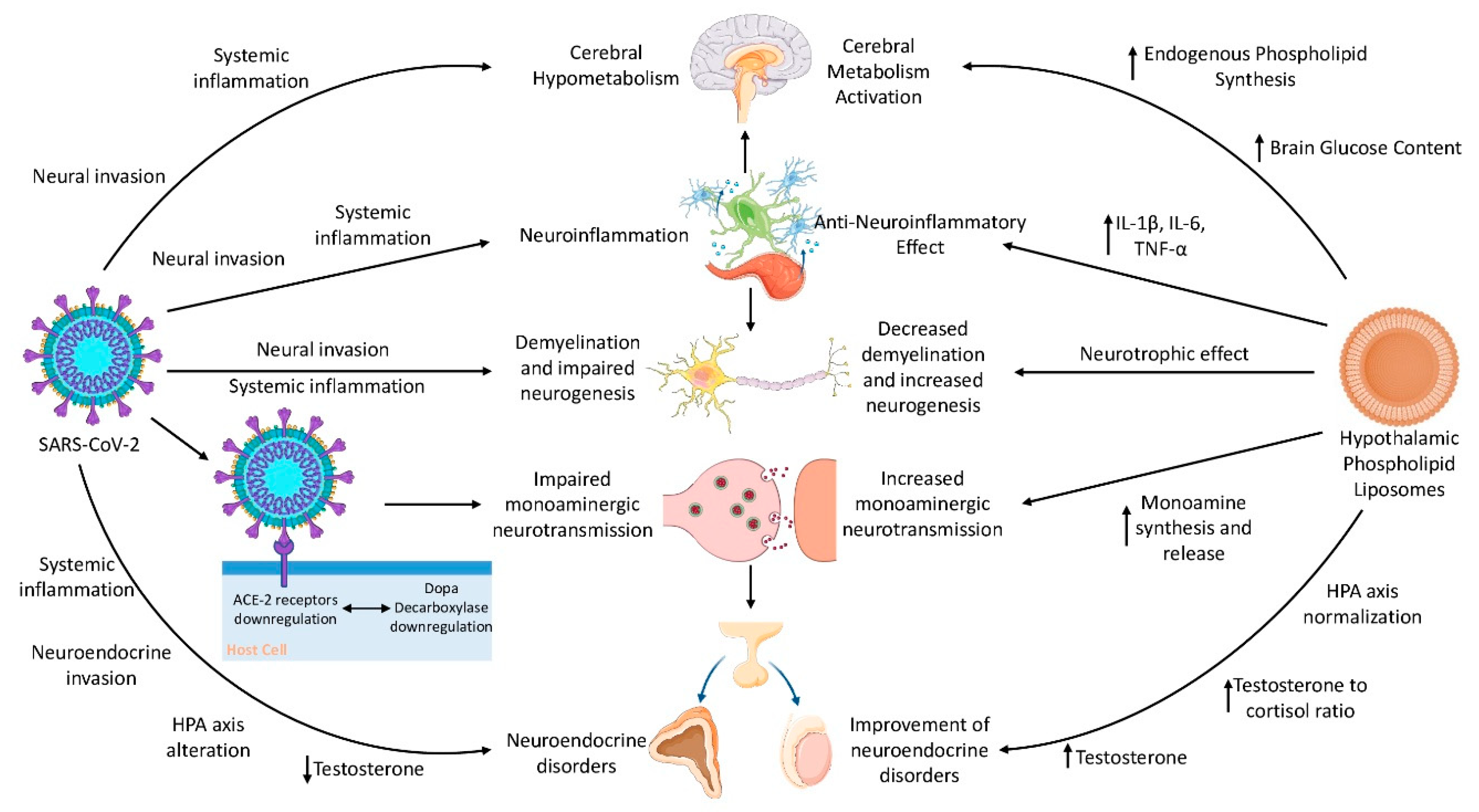
There are many mechanisms by which hypothalamic phospholipid liposomes could benefit patients with PCC, especially those affected by ME/CFS and brain fog. We explore here the pathophysiological mechanisms of PCC that may be the target of some of the pharmacological effects of hypothalamic phospholipid liposomes (Figure 3).
4.1.1. The monoaminergic hypothesis
Monoaminergic neurotransmission alterations have been proposed as a potential pathophysiological mechanism for the neuropsychiatric manifestations of PCC [49]. This is suggested by a significant link between Angiotensin I Converting Enzyme 2 (ACE2, encoding the main receptor to SARS-CoV-2) and Dopa Decarboxylase (DDC, encoding the enzyme that catalyzes the biosynthesis of dopamine, noradrenaline and serotonin). Indeed, the gene exhibiting the most statistically significant co-expression link with ACE2 is DDC [49]. The co-expression and co-regulation of ACE2 and DDC is corroborated by findings such as high ACE2 expression in dopaminergic neurons and its reduction in Parkinson’s disease (characterized by dopamine deficiency) [50], the increase in brain dopamine content following infusion of angiotensin 1–7 in the hypothalamus of rats [51], as well as dramatically low serotonin levels in the blood and the brain of ACE2 knockout mice [52]. SARS-CoV-2 is a neuroinvasive and neurotropic virus able to infect neural cells through binding of the ACE2 receptor [53]. Given that upon infection, SARS-CoV-2 down-regulates ACE2 [54], the defective expression of ACE2 might be paralleled by a DDC dysfunction, with consequent potentially altered neurotransmitters’ levels in the brain [43]. This mechanism could explain some of Post COVID-19 condition’s neuropsychiatric manifestations such as anxiety, depression and chronic fatigue [55]. Indeed, the alterations in dopamine and serotonin homeostasis are deeply involved in the development of fatigue [56,57].
On the other hand, there is extensive preclinical and clinical evidence that hypothalamic phospholipid liposomes increase monoaminergic neurotransmission, as shown by the activation of tyrosine hydroxylase (the rate limiting-enzyme in the synthetic pathway of dopamine and other catecholamines); the increase in monoamines turnover and release; the stimulation of the dopamine-dependent adenylyl cyclase and the increase in dopamine metabolite levels in human cerebrospinal fluid (CSF); the decrease of prolactin secretion, through a dopamine agonist activity (being dopamine the main inhibitor of the prolactin synthesis and release) and finally, the modification of the receptor adaptation of central aminergic neurons to chronic treatment with antidepressants [47,48,58,59,60,61]. The monoaminergic effect of hypothalamic phospholipid liposomes renders them highly relevant for the treatment of fatigue, where a dopaminergic effect is particularly needed, as well as for the treatment of other COVID-19 neuropsychiatric sequalae, such as anxiety and depression.
4.1.2. Neuroinflammation, demyelination and impaired neurogenesis
Other pathophysiological mechanisms potentially of great importance in PCC, such as neuroinflammation, demyelination and impaired neurogenesis, have also been corroborated from animal model and human studies [23,27,62,63]. Even in mild COVID-19 infection, the inflammatory response caused by the respiratory COVID-19 induces neuroinflammation through CSF cytokine elevation and microglial reactivity [23,64]. Interleukins with anti-neurogenic effects such as IL-1β and IL-6 are particularly elevated in the brain of COVID-19 subjects, which leads to neuronal damage and impaired neurogenesis in structures such as hippocampus, explaining learning, memory and executive dysfunctions [64]. Neuroinflammation, probably in combination with other factors such as direct effect of the virus on oligodendrocytes and cerebrovascular disorders, causes persistent loss of oligodendrocytes and demyelination [27,64]. Numerous reviews, theoretical and experimental studies convincingly indicate that demyelination may underlie many neuropsychiatric sequalae of COVID-19 [27].
Hypothalamic phospholipid liposomes exert e neurotrophic effect by improving the membrane structure and function, increasing endogenous phospholipid synthesis, and promoting dendritogenesis, as demonstrated by increased dendritic spines’ density [47,48]. Additionally, studies using animal models have demonstrated the antagonizing effect of phospholipids on demyelination, emphasizing the importance of phospholipid metabolism in myelination and myelin maintenance [65,66,67]. These studies suggest that phosphatidylcholine and phosphatidylethanolamine ameliorate myelination deficit [66], whereas phosphatidylserine prevents autoimmune demyelination [67]. Furthermore, recent preclinical studies have shown that hypothalamic phospholipid liposomes have a positive effect on hippocampal neurogenesis and an antagonizing effect on neuroinflammation [48]. Chronic treatment with hypothalamic phospholipid liposomes has been shown to reverse and prevent the reduction of neurogenesis induced by chronic stress in the dentate gyrus of the hippocampus in a study on rats [48]. Meanwhile, in a model of neuro-inflammation induced by lipopolysaccharide (LPS) injection, hypothalamic phospholipid liposomes antagonized in a dose-dependent manner the proinflammatory cytokine release elicited by LPS (IL-1β, IL-6, TNF-α) [47]. These effects on neuroplasticity and on the cytokines involved in COVID-induced neuroinflammation, further strengthen hypothalamic phospholipid liposomes’ relevance in the treatment of PCC.
4.1.3. Cerebral hypometabolism
Case-control, cohort and case studies using [18F] fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG-PET/CT) suggest that cerebral metabolic alterations may be responsible for the neurocognitive findings in PCC [68,69,70,71,72,73]. Hypometabolism of different brain areas (especially of the frontal cortex) in PCC patients suffering from neurocognitive symptoms is the main finding of these studies [72]. Hypothalamic phospholipid liposomes activate cerebral metabolism by increasing brain glucose content and phospholipid synthesis [47]. In addition, they are specifically indicated as adjuvant treatment in cerebral metabolic alterations caused by neuroendocrine disorders [48].
4.1.4. Male fertility alterations
Low serum testosterone levels have been encountered in as much as 30% of men, up to 12 months after COVID-19 infection [74]. Low testosterone in combination with other alterations such as psychological stress, activation of HPA axis and low dopamine levels, may contribute to erectile dysfunction and loss of libido [43,75,76,77]. Meanwhile, in male athletes, phosphatidylserine has been shown to increase plasma levels of testosterone compared to placebo [78] as well as increase testosterone to cortisol ratio in an exercise-related context [79]. Furthermore, it has been hypothesized that phospholipids increase the capacity of high-density lipoproteins (HDL) to take up free cholesterol from the cytoplasm membrane of peripheral cells and to transport it in the esterified form to the steroid producing glands where it serves as a precursor to steroid hormones such as testosterone [80]. These effects, together with the normalizing effect on HPA axis and the dopaminergic effect of hypothalamic phospholipid liposomes [47], may account for their potential beneficial role in male sexual health alterations.
Figure 3.
A schematic representation of Post COVID-19 condition’s pathophysiology and the relevant hypothalamic phospholipid liposomes’ mechanism of action (ACE-2—Angiotensin I Converting Enzyme 2; IL-1β—Interleukin 1β; IL-6—Interleukin 6; TNF-α—Tumor Necrosis Factor α; HPA axis—Hypothalamic-Pituitary-Adrenal axis). Parts of the figure were drawn by using pictures from Servier Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License (https://creativecommons.org/licenses/by/3.0/).
Figure 3.
A schematic representation of Post COVID-19 condition’s pathophysiology and the relevant hypothalamic phospholipid liposomes’ mechanism of action (ACE-2—Angiotensin I Converting Enzyme 2; IL-1β—Interleukin 1β; IL-6—Interleukin 6; TNF-α—Tumor Necrosis Factor α; HPA axis—Hypothalamic-Pituitary-Adrenal axis). Parts of the figure were drawn by using pictures from Servier Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License (https://creativecommons.org/licenses/by/3.0/).
4.2. Clinical evidence on hypothalamic phospholipid liposomes and its implications for Post COVID-19 condition
Although there are currently no published clinical studies on the efficacy of hypothalamic phospholipid liposomes in PCC, available evidence in other conditions supports their potential clinical relevance as a therapeutic option for PCC, in particular for symptoms such as anxiety and depression, chronic fatigue, brain fog, and potentially for orthostatic intolerance and male sexual health problems as well (Table 2).
Clinical evidence on the efficacy and safety of hypothalamic phospholipid liposomes (Liposom Forte®) has been generated in open studies with and without a control group, in drug-controlled trials and in double-blind, randomized, placebo-controlled trials [47]. Hypothalamic phospholipid liposomes, as add-on treatment to antidepressant therapy, further improve depressive symptomatology while reducing antidepressant effect latency compared to antidepressant therapy alone [47,81,82,83]. In a double-blind, randomized, placebo-controlled trial hypothalamic phospholipid liposomes in monotherapy were active against mild anxiety and depressive symptoms in menopausal women [84].
Furthermore, hypothalamic phospholipid liposomes have shown efficacy against other clinical symptoms which are commonly encountered in PCC. They improve asthenia caused by menopause [84] or induced by trazodone [83]. Additionally, hypothalamic phospholipid liposomes are effective against restlessness and dizziness [84]. Furthermore, hypothalamic phospholipid liposomes antagonized the hypotension and the reflex tachycardia caused by trazodone [83].
Taking into consideration that hypothalamic phospholipid liposomes contain different phospholipids, efforts have been made to identify the effect of the specific phospholipids in the mixture. Evidence during the initial phases of research suggested that phosphatidylserine might be the active ingredient of the mixture [85]. Phosphatidylserine is an essential component of the cerebral cortex and is associated with cognitive function [86]. In 2003, based on preliminary evidence, FDA authorized a Qualified Health Claim that phosphatidylserine may reduce the risk of dementia and cognitive dysfunction in the elderly [87]. In a more recent meta-analysis phosphatidylserine was shown to improve age-associated cognitive decline, especially memory, with no adverse effects [86]. Furthermore, phosphatidylserine has been shown to benefit the memory of a small group of patients with Alzheimer’s disease [88]. These data suggest that phosphatidylserine may also display its clinical benefits against cognitive dysfunction caused by PCC, widely known as brain fog.
Additionally, preliminary evidence from an open clinical study has demonstrated that phospholipids (mainly phosphatidylcholine) may be useful and well tolerated in the treatment of male sexual disorders such as erectile dysfunction and loss of libido [80].
Considering the clinical relevance of ME/CFS and brain fog, as well as the substantial lack of specific pharmaco-therapy, before considering drugs of the class of selective serotonin reuptake inhibitors (SSRIs) that could generate benefit in selected patients with ME/CFS [89], it seems reliable to try one or more treatment cycles with hypothalamic phospholipid liposomes, following a therapeutic regimen already proved to be safe and effective in previous clinical trials (one vial of Liposom Forte® twice a day) [83,90]. Indeed, our initial clinical experience seems to corroborate the scientific rationale on hypothalamic phospholipid liposomes’ effectiveness in PCC. Additionally, hypothalamic phospholipid liposomes, by providing a rapid clinical improvement [47,48,81,82,83,84], may also decrease the excess costs of patients suffering from PCC, another important burden of this condition [91]. Nevertheless, it must be emphasized that pharmacotherapy should be part of an integrated multidisciplinary approach including treatments such as physical and neuro-cognitive rehabilitation [8].
Therefore, it is imperative to make any effort to collect more extensive and robust clinical data, observing a cohort of treated patients, evaluating them with a point-by-point questionnaire administered before and after therapy and using an adequate follow-up of at least 3–6 months. The urgency to find adequate responses for patients with PCC must not exempt itself from adopting the research methods required by evidence-based medicine.
Table 2.
Post COVID-19 condition’s pathophysiology and clinical manifestations matched to the relevant hypothalamic phospholipid liposomes’ mechanism of action and clinical evidence (ACE2—Angiotensin I Converting Enzyme 2; IL-1β—Interleukin 1β; IL-6—Interleukin 6; TNF-α—Tumor Necrosis Factor α; PE—Phosphatidylethanolamine; PC—Phosphatidylcholine; PS—Phosphatidylserine).
Table 2.
Post COVID-19 condition’s pathophysiology and clinical manifestations matched to the relevant hypothalamic phospholipid liposomes’ mechanism of action and clinical evidence (ACE2—Angiotensin I Converting Enzyme 2; IL-1β—Interleukin 1β; IL-6—Interleukin 6; TNF-α—Tumor Necrosis Factor α; PE—Phosphatidylethanolamine; PC—Phosphatidylcholine; PS—Phosphatidylserine).
| Post COVID-19 condition | Hypothalamic phospholipid liposomes |
|---|---|
| Pathophysiology | Mechanism of action |
| Hypometabolic activity in certain brain areas [72] | Activation of cerebral metabolism (i.e., increased brain glucose content and phospholipid synthesis) [47] |
| ACE2-Dopa Decarboxylase co-expression which leads to impaired monoaminergic neurotransmission [49] | Increased catecholamine turnover and release, stimulation of tyrosine hydroxylase and dopamine dependent adenylyl cyclase, modification of monoaminergic receptor adaptation [47,48] |
| Neuroinflammation from CSF cytokine elevation (e.g., IL-1β, IL-6) and microglial reactivity [23,62,64] | Antagonizing effect on proinflammatory cytokines (IL-1β, IL-6, TNF-α) in different brain areas [47] |
| Demyelination and impaired neurogenesis [27,64] | Neurotrophic effect, increase in neurogenesis and dendritogenesis, as well as antagonizing effect of PE, PC and PS on demyelination [48,66,67] |
| Low testosterone [74,77] | PS increases plasma levels of testosterone compared to placebo and the testosterone to cortisol ratio in an exercise-related context [78,79] |
| Clinical manifestations | Clinical evidence |
| Fatigue | Improvement of asthenia [83,84] |
| Brain fog | PS: |
| Anxiety and depression | Improvement in the symptomatology of anxiety and depression as monotherapy or add-on to antidepressants [47,48] |
| Orthostatic intolerance | Antagonizing effect on hypotension and reflex tachycardia caused by trazodone [83] |
| Male sexual health problem | Phospholipids (PC in particular) improve erectile dysfunction and loss of libido [80] |
5. Conclusions
Post COVID-19 condition is a heterogeneous clinical condition in which ME/CFS and brain fog stand out among the different clinical symptoms and syndromes. The cerebral metabolic alterations and neuroendocrine disorders seem to constitute an important part of Post COVID-19 condition. Given the substantial lack of specific drugs and effective therapeutic strategies, hypothalamic phospholipid liposomes, which have been on the market for several years as adjuvant therapy of cerebral metabolic alterations resulting from neuroendocrine disorders, can be taken into consideration in an overall therapeutic strategy that aims to control the Post COVID-19 condition associated symptoms and syndromes. The pharmacological mechanisms and clinical effects of hypothalamic phospholipid liposomes strongly support their potential effectiveness in Post COVID-19 condition. Our initial clinical experience corroborates this rationale. Further clinical research is needed in order to obtain sufficient evidence on the role of hypothalamic phospholipid liposomes as an adjuvant treatment for some manifestations of Post COVID-19 condition.
Conflicts of Interest
The author declares no conflict of interest.
References
- Ministero della Salute. COVID-19—Situazione in Italia. Available online: https://www.salute.gov.it/portale/nuovocoronavirus/dettaglioContenutiNuovoCoronavirus.jsp?area=nuovoCoronavirus&id=5351&lingua=italiano&menu=vuoto (accessed on 24 July 2023).
- Nurek, M.; Rayner, C.; Freyer, A.; Taylor, S.; Järte, L.; MacDermott, N.; Delaney, B.C. Recommendations for the Recognition, Diagnosis, and Management of Long COVID: A Delphi Study. Br J Gen Pract 2021, 71, e815–e825. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Murthy, S.; Marshall, J.C.; Relan, P.; Diaz, J.V. A Clinical Case Definition of Post-COVID-19 Condition by a Delphi Consensus. The Lancet Infectious Diseases 2022, 22, e102–e107. [Google Scholar] [CrossRef]
- Montani, D.; Savale, L.; Noel, N.; Meyrignac, O.; Colle, R.; Gasnier, M.; Corruble, E.; Beurnier, A.; Jutant, E.-M.; Pham, T.; et al. Post-Acute COVID-19 Syndrome. Eur Respir Rev 2022, 31, 210185. [Google Scholar] [CrossRef] [PubMed]
- Yelin, D.; Moschopoulos, C.D.; Margalit, I.; Gkrania-Klotsas, E.; Landi, F.; Stahl, J.-P.; Yahav, D. ESCMID Rapid Guidelines for Assessment and Management of Long COVID. Clinical Microbiology and Infection 2022, 28, 955–972. [Google Scholar] [CrossRef]
- Department of Health and Human Services, Office of the Assistant Secretary for Health. 2022. National Research Action Plan on Long COVID, 200 Independence Ave SW, Washington, DC 20201.
- Centers for Disease Control and Prevention. Post-COVID Conditions: Information for Healthcare Providers. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/post-covid-conditions.html (accessed on 10 July 2023).
- Giuliano, M.; Tiple, D.; Agostoni, P.; Armocida, B.; Biardi, L.; Bonfigli, A.R.; Campana, A.; Ciardi, M.; Di Marco, F.; Floridia, M.; et al. Italian Good Practice Recommendations on Management of Persons with Long-COVID. Front. Public Health 2023, 11, 1122141. [Google Scholar] [CrossRef] [PubMed]
- Woodrow, M.; Carey, C.; Ziauddeen, N.; Thomas, R.; Akrami, A.; Lutje, V.; Greenwood, D.C.; Alwan, N.A. Systematic Review of the Prevalence of Long COVID. Open Forum Infectious Diseases 2023, 10, ofad233. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and Risk Factors for Long COVID in Non-Hospitalized Adults. Nat Med 2022, 28, 1706–1714. [Google Scholar] [CrossRef] [PubMed]
- Lam, I.C.H.; Wong, C.K.H.; Zhang, R.; Chui, C.S.L.; Lai, F.T.T.; Li, X.; Chan, E.W.Y.; Luo, H.; Zhang, Q.; Man, K.K.C.; et al. Long-Term Post-Acute Sequelae of COVID-19 Infection: A Retrospective, Multi-Database Cohort Study in Hong Kong and the UK. eClinicalMedicine 2023, 60, 102000. [Google Scholar] [CrossRef] [PubMed]
- Mizrahi, B.; Sudry, T.; Flaks-Manov, N.; Yehezkelli, Y.; Kalkstein, N.; Akiva, P.; Ekka-Zohar, A.; Ben David, S.S.; Lerner, U.; Bivas-Benita, M.; et al. Long COVID Outcomes at One Year after Mild SARS-CoV-2 Infection: Nationwide Cohort Study. BMJ 2023, e072529. [Google Scholar] [CrossRef] [PubMed]
- Ballouz, T.; Menges, D.; Anagnostopoulos, A.; Domenghino, A.; Aschmann, H.E.; Frei, A.; Fehr, J.S.; Puhan, M.A. Recovery and Symptom Trajectories up to Two Years after SARS-CoV-2 Infection: Population Based, Longitudinal Cohort Study. BMJ 2023, e074425. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. U.S. Census Bureau, Household Pulse Survey, 2022–2023. Long COVID. Generated interactively. Available online: https://www.cdc.gov/nchs/COVID19/pulse/long-COVID.htm.
- Walker, S.; Goodfellow, H.; Pookarnjanamorakot, P.; Murray, E.; Bindman, J.; Blandford, A.; Bradbury, K.; Cooper, B.; Hamilton, F.L.; Hurst, J.R.; et al. Impact of Fatigue as the Primary Determinant of Functional Limitations among Patients with Post-COVID-19 Syndrome: A Cross-Sectional Observational Study. BMJ Open 2023, 13, e069217. [Google Scholar] [CrossRef]
- Davis, H.E.; McCorkell, L.; Vogel, J.M.; Topol, E.J. Long COVID: Major Findings, Mechanisms and Recommendations. Nat Rev Microbiol 2023, 21, 133–146. [Google Scholar] [CrossRef]
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An Overview. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 2021, 15, 869–875. [Google Scholar] [CrossRef]
- Schiffl, H.; Lang, S.M. Long-Term Interplay between COVID-19 and Chronic Kidney Disease. Int Urol Nephrol 2023. [Google Scholar] [CrossRef] [PubMed]
- Bateman, L.; Bested, A.C.; Bonilla, H.F.; Chheda, B.V.; Chu, L.; Curtin, J.M.; Dempsey, T.T.; Dimmock, M.E.; Dowell, T.G.; Felsenstein, D.; et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management. Mayo Clinic Proceedings 2021, 96, 2861–2878. [Google Scholar] [CrossRef]
- Campos, M.C.; Nery, T.; Starke, A.C.; De Bem Alves, A.C.; Speck, A.E.; S Aguiar, A. Post-Viral Fatigue in COVID-19: A Review of Symptom Assessment Methods, Mental, Cognitive, and Physical Impairment. Neuroscience & Biobehavioral Reviews 2022, 142, 104902. [Google Scholar] [CrossRef]
- Sukocheva, O.A.; Maksoud, R.; Beeraka, N.M.; Madhunapantula, S.V.; Sinelnikov, M.; Nikolenko, V.N.; Neganova, M.E.; Klochkov, S.G.; Amjad Kamal, M.; Staines, D.R.; et al. Analysis of Post COVID-19 Condition and Its Overlap with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Journal of Advanced Research 2022, 40, 179–196. [Google Scholar] [CrossRef] [PubMed]
- Retornaz, F.; Rebaudet, S.; Stavris, C.; Jammes, Y. Long-Term Neuromuscular Consequences of SARS-Cov-2 and Their Similarities with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Results of the Retrospective CoLGEM Study. J Transl Med 2022, 20, 429. [Google Scholar] [CrossRef] [PubMed]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens De Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van Den Heede, K. Pathophysiology and Mechanism of Long COVID: A Comprehensive Review. Annals of Medicine 2022, 54, 1473–1487. [Google Scholar] [CrossRef]
- Quan, M.; Wang, X.; Gong, M.; Wang, Q.; Li, Y.; Jia, J. Post-COVID Cognitive Dysfunction: Current Status and Research Recommendations for High Risk Population. The Lancet Regional Health—Western Pacific 2023, 38, 100836. [Google Scholar] [CrossRef]
- Merad, M.; Blish, C.A.; Sallusto, F.; Iwasaki, A. The Immunology and Immunopathology of COVID-19. Science 2022, 375, 1122–1127. [Google Scholar] [CrossRef]
- Nicolai, L.; Kaiser, R.; Stark, K. Thromboinflammation in Long COVID—The Elusive Key to Postinfection Sequelae? Journal of Thrombosis and Haemostasis 2023, S1538783623004002. [Google Scholar] [CrossRef] [PubMed]
- Khodanovich, M.Y.; Kamaeva, D.A.; Naumova, A.V. Role of Demyelination in the Persistence of Neurological and Mental Impairments after COVID-19. Int. J. Mol. Sci. 2022, 23, 11291. [Google Scholar] [CrossRef]
- Kell, D.B.; Laubscher, G.J.; Pretorius, E. A Central Role for Amyloid Fibrin Microclots in Long COVID/PASC: Origins and Therapeutic Implications. Biochemical Journal 2022, 479, 537–559. [Google Scholar] [CrossRef] [PubMed]
- Davies, M. Long COVID Patients Travel Abroad for Expensive and Experimental “Blood Washing.”. BMJ 2022, o1671. [Google Scholar] [CrossRef] [PubMed]
- Auwaerter, P.G. The Race to Understand Post–COVID-19 Conditions. Ann Intern Med 2021, 174, 1458–1459. [Google Scholar] [CrossRef]
- Wang, C.; Yu, C.; Jing, H.; Wu, X.; Novakovic, V.A.; Xie, R.; Shi, J. Long COVID: The Nature of Thrombotic Sequelae Determines the Necessity of Early Anticoagulation. Front. Cell. Infect. Microbiol. 2022, 12, 861703. [Google Scholar] [CrossRef]
- Barrea, L.; Verde, L.; Grant, W.B.; Frias-Toral, E.; Sarno, G.; Vetrani, C.; Ceriani, F.; Garcia-Velasquez, E.; Contreras-Briceño, J.; Savastano, S.; et al. Vitamin D: A Role Also in Long COVID-19? Nutrients 2022, 14, 1625. [Google Scholar] [CrossRef]
- Corrao, S.; Mallaci Bocchio, R.; Lo Monaco, M.; Natoli, G.; Cavezzi, A.; Troiani, E.; Argano, C. Does Evidence Exist to Blunt Inflammatory Response by Nutraceutical Supplementation during COVID-19 Pandemic? An Overview of Systematic Reviews of Vitamin D, Vitamin C, Melatonin, and Zinc. Nutrients 2021, 13, 1261. [Google Scholar] [CrossRef]
- Wei, J.; Liu, X.; Xiao, W.; Lu, J.; Guan, L.; Fang, Z.; Chen, J.; Sun, B.; Cai, Z.; Sun, X.; et al. Phospholipid Remodeling and Its Derivatives Are Associated with COVID-19 Severity. Journal of Allergy and Clinical Immunology 2023, 151, 1259–1268. [Google Scholar] [CrossRef]
- Žarković, N.; Łuczaj, W.; Jarocka-Karpowicz, I.; Orehovec, B.; Baršić, B.; Tarle, M.; Kmet, M.; Lukšić, I.; Biernacki, M.; Skrzydlewska, E. Diversified Effects of COVID-19 as a Consequence of the Differential Metabolism of Phospholipids and Lipid Peroxidation Evaluated in the Plasma of Survivors and Deceased Patients upon Admission to the Hospital. IJMS 2022, 23, 11810. [Google Scholar] [CrossRef] [PubMed]
- Žarković, N.; Orehovec, B.; Baršić, B.; Tarle, M.; Kmet, M.; Lukšić, I.; Tatzber, F.; Wonisch, W.; Skrzydlewska, E.; Łuczaj, W. Lipidomics Revealed Plasma Phospholipid Profile Differences between Deceased and Recovered COVID-19 Patients. Biomolecules 2022, 12, 1488. [Google Scholar] [CrossRef] [PubMed]
- Kurano, M.; Okamoto, K.; Jubishi, D.; Hashimoto, H.; Sakai, E.; Saigusa, D.; Kano, K.; Aoki, J.; Harada, S.; Okugawa, S.; et al. Dynamic Modulations of Sphingolipids and Glycerophospholipids in COVID-19. Clinical & Translational Med 2022, 12. [Google Scholar] [CrossRef]
- Kaur, G.; Ji, X.; Rahman, I. SARS-CoV2 Infection Alters Tryptophan Catabolism and Phospholipid Metabolism. Metabolites 2021, 11, 659. [Google Scholar] [CrossRef] [PubMed]
- Clough, E.; Inigo, J.; Chandra, D.; Chaves, L.; Reynolds, J.L.; Aalinkeel, R.; Schwartz, S.A.; Khmaladze, A.; Mahajan, S.D. Mitochondrial Dynamics in SARS-COV2 Spike Protein Treated Human Microglia: Implications for Neuro-COVID. J Neuroimmune Pharmacol 2021, 16, 770–784. [Google Scholar] [CrossRef] [PubMed]
- Hornick, M.G.; Olson, M.E.; Jadhav, A.L. SARS-CoV-2 Psychiatric Sequelae: A Review of Neuroendocrine Mechanisms and Therapeutic Strategies. International Journal of Neuropsychopharmacology 2022, 25, 1–12. [Google Scholar] [CrossRef]
- Elkazzaz, M.; Ahmed, A.; Abo-Amer, Y.E.-E.; Hydara, T.; Haikal, A.; Razek, D.N.A.E.; Eltayb, W.A.; Wang, X.; Karpi’ nski, T.M.; Hamza, D.; et al. In Silico Discovery of GPCRs and GnRHRs as Novel Binding Receptors of SARS-CoV-2 Spike Protein Could Explain Neuroendocrine Disorders in COVID-19. Vaccines 2022, 10, 1500. [Google Scholar] [CrossRef]
- Hammad, R.; Elshafei, A.; Khidr, E.G.; El-Husseiny, A.A.; Gomaa, M.H.; Kotb, H.G.; Eltrawy, H.H.; Farhoud, H. Copeptin: A Neuroendocrine Biomarker of COVID-19 Severity. Biomarkers in Medicine 2022, 16, 589–597. [Google Scholar] [CrossRef]
- Raony, Í.; De Figueiredo, C.S.; Pandolfo, P.; Giestal-de-Araujo, E.; Oliveira-Silva Bomfim, P.; Savino, W. Psycho-Neuroendocrine-Immune Interactions in COVID-19: Potential Impacts on Mental Health. Front. Immunol. 2020, 11, 1170. [Google Scholar] [CrossRef]
- Jensterle, M.; Herman, R.; Janež, A.; Mahmeed, W.A.; Al-Rasadi, K.; Al-Alawi, K.; Banach, M.; Banerjee, Y.; Ceriello, A.; Cesur, M.; et al. The Relationship between COVID-19 and Hypothalamic–Pituitary–Adrenal Axis: A Large Spectrum from Glucocorticoid Insufficiency to Excess—The CAPISCO International Expert Panel. Int. J. Mol. Sci. 2022, 23, 7326. [Google Scholar] [CrossRef]
- Murga, I.; Aranburu, L.; Gargiulo, P.A.; Gómez Esteban, J.C.; Lafuente, J.-V. Clinical Heterogeneity in ME/CFS. A Way to Understand Long-COVID19 Fatigue. Front. Psychiatry 2021, 12, 735784. [Google Scholar] [CrossRef] [PubMed]
- Noor, N.; Urits, I.; Degueure, A.; Rando, L.; Kata, V.; Cornett, E.M.; Kaye, A.D.; Imani, F.; Narimani-Zamanabadi, M.; Varrassi, G.; et al. A Comprehensive Update of the Current Understanding of Chronic Fatigue Syndrome. Anesth Pain Med 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Biggio, G.; Mostallino, M.C.; Giusti, P.; Zusso, M.; Toffano, G. Overview of the Pharmacological Properties and Therapeutic Efficacy of Phospholipid Liposomes (Liposom Forte®) in Patients with Depressive Disorders. Minerva Psychiatry 2018, 59. [Google Scholar] [CrossRef]
- Biggio, G.; Mostallino, M.C.; Biggio, F.; Minervino, A.; Giannetti, F. Therapeutic Efficacy and Tolerability of Phospholipid Liposomes (Liposom Forte®) for the Management of Depressive Disorders in Elderly Patients. Evidence-Based Psychiatric Care 2020, 6, 76–91. [Google Scholar] [CrossRef]
- Nataf, S. An Alteration of the Dopamine Synthetic Pathway Is Possibly Involved in the Pathophysiology of COVID-19. J Med Virol 2020, 92, 1743–1744. [Google Scholar] [CrossRef]
- Antonini, A.; Leta, V.; Teo, J.; Chaudhuri, K.R. Outcome of Parkinson’s Disease Patients Affected by COVID -19. Mov Disord 2020, 35, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Pawlak, R.; Napiorkowska-Pawlak, D.; Takada, Y.; Urano, T.; Nagai, N.; Ihara, H.; Takada, A. The Differential Effect of Angiotensin II and Angiotensin 1-7 on Norepinephrine, Epinephrine, and Dopamine Concentrations in Rat Hypothalamus: The Involvement of Angiotensin Receptors. Brain Research Bulletin 2001, 54, 689–694. [Google Scholar] [CrossRef]
- Klempin, F.; Mosienko, V.; Matthes, S.; Villela, D.C.; Todiras, M.; Penninger, J.M.; Bader, M.; Santos, R.A.S.; Alenina, N. Depletion of Angiotensin-Converting Enzyme 2 Reduces Brain Serotonin and Impairs the Running-Induced Neurogenic Response. Cell. Mol. Life Sci. 2018, 75, 3625–3634. [Google Scholar] [CrossRef]
- Bauer, L.; Laksono, B.M.; De Vrij, F.M.S.; Kushner, S.A.; Harschnitz, O.; Van Riel, D. The Neuroinvasiveness, Neurotropism, and Neurovirulence of SARS-CoV-2. Trends in Neurosciences 2022, 45, 358–368. [Google Scholar] [CrossRef]
- Lu, Y.; Zhu, Q.; Fox, D.M.; Gao, C.; Stanley, S.A.; Luo, K. SARS-CoV-2 down-Regulates ACE2 through Lysosomal Degradation. MBoC 2022, 33, ar147. [Google Scholar] [CrossRef]
- Attademo, L.; Bernardini, F. Are Dopamine and Serotonin Involved in COVID-19 Pathophysiology? The European Journal of Psychiatry 2021, 35, 62–63. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, L.M.S.; Rabelo, P.C.R.; Moraes, M.M.; Teixeira-Coelho, F.; Coimbra, C.C.; Wanner, S.P.; Soares, D.D. Physical Exercise-Induced Fatigue: The Role of Serotonergic and Dopaminergic Systems. Braz J Med Biol Res 2017, 50, e6432. [Google Scholar] [CrossRef]
- Tornero-Aguilera, J.F.; Jimenez-Morcillo, J.; Rubio-Zarapuz, A.; Clemente-Suárez, V.J. Central and Peripheral Fatigue in Physical Exercise Explained: A Narrative Review. IJERPH 2022, 19, 3909. [Google Scholar] [CrossRef]
- Nizzo, M.C.; Tegos, S.; Gallaminia, A.; Toffano, G.; Polleri, A.; Massarottib, M. Brain Cortex Phospholipids Liposomes Effects on CSF HVA, 5-HIAA and on Prolactin and Somatotropin Secretion in Man. J. Neural Transmission 1978, 43, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Toffano, G.; Bruni, A. Pharmacological Properties of Phospholipid Liposomes. Pharmacological Research Communications 1980, 12, 829–845. [Google Scholar] [CrossRef]
- Canonico, P.L.; Annunziato, L.; Toffano, G.; Bernardini, R.; Stanzani, S.; Foti, M.; Clementi, G.; Drago, F.; Scapagnini, U. In Vivo and in Vitro Interference of Phosphatidylserine Liposomes on Prolactin Secretion in the Rat. Neuroendocrinology 1981, 33, 358–362. [Google Scholar] [CrossRef] [PubMed]
- Inukai, S.; Hara, S.; Ichinose, H. Tyrosine Hydroxylase Activity Is Regulated through the Modification of the 176th Cysteine Residue. Biochemical and Biophysical Research Communications 2022, 589, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Soung, A.L.; Vanderheiden, A.; Nordvig, A.S.; Sissoko, C.A.; Canoll, P.; Mariani, M.B.; Jiang, X.; Bricker, T.; Rosoklija, G.B.; Arango, V.; et al. COVID-19 Induces CNS Cytokine Expression and Loss of Hippocampal Neurogenesis. Brain 2022, 145, 4193–4201. [Google Scholar] [CrossRef]
- Leng, A.; Shah, M.; Ahmad, S.A.; Premraj, L.; Wildi, K.; Li Bassi, G.; Pardo, C.A.; Choi, A.; Cho, S.-M. Pathogenesis Underlying Neurological Manifestations of Long COVID Syndrome and Potential Therapeutics. Cells 2023, 12, 816. [Google Scholar] [CrossRef]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.-H.; Wood, J.; O’Dea, M.R.; Dutton, S.; Shamardani, K.; Nwangwu, K.; et al. Mild Respiratory COVID Can Cause Multi-Lineage Neural Cell and Myelin Dysregulation. Cell 2022, 185, 2452–2468. [Google Scholar] [CrossRef]
- Barnes-Vélez, J.A.; Aksoy Yasar, F.B.; Hu, J. Myelin Lipid Metabolism and Its Role in Myelination and Myelin Maintenance. The Innovation 2023, 4, 100360. [Google Scholar] [CrossRef]
- Fledrich, R.; Abdelaal, T.; Rasch, L.; Bansal, V.; Schütza, V.; Brügger, B.; Lüchtenborg, C.; Prukop, T.; Stenzel, J.; Rahman, R.U.; et al. Targeting Myelin Lipid Metabolism as a Potential Therapeutic Strategy in a Model of CMT1A Neuropathy. Nat Commun 2018, 9, 3025. [Google Scholar] [CrossRef] [PubMed]
- Monastra, G.; Cross, A.H.; Bruni, A.; Raine, C.S. Phosphatidylserine, a Putative Inhibitor of Tumor Necrosis Factor, Prevents Autoimmune Demyelination. Neurology 1993, 43 Pt 1, 153–153. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Galougahi, M.; Yousefi-Koma, A.; Bakhshayeshkaram, M.; Raad, N.; Haseli, S. 18FDG PET/CT Scan Reveals Hypoactive Orbitofrontal Cortex in Anosmia of COVID-19. Academic Radiology 2020, 27, 1042–1043. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Morbelli, S.; Ciccarelli, M.; Cecconi, M.; Aghemo, A.; Morelli, P.; Chiola, S.; Gelardi, F.; Chiti, A. Long COVID Hallmarks on [18F]FDG-PET/CT: A Case-Control Study. Eur J Nucl Med Mol Imaging 2021, 48, 3187–3197. [Google Scholar] [CrossRef]
- Guedj, E.; Campion, J.Y.; Dudouet, P.; Kaphan, E.; Bregeon, F.; Tissot-Dupont, H.; Guis, S.; Barthelemy, F.; Habert, P.; Ceccaldi, M.; et al. 18F-FDG Brain PET Hypometabolism in Patients with Long COVID. Eur J Nucl Med Mol Imaging 2021, 48, 2823–2833. [Google Scholar] [CrossRef] [PubMed]
- Donegani, M.I.; Miceli, A.; Pardini, M.; Bauckneht, M.; Chiola, S.; Pennone, M.; Marini, C.; Massa, F.; Raffa, S.; Ferrarazzo, G.; Arnaldi, D.; Sambuceti, G.; Nobili, F.; Morbelli, S. Brain Metabolic Correlates of Persistent Olfactory Dysfunction after SARS-Cov2 Infection. Biomedicines 2021, 9, 287. [Google Scholar] [CrossRef]
- Rudroff, T.; Workman, C.D.; Ponto, L.L.B. 18F-FDG-PET Imaging for Post-COVID-19 Brain and Skeletal Muscle Alterations. Viruses 2021, 13, 2283. [Google Scholar] [CrossRef]
- Ferrucci, R.; Cuffaro, L.; Capozza, A.; Rosci, C.; Maiorana, N.; Groppo, E.; Reitano, M.R.; Poletti, B.; Ticozzi, N.; Tagliabue, L.; Silani, V.; Priori, A. Brain Positron Emission Tomography (PET) and Cognitive Abnormalities One Year after COVID-19. J Neurol 2023, 270, 1823–1834. [Google Scholar] [CrossRef]
- Salonia, A.; Pontillo, M.; Capogrosso, P.; Pozzi, E.; Ferrara, A.M.; Cotelessa, A.; Belladelli, F.; Corsini, C.; Gregori, S.; Rowe, I.; Carenzi, C.; Ramirez, G.A.; Tresoldi, C.; Locatelli, M.; Cavalli, G.; Dagna, L.; Castagna, A.; Zangrillo, A.; Tresoldi, M.; Landoni, G.; Rovere-Querini, P.; Ciceri, F.; Montorsi, F. Testosterone in Males with COVID-19: A 12-month Cohort Study. Andrology 2023, 11, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Uckert, S.; Fuhlenriede, M.H.; Becker, A.J.; Stief, C.G.; Scheller, F.; Knapp, W.H.; Jonas, U. Is There an Inhibitory Role of Cortisol in the Mechanism of Male Sexual Arousal and Penile Erection? Urological Research 2003, 31, 402–406. [Google Scholar] [CrossRef]
- Salvio, G.; Martino, M.; Giancola, G.; Arnaldi, G.; Balercia, G. Hypothalamic–Pituitary Diseases and Erectile Dysfunction. JCM 2021, 10, 2551. [Google Scholar] [CrossRef] [PubMed]
- Adeyemi, D.H.; Odetayo, A.F.; Hamed, M.A.; Akhigbe, R.E. Impact of COVID 19 on Erectile Function. The Aging Male 2022, 25, 202–216. [Google Scholar] [CrossRef] [PubMed]
- Leema Rose, A.; Manickam, A.; Agrawal, M. A Mathematical Model For The Special Effects Of Phosphatidylserine On Endocrine Reaction To Reasonable Concentration Exercise In Healthy Male Subjects. TURCOMAT 2021, 12, 3555–3559. [Google Scholar] [CrossRef]
- Starks, M.A.; Starks, S.L.; Kingsley, M.; Purpura, M.; Jäger, R. The Effects of Phosphatidylserine on Endocrine Response to Moderate Intensity Exercise. Journal of the International Society of Sports Nutrition 2008, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Kiriakova, N.; Kiriakov, A.; Schneider, E.; Bonev, A. Therapeutic Effect of Essential Phospholipids on Functional Sexual Disorders in Males. J Eur Acad Dermatol Venerol 1998, 11, 191–193. [Google Scholar] [CrossRef] [PubMed]
- Casacchia, M.; Marola, W.; Meco, G.; Pirro, R.; Di Cesare, E.; Allegro, A.; Cusimano, G. Phospholipid Liposomes in Depression: A Double-Blind Study versus Placebo. Int Pharmacopsychiatry 1982, 17, 274–279. [Google Scholar] [CrossRef]
- Aguglia, E.; Calandra, C.; Rapisarda, V.; Maugeri, D. The Effect of Hypothalamic Phospholipid Liposomes in Patients Treated with Sulpiride or Haloperidol. Acta Ther 1984, 10, 133–144. [Google Scholar]
- Giannelli, A.; Rabboni, M.; Zarattini, F.; Malgeri, C.; Magnolfi, G. A Combination of Hypothalamic Phospholipid Liposomes with Trazodone for Treatment of Depression.: An Open Controlled Study. Acta Psychiatr Scand 1989, 79, 52–58. [Google Scholar] [CrossRef]
- Rachev, E.; Nalbansky, B.; Kolarov, G.; Agrosì, M. Efficacy and Safety of Phospholipid Liposomes in the Treatment of Neuropsychological Disorders Associated with the Menopause: A Double-Blind, Randomised, Placebo-Controlled Study. Curr Med Res Opin 2001, 17, 105–110. [Google Scholar] [CrossRef]
- Bruni, A.; Toffano, G.; Leon, A.; Boarato, E. Pharmacological Effects of Phosphatidylserine Liposomes. Nature 1976, 260, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.Y.; Cui, F.; Kim, H.K.; Nawaz, H.; Kang, S.; Kim, H.; Jang, J.; Go, G. Effect of Phosphatidylserine on Cognitive Function in the Elderly: A Systematic Review and Meta-Analysis. Korean Journal of Food Science and Technology 2022, 54, 52–58. [Google Scholar] [CrossRef]
- US Food and Drug Administration. Letter Updating the Phosphatidylserine and Cognitive Function and Dementia Qualified Health Claim. 2004. Available online: http://wayback.archive-it.org/7993/20171114183737/https://www.fda.gov/Food/IngredientsPackagingLabeling/LabelingNutrition/ucm072999.htm (accessed on 6 June 2023).
- Zhang, Y.Y.; Yang, L.Q.; Guo, L.M. Effect of Phosphatidylserine on Memory in Patients and Rats with Alzheimer’s Disease. Genet. Mol. Res. 2015, 14, 9325–9333. [Google Scholar] [CrossRef] [PubMed]
- Castro-Marrero, J.; Sáez-Francàs, N.; Santillo, D.; Alegre, J. Treatment and Management of Chronic Fatigue Syndrome/Myalgic Encephalomyelitis: All Roads Lead to Rome: Therapy and Management in CFS/ME. British Journal of Pharmacology 2017, 174, 345–369. [Google Scholar] [CrossRef] [PubMed]
- Licata, G. [Hypothalamic phospholipid liposomes. A drug for the treatment of anxiety-depressive syndromes in internal medicine]. Recenti Prog Med 1984, 75, 1076–1080. [Google Scholar] [PubMed]
- Wolff Sagy, Y.; Feldhamer, I.; Brammli-Greenberg, S.; Lavie, G. Estimating the Economic Burden of Long-COVID: The Additive Cost of Healthcare Utilisation among COVID-19 Recoverees in Israel. BMJ Glob Health 2023, 8, e012588. [Google Scholar] [CrossRef]
Figure 1.
Putative pathophysiological mechanisms involved in Post COVID-19 condition [23].
Figure 1.
Putative pathophysiological mechanisms involved in Post COVID-19 condition [23].
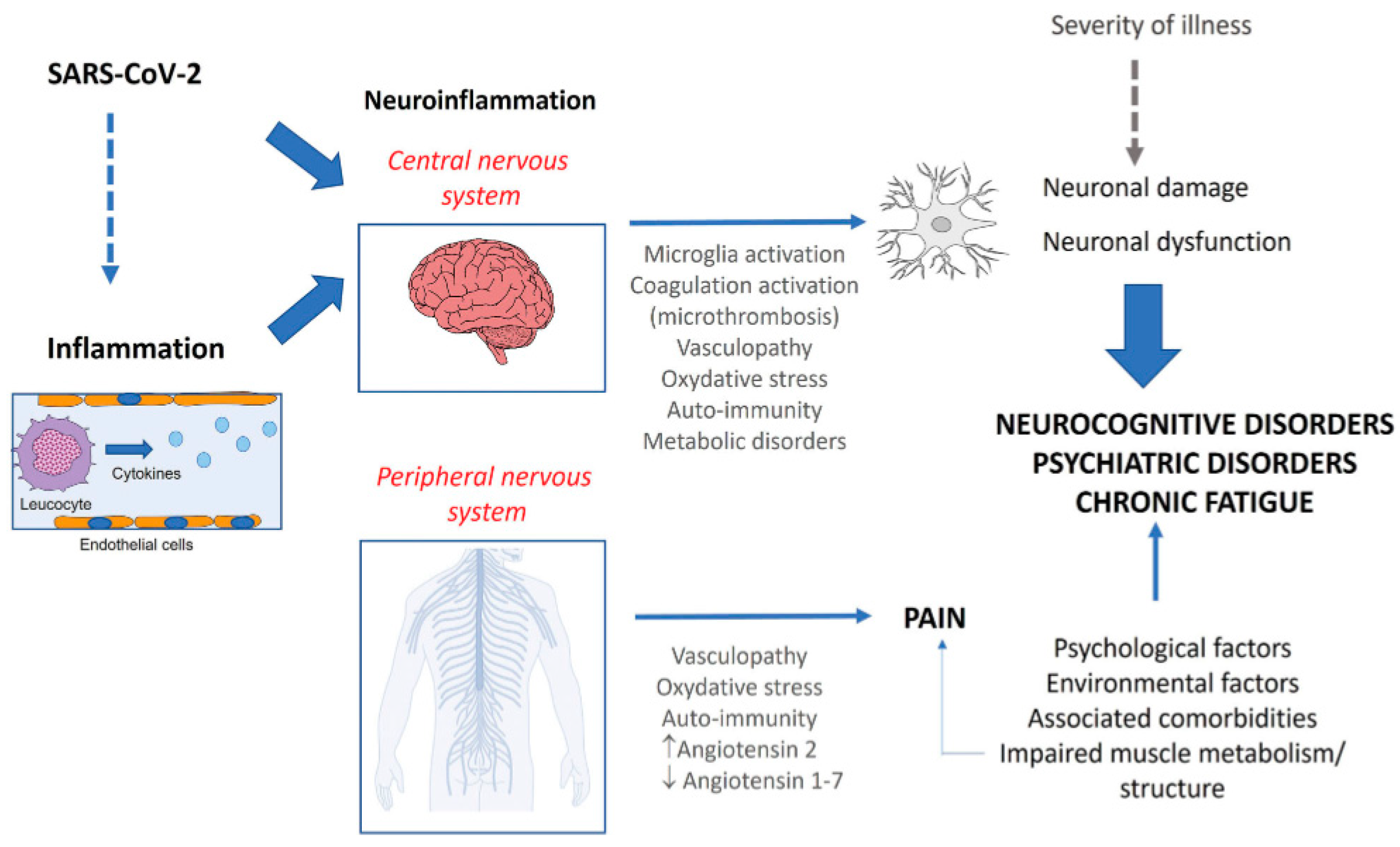
Figure 2.
A schematic representation of the relationships between COVID-19, demyelination and neuropsychiatric sequalae [27].
Figure 2.
A schematic representation of the relationships between COVID-19, demyelination and neuropsychiatric sequalae [27].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



