
Submitted:
04 July 2023
Posted:
06 July 2023
You are already at the latest version
Abstract
Attention deficit hyperactivity disorder (ADHD) results in various functioning impairments in children’s lives and families. Parents of children with ADHD report high levels of parenting stress, low levels of parental self-efficacy and use of more authoritarian and/or permissive parenting practices than parents of typically developing children. Intervention programs need to address both children’s and parents’ needs and multimodal intervention programs could cover this demand. The aim of this study was to examine the efficacy of “Child ViReal Support Program” - a multi-level evidence-based comprehensive program - on parenting stress, parental self-efficacy, parenting practices, and the core symptoms of children’s ADHD. Families with a child diagnosed with ADHD (n = 16) were randomly allocated to two groups (PC and CP; P = parent training, C = child training) and a cross-over design was utilized. Participating parents completed, in four different times during the study, the Parenting Stress Index-Short Form, the Parenting Sense of Competence Scale, the Parenting Styles and Dimensions Questionnaire-Short Version and the parent form of the ADHD Rating Scale-IV. Parents from both groups, after their participation in the parent training, demonstrated reduced parenting stress, enhanced parental self-efficacy and increased the employ of democratic parenting practices. More than that, they reported decreased levels of inattention and impulsivity/hyperactivity for their children. Evidence-based multi-level intervention programs could produce positive effects in parents and children by incorporating effective methods and tools in accordance with the needs and the demands of the family context.
Keywords:
attention deficits
; ADHD
; multi-level interventions
; RCT
; psychoeducation
; parent training
; parenting stress
; parental self-efficacy
; parenting styles
1. Introduction
Attention, a multifaceted cognitive ability, plays a decisive role in various domains of human functioning, including cognitive development, social interactions, and academic endeavors [1,2]. For optimum performance in these domains, it is essential to develop and enhance attention skills, including selecting relevant information, task-focused concentration, and inhibiting impulsive responses [3]. However, a large proportion of school-aged children experience attention deficits that are often associated with neurodevelopmental disorders such as Attention Deficit Hyperactivity Disorder (ADHD) and can significantly impact their daily lives and overall functioning [4,5]. Hence, children with attention deficits experience impairments in neuropsychological functioning (e.g., executive functions) [3,6,7] and emotional dysregulation (e.g., difficulty in the recognition and regulation of emotions, lack of empathy, emotional negativity, etc.) [8,9], academic difficulties (e.g., poor academic performance, etc.) [10,11], adversities in their social/peer relationships (e.g., difficulties in forming and maintaining relationships, etc.) [12,13] and degraded quality of family life [14,15].
The challenges associated with ADHD and attention deficits extend beyond the affected child, causing severe dysfunctions to the entire family system. Parents of children with ADHD often experience increased parenting stress and reduced parental self-efficacy, which could negatively affect their well-being and the parent-child relationship [16,17]. Parenting stress, defined as “the aversive psychological reaction to the demands of being a parent” [18], is determined by child and parent characteristics and the surrounding relationship dynamics [19,20]. Parental self-efficacy, an individual’s confidence about their ability to successfully raise children, contributes significantly in perceiving and resolving parenting challenges [21,22].
Quantitative and qualitative research consistently reveals that parents of children with ADHD experience higher levels of related stress compared to parents of typically developing children [16,17,23,24] and/or parents raising children with other neurodevelopmental disorders [16]. Parenting stress often arises when parents perceive that the demands of their role exceed their resources for dealing with them [25]. Elevated parenting stress has been linked to various negative outcomes including worsening of ADHD symptoms in children, reduced response to intervention, strained parent-child relationships, and decreased parental well-being [26,27,28]. Moreover, parents of children with ADHD often face adversities concerning family functioning and quality of life [14,15]. Thus, dysfunctional family dynamics coexisting with undermined daily life routines have been observed among parents and siblings of children with ADHD [14,15].
As far as parenting style is concerned, inadequate activity monitoring, an increase in punitive parenting techniques, and a decrease in supportive parenting practices are potentially signs of the negative impact of parenting stress on children with ADHD. Findings suggest a link between elevated parenting stress and more authoritarian and permissive parenting practices, as well as difficulties with behavior regulation in children [23], while lower levels of parental self-efficacy are linked to coercive parent-child interactions [29]. These unfavorable rearing practices have strongly correlated to exaggerated behavioral problems in children with ADHD [30] and poorer child executive functioning [23].
Considering the aforementioned challenges, several variables are highlighted in literature to mediate and/or moderate the impact of ADHD on parenting stress. Family impact, parental ADHD symptoms, the severity of a child’s symptoms, co-occurring emotional and behavioral difficulties, as well as contextual factors such as poor marriage quality and a lack of social support, have been included in relevant research [27,31,32,33].
Given the substantial impact of ADHD on children and family dynamics, the necessity to provide effective support and multifaceted interventions on the family system level seems to be impending. Pharmacotherapy, psychosocial interventions (such as behavior parent training, child training based on cognitive-behavioral therapy), and a combination of both are the most commonly implemented treatments for children with ADHD [34,35,36,37]. Pharmacological interventions have shown powerful short-term effects in reducing the core symptoms of ADHD [34,38], but these effects tend to diminish upon discontinuation [39,40,41]. Also, children need to get trained in skills that will help them with social and emotional functioning, while parents need to also get trained to be able to support their children and enhance their mental health.
In particular, psychoeducation of parents raising ADHD children constitutes a systematic and didactic approach providing substantial information on the disorder and its treatment, such as a detailed description of ADHD and its symptoms, informative knowledge about the epidemiology and etiology of ADHD, education on the available interventions and other data [42,43,44,45]. On psychoeducation-based interventions, parents are regularly trained in behavioral strategies along with their children, so as to gradually build a common understanding of the disorder, evolve their skills, and be actively engaged in the comprehensive management of ADHD [44,45,46,47]. Especially, for mothers who seem to be more vulnerable related to caregiving of children with ADHD and are at risk for depression and elevated stress [48] is essential to participate in parent training programs. Hence, as far as psychosocial interventions are considered, they seem to lead to changes in inattention, and behavioral difficulties often observed by children with ADHD [49,50,51], while they have positive effects on parents and family functioning [35,52]. Research indicates that parents report significant improvements in parenting stress and parental self-efficacy after participating in programs [46,53,54]. Likewise, their increased parenting sense of competence and decreased parenting stress after parent training have been associated with behavioral improvements in their children [54,55]. Also, parents’ participation leads to improvements in their parenting practices [52], their parent-child relationship, and the impact of child behavior on the family system [46,51,52].
Taking into consideration the aforementioned results and benefits of psychosocial interventions for children with ADHD and their parents, the “Child ViReal Support Program” - a comprehensive multi-level intervention program for children with attention deficits and their parents combining parent training and child training, while utilizing the potentials of immersive virtual reality (iVR) technology for attention training as part of the child training - was designed. In the present study and manuscript, we mainly focus on the parent training component of the intervention program, and we assessed the impact of the intervention “Child ViReal Support Program” specifically on parenting stress, parental self-efficacy and parenting practices, as well as on the core symptoms of children’s ADHD (inattention, hyperactivity/impulsivity). The study addressed the following hypotheses: (1) After completing the intervention program (Time 3), parents would report decreased levels of parenting stress compared to their initial assessment (Time 1), (2) After completing the intervention program (Time 3), parents would report increased levels of parental self-efficacy compared to their initial assessment (Time 1), (3) Parents would report decreased inattention and hyperactivity/impulsivity symptoms for their children at the end of the intervention program (Time 3) compared to their initial reports (Time 1), (4) After completing the intervention program (Time 3) parents would use more democratic parenting practices and less authoritarian and/or permissive parenting practices, (4) Parents participating in the PC group, who completed the parent training before the child training would report lower levels of parenting stress and higher levels of parental self-efficacy compared to parents who were randomized in the CP group (child training before parent training) at Time 2 assessment, (5) Parents would report lower levels of parenting stress and higher levels of parental self-efficacy at the follow-up assessment, four months after the end of the intervention program (Time 4), compared to their initial assessment (Time 1), (6) At the follow-up assessment (Time 4), children’s inattention and hyperactivity/impulsivity symptoms would be significantly reduced compared to the initial assessment (Time 1), and (7) Parents would use more democratic and less authoritarian and/or permissive parenting practices at the follow-up assessment (Time 4) compared to their initial assessment (Time 1).
2. Materials and Methods
2.1. Trial Design
A randomized controlled trial (RCT) study with a cross-over design was performed. Families were randomly assigned to either the PC group or the CP group (P=Parent training, C=Child training). Thus, families assigned to the PC group started with the parent training and continued with the child training, whereas families assigned to the CP group started with the child training and continued with the parent training. The study was registered in the Clinical Trials Registry (NCT05391698) [56].
2.2. Eligibility Criteria for Participants
Families were included in the study if (a) the child had Full-Scale IQ equal to or above 80 measured by the Wechsler Intelligence Scale for Children-Fifth Edition (WISC-V) [57,58], (b) the parents and the child could understand and speak fluently the Greek language, (c) the child had not been diagnosed with a comorbid disorder or other concurrent difficulties that may interfere with task performance during the assessments or the intervention program (e.g., autism spectrum disorder, pervasive developmental disorder, visual or hearing impairment, psychotic disorder), (d) the child or the parents had not previously participated in an intervention program based on the behavioral or cognitive-behavioral approach, and (e) the child was not under any medication treatment for ADHD.
2.3. Participant Recruitment
For recruiting families in the study, the research team contacted the experts and staff of the Interdisciplinary Evaluation, Counselling and Support Centers (KE.D.A.S.Y.) of Heraklion and Rethymnon in Crete, Greece. The objectives of the study were explained to the staff of the centers, who then proceeded to inform the parents of children diagnosed with ADD/ADHD about the study. Families interested in participating could contact the research team via phone call or by filling out a participation form on the program’s website (https://sites.google.com/view/childvireal/home). Those families that fulfilled the screening inclusion criteria for the study (b, c, d, e) were contacted by a research team member to schedule an appointment for the first assessment. Prior to participating in the study, both parents and children of the selected families provided separate written informed consent. During this 2-hour appointment, parents a) provided the researchers a copy of their child’s clinical assessment report supporting a primary clinical diagnosis of their child’s disorder, and b) they completed questionnaires about sociodemographic variables, child’s characteristics, diseases and comorbid problems, and family and/or other contextual factors. Regarding children, the WISC-V was performed to assess Full-Scale IQ [57,58]. Families that satisfied all the inclusion criteria for the study were contacted by the research team to participate in the “Child ViReal Support Program”.
The study was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines [59].
2.4. Ethics
The approval of the study was preceded by the Research Ethics Committee of the University of Crete (REC-UOC) (Approval Reference no. 51/25.02.2020). All participants had access to the information sheet and an online website for the study, which they were able to work through at their own pace. Furthermore, consent was obtained again after the first appointment as already mentioned.
2.5. Intervention Procedure
The comprehensive multi-level intervention program called the “Child ViReal Support Program” was designed by the research team and consists of a parent psychoeducational training program and a child training program. The main researcher developed both manuals of the training programs, noting in detail all the exercises and informative material that would be provided to participants. Both training programs were delivered by two licensed Educational/School Psychologists, who were recruited and trained in the use of the manuals. Systematic supervision sessions were delivered on a weekly basis by the designers of the intervention program, namely a licensed Educational/School Psychologist, and an Assistant Professor in Educational Psychology.
2.5.1. Parent Psychoeducational Training Program
Parents attended an in-person manualized psychoeducational training program focused on ADHD. The program was based on well-evidence-based interventions developed by Barkley [44], and Kazdin [45], incorporating neuropsychological findings about the cognitive functions of children with attention deficits [60,61] and neurocognitive training [62,63]. The parent training was delivered in eight weekly group sessions (1.5-2 hours), each focusing on a different thematic unit through lectures, group discussions, modeling, and role-playing. The first session provided an overview of ADHD diagnosis, including underlying neurobiology, associated executive function deficits, and behavioral difficulties faced by children with ADHD at home and school context. Subsequent sessions addressed parenting stress management techniques, behavior modification principles, effective communication techniques, and the design and implementation of a contingency management system. The fifth and sixth sessions focused on various executive functions (e.g., working memory, cognitive flexibility, emotional control, etc.) as well as strategies that parents could utilize to help their children concentrate, organize, remember, and learn more effectively. The seventh session was focused on social skills and emotional regulation and provided parents with techniques to support their children respectively. The eighth session was a wrap-up of the program, summarizing the main points of all previous meetings. Also, parents had to complete weekly homework assignments to facilitate the implementation of the newly learned skills at home. An overview of the sessions and thematic units covered in each session is presented in Appendix A.
Each of the two licensed Educational/School Psychologists delivered the parent training program in two groups: For the parents allocated in the PC group and the parents of the CP group. To maintain treatment fidelity, the psychologists covered the parent training program by conducting sessions following the manual. They were thoroughly trained, reviewed the topics to be covered before each session, and checked the coverage after the session by completing an Integrity Checklist of the meeting. Any topic omitted from a session (e.g., due to lack of time) was presented in the following one.
2.5.2. Child Training Program
The child training program, comprised of 16 individualized in-person sessions (1 hour per session), utilizes the potential of immersive virtual reality (iVR) technology for the training of focused and sustained attention and incorporates practices based on the cognitive-behavioral approach to foster behavioral and emotional self-regulation skills in children. During the program, children gained knowledge about the interconnection of emotions, thoughts, and behaviors. They received training in techniques aimed at transforming negative automatic thoughts into positive ones, as well as strategies for effective identification and expression of emotions and management of challenging emotions (e.g., anger, stress). In addition, the program included comprehensive training in a range of social skills, encompassing conversational initiation and maintenance, displaying polite interactions, and conflict resolution. Problem-solving techniques emphasizing skills such as goal setting, time management, and the breakdown of goals into manageable steps were introduced. Lastly, the program emphasized the development of self-observation, self-guidance, and self-reinforcement techniques to equip children with the necessary tools for pursuing their goals effectively.
2.5.3. Randomization
Sixteen families of children aged 9–12 years old (mean = 10.48, std = .94, 2 girls) with a diagnosis of ADHD disorder participated in the study. Participants resided in Heraklion and Rethymnon districts in Crete, Greece. As mentioned above, a randomized controlled trial (RCT) study with a cross-over design was performed. Therefore, using a web-based random number generator, families were allocated either to the PC group (n = 9) or to the CP group (n = 7). Two families dropped out of the intervention program for personal reasons. One family was assigned to the PC group, and the mother participated and finished the parent training program, but they dropped out after the Time 2 assessment. The second family was assigned to the CP group and dropped out during the child training (before the Time 2 assessment). A third family was not able to participate in the follow-up assessment, four months after the end of the intervention program (Time 4). The recruitment and randomization of families are illustrated in Figure 1.
2.6. Measures and procedure
2.6.1. Primary Measures
The measures of the RCT study are described below.
ADHD Rating Scale-IV (ADHD-IV RS) [64]. The ADHD-IV RS, which includes questionnaires for parents and teachers, is a tool for the early and accurate diagnosis of ADHD. For the purposes of the current study, the parent-report scale in its Greek adaptation [65] was used. This scale consists of 18 items addressing the different symptoms of ADHD as defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM IV-TR) [66], and parents are asked to rate the frequency with which their child has demonstrated these symptoms at home over the previous six months (e.g., [Over the past 6 months] “Fails to give close attention to details or makes careless mistakes in schoolwork.”, “Has difficulty playing or engaging in leisure activities quietly.”). Three ratings/indicators are elicited by this scale: (1) the Inattention Score, (2) the Impulsivity/Hyperactivity Score, and (3) the Total Score.
Parenting Stress Index-Short Form (PSI-SF) [67,68]. The PSI-SF is a widely used and well-documented self-report tool for measuring parenting stress of parents of children 12 years and younger. Families identify the sources and different types of stress that comes with parenting such as children's and parents’ characteristics, or different factors that are believed to affect their overall relationship. Thus, the PSI-SF provides an observation of parental stress levels as well as inadequate child rearing methods and a child’s adaptability in the family environment. Parents report their level of agreement with 36 items (e.g., “I feel trapped by my responsibilities as a parent.”, “I feel that my child is very moody and easily upset.”) using a 5-point Likert scale (1=Strongly disagree, 5=Strongly agree), that score three subscales: Parental Distress, Parent-Child Dysfunctional Interaction, and Difficult Child in addition to a Defensive Responding Scale, for an objective interpretation of parents’ responses, and a Total Score. The internal consistency reliability (a =.91) and the test-retest reliability (a =.84) with a 6-month interval are satisfied. The PSI-SF questionnaire was translated and adapted into the Greek language by Leze [69].
Parenting Sense of Competence Scale (PSOC) [70,71]. The PSOC is a self-report scale for parents of children from birth to 17 years old. It consists of 17 statements that are assessed on a 6-point Likert-type scale (1=Strongly disagree, 6=Strongly agree) and they relate to the parents’ sense and perceptions of their parenting ability and competence (e.g., “I honestly believe I have all the skills necessary to be a good parent (father/mother) to my child.”), as well as their satisfaction with their parental role (e.g., “Considering how long I’ve been a parent (father/mother), I feel thoroughly familiar with this role.”). The PSOC extracts an Overall Parenting Competence Perception Score. The scale was translated into the Greek language with the method of back-translation [72,73,74] by two independent bilingual psychologists, whose outcomes were identical to the original version.
Parenting Styles and Dimensions Questionnaire-Short Version (PSDQ-Short Version) [75]. The PSDQ is a self-report questionnaire consisting of 32 statements that are assessed on a 5-point Likert scale (1=Never, 5=Always). The PSDQ is based on Baumrind’s parental typology model [76] and assesses the typology of parents based on the parent-child relationship and communication, as well as on the practices applied by parents in the upbringing of their children. The questionnaire was adapted and standardized for the Greek population for fathers [77] and mothers [78] separately. The factor analysis applied to each questionnaire concluded in 29 statements (instead of 32), as three of them did not load on any factor and were removed. Four different factors (instead of three) emerged, which correspond to four dimensions of paternal and maternal parenting styles, respectively. These dimensions concern the democratic paternal and maternal styles (13 items, a = .88 and a = .88, respectively) (e.g., “I allow my child to give input into family rules.”), the authoritarian paternal and maternal styles (7 items, a = .84 and a = .83, respectively) (e.g., “I explode in anger towards my child.”), the permissive paternal and maternal styles (5 items, a =.63 and a = .65, respectively) (e.g., “I state punishments to my child and do not actually do them.”), and the strict paternal and maternal styles (4 items, a = .70 and a =.68, respectively) (e.g., “I scold or criticize when my child’s behavior doesn’t meet my expectations.”). The strict parenting style combines elements and features of the democratic and authoritarian types but constitutes a separate parenting style.
2.6.2. Procedure
The participants underwent an initial baseline assessment (Time 1, T1), followed by random assignment to either the PC or CP groups. Subsequently, after completing the first phase of the intervention program (8 weeks), which entailed parent training for the PC group and child training for the CP group, the participants participated in a second assessment completing the same measures (Time 2, T2). Then, they proceeded to the second phase of the intervention program, that involved child training and parent training, respectively. Upon the finalization of the intervention program (8 weeks), the participants were assessed again (Time 3, T3) with the same tools. Finally, a follow-up assessment was conducted four months after the intervention program’s conclusion (Time 4, T4), during which participants filled out the measures one last time. Summarizing, the time between baseline (T1) and Time 2 assessment was approximately 9 weeks, and between Time 2 and Time 3 was also approximately 9 weeks. The Time 4 assessment took place four months after the Time 3 phase was completed.
2.6.3. Feasibility and Acceptability Measures
The research team, considering the important questions for the evaluation of an evidence-based intervention program, designed two questionnaires for the evaluation of the parent training program. The questionnaires have been created based on well-known questionnaires that have proven to be reliable and valid for assessing the social validity and satisfaction of an intervention program, such as the Therapy Attitude Inventory (TAI) [79,80], the Treatment Evaluation Inventory (TEI) [81], and the Program Evaluation Questionnaires for the Incredible Years intervention program [82].
Evaluation of Parent Training-Weekly (EPT-W). The EPT-W questionnaire was completed by each parent at the end of each session of the parent psychoeducational training program. The questionnaire included five items, four of which utilized a 4-point Likert-type response format and one of which was an open-ended question aiming at eliciting parents’ personal aspects regarding each session. The four rated items inquired about the perceived usefulness of the session’s content, the acquisition of new knowledge, parent’s confidence in implementing the newly learned skills, and the effectiveness of the trainer.
Evaluation of Parent Training - Final (EPT-F). After the parent psychoeducational training program, each participating parent completed the EPT-F questionnaire. The questionnaire is composed of 33 items, with 31 of them utilizing a 5-point Likert scale response format (1=Strongly disagree, 5=Strongly agree) and two of them in the format of open-ended questions. The items assess the feasibility (e.g., “The knowledge gained, and skills developed through the program are useful for my relationship with my child”), satisfaction (e.g., “Overall, I feel satisfied with the program and its results”), and practicality of the program (e.g., “Practicing the exercises and newly acquired skills with my child at home proved to be useful”). The four sections of the EPT-F questionnaire are as follows: 1) Overall Program (9 items) that yields a Total Satisfaction Score, 2) Structure/Training (14 items) that provides a Program’s Usefulness Score, 3) Trainer’s Assessment (8 items) that produces a Trainer’s Assessment Score; and 4) Your Opinion (2 open-ended questions) in which parents could provide personal feedback regarding any aspects or features of the program they would like to alter, as well as their perceived main benefit from participating in the parent training program.
2.7. Statistical Analysis
Statistical analysis of our dataset initially focuses on descriptive statistics, computing the means, standard deviations, and correlations for each time point and group (PC and CP) separately; Friedman's two-way analysis of variance is used for assessing the equality of means across time. The multivariate nature of such problems and the existence of longitudinal data (repeated measures on parents across the four time points) make the use of classical approaches, such as the ordinary multiple linear regression model, inappropriate due to the potentially correlated errors between measures of the same subject. Therefore, to deal with these issues, among others, we turn our attention to marginal models, one of the available procedures for such kind of data [83], focusing on the average effect of the independent variables on our dependent variables. The data analysis was carried out using SPSS 28.0 [84] and r-project [85].
3. Results
3.1. Demographics
All children were diagnosed with ADHD disorder by child psychiatrists at the Interdisciplinary Evaluation, Counselling and Support Centers (KE.D.A.S.Y.) and the Community Children and Adolescents’ Mental Health Centers of Heraklion and Rethymnon in Crete, Greece. The ages of the participating children ranged from 9 to 12 years old (mean = 10.48, std = .94), and the ages of the parents (14 fathers and 16 mothers) ranged from 32 to 52 years old (mean = 42, std = 5.11). Most participating parents had completed secondary education (n = 18, 60%), whereas some of them had a higher education degree (Bachelor = 9, and Master/Ph.D. = 2, 36.7%). Also, most parents were in partnered relationships (married or living with an adult partner, n = 28, 93.3%) and were employed in full-time jobs (n = 23, 76.7%). The majority of parents were living in urban areas (n = 19, 63.3%), whereas some resided in semi-urban areas (n = 5, 16.7%) and rural areas (n = 6, 20%). Most of the parents actively participating in the intervention program were female (only one out of 15 was male), and their mean age was 40.1 years old (the mean age for those not participating was 43.9).
3.2. Main Analysis
The descriptive statistics of the measures across the four time points of assessment (Time 1-4) and for each group separately (PC and CP) can be found in Table 1. Hence, referring to Parenting styles for the PC group, we can see that Authoritarian and Permissive styles keep decreasing, whereas the Strict style seems to be constant across time. Moreover, although the Democratic style seems to increase slightly from Time 1 to 2, afterward, it remains constant. This pattern is different in the CP group, wherein the first two time points, the Democratic style remains constant, but there is an increase from Time 2 to 3. As for the Authoritarian and Permissive styles, they both decrease from Time 2 to 3. These results reveal that in general, all parents use more democratic and less authoritarian and/or permissive parenting practices after their participation in the parent training, since the change is obvious from Time 1 to 2 for PC group, and from Time 2 to 3 for CP group.
As far as Parenting Stress is considered, although a decreasing pattern across time seems to exist for all subscales, this pattern is more evident within the PC group than the CP group. The parental self-efficacy, as measured by the PSOC scale, is increasing for the CP group as time passes, whereas there is an increase from Time 1 to 2 for PC group, but it remains constant from Time 2 to 3.
Regarding the results from the ADHD-RS, the Inattention score, for the PC group, seems to keep decreasing from Time 1 to Time 3, but it remains constant from Time 3 to 4, whereas Impulsivity/Hyperactivity score reveals a decreasing pattern in all time points. As for the CP group, a more consistent decreasing pattern exists for both subscales. In general, all parents report fewer inattention and impulsivity/hyperactivity symptoms in their children after parents’ and/or children’s participation in the intervention program.
Figure 2 includes the means of parenting stress (total score), parental self-efficacy (parenting sense of competence; total score), and the two subscales of ADHD (Inattention and Impulsivity/Hyperactivity), across time and groups. Obviously, as hypothesized, all the variables are decreasing as time passes, except for parenting sense of competence, which is increasing. Note also that there is no evidence of interaction between time and group. Therefore, our hypothesis that parents of PC group would report lower levels of parenting stress and higher levels of parental self-efficacy at Time 2 assessment, compared to CP parents, was not supported.
The correlations between the variables of our study, separately for each time point and group (PC and CP; the assessment of significance must be treated with caution due to the small sample sizes), were calculated (Supplementary Table S1). The positive correlation between Democratic parenting style and Parental Distress at Time 1 (r = .341) for the PC group, becomes negative as time passes, while the negative correlation observed between the two variables, for the CP group, is further decreasing. Also, the negative correlation between the Democratic parenting style and the Parent-Child Dysfunctional Interaction score at the beginning of the program (r = -.292, r = -.216 for Time 1 and 2, respectively) is becoming much smaller after Time 2 for PC group; for the CP group, there is also an overall decrease from Time 1 to 4. The almost zero correlation between the Democratic parenting style and the Difficult Child subscale, becomes negative as time passes, for the PC group, but it seems to remain constant over time for the CP group. The same pattern seems to occur between the Democratic style and the total score of the parenting stress scale, for the PC group. However, this is not the case for the CP group, where the negative correlation between the two variables is further decreasing as time passes. Moreover, the negative correlation between Democratic style and Impulsivity/Hyperactivity at Time 1 (r = -.743) for the CP group becomes almost zero at Time 4 (r = .079). On the other hand, there is a positive correlation between the Democratic style and the total score of PSOC for both groups in each time point.
As far as Authoritarian style and its correlations with the subscales of PSI are considered, there are positive correlations between the Authoritarian style and the Parental Distress and Parent-Child Dysfunctional Interaction subscales for both groups (PC and CP). The negligible correlation between Authoritarian style and Difficult child subscale, becomes negative as time passes, for CP group. Reversely, the positive correlation between Authoritarian style and Impulsivity/Hyperactivity at Time 1, for CP group, becomes negligible at Time 4. The same pattern occurs between the Authoritarian style and Inattention score for PC group. Also, for both groups, there is a positive correlation between Authoritarian style and the total score of parenting stress, while the correlation with parental self-efficacy is negative.
The Permissive style seems to be more positively correlated with Parent-Child Dysfunctional Interaction, Difficult Child and Total score of PSI, as time passes, for both groups. In contrast, its correlation with total score of PSOC scale and Inattention, is becoming negative, especially for PC group.
The relatively small correlation of Inattention with the variables of PSI (Parental distress, Parent-child dysfunctional interaction, Difficult child and Total score), at first and last time point, are combined with the moderate positive correlation at Time 2 and 3, for PC group. Also, consistent positive correlations exist, between Impulsivity/Hyperactivity and the subscales of PSI, over time, for PC group. For CP group, however, the positive correlation at Time 1, between Inattention and Parental Distress, becomes negative at the end of the study (Time 4), while the negative correlation between Inattention and Parent-Child Dysfunctional Interaction at Time 1 and 2 becomes positive at Time 3 and 4. Moreover, the positive correlation between Inattention and Difficult Child at the start of the study became even larger at Time 4 (from r = .406 to r = .841). As far as Impulsivity/Hyperactivity, for CP group, is considered, it is worth mentioning the change of direction of the correlations with Parental distress and Parent-Child Dysfunctional Interaction, from positive at Time 1 (r = .255 and r = .238, respectively) to negative at Time 4 (r = -.323 and r = -.121, respectively). The same pattern is observed between Impulsivity/Hyperactivity and Total Score of PSI, for the CP group.
As far as Parenting Sense of Competence is considered, for PC group, the negligible negative and positive correlation with Inattention at Time 1 and 4 respectively, are combined with moderate negative correlations at Time 3 and 4. Conversely, the negative correlation with Impulsivity/Hyperactivity at Time 1 increases by Time 4 (from r = -.350 to r = -114). For the CP group, however, the negative correlation at Time 1 (r = -.266) becomes positive by Time 4 (r = .176).
The most important correlations, according to our aims, to be mentioned is the overall positive correlation of Democratic style with the parental self-efficacy (PSOC Total score) over time, and the mainly negative correlations with the variables of PSI for the parents of both groups. In contrast, there are positive correlations between the Authoritarian and Permissive parenting styles with parenting stress, and negative correlations with parental self-efficacy, for both groups, over time.
Moreover, as one would expect, there are mainly positive correlations between the subscales of PSI across time, for both groups. Conversely, there are mainly negative correlations between the parental self-efficacy (PSOC) with Parental Distress, Parent-Child Dysfunctional Interaction and Total Score of PSI. As far as ADHD-RS is considered, there are mainly positive correlations between the two subscales (Inattention and Impulsivity/Hyperactivity) with Difficult child and Total Score of PSI, while there are mainly negative correlations between the two subscales and PSOC for both groups across time.
The next step would be the assessment of the effect of the intervention (time), group (“PC” and “CP”), training participation (“yes” and “no”), age, and parent’s gender, on our dependent variables (parenting stress, parental self-efficacy, and core symptoms of children’s ADHD). Note that, although the correlation coefficients or the difference of means across groups or time, provide us with useful perspectives in assessing the relationship between variables, they both ignore the multivariate nature of our data. Hence, we initially fit a set of different marginal models (due to the potentially correlated errors), according to the assumed structure of the covariance matrix of errors, and then, the best model is given by the AIC and BIC criteria [86,87,88]. Two interaction terms were among the exploratory variables: between time and group, and between time and training participation.
Table 2 contains the estimated marginal models; note that, following a backward selection procedure, all the interaction terms have been excluded since their contribution is not significant. Thus, for each model, we have resulted in keeping only time and group, as exploratory variables. There is no evidence of a severe violation of model assumptions (i.e., linearity, normality of residuals, and independence between residuals and exploratory variables). All the assumptions have been checked based on the properties of the normalized residuals. Given the regression coefficients of Time, we can see that as time passes, the estimation for Parenting stress, Inattention, and Impulsivity/Hyperactivity decrease (keeping the group fixed). Therefore, we expect a decrease of 5.31 units in stress, on average, from one time point to another. Also, we expect, on average, a decrease of 1.11 units in Inattention and 1.47 units in Impulsivity/Hyperactivity, from one time point to another. In contrast, the effect of Time on Parental self-efficacy is positive and equal to 3.10 units on average.
Furthermore, the effect of the PC group on parental self-efficacy, as measured by the total score of the PSOC scale, and Impulsivity/Hyperactivity is significant. Thus, the estimation for the PC group for Parental self-efficacy is lower than that of the CP group, by 5.94 units, on average, while the estimation for Impulsivity/Hyperactivity is higher by 6.60 units, on average (and keeping time fixed).
Hence, as hypothesized, the results indicate that parents report lower levels of parenting stress and higher levels of parental self-efficacy following their participation in the intervention program compared to their initial (baseline) reports. In addition, as we predicted, parents report that their children's inattention and impulsivity/hyperactivity symptoms have decreased since enrolling in the intervention program.
3.3. Feasibility and Acceptability Outcomes
As previously stated, 14 mothers and 1 father with a mean age of 40.1 years old participated in the psychoeducational parent training. Over the course of the 8-week training, the participants attended on average 6.2 sessions (std = .77). In the final session, participants filled out the EPT-F questionnaire to rate their experience with the parent training. The descriptive statistics of the three scores that are extracted from the EPT-F (Total Satisfaction Score, Program’s Usefulness Score, and Trainers’ Assessment Score) and their correlation coefficients can be found in Table 3. It is worth mentioning that there were not any indications of correlations between the three scores of the evaluation of the program (EPT-F) and the dependent variables of our study.
In general, participants were largely satisfied with the program (mean = 40.60, std = 2.35). More specifically, the majority of parents (80% agree, 13.3% strongly agree) reported that the skills they had learned in the program helped to mitigate their children’s behavior problems and difficulties, while only one parent was not sure (neither agree nor disagree). Furthermore, they all stated (60% agree, 40% strongly agree) that they feel more confident in their ability to use the newly acquired skills to manage any future behavioral problem at home. When asked if their relationship with their child had improved since they began the program, the majority (73.3% agree, 6.7% strongly agree) agreed, while three of them neither agreed nor disagreed. Additionally, they all consented that the program met their expectations (13.3% agree, 86.7% strongly agree) and they would recommend it to parents with related issues (6.7% agree, 93.3% strongly agree).
As far as the usefulness and feasibility of the program’s structure are concerned, participants found the program useful (mean = 63.80, std = 4.24). More precisely, they all stated that the information offered in the program was understandable (26.7% agree, 73.3% strongly agree) and beneficial (20% agree, 80% strongly agree). Furthermore, the majority of parents reported that using the newly acquired skills at home was simple (53.3% agree, 13.3% strongly agree, 33.3% neither agree nor disagree) and useful (46.7% agree, 46.7% strongly agree, 6.7% neither agree nor disagree). Even though some participants (2 parents) expressed their desire for more sessions, the majority thought that the number of sessions was appropriate (40% agree, 46,7% strongly agree). Moreover, all parents reported that the content of the handouts given to them was concise and helpful and that they learned skills they intend to apply in the future.
Regarding the evaluation of the facilitators (trainers) of the program, the participants highly rated their instructors’ competence, preparation, and effectiveness during the sessions.
Taking into consideration the correlations between the three scores extracted from the EPT-F questionnaire, a high positive correlation between the parents’ perceived usefulness of the program and their overall satisfaction (r = .735, p < .01) is revealed. Also, there is a positive correlation between the evaluation of the trainers with both their overall satisfaction from the program (r = .560, p < .05) and their perceived usefulness of the program (r = 646, p < .01).
In addition to the quantitative data, the comments of the participants (qualitative feedback) for the parent training highlighted that they found the program of good quality and providing them with useful information about attention deficits and the co-occurring difficulties observed in children with ADHD. Also, the program contributed to organizing and comprehending their prior knowledge. More importantly, they acknowledged considerable progress on parenting skills and the acquisition of new techniques to interact and support their children effectively. They also pointed out that the psychoeducational training gave them the space to share experiences with other parents, which resulted in empowering each other to endure the adversities. Some of the parents’ insightful comments included the following: “The main benefit I got [from the program] is that I apply better techniques to my child to help him improve a lot.”, “...I gained new knowledge and I shared similar experiences with parents of children facing related adversities.”, “The truth is that I see quite a big change in my child.”, “I am more capable of managing my child.”, “Definitely, I became a more effective parent and was helped to understand my child better”.
4. Discussion
Attention deficits affect various domains in everyday lives of school-aged children that extend beyond the child’s struggles, harming well-being and disrupting the functioning of the entire family system [89,90]. Parents of children with ADHD disorder encounter unique adversities in their parenting journey as they navigate the demands of managing their child’s symptoms and supporting their overall development [91]. In this effort, parenting stress emerges as a prominent concern for parents of children with ADHD. Recent studies consistently demonstrate significantly higher levels of stress experienced by these parents compared to parents of typically developing children [92,93]. The daily demands associated with managing the child’s behavioral difficulties, academic failures and problematic social interactions contribute to elevated stress, adversely affecting parental well-being and influencing parent-child relationship [15,31]. Additionally, parents of children with ADHD commonly report diminished levels of parental self-efficacy [94]. The negative consequences of elevated parenting stress and reduced parental self-efficacy affect the parenting practices used by the parents and the quality of parent-child interactions [23,95]. Addressing these challenges and providing effective support and intervention strategies for parents and children is crucial.
The current study examined the efficacy of the “Child ViReal Support Program” - a comprehensive multi-level intervention program for children with attention deficits and their parents - on parenting stress, parental self-efficacy, and parenting practices, as well as on the core symptoms of children’s ADHD (inattention and impulsivity/hyperactivity). In terms of parenting styles, results indicate mainly negative correlations between democratic style and the subscales of PSI (Parental Distress, Parent-Child Dysfunctional Interaction, Difficult Child and Total Score of parenting stress), while the correlation with parental self-efficacy was positive. In contrast, authoritarian and permissive parenting styles were positively correlated with parenting stress and negatively with parental self-efficacy. These results indicate that parents who adopt a more democratic approach tend to have higher levels of self-efficacy in their parenting abilities, which results in lower parenting stress, while authoritarian and/or permissive parenting practices contribute to higher stress levels and lower self-efficacy among parents. This finding is in accordance with other research concluding that parents of children with ADHD tend to adopt more authoritarian and permissive parenting practices than parents of typically developing children [96], while the symptoms of children could predict the use of more controlling parenting [97,98].
Moreover, our results demonstrate a consistent decrease in authoritarian and permissive parenting styles among parents in both groups (PC and CP) over time. Conversely, there is a slight increase in the democratic style among parents in both groups, particularly from Time 1 to 2 for the PC group and from Time 2 to 3 for the CP group. Hence, it seems that parents, after participating in the training, managed to learn how to utilize more optimal parenting practices and engage in a better interaction with their children. This finding is consistent with the results from the quantitative and qualitative feedback from the feasibility and acceptability measures of the parent training program, in which parents reported that they found the program useful and gained knowledge to understand their children better and be more effective in their roles. These results align with previous research indicating the effectiveness of parent training programs in promoting positive changes in parenting styles [99].
Also, the correlations between the core symptoms of ADHD (inattention and impulsivity/hyperactivity) and the variables of PSI reveal consistent associations. In general, there are positive correlations between the ADHD symptomatology and the subscales of PSI, indicating that higher levels of ADHD symptoms are associated with increased parental distress, dysfunctional interactions between parents and children, and difficulties in managing a challenging child. These findings are similar with other research studies showing that parents of children with ADHD report higher levels of parenting stress and that the severity of ADHD symptoms is positively related to parenting stress [27,31,100]. Conversely, the correlations between the two subscales of ADHD-RS and the PSOC are negative, implying that when parents observe higher ADHD symptomatology in their children, they perceive themselves as less competent in their parenting abilities, a result which is also found in previous research [94].
Regarding parenting stress and parental self-efficacy, they seem to have a negative correlation across time. Research shows that their relations are reciprocal, with parents feeling more anxious if they feel less competent in their parenting role and vice versa [101]. Also, the results indicate that parents of both groups reported significantly lower parenting stress and enhanced levels of parental self-efficacy after their participation in the intervention program and these changes remained significant at a follow-up assessment, four months after the end of the program. Previous research shows that participation in parent training programs has positive effects on parents since they feel more competent and less anxious at the end of the programs [30,102]. These findings are also congruent with the feedback given by parents at the end of the program, in which they reported that they feel more confident in their ability to manage their children’s behavior currently and in the future.
As far as the core symptoms of ADHD are considered, parents observed fewer symptoms of inattention and impulsivity/hyperactivity in their children after their participation in the intervention program compared to their initial reports, and this decrease was present at a follow-up, namely four months after the completion of the intervention. The decrease is evident in both symptoms for both groups starting from Time 2, which supports that both components of the intervention program (parent training and child training) have positive effect on the inattention and impulsivity/hyperactivity of the children. This is consistent with previous research demonstrating the efficacy of intervention programs for alleviating ADHD symptoms [99,103].
Furthermore, the parents of the PC group reported significantly lower levels of parental self-efficacy and higher levels of their children’s impulsivity/hyperactivity compared to the parents of the CP group. The impact of the group on these two variables might be explained by the difference observed in the initial assessment (at Time 1) between the two groups. Hence, it seems that parents of PC group observed higher impulsivity/hyperactivity symptoms in their children, which could affect their perceived efficacy on managing their children’s behavior (parental self-efficacy) since the severity of symptoms can have a negative effect on parents' perceived competence. Another possible explanation for this finding, it could be that parents themselves have ADHD symptoms, which might result in lower levels of perceived efficacy in a variety of domains including their parenting role [94,104,105].
Overall, our study provides valuable evidence of the efficacy of the “Child ViReal Support Program” as an evidence-based intervention program for children with ADHD and their parents in improving parenting practices, diminishing parenting stress, enhancing parental self-efficacy, and reducing the core symptoms of ADHD. These findings are in accordance with prior research and highlight the importance of targeted interventions in supporting families affected by ADHD.
However, it is crucial to acknowledge the limitations of the study, including the small sample size and potential biases associated with self-report measures. The sample size was small, especially when broken down into the two groups (PC, CP) resulting in decreased power to find significant effects between the two components of the intervention program (parent training, child training). Nevertheless, it is of high importance and value that significant results were found even in this relatively small sample between the end of the intervention and the initial assessment of parents and children, indicating the necessity for follow-up research with larger samples. Another limitation of the study is the lack of information regarding parental ADHD symptoms, which could explain the differences observed in parental self-efficacy between the parents of the two groups.
In conclusion, the “Child ViReal Support Program” demonstrates positive outcomes for parents and children and these results contribute to the growing body of literature on effective interventions for families dealing with ADHD disorder, highlighting the importance of addressing both parent and child needs within evidence-based comprehensive treatment approaches.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Pearson correlation coefficients for each time point and group (PC and CP) separately.
Author Contributions
Conceptualization, I.P. and P.D.; methodology, I.P. and P.D.; formal analysis, F.S.M.; investigation, I.P.; resources, P.D. and I.P.; writing—original draft preparation, I.P., P.D. and F.S.M.; writing—review and editing, I.P., P.D. and F.S.M.; visualization, I.P. and F.S.M.; supervision, P.D.; project administration, I.P. and P.D.; funding acquisition, P.D. All authors have read and agreed to the published version of the manuscript.
Funding
The current research has received funding from the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie Grant agreement No.813546 (https://neoprismc.org/).
Institutional Review Board Statement
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. It was also approved by the Research Ethics Committee of the University of Crete (protocol code 51/25.02.2020 on 25 February 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available on reasonable request from the corresponding author.
Acknowledgments
We would like to acknowledge the support from the experts and staff of the Interdisciplinary Evaluation, Counselling and Support Centers (KE.D.A.S.Y.) of Heraklion and Rethymnon in Crete and the Community Children and Adolescents’ Mental Health Centers of Heraklion in Crete, as well as the support from the representatives of Social Space of Kalokairinos Foundation at Heraklion.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A

Table A1.
Sessions of Parent Training Program.
| Sessions | Content |
|---|---|
| Session 1 | Attention deficits and concurrent difficulties Neurobiological background |
| Session 2 | Parenting Stress Stress management strategies |
| Session 3 | Positive attention and Praise Effective instructions/commands |
| Session 4 | Contingency management system |
| Session 5 | Executive functions I Strategies for the enhancement of executive functions |
| Session 6 | Executive functions II Strategies for the enhancement of executive functions |
| Session 7 | Emotional control Self-monitoring and self-regulation Strategies for the enhancement of children’s emotional control and self-regulation |
| Session 8 | Wrap-up and review of the sessions and content covered through the parent training program |
References
- Amso, D.; Scerif, G. The Attentive Brain: Insights from Developmental Cognitive Neuroscience. Nat. Rev. Neurosci. 2015, 16, 606–619. [Google Scholar] [CrossRef] [PubMed]
- Tarver, J.; Daley, D.; Sayal, K. Attention-Deficit Hyperactivity Disorder (ADHD): An Updated Review of the Essential Facts. Child Care Health Dev. 2014, 40, 762–774. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A. Executive Functions. Annu. Rev. Psychol. 2013, 64, 135–168. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Yang, H.-J.; Chen, V.C.; Lee, W.-T.; Teng, M.-J.; Lin, C.-H.; Gossop, M. Meta-Analysis of Quality of Life in Children and Adolescents with ADHD: By Both Parent Proxy-Report and Child Self-Report Using PedsQLTM. Res. Dev. Disabil. 2016, 51–52, 160–172. [Google Scholar] [CrossRef]
- Franke, B.; Michelini, G.; Asherson, P.; Banaschewski, T.; Bilbow, A.; Buitelaar, J.K.; Cormand, B.; Faraone, S.V.; Ginsberg, Y.; Haavik, J.; et al. Live Fast, Die Young? A Review on the Developmental Trajectories of ADHD across the Lifespan. Eur. Neuropsychopharmacol. 2018, 28, 1059–1088. [Google Scholar] [CrossRef]
- Ramos, A.A.; Hamdan, A.C.; Machado, L. A Meta-Analysis on Verbal Working Memory in Children and Adolescents with ADHD. Clin. Neuropsychol. 2020, 34, 873–898. [Google Scholar] [CrossRef]
- Pievsky, M.A.; McGrath, R.E. The Neurocognitive Profile of Attention-Deficit/Hyperactivity Disorder: A Review of Meta-Analyses. Arch. Clin. Neuropsychol. 2018, 33, 143–157. [Google Scholar] [CrossRef]
- Graziano, P.A.; Garcia, A. Attention-Deficit Hyperactivity Disorder and Children’s Emotion Dysregulation: A Meta-Analysis. Clin. Psychol. Rev. 2016, 46, 106–123. [Google Scholar] [CrossRef]
- Sjöwall, D.; Roth, L.; Lindqvist, S.; Thorell, L.B. Multiple Deficits in ADHD: Executive Dysfunction, Delay Aversion, Reaction Time Variability, and Emotional Deficits. J. Child Psychol. Psychiatry 2013, 54, 619–627. [Google Scholar] [CrossRef]
- Fleming, M.; Fitton, C.A.; Steiner, M.F.C.; McLay, J.S.; Clark, D.; King, A.; Mackay, D.F.; Pell, J.P. Educational and Health Outcomes of Children Treated for Attention-Deficit/Hyperactivity Disorder. JAMA Pediatr. 2017, 171, e170691. [Google Scholar] [CrossRef]
- Arnold, L.E.; Hodgkins, P.; Kahle, J.; Madhoo, M.; Kewley, G. Long-Term Outcomes of ADHD: Academic Achievement and Performance. J. Atten. Disord. 2020, 24, 73–85. [Google Scholar] [CrossRef]
- Ros, R.; Graziano, P.A. Social Functioning in Children With or At Risk for Attention Deficit/Hyperactivity Disorder: A Meta-Analytic Review. J. Clin. Child Adolesc. Psychol. 2018, 47, 213–235. [Google Scholar] [CrossRef]
- Mikami, A.Y.; Miller, M.; Lerner, M.D. Social Functioning in Youth with Attention-Deficit/Hyperactivity Disorder and Autism Spectrum Disorder: Transdiagnostic Commonalities and Differences. Clin. Psychol. Rev. 2019, 68, 54–70. [Google Scholar] [CrossRef] [PubMed]
- Azazy, S.; Nour Eldein, H.; Salama, H.; Ismail, M. Quality of Life and Family Function of Parents of Children with Attention Deficit Hyperactivity Disorder. East. Mediterr. Health J. 2018, 24, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Peasgood, T.; Bhardwaj, A.; Biggs, K.; Brazier, J.E.; Coghill, D.; Cooper, C.L.; Daley, D.; De Silva, C.; Harpin, V.; Hodgkins, P.; et al. The Impact of ADHD on the Health and Well-Being of ADHD Children and Their Siblings. Eur. Child Adolesc. Psychiatry 2016, 25, 1217–1231. [Google Scholar] [CrossRef] [PubMed]
- Craig, F.; Operto, F.F.; De Giacomo, A.; Margari, L.; Frolli, A.; Conson, M.; Ivagnes, S.; Monaco, M.; Margari, F. Parenting Stress among Parents of Children with Neurodevelopmental Disorders. Psychiatry Res. 2016, 242, 121–129. [Google Scholar] [CrossRef]
- Leitch, S.; Sciberras, E.; Post, B.; Gerner, B.; Rinehart, N.; Nicholson, J.M.; Evans, S. Experience of Stress in Parents of Children with ADHD: A Qualitative Study. Int. J. Qual. Stud. Health Well-Being 2019, 14, 1690091. [Google Scholar] [CrossRef] [PubMed]
- Deater-Deckard, K. Parenting Stress and Child Adjustment: Some Old Hypotheses and New Questions. Clin. Psychol. Sci. Pract. 1998, 5, 314–332. [Google Scholar] [CrossRef]
- Abidin, R.R. Introduction to the Special Issue: The Stresses of Parenting. J. Clin. Child Psychol. 1990, 19, 298–301. [Google Scholar] [CrossRef]
- Abidin, R.R. The Determinants of Parenting Behavior. J. Clin. Child Psychol. 1992, 21, 407–412. [Google Scholar] [CrossRef]
- Bloomfield, L.; Kendall, S. Parenting Self-Efficacy, Parenting Stress and Child Behaviour before and after a Parenting Programme. Prim. Health Care Res. Dev. 2012, 13, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Albanese, A.M.; Russo, G.R.; Geller, P.A. The Role of Parental Self-efficacy in Parent and Child Well-being: A Systematic Review of Associated Outcomes. Child Care Health Dev. 2019, 45, 333–363. [Google Scholar] [CrossRef] [PubMed]
- Hutchison, L.; Feder, M.; Abar, B.; Winsler, A. Relations between Parenting Stress, Parenting Style, and Child Executive Functioning for Children with ADHD or Autism. J. Child Fam. Stud. 2016, 25, 3644–3656. [Google Scholar] [CrossRef]
- Corcoran, J. Parents’ Experience of Raising a Child with Attention Deficit Disorder. ADHD Rep. 2017, 25, 6–10. [Google Scholar] [CrossRef]
- Theule, J.; Cheung, K.; Aberdeen, K. Children’s ADHD Interventions and Parenting Stress: A Meta-Analysis. J. Child Fam. Stud. 2018, 27, 2744–2756. [Google Scholar] [CrossRef]
- Modesto-Lowe, V.; Danforth, J.S.; Brooks, D. ADHD: Does Parenting Style Matter? Clin. Pediatr. (Phila.) 2008, 47, 865–872. [Google Scholar] [CrossRef]
- Theule, J.; Wiener, J.; Tannock, R.; Jenkins, J.M. Parenting Stress in Families of Children With ADHD: A Meta-Analysis. J. Emot. Behav. Disord. 2013, 21, 3–17. [Google Scholar] [CrossRef]
- Corcoran, J.; Schildt, B.; Hochbrueckner, R.; Abell, J. Parents of Children with Attention Deficit/Hyperactivity Disorder: A Meta-Synthesis, Part I. Child Adolesc. Soc. Work J. 2017, 34, 281–335. [Google Scholar] [CrossRef]
- Sanders, M.R.; Woolley, M.L. The Relationship between Maternal Self-Efficacy and Parenting Practices: Implications for Parent Training: Self-Efficacy and Parenting Practices. Child Care Health Dev. 2005, 31, 65–73. [Google Scholar] [CrossRef]
- Marino, R.L.D.F.; Teixeira, M.C.T.V.; Cantiere, C.N.; Ribeiro, A.D.F.; Micieli, A.P.R.; Carreiro, L.R.R. Parenting Styles and Mental Health in Parents of Children with ADHD. Rev. Interam. Psicol. J. Psychol. 2019, 53, 417–430. [Google Scholar] [CrossRef]
- Muñoz-Silva, A.; Lago-Urbano, R.; Sanchez-Garcia, M.; Carmona-Márquez, J. Child/Adolescent’s ADHD and Parenting Stress: The Mediating Role of Family Impact and Conduct Problems. Front. Psychol. 2017, 8, 2252. [Google Scholar] [CrossRef] [PubMed]
- Theule, J.; Wiener, J.; Rogers, M.A.; Marton, I. Predicting Parenting Stress in Families of Children with ADHD: Parent and Contextual Factors. J. Child Fam. Stud. 2011, 20, 640–647. [Google Scholar] [CrossRef]
- Perez Algorta, G.; Kragh, C.A.; Arnold, L.E.; Molina, B.S.G.; Hinshaw, S.P.; Swanson, J.M.; Hechtman, L.; Copley, L.M.; Lowe, M.; Jensen, P.S. Maternal ADHD Symptoms, Personality, and Parenting Stress: Differences Between Mothers of Children With ADHD and Mothers of Comparison Children. J. Atten. Disord. 2018, 22, 1266–1277. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative Efficacy and Tolerability of Medications for Attention-Deficit Hyperactivity Disorder in Children, Adolescents, and Adults: A Systematic Review and Network Meta-Analysis. Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.W.; Owens, J.S.; Bunford, N. Evidence-Based Psychosocial Treatments for Children and Adolescents with Attention-Deficit/Hyperactivity Disorder. J. Clin. Child Adolesc. Psychol. 2014, 43, 527–551. [Google Scholar] [CrossRef] [PubMed]
- Pelham, W.E.; Fabiano, G.A.; Waxmonsky, J.G.; Greiner, A.R.; Gnagy, E.M.; Pelham, W.E.; Coxe, S.; Verley, J.; Bhatia, I.; Hart, K.; et al. Treatment Sequencing for Childhood ADHD: A Multiple-Randomization Study of Adaptive Medication and Behavioral Interventions. J. Clin. Child Adolesc. Psychol. 2016, 45, 396–415. [Google Scholar] [CrossRef]
- Pelham, W.E.; Altszuler, A.R. Combined Treatment for Children with Attention-Deficit/Hyperactivity Disorder: Brief History, the Multimodal Treatment for Attention-Deficit/Hyperactivity Disorder Study, and the Past 20 Years of Research. J. Dev. Behav. Pediatr. 2020, 41, S88–S98. [Google Scholar] [CrossRef]
- Storebø, O.J.; Ramstad, E.; Krogh, H.B.; Nilausen, T.D.; Skoog, M.; Holmskov, M.; Rosendal, S.; Groth, C.; Magnusson, F.L.; Moreira-Maia, C.R.; et al. Methylphenidate for Children and Adolescents with Attention Deficit Hyperactivity Disorder (ADHD). Cochrane Database Syst. Rev. 2015, 2016. [Google Scholar] [CrossRef]
- Van De Loo-Neus, G.H.H.; Rommelse, N.; Buitelaar, J.K. To Stop or Not to Stop? How Long Should Medication Treatment of Attention-Deficit Hyperactivity Disorder Be Extended? Eur. Neuropsychopharmacol. 2011, 21, 584–599. [Google Scholar] [CrossRef]
- Keilow, M.; Holm, A.; Fallesen, P. Medical Treatment of Attention Deficit/Hyperactivity Disorder (ADHD) and Children’s Academic Performance. PLOS ONE 2018, 13, e0207905. [Google Scholar] [CrossRef]
- Tsujii, N.; Okada, T.; Usami, M.; Kuwabara, H.; Fujita, J.; Negoro, H.; Kawamura, M.; Iida, J.; Saito, T. Effect of Continuing and Discontinuing Medications on Quality of Life After Symptomatic Remission in Attention-Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. J. Clin. Psychiatry 2020, 81. [Google Scholar] [CrossRef] [PubMed]
- Ferrin, M.; Perez-Ayala, V.; El-Abd, S.; Lax-Pericall, T.; Jacobs, B.; Bilbow, A.; Taylor, E. A Randomized Controlled Trial Evaluating the Efficacy of a Psychoeducation Program for Families of Children and Adolescents With ADHD in the United Kingdom: Results After a 6-Month Follow-Up. J. Atten. Disord. 2020, 24, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Ferrin, M.; Moreno-Granados, J.M.; Salcedo-Marin, M.D.; Ruiz-Veguilla, M.; Perez-Ayala, V.; Taylor, E. Evaluation of a Psychoeducation Programme for Parents of Children and Adolescents with ADHD: Immediate and Long-Term Effects Using a Blind Randomized Controlled Trial. Eur. Child Adolesc. Psychiatry 2014, 23, 637–647. [Google Scholar] [CrossRef]
- Barkley, R.A. Defiant Children: A Clinician’s Manual for Assessment and Parent Training, 3rd Ed; 3rd ed.; Guilford Press: New York, NY, US, 2013; pp. xii, 228; ISBN 978-1-4625-0950-8. [Google Scholar]
- Kazdin, A.E. Parent Management Training: Treatment for Oppositional, Aggressive, and Antisocial Behavior in Children and Adolescents; Parent management training: Treatment for oppositional, aggressive, and antisocial behavior in children and adolescents; Oxford University Press: New York, NY, US, 2005; pp. ix, 410; ISBN 978-0-19-515429-0. [Google Scholar]
- Dekkers, T.J.; Hornstra, R.; Van Der Oord, S.; Luman, M.; Hoekstra, P.J.; Groenman, A.P.; Van Den Hoofdakker, B.J. Meta-Analysis: Which Components of Parent Training Work for Children With Attention-Deficit/Hyperactivity Disorder? J. Am. Acad. Child Adolesc. Psychiatry 2022, 61, 478–494. [Google Scholar] [CrossRef]
- Gümüs, F.; Ergün, G.; Dikeç, G. Effect of Psychoeducation on Stress in Parents of Children With Attention-Deficit/Hyperactivity Disorder: A Randomized Controlled Study. J. Psychosoc. Nurs. Ment. Health Serv. 2020, 58, 34–41. [Google Scholar] [CrossRef]
- Chen, V.C.-H.; Yeh, C.-J.; Lee, T.-C.; Chou, J.-Y.; Shao, W.-C.; Shih, D.-H.; Chen, C.-I.; Lee, P.-C. Symptoms of Attention Deficit Hyperactivity Disorder and Quality of Life of Mothers of School-Aged Children: The Roles of Child, Mother, and Family Variables. Kaohsiung J. Med. Sci. 2014, 30, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Coates, J.; Taylor, J.A.; Sayal, K. Parenting Interventions for ADHD: A Systematic Literature Review and Meta-Analysis. J. Atten. Disord. 2015, 19, 831–843. [Google Scholar] [CrossRef]
- Yao, A.; Shimada, K.; Kasaba, R.; Tomoda, A. Beneficial Effects of Behavioral Parent Training on Inhibitory Control in Children With Attention-Deficit/Hyperactivity Disorder: A Small-Scale Randomized Controlled Trial. Front. Psychiatry 2022, 13, 859249. [Google Scholar] [CrossRef]
- Loren, R.E.A.; Vaughn, A.J.; Langberg, J.M.; Cyran, J.E.M.; Proano-Raps, T.; Smolyansky, B.H.; Tamm, L.; Epstein, J.N. Effects of an 8-Session Behavioral Parent Training Group for Parents of Children With ADHD on Child Impairment and Parenting Confidence. J. Atten. Disord. 2015, 19, 158–166. [Google Scholar] [CrossRef]
- Daley, D.; Van Der Oord, S.; Ferrin, M.; Danckaerts, M.; Doepfner, M.; Cortese, S.; Sonuga-Barke, E.J.S. Behavioral Interventions in Attention-Deficit/Hyperactivity Disorder: A Meta-Analysis of Randomized Controlled Trials Across Multiple Outcome Domains. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 835–847. [Google Scholar] [CrossRef]
- Lee, P.; Niew, W.; Yang, H.; Chen, V.C.; Lin, K. A Meta-Analysis of Behavioral Parent Training for Children with Attention Deficit Hyperactivity Disorder. Res. Dev. Disabil. 2012, 33, 2040–2049. [Google Scholar] [CrossRef] [PubMed]
- Heath, C.L.; Curtis, D.F.; Fan, W.; McPherson, R. The Association Between Parenting Stress, Parenting Self-Efficacy, and the Clinical Significance of Child ADHD Symptom Change Following Behavior Therapy. Child Psychiatry Hum. Dev. 2015, 46, 118–129. [Google Scholar] [CrossRef] [PubMed]
- Larsen, L.B.; Daley, D.; Lange, A.-M.; Sonuga-Barke, E.; Thomsen, P.H.; Rask, C.U. Effect of Parent Training on Health-Related Quality of Life in Preschool Children With Attention-Deficit/Hyperactivity Disorder: A Secondary Analysis of Data From a Randomized Controlled Trial. J. Am. Acad. Child Adolesc. Psychiatry 2021, 60, 734–744.e3. [Google Scholar] [CrossRef] [PubMed]
- Dimitropoulou, P.; Pachiti, I. Determinants of Treatment Response to State-of-the-Art Interventions for Attention Deficits: Child Temperament, Cognitive Profiles and Family Dynamics; clinicaltrials.gov. 2022. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children | Fifth Edition; Pearson: Bloomington, MN, US, 2014. [Google Scholar]
- Wechsler, D. Wechsler Intelligence Scale for Children-Fifth Edition. Technical and Interpretive Manual Supplement: Special Group Validity Studies with Other Measures and Additional Tables; Pearson: Bloomington, MN, US, 2014. [Google Scholar]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated Guidelines for Reporting Parallel Group Randomised Trials. J. Clin. Epidemiol. 2010, 63, e1–e37. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Ferrin, M.; Brandeis, D.; Buitelaar, J.; Daley, D.; Dittmann, R.W.; Holtmann, M.; Santosh, P.; Stevenson, J.; Stringaris, A.; et al. Cognitive Training for Attention-Deficit/Hyperactivity Disorder: Meta-Analysis of Clinical and Neuropsychological Outcomes From Randomized Controlled Trials. J. Am. Acad. Child Adolesc. Psychiatry 2015, 54, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.R.; Kim, H.-J.; Silvestri, R. Cognitive Constructs and Individual Differences Underlying ADHD and Dyslexia: A Cognitive Mosaic Approach. In Cognition, Intelligence, and Achievement: A tribute to J. P. Das; Papadopoulos, T.C., Parilla, R.K., Kirby, J.R., Eds.; Elsevier Academic Press, 2015; pp. 197–223 ISBN 978-0-12-410388-7.
- Rapport, M.D.; Orban, S.A.; Kofler, M.J.; Friedman, L.M.; Bolden, J. Executive Function Training for Children with ADHD. In Attention-Deficit Hyperactivity Disorder: A handbook for diagnosis and treatment; Barkley, R.A., Ed.; Guilford Press: New York, NY, US, 2015; pp. 1131–1171. [Google Scholar]
- Jolles, D.D.; Crone, E.A. Training the Developing Brain: A Neurocognitive Perspective. Front. Hum. Neurosci. 2012, 6. [Google Scholar] [CrossRef]
- DuPaul, G.J.; Power, T.J.; Anastopoulos, A.D.; Reid, R. ADHD Rating Scale—IV: Checklists, Norms, and Clinical Interpretation; The Guilford Press: New York, NY, US, 1998; ISBN 978-1-57230-423-9. [Google Scholar]
- Kalantzi-Azizi, A.; Ageli, K.; Efstathiou, G. Greek ADHD Rating Scale–IV; Hellenic Grammata: Athens, Greece, 2005. [Google Scholar]
- Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR; American Psychiatric Association, Ed.; 4th ed., text revision; American Psychiatric Association: Washington, DC, 2000; ISBN 978-0-89042-024-9.
- Abidin, R.R. Parenting Stress Index: Manual, Administration Booklet, [and] Research Update; Pediatric Psychology Press: Charlottesville, VA, US, 1983. [Google Scholar]
- Abidin, R.R. Parenting Stress Index, Third Edition: Professional Manual; Psychological Assessment Resources, Inc: Odessa, FL, US, 1995. [Google Scholar]
- Leze, E. Clinical genetic evaluation and developmental examination of children born with preimplantation genetic diagnosis: evaluation of parental stress. Ph.D. thesis, National and Kapodistrian University of Athens (NKUA): Athens, Greece, 2013.
- Gibaud-Wallston, J.; Wandersman, L.P. Development and Utility of the Parenting Sense of Competence Scale 1978.
- Johnston, C.; Mash, E.J. A Measure of Parenting Satisfaction and Efficacy. J. Clin. Child Psychol. 1989, 18, 167–175. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-Translation for Cross-Cultural Research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Brislin, R.W. The Wording and Translation of Research Instruments. In Field methods in cross-cultural research; Sage Publications, Inc: Thousand Oaks, CA, US, 1986; pp. 137–164. ISBN 978-0-8039-2549-6. [Google Scholar]
- Ozolins, U.; Hale, S.; Cheng, X.; Hyatt, A.; Schofield, P. Translation and Back-Translation Methodology in Health Research – a Critique. Expert Rev. Pharmacoecon. Outcomes Res. 2020, 20, 69–77. [Google Scholar] [CrossRef]
- Robinson, C.C.; Mandleco, B.; Olsen, S.F.; Hart, C.H. The Parenting Styles and Dimensions Questionnaire (PSDQ). In Handbook of family measurement techniques (Vol. 3). Instruments and index; Perlmutter, B.F., Touliatos, J., Holden, G.W., Eds.; Sage: Thousand Oaks, CA, 2001; Vol. 3, pp. 319–321. [Google Scholar]
- Baumrind, D. Child Care Practices Anteceding Three Patterns of Preschool Behavior. Genet. Psychol. Monogr. 1967, 75, 43–88. [Google Scholar]
- Maridaki-Kassotaki, A. Greek father’s parental typology according to child rearing practice: Adaptation and standardization of the “Parenting Styles and Dimensions Questionnaire (PSDQ). ” Epistimes Agogis 2009, 4, 23–33. [Google Scholar]
- Antonopoulou, K.; Tsitsas, G. Investigation of the Greek mother’s typology: Standardization of the Parenting Styles and Dimensions Questionnaire (PSDQ). Epistimes Agogis 2011, 2, 51–60. [Google Scholar]
- Brestan, E.V.; Jacobs, J.R.; Rayfield, A.D.; Eyberg, S.M. A Consumer Satisfaction Measure for Parent–Child Treatments and Its Relation to Measures of Child Behavior Change. Behav. Ther. 1999, 30, 17–30. [Google Scholar] [CrossRef]
- Eyberg, S. Consumer Satisfaction Measures for Assessing Parent Training Programs. In Innovations in clinical practice: A source book, Vol. 12; VandeCreek, L., Knapp, S., Jackson, T.L., Eds.; Professional Resource Press/Professional Resource Exchange: Sarasota, FL, US, 1993; pp. 377–382. ISBN 978-0-943158-98-3. [Google Scholar]
- Kazdin, A.E. Acceptability of Alternative Treatments for Deviant Child Behavior. J. Appl. Behav. Anal. 1980, 13, 259–273. [Google Scholar] [CrossRef]
- Webster-Stratton, C. The Incredible Years: Parents, Teachers, and Children Training Series. Resid. Treat. Child. Youth 2001, 18, 31–45. [Google Scholar] [CrossRef]
- Diggle, P.; Heagerty, P.; Liang, K.-Y.; Zeger, S.L. (Eds.) In Analysis of Longitudinal Data, 2nd. ed; OUP Oxford, 2002; ISBN 978-0-19-852484-7.
- IBM Corp. Released 2021. IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp.
- R Core Team (2020). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria.
- Akaike, H. Information Theory and an Extension of Maximum Likelihood Principle. Proc. 2nd Int. Symp. Inf. Theory 1973, 267–281. [Google Scholar]
- Akaike, H. A New Look at the Statistical Model Identification. In Selected Papers of Hirotugu Akaike; Parzen, E., Tanabe, K., Kitagawa, G., Eds.; Springer Series in Statistics; Springer: New York, NY, 1998; pp. 215–222; ISBN 978-1-4612-1694-0. [Google Scholar]
- Stone, M. Comments on Model Selection Criteria of Akaike and Schwarz. J. R. Stat. Soc. Ser. B Methodol. 1979, 41, 276–278. [Google Scholar] [CrossRef]
- Haack, L.M.; Villodas, M.T.; McBurnett, K.; Hinshaw, S.; Pfiffner, L.J. Parenting Mediates Symptoms and Impairment in Children With ADHD-Inattentive Type. J. Clin. Child Adolesc. Psychol. 2016, 45, 155–166. [Google Scholar] [CrossRef]
- Mofokeng, M.; Van Der Wath, A.E. Challenges Experienced by Parents Living with a Child with Attention Deficit Hyperactivity Disorder. J. Child Adolesc. Ment. Health 2017, 29, 137–145. [Google Scholar] [CrossRef]
- Dey, M.; Paz Castro, R.; Haug, S.; Schaub, M.P. Quality of Life of Parents of Mentally-Ill Children: A Systematic Review and Meta-Analysis. Epidemiol. Psychiatr. Sci. 2019, 28, 563–577. [Google Scholar] [CrossRef]
- Wiener, J.; Biondic, D.; Grimbos, T.; Herbert, M. Parenting Stress of Parents of Adolescents with Attention-Deficit Hyperactivity Disorder. J. Abnorm. Child Psychol. 2016, 44, 561–574. [Google Scholar] [CrossRef] [PubMed]
- Sollie, H.; Mørch, W.-T.; Larsson, B. Parent and Family Characteristics and Their Associates in a Follow-Up of Outpatient Children with ADHD. J. Child Fam. Stud. 2016, 25, 2571–2584. [Google Scholar] [CrossRef]
- Primack, B.A.; Hendricks, K.M.; Longacre, M.R.; Adachi-Mejia, A.M.; Weiss, J.E.; Titus, L.J.; Beach, M.L.; Dalton, M.A. Parental Efficacy and Child Behavior in a Community Sample of Children with and without Attention-Deficit Hyperactivity Disorder (ADHD). ADHD Atten. Deficit Hyperact. Disord. 2012, 4, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Cussen, A.; Sciberras, E.; Ukoumunne, O.C.; Efron, D. Relationship between Symptoms of Attention-Deficit/Hyperactivity Disorder and Family Functioning: A Community-Based Study. Eur. J. Pediatr. 2012, 171, 271–280. [Google Scholar] [CrossRef]
- Gau, S.S.-F.; Chang, J.P.-C. Maternal Parenting Styles and Mother–Child Relationship among Adolescents with and without Persistent Attention-Deficit/Hyperactivity Disorder. Res. Dev. Disabil. 2013, 34, 1581–1594. [Google Scholar] [CrossRef] [PubMed]
- Kopala-Sibley, D.C.; Jelinek, C.; Kessel, E.M.; Frost, A.; Allmann, A.E.S.; Klein, D.N. Parental Depressive History, Parenting Styles, and Child Psychopathology over 6 Years: The Contribution of Each Parent’s Depressive History to the Other’s Parenting Styles. Dev. Psychopathol. 2017, 29, 1469–1482. [Google Scholar] [CrossRef]
- Allmann, A.E.S.; Klein, D.N.; Kopala-Sibley, D.C. Bidirectional and Transactional Relationships between Parenting Styles and Child Symptoms of ADHD, ODD, Depression, and Anxiety over 6 Years. Dev. Psychopathol. 2022, 34, 1400–1411. [Google Scholar] [CrossRef]
- Daley, D.; Van Der Oord, S.; Ferrin, M.; Danckaerts, M.; Doepfner, M.; Cortese, S.; Sonuga-Barke, E.J.S. Behavioral Interventions in Attention-Deficit/Hyperactivity Disorder: A Meta-Analysis of Randomized Controlled Trials Across Multiple Outcome Domains. J. Am. Acad. Child Adolesc. Psychiatry 2014, 53, 835–847. [Google Scholar] [CrossRef]
- Si, Y.; Ma, J.L.C.; Zhang, J. Factors Influencing Parenting Stress among Chinese Families of Children with Attention-Deficit/Hyperactivity Disorder. Child. Youth Serv. Rev. 2020, 116, 105148. [Google Scholar] [CrossRef]
- Crnic, K.; Ross, E. Parenting Stress and Parental Efficacy. In Parental Stress and Early Child Development; Deater-Deckard, K., Panneton, R., Eds.; Springer International Publishing: Cham, 2017; pp. 263–284; ISBN 978-3-319-55374-0. [Google Scholar]
- Ciesielski, H.A.; Loren, R.E.A.; Tamm, L. Behavioral Parent Training for ADHD Reduces Situational Severity of Child Noncompliance and Related Parental Stress. J. Atten. Disord. 2020, 24, 758–767. [Google Scholar] [CrossRef]
- Rimestad, M.L.; Lambek, R.; Zacher Christiansen, H.; Hougaard, E. Short- and Long-Term Effects of Parent Training for Preschool Children With or at Risk of ADHD: A Systematic Review and Meta-Analysis. J. Atten. Disord. 2019, 23, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Williamson, D.; Johnston, C. Maternal ADHD Symptoms and Parenting Stress: The Roles of Parenting Self-Efficacy Beliefs and Neuroticism. J. Atten. Disord. 2019, 23, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Johnston, C. The Relationship Between ADHD Symptoms and Competence as Reported by Both Self and Others. J. Atten. Disord. 2012, 16, 418–426. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Participant flow diagram.
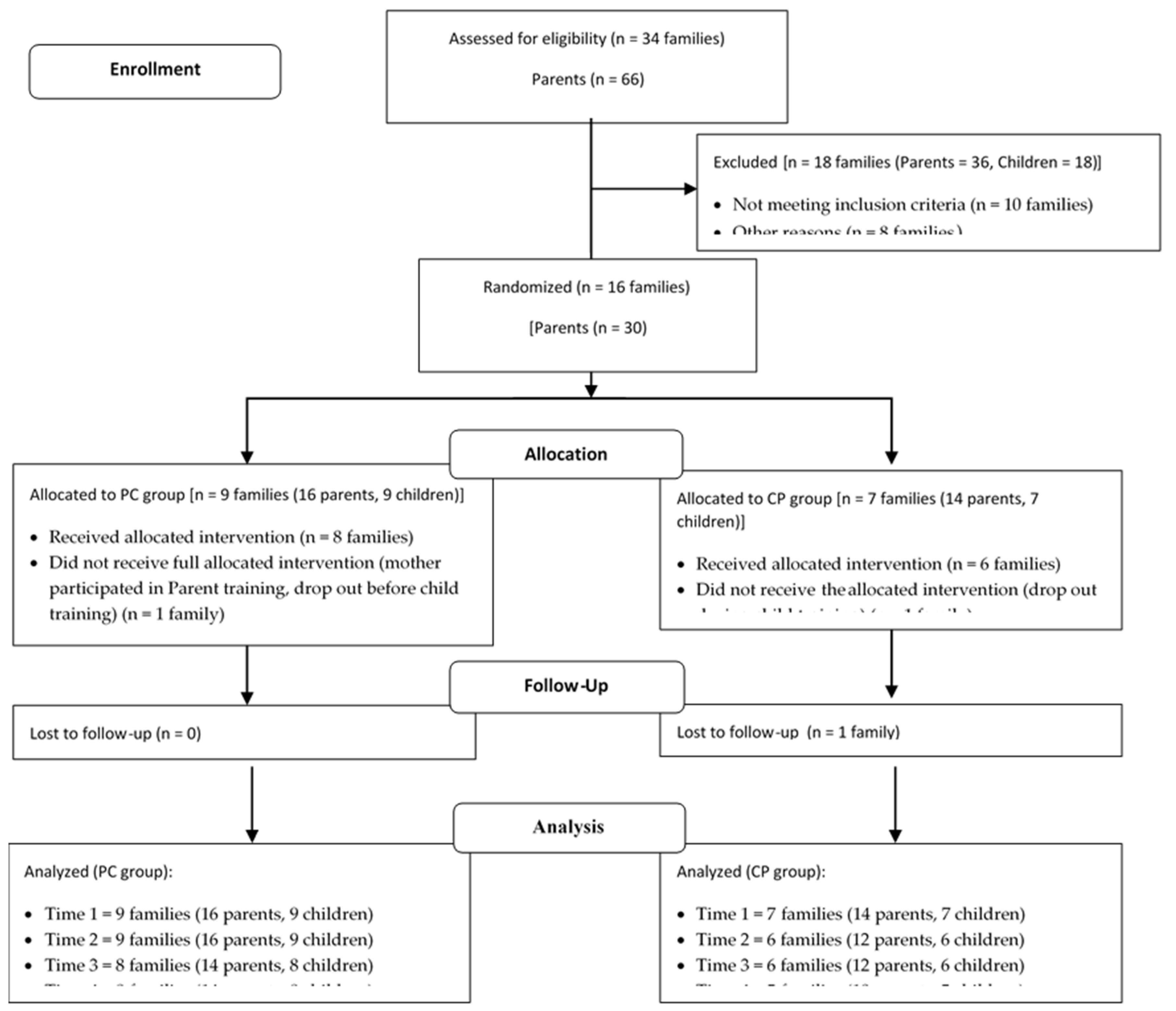
Figure 2.
Mean plots across time, and for each group (PC and CP), separately.
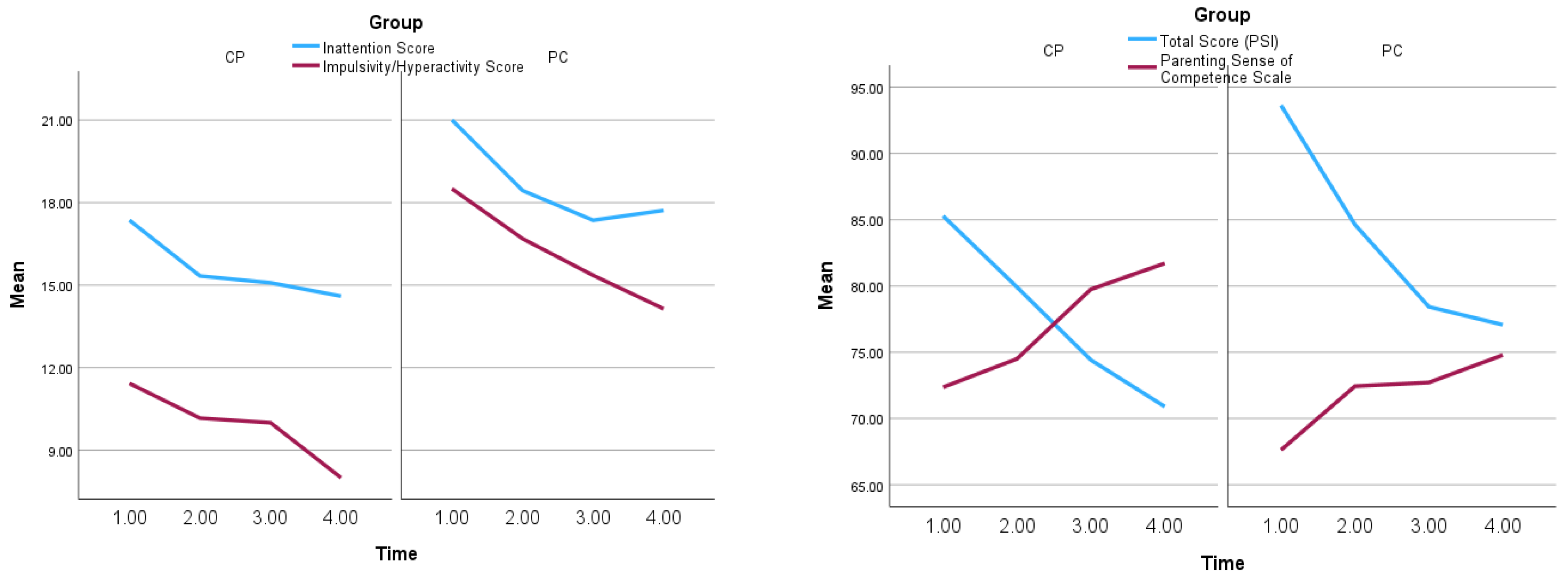
Table 1.
Means (std in parentheses) of subscales, for each time point and group, along with Friedman's two-way analysis of variance (testing equality of means across time).
Table 1.
Means (std in parentheses) of subscales, for each time point and group, along with Friedman's two-way analysis of variance (testing equality of means across time).
| Group | Scale | Subscale | Time 1 (n=30) | Time 2 (n=28) | Time 3 (n=26) | Time 4 (n=24) |
|---|---|---|---|---|---|---|
| PC | Parenting Styles and Dimensions Questionnaire | Democratic | 4.03 (0.74) | 4.16 (0.47) | 4.16 (0.57) | 4.15 (0.57) |
| Authoritarian* | 1.98 (0.51) | 1.94 (0.52) | 1.88 (0.61) | 1.67 (0.49) | ||
| Permissive** | 3.11 (0.65) | 3.09 (0.55) | 3.03 (0.54) | 2.66 (0.65) | ||
| Strict | 3.84 (0.52) | 3.88 (0.48) | 3.73 (0.5) | 3.71 (0.59) | ||
| Parenting Stress Index-Short Form (PSI-SF) | Parental Distress | 29.25 (8.19) | 26.25 (9.07) | 25.07 (9.41) | 25.93 (10.21) | |
| Parent-Child Dysfunctional Interaction** |
29.25 (8.64) | 25.88 (7.35) | 25.29 (7.28) | 23.14 (7.39) | ||
| Difficult Child*** | 35.13 (8.38) | 32.5 (7.85) | 28.07 (7.64) | 28 (7.54) | ||
| Total Score* | 93.63 (22.7) | 84.63 (20.61) | 78.43 (21.69) | 77.07 (22.43) | ||
| Parenting Sense of Competence (PSOC) | Total Score* | 67.63 (8.16) | 72.44 (9.42) | 72.71 (9.43) | 74.79 (11.41) | |
| ADHD Rating Scale-IV | Inattention* | 21 (3.37) | 18.44 (4.27) | 17.36 (4.27) | 17.71 (4.81) | |
| Impulsivity/ Hyperactivity* |
18.5 (5.09) | 16.69 (6.02) | 15.36 (4.77) | 14.14 (5.78) | ||
| CP | Parenting Styles and Dimensions Questionnaire | Democratic* | 4.18 (0.51) | 4.15 (0.44) | 4.38 (0.51) | 4.3 (0.55) |
| Authoritarian | 1.64 (0.62) | 1.67 (0.48) | 1.4 (0.35) | 1.47 (0.43) | ||
| Permissive** | 3.14 (0.49) | 3.18 (0.4) | 2.83 (0.61) | 2.78 (0.69) | ||
| Strict | 3.55 (0.5) | 3.5 (0.55) | 3.19 (0.54) | 3.45 (0.71) | ||
| Parenting Stress Index-Short Form (PSI-SF) | Parental Distress | 27.5 (6.6) | 27.58 (6.43) | 27.25 (6.45) | 25.4 (7.52) | |
| Parent-Child Dysfunctional Interaction** |
25.36 (6.83) | 23 (4.67) | 20.83 (5.8) | 21.6 (5.72) | ||
| Difficult Child*** | 32.43 (5.5) | 29.33 (8.04) | 26.33 (6.44) | 23.9 (5.69) | ||
| Total Score** | 85.29 (16.69) | 79.92 (10.77) | 74.42 (13.94) | 70.9 (13.63) | ||
| Parenting Sense of Competence (PSOC) | Total Score*** | 72.36 (9.08) | 74.5 (8.6) | 79.75 (7.48) | 81.7 (7.57) | |
| ADHD Rating Scale-IV | Inattention | 17.36 (4.96) | 15.33 (5.47) | 15.08 (4.32) | 14.6 (6.38) | |
| Impulsivity/ Hyperactivity |
11.43 (4.11) | 10.17 (4.57) | 10 (3.88) | 8 (4.16) |
*p<.05, **p<.01, ***p<.001
Table 2.
Estimation of marginal models, for each of the four dependent variables (using generalized least squares estimation method).
Table 2.
Estimation of marginal models, for each of the four dependent variables (using generalized least squares estimation method).
| Dependent Variable | ||||
|---|---|---|---|---|
| Parameters | Parenting Stress |
Parenting Sense of Competence | Inattention | Impulsivity/ Hyperactivity |
| Intercept | 91.54 | 70.01 | 18.42 | 13.05 |
| Group (PC:1, CP:0) |
5.56 | -5.94* | 2.84 | 6.60*** |
| Time (1-4) |
-5.31*** | 3.10*** | -1.11*** | -1.47*** |
| Correlation Structure | Autoregressive, AR (1) | Autoregressive, AR (1) | Compound symmetry |
Compound symmetry |
*p<.05, **p<.01, ***p<.001
Table 3.
Means (std in parentheses) and Pearson correlation coefficients of the scores extracted from the Evaluation of Parent Training Final Questionnaire.
Table 3.
Means (std in parentheses) and Pearson correlation coefficients of the scores extracted from the Evaluation of Parent Training Final Questionnaire.
| Evaluation of Parent Training_Final Questionnaire | ||||
|---|---|---|---|---|
| Sessions attended | Satisfaction Score | Program’s Usefulness Score | Trainers’ Assessment Score | |
| Mean (std) | 6.20 (0.77) | 40.60 (2.35) | 63.80 (4.24) | 39.33 (2.05) |
| Satisfaction Score | 0.439 | |||
| Program’s Usefulness Score | 0.035 | .735** | ||
| Trainers’ Assessment Score | 0.045 | .560* | .646** | |
*p<.05, **p<.01, ***p<.001
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



