Submitted:
09 July 2023
Posted:
10 July 2023
You are already at the latest version
Abstract
Our ability to cure common diseases is still in danger due to the creation and spread of bacteria and fungi that are resistant to drugs and has developed new resistance mechanisms. The increasing global expansion of multi- and pan-resistant bacteria commonly referred to as "superbugs," which cause diseases that cannot be treated with current antimicrobial medications like antibiotics, is particularly concerning. Indirect and direct risks to public health are posed by microorganisms that are resistant to antibiotics in food. Food can get contaminated via cross-contamination, intentionally introducing resistance genes during food preparation, and antibiotic-resistant bacteria in food. Consuming unprocessed or unpreserved food products increases the danger of transferring antimicrobial resistance to people and other animals. Stressed cells in food can have an impact on food quality, safety, and security. They can also contribute to the development of resistance and afterwards spread it to unintended organisms in the food chain. These reviews look at a variety of topics to address the question of how antimicrobial resistance mechanisms work. The various types of bacteria that make up infections are examined, as well as the usage of antimicrobial agents and the requirement for alternative antimicrobial agents that will discourage the use of synthetic antimicrobial agents. Additionally, specific details are provided regarding the uniqueness, interdependence, and phylogenicity of organisms as well as their interactions with various ecological media. Thus, it is clear why it is important to work with food producers and handlers to stop the spread of pathogenic organisms.
Keywords:
public health
; antimicrobial resistance
; food safety
; food poisoning
; pathogenic speciation
Introduction
In the previous 70 years, there has been a dramatic improvement in world health, and antibiotics have become the mainstay for the treatment of infectious diseases. Today, millions of patients survive once-fatal diseases. However, because they are limited resources, abuse has accelerated the development of antibiotic resistance and lowered efficacy within a few years of the release of each new antibiotic. Antibiotic resistance is ranked as a "global security threat" by the World Health Organization, at par with terrorism and climate change in terms of its impact on global health, food security, and safety. The goal of this review is to build a platform for food safety and security that is free from pathogenic diseases caused by their resistance to antimicrobial agents in the food chain. This will improve food quality. According to [1], there have been an increasing number of microorganisms emerging pathogens in our environment". In this review, it's important to keep in mind that "emerging" describes pathogens that appeared to have become more prevalent in specific media, were previously were unidentified or hard to identify, or for which foods are the only source to be identified as spread mediums. The range of pathogenic viruses that affect food and food-related products is different from that which is hazardous to other products. Most lately, the bacterial group has garnered the most interest when it comes to food pathogens and their resistance to antimicrobial agents. In most cases, outbreaks of foodborne illness are linked to Salmonella enteritidis, multidrug-resistant Salmonella typhimurium DT 104, Escherichia coli serotype O157:H7, and Campylobacter (jejuni or coli) [2]. Listeria monocytogenes, a psychrotrophic organism, can also be regarded as an emerging pathogen because recent outbreaks in developed nations such as Australia, France, the USA, and Switzerland were caused by Listeria monocytogenes growth in processed meat, milk, and fish products during storage. With the discovery of prions, a new class of infectious agent was discovered; for instance, the bovine spongiform encephalopathy (BSE-causing agent) from tainted bovine food has been connected to a novel type of transmissible spongiform encephalopathy in humans. The list of the most significant novel pathogens for food, both processed and raw food, is longer and includes bacteria (pathogenic E. coli, Yersinia, Legionella, and Aeromonas strains), viruses (Calici and other viruses), and protozoa (Cryptosporidium, Giardia, and Entamoeba histolytica) [3], see Table 1. Since antimicrobial resistance has the potential to have a detrimental effect on human health on a worldwide scale, it continues to be of great interest to various food producers. Food contamination can occur at any point, from the field to the store, due to antibiotic-resistant bacteria and/or genes (transfer in pathogenic microorganisms) [4]. Antibiotic-resistant bacterial infections are more common in low- and middle-income countries than in developed nations, [2]. Foodborne infections are the main cause of illness and mortality worldwide. Pathogenic microorganisms can be transmitted directly or indirectly from food to consumers. Therefore, a variety of national and international strategies are required to prevent the spread of foodborne diseases and to advance the safety and security of food.
The Use of Antimicrobial Agents and its Affects Resistance
Antimicrobial resistance occurs when bacteria, fungi, and other microorganisms learn to resist the medications meant to kill them. Treatment for resistant infections can be challenging and perhaps impossible. Antimicrobial resistance is a process that happens naturally [5]. However, a combination of bacteria exposed to antibiotics and antifungals, as well as the dissemination of those bacteria and their resistance mechanisms, is what causes an increase in antimicrobial resistance [6]. Antibiotic resistance does not imply that our bodies cannot be treated with antibiotics or antifungals [7]. It denotes that the infection-causing bacteria or fungi are immune to the antibiotic or antifungal treatment. While saving lives, antibiotics and antifungals can also help to breed resistant bacteria [7,8]. Antibiotics and antifungals force bacteria and fungi to adapt, which speeds up the development of antimicrobial resistance [8]. The microorganisms that are resistant to antibiotics endure and proliferate. The DNA of these resilient germs contains resistance features that they can pass on to other pathogens [8]. Germs can create defences against antibiotics and antifungals to survive. The germ's resistance is determined by certain proteins that DNA instructs the germ to produce. Genes for resistance may differ between bacteria and fungi. All antibiotics or antifungals lose their effectiveness when bacteria that are already difficult to treat have the ideal combination of resistance mechanisms, leading to untreatable infections. It is concerning that bacteria that are resistant to antibiotics and antifungals have resistance mechanisms in common with other bacteria [9], which is illustrated in Figure 1.
Mechanisms of Antimicrobial Resistance
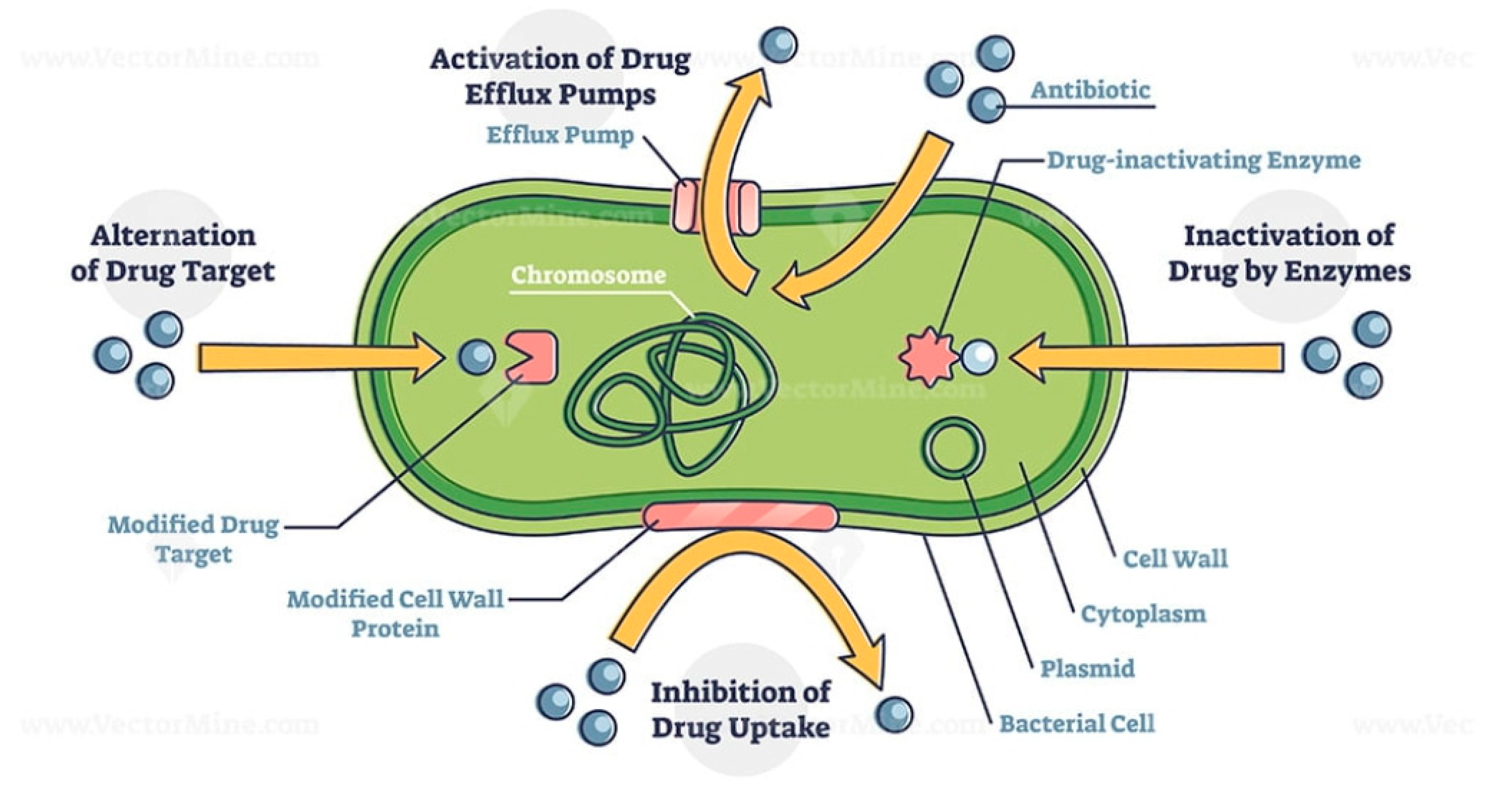
Bacterial pathogens can acquire genes and mutations that cause resistance to antibiotics in addition to the intrinsic mechanisms of resistance. In some circumstances, bacteria may develop numerous defence mechanisms against the same antibiotic, and multidrug-resistant bacteria develop resistance to various antibiotic classes. Below are the different ways in which antimicrobial agents post resistance to some antibiotics [11].
- Enzyme inactivation
Penicillin (a -lactam antibiotic) resistance was one of the first mechanisms of resistance to be identified. It was discovered that penicillin-resistant strains of Staphylococcus aureus had developed an enzyme called a -lactamase (formerly known as a penicillinase). The -lactam ring, a component of -lactam antibiotics that are present in all -lactam antibiotics, is the target of -lactamase enzymes. This ring is split apart by the -lactamase enzyme, which prevents the antibiotic from attaching to its intended target [11,12]. There are thousands of different types of the enzyme family known as -lactamases, which are present in many bacterial infections. Some of them will work against particular members of the -lactam family while others won't because they have different actions. The most problematic -lactamase family members are those known as Carbapenemases because they break down all antibiotics in the -lactam family, including carbapenems, drastically reducing the range of available treatments.
- b.
- Enzyme modification
Bacteria gaining enzymes is a second way that resistance is mediated. First off, bacteria can produce enzymes that chemically alter the antibiotic's target by including extra chemical groups. The erm (erythromycin ribosomal methylation) gene, which confers resistance against macrolide antibiotics such as erythromycin, is an illustration of this. The ribosome, which is the target of the drug erythromycin, is methylated by this enzyme (a methyl group, CH3, is added). As a result, erythromycin can no longer connect to the target, allowing the bacteria to survive and grow while the antibiotic is present. The second kind of enzyme works by chemically altering the antibiotic to stop it from attaching to its target spot. This is illustrated by aminoglycoside-modifying enzymes like N-acetyltransferases, which change aminoglycoside antibiotics like kanamycin by adding an extra acetyl group (CH3CO). Because it can no longer connect to the ribosome, the bacteria become resistant. These enzymes come in a wide variety of forms, each of which reacts differently with various classes of antibiotics, such as aminoglycosides, tetracyclines, phenicols, and lincosamides [11].
- c.
- Modification of the antibiotic target site
By altering the target of the antibiotic, microorganisms frequently develop resistance to that drug. Bacteria reproduce and copy their genome as they develop and proliferate. Sometimes when they do this, errors in the DNA sequences are included (for instance, an A might be changed to a C). These errors are extremely uncommon, but because bacteria have such enormous populations (billions and trillions), they occur frequently enough that occasionally these mutations can be found in bacterial populations when antibiotics are present. Sometimes these mutations result in the antibiotic's inability to function if they occur near a gene that codes for a protein that is the target of the antibiotic. The remainder of the population will perish, but the bacteria with the mutation will have an edge in terms of growth and survival. The accumulation of mutations in the penicillin-binding proteins (PBP), which are the drug's target, is a common mechanism for penicillin resistance in Streptococcus pneumoniae. Penicillin can no longer bind to the PBPs and kill the bacteria because of the alterations in these proteins. Similar to this, ciprofloxacin resistance in many bacterial infections is caused by mutations in the DNA gyrase and DNA topoisomerase IV genes, which are ciprofloxacin's targets [11,12].
- d.
- Replacement of the target site
An additional copy of the gene encoding a protein that nonetheless retains action (e.g., the antibiotic can't bind to it) in the presence of the antibiotic is another such mechanism of resistance used by bacteria like Streptococcus pneumoniae. This is how the organism Staphylococcus aureus develops resistance to penicillin and other -lactam drugs. Methicillin-resistant The Staphylococcus aureus strain known as MRSA, which is resistant to -lactam antibiotics, develops resistance by producing an additional copy of the penicillin-binding protein 2 that -lactam drugs target. Penicillin-binding protein 2a (PBP2a), the extra variant can still function in the presence of -lactam drugs [12].
- e.
- Overproduction of the target
The antibiotic target can also be overproduced by bacteria, which means that there is more of the antibiotic's protein target than there is of the antibiotic itself. This is a method of trimethoprim resistance in Escherichia coli and Haemophilus influenzae, and it indicates that there is enough of the target protein for it to continue playing its role in the cell in the presence of antibiotics. Overexpression and mutations that make an antibiotic less able to attach to its target can occasionally be detected together. (Note: Co-trimoxazole, or SXT, is the common name for the combination of trimethoprim and sulfamethoxazole) [12].
- f.
- Efflux and reduced permeability
We covered how reduced permeability and efflux pumps cause some bacterial species to be inherently resistant to specific antibiotics in the previous section. Additionally, bacteria can develop new efflux pumps that only discharge a single class of antibiotic, such as TetA efflux pumps that only discharge tetracycline from the cell. Porins are proteins that act as channels through the cell membrane, and mutations in these proteins can change how permeable a cell is. Porin loss, changes to the size or conductance of the porin channel, and decreased porin expression are a few examples of these alterations. Ultimately, by either exporting the antibiotic or preventing its importation, respectively, both mechanisms—efflux pumps and reduced permeability—reduce the intracellular antibiotic concentration in the bacterial cell [11,12,13].
Mechanisms of antibiotic resistance outline illustrated. Alternation of drug target, activation of drug efflux pumps, inhibition of drug uptake and inactivation of drug by enzymes.
Figure 2.
Schematic illustration of mechanisms of antibiotic resistance in microorganisms. Adapted from: https://www.pinterest.com/pin/919649186387837246/ [14].
Figure 2.
Schematic illustration of mechanisms of antibiotic resistance in microorganisms. Adapted from: https://www.pinterest.com/pin/919649186387837246/ [14].
Antimicrobial Resistance in Food Quality
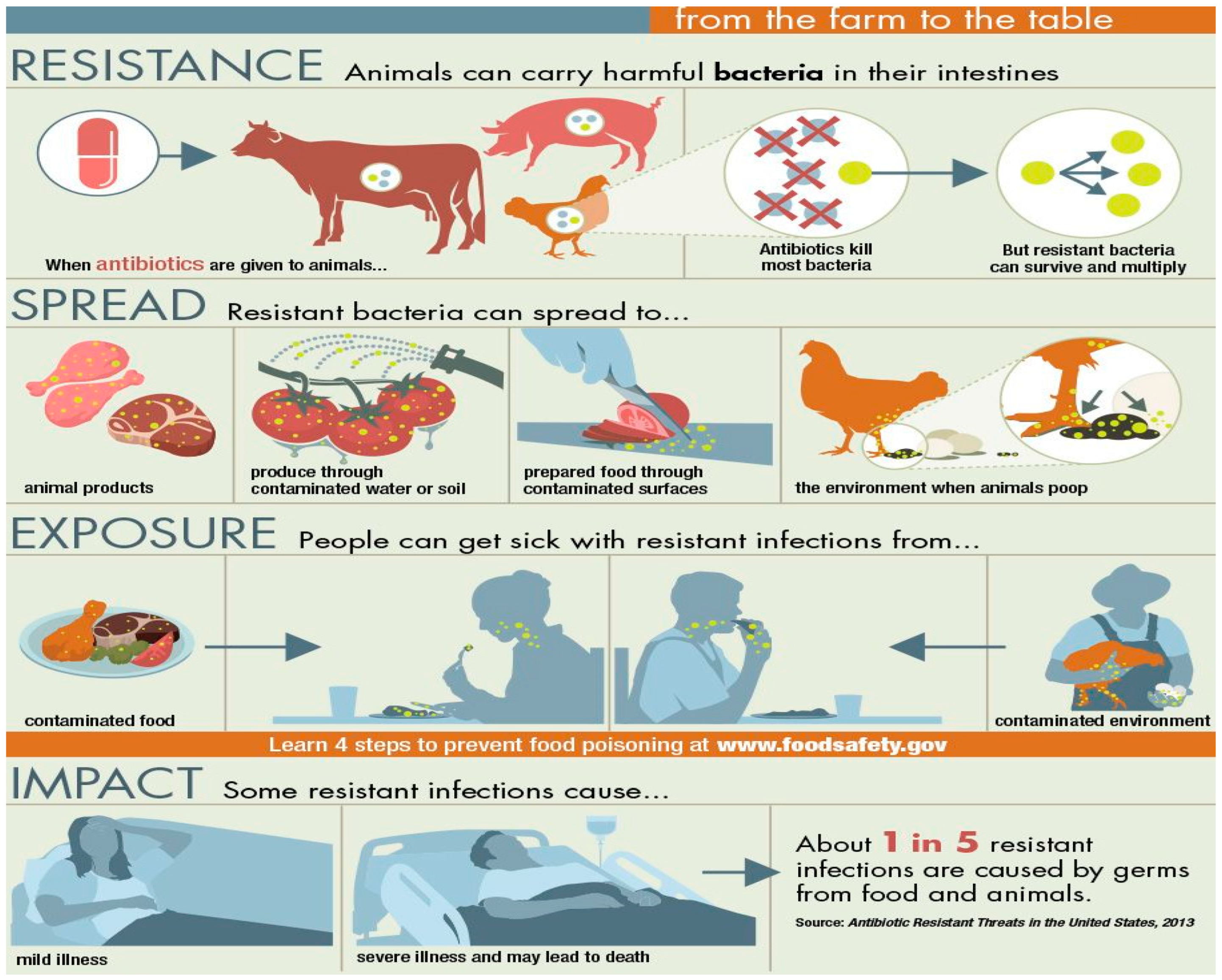
To ensure food safety and quality, animal health, welfare, and farmers' income, antimicrobial agents play a crucial role in treating land and aquatic organisms and plants that produce food. Antimicrobial agents can be used in food animal breeding to cure ill animals, stop the spread of infections, or hasten animal growth by adding low quantities of antimicrobial agents to animal feed [10]. Although this third use is being rejected more and more, it is nevertheless used in many nations. Antimicrobial agents like antibiotics and fungicides are also applied to crops and are employed in agro-industries, such as the manufacturing of biofuel by-products, even though the majority of antibacterial use in agriculture tends to be for food animal production [15]. Food consumption is rising as a result of an expanding global population. In turn, this is straining the infrastructure and supply chains for food. Due to a lack of restrictions and inadequate data collection in many nations, it is challenging to quantify the global antimicrobial use in food production. With a surge in the need for food and goods from animals, it is anticipated that a high volume would expand over time. Antimicrobials may be expelled in water and animal excrement up to 90% of the time after injection without being digested, which allows them to spread to different environmental media due to humans, animals, and plant interactions [16] Table 2 shows the different types of microorganisms possible in different food and a particular time.
Figure 2 is a pictorial illustration of how antimicrobial agents are randomly spread in the food chain and how they affect food quality. Consequently, exposure to antimicrobial residues may promote the growth of AMR microbes and enhance the spread of resistance through the transfer of resistance genes to other microorganisms. Antimicrobial agents can be used less frequently during food production by using several strategies. The use of feed constituents or additions that improve gut health and conversion of feed efficiency, among other things, would result in better animals or crops, reduced demand for antibiotics, and improved sanitation [18].
Figure 2.
Spread of antimicrobial agents in foods to animals and humans. Sources: [18], CDC 2022.
Figure 2.
Spread of antimicrobial agents in foods to animals and humans. Sources: [18], CDC 2022.
Pyrogenicity of different Organisms
When building phylogenies, the similarity between a species' traits is evaluated to indicate relatedness. This is often accomplished for pathogenic bacteria by sequencing the genome or other genetic data [19]. Gene sequences, 16S rRNA, and complete genomes are common candidates for organizational structures in pathogenic bacteria. But because the final phylogenetic trees might vary based on the sources of the data and the techniques employed to generate the trees, phylogenetic trees are always being updated and discussed. Aligning the sequences of the various species is typically one of the first steps in determining which sequences are modified and which sequences are conserved. Genes that are generally expressed in bacteria and other microbes can be transferred horizontally [20]. Then, based on whether certain regions have changed as well as how probable particular regions are to change, the similarities and differences in the genes or genomes are used to predict how closely related the species are. A change in a crucial gene between two species is likely to imply more distant relatedness since, for instance, critical genes required for certain cell functions are less likely to change than unused portions of the genome. When building phylogenies for harmful bacteria, numerous key features are of relevance. Genomic islands are regions of the genome that have undergone horizontal gene transfer and as a result, include genes beneficial to bacteria [21]. Phylogenies can demonstrate how specific bacterial strains acquire the characteristics that make them pathogenic microorganisms. In addition, because they influence how much a species can evolve, phylogenies are crucial for other types of evolutionary inference [22]. Because of their evolutionary relatedness, species within a family are not considered separate data points when assessing attributes, hence care must be given and the phylogenic information must be incorporated.
Figure 2.
Phylogenetic tree of microorganisms. Sources: [23] https://www.pinterest.com/pin/72128031523410933/.
Figure 2.
Phylogenetic tree of microorganisms. Sources: [23] https://www.pinterest.com/pin/72128031523410933/.

Phylogenies Application of Pathogens
Phylogenies of the pathogenic organism are frequently performed in the case of a significant epidemic to identify the source [19]. These investigations frequently try to comprehend and reduce the transmission of diseases. For instance, phylogenetic analyses of Enterobacteriaceae pathogens have revealed how antibiotic-resistance genes move within the genus and that phytopathogenic bacteria, or diseases that affect plants, are the source of virulent genomic islands [21]. Therefore, whether the target host is an animal or a plant, antibiotic resistance can spread across pathogenic families. When compared to other approaches, using phylogenies to understand pathogenic microbes can have certain obvious benefits. For instance, the relationships among Mycobacterium species typically demonstrate aggregation of non-pathogenic taxa and close relationships amongst pathogenic species. This in turn showed that a large number of genes from the non-pathogenic species had been lost in the pathogenic species, likely influencing their evolutionary process. Similarly, Leptospira has a third, intermediates pathogenic branch in addition to a pathogenic and non-pathogenic branch. When considered in the context of phylogeny, profound research into Leptospira proteins and genes that affect pathogenicity makes more sense. For instance, one study [24] demonstrating the genes acquired and lost by pathogenic and intermediately pathogenic species since their split from non-infectious species helps us to better comprehend how bacterial pathogens change and adapt in response to their hosts.
Food Quality and Antimicrobial Agents
In general, the issues facing the food manufacturing sector include meeting consumer demand for high-quality products with longer shelf lives, guaranteeing regulatory compliance, and assuring food safety through best practice methods. As companies look for practical solutions to enhance their capacity to prevent, control, and eliminate undesirable microorganisms in their products, Hazard Analysis and Critical Control Points (HACCP), Good Manufacturing Practices (GMP), and other food safety programs such as microbial intervention, or hurdle, strategies and technologies are important tools at the processor's disposal to meet these challenges [25,26]. Novel antimicrobial preservatives, which are components that, when included in the composition of a product, will prevent the growth of microorganisms, are some of the microbial intervention techniques that appear promising in achieving these aims. The need for natural antibacterial agents to replace synthetic ones is anticipated to grow gradually [27]. Health-conscious customers' expectations that natural antimicrobials solely combat foodborne pathogens and ignore the microbiome of the consumer have given rise to a fresh trend [28]. Researchers have long studied antimicrobial agents to see whether they can destroy or stop the growth of germs in food. This is done to extend the shelf life of food products and improve consumer food safety. Antimicrobial agents have been successfully used in food manufacturing companies as part of process control activities, in the product formulation stage as additives to food intended to mitigate or get rid of pathogens as well as spoilage organisms during the process of making food as aids for processing or secondary food additives [29,30,31]. Antimicrobial use is influenced by several variables, including the desired outcome, permissible usage levels, and impact on food. As part of process control in food manufacturing processes, direct and secondary food additives are undoubtedly some of the most effective and/or promising agents employed today. Organic acids including citric, lactic, and acetic acids are among the antimicrobials that have been the subject of extensive research [31]. These acids can also enhance the flavour of foods that have undergone fermentation or acidification, such as sausages, cheeses, pickles, and sauerkraut. Based on concentration, pH, molarity, and the concentration of the non-dissociated form, organic acids' antibacterial potency varies greatly. The antibacterial chemical trisodium phosphate (TSP) is used in chicken to treat raw, uncooked carcasses and giblets [32,33].
Combating the threat of antibiotic resistance
Hospitals and healthcare organizations can help reduce the threat of antibiotic resistance as it continues to spread throughout the world by giving priority to proper antibiotic use, policy changes to uphold consistent standards for antibiotic application, investments in vaccines, quicker diagnostic testing, and antibiotic stewardship initiatives. Not just for patients and communities in the here and now, but also for decades and generations to come, these activities are crucial. The transition from the antibiotic era to the post-antibiotic age is already underway. Therefore, it is crucial to take into account the following five tactics to combat antibiotic resistance:
- i.
- Utilize current antibiotics wisely
- ii.
- Control the use of antibiotics in crops, food, animals, and people.
- iii.
- Creation of vaccines in advance to reduce antibiotic use.
- iv.
- Improve diagnostic testing speed.
- v.
- Support programs for antibiotic stewardship.
Combination therapy using current antibiotics and intelligent antibiotic adjuvants is one of the various approaches to the rising AMR phenomenon that have been studied so far. In such a scenario, a previously ineffective antibiotic agent is made effective once more against the relevant resistant strain via a multi-targeted strategy.
Aminoglycoside and penicillin are the most popular antibiotic combinations for treating enterococcal infections. Because synergistic interactions are reached, this combination therapy performs significantly better than using just one drug alone. As a result, germs are eliminated more quickly, which also blocks resistance [34]. When taken in conjunction with other medications, antibiotic adjuvants increase the antibacterial activity of the pharmaceuticals rather than having no impact when used alone Willers et al. [35]. Antibiotic adjuvants present a viable strategy for combating antibiotic resistance in this new era of antibiotic resistance, either by directly obstructing resistance or by boosting the effectiveness of other medicines. To combat the formation of resistance, emphasis must be paid to researching novel adjuvant antibiotics Munita et al. [36]. The potential interaction between polyamine-isoprenyl derivatives and florfenicol was described by Borselli et al. By dissipating the proton-motive force (PMF) brought on by the induction of inner membrane depolarization, the molecules prevent efflux pumps [37]. Another study looked at the effects of farnesyl spermine compound in combination with minocycline and doxycycline and found that this significantly reduced P. aeruginosa's antibiotic resistance [38]. The antibacterial activity of medicines can occasionally be improved by coatings of substances. For instance, azelaic acid was pegylated to increase its antibacterial action [39]. In a recent study, computer-guided antibacterial foldamers were created. The MDR in K. pneumoniae, Shigella flexneri, and E. coli was significantly decreased when the foldamers and the antimicrobial peptide PGLa were supplied together [40].
Prevention and management of antimicrobial resistance
Global cooperation is required to combat the spread of antimicrobial resistance and promote the creation of novel medications to stem the tide of AMR. Working collaboratively is also necessary to make sure that healthcare systems worldwide are ready for increased levels of infection and resistance.
Antibiotic resistance can be prevented in part by using antibiotics only when necessary. Antibiotics won't help if they aren't necessary, and their side effects might even be harmful. To enhance patient outcomes, prevent the establishment of AMR, and stop the spread of illnesses brought on by multidrug-resistant organisms, antimicrobial management promotes the responsible use of antibiotics [41,42,43]. The individual's right to treatment should be balanced with society's longer-term requirement for ongoing access to good care [42]. Implementing regulations with evidence-based prescription guidelines is one way to accomplish this [42]. Monitoring programs have been said to be able to lower antibiotic use and resistance; however, it can be difficult to follow them. Lack of surveillance and adequate infection control methods make it difficult to prevent the sale of antibiotics over-the-counter when prescribers are scarce [41]. No conclusive evidence was discovered in a recent systematic analysis of eight management projects. Subpar research designs and varied program elements that preclude the collection of studies are blamed for this [43].
Another comprehensive analysis of the efficiency of 27 management programs in health care in two low- and eleven middle-income nations revealed, in the majority of research, the benefits of the use of antibiotics. However, due to program heterogeneity and inadequate study designs, it was challenging to draw clear findings [43]. In particular, it was determined that behavioural analysts should be involved in programs since management initiatives within medical settings attempt to alter prescribers' behaviour.
Education is a crucial component of stewardship, and there are several signs that medical students lack certain expertise while selecting a course of treatment, for instance. A comprehensive assessment of 57 research found that practitioners have little information about the true incidence of resistance. They agreed that antibiotic resistance was important, but they said that it was "not in their domain" [44]. Improper antibiotic use, can result in Clostridium difficile, can harm normal bacterial flora, and cause infections. Management programs may help stop the spread of these illnesses. In the US, this has been connected to about 14,000 deaths annually [45]. Over two years, an efficient management program in US healthcare facilities showed a drop in C. difficile rates, from 1.5 to 0.5 infections per 1000 beds [45]. Antibiotic-resistant bacteria and C. difficile colonizing rates were reduced, according to a comprehensive review of 32 trials that involved a total of nine million patients.
Fewer instances of community stewards programs that refer to children have been developed, and the majority are for adults. Sweden is once again a prime example, where the overall consumption of antibiotics in outpatient settings fell by 41% between 1992 and 2014. Purchases in the under-five age group dropped from 1,328 to 320 prescriptions per 1,000 people by 76%, Wall [46]. Management of antibiotics outside of the healthcare industry has primarily taken the shape of neighbourhood initiatives. The European Awareness Day, which was introduced on November 18, 2006, by the European Centre for Disease Prevention and Control, is one such instance [46]. Another is the May 5th inauguration of International Hand Hygiene Day, which has the slogan "Fight antibiotic resistance—it's in your hands!" [46].
There is less data from communities and public campaigns about the efficacy of antimicrobial resistance programs than there is from clinical settings. Additionally, the majority of studies have been conducted in regions of Australia, Europe, and the US. The WHO Global Action Plan's inclusion of antibiotic management covers both antibiotic use and universal access to them when necessary. Programs for antibiotic usage face difficulties due to a lack of testing facilities and uncontrolled prescribing. As a result, difficulties are unique in low-resource environments, and the relationship between consumption and resistance is more direct than in high-income environments Aryee and Price [47,48,49,50].
It has been suggested that antimicrobial resistance management can be used to prescribe social norms [49,50,51,52]. The link between individual conduct and population resistance must be made clear, but this is a difficult task. The social cost needs to be made more obvious. Nine out of ten general practitioners (GPs) claim to feel compelled to write antibiotic prescriptions, and 97% of patients who want them receive them, according to the UK's National Institute for Health and Care Excellence (NICE) [53,54,55]. A pragmatic randomized controlled study with 1581 of the UK's top GP prescribers illustrated how feedback might alter prescribing behaviour. The material provided to the first group of GPs explained how their high prescribing rates differed from the usual, while the second group was exposed to a campaign designed to educate people about prescribing. The first group had somewhat fewer people. At monitoring [56,57], the first group had noticeably fewer prescriptions than the second group. This once more demonstrates how behavioural processes, in this case, a person's desire to fit in and feel like a part of the group, may affect prescribing practices [58].
Antimicrobial resistance and alternative
There is a need for new medications that are effective at various periods of the life cycle. Yoshinaga et al. [59] have found that organoarsenic as a natural substance of arsinothricin (AST) is a strong, broad-spectrum antibiotic that stops the growth of a variety of prokaryotic infections. AST is a successful multistage antimalarial intended for Prokaryotic glutamine synthetase (GS) and is inhibited by the nonproteinogenic amino acid analogue of glutamate known as AST. Plasmodium GS, which is expressed at all phases of the parasite life cycle, is more closely linked to prokaryotic GS than eukaryotic GS, according to a phylogenetic study. AST has a strong inhibitory effect on Plasmodium GS, but not on human GS. Notably, AST successfully prevents Plasmodium erythrocytic proliferation and mosquito-borne parasite transmission. Contrarily, AST is not very toxic to a variety of human cell lines, indicating that it is selective for malaria pathogens and has no adverse impact on the human host. This suggests that the lead chemical AST is a good candidate for creating a new class of multistage antimalarials.
There isn't a single universal pathway that has been found to treat AMR. Using antibiotics responsibly while also creating novel products is safer. The most obvious course of action would be to introduce new medicines, but there is little hope based on what happened to earlier antibiotic classes [60,61,62]. Although new commercial structures in public-private partnerships may encourage the development of new drugs, it is also necessary to create alternate prevention and treatment techniques [63]. It's still unclear whether immunization will result in a workable solution [64,65,66]. The health implications for the targeted people to receive vaccinations pose a problem and may imply "fighting evolution with evolution" [67].
Finding antibiotic substitutes that could be combined with others should have an effect and be effective. Phage lysins (viruses that kill bacteria via their lysin enzymes), vaccines as prophylactics, antibodies as prophylactics (restraining the ability of bacteria to cause illness), and probiotics (preventing bacteria from colonizing in the gut) are the methods that are anticipated to have the greatest potential to provide antibiotic alternatives. Although there are differing opinions, [68] concluded that it is preferable to rely on antibiotic alternatives going forward. They proposed that the solutions would require a significant, 10-year-funded, worldwide science endeavour [69]. Numerous studies on probiotics' capacity for prevention have been assessed as alternatives or extra treatments. Probiotics may lessen symptoms, serve as an alternative to antibiotic treatment for less serious infections, and decrease the likelihood of recommending them. Following FAO and WHO definitions, probiotics are "live organisms that, when administered in sufficient amounts, confer a health benefit on the host" [70]. Although probiotics and food supplements have grown in popularity among consumers and businesses, research in these fields has lagged [71]. Single studies might offer little evidence on their own. Therefore, it is crucial to conduct reviews of the combined and distilled findings of resistant bacterial strains. A thorough investigation of probiotics examines their potential value in managing the symptoms of various illnesses, specifically whether they could take the place of antibiotics in the treatment of several infectious diseases.
Probiotics have been shown by [72] to be able to stabilize the intestinal microbiota (microflora), whose alterations are one of the major adverse effects of antibiotics in addition to the resistance issue. Probiotics' capacity to reduce antibiotic-associated diarrhoea (AAD), by co-administering probiotics while receiving antibiotics is one of their advantages.
Studies are encouraged to look at how probiotics regulate and maybe boost biodiversity because the microbiota is becoming a more important target for illness prevention and management [73]. Probiotics may necessitate the spread of resistance genes to antibiotics from the colon to other regions if they are the alternate antibiotic [74]. To determine the effectiveness and potential negative effects of probiotics as a means of slowing the establishment of resistance, more research is required. Probiotic-treated children had a 29% lower likelihood of receiving an antibiotic prescription than the control group, which was used to test if the use of probiotics would reduce the need for antibiotics for children's acute illnesses. Probiotics may be used to treat Helicobacter pylori infections, according to [75], there is significant debate regarding how probiotics affect the immune system. Probiotics have not been shown to significantly boost the rate of H. pylori eradication, primarily due to the lack of data that is statistically significant in clinical trials. However, it appears that there is enough data to support the use of probiotics instead of antibiotics for some less severe infectious disorders [76]. The use of faecal microbial transplantation (FMT) to treat CDAD [77] as an alternative to conventional antibiotic treatment is the most persuasive proof. In this case, the strategy is to transfer a healthy donor microbiota, boost the recipient's gut's microbial diversity, and compete with resistant or toxin-producing bacteria. As a result, a harmonious, diversified microbiome may hinder the growth of bacterial clones that are resistant to being treated. Future research must equally consider the efficacy and possible damage of such alternatives.
Conclusion
The goal of this review is to lay the groundwork for a food safety and security system free of pathogenic diseases brought on by the food chain's antimicrobial agent resistance. Pathogenic microbes like Salmonella enteritidis, Salmonella typhimurium that is multidrug-resistant, Escherichia coli serotype O157:H7, and Campylobacter are more common in particular media and are challenging to diagnose. Another developing pathogen is the psychrotrophic bacterium Listeria monocytogenes. A new class of infectious agents, such as bovine spongiform encephalopathy, has emerged as a result of the discovery of prions. Bacteria, viruses, and protozoa are on the list of major new pathogens for food. Food producers need to execute various national and international measures to combat antimicrobial resistance because it has the potential to negatively affect human health globally.
The local, national, and international uses and abuses of antibiotics are extensively documented. The One-Health approach recognizes the need for a scientifically sound intersection of biomedical, environmental, animal, and nutrition fields. Additionally, it is necessary to conduct implementation research in which treatments are developed and assessed based on already-known information. Since more antibiotics are used for animals than for humans to generate food, encourage development, and prevent disease, there is a need for closer cooperation and improved documentation of antibiotic use across sectors. It's important to address the economic factors driving the spread of infectious illnesses and drug resistance. Antimicrobial resistance in food must be addressed globally to comprehend the implications of inaction, which will be irreversible. Similar to cancer, the fight against smoking, and HIV/AIDS, the AMR crisis are required to be elevated to the status of a major societal issue. Everyone, across all cultures, must believe that AMR is relevant to their life. Understanding the population impact of various AMR diversity is necessary to create a preventive intervention platform. As well as determining the effects of dose, duration, and adherence in antibiotic therapy. On the emergence of resistance, research is required to evaluate the connections between the use of antibiotics in primary healthcare and serious illnesses that require treatment in a secondary care facility. We require rigorous unbiased research with appropriate control groups. The database for management initiatives is thin despite several assessments being conducted in some areas because of program variability and subpar study designs. There is a demand for evaluation models that combine qualitative and quantitative methodologies. The social and cultural norms around clinical practice and prescription should be considered. Programs that take place outside of a hospital, including community or public awareness campaigns, have not been evaluated. More studies are required, and their background is crucial, especially in food quality and safety. The cost and performance of healthcare management programs require thorough, applicable data to safeguard the health of the populace.
Disclaimer
the author hereby declares that there is no competing interest regarding the publication of this article.
References
- Samtiya, M.; Matthews, K.R.; Dhewa, T.; Puniya, A.K. Antimicrobial Resistance in the Food Chain: Trends, Mechanisms, Pathways, and Possible Regulation Strategies. Foods 2022, 11, 2966. [CrossRef]
- Tanvir, M. U.; Arka, J.; Chakraborty, A. K.; Redwan, M. Z.; Saikat, M. T. B. E.; Kuldeep, D. M.D.; Kamal, H. R.; Márió, G.; Muhammad, U. K.; Sahibzada, Md. J.; Hossain, N. K. Antibiotic resistance in microbes: History, mechanisms, therapeutic strategies and prospects, Journal of Infection and Public Health, 2021, 14, 12, 1750-1766. [CrossRef]
- Thomas, E.; Wolfgang, K; Leo, M. Pathogenic microbes in water and food: changes and challenges, FEMS Microbiology Reviews, 2002, 26(2), 111–112. [CrossRef]
- Jans, C.; Sarno, E.; Collineau, L.; Meile, L.; Stärk, K.D.C.; Stephan, R. Consumer Exposure to Antimicrobial Resistant Bacteria from Food at Swiss Retail Level. Front. Microbiol. 2018, 9:362. [CrossRef]
- David, W. N; John E. M.; Juluri, R. R. Antimicrobial resistance (AMR): significance to food quality and safety, Food Quality and Safety, 2019, 3, 15–22. [CrossRef]
- Jonathan, G. F.; Charlene R. J. Genetic mechanisms of antimicrobial resistance identified in Salmonella enterica, Escherichia Coli, and Enterococcus spp. Isolated from U.S. food animals. Frontier in Microbiology, 2013, 4, 35 1 - 22. [CrossRef]
- FOA 2017www.fao.org/food-chain-crisis; http://www.fao.org/antimicrobial-resistance, Retrieved 0n 24th June, 2023.
- Vikesland, P.; Garner, E.; Gupta, S.; Kang, S.; Maile-Moskowitz, A., Zhu, N. Differential Drivers of Antimicrobial Resistance across the World. Acc Chem Res. 2019 Apr 16;52(4):916-924. [CrossRef]
- https://www.pinterest.com/pin/325596248054170021/.
- Djordjevic, S. P.; Stokes, H. W.; Chowdhury, P. R. Mobile elements, zoonotic pathogens and commensal bacteria: conduits for the delivery of resistance genes into humans, production animals and soil microbiota. Front Microbiol. 2013; 4:86. [CrossRef]
- Peterson, E.; Kaur, P. Antibiotic Resistance Mechanisms in Bacteria: Relationships Between Resistance Determinants of Antibiotic Producers, Environmental Bacteria, and Clinical Pathogens. Frontiers in Microbiology, 2018; 9. DOI=10.3389/fmicb.2018.02928.
- Hallsworth, M.; Sallis, C. T. Provision of social norm feedback to high prescribers of antibiotics in general practice: a pragmatic national randomised controlled trial. Lancet. 2016; 387:1743–1752. [CrossRef]
- Kmietowicz, Z. New antibiotics: NHS will test “pay for usefulness” model to stimulate research. BMJ. 2019; 366:l4610. [CrossRef]
- García-Quintanilla, M.; Pulido, M. R.; Carretero-Ledesma, M. Vaccines for antibiotic-resistant bacteria: possibility or pipe dream? Trends Pharmacol Sci. 2016; 37:143–152. [CrossRef]
- Fletcher, S. Understanding the contribution of environmental factors in the spread of antimicrobial resistance. Environ Health Prev Med. 2015 20(4):243-52. [CrossRef]
- Hu, Y.; Yang, X.; Li, J.; Lv, N.; Liu, F.; Wu, J.; Lin, I. Y.; Wu, N.; Weimer, B. C.; Gao, G. F.; Liu, Y.; Zhu, B. The Bacterial Mobile Resistome Transfer Network Connecting the Animal and Human Microbiomes. Appl Environ Microbiol. 2016, 27, 82(22):6672-6681. https://doi: 10.1128/AEM.01802-16.
- Abdelhamid, A. G.; El-Dougdoug, N. K. Controlling foodborne pathogens with natural antimicrobials by biological control and antivirulence strategies. Heliyon. 2020; 6(9):e05020. [CrossRef]
- Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Division of Foodborne, Waterborne, and Environmental Diseases (DFWED), 2022.
- Ryding, Sara. (2019). Phylogenies of Pathogenic Microorganisms. News-Medical. Retrieved on June 25, 2023, from https://www.news-medical.net/life-sciences/Phylogenies-of-Pathogenic-Microorganisms.aspx.
- Piña-Iturbe, A.; Ulloa-Allendes, D.; Pardo-Roa, C. Comparative and phylogenetic analysis of a novel family of Enterobacteriaceae-associated genomic islands that share a conserved excision /integration module. Sci Rep 2018, 8, 1029. [CrossRef]
- Fouts, D. E.; Matthias, M. A.; Adhikarla, H.; Adler, B.; Amorim-Santos, L.; Berg, D. E. What Makes a Bacterial Species Pathogenic? Comparative Genomic Analysis of the Genus Leptospira. PLoS Negl Trop Dis. 2016 10(2): e0004403. [CrossRef]
- Prasanna, A. N.; Mehra, S. Comparative Phylogenomics of Pathogenic and Non-Pathogenic Mycobacterium. PLOS ONE, 2013, 8(8), e71248. [CrossRef]
- https://www.pinterest.com/pin/72128031523410933/.
- Skandalis, N.; Maeusli, M.; Papafotis, D.; Miller, S.; Lee, B.; Theologidis, I.; Luna, B. Environmental Spread of Antibiotic Resistance. Antibiotics (Basel). 2021 27;10(6):640. [CrossRef]
- Možina, S.; Klančnik, A.; Kovac, J.; Jeršek, B.; Bucar, F. Antimicrobial Natural Products Against Campylobacter. In: Mérillon, JM., Riviere, C. (eds) Natural Antimicrobial Agents. Sustainable Development and Biodiversity, 2018, 19. doi.org/10.1007/978-3-319-67045-4_1.
- Mathela, C. S.; Kumar, V. (2018). Antifungal Activities of Essential Oils from Himalayan Plants. In: Mérillon, JM., Riviere, C. (eds) Natural Antimicrobial Agents. Sustainable Development and Biodiversity, 2018, 19. doi.org/10.1007/978-3-319-67045-4_4.
- Rabin G.; Salam A. I. Natural products as antimicrobial agents, Food Control, 2014; 46, 412-429, doi.org/10.1016/j.foodcont.2014.05.047.
- Quinto, E.J.; Caro, I.; Villalobos-Delgado, L. H.; Mateo, J; De-Mateo-Silleras, B.; Redondo-Del-Río, M. P. Food Safety through Natural Antimicrobials. Antibiotics (Basel). 2019; 31;8(4):208. [CrossRef]
- Holley, R. A.; Patel, D. Improvement in shelf-life and safety of perishable foods by plant essential oils and smoke antimicrobials. Food Microbiol. 2005; 22:273–292. [CrossRef]
- Davidson, P. M.; Critzer, F. J.; Taylor, T. M.; Naturally occurring antimicrobials for minimally processed foods. Annu Rev Food Sci Technol. 2013; 4:163-90. [CrossRef]
- Teshome, E.; Forsido, S.F.; Rupasinghe, H. P. V.; Olika, K. E. Potentials of Natural Preservatives to Enhance Food Safety and Shelf Life: A Review. Scientific World Journal. 2022; 9901018. [CrossRef]
- https://www.fightbac.org/food-poisoning/foodborne-pathogens/.
- Verraes, C.; Van, B. S.; Van, M. E.; Van, C. E.; Butaye, P.; Catry. B.; de Schaetzen, M. A.; Van, H. X.; Imberechts, H.; Dierick, K.; Daube, G.; Saegerman, C.; De Block, J.; Dewulf, J.; Herman L. Antimicrobial resistance in the food chain: a review. Int J Environ Res Public Health. 2013 28;10(7):2643-69. [CrossRef]
- Reygaert, W. C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018 26;4(3):482-501. [CrossRef]
- Willers, C.; Wentzel, J. F.; du-Plessis, L. H.; Gouws, C.; Hamman, J. H. Efflux as a mechanism of antimicrobial drug resistance in clinical relevant microorganisms: the role of efflux inhibitors. Expert Opin Ther Targets. 2017 21(1):23-36. [CrossRef]
- Munita, J. M.; Arias, C. A.; Mechanisms of Antibiotic Resistance. Microbiol Spectr. 2016 4(2):10.1128/microbiolspec.VMBF-0016-2015. [CrossRef]
- Tegos, G. P.; Haynes, M.; Strouse, J. J.; Khan, M. M.; Bologa, C. G.; Oprea, T. I.; Sklar, L. A.; Microbial efflux pump inhibition: tactics and strategies. Curr Pharm Des. 2011; 17(13):1291-302. [CrossRef]
- Medina, E.; Pieper, D. H. Tackling Threats and Future Problems of Multidrug-Resistant Bacteria. Curr Top Microbiol Immunol. 2016; 398:3-33. [CrossRef]
- Kaye, K. S.; Fraimow, H. S.; Abrutyn E. Pathogens resistant to antimicrobial agents. Epidemiology, molecular mechanisms, and clinical management. Infect Dis Clin North Am. 2000; 14(2):293-319. [CrossRef]
- Williams, J. D.; Sefton, A. M. The prevention of antibiotic resistance during treatment. Infection. 1999; 27 Suppl 2:S29-31. [CrossRef]
- Editorial. NICE antimicrobial stewardship: right drug, dose, and time? Lancet. 2015; 386:717. [CrossRef]
- Annunziato, G.; Strategies to Overcome Antimicrobial Resistance (AMR) Making Use of Non-Essential Target Inhibitors: A Review. Int J Mol Sci. 2019;20(23):5844. [CrossRef]
- Uchil, R. R.; Kohli, G. S.; Katekhaye, V. M.; Swami, O. C.; Strategies to combat antimicrobial resistance. J Clin Diagn Res. 2014; 8(7):ME01-4. [CrossRef]
- Sarfraz, A.; Muhammad, Z. A.; Safa, R.; Seham, E. A.; Mohibullah, S.; Nur, A. C. J.; Suvash C. S. "Recent Approaches for Downplaying Antibiotic Resistance: Molecular Mechanisms", BioMed Research International, 2023, Article ID 5250040, 27 pages. [CrossRef]
- https://www.gavi.org/vaccineswork/what-antimicrobial-resistance-and-how-can-we-tackle-it?gclid=Cj0KCQjwnf-kBhCnARIsAFlg492wec2dzban88CsvAozlXO3gd_tHJJRl1-Q9rprteF-9Gy9XjNouTAaApN8EALw_wcB.
- Wall, S. Prevention of antibiotic resistance - an epidemiological scoping review to identify research categories and knowledge gaps. Glob Health Action. 2019; 12(1):1756191. [CrossRef]
- Aryee, A. Price, N. Antimicrobial stewardship – can we afford to do without it? Br J Clin Pharmacol. 2014; 79:173–181. [CrossRef]
- Dyar, O. J.; Huttner, B.; Schouten, J. What is antimicrobial stewardship? Clin Microbiol Infect. 2017; 23:793–798.
- Bertollo, L. G.; Lutkemeyer, D. S.; Levin, A. S. Are antimicrobial and stewardship programs effective strategies for preventing antibiotic resistance? A systematic review. Am J Infect Control. 2018; 46: 824–836. [CrossRef]
- Van Dijck, C.; Vlieghe, E.; Cox, J. A. Antibiotic stewardship interventions in hospitals in low-and middle- income countries: a systematic review. Bull World Health Organ. 2018; 96:266–280. [CrossRef]
- McCullough, A. R.; Rathbone, J.; Parekh, S. Not in my backyard: a systematic review of clinicians’ knowledge and beliefs about antibiotic resistance. J Antimicrob Chemother. 2015; 70: 2465–2473. [CrossRef]
- Piacenti, F. J.; Leuthner, K. D. Antimicrobial stewardship and clostridium difficile–associated diarrhoea. J Pharm Pract. 2013; 26:506–513. [CrossRef]
- Baur, D.; Gladstone, B. P.; Burkert, F. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017; 17:990–1001. [CrossRef]
- Principi, N. Esposito S. Antimicrobial stewardship in paediatrics. BMC Infect Dis. 2016; 16:424.
- McNulty, C. A. M. European Antibiotic Awareness Day 2012: general practitioners encouraged to target antibiotics through guidance, education and tools. J Antimicrob Chemother. 2012; 67: 2543–2546. [CrossRef]
- Pires, D.; deKraker, M. E. A.; Tartari, E.; ‘Fight Antibiotic Resistance—It’s in Your Hands’: call from the World Health Organization for 5th May 2017. Clinl Infect Dis. 2017; 64:1780–1783. [CrossRef]
- Cox, J. A.; Vlieghe, E.; Mendelson, M. Antibiotic stewardship in low- and middle-income countries: the same but different? Clin Microbiol Infect. 2017; 23:812–818. [CrossRef]
- Gould, I. M.; Lawes, T.; Antibiotic stewardship: prescribing social norms. Lancet (Editorial). NICE antimicrobial. 2016; 387:1699–1701. [CrossRef]
- Yoshinaga, M.; Niu, G.; Yoshinaga-Sakurai, K.; Nadar, V.S.; Wang, X.; Rosen, B.P.; Li, J. Arsinothricin Inhibits Plasmodium falciparum Proliferation in Blood and Blocks Parasite Transmission to Mosquitoes. Microorganisms 2023, 11, 1195. [CrossRef]
- Nichol, D. Jeavons, P.; Fletcher, A. G. Steering evolution with sequential therapy to prevent the emergence of bacterial antibiotic resistance. PLoS Comput Biol. 2015, 11:1004493. [CrossRef]
- Ojala, V.; Laitalainen, J.; Jalasvuori, M. Fight evolution with evolution: plasmid-dependent phages with a wide host range prevent the spread of antibiotic resistance. Evol Appl. 2013; 6:925–932.
- Guiton, P.S.; Sagawa, J.M.; Fritz, H.M.; Boothroyd, J.C. An in vitro model of intestinal infection reveals a developmentally regulated transcriptome of Toxoplasma sporozoites and a NF-κB-like signature in infected host cells. PLoS ONE 2017, 12, e0173018. [CrossRef]
- Hendaus, M.A.; Jomha, F.A.; Ehlayel, M. Allergic diseases among children: nutritional prevention and intervention. Ther Clin Risk Manag. 2016, 12:361-72. [CrossRef]
- Mack, D.R. Probiotics-mixed messages. Can Fam Physician. 2005, 51(11):1455-7, 1462-4.
- Holst, H.; Breves, G.P. Erfahrungsmedizin zum therapeutischen Standard [Probiotics--from empirical medicine to therapeutic standard]. Z Gastroenterol. 2005, 43(6):601-6. German. [CrossRef]
- Megha, S.; Shalini, G,; Varsha, S.A.; Abhishek, D.; Neetu, J. Effect of Short-Term Placebo-Controlled Consumption of Probiotic Yoghurt and Indian Curd on the Streptococcus mutanTs Level in Children Undergoing Fixed Interceptive Orthodontic Therapy. Turk J Orthod. 2019, 32(1):16-21. [CrossRef]
- Cabana, M.D.; Shane, A.L.; Chao, C.; Oliva-Hemker, M. Probiotics in primary care pediatrics. Clin Pediatr (Phila). 2006, 45(5):405-10. [CrossRef]
- Kahbazi, M.; Ebrahimi, M.; Zarinfar, N.; Arjomandzadegan, M.; Fereydouni, T.; Karimi, F.; Najmi, A.R. Efficacy of Synbiotics for Treatment of Bacillary Dysentery in Children: A Double-Blind, Randomized, Placebo-Controlled Study. Adv Med. 2016; 2016:3194010. [CrossRef]
- Buhl, M.R. Probiotika til behandling af infektiøs diaré [Probiotics in the treatment of infectious diarrhoea]. Ugeskr Laeger. 2005, 167(22):2427.
- Ouwehand, A.; Vesterlund, S. Health aspects of probiotics. I Drugs. 2003, 6(6):573-80.
- Manzanares, W.; Lemieux, M.; Langlois, P.L.; Wischmeyer, P.E. Probiotic and synbiotic therapy in critical illness: a systematic review and meta-analysis. Crit Care. 2016, 19:262. [CrossRef]
- Baştürk, A.; Artan, R.; Yılmaz, A. Efficacy of synbiotic, probiotic, and prebiotic treatments for irritable bowel syndrome in children: A randomized controlled trial. Turk J Gastroenterol. 2016, 27(5):439-443. [CrossRef]
- Hendaus, M.A.; Jomha, F.A.; Ehlayel, M. Allergic diseases among children: nutritional prevention and intervention. Ther Clin Risk Manag. 2016, 12:361-72. [CrossRef]
- Jiang, Z.; Yuping, Z.; Gang, S. Effect of Probiotic Yogurt Supplementation(Bifidobacterium animalis ssp. lactis BB-12) on Gut Microbiota of Female Taekwondo Athletes and Its Relationship with Exercise-Related Psychological Fatigue, Microorganisms 2023, 11(6), 1403. [CrossRef]
- Weili, S.; Hongpeng, S.; Chengyan, G.; Keyuan. L.; Guangyu, L. Effects of Different Yeast Selenium Levels on Rumen Fermentation Parameters, Digestive Enzyme Activity and Gastrointestinal Microflora of Sika Deer during Antler Growth, Microorganisms 2023, 11(6), 1444. [CrossRef]
- Jang Z.; Yuping, Z.; Gang, S. Effect of Probiotic Yogurt Supplementation(Bifidobacterium animalis ssp. lactis BB-12) on Gut Microbiota of Female Taekwondo Athletes and Its Relationship with Exercise-Related Psychological Fatigue. Microorganisms 2023, 11(6), 1403. [CrossRef]
- Krista, S.; Johanna, H.; Heli, A.; Ashley, A.H.; Ilmari Ahonen, M.T.; Saarinen, J.M.; Arthur C. O. The Effect of Human Milk Oligosaccharides and Bifidobacterium longum subspecies infantis Bi-26 on Simulated Infant Gut Microbiome and Metabolites. Microorganisms 2023, 11(6), 1553. [CrossRef]
Figure 1.
Action Mechanisms for Antimicrobial Agents. Adapted from [10] https://www.pinterest.com/pin/325596248054170021/.
Figure 1.
Action Mechanisms for Antimicrobial Agents. Adapted from [10] https://www.pinterest.com/pin/325596248054170021/.
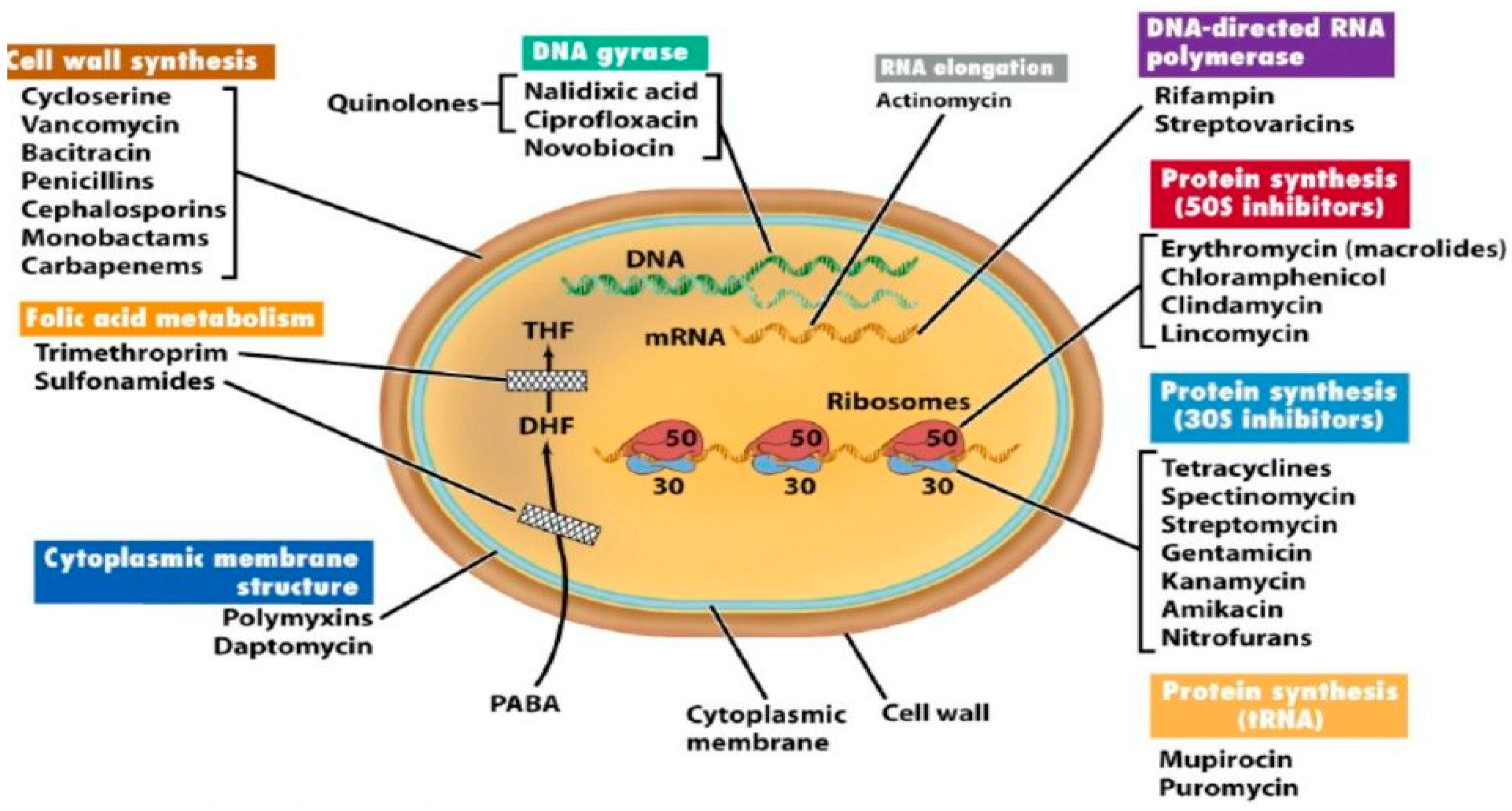

Table 1.
Classification of Common Pathogenic Bacteria.
| Type | Bacteria and associated infections |
|---|---|
|
Obligate aerobic (Gram-negative cocci) |
Moraxella catarrhalis is a gram-negative diplococcus that causes ear and upper and lower respiratory infections. M. catarrhalis was formerly known as Branhamella catarrhalis. Neisseria gonorrhoeae is caused by the bacterium Neisseria gonorrhoeae. It typically infects the epithelia of the urethra, cervix, rectum, pharynx, or conjunctivae, causing irritation or pain and purulence. N. meningitidis Meningococcal (Neisseria meningitidis) are gram-negative diplococci that cause meningitis and meningococcemia. Symptoms, usually severe, include headache, nausea, vomiting, photophobia, and Meningococcal diseases. |
| Gram-positive bacilli | Corynebacterium jeikeium |
| Acid-fast bacilli | Mycobacterium avium complex, M. kansasii, M. leprae, M. tuberculosis, Nocardia species |
| Nonfermentative, non-Enterobacterales (formerly Enterobacteriaceae) | Acinetobacter calcoaceticus, Elizabethkingia meningoseptica (formerly Flavobacterium meningosepticum), Pseudomonas aeruginosa Pseudomonas and Related Infections Pseudomonas aeruginosa and other members of this group of gram-negative bacilli are opportunistic pathogens that frequently cause hospital-acquired infections, particularly in ventilator, P. alcaligenes, others are Pseudomonas species, and Stenotrophomonas maltophilia |
| Fastidious gram-negative coccobacilli and bacilli | Brucella Brucellosis is caused by Brucella species, which are gram-negative bacteria. Symptoms begin as an acute febrile illness with few or no localized signs and may progress to a chronic stage. Bordetella, Francisella, Legionella, and Legionella pneumophila are gram-negative bacillus that most often cause pneumonia with extrapulmonary features. Diagnosis requires specific growth media, serologic or urine antigen. |
| Leptospiraceae (spiral bacteria) | Leptospira Leptospirosis is an infection caused by one of several pathogenic serotypes of the spirochete Leptospira. Symptoms are biphasic. Both phases involve acute febrile episodes. |
| Obligate anaerobic | |
| Gram-negative bacilli | Bacteroides fragilis, other Bacteroides Mixed Anaerobic Infections Anaerobes can infect normal hosts and hosts with compromised resistance or damaged tissues. Mixed anaerobic infections can include both single anaerobic species or multiple anaerobic species... read more species, Fusobacterium species, Prevotella species. |
| Gram-negative cocci | Veillonella species |
| Gram-positive cocci | Peptococcus niger, Peptostreptococcus Mixed Anaerobic Infections Anaerobes can infect normal hosts and hosts with compromised resistance or damaged tissues. Mixed anaerobic infections can include both single anaerobic species or multiple anaerobic species. |
| Non–spore-forming gram-positive bacilli | Actinomyces, Bifidobacterium, Eubacterium, and Cutibacterium (formerly Propionibacterium) species. |
| Endospore-forming gram-positive bacilli | Clostridium botulinum, Botulism is poisoning that is due to Clostridium botulinum toxin and that affects the peripheral nerves. Botulism may occur without infection if the toxin is ingested, injected, or inhaled. C. perfringens Clostridium perfringens is a Food Poisoning Clostridium perfringens Food poisoning is acute gastroenteritis caused by ingestion of contaminated food. Symptoms are watery diarrhoea and abdominal cramps. Diagnosis is by identifying. C. tetani, others are Clostridium species. |
| Facultative anaerobic | |
| Gram-positive cocci, catalase-positive | Staphylococcus aureus is a gram-positive aerobic organism. Staphylococcus aureus is the most pathogenic; it typically causes skin infections and sometimes pneumonia, endocarditis, and osteomyelitis. Staphylococcal Infections(coagulase-positive), S. epidermidis (coagulase-negative), and others are coagulase-negative staphylococci. |
| Gram-positive cocci, catalase-negative | Enterococcus faecalis are gram-positive, facultative anaerobic organisms. Enterococcus faecalis and E. faecium cause a variety of infections, including endocarditis, and urinary tract infections. E. faecium, Streptococcus agalactiae (group B streptococcus), S. bovis, S. pneumoniae Streptococcal Infections Streptococci are gram-positive aerobic organisms that cause many disorders, including pharyngitis, pneumonia, wound and skin infections, sepsis, and endocarditis. S. pyogenes (group A streptococcus), viridans group streptococci (S. mutans, S. mitis, S. salivarius, S. sanguis), S. anginosus group (S. anginosus, S. milleri, S. constellatus), Gemella morbillorum |
| Gram-positive bacilli | Bacillus anthracis Anthrax is caused by the gram-positive Bacillus anthracis, which are toxin-producing, encapsulated, facultative anaerobic organisms. Anthrax is a fatal disease of animals transmitted by Anthrax, Erysipelothrix rhusiopathiae, Gardnerella vaginalis (gram-variable) |
| Gram-negative bacilli | Enterobacterales (Citrobacter species, Enterobacter Klebsiella, Enterobacter, and Serratia Infections). The gram-negative bacteria Klebsiella, Enterobacter, and Serratia are closely related to normal intestinal flora that rarely cause disease in normal hosts. The gram-negative bacterium Escherichia coli is the most numerous aerobic commensal inhabitants of the large intestine. Certain strains cause diarrhoea, and all can cause infection when Klebsiella species, Morganella morganii, Proteus species, Plesiomonas shigelloides, Providencia rettgeri, Salmonella typhi whose genus Salmonella is divided into two species, S. enterica and S. bongori, which include over 2500 known serotypes. Some of these serotypes are named. In such cases, other Salmonella species, Serratia marcescens, Shigella Shigellosis Shigellosis is an acute infection of the intestine caused by the gram-negative Shigella species. Yersinia enterocolitica Plague and Other Yersinia Infections Plague is caused by the gram-negative bacterium Yersinia pestis. |
| Fermentative, non-Enterobacterales | Aeromonas hydrophila, Chromobacterium violaceum, and Pasteurella multocida |
| Fastidious gram-negative coccobacilli and bacilli | Aggregatibacter (formerly Actinobacillus) actinomycetemcomitans, Eikenella corrodens, Haemophilus influenzae Haemophilus Infections. The gram-negative bacteria Haemophilus species cause numerous mild and serious infections, including bacteremia, meningitis, pneumonia, sinusitis, otitis media, cellulitis, and epiglottitis and, other Haemophilus species. |
| Mycoplasma Mycoplasmas | Mycoplasma pneumoniae, Mycoplasmas Mycoplasmas are ubiquitous bacteria that differ from other prokaryotes in that they lack a cell wall. Mycoplasma pneumoniae is a common cause of pneumonia, particularly community-acquired. |
| Microaerophilic | |
| Curved bacilli | Campylobacter jejuni, Helicobacter pylori Infection Helicobacter pylori is a common gastric pathogen that causes gastritis, peptic ulcer disease, gastric adenocarcinoma, and low-grade gastric lymphoma. Infection may be asymptomatic or Vibrio cholerae, and V. vulnificus |
| Spirochaetaceae (spiral bacteria) | Borrelia burgdorferi Lyme is a tick-transmitted infection caused by the spirochete Borrelia species. Treponema pallidum Syphilis is caused by the spirochete Treponema pallidum and is characterized by three sequential symptomatic stages separated by periods of asymptomatic latent infection. |
| Obligate intracellular parasitic | |
| Chlamydiaceae | Chlamydia trachomatis Three species of Chlamydia cause human disease, including sexually transmitted infections and respiratory infections. |
| Coxiellaceae | Coxiella burnetii is an acute or chronic disease caused by the rickettsial-like bacillus Coxiella burnetii. Acute disease causes sudden onset of fever, headache, malaise, and interstitial pneumonitis. |
| Rickettsiales | Rickettsia prowazekii, R. rickettsii, R. typhi, Orientia tsutsugamushi Scrub Typhus Scrub typhus is a mite-borne disease caused by Orientia tsutsugamushi (formerly Rickettsia tsutsugamushi). Scrub Typhus, Ehrlichia chaffeensis Ehrlichiosis and Anaplasmosis Ehrlichiosis and anaplasmosis are caused by rickettsial-like bacteria. Ehrlichiosis is caused mainly by Ehrlichia chaffeensis; anaplasmosis is caused by Anaplasma phagocytophilum and Ehrlichiosis and Anaplasmosis, Anaplasma phagocytophilum. |
Table 2.
Pathogenic organisms and food sources of contamination.
| Types of organisms | Sources Foods |
|---|---|
| Vibrio vulnificus | raw or undercooked seafood, particularly shellfish. |
| Staphylococcus aureus: | cooked foods high in protein (e.g. cooked ham, salads, bakery products, dairy products) that are held too long at room temperature. |
| Shigella | salads, unclean water, and any food handled by someone who is infected with the bacterium |
| Toxoplasma gondii | raw or undercooked pork. |
| Salmonella | raw and undercooked eggs, undercooked poultry and meat, fresh fruits and vegetables, and unpasteurized dairy products |
| Listeria monocytogenes | unpasteurized dairy products, including soft cheeses; sliced deli meats; smoked fish; hot dogs; pate’; and deli-prepared salads (i.e. egg, ham, seafood, and chicken salads). |
| Norovirus | Any food contaminated by someone who is infected with this virus. |
| Clostridium botulinum | improperly prepared home-canned foods; honey should not be fed to children less than 12 months old. |
| E. coli O157:H7 | beef, especially undercooked or raw hamburger; produce; raw milk; and unpasteurized juices and ciders. |
| Campylobacter | raw and undercooked poultry and other meat, raw milk and untreated water. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



