
Submitted:
29 June 2023
Posted:
07 July 2023
You are already at the latest version
Abstract
: In Philadelphia chromosome positive B-cell (Ph+) acute lymphoblastic leukemia (LLA), growing evidence has accumulated about the efficacy of low-intensity and chemo-free regimens. Our objective was to analyse all recent trials evaluating these treatments and to compare them in terms of efficacy. We applied the Shiny method, an artificial intelligence technique, to analyse Kaplan-Meier curves and reconstruct patient-level data. Reconstructed patient data were then evaluated through standard survival statistics and subjected to indirect head-to-head treatment comparisons. The endpoint was progression-free survival (PFS). Based on 562 reconstructed patients, 8 trials were analyzed. The survival data from these trials were pooled into three types of treatment: i) treatments based on tyrosine kinase inhibitors (TKIs) combined with reduced-intensity chemotherapy (denoted as TKICHE); ii) TKIs associated to steroids with no chemotherapy (TKISTE); iii) chemotherapy-free combinations of blinatumomab plus TKIs (TKIBLI). According to the Shiny method, the three PFS curves were reported in a single Kaplan-Meier graph and subjected to survival statistics. In terms of PFS, TKIBLI ranked first, TKICHE second, and TKISTE third; the differences between these three regimens were statistically significant. In conclusion, the multi-treatment Kaplan-Meier graph generated in this study has effectively summarized the current evidence on these treatments in comparative terms.
Keywords:
acute lymphoblastic leukemia
; imatinib
; ponatinib
; dasatinib
; nilotinib
; blinatumomab
; reduced-intensity chemotherapy
; chemotherapy-free
; progression-free
1. Introduction
The Philadelphia (Ph) chromosome represents the most frequent cytogenetic abnormality in adults with acute lymphoblastic leukaemia (ALL), with an incidence that increases with age, reaching approximately 50% in patients aged 60 years and older [1,2,3]. The combination of Ph chromosome and BCR-ABL fusion gene is associated with the most unfavourable outcome, irrespective of age [4].
Induction chemotherapy rarely determines a sustained complete remission in these patients and so, after complete hematologic remission has been achieved, allogeneic stem cell transplant represents, when feasible, the only possibility of cure.[5]. Treatment options for Ph+ ALL have expanded over the past 15 years, mainly due to the advent of tyrosine kinase inhibitors (TKIs) that have significantly improved outcomes in various combination regimens [6,7,8].
The first-generation TKI (imatinib), the second-generation TKIs (dasatinib and nilotinib), and the third-generation TKI (ponatinib) have successfully been combined with chemotherapy in prospective studies conducted in adult patients with Ph+ ALL [9,10,11]. More recently, a further improvement has been achieved with a chemo-free induction/consolidation strategy based on the combination of a TKI with the CD3/CD19 bispecific antibody blinatumomab [12,13]. All in all, these novel regimens have determined very substantial improvements in the progression-free survival (PFS) of these patients.
In the field of survival analysis, important methodological improvements have occurred in the past two years. In particular, the IPDfromKM method [14] (also known as the “Shiny method”) has established itself as a powerful tool to reconstruct individual patient data from the graphs of Kaplan-Meier survival curves. The main characteristic of the Shiny method is that each Kaplan-Meier curve is analysed through an artificial intelligence software that reconstructs patient-level data over the study follow-up. In this way, treatments can be compared indirectly with one another and the results can be interpreted by application of standard survival statistics. Despite its theoretical complexity, the Shiny method is extremely easy-to-use. In fact, only three pieces of information are needed to generate a patient database from a Kaplan-Meier curve: i) the graph of the curve; ii) the total number of patients for the curve concerned; iii) the total number of events. A wide experience has rapidly accumulated on the use of this approach, particularly in the area of anti-cancer agents [15] In this report, we applied the Shiny method to analyse the most recent survival studies focused on the treatment of Ph+ ALL with TKIs combined with low-intensity regimens, steroids and chemo-free approaches.
2. Materials and Methods
Study design
Our analysis had the purpose to retrieve updated information on novel therapeutic approaches for ALL and to study in comparative terms the survival outcomes determined by these treatments. After a standard PubMed search, the datasets suitable for our analysis were identified. Our analysis included the datasets in which the information on PFS was reported (with follow-up of at least 2 years) and the graph of the Kaplan-Meier curve was available. As proposed in a recent review by Hadad et al [9], these datasets were grouped as follows: i) treatments based on TKIs combined with reduced-intensity chemotherapy (denoted as TKICHE); ii) TKIs associated to steroids with no chemotherapy (denoted as TKISTE); iii) chemotherapy-free combinations of blinatumomab plus TKIs (denoted as TKIBLI). The trials evaluating these three types of treatment were subjected to the procedure of individual-patient data reconstruction according to the Shiny method. Thereafter, the treatments identified as TKICHE, TKISTE, and TKIBLI were compared with one another using standard survival statistics. Our endpoint was PFS. The results of our analysis were summarized in a multi-trial Kaplan-Meier graph generated by application of the Shiny method.
Literature search
Our PubMed search covered the time interval from January 2015 to March 2023 (date of the last search: 15 March 2023; keyword, ”acute lymphoblastic leukaemia”; filters: “clinical trials” and “years from 2015 to 2023”). Original clinical trials and reviews extracted from PubMed were eligible for further scrutiny. Also abstracts were eligible if adequately indexed. Then, a further selection of this material identified some recent trials conducted in patients with ALL. When duplicate citations were found for the same trial, only the most updated dataset was included in our analysis.
Reconstruction of individual patient data from Kaplan-Meier survival curves
We used the Shiny method,14 which was implemented as in the other analyses published by our research group.15 Firstly, patient-level data were reconstructed from each of the treatment arms of the original trials. Thereafter, in cases where similar or identical treatments had been investigated in different trials, the reconstructed patients were pooled into a single patient group. In this way, three treatment groups were formed for TKICHE, TKISTE, and TKIBLI. Finally, these three treatment groups were subjected to a standard survival statistics, in which PFS was the endpoint.
Survival statistics
Survival statistics was carried out by standard methods using the Cox model; head-to-head comparisons were assessed according to the hazard ratio (HR) with 95% confidence interval (CI). Statistical analyses based on reconstructed patient-level data were conducted under the R-platform as in our previous analyses.15
Assessment of heterogeneity in studies pooled together
In three separate analyses, we examined the degree of heterogeneity within the trials assigned to the TKICHE, TKISTE, and TKIBLI groups, respectively. Heterogeneity was likely to depend on differences in patients’ inclusion criteria. Furthermore, in each of these three groups heterogeneity was assessed through a post-hoc analysis aimed at estimating the degree of concordance between similar studies expected to report similar survival patterns. For this purpose, the likelihood ratio test and the concordance test were employed. Further details about this assessment of heterogeneity are presented in the Appendix.
3. Results
Our PubMed search firstly identified 10 studies. The study by Ottman et al [16] was excluded owing to the absence of the KM curve; the study by Chalandon et al [17] was excluded because only induction was not intensive. Hence, a total of 8 studies (Table 1) were selected for our analysis [18,19,20,21,22,23,24,25]. The following agents were investigated in these 8 trials:
- trial [a]: dasatinib in combination with low-intensity chemotherapy (Rousselot et al [18]);
- trial[b]: nilotinib combined with low-intensity chemotherapy (Rousselot et al [19]);
- trial[c]: dasatinib plus steroids induction followed by dasatinib alone (Chiaretti et al [20]);
- trial[d]: imatinib combined with steroids (Vignetti et al [21]);
- trial[e]: dasatinib induction therapy combined with steroids (Foà et al [22]);
- trial[f]: ponatinib plus prednisone (Martinelli et al [23]);
- trial[g]: dasatinib plus blinatumomab (Chiaretti et al [24]);
- trial[h]: ponatinib plus blinatumomab (Jabbour et al [25]).
According to our study protocol, firstly individual patient data from these 8 trials were reconstructed by application of the Shiny method. Then, the treatments from different trials belonging to the same pharmacological class were pooled into a single patient group. The following three groups were formed:
- The regimen denoted as TKICHE (i.e. TKI plus low-intensity chemotherapy), which includes three trials, namely dasatinib plus low-intensity chemotherapy in the trial by Rousselot et al [18], nilotinib plus low-intensity chemotherapy in the GRAAPH-2014 Study by Rousselot et al [19], dasatinib plus steroids induction in the trial by Chiaretti et al [20].
The assignment to TKICHE of the trial Chiaretti et al [20] can be a matter of controversy because the regimen of this trial was chemo-free rather than based on low-intensity. Consistently with the review by Hadad et al [9] we kept this trial by Chiaretti in the TKICHE group.
In our main analysis, these three regimens (TKICHE, TKISTE, and TKIBLI) were compared with one another based on the endpoint of PFS. Figure 1 shows the Kaplan-Meier survival curves generated for these three regimens from reconstructed patients. In the statistical comparisons across these three regimens, the following values of HR were estimated:
- HR for the comparison of TKIBLI vs TKICHE = 0.042 (95%CI, 0.010 to 0.170);
- HR for the comparison of TKIBLI vs TKISTE = 0.022 (95%CI, 0.005 to 0.091);
- HR for the comparison of TKICHE vs TKISTE = 0.506 (95%CI, 0.370 to 0.692).
All these three values of HR are statistically significant. Medians for these three regimens were 33.7 months for TKICHE (95%CI, 25.5 to not computable), 14.7 months for TKISTE (95%CI, 11.5 to 21.7), and not computable for TKIBLI. According to these results, the advantage in PFS for TKIBLI compared with the other two regimens has a remarkable clinical relevance, along with its high level of statistical significance.
Finally, besides our main analysis, we separately assessed the degree of heterogeneity for the three regimes (TKICHE, TKISTE, and TKIBLI). For this purpose, we carried out three post-hoc analyses in which the likelihood ratio test was estimated. These post-hoc analyses are presented in detail in the Appendix.
4. Discussion
Elderly or unfit patients are not candidates for intensive chemotherapy owing to the high risk of morbidity and mortality. Hence, lower-intensity regimens have mainly been designed for these patients [18] even though they have also been explored in younger, more fit patients with newly diagnosed Ph+ ALL [20]. Similarly, the regimens based on induction therapy with steroids plus TKIs have mainly been tested in elderly or unfit patients, e.g. in three trials conducted by the GIMEMA group, namely GIMEMA LAL0201-B [21], GIMEMA LAL1205 [22] and GIMEMA LAL 1811 [23]. Findings from these studies suggest that low-intensity therapies are safe and feasible in patients with Ph+, particularly those who are older and/or unfit for intensive chemotherapy or allogeneic stem cell transplantation (allo-SCT).
It should be kept in mind that blinatumomab has been shown to be highly effective as a single agent in patients with relapsed/refractory Ph+ ALL [26]. A further improvement has been achieved with a chemo-free induction/consolidation strategy that includes the sequential administration of dasatinib followed by blinatumomab according to the D-ALBA GIMEMA LAL2116 trial [13]. In the updated analysis of the D-ALBA trial and the GIMEMA LAL2217 trial, Chiaretti et al [24] reported very favorable outcomes, with an estimated OS of 78% (95% CI: 66-92%) at 48 months and disease-free survival (DFS) of 75% (95% CI: 64-87%).
Furthermore, the results recently presented at the 2022 European Hematology Association (EHA) Congress by Short et al prove that a chemotherapy-free regimen of simultaneous ponatinib and blinatumomab is safe and effective, for newly diagnosed (ND) Ph+ ALL; the 2-year event-free survival (EFS) and OS were both 93% while in the relapsed/refractory Ph+ ALL cohort, the 2-year EFS rate was 42% and the 2-year OS rate was 61%.25 In contrast with the D-ALBA trial, blinatumomab plus ponatinib were started concomitantly beginning in cycle 1. Early results from these studies are encouraging even though the number of enrolled patients remains small.
Our analysis has some limitations. The first limitation is given by the presence of some differences in the eligibility criteria among the trials that we pooled into the same group. For example, regarding the TKICHE group of trials, patients older than age 55 years were eligible in the study by Rousselot et al [18], while patients aged 18 to 59 years with newly diagnosed Ph1 and/or BCRABL1–positive ALL were included in the GRAAPH-2005 study [17]. Furthermore, regarding the TKIBLI group, patients had a median age of 54 years in the D-ALBA trial [24], while in the study by Short et al [25] patients had a median age of 51 and required to have a performance status of ≤2 without comorbidities. These characteristics of patients included in the TKIBLI trials may have influenced the favorable outcome of this therapeutic approach compared with TKICHE and TKISTE. Finally, some caution is warranted in interpreting the results of the TKIBLI trials because the number of enrolled patients is quite limited.
Another aspect that deserves specific comments is safety. Chemotherapy-free regimens with blinatumomab combined with second or third generation TKIs permit to avoid cytotoxic therapies, thus contributing to improve prognosis. While most imatinib adverse events tend to be mild and often resolve spontaneously, rare but serious side effects have occasionally been reported with later generation TKIs [23,27]. Since most patients who do not undergo allo-SCT are recommended to receive indefinite TKI therapy, significant open questions remain concerning long-term outcomes in ALL patients besides mortality. Further prospective studies are needed to identify patients who can safely discontinue TKIs, an option that gains increasing interest with time.
5. Conclusions
In conclusion, major progress has been achieved in the management of Ph+ ALL. After the combination of TKIs with low intensive chemotherapy or steroids has considerably improved long-term survival, chemotherapy-free regimens with blinatumomab and TKIs seem to represent a further advancement that may revolutionize the landscape of Ph+ ALL. In particular, the combination of second generation dasatinib or third generation ponatinib plus blinatumomab is associated with deep and durable remissions while avoiding cytotoxic therapies and mitigating the need for allo-SCT. Our results based on indirect comparisons suggest that this strategy might be the most effective. In this context, the Shiny method has confirmed its value in improving the analysis and the interpretation of survival results in hematologic malignancies [28,29,30,31].
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Text S1.; Figure S1. Post-hoc analysis for the TKICHE regimen; Figure S2. Post-hoc analysis for the TKISTE regimen; Figure S3. Post-hoc analysis for the TKIBLI regimen.
Author Contributions
Author AM was responsible for study conception, design and acquisition of data; author MR was responsible for data analysis and drafting; authors AM, DM and MC were responsible for data quality assurance. All authors revised the manuscript and approved the final version of the manuscript to be published.
Funding
This research received no external funding.
Data Availability Statement
For each of the 9 treatments under comparison, the database of reconstructed patients is available from the author upon request.
Data Sharing Statement
For each treatment under comparison, the database of reconstructed patients is available from the author upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chiaretti S: Vitale, A.; Cazzaniga, G.; et al. Clinico-biological features of 5202 patients with acute lymphoblastic leukemia enrolled in the Italian AIEOP and GIMEMA protocols and stratified in age cohorts. Haematologica. 2013, 98, 1702–1710. [Google Scholar] [CrossRef] [PubMed]
- Ravandi, F.; Kebriaei, P. Philadelphia chromosome-positive acute lymphoblastic leukemia. Hematol Oncol Clin North Am. 2009, 23, 1043–1063. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, T.; Schwartz, S.; Bartram, C.R.; et al. Patients’ age and BCR–ABL frequency in adult B- precursor ALL: a retrospective analysis from the GMALL study group. Blood. 2008, 112, 918–919. [Google Scholar] [CrossRef] [PubMed]
- Moorman, A.V.; Harrison, C.J.; Buck, G.A.; et al. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/ Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood. 2007, 109, 3189–3197. [Google Scholar] [CrossRef]
- Dombret, H.; Gabert, J.; Boiron, J.M.; et al. Outcome of treatment in adults Philadelphia chromosome-positive acute lymphoblastic leukemia-results of the prospective multi-center LALA-94 trial. Blood. 2002, 100, 2357–2366. [Google Scholar] [CrossRef]
- Ottmann, O.G.; Wassmann, B.; Pfeifer, H.; et al. Imatinib compared with chemotherapy as front-line treatment of elderly patients with Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ALL). Cancer. 2007, 109, 2068–2076. [Google Scholar] [CrossRef]
- Talpaz, M.; Shah, N.P.; Kantarjian, H.; et al. Dasatinib in imatinib-resistant Philadelphia chromosome-positive leukemias. N Engl J Med. 2006, 354, 2531–2541. [Google Scholar] [CrossRef]
- Bassan, R.; Rossi, G.; Pogliani, E.M.; et al. Chemotherapy-phased imatinib pulses improve long- term outcome of adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia: Northern Italy Leukemia Group protocol 09/00. J Clin Oncol. 2010, 28, 3644–3652. [Google Scholar] [CrossRef]
- Haddad, F.G.; Sawyers, J.; Short, N.J. Treatment de-escalation in Philadelphia chromosome-positive B-cell acute lymphoblastic leukemia: the emerging role of chemotherapy-free regimens. Ther Adv Hematol. 2023, 14, 20406207231151294. [Google Scholar] [CrossRef]
- Chiaretti, S.; Vitale, A.; Vignetti, M.; et al. A sequential approach with imatinib, chemotherapy and transplant for adult Ph1 acute lymphoblastic leukemia: final results of the GIMEMA LAL 0904 study. Haematologica. 2016, 101, 1544–1552. [Google Scholar] [CrossRef]
- Jabbour, E.; Haddad, F.G.; Short, N.J.; Kantarjian, H. Treatment of Adults With Philadelphia Chromosome-Positive Acute Lymphoblastic Leukemia-From Intensive Chemotherapy Combinations to Chemotherapy-Free Regimens: A Review. JAMA Oncol. 2022, 8, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Assi, R.; Kantarjian, H.; Short, N.J.; et al. Safety and Efficacy of Blinatumomab in Combination With a Tyrosine Kinase Inhibitor for the Treatment of Relapsed Philadelphia Chromosome-positive Leukemia. Clin Lymphoma Myeloma Leuk. 2017, 17, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Foà, R.; Bassan, R.; Vitale, A.; et al. Dasatinib-Blinatumomab for Ph+ Acute Lymphoblastic Leukemia in Adults. N Engl J Med. 2020, 383, 1613–1623. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhou, Y.; Lee, J.J. IPDfromKM: reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2021, 21, 11. [Google Scholar] [CrossRef] [PubMed]
- Ossato, A.; Mengato, D.; Chiumente, M.; Messori, A.; Damuzzo, V. Progression-Free and Overall Survival of First-Line Treatments for Advanced Renal Cell Carcinoma: Indirect Comparison of Six Combination Regimens. Cancers (Basel). 2023, 15, 2029. [Google Scholar] [CrossRef] [PubMed]
- Ottmann, O.G.; Pfeifer, H.; Cayuela, J.M.; et al. Nilotinib (Tasigna®) and Low Intensity Chemotherapy for First-Line Treatment of Elderly Patients with BCR-ABL1-Positive Acute Lymphoblastic Leukemia: Final Results of a Prospective Multicenter Trial (EWALL-PH02). Blood 2018, 132 (Suppl. 1), 31. [Google Scholar] [CrossRef]
- Chalandon, Y.; Thomas, X.; Hayette, S.; et al. Randomized study of reduced-intensity chemotherapy combined with imatinib in adults with Ph+ acute lymphoblastic leukemia. Blood 2015, 125, 3711–3719, [published correction appears in Blood. 2015, 126, 1261]. [Google Scholar] [CrossRef]
- Rousselot, P.; Coudé, M.M.; Gokbuget, N.; et al. Dasatinib and low-intensity chemotherapy in elderly patients with Philadelphia chromosome-positive ALL. Blood 2016, 128, 774–782. [Google Scholar] [CrossRef]
- Rousselot, P.; Chalandon, Y.; Chevret, S.; Cayuela, J.M.; Huguet, F.; Chevallier, P.; et al. The Omission of High-Dose Cytarabine during Consolidation Therapy of Ph+ ALL Patients Treated with Nilotinib and Low-Intensity Chemotherapy Results in an Increased Risk of Relapses Despite Non-Inferior Levels of Late BCR-ABL1 MRD Response. First Results of the Randomized Graaph-2014 Study. Blood 2021, 138 (Suppl. 1), 512. [Google Scholar]
- Chiaretti, S.; Ansuinelli, M.; Vitale, A.; et al. A multicenter total therapy strategy for de novo adult Philadelphia chromosome positive acute lymphoblastic leukemia patients: final results of the GIMEMA LAL1509 protocol. Haematologica. 2021, 106, 1828–1838. [Google Scholar] [CrossRef]
- Vignetti, M.; Fazi, P.; Cimino, G.; et al. Imatinib plus steroids induces complete remissions and prolonged survival in elderly Philadelphia chromosome-positive patients with acute lymphoblastic leukemia without additional chemotherapy: results of the Gruppo Italiano Malattie Ematologiche dell'Adulto (GIMEMA) LAL0201-B protocol. Blood. 2007, 109, 3676–3678. [Google Scholar] [PubMed]
- Foà, R.; Vitale, A.; Vignetti, M.; et al. Dasatinib as first-line treatment for adult patients with Philadelphia chromosome-positive acute lymphoblastic leukemia. Blood. 2011, 118, 6521–6528. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, G.; Papayannidis, C.; Piciocchi, A.; et al. INCB84344-201: Ponatinib and steroids in frontline therapy for unfit patients with Ph+ acute lymphoblastic leukemia. Blood Adv. 2022, 6, 1742–1753. [Google Scholar] [CrossRef] [PubMed]
- Chiaretti, S.; Bassan, R.; Vitale, A.; et al. Forty Months Update Of The Gimema Lal2116 (D-alba) Protocol And Ancillary Lal2217 Study For Newly Diagnosed Adult Ph+ All [abstract]. EHA Library. 2022 Abstract: P353.
- Jabbour, E.; Short, N.J.; Jain, N.; Huang, X.; Montalban-Bravo, G.; Banerjee, P.; et al. Ponatinib and blinatumomab for Philadelphia chromosome-positive acute lymphoblastic leukaemia: a US, single-centre, single-arm, phase 2 trial. Lancet Haematol. 2023, 10, e24–e34. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, G.; Boissel, N.; Chevallier, P.; et al. Complete Hematologic and Molecular Response in Adult Patients With Relapsed/Refractory Philadelphia Chromosome-Positive B-Precursor Acute Lymphoblastic Leukemia Following Treatment With Blinatumomab: Results From a Phase II, Single-Arm, Multicenter Study [published correction appears in J Clin Oncol. 2017, 35, 2722] J Clin Oncol. 2017, 35, 1795–1802. [published correction appears in J Clin Oncol. 2017, 35, 2856]. 35.
- Steegmann, J.L.; Baccarani, M.; Breccia, M.; et al. European LeukemiaNet recommendations for the management and avoidance of adverse events of treatment in chronic myeloid leukaemia. Leukemia. 2016, 30, 1648–1671. [Google Scholar] [CrossRef]
- Messori, A.; Rivano, M.; Mengato, D.; Cancanelli, L.; Di Spazio, L.; Chiumente, M. A preliminary estimate of survival gain and cost-effectiveness of CAR-T in adult patients with acute lymphoblastic leukaemia. Leukemia & Lymphoma 2021 Dec 31:1-4. https://www.tandfonline.com/eprint/TWPDKPRVUQV6YKXDHKDX/full?target=10.1080/10428194.2021. 2022. [Google Scholar]
- Messori, A.; Chiumente, M.; Mengato, D. CAR T-cells in large B-cell lymphoma: analysis of overall survival based on reconstructed patient-level data. Clin Ther 2022 Dec 8:S0149-2918(22)00377-0.
- Messori, A.; Damuzzo, V.; Leonardi, L.; Agnoletto, L.; Chiumente, M.; Mengato, D. CAR-T Treatment: Determining the Survival Gain in Patients With Relapsed or Refractory Diffuse Large B-cell Lymphoma. Clin Lymphoma Myeloma Leuk. 2020, 20, 490–491. [Google Scholar] [CrossRef]
- Messori, A. Long-term progression-free survival in patients with chronic lymphocytic leukaemia treated with novel agents: an analysis based on indirect comparisons. Eur J Haematol. 2023, 110, 60–66. [Google Scholar] [CrossRef]
Figure 1.
Kaplan-Meier survival curves generated from reconstructed patients s for three combination regimens. Treatments from different trials belonging to the same pharmacological class were pooled into a single patient group (TKICHE or TKISTE or TKIBLI). In red, TKI plus chemotherapy (TKICHE); in green, TKI plus steroids (TKISTE); in blue, TKI plus blinatumomab (TKIBLI).
Figure 1.
Kaplan-Meier survival curves generated from reconstructed patients s for three combination regimens. Treatments from different trials belonging to the same pharmacological class were pooled into a single patient group (TKICHE or TKISTE or TKIBLI). In red, TKI plus chemotherapy (TKICHE); in green, TKI plus steroids (TKISTE); in blue, TKI plus blinatumomab (TKIBLI).
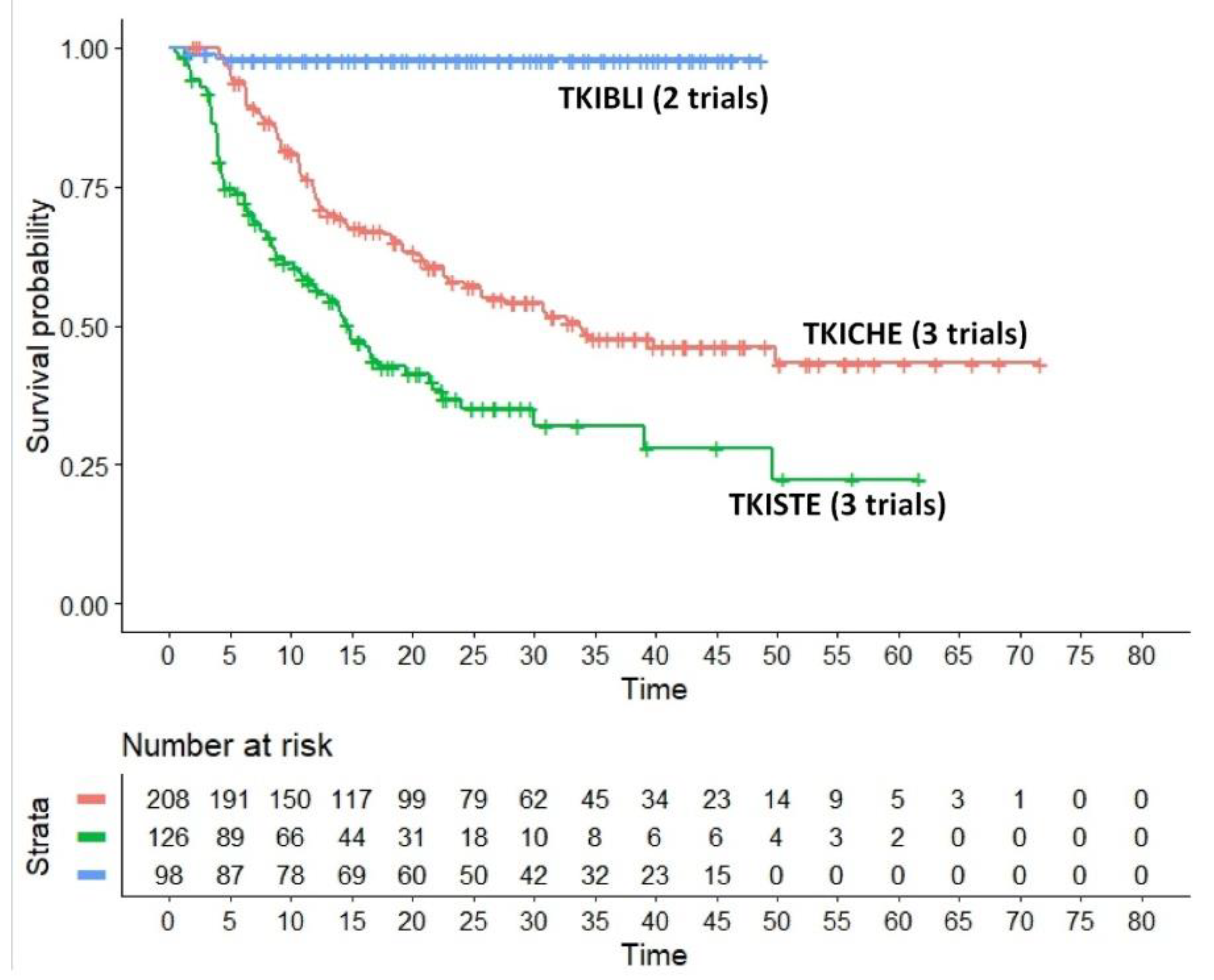

Table 1.
Main characteristics of the included trials.
| First Author |
Year | Trial | Treatment | Inclusion criteria | Events | N° of patients | Notes | |
|---|---|---|---|---|---|---|---|---|
| TKICHE | Chaladon et al [17] | 2015 | GRAAPH-2005 study | Imatinib combined with low-intensity chemotherapy | Patients aged 18 to 59 years with newly diagnosed Ph1 and/or BCRABL1–positive ALL were eligible | 65 | 135 | Excluded from our analysis because only induction was not intensive |
| Rousselot et al [18] | 2016 | EWALL-PH-01 international study |
Dasatinib in combination with low-intensity chemotherapy | Patients aged 55 years or older were eligible if they had newly diagnosed Ph1 and/or BCR-ABL ALL | 40 | 71 | Included | |
| Rousselot et al [19] | 2021 | Graaph-2014 Study | Nilotinib combined with low-intensity chemotherapy | Ph-Positive ALL patients aged 18-60 years old were randomized | 23 | 79 | Included | |
| Chiaretti et al [20] | 2020 | GIMEMA LAL1509 | Dasatinib plus steroids induction followed by dasatinib alone | Adult Ph+ ALL patients (18-60 years). | 13 | 58 | Included | |
| TKISTE | Vignetti et al [21] | 2007 | GIMEMA LAL0201-B | Imatinib combined with steroids | Patients with a diagnosis of ALL who were older than 60 years were eligible if they carried either the Ph chromosome or the BCR-ABL molecular translocation |
16 | 29 | Included |
| Foà et al [22] | 2011 | GIMEMA LAL1205 | Dasatinib induction therapy combined with steroids | Patients 18 years of age or older (with no upper age limit) were eligible if they had been diagnosed with Ph/BCR-ABLALL | 23 | 53 | Included | |
| Martinelli et al [23] | 2022 | GIMEMA LAL 1811 | Ponatinib plus prednisone | Patients had new-onset Ph+ ALL, and were ≥ 60 years or were ≥ 18 years but unfit for a program of intensive chemotherapy and SCT | 34 | 44 | Included | |
| TKIBLI | Chiaretti et al [24] | 2022 | GIMEMA LAL2117 | Dasatinib + blinatumomab |
Ph-Positive ALL Patients, median trial age of participants was 54 years ( 24-82; no upper age limit) |
9 | 58 | Included |
| Jabbour et al [25] | 2023 | NCT03263572 | Ponatinib + blinatumomab |
Patients with newly diagnosed, relapsed/refractory Ph+ ALL or CML in lymphoid blast phase |
2 | 40 | Included |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



