
Submitted:
12 July 2023
Posted:
13 July 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
During one of the worst global health crises, millions of people were vaccinated against SARS-CoV-2. In rare cases, new onset systemic inflammatory diseases were reported with temporal coincidence to the vaccination. We describe a case of severe Eosinophilic Granulomatosis with Polyangiitis (EGPA) in a young asthmatic woman, occurring after a 2nd dose of mRNA-1273 vaccine. She presented with multisystem EGPA with cardiac and central nervous system involve-ment, complicated by secondary immune thrombocytopenia (ITP). We review the reported cases of EGPA coinciding with SARS-CoV-2 mRNA vaccination. All potentially vaccine-related EGPA cases reported so far occurred within 14 days from immunization.
EGPA is very rare with an incidence of 1:1’000’000 inhabitants and the number of reported post-vaccination EGPA cases lies within the expected incidence rate for the period.
While we cannot prove a causal relationship between the vaccine and EGPA onset, the temporal relationship with the vaccine immune stimulation is intriguing, in a disease occurring almost always in adults with asthma and/or chronic rhinosinusitis and driven by an aberrant Th2 lym-phocyte activation with hypereosinophilia.
Nevertheless, cases of inflammatory diseases emerging in the context of vaccination remain rare and the benefits of preventing severe Covid presentations with SARS-CoV-2 mRNA vaccines remains unquestionable.
Keywords:
Eosinophilic Granulomatosis with Polyangiitis
; SARS-CoV-2 mRNA vaccine
; immune thrombocytopenia
1. Introduction
During the SARS-CoV-2 global health crisis, hundreds of millions of people were immunized against SARS-CoV-2 with various vaccines. In Switzerland, approximately 6 million people received at least one dose of mRNA SARS-CoV-2 vaccine by November 2022.[1]. From January 2021 to March 2022, the Swiss Agency for Therapeutic Products (Swissmedic) evaluated 13,388 reports of suspected adverse events to the vaccines, with mRNA 1273 vaccine accounting for 68% of cases [2]. About 38% of adverse events were classified as serious. In rare cases there were reports of immune-mediated inflammatory diseases (IMID) flares or even new-onset IMID after SARS-CoV-2 vaccines.[3] We report here a severe case of Eosinophilic Granulomatosis with Polyangiitis (EGPA), occurring in temporal relationship with SARS-CoV-2 vaccination and complicated by immune thrombocytopenia (ITP). This adds to the few reports of flares and new onset EGPA after mRNA vaccines reviewed below [4–8].
2. Materials and Methods
We describe a severe case of EGPA with multisystem manifestations complicated by ITP after mRNA SARS-CoV-2 vaccination. We also present other similar cases found in the literature, which are resumed in Table 1.
3. Case Presentation
A 46-year-old woman of European descent developed fever, asthenia and myalgia the day after her second dose of mRNA-1273 vaccine. She was known for allergic rhinosinusitis and moderate asthma but had no other health issues. The patient never tested positive for SARS-CoV-2 and the first vaccine, a month earlier, was well tolerated. Four days after the initial symptoms she developed severe watery diarrhoea with vomiting and consulted the emergency room. Upon admission, she was hemodynamically stable. Her temperature was 38°C and her oxygen saturation was normal. The abdomen was tender without guarding. The remaining clinical examination was normal. Blood test showed leucocytosis 17.6 G/l (reference range: 4-10) with neutrophilia 14 G/l (ref. 1.8-7.5), eosinophilia 1.2 G/l (< 0.3), and cholestasis. Eosinophilia increased, peaking at 8.4 G/l (Figure 1).
Total serum IgE was 1361 kU/l (ref. 5-50 kU/l). IgG 4 levels were in the normal range. Extensive search for parasitic, viral, and bacterial infection was negative, as were anti-neutrophil cytoplasmic antibodies (ANCA). Abdominal MRI showed diffuse inflammatory cholangiopathy (Figure 2).
Hematologic work-up including bone-marrow biopsy and oncogenomic and molecular analysis (BCR-ABL and FISH analysis for PDGFa, PDFGb, FGFR1, PCM-JAK2) showed no arguments for a clonal hypereosinophilic syndrome. Whole body 18-FDG PET-CT was inconspicuous. CT-scan showed pulmonary interstitial infiltration and lung function test confirmed an obstructive pattern. Endoscopy revealed ileum and colon eosinophilic infiltrates. During work-up, the patient developed left leg dystonia and right extrapyramidal syndrome. Brain MRI revealed multiple ischemic lesions (Figure 3).
High-sensitive troponins T were elevated [peak at 916 ng/l (ref. <14)] and cardiac MRI showed changes consistent with myocarditis (Figure 4).
The patient received intra-venous methylprednisolone pulses than switched with oral prednisone and anti-aggregation with acetylsalicylic acid, with normalization of eosinophils count (Figure 1). The day after starting methylprednisolone, she developed severe thrombocytopenia (Figure 1). Platelets decreased from 195 G/l (ref. 150-350) to 20 G/l in 24 hours with a nadir at 2 G/l three days later. The work-up for thrombocytopenia was negative (heparin induced thrombocytopenia, viral serologic panel, disseminated intravascular coagulation, thrombotic microangiopathy and antiphospholipid antibodies). Venous thrombosis was excluded and anti-PF4 antibodies were negative, which spoke against vaccine-induced immune thrombotic thrombocytopenia [9]. The diagnosis of immune thrombocytopenic purpura secondary to EGPA was retained. However, the platelet count did not increase under high-dose glucocorticoids, intravenous immunoglobulin and weekly romiplostim. Eventually, the thrombocytopenia subsided after four weekly rituximab courses of 375 mg/m2 (Figure 1) and blood count, including eosinophils, remained normal thereafter.
Upon achieving remission, monthly injections with the anti-IL-5 receptor antagonist benralizumab were added and Prednisone progressively reduced to 5mg/day. 6 months after the diagnosis, the patient still had moderate dystonia impairing her daily activities. Two years later, the patient is still receiving benralizumab and is doing fine.
4. Discussion
Our patient fulfils the latest ACR/EULAR criteria for EGPA (obstructive airway disease, blood eosinophil count >1 G/l and predominant extravascular eosinophilic inflammation on biopsy), [10] and had involvement of bowel, biliary tree, heart and central nervous system.
EGPA is an immune-mediated disease developing in patients with asthma and/or chronic rhinosinusitis. ANCA are found in a minority of patients [11]. EGPA may be separated in two clinical entities: a vasculitic and an eosinophilic phenotype. Patients with vasculitis are more often ANCA positive, while the eosinophilic subtype more often affects the myocardium and has worse prognosis [11]. There is considerable overlap between the two entities. In our ANCA-negative patient, the multiple ischemic cerebral infarctions seen on the MRI are consistent with a small-to medium size vasculitis. It is likely that the high eosinophil count had contributed to myocarditis and cerebral ischemia, due to cytotoxicity to cardiomyocytes and endothelial cells and pro-thrombotic effects [12].
The association of thrombocytopenia and EGPA is uncommon. There are reports of thrombotic microangiopathies complicating EGPA [13] but this was unlikely in our patient, in the absence of haemolysis and schistocytes.
The Five Factor Score, a useful tool to evaluate prognosis and guide the intensity of treatment in systemic vasculitis [14], was worryingly high, indicating the need of immunosuppressants in addition to systemic corticosteroids.
Given the concomitant presence of refractory ITP, the choice of rituximab over cyclophosphamide was made. Rituximab associated to corticoids as second line treatment or as induction therapy in ITP is reported efficacious [15]. Moreover, rituximab has shown efficacy in retrospective studies among patients with EGPA refractory to standard therapy [16]. A controlled trial to evaluated rituximab as induction treatment in EGPA is currently ongoing [17].
EGPA is a rare disease with an estimated prevalence of 10.7 per 14 million adults [11]. In Switzerland, 6 million people have received at least one dose of mRNA vaccine [1] and so far 4 cases of EGPA after mRNA vaccination have been reported from the Swiss Agency for Therapeutic Products. EGPA, a Th2 pathway mediated disease, is anecdotally associated with vaccines and allergen-specific immunization procedures [18]. To the best of our knowledge, there is no study on Th2 response after immunization with SARS-CoV-2 vaccines. A mRNA-1273 vaccine phase I clinical trial has shown a predominant Th1 response after in vitro spike protein stimulation of T cells collected from vaccinated participants [19]. We can hypothesize that in our patient, with her atopic predisposition, asthma and possibly pre-existing immune dysregulation, repeated administration of the mRNA induced an excessive Th2 response, leading to EGPA.
We compiled other reports of new onset EGPA or relapses after prolonged EGPA remission secondary to immunization with mRNA vaccine in (Table 1).
All but one case occurred in patients with pre-existing asthma and or rhinosinusitis. Peak peripheral blood eosinophil values ranged from 0.88–13.4 G/l. Half of cases presented with ANCA. Most needed treatment with immunosuppressants.
In addition to ours, three other cases of EGPA after mRNA vaccine had been reported to Swissmedic by November 2022, all aged 60 or more. We do not have more details concerning these patients. While we ignore how many spontaneous EGPA cases occurred in the same period, the incidence of the four potentially vaccine-related EGPA cases in a population of 8 Mio people corresponds to the reported natural occurrence of the disease.
As with EGPA, other cases of IMID were reported to flare or to newly occur after immunization with mRNA vaccines [3]. As in our case, while the temporal relationship to the immunization is evident, it is impossible to prove a causal relationship between the vaccine and the IMID. Up to the present day, these cases remain fortunately rare and do not preclude to use mRNA vaccines SARS-CoV2, given the established benefits in protecting from severe Covid-19 [2].
Funding
This study received no funding.
Disclosure statement
The authors have declared no conflicts of interest.
Authors Contributions
All authors contributed equally to this work.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Acknowledgments
Swissmedic, the Swiss Agency for Therapeutic Products.
References
- Swissmedic 2019, © Copyright Reports of Suspected Adverse Reactions to COVID-19 Vaccines in Switzerland Update 23 Available online: https://www.swissmedic.ch/swissmedic/en/home/news/coronavirus-covid-19/covid-19-vaccines-safety-update-13.html (accessed on 25 March 2022).
- Yan, M.Z.; Yang, M.; Lai, C.-L. Review of Clinical Trials of COVID-19 Vaccination Booster in SARS-CoV-2 Variants Era: To Take It or Not To Take It. Frontiers in Drug Discovery 2022, 2.
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-Mediated Disease Flares or New-Onset Disease in 27 Subjects Following MRNA/DNA SARS-CoV-2 Vaccination. Vaccines 2021, 9, 435. [CrossRef]
- Chan-Chung, C.; Ong, C.-S.; Chan, L.-L.; Tan, E.-K. Eosinophilic Granulomatosis with Polyangiitis after COVID-19 Vaccination. QJM 2021, hcab273. [CrossRef]
- Nappi, E.; De Santis, M.; Paoletti, G.; Pelaia, C.; Terenghi, F.; Pini, D.; Ciccarelli, M.; Selmi, C.F.; Puggioni, F.; Canonica, G.W.; et al. New Onset of Eosinophilic Granulomatosis with Polyangiitis Following MRNA-Based COVID-19 Vaccine. Vaccines (Basel) 2022, 10, 716. [CrossRef]
- Hakroush, S.; Tampe, B. Case Report: ANCA-Associated Vasculitis Presenting With Rhabdomyolysis and Pauci-Immune Crescentic Glomerulonephritis After Pfizer-BioNTech COVID-19 MRNA Vaccination. Front Immunol 2021, 12, 762006. [CrossRef]
- Ibrahim, H.; Alkhatib, A.; Meysami, A. Eosinophilic Granulomatosis With Polyangiitis Diagnosed in an Elderly Female After the Second Dose of MRNA Vaccine Against COVID-19. Cureus 2022, 14, e21176. [CrossRef]
- Lai, Y.W.; Chua, C.G.; Lim, X.R.; Francis, P.J.; Xu, C.; Howe, H.S. Autoimmune Rheumatic Disease Flares with Myocarditis Following COVID-19 MRNA Vaccination: A Case-Based Review. Vaccines (Basel) 2022, 10, 1772. [CrossRef]
- Klok, F.A.; Pai, M.; Huisman, M.V.; Makris, M. Vaccine-Induced Immune Thrombotic Thrombocytopenia. Lancet Haematol 2022, 9, e73–e80. [CrossRef]
- Grayson, P.C.; Ponte, C.; Suppiah, R.; Robson, J.C.; Craven, A.; Judge, A.; Khalid, S.; Hutchings, A.; Luqmani, R.A.; Watts, R.A.; et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology Classification Criteria for Eosinophilic Granulomatosis with Polyangiitis. Ann Rheum Dis 2022, annrheumdis-2021-221794. [CrossRef]
- Chakraborty, R.K.; Aeddula, N.R. Churg Strauss Syndrome. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2021.
- Barbind, K.L.; Boddu, R.; Shijith, K.P.; Mishra, K. Hypereosinophilia: A Rare Cause of Stroke and Multiorgan Dysfunction. BMJ Case Rep 2021, 14, e242619. [CrossRef]
- Badiola, J.; Navarrete-Navarrete, N.; Sabio, J.M. Thrombotic Microangiopathy in a Patient with Eosinophilic Granulomatosis with Polyangiitis: Case-Based Review. Rheumatol Int 2019, 39, 359–365. [CrossRef]
- Groh, M.; Pagnoux, C.; Baldini, C.; Bel, E.; Bottero, P.; Cottin, V.; Dalhoff, K.; Dunogué, B.; Gross, W.; Holle, J.; et al. Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss) (EGPA) Consensus Task Force Recommendations for Evaluation and Management. Eur J Intern Med 2015, 26, 545–553. [CrossRef]
- Ghanima, W.; Khelif, A.; Waage, A.; Michel, M.; Tjønnfjord, G.E.; Romdhan, N.B.; Kahrs, J.; Darne, B.; Holme, P.A.; RITP study group Rituximab as Second-Line Treatment for Adult Immune Thrombocytopenia (the RITP Trial): A Multicentre, Randomised, Double-Blind, Placebo-Controlled Trial. Lancet 2015, 385, 1653–1661. [CrossRef]
- Teixeira, V.; Mohammad, A.J.; Jones, R.B.; Smith, R.; Jayne, D. Efficacy and Safety of Rituximab in the Treatment of Eosinophilic Granulomatosis with Polyangiitis. RMD Open 2019, 5, e000905. [CrossRef]
- Assistance Publique - Hôpitaux de Paris Evaluation of Rituximab-Based Regimen Compared to Conventional Therapeutic Strategy For Remission Induction In Patients With Newly-Diagnosed or Relapsing Eosinophilic Granulomatosis With Polyangiitis. Prospective, Randomized, Controlled, Double-Blind Study; clinicaltrials.gov, 2021;
- Gioffredi, A.; Maritati, F.; Oliva, E.; Buzio, C. Eosinophilic Granulomatosis with Polyangiitis: An Overview. Frontiers in Immunology 2014, 5.
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and Immunogenicity of SARS-CoV-2 MRNA-1273 Vaccine in Older Adults. N Engl J Med 2020, 383, 2427–2438. [CrossRef]
- Gill, R.; Rizvi, M.; Sadiq, M.S.; Feldman, M. Recrudescence of Severe Polyneuropathy after Receiving Pfizer-BioNTech COVID-19 Vaccine in a Patient with a History of Eosinophilic Granulomatosis with Polyangiitis. BMJ Case Rep 2022, 15, e245749. [CrossRef]
- Costanzo, G.; Ledda, A.G.; Ghisu, A.; Vacca, M.; Firinu, D.; Del Giacco, S. Eosinophilic Granulomatosis with Polyangiitis Relapse after COVID-19 Vaccination: A Case Report. Vaccines 2022, 10, 13. [CrossRef]
Figure 1.
Disease course in a 46 year-old patient with new onset eosinophilic granulomatosis with polyangiitis occuring after SARS-CoV-2 mRNA 1273 vaccine. Disease manifestations with evolution of blood eosinophil and thrombocyte count and treatment received. Multiple ischemic strokes occurred at the peak of peripheral blood eosinophilia (8.4 G/l).
Figure 1.
Disease course in a 46 year-old patient with new onset eosinophilic granulomatosis with polyangiitis occuring after SARS-CoV-2 mRNA 1273 vaccine. Disease manifestations with evolution of blood eosinophil and thrombocyte count and treatment received. Multiple ischemic strokes occurred at the peak of peripheral blood eosinophilia (8.4 G/l).
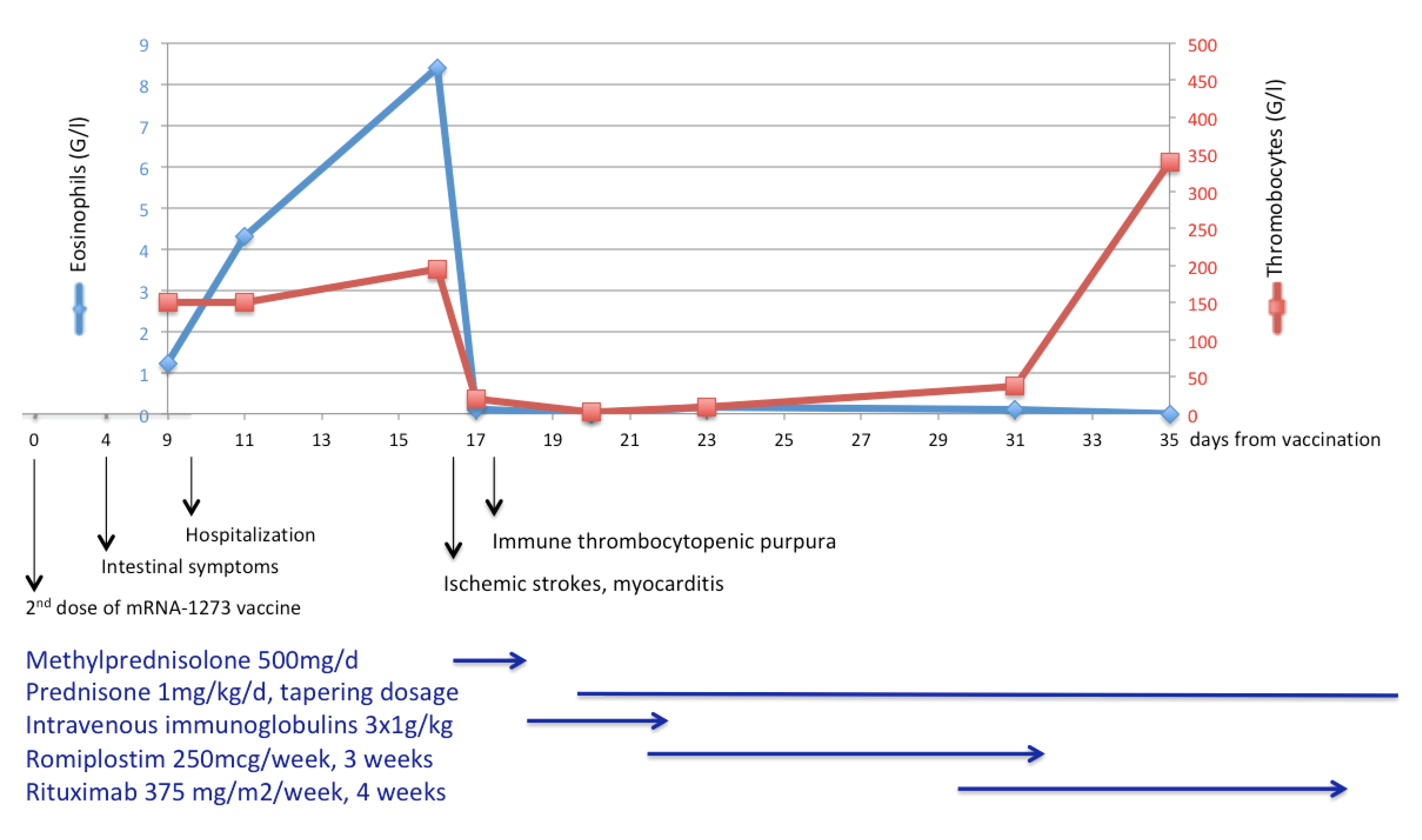
Figure 2.
Liver MRI showing cholangiopathy disease. Magnetic Resonance Imaging with WI-weighted images, performed 10 days after symptom onset, showing patchy and ill-defined T2 hypersignal lesions (A, arrow) with discrete arterial phase enhancement (B, arrow). Periportal oedema (C, arrow), diffuse gallbladder wall thickening (D, arrow) and biliary wall enhancement on portal venous phase (E) are seen on T2.
Figure 2.
Liver MRI showing cholangiopathy disease. Magnetic Resonance Imaging with WI-weighted images, performed 10 days after symptom onset, showing patchy and ill-defined T2 hypersignal lesions (A, arrow) with discrete arterial phase enhancement (B, arrow). Periportal oedema (C, arrow), diffuse gallbladder wall thickening (D, arrow) and biliary wall enhancement on portal venous phase (E) are seen on T2.
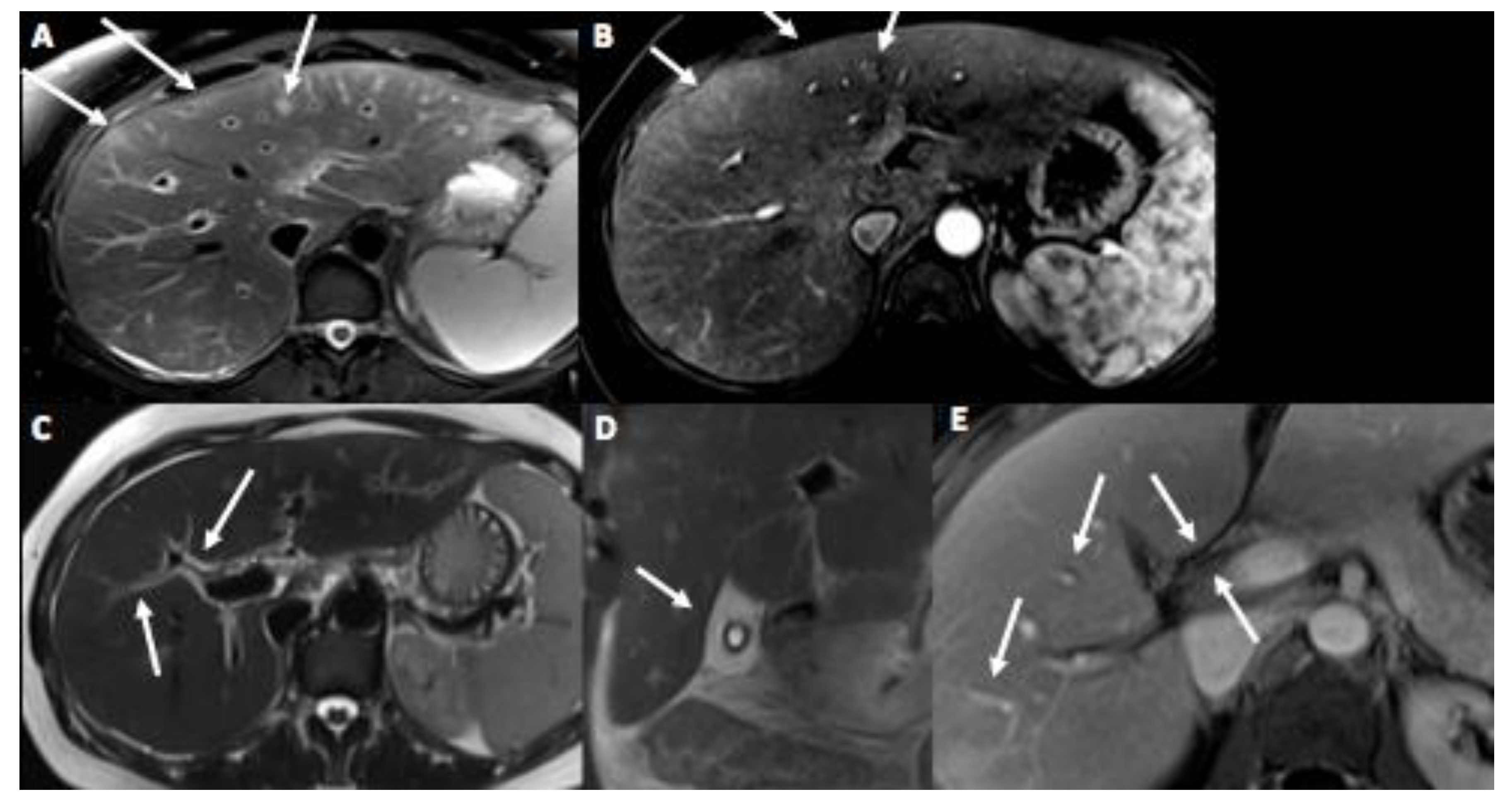
Figure 3.
Cranial MRI showing multiple ischemic lesions of the brain. Brain MRI performed 15 days after symptom onset (A, B, C). Diffusion weighted images denote multiple focal acute infarcts in the posterior and anterior circulation territories: in both cerebellar hemispheres (A, arrows), in the thalami (B, arrows), and bilateral cortical and subcortical fronto-parieto-occipital regions (C, arrows). (D) Axial T2 weighted MRI performed after 3 months shows residual infarction lesions in corona radiata (arrows).
Figure 3.
Cranial MRI showing multiple ischemic lesions of the brain. Brain MRI performed 15 days after symptom onset (A, B, C). Diffusion weighted images denote multiple focal acute infarcts in the posterior and anterior circulation territories: in both cerebellar hemispheres (A, arrows), in the thalami (B, arrows), and bilateral cortical and subcortical fronto-parieto-occipital regions (C, arrows). (D) Axial T2 weighted MRI performed after 3 months shows residual infarction lesions in corona radiata (arrows).
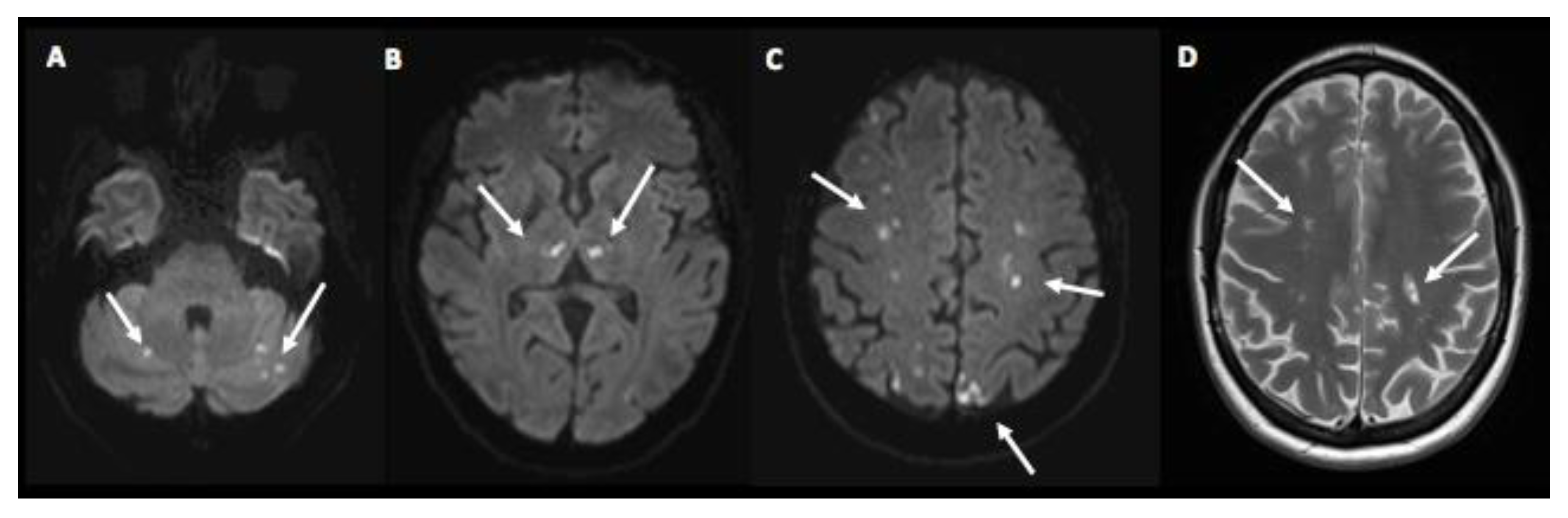
Figure 4.
Cardiac MRI consistent with myocarditis. Cardiac MRI performed initially (A, B, C) and after 3 months (D, E, F). Three chamber (A) and short axis (B) LGE images demonstrating a focal medio-mural lesion in the inferior and inferolateral apical myocardial segment (arrows), persistent on control MRI 3 months later (D, E, arrows). T2-imaging short axis apical images (C, E) showing a focal T2 hypersignal in the same territory, translating a myocardial inflammatory oedema. LGE: late gadolinium enhancement.
Figure 4.
Cardiac MRI consistent with myocarditis. Cardiac MRI performed initially (A, B, C) and after 3 months (D, E, F). Three chamber (A) and short axis (B) LGE images demonstrating a focal medio-mural lesion in the inferior and inferolateral apical myocardial segment (arrows), persistent on control MRI 3 months later (D, E, arrows). T2-imaging short axis apical images (C, E) showing a focal T2 hypersignal in the same territory, translating a myocardial inflammatory oedema. LGE: late gadolinium enhancement.
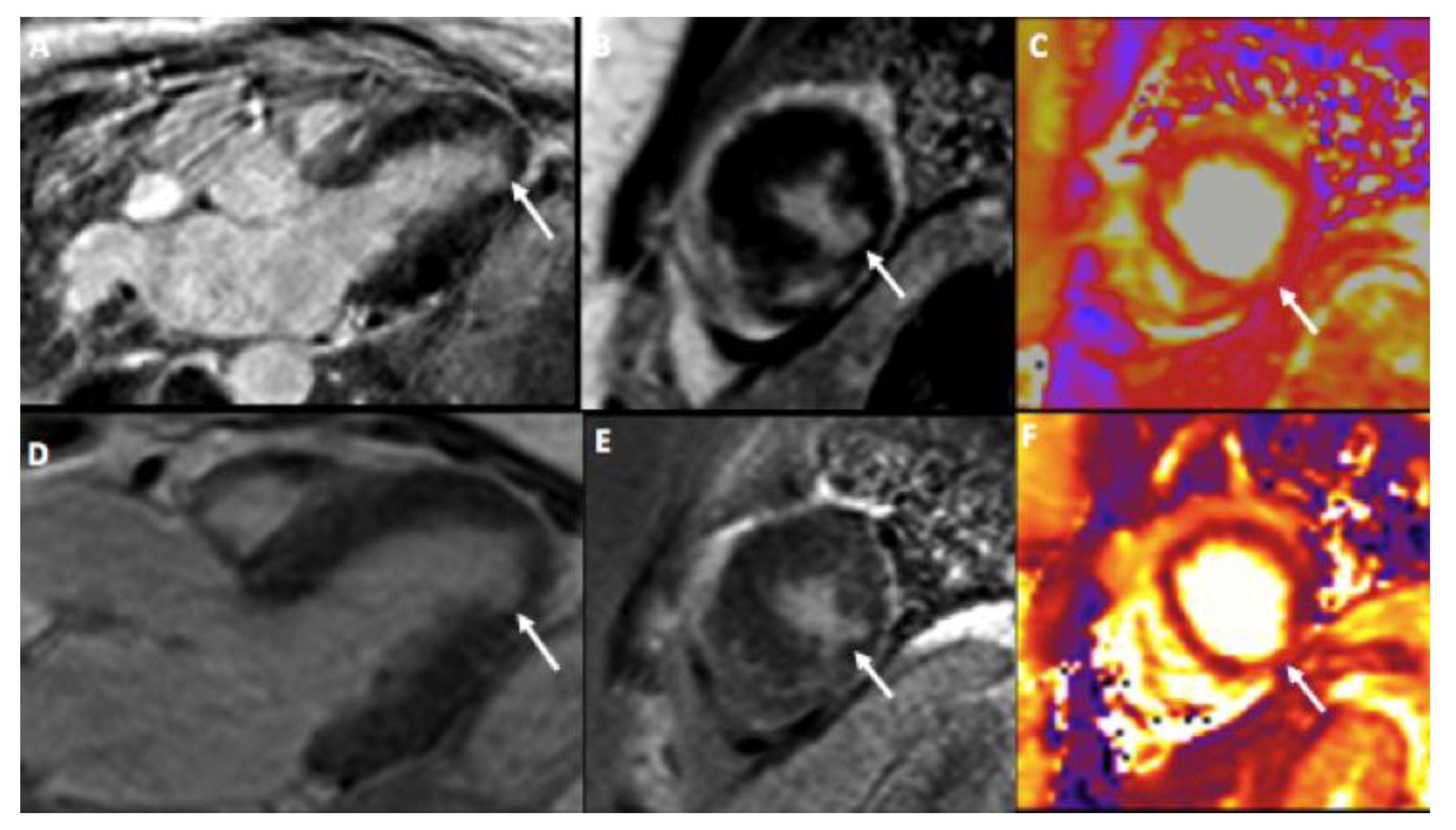

Table 1.
Reported cases of new-onset eosinophilic granulomatosis with polyangiitis or disease flares after immunization with mRNA vaccines.
Table 1.
Reported cases of new-onset eosinophilic granulomatosis with polyangiitis or disease flares after immunization with mRNA vaccines.
| Case | Age, gender | Pre-existing respiratory disease | Pre-existing EGPA (treatment) | mRNA vaccine type | Time between immunization and EGPA symptom onset in days (vaccine dose) | Clinical presentation | Complications | Peak blood eosinophil count (G/l) | ANCA positivity (type) |
FFS | Treatment received |
|---|---|---|---|---|---|---|---|---|---|---|---|
| [4] | 62, F | Asthma | No | BNT161b2 | Few days (2nddose) | Fever, numbness in feet and palms, walking disability, purpura, peri-orbital oedema |
Polyneuropathy, optic nerves inflammation, myocarditis, vasculitis at cutaneous biopsy |
13.4 | Yes (anti-MPO) | 1 | MP, RTX |
| [5] | 63, M | Allergic rhino-sinusitis and asthma | No | mRNA-1273 | 1 (1st dose) | Diplopia, headache, dry cough |
3rd cranial nerve palsy, myopericarditis | 12.4 | No | 2 | MP, P, CYC |
| [6] | 79, F | No | No | BNT162b2 | 14 (2nd dose) | Myalgia, Weakness | Rhabdomyolysis, acute kidney injury, pauci-immune crescentic glomerulonephritis and interstitial nephritis with prominent eosinophilia | 5.3 | Yes (p-ANCA, anti-MPO) | 1 | MP, P, CYC |
| [7] | 79, F | Asthma | No | mRNA-1273 | 14 (2nd dose) | Progressive paraesthesia of hands and feet, myalgia, walking disability | DVT, vasculitic neuropathy with eosinophil infiltration | 12.4 | Yes (p-ANCA, anti-MPO) | 0 | P, AZA |
| [20] | N/A, M | Rhino-sinusitis and asthma | Yes (untreated for 7 years) | BNT162b2 | 5 (1st dose) | Weakness, neuropathic pain, blurry vision | Polyneuropathy, mild left foot drop | 0.94 | No | 0 | P |
| [21] | 71, F | Rhino-sinusitis and asthma | Yes (MEP, ICS) | BNT162b2 | 10 (1st dose) | Myalgia, arthralgia, dyspnoea, cough, chest pain, paraesthesia | Mononeuritis multiplex | 4.3 | Yes (p-ANCA) | 0 | MP, P, BEN |
| [8] | 63, F | Allergic rhinitis and asthma | Yes (AZA) | mRNA-1273 | 14 (1st dose) | Dyspnoea, chest pain | Myocarditis | 0.88 | No | 1 | MP. P. CYC |
| [8] | 64, M | Asthma and rhinosinusitis with nasal polyps | No (but constitutional symptoms for 3 months) | BNT162b2 | 2 (1st dose) | Numbness thigh, purpura, chest pain | Endomyocarditis, cutaneous vasculitis, mononeuritis multiplex, possible glomerulonephritis | 5.39 | No | 1 | MP, P, CYC |
| Present case |
46, F | Allergic rhino-sinusitis and asthma | No | mRNA-1273 | 4 (2nd dose) | Enteritis, fever, fatigue, myalgia | Myocarditis, multiple strokes, immune thrombocytopenia | 8.4 | No | 2 | MP, P, IVIG, RPL, RTX, BEN |
AZA: azathioprine; FFS: Five factor score; MP: methylprednisolone pulses; P: Prednisone; IVIG: intravenous immunoglobulins; RPL: romiplostim; CYC: cyclophosphamide; RTX: rituximab; BEN: benralizumab.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



