
Submitted:
11 July 2023
Posted:
13 July 2023
You are already at the latest version
Abstract
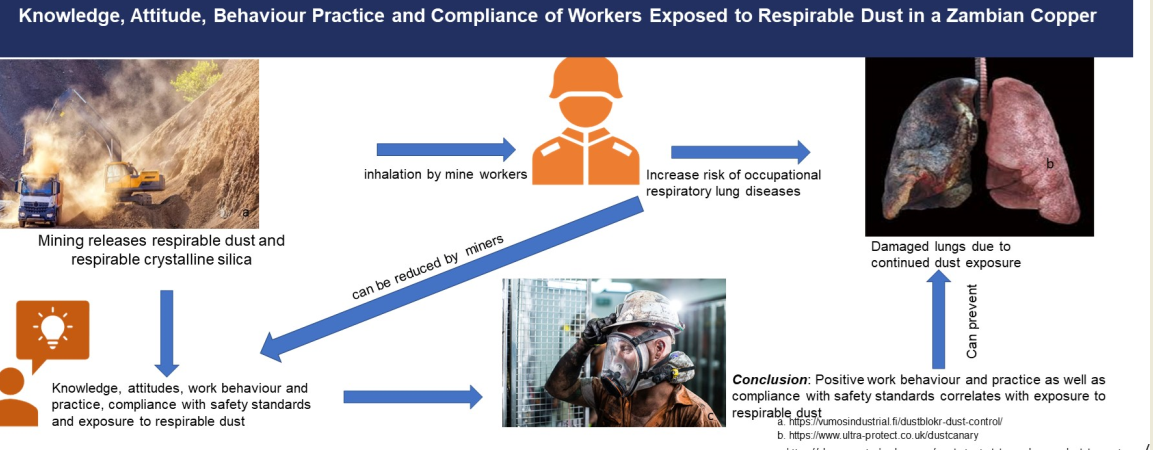
Work in the copper mining industry is often associated with exposure to respirable dust and respirable crystalline silica. This exposure has the potential to cause silicosis, a non-curable occupational respiratory lung disease. This study aimed at establishing the relationship between knowledge, attitudes, work behaviour and practice, compliance with safety standards and exposure to respirable dust. A cross-sectional descriptive survey was conducted on 528 mine workers. Statistical package for social sciences (SPSS) was used for descriptives. Structural Equation Modelling (SEM) with latent variables and partial least-squares (LVPLS) analysis was employed to determine the relationship among these variables. The results indicated that of the four (4) hypotheses, two (2) were supported and two (2) were rejected showing that there is a significant relationship between exposure to respirable dust and work behaviour and practice, as well as compliance with safety standards. Knowledge and attitudes towards respirable dust exposure did not significantly influence exposure. According to the results from the survey, positive work behaviour and practice as well as compliance with safety standards was significantly associated with exposure to respirable dust. It is recommended that the mine should focus on the miners’ work behaviour and practice and compliance with safety standards.
Keywords:
attitudes
; compliance and safety standards
; copper mine
; knowledge
; respirable dust
; work behaviour and practices
1. Introduction
Mining is considered one of the world's most predisposed environments for diseases and injuries. The mining industry has recorded a significant proportion of non-fatal and fatal injuries worldwide. Whether or not workers are familiar with occupational health and safety (OHS) concepts, many organizations globally continue to record losses and inefficiencies due to non-compliance [1]. Risks as a result of physical, emotional, mental and psychosocial factors are associated with the nature of someone’s work and management procedures in an organization. Besides this, one of the most dangerous occupational hazards affecting humans in the mining industry is respirable crystalline silica dust (primary quartz) mainly found in ores [2]. Exposure to crystalline silica dust exacerbates the risk of developing silicosis and cancer. Thus, the International Agency for Research on Cancer (IARC) has classified crystalline silica as a Group 1 lung cancer carcinogen [3].
To this effect, significant efforts are being made by the International Labour Organization (ILO) and World Health Organization (WHO) to prevent silicosis, an occupational respiratory disease which affects thousands of workers yearly. In 2020, a report by the ILO showed that annually approximately 340 million occupational accidents occur and 160 million victims succumb to work-related illnesses [4]. The ILO (2020) has provided standards on Occupational Health and Safety to guide governments, employers, and workers in ensuring maximum safety at workplaces. In 2019, the South African mining and quarry industries reported 2,406 work-related injuries and 51 deaths in the mining industry due to accidents and occupational exposure to hazards [5]. In Zambia, the Occupational Health and Safety Act No 36 of 2010 in the Zambian Constitution covers welfare in terms of health and safety at a workplace [6] and Act No 271 covers compensation for occupational-related injuries and disease [7]. The legislation lacks policies and regulations on specific hazard exposure such as respirable dust and crystalline silica which is capable of causing occupational respiratory diseases such as silicosis therefore, this is a gap that needs to be addressed.
1.1. Problem Statement
Silicosis is considered one of the diseases miners can contract over time during mining operations. Silicosis is a non-preventable incurable occupational respiratory disease caused by inhaling dust particles containing free crystalline silica from their environment [4]. Some environments require that workers are educated about exposure to respirable dust. The rationale behind the educational program is that workers’ knowledge gained is perceived to assist them to change ‘attitudes’ and ‘work behaviour’ as well as seriously complying with the health standards and regulations. Workers in developing countries are exposed to silica dust due to poor working conditions in industries such as mining and construction. Nguyen [8] stressed that many of the silica-exposed workers in the mining industry are unaware of the human health risks due to dust exposure.
The United Nations Sustainable Development Goal number 3 target 9 states that, “by the year 2030 substantially reduce the number of deaths and illnesses from hazardous chemicals and air, water and soil pollution and contamination” [9]. Poor working conditions and the environment within developing countries are substantial concerns because of the lack of preventive measures. Regardless of any industry, workers need to take some time to identify safety and health risks at workplaces, comply and implement appropriate measures for keeping them safe. The present study investigated the relationship between mine workers' knowledge, attitudes, work behaviour practices, and compliance with safety standards based on respirable dust exposure. In the literature, miners’ vulnerability and cause of death due to respirable dust exposure have been well reported [8,10]. However, scientific evidence is scarce in understanding the knowledge, attitudes and behaviour of employees regarding exposure to respirable dust [8]. Thus, the study aimed to empirically establish if knowledge, attitudes, and workplace behaviour significantly impact how workers respond to health and safety propositions with regard to respirable dust exposure.
1.2. Literature Review
Exposure to respirable dust is a major challenge in the mining industry because it is a component of raw ore material. Crystalline silica is one of the components most widely encountered minerals of the earth, with wide exposure in working environments and ambient environments [12]. In the past 15 years (i.e., 2008-2023) a significant number of studies on respirable dust exposure have been conducted in the mining and construction industries in some developing countries (South Africa, Ghana, Tanzania) and developed economies (China Australia, United States of America) [9,11]. According to World Bank [13], the mining industry provides a significant contribution to the economic wealth of many countries. This significant contribution to mining economies has often been at the cost of the health of employees involved in the mining industry. The most common hazard is the inhalation of dust, which can lead to lung damage. Dust control measures are used to reduce dust exposure and the effectiveness of these methods is dependent on how well they are used by workers, which is affected by their knowledge, attitude and behaviour.
A study conducted in Vietnam focused on workers knowledge, attitudes and practices in relation to silicosis among high-risk workers [8]. The outcome of the study was that knowledge, attitudes and practices were associated with high levels of health education, longer duration of work and non-smoking. Furthermore, the study concluded that health education should be prioritized for workers. In a similar study, Ahadzi [14] conducted research on stone quarry workers’ awareness on adverse effects of silica dust exposure. The research indicated that workers with secondary and higher education levels were more likely to be aware of silica dust exposure effects compared to workers without education. Another study by Aluko [15] investigated knowledge, attitudes and practices of occupational hazards and safety among healthcare workers revealed that most respondents were knowledgeable about hazards. However, in terms of practice and compliance, only 52% complied with preventive safety precautions as advised by the standard operating procedures, meaning that 48% did not comply.
In South Africa, Mavhunga [16] conducted a study on knowledge, attitudes and practices of coal miners in relation to occupational health and safety at a Mpumalanga mining site. It was found that, miners demonstrated lack of knowledge on health and safety legislation; thus, they did not portray sufficient knowledge of occupational diseases which affect their attitudes and non-compliance. In addition, a study focusing on unsafe behaviour propagation in miners’ social networks was conducted in China [17]. The outcome of the study was that knowledge played a mediating role in influencing unsafe behaviour among the workers. In addition, a study by Takemura [18] examined the effects of wearing masks and worker education on preventing occupational dust exposure. The outputs of the study showed that workers need to be educated on proper usage of masks which may prevent worsening of pulmonary function due to dust exposure.
In the United States of America, a study on formative research to reduce mine workers’ respirable silica dust exposure was conducted by Haas [19]. The research focused on assessing the feasibility of integrating technology into behaviour interventions and one of the objectives was to determine mine workers’ knowledge and attitudes towards respirable silica dust exposure. Participants were found to be knowledgeable on activities that may expose them to respirable silica dust and workers complied with safety standards towards dust exposure by wearing respirators to a point that they wore respirators even when it was not required. It also revealed that workers who had served longer years showed increased positive attitudes towards personal health compared to those that had less service years.
In another study focusing on mining engineering students being prepared for the mining sector, the research investigated the students’ knowledge, attitudes and practices on occupational safety and health issues [20]. The authors of the research showed that field work experience, interest in occupational safety and health and webinar attendance contributed to improving occupational safety and health knowledge, attitudes and practices in the mining industry.
From the literature, several limitations were identified which this study sought to overcome. When studying literature available on knowledge, attitudes, work behaviour and practices, compliance with safety standards among mine workers globally, it was found that there is a limitation in the literature of empirical research available relating knowledge, attitudes, work behaviour and practices, compliance with safety standards with exposure to occupational hazards.
The study by Sunanda and Yodang [20] used a limited sample size of (56) making the generalizations of the findings difficult. Two of the studies by Mavhunga and You [16,17] used cross-sectional research designs which limit conclusions on cause-and-effect relationships between variables, e.g., knowledge and unsafe behaviour [17]. Lastly, the study by Haas [19] was limited to respondents with knowledge of technology because the questionnaire was administered online excluding respondents who are unable to use the online platforms but could give relevant information on the topic. Compliance with safety standards is an equally important aspect in OHS as knowledge, attitudes, work behaviour and practices, because it helps to prevent accidents in a workplace. From the studies reviewed, no study focused on how compliant mine workers are in relation to hazard exposure. This study, therefore, incorporated compliance with safety standards as one of the moderators in reducing worker susceptibility to respirable dust exposure. This study also used a self-administered questionnaire with the help of knowledgeable research assistants present to help answer any questions that may seem not to be clear in the questionnaire for some respondents. In this study, knowledge refers to workers knowledgeability on the risks and dangers of respirable dust exposure, attitudes mean workers attitudes towards wearing personal protective equipment and respirable dust exposure in general, behaviour and practice refers to work behaviour and practice towards respirable dust exposure in a workplace, compliance refers to workers compliance with safety standards and exposure means reduced respirable dust exposure.
1.3. Theoretical Background
The theory provides an essential roadmap for investigating elements that can either prevent or promote the safety and health of workers in a workplace. This section presents different theoretical models/frameworks that have been used in similar studies. The first part discusses three used theoretical models/frameworks, which include, the Health Belief Model (HBM), the Theory of Planned Behaviour (TPB) and the Transtheoretical Model/ Stages of Change Mode (TTM/SOC). The second part discusses the conceptual model used in the study.
1.3.1. Health Belief Model (HBM)
The Health Belief Model (HBM) opined in the 1950s is widely used in determining the health behaviour of a person and postulates that the health behaviour of individuals is the consequence of perceptions, modifying behaviour and the likelihood of action [21]. The HBM focuses on four different dimensions which include: 1) perceived susceptibility of how an individual’s vulnerability to contracting a disease differs from the other, 2) perceived severity of how serious an individual may contract a particular disease may differ from one person to another; the same applies to 3) perceived benefits of acceptance to susceptibility towards a particular condition and 4) beliefs regarding the effectiveness of a particular action also differs between individuals and perceived barriers which is potential negativity of action to undertake a particularly recommended behaviour” [21]. In OHS the HBM helps in explaining the safety behaviour of workers. The HBM was selected as one of the underlying theories for the study because of its emphasis on perceived susceptibility as one of the influencers of behaviour in a workplace. This model helps to view a situation according to personal perception. The relevance of this model with the study is that individual workers are presumed to experience difficulties with breathing in a work environment where airborne particles are constantly present. Thus, all four dimensions highlighted above are likely to prevail. In such a situation, the pollution levels presumably will be high, hence making it riskier for the workers.
1.3.2. Theory of Planned Behaviour (TPB)
The Theory of Planned Behaviour (TPB) helps to understand behaviour changes in humans. This theory helps in providing guidelines which help to examine the beliefs and behaviour of individuals [22]. It postulates that attitudes toward a certain behaviour, subjective norms and perceived behaviour control a person to act in a particular way [23]. Thus, the purpose of displaying an action is determined by attitudes towards one’s action, subjective norms which are a person’s social influences or beliefs, and perceived behaviour control which is how easy or difficult one can engage in a behaviour. This theory highlights that for a person to behave in a particular way, attitudes, subjective norms, and perceived behaviour control must be combined. It is a fact that mining companies are equipped with human capital which is a very important resource and calls for safe behaviour in a workplace environment. Therefore, applying the TPB helps to determine the level of workplace safety and understanding of human behaviour changes. Like the Health Belief Model, the TPB is also perceived to be a relevant theoretical framework that directs the factors to be considered in the conceptualization of the research model to guide the hypothesis formulation.
1.3.3. Transtheoretical Model/Stages of Change Model (TTM)
The TTM theorizes that temporal behaviour integrated with processes and principles can change an individual’s behaviour. According to this theory, people are at different stages in acquiring a particular behaviour. [4]. Behaviour change is deemed as a process that combines several non-linear steps over a long period. The TTM can be explained using six (6); stages which are: 1) pre-contemplation, a stage that involves one’s aim of not taking action in the next 6 months, 2) contemplation, which involves probability or chance of taking action in 6 months; 3) preparation, which is organizing for change in the next 1 month, 4) action, which is taking on new behaviour’s in less than 6 months; 5) maintenance, which adopts a change in health behaviour and taking it up for more than 6 months and 6) termination, which involves continuing with a behaviour achieved over time [24]. The six processes of change are capable of associating a person’s progression from one phase to another.
1.3.4. Model Used in the Study
Based on the three theories some investigators proposed that unifying the models may provide a sure understanding of predicting behaviour in a workplace [25,26]. Dejoy [27] extracted 5 major constructs from the HBM, TPB, TTM and Theory of Reasoned Action (TRA) which were combined with 4 stages of workplace self-protective behaviour to include 1) hazard appraisal stage, 2) the decision-making stage, 3) initiation of self-protective action stage and 4) adherence of self-protection stage adopted from the TTM and created an integrative health protective behaviour model [27]. Five constructs from various theoretical models are combined in Dejoy's integrative model. These include threat-related beliefs, about one’s severity and vulnerability to hazards, response effectiveness of how a person views the benefits of self-protective behaviour, facilitating conditions for expanding concepts to use in value expectancy models, and safety climate which is a combination of social and organizational factors [28]. Based on the guidelines from Kim [26] and Dejoy [27], this study pursued a similar approach to integrate some of the theory tenets from the three theories. To this effect, the study reviewed the mine environment both surface and underground as characterized by respirable dust. All mine workers have a significant role to play in a particular behaviour which results in a blend of different behaviour factors. Figure 1 illustrates a constitution of the main thrusts of the two models, i.e., TPB and HBM. Based on the factors to explain respirable dust exposure (knowledge, attitudes, workplace behaviour and practice and compliance with safety standards) a conceptual model was formulated. Moderator factors were linked to helping explain the relationship that exists between exposure to respirable dust and knowledge. Workplace behaviour has been linked to occupational health and safety by some studies.
The conceptual framework was based on factors that can help to reduce respirable dust exposure, i.e., attitudes, work behaviour and practice, and compliance regarding respirable dust exposure are taken as primary predictors of a worker’s intention to engage in a particular behaviour [29] An outcome of a certain behaviour in a workplace can either be positive or negative, therefore linking three predictors to respirable dust exposure can be one of the major contributors to either being susceptible to respirable dust exposure or not [30]. Based on the concepts, the study measured workers emotional and environmental responses to stimuli (effects of respirable dust). Definitions of key terms used in the conceptual model in context with this study are given in Figure 1.
Attitudes
Attitude has been defined by different publications such as Ajzen and Fishbein [31] and Hogg and Vaughan [32]. According to Ajzen & Fishbein [31], an attitude refers to a learned tendency that makes an individual responsibility in a consistently favourable or unfavourable manner concerning a given object. Hogg and Vaughan [32] defined an attitude in a broader sense as a “mental and neutral state of readiness put up through experience and exerting an active or directive influence upon the individual's reaction in a situation” [32]. In addition, attitude has been defined as a relatively enduring organization of norms, beliefs and behavioural tendencies towards socially significant situations, groups, events or symbols [33]. The definition of attitude from a psychological perspective is a set of emotions, beliefs and behaviour towards a circumstance [34]. Given the different definitions, this study adopted the psychological perspective of attitude as forces arising from internal emotions and beliefs.
Behaviour
The term behaviour has become a commonplace feature in public health studies and definitions vary. In several definitions, the target focus has been the movement of an individual due to stimuli. Nonetheless, efforts were made to identify and review some definitions to give the contextual definition for the study. Some definitions include Tinbergen [35] who stated that behaviour is a total movement made by an animal in its entirety. Contrary, Alder [36] highlights that Dretske (1988) defines behaviour as a process of an inner entity bringing about bodily movement or environmental outcome. Furthermore, Shull [37] states that behaviour is an activity that an individual engages in. This study adopted the psychology perspective definition of behaviour which states that; “behaviour comprises of an organism's external reaction to its environment”.
Compliance
Cialdini and Goldstein [38] define compliance as “a kind of response to a particular communication upon request which may give an explicit or implicit outcome”. Interestingly, Cherry [34] on the definition of psychology disclosed that compliance is changing one's behaviour at the request or instruction of another person. Psychologists perceive compliance as a change in behaviour because another person asked you to do so. Based on the interrelatedness of the definition, this study adopted the simple definition propagated by the field of psychology which states that; “In psychology, compliance refers to changing one's behavior at the request or direction of another person”.
Given the aforesaid, a safe environment in a workplace is presumed to greatly influence how a worker will behave towards safety behaviour. Considering the two behaviour models adopted and modified (HBM and TPB), they can be helpful in foreseeing and understanding factors likely to positively improve the health of workers in a workplace. This justifies why modified HBM and TPB form the study framework in addressing occupational, health and safety challenges to respirable dust exposure. It is in this vein that the following hypotheses emerged.
Knowledge of risks and dangers of respirable dust and respirable dust exposure of mine workers
The concept of being knowledgeable about potential hazards in occupational health and safety of a workplace is cardinal to have a positive attitude that may help workers portray a particular behaviour, Aluko [15]. According to Nguyeni [8] a hazard or disease can be controlled if workers are knowledgeable about the risks and dangers of a particular hazard. To this effect, Takemura [18] carried out a study on factory workers’ occupational dust exposure. The study concluded that interventions of educating the workers helped in the prevention of respiratory diseases among the workers. Based on the aforementioned explanations highlighted by Aluko [15] Nguyeni [8] and Takemura [18] the following hypothesis was postulated:
H1: Knowledge of the risks and dangers of respirable dust positively reduces exposure to respirable dust in workers
Knowledge, attitudes of workers and respirable dust exposure of mine workers
The basis of attitudes in the framework shows that workers with positive attitudes are more likely to be cautious with the way they handle a hazard/disease. In addition, it is perceived that attitudes change due to the knowledge that the worker is provided within a workplace about the hazards present. The opportunity to be self-conscious and aware of dust-prone work environments. Hence, the wearing of personal protective gadgets like respirators is always upheld by the worker [8]. People assess outcomes and determine how they will perform in a particular situation. Thus, a person who believes in performing a particular behaviour will result in positive outcomes whereas an individual believing that performing a particular behaviour result in negative outcomes will hold a hostile attitude towards the behaviour. The reasoning behind this approach is that one’s attitudes can greatly influence decisions they make in a work environment, based on the discussion we hypothesized that:
H2: Knowledge of the risks and dangers of respirable dust is positively moderated by attitudes to reduce respirable dust exposure in workers.
Knowledge, work behaviour and practice and respirable dust exposure of mine workers.
The concept of safety behaviour has been put forward as the way someone acts to support or not support safety practices e.g., in training for safety or in complying with safety activities. Safety practices are key to minimizing workplace injuries and accidents. Work behaviour contributes to accidents in a workplace, therefore, the presence of good safety behaviour and practice results in workers complying with safety rules [39]. Zin ad Ismail [39] further stated that employees need a particular behaviour to engage in good safety practices. Hence, we hypothesized that:
H3: Knowledge of the risks and dangers of respirable dust is positively moderated by work behaviour and practice towards respirable dust exposure of workers
Knowledge, compliance with safety standards and respirable dust exposure on mine workers
Safety compliance is an act of sticking or adhering to safety rules set by an overseeing body or legislators to protect the welfare of workers in a workplace. Companies need to adhere to standards set by regulatory bodies for them to be considered compliant and this has to be done with the help of safety officers enforcing regulations set. Workers tend to engage in a belief that an accident cannot happen to them which justifies them in adopting unsafe behaviour in workplace practices. Hence the following hypothesis was postulated:
H4: Knowledge of the risks and dangers of respirable dust is positively moderated by compliance with safety standards towards respirable dust exposure
2. Methods
The methodology used during this study was a cross-sectional survey of mine workers in both underground and surface operations at a mining site located in the Copperbelt Province of Zambia. The sample frame focused on miners working in dusty environments such as operators, rock breakers, conveyer belt attendants, workmen, the person in charge, section bosses, shift bosses, mine captains and mine engineers. The total target of respondents was six hundred (600). Thirty-eight (38) qualitative statements based on the hypotheses from the conceptual framework were grouped under the knowledge of the risks and dangers of respirable dust, attitudes of working in a respirable dust environment, working behaviour and practice in a workplace, compliance with safety standards and exposure to respirable dust. The statements were measured using a 5-point Likert scale questionnaire with the lowest scale being 1 representing strongly disagree and the highest was 5 representing strongly agree which is provided in the supplementary material.
The questionnaire was first piloted on fifty (50) mine workers twenty-five (25) surface and twenty-five (25) underground, from one mining shaft. Respondents highlighted that some questions needed clarity but the time to complete the questionnaire was good because it was completed within 7 minutes, which did not interfere with their work schedules. Compliance as a topic was missing in the questionnaire so it was later added. Six hundred (600) potential respondents were given the revised questionnaire through the human resource department. The actual responses received were 528 out of the 600 questionnaires handed out, thus the response rate of 88%. Respondents answered all the questions indicating that there were no missing values. Respondents included 217 (41%) surface mine workers and 311 (59%) underground mine workers.
3. Data Analysis and Results
Collected data were entered in Microsoft Excel and later exported to statistical analysis for social sciences (SPSS) for descriptive analysis and structural equation modelling (SEM) with latent variables of partial least-squares (LVPLS) embedded in SmartPLS4 for model analysis. The data was initially tested for the presence of outliers using skewness and kurtosis. This test proved that the data was normally distributed. Secondly, data were subjected to validity and reliability tests. This helped in reducing the variables from the initial 38 using a cutoff factor loading of 0.7. Three factors K1 (K = knowledge), ERD1 (Exposure to Respirable Dust) and ERD8 were deleted because the study aimed at exploring relationships at high factor loading. No factors for BP (Work Behaviour and Practice), A (Attitudes), CSS (Compliance and Safety Standards)
Therefore, the average factor loading was specified at the 0.7 thresholds. BP4 was eliminated because it was a multi-collinear statement with a Variance Inflation Factor (VIF) of greater than 5. Thirty-six (35) factors were loaded as summarized in Table 1. Loading relevance was conducted on the 35 indicator factors to check if the model could be maintained using PLS model 4. Indicators with problems were identified and removed from the PLS to improve the value of Average Variance Extracted (AVE) and composite reliability of their constructs over the 0.5 thresholds as shown in Figure 2.
Additionally, internal consistency of the model to determine composite reliability for constructs knowledge, attitudes, behaviour practice, compliance safety standards and exposure to respirable dust were estimated as 0.942,0.932, 0.919, 0.936 and 0.893 respectively. From the results, it was observed that internal consistency reliabilities on the factors were very good.
3.1.1. Descriptive Analysis
Mean scores for responses on each questionnaire item and overall score for each variable were computed. According to Likert [40] and Boone and Boone [41] Likert scale items can be computed and interpreted as follows: between 1 – 1.8 (strongly disagree), 1.9 – 2.6 (disagree), 2.7 – 3.4 (Neutral), 3.5 – 4.2 (agree) and 4.3 – 5 (strongly disagree).
It can be seen that the majority of the workers agreed with the statements on the questionnaire items about knowledge, attitudes, work behaviour and compliance with safety standards since the mean scores of the entire group ranged between 3.5 and 4.2. Concerning respirable dust exposure majority of the workers gave a neutral response. It was observed that mean scores for underground workers were slightly higher for all variables compared to surface workers.
3.1.2. Outer Loadings
The outer loadings for knowledge ranged between 0.812 and 0.898, attitudes ranged between 0.772 and 0.923, behaviour practice ranged between 0.721 and 0.866, compliance and safety standards ranged between 0.769 and 0.882 and lastly reduced exposure to respirable dust ranged between 0.702 and 0.867.
3.1.3. Convergent Validity
Convergent validity is determined using Average Variance Extracted (AVE), if the AVE for the latent variable is greater than the 0.5 threshold then the variable can explain the variability. The following AVE values were obtained, knowledge obtaining 0.699, attitudes obtaining 0.692, behaviour practice attaining 0.665, compliance and safety standards 0.633 and exposure to respirable dust 0.530. Therefore, the measures of the five variables showed that constructs recorded high levels of convergent validity because they were all above the 0.5 thresholds.
3.1.4. Discriminant Validity
The study went further to assess the relationship between indicator variables which is a requirement in PLS-SEM. This was achieved by applying the Fornell-Larcker criterion to assess discriminant validity, as shown in Table 2. Discriminant validity was met because the square root of AVE for the indicator variables knowledge, attitudes, behaviour practice, compliance and safety standards and Exposure to respirable dust were larger than the corresponding latent variable correlations (LVC).
3.1.5. Collinearity Assessment for the Structural Model in PLS-SEM
Collinearity was tested using the Variance Inflation Factor (VIF). It is a significant test in the structural model, if the VIF value is above 5 then a factor is considered to be collinear with other factors and therefore, it is problematic. The collinearity results are summarized in Table 3. From the Table, the VIF values were less than 5 suggesting that Attitudes, Behaviour practice, Compliance and Safety Standards and Knowledge were non-collinear. All the values were less than 5 for each factor variable.
3.1.6. Coefficient of Determination (R2)
The model in PLS-SEM Exposure to Respirable dust was the dependent variable. How much change was accounted for by each predictor variable was explained using the coefficient of determination (R2). The rule of thumb for R2 is that the values 0.25,0.50 and 0.75 are considered to be weak, moderate and strong coefficients of determination respectively. In this research, the R2 value of 0.187 was considered weak for knowledge, attitudes, behaviour practice and compliance and safety standards. This means that by putting the variables jointly, they explain 18.7% of the variance of the dependent variable exposure to respirable dust. In other words, there is a likelihood that other factors not considered as variables for the study might account for the remaining 81.3%.
3.1.7. Path Coefficient
From the conceptual model, results indicate that two out of four structural models had significant relationships. For example, behaviour practice and exposure to respirable dust, compliance and safety standards, knowledge and attitudes, knowledge and compliance with safety standards, knowledge and behaviour practice. Attitudes and exposure to respirable dust and knowledge and exposure to respirable dust were non-significant as summarized in Table 4.
3.1.8. Predictive Relevance (Q2)
The predictive relevance (Q2) establishes the predictive power of the endogenous constructs in a model. If Q2 is greater than zero, it indicates that the values in the model were well constructed and that the model has predictive power. Attitudes (0.682), behaviour practice (0.520), compliance and safety standards (0.470) and exposure to respirable dust (0.100) were the only endogenous constructs that were used in the model for running PLS-predict. They all indicated good predictive relevance for the endogenous variables because the Q2 were all greater than zero.
3.1.9. Effect Size
Effect size determines how variables influence each other in a model. Effect size can be interpreted as 0.02, 0.15 and 0.35 which are small, medium and large respectively. The structural model was explored to assess the effect of how exogenous constructs affected endogenous constructs. It was observed that, knowledge, had a large effect (3.514) on attitudes, behaviour practice and compliance and safety standards (1.528 and 1.152), while a small effect size was observed on attitudes (0.004), behaviour practice (0.013), compliance and safety standards (0.004) and knowledge (0.004) on exposure to respirable dust.
3.1.10. Multi-Group Analysis
This data set comprised of mine workers in dusty jobs both underground and surface operations Therefore, it was imperative to conduct a multi group analysis (PLS-MGA) using a parametric approach. This approach compares path coefficients of different groups by modifying independent -sample t test using bootstrapping, standard deviation of the path coefficients was calculated to see if surface and underground, male and female and education level had moderating effects on the findings of the research. The concern arose because heterogeneity may exist in model significant differences of the categorical groups. Results revealed that in terms of location of operations underground miners and surface miners differed in knowledge of risks and dangers of respirable dust exposure (p<0.05) and exposure to respirable dust (p<0.05). In relation to gender there were no significant differences and in relation to education level of education significant differences were seen between those with secondary and tertiary education in relation to attitudes and compliance with safety standards (p<0.05).
3.1.11. Hypotheses Testing Results
Out of the four (4) main hypotheses generated in the conceptual model, two (2) were supported and 2 were not supported as shown in Table 5. Knowledge is found to have significant relationships with attitudes, behaviour practice and compliance and safety standards. Therefore, the hypothesis was retained. Nonetheless, the relationships between knowledge and attitudes toward exposure to respirable dust were non-significant hence the hypothesis was rejected.
4. Discussion
Concerning the descriptive statistics given in Table 1, the majority of the workers knew the health risks associated with respirable dust exposure, they had positive attitudes towards wearing respiratory protective equipment (RPE) and the company provided the RPE whenever necessary. With work behaviour, most of the workers showed good behaviour and practice towards the dusty environments where they worked and the majority of the workers complied with the safety standards of dust exposure. It is important to note that these workers showed a neutral stance on the aspect of exposure to respirable dust items because they were not sure if they have exposed to dust the entire shift or not and if they needed job rotations during operations. There were no significant differences in gender, age or education level. However, the groups (surface and underground miners) differed in the mean values about knowledge, work behaviour, compliance with safety standards and work area. Work areas were one of the variables that were explored with mean scores and mean scores for underground miners were on average higher than for surface miners. This implied that underground miners were more knowledgeable of risks related to respirable dust exposure than surface miners, they had better attitudes to wearing PPE than surface miners, the work behaviour and practice towards exposure to respirable dust was better than that of surface miners, and they were more compliant with safety standards than surface miners.
H1: Knowledge of the risks and dangers of respirable dust positively reduces exposure to respirable dust in workers
The results for Hypothesis One (1) show that there is no significant relationship between knowledge of the risks and dangers of respirable dust and exposure for the miner workers studied. The results show that workers may have knowledge of the risks and dangers of respirable dust exposure but it may not have an impact on their exposure to respirable dust during operations. However, the finding of this study is contradicted by Ahadzi [14] who established a relationship between workers' awareness of silica dust and workers’ knowledge of how it adversely affects their geographical location in two (2) Ghanaian regions. Another study that contradicted the finding was that of Haas [19] which indicated a relationship between knowledgeability on respirable silica dust and sources of exposure amongst workers. Even though the hypothesis was not supported in this study there is a need for the management of the mining site to seriously undertake appropriate measures in educating workers on the risks and dangers of respirable dust exposure because this can reduce the chances of contracting respiratory diseases.
H2: Knowledge of the risks and dangers of respirable dust is positively moderated by attitudes to reduce respirable dust exposure in workers.
Knowledge is important to creating positive attitudes that will infuse good behaviour in a workplace to reduce respirable dust exposure. The results in Table 5 show that knowledge was not positively moderated by attitudes to reduce respirable dust effects on miners, implying that even though the workers know, their attitudes will not necessarily influence exposure to respirable dust. The result of this hypothesis, therefore, implies that even though management makes efforts to sensitize workers on their attitudes towards respirable dust exposure it does not necessarily influence exposure significantly. The findings of the current study are in contrast with what Mavhunga [16] found in a coal mine where workers had a good appreciation of attitudes towards occupational exposure.
H3: Knowledge of the risks and dangers of respirable dust is positively moderated by work behaviour and practice towards respirable dust exposure
Hypothesis number 3 was supported, stating that the workers’ knowledge was moderated by positive perceived behaviour towards respirable dust exposure as seen in Table 5. This is supported by the findings of Haas [19] who found that mine workers were knowledgeable on health-protective behaviour towards respirable silica dust exposure to the point that, they ensure that they wear their respirators even in areas where it was not required. Further, the study conducted by You [17] in China disclosed that knowledge of safety played a role as a mediator in the unsafe behaviour propagation of mine workers The result means that management of the mining site should continue with awareness programs on the knowledge of risks and dangers of respirable dust exposure so that miners can integrate them into positive behaviour and practice. Table 5 shows that there is a significant relationship between the variables. The result is in agreement with the finding of the study by You [17] that focused on miners’ unsafe behaviour towards safety during operations at a mining site in China. The authors found that unsafe behaviour propagation significantly affected the safety of miners. The outcome of this hypothesis implies that the perceived behaviour practice of miners should remain positive towards reducing respirable dust exposure during mining operations.
H4: Knowledge of the risks and dangers of respirable dust is positively moderated by compliance with safety standards towards respirable dust exposure.
Table 5 shows that the knowledge of miners regarding the risks and dangers of respirable dust is positively moderated by compliance. Therefore, concerning compliance with safety standards, workers at the mining site need to comply with the regulations on respirable dust to reduce exposure. The finding is supported by the study conducted in Siaya County in Kenya which found that knowledge was one of the key indicators that influence regulatory compliance regarding safety miners [42] This is consistent with our study regarding knowledge and compliance with safety standards. The outcome of the hypothesis implies that miners need to know the health risks to comply with the safety standards at the mining site. Beth [42] recommended that predictors influencing compliance with safety regulations in small-scale mines were concerning the perceived cost of compliance, awareness of safety requirements and administrative failures which aligns with the current study. Since the result was significant, there is a need for mining companies to make compliance with safety standards regarding exposure to respirable dust a priority during mining operations to reduce exposure to respirable dust.
The current study aimed at empirically establishing the relationship between knowledge, attitudes, work behaviour and practice, and compliance with safety standards to respirable dust exposure at the mining site. The findings of the study revealed that there is no direct significant relationship between knowledge of the risks and dangers of respirable dust, attitudes of workers to respirable dust and exposure to respirable dust. However, there were significant relationships between working behaviour and practice at the workplace and compliance with safety standards and respirable dust exposure of workers. This implies that workers have the knowledge of health risks associated with respirable dust exposure through awareness programs at the mine but there is a need continuously monitor the work behaviour of miners concerning compliance with standards such as the routine wearing of PPE during operations.
Another observation from the study was that work behaviour and practice, and compliance with safety standards are moderators between knowledge of the risks and dangers of respirable dust exposure and reduced susceptibility to respirable dust. Therefore, being knowledgeable on the risks and dangers of respirable dust exposure is not enough to reduce exposure among workers but being knowledgeable on promoting good work behaviour and practice, and implementing compliance with safety standards will reduce worker exposure to respirable dust because knowledge of ownership is not good enough to influence exposure. Therefore, mining companies should embark on prompt awareness monitoring programs on knowledge on good worker behaviour and practice which will highlight how workers should behave during operations and give them consequences of how they will deal with workers not complying with safety standards.
The study recommends that the management of the mining company through awareness programs should ensure that workers’ attitudes, work behaviour and practice are monitored constantly so that respirable dust exposure is reduced to reasonable standards during operations. This can be achieved by standardized continued monitoring programs. On this basis, future studies should be conducted in different mining companies across Zambia to determine how these factors influence respirable dust exposure in other mines. In addition to this, future studies should include measurement data to relate to the findings of this study and observations, interviews and focused group discussions. Further, other studies should explore the current conceptual model by determining respirable dust effects on mine workers' compliance and safety standards through knowledge and behaviour practice.
4.1. Limitations
The limitation of the study is that it measured knowledge, attitudes, work behaviour and practice, and compliance from miners at one mining site which makes it difficult to generalize results to other mining sites.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
The manuscript is as a result of a compilation from contributions of all authors.
Funding
The authors would like to gratefully acknowledge financial aid received from the Copperbelt University Africa Center of Excellence for Sustainable Mining (Zambia) and the Ministry of Technology and Science.
Acknowledgments
We would like to thank the mining company for availing the information.
Ethical Approval
Ethical clearance was obtained from the Copperbelt University research ethical clearance committee and the participants signed a consent form before answering the questionnaire.
Consent for Publication
All authors have given approval to the final version of this manuscript.
Availability of Data and Material
Data available on reasonable request from the corresponding author.
References
- Cagno E, Micheli GJL, Jacinto C, Masi D. An interpretive model of occupational safety performance for Small- and Medium-sized Enterprises. Int J Ind Ergon. 2014 Jan 1;44(1):60–74. [CrossRef]
- Scarselli A, Corfiati M, Di Marzio D, Iavicoli S. Evaluation of workplace exposure to respirable crystalline silica in Italy. Int J Occup Environ Health. 2014. [CrossRef]
- International Agency for Research on Cancer. IARC Working group on the evaluation of carcinogenic risks to humans: Silica, some silicates, coal dust and para-aramid fibrils. Lyon, 15-22 October 1996. IARC Monogr Eval Carcinog risks to humans. 1997 [cited 2020 Mar 3];68:1–475. Available online: http://www.ncbi.nlm.nih.gov/pubmed/9303953.
- International Labour Organization. World Statistics: The enormous burden of poor working conditions. 2020 [cited 2023 Jan 22]. Available online: https://www.ilo.org/moscow/areas-of-work/occupational-safety-and-health/WCMS_249278/lang--en/index.htm#:~:text=The enormous burden of poor working conditions&text=Worldwide%2C there are around 340,of accidents and ill health.
- Department of Mineral Resources. 2019 Mine Health and Safety Statistics | South African Government. 2020 [cited 2023 Jan 22]. Available online: https://www.gov.za/speeches/2019-mine-heatlh-and-safety-statistics-24-jan-2020-0000.
- Zambian Parliament. The Occupational Health and Safety Act No. 36 of 2010. 2010;(36):53–66. Available online: http://www.parliament.gov.zm/node/3409.
- Government of the Republic of Zambia. The Workers’ Compesation ACT Chapter 271 of the Laws of Zambia. 2010.
- Nguyen V, Thu HNT, Le Thi H, Ngoc AN, Van DK, Thi QP, et al. Knowledge, attitude, and practices (KAP) on silicosis among high-risk worker population in five provinces in Vietnam. In: Xuan-Nam Bui, Changwoo Lee CD, editor. Proceedings of the international conference on innovations for sustainable and responsible mining. Hanoi, Vietnam: Springer Science and Business Media Deutschland GmbH; 2021 [cited 2022 Nov 11]. p. 469–84. Available online: https://link.springer.com/chapter/10.1007/978-3-030-60839-2_25. [CrossRef]
- United Nations. Sustainable Development Goal 3: Good Health and Well-being. 2023 [cited 2023 Jan 23]. p. 61–78. Available online: https://zambia.un.org/en/sdgs/3.
- Scarselli A, Binazzi A, Forastiere F, Cavariani F, Marinaccio A. Industry and job-specific mortality after occupational exposure to silica dust. Occup Med (Chic Ill). 2011 Sep 1;61(6):422–9. Available online: https://academic.oup.com/occmed/article-lookup/doi/10.1093/occmed/kqr060. [CrossRef]
- Arrandale VH, Kalenge S, Demers PA. Silica exposure in a mining exploration operation. Arch Environ Occup Heal. 2018 Nov 2;73(6):351–4. [CrossRef]
- Kim HR, Kim B, Jo BS, Lee JW. Silica exposure and work-relatedness evaluation for occupational cancer in Korea. Vol. 30, Annals of Occupational and Environmental Medicine. BioMed Central Ltd.; 2018 [cited 2020 Sep 18]. Available online: /pmc/articles/PMC5791359/?report=abstract. [CrossRef]
- The World Bank. Zambia Mining Investment and Governance Review. Zambia Mining Investment and Governance Review. World Bank; 2016. Available online: http://elibrary.worldbank.org/doi/book/10.1596/24317. [CrossRef]
- Ahadzi DF. Awareness of adverse health effects of silica dust exposure among stone quarry workers in Ghana. 2021;0171119931(February):1–41. [CrossRef]
- Aluko OO, Adebayo AE, Adebisi TF, Ewegbemi MK, Abidoye AT, Popoola BF. Knowledge, attitudes and perceptions of occupational hazards and safety practices in Nigerian healthcare workers. BMC Res Notes. 2016;9(1). [CrossRef]
- Mavhunga K. Knowledge, attitude and practice of coal mineworkers pertaining to Occupational Health and Safety at the Leeuwpan Mine in Mpumalanga Province, South Africa. 2018. Available online: http://univendspace.univen.ac.za/handle/11602/1183.
- You M, Li S, Li D, Xia Q. Study on the Influencing Factors of Miners’ Unsafe Behavior Propagation. Front Psychol. 2019;10(November):1–12. [CrossRef]
- Takemura Y, Kishimoto T, Takigawa T, Kojima S, Wang BL, Sakano N, et al. Effects of mask fitness and worker education on the prevention of occupational dust exposure. Acta Med Okayama [Internet]. 2008;62(2):75–82. Available online: https://www.ptonline.com/articles/how-to-get-better-mfi-results.
- Haas EJ, Willmer D, Cecala AB. Formative research to reduce mine worker respirable silica dust exposure: A feasibility study to integrate technology into behavioral interventions. Pilot Feasibility Study. 2016;2(1):1–11. [CrossRef]
- Sunandar S, Yodang Y. Analysis of Mining Engineering Students’ Knowledge, Attitudes and Practices on Occupational Safety and Health in Mining Industry Field. J Aisyah J Ilmu Kesehat. 2021;6(1):127–32. [CrossRef]
- Janz NK, Becker MH. The Health Belief Model: A Decade Later. Heal Educ Behav. 1984;11(1):1–47. [CrossRef]
- Guerin RJ, Sleet DA. Using Behavioral Theory to Enhance Occupational Safety and Health: Applications to Health Care Workers. Am J Lifestyle Med. 2021;15(3):269–78. [CrossRef]
- Prochaska J, Diclemente CC, Norcross JC. How people change, Prochaska, 1992. Am Psychol. 1992;47(Septembe9):1102–14. Available online: https://pubmed.ncbi.nlm.nih.gov/1329589/. [CrossRef]
- Kyaw WM, Chow A, Hein AA, Lee LT, Leo YS, Ho HJ. Factors influencing seasonal influenza vaccination uptake among health care workers in an adult tertiary care hospital in Singapore: A cross-sectional survey. Am J Infect Control. 2019;47(2):133–8. [CrossRef]
- Glanz K, Bishop DB. The role of behavioral science theory in development and implementation of public health interventions. Annu Rev Public Health. 2010;31:399–418. [CrossRef]
- Kim SA, Oh HS, Suh YO, Seo WS. An integrative model of workplace self-protective behavior for Korean nurses. Asian Nurs Res (Korean Soc Nurs Sci). 2014;8(2):91–8. [CrossRef]
- DeJoy DM. Theoretical models of health behavior and workplace self-protective behavior. J Safety Res. 1996;27(2):61–72. [CrossRef]
- Ajzen I. The Theory of Planned Behavior. Disabil CBR Incl Dev. 1991;33(1):52–68.
- Guerin RJ, Toland MD. An application of a modified theory of planned behavior model to investigate adolescents’ job safety knowledge, norms, attitude and intention to enact workplace safety and health skills. J Safety Res. 2020;72(December):189–98. [CrossRef]
- Hill RJ. Contemporary Sociology,. 2015;6(2):244–5.
- Ajzen I, Fishbein M. Attitudes and the AttitudeBehavior Relation: Reasoned and Automatic Processes. Eur Rev. 2007;(770853977):37–41. [CrossRef]
- Hogg MA, Vaughan GM. Social psychology. New York: Pearson Education Limites; 2005.
- Haddock G, Maio GR. Attitudes: Content, Structure and Functions. Introd to Soc Psychol a Eur Perspect [Internet]. 2008;112–33. Available online: http://www.blackwellpublishing.co.uk/content/hewstonesocialpsychology/chapters/chapter6.pdf.
- Cherry K. Attitudes and Behavior in Psychology. Very Well Mind. 2021;1–7. Available online: https://www.verywellmind.com/attitudes-how-they-form-change-shape-behavior-2795897.
- Tinbergen N. The study of instinct. 1951.
- Alder H. Representational Systems. In: Handbook of NLP. 2019. p. 99–113.
- Shull RL. Interpreting Cognitive Phenomena: Review of Donahoe and Palmer’s Learning And Complex Behavior 1. J Exp Anal Behav. 1995;63(3):347–58. [CrossRef]
- Cialdini RB, Goldstein NJ. Social influence: Compliance and conformity. Annu Rev Psychol. 2004;55(1974):591–621. [CrossRef]
- Zin SM, Ismail F. Employers’ Behavioural Safety Compliance Factors toward Occupational, Safety and Health Improvement in the Construction Industry. Procedia - Soc Behav Sci. 2012;36(June 2011):742–51. [CrossRef]
- Likert R. A Technique for the Measurment of Attitudes. WoodsWorth, editor. Vol. 140. New York: Archives of Psychology; 1932.
- Boone HN, Boone DA. Analyzing Likert data. J Ext. 2012;50(2). [CrossRef]
- Beth AA. Assessment of occupational safety compliance in small-scale gold mines in siaya county, kenya. 2018;1–90. Available online: http://erepository.uonbi.ac.ke/bitstream/handle/11295/104630/Beth_Assessment Of Occupational Safety Compliance In Small-Scale Gold Mines In Siaya County%2C Kenya..pdf?sequence=1&isAllowed=y.
Figure 1.
The relationship between knowledge and exposure to respirable dust exposure among mine workers which is moderated by attitudes, behaviour and practice and compliance.
Figure 1.
The relationship between knowledge and exposure to respirable dust exposure among mine workers which is moderated by attitudes, behaviour and practice and compliance.
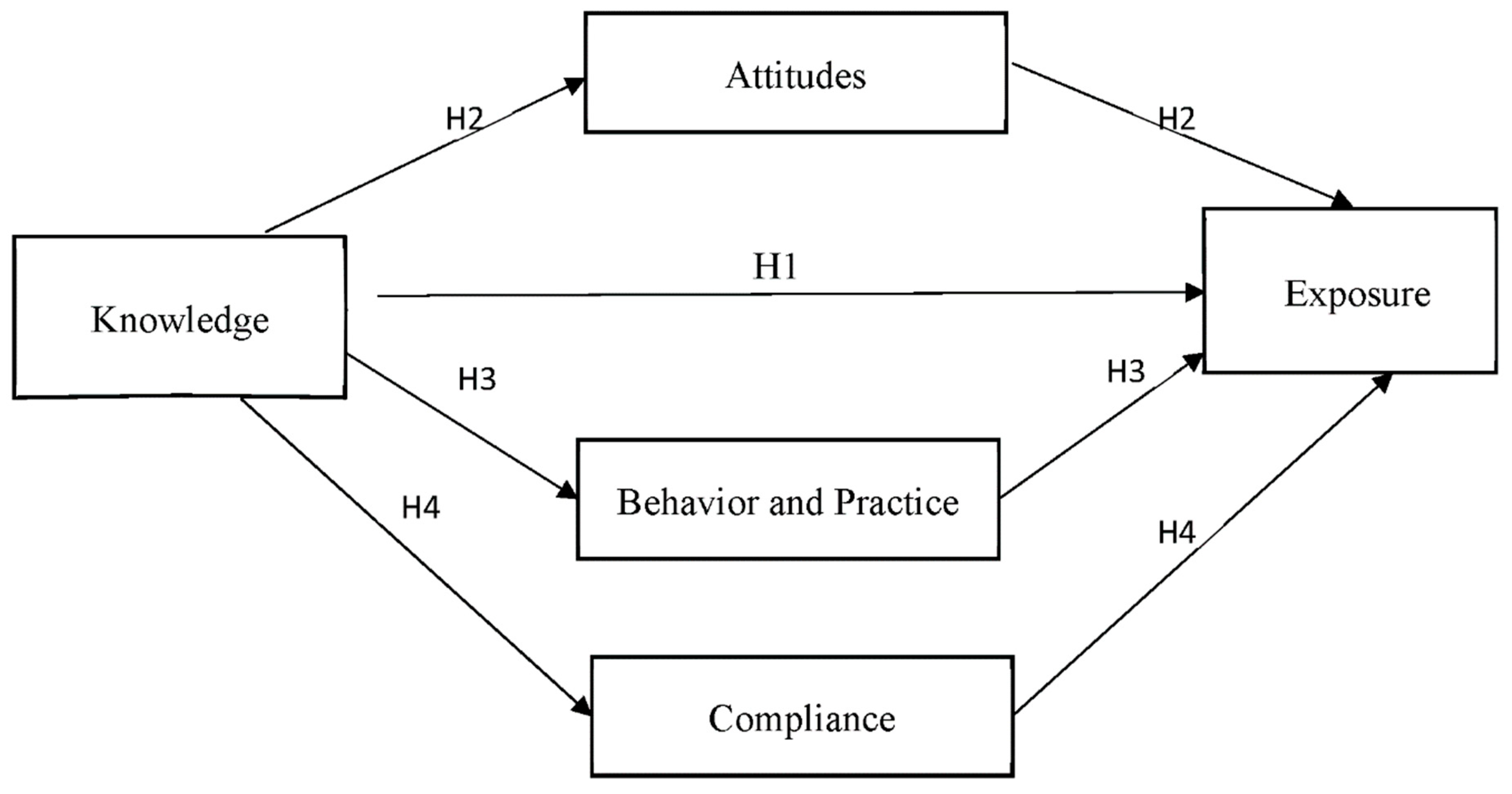
Figure 2.
PLS Path Model Estimation.
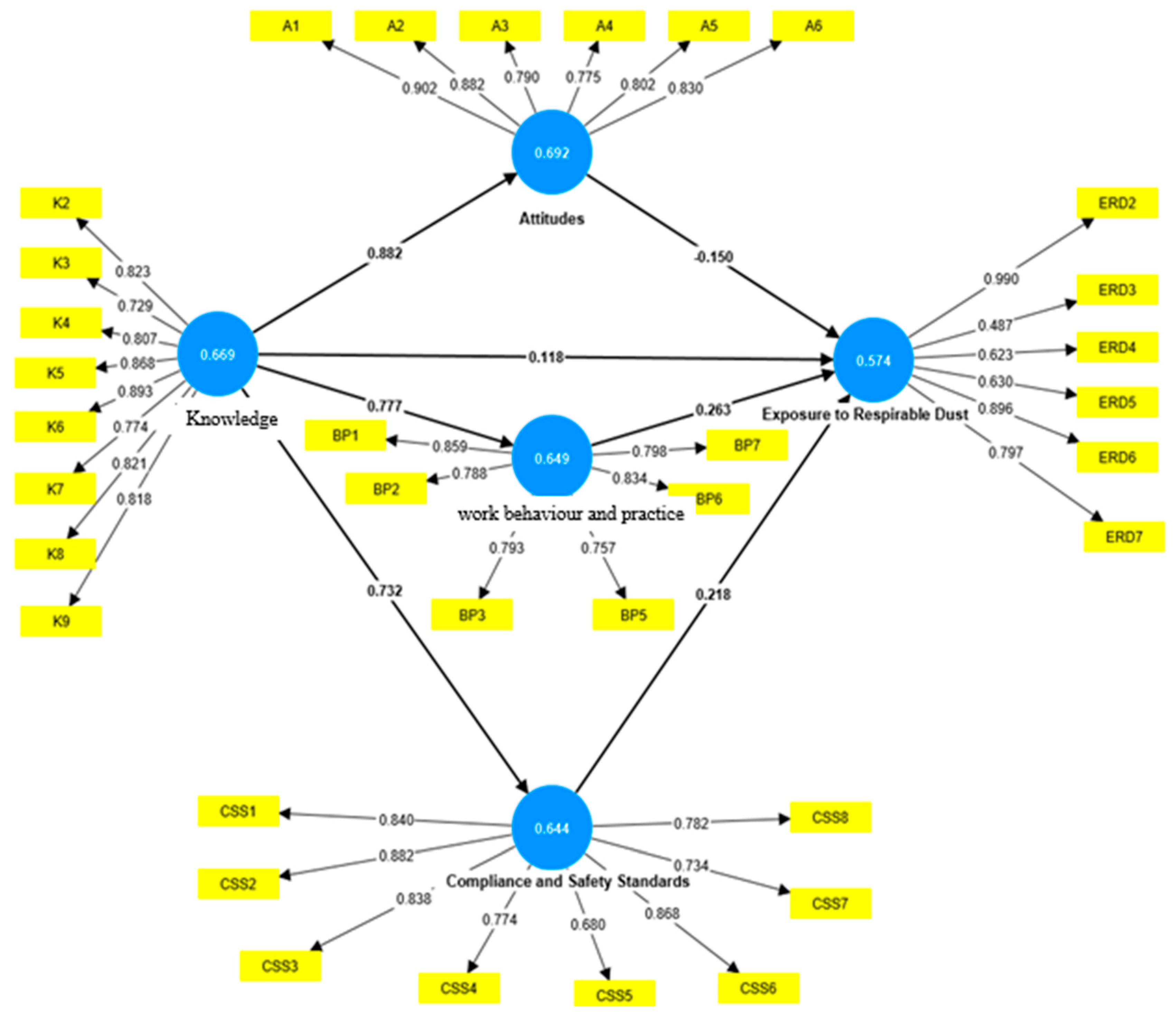

Table 1.
Mean scores for individual items and overall variables organized by work area.
| Variable | Work area | Mean for Individual Items (Range) | Overall Mean Score | Overall Standard Deviation |
|---|---|---|---|---|
| Knowledge | All | 3.31-3.59 | 3.50 | 1.14 |
| Underground | 3.31-3.59 | 3.58 | 1.13 | |
| Surface | 3.43-4.49 | 3.39 | 1.15 | |
| Attitudes | All | 3.37-3.80 | 3.71 | 1.15 |
| Underground | 3.72-3.80 | 3.76 | 1.01 | |
| Surface | 3.37-3.70 | 3.60 | 1.15 | |
| Work behaviour and practice | All | 3.29-3.64 | 3.50 | 1.16 |
| Underground | 3.49-3.64 | 3.59 | 1.20 | |
| Surface | 3.29-3.41 | 3.38 | 1.09 | |
| Compliance with safety standards | All | 3.41-3.64 | 3.53 | 1.06 |
| Underground | 3.31-3.64 | 3.57 | 1.09 | |
| Surface | 3.41-3.49 | 3.47 | 1.03 | |
| Exposure to respirable dust | All | 3.20-3.57 | 3.38 | 0.96 |
| Underground | 3.45-3.57 | 3.48 | 0.92 | |
| Surface | 3.20-3.42 | 3.22 | 0.99 |
(Source: Generated from the Components of Analysis, 2023).
Table 2.
Fornell-Larker Criterion.
| Attitudes | Behavioural Practice | Compliance and Safety Standards | Exposure to Respirable Dust | Knowledgeability | |
|---|---|---|---|---|---|
| Attitudes | 0.865 | ||||
| Work Behaviour and Practice | 0.778 | 0.845 | |||
| Compliance and Safety Standards | 0.751 | 0.835 | 0.831 | ||
| Exposure to Respirable Dust | 0.325 | 0.391 | 0.391 | 0.806 | |
| Knowledge | 0.828 | 0.724 | 0.688 | 0.326 | 0.843 |
(Source: Generated from the Components of Analysis, 2023).
Table 3.
Collinearity Assessment.
| VIF | |
|---|---|
| Attitudes | 3.238 |
| Work Behaviour and Practice | 2.839 |
| Compliance and Safety Standards | 2.849 |
| Exposure to Respirable Dust | 2.227 |
| Knowledge | 2.958 |
(Source: Generated from the Components of Analysis, 2023).
Table 4.
Path Coefficients and Significance Testing Results.
| Sample mean (M) | Standard deviation (STDEV) | t-statistics (|O/STDEV|) | p values | |
|---|---|---|---|---|
| Knowledge -> Exposure to Respirable Dust | 0.085 | 0.079 | 1.103 | 0.27 |
| Knowledge -> Attitudes | 0.828 | 0.015 | 54.139 | 0.00 |
| Knowledge -> Work Behaviour and Practice | 0.723 | 0.026 | 27.627 | 0.00 |
| Knowledge -> Compliance and Safety Standards | 0.688 | 0.027 | 25.61 | 0.00 |
| Attitudes -> Exposure to Respirable Dust | -0.058 | 0.079 | 0.751 | 0.453 |
| Work Behaviour and Practice -> Exposure to Respirable Dust | 0.2 | 0.083 | 2.407 | 0.016 |
| Compliance and Safety Standards -> Exposure to Respirable Dust | 0.211 | 0.086 | 2.429 | 0.015 |
(Source: Generated from the Components of Analysis, 2023).
Table 5.
Results of Hypotheses Testing.
| Hypotheses | Remark | |
|---|---|---|
| H1 | Knowledge of the risks and dangers of respirable dust positively reduces exposure to respirable dust in workers | Not Supported |
| H2 | Knowledge of the risks and dangers of respirable dust is positively moderated by attitudes to reduce respirable dust exposure in workers. | Not Supported |
| H3 | Knowledge of the risks and dangers of respirable dust is positively moderated by work behaviour and practice towards respirable dust exposure | Supported |
| H4 | Knowledge of the risks and dangers of respirable dust is positively moderated by compliance with safety standards towards respirable dust exposure | Supported |
(Source: Generated from the Components of Analysis, 2023).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



