
Submitted:
11 July 2023
Posted:
12 July 2023
You are already at the latest version
Abstract
The natural distribution of stress in the femur is altered when total hip arthroplasty (THA) is performed. In fact, when a stem is inserted inside the femur, there is a variation in stress due to the difference in rigidity between the material with which the stem is made and the femur. This generates the phenomenon of stress-shielding. The aim of this study is to design an optimized prosthesis that guarantees excellent rotational stability and re-duced stress shielding. Methods: through the finite element method (FEM) the mechanical behavior of the stem subjected to the loads described by ISO 7206-4: 2010 is studied. Re-sults: Through topological optimization, there is a reduction in stress shielding in the proximal zone of 31.46%. The addition of ridges on the dorsal side of the stem also im-proves rotational stability by 27.82%. Conclusions: The decrease in stiffness that is rec-orded with the optimized stem, guarantees a greater distribution of stress on the bone. The presence of dorsal ridges also favors the corticalization of the bone as it loads the bone near the dorsal ensuring further stability. The perforated prosthesis presented in this study, shows an increase in primary stability and an improvement in rotational stability. As there is also a bone regrowth inside the prosthesis.
Keywords:
prosthesis
; stress shielding
; topological optimization
; Fem analysis
1. Introduction
Total hip arthroplasty (THR) is the therapy to treat degenerative diseases, such as hip osteoarthritis or degenerative cartilage diseases and trauma. In the case of trauma, intracapsular fractures may be found at the level of the head, intratrochanteric, included in the area between the small and the great trochanter and subtrochanter, at the diaphyseal level. [1] The purpose of a hip replacement is to restore the motility and functionality of the joint without causing pain to the patient. Both the stem and the components that make up the joint must be designed to ensure long-term mechanical reliability and reliability at the implantation site. [2] The use of THR is increasing, particularly in young patients. This factor influences the number of revision surgeries, as the increased life expectancy of the younger population has led to an increase in revision surgeries. In revision surgery, numerous technical difficulties are encountered due to bone loss as a result of mobilization. [3] The search for prosthetic alternatives has led to the modification of the primary components, improvements introduced and changes to obtain a more proximal load transfer to the femur in order to reduce the phenomenon of stress-shielding [4,5,6,7] therefore preserving the bone for possible revision surgery. In the last two decades, several conservative femoral prostheses have been designed and some authors have supported their use. Traditionally, tapered anatomical or cylindrical are used. The classic tapered stem has a rectangular cross section, 4 corners and 4 flat surfaces that are compressed in the proximal femur, the second type, the stem in the mid-distal view follows the curvature of the femoral canal. [8,9,10,11,12] The anatomy of the femur, in fact, has two curvatures called curved and procurvate. Figure 1
Studies comparing right and curved stems have shown that curved stems have greater torsional stability both proximal and distal. [8] It has also been shown that the torsional stability of the anatomical stems and is not proportional to the length of the stem itself. Despite the positive results of long-stem femoral prostheses, there are still concerns about the relatively high rate of early periprosthetic fractures, pain in the front of the thigh, bone loss, and high skin stress[13,14,15], mainly due to stress-shielding and rotational instability.
1.1. Rotational instability
It is a problem that is noted in many revisions. The result of the forces acting on the femoral head turns out to be eccentric with respect to the axis of the stem, thus exerting a high torsional moment to the prosthesis during walking, exposing it to rotational stresses as well as compression, flexion and traction stresses Figure 2.
Sections of the stem with carvings or with edges improve the anchorage of the stem. For example, rectangular sections with horizontal grooves (Figure 3a) and vertical ones ensure the anchorage of the stem to several points of the proximal cortical.
Thanks to the overstresses induced by both the notch sections and grooves, bone regrowth is stimulated which favors the anchoring of the stem. In the same way, the presence of ridges on the stem Figure 3b increases the stresses on the surrounding spongy bone, which corticalizing creates islands of cortical bone that stabilize the prosthesis
F2= force transmitted to the bone.
L2=lever arm of F2
Rotational stability is defined as the resistance of the implant to the joint forces that induce rotation around the longitudinal axis of the implant. Walking, climbing stairs and getting up from a sitting cause a moment M around the axis of the stem Figure 4. According to equation (1), the lever arm L2 depends on various anatomical configurations used. Figure 5.
We can see that the greater the lever arm (L 2) the lower the force (F) transmitted to the bone; and contrarywise, the smaller the lever arm (L 2), the greater the force (F) transmitted to the bone. Prostheses with a reduced radius (L 2) are not as strong because they produce a higher surface load leading to early prosthetic failure caused by local overload per unit area (N/mm2). A large medial and/or lateral radius produces greater resistance to rotation. The cortical support of the prosthesis is indispensable for stability and transmission of force, since the larger the area, the lower the specific surface load. The spongy bone is a dynamic element of minor importance in this sense since it yields when subjected to a specific axial load. Studies carried out [32] have shown that the design of the stem in the proximal zone plays a fundamental role in ensuring rotational stability. Stems with rectangular or trapezoidal section, have better behaviors in terms of stability to rotation because they provide greater anchoring surfaces than oval or elliptical shapes.
1.2. Stress-shielding
According to Wolff’s law,[16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33] bone remodeling occurs to adapt bone structure and geometry to loads acting from the outside. Before the implant is inserted into the femur, all the load is discharged along the bone surfaces, after insertion of the prosthesis, the bone turns out to be subjected to lower stresses. What occurs is an uneven distribution of stresses since we have the upper part of the femur which undergoes less loads while the distal part is overstressed by compression by the presence of the stem. Figure 6 Bone density decreases when the stress acting on the bone is lower than physiological stress [34]. While it increases, the acting loads turn out to be higher. This phenomenon is mainly due to the difference between the stiffness of the implant and that of the femur. The implants are made of metal alloys (steel, cobalt-chrome, titanium alloys), which are more stiff (100-200 Gpa) compared to that of the human femur (1-30 GPa) [35].
Therefore, in order to fill the problem of Stress-shielding, it is necessary to ensure that there is a decrease in the stiffness of the stem so as to have an increase in the transfer of the load to the bone, as also observed by (Diegel et al) [36] . The stiffness turns out to be dependent on the section and the material. In this study, we will vary the stiffness by acting on the section and through the finite element method we will compare the stiffness expressed by equation (2) of a modified stem, with the stiffness of a traditional solid stem.
In addition, stress shielding will be evaluated, comparing the Von Mises stress of the intact cortical bone with the Von Mises stress of the cortical bone with the implant. Fraldi and Esposito [37], defined stress shielding (SS) according to equation 3.
Low (SS) reflect changes in local stress in a region after implantation. A positive (SS) implies that the local region undergoes less stress than pre-surgical conditions, which induces stress-shielding; a negative (SS) suggests instead an increase in local stress or a potential concentration of stress. Rotational stability will be studied through the evaluation of stem rotations within the femur and comparing these results with those reported in the literature [38]. This study hypothesizes that comparing a traditional solid stem to an optimized Figure 7 stem will effectively reduce the effect of stress shielding and improve rotational stability. Moreover, thanks to the finite elements, important results can be obtained that provide the designer with the recommendations to be adopted to ensure implant stability.
2. Materials and Methods
2.1. Evaluation of stem stiffness
The finite element models were created in accordance with the load and constraint requirements of ISO 7206-4:2010. This standard provides with a good indication the ability that the femoral prosthesis possesses to withstand load conditions. ANSYS® Workbench software is used for finite element simulation Figure 8. The finite element analysis (FEA) model includes a suppression block (transmits 2300N compression to the stem), a femur head and the implant embedded in the cement 80 mm away from the center of the femoral head with an adduction angle of 10° and a flexion of 9°. Both made and assembled with 3D Inventor software. For the above parts, the material properties used in FEA are given in Table 1. The type of delimited contact was defined for bone cement – implant, conical head of the implant – inner surface of the femoral head, outer surface of the head of the. The concrete block was constrained in all directions. For all parts of the FEA model, tetrahedral elements with an average element size of 2 mm were used.
2.2. Bone implant stress assessment
To model the stem inserted inside the femur, a cylindrical 3D model Figure 9 was prepared, dividing it into the cortical and spongy part. [33]. Once assembled, the model was converted to an .stp file and exported to Ansys Workbench to prepare the mesh, define the contact, and set boundary conditions. The assembled model consists of 3 parts (cortical bone, spongy bone, femoral stem), this classification of the CAD model served to assign the properties of the material independently. It was assumed that both cortical and spongy bone had linear, orthotropic and homogeneous mechanical properties. The bone properties listed in Table 1 were taken from [34,35,36]. As for the stem, it was made of Ti6Al4V titanium alloy. The properties of titanium alloy are shown in Table 1. The base of the bone model was constrained in all directions. The contacts between prosthesis and bone have been set as: bonded and no separation. The loads were taken from the work of Wen-Chen et al., 2014 [37] and Bergmann et al., respectively. [38]. Figure 10
2.3. Meshing.
The stem-bone model was assembled with approximately 614904 tetrahedral elements Figure 11 adopting an average element size of 2.4 mm as also reported in [39] for the stem. Instead, with regards to the bone, since it is the main object of study we want to investigate about the distribution of tensions, a mesh size of 2mm has been adopted to have greater accuracy in the results.
Figure 12 shows the mesh convergence verification that displays how adopting an element size of 2mm, the error committed is 0.20%.[39,40] Mesh convergence analysis is an important process in finite element analysis (FEA) to ensure the accuracy and reliability of results. Mesh convergence refers to achieving stable and consistent results as the mesh size and density is refined. If the results do not converge as expected, you may need to repeat the process of meshing and analysis with a different strategy to achieve adequate convergence. This could include the use of localized mesh refinement techniques or optimization of analysis parameters.
3. Results
Figure 13 shows the displacement load graph and the stiffness obtained with the first FEM model (ISO 7206-4:2010) according to equation 4 for the standard stem and for the optimized one comparing it with that of the human femur [41].
Based on these early stiffness results, we should expect the stem femur in Ti6Al4V to have lower stress after THA, as the Ti6Al4V stem is stiffer than the femur; the femur with optimized stem instead should have the opposite case, in which greater stress is expected after THA. Through the second FEA study, in Figure 14, the results of the Von Mises stress for the traditional and optimized stem are reported.
Regarding the stems instead, in Figure 15 the results of the Von Mises stress are reported.
As shown in Figure 14, stress is mainly concentrated in the proximal zone, as also shown by Swanson et,al [42]. Observing the distribution of stress for the full stem and the optimized stem, it is clear that there is a global increase in stress from the proximal to the distal zone. This phenomenon can also be explained by observing Figure 15 in which we see how the optimized stem has a lower stress than the traditional solid stem, this phenomenon makes it clear how part of the load is distributed more on the bone in contact, with a reduction in stress-shielding. Moreover, considering the yield stress (110 Mpa) of the cortical bone detected by a study on cadavers [43] we can affirm that the insertion of the prostheses does not involve risks of fracture for the femur.
Through equation 3 we can calculate the stress shielding for the two stems Table 2 taking as reference the Von Mises stress of the stemless bone Figure 14 and the results of the Von Mises stress for the bone in the two cases, summarized in Figure 16.
From the table, we observe how in the proximal area where there are higher loads, with the optimized stem we obtain a reduction in stress-shielding of 31.47% compared to the traditional stem 24.08%. This result is also part of the percentages obtained from other studies in the literature [44,45,46,47]
Figure 17 shows the deformation of the stem in the bone.
Micromovements of femoral prostheses refer to small sliding or rotational movements that can occur between the femoral stem of the prosthesis and the surrounding bone after implantation. These movements can be influenced by various factors, including implant design, bone fixation, the characteristics of the patient’s bone, and physical activity. The goal of implanting a femoral prosthesis is to achieve adequate stability and integration with the surrounding bone. However, it is not always possible to completely avoid micro-movements. Some micromovements can be considered normal and can help in the stimulation of bone growth and osseointegration of the implant. However, excessive or uncontrolled movements can lead to problems such as premature wear of the implant, detachment of the coating or overall instability of the implant. Therefore, it is important to try to minimize unwanted micro-movements during the design and implantation of femoral prostheses. The maximum displacement values of the center of the head are 0.023 mm for the standard stem and 0.0166 mm for the optimized stem, thus reducing torsional deformation by 27.82%. From which it is therefore clear that the optimized prosthesis has a greater rotoational stability than the standard prosthesis. This can be explained by considering that during the insertion of the standard stem, the greater trochanter turns out to be weakened more due to the design of the proximal zone of the stem. Therefore, the optimized stem has a less invasive design which preserves the trochanter that, in contact with the stem, gives greater stability.
4. Discussion
The stiffness of the femoral stem of a prosthesis is an important factor to consider in the design and choice of the implant, it can influence the load transferred to the surrounding bone and the overall mechanical behavior of the implant. The stiffness of the femoral stem depends on several factors, Materials: however metallic materials are used, such as titanium alloys or stainless steel, which have different stiffness characteristics. For example, titanium has greater ductility than stainless steel, which can affect the overall stiffness of the stem. Geometry: A no stem with a larger diameter or a larger cross-section will have greater stiffness than one with a smaller diameter. In addition, the stem can be designed with a cylindrical, conical, or modular geometry, which will affect its overall stiffness. Bone fixation, for example, a cemented stem will have greater rigidity than a stem with press-fit fixation, since acrylic cement contributes to the overall rigidity of the system. The choice of fixation method depends on the characteristics of the patient’s bone and the preferences of the surgeon. Stem-bone interface: The interaction between the femoral stem and the surrounding bone can affect the overall stiffness of the implant. For example, if the stem is designed with a porous surface or hydroxyapatite coating, this can promote osseointegration and increase the stability of stem-bone contact, thus affecting overall stiffness. It is important to carefully consider the stiffness of the femoral stem according to the specific needs of the patient.[48] Excessive stiffness of the stem could cause excessive stress on the surrounding bone, while insufficient stiffness could compromise the stability of the implant. Therefore, the choice of stem type, size and overall implant design should be carefully evaluated by the orthopedic surgeon based on the characteristics of the femur bone, the patient’s health, and functional needs. Contact between the femoral shaft of a prosthesis and the surrounding bone is critical to the success and durability of the implant. During femur arthroplasty, the stem of the prosthesis is inserted inside the medullary canal of the femur bone. The goal is to achieve stable and long-lasting contact between the stem and bone to ensure good load transmission and prevent unwanted movements or implant failures. There are several factors to consider when optimizing the contact between the femoral stem and the bone [49,50,51]: Stem profile design: The geometry of the stem profile can affect contact with the surrounding bone. Several designs of femoral stems are available, including cylindrical, conical, or anatomical stems. The choice of stem profile depends on the anatomical features of the patient and the condition of the femur bone. Surface coatings: Some femoral dentures may have special surface coatings to improve contact with the bone. For example, the coating of hydroxyapatite or other porous coatings can promote bone growth and promote better integration of the implant with the bone. Bone fixation: Implant stability can be improved through bone fixation techniques, such as the use of acrylic cement or press-fit fixation. The method of fixation depends on the characteristics of the patient’s bone and the design of the prosthesis. Dimensional adaptation: it is important that the size of the femoral stem is appropriate for the medullary canal of the bone. [52]Proper adaptation avoids excessive stress on the walls of the surrounding bone and promotes the stability of the implant. Load and activity: Optimizing contact between the femoral shaft and bone also requires consideration of the patient’s load and activities. The stem design and material must be able to withstand the mechanical stresses associated with everyday activities, such as walking, climbing stairs and other movements. It is important that the contact between the femoral shaft and the bone is stable and long-lasting to ensure good functionality of the prosthesis and reduce the risk of complications, such as implant failure or detachment of the coating. The choice of stem type, fixation technique and overall implant design should be carefully evaluated by the orthopedic surgeon based on the patient’s specific needs and femoral bone characteristics. In non-cemented prostheses it is essential to obtain a proximal fixation of the stem in such a way as to increase the load on the area near the femur, thus reducing the possibility of bone atrophy. If sufficient adaptation is not achieved, the phenomenon of stress shielding is generated [48]. Therefore, the distal part must be flexible to transfer loads to the bone. Solid sections have the disadvantage of stiffening the stem and presenting maximum torsional instability, while grooved or windowed sections increase the flexibility of the stem and guarantee torsional stability. The stiffness of the stem, which is determined by the geometry of its cross section and elastic modulus, affects the stresses in the entire system. Studies show that it is possible to achieve a reduction in stress shielding with hollow section stems compared to solid stems, some hollow forms work better than others. [37] The advantage of the hollow stem lies in greater rigidity control, while maintaining acceptable anatomical adaptation. This is possible thanks to the wide range of rigidities offered by hollow sections. The external shape of the stem can be chosen according to anatomical criteria and the internal dimensions can be adjusted to optimize bone stresses. In any case, it is necessary to find a compromise to optimize both the stability and flexibility of the prosthesis. In fact, as reported in [49] a reduction in stem stiffness certainly leads to a reduction in stress shielding but also to an increase in stress in the proximal area of the femur inducing the risk of fractures. Figure 18
Proximally wide prostheses have greater prosthetic support and therefore greater rotational stability. In fact, as explained in [50] a height of the proximal segment exerts a greater load on the bone surface, when the resistance to rotation is exceeded the torque can no longer be transmitted completely to the bone and the stem begins to rotate. Consequently, a low transmitted moment is indicative of lower rotoational stability. Torsional resistance can be increased in relation to femoral neck geometry [51] and by adding ridges on the lateral surfaces of the stem. The addition of ridges anteriorly, posteriorly and laterally, increases rotoational stability by 50% [52]. When porously coated implants are used, rotoational stability is guaranteed only if the diaphysis is under boring and very narrow diaphyseal fixation is achieved [53]. The current study conducted with the finite element method (FEA), is limited by the use of mechanical properties of materials found in the literature. But comparing the results obtained with those performed by other scholars [54,55,56,57] we note a certain numerical correspondence; In fact, in this study a reduction of about 32% was achieved with regard to stress shielding, compared to (15-40%) obtained by other studies.
5. Conclusions
Reducing stress shielding is an important goal in the design of femoral prostheses. Stress shielding occurs when the implant replaces the loading function of the surrounding bone, leading to a decrease in stress and mechanical charge on the bone. This can cause a reduction in bone density and a weakening of the bone around the implant. To reduce stress shielding and promote the preservation of the surrounding bone, several strategies can be adopted:[53,54,55]
- Stem flexibility: A femoral stem designed with an appropriate degree of flexibility may allow for better load distribution between the implant and the surrounding bone. This helps reduce stress focused on specific regions of the bone and minimize stress shielding.
- Neck geometry: The geometry of the stem neck can affect the distribution of forces and the stress transferred to the bone. A neck with a proper shape and length can contribute to a more even distribution of the load and reduce stress shielding.
- Surface coatings: The use of surface coatings, such as porous coatings or hydroxyapatite coatings, can promote osseointegration of the implant and improve load transmission to the surrounding bone. This helps reduce stress shielding and promote better long-term stability of the implant.
- Selective fixation: Selective fixation refers to the use of different fixation methods in different regions of the femoral stem. For example, cemented fixation or press-fit fixation may be used in regions where greater stability is desired, while in other regions less rigid fixation may be preferable. This strategy helps reduce overall stem stiffness and minimize stress shielding.
- Gradual loading: A gradual post-operative loading and appropriate rehabilitation can contribute to a better adaptation of the bone to the implant and a reduction in stress shielding. A gradual loading process allows the bone to gradually adapt to new mechanical conditions and promotes bone remodeling
This study outlined a new single-stem design for the (THR) through finite element modelling to reduce the phenomenon of stress shielding leading to aseptic loosening and improve rotoational stability. It has been shown that by using a prosthesis with holes and windows, stiffness can be greatly reduced and stress shielding can suffer a decrease of 31.46% compared to 24.08% of the complete stem. This study also showed that drilling transverse holes in the prosthesis improves rotoational stability by 27.82% compared to the full stem, as bone regrowth both on the surface and inside the prosthesis would improve stability. The main limitations of this study derive from the modelling carried out and the properties of the materials used in the simulation. It is important to note that reducing stress shielding should not compromise the stability and integration of the system.[56,57] Therefore, implant design and load management decisions should be based on an accurate assessment of patient bone characteristics, functional needs, and clinical considerations. Future studies should take a deeper look at the actual mechanical properties of bone and its dynamic remodeling at applied loads for more accurate modeling. The potential benefits for the patient from reducing stress shielding are better integration with the bone, which should lead to a reduction in aseptic loosening failures and better patient recovery.
Author Contributions
Conceptualization, M.C. and B.T.; methodology, M.C.; software, M.C.; validation, B.T.,. formal analysis, M.C. and B.T.; investigation, M.C.; resources, M.C. and B.T.; data curation ,M.C.; writing—original draft preparation, M.C. and B.T.; writing—review and editing,M.C, B.T,.; visualization, B.T, .; supervision,. and B.T.; project administration,. and B.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All experimental data to support the findings of this study are available contacting the corresponding author upon request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Hampton, S.J.; Andriacchi, T.P.; Galante, J.O. Three dimensional stress analysis of the femoral stem of a total hip prosthesis. J. Biomech. 1980, 13, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J. Movements at the hip joint, Ann. R. Coll. Surg. Engl. 1975, 56, 192–201. [Google Scholar]
- Joshi, M.G.; Advani, S.G.; Miller, F.; Santare, M.H. Analysis of a femoral hip prosthesis designed to reduce stress shielding. Journal of Biomechanics 2000, 33, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Gross, S.; Abel, E.W. A finite element analysis of hollow stemmed hip prostheses as a means of reducing stress shielding of the femur. Journal of Biomechanics 2001, 34, 995–1003. [Google Scholar] [CrossRef]
- Rometsch, E.; Bos, P.K.; Koes, B.W. Survival of short hip stems with a “modern”, trochanter-sparing design - a systematic literature review. Hip Int 2012, 22, 344–354. [Google Scholar] [CrossRef]
- Banerjee, S.; Pivec, R.; Issa, K.; et al. Outcomes of short stems in total hip arthroplasty. Orthopedics 2013, 36, 700–707. [Google Scholar] [CrossRef]
- Moskal, J.T.; Capps, S.G. Is limited incision better than standard total hip arthroplasty? A meta-analysis. Clin Orthop Relat Res 2013, 471, 1283–1294. [Google Scholar] [CrossRef]
- Berstock, J.R.; Blom, A.W.; Beswick, A.D. A systematic review and meta-analysis of the standard versus miniincision posterior approach to total hip arthroplasty. J Arthroplasty 2014, 29, 1970–1982. [Google Scholar] [CrossRef]
- Yue, C.; Kang, P.; Pei, F. Comparison of direct anterior and lateral approaches in total hip arthroplasty: A systematic review and meta-analysis (PRISMA). Medicine (Baltimore) 2015, 94, e2126. [Google Scholar] [CrossRef]
- Feyen, H.; Shimmin, A.J. Is the length of the femoral component important in primary total hip replacement? Bone Joint J 2014, 96-B, 442–448. [Google Scholar] [CrossRef]
- Khanuja, H.S.; Banerjee, S.; Jain, D.; et al. Short bone-conserving stems in cementless hip arthroplasty. J Bone Joint Surg Am 2014, 96, 1742–1752. [Google Scholar] [CrossRef] [PubMed]
- Courpied, J.P.; Caton, J.H. Total hip arthroplasty, state ofthe art for the 21st century. Int Orthop 2011, 35, 149–150. [Google Scholar] [CrossRef] [PubMed]
- Khanuja, H.S.; Vakil, J.J.; Goddard, M.S.; et al. Cementless femoral fixation in total hip arthroplasty. J Bone Joint Surg Am 2011, 93, 500–509. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.E.; Larson, B.; Shen, F.; et al. Thigh pain after cementless total hip arthroplasty: Evaluation and management. J Am Acad Orthop Surg 2002, 10, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Engh, C.A., Jr.; Young, A.M.; Engh, C.A., Sr.; et al. Clinical consequences of stress shielding after porous-coated total hip arthroplasty. Clin Orthop Relat Res 2003, 417, 157–163. [Google Scholar] [CrossRef]
- Wilson, D.A.; Dunbar, M.J.; Amirault, J.D.; Farhat, Z. Early failure of a modular femoral neck total hip arthroplasty component: A case report. J Bone Joint Surg Am 2010, 92, 1514e7. [Google Scholar] [CrossRef] [PubMed]
- Lakstein, D.; Eliaz, N.; Levi, O.; Backstein, D.; Kosashvili, Y.; Safir, O.; et al. Fracture of cementless femoral stems at the mid-stem junction in modular revision hip arthroplasty systems. J Bone Joint Surg Am 2011, 93, 57e65. [Google Scholar] [CrossRef]
- Wright, G.; Sporer, S.; Urban, R.; Jacobs, J. Fracture of a modular femoral neck after total hip arthroplasty: A case report. J Bone Joint Surg Am 2010, 92, 1518e21. [Google Scholar] [CrossRef]
- Quintana, J.M.; Arostegui, I.; Azkarate, J.; Goenaga, J.I.; Elexpe, X.; Letona, J.; Arcelay, A. Evaluation of explicit criteria for total hip joint replacement. J. Clin. Epidemiol. 2000, 53, 1200–1208. [Google Scholar] [CrossRef]
- Gademan, M.G.J.; Hofstede, S.N.; Vlieland, T.P.M.V.; Nelissen, R.G.H.H.; De Mheen, P.J.M.-V. Indication criteria for total hip or knee arthroplasty in osteoarthritis: A state-of-the-science overview. BMC Musculoskelet. Disord. 2016, 17, 463. [Google Scholar] [CrossRef]
- Lucchini, S.; Castagnini, F.; Giardina, F.; Tentoni, F.; Masetti, C.; Tassinari, E.; Bordini, B.; Traina, F. Cementless ceramic-on ceramic total hip arthroplasty in post-traumatic osteoarthritis after acetabular fracture: Long-term results. Arch. Orthop. Trauma. Surg. 2021, 141, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Fokter, S.K.; Levašič, V.; Kovač, S. The Innovation Trap: Modular Neck in Total Hip Arthroplasty. ZdravVestn 2017, 86, 115–126. [Google Scholar]
- Aljenaei, F.; Catelas, I.; Louati, H.; Beaulé, P.E.; Nganbe, M. Effects of hip implant modular neck material and assembly method on fatigue life and distraction force. J. Orthop. Res. 2017, 35, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- Zajc, J.; Moličnik, A.; Fokter, S. Dual Modular Titanium Alloy Femoral Stem Failure Mechanisms and Suggested Clinical Approaches. Materials 2021, 14, 3078. [Google Scholar] [CrossRef]
- Weiser, M.C.; Chen, D.D. Revision for taper corrosion at the neck-body junction following total hip arthroplasty: Pearls and pitfalls. Curr. Rev. Musculoskelet. Med. 2016, 9, 75–83. [Google Scholar] [CrossRef]
- Wright, C.G.; Sporer, S.; Urban, R.; Jacobs, J. Fracture of a Modular Femoral Neck After Total Hip Arthroplasty: A Case Report. J. Bone Jt. Surg. 2010, 92, 1518–1521. [Google Scholar] [CrossRef]
- Vucajnik, I.; Fokter, S.K. Modular Femoral Neck Fracture After Total Hip Arthroplasty. In Recent Advances in Hip and Knee Arthroplasty; IntechOpen: London, UK, 2012. [Google Scholar]
- Grupp, T.M.; Weik, T.; Bloemer, W.; Knaebel, H.-P. Modular titanium alloy neck adapter failures in hip replacement—Failure mode analysis and influence of implant material. BMC Musculoskelet. Disord. 2010, 11, 3. [Google Scholar] [CrossRef]
- Meftah, M.; Haleem, A.M.; Burn, M.B.; Smith, K.M.; Incavo, S.J. Early Corrosion-Related Failure of the Rejuvenate Modular Total Hip Replacement. J. Bone Jt. Surg. Am. 2014, 96, 481–487. [Google Scholar] [CrossRef]
- Bernstein, D.T.; Meftah, M.; Paranilam, J.; Incavo, S.J. Eighty-six Percent Failure Rate of a Modular-Neck Femoral Stem Design at 3 to 5 Years: Lessons Learned. J. Bone Jt. Surg. 2016, 98, e49. [Google Scholar] [CrossRef]
- Pipino, F. CFP Prosthetic Stem in Mini-Invasive Total Hip Arthroplasty. Journal ofOrthopaedics and Traumatology 2004, 4, 165–171. [Google Scholar] [CrossRef]
- Effenberger, H.; Heiland, A.; Ramsauer, T.; Plitz, W.; Dorn, U. A model for assessing the rotational stability of uncemented femoral implants. Arch Orthop Trauma Surg. 2001, 121, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Wolff, J. Das Gesetz der Transformation der Knochen; Verlag von August Hirschwald: Berlin, Germany, 1892. [Google Scholar]
- Huiskes, R.; Weinans, H.; Van Rietbergen, B. The Relationship between Stress Shielding and Bone Resorption around Total Hip Stems and the Effects of Flexible Materials. Clin. Orthop. Relat. Res. 1992, 274, 124–134. [Google Scholar] [CrossRef]
- Wang, X.; Xu, S.; Zhou, S.; Xu, W.; Leary, M.; Choong, P.; Qian, M.; Brandt, M.; Xie, Y.M. Topological Design and Additive Manufacturing of Porous Metals for Bone Scaffolds and Orthopaedic Implants: A Review. Biomaterials 2016, 83, 127–141. [Google Scholar] [CrossRef] [PubMed]
- Diegel, P.D.; Daniels, A.U.; Dunn, H.K. “Initial effect of collarless stem stiffness on femoral bone strain. ” The Journal of arthroplasty 1989, 4, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Fraldi, M.; Esposito, L.; Perrella, G.; Cutolo, A.; Cowin, S.C. Topological Optimization in Hip Prosthesis Design. Biomech. Model. Mechanobiol. 2010, 9, 389–402. [Google Scholar] [CrossRef]
- Kappe, T.; et al. Minimally Invasive Total Hip Arthroplastytrend or State of the Art?: A Meta-analysis. Ortopade Journal, 2011; Epub ahead of print. [Google Scholar]
- Chen, W.C.; Lai, Y.S.; Cheng, C.K.; Chang, T.K. A cementless, proximally fixed anatomic femoral stem induces high micromotion with nontraumatic femoral avascular necrosis: Afinite element study. J. Orthop. Transl. 2014, 2, 149–156. [Google Scholar] [CrossRef]
- Bergmann, G.; et al. Hip contact forces and gait patterns from routine activities. Journal of Biomechanics 2001, 34, 859–871. [Google Scholar] [CrossRef]
- Naghavi, S.; Tamaddon, M.; Hejazi, M.; Moazen, M.; Liu, C. On the Mechanical Aspect of Additive Manufactured Polyether– Ether–Ketone Scaffold for Repair of Large Bone Defects. Biomater. Transl. 2022, 3, 142–151. [Google Scholar]
- Svesnsson, N.L.; Valliappan, S.; Wood, R.D. Stress analysis of human femur with implanted Charnley prosthesis. Journal of Biomechanics 1977, 10, 581–588. [Google Scholar] [CrossRef]
- Papini, M.; Zdero, R.; Schemitsch, E.H.; Zalzal, P. The Biomechanics of Human Femurs in Axial and Torsional Loading: Comparison of Finite Element Analysis, Human Cadaveric Femurs, and Synthetic Femurs. J. Biomech. Eng. 2007, 129, 12–19. [Google Scholar] [CrossRef]
- Tan, N.; van Arkel, R.J. Topology Optimisation for Compliant Hip Implant Design and Reduced Strain Shielding. Materials 2021, 14, 7184. [Google Scholar] [CrossRef] [PubMed]
- Cortis, G.; Mileti, I.; Nalli, F.; Palermo, E.; Cortese, L. Additive Manufacturing Structural Redesign of Hip Prostheses for Stress–Shielding Reduction and Improved Functionality and Safety. Mech. Mater. 2022, 165, 104173. [Google Scholar] [CrossRef]
- Mehboob, H.; Tarlochan, F.; Mehboob, A.; Chang, S.H.; Ramesh, S.; Harun, W.S.W.; Kadirgama, K. A Novel Design, Analysis and 3D Printing of Ti–6Al–4V Alloy Bio–Inspired Porous Femoral Stem. J. Mater. Sci. Mater. Med. 2020, 31, 104173. [Google Scholar] [CrossRef] [PubMed]
- Kladovasilakis, N.; Tsongas, K.; Tzetzis, D. Finite Element Analysis of Orthopedic Hip Implant with Functionally Graded Bioinspired Lattice Structures. Biomimetics 2020, 5, 44. [Google Scholar] [CrossRef]
- Engh, C.A.; Bobyn, J.D.; Glassman, A.H. Porous-coated hip replacement. The factors governing bone ingrowth, stress shielding, and clinical results. J Bone Joint Surg Br 1987, 69, 45. [Google Scholar] [CrossRef]
- Gross, S.; Abel, E.W. A finite element analysis of hollow stemmed hip prostheses as a means of reducing stress shielding of the femur. J Biomech. 2001, 34, 995–1003. [Google Scholar] [CrossRef]
- Effenberger, H.; Heiland, A.; Ramsauer, T.; Plitz, W.; Dorn, U. A model for assessing the rotational stability of uncemented femoral implants. Arch Orthop Trauma Surg. 2001, 121, 60–64. [Google Scholar] [CrossRef]
- Nunn, D.; Freeman, M.A.R.; Tanner, K.E.; Bonfield, W. Torsional stability of the femoral component of hip arthroplasty. Response to an anteriorly applied load. J Bone Joint Surg Br 1989, 71, 452–455. [Google Scholar] [CrossRef]
- Freeman, M.A.R. Why resect the neck? J Bone Joint Surg Br 1986, 68, 346–349. [Google Scholar] [CrossRef]
- Sugiyama, H.; Whiteside, L.A.; Engh, C.A. Torsional fixation of the femoral component in total hip arthroplasty. The effect of surgical press-fit technique. Clin Orthop 1992, 275, 187–193. [Google Scholar] [CrossRef]
- Hanada, S.; Masahashi, N.; Jung, T.K.; Yamada, N.; Yamako, G.; Itoi, E. Fabrication of a High–Performance Hip Prosthetic Stem Using Ti–33.6Nb–4Sn. J. Mech. Behav. Biomed. Mater. 2014, 30, 140–149. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Wang, L.; Kang, J.; Li, D.; Jin, Z. Biomechanical Optimization of Elastic Modulus Distribution in Porous Femoral Stem for Artificial Hip Joints. J. Bionic Eng. 2018, 15, 693–702. [Google Scholar] [CrossRef]
- Cortis, G.; Mileti, I.; Nalli, F.; Palermo, E.; Cortese, L. Additive Manufacturing Structural Redesign of Hip Prostheses for Stress–Shielding Reduction and Improved Functionality and Safety. Mech. Mater. 2022, 165, 104173. [Google Scholar] [CrossRef]
- Mehboob, H.; Tarlochan, F.; Mehboob, A.; Chang, S.H.; Ramesh, S.; Harun, W.S.W.; Kadirgama, K. A Novel Design, Analysis and 3D Printing of Ti–6Al–4V Alloy Bio–Inspired Porous Femoral Stem. J. Mater. Sci. Mater. Med. 2020, 31, 104173. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) curvature of the femur in frontal and sagittal view, (b) right stem, (c) curved stem.
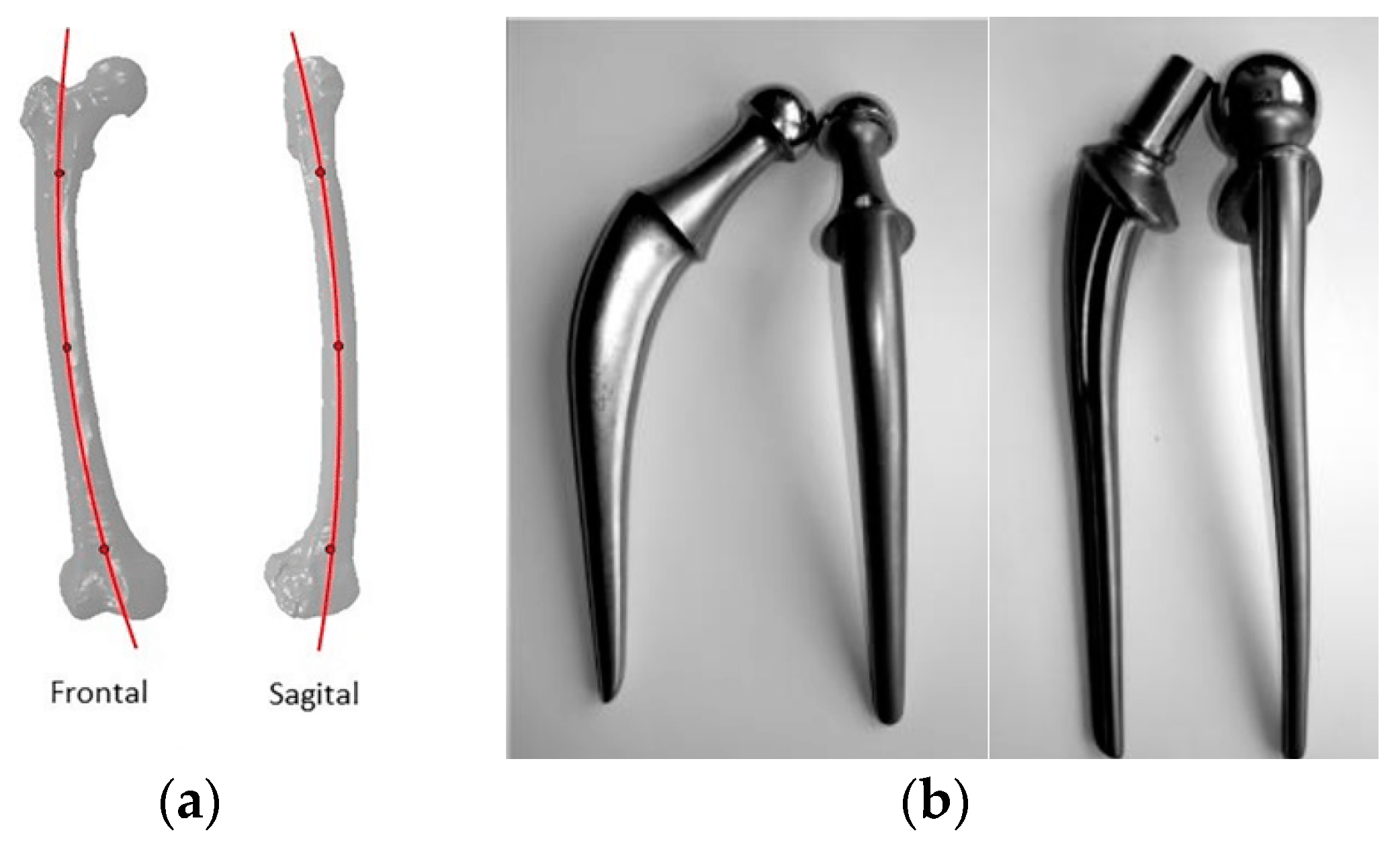
Figure 2.
Direction of application loads and moments.
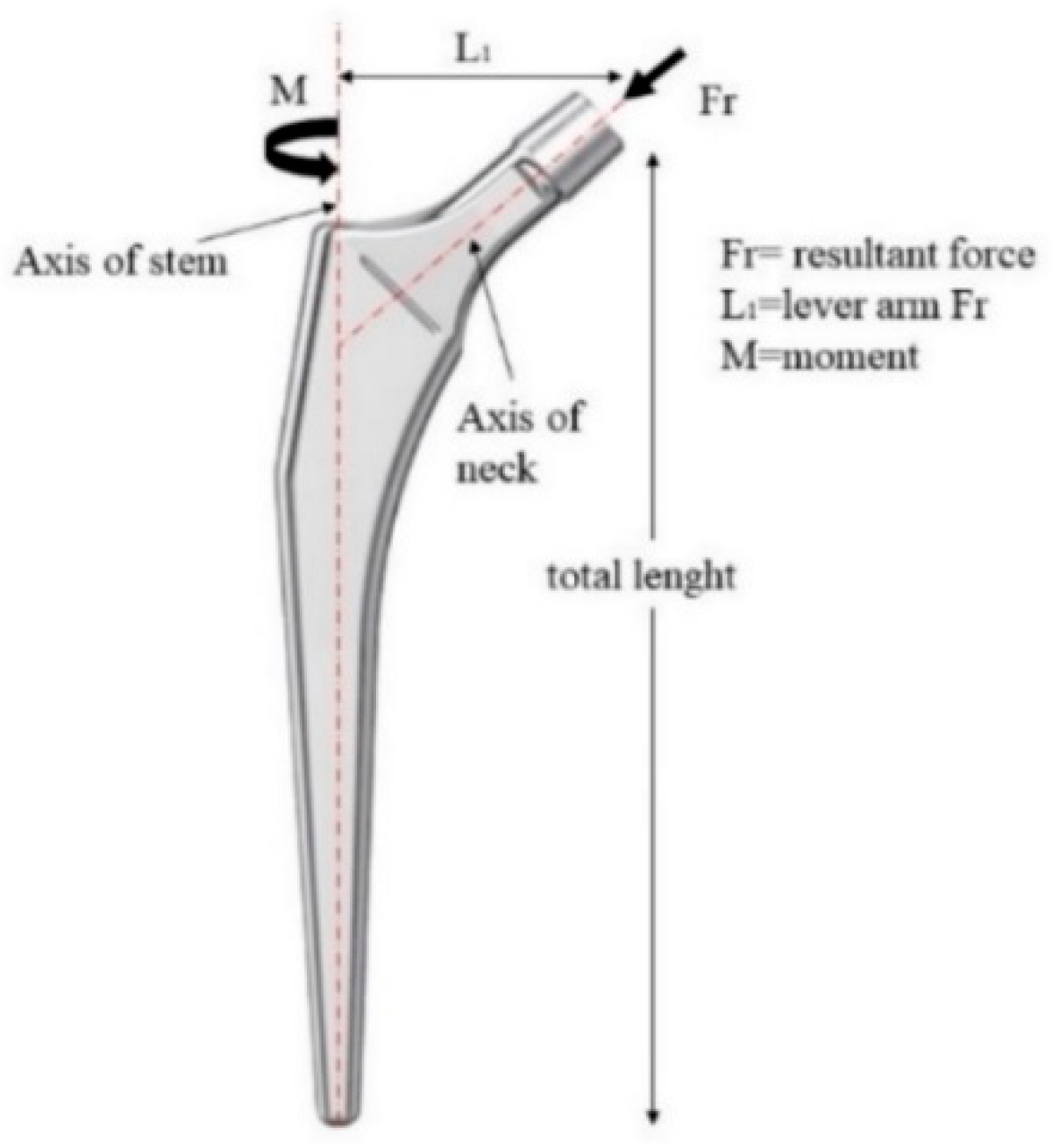
Figure 3.
(a) sheet with horizontal grooves, (b) stem with ridges.
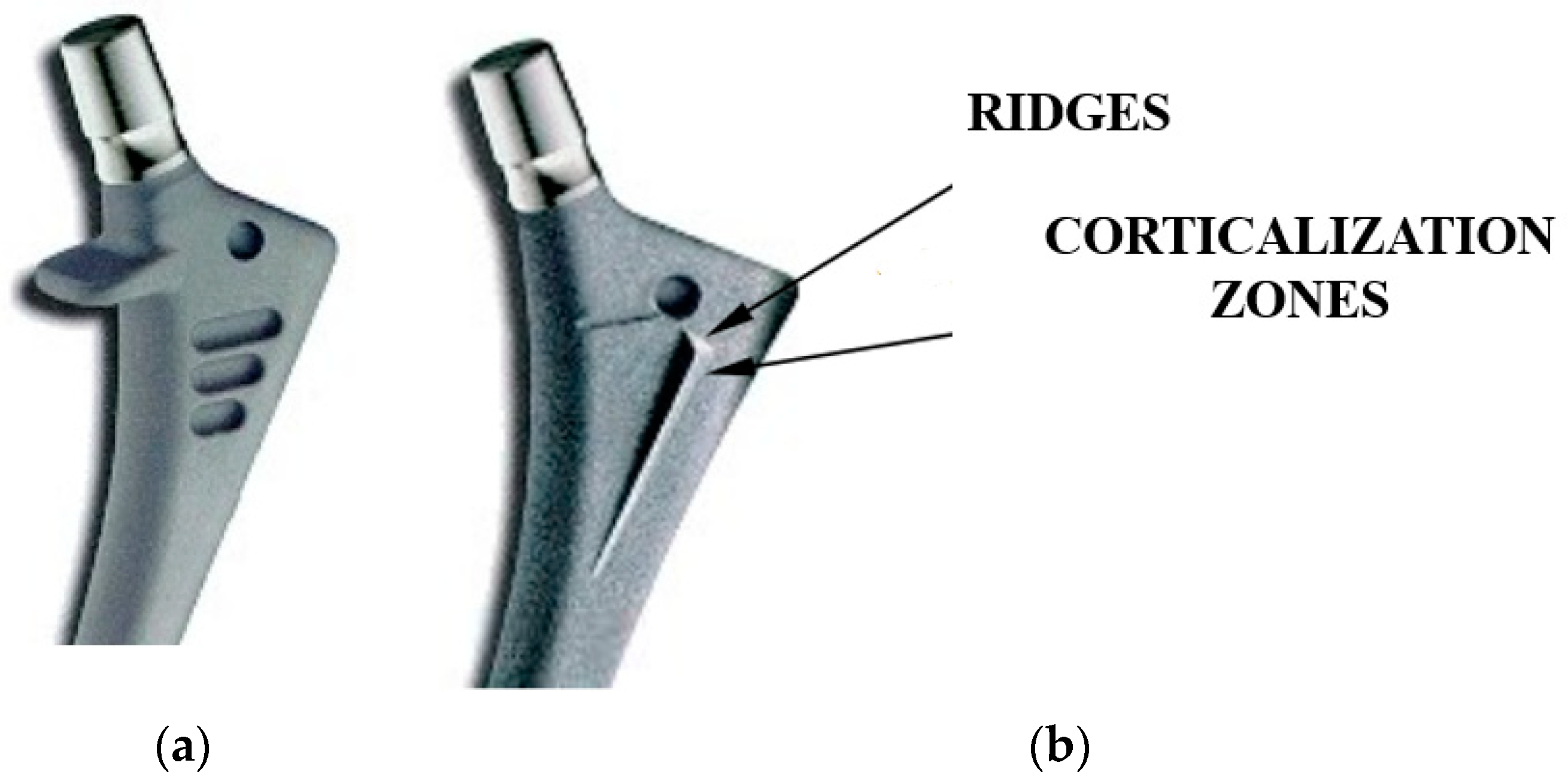
Figure 4.
Torsional moment (M) produced by the introduced force (F 2) and the active lever arm (L2).
Figure 4.
Torsional moment (M) produced by the introduced force (F 2) and the active lever arm (L2).
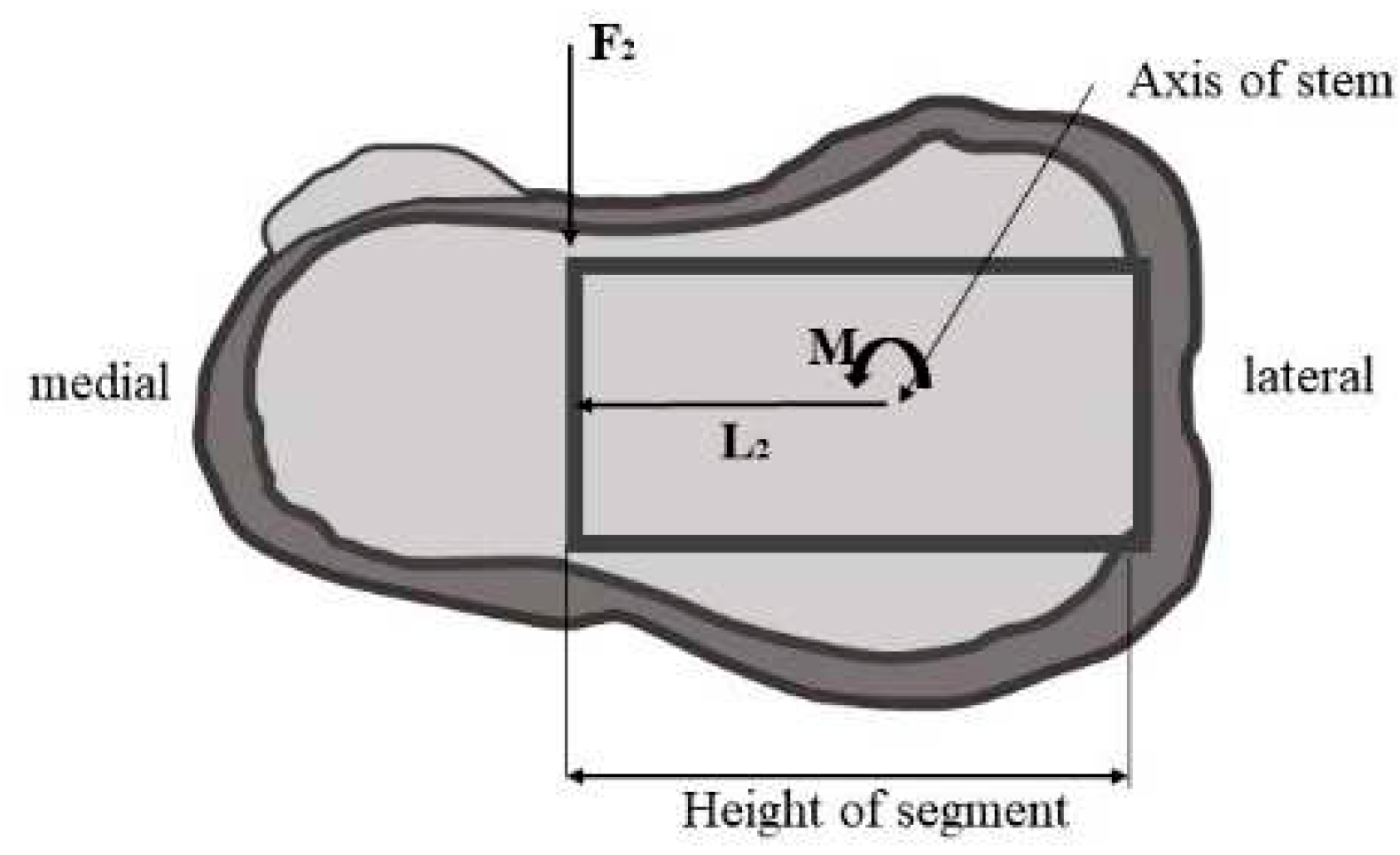
Figure 5.
Lever arm configuration.
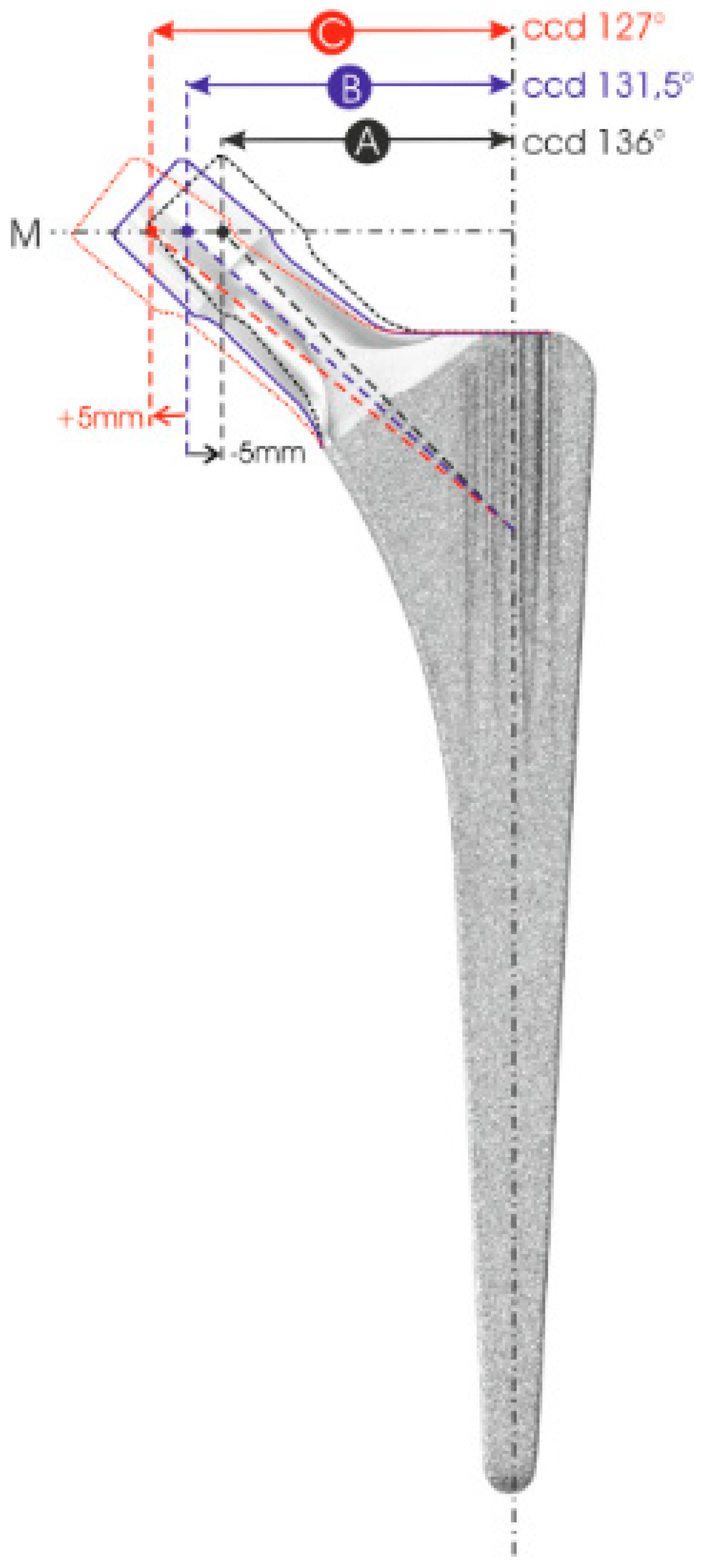
Figure 6.
Simple scheme of stress shielding [36].
Figure 6.
Simple scheme of stress shielding [36].
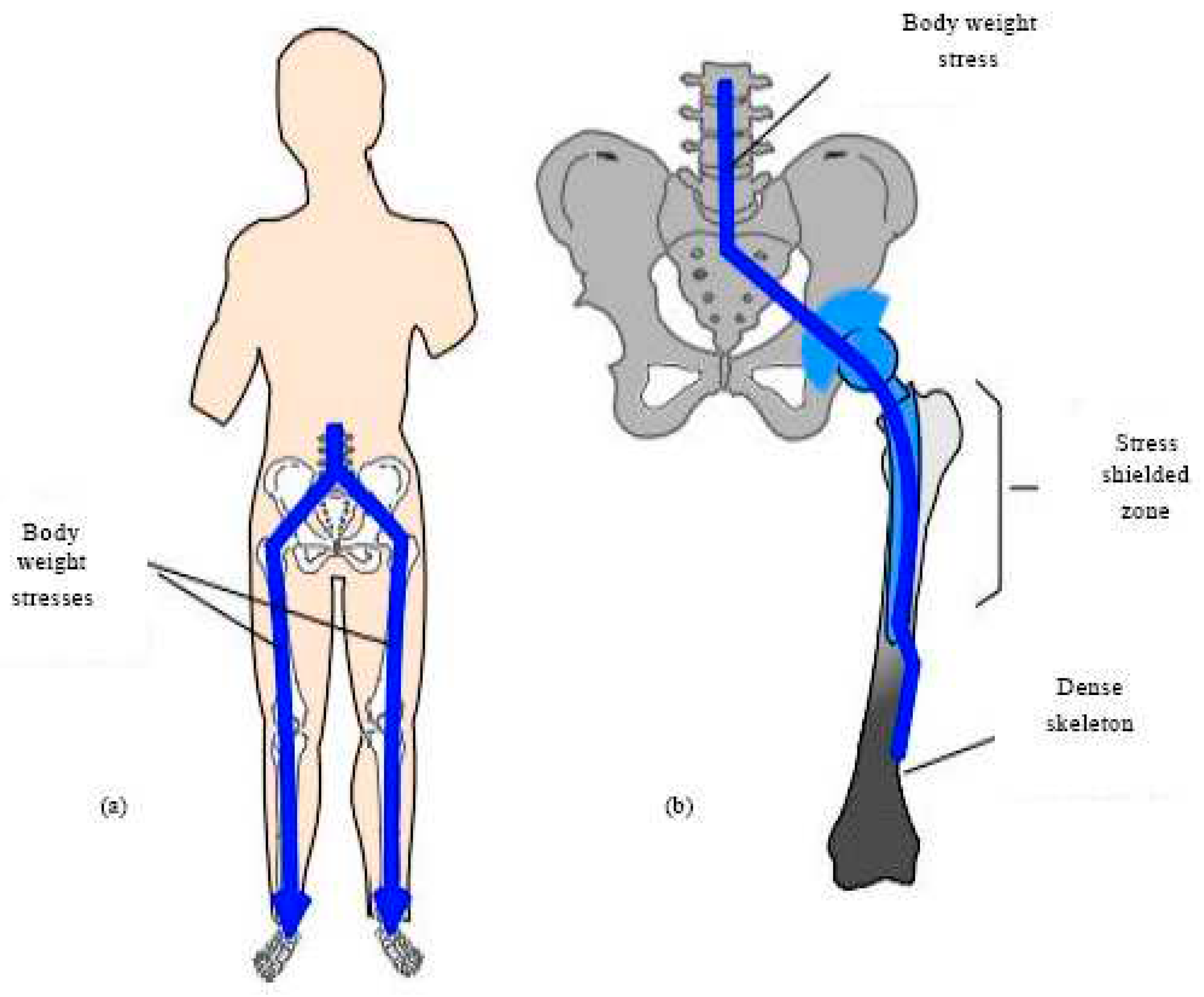
Figure 7.
On the left a traditional full-stem prosthesis with rectangular section, on the right prosthesis with minimization in the proximal area having holes, ridges and slots to improve rotation stability.
Figure 7.
On the left a traditional full-stem prosthesis with rectangular section, on the right prosthesis with minimization in the proximal area having holes, ridges and slots to improve rotation stability.
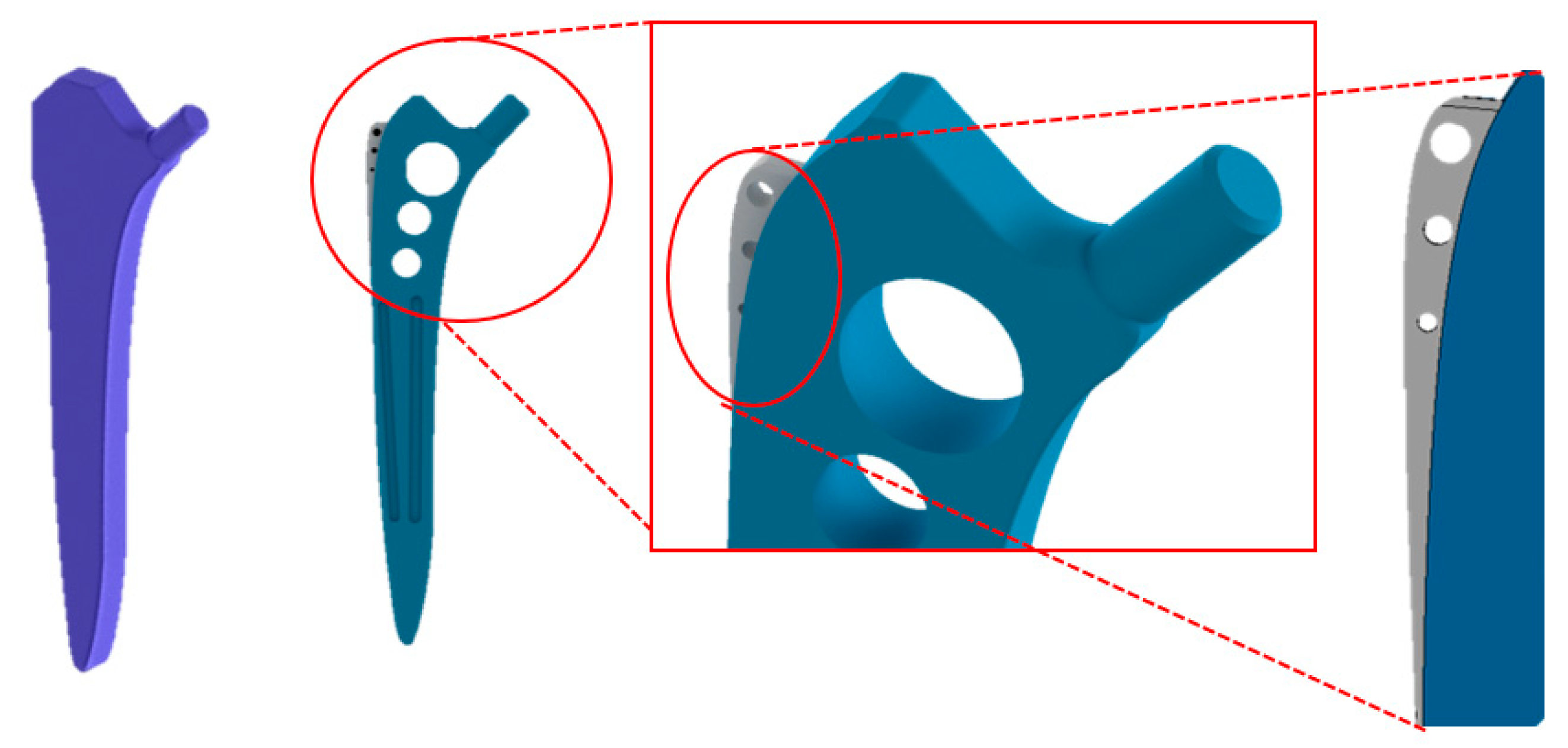
Figure 8.
FEM model of ISO 7206-4 test (a) standard stem, (b) optimized stem.
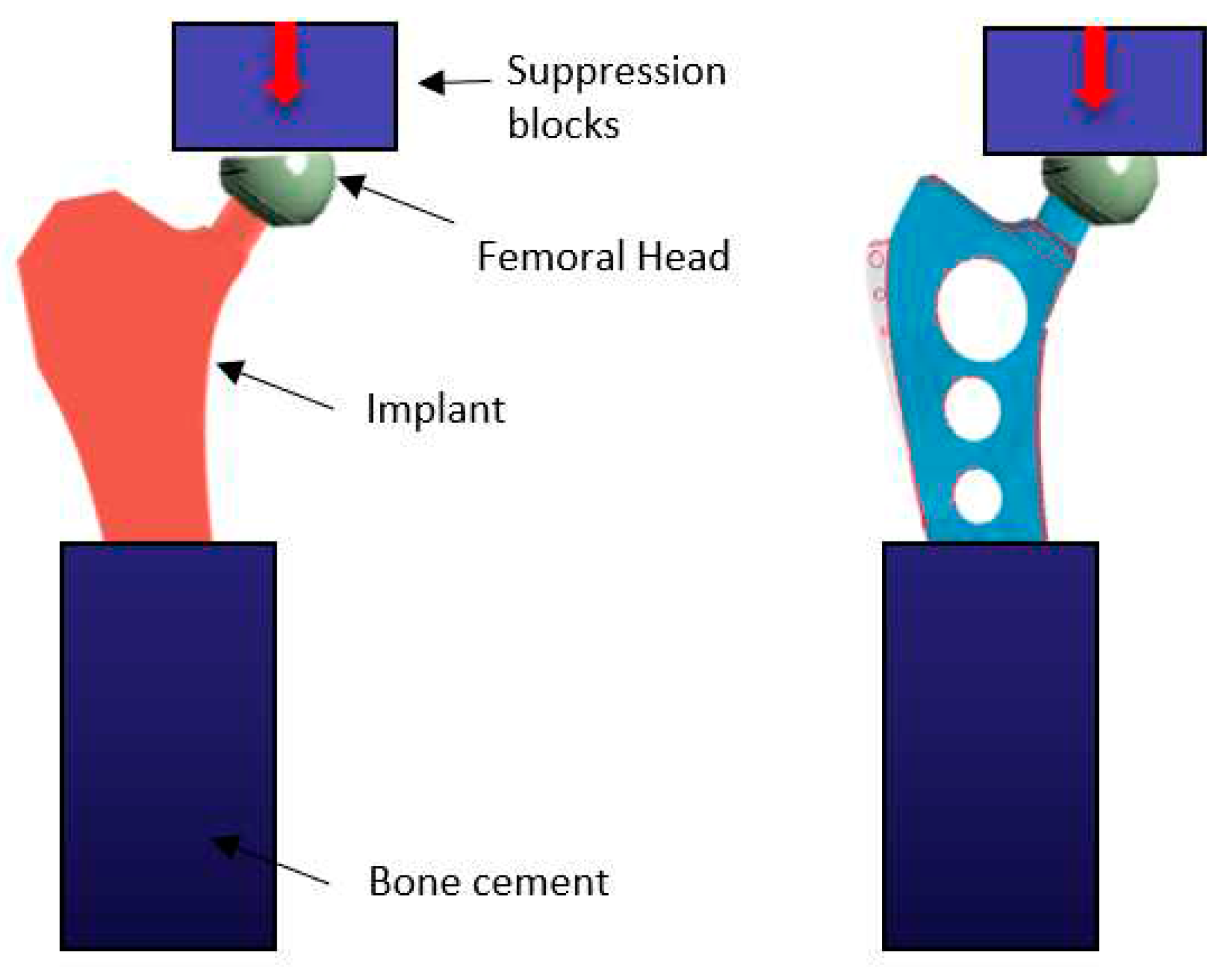
Figure 9.
Representative model of the stem inserted into the femur; cortical thickness considered 3 mm.
Figure 9.
Representative model of the stem inserted into the femur; cortical thickness considered 3 mm.
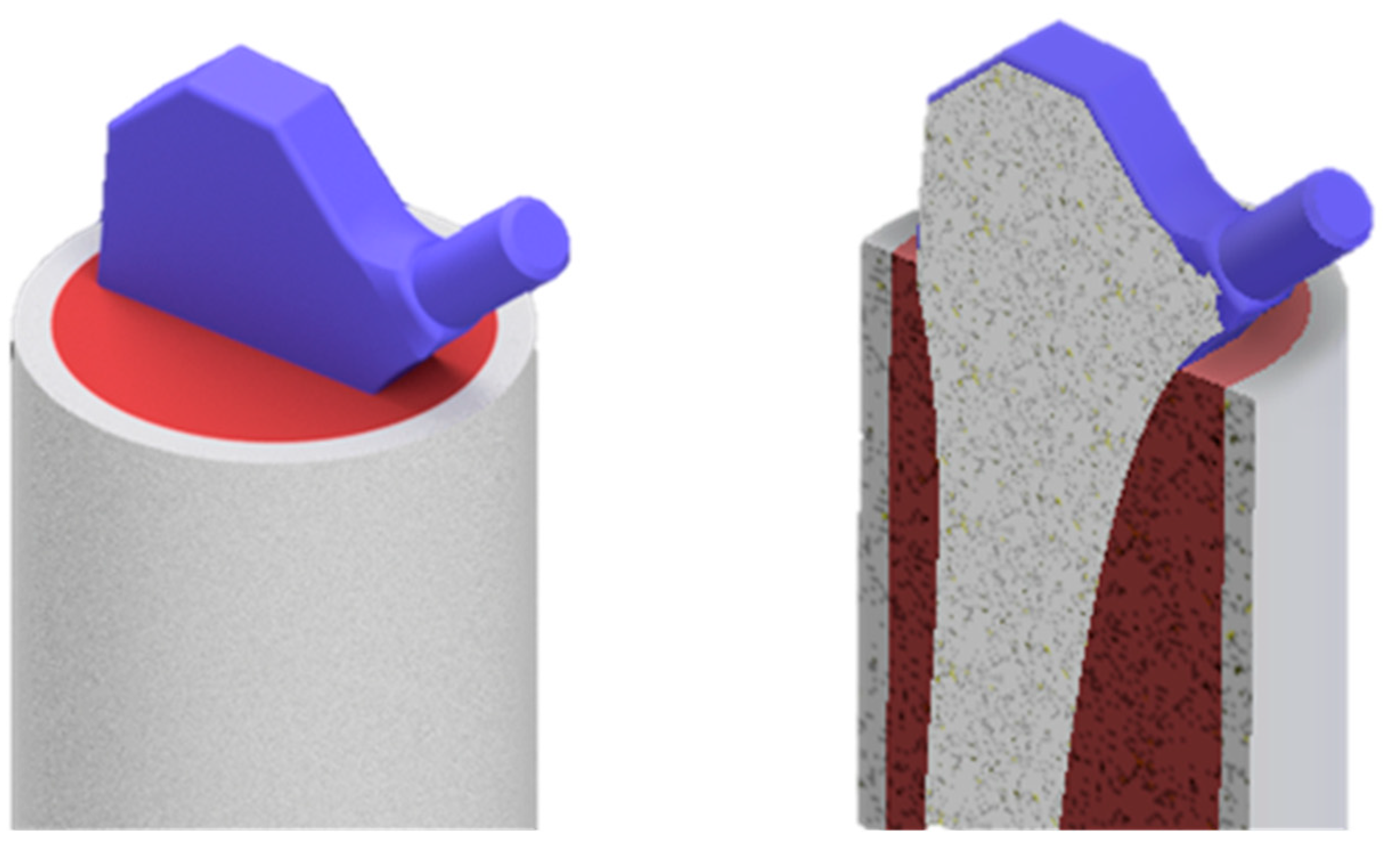
Figure 10.
The direction and application of loads and time for the numerical model studied. [39].
Figure 10.
The direction and application of loads and time for the numerical model studied. [39].
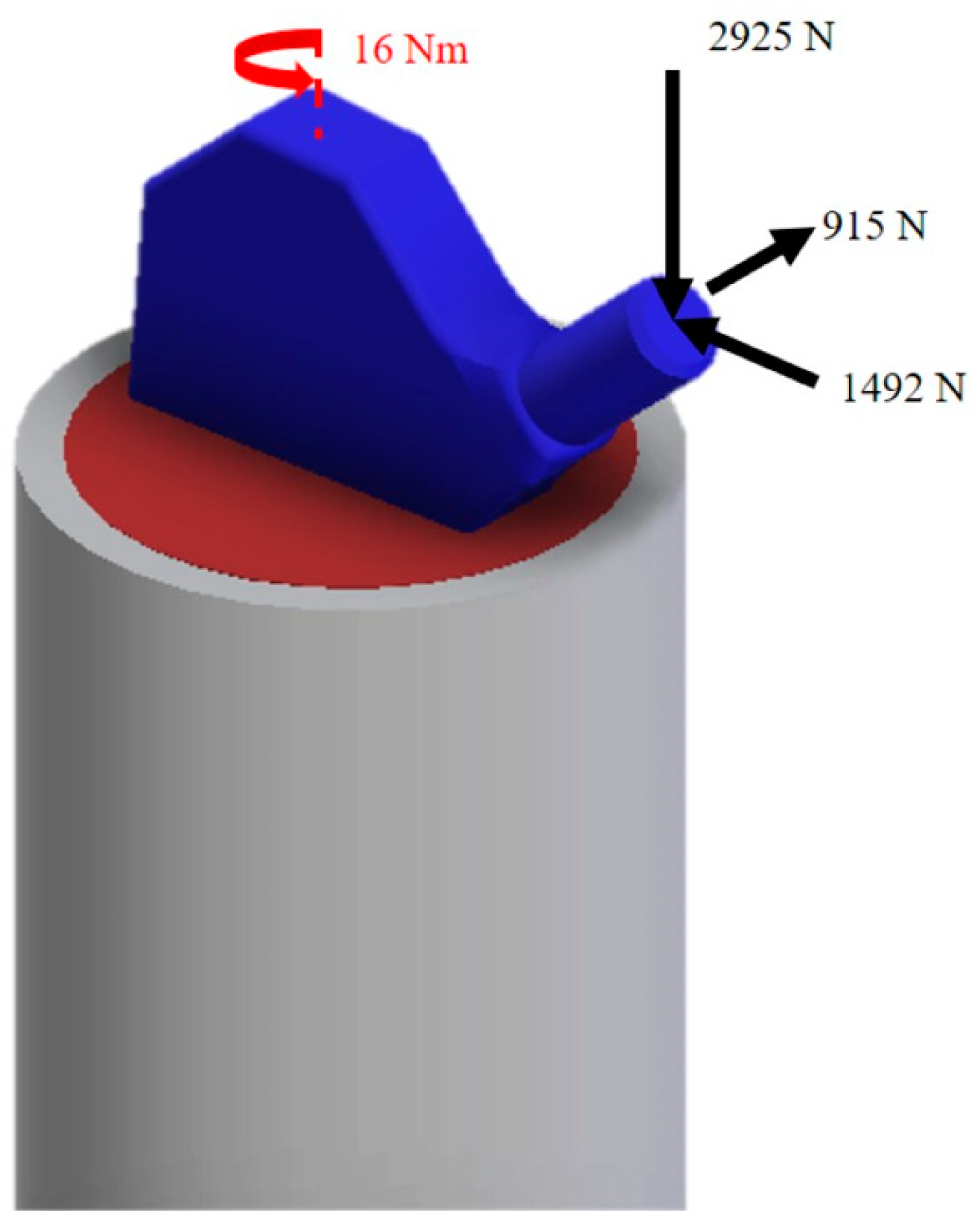
Figure 11.
Mesh characteristics used for the stem size=2,4mm for the bone size=2 mm.
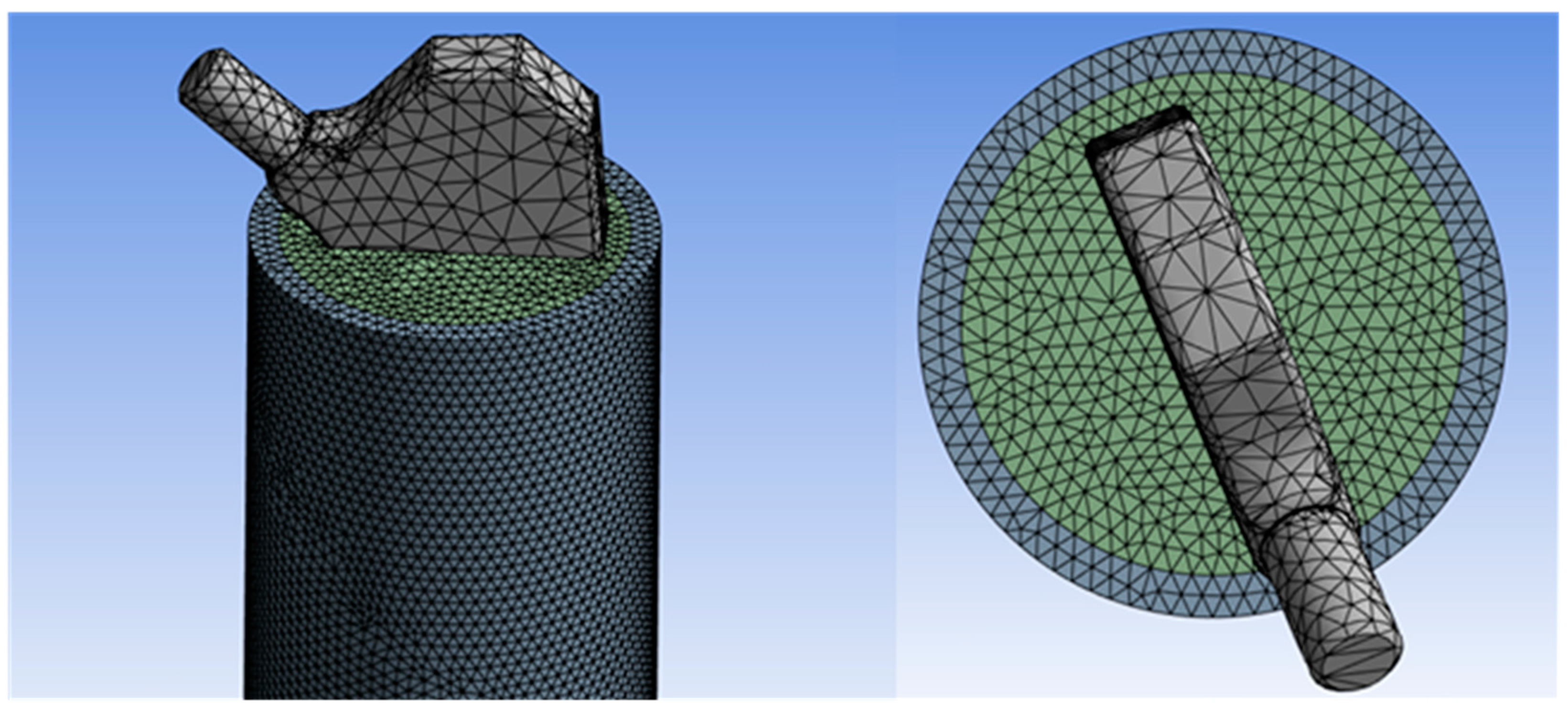
Figure 12.
Mesh convergence analysis between element dimension and Von Mises stress.
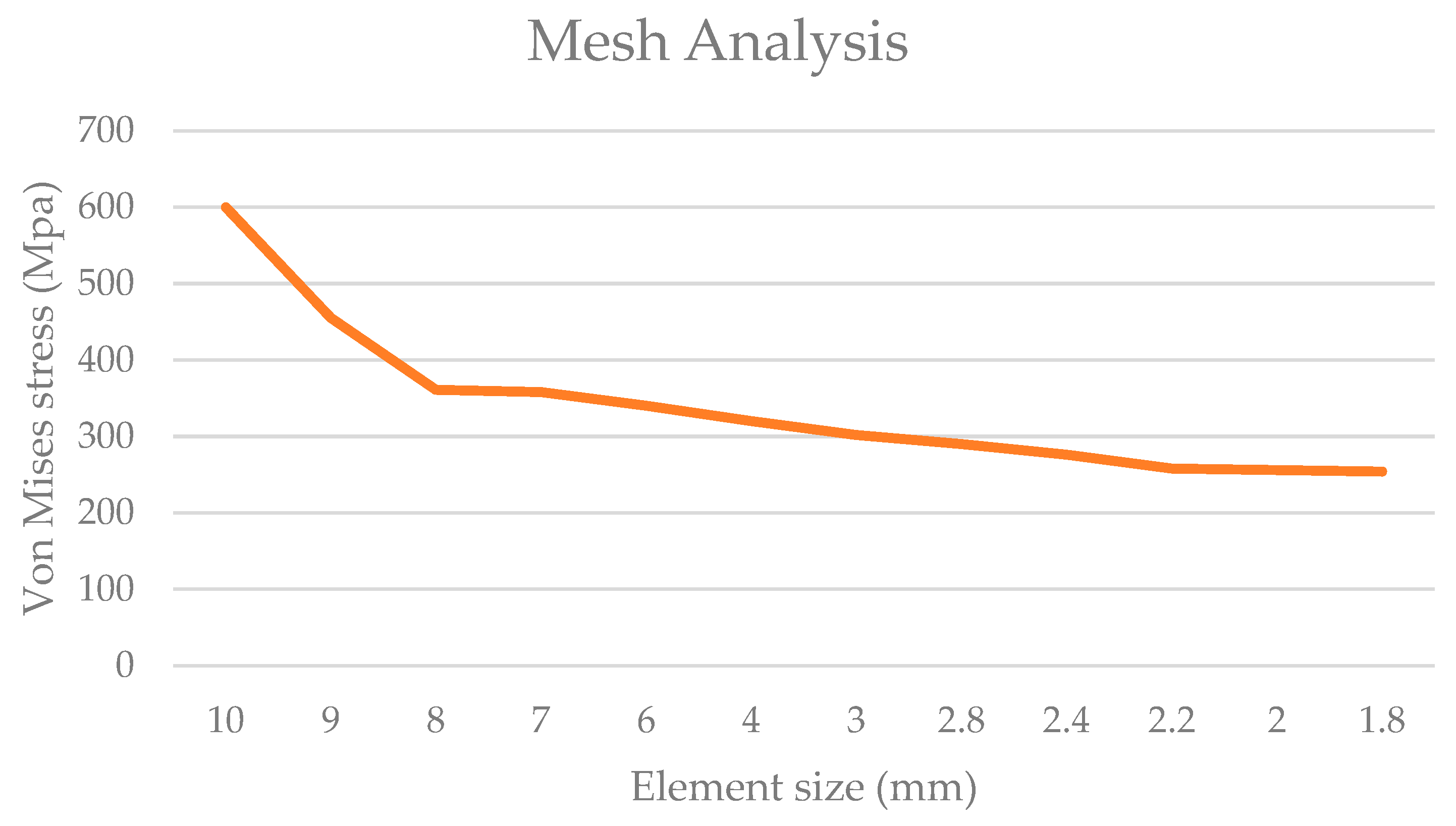
Figure 13.
Load-displacement graph for Ti6Al4V stem, optimized stem and intact femur. The stiffness value of each configuration is presented above the respective slopes on the diagram.
Figure 13.
Load-displacement graph for Ti6Al4V stem, optimized stem and intact femur. The stiffness value of each configuration is presented above the respective slopes on the diagram.
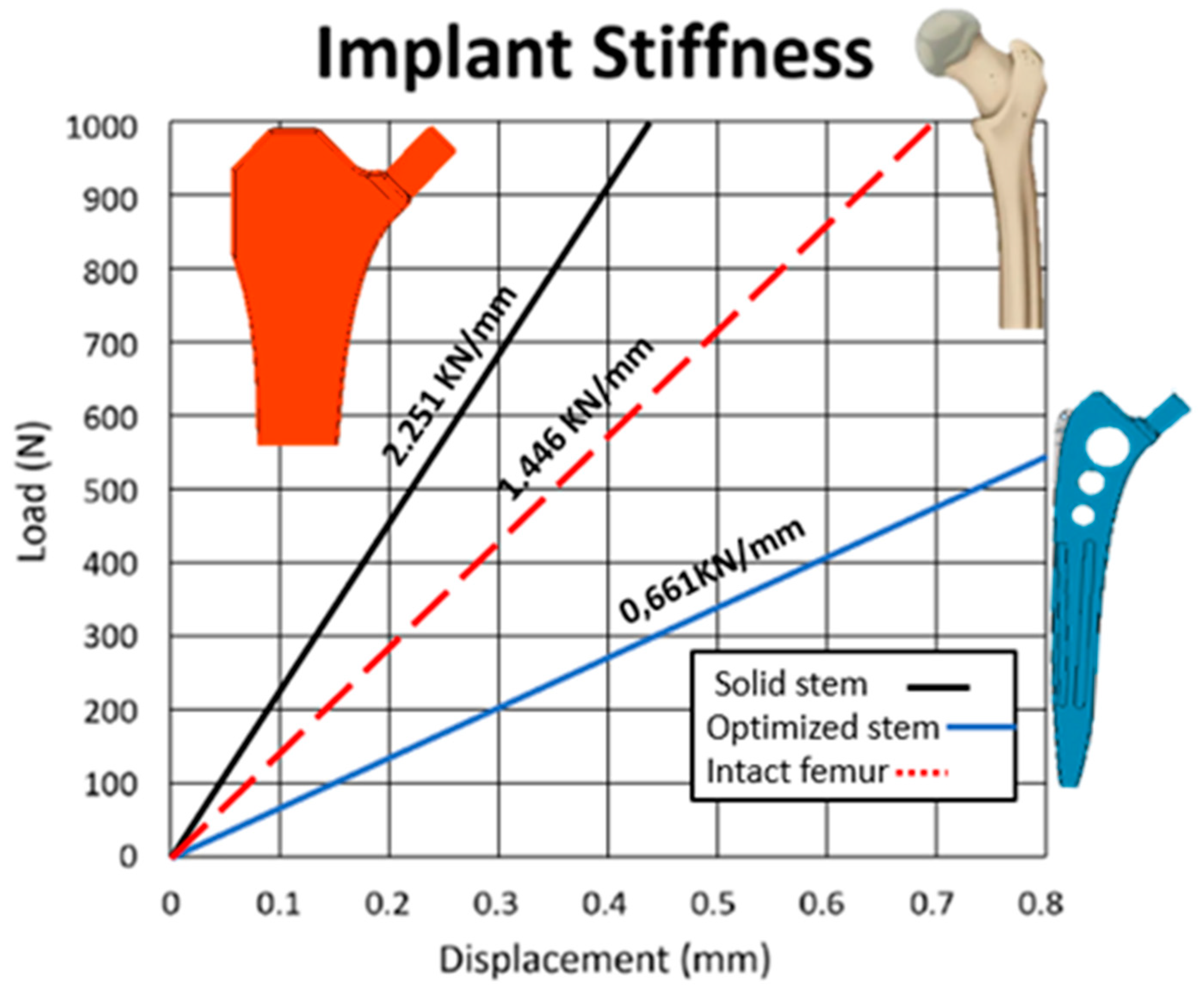
Figure 14.
Von Mises stress distribution on bone (a) traditional stem (b) optimized stem (c) intact bone [35].
Figure 14.
Von Mises stress distribution on bone (a) traditional stem (b) optimized stem (c) intact bone [35].
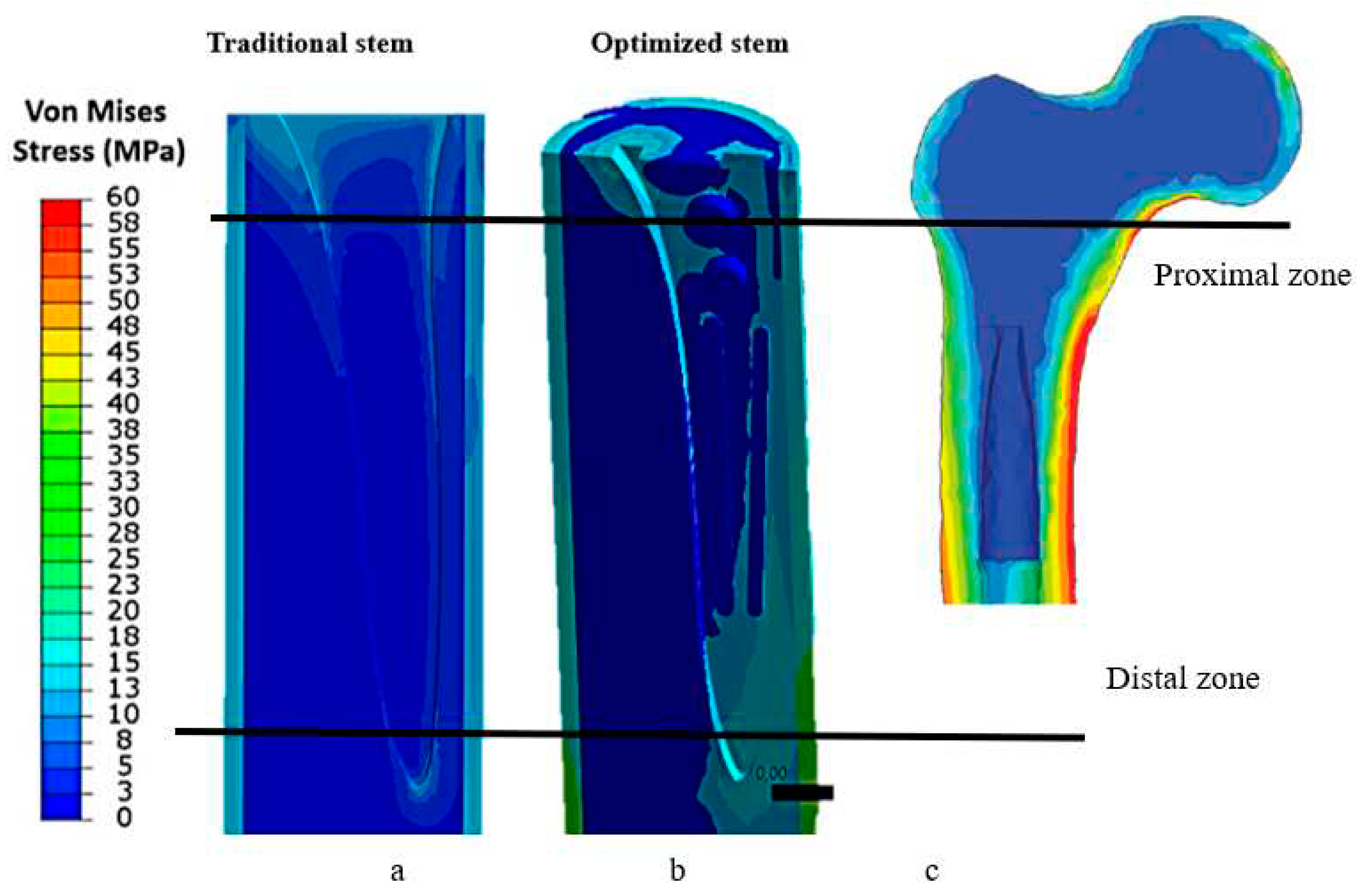
Figure 15.
Von-Mises stress for stems.
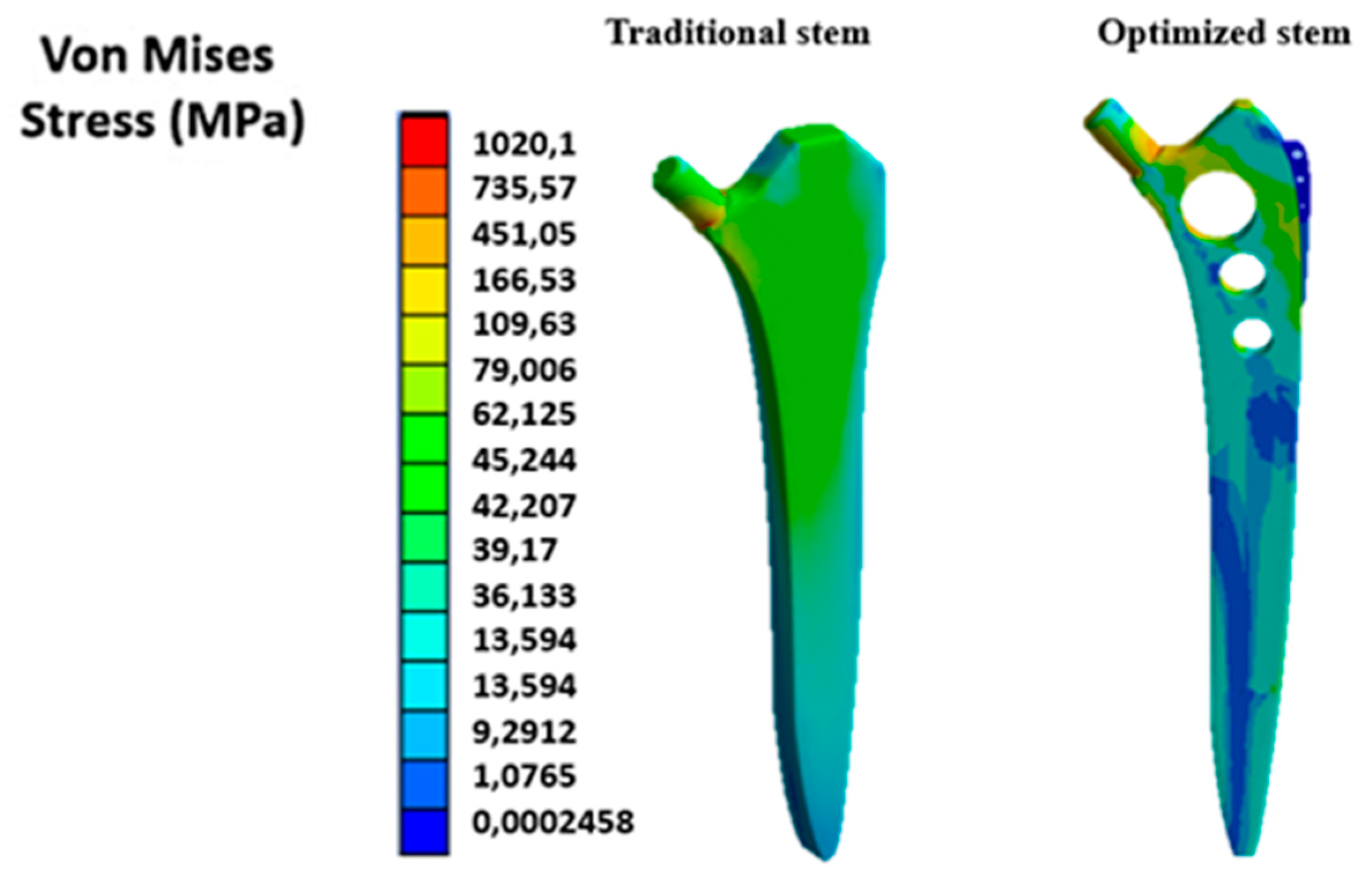
Figure 16.
Trend of Von Mises stresses in the bone.
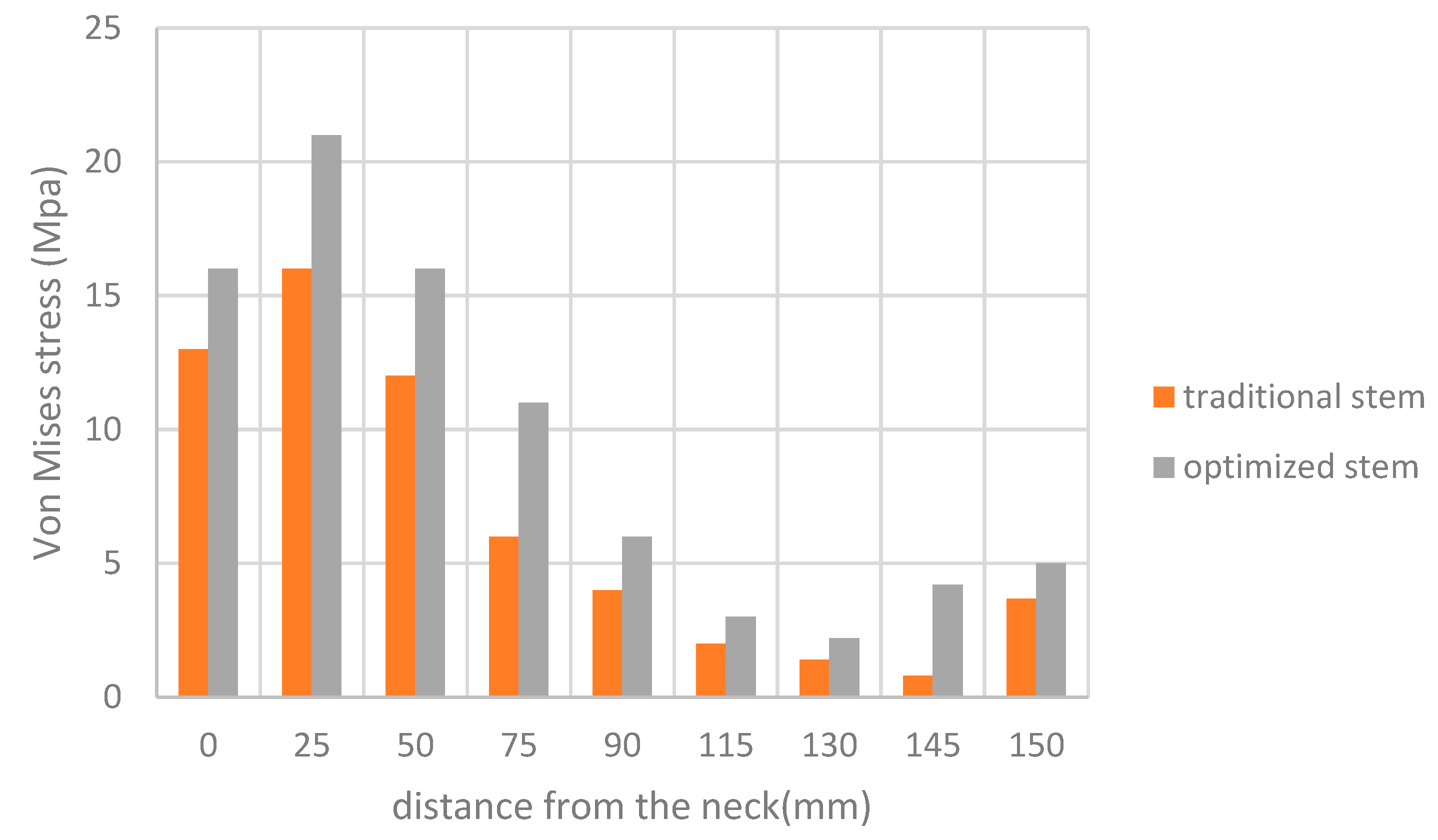
Figure 17.
Equivalent deformation of the implant.
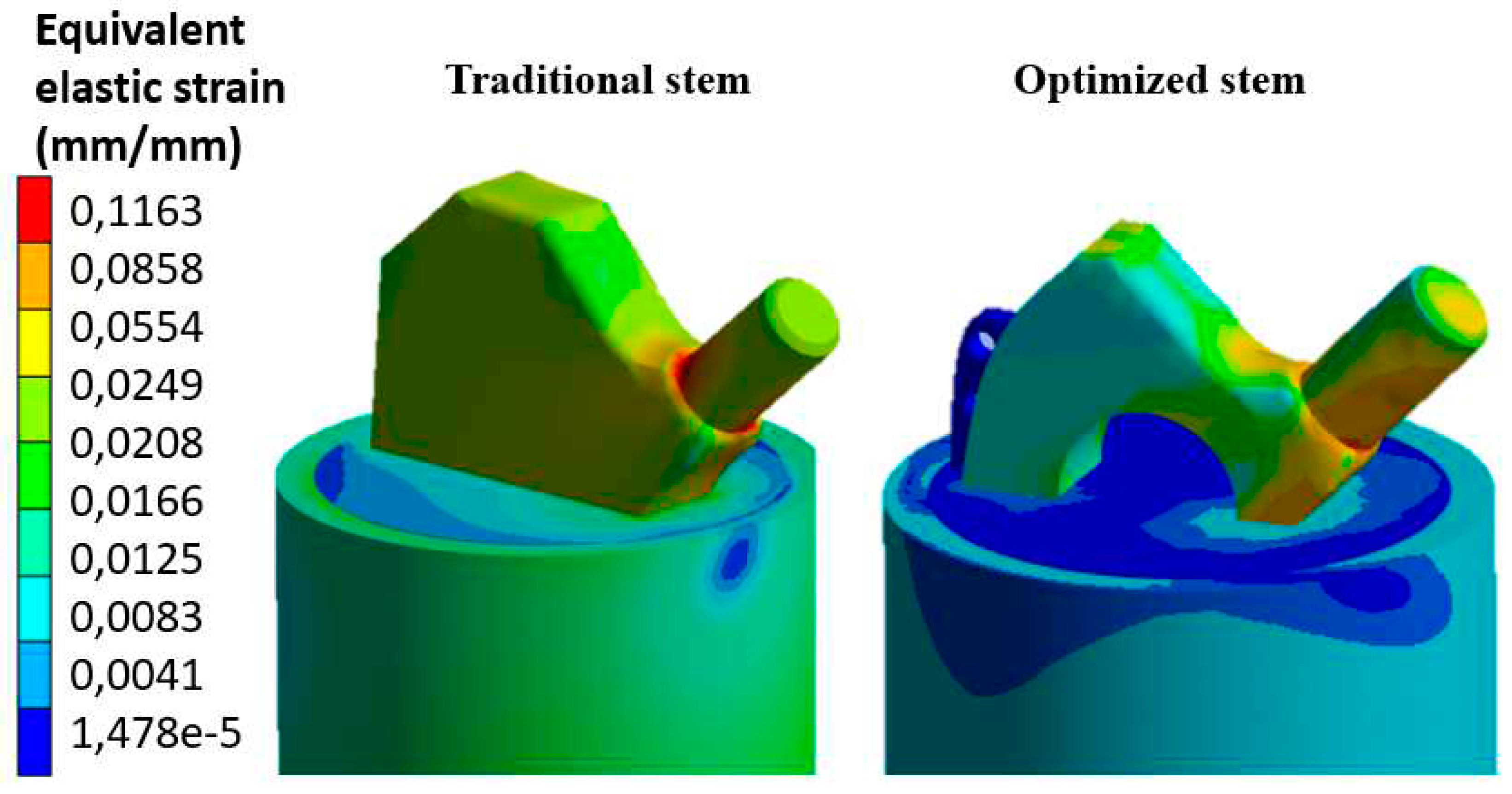
Figure 18.
Relative relationships between stress-shielding and stress of the proximal interface with stem stiffness. This chart clearly illustrates the main design conflict.
Figure 18.
Relative relationships between stress-shielding and stress of the proximal interface with stem stiffness. This chart clearly illustrates the main design conflict.
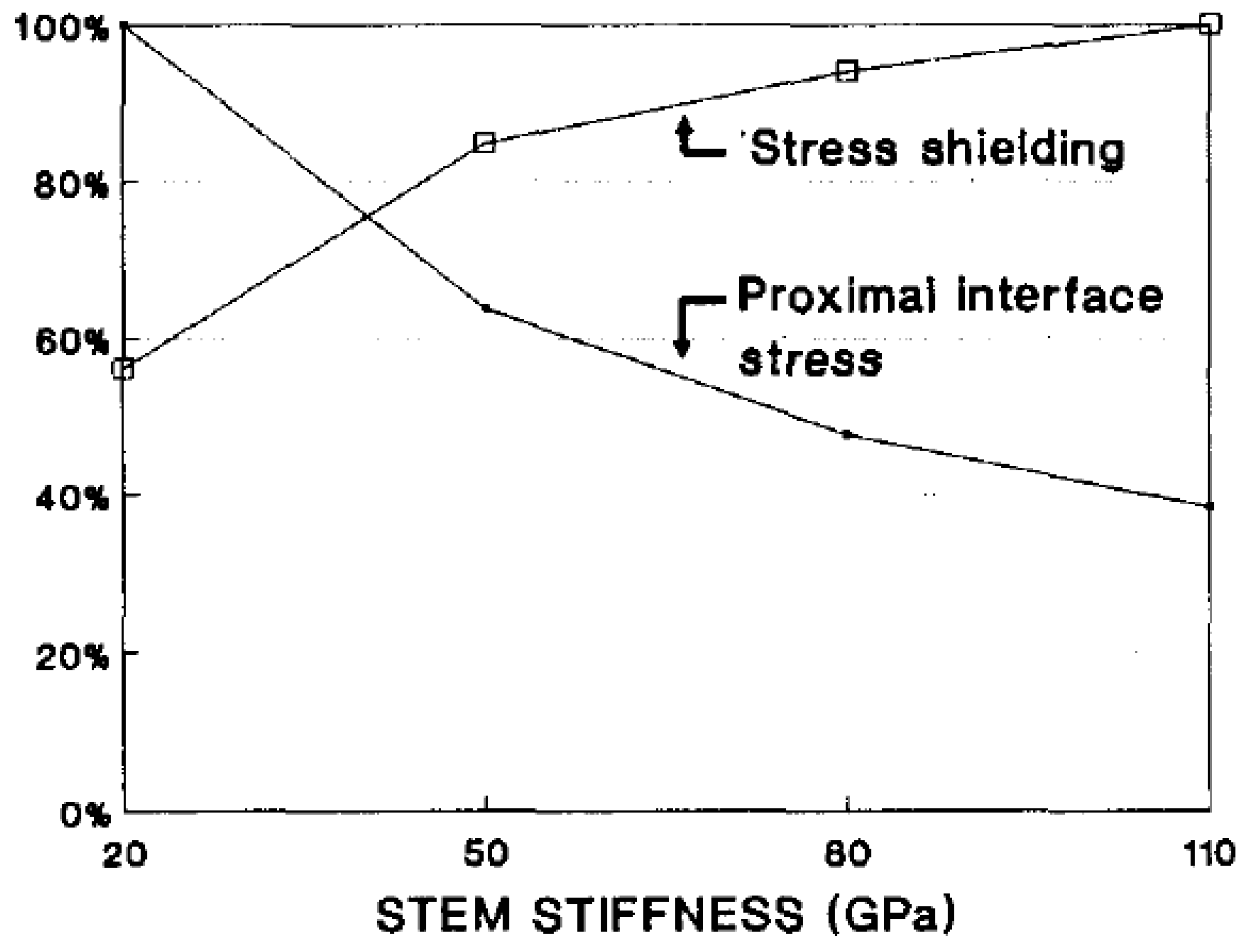

Table 1.
Mechanical properties of various materials.
| Material | Modulus of Elasticity | Shear modulus (Gpa) | Poisson’s ratio | Compressive Strength (Mpa) | Yield strength (Mpa) | Density g/cm3 |
|---|---|---|---|---|---|---|
| Cortical bone | Ex=6979 (Mpa) Ey=18132 (Mpa) Ez=6979 (Mpa) |
Gyz=5.6 Gzx=4.5 Gxy=6.2 |
195 | 2.02 | ||
| Cancellous bone | Ex=660 (Mpa) Ey=1740 (Mpa) Ez=660 (Mpa) |
Gyz=0.211 Gzx=0.165 Gxy=0.260 |
16 | 1.37 | ||
| Ti6Al4V | 110 (GPa) | 0.3 | 970 | 930 | 4.42 |
|
| Steel (suppression blocks) | 210 (Gpa) | 0.3 | ||||
| Bone cement | 3.8 (Gpa) | 0.3 | ||||
| Cr-Co (femoral head) | 200 (Gpa) | 0.33 |
Table 2.
Reduction of stress-shielding for the three zones: prosimal, central, distal.
| Von Mises stress bone with traditional stem | Von Mises bone stress with optimized stem | Stress-shielding reduction% | |
|---|---|---|---|
| Traditional stem | optimized stem | ||
| Proximal 13 Mpa | Proximal 17 Mpa | 24.08% | 31.46% |
| Central 3.1 Mpa | Central 4.2 Mpa | 5.54% | 7.5% |
| Distal 4.6 Mpa | Distal 5 Mpa | 9.59% | 10.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



