
Submitted:
05 July 2023
Posted:
07 July 2023
You are already at the latest version
Abstract
Background and Objectives: Jehovah's Witnesses (JW) reject the transfusion of blood components based on their religious beliefs even if they are in danger of harm or death. In cardiac surgery, this significantly reduces the margin of safety and leads to ethical conflicts. Informed consent should be carefully documented and the patient's family should be involved. This study aims to compare the postoperative course of JW who underwent major cardiac surgery with a similar population of non-Witnesses (NW). Patients and Methods: Demographic, procedural, and postoperative data of all consecutive JW who underwent cardiac surgery at our institution were obtained from the records. They were compared with a propensity score matched group of NW. Anemic JW were treated with erythropoietin and/or iron as needed. Cardiac surgery was performed by experienced surgeons using median sternotomy and cardiopulmonary bypass. Common blood-sparing techniques were routinely used. Periprocedural morbidity and mortality were statistically evaluated for both groups. Results: 32 JW and 64 NW were part of the matched dataset showing no demographic or procedural differences. EPO was used preoperatively in 34.4% and postoperatively in 15.6% of JW but not in NW. Preoperative hemoglobin levels were similar (JW, 8.09±0.99 mmol/l; NW, 8.18±1.06; p=0.683). JW did not receive any transfusions except for one who revoked, while NW transfusion rates were 2.5±3.1 units for red cells (p<0.001) and 0.3±0.8 for platelets (p=0.018). Postoperative levels differed significantly for hemoglobin (JW, 6.05±1.00 mmol/l; NW, 6.88±0.87; p<0.001), and hematocrit (JW, 0.29±0.04; NW, 0.33±0.04; p<0.001) but not for creatinine. Early mortality was similar (JW, 6.3%; NW, 4.7%; p=0.745). There were more pacemakers and pneumonias in JW, while all other postoperative conditions were not different. Conclusions: Real-world data indicate that Jehovah's Witnesses can safely undergo cardiac surgery provided that patients are preconditioned and treated by experienced surgeons who use blood-saving strategies. Postoperative anemia is observed but does not translate into a worse clinical outcome. This is consistent with other studies.
Keywords:
Jehovah’s Witnesses
; cardiac surgery
; outcome
; transfusion
; blood
1. Introduction
Jehovah's Witnesses reject the transfusion of blood and blood components based on their religious beliefs. Specifically, this involves the administration of red blood cell concentrates, fresh plasma, platelets, or white blood cells. They do so in accordance with their right to self-determination, even if refusal would result in physical harm or death [1,2,3,4,5,6]. Autologous blood predonation is also refused as blood must not leave the body to remain clean, according to their belief [7,8]. In contrast, cell salvage and autologous retransfusion is generally accepted as long as the blood circulates in a closed loop and thus remains in continuity with the body [3,8]. As a rule, corresponding declarations of intent are submitted in written form and contain detailed information about the products and methods accepted or rejected [2,9].
Surgery without the use of blood products is a challenge for the surgeon in charge. Every surgeon strives to operate in a blood-saving manner, but unforeseen situations can always arise. In this case, the blood loss cannot be compensated and impaired coagulation can only be treated with restrictions. Taken together, this leads to a narrowing of the safety margin and can thus cause ethical conflicts between the patient and the treating physicians. This is particularly true when minors or otherwise vulnerable individuals are involved. To date, there are no strict guidelines, and many clinics do not want to take this risk and therefore refuse such patients. Furthermore, no physician can be forced to provide treatment if it causes ethical conflicts.
The patient and family must be thoroughly informed about blood-sparing treatment options and the consequences of not receiving a transfusion. If this is a realistic possibility, they should be explicitly informed about permanent damage or death. Another concern in this context is the management of patients who are already anemic. Jehovah's Witnesses usually provide prefabricated forms in which the refusal of the blood transfusion is explicitly documented. It should be clarified in detail which blood components and procedures are acceptable and which are not [2,10]. All conversations should be documented with particular care and the results of the conversation should be countersigned in the presence of a witness, if necessary. However, the patient's will should be re-evaluated again and again during the treatment, especially when the situation becomes critical [11].
As of 2022, there are nearly 8.7 million Jehovah's Witnesses in 239 countries worldwide, according to their website [12]. Jehovah's Witnesses are occasionally encountered in a cardiac surgical department. They may even be older and frailer than the standard population. The purpose of this retrospective observational study is to compare the clinical outcome of Jehovah's Witnesses who underwent cardiac surgery at our institution with those of non-Witnesses. Propensity score matching was required to adjust for differences in patient characteristics.
2. Patients and Methods
2.1. Study design
We retrospectively analyzed the medical records of all consecutive Jehovah's Witnesses who underwent major cardiac surgery at our institution between 2003 and 2022. The study was conducted as an observational all-comers study with no specific inclusion criteria and no specific protocols. Data were completely anonymized so that no written informed consent was required. The study was approved by our institutional ethics committee (No. E-01-20230411). Demographic characteristics, procedural data, and short-term postoperative outcomes were obtained from patient records.
2.2. Surgical management
In all elective patients, anticoagulants and antiplatelet agents, except for acetylsalicylic acid, were discontinued preoperatively in a timely manner and replaced with a bridging therapy as needed. Jehovah’s Witnesses received erythropoietin and/or iron preoperatively only in case of relevant anemia (i.e., hemoglobin <8 mmol/l, hematocrit <40%), although there was no specific protocol for this. In this case, epoetin alfa was administered 3 times per week at a dose of 50 IU/kg. In case of iron deficiency, EPO was accompanied by oral iron (Fe2+ 100-200 mg per day) until hemoglobin reached acceptable levels. This treatment was carried out after admission as an inpatient and surgery was postponed for 1-2 weeks. All other patients did not receive EPO.
Cardiac surgery was performed in a standard fashion in all patients. Only a few surgeons were involved who had the highest level of experience. Access was gained through a median sternotomy. Cardiopulmonary bypass was performed in all cases, with cannulation and temperature level as needed. We did not use a dedicated minimally invasive extracorporeal circuit. However, retrograde autologous priming and intraoperative ultrafiltration for hemoconcentration were routinely used in Jehovah’s Witnesses. No particular surgical strategy was applied to Jehovah’s Witnesses except for general blood-sparing techniques, including meticulous hemostasis and squeezing of all surgical swabs. Administration of blood derivatives such as clotting factors or local hemostatic agents as well as cell salvage were permitted in most cases. However, autologous blood collection (hypovolemic hemodilution) was generally not an option. In all cases, strategies strictly adhered to the individual patient’s written decision. Postoperative collection of blood samples was kept to a minimum.
2.3. Statistical Methods
Statistics were calculated using IBM SPSS 23 (IBM, Armonk, NY, USA) and R 4.2.2 (R Core Team 2022. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/).
Continuous values are given as mean ± SD, categorical values as percentages and their counts in round brackets. Tests for normal distribution were performed with SPSS. The Kolmogorov-Smirnov test is used for larger sample sizes (>50) but becomes significant for exceptionally large samples, which is true for our dataset. Visual evaluation of Q-Q plots was preferred here. The Shapiro-Wilk test is appropriate for smaller sample sizes and was therefore used for the matched dataset. Differences between means were tested using either Student’s independent t-test or Mann-Whitney’s U-Test, depending on normality. Categorical values were tested for differences using the Chi-square test. Paired values (before-after) were tested with the dependent t-test or Wilcoxon’s test, depending on normality. R was used with the “MatchIt”-Package for propensity score matching.
3. Results
There were 32 Jehovah’s Witnesses (JW) and 24,285 non-Witnesses (NW) until June 2022. The dataset was not only extremely unbalanced, but also highly disparate in terms of gender, weight, and BMI. In particular, the gender distribution in the small group of Jehovah’s Witnesses was almost even, while men predominated in the general cardiosurgical population. In addition, the JW patients were significantly less obese (Table 1).
To adjust for this difference, a two-step propensity score matching was performed. In the first step, a 3:1 matching by age, sex, BMI, urgency, and logistic EuroSCORE was performed because these values were consistently available since the past. Missing information such as EuroSCORE II, procedural times, laboratory results, and medical history were then recollected and added to the contracted dataset. In the second step, final 2:1 propensity score matching was performed according to age, gender, BMI, EuroSCORE II, repeat surgery, temperature, and duration of surgery. The matched dataset showed no more significant differences in body measurements, risk profiles, and spectrum of preexisting conditions (Table 2). The definitions of these conditions are either commonplace or based on those of EuroSCORE as follows:
Endocarditis is defined as active infective endocarditis (meeting Duke criteria) requiring surgery due to increased risk of embolism, heart failure, valve destruction, abscess formation, or persistent infection. Patients are treated with antibiotics at the time of surgery. Malignant disease is present when the patient has a malignant neoplasm that limits life expectancy. Arterial hypertension is defined according to the European Society of Cardiology, when blood pressure exceeds 140/90 mmHg at rest. Hyperlipidemia refers to increased levels of total cholesterol (>5.2 mmol/l), LDL cholesterol (>3 mmol/l), or triglycerides (>2.3 mmol/l). NIDDM and IDDM differ by current use of insulin at the time of admission. Stroke is defined as a preceding ischemic neurologic event with or without permanent deficits. Peripheral, cerebrovascular, or coronary artery disease follow the common definitions. The COPD definition is linked to the administration of steroids or bronchodilators. Atrial fibrillation is counted if this disorder is present in chronic intermittent or permanent form at the time of admission. Pacemaker carrier status applies to any pacemaker or ICD already in place prior to surgery, thus excluding the same patient from counting for postoperative pacemaker implantation.
Procedural data are shown in Table 3. EPO was administered to about one third of Jehovah’s Witnesses but not to other patients. Surgical procedures were evenly distributed among the groups. Due to many combined procedures, the proportion of surgical procedures (valves, CABG, aorta, arch, other) amount to more than 100% in both groups. Notably, there was a considerable proportion of ascending aorta and arch surgery in the JW group without reaching statistical significance. Data on blood loss were not available. Finally, there were no differences regarding lowest temperature, length of stay, or surgery-related times.
Table 4 shows the clinical short-term outcomes. Almost all postoperative conditions occurred at statistically equal rates, with the exception of pneumonia, which was clinically more common in Jehovah’s Witnesses. However, pre-discharge hemoglobin and hematocrit levels were significantly lower in the JW group. One in six Witnesses was treated with EPO during the postoperative course but none of the non-Witnesses. As Jehovah’s Witnesses did not receive any blood components, there was a strong statistical difference with the NW group in terms of administration of red blood cells and platelets. The only exception was one patient who revoked and allowed postoperative transfusion of 2 red cell concentrates in the face of severe anemia. Of note, there was no difference in-hospital mortality.
Figure 1 shows the changes of hemoglobin, creatinine, creatinine clearance, and LVEF grouped by Jehovah’s Witnesses and non-Witnesses. For both groups (JW, NW), the changes were significant for LVEF, hemoglobin, and hematocrit (not shown) but not significant for creatinine and its clearance.
4. Discussion
Our current study compared 32 consecutive Jehovah’s Witnesses who underwent cardiac surgery with a matched cohort of non-Witnesses. Although the sample size appears relatively small, it is consistent with similar group sizes in other published studies [9,13,14,15,16]. The small cohort was characterized by a nearly balanced gender ratio and a below-average weight and BMI. This was in contrast with the dominance of male gender and elevated BMI in the non-Witness cohort and thus required statistical matching. The reason for this is unclear. Jehovah's Witnesses have no specific dietary requirements. However, they practice a Bible-compliant lifestyle that avoids impure or unhealthy behavior. They do not eat foods containing blood, some are vegetarian, and alcohol is allowed only in moderation. Smoking and drug use are banned [6]. In this context, they presented with less hypertension, less smoking and fewer myocardial infarctions in their history, although this did not reach statistical significance in the matched cohort.
We demonstrated that Jehovah’s Witnesses had significantly lower postoperative hemoglobin and hematocrit levels due to their refusal of blood transfusions. The perioperative decrease in hemoglobin and hematocrit was more pronounced in Jehovah’s Witnesses. Accordingly, there was a significant statistical difference between the two groups in terms of transfusion rate. Instead, Jehovah’s Witnesses received erythropoietin postoperatively in case of unacceptable anemia. Although only a symptomatic treatment for anemia, the benefit for surgical patients is well known, and administration of EPO is recommended by the EACTS guidelines 2017 especially in the preoperative setting [17]. There are advanced protocols for treatment of anemic patients that show gradual improvement as early as 1 to 2 weeks after initiation [2,3,4,10,18,19,20]. This should not only apply to Jehovah's Witnesses, but should be practiced generally in all anemic patients [21]. A target hemoglobin of >12 g/dl by elective administration of erythropoietin or iron has been shown to improve both morbidity and mortality during cardiovascular surgery in JW patients [20].
Remarkably, the refusal of blood transfusion did not translate into a worse clinical outcome. This is consistent with a number of other studies [7,13,15,22,23,24]. In particular, our in-hospital mortality was not different between the two groups. There was also no difference regarding rethoracotomy or pericardiocentesis or in the other common endpoints such as atrial fibrillation, myocardial infarction, renal failure, septicemia, stroke, or delirium. The only detectable difference was a higher incidence of pneumonia and new pacemaker implantation in the JW group. As an exception to the rule, we had one JW patient who had allowed the transfusion of a red blood cell concentrate when he/she was not progressing in the healing process due to his/her poor general condition.
Other studies have also demonstrated that Jehovah’s Witnesses are not at higher risk for in-hospital adverse events or mortality, and do not show impaired long-term survival compared to non-Witnesses unless they are severely anemic (<8 g/dl) in the postoperative course [22]. In this case, mortality in the JW group reached up to 40%. We were unable to verify this in our patient cohort. Other groups reported in-hospital mortality as low as 2.9-5.0% in Jehovah’s Witnesses [9,13,15]. A pooled analysis has also found a 2.6% in-hospital mortality rate and a non-significant trend toward lower rates of stroke, myocardial infarction, atrial fibrillation, reoperation for bleeding, and shorter ICU stay [25]. In our cohort, we observed a slightly higher mortality rate in both groups compared to other studies. This may be related to the more complex and bleeding-prone procedures in our JW, in which replacement of the ascending aorta or aortic arch was involved in 21.9% of cases, endocarditis occurred in 12.5%, redo surgery in 6.7%, and logistic EuroSCORE was 10.18 ± 14.91%. In comparison, Müller et al. reported 5.8% aortic procedures, 2.9% endocarditis, and a logistic EuroSCORE of 6.93 ± 7.51% [13]. The pooled analysis by Vasques et al. reported only 3.2% other major procedures (non-CABG, non-valve) and no explicit endocarditis or redo cases [25]. In Marinakis’ study, the rate of aortic interventions was 6%, redo cases 10%, and no reported endocarditis [15]. Moreover, some past studies presented JW patients aged 62 to 64 years [14,15,16,25], while our Witnesses average 68.1 ± 9.4 years of age. Although not really geriatric patients, this may reflect an increasingly aging society. This does not stop at Jehovah's Witnesses. However, since the risk of surgery is directly related to age, the indication for bloodless surgery must be even more narrowly defined.
Furthermore, long-term survival is not different from that of the standard patient population. Wauthy et al. demonstrated a median survival after cardiac surgery of 21.1 years in Jehovah’s Witnesses and 20.3 years in the control group (p=0.37) [14]. Quality of life is also unaffected based on questionnaires in terms of physical, emotional, social, and global scores, as shown by the same Belgian research group [14]. However, we did not assess long-term outcomes in our patients.
Our pre-treatment with EPO was similar to other groups and included only one third of all patients presenting with unacceptable hemoglobin levels. We were aware that such treatment would be costly and time-consuming while many patients were considered urgent. For the same reason, there was no outpatient treatment with EPO. Similarly, Müller et al. reported a rate of 34.3% of EPO administration in a group of 35 JW, resulting in an average hemoglobin increase of 2.0 g/dl [13]. Their patients presented with hemoglobin levels similar to ours on admission (JW, 14.1 ± 1.1 compared to 13.0 ± 1.6 g/dl; non-Witnesses, 13.2 ± 2.0 compared to 13.2 ± 1.7 g/dl). However, their Witnesses had significantly higher postoperative hemoglobin than the non-Witnesses (11.5 ± 1.5 vs. 10.3 ± 1.3 g/dl, p<0.001), even though the latter were transfused. The authors explained this by the high efficacy of multimodal blood preservation strategies. Higher postoperative Hb levels in Jehovah’s Witnesses were also demonstrated in a meta-analysis (11.5 g/dl vs. 9.8 g/dl, p<0.001) [25] and in a large Australian database (10.8 ± 1.5 vs. 9.9 ± 1.2 g/dl, p=0.003) [26]. Other studies showed no postoperative Hb differences between groups (10.7 ± 2.5 vs. 11.4 ± 1.8 g/dl) [15]. However, this could not be confirmed in our study, in which JW patients showed markedly lower postoperative hemoglobin (9.8 ± 1.6 vs. 11.1 ± 1.4 g/dl, p<0.001). We treated only one-sixth of all JW who had severe postoperative anemia and were in poor condition, while most of them could be discharged in time. Our study truly reflects our daily practice in the real world, without strict application of defined optimization protocols.
Transfusions are generally known to have adverse effects in cardiac surgery patients [21]. Patients with advanced age, high EuroSCORE, low preoperative hemoglobin, combined surgery, and prolonged operations are associated with higher transfusion rates. These patients have more than three times the risk of early mortality [27]. Octogenarians are at particular risk after cardiac surgery. Transfusion of more than 2 units of red blood cells significantly increases their postoperative mortality. It also significantly prolongs their stay in the intensive care unit and hospital [28]. In addition, red blood cell transfusion increases the risk of infection [29] and stroke [30] after cardiac surgery. Platelet transfusion, in contrast, has not been identified as a risk factor for morbidity in such patients [31]. For the above reasons, a blood-sparing strategy and avoidance of transfusion seem generally advisable for all cardiac surgery patients. Given the scarcity of blood supplies and the high price of blood products, cost considerations also support this approach [32]. Implementation of a dedicated blood management program not only results in reduced blood product use and cost savings, but even improves patient outcomes [33]. A restrictive transfusion strategy has been found to be non-inferior to a liberal strategy in terms of morbidity and mortality in intermediate- to high-risk cardiac surgery patients [34]. Some authors have raised the question why this should only apply to Jehovah's Witnesses and not to all patients [16]. A useful summary of alternatives to transfusion is provided in [7] or [10]. There are also powerful tools for postoperative coagulation management such as ROTEM [16]. As a future perspective, there are new developments in the field of synthetic blood alternatives and hemoglobin-based oxygen carriers to overcome the religious problem of conventional blood transfusion [35]. Last but not least, the principle of medical action "Primum non nocere, secundum cavere, tertium sanare" should apply to all patients without exception.
Limitations
The present work has the known limitations of a multicenter retrospective study. The group size is relatively small given the sporadic occurrence of such patients. Moreover, selection bias may have occurred as the subgroup of Jehovah’s Witnesses was treated by the most experienced surgeons and likely received more attention in terms of blood-sparing strategies, anemia management, optimized coagulation treatment, and expedited surgery. This fact has also been recognized by other authors [16].
5. Conclusions
Our real-world data indicate that Jehovah's Witnesses can safely undergo bloodless surgery without compromising clinical outcome. The reduced hemoglobin level was mostly well tolerated without affecting morbidity and mortality. This is consistent with other studies. Given the limited number of patients available worldwide, we believe that our data contribute to the existing evidence. Based on our experience, it is important to respect the patient's wishes, discuss blood-sparing strategies on an individual basis, present alternatives, and involve the family in the process. Three final considerations are right on the table: given the identical outcomes in both groups, why do the non-JW patients receive blood products at all? And second, if non-transfusion does create additional risk, is it outweighed by the surgeon's experience? In the end, does this even mean that all procedures should be performed on every patient without blood and with experienced surgeons only? Certainly a controversial question.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table xx: Raw Data.
Author Contributions
Conceptualization, M.H. and J.M.A.; Data curation, M.H. and F.S., Formal Analysis, M.H. and F.S., Investigation, M.H., R.U.K. and R.O.; Methodology, J.M.A.; Supervision, J.M.A.; Validation, F.S.; Visualization, M.H.; Writing - original draft, M.H.; Writing - review & editing, R.U.K., R.O. and J.M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of Brandenburg Medical School (Theodor Fontane) under No. E-01-20230411.
Informed Consent Statement
Patient consent was waived due to the retrospective and fully anonymized nature of the study
Data Availability Statement
The data underlying this article are available in the article and in its online Supplementary Materials.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jehovah’s Witnesses. Why Don't Jehovah's Witnesses Accept Blood Transfusions? Available online:. Available online: https://www.jw.org/en/jehovahs-witnesses/faq/jehovahs-witnesses-why-no-blood-transfusions/ (accessed on 29 December 2022).
- Chae, C.; Okocha, O.; Sweitzer, B. Preoperative considerations for Jehovah's Witness patients: a clinical guide. Curr Opin Anaesthesiol 2020, 33, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Scharman, C.D.; Burger, D.; Shatzel, J.J.; Kim, E.; DeLoughery, T.G. Treatment of individuals who cannot receive blood products for religious or other reasons. Am J Hematol 2017, 92, 1370–1381. [Google Scholar] [CrossRef] [PubMed]
- Lawson, T.; Ralph, C. Perioperative Jehovah's Witnesses: a review. Br J Anaesth 2015, 115, 676–687. [Google Scholar] [CrossRef]
- Remmers, P.A.; Speer, A.J. Clinical strategies in the medical care of Jehovah's Witnesses. Am J Med 2006, 119, 1013–1018. [Google Scholar] [CrossRef]
- Pavlikova, B.; van Dijk, J.P. Jehovah's Witnesses and Their Compliance with Regulations on Smoking and Blood Treatment. Int J Environ Res Public Health 2021, 19. [Google Scholar] [CrossRef] [PubMed]
- Chambault, A.L.; Brown, L.J.; Mellor, S.; Harky, A. Outcomes of cardiac surgery in Jehovah's Witness patients: A review. Perfusion 2021, 36, 661–671. [Google Scholar] [CrossRef]
- Wade, P. Treating Jehovah's Witnesses. Br J Perioper Nurs 2004, 14, 254–257. [Google Scholar] [CrossRef]
- Moraca, R.J.; Wanamaker, K.M.; Bailey, S.H.; McGregor, W.E.; Benckart, D.H.; Maher, T.D.; Magovern, G.J., Jr. Strategies and outcomes of cardiac surgery in Jehovah's Witnesses. J Card Surg 2011, 26, 135–143. [Google Scholar] [CrossRef]
- Crowe, E.P.; DeSimone, R.A. Transfusion support and alternatives for Jehovah's Witness patients. Curr Opin Hematol 2019, 26, 473–479. [Google Scholar] [CrossRef]
- Düsseldorf, K.E.d.U. Handlungsempfehlungen für die Behandlung von Zeugen Jehovas bei Bluttransfusionen. Available online: https://www.uniklinik-duesseldorf.de/fileadmin/Ausbildung_und_Karriere/KEK/Handlungsempfehlungen_fuer_den_Umgang_mit_Jehovas_Zeugen_Patienten_bei_geplanter_oder_unvorhergesehener_Bluttransfusion.pdf (accessed on 29 December 2022).
- Jehovah’s Witnesses. How Many of Jehovah’s Witnesses Are There Worldwide? Available online:. Available online: https://www.jw.org/en/jehovahs-witnesses/faq/how-many-jw/ (accessed on 3 February 2023).
- Müller, H.; Ratschiller, T.; Schimetta, W.; Meier, J.; Gombotz, H.; Zierer, A. Open Heart Surgery in Jehovah's Witnesses: A Propensity Score Analysis. Ann Thorac Surg 2020, 109, 526–533. [Google Scholar] [CrossRef]
- Wauthy, P.; Pierrakos, C.; Chebli, L.; Tortora, R. Long-term survival and quality of life in Jehovah's witnesses after cardiac surgery: a case control study. BMC Cardiovasc Disord 2019, 19, 73. [Google Scholar] [CrossRef] [PubMed]
- Marinakis, S.; Van der Linden, P.; Tortora, R.; Massaut, J.; Pierrakos, C.; Wauthy, P. Outcomes from cardiac surgery in Jehovah's witness patients: experience over twenty-one years. J Cardiothorac Surg 2016, 11, 67. [Google Scholar] [CrossRef] [PubMed]
- Emmert, M.Y.; Salzberg, S.P.; Theusinger, O.M.; Felix, C.; Plass, A.; Hoerstrup, S.P.; Falk, V.; Gruenenfelder, J. How good patient blood management leads to excellent outcomes in Jehovah's witness patients undergoing cardiac surgery. Interact Cardiovasc Thorac Surg 2011, 12, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Boer, C.; Meesters, M.I.; Milojevic, M.; Benedetto, U.; Bolliger, D.; von Heymann, C.; Jeppsson, A.; Koster, A.; Osnabrugge, R.L.; Ranucci, M.; et al. 2017 EACTS/EACTA Guidelines on patient blood management for adult cardiac surgery. J Cardiothorac Vasc Anesth 2018, 32, 88–120. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Lee, M.; Kang, Y.; Cho, S.H. Patient blood management when blood is not an option: a report of two cases. Ann Palliat Med 2022, 11, 2768–2772. [Google Scholar] [CrossRef]
- Shander, A.; Goodnough, L.T. Management of anemia in patients who decline blood transfusion. Am J Hematol 2018, 93, 1183–1191. [Google Scholar] [CrossRef]
- Tanaka, A.; Ota, T.; Uriel, N.; Asfaw, Z.; Onsager, D.; Lonchyna, V.A.; Jeevanandam, V. Cardiovascular surgery in Jehovah's Witness patients: The role of preoperative optimization. J Thorac Cardiovasc Surg 2015, 150, 976–983.e971-973. [Google Scholar] [CrossRef]
- Dhir, A.; Tempe, D.K. Anemia and Patient Blood Management in Cardiac Surgery-Literature Review and Current Evidence. J Cardiothorac Vasc Anesth 2018, 32, 2726–2742. [Google Scholar] [CrossRef]
- Nanni, G.; Vitolo, M.; Imberti, J.F.; Girolami, D.; Bonini, N.; Valenti, A.C.; Cimato, P.; Boriani, G. Short and long-term outcomes after cardiac surgery in Jehovah's Witnesses patients: a case-control study. Intern Emerg Med 2022. [CrossRef]
- Jassar, A.S.; Ford, P.A.; Haber, H.L.; Isidro, A.; Swain, J.D.; Bavaria, J.E.; Bridges, C.R. Cardiac surgery in Jehovah's Witness patients: ten-year experience. Ann Thorac Surg 2012, 93, 19–25. [Google Scholar] [CrossRef]
- Stamou, S.C.; White, T.; Barnett, S.; Boyce, S.W.; Corso, P.J.; Lefrak, E.A. Comparisons of cardiac surgery outcomes in Jehovah's versus Non-Jehovah's Witnesses. Am J Cardiol 2006, 98, 1223–1225. [Google Scholar] [CrossRef]
- Vasques, F.; Kinnunen, E.M.; Pol, M.; Mariscalco, G.; Onorati, F.; Biancari, F. Outcome of Jehovah's Witnesses after adult cardiac surgery: systematic review and meta-analysis of comparative studies. Transfusion 2016, 56, 2146–2153. [Google Scholar] [CrossRef]
- Bhaskar, B.; Jack, R.K.; Mullany, D.; Fraser, J. Comparison of outcome in Jehovah's Witness patients in cardiac surgery: an Australian experience. Heart Lung Circ 2010, 19, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Vlot, E.A.; Verwijmeren, L.; van de Garde, E.M.W.; Kloppenburg, G.T.L.; van Dongen, E.P.A.; Noordzij, P.G. Intra-operative red blood cell transfusion and mortality after cardiac surgery. BMC Anesthesiol 2019, 19, 65. [Google Scholar] [CrossRef]
- Veenith, T.; Sharples, L.; Gerrard, C.; Valchanov, K.; Vuylsteke, A. Survival and length of stay following blood transfusion in octogenarians following cardiac surgery. Anaesthesia 2010, 65, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Horvath, K.A.; Acker, M.A.; Chang, H.; Bagiella, E.; Smith, P.K.; Iribarne, A.; Kron, I.L.; Lackner, P.; Argenziano, M.; Ascheim, D.D.; et al. Blood transfusion and infection after cardiac surgery. Ann Thorac Surg 2013, 95, 2194–2201. [Google Scholar] [CrossRef]
- Bahrainwala, Z.S.; Grega, M.A.; Hogue, C.W.; Baumgartner, W.A.; Selnes, O.A.; McKhann, G.M.; Gottesman, R.F. Intraoperative hemoglobin levels and transfusion independently predict stroke after cardiac operations. Ann Thorac Surg 2011, 91, 1113–1118. [Google Scholar] [CrossRef]
- McGrath, T.; Koch, C.G.; Xu, M.; Li, L.; Mihaljevic, T.; Figueroa, P.; Blackstone, E.H. Platelet transfusion in cardiac surgery does not confer increased risk for adverse morbid outcomes. Ann Thorac Surg 2008, 86, 543–553. [Google Scholar] [CrossRef]
- Frank, S.M.; Sikorski, R.A.; Konig, G.; Tsilimigras, D.I.; Hartmann, J.; Popovsky, M.A.; Pawlik, T.M.; Waters, J.H. Clinical Utility of Autologous Salvaged Blood: a Review. J Gastrointest Surg 2020, 24, 464–472. [Google Scholar] [CrossRef]
- Leahy, M.F.; Hofmann, A.; Towler, S.; Trentino, K.M.; Burrows, S.A.; Swain, S.G.; Hamdorf, J.; Gallagher, T.; Koay, A.; Geelhoed, G.C.; et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: a retrospective observational study in four major adult tertiary-care hospitals. Transfusion 2017, 57, 1347–1358. [Google Scholar] [CrossRef]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Médicis, É.; McGuinness, S.; et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery. N Engl J Med 2017, 377, 2133–2144. [Google Scholar] [CrossRef] [PubMed]
- Rashid, M.; Kromah, F.; Cooper, C. Blood transfusion and alternatives in Jehovah's Witness patients. Curr Opin Anaesthesiol 2021, 34, 125–130. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Perioperative changes of mean levels according to patient groups. Blue, Jehovah’s Witnesses (JW); Red, non-Witnesses (NW). Upper left, hemoglobin (Hb) [mmol/l]; Upper right, creatinine [µmol/l]; Lower left, creatinine clearance [ml/min]; Lower right, LVEF [%]. The corresponding p-values of the paired changes are also shown. The changes are significant for hemoglobin, hematocrit (not shown) and LVEF, but not for creatinine and its clearance.
Figure 1.
Perioperative changes of mean levels according to patient groups. Blue, Jehovah’s Witnesses (JW); Red, non-Witnesses (NW). Upper left, hemoglobin (Hb) [mmol/l]; Upper right, creatinine [µmol/l]; Lower left, creatinine clearance [ml/min]; Lower right, LVEF [%]. The corresponding p-values of the paired changes are also shown. The changes are significant for hemoglobin, hematocrit (not shown) and LVEF, but not for creatinine and its clearance.
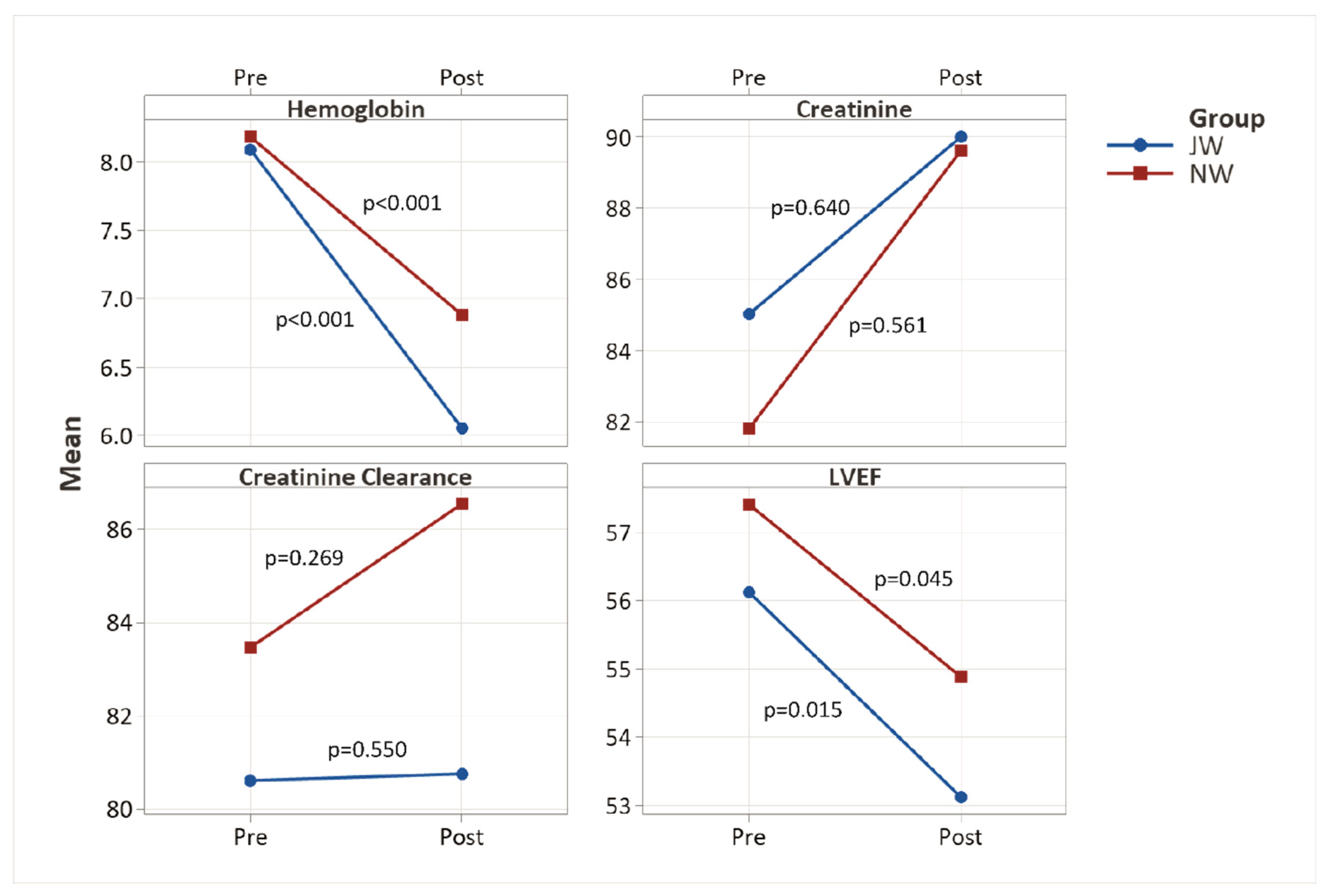

Table 1.
Unmatched preoperative data (raw data).
| JW n=32 |
NW n>20,000 |
p Value | ||
|---|---|---|---|---|
| Age | years | 68.1 ± 9.4 | 67.6 ± 10.0 | 0.786 |
| Gender | male | 53.1% (17) | 72.4% (17571) | 0.015 |
| Height | cm | 169 ± 9 | 171 ± 9 | 0.200 |
| Weight | kg | 76 ± 14 | 83 ± 16 | 0.011 |
| BMI | kg/m2 | 26.43 ± 4.73 | 28.50 ± 4.82 | 0.005 |
| BSA | m2 | 1.88 ± 0.21 | 1.81 ± 0.59 | 0.510 |
| log ES | % | 10.25 ± 14.89 | 10.50 ± 14.79 | 0.293 |
| Emergency | 9.4% (3) | 9.2% (2236) | 0.976 | |
| Redo | 6.7% (2) | 4.4% (1072) | 0.549 |
JW=Jehovah’s Witnesses, NW=non-Witnesses. Continuous values are shown as mean ± SD, categorical values as percentages and count. P values below 0.05 were considered significant. BMI, body mass index; BSA, body surface area; log ES, logistic EuroSCORE.
Table 2.
Patient characteristics (propensity score matched dataset).
| JW n=32 |
NW n=64 |
p Value | ||
|---|---|---|---|---|
| Age | years | 68.1 ± 9.4 | 67.4 ± 9.6 | 0.735 |
| Gender | male | 53.1% (17) | 57.8% (37) | 0.663 |
| Height | cm | 168 ± 9 | 168 ± 12 | 0.995 |
| Weight | kg | 76 ± 14 | 77 ± 15 | 0.772 |
| BMI | kg/m2 | 26.84 ± 4.79 | 27.16 ± 4.59 | 0.746 |
| BSA | m2 | 1.86 ± 0.19 | 1.87 ± 0.23 | 0.811 |
| log ES | % | 10.18 ± 14.91 | 8.07 ± 10.92 | 0.214 |
| ES II | % | 7.59 ± 15.97 | 5.30 ± 11.24 | 0.087 |
| LVEF preop | % | 56 ± 11 | 57 ± 11 | 0.749 |
| Emergency | 9.4% (3) | 6.3% (4) | 0.579 | |
| Redo surgery | 6.3% (2) | 7.8% (5) | 0.781 | |
| Hemoglobin | mmol/l | 8.09 ± 0.99 | 8.18 ± 1.06 | 0.683 |
| g/dl | 13.04 ± 1.60 | 13.18 ± 1.71 | ||
| Hematocrit | 0.39 ± 0.05 | 0.39 ± 0.05 | 0.645 | |
| Creatinine | µmol/l | 85.0 ± 21.6 | 81.8 ± 18.6 | 0.452 |
| Crea Clearance | ml/min | 80.6 ± 39.7 | 83.5 ± 31.9 | 0.499 |
| Endocarditis | 12.5% (4) | 3.1% (2) | 0.074 | |
| Malignant disease | 3.1% (1) | 4.7% (3) | 0.718 | |
| Arterial hypertension | 59.4% (19) | 78.1% (50) | 0.054 | |
| Hyperlipidemia | 50.0% (16) | 46.9% (30) | 0.773 | |
| Smoking history | 3.1% (1) | 14.1% (9) | 0.098 | |
| NIDDM | 12.5% (4) | 25.0% (16) | 0.155 | |
| IDDM | 9.4% (3) | 9.4% (6) | 1.000 | |
| Stroke | 3.1% (1) | 1.6% (1) | 0.613 | |
| PVD | 6.3% (2) | 10.9% (7) | 0.458 | |
| CVD | 3.1% (1) | 3.1% (2) | 1.000 | |
| Myocardial infarction | 9.4% (3) | 25.0% (16) | 0.070 | |
| COPD | 9.4% (3) | 9.4% (6) | 1.000 | |
| Atrial fibrillation | 25.0% (8) | 10.9% (7) | 0.074 | |
| Pacemaker | 3.1% (1) | 6.3% (4) | 0.516 |
JW=Jehovah’s Witnesses, NW=non-Witnesses. Continuous values are shown as mean ± SD, categorical values as percentages and count. P values below 0.05 were considered significant. BMI, body mass index; BSA, body surface area; COPD, chronic obstructive pulmonary disease; CVD, cerebrovascular disease; ES II, EuroSCORE II; log ES, logistic EuroSCORE; LVEF, left ventricular ejection fraction; PVD, peripheral vascular disease.
Table 3.
Perioperative data (propensity score matched dataset).
| JW n=32 |
NW n=64 |
p Value | ||
|---|---|---|---|---|
| Preoperative EPO | 34.4% (11) | 0.0% (0) | 0.006 | |
| Valve surgery | 56.3% (18) | 48.4% (31) | 0.470 | |
| CABG | 56.3% (18) | 67.2% (43) | 0.294 | |
| Ascending aorta | 15.6% (5) | 4.7% (3) | 0.068 | |
| Aortic arch | 6.3% (2) | 1.6% (1) | 0.213 | |
| Other cardiac procedures | 9.4% (3) | 10.9% (7) | 0.813 | |
| Temperature | °C | 34.1 ± 3.3 | 34.3 ± 3.0 | 0.444 |
| Duration of surgery | min | 226 ± 74 | 227 ± 88 | 0.661 |
| ECC time | min | 132 ± 64 | 124 ± 60 | 0.341 |
| Clamp time | min | 81 ± 40 | 73 ± 32 | 0.159 |
| Total length of stay | hours | 20.8 ± 10.1 | 18.4 ± 8.2 | 0.343 |
| ICU length of stay | hours | 4.0 ± 6.5 | 3.0 ± 6.5 | 0.252 |
| Postop length of stay | hours | 16.4 ± 8.4 | 14.7 ± 7.5 | 0.351 |
JW=Jehovah’s Witnesses, NW=non-Witnesses. Continuous values are shown as mean ± SD, categorical values as percentages and count. P values below 0.05 were considered significant. CABG, coronary artery bypass grafting; ECC, extracorporeal circulation; EPO, erythropoietin; ICU, intensive care unit.
Table 4.
Postoperative data (propensity score matched dataset).
| JW n=32 |
NW n=64 |
p Value | ||
|---|---|---|---|---|
| LVEF postop | % | 53 ± 11 | 55 ± 11 | 0.521 |
| Hemoglobin | mmol/l | 6.05 ± 1.00 | 6.88 ± 0.87 | <0.001 |
| g/dl | 9.75 ± 1.61 | 11.09 ± 1.40 | ||
| Hematocrit | 0.29 ± 0.04 | 0.33 ± 0.04 | <0.001 | |
| Creatinine | µmol/l | 90.0 ± 41.3 | 89.6 ± 70.7 | 0.614 |
| Crea Clearance | ml/min | 80.8 ± 34.6 | 86.5 ± 38.2 | 0.603 |
| Red blood cell administration | units | 0.1 ± 0.7 | 2.5 ± 3.1 | <0.001 |
| Platelet administration | units | 0.0 ± 0.0 | 0.3 ± 0.8 | 0.018 |
| Postoperative EPO | 15.6% (5) | 0.0% (0) | 0.001 | |
| Rethoracotomy (bleeding, tamponade) | 6.3% (2) | 6.3% (4) | 1.000 | |
| Pericardiocentesis | 6.3% (2) | 1.6% (1) | 0.213 | |
| New onset atrial fibrillation | 12.5% (4) | 21.9% (14) | 0.267 | |
| New pacemaker | 6.3% (2) | 0.0% (0) | 0.043 | |
| Myocardial infarction | 0.0% (0) | 1.6% (1) | 0.477 | |
| Wound healing disorders | 6.3% (2) | 7.8% (5) | 0.781 | |
| New onset dialysis | 9.4% (3) | 3.1% (2) | 0.194 | |
| Pneumonia | 6.3% (2) | 0.0% (0) | 0.043 | |
| Tracheostomy | 6.3% (2) | 3.1% (2) | 0.470 | |
| Septicemia | 0.0% (0) | 3.1% (2) | 0.312 | |
| Stroke | 0.0% (0) | 1.6% (1) | 0.477 | |
| Delirium | 18.8% (6) | 20.3% (13) | 0.856 | |
| Early Mortality | 6.3% (2) | 4.7% (3) | 0.745 |
JW=Jehovah’s Witnesses, NW=non-Witnesses. Continuous values are shown as mean ± SD, categorical values as percentages and count. P values below 0.05 were considered significant. EPO, erythropoietin; LVEF, left ventricular ejection fraction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



