
Submitted:
13 July 2023
Posted:
13 July 2023
You are already at the latest version
Abstract
Background: Epileptic patients frequently encounter cognitive impairment. Functions that are mostly affected involve memory, attention and executive function; however this is mainly dependant on the location of the epileptic activity. The aim of the study is to assess cognitive functions in MRI-negative epilepsy patients by means of neurophysiological and neuropsychological measures. Methods: The patients were enrolled from the outpatient Epilepsy/Clinical Neurophysiology clinic over a time period of 6 months. The study sample comprised 20 MRI negative epilepsy patients [mean age ± standard deviation (SD), 30.3 ± 12.56 years; age range 16-60 years; average disease duration, 13.95 years) and 10 age-matched controls (mean age ± SD, 24.22 ± 15.39 years), that were also education-matched (p>0.05) Patients with epileptogenic lesions were excluded from the study. Informed consent was obtained from all subjects involved in the study. Auditory ERPs and the cognitive screening tool EpiTrack, were administered to all subjects. Results: Latencies of P300 and slow waves were prolonged in patients compared to controls (p<0.05). ASM load and the patients’ performance in the EpiTrack maze subtest were the most significant predictors of P300 latency. A decline in memory, attention, and speed of information processing has been observed in patients with cryptogenic epilepsy compared to age-matched controls, as reflected by P300 latency and EpiTrack scores.
Keywords:
Event Related Potentials
; Epilepsy
; P300
; Anti-Seizure Medication
1. Introduction
Cognitive deficits and behavioral sequels are frequently encountered in patients with epilepsy (in approximately 70% of chronic epilepsy cases). The deleterious effects of epilepsy in patients’ neurobehavioral function can be determined by a variety of causes such as structural brain lesions, seizures, epileptic dysfunction, and medical treatment [1].
Besides the aforementioned chronic and progressive effects of epilepsy on cognition, transient cognitive impairment (TCI), first introduced by Aarts et al., [2], is a transient state of aberrant cognitive function associated with subclinical interictal epileptiform discharges. In this study, 50% of the patients showed transient cognitive impairment that was associated to interictal epileptiform discharges (ED). TCI caused by these epileptiform discharges followed a lateralized pattern ie EDs starting in the left hemisphere caused errors in verbal tasks, while those generated in the right hemisphere caused impairments in non-verbal tests. It seems that EDs cause a temporal disruption of the function of the brain region involved in the generation of the epileptiform activity as well as nearby interconnected area. ED have been often associated to memory impairment, executive dysfunction as well as behavioral disturbances in adults and children with epilepsy.The prevalence of TCI is believed to be low, occurring in approximately 2.2% of patients referred for routine electroencephalogram (EEG). However, others reported a TCI prevalence of 33% [3].
Studies specifically addressing neuropsychological function in cryptogenic epilepsy are relatively scarce [4]. Cognition is more likely impaired in patients suffering seizures of symptomatic than idiopathic and cryptogenic etiology [5,6]. Attention and memory problems have been estimated in about 30% in newly diagnosed patients with single or several seizures of cryptogenic origin [7]. The most important factor in shaping cognitive performance in cryptogenic epilepsy seems to be lower educational status, a fact consistent with cognitive reserve theory in epilepsy [8], while the number of seizure types, epilepsy duration, and polytherapy seems to account, too [9]. An increased number of seizure types leads to the disturbance of more complex brain circuits (e.g., hippocampal circuits) determining neuropsychological impairment in cryptogenic epilepsies [10]. Neuronal loss is also proportional to the duration of epilepsy [11], while adequate treatment can improve cognitive function in previously cognitively impaired patients [9]. The lack of morphological abnormalities is likely to render seizure localization and lateralization more challenging in cryptogenic than in lesional epilepsy. In such cases, neuropsychological assessment may be of help in the detection of the epileptogenic zone. These patients are also at increased risk for postoperative cognitive decline when neurosurgery is considered to control their seizures [9].
TCI has also been studied in animal models, although studies observing the acute effect of ED on cognitive functions are fewer compared to human studies. Petrucco et al [12] studied epileptic activity in the visual cortex of mouse models and observed that cortical processing can be impaired in areas that are far from the brain region responsible for the generation of EDs. The results of this study agrees with several EEG and fMRI studies in humans that observed changes of the BOLD signal in brain structures far from the epileptic generator [13]. Therefore, it seems that the propagation of ED to connected brain regions may also contribute to TCI. [14]
A representative example of how chronic epileptiform activities cause neurodevelopmental deficits is observed in epileptic encephalopathies such as Landau-Kleffner and West syndrome. On the other hand, in epileptic syndromes like Dravet syndrome cognitive impairment is not only due to EEG abnormalities, but also to the underlying genetic pathology of the syndrome [15]
Event-related potentials (ERPs) reflect the summed activity of postsynaptic potentials and are generated when millions of similarly oriented pyramidal neurons depolarize synchronously in response to an infrequent or so called “target” stimulus [16]. P300 wave is a positive deflection that occurs at a latency of about 300 ms after stimulus onset It is elicited by the selection of a specific processing information strategy, while it depends on the way a subject is akin to respond to future stimuli; it reflects expectancies formation process, strategic solutions, and memory processing [17]. P300 amplitude represents cognitive events underlying "tasks that are required in the maintenance of working memory" [18], since it is an ERP component thought to reflect updating operations of the stimulus context [19,20]. P300 latency has been linked to the speed of stimulus classification during memory-updating [21]. In healthy subjects, P300 latency negatively correlates with the timing of attentional allocation processes that varies across individuals [22]. In general two P300 components are described [14] . The earlier frontocentral P3a component that occurs when the subject is presented with an unexpected stimulus in the absence of any prior instruction and the temporoparietal P3b component that reflects update in working memory processes following the presentation of new information according to the context updating theory (Figure 1)
P300 wave has been previously studied as a marker of cognitive dysfunction in numerous neurological diseases, including epilepsy, since it reflects attention and memory processing [6,10]. Studies of P300's characteristics in epileptic patients have mainly observed increased P300 latencies and lower P300 amplitudes compared to normal subjects. Prolonged P300 latency has been linked to reduced speed of information processing [18]. This study aimed to evaluate cognitive processing in patients suffering cryptogenic epilepsy by means of neurophysiological and neuropsychological measures and seek possible correlations.
2. Materials and Methods
This study was conducted at the Laboratory of Clinical Neurophysiology in AHEPA University Hospital of Thessaloniki after approval by the research ethics committee of the International Hellenic University. The patients were enrolled from the outpatient Epilepsy/Clinical Neurophysiology clinic over a time period of 6 months. The study sample comprised 20 epilepsy patients that were followed regularly in the outpatient cliniv with no identifiable etiological lesion detected on MRI imaging (MRI-negative epilepsy) [mean age ± standard deviation (SD), 30.3 ± 12.56 years; age range 16-60 years; average disease duration, 13.95 years) and 10 age-matched controls (mean age ± SD, 24.22 ± 15.39 years), that were also education-matched (p>0.05) Patients with epileptogenic lesions were excluded from the study. The diagnosis was made by experienced adult neurologists specialized in epilepsy. The participants underwent thorough neurological examination and structural brain MRI (high-resolution T1, T2, FLAIR, and diffusion-weighted imaging sequences) before inclusion in this study. All participants provided written informed consent. The anti-seizure medication (ASM) load was calculated using the ratio of the prescribed daily dose to the defined daily dose (DDD). DDD is the assumed average daily drug dose defined by WHO . Our patients were all set in polytherapy regimen with mainly Levetiracetam (LEV) and valproic acid (VAP).
2.1. Neuropsychological testing
EpiTrack, a brief screening tool for detecting cognitive impairment, was administered to all patients by a trained psychologist. This tool comprises six subtests (the Trail-Making Test A & B parts, a test of response inhibition, digit span backward, written word fluency, and a maze test) covering the domains of processing speed, planning, word fluency, and working memory [23]. It is especially sensitive to cognitive changes associated with antiepileptic medication. The duration of the test was approximately 10–15 min. The maximum score is 49 points and the cutoff for significant impairment is ≤ 28 points
2.2. Recording parameters
Auditory ERPs were assessed using a Nihon Kohden Neuropack MEB2300 device. All participants were subjected to the classic oddball paradigm with binaural auditory stimuli at 70 dB sound pressure level and a 10-ms rise/fall and a 100-ms plateau time, presented by earphones. The auditory stimuli were presented in a random sequence with target tones (oddball) of 2000 Hz that occurred 20% of the time and standard tones of 1000 Hz that occurred 80% of the time at a 0.5-Hz rate. All subjects were asked to press a button with their right thumb after every oddball tone was heard, and the reaction time (RT) was subsequently measured.
EEG activity was recorded (filter bandpass, 0.1–50 Hz; analysis time, 1 s) using scalp AgCl electrodes affixed with electrode paste (Elefix Nihon Kohden, EEG paste Z-401 CE) at Fz, Cz, CPz, Pz, T3 and T4 sites according to the 10/20 system referred to linked earlobe electrodes, with a left hand ground. All electrode impedances were <5 kΩ. [24].
Thirty responses recorded by the target stimuli were averaged, and data from two consecutive trials were obtained. Latencies and amplitudes of N200, P300, and SW, recorded from the Cz site, were considered for this study. In seven patients, epileptiform discharges (ED) occurred during ERP acquisition. ED were defined as spike and/or sharp wave discharges alone or followed by slow waves which clearly stand out from background rhythms. The short-term impact of EDs on cognition was tested by calculating ERPs and RTs in two different conditions: with and without EDs.
2.3. Statistical analysis
Statistical analysis was performed using SPSS 23.0 for Windows (SPSS, Inc., Chicago). All data were normally distributed (Shapiro–Wilk test). Neuropsychological test scores and ERP parameters of the two groups were compared using an unpaired Student’s t-test. The linear relations between the neurophysiological (ERP parameters) and neuropsychological test scores (EpiTrack total score and subtest scores) were studied using Pearson’s correlation r. Multiple regression analysis was performed with P300 wave latency as the dependent variable P <0.05 was considered statistically significant.
3. Results
Demographical and clinical characteristics of the patients and controls are shown in Table 1. The grand average ERP waveforms of each electrode site are depicted in Figure 2. The mean ± SD P300 latency was 359.73 ± 39.1 ms in the patients and 318.13 ± 23 ms in the controls. P300 and SW latencies were significantly longer in patients than controls (P = 0.005 and P = 0.05, respectively).
The mean amplitude of the P300 wave was 16.11 mV in patients and 17.86 mV in controls, with no statistically significant differences (P = 0.6). Conversely, a statistically significant difference was evident in the Trail-Making A and B subtests of EpiTrack (Table 2). Significant negative correlations were observed between P300 latency and all EpiTrack subtests (P < 0.05).
In patients who developed ED during EEG recording, the total number of single trials with EDs was 300, and that without EDs was 683.
No difference was observed between ERP characteristics of N200, P300, SW waves and RT (P > 0.05) in single trials with or without ED.
P300 latency and the interference subtest of EpiTrack were significantly correlated with ASM load (P = 0.041 and P = 0.023, respectively). Multiple regression analysis with P300 latency as dependent variable, revealed that ASM load and the patients’ performance in the EpiTrack maze subtest were the most significant predictors of P300 latency (R=0.802, F=2.702; p<0.05). No association was found between the disease duration and ERP characteristics.
4. Discussion
A decline in memory, attention, and speed of information processing has been observed in patients with cryptogenic epilepsy compared to age-matched controls, as reflected by P300 latency and EpiTrack scores. This was mostly due to ASM load, a finding that agrees with those of previous studies [25,26]. ASM effects are considered to be toxic for cognitive functions since their negative impact on attention, RTs, and speed of information processing. A few studies have assessed ASM effects on cognition by means of neurophysiological markers such as ERPs. In particular, Chen et al [27], showed that phenobarbital increased P300 latency, which was unaffected by VAP and carbamazepine. Data from both healthy volunteers and epilepsy patients suggest that LEV exerts few adverse effects on cognition [28,29] while among the older generation ASMs, VAP, carbamazepine and phenytoin are less aggressive with respect to cognitive functions with relatively little effects on concentration, memory, information processing speed or word fluency [30]. Interestingly, evidence on ASMs’ cognitive side effects over short periods of up to a year remains inconclusive because of methodological issues. Overall, older ASMs (e.g., phenobarbital) have a more negative impact on cognition than placebo, nondrug condition, and newer ASMs, with the exception of topiramate that has the greatest risk of cognitive impairment irrespective of the comparator group [28]
Although early evidence report a significant correlation between the serum concentration of ASM and the P300 [31,32], others [33,34] however failed to replicate these findings. In line with the latter studies, Soysal and associates [35], found a greater prolongation of the P300 latency in cryptogenic focal epilepsy as to their age matched control group, pointing to the role of the type of epilepsy rather that of the type or serum level of ASM.
Evidence [36] on patients with cryptogenic focal epilepsy of temporal and extra temporal origin points to the influence of epileptic activity on the prefrontal network integrity as a possible underlying problem of memory impairment. This study showed impaired working memory and encoding, which represent processing milestones for episodic memory. Such findings are related to reduce functional connectivity in the prefrontal areas, rather than to hippocampal pathology as in the case of mesial temporal lobe epilepsy.
Working memory impairment links to aberrant prefrontal cortex dynamics [37]. In particular, the frontal prominence of classical generalized 3/sec spike-wave absences may be of help in understanding ictal neurobehavioral phenomena arising within the frontal lobes. From a neuropsychological point of view, the distinctive type of disturbed consciousness in classical absences is supposed to rely upon the ictal “arrest of the working memory” [38]. This may also serve to account for working memory impairments in cryptogenic epilepsies, since working memory represents the very early, transient aspects of information processing [39]
Several previous studies have shown significant correlations between P300 latencies and neuropsychological tests performance. In particular, an inverse correlation was observed between P300 latency and the total scores of the Wechsler Intelligence Scale for Children-Revised (WISC-R) and those of the Wechsler memory scale in pediatric epilepsy [33]. In the present study, P300 latency correlated with all EpiTrack subtests, and a statistical significance was evident. Our patients’ decreased performance in Trail-Making A and B subtests is suggestive of problems in visual scanning, concentration and motor speed, as well as dividing and shifting attention (mental flexibility), respectively. ASM exert their negative influence on cognition by suppressing neuronal excitability or enhancing neuronal inhibition. Attention, vigilance, and psychomotor speed are among the most common domains affected by ASM, a fact also observed in our patients’ in Trail-Making A performance. Secondary effects can also manifest on other aspects of cognition, as problems with executive functions. Depressed Trail-Making B performance may either link to executive dysfunction and/or the known secondary-systemic effects of arousal deregulation (see below[40]), the latter emphasizing the role of aberrant reticulo-thalamo-cortical functional rapports in determining, among other clinical factors, cognitive malfunction.
We herewith found that the Porteus Maze test, a measure of executive functioning and visuospatial abilities (planning and foresight) emerged as an important predictor of patients’ overall cognitive impairment, a finding consistent with existing studies, which highlight the presence of executive dysfunction in adolescents suffering Idiopathic Generalized Epilepsy (IGE) [e.g., 1]. In addition, we found no association between disease duration and ERPs characteristics, in line with previous evidence [12].
Our findings are likely to replicate those of previous research, which revealed impaired speed of information processing in patients with epilepsy [41,42]. Speed of information processing is a salient neuropsychological affection in patients with MRI-negative epilepsy, a fact possibly linking to the pathophysiological processes underling epilepsy and the effects of ASM load than with interictal epileptic activity [21,22]. Recently it has been suggested that IGE patients’ neuropsychological deficits may represent indirect-secondary manifestations of a primary cortical tone deregulation inherent to IGEs’ pathophysiology. In particular, IGEs’ worse auditory-vigilance- and -inhibitory control performance, as compared to its visual counterpart, seems to account for a greater vulnerability of the auditory information processing system to the effects of idiopathic generalized seizures [40]. These findings may apply to our patients’ affected auditory oddball P300 latency and executive and visuospatial dysfunction, since the frontal lobes, especially the right one, are likely to modulate the arousal levels to produce adequate orientation responses towards the at hand task. The prefrontal cortex disposes rich bilateral connections with the inferior parts of the reticular formation strongly contributing to cortical tone modulation, which is modified in the light of various tasks demands, and through the mediation of language i.e., a given “problem’s’” formulation induces orienting responses and thus a raise of vigilance [43].
We were unable to identify any TCI in those few patients presenting frequent EDs, a fact that may be partly due to the small-sized group, as well as the brief duration of the neuropsychological measures implemented, constituting a limitation of this study. Future studies may benefit from the administration of Continuous Performance Tests in which larger time interval transient aberrant neurophysiological phenomena may arise. Consequently, we can only speculate that a direct impact of EDs on cognitive functions may not be as prominent in epilepsy patients as mentioned in other studies [2]. Various factors may account for the above finding: First, most EDs occurred during non-target stimuli, and only a small percentage of them occurred during target stimuli typically eliciting P300; this is in accordance with evidence [44] showing TCI when EDs occurred during a stimulus. Second, the type of ED may also affect the occurrence of TCI. Patients with generalized discharges of >3s are more likely to develop TCI than those with focal ED or with generalized discharges of <3 s [45]. Possibly, an ERP paradigm, making use of more demanding task, should be implemented to detect TCI more accurately in patients with increased frequency of EDs. Thus, conclusions of this study should be considered with caution, since further research with larger sample size is needed to obtain evidence that is more reliable. Moreover, as observed in previous ERP studies, the P300 wave is a reliable and robust electrophysiological marker for objectively assessing cognitive functions in patients with epilepsy, and the combined approach with sensitive neuropsychological screening tools, such as EpiTrack, can provide valuable and accurate data for detecting and evaluating cognitive deficits in patients with epilepsy. Hopefully, future studies including wider neuropsychological batteries assessing multiple cognitive domains along with their registered ERPs would address more carefully the issue of cognitive impairment and its’ neurophysiological correlates in cryptogenic epilepsy.
Author Contributions
Conceptualization, V.P. an V.K.K..; methodology, V.P., M.K., M.A., V.K.K. formal analysis, V.P, P.P..; investigation, C.L., M.S., T.A..; resources, X.X.; data curation, X.X.; writing—original draft preparation, V.P., V.K..; writing—review and editing, V.P., V.K.K.., P.P.; supervision, V.K.K., M.K project administration, V.P., G.Z.. All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The results were presented as conference abstract with title: Cognitive impairment in MRI-negative epilepsy: Relationship between neurophysiological and neuropsychological assessments. EPR 2046 EAN Lisbon 2018.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gelžinienė G, Jurkevičienė G, Marmienė V, Adomaitienė V, Endzinienė M. Executive functions in adolescents with idiopathic generalized epilepsy. Medicina (Kaunas) 2011, 47, 313–319.
- Aarts JHP, Binnie CD, Smith AM, Wilkins AJ. Selective cognitive impairment during focal and generalised epileptiform EEG activity. Brain. 1984, 107, 293–308. [CrossRef] [PubMed]
- Fonseca LC, Tedrus GM, Lalloni DT, Tella LM, Maluf P, Sousa VD. [Transient cognitive impairment during generalized or diffuse epileptiform EEG discharges]. Arq Neuropsiquiatr. 2005, 63, 817–24.
- Mataró, M.; Junqué, C.; Viñas, J.; Escartín, A. Learning and memory skills in patients with cryptogenic epilepsy. Neurologia 1996, 11, 280–6. [Google Scholar] [PubMed]
- Meador, K.J. Cognitive outcomes and predictive factors in epilepsy. Neurology 2002, 58, S21–S26. [Google Scholar] [CrossRef]
- Bulteau C, Jambaque I, Viguier D, Kieer V, Dellatolas G, Dulac O. Epileptic syndromes, cognitive assessment and school placement: a study of 251 children. Dev Med Child Neurol 2000, 42, 319–27. [CrossRef] [PubMed]
- Kälviäinen, R.; Äikiä, M.; Helkala, E.-L.; Mervaala, E.; Riekkinen, P.J. Memory and attention in newly diagnosed epileptic seizure disorder. Seizure 1992, 1, 255–262. [Google Scholar] [CrossRef]
- Pai, M.-C.; Tsai, J.-J. Is Cognitive Reserve Applicable to Epilepsy? The Effect of Educational Level on the Cognitive Decline After Onset of Epilepsy. Epilepsia 2005, 46, 7–10. [Google Scholar] [CrossRef]
- Huang, C.-W.; Hsieh, Y.-J.; Tsai, J.-J.; Pai, M.-C. Cognitive performance in cryptogenic epilepsy. Acta Neurol. Scand. 2005, 112, 228–233. [Google Scholar] [CrossRef]
- Kotloski, R.; Lynch, M.; Lauersdorf, S.; Sutula, T. Repeated brief seizures induce progressive hippocampal neuron loss and memory deficits. Prog Brain Res 2002, 135, 95–110. [Google Scholar] [CrossRef]
- Fuerst D, Shah J, Kupsky W et al. Is hippocampal sclerosis a progressive disorder? A volumetric MRI, pathological and neuropsychological study. Neurology 2001, 57, 184–8. [CrossRef]
- Petrucco L., Pracucci E., Brondi M., Ratto G. M., Landi S. Epileptiform activity in the mouse visual cortex interferes with cortical processing in connected areas. Sci. Rep. 2017, 7, 40054. [CrossRef]
- Kobayashi, E. , Bagshaw A. P., Jansen A., Andermann F., Andermann E., Gotman J., et al. Intrinsic epileptogenicity in polymicrogyric cortex suggested by EEG-fMRI BOLD responses. Neurology. 2005, 64, 1263–1266. [Google Scholar] [CrossRef] [PubMed]
- Ung, H.; Cazares, C.; Nanivadekar, A.; Kini, L.; Wagenaar, J.; Becker, D.; Krieger, A.; Lucas, T.; Litt, B.; Davis, K.A. Interictal epileptiform activity outside the seizure onset zone impacts cognition. Brain 2017, 140, 2157–2168. [Google Scholar] [CrossRef] [PubMed]
- Landi, S.; Petrucco, L.; Sicca, F.; Ratto, G.M. Transient Cognitive Impairment in Epilepsy. Front. Mol. Neurosci. 2019, 11, 458. [Google Scholar] [CrossRef] [PubMed]
- Artemiadis, A.K.; Fili, M.; Papadopoulos, G.; Christidi, F.; Gatzonis, S.; Zalonis, I.; Nikolaou, G.; Triantafyllou, N. Auditory event-related potentials (P300) and mesial temporal sclerosis in temporal lobe epilepsy patients. Epileptic Disord. 2014, 16, 67–73. [Google Scholar] [CrossRef]
- Zhong, R.; Li, M.; Chen, Q.; Li, J.; Li, G.; Lin, W. The P300 Event-Related Potential Component and Cognitive Impairment in Epilepsy: A Systematic Review and Meta-analysis. Front. Neurol. 2019, 10, 943. [Google Scholar] [CrossRef] [PubMed]
- Polich, J. Updating P300: An integrative theory of P3a and P3b. Clin. Neurophysiol. 2007, 118, 2128–2148. [Google Scholar] [CrossRef]
- Dien, J.; Spencer, K.M.; Donchin, E. Localization of the event-related potential novelty response as defined by principal components analysis. Cogn. Brain Res. 2003, 17, 637–650. [Google Scholar] [CrossRef]
- Gratton, G.; Bosco, C.M.; Kramer, A.F.; Coles, M.G.; Wickens, C.D.; Donchin, E. Event-related brain potentials as indices of information extraction and response priming. Electroencephalogr. Clin. Neurophysiol. 1990, 75, 419–432. [Google Scholar] [CrossRef]
- Steiner GZ, Barry RJ, Gonsalvez CJ. Can working memory predict target-to-target interval effects in the P300? Int J Psychophysiol. 2013, 89, 399–408. [CrossRef]
- van Dinteren, R.; Arns, M.; Jongsma, M.L.A.; Kessels, R.P.C. P300 Development across the Lifespan: A Systematic Review and Meta-Analysis. PLOS ONE 2014, 9, e87347. [Google Scholar] [CrossRef] [PubMed]
- Lutz, M.; Helmstaedter, C. EpiTrack: Tracking cognitive side effects of medication on attention and executive functions in patients with epilepsy. Epilepsy Behav. 2005, 7, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Papaliagkas, V.; Kimiskidis, V.; Tsolaki, M.; Anogianakis, G. Usefulness of event-related potentials in the assessment of mild cognitive impairment. BMC Neurosci. 2008, 9, 107–107. [Google Scholar] [CrossRef]
- Deckers, C.L.P.; Hekster, Y.A.; Keyser, A.; Meinardi, H.; Renier, W.O. Reappraisal of polytherapy in epilepsy: a critical review of drug load and adverse effects. Epilepsia 1997, 38, 570–575. [Google Scholar] [CrossRef]
- Witt, J.-A.; Elger, C.E.; Helmstaedter, C. Adverse cognitive effects of antiepileptic pharmacotherapy: Each additional drug matters. Eur. Neuropsychopharmacol. 2015, 25, 1954–1959. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.-C.; Tsai, S.-Y.; Chang, Y.-C.; Liou, H.-H. Seizure frequency affects event-related potentials(P300) in epilepsy. J. Clin. Neurosci. 2001, 8, 442–446. [Google Scholar] [CrossRef]
- Park, S.-P.; Kwon, S.-H. Cognitive Effects of Antiepileptic Drugs. J. Clin. Neurol. 2008, 4, 99–106. [Google Scholar] [CrossRef]
- Moavero, R.; Santarone, M.E.; Galasso, C.; Curatolo, P. Cognitive and behavioral effects of new antiepileptic drugs in pediatric epilepsy. Brain Dev. 2017, 39, 464–469. [Google Scholar] [CrossRef]
- Brückner, K. E. (2020). Cognitive and Psychological Side Effects of Antiepileptic Drugs. In Epilepsy-Update on Classification, Etiologies, Instrumental Diagnosis and Treatment. IntechOpen.
- van Rijckevorsel-Harmant, K.; Flahaut, D.; Harman, J.; de Barsy, T. Event-Related Potentials and Cognitive Functions in Epileptic Treated Patients. Clin. Electroencephalogr. 1990, 21, 67–73. [Google Scholar] [CrossRef]
- Naganuma, Y.; Konishi, T.; Hongou, K.; Murakami, M.; Yamatani, M.; Yagi, S.; Okada, T. Auditory Event-related Potentials in Benign Childhood Epilepsy with Centrotemporal Spike: The Effects of Carbamazepine. Clin. Electroencephalogr. 1994, 25, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Naganuma, Y.; Konishi, T.; Matsui, M.; Hongou, K.; Murakami, M.; Yamatani, M.; Okada, T. [The relationship between P300 latencies, and WISC-R and Wechsler memory scale results in epileptic children]. No hattatsu. Brain Dev. 1993, 25. [Google Scholar]
- Helmstaedter C, Witt JA. Epilepsy and cognition - A bidirectional relationship? Seizure 2017, 49, 83–89. [CrossRef] [PubMed]
- Soysal, A.; Atakli, D.; Atay, T.; Altintas, H.; Baybas, S.; ArpacI, B. Auditory event-related potentials (P300) in partial and generalized epileptic patients. Seizure 1999, 8, 107–110. [Google Scholar] [CrossRef]
- Vlooswijk, M.C.G.; Jansen, J.F.A.; Jeukens, C.R.L.P.N.; Majoie, H.J.M.; Hofman, P.A.M.; de Krom, M.C.T.F.M.; Aldenkamp, A.P.; Backes, W.H. Memory processes and prefrontal network dysfunction in cryptogenic epilepsy. Epilepsia 2011, 52, 1467–1475. [Google Scholar] [CrossRef]
- Funahashi, S. Working Memory in the Prefrontal Cortex. Brain Sci. 2017, 7, 49. [Google Scholar] [CrossRef] [PubMed]
- Niedermeyer, E. Frontal Lobe Epilepsy: The Next Frontier. Clin. Electroencephalogr. 1998, 29, 163–169. [Google Scholar] [CrossRef]
- Baddeley, A. D. Baddeley, A. D., & Hitch, G. (1974). Working memory. In Psychology of learning and motivation (Vol. 8, pp. 47-89); Academic press.
- Patrikelis, P.; Lucci, G.; Fasilis, T.; Korfias, S.; Messinis, L.; Kosmidis, M.H.; Lagogianni, C.; Konstantakopoulos, G.; Manolia, S.; Sakas, D.; et al. Selective impairment of auditory attention processing in idiopathic generalized epilepsies: Implications for their cognitive pathophysiology. Appl. Neuropsychol. Adult 2020, 29, 1131–1140. [Google Scholar] [CrossRef]
- Novak, A.; Vizjak, K.; Rakusa, M. Cognitive Impairment in People with Epilepsy. J. Clin. Med. 2022, 11, 267. [Google Scholar] [CrossRef]
- McMillan, T.M.; Mason, C.A.; Seidenberg, M.; Jones, J.; Hermann, B. The impact of processing speed on cognition in temporal lobe epilepsy. Epilepsy Behav. 2021, 122, 108203. [Google Scholar] [CrossRef]
- Luria, A. R. (1976). The working brain: An introduction to neuropsychology.
- Binnie, C.; Trenité, D.K.-N.; Smit, A.; Wilkins, A. Interactions of epileptiform EEG discharges and cognition. Epilepsy Res. 1987, 1, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Binnie, CD. Cognitive impairment during epileptiform discharges: is it ever justifiable to treat the EEG? Lancet Neurol. 2003, 2, 725–730 515. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Context updating theory of P300 (Adopted by Polich [18]).
Figure 1.
Context updating theory of P300 (Adopted by Polich [18]).
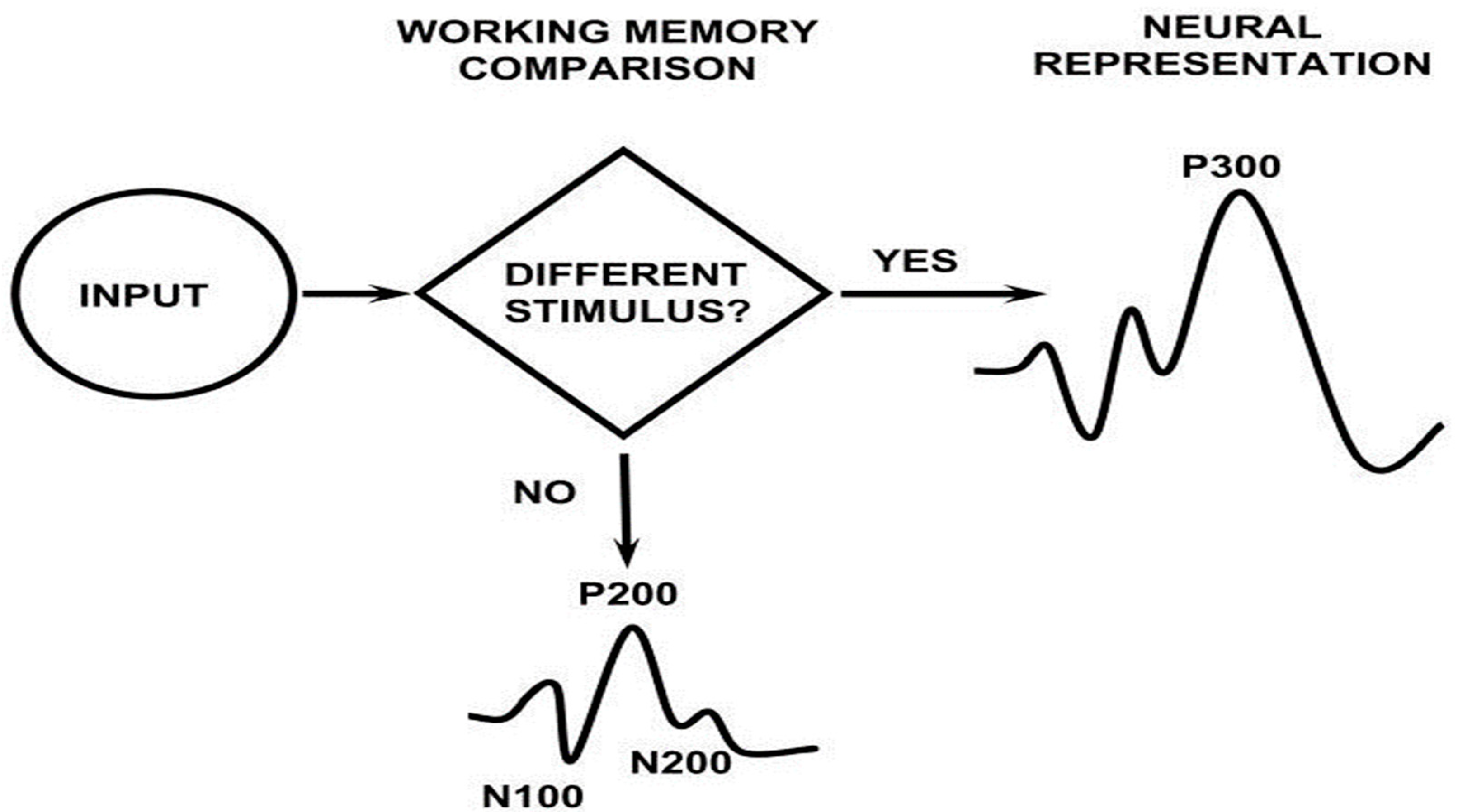
Figure 2.
Average of ERP waveforms in epileptic patients recorded with the following electrodes: A11, Fz; A21, Cz; A31, CPz; A41, Pz; A51, T3; A61, T4. The recording with Cz electrode is depicted in green.
Figure 2.
Average of ERP waveforms in epileptic patients recorded with the following electrodes: A11, Fz; A21, Cz; A31, CPz; A41, Pz; A51, T3; A61, T4. The recording with Cz electrode is depicted in green.
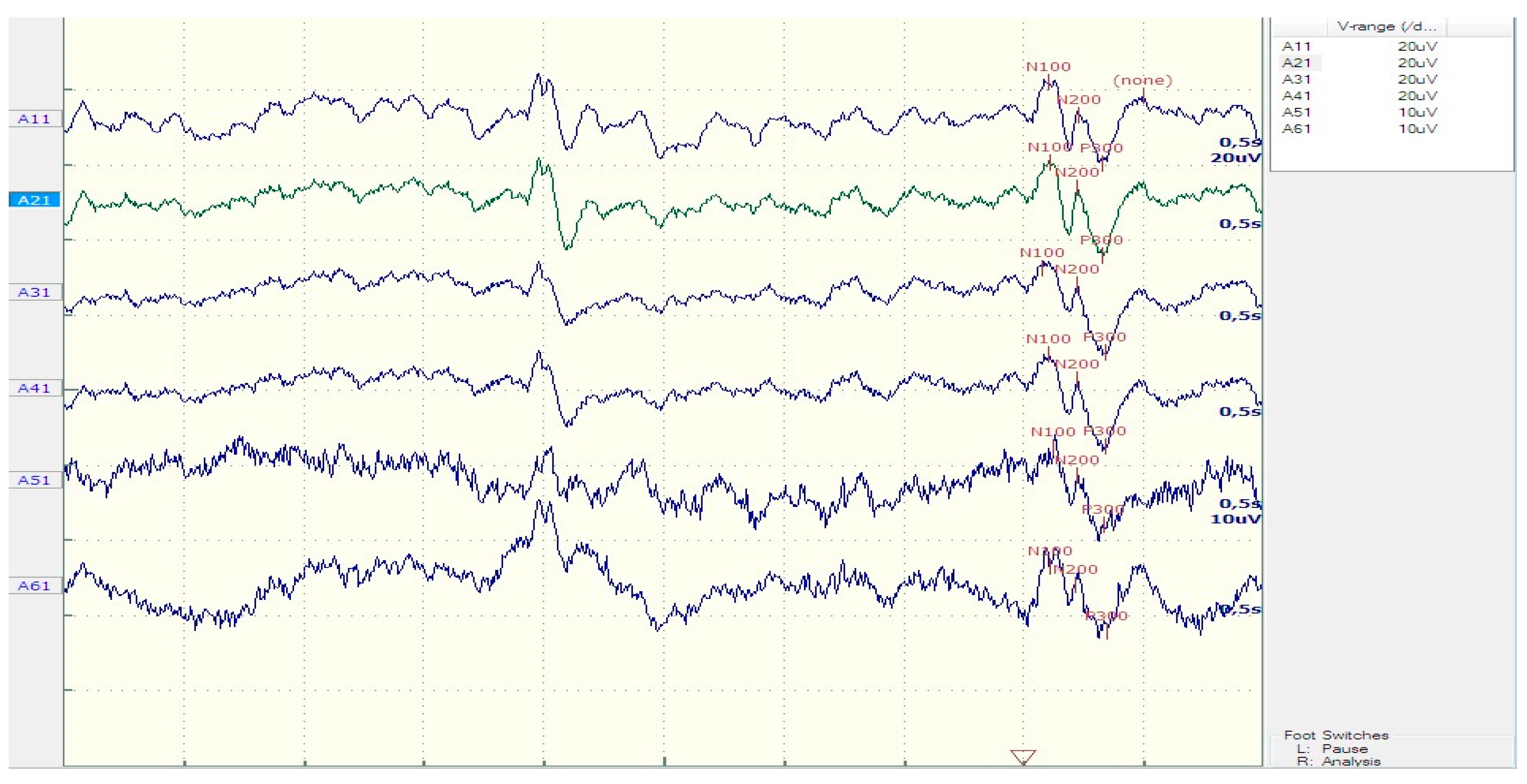

Table 1.
Demographic and ERP characteristics of patients and controls.
| Patients | Controls | t-test (P) | |
|---|---|---|---|
| Age (years) | 30.3 ± 12.56 | 24.22 ± 15.39 | 0.07 |
| N200 latency (ms) | 223.75 ± 26.9 | 212.5 ± 18.3 | 0.23 |
| P300 latency (ms) | 359.73 ± 39.1 | 318.13 ± 23 | 0.005* |
| Sw latency (ms) | 492.36 ± 50.72 | 451.25 ± 41.1 | 0.05* |
| N200 amplitude (μV) | 8.64 ±3.8 | 7.83 ±1.85 | 0.52 |
| P300 amplitude (μV) | 16.12 ±7.45 | 17.86 ±7.02 | 0.59 |
| Reaction time (ms) | 900.25 ± 206.9 | 833.38 ± 94 | 0.59 |
statistically significant correlations are marked with an asterisk (*).
Table 2.
Performance of patients and controls in Epitrack subtests.
| Patients | Controls | t-test (P) | |
|---|---|---|---|
| Total Score | 26.94± 3.77 | 29.87± 2.16 | 0.055 |
| Interference | 5.44± 1.03 | 5.75± 0.7 | 0.62 |
| Trail A | 5.31 ± 0.79 | 6 ± 0.53 | 0.038* |
| Trail B | 5.31 ± 1.01 | 6.12 ± 0.35 | 0.040* |
| Maze | 5.68±1.19 | 6.37 ±0.51 | 0.137 |
| Verbal fluency test | 5.06 ±0.85 | 5.62 ±0.74 | 0.128 |
| ASM load | 2.54 ±1.70 |
statistically significant correlations are marked with an asterisk (*).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



