
Submitted:
10 July 2023
Posted:
11 July 2023
You are already at the latest version
Abstract
Background: The aim of this study has been to investigate if inflammatory biomarkers such as the systemic immune-inflammation index (SII), neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) have any correlation with the recurrence of pleomorphic adenomas (PA) in patients afflicted by this disease.
Methods: A retrospective multicentre study involving two Italian centres, the Maxillofacial Sur-gery at the Policlinico Federico II in Naples and the ENT and Maxillofacial Surgery at the IRCCS G. Pascale National Cancer Institute in Naples, has been performed. The study, involving 608 pa-tients who had received a diagnosis of PA, was conducted between January 2000 and January 2020. A Receiver Operating Characteristic (ROC) curve was used to calculate the optimal cut-off values for the SII, PLR and NLR. A linear regression model (LRM) and a non-linear logistic re-gression model (NLRM) were realized with respect to the NLR, PLR and SII.
Results: The highest performance was achieved by the NLR (cut-off 2.960) with the AUC = 0.91, with an accuracy of 96.1%, sensitivity of 78.4% and specificity of 97.2%, PPV = 64.4% and NPV = 98.6%. The LRM and NLRM including all the haematological parameters did not increase the per-formance in terms of recurrence detection.
Conclusion: The NLR is an excellent support tool in predicting the recurrence of PA with a cut-off of 2.960. It can be a good reference point for surgical decision-making and follow-up in clinical practice.
Keywords:
pleomorphic adenoma
; recurrence
; inflammatory biomarkers
; systemic immune-inflammation index
; platelet to lymphocyte ratio
; neutrophil to lymphocyte ratio
1. Introduction
Pleomorphic adenomas (PA) are the most common benign salivary gland tumours (SGT), comprising 70–80% of benign parotid neoplasms. PA of the submandibular and sublingual gland are quite uncommon and account for only around 18–20% of such tumours.[1] In a smaller percentage, they can also be located in the hard palate and soft palate glands of the saliva, upper lip, cheek, tongue and floor of the mouth.[2]
PA are also known as benign mixed tumours (BMTs). The definition of a mixed tumour was established by Minssen in Ahlbom's monograph in 1874 in reference to the simultaneous presence of epithelial and connective tissue elements. The tumour consists essentially of three components: an epithelial component, a component of myoepithelial cells and a mesenchymal component. The histological presentation of PA shows a variable pattern of the epithelium with a fibrous stroma of a myxoid, chondroid or mucoid type. [3]
Women younger than 50 years old are most commonly affected by PA. They present as a slowly progressing, non-symptomatic swelling that does not involve the facial nerve. [3] No relationship with smoking has been observed with respect to PA.[4]
The pre-surgical diagnosis of PA is based on performing a needle aspiration cytology (FNAC) of the tumour and an imaging examination such as CT or MRI. In most cases, PA of the parotid gland shows an inhomogeneous pattern on CT images, with delayed enhancement and contrast material filling over time.[5] The aetiology of PA is still unknown, with several factors determining its recurrence.
The recurrence rate varies greatly, depending on the initial surgical treatment. When an initial superficial parotidectomy has been performed the recurrence rate may be below 3%. [5]
After a first tumour recurrence there is an increased risk of a further recurrence and of a malignant transformation. Re-recurrence (when the disease recurs after treatment of the first relapse) is much more common, with rates typically ranging from 16% to 46%, but reaching as high as 75% in some single-centre series.[6]
Risk of a malignant transformation to a carcinoma ex- pleomorphic adenoma (cxPA) is about 3.3%. [7,8] The recurrence rates are lower for patients presenting with an interval of more than 10 years since their last surgery.[6] Recurrence is determined by various factors, although there is some ambiguity in the literature regarding the determining factor. The factors discussed include tumour size, lack of capsule or capsule thickness, rupture of the capsule, spillage of tumour contents and satellite nodules.[9,10,11]
Often, as the PA lacks a true capsule and is surrounded by a fibrous pseudo-capsule of a variable thickness, the tumour extends through the normal glandular parenchyma in the form of a pseudopodia. These microscopic extensions could explain the high risk of recurrence of this benign tumour compared to other SGT. [12,13]
Inflammation could be triggered by the immune system in an attempt to confine cell proliferative activity. In recent years, inflammatory biomarkers have been playing an important role in predicting tumour behaviour, in particular the malignancy of certain tumours, including those involving the head and neck. [14,15,16,17,18,19] Given the aetiopathological features of PA, our aim has been to determine whether there is a relationship between inflammatory biomarkers (the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII) ) and the recurrence of this tumour.
2. Materials and Methods
2.1. Study Population
This is a retrospective multicentre study involving two Italian centres, the Maxillofacial Surgery at the Policlinico Federico II in Naples and the ENT and Maxillofacial Surgery at the IRCCS G. Pascale National Cancer Institute in Naples. The study, involving 608 patients who had received a diagnosis of PA, was conducted between January 2000 and January 2020. The diagnosis was confirmed by histological examination and all the patients underwent maxillofacial computed tomography (CT) or maxillofacial magnetic resonance imaging ( MRI) and cytological examination prior to surgery. The study was conducted in accordance with the Declaration of Helsinki, Informed consent was not required by the local ethics committee due to the retrospective nature of the study.
The inclusion criteria were: age over 18 years, an established histology of PA with preoperative cytological examination, an extracapsular dissection performed for tumour located in the parotid gland, submandibular sialoadenectomy performed for a tumour located in the submandibular gland, the availability of clinical and haematological parameters, and a minimum of 36 months post-operative follow-up to assess any possible tumour recurrence.
The exclusion criteria were: other initial surgical treatments such as a partial or total parotidectomy, a previous tumour at another site, previous radiotherapy or chemotherapy in the clinical history, a chronic inflammatory disease influencing the indices of inflammation (infections with chronic inflammatory or autoimmune diseases, viral markers in the serum, haematological disorders and simultaneous or long-term anti-inflammatory or steroid drug treatments). The clinical and haematological parameters included: age; sex; smoking and/or drinking habit; tumour location; NLR; PLR; SII. Haematological parameters, such as the platelet count, neutrophil count, monocyte count and lymphocyte count, were measured around one week before the surgery.
The pre-treatment baseline values of the NLR, PLR and SII were calculated using the following formulae:
NLR = neutrophil count/lymphocyte count,
PLR = platelet count/lymphocyte count,
SII = platelet count × neutrophil count/lymphocyte count.
2.2. Follow-up Investigation
Post-operative follow-up evaluations were performed one week and one month after the surgery, then every six months for two years and thereafter every year until 3/5 years in every case without any recurrence. The last follow-up evaluation was conducted in February 2022. The routine follow-up evaluation included a physical examination, ultrasound of the major salivary glands and/or a maxillofacial/neck computed tomography (CT).
2.3. Statistical Analysis
The presence of recurrence was used in both the univariate and multivariate analysis. An analysis of the receiver operating characteristics (ROC), area under the ROC curve (AUC), sensitivity (SENS), specificity (SPEC), positive predictive value (PPV), negative predictive value (NPV) and accuracy (ACC) was performed.
A linear regression model (LRM) and non-linear logistic regression model (NLRM) were realized with respect to the NLR, PLR and SII.
A p-value <0.05 was considered significant for univariate analysis.
All the statistical analyzes were performed using the MATLAB R2021b Statistics and Machine Toolbox (MathWorks, Natick, MA, USA).
3. Results
3.1. Patient Characteristics
The study sample included 608 patients with PA tumours. The patients (344 females and 264 males) had a median age of 47 years (range 19-83 years). In particular, 362 (60%) were ≤50 years old and 246 (40%) >50 years old. A small percentage of the patients had a smoking and/or drinking habit: 51 patients were smokers (9%) and 27 patients drank alcohol (4.5%). The main demographic, clinical and pathological findings are shown in Table 1.
The tumours were mainly located in the parotid gland (98%), with a small percentage present in the submandibular gland (2%). Recurrence was reported in 33 patients (5%), with in each case the PA located in the parotid gland. Among the 33 patients who relapsed, 20 were females (60%) and 13 were males (40%). The mean age at the first relapse in the females was 44 +/- 11 years; whereas in the males it was 37 +/- 13 years. Furthermore, among the 33 who relapsed only 5 smoked, of whom 3 were males and 2 females, and only 2, both males, had a drinking habit.
3.2. Optimal Cut-Off Values for the Biomarkers (NLR,PLR and SII)
An ROC analysis was performed to identify the optimal threshold with the highest sensitivity and specificity in terms of predicting mortality. In Table 2 the performance with respect to recurrence detection is reported. The highest performance was achieved by the NLR with the AUC = 0.91, an accuracy of 96.1%, a sensitivity of 78.4%, a specificity of 97.2%, PPV = 64.4% and NPV = 98.6%.
The LRM and NLRM including all the haematological parameters did not increase the performance in terms of recurrence detection.
In Figure 1 the ROC curves for the NLR, PLR and SII and for the LRM and NLRM are reported.
4. Discussion
PA tumours are the most common SGTs and their incidence trend is increasing.
The treatment of PA remains challenging because of the various factors that can lead to tumour recurrence and the complications that can occur during surgery.
There are two common techniques which are performed, extracapsular dissection (ECD), and superficial parotidectomy (SP), but there is no consensus regarding which is the most effective.
In 1996 McGurk et al. showed no difference in terms of recurrence between patients treated with ECD and SP. A reduction in the incidence of Frey's syndrome from 32% in SP-treated cases to 5% in ECD cases was reported.[22]
Cristofaro et al. in 2014 showed that, when comparing the two surgical techniques (ECD vs SP), no significant differences were observed in terms of capsular rupture, recurrence and salivary fistulas. In contrast, transient facial nerve injuries and facial paralysis were significantly more frequent after SP than after ECD.[23]
Kadletz et al. in 2017 showed that recurrence of the disease (7.2% in ECD and 2.2% in SP) and permanent facial palsy (2.2% in ECD and 0.6% in SP) were significantly more frequent after ECD than after SP. [24] Bonavolontà et al in 2019 recommended ECD as a viable alternative to SP in terms of successful outcome for tumours under 3 cm. Transient facial nerve injury, hypoaesthesia, Frey syndrome, and facial paralysis were significantly more common after SP than ECD. No statistically significant difference in the recurrence rate was reported between ECD and SP.[25] Quer et al in 2017 proposed the following new guidelines for parotid PA surgery: ECD may be considered a good option in PA located very superficially or at the periphery and less than or equal to 3 cm in size; a level I or II parotidectomy may be considered in PA less than or equal to 3 cm, deep or far from the parotid border; finally, for tumours >3 cm involving two or more than 2 levels, a conventional parotidectomy is recommended.[26]
In the correct management of PA in addition to considering which is the most appropriate surgical treatment in accordance with the size and location of the tumour, other factors must also be evaluated. Li et al, due to the measured spread of satellite nodules, recommended margins of healthy parotid tissue of about 1 cm.[27]
Unfortunately, a complete resection of the margins is often impossible because of the adjacent branches of the facial nerve. The anatomic pathologist will only have a very thin capsule to examine, which may raise doubts about the reliability of the data. In the presence of an ambiguous assessment of positive margins, it is highly plausible to expect a higher recurrence. Indeed, this is one of the main risk factors in relation to recurrence.
Tumour spillage is another risk factor to consider which can sometimes be avoided. It generally occurs when the tumour reaches a larger size and the tumour capsule is very thin. In these cases, the pressure exerted to remove the deepest parts of the tumour may cause the capsule to rupture in the most superficial area, facilitating visible aspiration and the removal of the tumour. When, on the other hand, the capsule rupture occurs in the deepest region a complete resection may be difficult, leading to dissemination of the tumour. [28]
Some authors have shown that some subtypes of PA tend to have incomplete capsules. This could be another reason for recurrence. The thickness of the capsule varies from 0.015 to 1.75 mm. It is thicker in parenchyma-rich tumours than in stroma-rich ones. Some authors in the literature have even reported the absence of the capsule in some PA subtypes.
Naeim et al.[13] were the first to establish this relationship, finding that 69% of myxoid PA had incomplete capsules compared to 30% of classical and 18% of hypercellular subtypes. Stennert et al. [29] also described larger areas of incomplete capsule in the myxoid type, as much as 28% of the entire tumour circumference.
Valstar et al showed that, in addition to tumour spillage, positive and uncertain resection margins, a younger age at diagnosis and a tumour localisation in the parotid gland compared to the minor salivary glands result in a higher probability of recurrence.[30] In fact, recurrence occurs in younger patients, with females being affected 1.6 times more frequently than males.[31]
Additionally, in the study performed, the recurrence rate affected females more significantly (60%) than males (40%). Furthermore, the mean age of the first relapse in females was 44 +/- 11 years, whereas in males it was 37 +/- 13 years
On the other hand, no relationship was found with smoking and drinking. Among the 33 who relapsed only 5 smoked, of whom 3 were males and 2 females, and only 2, both males, had a drinking habit.
Many relapses of PA can be extremely difficult to manage. Moreover, after repeated recurrences, it appears that PA may slowly acquire malignant characteristics.
The main problem with multiple surgeries due to the recurrence of PA is the risk of permanent damage to the facial nerve, which increases with the number of surgeries. Valstar et al showed facial nerve damage between 3% and 16%, at the first recurrence, rising to 15%-21% for the second recurrence and 18%-30% for the third recurrence. [32]
Radiotherapy (RT) seems to be recommended as a good treatment modality in PA recurrences. In detail, in cases of an incomplete tumour excision, intra-operative tumour spillage, RT appears to be a good option in terms of reducing the rate of recurrence.
Chen et al. evaluated the role of RT in the management of 34 patients with recurrent PA of the parotid gland. The use of post-operative RT resulted in an excellent long-term local control rate of about 94%, with an acceptable late toxicity. Only one patient developed a second neoplasm, approximately 14 years after the completion of the therapy.[33]
According to the French Society of Radiotherapy and Oncology (SFRO), post-operative RT can be used in addition to incomplete resection margins also in relation to recurrent PA larger than 5 cm, or those which pose a significant risk to the facial nerve.[34]
In cases where the PA presented as multimodular at the first recurrence, RT as an adjuvant therapy was strongly recommended. Indeed, it was demonstrated that patients presenting with a multinodular PA were significantly more likely to suffer from recurrence than those with a non-multinodular recurrence.[35]
Therefore, RT of salivary gland tumours requires a degree of personalisation.
In our study with respect to only one initial type of surgical treatment, namely ECD, considering that most PA originate in the superficial lobe, we aimed to evaluate if there are factors that can help the surgeon to perform a more aggressive treatment to reduce the rate of recurrence.[36] In PA, the state of inflammation plays an important role in determining the aggressiveness of the tumour in terms of recurrence and possible malignant transformation. Such inflammation depends on a number of previously described factors which promote these tumour characteristics.
The presence of chronic inflammatory cells is often observed in the peritumoral area and stroma of PA. In particular, they present in the connective tissue capsule and stroma of almost all cases of tumours in major and minor salivary glands.
The most frequently observed cells are plasmacytoids, predominantly in tumours of the major salivary glands. In addition, a higher density of blood vessels has been found in the major salivary glands, indicating their role in angiogenesis.[37]
Moreover, pseudopodia, tumour nodules that protrude from the edges of the tumour and are separated by fibrous tissue from the main tumour mass, have been recognised as a cause of recurrence by Patey and Thackray.[38]
Pseudopodia were found in 28% of cases of tumour recurrence by Stennert [29], 40% by Zbären and Stauffer [39] and 54% by Park et al. [40].For these reasons, inflammation may be triggered by the immune system in an attempt to limit proliferative activity. Abbate et al. showed that inflammation plays a primary role in the genesis of some SGT, as confirmed by the high value of the inflammatory biomarkers. In particular, the PLR was significantly higher in PA than in Warthin tumours, with a cut-off of 135.55.[41] In recent literature, inflammatory biomarkers have been evaluated as prognostic elements in predicting the degree of malignancy in various tumours, including SGT. An increase in the NLR, PLR and SII indicated a poor prognosis. Damar et al. were the first to establish in SGT that an elevated NLR could be used as an inflammatory marker to distinguish low-grade from high-grade parotid gland malignancies. [42] Moreover, Kuzucu et al indicated that pre-operative NLR and PLR values are higher in patients with malignant salivary gland tumors ( mSGTs) than in patients with benign salivary gland tumors ( bSGTs). No statistically significant differences in terms of NLR and PLR were found between patients with mSGTs in relation to their stages.[43]
More recently Abbate et al. have demonstrated that there are statistically significant increases in the NLR, PLR, and SII indices in malignant SGT compared with benign SGT, establishing a cut-off value.[44]
In our study, it has been demonstrated that increased inflammatory biomarkers, in particular the NLR, can be related to the recurrence of PA. An analysis of the results has shown that the NLR (cut-off 2.960) has an accuracy of 96.1%, sensitivity of 78.4% and specificity of 97.2% in predicting such a recurrence. This result, revealed in a simple pre-operative analysis, could play an important role in the decision-making process in relation to the initial treatment of these tumours, enabling an evaluation of the most appropriate approach by means of close post-surgical follow-up or subsequent radiotherapy treatment.
Our study has certain limitations. It is a retrospective study of 608 patients with PA. However, unknown inflammatory diseases which remained unreported when taking each patient’s history could have influenced the results of the inflammatory biomarkers. Further studies in other centres with larger patient cohorts are mandatory for any validation of our results.
5. Conclusions
In conclusion, the encouraging results of our study demonstrate that the NLR, with a cut-off of 2.960, is the best biomarker in terms of predicting the recurrence of PA and can be used as a support tool in relation to pre-operative instrumental investigations to guide the treatment strategy and post-operative follow-up of PA patients.
Author Contributions
Conceptualization, Giovanni Salzano; methodology,Umberto Committeri; software,Vincenza Granata, Francesco Perri ; validation, Luigi Angelo Vaira; formal analysis, Arianna Di Stadio; investigation, Marzia Petrocelli, Fabio Di Blasi; resources, Maria Esposito; data curation, Gerardo Borriello; writing—original draft preparation, Simona Barone; writing—review and editing, Franco Ionna, Vincenzo Abbate; visualization, Giovanni Salzano; supervision, Luigi Califano; project administration, Giovanni Dell’Aversana Orabona. All the authors have read and agreed to the published version of the manuscript.
Funding
This research has received no external funding
Institutional Review Board Statement
An ethical review and approval were waived in relation to this study due to its observational retrospective nature.
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study in accordance with the declaration of Helsinki.
Data Availability Statement
Not applicable here.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhan, K.Y.; Khaja, S.F.; Flack, A.B.; Day, T.A. Benign Parotid Tumors. Otolaryngol Clin North Am. 2016, 49, 327–342. [Google Scholar] [CrossRef] [PubMed]
- Vincente, O.P.; Marques, N.A.; Aytes, L.B.; Escoda, C.G. Minor salivary gland tumors: A clinicopathological study of 18 cases. Med Oral Patol Oral Cir Buccal. 2008, 13, 582–588. [Google Scholar]
- Chhabra, S.; Bhutani, N.; Jain, P.; Gill, M.; Nishisth, N.; Sen, R. 'Pleomorphic adenoma of the tongue: A common entity at the uncommon location'. Ann Med Surg (Lond). 2018, 23, 34–36. [Google Scholar] [CrossRef] [PubMed]
- Almeslet, A.S. Pleomorphic Adenoma: A Systematic Review. Int J Clin Pediatr Dent. 2020, 13, 284–287. [Google Scholar] [CrossRef]
- Kakimoto, N.; Gamoh, S.; Tamaki, J.; Kishino, M.; Murakami, S.; Furukawa, S. CT and MR images of pleomorphic adenoma in major and minor salivary glands. Eur J Radiol. 2009, 69, 464–472. [Google Scholar] [CrossRef]
- Sadetzki, S.; Oberman, B.; Mandelzweig, L.; Chetrit, A.; Ben-Tal, T.; Jarus-Hakak, A. Smoking and risk of parotid gland tumors: A nationwide case-control study. Cancer, 2008, 112, 1974–1982. [Google Scholar] [CrossRef]
- Papadogeorgakis, N. Partial superficial parotidectomy as the method of choice for treating pleomorphic adenomas of the parotid gland. Br J Oral Maxillofac Surg 2011, 49, 447–450. [Google Scholar] [CrossRef]
- Rooker, S.A.; Van Abel, K.M.; Yin, L.X.; Nagelschneider, A.A.; Price, D.L.; Olsen, K.D.; et al. Risk factors for subsequent recurrence after surgical treatment of recurrent pleomorphic adenoma of the parotid gland. Head & Neck 2021, 43, 1088–1096. [Google Scholar]
- Antony, J.; Gopalan, V.; Smith, R.A.; Lam, A.K. Carcinoma ex pleo- morphic adenoma: A comprehensive review of clinical, patho logical and molecular data. Head Neck Pathol. 2012, 6, 1–9. [Google Scholar] [CrossRef]
- Olsen, K.D.; Lewis, J.E. Carcinoma ex pleomorphic adenoma: A clinicopathologic review. Head Neck 2001, 23, 705–712. [Google Scholar] [CrossRef]
- Riad, M.A.; Abdel-Rahman, H.; Ezzat, W.F.; Adly, A.; Dessouky, O.; Shehata, M. Variables related to recurrence of pleomorphic adenomas: Outcome of parotid surgery in 182 cases. Laryngoscope 2011, 121, 1467–1472. [Google Scholar] [CrossRef]
- Seifert, G.; Langrock, I.; Donath, K. Pathomorphologische Subklassifikation der pleomorphen Speicheldrusenadenome. Analyse von 310 pleomorphen Parotisadenomen. HNO 1976, 24, 415–426. [Google Scholar]
- Naeim, F.; Forsberg, M.I.; Waisman, J.; Coulson, W.F. Mixed tumors of the salivary glands. Growth pattern and recurrence. Arch Pathol Lab Med. 1976, 100, 271–275. [Google Scholar]
- Bokhari, M.R.; Greene, J. Pleomorphic Adenoma. 2022 Jul 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Savera, A.T.; Zarbo, R.J. Defining the role of myoepithelium in salivary gland neoplasia. Adv Anat Pathol 2004, 11, 69–85. [Google Scholar] [CrossRef] [PubMed]
- Moon, H.; Roh, J.L.; Lee, S.W.; Kim, S.B.; Choi, S.H.; et al. Prognostic value of nutritional and hematologic markers in head and neck squamous cell carcinoma treated by chemoradiotherapy. Radiotherapy and oncology; 2016, 118, 330–334. [Google Scholar] [CrossRef]
- Tham, T.; Wotman, M.; Chung, C.; Ahn, S.; Dupuis, H.; Gliagias, V. Systemic immune response in squamous cell carcinoma of the head and neck: A comparative concordance index analysis. European Archives of Oto-Rhino-Laryngology 2019, 276, 2913–2922. [Google Scholar] [CrossRef] [PubMed]
- Abbate, V.; Barone, S.; Troise, S.; Laface, C.; Bonavolontà, P.; Pacella, D.; et al. The Combination of Inflammatory Biomarkers as Prognostic Indicator in Salivary Gland Malignancy. Cancers 2022, 14, 5934. [Google Scholar] [CrossRef]
- Committeri, U.; Barone, S.; Salzano, G.; Arena, A.; Borriello, G.; Giovacchini, F.; et al. Support Tools in the Differential Diagnosis of Salivary Gland Tumors through Inflammatory Biomarkers and Radiomics Metrics: A Preliminary Study. Cancers; 2023, 15, 1876. [Google Scholar] [CrossRef] [PubMed]
- Iuchi, H.; Ohori, J.; Haraguchi, M.; Ando, Y.; Toge, S.; Yamashita, M. (Predictive Value of Combined Peripheral Inflammatory Markers in Patients with Head and Neck Cancers. Research Square 2023. [Google Scholar] [CrossRef]
- Salzano, G.; Dell'Aversana Orabona, G.; Abbate, V.; Vaira, L.A.; Committeri, U.; Bonavolontà, P.; et al. The prognostic role of the pre-treatment neutrophil to lymphocyte ratio (NLR) and tumor depth of invasion (DOI) in early-stage squamous cell carcinomas of the oral tongue. Oral Maxillofac Surg. 2022, 26, 21–32. [Google Scholar] [CrossRef]
- McGurk, M.; Renehan, A.; Gleave, E.N.; Hancock, B.D. Clinical significance of the tumour capsule in the treatment of parotid pleomorphic adenomas. Br J Surg. 1996, 83, 1747–1749. [Google Scholar] [CrossRef]
- Cristofaro, M.G.; Allegra, E.; Giudice, A.; Colangeli, W.; Caruso, D.; Barca, I.; et al. Pleomorphic adenoma of the parotid: Extracapsular dissection compared with superficial parotidec- tomy—A 10-year retrospective cohort study. Sci World J 2014, 564053. [Google Scholar] [CrossRef]
- Kadletz, L.; Grasl, S.; Grasl, M.C.; Perisanidis, C.; Erovic, B.M . Extracapsular dissection versus superficial parotidectomy in benign parotid gland tumors: The Vienna Medical School experience. Head Neck 2017, 39, 356–360. [Google Scholar] [CrossRef] [PubMed]
- Bonavolontà, P.; Orabona, G.D.A.; Maglitto, F.; Abbate, V.; Committeri, U.; Salzano, G.; et al. Postoperative complications after removal of pleomorphic adenoma from the parotid gland: A long-term follow up of 297 patients from 2002 to 2016 and a review of publications. British Journal of Oral and Maxillofacial Surgery, 2019, 57, 998–1002. [Google Scholar] [CrossRef] [PubMed]
- Quer, M.; Vander Poorten, V.; Takes, R.P.; Silver, C.E.; Boedeker, C.C.; de Bree, R.; et al. Surgical options in benign parotid tumors: A proposal for classification. European Archives of Oto-Rhino-Laryngology 2017, 274, 3825–3836. [Google Scholar] [CrossRef]
- Li, C.; Xu, Y.; Zhang, C.; Sun, C.; Chen, Y.; Zhao, H.; et al. Modified partial superficial parotidectomy versus conventional superficial parotidectomy improves treatment of pleomorphic adenoma of the parotid gland. The American Journal of Surgery 2014, 208, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Panarese, A.; Bull, P.D.; Lee, J.A. Marginally excised parotid pleomorphic salivary adenomas: Risk factors for recurrence and management. A 12.5-year mean follow-up study of histologically marginal excisions. Clin Otolaryngol Allied Sci. 2003, 28, 262–266. [Google Scholar] [CrossRef]
- Stennert, E.; Guntinas-Lichius, O.; Klussmann, J.P.; Arnold, G. Histopathology of pleomorphic adenoma in the parotid gland: A prospective unselected series of 100 cases. The Laryngoscope, 2001, 111, 2195–2200. [Google Scholar] [CrossRef]
- Valstar, M.H.; De Ridder, M.; van den Broek, E.C.; Stuiver, M.M.; Van Dijk, B.A.C.; et al. Salivary gland pleomorphic adenoma in the Netherlands: A nationwide observational study of primary tumor incidence, malignant transformation, recurrence, and risk factors for recurrence. Oral oncology, 2017, 66, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, S.; Therkildsen, M.H.; Bjørndal, K.; Homøe, P. Pleomorphic adenoma of the parotid gland 1985-2010: A Danish nationwide study of incidence, recurrence rate, and malignant transformation. Head Neck. 2016, 38 (Suppl. S1), E1364–E1369. [Google Scholar] [CrossRef]
- Valstar, M.H.; Andreasen, S.; Bhairosing, P.A.; McGurk, M. Natural history of recurrent pleomorphic adenoma: Implications on management. Head & Neck 2020, 42, 2058–2066. [Google Scholar]
- Chen, A.M.; Garcia, J.; Bucci, M.K.; Quivey, J.M.; Eisele, D.W. Recurrent pleomorphic adenoma of the parotid gland: Long-term outcome of patients treated with radiation therapy. Int J Radiat Oncol Biol Phys. 2006, 15, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Larnaudie, A.; Marcy, P.Y.; Delaby, N.; Costes Martineau, V.; Troussier, I.; Bensadoun, R.J.; et al. Radiotherapy of salivary gland tumours. Cancer Radiother. 2022, 26, 213–220. [Google Scholar] [CrossRef]
- Wierzbicka, M.; Fijuth, J.; Składowski, K.; Jurkiewicz, D.; Burduk, P.; Miłoński, J.; Niemczyk, K.; Pietruszewska, W.; Rogowski, M.; Stodulski, D.; Mikaszewski, B. Adjuvant radiotherapy in parotid gland pleomorphic adenoma - recommendations. Otolaryngol Pol. 2022, 76, 1–7. [Google Scholar] [CrossRef]
- Sergi, B.; Limongelli, A.; Scarano, E.; Fetoni, A.R.; Paludetti, G. Giant deep lobe parotid gland pleomorphic adenoma involving the parapharyngeal space. report of three cases and review of the diagnostic and therapeutic approaches. Acta Otorhinolarngol Ital. 2008, 28, 261–265. [Google Scholar]
- Nonitha, S.; Yogesh, T.L.; Nandaprasad, S.; Maheshwari, B.U.; Mahalakshmi, I.P.; Veerabasavaiah, B.T. Histomorphological comparison of pleomorphic adenoma in major and minor salivary glands of oral cavity: A comparative study. Journal of Oral and Maxillofacial Pathology: JOMFP, 2019, 23, 356. [Google Scholar] [CrossRef] [PubMed]
- Patey, D.H.; Thackray, A.C. The treatment of parotid tumours in the light of a pathological study of parotidectomy material. British Journal of Surgery, 1958, 45, 477–487. [Google Scholar] [CrossRef]
- Zbären, P.; Stauffer, E. Pleomorphic adenoma of the parotid gland: Histopathologic analysis of the capsular characteristics of 218 tumors. Head & Neck: Journal for the Sciences and Specialties of the Head and Neck, 2007, 29, 751–757. [Google Scholar]
- Park, G.C.; Cho, K.J.; Kang, J.; Roh, J.L.; Choi, S.H.; Kim, S.Y.; et al. Relationship between histopathology of pleomorphic adenoma in the parotid gland and recurrence after superficial parotidectomy. Journal of surgical oncology, 2012, 106, 942–946. [Google Scholar] [CrossRef]
- Abbate, V.; Barone, S..; Orabona, G.D.A.; Bonavolontà, P.; Galdiero, M.R.; Cristinziano, L.; et al. Role of Inflammation in Benign Salivary Gland Tumor Etiopathogenesis: An Evaluation through the Blood Inflammatory Biomarkers. Eurasian Journal of Medicine and Oncology 2022, 6, 150–155. [Google Scholar]
- Damar, M.; Dinç, A.E.; Erdem, D.; Aydil, U.; Kizil, Y.; Eravcı, F.C.; et al. Pretreatment Neutrophil-Lymphocyte Ratio in Salivary Gland Tumors Is Associated with Malignancy. Otolaryngol. Head Neck Surg. 2016, 155, 988–996. [Google Scholar] [CrossRef] [PubMed]
- Kuzucu, İ.; Güler, İ.; Kum, R.O.; Baklacı, D.; Özcan, M. Increased neutrophil lymphocyte ratio and platelet lymphocyte ratio in malignant parotid tumors. Braz J Otorhinolaryngol. 2020, 86, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Abbate, V.; Orabona, G.D.A.; Barone, S.; Troise, S.; Bonavolontà, P.; Pacella, D.; et al. Relevance of Inflammatory Biomarkers in Salivary Gland Cancers Management. Eurasian, J. Med. Oncol. 2021, 5, 311–317. [Google Scholar] [CrossRef]
Figure 1.
ROC curves for the NLR, PLR and SII (A) and for the LRM and NLRM (B).
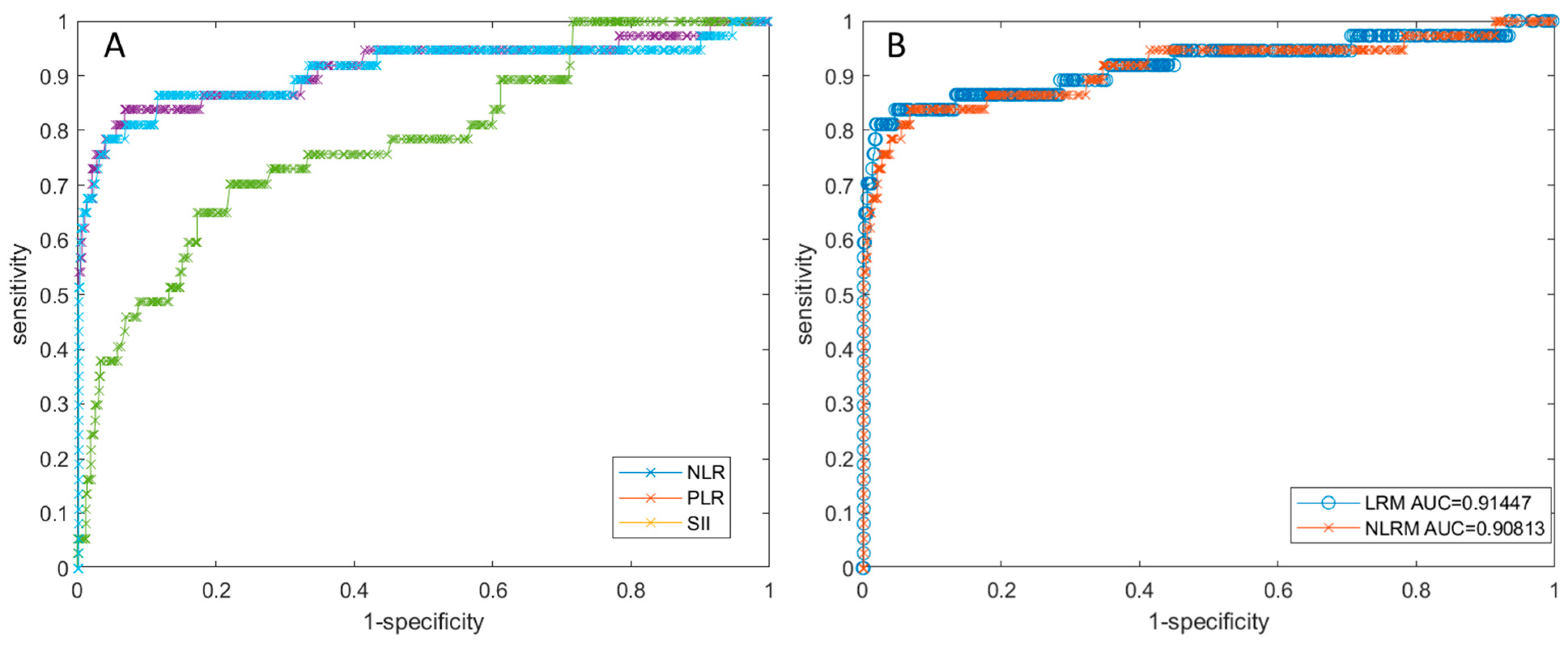

Table 1.
Sample characteristics.
| VARIABLES | TOTAL CASES 608 |
|---|---|
| Age( years) | |
| ≤50 | 362 (60%) |
| >50 | 246(40%) |
| Gender | |
| Female | 344 (56.5%) |
| Male | 264 (43.5%) |
| Smoking | |
| Yes | 51 (9%) |
| No | 557 (91%) |
| Alcohol | |
| Yes | 27 (4.5%) |
| No | 581 (95.5%) |
| Tumour location | |
| Parotid glands | 599 ( 98%) |
| Submandibolar glands | 9 (2%) |
| Recurrence | |
| Yes | 33 (5%) |
| No | 575 (95%) |
Table 2.
Performance to recurrence detection.
| Performance | NLR | PLR | SII | LRM | NLRM |
|---|---|---|---|---|---|
| AUC | 0.909 | 0.776 | 0.906 | 0.914 | 0.908 |
| Sensitivity [%] | 0.784 | 0.703 | 0.865 | 0.811 | 0.838 |
| Specificity [%] | 0.972 | 0.779 | 0.883 | 0.981 | 0.932 |
| PPV [%] | 0.644 | 0.171 | 0.323 | 0.732 | 0.443 |
| NPV [%] | 0.986 | 0.976 | 0.990 | 0.988 | 0.989 |
| Accuracy [%] | 0.961 | 0.775 | 0.882 | 0.970 | 0.926 |
| Cut-off | 2.960 | 153.911 | 645.760 | 0.227 | 0.066 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



