
Submitted:
05 July 2023
Posted:
06 July 2023
You are already at the latest version
Abstract
We aimed to assess the prognostic value of BRAFV600E mutation in a series of 127 papillary thyroid carcinoma (PTC) cases as a single factor, as well as in synergic interaction with other standard risk factors. All cases were tested for BRAFV600E mutation by real-time PCR. Event-free survival (EFS) was calculated between the date of the first evaluation and the date of occurrence of an adverse event (tumor recurrence/distant metastasis) or the date of the last known status. The prevalence of BRAFV600E mutation was 57.2%. The Kaplan-Meyer analysis showed a significant reduction of EFS among cases harboring BRAFV600E mutation compared to non-mutated cases (p=0.010). In addition, BRAFV600E mutation was found to better predict adverse outcomes when associated with the following risk factors: age≥55 years-old (p<0.001), male gender (p<0.001), conventional (p=0.005) and tall cell (p=0.014) histology, tumor size>40mm (p=0.001), extrathyroidal extension (p=0.001), multifocality (p=0.001) and lymph node metastasis (p<0.001). In univariate analysis, a 3.74-fold increased risk for a reduced EFS (p=0.018) was found for BRAFV600E mutated cases. Our results highlight the prognostic value of BRAFV600E mutation in PTCs. Moreover, the synergic interaction between BRAFV600E mutation and other risk factors seems more valuable in terms of prognosis, compared to BRAFV600E mutation alone.
Keywords:
papillary thyroid cancer
; BRAFV600E mutation
; lymph node metastasis
; prognosis
; outcomes.
1. Introduction
Papillary thyroid carcinoma (PTC) is the most common endocrine malignancy, accounting for 80% of all thyroid cancers [1]. Worldwide, the incidence of PTC has significantly increased over the last 30 years [2,3], yet with no increase in the mortality rate [4].
Although PTC is generally a highly curable disease, there is a small subgroup of PTC cases that tend to behave aggressively, with high rates of disease recurrence, tumor progression or even distant metastases leading to poor prognosis [5,6]. These patients need to be accurately identified for an appropriate, more-aggressive therapeutical approach to reduce the chance of disease recurrence and worse outcomes. Moreover, patient’s quality of life is of paramount importance, so it is important to aggressively treat an aggressive cancer, but also to take off the physiological burden of an indolent one [5].
In recent years, the development of targeted therapies has led to increased interest in the identification of molecular alterations present in thyroid cancer and their prognostic impact [7]. BRAFV600E mutation has received the widest attention, being by far the most prevalent genetic event in patients with PTC, with a reported prevalence of 25-82.3% [8]. BRAFV600E mutation is caused by a thymine to adenine transversion at nucleotide 1799 (T1799A) [9], leading to a substitution of Valine by Glutamic acid at residue 600 of the protein (V600E). A result of the genetic alteration is the activation of the mitogen-activated protein kinase (MAPK) signaling pathway [10], which plays a major role in the regulation of cell growth, division, and proliferation [11]. Many studies have demonstrated an association of BRAFV600E mutation with aggressive clinicopathologic characteristics of PTC, showing promise of this mutation as a prognostic molecular marker for PTC [8,12,13,14,15,16]. Nevertheless, literature data is controversial and the prognostic value of BRAFV600E mutation has been questioned, other studies failing to demonstrate that BRAFV600E is an independent prognostic factor for PTC [17,18]. Moreover, in PTC patients the frequency of BRAFV600E mutation is high (up to 80%) [8], while the prevalence of negative outcome is low (10-15%) [17,18]. Therefore, based only on the analysis of BRAFV600E mutation, a considerable number of PTC patients would face the risk of over- or undertreatment [6]. Thus, BRAFV600E mutation should be considered one of the factors influencing the prognosis of PTC patients, but it should be evaluated together with other prognostic factors [6]. In the study performed by Gan X. et al. [19] BRAFV600E mutation was found to better predict aggressive and recurrent PTC based on age stratification with the cut-off age of 55 years-old. The authors concluded that synergic interaction between BRAFV600E mutation and age stratification may help clinicians in terms of optimal decision-making regarding surgical approach and extent of surgery.
In the present study we first evaluated the relationship between BRAFV600E mutational status and demographic, pathological and outcome characteristics of PTC patients in a series of 127 cases. Further on, we aimed to assess the prognostic value of BRAFV600E mutation in our series of PTC cases, as a single factor, as well as in synergic interaction with other standard demographic and pathological risk factors.
2. Materials and Methods
2.1. Case selection
All consecutive PTC cases registered at the Pathology Department, Târgu-Mureş Emergency Hospital, Romania, between 2008-2015 were evaluated. Criteria for inclusion in the study were: (1) a histopathological diagnosis consistent with PTC; (2) tumor size of at least 10 mm; (3) availability of hematoxylin/eosin (HE)-stained slides for case review; (4) well-preserved formalin-fixed paraffin-embedded (FFPE) tumor blocks of the corresponding cases available in the archive for molecular assay; and (5) available follow-up data.
2.2. Pathological data
The corresponding HE-stained slides for all the cases included in the study were reviewed by two endocrine pathologists (ANB and AB). Tumor histology and pathological stage were reassessed according to the 2017 WHO (World Health Organization) Classifications of Tumors of the Thyroid Gland [20] (p 81-91) and the 2017 American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) TNM Classification of Tumors [21] (p 87-96). All cases with controversial features were discussed and a consensus was reached using a multi-headed microscope.
The diagnosis of PTC was based on nuclear features (enlargement, overlapping, irregularity of the nuclear contours, grooves, clearing or ground glass appearance, nuclear pseudoinclusions) and evidence of either papillary architecture or follicular pattern with invasive characteristics.
The following demographic and pathological features with prognostic significance were evaluated: (1) patients’ age at diagnosis with cut-off values of 55 years-old; (2) patients’ gender; (3) tumor size and (4) histological type (conventional, or variant of PTC such as follicular, tall-cell, Warthin-like, oncocytic or solid); (5) extrathyroidal extension defined as tumor extension into strap muscles (sternohyoid, sternothyroid or omohyoid muscles); (6) multifocality defined as the presence of two or more isolated/non-contiguous tumor foci in one or both thyroid lobes; (7) lymph node metastasis defined as involvement of at least one regional lymph node; (8) surgical resection margins status; (9) vascular invasion and (10) stage grouping.
2.3. Molecular analysis
For each case, one representative FFPE block was selected for the molecular assay. The selected FFPE block corresponded to well-preserved, high-density tumor areas, with absence of hemorrhage and calcifications. The area of interest (the tumor area) was circled on the HE stained slides. Using the HE stained slide as a guide and a standard microscope, a manual microdissection of the marked area was performed. DNA isolation was accomplished using MasterPureTM DNA purification kit (Epicentre, Madison), as previously described [22]. All real-time PCR experiments were performed at the Platform of Molecular Biology, Center for Advanced Medical and Pharmaceutical Research, George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu-Mureș, using a 7500 Fast Dx RT-PCR Instrument (Applied Biosystems, USA). The Thyroid Cancer Mutation Analysis Kit (EntroGen, USA) was used for the detection of the somatic BRAFV600E mutation.
2.4. Follow-up data
Follow-up was defined as the period between the initial surgical treatment and the last clinical evaluation and covered the period between January 2001 and December 2017. Follow-up data were collected from the Department of Nuclear Medicine, “Ion Chiricuţă” Institute of Oncology, Cluj-Napoca, Romania, where all patients surgically treated in our hospital (Târgu-Mureş Emergency County Hospital) were further referred to for adjuvant treatment (131I ablation) and follow-up.
Disease status was set in accordance with the 2015 American Thyroid Association (ATA) risk of recurrence stratification system [23], based on the data available from the last clinical evaluation. A disease-free status was defined as the absence of detectable residual disease (on ultrasound and whole-body scans (WBS)) and low basal (<0.2 ng/mL) and stimulated (<1 ng/mL) thyroglobulin (Tg) serum levels. Persistent disease was defined as the presence of a detectable residual or metastatic tumor (on ultrasound, WBS, CT (Computed Tomography) and 18FDG-PET-CT (Positron Emission Tomography with 2-deoxy-2-[fluorine-18] fluoro-D-glucose integrated with Computed Tomography)) and/or elevated basal (>0.2 ng/mL) and stimulated (>1 ng/mL) Tg serum levels. Recurrent disease, on the other hand, was considered as the appearance of a new biochemical disease or tumor recurrence in patients previously classified as disease free. Distant metastases were defined as secondary, metastatic tumors identified at the time of diagnosis or during the follow-up period.
2.5. Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS, version 20, Chicago, IL, USA). Data were labeled as nominal or quantitative variables. Nominal variables were expressed as number and percentages and were compared using the chi-squared test or Fisher’s exact test (when the conditions of application of chi-square test were not met).
Quantitative variables were tested for normality of distribution using the Kolmogorov-Smirnov test, graphically confirmed with a histogram, and were described by mean ± standard deviation or median and percentiles (25; 75%), whenever appropriate. The student’s t test was applied to compare continuous values with Gaussian distribution.
Survival curves were obtained using a Kaplan-Meyer model and compared using the long-rank test. Persistent disease, recurrent disease, or distant metastases occurring during the follow-up period were considered as adverse events. Event-free survival (EFS) was calculated between the date of the first evaluation and the date of occurrence of an adverse event or the date of the last known status.
Prognostic factors of adverse events were determined using a Cox model after assessment of the proportionality of risk hypothesis, first in univariate analysis, and if appropriate in multivariate analysis, including factors found significant in univariate analysis.
All p-values were two-sided, and a p<0.05 was considered to indicate statistically significant differences.
3. Results
3.1. Patient’s characteristics
Our study included 127 patients (110 females and 17 males; mean ±standard deviation [SD] age 48.6 ± 1.28 years). Demographic, pathological and follow-up data for the study cases are illustrated in Table 1.
More than half of the patients included in the study were younger than 55 years-old (n=79, 62.2%); the mean tumor size was 22.88 ±1.5 mm. Most of the cases were conventional PTCs (n=88, 69.3%), while PTC variants were less numerous (tall cell n=9, 7.1%; Warthin-like n=7, 5.5%; oncocytic n=3, 2.4%; solid n=2, 1.6%; follicular, infiltrative n=13, 10.2%; follicular, encapsulated, invasive n=5, 3.9%). Extrathyroidal extension was documented in 18.9% (n=24) cases; 40.2% (n=51) PTCs were multifocal. Lymph node dissection was performed in 39 (30.7%) PTCs. Of these, 26 cases displayed lymph node involvement. With regard to the primary tumor (T), 51 (40.2%), 44 (34.6%), 8 (6.3%) and 24 (18.9%) PTCs were pT1b, pT2, pT3a and pT3b, respectively. Most of the cases included in the study were stage I PTCs (79.5%, n=101).
The mean follow-up period was 57 months (CI: 9-130). All patients were treated with total thyroidectomy or total thyroidectomy with lymph node dissection, and all received radioactive iodine (I131) therapy. At the last clinical assessment, most of the patients had a disease-free status (84.3%, n=107). A persistent disease status was observed only in 14 (11%) patients; recurrence was also rare, found in only 6 (4.7%) PTC cases. Four patients with conventional PTCs and 1 with tall cell variant of PTC developed distant metastases during the follow-up period (all in the lung, and one case also in the bone).
3.2. Prevalence of BRAFV600E mutation and relationship with demographic, pathological and outcomes characteristics
The prevalence of BRAFV600E mutation in our study was 57.2% (67/127). The demographic, pathological and outcomes characteristics of the study cases were compared between PTCs harboring BRAFV600E mutation and those without (Table 1). Our data showed that BRAFV600E mutation was strongly associated with age ≥55 years-old (p=0.037), male gender (p=0.035), conventional histology (p<0.0005), extrathyroidal extension (p=0.004), pT3b tumor stage (p=0.007), lymph node metastasis (p=0.001) and positive surgical resection margins. With regard to patient’s outcomes, although most of the patients included in our study revealed a disease-free status at the last clinical assessment, patients without BRAFV600E mutation were significantly more likely to be disease free (p=0.008). By contrast, a persistent disease status was significantly more prevalent among PTC patients with tumors harboring BRAFV600E mutation (p=0.009). Furthermore, all five PTC cases that developed distant metastasis during the follow-up period were BRAFV600E mutated (p=0.031).
In univariate analysis, the presence of BRAFV600E mutation was associated with age ≥55 years-old (p=0.039), male gender (p=0.043), conventional histology (p=0.008), extrathyroidal extension (p=0.006), lymph node metastasis (p<0.001) and positive resection margins (p=0.028). In multivariate analysis, conventional histology, extrathyroidal extension and lymph node metastasis remained significantly associated with the mutation (Table 2).
3.3. Predictive factors
The Kaplan-Meyer analysis revealed a significant impact of BRAFV600E mutation on EFS among our study cases. EFS at 60 months was documented in only 62.4% [CI: 54.2-70.6] PTC patients with tumors harboring BRAFV600E mutation compared to 91.7% [CI: 87.7-95.7] PTC patients with wild-type BRAFV600E tumors (long-rank test, p=0.010) (Figure 1).
Moreover, our data showed that concurrent presence of BRAFV600E mutation with various demographic and pathological features bearing prognostic value increases even more the risk for a reduced EFS. The results are illustrated in Table 3 and Figure 2.
p-values were obtained by applying the Log Rank test; multiple comparisons were performed with patients harboring wild-type BRAFV600E tumors, aged <55 years-old (a), of female gender (b), without extrathyroidal extension (c) and lymph node metastasis (d), respectively.
Nevertheless, BRAFV600E mutation was significantly associated with worse outcomes also among lower-risk groups of PTC patients. Patients aged <55 years-old (p<0.021), female patients (p=0.022), patients with tumors measuring ≤ 40 mm (p=0.034) or with a single tumor focus (p=0.023) but harboring BRAFV600E mutation revealed a significantly lower EFS compared to same PTC patients with non-BRAFV600E mutated tumors (see Table 3), data further supporting the prognostic value of BRAFV600E mutation.
In univariate analysis, a 3.74-fold increased risk for a reduced EFS (95%CI: [1.25 - 11.21], p=0.018) was found for BRAFV600E mutated cases. A reduced EFS was also associated with age at surgery equal to 55 years-old or above (p=0.027), male gender (p=0.005), extrathyroidal extension (p=0.016), multifocality (p=0.027) and lymph node metastasis (p<0.001). In multivariate analysis, male gender and lymph node metastasis remained significantly associated with worse EFS (Table 4)
4. Discussion
BRAFV600E mutation represents a very specific marker for PTC, also referred to as the “genetic signature of PTC” [24,25,26]. As this mutation appears to play an important role in PTC tumorigenesis, it has been postulated that it might also have a prognostic value. Nevertheless, whether BRAFV600E mutation relates to more aggressive clinicopathologic features and worse outcome in PTC patients remains variable and controversial, as highlighted by many different studies over the time [5,8,12,13,15,18,19,27,28,29].
The 2015 ATA Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer [23] emphasized that BRAFV600E mutational status, although not routinely recommended for initial postoperative risk stratification in differentiated thyroid cancer, has the potential to refine risk estimates when interpreted in the context of other clinicopathologic risk factors. Therefore, it appears that BRAFV600E mutation in isolation is not sufficient to substantially contribute to risk stratification, but an incremental improvement can be achieved if synergic interaction between BRAFV600E mutation and other risk factors is considered.
In the present study we evaluated the prevalence of BRAFV600E mutation and its relationship with demographic, pathological and outcome characteristics in a series of PTC patients. Further on, we assessed the prognostic value of BRAFV600E mutation in our series of cases, first as a single factor, and then in synergic interaction with other demographic and pathological risk factors.
In our study, BRAFV600E mutation was positive in 57.2% of CPT cases; it was found to be strongly associated with adverse demographic and pathological features, like older age, ≥55 years-old (p=0.037), male gender (p=0.035), conventional histology (p<0.0005), extrathyroidal extension (p=0.004), pT3b tumor stage (p=0.007), lymph node metastasis (p=0.001), positive surgical resection margins (p=0.022), a persistent disease status (p=0.009) and distant metastases (p=0.031). The univariate analysis confirmed these results, while in multivariate analysis, conventional histology, extrathyroidal extension and lymph node metastasis remained significantly associated with the mutation. Our results are in line with previously reported data from the literature [8,30]. In their large meta-analysis, including 63 studies and 20764 PTC patients with different ethnic and geographic backgrounds, Liu et al. [8] also reported a significant association between BRAFV600E mutation and extrathyroidal extension (p<0.00001), BRAFV600E mutation and an advanced TNM stage (III/IV) (p<0.00001), BRAFV600E mutation and lymph node metastasis (p<0.00001), BRAFV600E mutation and tumor recurrence (p<0.00001), respectively.
When looking at the impact of BRAFV600E mutation on patient’s outcomes and occurrence of adverse events (recurrent/persistent disease, distant metastasis), our data demonstrated the value of BRAFV600E mutation as a prognostic marker in the risk stratification assessment of PTC patients. The Kaplan-Meyer analysis showed a significant reduction of EFS among PTC patients with tumors harboring BRAFV600E mutation compared to PTC patients without mutation (p=0.010). In univariate analysis, BRAFV600E mutation was also significantly associated with a reduced EFS (p=0.018). In addition, concurrent presence of BRAFV600E mutation with other risk factors (age≥55 years-old, male gender, conventional and tall cell histology, tumor size>40mm, extrathyroidal extension, multifocality and lymph node metastasis) resulted in being a better predictor of adverse outcomes for PTC patients in our study, compared to BRAFV600E mutation alone.
The literature data is currently divided and highly controversial regarding the association between BRAFV600E mutation and poor prognosis in PTC. In accordance with the results present herein, there are studies that have found BRAFV600E mutation to be an independent predictor of poor outcomes [8,12,31]. Xing et al., for example, in their large multicenter study including more than 2000 patients demonstrated an independent prognostic value of BRAFV600E mutation for PTC recurrence even in patients with low TNM stage and micro-PTC [12]. Conversely, other authors have failed to demonstrate this [7,29,32,33]. In their recent systemic review including 11 studies and 4674 patients, Li. et al [33] have reported comparable rates of tumor recurrence between patients with PTC harboring BRAFV600E mutation and patients without mutation (HR 1.16, 95% CI 0.78–1.71). However, in a subgroup analysis, the authors found both geographical region and tumor stage as factors influencing the risk of recurrence associated with BRAFV600E mutation. These findings offer further support to the observation that heterogeneity of the data is relevant and should be considered when interpreting the impact of a BRAFV600E mutation on clinical outcomes [34].
Interestingly, when focusing on lower-risk patients with PTC (aged <55 years-old, female, with tumors measuring ≤ 40 mm or with a single tumor foci), BRAFV600E mutation was strongly associated with a worse EFS in our study. Thus, in these subgroups of PTCs, BRAFV600E mutation could help to identify patients requiring more intensive treatment and follow-up. The potential role of BRAFV600E mutation as an aid to risk stratification in low-risk PTC patients (classified as such based on clinico-pathological criteria) has been an issue raised by others before. In a study focused on low-risk patients with intrathyroidal PTC (<4cm, N0, M0) conducted by Elisei R et al [35], BRAFV600E mutated tumors had a recurrence rate of 8%, compared to only 1% in BRAFV600E wild-type tumors (p=0.003, Fisher’s exact). These results offer some new, promising perspectives, but need to be further confirmed by additional studies.
The oncogenic molecular mechanisms of BRAFV600E mutation in the pathogenesis of PTC and thyroid cancer in general are well documented in the literature. BRAFV600E mutation mimics a phosphorylation in the active segment of BRAF leading to a constitutive activation of the kinase. As a result, BRAFV600E driven tumors exhibit high extracellular signal-regulated kinase phosphorylation, leading to unregulated cell proliferation. The MAPK signaling inhibits at variable degree the expression of genes required for iodine uptake, which are hallmarks of the treatment of PTC [34,36]. Nevertheless, the mechanism associated with tumor aggressiveness in BRAFV600E mutated PTCs remains unclear and probably other pathways cooperate to promote cancer progression [34]. Notch putative pathway, a highly conserved signaling pathway, crucial in development and with an important role in malignant transformation might be implicated, as BRAFV600E mutation coupled with overexpression of the Notch intracellular domain leads to larger thyroid tumors, more aggressive disease and decreased overall survival [37]. Other pathways might be the overexpression of lysyl oxidase (LOX) [38] and the loss of individual SWI/SNF (switch/sucrose non-fermentable) subunits [39] that have been demonstrated as promoting disease progression and decrease survival in BRAFV600E mutated tumors.
Our study has some limitations: the relatively small number of cases and the retrospective nature of the study, which might have caused a certain degree of selection bias. Yet, to the best of our knowledge, this is first study addressing this topic in a Romanian population and, despite these limitations, our study covered a large time period (between 2008-2015) and included all PTCs registered at our hospital that fulfilled the inclusion criteria. Moreover, we performed a complete morphological characterization and obtained relevant follow-up data for all PTC cases included in the study.
5. Conclusions
To sum up, our results demonstrate the prognostic value of BRAFV600E mutation in the risk stratification assessment of PTC patients. Nevertheless, BRAFV600E mutation status should not be used in isolation but integrated in the context of other clinicopathological risk factors. In our study, the synergic interaction between BRAFV600E mutation and age≥55 years-old, male gender, conventional and tall cell histology, tumor size>40mm, extrathyroidal extension, multifocality and lymph node metastasis, respectively, resulted in being a better predictor of adverse outcomes for PTC patients, compared to BRAFV600E mutation alone. BRAFV600E mutation status is prognostically valuable also among lower-risk subgroups of PTC patients (aged <55 years-old, female, with tumors measuring ≤ 40 mm or with a single tumor foci), where it could help identifying patients requiring more intensive treatment and follow-up. Further studies are needed to confirm this.
Author Contributions
Conceptualization, ANB, AC and AB; Methodology, ANB, AC and AB; Software: AC and SV; Validation, ANB, CB and AB; Formal analysis: AC and SV; Investigation: ANB, AC, CB, VM and DP; Resources: ANB, AC, CB, DP and AB; Data Curation: ANB, AC, VM and AB; Writing – Original Draft Preparation: ANB; Writing – Review &Editing: CB and AB; Visualization: ANB; Supervision: AB; Project Administration, ANB; Funding Acquisition, ANB and AC.
Funding
This work was supported by the George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu-Mureș Research Grant No. 10127/4/17.12.2020.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the George Emil Palade University of Medicine, Pharmacy, Sciences and Technology of Târgu-Mureş, Romania protocol code no.36/07.03.2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical restrictions (personal data protection of the patients included in the study).
Acknowledgments
We would like to thank Ciurcă Dorina and Valeria Mesaroș for their highly valued technical help.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Xing, M. Molecular Pathogenesis and Mechanisms of Thyroid Cancer. Nat Rev Cancer 2013, 13, 184–199. [Google Scholar] [CrossRef]
- Holmes, D. Thyroid Cancer: Incidence Trends in the USA. Nat Rev Endocrinol 2016, 12, 312. [Google Scholar] [CrossRef] [PubMed]
- Mao, Y.; Xing, M. Recent Incidences and Differential Trends of Thyroid Cancer in the USA. Endocr Relat Cancer 2016, 23, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Amphlett, B.; Lawson, Z.; Abdulrahman, G.O.; White, C.; Bailey, R.; Premawardhana, L.D.; Okosieme, O.E. Recent Trends in the Incidence, Geographical Distribution, and Survival from Thyroid Cancer in Wales, 1985-2010. Thyroid 2013, 23, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Póvoa, A.A.; Teixeira, E.; Bella-Cueto, M.R.; Melo, M.; Oliveira, M.J.; Sobrinho-Simões, M.; Maciel, J.; Soares, P. Clinicopathological Features as Prognostic Predictors of Poor Outcome in Papillary Thyroid Carcinoma. Cancers (Basel) 2020, 12, 1–16. [Google Scholar] [CrossRef]
- Ulisse, S.; Baldini, E.; Lauro, A.; Pironi, D.; Tripodi, D.; Lori, E.; Ferent, I.C.; Amabile, M.I.; Catania, A.; Di Matteo, F.M.; et al. Papillary Thyroid Cancer Prognosis: An Evolving Field. Cancers (Basel) 2021, 13, 5567. [Google Scholar] [CrossRef]
- Bournaud, C.; Descotes, F.; Decaussin-Petrucci, M.; Berthiller, J.; de la Fouchardière, C.; Giraudet, A.L.; Bertholon-Gregoire, M.; Robinson, P.; Lifante, J.C.; Lopez, J.; et al. TERT Promoter Mutations Identify a High-Risk Group in Metastasis-Free Advanced Thyroid Carcinoma. Eur J Cancer 2019, 108, 41–49. [Google Scholar] [CrossRef]
- Liu, C.; Chen, T.; Liu, Z. Associations between BRAF and Prognostic Factors and Poor Outcomes in Papillary Thyroid Carcinoma: A Meta-Analysis. World J Surg Oncol 2016, 14, 241. [Google Scholar] [CrossRef]
- Garnett, M.J.; Marais, R. Guilty as Charged: B-RAF Is a Human Oncogene. Cancer Cell 2004, 6, 313–319. [Google Scholar] [CrossRef]
- Davies, H.; Bignell, G.R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M.J.; Bottomley, W.; et al. Mutations of the BRAF Gene in Human Cancer. Nature 2002, 417, 949–954. [Google Scholar] [CrossRef]
- Hilger, R.A.; Scheulen, M.E.; Strumberg, D. The Ras-Raf-MEK-ERK Pathway in the Treatment of Cancer. Onkologie 2002, 25, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Shong, Y.K.; Kim, T.Y.; Viola, D.; Elisei, R.; Bendlová, B.; Yip, L.; Mian, C.; et al. Association between BRAF V600E Mutation and Recurrence of Papillary Thyroid Cancer. J Clin Oncol 2015, 33, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yan, K.; Lin, X.; Zhao, L.; An, W.; Wang, C.; Liu, X. The Association between BRAF (V600E) Mutation and Pathological Features in PTC. Eur Arch Otorhinolaryngol 2014, 271, 3041–3052. [Google Scholar] [CrossRef] [PubMed]
- Attia, A.S.; Hussein, M.; Issa, P.P.; Elnahla, A.; Farhoud, A.; Magazine, B.M.; Youssef, M.R.; Aboueisha, M.; Shama, M.; Toraih, E.; et al. Association of BRAFV600E Mutation with the Aggressive Behavior of Papillary Thyroid Microcarcinoma: A Meta-Analysis of 33 Studies. Int J Mol Sci 2022, 23, 15626. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, Y.J.; Lim, J.A.; Ahn, H.Y.; Lee, E.K.; Lee, Y.J.; Kim, K.W.; Hahn, S.K.; Youn, Y.K.; Kim, K.H.; et al. The Association of the BRAF(V600E) Mutation with Prognostic Factors and Poor Clinical Outcome in Papillary Thyroid Cancer: A Meta-Analysis. Cancer 2012, 118, 1764–1773. [Google Scholar] [CrossRef] [PubMed]
- Xing, M. BRAF Mutation in Papillary Thyroid Cancer: Pathogenic Role, Molecular Bases, and Clinical Implications. Endocr Rev 2007, 28, 742–762. [Google Scholar] [CrossRef]
- Vuong, H.G.; Duong, U.N.P.; Altibi, A.M.A.; Ngo, H.T.T.; Pham, T.Q.; Tran, H.M.; Gandolfi, G.; Hassell, L. A Meta-Analysis of Prognostic Roles of Molecular Markers in Papillary Thyroid Carcinoma. Endocr Connect 2017, 6, R8–R17. [Google Scholar] [CrossRef] [PubMed]
- Ulisse, S.; Baldini, E.; Sorrenti, S.; Barollo, S.; Prinzi, N.; Catania, A.; Nesca, A.; Gnessi, L.; Pelizzo, M.R.; Mian, C.; et al. In Papillary Thyroid Carcinoma BRAFV600E Is Associated with Increased Expression of the Urokinase Plasminogen Activator and Its Cognate Receptor, but Not with Disease-Free Interval. Clin Endocrinol (Oxf) 2012, 77, 780–786. [Google Scholar] [CrossRef]
- Gan, X.; Shen, F.; Deng, X.; Feng, J.; Lu, J.; Cai, W.; Peng, L.; Zheng, W.; Wang, W.; Huang, P.; et al. Prognostic Implications of the BRAF-V600E Mutation in Papillary Thyroid Carcinoma Based on a New Cut-off Age Stratification. Oncol Lett 2020, 19, 631–640. [Google Scholar] [CrossRef]
- Lloyd, R. V.; Osamura, R.Y.; Klöppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs; Lloyd, R. V. , Osamura, R.Y., Klöppel, G., Rosai, J., Eds.; International Agency for Research on Cancer, 2017. ISBN 978-92-832-4493-6.
- American Joint Committee on, Cancer.; Amin, M.B. American Joint Committee on Cancer.; Amin, M.B. AJCC Cancer Staging Manual. 2017.
- Nechifor-Boila, A.; Loghin, A.; Descotes, F.; Decaussin-Petrucci, M.; Borda, A. Evaluation of a DNA Extraction and Purification Protocol Using Archived Formalin-Fixed Paraffin-Embedded Tissues for BRAF Mutations Analysis in Papillary Thyroid Microcarcinomas. Appl Immunohistochem Mol Morphol 2019, 27, 70–76. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Costa, V.; Esposito, R.; Pallante, P.; Ciccodicola, A.; Fusco, A. The “next-Generation” Knowledge of Papillary Thyroid Carcinoma. Cell Cycle 2015, 14, 2018–2021. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Akbani, R.; Aksoy, B.A.; Ally, A.; Arachchi, H.; Asa, S.L.; Auman, J.T.; Balasundaram, M.; Balu, S.; Baylin, S.B.; et al. Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef] [PubMed]
- Kucukodaci, Z.; Akar, E.; Haholu, A.; Baloglu, H. A Valuable Adjunct to FNA Diagnosis of Papillary Thyroid Carcinoma: In-House PCR Assay for BRAF T1799A (V600E). Diagn Cytopathol 2011, 39, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Wei, X.; Wang, X.; Xiong, J.; Li, C.; Liao, Y.; Zhu, Y.; Mao, J. Risk and Prognostic Factors for BRAFV600E Mutations in Papillary Thyroid Carcinoma. Biomed Res Int 2022, 2022. [Google Scholar] [CrossRef]
- Daliri, M.; Abbaszadegan, M.R.; Mehrabi Bahar, M.; Arabi, A.; Yadollahi, M.; Ghafari, A.; Taghehchian, N.; Zakavi, S.R. The Role of BRAF V600E Mutation as a Potential Marker for Prognostic Stratification of Papillary Thyroid Carcinoma: A Long-Term Follow-up Study. Endocr Res 2014, 39, 189–193. [Google Scholar] [CrossRef]
- Al-Masri, M.; Al-Shobaki, T.; Al-Najjar, H.; Iskanderian, R.; Younis, E.; Abdallah, N.; Tbakhi, A.; Haddad, H.; Al-Masri, M.; Obeid, Z.; et al. BRAF V600E Mutation in Papillary Thyroid Carcinoma: It’s Relation to Clinical Features and Oncologic Outcomes in a Single Cancer Centre Experience. Endocr Connect 2021, 10, 1531–1537. [Google Scholar] [CrossRef]
- Zhang, Q.; Liu, S.Z.; Guan, Y.X.; Chen, Q.J.; Zhu, Q.Y. Meta-Analyses of Association Between BRAF(V600E) Mutation and Clinicopathological Features of Papillary Thyroid Carcinoma. Cell Physiol Biochem 2016, 38, 763–776. [Google Scholar] [CrossRef]
- Xing, M.; Westra, W.H.; Tufano, R.P.; Cohen, Y.; Rosenbaum, E.; Rhoden, K.J.; Carson, K.A.; Vasko, V.; Larin, A.; Tallini, G.; et al. BRAF Mutation Predicts a Poorer Clinical Prognosis for Papillary Thyroid Cancer. J Clin Endocrinol Metab 2005, 90, 6373–6379. [Google Scholar] [CrossRef]
- Damiani, L.; Lupo, S.; Rossi, R.; Bruni, S.; Bartolomei, M.; Panareo, S.; Franceschetti, P.; Carcoforo, P.; Lanza, G.; Pelucchi, S.; et al. Evaluation of the Role of BRAF V600E Somatic Mutation on Papillary Thyroid Cancer Disease Persistence: A Prospective Study. Eur Thyroid J 2018, 7, 251–257. [Google Scholar] [CrossRef]
- Li, X.; Kwon, H. The Impact of BRAF Mutation on the Recurrence of Papillary Thyroid Carcinoma: A Meta-Analysis. Cancers (Basel) 2020, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Scheffel, R.S.; Dora, J.M.; Maia, A.L. BRAF Mutations in Thyroid Cancer. Curr Opin Oncol 2022, 34, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Elisei, R.; Viola, D.; Torregrossa, L.; Giannini, R.; Romei, C.; Ugolini, C.; Molinaro, E.; Agate, L.; Biagini, A.; Lupi, C.; et al. The BRAF(V600E) Mutation Is an Independent, Poor Prognostic Factor for the Outcome of Patients with Low-Risk Intrathyroid Papillary Thyroid Carcinoma: Single-Institution Results from a Large Cohort Study. J Clin Endocrinol Metab 2012, 97, 4390–4398. [Google Scholar] [CrossRef] [PubMed]
- Romei, C.; Elisei, R. A Narrative Review of Genetic Alterations in Primary Thyroid Epithelial Cancer. Int J Mol Sci 2021, 22, 1–16. [Google Scholar] [CrossRef]
- Guenter, R.; Patel, Z.; Chen, H. Notch Signaling in Thyroid Cancer. Adv Exp Med Biol 2021, 1287, 155–168. [Google Scholar] [CrossRef]
- Boufraqech, M.; Patel, D.; Nilubol, N.; Powers, A.; King, T.; Shell, J.; Lack, J.; Zhang, L.; Gara, S.K.; Gunda, V.; et al. Lysyl Oxidase Is a Key Player in BRAF/MAPK Pathway-Driven Thyroid Cancer Aggressiveness. Thyroid 2019, 29, 79–92. [Google Scholar] [CrossRef]
- Saqcena, M.; Leandro-Garcia, L.J.; Maag, J.L.V.; Tchekmedyian, V.; Krishnamoorthy, G.P.; Tamarapu, P.P.; Tiedje, V.; Reuter, V.; Knauf, J.A.; de Stanchina, E.; et al. SWI/SNF Complex Mutations Promote Thyroid Tumor Progression and Insensitivity to Redifferentiation Therapies. Cancer Discov 2021, 11, 1158–1175. [Google Scholar] [CrossRef]
Figure 1.
Kaplan-Meier analysis of the impact of BRAFV600E mutation on event-free survival of the total patients included in the study. The presence of BRAFV600E mutation was significantly associated with poor event-free survival among all study cases.
Figure 1.
Kaplan-Meier analysis of the impact of BRAFV600E mutation on event-free survival of the total patients included in the study. The presence of BRAFV600E mutation was significantly associated with poor event-free survival among all study cases.
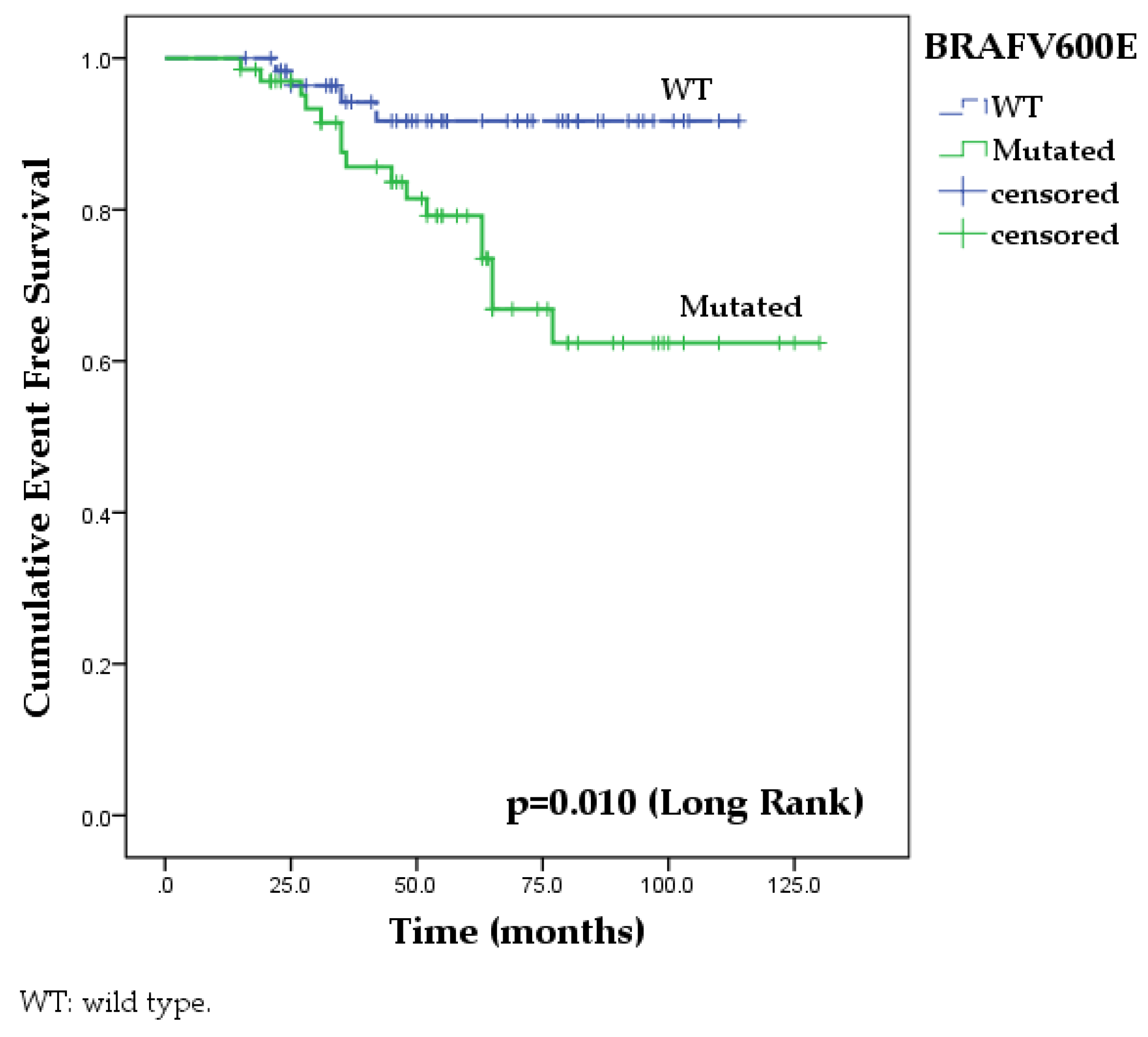
Figure 2.
Kaplan-Meier analysis of the impact of BRAFV600E mutation associated with demographic and histological features on event-free survival of the total patients included in the study: (a) BRAFV600E mutation and patient’s age (<55 versus ≥55 years-old); (b) BRAFV600E mutation and male gender; (c) BRAFV600E mutation and extrathyroidal extension; (d) BRAFV600E mutation and lymph node metastasis.
Figure 2.
Kaplan-Meier analysis of the impact of BRAFV600E mutation associated with demographic and histological features on event-free survival of the total patients included in the study: (a) BRAFV600E mutation and patient’s age (<55 versus ≥55 years-old); (b) BRAFV600E mutation and male gender; (c) BRAFV600E mutation and extrathyroidal extension; (d) BRAFV600E mutation and lymph node metastasis.
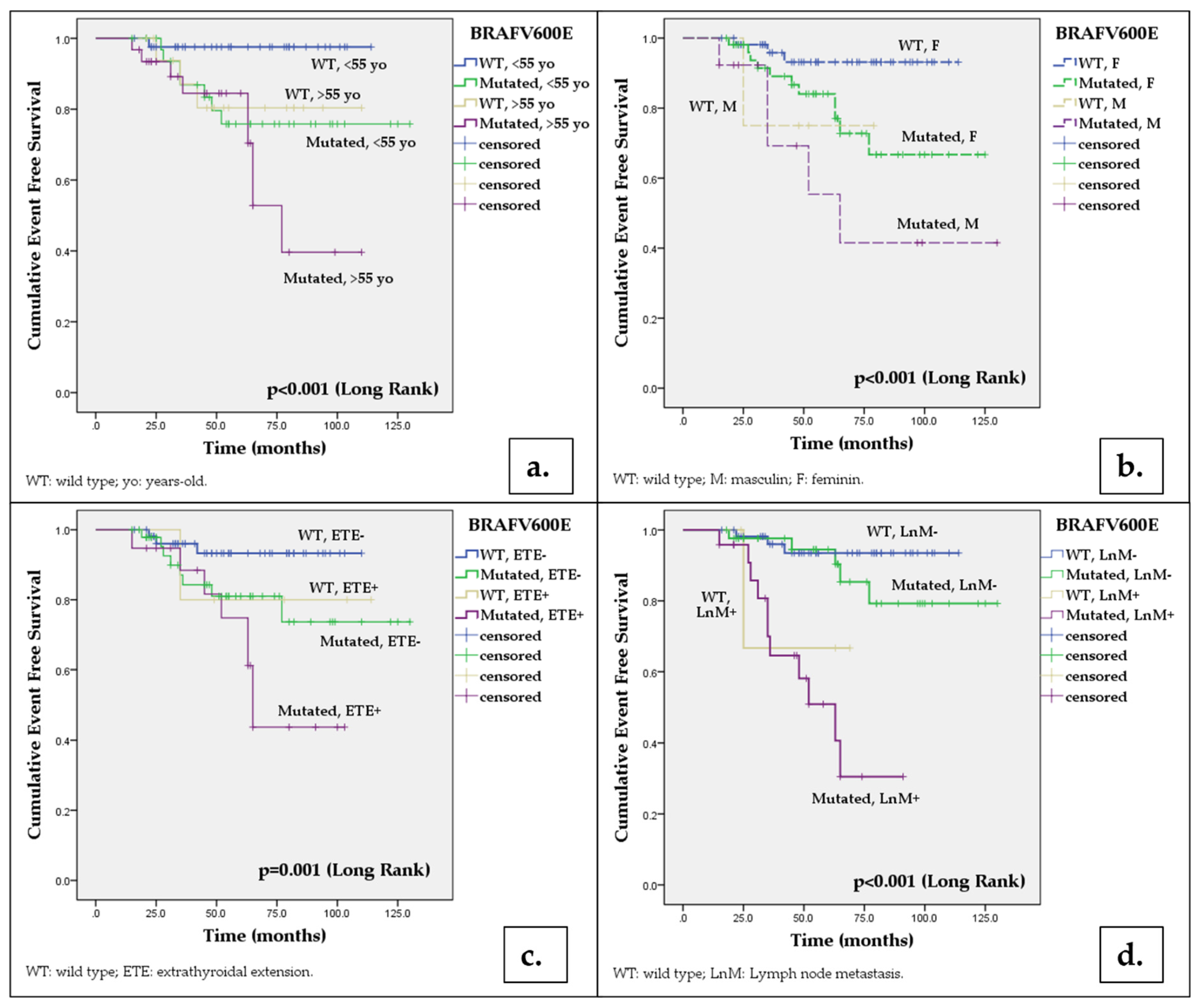

Table 1.
Clinical and histopathological data for the study cases.
| Factors | Total n= 127 |
BRAFV600E wild-type n=60 |
BRAFV600E mutated n=67 |
pa |
|---|---|---|---|---|
| Age at surgery (mean±SD, years) | 48.6 ± 1.28 | 46.18 ± 1.17 | 50.76 ± 1.72 | 0.075* |
| Age (n, %) | ||||
| < 55 years | 79 (62.2) | 43 (71.7) | 36 (53.7) | 0.037 |
| ≥ 55 years | 48 (37.8) | 17 (28.3) | 31 (46.3) | 0.037 |
| Gender, female (n, %) | 110 (86.6) | 56 (93.3) | 54 (80.6) | 0.035 |
| Tumor size (mean±SD, mm) | 22.88 ±1.5 | 23.35 ± 1.42 | 21.90 ± 1.33 | 0.458* |
| Tumor size (n, %) | ||||
| 11-20 mm | 67 (52.8) | 29 (48.3) | 38 (56.7) | 0.442 |
| 21-40 mm | 51 (40.2) | 27 (45.0) | 24 (35.8) | 0.225 |
| >40 mm | 9 (7.1) | 4 (6.7) | 5 (7.5) | 0.864 |
| Multifocality (n, %) | 51 (40.2) | 20 (33.3) | 31 (46.3) | 0.138 |
| Histological variant (n, %) | ||||
| Conventional | 88 (69.3) | 32 (53.3) | 56 (83.6) | 0.0005 |
| Tall cell variant | 9 (7.1) | 3 (5) | 6 (9) | 0.596 |
| Warthin-like | 7 (5.5) | 3 (5) | 4 (6) | 0.886 |
| Oncocytic | 3 (2.4) | 3 (5) | 0 | 0.205 |
| Solid | 2 (1.6) | 2 (3.3) | 0 | 0.434 |
| Follicular variant, infiltrative | 13 (10.2) | 12 (20) | 1 (1.5) | 0.001 |
| Follicular variant, encapsulated, invasive | 5 (3.9) | 5 (8.3) | 0 | 0.051 |
| Extrathyroidal extension (n, %) | 24 (18.9) | 5 (8.3) | 19 (28.4) | 0.004 |
| Primary tumor, pT (n, %) | ||||
| 1b | 51 (40.2) | 25 (41.7) | 26 (38.8) | 0.879 |
| 2 | 44 (34.6) | 25 (41.7) | 19 (28.4) | 0.165 |
| 3a | 8 (6.3) | 5 (8.3) | 3 (4.5) | 0.607 |
| 3b | 24 (18.9) | 5 (8.3) | 19 (28.4) | 0.007 |
| Lymph node involvement | 26/39 | 2/8 (25) | 24/31 (77.4) | 0.001 |
| Vascular invasion (n, %) | 4 (3.3) | 2 (3.1) | 2 (3) | 0.911 |
| Positive surgical resection margin | 18 (14.2) | 4 (6.7) | 14 (20.9) | 0.022 |
| Stage grouping | ||||
| I | 101 (79.5) | 54 (90) | 47 (70.1) | 0.010 |
| II | 22 (17.3) | 6 (10) | 16 (23.9) | 0.067 |
| III | 4 (3.1) | 0 | 4 (6) | 0.155 |
| Type of surgery | ||||
| Lobectomy | 0 | 0 | 0 | - |
| Total thyroidectomy | 88 (69.3) | 52 (86.7) | 36 (53.7) | 0.0001 |
| Total thyroidectomy with lymph node dissection | 39 (30.7) | 8 (13.3) | 31 (46.2) | 0.0001 |
| Follow-up data (n, median, months) | 57 (CI:9-130) | 58 (CI:17-114) | 57 (CI: 9-130) | - |
| I131 therapy (n, %) | 133 (100) | 66 (100) | 67 (100) | - |
| Disease free (n, %) | 107 (84.3) | 56 (93.4) | 51 (76.1) | 0.008 |
| Persistent disease (n, %) | 14 (11) | 2 (3.3) | 12 (17.9) | 0.009 |
| Recurrence (n, %) | 6 (4.7) | 2 (3.3) | 4 (6) | 0.484 |
| Distant metastasis (n, %) | 5 (3.9) | 0 | 5 (7.5) | 0.031 |
a Fisher test; *Chi square test and *student test. Statistically significant differences are shown in bold and italics.
Table 2.
Univariate and multivariate analysis of prognostic factors associated with BRAFV600E mutation for the study cases.
Table 2.
Univariate and multivariate analysis of prognostic factors associated with BRAFV600E mutation for the study cases.
| Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|
| Factors | BRAFV600E positive (67)/N | OR | [95% CI] | p | OR | [95% CI] | p |
| Age ≥55 years | 31/48 | 2.18 | [1.04 - 4.56] | 0.039 | 2.20 | [0.90- 5.37] | 0.081 |
| Sex, male | 13/17 | 3.37 | [1.03 -10.98] | 0.043 | 2.81 | [0.67 - 11.72] | 0.155 |
| PTC, conventional | 56/88 | 4.44 | [1.95- 10.13] | 0.008 | 6.33 | [2.18 - 18.40] | <0.001 |
| PTC, “tall cell” | 4/9 | 1.88 | [0.44 -7.82] | 0.392 | |||
| Tumor size >40mm | 5/9 | 1.13 | [0.28- 4.41] | 0.861 | |||
| Extrathyroidal extension | 19/24 | 4.35 | [1.51 -12.54] | 0.006 | 5.83 | [1.60- 21.27] | 0.007 |
| Multifocality | 31/51 | 1.72 | [0.83 - 3.53] | 0.139 | |||
| Lymph node metastasis | 24/26 | 7.81 | [2.52 - 24.20] | <0.001 | 4.77 | [1.44 - 15.79] | 0.010 |
| Positive resection margin | 14/18 | 3.69 | [1.14- 11.95] | 0.028 | 2.25 | [0.56 - 9.00] | 0.249 |
OR- Odds ratio, 95% CI- 95% confidence interval, p<0.05, PTC: papillary thyroid carcinoma. Statistically significant differences are shown in bold and italics.
Table 3.
Event free survival at 12, 24, 48 and 60 months, respectively, for our study patients in relation to BRAFV600E mutation status and other demographic and pathological factors.
Table 3.
Event free survival at 12, 24, 48 and 60 months, respectively, for our study patients in relation to BRAFV600E mutation status and other demographic and pathological factors.
| BRAFV600E wild type | BRAFV600E mutated | Log Rank | p | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Factors |
*12 months (%) (95%CI) |
*24 months (%) (95%CI) |
*48 months (%) (95%CI) |
*60 months (%) (95%IC) |
*12 months (%) (95%CI) |
*24 months (%) (95%CI) |
*48 months (%) (95%CI) |
*60 months (%) (95%CI) |
||
| Total | 98.3 (96.6-100) | 96.4 (93.9- 98.4) | 94.2 (90.9-97.5) | 91.7 (87.7-95.7) | 98.5 (97-100) | 95.1 (92.3-97.9) | 81.4 (76-86.8) | 62.4 (54.2-70.6) | 6.581 | 0.010 |
| Age (n,%) | ||||||||||
| < 55 years | 97.6 (95.2-100) | 97.6 (95.2-100) | 97.6 (95.2-100) | 97.6 (95.2-100) | 96.8 (96.4-100) | 93.5 (89.1-97.8) | 79.6 (72.1-87.1) | 75.8 (67.8-83.8) | 5.314a | 0.021 |
| ≥ 55 years | 93.8 (93.1-100) | 93.8 (93.1-100) | 80.4 (70.2-90.6) | 80.4 (70.2-90.6) | 96.8 (93.6-100) | 93.4 (88.9-97.9) | 84.5 (77.2-91.8) | 52.8 (39.3-66.3) | 12.641a | <0.001 |
| Gender (n, %) | ||||||||||
| Female | 98.1 (96.3-100) | 98.1 (96.3-100) | 93.1 (89.2-97) | 93.1 (89.2-97) | 98.1 (96.2-100) | 95.9 (93-98.8) | 84 (78.4-89.6) | 72.8 (65-80.6) | 5.274b | 0.022 |
| Male | 75 (53.3-96.7) | 75 (53.3-96.7) | 75 (53.3-96.7) | 75 (53.3-96.7) | 92.3 (84.9-100) | 92.3 (84,9-100) | 69.2 (47.7-78.1) | 55.4 (38.1-72.7) | 13.427b | <0.001 |
| Histology | ||||||||||
| PTC conventional | 96.7 (93.4-100) | 94.3 (90-98.6) | 92.1 (87.2-97) | 89.3 (83.7-94.9) | 98.1 (96.2-100) | 93.6 (90-97.2) | 78.6 (72.2-85) | 68.5 (59.8-77.2) | 7.973 | 0.005 |
| PTC tall cell variant | 98.4 (96.8-100) | 85.4 (81.5-89.3) | 66.7 (39.5-93.9) | 66.7 (39.5-93.9) | 83.3 (68.1-98.5) | 83.3 (68.1-96.5) | 62.5 (41.2-83.8) | 41.7 (19.5-63.9) | 5.997 | 0.014 |
| Tumor size | ||||||||||
| ≤ 40 mm | 98.2(96.4-100) | 96.2 (93.5-98,9) | 91.2 (86.9-95.5) | 91.2(86.9-95.5) | 98.4(96.8-100) | 96.7 (94.4-99) | 81.7 (76.1-87.3) | 68.3 (60.6-76) | 4.505c | 0.034 |
| > 40 mm | - | - | - | - | - | - | 80 (62.1-97.9) | 26.7 (4.1-49.3) | 8.221c | 0.004 |
| Extrathyroidal extension | ||||||||||
| Absent | 98.1 (96.3-100) | 96 (93.2-98.8) | 93.3 (89.5-97.1) | 93.3 (89.5-97.1) | 97.8 (95,6-100) | 95.2 (91.9-98.5) | 81 (74.5-87.5) | 73.7 (64.5-82.9) | 3.608d | 0.057 |
| Present | 99 (98-100) | 80 (62.1-97.9) | 80 (62.1-97.9) | 80 (62.1-97.9) | 94.7 (89.6-100) | 88,4 (80.6-96.2) | 74.8 (63.8-85.8) | 43.7 (29.9-57.5) | 11.243d | 0.001 |
| Multifocality | ||||||||||
| Absent | 97.2 (94.5-100) | 97.2 (94.5-100) | 97.2 (94.5-100) | 97.2 (94.5-100) | 97.2 (94.5-100) | 97.2 (94.5-100) | 85.8 (79.1-92.5) | 74 (64.3-83.7) | 5.193e | 0.023 |
| Prezent | 95 (90-100) | 95 (90-100) | 88.7 (81.1-96.3) | 81.8 (72.2-91.4) | 96.7 (93.4-100) | 92.9 (88.1-97.7) | 77.4 (69.2-85.6) | 59.7 (48.7-70.7) | 11.639e | 0.001 |
| Lymph node metastases | ||||||||||
| Absent | 98.1 (96.3-100) | 98.1 (96.3-100) | 93.5 (89.8-97.2) | 93.5 (89.8-97,2) | 97.6 (95.2-100) | 97.5 (95.2-100) | 94.5 (90.7-98.3) | 85.3 (92.4-78.2) | 1.155f | 0.282 |
| Present | - | 66.7(39.5-93.9) | 66.7(39.5-93.9) | - | 95.8 (91.7-100) | 90.8 (84.6-97) | 58.1 (46.6-69.6) | 30.5 (17.2-43.8) | 23.84f | <0.001 |
95% CI - 95% confidence interval, p<0.05; PTC: papillary thyroid carcinoma. *Percentage of patients without adverse events at that precise moment (event including persistent disease, recurrent disease, distant metastasis). a Log Rank obtained by comparison with patients aged < 55 years-old and wild-type BRAFV600E tumors. b Log Rank obtained by comparison with female patients with wild-type BRAFV600E tumors. c Log Rank obtained by comparison with patients harboring wild-type BRAFV600E tumors ≤ 4 cm. d Log Rank obtained by comparison with patients harboring wild-type BRAFV600E tumors without extrathyroidal extension. e Log Rank obtained by comparison with patients harboring unifocal, wild-type BRAFV600E tumors. f Log Rank obtained by comparison with patients harboring wild-type BRAFV600E tumors and no lymph node involvement.The percentage of patients with EFS at 60 months was significantly reduced when BRAFV600E mutation was associated with age≥55 years-old (p<0.001), male gender (p<0.001), conventional (p=0.005) and tall cell histology (p=0.014), tumor size>40mm (p=0.001), extrathyroidal extension (p=0.001), multifocality (p=0.001) and lymph node metastasis (p<0.001). Statistically significant differences are shown in bold and italics.
Table 4.
Univariate and multivariate analysis of prognostic factors for event-free survival among patients with PTC in our study.
Table 4.
Univariate and multivariate analysis of prognostic factors for event-free survival among patients with PTC in our study.
| Univariate analysis | Multivariate analysis | ||||||
|---|---|---|---|---|---|---|---|
| Factors | Event/N (total =127) |
HR | [95% CI] | p | HR | [95% CI] | p |
| Age ≥55 years | 12/48 | 2.74 | [1.12 - 6.73] | 0.027 | 2.39 | [0.82-6.96] | 0.109 |
| Sex, male | 6/17 | 3.91 | [1.4 - 10.21] | 0.005 | 3.80 | [1.30-11.06] | 0.014 |
| PTC, conventional | 12/88 | 0.82 | [0.33 - 2.01] | 0.620 | |||
| PTC, “tall cell” variant | 4/9 | 2.71 | [0.91 - 8.12] | 0.075 | |||
| Tumor size >40mm | 3/9 | 2.40 | [0.70 - 8.23] | 0.163 | |||
| Extrathyroidal extension | 9/24 | 2.96 | [1.22 - 7.15] | 0.016 | 1.02 | [0.31 – 3.47] | 0.905 |
| Multifocality | 13/51 | 2.81 | [1.12 - 7.05] | 0.027 | 3.11 | [0.97 - 9.95] | 0.055 |
| Lymph node metastasis | 12/26 | 9.14 | [3.63 - 22.97] | <0.001 | 6.71 | [2.29-19.69] | <0.001 |
| Positive resection margin | 5/18 | 2.79 | [0.99 - 7.89] | 0.05 | |||
| Positive BRAFV600E mutation | 16/67 | 3.74 | [1.25 - 11.21] | 0.018 | 1.02 | [0.27-3.61] | 0.998 |
HR - Hazard ratio, 95% CI- 95% confidence interval, p<0.05, PTC: papillary thyroid carcinoma. The event included persistent disease, recurrent disease, distant metastasis. Statistically significant differences are shown in bold and italics.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



