
Submitted:
04 July 2023
Posted:
10 July 2023
You are already at the latest version
Abstract
Objectives The aim of the study is to evaluate the effectiveness of extra virgin olive oil (EVO) and fruity oil for the treatment of gingivitis. Materials and Methods. A sample of 75 patients with gingivitis induced by plaque bacteria, over 18 years of age, was divided into three groups: a study group A with extra virgin olive oil, a study group B with fruity oil and a control group C. In the two study groups, Evo oil was administered as a mouthwash in patients with gingival inflammation. The protocol included a daily application of the product for 30 days, with three recalls 15 days apart. Clinical parameters of plaque formation and gingivitis - plaque index (PI), bleeding index (BI) were assessed at each recall and scored on a specific periodontal chart. The control group re-ceived no mouthwash treatment to normal daily oral hygiene procedures, and the same clinical parameters as the study group were evaluated. Data were evaluated using SPSS 27.0 software for Windows (SPSS Inc., Chica-go, IL, USA). Then, the pre- and post-treatment values of the groups were compared using the t-student test, set-ting P < 0.05 as the significance level. Results Comparison with the three groups showed that extra virgin olive oil was an adjuvant in the treatment of gingival inflammation, improving PI and BI. In group A, mean plaque index had a 48% reduction and bleeding index 64% reduction, after 30 days. In group B, the mean plaque index had a 35% reduction and a bleeding index reduction of 43%, after 30 days. Conclusion The collected data showed significant improvements in the formation of bacterial plaque and gingi-vitis. the exact mechanism of such treatment is still to be elucidated. As a result of this, further studies with a different sample of patients to those used and a comparison with other products need to be addressed to verify and demonstrate the antibacterial and anti-inflammatory effect of the components of this natural product.
Keywords:
oil pulling
; oral health
; gingivitis
; dentistry
; dentistry innovations
; polyphenols
1. Introduction
Gingivitis is a reversible inflammatory pathology, clinically characterized by redness, swelling, bleeding and pain.
If left untreated it can progress into more severe forms and lead to periodontal disease with the loss of supporting tissues including periodontal ligament and alveolar bone, deepening of the periodontal pocket, gingival recession, increased tooth mobility furcation exposure and, ultimately, loss of teeth. [1]
The Mediterranean diet is characterized by the high use of olive oil, vegetables and fruit rich in antioxidants and vitamins. The adherence to Mediterranean diet has been correlated with a lower risk of systemic and inflammatory diseases. [2]
Fatty acids are increasingly recognized as a central feature of many biological processes. [3] They are essential components of phospholipids, serving as ligands for receptors of immune cells and many of their derivatives are strong immunoregulators.[4]
Lipid mediators are linked to the progression of periodontal disease due to the production of proinflammatory mediators, such as prostaglandins and leukotrienes, via the arachidonic acid cyclooxygenase/lipoxygenase pathways, such as lipoxins, resolvins and protectins, that are able to modulate the response of the host to promote resolution of inflammation and in response to periodontal pathogens. Lipoxins are natural pro-resolving molecules derived from endogenous fatty acids.
They stimulate the resolution of inflammation and promote the restoration of tissue homeostasis through several mechanisms, such as limiting the migration of polymorphonuclear neutrophils to sites of inflammation and modulating macrophage activity by inhibiting the secretion of proinflammatory cytokines. [5,6]
It has been described that the release of interleukin (IL) 1 beta (IL-1B) and tumor necrosis alpha factor (TNF-A), inibite leukocyte trafficking and attenuate the inflammatory reactions caused by porpgyromonas gingivalis, gives strenght to the potential protective role in periodontal disease. [6]
Resolvins are dietary omega-3 polyunsaturated fatty acids products (PUFA) that also stimulate the resolution of inflammation through multiple mechanisms.
Some studies have shown that resolvin E1 promotes the resolution of the inflammatory reaction, preventing a chronic response after P gingivalis infection and also promoting the regeneration of periodontal connective tissue and bone.[7] The recently discovered properties of resolvins may show that these mediators may represent a new family of analgesics useful in the treatment of pain states associated with inflammation, such as arthritic and post-operative pain [8].
Many substances can be used as adjuvants in reducing the formation of plaque, but there is still little scientific evidence to validate it.
Several oil pulling studies have been done with sunflower oil, sesame oil, and coconut oil to reduce plaque-induced gingivitis. “Oil pulling” is a term that defines a traditional Ayurvedic remedy which consists of rinsing the mouth with oil [9,10,11,12]. There is still little evidence in the literature of studies concerning the properties of extra virgin olive oil and fruity in relation to the oral cavity [13,14,15,16].
Extra virgin olive oil is one of the most valuable and appreciated products of the agri-food industry, constituting an important element of the Mediterranean diet thanks to its organoleptic characteristics and its contribution to a healthy diet.
Extra virgin olive oil (EVO) is enriched by phenolic components which are completely absent in other types of oils derived from seeds or fruits. The concentration of phenolics in virgin olive oil depends on various agronomic (genetic and geographical origin of the fruit) and technological factors. Monovarietal EVOs show different phenolic profiles, thanks to the different abundance of secoiridoids and their derivatives. It is important to remark that the process used for olive oil extraction has a major influence on the phenolic concentration. Eventually, differences in the abundance and composition of phenolics could contribute to the health beneficial properties, in order that different monovarietal virgin olive oils exert different effects at the cellular level, also due to their specific level of absorption and bioavailability. Supposedly, the multiple phenolic compounds, present in virgin olive oil, act synergistically or complementary to confer benefits to the whole organism. [17]
- Polyphenols in Olive Oil
Extra virgin olive oil is rich in polyphenol molecules, especially tocopherols and biophenols, aromatic compounds, antioxidants, which act both on the taste of the oil and on its shelf life and quality. These phenols delay the oxidation of fatty acids and the rancidity of the oil. The EFSA (European Food Safety Authority) has certified hydroxytyrosol, a polyphenol present in olives, as a substance capable of protecting blood lipids from the harmful effects of oxidative stress. The daily use of extra virgin olive oil in the recommended doses plays an important role in human health and is recommended in a balanced diet. The phenolic compounds contained in extra virgin olive oil, such as oleuropein and protocateuic acid, significantly increase the GPx activities [18]. The high content of monounsaturated fatty acids, in particular of oleic acid, is mainly responsible for the beneficial effects of EVO. The effects of the main polyphenols in the oil improved the function and survival of pancreatic beta-cells and improve insulin secretion, promoting glycemic control in patients with type 2 diabetes mellitus.[19]
The aim of the study was to evaluate the efficacy of extra virgin olive oil (EVO) and fruity oil for the treatment of gingivitis.
2. Materials and Methods
- Project of the Study
The study was conducted from March to October 2022, at the outpatient dental clinic of ASL Latina, Gaeta district. Seventy-five patients with bacterial plaque-induced gingivitis aged over 18 years were evaluated.
The study was approved by the Institutional Local Review Board of Sapienza University of Rome in Latina (Protocol n. 2103/2022). All subjects signed an informed consent for inclusion before they participated in the study, regarding details about the nature and objectives of the study, treatment effects, and clinical conditions. The study was conducted in accordance with the Declaration of Helsinki.
At time T0 (before nonsurgical periodontal therapy), anamnestic data were collected from individual patients to assess their readiness for and inclusion in the treatment protocol.
During the initial phase of the first visit, patients were asked various questions, focusing in particular, on the patient’s health status, gender, medication intake, tobacco use, toothbrush use and which type, whether manual, electric, or both. The selected patients were well motivated, instructed in the proper use of oral hygiene tools, and made aware of the prevention and treatment of gum disease and the importance of home oral hygiene. During the professional oral hygiene session, parameters for inclusion/exclusion in the experimental study were assessed.
After the professional oral hygiene session, patients were divided into three groups
- Group A: Extra Virgin Olive oil mouthwash
- Group B: Fruity mouthwash
- Group C: control without mouthwash
Inclusion criteria
- Age over 18 years;
- Presence of at least 20 teeth in the oral cavity, excluding third molars;
- 1 < GI > 3;
- 1 < PI > 3;
- Bleeding on probing;
- Presence of pseudotasks;
- Absence of clinical attachment loss, mobility, periodontitis;
Exclusion criteria
- Poorly motivated and/or uncooperative patients;
- Patients with systemic diseases;
- Patient being treated with hormones, calcium channel blockers, cyclosporine and phenytoin;
- Pregnant women;
A periodontal chart (Figure 1) was then completed containing gingival index, plaque, bleeding, presence of mobility, recessions.
The gingival index was Silness- Löe’s, a periodontal probe was used on the outer surface to determine its consistency and assess bleeding, for each tooth surface element (mesial, distal, buccal, oral). The plaque index used was the O’leary index, examining the 4 tooth surfaces (mesial, distal, buccal, oral) and reporting the presence or absence of plaque. The index was calculated by adding the number of surfaces with plaque to the number of total surfaces examined and multiplying by 100.
The bleeding index used was the Ainamo & Bay index, which was performed by probing the 4 tooth surfaces (mesial, distal, buccal, oral) and reporting the presence or absence of bleeding. The index was calculated by summing the number of surfaces with bleeding in relation to the number of total surfaces examined and multiplied by 100.
The presence of recessions was assessed by Miller’s Index, while any dental discoloration was assessed by the dichotomous method: presence/absence, followed by the mean value expressed as a percentage. Finally, gustatory perception reported to the patient was assessed.
Following completion of the chart, the patient underwent nonsurgical mechanical causal therapy. During scaling, hard and soft deposits were removed above and below the gumline using ultrasound and teeth were polished with a toothbrush and abrasive paste.
Candidate patients were randomly divided into three groups consisting of 25 people: two test groups and a control group.
Patients in the test group were explained the experimental treatment to be carried out at home with the evo olive oil and fruity oil mouthwash: a 5-minute rinse to be performed after brushing and interproximal cleaning before going to bed, for 30 days.
These patients were given 50 predosed bottles containing 10ml of olive oil from the ‘cultivar Evo’ of the Lazio region, Itrana precisely.
Patients in the control group were asked not to rinse with mouthwashes for 30 days while maintaining usual home oral hygiene. Recalls were performed at 15 (T1) and 30 (T2) days after the first session and in these, the plaque index, bleeding, presence of recessions, noting information such as pleasantness or not pleasantness of taste, taste alterations, presence of dental discoloration, cosmetic improvements, noted during the course of treatment, were re-evaluated.
Data analysis, plaque index and bleeding values, were performed using SPSS 27.0 software for Windows (SPSS Inc., Chicago, IL, USA). Then, the pre- and post-treatment values of the groups were compared using the t-student test, setting P< 0.05 as the significance level.
3. Results
The results of the present study are described in Figure 2, which highlights the characteristics of the examined subjects who participated in the study with Evo oil treatment and fruity oil, and the subjects who participated without the use of natural mouthwash.
- Test Group
At time T0 (before non-surgical periodontal therapy) and times T1 and T2 (15 and 30 days after the first session, respectively), the following data were collected: plaque index and bleeding index. The following graphs (fig 3-4) show the processed percentages of the collection of these data, which are intended to show the variation of the parameters during therapy, associated with non-surgical periodontal treatment with home treatment with Evo oil mouthwash and fruity oil mouthwash.
Figure 3 shows the change in plaque index of the test group over time during home treatment with oil mouthwash.
It can be seen that from t0 to t2, both test groups, experienced a significant decrease in plaque.
Figure 4 shows the change in bleeding index over time, consequently the degree of tissue inflammation during treatment with evo and fruity olive oil. This graph was developed by entering the bleeding indices of each patient before non-surgical mechanical therapy (t0), at two weeks (t1) and at four weeks (t2).
In the test group, slight variations were found for the values regarding probing depth during the recalls. These values never exceeded 3 mm in depth, therefore, always falling within a healthy periodontal condition. No variations were found in patients with recessions. No patient in the test group presented mobility greater than Miller index grade 0.
None of the patients reported allergic reactions to the product.
- Control Group
The following graphs (Figure 5 and Figure 6) show data collected before, during and after non-surgical mechanical causal therapy alone and aim to show the change in these parameters over time. Recalls for the control group were made, from the first session, at 15 days and at 30 days where the same parameters as in the test group were collected: plaque index, bleeding index, pocket depth and presence of recessions.
Figure 4 shows the graph with the plaque index data of the control group before non-surgical mechanical causal therapy and at 30 days after it.
Figure 6 represents the bleeding index values of the control group at t0, t1 and t2.
In the control group, no changes regarding probing depth and recessions were shown during recalls. None of the patients in the control group presented a mobility index above Miller’s index grade 0.
- Data Elaboration
Figure 7 and Figure 8 compare the plaque index and bleeding index of the two test grips and the control group. The graphs were developed by averaging the indices of the three groups at both T0, before non-surgical mechanical causative treatment, T1, after 15 days, and T2, after 30 days.
Figure 7 compares the plaque percentage, found during the three visits, of the evo test group, fruity test group and control group at T0 on the left, T1 in the middle and T2 on the right.
Figure 8 compares the bleeding percentage, during the three visits encountered, of the evo test group, fruity test group and control group at T0 on the left, T1 in the middle and T2 on the right.
At the end of each visit, patients in the two test groups were asked questions about their enjoyment of taste and whether they had noticed any improvement. Figure 9 shows the patients’ perceived liking during the treatment with evo oil and fruity oil.
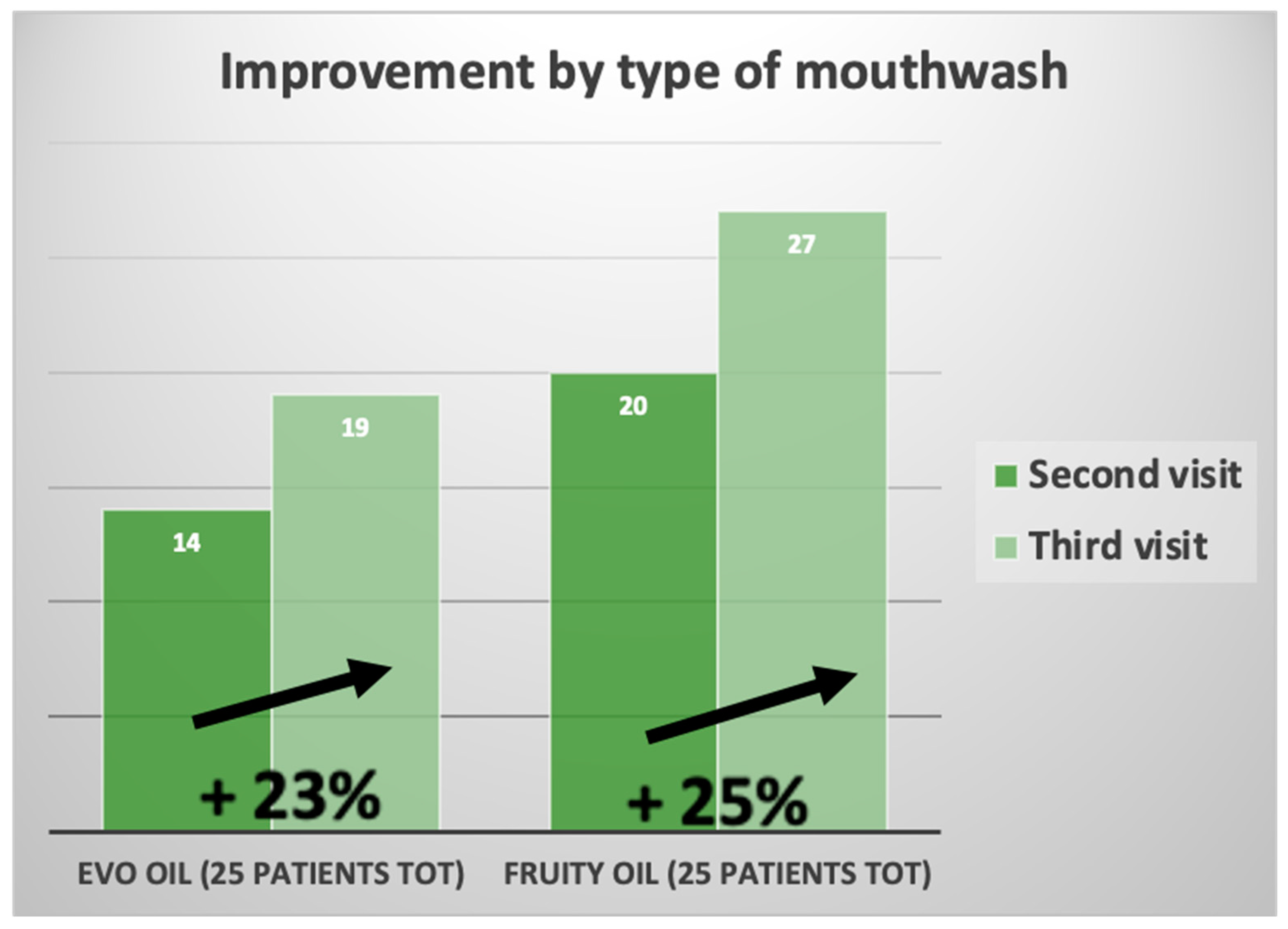
Figure 10 shows data on the feeling of improvement that patients perceived during treatment with the olive oil mouthwash.
As can be seen from the graphs, patients with Fruity oil treatment liked the mouthwash more than patients with Evo oil treatment (Figure 9). The improvement that was evaluated is indicated by the patient’s own perception, in the daily application of extra virgin olive oil mouthwash, found an improvement for both types of mouthwashes with minimal difference in fruity oil treatment. The values of plaque and bleeding indices, were shown in Figure 10, Figure 11 and Figure 12. Next, the pre- and post-treatment values of the groups were compared using the t-student test, setting P<0.05 as the significance level (Figure 13).
- Single Sample Stats
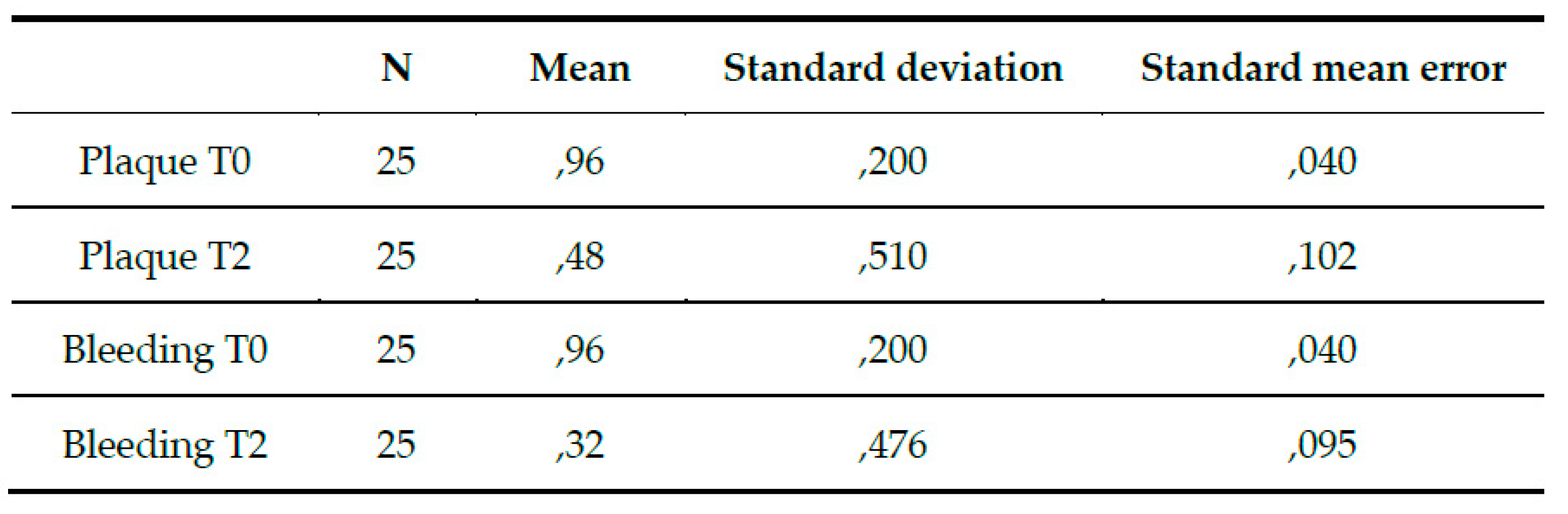
Figure 10.
Comparison of evo group mean values of plaque index and bleeding index at t0 and t2. Dev.St: standard deviation, standard error of the mean t0: before treatment, t2: 30 days after Evo oil treatment.
Figure 10.
Comparison of evo group mean values of plaque index and bleeding index at t0 and t2. Dev.St: standard deviation, standard error of the mean t0: before treatment, t2: 30 days after Evo oil treatment.
- Single Sample Stats
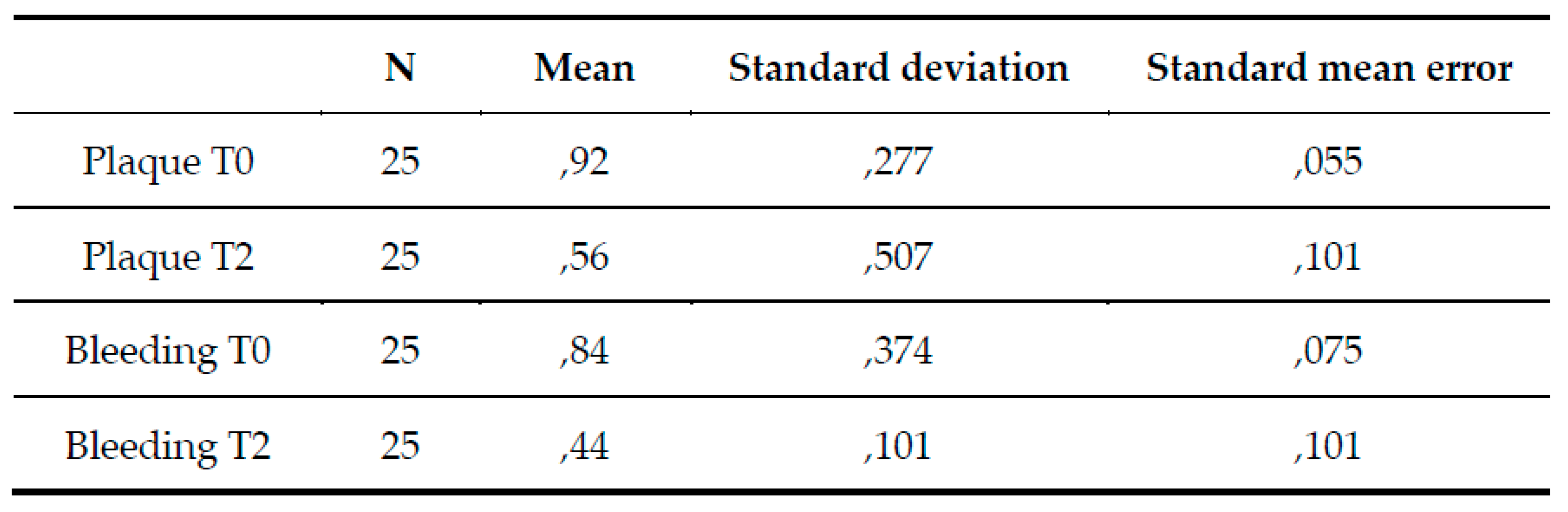
Figure 11.
Comparison of fruity group mean values of plaque index and bleeding index at t0 and t2. Dev.St: standard deviation, standard error of the mean t0: before treatment, t2: 30 days after treatment with Fruity oil.
Figure 11.
Comparison of fruity group mean values of plaque index and bleeding index at t0 and t2. Dev.St: standard deviation, standard error of the mean t0: before treatment, t2: 30 days after treatment with Fruity oil.
- Single Sample Stats
Figure 12.
(a): Comparison of control group mean values of plaque index and bleeding index at t0 and t2. Dev.St: standard deviation, standard error of the mean t0: before treatment, t2: 30 days after treatment without any mouthwash. (b): Comparison of mean values of the three groups of IP (plaque index) and IS (bleeding index) at t0 and t2 *A P value (significance level) < 0.05 is considered statistically significant (T- student test). IP: plaque index, IS: bleeding index, Dev.St: standard deviation, t0: before treatment, t2: 30 days after treatment.
Figure 12.
(a): Comparison of control group mean values of plaque index and bleeding index at t0 and t2. Dev.St: standard deviation, standard error of the mean t0: before treatment, t2: 30 days after treatment without any mouthwash. (b): Comparison of mean values of the three groups of IP (plaque index) and IS (bleeding index) at t0 and t2 *A P value (significance level) < 0.05 is considered statistically significant (T- student test). IP: plaque index, IS: bleeding index, Dev.St: standard deviation, t0: before treatment, t2: 30 days after treatment.
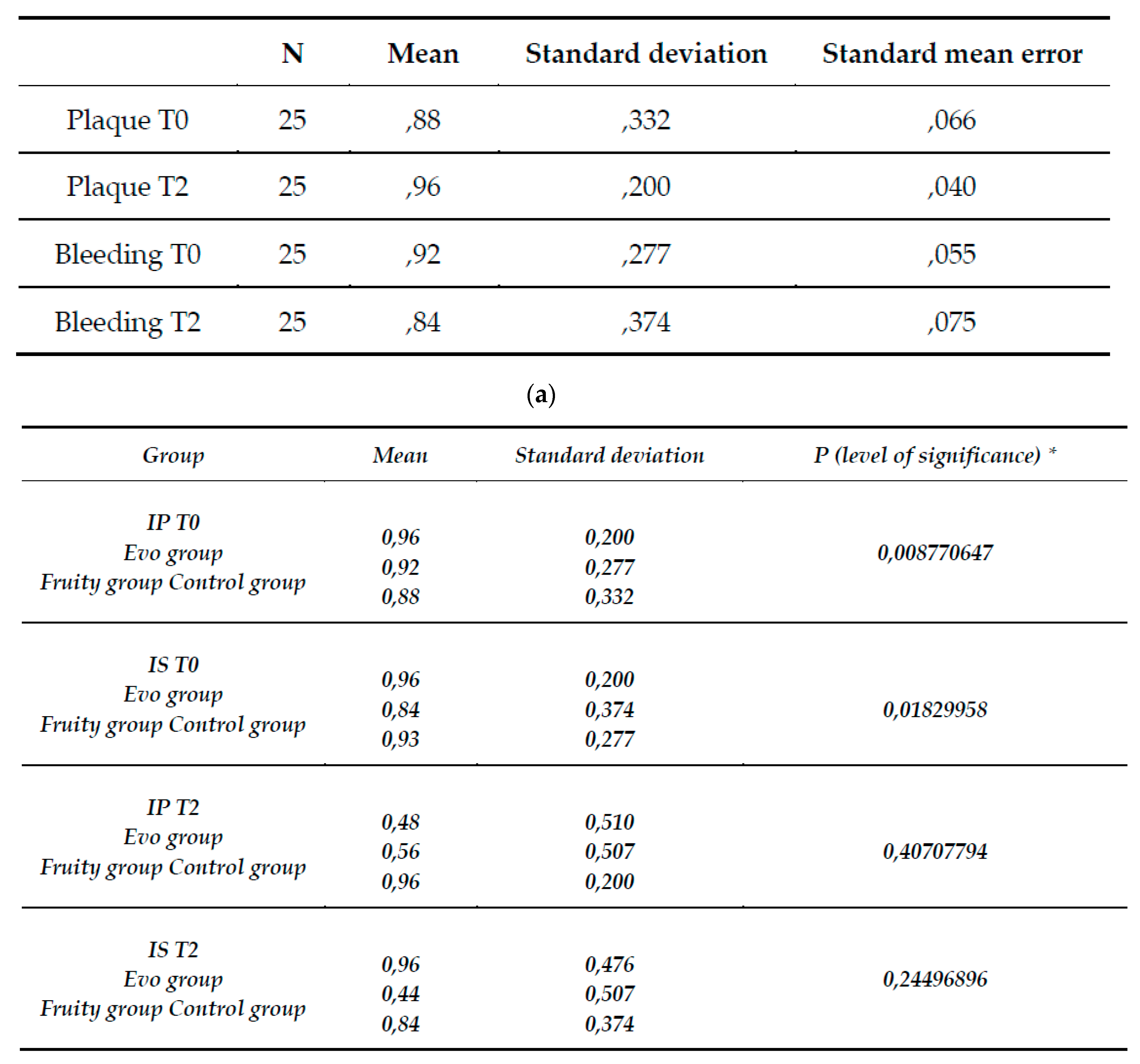
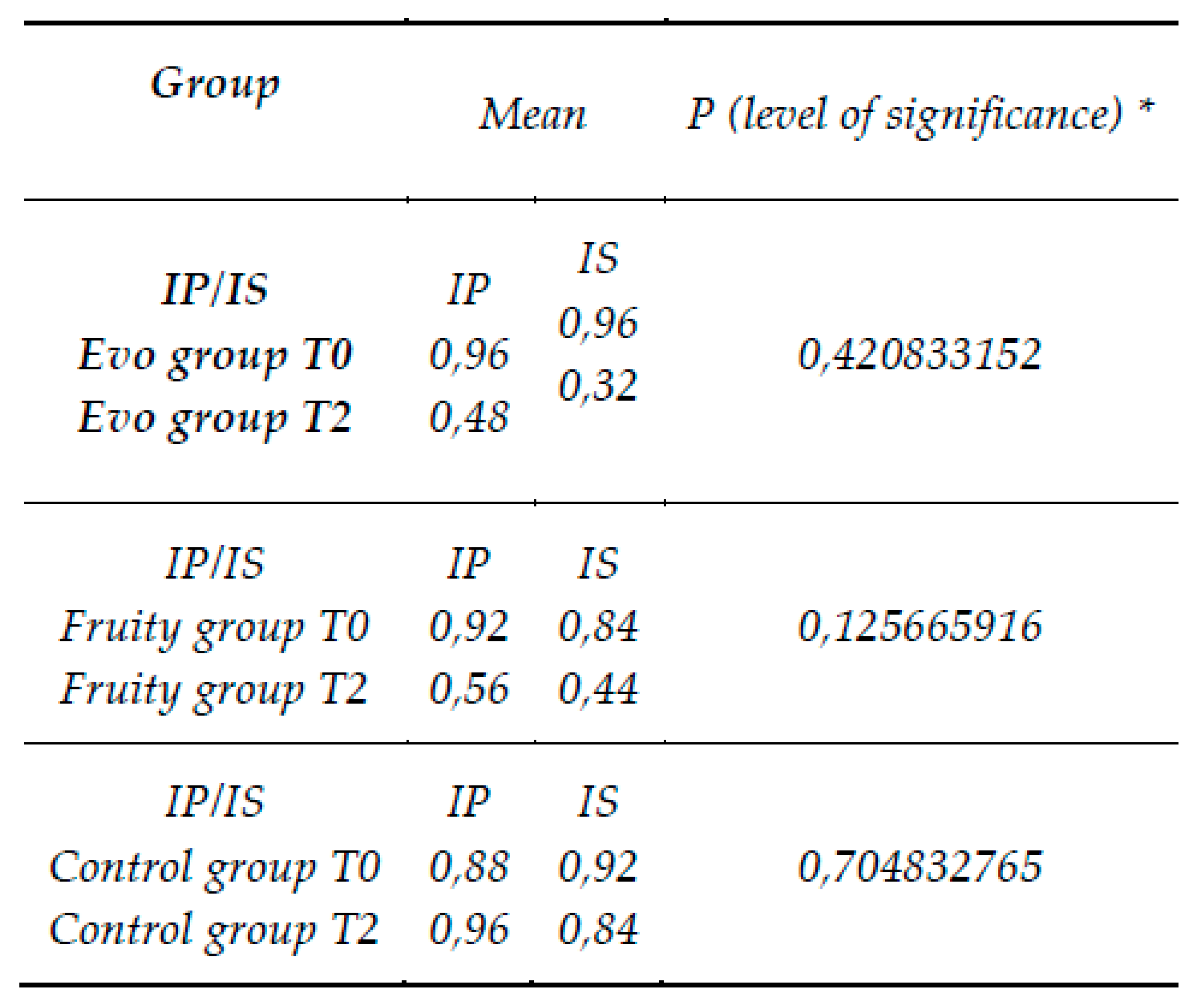
Figure 13.
Comparison of pre- and post-treatment IP and IS of the evo group, fruited group and control group. *A P value (significance level) < 0.05 is considered statistically significant (T- student test). IP: plaque index, IS: bleeding index.
Figure 13.
Comparison of pre- and post-treatment IP and IS of the evo group, fruited group and control group. *A P value (significance level) < 0.05 is considered statistically significant (T- student test). IP: plaque index, IS: bleeding index.
Comparing the results of the clinical data obtained following the treatments to which the patients in the evo group and the fruited group underwent with the control group, positive results can be found in both test groups, emphasizing, however, a higher percentage of those obtained than in the control group.
In the Evo test group, the average plaque index before non-surgical causal treatment stood at 96 percent and then decreased to an average value of 48 percent, after 30 days.
In the Fruity test group, the plaque index before treatment stood at 92% and then decreased to an average value of 56% after 30 days.
In the control group, the average plaque index before treatment stood at an average value of 88% and then increased to a value of 96%, after 30 days. The evo test group had a decrease in plaque index of 45%, the fruity test group had a decrease in plaque index of 35%, and the control group had an increase of 8%. (fig8) The bleeding index of the evo test group, before non-surgical causative treatment was 96% and then decreased to a value of 32%. In the fruity test group, the bleeding index stood at a value of 84% and then decreased to a value of 44%, while for the control group it stood at a value of 92% and then decreased to a value of 84%. The evo test group had a decrease in bleeding index of 64%, the fruity test group had a decrease in bleeding index of 43%, while the control group had a decrease of only 8%. (Figure 9)
Comparison of the plaque and bleeding indices of the three test groups with the t-student test showed a slight difference in the averages, before treatment, with a P value (significance level) <0.05. The plaque index was found to be P= 0.008 while the bleeding index was P=0.018. After 30 days, the plaque index was found to be P=0.40 and the bleeding index P=0.24. Comparison of pre- and post-treatment plaque and bleeding values of the two test groups and the control group showed a statistically significant result for P<0.01.
4. Discussion
Traditionally the beneficial properties of extra virgin olive oil have been attributed to its high content of monounsaturated fatty acids which represent up to 80% of its total lipid composition. Recent evidence has shown that the minor components of extra virgin olive oil, such as phenolic compounds and other compounds with an antioxidant action, determine an increase in the healthy characteristics of the oil itself.
In the scientific literature there are few studies on the treatment of extra virgin olive oil as an adjuvant for gingival inflammation. In the previous chapter, some scientific articles described the state of the art, in which natural mouthwashes are used. The data obtained in the literature can be compared with the results obtained from the experimental study conducted [20,21]. This study showed that the two groups, which used the mouthwash with olive oil, had a statistically significant result. The groups subjected to the treatment had a very positive change in the bleeding and plaque indices, in percentage better compared to those of the group subjected to non-surgical mechanical therapy. As in the study carried out in 2003 by Pretty IA et al. [20], on the use of an olive oil-based toothpaste, and that of 2020 carried out by Nardi G.M [21] et al., on the use of mouthwash of ozonized olive oil, the treatment with olive tree-based products is an excellent adjuvant for maintaining oral hygiene at home.
5. Conclusions
The oil pulling treatment with extra virgin olive oil mouthwash was effective in the treatment of plaque-induced gingivitis, it did not show any negative effects or disadvantages except for the longer duration of the procedure (5 min) compared to other mouthwashes (2 mins). This type of oil pulling treatment with extra virgin olive oil has proven to be a good adjuvant in maintaining home oral hygiene, thanks to the ability to reduce the adhesion and formation of bacterial plaque. While there were improvements in this study, the exact mechanism of this treatment remains to be elucidated. Because of this, it is necessary to carry out further studies with a sample of patients different from those used and a comparison with other products, to verify and demonstrate the antibacterial and anti-inflammatory effect of the components of this natural product.
Author Contributions
Conceptualization, I.V., F.G., D.C. and S.S.; methodology, D.C. and C.S.; validation, I.V., F.G. and A.P.; formal analysis, D.C., C.S. and G.Z.; investigation, S.S. and I.V.; resources, I.V., F.G. and A.P.; data curation, D.C., S.S. and G.Z.; writing—original draft preparation, D.C., S.S. and G.Z.; writing—review and editing, D.C., S.S. and G.Z.; supervision, C.S., I.V., F.G. and A.P.; project administration, I.V., F.G. and A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study was approved by the Institutional Local Review Board of Sapienza University of Rome in Latina (Protocol n. 2103/2022). All subjects gave their informed consent for inclusion before they participated in the study. The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kumar, S. Evidence-based update on diagnosis and management of gingivitis and periodontitis. Dent Clin North Am. 2019;63(01):69–81.
- Rasperini G, Pellegrini G, Sugai J, Mauro C, Fiocchi S, Corvi Mora P, Dellavia C. Effects of food supplements on periodontal status and local and systemic inflammation after nonoperative periodontal treatment. J Oral Sci. 2019 Jun 18;61(2):213-220.
- Lopez-Vicario, C, Rius, B, Alcaraz-Quiles, J, et al. Pro-resolving mediators produced from EPA and DHA: overview of the pathways involved and their mechanisms in metabolic syndrome and related liver diseases. Eur J Pharmacol 2016; 785: 133–143.
- Rodrigues, HG, Takeo Sato, F, Curi, R, et al. Fatty acids as modulators of neutrophil recruitment, function and survival. Eur J Pharmacol 2016; 785: 50–58.
- Cekici, A, Kantarci, A, Hasturk, H, et al. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol 2000 2014; 64: 57–80.
- Garlet, GP. Destructive and protective roles of cytokines in periodontitis: a re-appraisal from host defense and tissue destruction viewpoints. J Dent Res 2010; 89: 1349–1363.
- Van Dyke, TE. Pro-resolving mediators in the regulation of periodontal disease. Mol Aspects Med 2017; 58: 21–36.
- Poorani, R, Bhatt, AN, Dwarakanath, BS, et al. COX-2, aspirin and metabolism of arachidonic, eicosapentaenoic and docosahexaenoic acids and their physiological and clinical significance. Eur J Pharmacol 2016; 785: 116–132.
- Serhan, CN. Pro-resolving lipid mediators are leads for resolution physiology. Nature 2014; 510: 92–101.
- Souza, PR, Norling, LV. Implications for eicosapentaenoic acid- and docosahexaenoic acid-derived resolvins as therapeutics for arthritis. Eur J Pharmacol 2016; 785: 165–173.
- Viladomiu, M, Hontecillas, R, Bassaganya-Riera, J. Modulation of inflammation and immunity by dietary conjugated linoleic acid. Eur J Pharmacol 2016; 785: 87–95.
- Vangaveti, VN, Jansen, H, Kennedy, RL, et al. Hydroxyoctadecadienoic acids: oxidised derivatives of linoleic acid and their role in inflammation associated with metabolic syndrome and cancer. Eur J Pharmacol 2016; 785: 70–76.
- Hasturk, H, Jones, VL, Andry, C, et al. 1-Tetradecanol complex reduces progression of porphyromonas gingivalis-induced experimental periodontitis in rabbits. J Periodontol 2007; 78: 924–932.
- Hasturk, H, Goguet-surmenian, E, Blackwood, A, et al. 1-Tetradecanol complex: therapeutic actions in experimental periodontitis. J Periodontol 2009; 80: 1103–1113.
- De Caterina, R, Liao, JK, Libby, P. Fatty acid modulation of endothelial activation. Am J Clin Nutr 2000; 71 1 Suppl: 213S–223S.
- Vadhana V C, Sharath A, Geethapriya P R, Vijayasankari V. Effect of sesame oil, ozonated sesame oil, and chlorhexidine mouthwash on oral health status of adolescents: a randomized controlled pilot trial. J Indian Soc Pedod Prev Dent. 2019;37(04):365–371.
- Cariello M, Contursi A, Gadaleta RM, Piccinin E, De Santis S, Piglionica M, Spaziante AF, Sabbà C, Villani G, Moschetta A. Extra-Virgin Olive Oil from Apulian Cultivars and Intestinal Inflammation. Nutrients. 2020 Apr 14;12(4):1084. [CrossRef]
- C. Giovannini, C. Filesi, M. D’Archivio, B. SCazzocchio, C. Santangelo e R. Masella “Polifenoli e difese antiossidanti endogene: effetti sul glutatione e sugli enzimi ad esso correlati”.
- N. Marrano, R. Spagnuolo, G. Biondi, A. Cignarelli, S. Perrini, L. Vincenti “Effects of Extra Virgin Olive Oil Polyphenols on Beta-Cell Function and Survival”.
- Servili, M., Piacquadio P., De Stefano G., Taticchi A., Sciancalepore V. (2002). Influence of a new crushing technique on the composition of the volatile compounds and related sensory quality of virgin olive oil.
- Cicerale S, Conlan XA, Sinclair AJ, Keast RS. Chemistry and health of olive oil phenolics. Crit Rev Food Sci Nutr. 2009 Mar;49(3):218-36. [CrossRef] [PubMed]
Figure 1.
Periodontal chart used in the trial.
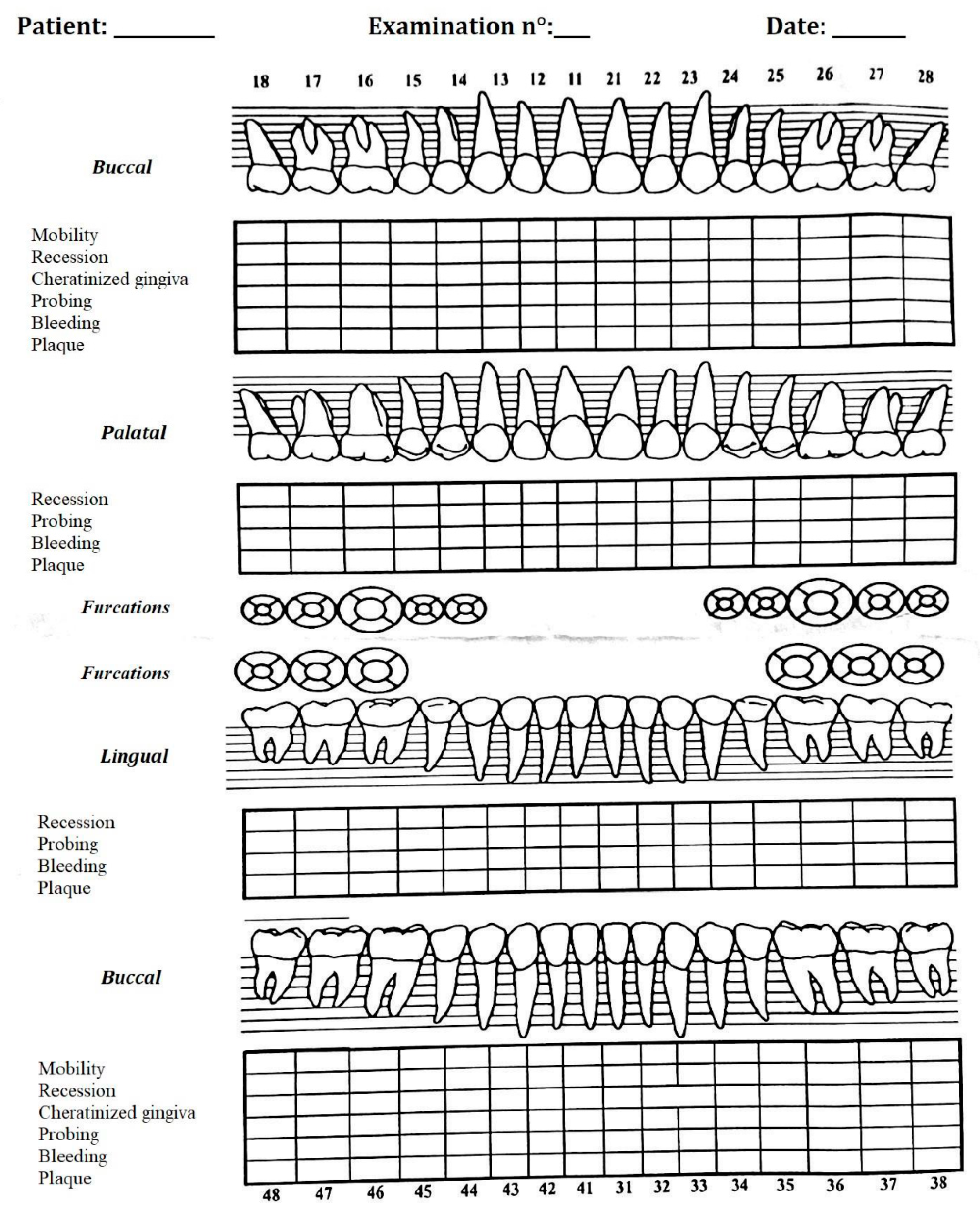
Figure 2.
Percentages history sheet test group and control group.
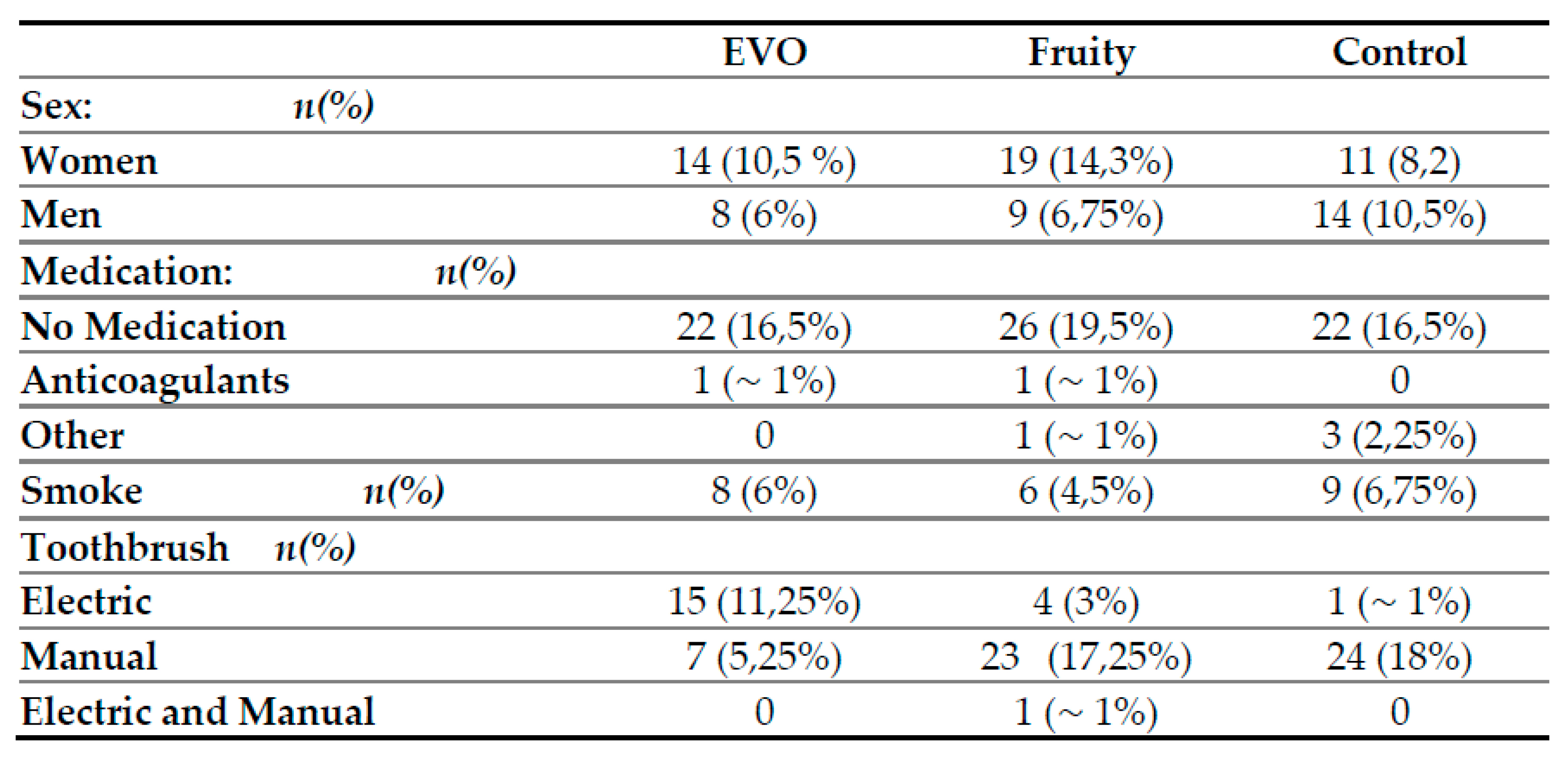
Figure 3.
Change over time in plaque index of the test group at t0, t1 and t2.
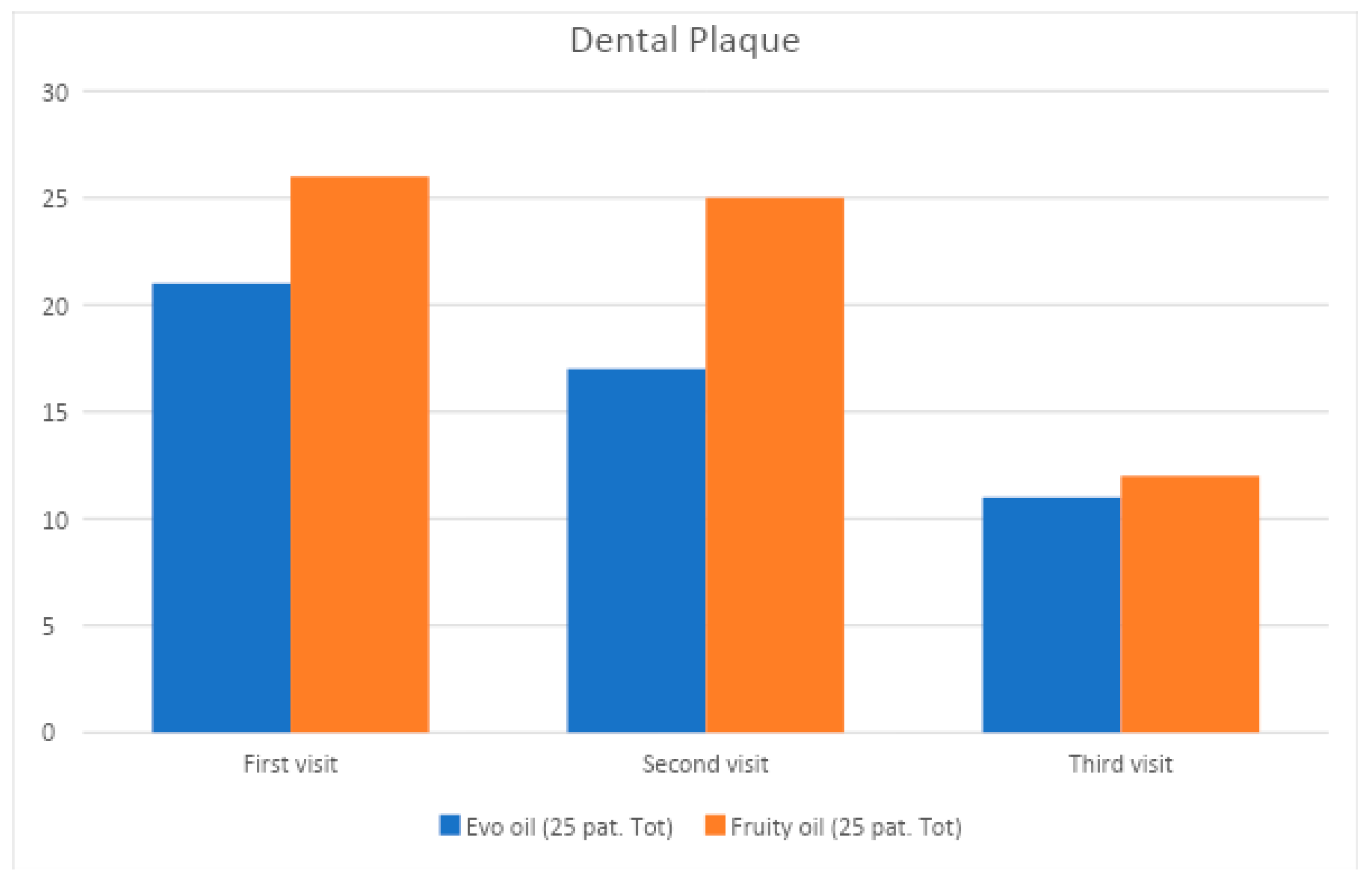
Figure 4.
Change in bleeding index of test group at t0, t1 and t2.
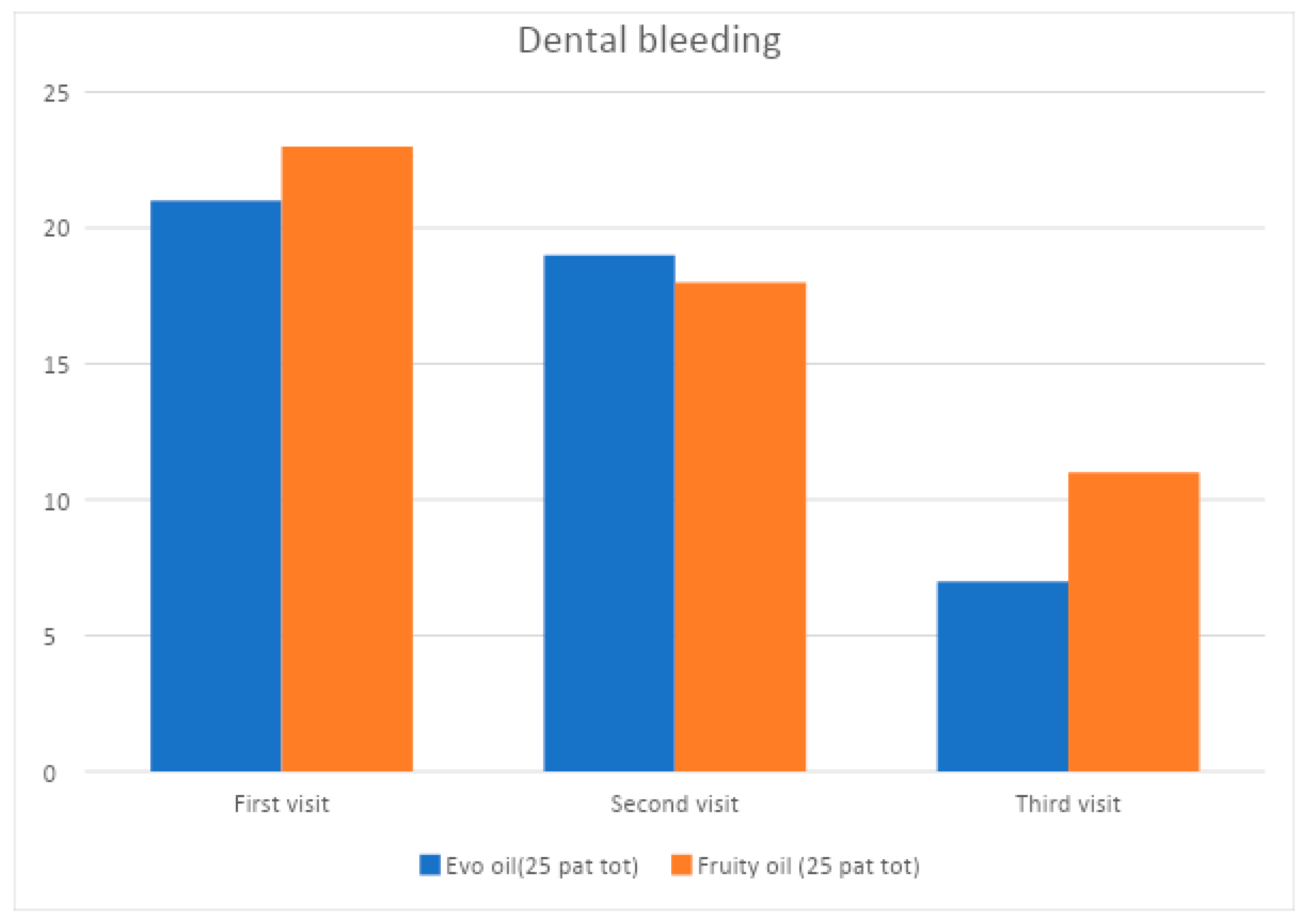
Figure 5.
Change over time of the plaque index of the control group.
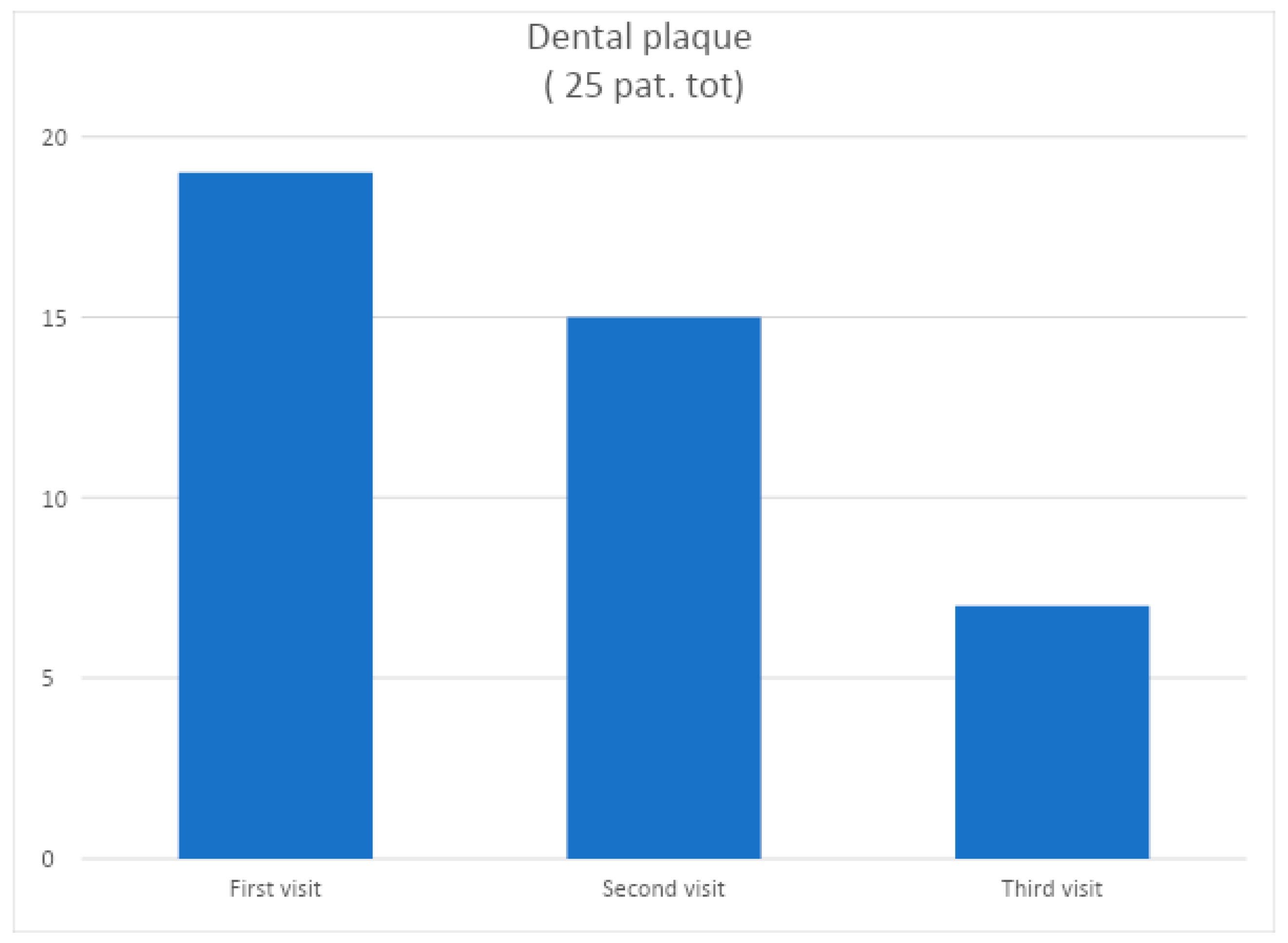
Figure 6.
Change in bleeding indices over time in the control group.
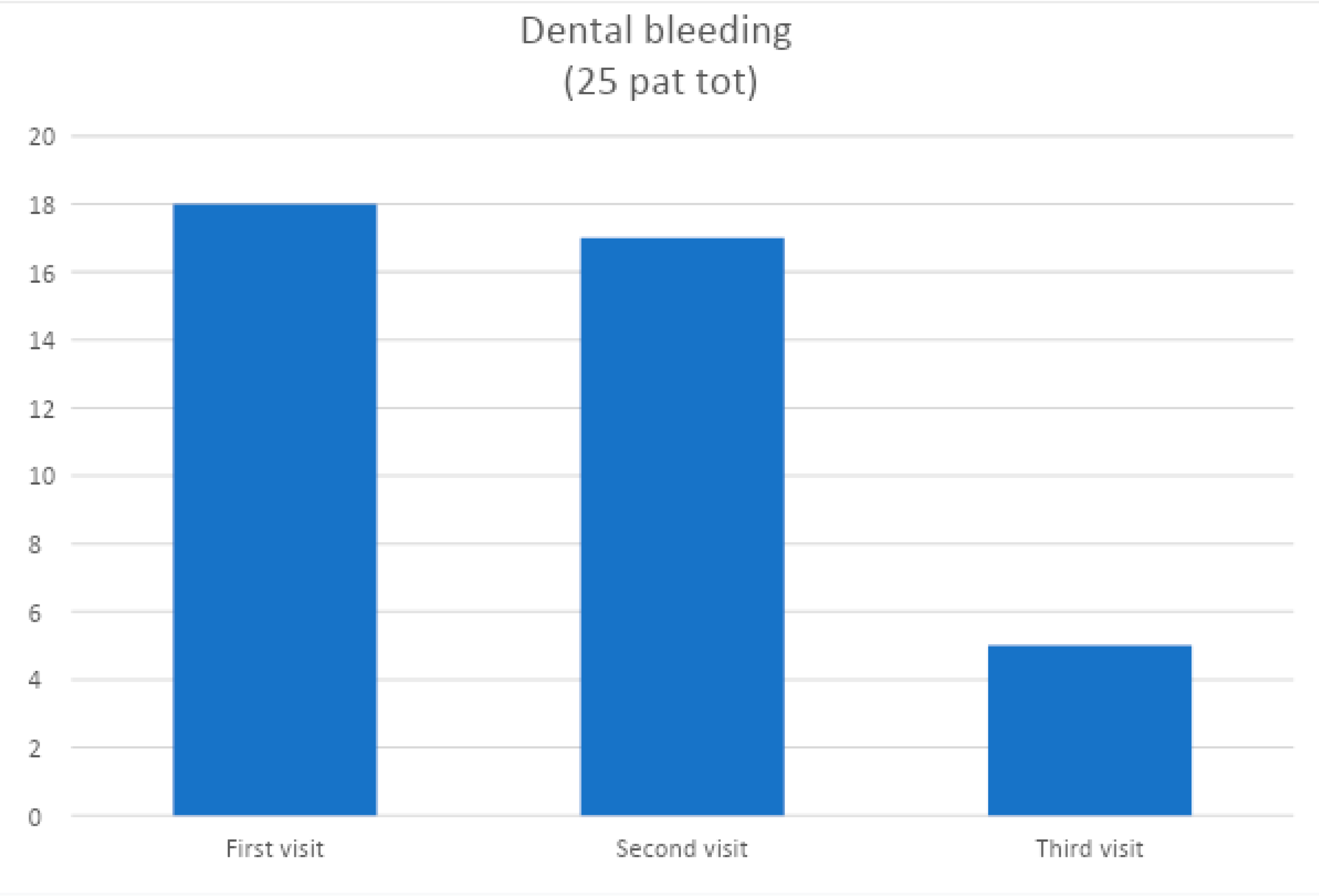
Figure 7.
Plaque percentage over time of the test group and control group.
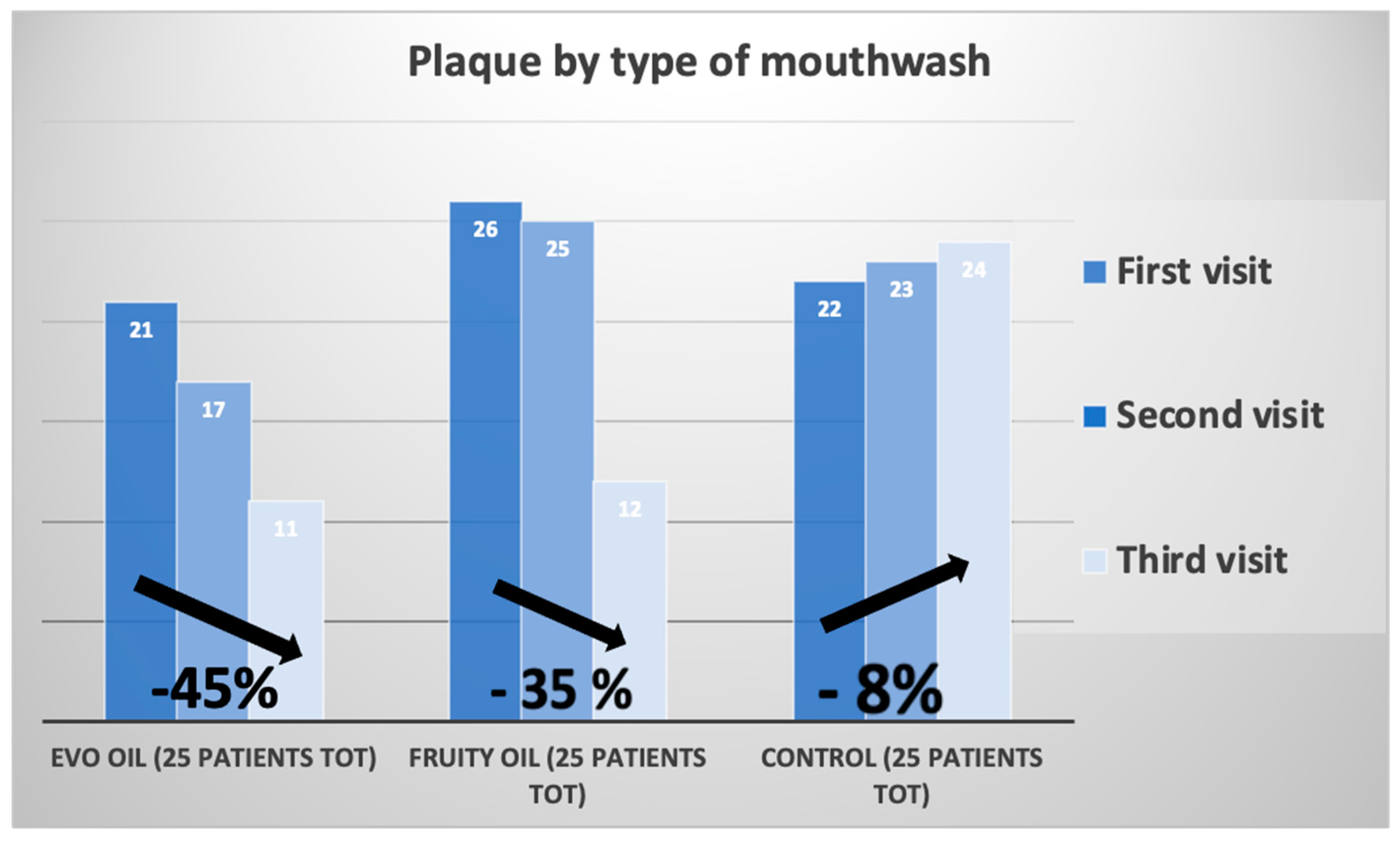
Figure 8.
Bleeding percentage over time of the test group and control group.
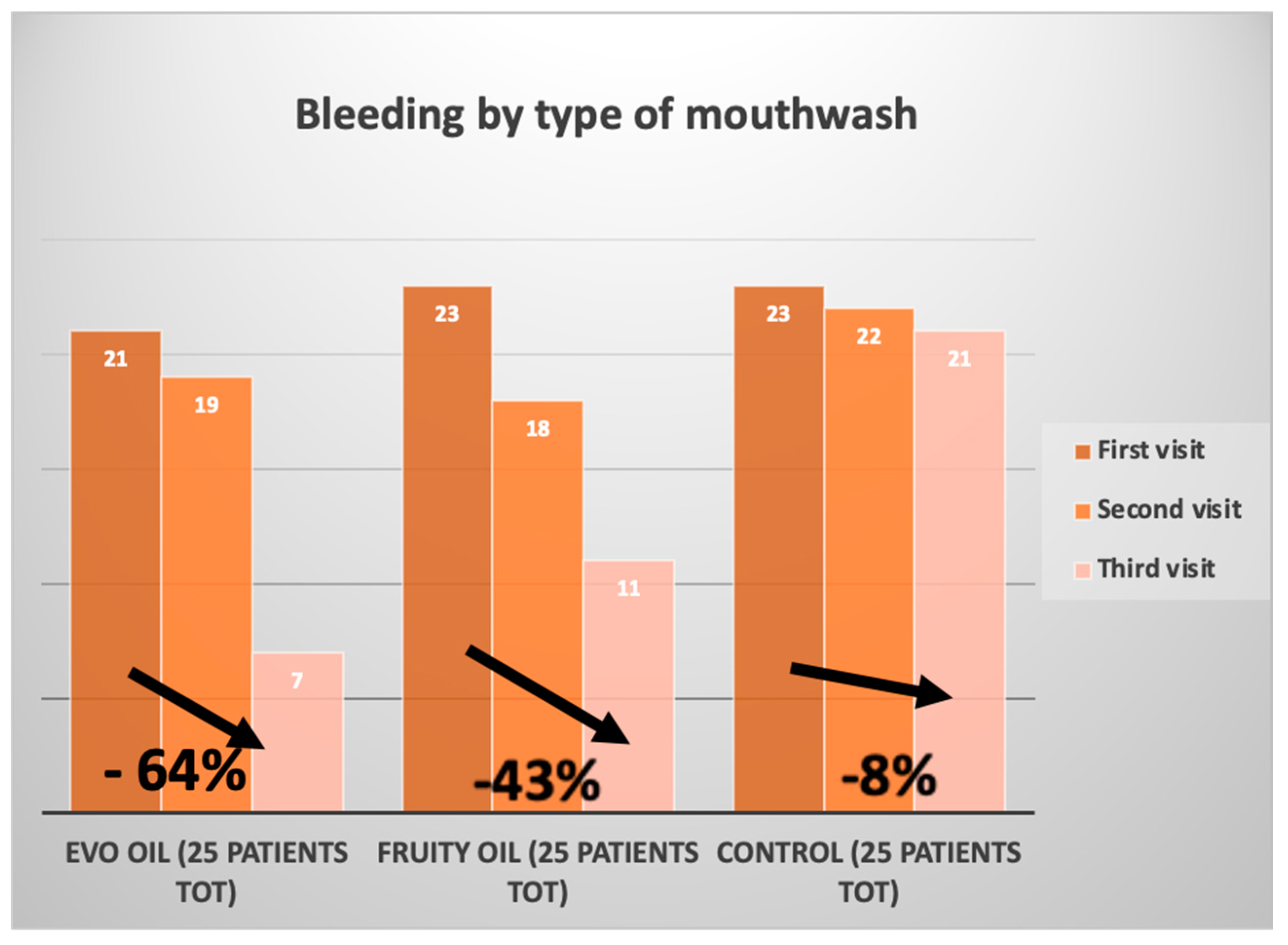
Figure 9.
percentage liking of the two oil-based mouthwashes.
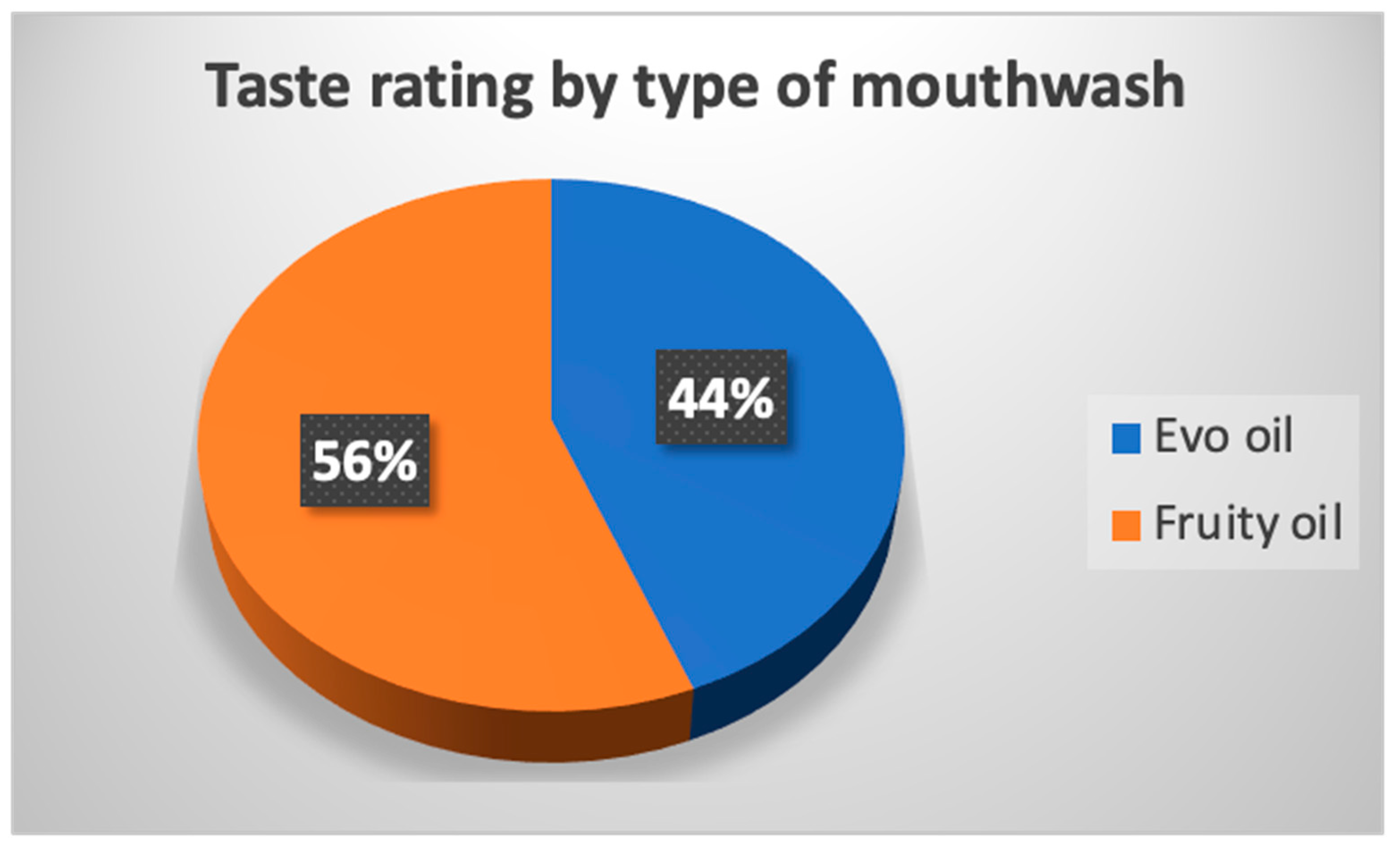
Figure 10.
Percentage of improvement by type of mouthwash.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



