
Submitted:
11 July 2023
Posted:
12 July 2023
You are already at the latest version
Abstract
Background: PFO (Patent foramen ovale) is a common defect that affects about 25% of the population. Although its presence is asymptomatic in the majority of the cases, the remaining part becomes overt with different symptoms, including cryptogenic stroke. The PFO closure procedure is widely available to date with the most used Amplatzer PFO Occluder, also in complex anatomy, but the performance of another device, the GORE Septal Occluder (GSO), has not been completely explored with regard to different septal anatomies.
Methods: From March 2012 to June 2020, 118 consecutive patients with an indication for PFO closure were treated using the GSO system and included in a prospective analysis and followed. After 12 months, every patient underwent transcranial Doppler to evaluate the effectiveness of treatment.
Results: of 111 patients evaluated, 107 showed effective PFO closure (96,4%) and 4 showed a residual shunt (3,6%). To better evaluate the device performance, the overall population was sorted into 2 clusters based on the echocardiographic characteristics. The main difference between groups was for PFO width (4,85 ± 1,8 vs 2,9 ± 1 mm, p <0,001) and PFO tunnel length (12,6 ± 3,8 vs 7,2 ± 2 respectively, p <0,001), allowing identification of complex anatomy and simple anatomy, respectively. Regardless of the aforementioned cluster, the GSO performance to reach an effective closure was independent of anatomy type and the chosen device size.
Conclusion: GSO device showed efficacy and safety at 1-year follow-up in patients with at least 1 anatomical factor of complexity of PFO, irrespectively from the level of complexity itself.
Keywords:
patent foramen ovale
; complex PFO anatomy
; GSO
; long-term residual shunt
1. Introduction
Patent foramen ovale (PFO) is involved in several types of disease and pathological situations and the initial enthusiasm and wide spreading of closure procedures and device has been replaced by cautions in the last years due to the increasing evidence about long-term complication[1,2,3].
Currently, the procedure of PFO closure should be performed after multidisciplinary evaluation taking into account carefully the balance between risk and benefit. Furthermore, an accurate imaging evaluation of septal anatomy is pivotal because of the fact that several factors have been demonstrated to be associated with a higher risk of relapsing ischemic events and a higher risk of complications[4].
Several devices for percutaneous PFO closure have been developed and the optimal prosthesis should be that one provides: i) effective PFO closure; ii) simplicity in the procedure for implant; ii) suitability for every anatomical situation and complexity of septum; iii) low interference with other intracardiac structures; iv) possibility to be removed if required; v) low incidence of complications. Each of the available devices fits only one or more of these characteristics and therefore the choice of device should depend on the experience of the center and on the simple manufacturer’s characteristics. Currently, the most broadly used prosthesis is the Amplatzer Occluder (Abbott Vascular); this prosthesis has demonstrated its benefit in clinical randomized studies and is easy to be implanted; however, it’s almost rigid structure raised some concerns about device erosion and interference with venous surrounding structures and valvular function[1,2,3].
To overcome this issue, Gore Helex occluder (Gore Medical, Flagstaff - Arizona) was developed as a single-wire nitinol structure covered with polytetrafluoroethylene (ePTFE) that provides greater conformability and good apposition to septal structures[3]. After initial complications[5,6], consistent modification in the delivery system and technical characteristics were done and the second generation Gore septal occluder (GSO; Gore Medical) replaced the first. Full details of the device have been described elsewhere[7]. With its low device profile and a relatively simple procedure, GSO showed its efficacy and safety in the first clinical series[7,8] and confirmed them in a larger randomized trial[9].
Despite this huge experience, no precise demonstration of its performance in real life, in different anatomical settings of interatrial septum has been published till now in order to assess the advantages of Gore better. The present study aims to present a prospective single-center experience with GSO for PFO closure and to define which anatomical characteristics of the included population are related to anatomical and clinical results at mid-term follow-up.
2. Materials and Methods
2.1. Patient Population and Imaging
Between March 2012 and June 2020, all consecutive patients with an indication for PFO closure treated using the GSO system in a single Italian center were included in a prospective analysis and followed. They were treated at the department of cardiology, whereas the diagnosis of cryptogenic stroke or transient ischemic attack (TIA) was performed either by the department of neurology or the referring cardiologist or neurologist. Neuroradiologic imaging (computer tomography, CT, or magnetic resonance imaging CMR) was performed according to specific indications (suspected cerebrovascular events).
Indication for PFO closure was posed after collegial discussion and according to most recent guidelines[4], therefore mainly accounting for the occurrence of one or more documented cerebral thromboembolic event related to paradoxical embolism on top of antithrombotic regimens. Before the procedure, all other embolism sources or prothrombotic factors were excluded (atrial fibrillation, pulmonary shunts, coagulation defects, active cancer, or orthopedic surgery history <3 months).
2.2. Procedural Details
The PFO closure procedure was performed with fluoroscopic guidance, under local anesthesia and slight sedation, through a femoral vein access with a Multipurpose 5F catheter (Cordis, Hialeah, Florida) and 0.035” J-tip wire to cross the defect. The imaging was done with intracardiac echocardiography (ICE) through contralateral femoral vein access with 8F sheath (8 MHz ACUNAV ultrasound catheter – Biosense Webster, Johnson & Johnson, CA). After crossing the defect, a stiff wire was positioned in the left superior pulmonary vein to advance a 14F sheath and the delivery system. The occluder device size was chosen according to the echocardiographic findings. As fully described elsewhere[7], the GSO is available in disc diameters from 20-30 mm (in 5 mm increments); it is preassembled and loaded into a delivery catheter that is inserted and advanced into the left atrium along the stiff guidewire using the preformed monorail port. Expansion of the left and then right atrial discs of the device was performed under fluoroscopy and echocardiography; then the device detaches from the delivery mandril, removing tension from the system and allowing the reach of the final positioning with the correct orientation on the atrial septum. The device is retrievable at any stage during the delivery until it is locked to the mandril. After septal crossing, a single unfractionated heparin (UFH) bolus ranging from 5000 to 7500 UI was routinely administered. In the perioperative period, all patients received antibiotic prophylaxis (cefazolin 2 g); moreover, a double antiplatelet therapy with Acetylsalicylic Acid 100 mg/daily and Clopidogrel 75 mg/daily was started on the day of the procedure, with a loading dose if the drug was not already taken by the patient. The double antiplatelets therapy (DAPT) regimen was maintained until 6 months after the procedure, then one antiplatelet drug was stopped and the other was assumed lifelong. After discharge, the patients were followed with a 1-month clinical evaluation for events monitoring and a 12-month clinical and instrumental with transcranial doppler (TCD) evaluation, to identify residual relevant shunt.
2.3. Endpoint and Follow-Up
The main outcome measure was the presence of a residual interatrial shunt at 12- months follow-up, detected by TCD or TTE after intravenous injection of agitated saline contrast and device size impact on residual long-term shunt. Differences in clinical, procedural, and echocardiographic characteristics between patients in the overall population were tested in a cluster analysis performed by using the echocardiographic characteristics related to the main outcome.
2.4. Statistical Analysis
All continuous variables were presented as mean (or median) ± standard deviation (or interquartile range) and categorical variables as numbers and percentages. The normal distribution of continuous variables was evaluated with the Kolmogorov-Smirnoff test A one-way ANOVA (with Bonferroni post-hoc correction) was elaborated to explore the difference in means; for the association of categorical variables, Chi-square test was used. A univariable logistic regression was made to identify the potential impact of the cluster on the residual shunt after 12 months. The two-sided statistical significance was established for p-value <0,05. All statistical analyses were performed using R (R Foundation for Statistical Computing, vers 4.3.0) with the Jamovi interface and SPSS v.25 (SPSS Inc., Chicago, IL) for Windows.
3. Results
3.1. Population Characteristics: Clinical and Echocardiography
Between March 2012 and June 2020, 118 patients underwent PFO closure with Gore Septal occluder device. All demographic characteristics are reported in Table 1.
The PFO closure indications were a TIA in 50 (42%) patients and stroke in 68 (58%). Within the overall population, 101 patients (86,1%) have a CT or CMR positive for de-novo cerebral lesion.
Before the procedure, the antiplatelet therapy consisted of ASA or Clopidogrel (SAPT) for 97 patients (82%). All the procedures were successful; Table 1 summarizes all the morphological characteristics and the procedural features. To choose the most appropriate device size, TEE was carefully reviewed before every procedure in 100% of the included population. The decision whether to use a 20 mm, 25-mm, or a 30-mm device was based on a qualitative assessment of the size of the ASA and the size of the PFO on preprocedural TEE. The device size ranged between 20 to 30 mm within the study population. A 20-mm was used in 5 patients (5% of the whole population), while the 25-mm was the most used in 92 patients (78%). Only in 19 patients (16%) atrial septum aneurysm (ASA) was found.
Cluster classification and analysis of septal anatomy.
Since overall population included had complex anatomy when using conventional parameters and assessing it based on the presence of 1 parameter, a cluster analysis was performed to differentiate the different patterns of complexity. Accounting for the available echocardiography characteristics and previous literature, the 3 chosen continuous variables for clustering were the PFO width (mm), tunnel length (mm), and septum secundum thickness (mm). From cluster analysis, 2 clusters were obtained with similar size (54 patients in the first group and 57 in the second one). Comparing the 2 clusters within the study population, we found no differences in baseline characteristics. However, a significant difference between clusters was found in tunnel length (12,6 ± 3,8 vs 7,2 ± 2 mm respectively, p <0,001) and PFO width (4,85 ± 1,8 vs 2,9 ± 1 mm, p <0,001). At the same time, in the septum secundum dimension, there is no relevant difference (p=0,99) [Figure 1]. Based on the aforementioned characteristics, the first group was identified as “complex anatomy” and the second one as “simple anatomy” [Table 2].
3.2. Outcomes and Correlates
At 1-month follow-up, all patients (n=118, 100%) were screened for major events and 1 death from stroke, and 4 paroxysmal atrial fibrillations with spontaneous resolution were reported. The 1-year follow-up was completed in 111 patients (94% of the population); TCD showed an anatomical or functional closure (< 10 bubbles residual shunt) in 107 patients (96,4% of patients with complete FU) and residual shunt in 4 (3,6%) [Figure 2]. 7 patients were lost to follow-up or did not perform a pre-procedural screening for anatomical assessment of the defect. At univariate logistic regression analysis, no significant impact of the cluster (complex vs simple) in the prediction of anatomical or functional closure after 12 months (OR 0.36, CI 95% 0.04-3.6, p=0.39) was found [Table 3]. Otherwise, the long-term closure rate is high, regardless of the device size chosen for defect closure (chi-square 1,27, p=0.53) [Figure 2]. No association was found between the presence of ASA and residual shunt in both clusters (also 1 patient with a residual shunt has ASA, 3 patients with a residual shunt has not, p=0.67).
4. Discussion
In this paper, we reported 1 year-results of a real-world single-center experience of PFO closure performed with a GORE device and the anatomical features of the treated patients in order to understand the correlation between outcomes and anatomical complexity of PFO. The main findings of our study are summarized as: i) PFO closure with GSO device is feasible and safe in a real-world experience on consecutive patients with high efficacy (96% of effective closure at 12 months-FU) and safety (no procedural access-related or device-related complications); ii) the complexity of the anatomy does not affect the 1-y results.
Percutaneous closure of PFO is a procedure whose main indication is the prevention of cardioembolic stroke recurrence. It is therefore a prophylactic intervention and not therapeutic. For these reasons, the maneuver is currently approved and justifiable in case it is performed with very high standards of success (efficacy) and minimal incidence of periprocedural complications and "discomfort" for the patient (safety). To date, the PFO procedure is widely available and in the hands of expert operators, it carries a very low risk of complications (overall rate 2.6% in RCTs) and a high success rate (93-96% of complete closure after 1 year with Amplatzer). A recent position paper has shown an advantage of percutaneous closure over medical treatment[4] and has established the clinical indications[12].
Once the procedure is considered to be indicated by a mean of multidisciplinary discussion, the main aim of the accurate TEE evaluation before procedures is to identify the following features: i) presence of ASA, ii) thickening of the septum secundum, iii) morphology and length of the tunnel; iv) concomitant presence of interatrial defects or fenestrations of the septum primum, prominent Eustachian valve, Chiari network, and any other finding that might contraindicate the procedure.
Indeed, the risk of residual shunt has been related to thromboembolic recurrence after PFO closure[13], and, therefore, a correction that is as complete as possible is desirable.
Classically, the anatomy of the septum can be distinguished into 2 categories: simple and complex. The latest is related to a higher rate of the residual shunt[14] and is characterized by the presence of at least one of the complexity factors: the presence of interatrial septal aneurysm (ASA), a long tunnel > 8 mm, a wide defects > 4 mm, a lipomatous septum secundum with diameter > 10 mm and the presence of Chiari's network or Eustachian valve[10,14].When no one of these factors is present, then the septum anatomy is considered “simple”, similar to the simple anatomy cluster in our study population. Since only one of the features described above is sufficient to define complex anatomy and no differentiation between the type of complexity has been done, the final results of the published evidence are really heterogeneous: to have a long tunnel is considered the same complex level as having a thick septum[15]. Several devices are currently available for the treatment of PFO and they consist of a double disk structure with a larger disk aimed at the right side of the septum and a smaller one on the left side[16].
The devices with the largest experience currently are Amplatzer PFO occluder, STARflex septal closure system, Gore Septal Occluder. Clinical trials exist for these devices and few details make each of them more useful in different situations. For example, Amplatzer is an almost rigid device, with a rigid waist not fitting long tunnel morphologies; in complex anatomies, a high failure incidence was shown[17]. STARflex septal closure system as well as a rigid waist not fitting long-tunnel morphologies; anyway, it has a soft structure limiting erosion; complex anatomies are not suitable to be efficacy treated with STARflex[6]. The second generation of GSO has been improved; it has a soft waist and structure and has been demonstrated to highly reduce the risk of septal distortion in long-tunnel morphology because of its better adaptation to PFO and surrounding structures anatomy, therefore also limiting the risk of erosion.
Regarding the complexity factors, a huge heterogeneity exists among different studies. For example, Greutmann et al 2009[18] found that the presence of ASA in patients undergoing percutaneous PFO closure with an Amplatzer PFO occluder significantly increases the rate of residual shunts at 6 months follow-up, even if 35-mm devices are used; no other significant anatomical factors were studied except for RA length and Chiari network. In this study, both resulting not related to the incidence of the residual shunt. Von Bardeleben et al[6] published the long-term results of a large population of 357 patients treated with 3 types of devices: Helex, Starflex, and Amplatzer PFO Occluder. Long follow-up was performed to assess the anatomical and functional closure during the time and a significant difference in time of closure was observed in the case of ASA only for Helex and Starflex devices. In the study of Giordano et al., complex PFO was found in 25% of the included population; it was defined as PFO width >13 mm, ASA or multi-fenestrated defect; in that study, the authors have underlined a difference in residual shunt after 12 months in the group treated by dedicated PFO device[19]. Tunnel length, ASA, and the presence of Eustachian Valve were considered to be complex anatomies in the study of Vitarelli et al[14] in which 50% of the included population had at least 1 of these criteria and R-to-L shunt was found in 12 % of the population during FU.
Considering the last generation of GSO device, Butera et al. published the first early and mid-term multicenter Italian experience and they did not differentiate the complexity of anatomies of PFO; they found a very low rate of procedural complication with device malposition in 3% of patients, vascular venous bleeding in 6%, residual significant shunt in only 3% of which 1.5% only more than trivial[8]. Other very small studies have been published[20], each of them including a small population and without differentiating between the complexity of the anatomy[15,21].
In contrast to previous studies, the overall population of our study presents a complex anatomy with 2 anatomical factors related to more complex procedures. The complexity of anatomy in this population is mainly defined by PFO tunnel length and PFO size, as stated by cluster analysis that identified the first group as more “complex” than the second one; no difference in outcomes was found between the 2 groups.
Therefore, our results are highly clinically relevant since they confirm a high rate of 12-month anatomical closure at TCD in patients treated with Gore device even in complex anatomies with good performance of device; this was true also irrespectively from the chosen size[7,8].
The fact that the presence of ASA was not related to PFO closure rate at 12 months in our experience, may be due to the low incidence of ASA in the study population (<20%). Moreover, the high stretching capacity of GSO and related sealing performance ensures a low rate of residual right-to-left shunt also in high-risk patients like those who present an ASA associated with PFO. The aforementioned stretching capacity may represent the main characteristic that ensures a good performance in the long tunnel defect (>8-10 mm), like in our population.
Limitations
This study has some limitations. First of all, the retrospective nature of the study and the relatively small population size. Although the 1-year FU is among the longest available in the literature, there is a considerable proportion of patients lost in fu, which couldn’t allow us to make definite conclusions. Otherwise, our patients did not undergo a transesophageal echocardiographic study to check for the presence of anatomical closure. A dedicated randomized controlled trial for a head-to-head comparison of the GSO with the most used device (Amplatzer) is needed to identify the best one in terms of implantation and long-term efficacy and safety.
5. Conclusions
The GSO device allows good PFO closure in the majority of patients, regardless of the defect’s anatomy. Noteworthy, the definition of complex anatomy is an already developing concept, due to the not uniform opinion in the studies performed until now. In this way, a device with good versatility may allow it to overcome this limit, also in consideration of the long-term effective defect’s closure.
Author Contributions
Conceptualization, G.V., M.G. and P.S.; methodology, G.V., M.G.; validation, P.S., M.G. and G.V.; formal analysis, G.V.; writing—original draft preparation, G.V., M.G.; writing—review and editing, M.G., G.V., D.C., D.S., and P.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
not required.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
M.G was a proctor for Abbott Medical. All other authors declare no conflict of interest.
References
- El-Said, H.G.; Moore, J.W. Erosion by the Amplatzer Septal Occluder: Experienced Operator Opinions at Odds with Manufacturer Recommendations? Catheter. Cardiovasc. Interv. 2009, 73, 925–930. [Google Scholar] [CrossRef]
- Schoen, S.P.; Boscheri, A.; Lange, S.A.; Braun, M.U.; Fuhrmann, J.; Kappert, U.; Strasser, R.H. Incidence of Aortic Valve Regurgitation and Outcome after Percutaneous Closure of Atrial Septal Defects and Patent Foramen Ovale. Heart 2008, 94, 844–847. [Google Scholar] [CrossRef]
- Zahn, E.M.; Wilson, N.; Cutright, W.; Latson, L.A. Development and Testing of the Helex Septal Occluder, a New Expanded Polytetrafluoroethylene Atrial Septal Defect Occlusion System. Circulation 2001, 104, 711–716. [Google Scholar] [CrossRef]
- Pristipino, C.; Sievert, H.; D’Ascenzo, F.; Louis Mas, J.; Meier, B.; Scacciatella, P.; Hildick-Smith, D.; Gaita, F.; Toni, D.; Kyrle, P.; et al. European Position Paper on the Management of Patients with Patent Foramen Ovale. General Approach and Left Circulation Thromboembolism. Eur. Heart J. 2019, 40, 3182–3195. [Google Scholar] [CrossRef] [PubMed]
- Thaman, R.; Faganello, G.; Gimeno, J.R.; Szantho, G. V.; Nelson, M.; Curtis, S.; Martin, R.P.; Turner, M.S. Efficacy of Percutaneous Closure of Patent Foramen Ovale: Comparison among Three Commonly Used Occluders. Heart 2011, 97, 394–399. [Google Scholar] [CrossRef] [PubMed]
- von Bardeleben, R.S.; Richter, C.; Otto, J.; Himmrich, L.; Schnabel, R.; Kampmann, C.; Rupprecht, H.J.; Marx, J.; Hommel, G.; Münzel, T.; et al. Long Term Follow up after Percutaneous Closure of PFO in 357 Patients with Paradoxical Embolism: Difference in Occlusion Systems and Influence of Atrial Septum Aneurysm. Int. J. Cardiol. 2009, 134, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Sganzerla, P.; Rondi, M.; Pavone, A.; Aiolfi, E.; Facchinetti, A.; Funaro, A.; Negrini, P. Clinical Performance of the New Gore Septal Occluder in Patent Foramen Ovale Closure: A Single-Center Experience. J. Invasive Cardiol. 2015, 27, 430–434. [Google Scholar] [PubMed]
- Butera, G.; Saracino, A.; Danna, P.; Sganzerla, P.; Chessa, M.; Carminati, M. Transcatheter PFO Closure with GORE® Septal Occluder: Early and Mid-Term Clinical Results. Catheter. Cardiovasc. Interv. 2013, 82, 944–949. [Google Scholar] [CrossRef]
- Søndergaard, L.; Kasner, S.E.; Rhodes, J.F.; Andersen, G.; Iversen, H.K.; Nielsen-Kudsk, J.E.; Settergren, M.; Sjöstrand, C.; Roine, R.O.; Hildick-Smith, D.; et al. Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke. N. Engl. J. Med. 2017, 377, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Rana, B.S.; Shapiro, L.M.; McCarthy, K.P.; Ho, S.Y. Three-Dimensional Imaging of the Atrial Septum and Patent Foramen Ovale Anatomy: Defining the Morphological Phenotypes of Patent Foramen Ovale. Eur. J. Echocardiogr. 2010, 11, 19–25. [Google Scholar] [CrossRef]
- Rana, B.S.; Thomas, M.R.; Calvert, P.A.; Monaghan, M.J.; Hildick-Smith, D. Echocardiographic Evaluation of Patent Foramen Ovale Prior to Device Closure. JACC Cardiovasc. Imaging 2010, 3, 749–760. [Google Scholar] [CrossRef] [PubMed]
- Kavinsky, C.J.; Szerlip, M.; Goldsweig, A.M.; Amin, Z.; Boudoulas, K.D.; Carroll, J.D.; Coylewright, M.; Elmariah, S.; MacDonald, L.A.; Shah, A.P.; et al. SCAI Guidelines for the Management of Patent Foramen Ovale. J. Soc. Cardiovasc. Angiogr. Interv. 2022, 1, 100039. [Google Scholar] [CrossRef]
- Martín, F.; Sánchez, P.L.; Doherty, E.; Colon-Hernandez, P.J.; Delgado, G.; Inglessis, I.; Scott, N.; Hung, J.; King, M.E.E.; Buonanno, F.; et al. Percutaneous Transcatheter Closure of Patent Foramen Ovale in Patients with Paradoxical Embolism. Circulation 2002, 106, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Vitarelli, A.; Mangieri, E.; Capotosto, L.; Tanzilli, G.; D’Angeli, I.; Toni, D.; Azzano, A.; Ricci, S.; Placanica, A.; Rinaldi, E.; et al. Echocardiographic Findings in Simple and Complex Patent Foramen Ovale before and after Transcatheter Closure. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 1377–1385. [Google Scholar] [CrossRef] [PubMed]
- Marshall, A.C.; Lock, J.E. Structural and Compliant Anatomy of the Patent Foramen Ovale in Patients Undergoing Transcatheter Closure. Am. Heart J. 2000, 140, 303–307. [Google Scholar] [CrossRef]
- Vizzari, G.; Pizzino, F.; Zwicke, D.; Tajik, A.J.; Carerj, S.; Di Bella, G.; Micari, A.; Khandheria, B.K.; Zito, C. Patent Foramen Ovale: Anatomical Complexity and Long-Tunnel Morphology Related Issues. Am. J. Cardiovasc. Dis. 2021, 11, 316–329. [Google Scholar]
- Calvert, P.A.; Rana, B.S.; Kydd, A.C.; Shapiro, L.M. Patent Foramen Ovale: Anatomy, Outcomes, and Closure. Nat. Rev. Cardiol. 2011, 8, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Greutmann, M.; Greutmann-Yantiri, M.; Kretschmar, O.; Senn, O.; Roffi, M.; Jenni, R.; Luescher, T.F.; Eberli, F.R. Percutaneous PFO Closure with Amplatzer PFO Occluder: Predictors of Residual Shunts at 6 Months Follow-Up. Congenit. Heart Dis. 2009, 4, 252–257. [Google Scholar] [CrossRef]
- Giordano, M.; Gaio, G.; Santoro, G.; Palladino, M.T.; Sarubbi, B.; Golino, P.; Russo, M.G. Patent Foramen Ovale with Complex Anatomy: Comparison of Two Different Devices (Amplatzer Septal Occluder Device and Amplatzer PFO Occluder Device 30/35). Int. J. Cardiol. 2019, 279, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Geis, N.A.; Pleger, S.T.; Katus, H.A.; Hardt, S.E. Using the GORE® Septal Occluder (GSO) in Challenging Patent Foramen Ovale (PFO) Anatomies. J. Interv. Cardiol. 2015, 28, 190–197. [Google Scholar] [CrossRef]
- Lockhart, C.J.; Johnston, N.G.; Spence, M.S. Experience Using the New GORE® Septal Occluder at the Margins. Catheter. Cardiovasc. Interv. 2013, 81, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Bar graph with complex and simple anatomy group mean values for PFO width and tunnel length.
Figure 1.
Bar graph with complex and simple anatomy group mean values for PFO width and tunnel length.
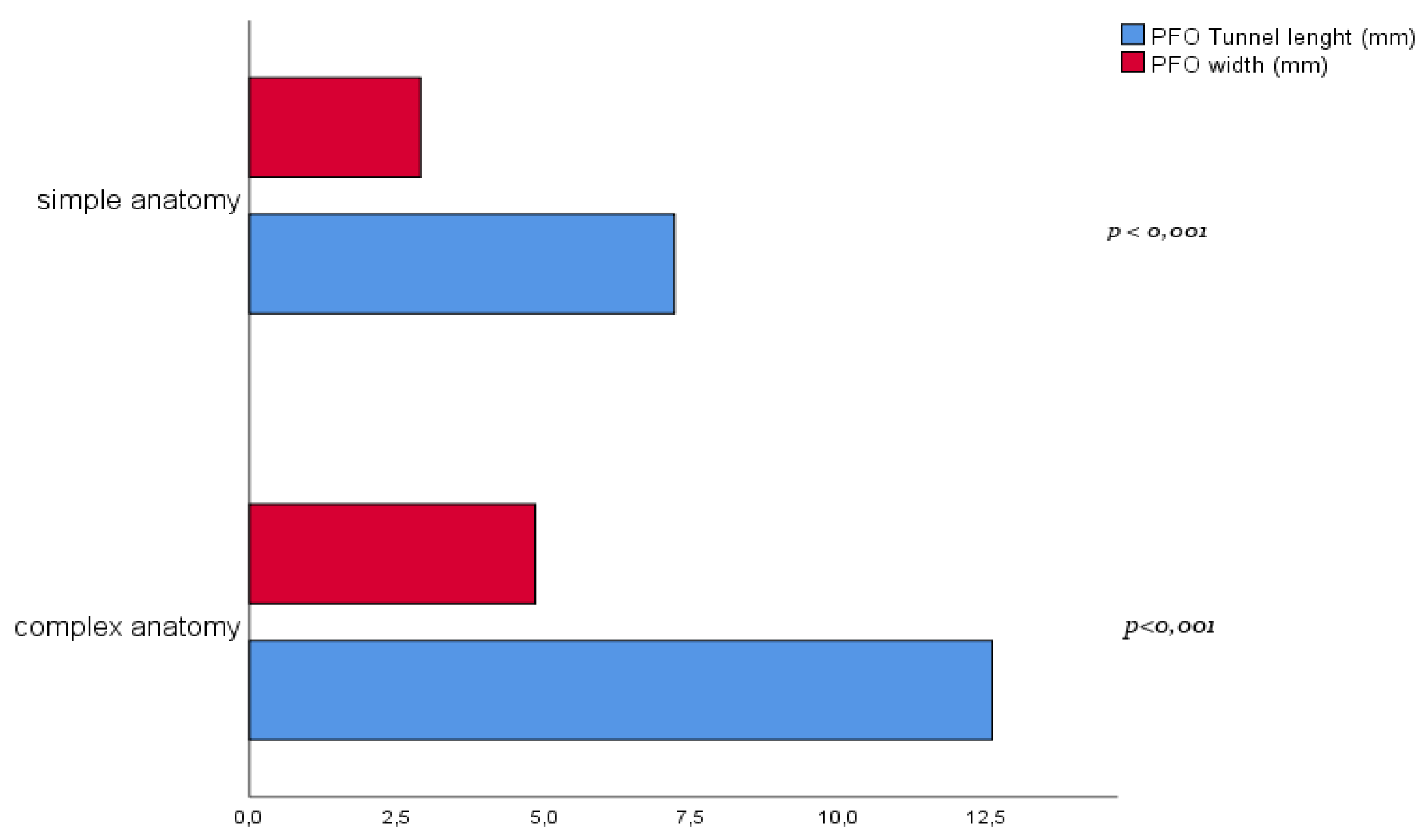
Figure 2.
Association of device size and 12-month follow-up transcranial doppler (TCD) result. The number within the white squares indicates the patient’s number for each device subgroup.
Figure 2.
Association of device size and 12-month follow-up transcranial doppler (TCD) result. The number within the white squares indicates the patient’s number for each device subgroup.
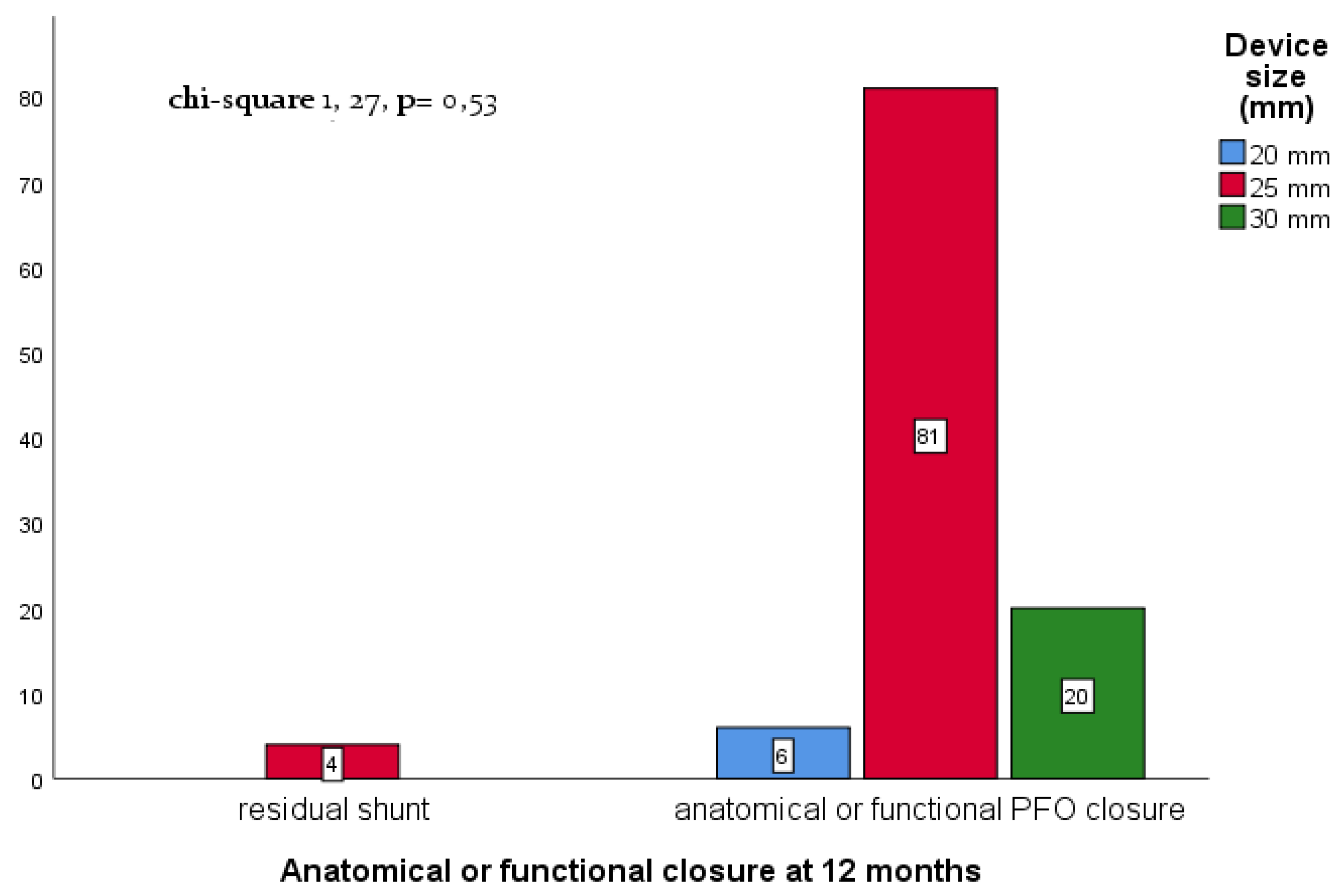

Table 1.
Patient demographic and procedural data.
| Patient population [n] | 118 |
| Male gender [n] | 60 (50,8%) |
| Age [years] | 55,4 ± 12,7 |
| Current smoker (n, %) | 19 (16,1%) |
| Indication for closure | |
| Stroke (n,%) | 68 (57,6%) |
| Transient Ischemic Attack (n,%) | 50 (42,4%) |
| Head CT or MRI de-novo lesion (n,%) | 101 (85,6%) |
| TEE Doppler study | |
| Small shunt (n,%) | 15 (12,7%) |
| Moderate-to-severe shunt (n,%) | 37 (31,4%) |
| Anatomical setting | |
| PFO only (n,%) | 105 (89%) |
| PFO+ASA (n,%) | 13 (11%) |
| Median procedure time [minutes] | 37 (range 33-45) |
| Median fluoroscopic time [minutes] | 7.3 (range 5.5-10.2) |
| Device used | |
| 20 mm (n,%) | 6 (5,0%) |
| 25 mm (n,%) | 92 (78%) |
| 30 mm (n,%) | 20 (17%) |
| Median contrast administration [ml] | 36 (range 25-54) |
1 Data are presented as mean ± SD, median (IQR) or n (%).
Table 2.
Cluster matching for procedural and anatomical characteristics.
| Complex anatomy (n. 57) | Simple anatomy (n. 54) | p-value | |
| Age | 53.9 ± 12.4 | 56.6 ± 13.0 | 0.279 |
| Procedure time (min) | 39.6 ± 12.1 | 41.5 ± 15.2 | 0.502 |
| Fluoroscopy time (min) | 10.1 ± 16.5 | 9.4 ± 5.8 | 0.748 |
| Contrast dye (ml) | 38.2 ± 26.1 | 47.1 ± 26.1 | 0.090 |
| SS thickness (mm) | 5.7 ± 2.3 | 5.7 ± 1.9 | 0.995 |
| Tunnel length (mm) | 12.6 ± 3.8 | 7.2 ± 2.0 | <0.001 |
| PFO width (mm) | 4.9 ± 1.8 | 2.9 ± 1.1 | <0.001 |
* Data are presented as mean ± SD.
Table 3.
Univariate predictor of anatomical or functional PFO closure at 12-months follow-up.
| Predictor | Anatomical or functional closure at 12-m (%) | OR | C.I. 95% | p-value |
|---|---|---|---|---|
| Complex vs simple anatomy¶ | 107/111 (96,4%) | 0,36 | 0,04 – 3,6 | 0,39 |
For logistic regression, complex anatomy was chosen as reference group. C.I. 95%: confidence interval at 95%, OR: odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



