
Submitted:
06 July 2023
Posted:
07 July 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Metabolic-associated fatty liver disease (MAFLD) and its potential impact on the severity of COVID-19 have gained significant attention during the pandemic. This review aimed to explore the genetic determinants associated with MAFLD, previously recognized as non-alcoholic fatty liver disease (NAFLD), and their potential influence on COVID-19 outcomes. Various genetic polymorphisms, including PNPLA3 (rs738409), GCKR (rs780094), TM6SF2 (rs58542926), and LYPLAL1 (rs12137855), have been investigated in relation to MAFLD susceptibility and progression. Genome-wide association studies and meta-analyses have revealed associations between these genetic variants and MAFLD risk, as well as their effects on lipid metabolism, glucose regulation, and liver function. Furthermore, emerging evidence suggests a possible connection between these MAFLD-associated polymorphisms and the severity of COVID-19. Studies exploring the association between indicated genetic variants and COVID-19 outcomes have shown conflicting results. Some studies observed a potential protective effect of certain variants against severe COVID-19, while others reported no significant associations. This review highlights the importance of understanding the genetic determinants of MAFLD and its potential implications for COVID-19 outcomes. Further research is needed to elucidate the precise mechanisms linking these genetic variants to disease severity and to develop gene profiling tools for early prediction of COVID-19 outcomes. If confirmed as determinants of disease severity, these genetic polymorphisms could aid in identifying high-risk individuals and improving the management of COVID-19.
Keywords:
MAFLD
; COVID-19
; NAFLD
; SARS-CoV-2
; PNPLA
; rs738409
; GCKR
; rs780094
; TM6SF2
; rs58542926
; LYPLAL1
; rs12137855
1. Introduction
As of June 18, 2023, the global reported cases of Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have exceeded 767 million, resulting in over 6.9 million fatalities [1].
The clinical manifestations of this infection range widely, encompassing mild or asymptomatic cases to severe acute respiratory syndrome.
However, it has become evident that the outcome of infection is heavily influenced by host-related factors, including advanced age [2,3,4,5], male gender [2,4,5], and the presence of various comorbidities such as hypertension [6,7], cardiovascular disease [5], obesity [2,3,8,9], and type 2 diabetes [5,10,11,12,13].
While the role of virally driven hyperinflammation, which leads to an excessive release of cytokines and triggers a phenomenon known as a "Cytokine storm," remains a topic of controversy [14], the involvement of inflammatory processes in the severity of COVID-19, particularly among patients with comorbidities, is widely acknowledged [15].
Since the initial phase of the pandemic, the observation of familial clustering of severe COVID-19 cases has suggested the potential contribution of a genetic predisposition [16].
Therefore, it is plausible to consider that the intricate nature of the host's genetic background, characterized by various polymorphisms, could significantly impact the pathogenesis and outcome of COVID-19.
While advanced age, male sex, obesity, diabetes mellitus (DM), and other comorbidities have been established as risk factors for severe forms of the disease, these factors alone do not adequately explain the wide-ranging inter-individual variations observed in the severity of COVID-19 [17,18].
Therefore, the influence of genetic variations on clinical outcomes must be considered [18,19]. In this regard, multiple studies have elucidated the involvement of genetic polymorphisms in susceptibility to and severity of COVID-19, with these polymorphisms being implicated in various biological pathways associated with the disease [18,19].
Interferons (IFN) serve as key mediators of antiviral signaling, stimulating the release of numerous vital components involved in the early host response to viral infection.
Consequently, polymorphisms occurring in IFN genes or their receptors have been linked to an increased susceptibility to COVID-19 or more severe clinical outcomes [19,20,21].
Another crucial genetic mechanism involved in combating viral infections involves a genomic locus that harbors three genes responsible for encoding antiviral 2',5'-oligoadenylate synthetase (OAS) enzymes (OAS1, OAS2, and OAS3). These enzymes are interferon-inducible antiviral proteins that activate the latent form of ribonuclease L (RNase L) [22,23]. Particularly, the RNase L pathway assumes specific significance in the immune response mounted against SARS-CoV-2, an RNA virus [19].
Regarding susceptibility to COVID-19, considerable attention has been directed toward investigating polymorphisms located in the Angiotensin-converting enzyme 2 (ACE2) and Transmembrane serine protease 2 (TMPRSS2) genes, which are directly involved in viral binding and the subsequent entry of the virus into host cells [24,25].
Non-alcoholic fatty liver disease (NAFLD), currently recognized as metabolic-associated fatty liver disease (MAFLD), encompasses a spectrum of conditions that range from simple steatosis with or without mild inflammation to a necroinflammatory subtype characterized by hepatocellular injury, known as non-alcoholic steatohepatitis (NASH), and eventual progression to cirrhosis [26,27]. MAFLD represents the most prevalent cause of chronic liver disease globally, with an estimated impact on approximately one-fourth of the global population [28,29]. The adoption of a novel definition for MAFLD has been proposed as a more suitable characterization of the hepatic manifestation of metabolic syndrome compared to the conventional definition of NAFLD [30,31,32].
While the relationship remains contentious, initial reports during the COVID-19 pandemic suggested that patients with MAFLD may face an elevated risk of experiencing a more severe disease course [33,34,35,36]. However, it remains unclear whether MAFLD merely associates with adverse outcomes or whether it plays a causal role [37]. Furthermore, it is crucial not only to acknowledge the potential impact of MAFLD on the course of COVID-19 but also to recognize the effects of the COVID-19 pandemic itself on patients with MAFLD and the overall epidemiology of the disease [37].
The pathogenesis of fatty liver is influenced by genetic factors as well. Notably, a large-scale genome-wide association study (GWAS) identified specific DNA sequence variants, including Patatin-like phospholipase domain containing 3 (PNPLA3, rs738409-G), Glucokinase regulator (GCKR, rs780094-T), and Lysophospholipase-like 1 (LYPLAL1, rs12137855-C) that were associated with computed tomography-defined steatosis and biopsy-proven NAFLD characterized by lobular inflammation and fibrosis [38]. Moreover, other investigations have elucidated the functional significance of Transmembrane 6 superfamily member 2 (TM6SF2, rs58542926-T), a variant at the NCAN loci [39,40]. Among these genetic variants, PNPLA3 rs738409-G emerges as the most robust risk factor for NAFLD, exhibiting an odds ratio of 3.24 for histologic NAFLD [38]. Additionally, GCKR rs780094-T and TM6SF2 rs58542926-T have been recognized as significant determinants contributing to inter-individual variation in liver fat content [41,42,43]. Nevertheless, the functional implications of LYPLAL1 rs12137855-C remain relatively less explored.
Regarding the impact of these NAFLD-associated genetic polymorphisms on the course of COVID-19, the precise mechanisms remain incompletely understood (Figure 1). Nonetheless, several studies have already emerged, revealing unexpected associations between these genetic factors and COVID-19 outcomes [44,45,46,47].
2. Genetic Polymorphisms Associated with Susceptibility COVID-19
2.1. ACE2
ACE2 serves as a transmembrane protein and functions as the principal entry receptor for certain coronaviruses, including SARS-CoV, MERS-CoV, and SARS-CoV-2, facilitating their entry into host cells [48]. The expression of ACE2 has been associated with an increased number of viral binding sites on cell membranes, rendering carriers susceptible to infection. In particular, the ACE2 single nucleotide polymorphism (SNP) rs2074192 has been identified as a risk factor for hypertension in adult males with obesity [49]. Moreover, rs2074192 has been implicated in the development of type 2 diabetes mellitus and cardiovascular disease [50].
The presence of the intronic variant rs2074192 has been associated with modifications in RNA secondary structure, which may disrupt the delicate equilibrium between ACE2 transcription and translation. This dysregulation has implications for the binding affinity of SARS-CoV-2 to angiotensin receptors [51]. Additionally, earlier studies have demonstrated that COVID-19 patients with coexisting hypertension experienced reduced mortality rates when treated with ACE inhibitors or angiotensin II receptor blockers (ARBs) compared to individuals who did not receive these medications [52].
ACE2 polymorphism (rs2074192) in obese, smoking males has been associated with greater variability in outcomes for COVID-19 disease, leading to more divergent outcomes [53].
Several investigations have highlighted a potential link between ACE2 gene polymorphisms and disease severity in individuals infected with SARS-CoV-2 (Table 1). Notably, a study conducted by Sienko et al. demonstrated a significant correlation between the ACE2 receptor gene rs2074192 polymorphism and the severity of COVID-19 in adult patients [54]. The authors observed a strong association between the ACE2 rs2074192 TT-genotype and adverse outcomes in patients with severe forms of COVID-19 (p = 0.0016). These findings align with a separate study conducted by Cafiero et al., which reported a higher prevalence of the T-allele of ACE2 rs2074192 in symptomatic individuals compared to asymptomatic Italian patients [55].
Ma et al. investigated the association between rs2074192 and COVID-19 in the Chinese population, revealing a significant relationship (p < 0.05)[56]. Additionally, Molina et al. found that heterozygosity of rs2074192 SNPs in ACE2 was associated with disease severity caused by SARS-CoV-2, acting as a protective factor specifically in women.
2.2. IFNAR2
Interferons (IFNs) encompass a diverse group of cytokines that elicit various biological activities through the induction of thousands of interferon-stimulated genes (ISGs). These ISGs exhibit antiviral, antiproliferative, antiangiogenic, and immunomodulatory functions [60]. The antiviral response is amplified and disseminated by innate IFN types I and III (IFN-α/β and IFN-γ, respectively). While IFN-λ mainly acts on mucosal epithelium due to receptor expression constraints, IFN-α/β exerts its effects on all nucleated cells, making it indispensable in the antiviral defense mechanism [61,62,63].
The genetic association studies conducted during the coronavirus disease 2019 (COVID-19) outbreak has highlighted the notable involvement of IFNAR2 (Table 1). Pairo-Castineira et al., in collaboration with a group of researchers, carried out an extensive genome-wide association study known as GenOMICC (genetics of mortality in critical care). This study encompassed a cohort of 2,244 critically ill COVID-19 patients admitted to 208 intensive care units across the United Kingdom. The findings of this study demonstrated a significant association between the IFNAR2 rs2236757 gene variant and increased severity of the disease [19].
Likewise, various studies employing diverse methodologies have corroborated the significance of IFNAR2 as a crucial gene implicated in the severity of COVID-19 [64,65,66,67,68].
In their research, Fricke-Galindo et al. (2022) discovered a notable association between genetic polymorphisms of IFNAR2 (rs2236757, rs1051393, rs3153, rs2834158, and rs2229207) and an increased mortality risk in individuals afflicted with COVID-19 [20]. Intriguingly, the non-surviving group exhibited significantly lower levels of soluble receptors in comparison to the surviving group. These findings are consistent with previous studies that have elucidated the suppression of the IFN-I activation pathway by SARS-CoV-2, resulting in reduced levels of IFN-α and -β among COVID-19 patients [69,70,71]. Furthermore, the group of survivors displayed higher levels of sIFNAR2 in comparison to the non-survivors, indicating an augmented antiviral activity of IFN facilitated by the stability conferred by sIFNAR2 [20].
The findings from the investigation conducted by Dieter K. et al. (2022) [21] further support the existing body of research [19,20] by confirming the association between the rs2236757 genotype of IFNAR2 and an elevated risk of hospitalization in intensive care units and mortality among patients with COVID-19.
These results suggest that the rs2236757 polymorphism may contribute to reduced expression of IFNAR2, consequently predisposing individuals to more severe manifestations of COVID-19.
2.3. OAS
Following viral infection, the immune system initiates the production of antiviral cytokines, with interferons (IFNs) being particularly prominent. Among the IFN-stimulated genes, the 2´, 5´- oligoadenylate synthetases (OAS) family plays a crucial role in the innate immune response. OAS proteins exhibit antiviral functions by serving as nucleotidyltransferases, facilitating the oligomerization of ATP into 2´, 5- linked oligoadenylates (2-5A). This process leads to the activation of latent RNase L, which provides antiviral protection through the degradation of viral RNA [72,73,74,75]. The human OAS gene family comprises four genes, namely OAS1, OAS2, OAS3, and OAS-like (OASL), which are located on chromosome 12. Alternative splicing of these genes gives rise to 10 isoforms [76,77,78].
Several genome-wide association studies (GWASs) have identified various genetic variants at specific loci that are associated with susceptibility to COVID-19 (Table 1), either in general or in severe cases, when compared to controls from the general population [19,79].
One of the prominent variants identified within these loci is rs10774671 located at 12q24.13, which encompasses three genes responsible for encoding OAS enzymes, namely OAS1, OAS2, and OAS3 [19,79].
The investigation carried out by Banday et al. (2022) provided compelling evidence of the substantial influence of rs10774671 on the expression of OAS1, a crucial antiviral protein involved in the eradication of SARS-CoV-2, and its overall impact on the hospitalization outcomes of individuals with COVID-19 [80]. They propose that the functional impact of rs10774671 contributes to the association with COVID-19 severity by modulating the abundance of the OAS1 protein [80].
In a separate study, Pairo-Castineira et al. identified an association between the polymorphism OAS3 rs10735079 and the development of critical illness in individuals with COVID-19 [19].

Table 1.
Summary of commonly reported single nucleotide polymorphisms associated with susceptibility to COVID-19.
Table 1.
Summary of commonly reported single nucleotide polymorphisms associated with susceptibility to COVID-19.
| Gene | SNP | Patient # | SNP Effects | Significans | Features | Population | References |
|---|---|---|---|---|---|---|---|
| IFNAR2 | rs 2236757 G/A | 694 | Associated with severe forms of COVID-19 and increased mortality | p = 0,031 | In patients of non-white ethnicity, the presence of the A allele was linked to an increased risk of both intensive care unit (ICU*) admission and mortality | Brazil population | [21] |
| 2244 | Associated with severe forms of COVID-19 | p < 0,005 | The A allele demonstrated an association with an elevated risk of developing severe COVID-19. Additionally, lower expression of IFNAR2 was observed in individuals with life-threatening cases of COVID-19 | UK population | [19] | ||
| 1202 | Associated with mortality risk among patients with severe COVID-19 | p = 0,023 | N/A | Mexico population | [20] | ||
| ACE2 | rs 2074192 G/A | 318 | Associated with the disease severity caused by SARS-CoV-2 | p = 0,016 | Heterozygosity of rs2074192 was identified as a protective factor against COVID-19 infection in women | Spain population | [81] |
| rs 2074192 C/T | 104 | Correlated with more severe outcomes of SARS-CoV-2 infection | p = 0,0088 (for female) p < 0,0001 (for male) |
The T allele exhibited a higher prevalence in symptomatic patients compared to asymptomatic individuals | Italian population | [55] | |
| 293 | Was not associated with COVID-19 | p > 0,005 | The ACE2 rs2074192 variant does not confer a predisposition to the development of long-COVID symptoms in individuals who were previously hospitalized due to COVID-19 | Spain population | [59] | ||
| 191 | Was not associated with COVID-19 | p > 0,005 | N/A | China population | [58] | ||
| 481 | Was not associated with COVID-19 | Severe: p = 0,49 Critical: p = 0,6 |
N/A | Mexico population | [57] | ||
| 456 | Associated with COVID-19 | p < 0,001 | Rs2074192 may potentially correlate with susceptibility to COVID-19-related cardiovascular complications and acute inflammatory infections | China population | [56] | ||
| 188 | Associated with an increased risk of a more severe disease course of SARS-CoV-2 infection | p = 0,002 | A strong correlation was observed between the TT-genotype of ACE2 rs2074192 and unfavorable outcomes in individuals with severe forms of COVID-19 | [54] | |||
| OAS1 | rs10774671 A allele | 3084 | Associated with susceptibility to COVID-19 | Europeans: p < 0,005; Africans: p = 0,079 |
The presence of the A allele in rs10774671 may lead to decreased expression of OAS1, thereby increasing the specific human risk of developing severe COVID-19 | Europeans, Asians, Africans, African American, Hispanic | [80] |
| OAS3 | rs10735079 A/G | 2244 | Associated with severe forms of COVID-19 | p < 0,001 | N/A | UK population | [19] |
* ICU - intensive care unit;.
3. Genetic Polymorphisms Associated with Susceptibility to MAFLD
3.1. PNPLA3
An integral aspect of MAFLD pathogenesis involves the perturbation of lipid metabolism, resulting in the aberrant accumulation of lipids within the liver, specifically steatosis. The principal source of hepatic triglycerides (TG) arises from adipocytes-released free fatty acids (FFAs), which are facilitated by lipase enzymes [82,83]. Adipose triglyceride lipase (ATGL), encoded by the Patatin-like phospholipase domain containing 2 (PNPLA2) gene, represents a significant enzyme involved in this cascade. In 2008, a pioneering genome-wide association study (GWAS) investigating NAFLD patients, encompassing diverse cohorts of Hispanics, African Americans, and European Americans, revealed noteworthy findings [84]. Specifically, the presence of a genetic variant in Patatin-like phospholipase domain-containing 3 (PNPLA3), known as rs738409 or I148M, was linked to heightened lipid accumulation, even after adjusting for crucial factors such as ethnicity, body mass index (BMI), diabetes status, and alcohol consumption [84]. Furthermore, a range of studies conducted across distinct populations has further elucidated the impact of the I148M variant and other variants associated with NAFLD (Table 2).
Within the PNPLA3 gene, the production of adiponutrin, a triacylglycerol lipase, takes place, enabling the hydrolysis of triacylglycerols. However, the presence of the I148M variant has been shown to impede the enzymatic activity of this lipase, thereby fostering the onset of hepatic steatosis [85]. A recent meta-analysis investigating the impact of the I148M variant on NAFLD risk revealed that individuals carrying the minor G-allele had a 19% increased risk of developing NAFLD. Notably, the risk escalated to 105% among individuals harboring both GG alleles [86].
The I148M variant of PNPLA3 exhibits a comparable effect to more advanced stages of NAFLD. A meta-analysis encompassing 16 studies demonstrated that individuals carrying homozygous GG alleles have a 3.5-fold increased risk of developing NASH and a 3.2-fold elevated risk of experiencing fibrosis [87]. Furthermore, another meta-analysis revealed a significant association between the I148M variant and a 2.54-fold increased risk of NASH development [88]. Notably, a significant dose-dependent relationship of the G allele was observed concerning this risk [86,88]. Similarly, an association between the I148M variant and cirrhosis progression was also noted. Specifically, the presence of a single G allele conferred a 2-fold increased risk of developing cirrhosis, while individuals with homozygous GG alleles had a 3-fold higher risk compared to those with CC genotypes [89].
3.2. TM6SF2
The rs58542926 (E167K) variant, derived from the Transmembrane 6 superfamily, member 2 (TM6SF2) gene, represents another significant single nucleotide polymorphism (SNP) associated with NAFLD (Table 2). TM6SF2 is an endoplasmic reticulum (ER) transmembrane protein primarily expressed in hepatocytes, renal cells, and intestinal cells, playing a crucial role in the regulation of lipoprotein secretion [90]. The presence of the E167K variant disrupts the protein's functionality, leading to a loss of its normal function and subsequently reducing the secretion of very low-density lipoprotein (VLDL) [91]. This variant has been linked to an increased susceptibility to NAFLD, hepatic steatosis, and advanced fibrosis (Table 2), while its association with inflammation remains inconclusive [92,93,94]. Although the impact of the E167K variant is relatively modest when compared to the PNPLA3 I148M variant, individuals harboring both the I148M and E167K variants exhibit a synergistic or additive effect, resulting in a twofold or cumulative risk of developing NAFLD [95]. These findings suggest the existence of gene-gene interactions contributing to the pathogenesis of the disease.
The E167K variant is present in lean individuals with NAFLD, in addition to those who are obese or overweight [96]. This observation underscores the specific involvement of the E167K variant in the development of NAFLD. Notably, the majority of studies examining "lean" NAFLD cases have predominantly focused on Asian populations [97], which aligns with the higher prevalence of the E167K variant in East Asians. The minor T allele frequency of this variant is more prevalent in East Asian populations (~34%) compared to Europeans (~26%), Hispanics (~10%), and Africans (~6%) [98].
A study conducted by Liu et al. [99] demonstrated the potential impact of the TM6SF2 rs58542926 variant on fibrosis progression in NAFLD participants of European Caucasian descent. However, in contrast, Wong et al. [100] reported that the TM6SF2 rs58542926 variant did not contribute to the development of liver fibrosis or cirrhosis in Chinese individuals with NAFLD. These findings highlight the potential influence of genetic and ethnic variations on the association between the TM6SF2 variant and fibrosis progression in different populations.
In a recent exome-wide association study focusing on liver fat content, the TM6SF2 rs58542926 variant demonstrated a significant association with alanine aminotransferase (ALT) levels in both the Dallas Biobank and the Copenhagen Study. However, this variant did not show a statistically significant relationship with aspartate aminotransferase (AST) levels [39]. Nevertheless, these findings were not replicated in genome-wide association studies (GWASs) [101]. Conversely, certain GWASs have suggested a close association between the TM6SF2 rs58542926 variant and serum lipid levels [102,103].
In a meta-analysis conducted by Li et al., the TM6SF2 rs58542926 T allele was confirmed as a risk factor for the susceptibility and development of NAFLD and its associated metabolic phenotypes in both adults and children [93]. Interestingly, the rs58542926 T allele was found to be a protective factor for serum lipid levels. Notably, in this study, the risk of NAFLD associated with carrying the T allele was higher in children compared to adults. The effect size of the rs58542926 T allele was more pronounced in pediatric NAFLD than in adult NAFLD. Furthermore, their findings revealed that the rs58542926 variant was associated with the progression of steatosis, severe steatosis, fibrosis stages, and fibrosis progression in adults. However, there was no statistically significant difference observed in the fibrosis stages [93].
3.3. GCKR
The GCKR gene is responsible for encoding a glucokinase regulator that forms a complex with glucokinase and influences hepatic glucose storage and metabolism by directing its localization to the nucleus [104]. Any genetic variant that affects the functionality of the GCKR protein may contribute to the risk of NAFLD. In previous genome-wide association studies (GWAS) focusing on NAFLD, a common single nucleotide polymorphism (SNP) in the GCKR gene, namely rs780094, was identified and found to be associated with NAFLD [38]. This GWAS included 592 NAFLD patients with biopsy-proven cases from the NASH Clinical Research Network [38] and was the first to report the role of rs780094 in NAFLD. Furthermore, this study revealed a significant and robust association between rs780094 and lipid and glycemic traits. Subsequently, several genetic association studies have replicated and supported this association [43,105,106,107] (Table 2).
A meta-analysis conducted by Zain et al. examined the association of the GCKR rs780094 SNP with NAFLD, revealing a pooled effect of a 1.25-fold increased risk when comparing individuals carrying the T-allele with those carrying the C-allele [108]. This meta-analysis further demonstrated a significant association between rs780094 and NAFLD across different genetic models, including the dominant, recessive, and homozygote models [108].
The potential risk effect of the T-allele in NAFLD susceptibility has been observed in the initial studies, which reported a significant association between the rs780094-T-allele and an increased risk of NAFLD. While two studies conducted by Yang et al. [107] and Gorden et al. [43] did not find a statistically significant association between the T-allele and the risk of NAFLD, the direction of the effect and the effect size demonstrated similar trends to the findings of the GOLD's consortium [38]. It is worth noting that the pooled effective allele frequency exceeded 40% in each study population, emphasizing the substantial impact it can have on the risk of NAFLD.
In a comprehensive meta-analysis conducted by Li et al., which encompassed 25 studies with a total of 6,598 cases and 19,954 controls, the objective was to precisely evaluate the association between GCKR polymorphisms and the risk of NAFLD [109]. The pooled estimates from the analysis revealed a significant predisposition to NAFLD in individuals carrying the T allele of the GCKR rs780094 polymorphism [109].
3.4. LYPLAL1
The LYPLAL1 gene encodes a 26 kDa cytosolic protein known as lysophospholipase-like protein 1, which belongs to a subclass of the lysophospholipase family [110]. Several single nucleotide polymorphisms (SNPs) located near the LYPLAL1 gene have been found to exhibit a significant association with fat distribution, displaying a relatively sex-specific pattern [111]. In a large-scale genome-wide association study (GWAS) conducted by The Genetics of Obesity-Related Liver Disease Consortium, LYPLAL1 rs12137855 was identified as being associated with NAFLD in a cohort of 7,177 adults of European ancestry [38]. This variant was found to be linked to steatosis as defined by computed tomography, as well as biopsy-proven NAFLD characterized by lobular inflammation and fibrosis [38].
In a study conducted by Sliz et al., the influence of genetic polymorphisms on the risk of NAFLD was investigated. It was observed that the metabolic effects associated with LYPLAL1 rs12137855-C were similar, albeit statistically less robust, to those observed with GCKR rs1260326-T. These findings suggest that LYPLAL1 may contribute to the regulation of circulating and hepatic triglyceride levels by influencing hepatic glucose metabolism, similar to the role played by GCKR. This hypothesis is supported by the findings of Ahn et al., who demonstrated that inhibiting LYPLAL1 leads to an increase in glucose production in the hepatocytes of humans, rats, and mice [112].
Nevertheless, conflicting results have been reported regarding the impact of LYPLAL1 rs12137855 on NAFLD steatosis. Several studies [105,112,113,114,115] do not provide evidence supporting the association between LYPLAL1 rs12137855 and NAFLD steatosis. As such, among all the genetic polymorphisms discussed, the influence of LYPLAL1 rs12137855 on the development of NAFLD remains the most contentious and subject to debate.
Table 2.
Summary of Commonly Reported Single Nucleotide Polymorphisms Associated with Susceptibility to MAFLD.
Table 2.
Summary of Commonly Reported Single Nucleotide Polymorphisms Associated with Susceptibility to MAFLD.
| Gene | SNP | The number of patients | SNP Effects | Significance | Features | NAFLD diagnosed by | Population | Reference(s) |
|---|---|---|---|---|---|---|---|---|
| PNPLA3 | rs738409 C > G (I148M) | 9515 | Associated with NAFLD risk, steatosis and NASH | p > 0,001 | Hepatic fat content exhibited a more than twofold increase in PNPLA3-148M homozygotes compared to individuals without this genetic variant | H-MRS | African American; European American; Hispanic; | [84] |
| 1117 | Associated with steatosis and histological severity of NAFLD | p = 0,039 steatosis); p < 0,001 (portal inflammation);, p = 0.004 (NAS); p < 0.001 (fibrosis | The presence of the G allele in rs738409 was associated with the development of steatosis and greater histological severity of NAFLD. In pediatric patients, the high-risk G allele in rs738409 was linked to an earlier onset of the disease | Histologically | Americans (894 adults/223 children) | [116] | ||
| 1092 | Associated with steatosis and hepatocyte ballooning | p > 0,001 (steatosis); p=0,006 (ballooning); | PNPLA3 rs738409 G allele was correlated with liver steatosis and an elevated risk of progression from simple steatosis to NASH | Histologically | Americans | [43] | ||
| 126 | Increased the risk for NAFLD | p < 0,001 | The risk of NAFLD increased by 3,7-fold in subjects carrying the PNPLA3 GG genotype | Ultrasonography | Hispanic children | [117] | ||
| 1709 | Associated with NAFLD steatosis | p < 0,001 | The G allele was associated with elevated levels ALT, HOMA-IR*, and insulin | Magnetic resonance imaging (MRI) | African Americans; Japanese Americans; Latinos; Native Hawaiians; European Americans |
[118] | ||
| 7176 | Associated with NAFLD risk and steatosis | p < 0,001 (both) | N/A | CT, Histologically | European population | [38] | ||
| 417 | Associated with steatosis | p < 0,0001 | Individuals with the PNPLA3 GG genotype at rs738409 exhibited 2,7-fold higher liver fat content compared to those with the CC genotype | proton NMR (Proton nuclear magnetic resonance) | Finnish population | [119] | ||
| 405 | Associated with the ultrasonography-determined steatosis | p < 0,001 | The 148M allele was linked to reduced levels of LDL-C* in patients with NAFLD | Ultrasonography | Chinese population | [120] | ||
| 1027 | Associated with NAFLD and moderate-to-severe steatosis | p = 0,006 (NAFLD); p = 0,001 (steatosis). | The G-allele of PNPLA3 rs738409 exhibited an association with NAFLD and a 1,09 IU/L increase in ALT levels | Ultrasonography | Chinese children | [121] | ||
| 768 | Associated with NAFLD | p = 0.00087 | PNPLA3 GC and GG genotypes were significantly linked to an elevated risk of the disease | Ultrasonography | Chinese population. | [113] | ||
| 4300 | Associated with hepatic steatosis, and developed NAFLD and liver fibrosis | p <0,001 (NAFLD) |
Compared to CC homozygotes, GG homozygotes presented higher liver fat and liver fibrosis scores, despite having a better metabolic status (P < 0,05) | Ultrasonography | Chinese population | [122] | ||
| 879 | Associated with NAFLD and insulin resistance | p = 0,004 | The prevailing paradigm surrounding the PNPLA3 I148M (GG+GC) polymorphism indicates a positive correlation with elevated waist circumference, fasting insulin levels, HOMA-IR* scores, as well as higher concentrations of ALT and ferritin | Ultrasonography | Normoglycaemic population | [123] | ||
| 270 | Associated with NAFLD risk, steatosis, and fibrosis | p < 0,001 (NAFLD); p = 0,0003 (steatosis); p = 0,0445 (fibrosis) |
Characterized by a pattern of steatosis, inflammation, and fibrosis, which are interconnected factors | Histologically | German population (70 adolescents; 200 adult control cohort) | [124] | ||
| 515 | Associated with liver steatosis, and fibrosis | p < 0,001 (steatosis); p < 0,001 (fibrosis) |
The presence of the PNPLA3 risk allele exhibited heightened serum AST and ALT activities, with statistical significance observed at a p-value less than 0,05 | Histologically (320 biopsied patients) | German population | [125] | ||
| 1326 | Associated with steatosis, NAS* and fibrosis | p < 0,001 (NAFLD); p = 0,0016 (steatosis); p < 0,001 (NAS*) |
The PNPLA3 risk allele was found to be linked with elevated levels of AST and ALT in individuals diagnosed with NAFLD | Histologically and CT | Japanese population | [126] | ||
| 445 | Associated with NAFLD risk, steatosis, fibrosis, and cirrhosis | p < 0,001 (NAFLD) |
The ability to export VLDLs* from the liver is influenced by certain factors. | Ultrasonography | Italian population | [127] | ||
| 574 | Associated with the severity of steatosis and fibrosis and the presence of NASH | 95% CI = 1,04-1,76 (steatosis); CI = 1,12-2,04 (NASH) |
The G allele was observed to be disproportionately transmitted to children affected by the condition | Histologically | Italian (253) and United Kingdom (321) population | [128] | ||
| 246 | Associated with the risk of cirrhotic evolution | р < 0,001 | In the NAFLD population, each copy of the G allele was found to be associated with nearly a twofold increase in the risk of cirrhosis. Furthermore, individuals who were GG homozygous exhibited a tripled risk compared to those who were CC homozygous | Histologically | Italian population | [89] | ||
| 1380 | Associated with NAFLD risk, steatosis, NASH, fibrosis, cirrhosis and HCC* | p < 0,0001 (steatosis, NASH, fibrosis); p = 0,0007 (cirrhosis) |
Such results are caused by the co-presence of the 3 at-risk variants: rs738409 C>G (PNPLA3 I148M), rs58542926 C>T (TM6SF2 E167K), and rs641738 C>T MBOAT7 | Histologically | European population | [129] | ||
| 470 | Associated with NAFLD risk, steatosis and NASH | p < 0.001 (steatosis); p < 0,001 (lobular inflammation); p = 0,002 (ballooning) | The presence of specific features of steatohepatitis was found to be linked to the identified factor, but no significant associations were observed with liver fibrosis, anthropometry (body measurements), or insulin resistance | Histologically | Belgian population | [130] | ||
| 285 | Associated with NAFLD risk and NASH | p = 0,002 (NAFLD); p <0,001 (NASH) |
While the PNPLA3 genotype did not exhibit an association with the grade of steatosis, individuals with GG homozygosity had an increased likelihood of significant NASH activity and fibrosis | Ultrasonography | Brazilian population | [131] | ||
| 342 | Associated with NAFLD risk, NASH severity and fibrosis | p < 0,0001 (NAFLD); p < 0,0001 (NASH); p = 0,013 (fibrosis) |
No associations were identified between the PNPLA3 genotype and simple steatosis or other histological parameters | Histologically | Chinese, Indian and Malay | [132] | ||
| 365 | Associated with the development of NAFLD and the severity of liver histology | p = 0,002 (NAFLD development); p < 0,005 (NAFLD severity) |
Patients who possessed the PNPLA3 GG genotype exhibited higher levels of NAS* compared to those with the PNPLA3 CC genotype | Histologically | Turkish population | [133] | ||
| 225 | Associated with NAFLD and NASH risk, and fibrosis | p = 0,04 (NASH); p = 0,016 (fibrosis) |
The GG genotype demonstrated an association with decreased platelet counts | Histologically | Turkish population | [134] | ||
| 232 | Associated with NAFLD, fibrosis but not steatosis | 95% [CI] = 1,98-6,71 (NAFLD) |
No significant associations were found between the GG genotype and body mass index, triglyceride levels, high- and low-density lipoprotein levels, or diabetes, as well as the steatosis grade (with a p-value greater than 0,05) | Histologically | Chinese population | [135] | ||
| 904 | Associated with NAFLD in lean individuals | p = 0,003 (NAFLD) |
Among individuals diagnosed with (NAFLD, a higher frequency of lean subjects (30.3%) carried the PNPLA3 rs738409 GG genotype compared to overweight (17.9%) and obese subjects (17.4%) | Proton-magnetic resonance spectroscopy | Chinese population | [136] | ||
| 831 | Associated with NAFLD and fibrosis, but not steatosis | p < 0,0001 (NAFLD); p = 0,011 (fibrosis) |
The GG genotype was associated with elevated levels of AST (p = 0,00013), ALT (p < 0,0001), and ferritin (p = 0,014) | Histologically | Japanese population | [137] | ||
| 1461 | Associated with NAFLD and NASH | p < 0,0001 (NAFLD, NASH) | Was also linked to hyaluronic acid levels, HbA1c* levels, and iron deposition in the liver | Histologically | Japanese population | [138] | ||
| 339 | Associated with NAFLD and fibrosis | p = 0,028 (NAFLD); p = 0,01 (fibrosis) |
Within the NAFLD patient population, the frequency of CG+GG genotypes was significantly higher in individuals with advanced fibrosis | Ultrasonography | Korean population | [139] | ||
| 1363 | Associated with NAFLD | p < 0,0001 (NAFLD) | Carriers of the rs738409-G allele had a 1,19-fold increased risk for NAFLD and exhibited significantly lower levels of visceral and subcutaneous adiposity, body mass index, triglycerides, and insulin resistance compared to CC carriers | Ultrasonography and CT | Korean population | [140] | ||
| 244 | Associated with NAFLD, NASH risk. | p < 0,0005 (NAFLD); p < 0,05 (NASH) | N/A | Proton magnetic resonance spectroscopy | Indian population | [141] | ||
| 335 | Associated with NAFLD risk | p = 0,04 (NAFLD) | The presence of the G allele exhibited a significant association with higher levels of fasting insulin, HOMA-IR*, ALT, and AST values specifically among affected cases, while no such association was observed in the control group | Ultrasonography | Asian Indians | [142] | ||
| 200 | Associated with NAFLD risk and steatosis | p < 0,05 (steatosis) | Patients carrying the G allele demonstrated elevated levels of ALT, dyslipidemia, and insulin resistance | Ultrasonography | Indian population | [143] | ||
| 306 | Associated with NAFLD risk | p = 0,001 (NAFLD) | PNPLA3 gene polymorphism was found to be linked to higher levels of ALT | Ultrasonography | Indian population | [144] | ||
| 207 | Associated with NAFLD risk | p < 0,001 (NAFLD) | The PNPLA3 rs738409 gene polymorphism significantly increases the risk of NAFLD by up to four-fold in individuals with elevated triglyceride levels | Ultrasonography | Indian population | [145] | ||
| 224 | Associated with NAFLD, NASH, fibrosis, and cirrhosis. | p < 0,05 | The GG genotype exhibited a 20,25-fold higher odds of developing NAFLD, as well as a 6,53-fold higher odds of experiencing non-alcoholic steatohepatitis (NASH) | Ultrasonography | Indian population | [146] | ||
| 144 | Associated with MAFLD | p = 0,017 | In a multivariable analysis, hypertriglyceridemia, BMI, and the PNPLA3 GG genotype were identified as factors associated with MAFLD | CT, MRT | Chinese population. | [147] | ||
| 143 | Associated with NAFLD | p = 0,002 | The presence of PNPLA3 risk alleles impairs the response to dietary interventions in individuals diagnosed with NAFLD | Ultrasonography | German population | [148] | ||
| 525 | Associated with NASH and fibrosis | p = 0,008 (NASH); p = 0,020 (fibrosis) |
The PNPLA3 genotype showed an association with the HOMA-IR* and insulin resistance in adipose tissue | Histologically | Korean population | [149] | ||
| 211 | Associated with NAS* (NAFLD Activity Score) | NAS: ≤2 vs ≥3, p = 0,667; ≤4 vs ≥5, p = 0,034) |
The PNPLA3 genotype was found to have a partial impact on the NAFLD activity score |
Histologically | Japanese population | [150] | ||
| 4804 | Associated with steatosis | p = 0,01 | The presence of PNPLA3 variants was found to be associated with elevated levels of ALT | Ultrasonography | Non-Hispanic white, non-Hispanic black, and Mexican American participants in the US population | [151] | ||
| 797 | Associated with NAFLD | p = 0,008 | PNPLA3 variants may contribute to the susceptibility of NAFLD in obese individuals across various ethnic groups | Ultrasonography | Chinese children | [105] | ||
| 307 | Associated with NAFLD | p < 0,01 | No significant effect modification was observed with BMI | FibroScan | Mexican population | [114] | ||
| 382 | Associated with NAFLD, and fibrosis | p = 0,0044 (NAFLD); p = 0,0272 (fibrosis) |
Individuals with the PNPLA3 GG genotype had a significantly increased risk (3,29-fold) of developing NAFLD compared to those with the CC genotype | Histologically | Brazilian population | [152] | ||
| 349 | Increased the risk of NAFLD | p = 0,29 | Although the presence of the GG genotype showed a 1.39 times increased risk of NAFLD, this association did not reach statistical significance | Histologically and Ultrasonography | Turkey population | [153] | ||
| GCKR | rs780094 C > T | 1092 | Was not associated with NAFLD | p > 0,05 | The GCKR SNP rs780094 exhibited a significant association with elevated serum triglyceride levels (p = 0,04) | Histologically | American | [43] |
| 270 | Associated with NAFLD risk, steatosis, and especially fibrosis | p = 0,0281 (NAFLD); p = 0,0275 (fibrosis) |
In individuals with the rs738409 G/G genotype, proteome profiling analysis revealed a reduction in the levels of GCKR protein and a downregulation of the retinol pathway | Histologically | German population (70 adolescents; 200 adult control cohort) | [124] | ||
| 7176 | Associated with NAFLD risk and steatosis | p < 0,001 (NAFLD risk); p = 0,01 (steatosis) |
N/A | CT; Histologically | European population | [38] | ||
| 4804 | Associated with steatosis | p = 0,03 | Was associated with a high level of ALT | Ultrasonography | Non-Hispanic white, non-Hispanic black, and Mexican American participants in the US population | [151] | ||
| 366 | Associated with the severity of liver fibrosis | p < 0,001 | Associated with higher serum triglyceride levels (p = 0,02) | Histologically | Italian population | [154] | ||
| 797 | Associated with NAFLD | p = 0,008 | Associated with higher mean serum ALT concentration | Ultrasonography | Chinese children | [105] | ||
| 620 | Associated with NAFLD | 95% CI: 1,14-1,28 (NAFLD) | Demonstrated an association with specific dietary habits, such as the consumption of soda, eggs, and soybean. | Ultrasonography | Uyghur population | [115] | ||
| 342 | Associated with NAFLD, NASH, and fibrosis | p = 0,013 (NAFLD); р = 0,012 ( NASH); p = 0,038 ( fibrosis) |
The combined effect of GCKR and adiponutrin rs738409 indicated a substantially increased risk of NAFLD (p = 0,010) | Histologically | Malaysians (Malays, Chinese, and Indians) | [106] | ||
| 903 | Associated with NAFLD | p = 0,0072 | The T-allele of GCKR rs780094 showed a significant association with an elevation in fasting triglyceride levels | Ultrasonography | Chinese population | [107] | ||
| TM6SF2 | rs58542926 C>T | 768 | Associated with NAFLD | p = 0,0016 | The T allele of TM6SF2 rs58542926 showed a higher prevalence among subjects diagnosed with NAFLD | Ultrasonography | Chinese population | [113] |
| 515 | Associated with NAFLD risk and steatosis but not fibrosis | p = 0,003 (steatosis) | Associated with significantly increased AST but not ALT | Histologically (320 biopsied patients) | German population | [125] | ||
| 445 | Associated with NAFLD risk | p = 0,008 (NAFLD) | Affects the liver's ability to export very low-density lipoproteins (VLDLs) | Ultrasonography | Italian population | [127] | ||
| 1380 | Associated with NAFLD risk, steatosis, NASH, fibrosis, cirrhosis and HCC* | p < 0,0001 (steatosis, NASH, fibrosis); p = 0,0007 (cirrhosis) |
Such results are caused by the co-presence of the 3 at-risk variants: rs738409 C > G (PNPLA3 I148M), rs58542926 C>T (TM6SF2 E167K), and rs641738 C > T MBOAT7 | Histologically | European population | [129] | ||
| 3260 | Associated with NAFLD | p = 0,02 | No significant effect on inflammation was observed for the rs58542926 T allele | Histologically | International | [155] | ||
| 361 | Associated with NAFLD, steatosis and disease severity | p = 0,038 (NAFLD) | rs58542926 was not associated with levels of liver enzymes, lobular inflammation and fibrosis | Ultrasonography and Histologically | Argentina population | [101] | ||
| 300 | Associated with liver fat | p < 0,05 | Individuals with this variant exhibit preserved insulin sensitivity in relation to processes such as lipolysis and hepatic glucose production, and they do not typically experience hypertriglyceridemia | H-MRS | Finnish population | [156] | ||
| 143 | Associated with NAFLD | p = 0,041 | The presence of TM6SF2 risk alleles hinders the response to dietary interventions in individuals diagnosed with NAFLD | Ultrasonography | German population | [148] | ||
| 1010 | Associated with steatosis | p < 0,0001 (steatosis) | It is associated with higher levels of ALT and lower levels of total cholesterol, low-density lipoprotein cholesterol, triglycerides, and non-high-density lipoprotein cholesterol | Ultrasonography | Italian children | [157] | ||
| 878 | Associated with steatosis | p = 0,002 | Carriers of the TM6SF2 167K variant have a threefold increased risk of developing hepatic steatosis, which often manifests early in life | Ultrasonography | Italian children | [158] | ||
| 957 | Associated with NAFLD risk, steatosis and fibrosis | p = 0,05 (NAFLD); p < 0,05 (steatosis) |
Associated with high HFF% in Caucasians and African Americans, with high ALT levels in Hispanics and with a more favorable lipoprotein profile in Caucasians and Hispanics | Magnetic resonance imaging (MRI) and Histologically | Caucasians, African, Americans, and Hispanics children and adolescents | [42] | ||
| 1074 | Associated with NAFLD risk, steatosis, NASH, advanced hepatic fibrosis | p = 0,0008 (NAFLD); P < 0,001 (steatosis); p = 0,039 (NASH); p = 0,0074 (fibrosis) |
Carriage of the TM6SF2 variant does not appear to further increase HCC* risk independent of its effect on fibrosis stage | Histologically | Caucasians and Europeans | [99] | ||
| 316 | Associated with NAFLD risk and steatosis | p = 0,003 (NAFLD); p = 0.023 (steatosis) |
Associated with increased ALT but no other clinical parameters, such as AST, ALP* and lipids | FibroScan | Chinese population | [95] | ||
| 768 | Associated with NAFLD risk | p = 0,0007 | TM6SF2 167K allele was associated with NAFLD after adjustment for age, sex, body mass index and status of diabetes |
Ultrasonography | Chinese population | [159] | ||
| 1201 | Associated with NASH and fibrosis | p < 0,05 | Associated with more-severe steatosis, necroinflammation, ballooning, and fibrosis | Histologically | Italian, Finnish, and Swedish | [160] | ||
| 525 | Associated with NASH and fibrosis | p = 0.008 (NASH); p = 0.020 (fibrosis) |
Even after adjustment for metabolic risk factors rs58542926 increased the risk of NASH and significant fibrosis | Histologically | Korean population | [149] | ||
| 503 | Associated with NAFLD risk | p = 0,0004 | The presence of rs58542926 variant in the TM6SF2 gene exhibited a significant association with NAFLD, indicating a 2,7-fold higher risk of developing the condition | Ultrasonography | South Indians and North-East Indians | [161] | ||
| 285 | Was not associated with NAFLD risk | p = 0,78 | The presence of the T allele was not found to be associated with NAFLD or NASH, and it did not show any association with histological features related to these conditions | Ultrasonography | Brazilian population | [131] | ||
| 144 | Was not associated with NAFLD risk | p > 0,05 | There was no association between rs58542926 and liver steatosis (p = 0.62), ballooning (p = 0.14), lobular inflammation (p = 0.99) and fibrosis (p = 0.89) | CT, MRT | Chinese population | [147] | ||
| 211 | Was not associated with NAS | p > 0,05 | The TM6SF2 genotype did not affect the NAFLD activity score ( ≤ 2 vs ≥ 3, p = 0.867; ≤ 4 vs ≥ 5, p = 0,936) | Histologically | Japanese population | [150] | ||
| LYPLAL1 | rs12137855 C > T | 7176 | Associated with NAFLD risk and steatosis | p < 0,001; (NAFLD risk) | C-allele was associated with CT defined steatosis and biopsy-proven NAFLD | CT; Histologically | European | [38] |
| 797 | Was not associated with NAFLD | p > 0,05 | N/A | Ultrasonography | Chinese children | [105] | ||
| 307 | Was not associated with NAFLD | p > 0,05 | N/A | FibroScan | Mexican population | [114] | ||
| 620 | Was not associated with NAFLD | p > 0,05 | N/A | Ultrasonography | Uyghur population | [115] |
* LDL-C - low-density lipoprotein cholesterol; HOMA-IR - Homeostasis Model Assessment of Insulin Resistance; NAS - NAFLD activity score; VLDLs - very low-density lipoproteins; HCC - hepatocellular carcinoma; HbA1c - hemoglobin A1C; ALP - Alkaline Phosphatase; CT - computerized tomography.
4. The Influence of MAFLD-Associated Polymorphisms on the Severity of COVID-19
The COVID-19 pandemic has brought to light the association between NAFLD and increased susceptibility to severe SARS-CoV-2 infection [33,34,35,162].
Consequently, it has been hypothesized that genetic variants associated with NAFLD may indirectly influence the severity of COVID-19 infection. This intriguing hypothesis has motivated investigations into candidate genes through association studies. One such study utilized the UK Biobank dataset to develop a genetic risk score for NAFLD, considering the combined effects of variants involved in hepatic fat accumulation (PNPLA3-TM6SF2-MBOAT7-GCKR) [45]. Building upon this knowledge, Valenti et al. examined the impact of this NAFLD-genetic risk score on the susceptibility to COVID-19 and observed a trend suggesting that the rs738409 variant conferred protection against COVID-19 [45].
Grimaudo et al. conducted a study that revealed a significant association between the rs738409 G-allele and severe COVID-19 outcomes in patients aged 65 years or younger [44].
In contrast, Innes et al. reported a striking inverse association between rs738409 and the severity of COVID-19 outcomes in a cohort of 1585 participants from the UK Biobank [46]. Their findings indicated that the rs738409-G allele was independently associated with a reduced risk of COVID-19 hospitalization and mortality. Importantly, this protective effect persisted even after adjusting for major demographic factors and underlying metabolic and liver co-morbidities [46].
From a functional perspective, the observed association between lipid metabolism and the immune response to COVID-19 could be attributed to various factors. For instance, retinoids are stored as retinyl esters in hepatic mesenchymal cells and adipose tissue, where the PNPLA3 gene is expressed. When the need arises, retinoids are mobilized to extrahepatic tissues, where they play a crucial role in stimulating the production of interferon type 1, a potent cytokine response to viral infections [163]. Conversely, certain risk factors associated with severe COVID-19, such as obesity and liver disease [164], are known to be linked to decreased retinoid levels and impaired retinoid signaling. This impairment could potentially limit the availability of retinoids during infection. Moreover, individuals with the rs738409 G allele may exhibit a lower ratio of omega-6 to omega-3 polyunsaturated fatty acids, which has been implicated in modulating inflammation and providing protection against cytokine storm syndrome [165].
Furthermore, Innes et al. [46] conducted a comprehensive meta-analysis encompassing three distinct data sources to explore the potential relationship between the rs738409 variant and COVID-19. The study incorporated data from the FinnGen study, which consisted of 83 individuals with COVID-19 hospital admissions and 274 SARS-CoV-2-positive patients without hospital admission. Additionally, the Geisinger Health System dataset included 854 subjects of European Ancestry, with 165 individuals experiencing COVID-19 hospitalization and 689 SARS-CoV-2-positive patients without hospital admission. Lastly, the study by Grimaudo et al. contributed data from a total of 383 COVID-19 patients [44]. The pooled analysis of these aforementioned data sources revealed that the presumed protective effect of the G "NASH-risk allele" on COVID-19 morbidity and mortality could not be definitively confirmed. Nevertheless, there was a discernible trend suggesting an association with a reduced risk of COVID-19 hospitalization and severe disease, although this trend did not reach statistical significance [46].
Similarly, Bianco et al. conducted a study examining the potential impact of the rs738409 G allele on COVID-19 outcomes. Their findings indicated that this allele exhibited a tendency not only to be associated with protection against COVID-19 but also with lower levels of C-reactive protein, despite higher ALT and lower albumin levels in severe COVID-19 patients of European ancestry [47].
Currently, the body of research investigating the influence of genetic polymorphisms associated with NAFLD on the progression and severity of coronavirus disease remains limited (Table 3). However, these studies shed light on the potential interplay between NAFLD-related genetic variants and the course of COVID-19. Further investigations are warranted to elucidate the underlying mechanisms and determine the clinical implications of these associations.
5. How do MAFLD-Associated Polymorphisms Affect Gene Expression in Different Tissues?
Understanding the causality between genotypes and phenotypes provides valuable insights into the genes and their interactions that contribute to the expression of specific traits in organisms. This is particularly relevant for comprehending complex traits that result from the combined effects of multiple genes and environmental factors.
Currently, the investigation of expression quantitative trait loci (eQTLs) represents a prominent and extensively explored avenue for understanding the functional consequences of genetic variation [166]. Numerous genetic studies focusing on gene expression have successfully identified thousands of eQTLs across diverse tissue types, encompassing a large proportion of human genes.
The comprehensive collection of eQTLs serves as a valuable tool for exploring the underlying molecular mechanisms of prevalent genetic disorders [167,168].
Our current knowledge of gene expression genetics heavily relies on the identification of eQTLs, which represent the associations between gene expression levels and specific genotypes at particular genomic loci. Genome-wide investigations of eQTLs have revealed that these loci contribute significantly to the variation in gene expression, with certain genes exhibiting up to 90% of their expression variation attributable to nucleotide variants.
By utilizing the eQTL database available at http://www.mulinlab.org/qtlbase/index.html, we can examine whether the four aforementioned SNPs exhibit eQTL effects in various tissue types. Selected findings are presented in Table 4 for reference. Notably, these data shed light on the potential impact of single nucleotide polymorphisms within the GCKR (rs780094), PNPLA3 (rs738409), TM6SF2 (rs58542926), and LYPLAL1 (rs12137855) genes on gene expression patterns in immune cells and blood (Figure 2). This implies that these genetic variants could potentially influence the immune response against infectious diseases, including COVID-19.
In light of these findings, it is evident that these genetic polymorphisms hold promise as prospective targets for future research endeavors. Their potential influence on gene expression, particularly in immune cells and blood, suggests their potential involvement in modulating the immune response to infectious diseases, including COVID-19. As such, investigating the functional implications of these genetic variants could provide valuable insights into disease susceptibility, pathogenesis, and therapeutic strategies. Therefore, further exploration of these genetic polymorphisms is warranted to deepen our understanding of their role and potentially identify novel avenues for therapeutic interventions.
6. Conclusions
The available genetic data thus far do not provide strong evidence for a significant predisposition conferred by MAFLD to the development of severe COVID-19. However, the COVID-19 pandemic has underscored the importance of obtaining a comprehensive understanding of not only the associations attributed to the PNPLA3 gene with liver-related traits but also the intricate protein interactions, active protein ligands, and, crucially, the accurate and comprehensive assessment of the variant pleiotropic effects.
Considering these factors, we advocate for a comprehensive approach to evaluating polymorphisms of the host's genetic determinants, particularly those associated with susceptibility to MAFLD. This approach should aim to develop gene profiling tools that can support early prediction at the individual level during the course of COVID-19. If confirmed as determinants of disease severity, these host polymorphisms could enable the identification of vulnerable populations or patients at higher risk for severe outcomes, thereby facilitating improved diagnosis, treatment, and prognosis of COVID-19.
Author Contributions
Conceptualization, and writing—original draft preparation, M.B. and A.K.; writing—review and editing, M.B., V.O., I.K., and S.G.V.; supervision, A.K., V.O. and S.G.V; project administration, V.O. and A.K.; visualization, I.K.; funding acquisition, M.B. and V.O. All authors have read and agreed to the published version of the manuscript.
Funding
RECOOP Grant #36 – CSMC Senior Scientists (RCSS) "Comprehensive Analysis of Genetic Predictors for MAFLD Development in patients with COVID-19".
Data Availability Statement
Data is contained within the article or supplementary material.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization WHO Coronavirus Disease (COVID-19) Dashboard With Vaccination Data | WHO Coronavirus (COVID-19) Dashboard With Vaccination Data. World Heal. Organ. 2021, 1–5.
- Rapp, J.L.; Lieberman-Cribbin, W.; Tuminello, S.; Taioli, E. Male Sex, Severe Obesity, Older Age, and Chronic Kidney Disease Are Associated With COVID-19 Severity and Mortality in New York City. Chest 2021, 159, 112–115. [Google Scholar] [CrossRef]
- Zhang, J. jin; Cao, Y. yuan; Tan, G.; Dong, X.; Wang, B. chen; Lin, J.; Yan, Y. qin; Liu, G. hui; Akdis, M.; Akdis, C.A.; et al. Clinical, Radiological, and Laboratory Characteristics and Risk Factors for Severity and Mortality of 289 Hospitalized COVID-19 Patients. Allergy Eur. J. Allergy Clin. Immunol. 2021, 76, 533–550. [Google Scholar] [CrossRef] [PubMed]
- Ebinge, J.E.; Achamallah, N.; Ji, H.; Clagget, B.L.; Sun, N.; Botting, P.; Nguyen, T.T.; Luong, E.; Ki, E.H.; Park, E.; et al. Pre-Existing Traits Associated with COVID-19 Illness Severity. PLoS One 2020, 15. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors Associated with COVID-19-Related Death Using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk Factors for Severity and Mortality in Adult COVID-19 Inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Kamyshnyi, A.; Krynytska, I.; Matskevych, V.; Marushchak, M.; Lushchak, O. Arterial Hypertension as a Risk Comorbidity Associated with COVID-19 Pathology. Int. J. Hypertens. 2020, 2020, 8019360. [Google Scholar] [CrossRef]
- Gao, F.; Zheng, K.I.; Wang, X.B.; Sun, Q.F.; Pan, K.H.; Wang, T.Y.; Chen, Y.P.; Targher, G.; Byrne, C.D.; George, J.; et al. Obesity Is a Risk Factor for Greater COVID-19 Severity. Diabetes Care 2020, 43, E72–E74. [Google Scholar] [CrossRef]
- Valentino, M.S.; Marzuillo, P.; Esposito, C.; Bartiromo, M.; Nardolillo, M.; Villani, A.V.; Maresca, A.; Furcolo, G.; Guarino, S.; Miraglia Del Giudice, E.; et al. The Impact of COVID-19 Pandemic Lockdown on the Relationship between Pediatric MAFLD and Renal Function. J. Clin. Med. 2023, 12. [Google Scholar] [CrossRef]
- You, J.H.; Lee, S.A.; Chun, S.Y.; Song, S.O.; Lee, B.W.; Kim, D.J.; Boyko, E.J. Clinical Outcomes of COVID-19 Patients with Type 2 Diabetes: A Population-Based Study in Korea. Endocrinol. Metab. 2020, 35, 901–908. [Google Scholar] [CrossRef]
- Dennis, J.M.; Mateen, B.A.; Sonabend, R.; Thomas, N.J.; Patel, K.A.; Hattersley, A.T.; Denaxas, S.; McGovern, A.P.; Vollmer, S.J. Type 2 Diabetes and COVID-19– Related Mortality in the Critical Care Setting: A National Cohort Study in England, March–July 2020. Diabetes Care 2021, 44, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Petakh, P.; Kamyshna, I.; Nykyforuk, A.; Yao, R.; Imbery, J.F.; Oksenych, V.; Korda, M.; Kamyshnyi, A. Immunoregulatory Intestinal Microbiota and COVID-19 in Patients with Type Two Diabetes: A Double-Edged Sword. Viruses 2022, 14. [Google Scholar] [CrossRef]
- Kamyshnyi, O.; Matskevych, V.; Lenchuk, T.; Strilbytska, O.; Storey, K.; Lushchak, O. Metformin to Decrease COVID-19 Severity and Mortality: Molecular Mechanisms and Therapeutic Potential. Biomed. Pharmacother. 2021, 144, 112230. [Google Scholar] [CrossRef]
- Sinha, P.; Matthay, M.A.; Calfee, C.S. Is a “Cytokine Storm” Relevant to COVID-19? JAMA Intern. Med. 2020, 180, 1152–1154. [Google Scholar] [CrossRef] [PubMed]
- de la Rica, R.; Borges, M.; Gonzalez-Freire, M. COVID-19: In the Eye of the Cytokine Storm. Front. Immunol. 2020, 11, 558898. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; et al. A Familial Cluster of Pneumonia Associated with the 2019 Novel Coronavirus Indicating Person-to-Person Transmission: A Study of a Family Cluster. Lancet (London, England) 2020, 395, 514–523. [Google Scholar] [CrossRef]
- Baj, J.; Karakuła-Juchnowicz, H.; Teresiński, G.; Buszewicz, G.; Ciesielka, M.; Sitarz, R.; Forma, A.; Karakuła, K.; Flieger, W.; Portincasa, P.; et al. COVID-19: Specific and Non-Specific Clinical Manifestations and Symptoms: The Current State of Knowledge. J. Clin. Med. 2020, 9. [Google Scholar] [CrossRef]
- Fricke-Galindo, I.; Falfán-Valencia, R. Genetics Insight for COVID-19 Susceptibility and Severity: A Review. Front. Immunol. 2021, 12, 622176. [Google Scholar] [CrossRef]
- Pairo-Castineira, E.; Clohisey, S.; Klaric, L.; Bretherick, A.D.; Rawlik, K.; Pasko, D.; Walker, S.; Parkinson, N.; Fourman, M.H.; Russell, C.D.; et al. Genetic Mechanisms of Critical Illness in COVID-19. Nat. 2020 5917848 2020, 591, 92–98. [Google Scholar] [CrossRef]
- Negi, K.; Agarwal, M.; Pahuja, I.; Bhardwaj, B.; Rawat, M.; Bhaskar, A.; Dwivedi, V.P. Combating the Challenges of COVID-19 Pandemic: Insights into Molecular Mechanisms, Immune Responses and Therapeutics against SARS-CoV-2. Oxford open Immunol. 2023, 4, iqad001. [Google Scholar] [CrossRef]
- Fricke-Galindo, I.; Martínez-Morales, A.; Chávez-Galán, L.; Ocaña-Guzmán, R.; Buendía-Roldán, I.; Pérez-Rubio, G.; Hernández-Zenteno, R. de J.; Verónica-Aguilar, A.; Alarcón-Dionet, A.; Aguilar-Duran, H.; et al. IFNAR2 Relevance in the Clinical Outcome of Individuals with Severe COVID-19. Front. Immunol. 2022, 13, 949413. [Google Scholar] [CrossRef]
- Dieter, C.; de Almeida Brondani, L.; Lemos, N.E.; Schaeffer, A.F.; Zanotto, C.; Ramos, D.T.; Girardi, E.; Pellenz, F.M.; Camargo, J.L.; Moresco, K.S.; et al. Polymorphisms in ACE1, TMPRSS2, IFIH1, IFNAR2, and TYK2 Genes Are Associated with Worse Clinical Outcomes in COVID-19. Genes (Basel). 2022, 14. [Google Scholar] [CrossRef]
- Sadler, A.J.; Williams, B.R.G. Interferon-Inducible Antiviral Effectors. Nat. Rev. Immunol. 2008, 8, 559–568. [Google Scholar] [CrossRef]
- Kerr, I.M.; Brown, R.E.; Hovanessian, A.G. Nature of Inhibitor of Cell-Free Protein Synthesis Formed in Response to Interferon and Double-Stranded RNA. Nature 1977, 268, 540–542. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, Y.; Wu, L.; Niu, S.; Song, C.; Zhang, Z.; Lu, G.; Qiao, C.; Hu, Y.; Yuen, K.-Y.; et al. Structural and Functional Basis of SARS-CoV-2 Entry by Using Human ACE2. Cell 2020, 181, 894–904.e9. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Shevchuk, O.; Pak, A.; Palii, S.; Ivankiv, Y.; Kozak, K.; Korda, M.; Vari, S.G. Blood ACE2 Protein Level Correlates with COVID-19 Severity. Severity 2023. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wai-Sun Wong, V.; Dufour, J.-F.; Schattenberg, J.M.; et al. A New Definition for Metabolic Dysfunction-Associated Fatty Liver Disease: An International Expert Consensus Statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; Sanyal, A.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease-Meta-Analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef]
- Powell, E.E.; Wong, V.W.-S.; Rinella, M. Non-Alcoholic Fatty Liver Disease. Lancet (London, England) 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Wong, G.L.-H.; Woo, J.; Abrigo, J.M.; Chan, C.K.-M.; Shu, S.S.-T.; Leung, J.K.-Y.; Chim, A.M.-L.; Kong, A.P.-S.; Lui, G.C.-Y.; et al. Impact of the New Definition of Metabolic Associated Fatty Liver Disease on the Epidemiology of the Disease. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2021, 19, 2161–2171.e5. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, Y.; Byrne, C.D.; Musso, G. A Single-Letter Change in an Acronym: Signals, Reasons, Promises, Challenges, and Steps Ahead for Moving from NAFLD to MAFLD. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 345–352. [Google Scholar] [CrossRef]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global Perspectives on Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef]
- Ji, D.; Qin, E.; Xu, J.; Zhang, D.; Cheng, G.; Wang, Y.; Lau, G. Non-Alcoholic Fatty Liver Diseases in Patients with COVID-19: A Retrospective Study. J. Hepatol. 2020, 73, 451–453. [Google Scholar] [CrossRef]
- Hegyi, P.J.; Váncsa, S.; Ocskay, K.; Dembrovszky, F.; Kiss, S.; Farkas, N.; Erőss, B.; Szakács, Z.; Hegyi, P.; Pár, G. Metabolic Associated Fatty Liver Disease Is Associated With an Increased Risk of Severe COVID-19: A Systematic Review With Meta-Analysis. Front. Med. 2021, 8, 626425. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Hussain, S.; Antony, B. Non-Alcoholic Fatty Liver Disease and Clinical Outcomes in Patients with COVID-19: A Comprehensive Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 813–822. [Google Scholar] [CrossRef]
- Tao, Z.; Li, Y.; Cheng, B.; Zhou, T.; Gao, Y. Risk of Severe COVID-19 Increased by Metabolic Dysfunction-Associated Fatty Liver Disease: A Meta-Analysis. J. Clin. Gastroenterol. 2021, 55, 830. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, Y.; Duan, G.; Yang, H. NAFLD Was Independently Associated with Severe COVID-19 among Younger Patients Rather than Older Patients: A Meta-Analysis. J. Hepatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Mushtaq, K.; Khan, M.U.; Iqbal, F.; Alsoub, D.H.; Chaudhry, H.S.; Ata, F.; Iqbal, P.; Elfert, K.; Balaraju, G.; Almaslamani, M.; et al. NAFLD Is a Predictor of Liver Injury in COVID-19 Hospitalized Patients but Not of Mortality, Disease Severity on the Presentation or Progression – The Debate Continues. J. Hepatol. 2021, 74, 482–484. [Google Scholar] [CrossRef] [PubMed]
- Buchynskyi, M.; Kamyshna, I.; Oksenych, V.; Zavidniuk, N.; Kamyshnyi, A. The Intersection of COVID-19 and Metabolic-Associated Fatty Liver Disease: An Overview of the Current Evidence. Viruses 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Pirola, C.J.; Sookoian, S. COVID-19 and Non-Alcoholic Fatty Liver Disease: Biological Insights from Multi-Omics Data. Liver Int. 2023, 43, 580–587. [Google Scholar] [CrossRef] [PubMed]
- Speliotes, E.K.; Yerges-Armstrong, L.M.; Wu, J.; Hernaez, R.; Kim, L.J.; Palmer, C.D.; Gudnason, V.; Eiriksdottir, G.; Garcia, M.E.; Launer, L.J.; et al. Genome-Wide Association Analysis Identifies Variants Associated with Nonalcoholic Fatty Liver Disease That Have Distinct Effects on Metabolic Traits. PLoS Genet. 2011, 7, e1001324. [Google Scholar] [CrossRef] [PubMed]
- Kozlitina, J.; Smagris, E.; Stender, S.; Nordestgaard, B.G.; Zhou, H.H.; Tybjærg-Hansen, A.; Vogt, T.F.; Hobbs, H.H.; Cohen, J.C. Exome-Wide Association Study Identifies a TM6SF2 Variant That Confers Susceptibility to Nonalcoholic Fatty Liver Disease. Nat. Genet. 2014, 46, 352–356. [Google Scholar] [CrossRef]
- Holmen, O.L.; Zhang, H.; Fan, Y.; Hovelson, D.H.; Schmidt, E.M.; Zhou, W.; Guo, Y.; Zhang, J.; Langhammer, A.; Løchen, M.-L.; et al. Systematic Evaluation of Coding Variation Identifies a Candidate Causal Variant in TM6SF2 Influencing Total Cholesterol and Myocardial Infarction Risk. Nat. Genet. 2014, 46, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Santoro, N.; Zhang, C.K.; Zhao, H.; Pakstis, A.J.; Kim, G.; Kursawe, R.; Dykas, D.J.; Bale, A.E.; Giannini, C.; Pierpont, B.; et al. Variant in the Glucokinase Regulatory Protein (GCKR) Gene Is Associated with Fatty Liver in Obese Children and Adolescents. Hepatology 2012, 55, 781–789. [Google Scholar] [CrossRef]
- Goffredo, M.; Caprio, S.; Feldstein, A.E.; D’Adamo, E.; Shaw, M.M.; Pierpont, B.; Savoye, M.; Zhao, H.; Bale, A.E.; Santoro, N. Role of TM6SF2 Rs58542926 in the Pathogenesis of Nonalcoholic Pediatric Fatty Liver Disease: A Multiethnic Study. Hepatology 2016, 63, 117–125. [Google Scholar] [CrossRef]
- Gorden, A.; Yang, R.; Yerges-Armstrong, L.M.; Ryan, K.A.; Speliotes, E.; Borecki, I.B.; Harris, T.B.; Chu, X.; Wood, G.C.; Still, C.D.; et al. Genetic Variation at NCAN Locus Is Associated with Inflammation and Fibrosis in Non-Alcoholic Fatty Liver Disease in Morbid Obesity. Hum. Hered. 2013, 75, 34–43. [Google Scholar] [CrossRef]
- Parisinos, C.A.; Wilman, H.R.; Thomas, E.L.; Kelly, M.; Nicholls, R.C.; McGonigle, J.; Neubauer, S.; Hingorani, A.D.; Patel, R.S.; Hemingway, H.; et al. Genome-Wide and Mendelian Randomisation Studies of Liver MRI Yield Insights into the Pathogenesis of Steatohepatitis. J. Hepatol. 2020, 73, 241–251. [Google Scholar] [CrossRef]
- Grimaudo, S.; Amodio, E.; Pipitone, R.M.; Maida, C.M.; Pizzo, S.; Prestileo, T.; Tramuto, F.; Sardina, D.; Vitale, F.; Casuccio, A.; et al. PNPLA3 and TLL-1 Polymorphisms as Potential Predictors of Disease Severity in Patients With COVID-19. Front. cell Dev. Biol. 2021, 9, 627914. [Google Scholar] [CrossRef]
- Valenti, L.; Jamialahmadi, O.; Romeo, S. Lack of Genetic Evidence That Fatty Liver Disease Predisposes to COVID-19. J. Hepatol. 2020, 73, 709–711. [Google Scholar] [CrossRef] [PubMed]
- Innes, H.; Buch, S.; Barnes, E.; Hampe, J.; Marjot, T.; Stickel, F. The Rs738409 G Allele in PNPLA3 Is Associated With a Reduced Risk of COVID-19 Mortality and Hospitalization. Gastroenterology 2021, 160, 2599–2601.e2. [Google Scholar] [CrossRef] [PubMed]
- Bianco, C.; Baselli, G.; Malvestiti, F.; Santoro, L.; Pelusi, S.; Manunta, M.; Grasselli, G.; Bandera, A.; Scudeller, L.; Prati, D.; et al. Genetic Insight into COVID-19-Related Liver Injury. Liver Int. Off. J. Int. Assoc. Study Liver 2021, 41, 227–229. [Google Scholar] [CrossRef] [PubMed]
- Li, F. Receptor Recognition and Cross-Species Infections of SARS Coronavirus. Antiviral Res. 2013, 100, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Cui, N.; Tong, H.; Li, Y.; Ge, Y.; Shi, Y.; Lv, P.; Zhao, X.; Zhang, J.; Fu, G.; Zhou, Y.; et al. Role of Prealbumin in Predicting the Prognosis of Severely and Critically Ill COVID-19 Patients. Am. J. Trop. Med. Hyg. 2021, 105, 718–726. [Google Scholar] [CrossRef]
- Liu, C.; Li, Y.; Guan, T.; Lai, Y.; Shen, Y.; Zeyaweiding, A.; Zhao, H.; Li, F.; Maimaiti, T. ACE2 Polymorphisms Associated with Cardiovascular Risk in Uygurs with Type 2 Diabetes Mellitus. Cardiovasc. Diabetol. 2018, 17, 127. [Google Scholar] [CrossRef]
- Pouladi, N.; Abdolahi, S. Investigating the ACE2 Polymorphisms in COVID-19 Susceptibility: An in Silico Analysis. Mol. Genet. genomic Med. 2021, 9, e1672. [Google Scholar] [CrossRef]
- Zhang, P.; Zhu, L.; Cai, J.; Lei, F.; Qin, J.-J.; Xie, J.; Liu, Y.-M.; Zhao, Y.-C.; Huang, X.; Lin, L.; et al. Association of Inpatient Use of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Receptor Blockers With Mortality Among Patients With Hypertension Hospitalized With COVID-19. Circ. Res. 2020, 126, 1671–1681. [Google Scholar] [CrossRef]
- Hamet, P.; Pausova, Z.; Attaoua, R.; Hishmih, C.; Haloui, M.; Shin, J.; Paus, T.; Abrahamowicz, M.; Gaudet, D.; Santucci, L.; et al. SARS-CoV-2 Receptor ACE2 Gene Is Associated with Hypertension and Severity of COVID 19: Interaction with Sex, Obesity, and Smoking. Am. J. Hypertens. 2021, 34, 367–376. [Google Scholar] [CrossRef]
- Sienko, J.; Marczak, I.; Kotowski, M.; Bogacz, A.; Tejchman, K.; Sienko, M.; Kotfis, K. Association of ACE2 Gene Variants with the Severity of COVID-19 Disease-A Prospective Observational Study. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Cafiero, C.; Rosapepe, F.; Palmirotta, R.; Re, A.; Ottaiano, M.P.; Benincasa, G.; Perone, R.; Varriale, E.; D’Amato, G.; Cacciamani, A.; et al. Angiotensin System Polymorphisms’ in SARS-CoV-2 Positive Patients: Assessment Between Symptomatic and Asymptomatic Patients: A Pilot Study. Pharmgenomics. Pers. Med. 2021, 14, 621–629. [Google Scholar] [CrossRef]
- Ma, Y.; Li, Q.; Chen, J.; Liu, S.; Liu, S.; He, X.; Ling, Y.; Zheng, J.; Corpe, C.; Lu, H.; et al. Angiotensin-Converting Enzyme 2 SNPs as Common Genetic Loci and Optimal Early Identification Genetic Markers for COVID-19. Pathog. (Basel, Switzerland) 2022, 11. [Google Scholar] [CrossRef]
- Martínez-Gómez, L.E.; Herrera-López, B.; Martinez-Armenta, C.; Ortega-Peña, S.; Camacho-Rea, M.D.C.; Suarez-Ahedo, C.; Vázquez-Cárdenas, P.; Vargas-Alarcón, G.; Rojas-Velasco, G.; Fragoso, J.M.; et al. ACE and ACE2 Gene Variants Are Associated With Severe Outcomes of COVID-19 in Men. Front. Immunol. 2022, 13, 812940. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zou, H.; Corpe, C. An Observed Association between Angiotensin-Converting Enzyme 2 Polymorphisms and COVID-19 Severity in China. J. Infect. 2022, 84, e21–e22. [Google Scholar] [CrossRef]
- Fernández-de-Las-Peñas, C.; Arendt-Nielsen, L.; Díaz-Gil, G.; Gómez-Esquer, F.; Gil-Crujera, A.; Gómez-Sánchez, S.M.; Ambite-Quesada, S.; Palomar-Gallego, M.A.; Pellicer-Valero, O.J.; Giordano, R. Genetic Association between ACE2 (Rs2285666 and Rs2074192) and TMPRSS2 (Rs12329760 and Rs2070788) Polymorphisms with Post-COVID Symptoms in Previously Hospitalized COVID-19 Survivors. Genes (Basel). 2022, 13. [Google Scholar] [CrossRef] [PubMed]
- Takaoka, A. Interferons. Handb. Horm. Comp. Endocrinol. Basic Clin. Res. 2021, 447–452. [Google Scholar] [CrossRef]
- Duncan, C.J.A.; Mohamad, S.M.B.; Young, D.F.; Skelton, A.J.; Leahy, T.R.; Munday, D.C.; Butler, K.M.; Morfopoulou, S.; Brown, J.R.; Hubank, M.; et al. Human IFNAR2 Deficiency: Lessons for Antiviral Immunity. Sci. Transl. Med. 2015, 7, 307ra154. [Google Scholar] [CrossRef] [PubMed]
- Buchynskyi, M.; Kamyshna, I.; Lyubomirskaya, K.; Moshynets, O.; Kobyliak, N.; Oksenych, V.; Kamyshnyi, A. Efficacy of Interferon Alpha for the Treatment of Hospitalized Patients with COVID-19: A Meta-Analysis. Front. Immunol. 2023, 14, 250. [Google Scholar] [CrossRef]
- Kamyshnyi, A.; Koval, H.; Kobevko, O.; Buchynskyi, M.; Oksenych, V.; Kainov, D.; Lyubomirskaya, K.; Kamyshna, I.; Potters, G.; Moshynets, O. Therapeutic Effectiveness of Interferon-A2b against COVID-19 with Community-Acquired Pneumonia: The Ukrainian Experience. Int. J. Mol. Sci. 2023, 24. [Google Scholar] [CrossRef]
- Liu, D.; Yang, J.; Feng, B.; Lu, W.; Zhao, C.; Li, L. Mendelian Randomization Analysis Identified Genes Pleiotropically Associated with the Risk and Prognosis of COVID-19. J. Infect. 2021, 82, 126–132. [Google Scholar] [CrossRef]
- Liu, B.M.; Hill, H.R. Role of Host Immune and Inflammatory Responses in COVID-19 Cases with Underlying Primary Immunodeficiency: A Review. J. Interf. cytokine Res. Off. J. Int. Soc. Interf. Cytokine Res. 2020, 40, 549–554. [Google Scholar] [CrossRef] [PubMed]
- Baranova, A.; Cao, H.; Zhang, F. Unraveling Risk Genes of COVID-19 by Multi-Omics Integrative Analyses. Front. Med. 2021, 8, 738687. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Zhu, J.; Liu, D.; Sun, Y.; Wu, C. An Integrative Multiomics Analysis Identifies Putative Causal Genes for COVID-19 Severity. Genet. Med. Off. J. Am. Coll. Med. Genet. 2021, 23, 2076–2086. [Google Scholar] [CrossRef] [PubMed]
- Smieszek, S.P.; Polymeropoulos, V.M.; Xiao, C.; Polymeropoulos, C.M.; Polymeropoulos, M.H. Loss-of-Function Mutations in IFNAR2 in COVID-19 Severe Infection Susceptibility. J. Glob. Antimicrob. Resist. 2021, 26, 239–240. [Google Scholar] [CrossRef]
- Contoli, M.; Papi, A.; Tomassetti, L.; Rizzo, P.; Vieceli Dalla Sega, F.; Fortini, F.; Torsani, F.; Morandi, L.; Ronzoni, L.; Zucchetti, O.; et al. Blood Interferon-α Levels and Severity, Outcomes, and Inflammatory Profiles in Hospitalized COVID-19 Patients. Front. Immunol. 2021, 12, 648004. [Google Scholar] [CrossRef]
- Schreiber, G. The Role of Type I Interferons in the Pathogenesis and Treatment of COVID-19. Front. Immunol. 2020, 11, 595739. [Google Scholar] [CrossRef]
- da Silva, R.P.; Gonçalves, J.I.B.; Zanin, R.F.; Schuch, F.B.; de Souza, A.P.D. Circulating Type I Interferon Levels and COVID-19 Severity: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 657363. [Google Scholar] [CrossRef]
- Kristiansen, H.; Gad, H.H.; Eskildsen-Larsen, S.; Despres, P.; Hartmann, R. The Oligoadenylate Synthetase Family: An Ancient Protein Family with Multiple Antiviral Activities. J. Interf. cytokine Res. Off. J. Int. Soc. Interf. Cytokine Res. 2011, 31, 41–47. [Google Scholar] [CrossRef]
- Fagone, P.; Nunnari, G.; Lazzara, F.; Longo, A.; Cambria, D.; Distefano, G.; Palumbo, M.; Nicoletti, F.; Malaguarnera, L.; Di Rosa, M. Induction of OAS Gene Family in HIV Monocyte Infected Patients with High and Low Viral Load. Antiviral Res. 2016, 131, 66–73. [Google Scholar] [CrossRef]
- Al-Ahmadi, W.; Al-Haj, L.; Al-Mohanna, F.A.; Silverman, R.H.; Khabar, K.S.A. RNase L Downmodulation of the RNA-Binding Protein, HuR, and Cellular Growth. Oncogene 2009, 28, 1782–1791. [Google Scholar] [CrossRef]
- Lin, R.-J.; Yu, H.-P.; Chang, B.-L.; Tang, W.-C.; Liao, C.-L.; Lin, Y.-L. Distinct Antiviral Roles for Human 2’,5’-Oligoadenylate Synthetase Family Members against Dengue Virus Infection. J. Immunol. 2009, 183, 8035–8043. [Google Scholar] [CrossRef] [PubMed]
- Hovanessian, A.G. On the Discovery of Interferon-Inducible, Double-Stranded RNA Activated Enzymes: The 2’-5’oligoadenylate Synthetases and the Protein Kinase PKR. Cytokine Growth Factor Rev. 2007, 18, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Hovnanian, A.; Rebouillat, D.; Levy, E.R.; Mattei, M.G.; Hovanessian, A.G. The Human 2’,5’-Oligoadenylate Synthetase-like Gene (OASL) Encoding the Interferon-Induced 56-KDa Protein Maps to Chromosome 12q24.2 in the Proximity of the 2’,5’-OAS Locus. Genomics 1999, 56, 362–363. [Google Scholar] [CrossRef]
- Mashimo, T.; Glaser, P.; Lucas, M.; Simon-Chazottes, D.; Ceccaldi, P.E.; Montagutelli, X.; Desprès, P.; Guénet, J.L. Structural and Functional Genomics and Evolutionary Relationships in the Cluster of Genes Encoding Murine 2’,5’-Oligoadenylate Synthetases. Genomics 2003, 82, 537–552. [Google Scholar] [CrossRef] [PubMed]
- Mapping the Human Genetic Architecture of COVID-19. Nature 2021, 600, 472–477. [CrossRef]
- Banday, A.R.; Stanifer, M.L.; Florez-Vargas, O.; Onabajo, O.O.; Papenberg, B.W.; Zahoor, M.A.; Mirabello, L.; Ring, T.J.; Lee, C.-H.; Albert, P.S.; et al. Genetic Regulation of OAS1 Nonsense-Mediated Decay Underlies Association with COVID-19 Hospitalization in Patients of European and African Ancestries. Nat. Genet. 2022, 54, 1103–1116. [Google Scholar] [CrossRef]
- Sabater Molina, M.; Nicolás Rocamora, E.; Bendicho, A.I.; Vázquez, E.G.; Zorio, E.; Rodriguez, F.D.; Gil Ortuño, C.; Rodríguez, A.I.; Sánchez-López, A.J.; Jara Rubio, R.; et al. Polymorphisms in ACE, ACE2, AGTR1 Genes and Severity of COVID-19 Disease. PLoS One 2022, 17, e0263140. [Google Scholar] [CrossRef]
- Dorairaj, V.; Sulaiman, S.A.; Abu, N.; Abdul Murad, N.A. Nonalcoholic Fatty Liver Disease (NAFLD): Pathogenesis and Noninvasive Diagnosis. Biomedicines 2021, 10. [Google Scholar] [CrossRef]
- Pafili, K.; Roden, M. Nonalcoholic Fatty Liver Disease (NAFLD) from Pathogenesis to Treatment Concepts in Humans. Mol. Metab. 2021, 50, 101122. [Google Scholar] [CrossRef]
- Romeo, S.; Kozlitina, J.; Xing, C.; Pertsemlidis, A.; Cox, D.; Pennacchio, L.A.; Boerwinkle, E.; Cohen, J.C.; Hobbs, H.H. Genetic Variation in PNPLA3 Confers Susceptibility to Nonalcoholic Fatty Liver Disease. Nat. Genet. 2008, 40, 1461–1465. [Google Scholar] [CrossRef]
- Pirazzi, C.; Adiels, M.; Burza, M.A.; Mancina, R.M.; Levin, M.; Ståhlman, M.; Taskinen, M.-R.; Orho-Melander, M.; Perman, J.; Pujia, A.; et al. Patatin-like Phospholipase Domain-Containing 3 (PNPLA3) I148M (Rs738409) Affects Hepatic VLDL Secretion in Humans and in Vitro. J. Hepatol. 2012, 57, 1276–1282. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Darvishi, N.; Mansouri, K.; Ghasemi, H.; Hosseinian-Far, M.; Darvishi, F.; Mohammadi, M. Association between PNPLA3 Rs738409 Polymorphism and Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. BMC Endocr. Disord. 2021, 21, 125. [Google Scholar] [CrossRef]
- Sookoian, S.; Pirola, C.J. Meta-Analysis of the Influence of I148M Variant of Patatin-like Phospholipase Domain Containing 3 Gene (PNPLA3) on the Susceptibility and Histological Severity of Nonalcoholic Fatty Liver Disease. Hepatology 2011, 53, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Salameh, H.; Hanayneh, M. Al; Masadeh, M.; Naseemuddin, M.; Matin, T.; Erwin, A.; Singal, A.K. PNPLA3 as a Genetic Determinant of Risk for and Severity of Non-Alcoholic Fatty Liver Disease Spectrum. J. Clin. Transl. Hepatol. 2016, 4, 175–191. [Google Scholar] [CrossRef]
- Vespasiani-Gentilucci, U.; Gallo, P.; Porcari, A.; Carotti, S.; Galati, G.; Piccioni, L.; De Vincentis, A.; Dell’Unto, C.; Vorini, F.; Morini, S.; et al. The PNPLA3 Rs738409 C > G Polymorphism Is Associated with the Risk of Progression to Cirrhosis in NAFLD Patients. Scand. J. Gastroenterol. 2016, 51, 967–973. [Google Scholar] [CrossRef] [PubMed]
- Luo, F.; Oldoni, F.; Das, A. TM6SF2: A Novel Genetic Player in Nonalcoholic Fatty Liver and Cardiovascular Disease. Hepatol. Commun. 2022, 6, 448–460. [Google Scholar] [CrossRef]
- Smagris, E.; Gilyard, S.; BasuRay, S.; Cohen, J.C.; Hobbs, H.H. Inactivation of Tm6sf2, a Gene Defective in Fatty Liver Disease, Impairs Lipidation but Not Secretion of Very Low Density Lipoproteins. J. Biol. Chem. 2016, 291, 10659–10676. [Google Scholar] [CrossRef]
- Liu, Z.; Que, S.; Zhou, L.; Zheng, S.; Romeo, S.; Mardinoglu, A.; Valenti, L. The Effect of the TM6SF2 E167K Variant on Liver Steatosis and Fibrosis in Patients with Chronic Hepatitis C: A Meta-Analysis. Sci. Rep. 2017, 7, 9273. [Google Scholar] [CrossRef]
- Li, X.-Y.; Liu, Z.; Li, L.; Wang, H.-J.; Wang, H. TM6SF2 Rs58542926 Is Related to Hepatic Steatosis, Fibrosis and Serum Lipids Both in Adults and Children: A Meta-Analysis. Front. Endocrinol. (Lausanne). 2022, 13, 1026901. [Google Scholar] [CrossRef]
- Sookoian, S.; Pirola, C.J. Meta-Analysis of the Influence of TM6SF2 E167K Variant on Plasma Concentration of Aminotransferases across Different Populations and Diverse Liver Phenotypes. Sci. Rep. 2016, 6, 27718. [Google Scholar] [CrossRef]
- Xu, M.; Li, Y.; Zhang, S.; Wang, X.; Shen, J.; Zhang, S. Interaction of TM6SF2 E167K and PNPLA3 I148M Variants in NAFLD in Northeast China. Ann. Hepatol. 2019, 18, 456–460. [Google Scholar] [CrossRef]
- Chen, F.; Esmaili, S.; Rogers, G.B.; Bugianesi, E.; Petta, S.; Marchesini, G.; Bayoumi, A.; Metwally, M.; Azardaryany, M.K.; Coulter, S.; et al. Lean NAFLD: A Distinct Entity Shaped by Differential Metabolic Adaptation. Hepatology 2020, 71, 1213–1227. [Google Scholar] [CrossRef]
- Young, S.; Tariq, R.; Provenza, J.; Satapathy, S.K.; Faisal, K.; Choudhry, A.; Friedman, S.L.; Singal, A.K. Prevalence and Profile of Nonalcoholic Fatty Liver Disease in Lean Adults: Systematic Review and Meta-Analysis. Hepatol. Commun. 2020, 4, 953–972. [Google Scholar] [CrossRef]
- Kozlitina, J. Genetic Risk Factors and Disease Modifiers of Nonalcoholic Steatohepatitis. Gastroenterol. Clin. North Am. 2020, 49, 25–44. [Google Scholar] [CrossRef]
- Liu, Y.-L.; Reeves, H.L.; Burt, A.D.; Tiniakos, D.; McPherson, S.; Leathart, J.B.S.; Allison, M.E.D.; Alexander, G.J.; Piguet, A.-C.; Anty, R.; et al. TM6SF2 Rs58542926 Influences Hepatic Fibrosis Progression in Patients with Non-Alcoholic Fatty Liver Disease. Nat. Commun. 2014, 5, 4309. [Google Scholar] [CrossRef] [PubMed]
- Wong, V.W.-S.; Wong, G.L.-H.; Tse, C.-H.; Chan, H.L.-Y. Prevalence of the TM6SF2 Variant and Non-Alcoholic Fatty Liver Disease in Chinese. J. Hepatol. 2014, 61, 708–709. [Google Scholar] [CrossRef] [PubMed]
- Sookoian, S.; Castaño, G.O.; Scian, R.; Mallardi, P.; Fernández Gianotti, T.; Burgueño, A.L.; San Martino, J.; Pirola, C.J. Genetic Variation in Transmembrane 6 Superfamily Member 2 and the Risk of Nonalcoholic Fatty Liver Disease and Histological Disease Severity. Hepatology 2015, 61, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Aulchenko, Y.S.; Ripatti, S.; Lindqvist, I.; Boomsma, D.; Heid, I.M.; Pramstaller, P.P.; Penninx, B.W.J.H.; Janssens, A.C.J.W.; Wilson, J.F.; Spector, T.; et al. Loci Influencing Lipid Levels and Coronary Heart Disease Risk in 16 European Population Cohorts. Nat. Genet. 2009, 41, 47–55. [Google Scholar] [CrossRef]
- Willer, C.J.; Schmidt, E.M.; Sengupta, S.; Peloso, G.M.; Gustafsson, S.; Kanoni, S.; Ganna, A.; Chen, J.; Buchkovich, M.L.; Mora, S.; et al. Discovery and Refinement of Loci Associated with Lipid Levels. Nat. Genet. 2013, 45, 1274–1283. [CrossRef]
- Fang, Y.-L.; Chen, H.; Wang, C.-L.; Liang, L. Pathogenesis of Non-Alcoholic Fatty Liver Disease in Children and Adolescence: From “Two Hit Theory” to “Multiple Hit Model”. World J. Gastroenterol. 2018, 24, 2974–2983. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-C.; Chang, P.-F.; Chang, M.-H.; Ni, Y.-H. Genetic Variants in GCKR and PNPLA3 Confer Susceptibility to Nonalcoholic Fatty Liver Disease in Obese Individuals. Am. J. Clin. Nutr. 2014, 99, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Tan, H.-L.; Zain, S.M.; Mohamed, R.; Rampal, S.; Chin, K.-F.; Basu, R.C.; Cheah, P.-L.; Mahadeva, S.; Mohamed, Z. Association of Glucokinase Regulatory Gene Polymorphisms with Risk and Severity of Non-Alcoholic Fatty Liver Disease: An Interaction Study with Adiponutrin Gene. J. Gastroenterol. 2014, 49, 1056–1064. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Wen, J.; Tao, X.; Lu, B.; Du, Y.; Wang, M.; Wang, X.; Zhang, W.; Gong, W.; Ling, C.; et al. Genetic Variation in the GCKR Gene Is Associated with Non-Alcoholic Fatty Liver Disease in Chinese People. Mol. Biol. Rep. 2011, 38, 1145–1150. [Google Scholar] [CrossRef] [PubMed]
- Zain, S.M.; Mohamed, Z.; Mohamed, R. Common Variant in the Glucokinase Regulatory Gene Rs780094 and Risk of Nonalcoholic Fatty Liver Disease: A Meta-Analysis. J. Gastroenterol. Hepatol. 2015, 30, 21–27. [CrossRef] [PubMed]
- Li, J.; Zhao, Y.; Zhang, H.; Hua, W.; Jiao, W.; Du, X.; Rui, J.; Li, S.; Teng, H.; Shi, B.; et al. Contribution of Rs780094 and Rs1260326 Polymorphisms in GCKR Gene to Non-Alcoholic Fatty Liver Disease: A Meta-Analysis Involving 26,552 Participants. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 1696–1708. [Google Scholar] [CrossRef]
- Fischer, M.; Pleiss, J. The Lipase Engineering Database: A Navigation and Analysis Tool for Protein Families. Nucleic Acids Res. 2003, 31, 319–321. [Google Scholar] [CrossRef] [PubMed]
- Lei, X.; Callaway, M.; Zhou, H.; Yang, Y.; Chen, W. Obesity Associated Lyplal1 Gene Is Regulated in Diet Induced Obesity but Not Required for Adipocyte Differentiation. Mol. Cell. Endocrinol. 2015, 411, 207–213. [Google Scholar] [CrossRef]
- Yuan, C.; Lu, L.; An, B.; Jin, W.; Dong, Q.; Xin, Y.; Xuan, S. Association Between LYPLAL1 Rs12137855 Polymorphism With Ultrasound-Defined Non-Alcoholic Fatty Liver Disease in a Chinese Han Population. Hepat. Mon. 2015, 15, e33155. [Google Scholar] [CrossRef]
- Wang, X.; Liu, Z.; Wang, K.; Wang, Z.; Sun, X.; Zhong, L.; Deng, G.; Song, G.; Sun, B.; Peng, Z.; et al. Additive Effects of the Risk Alleles of PNPLA3 and TM6SF2 on Non-Alcoholic Fatty Liver Disease (NAFLD) in a Chinese Population. Front. Genet. 2016, 7, 140. [Google Scholar] [CrossRef]
- Trejo, M.J.; Morrill, K.E.; Klimentidis, Y.C.; Garcia, D.O. Examining Genetic Associations with Hepatic Steatosis in Mexican-Origin Adults. Ann. Hepatol. 2023, 101120. [Google Scholar] [CrossRef]
- Cai, W.; Weng, D.-H.; Yan, P.; Lin, Y.-T.; Dong, Z.-H.; Mailamuguli; Yao, H. Genetic Polymorphisms Associated with Nonalcoholic Fatty Liver Disease in Uyghur Population: A Case-Control Study and Meta-Analysis. Lipids Health Dis. 2019, 18, 14. [Google Scholar] [CrossRef]
- Rotman, Y.; Koh, C.; Zmuda, J.M.; Kleiner, D.E.; Liang, T.J. The Association of Genetic Variability in Patatin-like Phospholipase Domain-Containing Protein 3 (PNPLA3) with Histological Severity of Nonalcoholic Fatty Liver Disease. Hepatology 2010, 52, 894–903. [Google Scholar] [CrossRef]
- Mansoor, S.; Maheshwari, A.; Di Guglielmo, M.; Furuya, K.; Wang, M.; Crowgey, E.; Molle-Rios, Z.; He, Z. The PNPLA3 Rs738409 Variant but Not MBOAT7 Rs641738 Is a Risk Factor for Nonalcoholic Fatty Liver Disease in Obese U.S. Children of Hispanic Ethnicity. Pediatr. Gastroenterol. Hepatol. Nutr. 2021, 24, 455–469. [Google Scholar] [CrossRef]
- Park, S.L.; Li, Y.; Sheng, X.; Hom, V.; Xia, L.; Zhao, K.; Pooler, L.; Setiawan, V.W.; Lim, U.; Monroe, K.R.; et al. Genome-Wide Association Study of Liver Fat: The Multiethnic Cohort Adiposity Phenotype Study. Hepatol. Commun. 2020, 4, 1112–1123. [Google Scholar] [CrossRef]
- Hyysalo, J.; Stojkovic, I.; Kotronen, A.; Hakkarainen, A.; Sevastianova, K.; Makkonen, J.; Lundbom, N.; Rissanen, A.; Krauss, R.M.; Melander, O.; et al. Genetic Variation in PNPLA3 but Not APOC3 Influences Liver Fat in Non-Alcoholic Fatty Liver Disease. J. Gastroenterol. Hepatol. 2012, 27, 951–956. [Google Scholar] [CrossRef]
- Li, Y.; Xing, C.; Tian, Z.; Ku, H.-C. Genetic Variant I148M in PNPLA3 Is Associated with the Ultrasonography-Determined Steatosis Degree in a Chinese Population. BMC Med. Genet. 2012, 13, 113. [Google Scholar] [CrossRef] [PubMed]
- Shang, X.-R.; Song, J.-Y.; Liu, F.-H.; Ma, J.; Wang, H.-J. GWAS-Identified Common Variants With Nonalcoholic Fatty Liver Disease in Chinese Children. J. Pediatr. Gastroenterol. Nutr. 2015, 60, 669–674. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.-F.; Ling, Y.; Bian, H.; Lin, H.-D.; Yan, H.-M.; Chang, X.-X.; Li, X.-M.; Ma, H.; Wang, D.; Zhang, L.-S.; et al. I148M Variant of PNPLA3 Increases the Susceptibility to Non-Alcoholic Fatty Liver Disease Caused by Obesity and Metabolic Disorders. Aliment. Pharmacol. Ther. 2016, 43, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-W.; Lin, H.-Y.; Shin, S.-J.; Yu, M.-L.; Lin, Z.-Y.; Dai, C.-Y.; Huang, J.-F.; Chen, S.-C.; Li, S.S.-L.; Chuang, W.-L. The PNPLA3 I148M Polymorphism Is Associated with Insulin Resistance and Nonalcoholic Fatty Liver Disease in a Normoglycaemic Population. Liver Int. Off. J. Int. Assoc. Study Liver 2011, 31, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Hudert, C.A.; Selinski, S.; Rudolph, B.; Bläker, H.; Loddenkemper, C.; Thielhorn, R.; Berndt, N.; Golka, K.; Cadenas, C.; Reinders, J.; et al. Genetic Determinants of Steatosis and Fibrosis Progression in Paediatric Non-Alcoholic Fatty Liver Disease. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39, 540–556. [Google Scholar] [CrossRef]
- Krawczyk, M.; Rau, M.; Schattenberg, J.M.; Bantel, H.; Pathil, A.; Demir, M.; Kluwe, J.; Boettler, T.; Lammert, F.; Geier, A. Combined Effects of the PNPLA3 Rs738409, TM6SF2 Rs58542926, and MBOAT7 Rs641738 Variants on NAFLD Severity: A Multicenter Biopsy-Based Study. J. Lipid Res. 2017, 58, 247–255. [Google Scholar] [CrossRef]
- Kitamoto, T.; Kitamoto, A.; Yoneda, M.; Hyogo, H.; Ochi, H.; Nakamura, T.; Teranishi, H.; Mizusawa, S.; Ueno, T.; Chayama, K.; et al. Genome-Wide Scan Revealed That Polymorphisms in the PNPLA3, SAMM50, and PARVB Genes Are Associated with Development and Progression of Nonalcoholic Fatty Liver Disease in Japan. Hum. Genet. 2013, 132, 783–792. [Google Scholar] [CrossRef]
- Di Costanzo, A.; Belardinilli, F.; Bailetti, D.; Sponziello, M.; D’Erasmo, L.; Polimeni, L.; Baratta, F.; Pastori, D.; Ceci, F.; Montali, A.; et al. Evaluation of Polygenic Determinants of Non-Alcoholic Fatty Liver Disease (NAFLD) By a Candidate Genes Resequencing Strategy. Sci. Rep. 2018, 8, 3702. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Al-Serri, A.; Daly, A.K.; Galmozzi, E.; Rametta, R.; Dongiovanni, P.; Nobili, V.; Mozzi, E.; Roviaro, G.; Vanni, E.; et al. Homozygosity for the Patatin-like Phospholipase-3/Adiponutrin I148M Polymorphism Influences Liver Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Hepatology 2010, 51, 1209–1217. [Google Scholar] [CrossRef]
- Longo, M.; Meroni, M.; Paolini, E.; Erconi, V.; Carli, F.; Fortunato, F.; Ronchi, D.; Piciotti, R.; Sabatini, S.; Macchi, C.; et al. TM6SF2/PNPLA3/MBOAT7 Loss-of-Function Genetic Variants Impact on NAFLD Development and Progression Both in Patients and in In Vitro Models. Cell. Mol. Gastroenterol. Hepatol. 2022, 13, 759–788. [Google Scholar] [CrossRef]
- Verrijken, A.; Beckers, S.; Francque, S.; Hilden, H.; Caron, S.; Zegers, D.; Ruppert, M.; Hubens, G.; Van Marck, E.; Michielsen, P.; et al. A Gene Variant of PNPLA3, but Not of APOC3, Is Associated with Histological Parameters of NAFLD in an Obese Population. Obesity (Silver Spring). 2013, 21, 2138–2145. [Google Scholar] [CrossRef] [PubMed]
- Lisboa, Q.C.; Nardelli, M.J.; Pereira, P. de A.; Miranda, D.M.; Ribeiro, S.N.; Costa, R.S.N.; Versiani, C.A.; Vidigal, P.V.T.; Ferrari, T.C. de A.; Couto, C.A. PNPLA3 and TM6SF2 Polymorphisms in Brazilian Patients with Nonalcoholic Fatty Liver Disease. World J. Hepatol. 2020, 12, 792–806. [Google Scholar] [CrossRef] [PubMed]
- Zain, S.M.; Mohamed, R.; Mahadeva, S.; Cheah, P.L.; Rampal, S.; Basu, R.C.; Mohamed, Z. A Multi-Ethnic Study of a PNPLA3 Gene Variant and Its Association with Disease Severity in Non-Alcoholic Fatty Liver Disease. Hum. Genet. 2012, 131, 1145–1152. [Google Scholar] [CrossRef]
- Uygun, A.; Ozturk, K.; Demirci, H.; Oztuna, A.; Eren, F.; Kozan, S.; Yilmaz, Y.; Kurt, O.; Turker, T.; Vatansever, S.; et al. The Association of Nonalcoholic Fatty Liver Disease with Genetic Polymorphisms: A Multicenter Study. Eur. J. Gastroenterol. Hepatol. 2017, 29, 441–447. [Google Scholar] [CrossRef]
- Idilman, R.; Karatayli, S.C.; Kabacam, G.; Savas, B.; Elhan, A.H.; Bozdayi, A.M. The Role of PNPLA3 (Rs738409) C>g Variant on Histological Progression of Non-Alcoholic Fatty Liver Disease. Hepatol. forum 2020, 1, 82–87. [Google Scholar] [CrossRef]
- Li, X.; Zhao, Q.; Wu, K.; Fan, D. I148M Variant of PNPLA3 Confer Increased Risk for Nonalcoholic Fatty Liver Disease Not Only in European Population, but Also in Chinese Population. Hepatology 2011, 54, 2275. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Wong, G.L.-H.; Whatling, C.; Chan, A.W.-H.; Leung, H.H.-W.; Tse, C.-H.; Shu, S.S.-T.; Chim, A.M.-L.; Lai, J.C.-T.; Yip, T.C.-F.; et al. Association of Genetic Variations with NAFLD in Lean Individuals. Liver Int. Off. J. Int. Assoc. Study Liver 2022, 42, 149–160. [Google Scholar] [CrossRef]
- Hotta, K.; Yoneda, M.; Hyogo, H.; Ochi, H.; Mizusawa, S.; Ueno, T.; Chayama, K.; Nakajima, A.; Nakao, K.; Sekine, A. Association of the Rs738409 Polymorphism in PNPLA3 with Liver Damage and the Development of Nonalcoholic Fatty Liver Disease. BMC Med. Genet. 2010, 11, 172. [Google Scholar] [CrossRef]
- Kawaguchi, T.; Sumida, Y.; Umemura, A.; Matsuo, K.; Takahashi, M.; Takamura, T.; Yasui, K.; Saibara, T.; Hashimoto, E.; Kawanaka, M.; et al. Genetic Polymorphisms of the Human PNPLA3 Gene Are Strongly Associated with Severity of Non-Alcoholic Fatty Liver Disease in Japanese. PLoS One 2012, 7, e38322. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.S.; Byoun, Y.-S.; Jeong, S.-H.; Woo, B.H.; Jang, E.S.; Kim, J.-W.; Kim, H.Y. Role of the PNPLA3 I148M Polymorphism in Nonalcoholic Fatty Liver Disease and Fibrosis in Korea. Dig. Dis. Sci. 2014, 59, 2967–2974. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Cho, B.; Kwon, H.; Prilutsky, D.; Yun, J.M.; Choi, H.C.; Hwang, K.-B.; Lee, I.-H.; Kim, J.-I.; Kong, S.W. I148M Variant in PNPLA3 Reduces Central Adiposity and Metabolic Disease Risks While Increasing Nonalcoholic Fatty Liver Disease. Liver Int. Off. J. Int. Assoc. Study Liver 2015, 35, 2537–2546. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, A.; Basu, A.; Das, K.; Chowdhury, A.; Basu, P. Exome-Wide Scan Identifies Significant Association of Rs4788084 in IL27 Promoter with Increase in Hepatic Fat Content among Indians. Gene 2021, 775, 145431. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, S.P.; Nigam, P.; Misra, A.; Guleria, R.; Pandey, R.M.; Pasha, M.A.Q. Genetic Variation in the Patatin-like Phospholipase Domain-Containing Protein-3 (PNPLA-3) Gene in Asian Indians with Nonalcoholic Fatty Liver Disease. Metab. Syndr. Relat. Disord. 2013, 11, 329–335. [Google Scholar] [CrossRef]
- Karoli, R.; Fatima, J.; Singh, P.S.; Siddiqi, Z.; Varshney, S.; Beg, M.S.; Khan, M.A. Association of Genetic Non-Alcoholic Fatty Liver Disease with Insulin Resistance-Are We Different? J. Assoc. Physicians India 2019, 67, 34–38. [Google Scholar]
- Kanth, V.V.R.; Sasikala, M.; Rao, P.N.; Steffie Avanthi, U.; Rao, K.R.; Nageshwar Reddy, D. Pooled Genetic Analysis in Ultrasound Measured Non-Alcoholic Fatty Liver Disease in Indian Subjects: A Pilot Study. World J. Hepatol. 2014, 6, 435–442. [Google Scholar] [CrossRef]
- Narayanasamy, K.; Karthick, R.; Panneerselvam, P.; Mohan, N.; Ramachandran, A.; Prakash, R.; Rajaram, M. Association of Metabolic Syndrome and Patatin-like Phospholipase 3 - Rs738409 Gene Variant in Non-Alcoholic Fatty Liver Disease among a Chennai-Based South Indian Population. J. Gene Med. 2020, 22, e3160. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Islam, M.S.; Islam, S.; Mustafa, G.; Saleh, A.A.; Ahmad, N. Association of Single Nucleotide Polymorphism at PNPLA3 with Fatty Liver, Steatohepatitis, and Cirrhosis of Liver. Indian J. Gastroenterol. Off. J. Indian Soc. Gastroenterol. 2017, 36, 366–372. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.H.; Phyo, W.W.; Loo, W.M.; Kwok, R.; Ahmed, T.; Shabbir, A.; So, J.; Koh, C.J.; Hartono, J.L.; Muthiah, M.; et al. Validation of Genetic Variants Associated with Metabolic Dysfunction-Associated Fatty Liver Disease in an Ethnic Chinese Population. World J. Hepatol. 2020, 12, 1228–1238. [CrossRef] [PubMed]
- Krawczyk, M.; Stachowska, E.; Milkiewicz, P.; Lammert, F.; Milkiewicz, M. Reduction of Caloric Intake Might Override the Prosteatotic Effects of the PNPLA3 p.I148M and TM6SF2 p.E167K Variants in Patients with Fatty Liver: Ultrasound-Based Prospective Study. Digestion 2016, 93, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Koo, B.K.; Joo, S.K.; Kim, D.; Bae, J.M.; Park, J.H.; Kim, J.H.; Kim, W. Additive Effects of PNPLA3 and TM6SF2 on the Histological Severity of Non-Alcoholic Fatty Liver Disease. J. Gastroenterol. Hepatol. 2018, 33, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Akuta, N.; Kawamura, Y.; Arase, Y.; Suzuki, F.; Sezaki, H.; Hosaka, T.; Kobayashi, M.; Kobayashi, M.; Saitoh, S.; Suzuki, Y.; et al. Relationships between Genetic Variations of PNPLA3, TM6SF2 and Histological Features of Nonalcoholic Fatty Liver Disease in Japan. Gut Liver 2016, 10, 437–445. [Google Scholar] [CrossRef]
- Hernaez, R.; McLean, J.; Lazo, M.; Brancati, F.L.; Hirschhorn, J.N.; Borecki, I.B.; Harris, T.B.; Nguyen, T.; Kamel, I.R.; Bonekamp, S.; et al. Association between Variants in or near PNPLA3, GCKR, and PPP1R3B with Ultrasound-Defined Steatosis Based on Data from the Third National Health and Nutrition Examination Survey. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2013, 11, 1183–1190. [Google Scholar] [CrossRef]
- Mazo, D.F.; Malta, F.M.; Stefano, J.T.; Salles, A.P.M.; Gomes-Gouvea, M.S.; Nastri, A.C.S.; Almeida, J.R.; Pinho, J.R.R.; Carrilho, F.J.; Oliveira, C.P. Validation of PNPLA3 Polymorphisms as Risk Factor for NAFLD and Liver Fibrosis in an Admixed Population. Ann. Hepatol. 2019, 18, 466–471. [Google Scholar] [CrossRef]
- Delik, A.; Akkız, H.; Dinçer, S. The Effect of PNPLA3 Polymorphism as Gain in Function Mutation in the Pathogenesis of Non-Alcoholic Fatty Liver Disease. Indian J. Gastroenterol. Off. J. Indian Soc. Gastroenterol. 2020, 39, 84–91. [Google Scholar] [CrossRef]
- Petta, S.; Miele, L.; Bugianesi, E.; Cammà, C.; Rosso, C.; Boccia, S.; Cabibi, D.; Di Marco, V.; Grimaudo, S.; Grieco, A.; et al. Glucokinase Regulatory Protein Gene Polymorphism Affects Liver Fibrosis in Non-Alcoholic Fatty Liver Disease. PLoS One 2014, 9, e87523. [Google Scholar] [CrossRef]
- Eslam, M.; Mangia, A.; Berg, T.; Chan, H.L.Y.; Irving, W.L.; Dore, G.J.; Abate, M.L.; Bugianesi, E.; Adams, L.A.; Najim, M.A.M.; et al. Diverse Impacts of the Rs58542926 E167K Variant in TM6SF2 on Viral and Metabolic Liver Disease Phenotypes. Hepatology 2016, 64, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Llauradó, G.; Orešič, M.; Hyötyläinen, T.; Orho-Melander, M.; Yki-Järvinen, H. Circulating Triacylglycerol Signatures and Insulin Sensitivity in NAFLD Associated with the E167K Variant in TM6SF2. J. Hepatol. 2015, 62, 657–663. [Google Scholar] [CrossRef] [PubMed]
- Grandone, A.; Cozzolino, D.; Marzuillo, P.; Cirillo, G.; Di Sessa, A.; Ruggiero, L.; Di Palma, M.R.; Perrone, L.; Miraglia Del Giudice, E. TM6SF2 Glu167Lys Polymorphism Is Associated with Low Levels of LDL-Cholesterol and Increased Liver Injury in Obese Children. Pediatr. Obes. 2016, 11, 115–119. [Google Scholar] [CrossRef]
- Mancina, R.M.; Sentinelli, F.; Incani, M.; Bertoccini, L.; Russo, C.; Romeo, S.; Baroni, M.G. Transmembrane-6 Superfamily Member 2 (TM6SF2) E167K Variant Increases Susceptibility to Hepatic Steatosis in Obese Children. Dig. liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2016, 48, 100–101. [Google Scholar] [CrossRef]
- Wang, X.; Liu, Z.; Peng, Z.; Liu, W. The TM6SF2 Rs58542926 T Allele Is Significantly Associated with Non-Alcoholic Fatty Liver Disease in Chinese. J. Hepatol. 2015, 62, 1438–1439. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; Petta, S.; Maglio, C.; Fracanzani, A.L.; Pipitone, R.; Mozzi, E.; Motta, B.M.; Kaminska, D.; Rametta, R.; Grimaudo, S.; et al. Transmembrane 6 Superfamily Member 2 Gene Variant Disentangles Nonalcoholic Steatohepatitis from Cardiovascular Disease. Hepatology 2015, 61, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Bale, G.; Steffie, A.U.; Ravi Kanth, V.V.; Rao, P.N.; Sharma, M.; Sasikala, M.; Reddy, D.N. Regional Differences in Genetic Susceptibility to Non-Alcoholic Liver Disease in Two Distinct Indian Ethnicities. World J. Hepatol. 2017, 9, 1101–1107. [Google Scholar] [CrossRef]
- Pan, L.; Huang, P.; Xie, X.; Xu, J.; Guo, D.; Jiang, Y. Metabolic Associated Fatty Liver Disease Increases the Severity of COVID-19: A Meta-Analysis. Dig. Liver Dis. 2021, 53, 153–157. [Google Scholar] [CrossRef]
- Trottier, C.; Chabot, S.; Mann, K.K.; Colombo, M.; Chatterjee, A.; Miller, W.H.J.; Ward, B.J. Retinoids Inhibit Measles Virus in Vitro via Nuclear Retinoid Receptor Signaling Pathways. Antiviral Res. 2008, 80, 45–53. [Google Scholar] [CrossRef]
- Trasino, S.E.; Tang, X.-H.; Jessurun, J.; Gudas, L.J. Obesity Leads to Tissue, but Not Serum Vitamin A Deficiency. Sci. Rep. 2015, 5, 15893. [Google Scholar] [CrossRef]
- Peter, A.; Kovarova, M.; Nadalin, S.; Cermak, T.; Königsrainer, A.; Machicao, F.; Stefan, N.; Häring, H.-U.; Schleicher, E. PNPLA3 Variant I148M Is Associated with Altered Hepatic Lipid Composition in Humans. Diabetologia 2014, 57, 2103–2107. [Google Scholar] [CrossRef]
- Wen, J.; Nodzak, C.; Shi, X. QTL Analysis Beyond EQTLs. Methods Mol. Biol. 2020, 2082, 201–210. [Google Scholar] [CrossRef]
- Yang, S.; Liu, Y.; Jiang, N.; Chen, J.; Leach, L.; Luo, Z.; Wang, M. Genome-Wide EQTLs and Heritability for Gene Expression Traits in Unrelated Individuals. BMC Genomics 2014, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Kamyshna, I.; Pavlovych, L.; Pankiv, I.; Pankiv, V.; Kamyshnyi, A.I.; Kamyshna, L.; Pavlovych, I.; Pankiv, V.; Pankiv, A.K. Evaluation of the Influence of Single-Nucleotide Polymorphisms of Vitamin D Receptor ( Rs2228570 ), BDNF ( Rs6265 ), and NMDA ( Rs4880213 ) Genes on Gene Expression in Different Tissues. Int. J. Endocrinol. 2023, 19, 83–88. [Google Scholar] [CrossRef]
- Kamyshna, I.I.; Pavlovych, L.B.; Sydorchuk, L.P.; Malyk, I. V; Kamyshnyi, A.M. BDNF Blood Serum Linkage with BDNF Gene Polymorphism (Rs6265) in Thyroid Pathology Patients in the West-Ukrainian Population. Endocr. Regul. 2021, 55, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Kamyshna, I.I.; Pavlovych, L.B.; Kamyshnyi, A.M. Association between NMDA Gene Polymorphism (Rs4880213) and GRIN2B Blood Serum Levels in Thyroid Pathology Patients. J. Med. Life 2022, 15, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Dzhuryak, V.; Sydorchuk, L.; Sydorchuk, A.; Kamyshnyi, O.; Kshanovska, A.; Levytska, S.; Knut, R.; Sheremet, M.; Ivashchuk, S.; et al. Biointerface Research in Applied Chemistry. ultrasound 2020, 10, 5556–5563. [Google Scholar] [CrossRef]
- Lyubomirskaya, E.S.; Kamyshnyi, A.M.; Krut, Y.Y.; Smiianov, V.A.; Fedoniuk, L.Y.; Romanyuk, L.B.; Kravets, N.Y.; Mochulska, O.M. SNPs and Transcriptional Activity of Genes of Innate and Adaptive Immunity at the Maternal-Fetal Interface in Woman with Preterm Labour, Associated with Preterm Premature Rupture of Membranes. Wiad. Lek. 2020, 73, 25–30. [Google Scholar]
- Kamyshna, I.I.; Pavlovych, L.B.; Malyk, I.V.; Kamyshnyi, A.M. 25-OH Vitamin D Blood Serum Linkage with VDR Gene Polymorphism (Rs2228570) in Thyroid Pathology Patients in the West-Ukrainian Population. J. Med. Life 2021, 14, 549–556. [Google Scholar] [CrossRef]
- Tapper, E.B.; Asrani, S.K. The COVID-19 Pandemic Will Have a Long-Lasting Impact on the Quality of Cirrhosis Care. J. Hepatol. 2020, 73, 441–445. [Google Scholar] [CrossRef]
- Gao, X.; Lv, F.; He, X.; Zhao, Y.; Liu, Y.; Zu, J.; Henry, L.; Wang, J.; Yeo, Y.H.; Ji, F.; et al. Impact of the COVID-19 Pandemic on Liver Disease-Related Mortality Rates in the United States. J. Hepatol. 2023, 78, 16–27. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Genetic polymorphisms contributing to the risk of NAFLD and COVID-19.
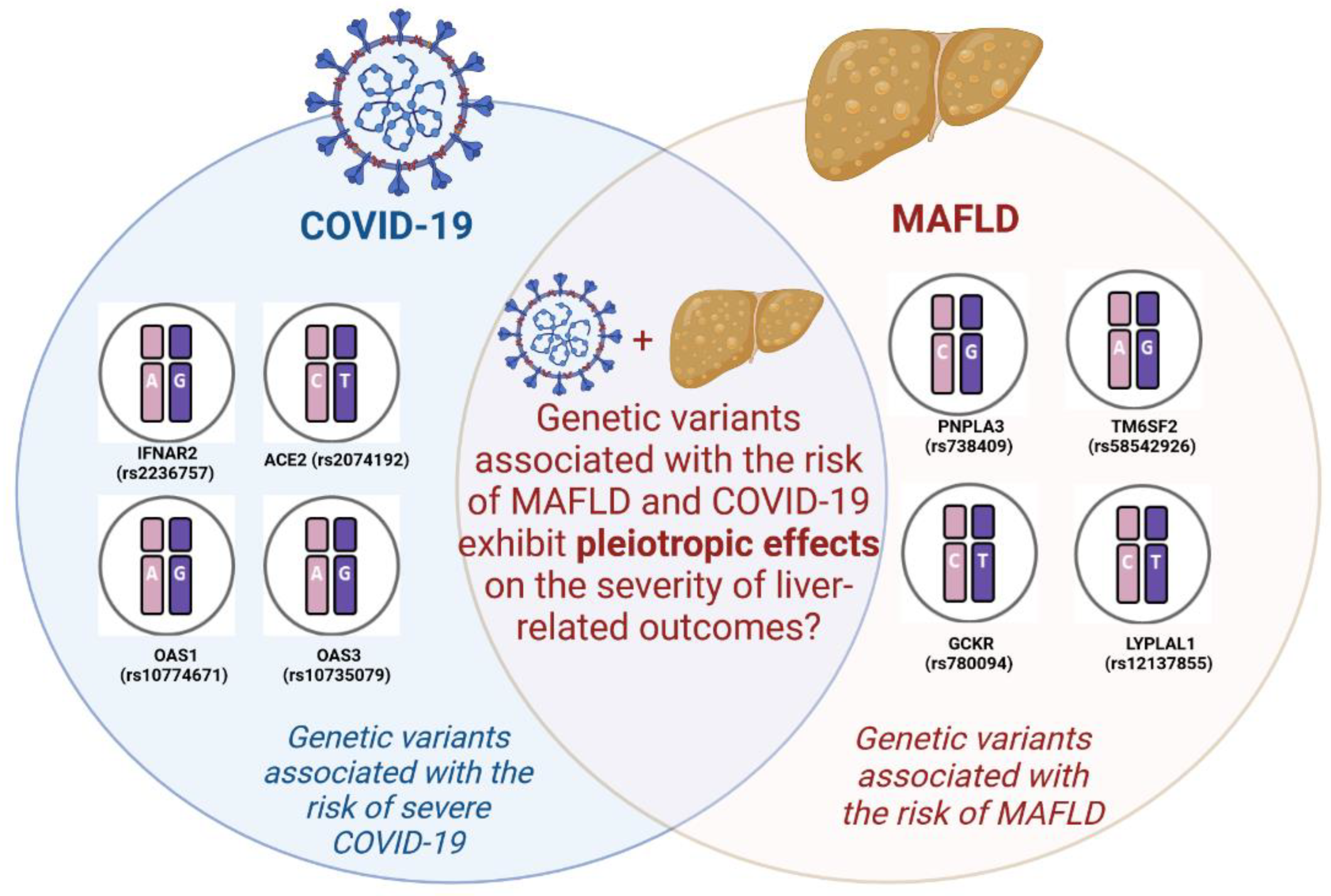
Figure 2.
The heatmap plot illustrates the distribution of molecular traits associated with various tissue/cell types and compares them to eQTL-associated traits (genes). Each row corresponds to a unique tissue or cell type, and each column represents a distinct eQTL-associated trait (gene). The color of each grid cell indicates the median P-value of the eQTLs associated with the specific tissue and trait combination. Overview of eQTL for: TM6SF2 rs58542926 (a) 47 tissues and 25 traits; PNPLA3rs738409 (b) 13 tissues and 22 traits; GCKR rs780094 (c) 44 tissues and 50 traits; GCKR rs780094 (d) 11 tissues and 5 traits.
Figure 2.
The heatmap plot illustrates the distribution of molecular traits associated with various tissue/cell types and compares them to eQTL-associated traits (genes). Each row corresponds to a unique tissue or cell type, and each column represents a distinct eQTL-associated trait (gene). The color of each grid cell indicates the median P-value of the eQTLs associated with the specific tissue and trait combination. Overview of eQTL for: TM6SF2 rs58542926 (a) 47 tissues and 25 traits; PNPLA3rs738409 (b) 13 tissues and 22 traits; GCKR rs780094 (c) 44 tissues and 50 traits; GCKR rs780094 (d) 11 tissues and 5 traits.
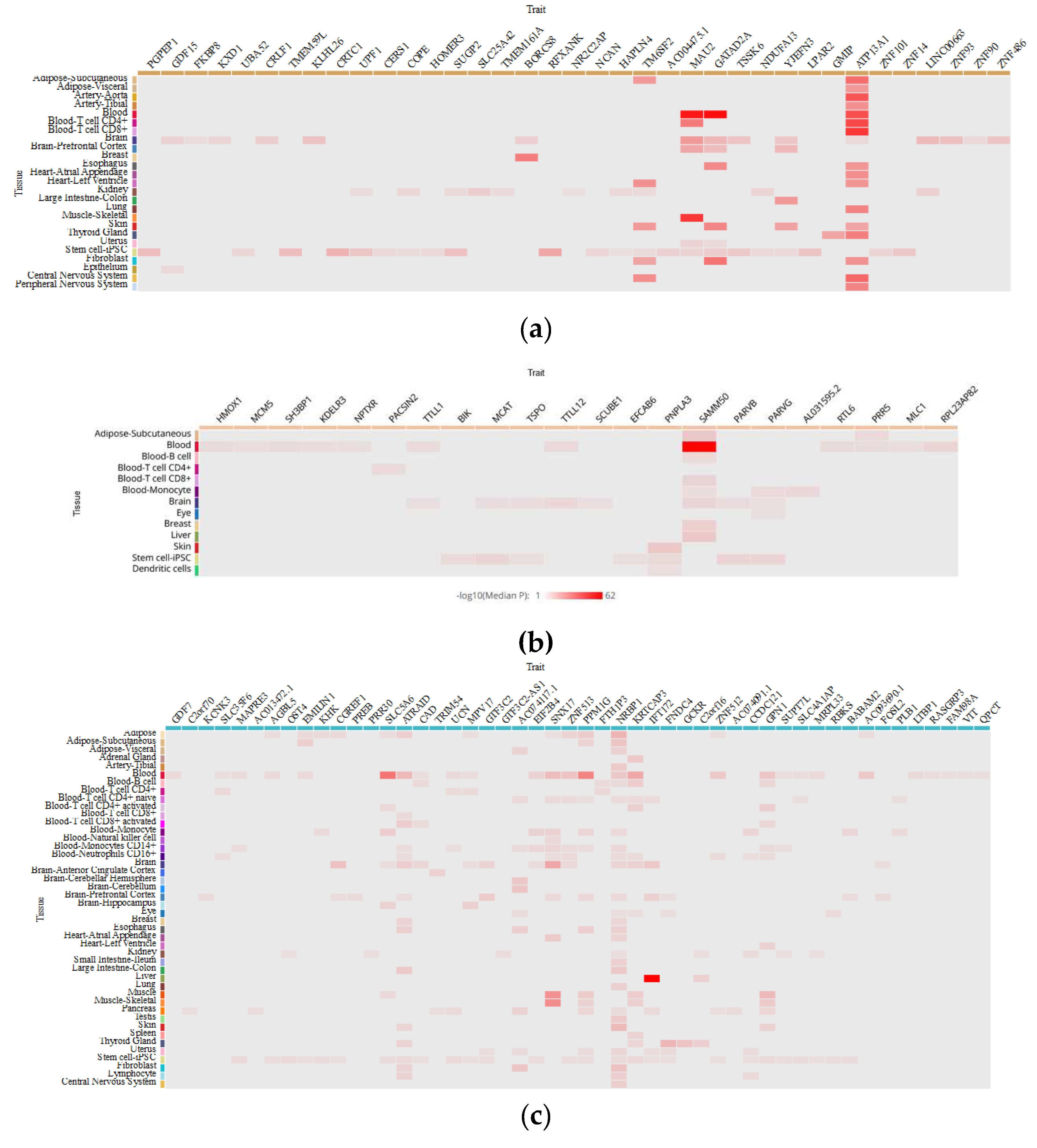
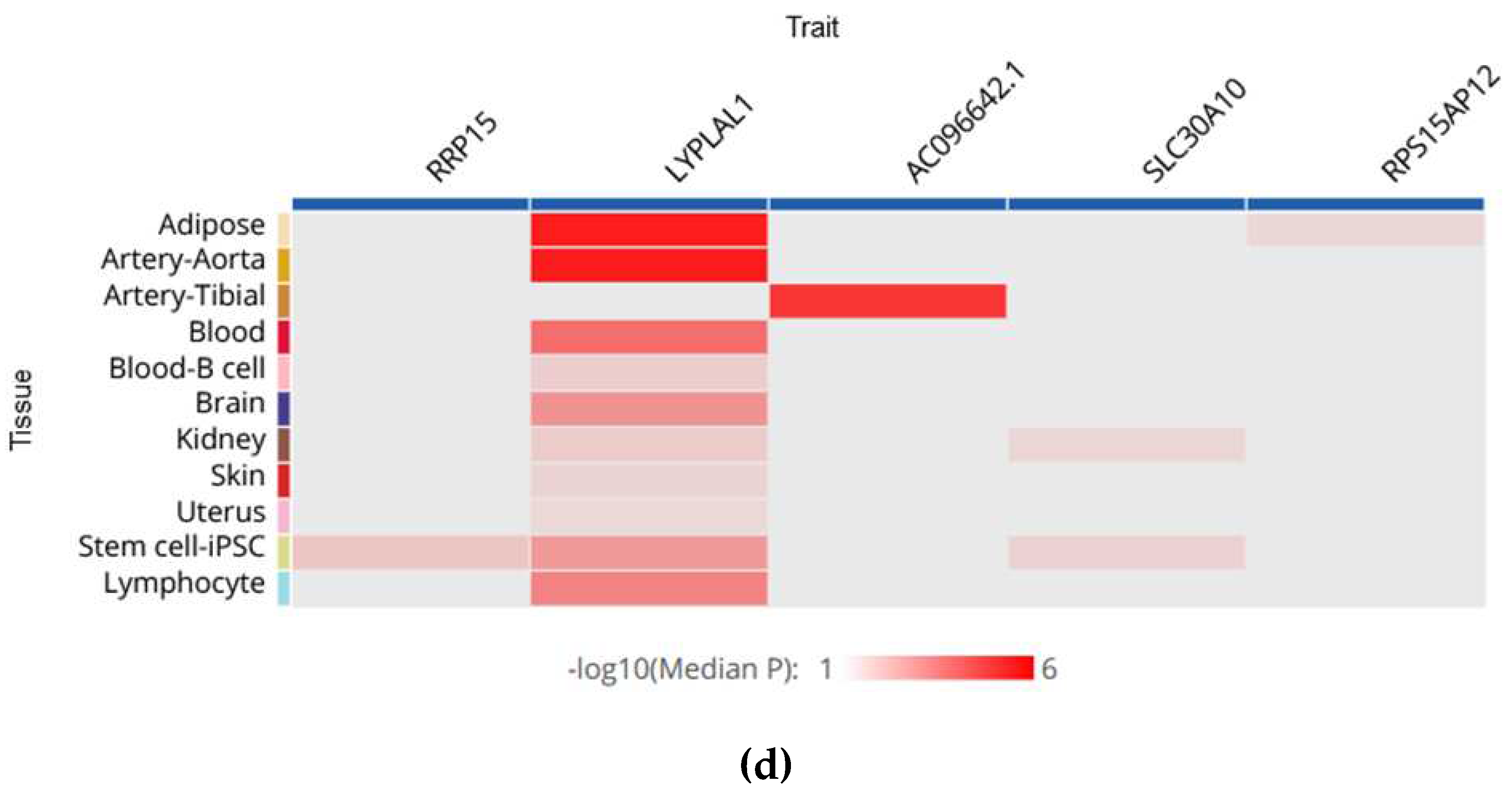
Table 3.
The impact of MAFLD-associated polymorphisms on the severity course of COVID-19.
| Gene | SNP | The number of patients | SNP ’s effect | Significance | Features | Patient cohorts | References |
|---|---|---|---|---|---|---|---|
| PNPLA3 | rs738409 (C > G) (I148M) | 383 | Associated with an increased risk of severe COVID-19 outcomes | p = 0,035 (GG genotype) | Individuals harboring a GG genotype in the PNPLA3 gene may exhibit inherent upregulation of the NLRP3 inflammasome, rendering them more susceptible to tissue damage upon infection with SARS-CoV-2 | Italian populations | [44] |
| 1460 | Was not associated with the risk of severe COVID-19 | p > 0,1 | There appears to be an inclination towards protection against COVID-19 when considering the aforementioned genotype. These findings imply that the genetic inclination towards hepatic fat accumulation does not independently heighten the susceptibility to severe COVID-19. Moreover, this indicates that MAFLD does not assume a causal role in this particular condition | UK populations | [45] | ||
| 1585 | Associated with a lower risk of COVID-19 hospitalization and death | p = 0,027 (hospitalization); p = 0,037 (death) | On average, the presence of each additional G allele was associated with a notable decrease of 21% in the likelihood of COVID-19 hospitalization and a further decrease of 25% in the likelihood of COVID-19-related mortality | UK populations | [46] | ||
| 1397 | Was not associated with the risk of severe COVID-19 in hospitalized patients |
p = 0,46 | Intriguingly, a genetic predisposition to accumulate fat in the liver may paradoxically confer protection during the course of COVID-19 |
Hospital-based Fondazione IRCCS Ca' Granda cohort | [47] |
Table 4.
EQTL data for SNPs association in tissues.
| Trait | CHR | Effective Allele | Tissue | Effect Size | p-value | Population | Sample Size | |
|---|---|---|---|---|---|---|---|---|
| GCKR rs780094 | ||||||||
| AC074117.1 | 2 | C | Fibroblast | -0,206732 | 3,23E-09 | MIX | 483 | |
| ATRAID | 2 | T | Blood | -0,20743 | 2,2E-13 | MIX | 2765 | |
| ATRAID | 2 | C | Blood-T cell CD8+ activated | 0,130598 | 0,00000114 | EAS | 416 | |
| ATRAID | 2 | C | Lymphocyte | 0,163788 | 0,0000466 | EUR | 368 | |
| EIF2B4 | 2 | C | Blood | -0,00922729 | 0,0000631 | MIX | 5257 | |
| EMILIN1 | 2 | T | Adipose-Subcutaneous | 0,24 | 0,00000333 | EUR | 770 | |
| GPN1 | 2 | C | Blood-T cell CD4+ activated | 0,188994 | 0,00000277 | EAS | 416 | |
| KRTCAP3 | 2 | T | Blood | -0,237548 | 6,3E-17 | MIX | 2765 | |
| KRTCAP3 | 2 | C | Blood-T cell CD4+ activated | 0,234009 | 0,0000181 | EAS | 416 | |
| NRBP1 | 2 | C | Lymphocyte | -0,141265 | 0,00000365 | EUR | 368 | |
| NRBP1 | 2 | C | Blood | -0,013931 | 2,04E-12 | MIX | 5257 | |
| NRBP1 | 2 | T | Blood | 0,153229 | 0,000000044 | MIX | 2765 | |
| NRBP1 | 2 | NA | Blood-Monocyte | 5,524902 | 6,21E-08 | EUR | 432 | |
| PPM1G | 2 | C | Adipose | -0,331022 | 0,0000007 | EUR | 434 | |
| SLC5A6 | 2 | T | Blood | 0,165322 | 4,7E-09 | MIX | 2765 | |
| SLC5A6 | 2 | NA | Blood-Monocyte | 0,233295 | 0,00000113 | MIX | 696 | |
| SNX17 | 2 | C | Blood-Monocytes CD14+ | -0,03898 | 0,00000409 | MIX | 197 | |
| SNX17 | 2 | T | Blood | 0,141788 | 0,00000034 | MIX | 2765 | |
| SNX17 | 2 | NA | Blood-Monocyte | 4,2447721 | 0,0000286 | EUR | 432 | |
| ZNF512 | 2 | C | Blood | 0,0147365 | 7,47E-08 | MIX | 5257 | |
| AC074117.1 | 2 | C | Fibroblast | -0,206732 | 3,23E-09 | MIX | 483 | |
| ATRAID | 2 | T | Blood | -0,20743 | 2,2E-13 | MIX | 2765 | |
| ATRAID | 2 | C | Blood-T cell CD8+ activated | 0,130598 | 0,00000114 | EAS | 416 | |
| ATRAID | 2 | C | Lymphocyte | 0,163788 | 0,0000466 | EUR | 368 | |
| PNPLA3 rs738409 | ||||||||
| SAMM50 | 22 | G | Blood-T cell CD8+ | -3,90455 | 9,44E-05 | EUR | 283 | |
| PNPLA3 | 22 | G | Skin | -0,13586 | 1,54E-06 | MIX | 605 | |
| SAMM50 | 22 | C | Blood | -0,07719 | 5,67E-106 | MIX | 5257 | |
| SAMM50 | 22 | G | Adipose-Subcutaneous | 0,188769 | 9,6E-07 | EUR | 385 | |
| AL031595.2 | 22 | G | Blood-Monocyte | 0,220815 | 0,00188 | EAS | 416 | |
| TM6SF2 rs58542926 | ||||||||
| ATP13A1 | 19 | G | Blood | 0,442548 | 3,13E-08 | EUR | 121 | |
| ATP13A1 | 19 | T | Blood-T cell CD4+ | 5,639089 | 1,71E-08 | EUR | 293 | |
| ATP13A1 | 19 | T | Blood-T cell CD8+ | 5,943743 | 2,79E-09 | EUR | 283 | |
| BORCS8 | 19 | T | Breast | -0,27489 | 4,48E-06 | MIX | 396 | |
| GATAD2A | 19 | C | Blood | -0,03402 | 5,07E-15 | MIX | 5257 | |
| GATAD2A | 19 | T | Blood | 0,163165 | 3,74E-06 | MIX | 670 | |
| MAU2 | 19 | T | Blood-T cell CD4+ | -4,67124 | 2,99E-06 | EUR | 293 | |
| MAU2 | 19 | T | Blood | -0,19358 | 6,75E-14 | MIX | 670 | |
| MAU2 | 19 | T | Blood | -0,18721 | 2,07E-07 | EUR | 369 | |
| TM6SF2 | 19 | T | Adipose-Subcutaneous | 0,32323 | 7,09E-05 | MIX | 581 | |
| YJEFN3 | 19 | T | Large Intestine-Colon | 0,200617 | 7,71E-05 | MIX | 318 | |
| LYPLAL1 rs12137855 | ||||||||
| LYPLAL1 | 1 | C | Lymphocyte | -0,122143 | 0,00085 | EUR | 368 | |
| LYPLAL1 | 1 | NA | Blood | -0,220481 | 0,000305 | EUR | 240 | |
| SLC30A10 | 1 | NA | Stem cell-iPSC | -0,143156 | 0,0313 | EUR | 215 | |
| LYPLAL1 | 1 | T | Blood-B cell | -2,04427 | 0,0409 | EUR | 45 | |
| RPS15AP12 | 1 | T | Adipose | 0,146055 | 0,0723 | EUR | 434 | |
| AC096642.1 | 1 | T | Artery-Tibial | -0,14702 | 1,58E-05 | MIX | 584 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



