
Submitted:
13 July 2023
Posted:
14 July 2023
You are already at the latest version
Abstract
Over the last 20 years, gliomas have made up over 89% of malignant CNS tumor cases in the American population (NIH SEER). Within this, glioblastoma is the most common subtype, comprising 57% of all glioma cases. Highly aggressive, this deadly disease is known for its high genetic and phenotypic heterogeneity, rendering a complicated disease course. The current standard-of-care consists of maximally safe tumor resection concurrent with chemoradiotherapy. However, despite advances in technology and therapeutic modalities, rates of disease recurrence are still high and survivability remains low. Given the delicate nature of the tumor location, remaining margins following resection often initiate disease recurrence. Photodynamic therapy (PDT) is a therapeutic modality that, following the administration of a non-toxic photosensitizer, induces tumor-specific anti-cancer effects after localized, wavelength-specific illumination. Its effect against malignant glioma has been studied extensively over the last 30 years, in pre-clinical and clinical trials. Here, we provide a comprehensive review of the three generations of photosensitizers alongside their mechanisms of action, limitations, and future directions.
Keywords:
glioblastoma
; photomedicine
; photodynamic therapy
; photosensitizer
1. Introduction
Glioma is the most common malignant primary central nervous system tumor type and consists of several subtypes, including glioblastoma (GBM) which make up 57.3% of all gliomas [1]. An extremely aggressive subtype, GBM is characterized by its high infiltrative and angiogenic attributes [2]. The current standard of care for gliomas involves maximal surgical resection followed by radiation therapy with concurrent and adjuvant temozolomide (TMZ). For GBM, in particular, this regimen is known as the Stupp protocol and yields a median survival of 14.6 months, median progression free survival (PFS) of 6.9 months, and a two year overall survival (OS) rate of 26.5% [3,4,5]. Often, treatment failure can be attributed to factors including inter- and intratumoral heterogeneity, reacquisition of stemness in glioblastoma stem cells, the evolution of therapy-resistant clonal subpopulations, the tumor-promoting microenvironment, multiple drug efflux mechanisms, metabolic adaptations, and enhanced repair of drug-induced DNA damage [6,7]. As such, disease recurrence is nearly inevitable in patients with high-grade gliomas. Despite advances in treatment strategies, there are currently no standard therapeutic options for recurrent glioma and recurrent GBM (rGBM) management. Over the past two decades, therapeutic strategies have been explored but with minimal success. Trials using monotherapeutic and combinatorial drugs have explored the use of nitrosoureas, antiangiogenics, and EGFR inhibitors to treat rGBM [8,9]. Of these therapies, trials involving the use of bevacizumab in TMZ-pretreated patients have shown promising results [10]. However, there have been no significant differences in patient survival across the large host of regimens, with many trials often resulting in an increased risk of toxicity and adverse events [9,11,12]. With no standard treatments, patients are treated conditionally according to clinical characteristics and conventional prognostic factors.
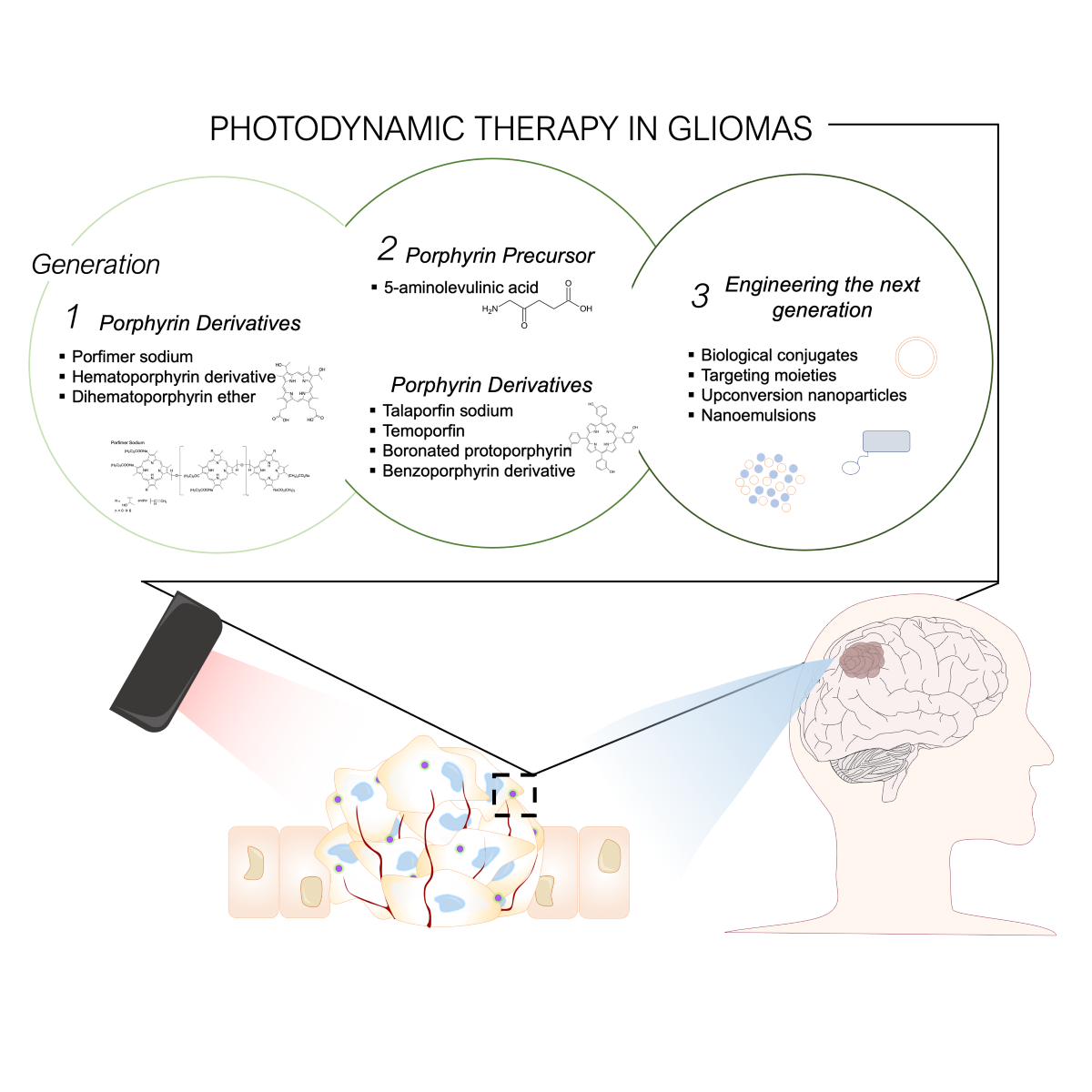
Over the last almost 50 years, the utility of photosensitizers (PS) in the context of fluorescence guided surgery (FGS) and photodynamic therapy (PDT) in glioma have advanced with rapidly growing momentum [13,14,15,16]. PDT is a two-stage treatment that combines light energy with a drug (photosensitizer, PS) designed to destroy cancerous and precancerous cells after light activation (Figure 1). PDT relies on a tumor-selective, otherwise inert, PS molecule that is administered locally or systemically. Whereas standard radio and chemotherapies act non-specifically, PDT selectively targets tumor tissue due to the preferential accumulation of the drug in malignant tissue. When excited by light of a particular wavelength, PSs will absorb the energy, convert into an intermediary byproduct, and undergo intersystem crossing [17]. This phenomenon leads to the buildup of tumoricidal molecules, such as reactive oxidative species (ROS), resulting in localized destruction of the tumor [18,19,20,21]. Given the tumor-specific and tumor-targeting nature of PSs, the use of PDT becomes extremely attractive for treating both GBM and rGBM given its high cytotoxicity, minimal normal tissue toxicity and systemic effects, and minimized risk of local recurrence [22,23].
In this review, we explore the key advancements of photosensitizers and photodynamic therapy, as well as their advantages and pitfalls, focusing on future therapeutic perspectives for the management of gliomas.
2. Photodynamic therapy mediated tumoricidal effect
2.1. PDT induces cell death following uptake and accumulation
Unlike temozolomide (TMZ) which acts by destabilizing DNA, the tumoricidal effect of photodynamic therapy (PDT) manifests by causing oxidative damage to cell membranes, proteins and organelles. This triggers a combination of necrosis and apoptosis as well as immunogenic and autophagy pathways [18,19,20]. It is well known that standard radiation therapy for malignant glioma can cause radiation necrosis of the treated tissue. This may induce headache, vomiting, loss of consciousness, and hemiplegia in patients, but can be relieved by surgical removal of necrotic areas [24]. Therefore, apoptosis and autophagy are considered the preferred cell death mechanisms for glioma treatment modalities. Distinct types of PDT-induced cell death vary depending on (i) PS subcellular localization, pharmacokinetics, and chosen drug dose, (ii) light dosimetry, (iii) tissue oxygenation status, and (iv) tumor-subtype specific properties [25,26,27]. PSs that localize in the mitochondria have been shown to induce apoptosis, whereas PSs that localize in lysosomes and plasma membranes generally demonstrate a necrotic cellular response [28]. However, these different cell death types are not mutually exclusive and have the potential to co-occur or shift from one survival pathway to another by altering just one variable in the treatment schema [24,29].
2.2. PDT controls glioma stem cell (GSC) processes
In addition to their effects on the glioma cells, PDT can also curtail the growth of GSCs and induce their death [30,31]. GSCs are multipotent cells with tumorigenic capability [32], driving tumor regeneration and disease progression, and are predominantly involved in the recurrence of GBM [33]. Studies have shown that long-term TMZ exposure increases GSC subpopulations [32]. Recent evidence also suggests that in vitro GSCs accumulate protoporphyrin IX (PpIX), a downstream product of the second-generation PS 5-aminolevulinic acid (5-ALA), to therapeutic levels in a dose- and time-dependent manner inducing cell death [30]. More recently, Fisher et al. described a doubling of median OS in rats bearing GSC-30 tumors following low-dose ALA-PDT combined with lapatinib, an EGFR inhibitor, as compared to rats with conventional U87 human glioma cell line tumors [34].
2.3. PDT modulates neurovasculature: disruption of the blood brain barrier (BBB) and destruction of tumor vasculature
PDT mediates the breakdown of the BBB, facilitating the diffusion of PSs into the brain and tumoral area. It is little known if PSs, such as 5-ALA, are proxies for the tumor tissue or just a manifestation of BBB disruption. In a proof-of-concept report, Madsen et al. showed exogenous macrophage migration into the brain of non-tumor bearing mice following PDT-induced BBB disruption [35]. The breakdown of the BBB can result in increased accumulation of PS, over nonspecific therapeutic delivery vehicles, in the tumor tissue, compounding the antitumor effect.
Similarly, PDT also bears an effect on tumor vasculature. Angiogenesis is an important hallmark of cancer, contributing to tumor resilience and aggressive growth [36]. Intriguingly, there is evidence of microvascular constriction, collapse, and thrombus formation following PDT, ultimately delaying or inhibiting tumor growth [37]. Characterization of tumor morphology following PDT has revealed lapsed sinusoids, intumescent endothelial cells within tumor capillaries, luminal occlusion, and thrombosis [38]. Combined, these two effects on the neurovascular system compound the therapeutic effects of PDT on malignant gliomas.
2.4. PDT stimlates anti-tumor immunity
Emerging studies have also described an increased migration of antigen-presenting cells, such as macrophages [35], dendritic cells [39], and cytokines [40] to brain tissue treated with PDT. This immunological effect is mediated by an upregulation of damage-associated molecular patterns (DAMPs), such as heat shock proteins (HSP) [41,42], surface calreticulin (CRT), secreted adenosine triphosphate (ATP), and high-mobility group box 1 protein (HMGB1) [43]. DAMPs are released by damaged or dying cells to stimulate vascular permeability and production of proinflammatory cytokines, thereby mediating leukocyte migration to the site of tissue damage. Through both in vitro and in vivo studies, there is significant evidence of PDT treatment-induced upregulation of HSP70 surface expression [41,44,45]. In rat models, accumulation of CD8+ T cells and macrophages/microglia were seen in conjunction with HSP70 upregulation following nanoparticle-based PDT [42]. Studies employing mixtures of photosensitizers have also prompted phagocytosis of glioma cells via bone marrow dendritic cells (BMDCs), via BMDC maturation and production of IL-6 in a cell ratio-dependent manner [43]. Genes for immune protein markers IL-6 and IL-6R have also been found to be upregulated alongside ROS-inducible genes after PDT [46]. Over the last few years, in vitro studies have moved towards investigating non-porphyrin, third generation PSs, with many utilizing cross-linked polymers and nanoplatforms for targeted delivery to enhance PDT-induced immunological tumoricidal effects [47,48,49,50,51,52,53,54].
3. Photosensitizers
Clinically efficacious photosensitizers (PS) are constrained by several properties, namely (i) ability to penetrate the BBB, (ii) selective accumulation in malignant tissue, and (iii) photoactivity at long light wavelengths for deep tissue penetration [55]. PSs are categorized into three generations based on molecular properties (Table 1 [22,56,57,58,59,60,61,62,63,64,65,66]): first-generation PSs are naturally occurring porphyrins, second-generation PSs comprise more chemically pure and tumor-selective compounds, and third-generation PSs broad cover engineered nanoplatforms, gene-engineered, and carrier-bound systems that further enhance tumor-selective cytotoxicity [67,68,69].
3.1. First Generation: naturally occurring porphyrins
First-generation PSs include hematoporphyrin (HP) and the purified derivatives of porfimer sodium (Photofrin), hematoporphyrin derivative (HpD, Photofrin I), and dihematoporphyrin ether (HPE, Photofrin II) [28]. The use of hematoporphyrin derivatives in malignancies was reported as early as 1960-1961 [70,71], with their use as a PS in glioma PDT ensuing a few decades later. The notable tumor-localizing characteristic of PSs was identified twenty years later [72] and shown to be attained following alkaline hydrolysis of the drug. Interestingly, these porphyrin-based PSs bear extreme structural resemblance to that of heme. Yet, unlike heme, these structures lack Fe ion coordination, thereby preventing downstream oxidative conversion and catabolism, resulting in cellular accumulation and subsequent PDT-induced toxicity [73,74].
Since the 1980s, first-generation photosensitizers have been clinically tested in numerous safety and feasibility studies for malignant glioma treatment (Table 2 [13,59,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93]). In comparison to the current standard of care and results from other PS studies, HP and its derivatives have demonstrated modest survival outcomes. From 1980 to 1990 several groups from Italy [75,94], Australia [76,95], and the United States [13] reported successful use of PDT with HpD for treatment of glioma in small cohorts of patients. Across these studies, low doses of HpD (1-5 mg/kg) were administered via intratumoral, intra-arterial, or intravenous injections prior to photo-illumination via a variety of light delivery and optical energies [96].
To further improve patient survival, studies combining PDT with standard therapeutic modalities such as radiation were implemented [80]. In 1988, a Phase I/II clinical trial combined PDT with single shot ionizing radiation and/or conventional radiotherapy to assess combined treatment efficacy across three populations of patients: primary glioma, single recurrence GBM, and multiple rGBM [81]. HPD was administered either through the internal carotid artery or directly into the tumor bed. Using low to moderate light doses (60-200 J/cm2), subsequent PDT was performed. In general, outcomes for recurrent disease patients were unimpressive, with patient progression free survival (PFS) ranging from 2-15 months. Furthermore, patients who had previously failed conventional radio- or chemotherapy did not benefit from the PDT-RT combination. In a larger follow-up study with 50 GBM patients, the authors increased light dose (200 J/cm2 to 250 J/cm2) and PS concentration (1 mg/kg to 2.5 mg/kg), noting improved PFS for both primary GBM (n=11) and rGBM (n=39) at 13 months and 7 months, respectively [97,98].
Interestingly, a positive association has been shown between increased light doses and improved outcomes across several groups ranging from initial to current studies. A retrospective study on HpD treated patients (n=136) treated from 1986 to 2000 noted significantly improved prognosis (hazard ratio = 0.502) in primary tumor cases treated with doses of 230 J/cm2 or higher [91]. In recurrent tumor cases, however, increased light doses effectuated only a slight improvement in the hazard ratio (HR = 0.747). While it may be argued that these improvements are confounded by advances in technology, namely increased laser light stability across different laser sources, other concurrent studies on similar patient populations (age, baseline Karnofsky score) [88] identified similar improvements in median OS as laser light dosage increased (<1200 J: 39 weeks, >1200 J: 52 weeks).
As with first and second-generation PDT in other systemic cancers [99], other light sources such as LEDs have also been explored. A study comparing laser and LED-based PDT demonstrated similar levels of tissue toxicity at equivalent light doses across several types of tumors, including GBM [59]. Given the broader emission spectrum and increased major emission wavelength of LED light, however, the study concluded that PSs with higher absorption peaks, such as benzoporphyrin derivatives (BPD, a second-generation PS), were more suitable for LED-based PDT.
While first-generation PSs have demonstrated successful PDT effects in glioma [100,101], the chemical properties of these compounds limit their efficacy as ideal PDT candidates. Firstly, this generation of PSs is limited not only by their low therapeutic efficacy, these drugs bear low singlet oxygen quantum yield [102]. Furthermore, PDT response using first-generation PSs has been inconsistent across different glioma cell lines [103]. When compared to second-generation PSs, there are notable differences in efficacy, as described by relatively higher non-specific PS accumulation in normal brain tissue, longer extended illumination times, and increased elimination half-life. While porfimer sodium has a higher absorption spectrum than HpD, both HpD and porfimer sodium have extended half-lives and renal clearance time [104], with porfimer sodium persisting in circulation over 2 months, increasing the risk of unwanted photo-related toxicities [67,69,105]. The structural nature and size of these naturally occurring porphyrins, large tetrapyrrole macrocycles connected via methine bridges, respectively, exhibit aggregation in water and additionally complicate delivery across the blood-brain barrier. Combined, first-generation PSs exhibited several limiting characteristics that hindered their utility for glioma care. As such, the development of second-generation photosensitizers was warranted to expand the efficacy of glioma photodynamic therapy.
3.2. Second Generation: increased singlet oxygen potency
In contrast to first-generation PSs, second-generation therapeutics showed improved purity, more efficient ROS production, and enhanced tumor selectivity with limited adverse effects. Second-generation PSs mostly consist of porphyrin or chlorin-based structures and precursors. Those include 5-aminolevulinic acid (5-ALA; Gliolan), Talaporfin sodium (mono-L-aspartyl chlorin e6, NPe6, TS; Laserphyrin, boronated porphyrins (BOPP), Temoporfin (m-THPC, Foscan and Foslip), and benzoporphyrin derivatives (BPD, Verteporfin) [57,67]. These newer second-generation PSs bear phototoxic properties at a longer light wavelength than first-generation PSs and can be excited at lower energies (down to 20 J/cm2), yielding a greater potential to target deeper tumor tissue [106]. Over the last three decades, clinical trials have assessed second-generation PSs for their treatment of gliomas (Table 3 [23,56,59,66,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123]). Below, we discuss two of the most common second-generation photosensitizers studied under in vitro, in vivo, and clinical conditions. However, extensive evaluation of other second-generation PSs such as metallo-phthalocyanines have also ensued in parallel for both pediatric and adult brain tumors [124,125,126,127].
To this day, 5-ALA is one of the most heavily explored and utilized PSs, and has been established as a valuable tool for both real-time intraoperative visualization (fluorescence guided surgery, FGS) for malignant glioma resection and as a tumor-selective PS for PDT. Administered orally, 5-ALA is an endogenous compound that is metabolized via the heme pathway. Unlike first-generation photosensitizers, 5-ALA is a molecular precursor for heme, therefore relying on a different mechanism of action for therapeutic activation. In tumor cells, suppression of membrane transport proteins and dysregulation of the Ras/MEK and FECH/heme oxygenase pathways result in the buildup of protoporphyrin IX (PpIX), particularly following exogenous dosage [128,129,130,131]. The subsequent buildup of PpIX exerts fluorescent and phototoxic properties on the tumor cell upon excitation with blue (405 nm, FGS) or red (635 nm, PDT) light [132]. 5-ALA offers advantageous clinical benefits due to its high tumor selectivity, rapid renal clearance, and limited adverse effect on normal brain tissue [55]. Several clinical studies have demonstrated high drug efficacy and improved survival in malignant glioma patients. Particularly, a study comparing the effects of 5-ALA PDT on median survival in patients with GBM distinguished an improvement of over 2-fold (62.9 weeks vs. 20.6 weeks) following intraoperative cavitary therapy [114].
Compared to 5-ALA, talaporfin sodium (TS) is delivered intravenously and does not exert tumor selectivity through metabolic pathways. Rather, it circulates in the blood, conjugated to albumin, and accumulates selectively in tumor cells via lysosome endocytosis, relying on increased vascular permeability at the blood-tumor barrier. Consequently, blood vessel endothelium, blood that has accumulated in the resection cavity, and non-glioma vascularized CNS neoplasms have been observed to exhibit marked fluorescence, a characteristic that negatively impacts its performance as a tumor-selective PS [66,133]. Shimizu et al. have demonstrated the feasibility of TS-based FGS for GBM, demonstrating a specificity of 80% and sensitivity of 71% with strong fluorescence was noted in both newly diagnosed and rGBM [66]. Recent studies have reported the feasibility of TS-based PDT, via mitochondrial-mediated apoptosis and necroptosis at low TS doses and low laser irradiation [24,134,135]. However, as TS doses increased, evidence suggests that the dominant modality of cell death shifts from apoptosis to necrosis [29]. The mechanisms underlying these variations in mechanisms and the extent of cell death in different glioma cells require further exploration to optimize clinical application [134].
Current PDT clinical trials around the world continue to assess the efficacy of second-generation photosensitizers for malignant gliomas (Table 4). In recent years, in particular, studies have begun investigating the utility of both TS and 5-ALA in pediatric brain tumor patients, with age enrollment criteria ranging from 3 to 20 years old (UMIN000030883: 6 years to 20 years; NCT04738162: 3 years to 17 years). While the listed studies have yet to report findings, study outcomes will encompass drug safety and tolerability, OS, and PFS.
3.2.1. Combining second-generation PDT with standard therapies
In addition to single-drug PDT, studies have investigated the synergistic effect of second-generation PSs with standard care modalities. A notable study, performed in 2012, investigated the efficacy of 5-ALA PDT alone, against standard maximum safe resection (MSR) and alongside intraoperative radiotherapy (IORT) to assess patient PFS across four different cohorts: (i) MSR only, (ii) MSR + IORT, (iii) MSR + PDT, (iv) MSR + PDT + IORT (Table 3, Lyons et al. (2012)) [114]. Aside from the significant effect of PDT on median survival, adding IORT to the treatment regimen (iii vs. iv) increased PFS from 39.7 weeks to 79 weeks.
Studies combining PDT with standard chemotherapies have been performed as well. Two separate groups utilizing different PS-based PDT protocols found that TMZ concomitant therapy potentiates PDT-induced apoptotic cell death in vitro [136,137]. The combination of TS and TMZ delivery increased intracellular concentrations of PS and upregulation of ROS production following cotreatment [137]. Additionally, in vitro study has shown that second-generation guided PDT and TMZ act synergistically to decrease glioma migration and invasiveness in glioma cells by downregulating the protein NHE1, preventing escape from TMZ-mediated toxicity [136,138]. Further building on this combined efficacy, in vivo rat models have found that PDT increases TMZ tissue concentrations and combinatorial treatment decreases tumor volume and prolongs survival [139]. In addition to co-delivery with the standard TMZ, studies have investigated the use of PDT with anti-angiogenic drugs. A combination of PDT with bevacizumab has demonstrated increased median survival time in glioma-bearing rats as compared to PDT or bevacizumab alone [140]. Further study on the co-effects of PDT and chemotherapies has been further elucidated with the development of third-generation photosensitizers.
3.3. Third Generation PS: increased tumor selectivity
Beginning in the early 2000s, in vitro PDT studies for GBM shifted towards developing and optimizing nanomedicine delivery systems [141]. Compared to first and second-generation PSs, third-generation PSs tend to have increased local specificity [141], enhanced cellular PS internalization, and improved PS retention. Broadly, third-generation PSs are composed of a broad spectrum of delivery vehicles that have been expounded on, including polymer or lipid based carriers such as liposomes [42,142], organometallic complexes [143,144,145,146], albumin- or antibody-conjugated nanospheres and nanocapsules [147,148,149], micelles [150,151], dendrimers, nanocrystals, and nanogold [152]. Most commonly, many groups have attempted to encapsulate a clinically-approved PS, such as BPD [153,154], m-THPC [155], chloro-aluminum phthalocyanine (AlClPc) [156,157], or indocyanine green [42], within biocompatible nanoparticles and nanoemulsions for more controlled drug delivery and release. In recent years, studies inducing PDT via other anti-tumor drugs [143], chemotherapy combination [158], and upconversion [159] modalities have developed as well.
Upconversion nanoparticles (UCNP) are nanoparticles (NP) that are doped with heavy metals which, when excited, upconvert wavelengths (such as near-infrared) to produce shorter emission wavelengths on the visible or UV scale [160]. Functionalized UCNPs, produced following conjugation with PSs, have been found to induce photodynamic therapeutic effects in GBM via near-infrared triggering [159,161]. Groups have also focused on developing synthetic chlorin derivatives [162]. For instance, synthetic carbonyl-containing chlorin and boron-based PSs have shown dual applications in PDT and boron neutron capture therapy, a tumor specific radiotherapy, in F98 rat glioma-bearing models [163]. Intriguingly, several studies have designed PS-loaded nanocarriers with the ability to deliver exogenous oxygen to tumor tissue to overcome tumor hypoxic conditions. Among these are perfluorocarbon-loaded NPs, oxygen-encapsulating nanobubbles and nanosystems with the ability to convert hydrogen peroxide to oxygen [150,164,165]. In another vein, studies have compounded on PDT-induced hypoxia by co-loading PSs with hypoxia-activated prodrugs into NPs to simultaneously induce photodynamic therapy and deliver chemotherapy [166]. Numerous other groups are working towards designing nanoplatforms that can encapsulate multiple cargos to deliver concomitant PDT/chemotherapy [147,153]. While preliminary results are promising, studies have shown that nanosystem-mediated PDT still exhibits poor drug targeting, premature release into circulation, and lack of real-time drug monitoring [152]. Further work is required before advancing to Phase 0 studies.
4. Optimizing Light Delivery
The extent of PDT therapeutic effect is dependent on the delivery of light. At the optimal excitation wavelength of first-generation PSs (630 nm), light can penetrate tissue to a depth of between 0.8-1.0 cm, with subsequent necrosis expanding 2-7 mm from the point of maximum intensity. While dependent on tissue type and protocol, light dosimetry can be improved by altering light delivery geometry (planar, spherical, cylindrical), light wavelength (longer wavelengths penetrate deeper tissue), light localization (spot delivery vs. interstitial delivery), and light delivery timing (continuous vs. fractionated illumination) [97]. In earlier studies, light was superficially administered by illuminating the margins of the resection cavity or directly onto the tumor tissue surface using laser sources or conventional lamps. To penetrate deeper tissue, later studies have moved toward interstitial (iPDT) or cavitary photoirradiation methods. Interstitial photo-illumination includes the insertion of single or multiple optical fibers into the resection cavity [89]. This type of photoirradiation can be completed following tumor de-bulking or as adjuvant therapy alone. Cavitary photo-illumination occurs following maximum safe tumor resection and includes using a light diffusing medium or inflatable balloon to evenly disperse the light dose. Geometrically, cavitary photoirradiation covers a larger surface area than interstitially inserted fibers [92]. Several novel devices for cavitary PDT have been developed, including a balloon-based device that is currently being tested in the INDYGO trial, a phase I trial in recruitment in Lille, France [167]. One of the most interesting devices, however, has been an inflatable indwelling balloon catheter developed by Madsen et al. that allows for post-operative photo illumination. The device consists of a balloon applicator and a two-lumen catheter with a self-sealing penetrable membrane. Following surgical insertion and wound healing, the skin can be punctured with a needle mandrill, the balloon expanded with a diffusion medium, and threaded with an optical fiber through the lumen to photo irradiate the resection cavity. The balloon can later be deflated and removed after the completion of treatment [168].
In general, conventional laser sources are expensive and carry the risk of unwanted tissue heating. As such, more recent studies have moved toward utilizing light emitting diode (LED) technologies. LEDs have a broad emission spectrum (630-940 nm) and therefore, have the potential to penetrate deeper brain tissue at lower light energies [59]. LED equipment is smaller, easier to use, inexpensive, and provides a wider irradiation area in comparison to lasers. In addition to the aforementioned clinical trial combining LEDs with both HpD and BPD [59], 5-ALA PDT studies have shown that blue LEDs more effectively decrease human glioma cell line viability when compared to conventional red LEDs [169].
Delivering a therapeutic light dose to the targeted tissue remains one of the main clinical challenges of PDT. In 1993, Origitano and colleagues were the first to develop an image-based, computer-assisted treatment planning protocol that individualized light dose volume and geometry with promising results [85]. Since then, many other groups have used mathematical modeling, most commonly Monte Carlo simulations, to predict light propagation and absorption within tissue. This helps ensure adequate light delivery while limiting off-target heating effects [170]. In fact, a pilot trial utilizing theoretical models and 3-D treatment planning to establish patient-specific irradiation schemes has exhibited one of the highest median OS out of all 5-ALA based clinical trials [109].
For 5-ALA-based PDT in particular, fractionated light delivery, rather than continuous illumination, has proven to be more efficacious at inducing a phototoxic response. Fractionation is induced when light irradiation alternates between incremental “light” and “dark” periods, rather than continuous illumination to the treatment field. These transient periods of light interruption allow for tissue re-oxygenation, which enhances PDT efficacy by (i) maximizing the phototoxic effect of the subsequent light period, (ii) allowing re-localization of the PS to tumor areas following PDT-induced PS photobleaching, and (iii) promoting reperfusion injury, a tissue-damaging mechanism that results from re-vascularization of ischaemic tissue [171,172]. Since HpD has been shown to accumulate in cutaneous tissues, often for long periods of time, a fractionated treatment schema is not compatible with HpD or Photofrin-mediated PDT due to toxicity [168]. Over the last decade, a series of in vitro and in vivo pre-clinical studies have been performed comparing 2-fraction, 5-fraction, and continuous light at high and low power for 5-ALA-based PDT. A 5-fraction treatment schema delivered at low power (5 mW) was shown to induce degrees of apoptosis and peripheral pro-vascular effect with limited necrosis higher than those produced by other schemas [172,173,174,175]. The authors also noted that rats with larger tumor volumes and were treated at higher fluence rates more frequently exhibited fatal intracranial pressures. This condition may be a contraindication of PDT in future studies. While the reported effects of fractionated light delivery show promise, further studies are needed to account for the low diversity in single cell line-derived xenograft models. Single cell line-derived tumor models create homogeneous and hypervascularized tumors that do not exhibit spontaneous tumor necrosis and infiltrative patterns characteristic of GBM.
In contrast to phasic and single-shot (25 mW/cm2) photoirradiation, repeated illumination over long durations (weeks) at low fluence rates (≤5 mW/cm2) has seen reduced glioma growth [176]. This finding has initiated a new type of PDT called metronomic photodynamic therapy (mPDT), which involves administering light at subthreshold fluences over extended periods of time. mPDT using LED-coupled fiber light delivered continuously over 24 hours has increased survival and inhibited tumor re-growth in astrocytoma-bearing rats [177]. Other studies have also shown, under both in vitro and in vivo conditions, that low fluence, long duration organic LED-based PDT bears significant anti-tumor effect [176,178]. Currently, the only Phase III PDT clinical trial for brain tumors has implemented mPDT, combining 5-day repetitive 5-ALA/Photofrin mPDT with FGS, yielding outcomes that are comparable to current standards of care [110].
Automation of mPDT has also been explored via telemetric device development in rat GBM models. This implant is placed subcutaneously and contains dual functionality for light delivery and light fluence rate monitoring via a tetherless inductive link. While further work is needed to improve device design and therapeutic administration, the reported model demonstrated successful functionality during a two week implantation period without serious biological complications [179].
5. PDT in other CNS tumors
The use of PDT has also been explored in several other common CNS tumors as well, including meningiomas, pituitary adenomas, and pediatric brain tumors. While these studies have surpassed pre-clinical testing to include clinical application, the bulk of reported results are from in vitro testing.
The utility of PDT in meningioma has been explored using both first- [81,82,92,98,180,181,182,183,184] and second-generation [185,186,187,188,189,190,191,192,193] PSs under both in vitro and clinical conditions. The majority of clinical studies in malignant meningioma (MM) have been conducted using first-generation PSs. However, clinical cohort sizes are not large enough to determine conclusive outcomes of therapeutic efficacy. Similar to malignant glioma studies, PS use quickly shifted to second-generation drugs following their development due to their reduced phototoxicity and improved selectivity. Studies using 5-ALA-induced PDT have found that meningiomas demonstrate irregular fluorescent distribution across the tumor, which implicates higher variability in PS metabolism as compared to malignant glioma. In addition to variable PpIX fluorescence, meningioma cells show lower fluorescence intensity, and therefore PDT efficacy, an attribute that has been remedied by the co-delivery of drugs such as gefitinib (anti-cancer) [189] and ciprofloxacin (antibiotic) [190]. In TS PDT, pre-clinical studies demonstrated two PDT-induced morphologies, both of which mediate tumoricidal effects: apoptotic presentation as characterized by cell body shrinkage and cell necrosis via swelling of the cell body. Additional evidence of cell necrosis was identified at high TS dosages by increased levels of lactate dehydrogenase leakage, a biochemical marker for cell necrosis [191]. Yet, like 5-ALA, TS PDT efficacy in MM is still below that of malignant glioma, warranting further investigation to improve anti-tumor effect [191]. Continued development of third-generation PSs may also further improve PDT utility in malignant meningiomas.
The merit of PDT is particularly notable in cases of highly invasive or diffuse tumors with ambiguous margins. The potential use of PDT for the treatment of native pituitary adenomas (PA) presents a very intriguing option as complete resection of these tumors is often unachievable. Pre-clinical studies of first-generation PS-guided PDT in PAs reported successful cytotoxicity and anti-tumor effect in both in vitro and mice models [194,195]. Currently, clinical studies on PDT use for PAs have used first-generation PSs for therapy. These reports demonstrated high feasibility for PDT use, yielding an approximately 50% increase in tumor tissue retention than gliomas [196]. Additionally, longitudinal monitoring of this cohort found that the majority of patients recovered partial/full acuity of their visual fields [197]. In vitro studies have also probed 5-ALA PDT efficacy across various dosages using immortalized rat pituitary adenoma cells (GH3), AtT-20 cell lines, and human pituitary adenoma cells, quantifying PpIX fluorescence and probing cytotoxicity within surviving cells. These two studies yielded conflicting results which may be attributed to different culture conditions and inconsistent protocols. However, it can be said that all cell lines displayed a 5-ALA-induced, cell line-dependent endogenous fluorescence, suggesting varying PS uptake and metabolism [198], and that dose-dependent toxicity unique to each cell line was evident as well [199]. Further work will be required to better understand the feasibility and efficacy of second-generation PSs before proceeding to in vivo and clinical studies.
Another class of CNS tumors that are generally restrained to subtotal surgical resection and adjuvant treatment are chordomas, a rare, aggressive sarcoma of the skull base and sacrum. Not only do post-resection margins facilitate high rates of infiltrative recurrence, but these tumors are also typically both chemo- and radiotherapy resistant, stipulating alternative anti-tumor treatment modalities. While PDT for chordomas has not been very well studied, two consecutive in vitro cytotoxicity studies have demonstrated tumoricidal effect following 5-ALA PDT [200], with elevated efficacy following the administration of the antibiotic, ciprofloxacin [201]. Given the similar pattern of antibiotic-elevated PDT performance as is found in gliomas, it is likely that, through further study, PDT may be highly efficacious for chondromas, holding promise for future clinical chondroma management.
Although all the aforementioned studies on PDT efficacy have been performed on adult CNS tumors, pre-clinical and clinical studies have also been performed evaluating the performance of PDT in pediatric brain tumors via second-generation PSs such as 5-ALA and TS [202,203,204]. One of the most recent reports evaluating PDT feasibility for malignant pediatric brain tumors has reported on treatment using TS in children and young adolescents with brain tumors, including diffuse midline glioma (DMG), glioblastoma, and high-grade glioma. Not only was TS PDT found to be safe for use at dosages comparable to those used in adults, but adverse events commonly identified in adult patients also were not found in children following therapy [205]. These results are incredibly encouraging for PDT usage for pediatric CNS tumors. Further reports, such as those from current clinical trials (UMIN000030883 and NCT04738162), however, are required to better define the efficacy of PDT in this application.
6. Limitations
6.1. Limitations of PDT and its synergistic agents
The application of PDT for the treatment of gliomas is not without limitations. Technical limitations include relatively high costs, the requirement of specialized equipment, multiport lasers, and medical device class III approved light applicators which are limited to few neurosurgical centers [206]. Biological limitations include variable PS accumulation in tissues, inadequate penetration of light into deeper regions, heterogeneity of response from variant light penetration depth, reduced efficacy in hypoxic regions, and photobleaching [105]. Furthermore, PS uptake is highly dependent on the cell metabolic state. For example, in vitro studies have demonstrated an enhanced PpIX accumulation in the tumor tissues and a complementary increase in the efficacy of PDT following the upregulation or presence of ATP-binding cascade (ABC) transporters inhibitors [207], iron chelators [208], calcitriol [209], arsenic trioxide [210], NF-kappaB inhibitors [211]. Despite this high relevance to malignant glioma states, further investigation, as is currently being done in third-generation PS testing, to improve tumor specificity through alternative avenues such as protein markers is warranted.
6.2. PDT efficacy negatively influenced by harsh glioma microenvironment
Largely, there are two limitations to PDT efficacy that occur as a function of the tumor microenvironment (TME). The highly hypoxic nature of the TME reduces oxygen availability for subsequent singlet oxygen production, thereby reducing the success of PDT [150,164]. This limitation must be taken into account during the literature review, as most reports investigating PDT do so in cell lines at atmospheric oxygen concentrations (~20%) as compared to the hypoxic concentrations typical of glioma (~5-15%) [150,212]. This is especially relevant for 5-ALA-driven PDT, which requires approximately 20% more irradiation under hypoxic conditions to invoke equitable rates of therapeutic success as seen under normoxic environments [212].
The second limitation is the competitive uptake of PS by surrounding glial cells and neurons. Competitive uptake reduces PS availability, thereby decreasing photosensitizer accumulation in tumor cells. Successful efforts, however, have modulated local temperature and demonstrated increased PS uptake solely in cancer cells. Studies from as early as 1995 have shown that induction of moderate hyperthermia or hypothermia increases the efficacy of PDT in normal brain [213] and cancer cells. Moderate hypothermia (32-34°C) has been shown to increase PpIX concentrations in glioma cell lines in addition to conferring neuroprotection and increasing PDT therapeutic index [214]. Interestingly, moderate hypothermia has also been demonstrated to increase synergism between PDT and concurrent adjuvant therapies such as conventional chemotherapy [215] or targeted inhibitors [216].
Other studies have also utilized innovative strategies to combat these limitations in a joint fashion. Micro-optical devices and nanoparticle lipid emulsions have been designed to co-deliver photosensitizer and exogenous oxygen to increase local oxygen concentrations [150,217]. These lipid emulsions and nanoparticles also improve cellular uptake of various photosensitizers, including Ce6 and 5-ALA, and have been shown to lead to significant increases in PDT efficacy and survival rates in glioma bearing mice [150,164,165].
6.3. Innate PDT resistance
While one of the main advantages of PDT is its ability to circumvent chemotherapeutic resistance, there are certain pathways of resistance to PDT that are either found in or acquired by glioma. This is primarily facilitated by nitric oxide synthase (NOS) and its inducible counterpart (iNOS), which produce intracellular nitric oxide [218]. In fact, exposure to 5-ALA PDT leads to an increase in cytoprotective iNOS expression, resulting in a change in phenotype to iNOS/NO dependent proliferation, migration, and invasion rate [219]. Further study of this pathway revealed that iNOS expression is regulated by acetylation of NF-κB by bromodomain and extra-terminal (BET) protein. However, NO scavengers, iNOS inhibitors, and BET inhibitors can be used to inhibit iNOS/NO dependent tumor progression while also increasing the rate of apoptosis and PDT therapeutic efficacy [219,220].
While nitric oxide synthesis is one of the more well-studied mechanisms of PDT resistance, there is another mechanism of PDT resistance that has been characterized in gliomas. Studies in U87 cells show that TP53 upregulates ALKBH2 in cells that survive PDT by binding to its promoter, contributing to the reversal of DNA damage, thereby promoting tumor proliferation [221].
6.4. Peri-tumor edema limits PDT efficacy
While PDT can act synergistically with chemotherapy, it also increases the extent of peritumoral edema, which in turn decreases the therapeutic efficacy of PDT. To address this, researchers have investigated using different loop diuretics, such as torasemide [222] and bumetanide [223], to relieve peritumoral edema. In rats and xenograft models, this has been shown to supplement PDT efficacy, inhibiting tumor growth and prolonging survival.
6.5. PDT drug interactions and synergistic agents
Other limitations of PDT include dose-dependence and unwanted drug reactions. Studies have shown that the effects of PDT can be dose-dependent in a non-linear fashion for certain photosensitizers, and that exceeding a certain dosage may decrease photodynamic toxicity due to changes in intracellular localization [224]. PDT efficacy can be limited by drugs such as phenytoin, an anti-seizure medication, which reduces the accumulation of 5-ALA in glioma cell lines [225]. As such, there is an imminent need for synergistic agents that increase PDT efficacy. While few in number, there are several FDA-approved drugs found on the market that show promise in this arena. Reports have shown that polyphenol PKCδ regulators, such as hypericin and rottlerin, enhance PDT-induced apoptosis of GBM cells. Further, drugs such as atorvastatin have shown reduced PDT-induced functional deficits in rats [226,227]. The need for synergistic agents has also resulted in the development of novel technologies and the identification of targets for gene therapy. Recent reports show that delivery of micelles with peptide irDG conjugated photosensitizers results in greater BBB penetration and that upregulation of Cx43, affiliated with poor GBM prognosis [228], improves the efficacy of PDT [151,229].
7. Conclusions and future directions
While the literature depicts a series of PDT advancements in glioma care beginning in the 1980′s, the majority of notable studies have been conducted out of a limited number of institutions. These clinical trials have consisted of small, non-randomized, and histologically diverse patient cohorts, and lack “alternative therapeutic” control cohorts, complicating robust assessment. Furthermore, many photosensitizers (PS) and light delivery methods each produce different phototoxic outcomes, which are further convoluted by the cell-dependent response. This variability is reflected in the diversity of preclinical glioma PDT studies.
Photodynamic therapy is a promising avenue for malignant glioma management, addressing several current challenges in treatment, such as targeted tumor treatment. However, it is unlikely that single drug PDT will be sufficient to treat the genetically and phenotypically diverse landscape of glioma. While further studies are required, a multimodal regimen of PDT in combination with standard radiotherapy and targeted immunotherapies, or engineered delivery modalities bears promising effects and may elevate the current efficacy of PDT to a higher level.
Author Contributions
Hsia, T. and Small, J.L. performed literature search, drafted, and edited the manuscript. Yekula, A., Batool, S.M., Escobedo, A.K., Ekanayake, E., You, D.G., and Lee, H. reviewed and edited the manuscript. Carter, B.S. and Balaj, L. reviewed, edited, and oversaw manuscript preparation. All authors have read and agreed to the published version of the manuscript.
Funding
This work is supported by grants awarded by the National Institutes of Health: R01 CA239078 (BSC, HL, LB), R01 CA237500 (BSC, LB, HL), U01 CA230697 (BSC, LB). The funding sources had no role in either the writing of the manuscript or the decision to submit the manuscript for publication. The authors have not been paid to write this article. The corresponding author has full access to the manuscript and assumes final responsibility for the decision to submit for publication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30.
- Das, S. & Marsden, P. A. Angiogenesis in Glioblastoma. New England Journal of Medicine vol. 369 1561–1563. 2013. [CrossRef]
- Stupp, R. Stupp, R. et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. The Lancet Oncology vol. 10 459–466. 2009. [Google Scholar] [CrossRef]
- Stupp, R. et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [CrossRef] [PubMed]
- Majewska, P. et al. Postprogression survival in patients with glioblastoma treated with concurrent chemoradiotherapy: a routine care cohort study. CNS Oncol 2017, 6, 307–313. [CrossRef]
- Parker, N. R. , Khong, P., Parkinson, J. F., Howell, V. M. & Wheeler, H. R. Molecular Heterogeneity in Glioblastoma: Potential Clinical Implications. Front. Oncol. 0, (2015).
- DeCordova, S. et al. Molecular Heterogeneity and Immunosuppressive Microenvironment in Glioblastoma. Front. Immunol. 0, (2020).
- Management of glioblastoma after recurrence: A changing paradigm. J. Egypt. Natl. Canc. Inst. 2016, 28, 199–210. [CrossRef] [PubMed]
- Gallego, O. Nonsurgical treatment of recurrent glioblastoma. Curr. Oncol. 22, (2015).
- Weller, M. , Cloughesy, T., Perry, J. R. & Wick, W. Standards of care for treatment of recurrent glioblastoma--are we there yet? Neuro. Oncol. 15, (2013).
- dos Santos, M. A. et al. Systematic review and meta-analysis of phase I/II targeted therapy combined with radiotherapy in patients with glioblastoma multiforme: quality of report, toxicity, and survival. J. Neurooncol. 2015, 123, 307–314. [CrossRef]
- Su, J. et al. Molecularly Targeted Drugs Plus Radiotherapy and Temozolomide Treatment for Newly Diagnosed Glioblastoma: A Meta-Analysis and Systematic Review. 2016. [Google Scholar] [CrossRef]
- Laws, E. R., Jr, Cortese, D. A., Kinsey, J. H., Eagan, R. T. & Anderson, R. E. Photoradiation therapy in the treatment of malignant brain tumors: a phase I (feasibility) study. Neurosurgery. 1981, 9, 672–678.
- Dougherty, T. J. et al. Photoradiation therapy for the treatment of malignant tumors. Cancer Res. 1978, 38, 2628–2635.
- da Silva, B. A. et al. Novel Scintillating Nanoparticles for Potential Application in Photodynamic Cancer Therapy. Pharmaceutics 14, (2022).
- Vedunova, M. et al. DC vaccines loaded with glioma cells killed by photodynamic therapy induce Th17 anti-tumor immunity and provide a four-gene signature for glioma prognosis. Cell Death Dis. 2022, 13, 1062.
- Plaetzer, K., Krammer, B., Berlanda, J., Berr, F. & Kiesslich, T. Photophysics and photochemistry of photodynamic therapy: fundamental aspects. Lasers Med. Sci. 2009, 24, 259–268.
- Hirschberg, H. , Berg, K. & Peng, Q. Photodynamic therapy mediated immune therapy of brain tumors. Neuroimmunol Neuroinflamm 5, (2018).
- Cramer, S. W. & Chen, C. C. Photodynamic Therapy for the Treatment of Glioblastoma. Front Surg. 2019, 6, 81.
- Castano, A. P., Mroz, P. & Hamblin, M. R. Photodynamic therapy and anti-tumour immunity. Nature Reviews Cancer 2006, vol. 6 535–545 . [CrossRef]
- Dougherty, T. J. et al. Photodynamic therapy. J. Natl. Cancer Inst. 1998, 90, 889–905. [CrossRef] [PubMed]
- Cramer, S. W. & Chen, C. C. Photodynamic Therapy for the Treatment of Glioblastoma. Front Surg. 2019, 6, 81.
- Agostinis, P. et al. Photodynamic therapy of cancer: an update. CA Cancer J. Clin. 2011, 61, 250–281. [CrossRef] [PubMed]
- Miki, Y., Akimoto, J., Moritake, K., Hironaka, C. & Fujiwara, Y. Photodynamic therapy using talaporfin sodium induces concentration-dependent programmed necroptosis in human glioblastoma T98G cells. Lasers Med. Sci. 2015, 30, 1739–1745.
- Castano, A. P., Demidova, T. N. & Hamblin, M. R. Mechanisms in photodynamic therapy: part one-photosensitizers, photochemistry and cellular localization. Photodiagnosis Photodyn. Ther. 2004, 1, 279–293.
- Castano, A. P., Demidova, T. N. & Hamblin, M. R. Mechanisms in photodynamic therapy: part two—cellular signaling, cell metabolism and modes of cell death. Photodiagnosis and Photodynamic Therapy 2005, vol. 2 1-23. [CrossRef]
- Castano, A. P., Demidova, T. N. & Hamblin, M. R. Mechanisms in photodynamic therapy: Part three—Photosensitizer pharmacokinetics, biodistribution, tumor localization and modes of tumor destruction. Photodiagnosis and Photodynamic Therapy 2005, vol. 2 91–106. [CrossRef]
- Stylli, S. S. & Kaye, A. H. Photodynamic therapy of cerebral glioma – A review Part I – A biological basis. Journal of Clinical Neuroscience 2006, vol. 13 615-625 . [CrossRef]
- Miki, Y., Akimoto, J., Hiranuma, M. & Fujiwara, Y. Effect of talaporfin sodium-mediated photodynamic therapy on cell death modalities in human glioblastoma T98G cells. J. Toxicol. Sci. 2014, 39, 821–827.
- Schimanski, A. et al. Human glioblastoma stem-like cells accumulate protoporphyrin IX when subjected to exogenous 5-aminolaevulinic acid, rendering them sensitive to photodynamic treatment. Journal of Photochemistry and Photobiology B: Biology 2016, vol. 163 203–210 . [CrossRef]
- Fujishiro, T. et al. 5-Aminolevulinic acid-mediated photodynamic therapy can target human glioma stem-like cells refractory to antineoplastic agents. Photodiagnosis Photodyn. Ther. 2018, 24, 58–68. [CrossRef]
- Auffinger, B. et al. Conversion of differentiated cancer cells into cancer stem-like cells in a glioblastoma model after primary chemotherapy. Cell Death & Differentiation 2014, vol. 21 1119–1131 . [CrossRef]
- Jackson, M., Hassiotou, F. & Nowak, A. Glioblastoma stem-like cells: at the root of tumor recurrence and a therapeutic target. Carcinogenesis. 2015, 36, 177–185.
- Fisher, C. et al. Liposomal Lapatinib in Combination with Low-Dose Photodynamic Therapy for the Treatment of Glioma. J. Clin. Med. Res. 8, (2019).
- Madsen, S. J. et al. Increased nanoparticle-loaded exogenous macrophage migration into the brain following PDT-induced blood-brain barrier disruption. Lasers Surg. Med. 2013, 45, 524–532. [CrossRef]
- Hanahan, D. & Weinberg, R. A. Hallmarks of cancer: the next generation. Cell. 2011, 144, 646–674.
- Dolmans, D. E. J. G. J., Fukumura, D. & Jain, R. K. Photodynamic therapy for cancer. Nat. Rev. Cancer. 2003, 3, 380–387.
- Yi, W. et al. Photodynamic therapy mediated by 5-aminolevulinic acid suppresses gliomas growth by decreasing the microvessels. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2015, 35, 259–264. [CrossRef] [PubMed]
- Etminan, N. et al. Modulation of migratory activity and invasiveness of human glioma spheroids following 5-aminolevulinic acid-based photodynamic treatment. Laboratory investigation. J. Neurosurg. 2011, 115, 281–288. [CrossRef] [PubMed]
- Li, F. et al. Photodynamic therapy boosts anti-glioma immunity in mice: a dependence on the activities of T cells and complement C3. J. Cell. Biochem. 2011, 112, 3035–3043. [CrossRef] [PubMed]
- Etminan, N. et al. Heat-shock protein 70-dependent dendritic cell activation by 5-aminolevulinic acid-mediated photodynamic treatment of human glioblastoma spheroids in vitro. Br. J. Cancer 2011, 105, 961–969. [CrossRef] [PubMed]
- Shibata, S. et al. Photo-immune therapy with liposomally formulated phospholipid-conjugated indocyanine green induces specific antitumor responses with heat shock protein-70 expression in a glioblastoma model. Oncotarget vol. 10 175–183. 2019. [CrossRef]
- Turubanova, V. D. et al. Immunogenic cell death induced by a new photodynamic therapy based on photosens and photodithazine. J Immunother Cancer 2019, 7, 350. [CrossRef]
- Helbig, D., Simon, J. C. & Paasch, U. Photodynamic therapy and the role of heat shock protein 70. Int. J. Hyperthermia. 2011, 27, 802–810.
- Zhou, F., Xing, D. & Chen, W. R. Regulation of HSP70 on activating macrophages using PDT-induced apoptotic cells. Int. J. Cancer. 2009, 125, 1380–1389.
- Kammerer, R. et al. Induction of immune mediators in glioma and prostate cancer cells by non-lethal photodynamic therapy. PLoS One 6, e21834 (2011).
- Xie, W. et al. The Destruction Of Laser-Induced Phase-Transition Nanoparticles Triggered By Low-Intensity Ultrasound: An Innovative Modality To Enhance The Immunological Treatment Of Ovarian Cancer Cells. Int. J. Nanomedicine 2019, 14, 9377–9393. [CrossRef]
- Yang, W. et al. Smart Nanovesicle-Mediated Immunogenic Cell Death through Tumor Microenvironment Modulation for Effective Photodynamic Immunotherapy. ACS Nano 2020, 14, 620–631. [CrossRef]
- Ni, J. et al. Dendritic cell vaccine for the effective immunotherapy of breast cancer. Biomed. Pharmacother. 2020, 126, 110046. [CrossRef] [PubMed]
- He, H. et al. Tumor-targeted nanoplatform for in situ oxygenation-boosted immunogenic phototherapy of colorectal cancer. Acta Biomater. 2020, 104, 188–197. [CrossRef] [PubMed]
- Wang, H. et al. Engineering antigen as photosensitiser nanocarrier to facilitate ROS triggered immune cascade for photodynamic immunotherapy. Biomaterials 2020, 244, 119964. [CrossRef] [PubMed]
- Wang, T. et al. Light-Enhanced O2-Evolving Nanoparticles Boost Photodynamic Therapy To Elicit Antitumor Immunity. ACS Applied Materials & Interfaces vol. 11 16367–16379. 2019. [CrossRef]
- Doix, B., Trempolec, N., Riant, O. & Feron, O. Low Photosensitizer Dose and Early Radiotherapy Enhance Antitumor Immune Response of Photodynamic Therapy-Based Dendritic Cell Vaccination. Front. Oncol. 2019, 9, 811.
- Liu, D. et al. Correction to Redox-Activated Porphyrin-Based Liposome Remote-Loaded with Indoleamine 2,3-Dioxygenase (IDO) Inhibitor for Synergistic Photoimmunotherapy through Induction of Immunogenic Cell Death and Blockage of IDO Pathway. Nano Lett. 2020, 20, 1476. [CrossRef]
- Olzowy, B. et al. Photoirradiation therapy of experimental malignant glioma with 5-aminolevulinic acid. J. Neurosurg. 2002, 97, 970–976. [CrossRef]
- Kostron, H., Obwegeser, A., Jakober, R., Zimmermann, A. & Rueck, A. C. Experimental and clinical results of mTHPC (Foscan)-mediated photodynamic therapy for malignant brain tumors. Optical Methods for Tumor Treatment and Detections: Mechanisms and Techniques in Photodynamic Therapy VII. Optical Methods for Tumor Treatment and Detections, 1998. [CrossRef]
- Callahan, D. E. et al. Boronated protoporphyrin (BOPP): localization in lysosomes of the human glioma cell line SF-767 with uptake modulated by lipoprotein levels. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 761–771. [Google Scholar] [CrossRef]
- Aveline, B., Hasan, T. & Redmond, R. W. Photophysical and photosensitizing properties of benzoporphyrin derivative monoacid ring A (BPD-MA). Photochem. Photobiol. 1994, 59, 328–335.
- Schmidt, M. H. et al. Evaluation of photodynamic therapy near functional brain tissue in patients with recurrent brain tumors. J. Neurooncol. 2004, 67, 201–207. [Google Scholar] [CrossRef]
- Fingar, V. H. et al. Analysis of acute vascular damage after photodynamic therapy using benzoporphyrin derivative (BPD). Br. J. Cancer 1999, 79, 1702–1708. [Google Scholar] [CrossRef]
- Fingar, V. H., Wieman, T. J. & Haydon, P. S. The effects of thrombocytopenia on vessel stasis and macromolecular leakage after photodynamic therapy using photofrin. Photochem. Photobiol. 1997, 66, 513–517.
- Sharman, W. M., Allen, C. M. & van Lier JE. Photodynamic therapeutics: basic principles and clinical applications. Drug Discov. Today. 1999, 4, 507–517.
- Gao, S.-G. et al. [Absorption and elimination of photofrin-II in human immortalization esophageal epithelial cell line SHEE and its malignant transformation cell line SHEEC]. Ai Zheng 2009, 28, 1248–1254. [Google Scholar] [CrossRef]
- Schweitzer, V. G. Photodynamic therapy for treatment of head and neck cancer. Otolaryngol. Head Neck Surg. 1990, 102, 225–232. [Google Scholar] [CrossRef]
- Kim, M. M. & Darafsheh, A. Light Sources and Dosimetry Techniques for Photodynamic Therapy. Photochem. Photobiol. 2020, 96, 280–294.
- Shimizu, K. et al. Intraoperative Photodynamic Diagnosis Using Talaporfin Sodium Simultaneously Applied for Photodynamic Therapy against Malignant Glioma: A Prospective Clinical Study. Front. Neurol. 2018, 9, 24. [Google Scholar] [CrossRef]
- Tetard, M.-C., Vermandel, M., Mordon, S., Lejeune, J.-P. & Reyns, N. Experimental use of photodynamic therapy in high grade gliomas: a review focused on 5-aminolevulinic acid. Photodiagnosis Photodyn. Ther. 2014, 11, 319–330.
- Mahmoudi, K. et al. 5-aminolevulinic acid photodynamic therapy for the treatment of high-grade gliomas. J. Neurooncol. 2019, 141, 595–607. [Google Scholar] [CrossRef]
- Cramer, S. W. & Chen, C. C. Photodynamic Therapy for the Treatment of Glioblastoma. Front Surg. 2019, 6, 81.
- Lipson, R. L., Baldes, E. J. & Olsen, A. M. HEMATOPORPHYRIN DERIVATIVE: A NEW AID FOR ENDOSCOPIC DETECTION OF MALIGNANT DISEASE. The Journal of Thoracic and Cardiovascular Surgery vol. 42 623–629. 1961. [CrossRef]
- Lipson, R. L. & Baldes, E. J. The photodynamic properties of a particular hematoporphyrin derivative. Arch. Dermatol. 1960, 82, 508–516.
- Kessel, D. Hematoporphyrin and HPD: photophysics, photochemistry and phototherapy. Photochem. Photobiol. 1984, 39, 851–859. [Google Scholar] [CrossRef] [PubMed]
- Tomio, L. et al. Elimination pathway of hematoporphyrin from normal and tumor-bearing rats. Tumori 1982, 68, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.-X. et al. Underlying mechanism of the photodynamic activity of hematoporphyrin induced apoptosis in U87 glioma cells. Int. J. Mol. Med. 2018, 41, 2288–2296. [Google Scholar] [CrossRef] [PubMed]
- Perria, C. et al. Fast attempts at the photodynamic treatment of human gliomas. J. Neurosurg. Sci. 1980, 24, 119–129. [Google Scholar]
- McCulloch, G. A. et al. Phototherapy in malignant brain tumors. Prog. Clin. Biol. Res. 1984, 170, 709–717. [Google Scholar]
- Kaye, A. H., Morstyn, G. & Brownbill, D. Adjuvant high-dose photoradiation therapy in the treatment of cerebral glioma: a Phase 1–2 study. Journal of Neurosurgery vol. 67 500–505. 1987. [CrossRef]
- Muller, P. J. & Wilson, B. C. Photodynamic therapy: cavitary photoillumination of malignant cerebral tumours using a laser coupled inflatable balloon. Can. J. Neurol. Sci. 1985, 12, 371–373.
- Kostron, H., Weiser, G., Fritsch, E. & Grunert, V. Photodynamic therapy of malignant brain tumors: clinical and neuropathological results. Photochem. Photobiol. 1987, 46, 937–943.
- Muller, P. J. & Wilson, B. C. Photodynamic therapy of malignant primary brain tumours: clinical effects, post-operative ICP, and light penetration of the brain. Photochem. Photobiol. 1987, 46, 929–935.
- Kostron, H., Fritsch, E. & Grunert, V. Photodynamic therapy of malignant brain tumours: a phase I/II trial. Br. J. Neurosurg. 1988, 2, 241–248.
- Kostron, H., Plangger, C., Fritsch, E. & Maier, H. Photodynamic treatment of malignant brain tumors. Wien. Klin. Wochenschr. 1990, 102, 531–535.
- Powers, S. K. , Cush, S. S., Walstad, D. L. & Kwock, L. Stereotactic intratumoral photodynamic therapy for recurrent malignant brain tumors. Neurosurgery 29, 688–95; discussion 695–6 (1991).
- Muller, P. J. & Wilson, B. C. Photodynamic therapy of malignant brain tumours. Lasers Med. Sci. 1990, 5, 245–252.
- Origitano, T. C. & Reichman, O. H. Photodynamic therapy for intracranial neoplasms: development of an image-based computer-assisted protocol for photodynamic therapy of intracranial neoplasms. Neurosurgery 32, 587–95; discussion 595–6 (1993).
- Muller, P. J. & Wilson, B. C. Photodynamic therapy for recurrent supratentorial gliomas. Semin. Surg. Oncol. 1995, 11, 346–354.
- Popovic, E. A., Kaye, A. H. & Hill, J. S. Photodynamic therapy of brain tumors. Seminars in Surgical Oncology vol. 11 335–345. [CrossRef]
- Muller, P. J. & Wilson, B. C. Photodynamic therapy of supratentorial gliomas. in Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy VI vol. 2972 14–26 (SPIE, 1997).
- Muller, P. J. et al. Photofrin photodynamic therapy for malignant brain tumors. Optical Methods for Tumor Treatment and Detection: Mechanisms and Techniques in Photodynamic Therapy X. 2001. [CrossRef]
- Stylli, S. S., Howes, M., MacGregor, L., Rajendra, P. & Kaye, A. H. Photodynamic therapy of brain tumours: evaluation of porphyrin uptake versus clinical outcome. J. Clin. Neurosci. 2004. 2004, 11, 584–596.
- Stylli, S. S., Kaye, A. H., MacGregor, L., Howes, M. & Rajendra, P. Photodynamic therapy of high grade glioma - long term survival. 2005, 12, 389–398.
- Muller, P. J. & Wilson, B. C. Photodynamic therapy of brain tumors--a work in progress. Lasers Surg. Med. 2006, 38, 384–389.
- Kaneko, S. Recent Advances in PDD and PDT for Malignant Brain Tumors. The Review of Laser Engineering 2008, 36, 1351–1354. [Google Scholar] [CrossRef]
- Perria, C. et al. Photodynamic therapy of malignant brain tumors: clinical results of, difficulties with, questions about, and future prospects for the neurosurgical applications. Neurosurgery 1988, 23, 557–563. [Google Scholar] [CrossRef]
- Forbes, I. J. et al. PHOTOTHERAPY OF HUMAN TUMOURS USING HAEMATOPORPHYRIN DERIVATIVE. Medical Journal of Australia vol. 2 489–493. 1980. [CrossRef]
- Kostron, H., Obwegeser, A. & Jakober, R. Photodynamic therapy in neurosurgery: a review. J. Photochem. Photobiol. B. 1996, 36, 157–168.
- Quirk, B. J. et al. Photodynamic therapy (PDT) for malignant brain tumors – Where do we stand? Photodiagnosis and Photodynamic Therapy 2015, vol. 12 530–544 . [CrossRef]
- Kostron, H. , Hochleitner, B. W., Obwegeser, A. & Seiwald, M. Clinical and experimental results of photodynamic therapy in neurosurgery. in 5th International Photodynamic Association Biennial Meeting (ed. Cortese, D. A.) vol. 2371 126–128 (SPIE, 1994).
- Gunaydin, G., Gedik, M. E. & Ayan, S. Photodynamic Therapy for the Treatment and Diagnosis of Cancer-A Review of the Current Clinical Status. Front Chem. 2021, 9, 686303.
- Du, P. et al. Photodynamic therapy leads to death of C6 glioma cells partly through AMPAR. Brain Res. 2012, 1433, 153–159. [Google Scholar] [CrossRef]
- Hu, S.-L., Du, P., Hu, R., Li, F. & Feng, H. Imbalance of Ca2+ and K+ fluxes in C6 glioma cells after PDT measured with scanning ion-selective electrode technique. Lasers Med. Sci. 2014, 29, 1261–1267.
- Dąbrowski, J. M. & Arnaut, L. G. Photodynamic therapy (PDT) of cancer: from local to systemic treatment. Photochem. Photobiol. Sci. 2015, 14, 1765–1780.
- Tirapelli, L. F. et al. Apoptosis in glioma cells treated with PDT. Photomed. Laser Surg. 2011, 29, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Park, J. , Lee, Y.-K., Park, I.-K. & Hwang, S. R. Current Limitations and Recent Progress in Nanomedicine for Clinically Available Photodynamic Therapy. Biomedicines 9, (2021).
- Baskaran, R., Lee, J. & Yang, S.-G. Clinical development of photodynamic agents and therapeutic applications. Biomater Res. 2018, 22, 25.
- Kostron, H., Fiegele, T. & Akatuna, E. Combination of FOSCAN® mediated fluorescence guided resection and photodynamic treatment as new therapeutic concept for malignant brain tumors. Medical Laser Application 2006, vol. 21 285–290 . [CrossRef]
- Rosenthal, M. A. et al. Phase I and pharmacokinetic study of photodynamic therapy for high-grade gliomas using a novel boronated porphyrin. J. Clin. Oncol. 2001, 19, 519–524. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, M. A., Kavar, B., Uren, S. & Kaye, A. H. Promising survival in patients with high-grade gliomas following therapy with a novel boronated porphyrin. J. Clin. Neurosci. 2003, 10, 425–427.
- Beck, T. J. et al. Interstitial photodynamic therapy of nonresectable malignant glioma recurrences using 5-aminolevulinic acid induced protoporphyrin IX. Lasers Surg. Med. 2007, 39, 386–393. [Google Scholar] [CrossRef]
- Eljamel, M. S., Goodman, C. & Moseley, H. ALA and Photofrin fluorescence-guided resection and repetitive PDT in glioblastoma multiforme: a single centre Phase III randomised controlled trial. Lasers Med. Sci. 2008, 23, 361–367.
- Stepp, H. G. et al. Fluorescence-guided resections and photodynamic therapy for malignant gliomas using 5-aminolevulinic acid. in Photonic Therapeutics and Diagnostics vol. 5686 547–557 (SPIE, 2005).
- Stepp, H. et al. ALA and malignant glioma: fluorescence-guided resection and photodynamic treatment. J. Environ. Pathol. Toxicol. Oncol. 2007, 26, 157–164. [Google Scholar] [CrossRef]
- Akimoto, J., Haraoka, J. & Aizawa, K. Preliminary clinical report on safety and efficacy of photodynamic therapy using talaporfin sodium for malignant gliomas. Photodiagnosis Photodyn. Ther. 2012, 9, 91–99.
- Lyons, M., Phang, I. & Eljamel, S. The effects of PDT in primary malignant brain tumours could be improved by intraoperative radiotherapy. Photodiagnosis Photodyn. Ther. 2012, 9, 40–45.
- Johansson, A. et al. Protoporphyrin IX Fluorescence and Photobleaching During Interstitial Photodynamic Therapy of Malignant Gliomas for Early Treatment Prognosis. Lasers in Surgery and Medicine vol. 45 225–234. 2013. [CrossRef]
- Muragaki, Y. et al. Phase II clinical study on intraoperative photodynamic therapy with talaporfin sodium and semiconductor laser in patients with malignant brain tumors. J. Neurosurg. 2013, 119, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, C., Rühm, A., Tonn, J.-C., Kreth, S. & Kreth, F.-W. SURG-25INTERSTITIAL PHOTODYNAMIC THERAPY OF DE-NOVO GLIOBLASTOMA MULTIFORME WHO IV. Neuro-Oncology vol. 17 v219.5–v220. 2015. [CrossRef]
- Vanaclocha, V. et al. Photodynamic therapy in the treatment of brain tumours. A feasibility study. Photodiagnosis Photodyn. Ther. 2015, 12, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Nitta, M. et al. Role of photodynamic therapy using talaporfin sodium and a semiconductor laser in patients with newly diagnosed glioblastoma. J. Neurosurg. 1–8 (2018).
- Lietke, S. et al. Interstitial Photodynamic Therapy Using 5-ALA for Malignant Glioma Recurrences. Cancers 13, (2021).
- Vermandel, M. et al. Standardized intraoperative 5-ALA photodynamic therapy for newly diagnosed glioblastoma patients: a preliminary analysis of the INDYGO clinical trial. J. Neurooncol. 2021, 152, 501–514. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, T. et al. Therapeutic Options for Recurrent Glioblastoma-Efficacy of Talaporfin Sodium Mediated Photodynamic Therapy. Pharmaceutics 14, (2022).
- Kozlikina, E. I. , Trifonov, I. S., Sinkin, M. V., Krylov, V. V. & Loschenov, V. B. The Combined Use of 5-ALA and Chlorin e6 Photosensitizers for Fluorescence-Guided Resection and Photodynamic Therapy under Neurophysiological Control for Recurrent Glioblastoma in the Functional Motor Area after Ineffective Use of 5-ALA: Preliminary Results. Bioengineering (Basel) 9, (2022).
- Neagu, M. et al. Toxicological and efficacy assessment of post-transition metal (Indium) phthalocyanine for photodynamic therapy in neuroblastoma. Oncotarget 2016, 7, 69718–69732. [Google Scholar] [CrossRef]
- Velazquez, F. N. et al. Effectiveness of ZnPc and of an amine derivative to inactivate Glioblastoma cells by Photodynamic Therapy: an in vitro comparative study. Sci. Rep. 2019, 9, 3010. [Google Scholar] [CrossRef]
- Stylli, S., Hill, J., Sawyer, W. & Kaye, A. Aluminium phthalocyanine mediated photodynamic therapy in experimental malignant glioma. J. Clin. Neurosci. 1995, 2, 146–151.
- de Paula, L. B., Primo, F. L., Pinto, M. R., Morais, P. C. & Tedesco, A. C. Evaluation of a chloroaluminium phthalocyanine-loaded magnetic nanoemulsion as a drug delivery device to treat glioblastoma using hyperthermia and photodynamic therapy. RSC Adv. 2017, 7, 9115–9122.
- Chelakkot, V. S. et al. MEK reduces cancer-specific PpIX accumulation through the RSK-ABCB1 and HIF-1α-FECH axes. Sci. Rep. 2020, 10, 22124. [Google Scholar] [CrossRef]
- Hagiya, Y. et al. Pivotal roles of peptide transporter PEPT1 and ATP-binding cassette (ABC) transporter ABCG2 in 5-aminolevulinic acid (ALA)-based photocytotoxicity of gastric cancer cells in vitro. Photodiagnosis Photodyn. Ther. 2012, 9, 204–214. [Google Scholar] [CrossRef]
- Kobuchi, H. et al. Mitochondrial localization of ABC transporter ABCG2 and its function in 5-aminolevulinic acid-mediated protoporphyrin IX accumulation. PLoS One 7, e50082 (2012).
- Ishizuka, M. et al. Novel development of 5-aminolevurinic acid (ALA) in cancer diagnoses and therapy. Int. Immunopharmacol. 2011, 11, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Markwardt, N. A. et al. 405 nm versus 633 nm for protoporphyrin IX excitation in fluorescence-guided stereotactic biopsy of brain tumors. J. Biophotonics 2016, 9, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Akimoto, J., Fukami, S., Ichikawa, M., Mohamed, A. & Kohno, M. Intraoperative Photodiagnosis for Malignant Glioma Using Photosensitizer Talaporfin Sodium. Front Surg. 2019, 6, 12.
- Tsutsumi, M. et al. Photodynamic therapy with talaporfin sodium induces dose-dependent apoptotic cell death in human glioma cell lines. Photodiagnosis Photodyn. Ther. 2013, 10, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Miki, Y. et al. Photodynamic therapy in combination with talaporfin sodium induces mitochondrial apoptotic cell death accompanied with necrosis in glioma cells. Biol. Pharm. Bull. 2013, 36, 215–221. [Google Scholar] [CrossRef]
- Jia, Y. et al. Photodynamic therapy combined with temozolomide inhibits C6 glioma migration and invasion and promotes mitochondrial-associated apoptosis by inhibiting sodium-hydrogen exchanger isoform 1. Photodiagnosis Photodyn. Ther. 2019, 26, 405–412. [Google Scholar] [CrossRef]
- Miki, Y. et al. Concomitant treatment with temozolomide enhances apoptotic cell death in glioma cells induced by photodynamic therapy with talaporfin sodium. Photodiagnosis Photodyn. Ther. 2014, 11, 556–564. [Google Scholar] [CrossRef]
- Cong, D. et al. Upregulation of NHE1 protein expression enables glioblastoma cells to escape TMZ-mediated toxicity via increased H+ extrusion, cell migration and survival. Carcinogenesis 2014, 35, 2014–2024. [Google Scholar] [CrossRef]
- Zhang, X., Guo, M., Shen, L. & Hu, S. Combination of photodynamic therapy and temozolomide on glioma in a rat C6 glioma model. Photodiagnosis and Photodynamic Therapy 2014, vol. 11 603–612 . [CrossRef]
- Tzerkovsky, D. A., Osharin, V. V., Istomin, Y. P., Alexandrova, E. N. & Vozmitel, M. A. Fluorescent diagnosis and photodynamic therapy for C6 glioma in combination with antiangiogenic therapy in subcutaneous and intracranial tumor models. Exp. Oncol. 2014, 36, 85–89.
- Josefsen, L. B. & Boyle, R. W. Photodynamic therapy: novel third-generation photosensitizers one step closer? British journal of pharmacology vol. 154 1–3 (2008).
- Luiza Andreazza, N. et al. Berberine as a photosensitizing agent for antitumoral photodynamic therapy: Insights into its association to low density lipoproteins. Int. J. Pharm. 2016, 510, 240–249. [Google Scholar] [CrossRef]
- Zhu, X. et al. Transferrin/aptamer conjugated mesoporous ruthenium nanosystem for redox-controlled and targeted chemo-photodynamic therapy of glioma. Acta Biomater. 2018, 82, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Sudheesh, K. V. et al. A Cyclometalated Ir Complex as a Lysosome-Targeted Photodynamic Therapeutic Agent for Integrated Imaging and Therapy in Cancer Cells. Chemistry 2018, 24, 10999–11007. [Google Scholar] [CrossRef] [PubMed]
- Ibarra, L. E. et al. Metallated porphyrin-doped conjugated polymer nanoparticles for efficient photodynamic therapy of brain and colorectal tumor cells. Nanomedicine 2018, 13, 605–624. [Google Scholar] [CrossRef] [PubMed]
- Boreham, E. M. et al. A cyclometallated fluorenyl Ir(iii) complex as a potential sensitiser for two-photon excited photodynamic therapy (2PE-PDT). Dalton Trans. 2015, 44, 16127–16135. [Google Scholar] [CrossRef]
- Tang, X.-L. et al. pH-Responsive Magnetic Mesoporous Silica-Based Nanoplatform for Synergistic Photodynamic Therapy/Chemotherapy. ACS Appl. Mater. Interfaces 2018, 10, 15001–15011. [Google Scholar] [CrossRef] [PubMed]
- Jamali, Z. et al. Evaluation of targeted curcumin (CUR) loaded PLGA nanoparticles for in vitro photodynamic therapy on human glioblastoma cell line. Photodiagnosis Photodyn. Ther. 2018, 23, 190–201. [Google Scholar] [CrossRef]
- Xu, J. et al. High Affinity of Chlorin e6 to Immunoglobulin G for Intraoperative Fluorescence Image-Guided Cancer Photodynamic and Checkpoint Blockade Therapy. ACS Nano 2019, 13, 10242–10260. [Google Scholar] [CrossRef]
- Wang, Q. et al. Fluorinated polymeric micelles to overcome hypoxia and enhance photodynamic cancer therapy. Biomater Sci 2018, 6, 3096–3107. [Google Scholar] [CrossRef]
- Lu, L. et al. An iRGD-conjugated prodrug micelle with blood-brain-barrier penetrability for anti-glioma therapy. Biomaterials 2020, 230, 119666. [Google Scholar] [CrossRef]
- de Paula, L. B., Primo, F. L. & Tedesco, A. C. Nanomedicine associated with photodynamic therapy for glioblastoma treatment. Biophys. Rev. 2017, 9, 761–773.
- Pellosi, D. S., Paula, L. B., de Melo, M. T. & Tedesco, A. C. Targeted and Synergic Glioblastoma Treatment: Multifunctional Nanoparticles Delivering Verteporfin as Adjuvant Therapy for Temozolomide Chemotherapy. Mol. Pharm. 2019, 16, 1009–1024.
- Yan, L. et al. Dextran-Benzoporphyrin Derivative (BPD) Coated Superparamagnetic Iron Oxide Nanoparticle (SPION) Micelles for T2-Weighted Magnetic Resonance Imaging and Photodynamic Therapy. Bioconjug. Chem. 2019, 30, 2974–2981. [Google Scholar] [CrossRef] [PubMed]
- Bœuf-Muraille, G. et al. Evaluation of mTHPC-loaded PLGA nanoparticles for in vitro photodynamic therapy on C6 glioma cell line. Photodiagnosis Photodyn. Ther. 2019, 25, 448–455. [Google Scholar] [CrossRef]
- Castilho-Fernandes, A., Lopes, T. G., Primo, F. L., Pinto, M. R. & Tedesco, A. C. Photodynamic process induced by chloro-aluminum phthalocyanine nanoemulsion in glioblastoma. Photodiagnosis Photodyn. Ther. 2017, 19, 221–228.
- Davanzo, N. N., Pellosi, D. S., Franchi, L. P. & Tedesco, A. C. Light source is critical to induce glioblastoma cell death by photodynamic therapy using chloro-aluminiumphtalocyanine albumin-based nanoparticles. Photodiagnosis Photodyn. Ther. 2017, 19, 181–183.
- Lv, Z. et al. A multiphoton transition activated iron based metal organic framework for synergistic therapy of photodynamic therapy/chemodynamic therapy/chemotherapy for orthotopic gliomas. J. Mater. Chem. B Mater. Biol. Med. 2023. [Google Scholar] [CrossRef]
- Tsai, Y.-C. et al. Targeted Delivery of Functionalized Upconversion Nanoparticles for Externally Triggered Photothermal/Photodynamic Therapies of Brain Glioblastoma. Theranostics 2018, 8, 1435–1448. [Google Scholar] [CrossRef] [PubMed]
- Chen, G., Qiu, H., Prasad, P. N. & Chen, X. Upconversion nanoparticles: design, nanochemistry, and applications in theranostics. Chem. Rev. 2014, 114, 5161–5214.
- Tang, X.-L. et al. Near-infrared light-activated red-emitting upconverting nanoplatform for T-weighted magnetic resonance imaging and photodynamic therapy. Acta Biomater. 2018, 74, 360–373. [Google Scholar] [CrossRef]
- Wang, L.-X. et al. Antitumor activity of photodynamic therapy with a chlorin derivative in vitro and in vivo. Tumour Biol. 2015, 36, 6839–6847. [Google Scholar] [CrossRef]
- Hiramatsu, R. et al. Tetrakis(p-carboranylthio-tetrafluorophenyl)chlorin (TPFC): application for photodynamic therapy and boron neutron capture therapy. J. Pharm. Sci. 2015, 104, 962–970. [Google Scholar] [CrossRef]
- Song, R., Hu, D., Chung, H. Y., Sheng, Z. & Yao, S. Lipid-Polymer Bilaminar Oxygen Nanobubbles for Enhanced Photodynamic Therapy of Cancer. ACS Appl. Mater. Interfaces. 2018, 10, 36805–36813.
- Wang, X. et al. Enhancing selective photosensitizer accumulation and oxygen supply for high-efficacy photodynamic therapy toward glioma by 5-aminolevulinic acid loaded nanoplatform. J. Colloid Interface Sci. 2020, 565, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Huang, X. et al. Combined Cancer Chemo-Photodynamic and Photothermal Therapy Based on ICG/PDA/TPZ-Loaded Nanoparticles. Mol. Pharm. 2019, 16, 2172–2183. [Google Scholar] [CrossRef] [PubMed]
- Dupont, C., Mordon, S., Deleporte, P., Reyns, N. & Vermandel, M. A novel device for intraoperative photodynamic therapy dedicated to glioblastoma treatment. Future Oncol. 2017, 13, 2441–2454.
- Madsen, S. J., Sun, C. H., Tromberg, B. J. & Hirschberg, H. Development of a novel indwelling balloon applicator for optimizing light delivery in photodynamic therapy. Lasers Surg. Med. 2001, 29, 406–412.
- Jamali, Z., Hejazi, S. M., Ebrahimi, S. M., Moradi-Sardareh, H. & Paknejad, M. Effects of LED-Based photodynamic therapy using red and blue lights, with natural hydrophobic photosensitizers on human glioma cell line. Photodiagnosis Photodyn. Ther. 2018, 21, 50–54.
- Whelan, H. T. High-grade glioma/glioblastoma multiforme: is there a role for photodynamic therapy? J. Natl. Compr. Canc. Netw. 10 Suppl 2, S31–4 (2012).
- Curnow, A. & Bown, S. G. The role of reperfusion injury in photodynamic therapy with 5-aminolaevulinic acid – a study on normal rat colon. British Journal of Cancer vol. 86 989–992. 2002. [CrossRef]
- Tetard, M.-C. et al. Interstitial 5-ALA photodynamic therapy and glioblastoma: Preclinical model development and preliminary results. Photodiagnosis Photodyn. Ther. 2016, 13, 218–224. [Google Scholar] [CrossRef]
- Vermandel, M. et al. Comparison of different treatment schemes in 5-ALA interstitial photodynamic therapy for high-grade glioma in a preclinical model: An MRI study. Photodiagnosis Photodyn. Ther. 2019, 25, 166–176. [Google Scholar] [CrossRef]
- Leroy, H.-A. et al. MRI assessment of treatment delivery for interstitial photodynamic therapy of high-grade glioma in a preclinical model. Lasers Surg. Med. 2018, 50, 460–468. [Google Scholar] [CrossRef]
- Leroy, H.-A. et al. Interstitial photodynamic therapy and glioblastoma: Light fractionation in a preclinical model. Lasers Surg. Med. 2017, 49, 506–515. [Google Scholar] [CrossRef]
- Hirschberg, H. et al. Repetitive photodynamic therapy of malignant brain tumors. J. Environ. Pathol. Toxicol. Oncol. 2006, 25, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Davies, N. & Wilson, B. C. Interstitial in vivo ALA-PpIX mediated metronomic photodynamic therapy (mPDT) using the CNS-1 astrocytoma with bioluminescence monitoring. Photodiagnosis Photodyn. Ther. 2007, 4, 202–212.
- Guo, H.-W. et al. Low-fluence rate, long duration photodynamic therapy in glioma mouse model using organic light emitting diode (OLED). Photodiagnosis Photodyn. Ther. 2015, 12, 504–510. [Google Scholar] [CrossRef]
- van Zaane, F. et al. A telemetric light delivery system for metronomic photodynamic therapy (mPDT) in rats. J. Biophotonics 2010, 3, 347–355. [Google Scholar] [CrossRef] [PubMed]
- Plattner, M. , Bernwick, W. & Kostron, H. Hematoporphyrin-derivative photodynamic in-vitro sensitivity testing for brain tumors. in International Conference on Photodynamic Therapy and Laser Medicine vol. 1616 182–185 (SPIE, 1993).
- Chen, Z.-Q. , Wu, S.-E. & Zhu, S.-G. Adjuvant photodynamic therapy in surgical management of cerebral tumors. in International Conference on Photodynamic Therapy and Laser Medicine vol. 1616 94–97 (SPIE, 1993).
- Marks, P. V. , Furneaux, C. & Shivvakumar, R. An in vitro study of the effect of photodynamic therapy on human meningiomas. Br. J. Neurosurg. 1992, 6, 327–332. [Google Scholar]
- Neurosurgery. https://academic.oup.com/neurosurgery/article-abstract/32/3/357/2755000.
- Malham, G. M., Thomsen, R. J., Finlay, G. J. & Baguley, B. C. Subcellular distribution and photocytotoxicity of aluminium phthalocyanines and haematoporphyrin derivative in cultured human meningioma cells. Br. J. Neurosurg. 1996, 10, 51–57.
- Tsai, J. C., Hsiao, Y. Y., Teng, L. J., Chen, C. T. & Kao, M. C. Comparative study on the ALA photodynamic effects of human glioma and meningioma cells. Lasers Surg. Med. 1999, 24, 296–305.
- Sam Eljamel, M. Which intracranial lesions would be suitable for fluoresce guided resection?: A prospective review of 110 consecutive lesions. in Photodynamic Therapy: Back to the Future vol. 7380 112–125 (SPIE, 2009).
- El-Khatib, M. et al. Aminolevulinic acid-mediated photodynamic therapy of human meningioma: an in vitro study on primary cell lines. Int. J. Mol. Sci. 2015, 16, 9936–9948. [Google Scholar] [CrossRef]
- Hefti, M., Holenstein, F., Albert, I., Looser, H. & Luginbuehl, V. Susceptibility to 5-Aminolevulinic Acid Based Photodynamic Therapy in WHO I Meningioma Cells Corresponds to Ferrochelatase Activity. Photochemistry and Photobiology vol. 87 235–241. 2011. [CrossRef]
- Sun, W. et al. Gefitinib enhances the efficacy of photodynamic therapy using 5-aminolevulinic acid in malignant brain tumor cells. Photodiagnosis Photodyn. Ther. 2013, 10, 42–50. [Google Scholar] [CrossRef]
- Cornelius, J. F. et al. Enhancing the effect of 5-aminolevulinic acid based photodynamic therapy in human meningioma cells. Photodiagnosis Photodyn. Ther. 2014, 11, 1–6. [Google Scholar] [CrossRef]
- Ichikawa, M. et al. Photodynamic therapy with talaporfin sodium induces dose- and time-dependent apoptotic cell death in malignant meningioma HKBMM cells. Photodiagnosis Photodyn. Ther. 2019, 25, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T. et al. Photodynamic therapy using talaporfin sodium induces heme oxygenase-1 expression in rat malignant meningioma KMY-J cells. J. Toxicol. Sci. 2018, 43, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, T. et al. Possible mechanism of heme oxygenase-1 expression in rat malignant meningioma KMY-J cells subjected to talaporfin sodium-mediated photodynamic therapy. Photodiagnosis Photodyn. Ther. 2020, 32, 102009. [Google Scholar] [CrossRef] [PubMed]
- Kirollos, R. W., Marks, P. V., Igbaseimokumo, U. & Chakrabarty, A. A preliminary experimental in vivo study of the effect of photodynamic therapy on human pituitary adenoma implanted in mice. Br. J. Neurosurg. 1998, 12, 140–145.
- Marks, P. V., Buxton, T. & Furneaux, C. E. In vitro study of the effect of photodynamic therapy on pituitary adenomas. Br. J. Neurosurg. 1993, 7, 401–406.
- Igbaseimokumo, U. Quantification of in vivo Photofrin uptake by human pituitary adenoma tissue. J. Neurosurg. 2004, 101, 272–277. [Google Scholar] [CrossRef]
- Marks, P. V. et al. Effect of photodynamic therapy on recurrent pituitary adenomas: clinical phase I/II trial--an early report. Br. J. Neurosurg. 2000, 14, 317–325. [Google Scholar] [CrossRef]
- Nemes, A. et al. 5-ALA Fluorescence in Native Pituitary Adenoma Cell Lines: Resection Control and Basis for Photodynamic Therapy (PDT)? PLoS One 11, e0161364 (2016).
- Neumann, L. M. et al. Efficacy of 5-aminolevulinic acid based photodynamic therapy in pituitary adenomas-experimental study on rat and human cell cultures. Photodiagnosis Photodyn. Ther. 2016, 14, 77–83. [Google Scholar] [CrossRef]
- Cornelius, J. F. et al. 5-Aminolevulinic acid-based photodynamic therapy of chordoma: In vitro experiments on a human tumor cell line. Photodiagnosis Photodyn. Ther. 2017, 20, 111–115. [Google Scholar] [CrossRef]
- Gull, H. H. et al. Ciprofloxacin enhances phototoxicity of 5-aminolevulinic acid mediated photodynamic treatment for chordoma cell lines. Photodiagnosis Photodyn. Ther. 2021, 35, 102346. [Google Scholar] [CrossRef]
- Briel-Pump, A. et al. Accumulation of protoporphyrin IX in medulloblastoma cell lines and sensitivity to subsequent photodynamic treatment. J. Photochem. Photobiol. B 2018, 189, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Schwake, M. et al. In-Vitro Use of 5-ALA for Photodynamic Therapy in Pediatric Brain Tumors. Neurosurgery 2018, 83, 1328–1337. [Google Scholar] [CrossRef] [PubMed]
- Kast, R.E.; Michael, A.P.; Sardi, I.; Burns, T.C.; Heiland, T.; Karpel-Massler, G.; Kamar, F.G.; Halatsch, M.-E. A New Treatment Opportunity for DIPG and Diffuse Midline Gliomas: 5-ALA Augmented Irradiation, the 5aai Regimen. Brain Sci. 2020, 10, 51. [CrossRef]
- Chiba, K. et al. Photodynamic therapy for malignant brain tumors in children and young adolescents. Front. Oncol. 2022, 12, 957267. [Google Scholar] [CrossRef] [PubMed]
- Stepp, H. & Stummer, W. 5-ALA in the management of malignant glioma. Lasers Surg. Med. 2018, 50, 399–419.
- Kawai, N. et al. ABCG2 expression is related to low 5-ALA photodynamic diagnosis (PDD) efficacy and cancer stem cell phenotype, and suppression of ABCG2 improves the efficacy of PDD. PLoS One 14, e0216503 (2019).
- Blake, E. & Curnow, A. The hydroxypyridinone iron chelator CP94 can enhance PpIX-induced PDT of cultured human glioma cells. Photochem. Photobiol. 2010, 86, 1154–1160.
- Chen, X. et al. Calcitriol enhances 5-aminolevulinic acid-induced fluorescence and the effect of photodynamic therapy in human glioma. Acta Oncol. 2014, 53, 405–413. [Google Scholar] [CrossRef]
- Wang, C. et al. Low-dose arsenic trioxide enhances 5-aminolevulinic acid-induced PpIX accumulation and efficacy of photodynamic therapy in human glioma. J. Photochem. Photobiol. B 2013, 127, 61–67. [Google Scholar] [CrossRef]
- Coupienne, I. et al. NF-kappaB inhibition improves the sensitivity of human glioblastoma cells to 5-aminolevulinic acid-based photodynamic therapy. Biochem. Pharmacol. 2011, 81, 606–616. [Google Scholar] [CrossRef]
- Albert, I., Hefti, M. & Luginbuehl, V. Physiological oxygen concentration alters glioma cell malignancy and responsiveness to photodynamic therapy in vitro. Neurol. Res. 2014, 36, 1001–1010.
- Dereski, M. O., Madigan, L. & Chopp, M. The Effect of Hypothermia and Hyperthermia on Photodynamic Therapy of Normal Brain. Neurosurgery 1995, vol. 36 141-146 . [CrossRef]
- Fisher, C. J. et al. ALA-PpIX mediated photodynamic therapy of malignant gliomas augmented by hypothermia. PLoS One 12, e0181654 (2017).
- Christie, C. Synergistic chemotherapy by combined moderate hyperthermia and photochemical internalization. Biomed. Opt. Express 2016, 7, 1240–1250. [Google Scholar] [CrossRef]
- Fisher, C. J. et al. Modulation of PPIX synthesis and accumulation in various normal and glioma cell lines by modification of the cellular signaling and temperature. Lasers Surg. Med. 2013, 45, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Ghogare, A. A., Rizvi, I., Hasan, T. & Greer, A. ‘Pointsource’ delivery of a photosensitizer drug and singlet oxygen: eradication of glioma cells in vitro. Photochem. Photobiol. 2014, 90, 1119–1125.
- Girotti, A. W. et al. Upregulation of nitric oxide in tumor cells as a negative adaptation to photodynamic therapy. Lasers Surg. Med. 2018, 50, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Fahey, J. M., Emmer, J. V., Korytowski, W., Hogg, N. & Girotti, A. W. Antagonistic Effects of Endogenous Nitric Oxide in a Glioblastoma Photodynamic Therapy Model. Photochem. Photobiol. 2016, 92, 842–853.
- Fahey, J. M., Stancill, J. S., Smith, B. C. & Girotti, A. W. Nitric oxide antagonism to glioblastoma photodynamic therapy and mitigation thereof by BET bromodomain inhibitor JQ1. J. Biol. Chem. 2018, 293, 5345–5359.
- Lee, S. Y. et al. TP53 regulates human AlkB homologue 2 expression in glioma resistance to Photofrin-mediated photodynamic therapy. Br. J. Cancer 2010, 103, 362–369. [Google Scholar] [CrossRef]
- Li, B. O. et al. Effect of photodynamic therapy combined with torasemide on the expression of matrix metalloproteinase 2 and sodium-potassium-chloride cotransporter 1 in rat peritumoral edema and glioma. Oncol. Lett. 2016, 11, 2084–2090. [Google Scholar] [CrossRef]
- Zhang, X. et al. The effect of bumetanide on photodynamic therapy-induced peri-tumor edema of C6 glioma xenografts. Lasers Surg. Med. 2014, 46, 422–430. [Google Scholar] [CrossRef]
- Gupta, S., Dwarakanath, B. S., Muralidhar, K., Koru-Sengul, T. & Jain, V. Non-monotonic changes in clonogenic cell survival induced by disulphonated aluminum phthalocyanine photodynamic treatment in a human glioma cell line. J. Transl. Med. 2010, 8, 43.
- Hefti, M., Albert, I. & Luginbuehl, V. Phenytoin reduces 5-aminolevulinic acid-induced protoporphyrin IX accumulation in malignant glioma cells. J. Neurooncol. 2012, 108, 443–450.
- Misuth, M., Horvath, D., Miskovsky, P. & Huntosova, V. Synergism between PKCδ regulators hypericin and rottlerin enhances apoptosis in U87 MG glioma cells after light stimulation. Photodiagnosis Photodyn. Ther. 2017, 18, 267–274.
- Zheng, X. et al. Atorvastatin reduces functional deficits caused by photodynamic therapy in rats. Int. J. Oncol. 2011, 39, 1133–1141. [Google Scholar] [PubMed]
- Pridham, K. J. et al. Connexin 43 confers chemoresistance through activating PI3K. Oncogenesis 2022, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.-P. et al. A novel role of Cx43-composed GJIC in PDT phototoxicity: an implication of Cx43 for the enhancement of PDT efficacy. Int. J. Biol. Sci. 2019, 15, 598–609. [Google Scholar] [CrossRef]
Figure 1.
Photodynamic therapy mechanism of action. PDT occurs by light excitation of the tumor-accumulated photosensitizer, which exists at “ground state” (0PS). Following excitation, 0PS transitions to the singlet, excited state (1PS*). As the energy is released, 1PS* either drops to the ground state, emitting fluorescence, or drops to the excited triplet state (3PS*) through intersystem crossing. Electrons are subsequently released as the triplet state returns to 0PS by way of phosphorescence. PDT is executed via two types of photosensitization: Type I, which converts O2 to reactive oxygen species such as H2O2, O2-, or OH-; and Type II, which converts 3O2 to 1O2. Downstream biological effects on tumor cells include direct tumor cell destruction (apoptosis, necrosis, autophagy), tumor vasculature damage (microvascular stasis, increased vascular gaps, vessel pruning), and immune cell recruitment via localized inflammation.
Figure 1.
Photodynamic therapy mechanism of action. PDT occurs by light excitation of the tumor-accumulated photosensitizer, which exists at “ground state” (0PS). Following excitation, 0PS transitions to the singlet, excited state (1PS*). As the energy is released, 1PS* either drops to the ground state, emitting fluorescence, or drops to the excited triplet state (3PS*) through intersystem crossing. Electrons are subsequently released as the triplet state returns to 0PS by way of phosphorescence. PDT is executed via two types of photosensitization: Type I, which converts O2 to reactive oxygen species such as H2O2, O2-, or OH-; and Type II, which converts 3O2 to 1O2. Downstream biological effects on tumor cells include direct tumor cell destruction (apoptosis, necrosis, autophagy), tumor vasculature damage (microvascular stasis, increased vascular gaps, vessel pruning), and immune cell recruitment via localized inflammation.
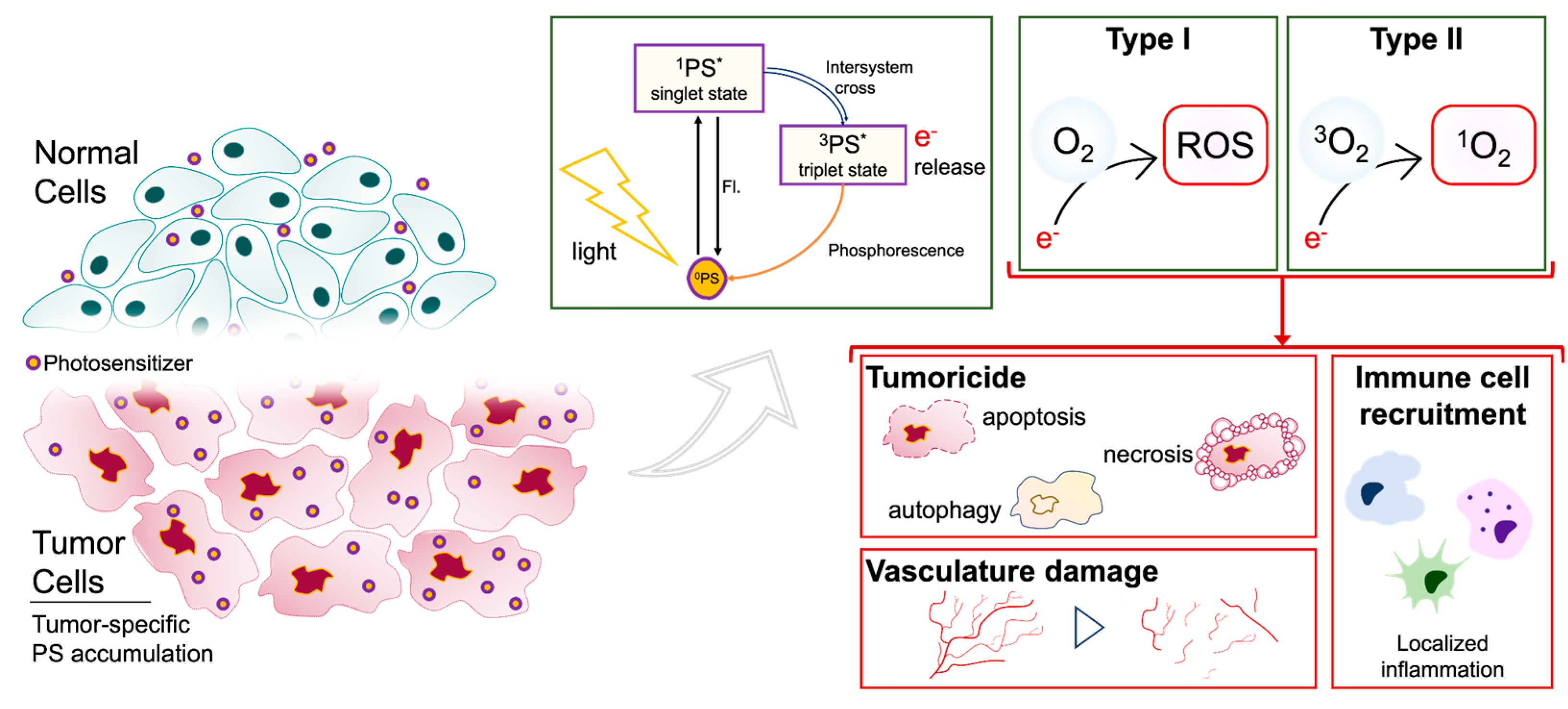

Table 1.
Clinical properties of select, relevant first- and second- generation photosensitizers.
| Photosensitizer | Intracellular Localization | Excitation Wavelength (nm) | Treatment Windowa | Clearance Time | Tumor : Normal Fluorescence Ratiob | Administration | Side effects | |
|---|---|---|---|---|---|---|---|---|
| First Generation | Porfimer Sodium | Inner mitochondrial membrane | 630 | 48 – 150 h | 4 – 8 weeks | 2.5 – 4 : 1 | Systemic | Skin sensitization, thrombocytopenia |
| Hematoporphyrin derivative [HpD] | 408, 510, 630c | 24 – 48 h | 4 – 6 weeks | Systemic | ||||
| Dihematoporphyrin ether [DHE] | 395, 630c | 24 – 72 h | 4 – 6 weeks | Systemic | ||||
| Second Generation | 5-Aminolevulinic Acid (Levulin®, Gliolan®) | Early: mitochondria Late: plasma membrane, lysosomes | 410, 510, 635c | 4 – 8 h | 2 days | 10 – 20 : 1 | Oral | Skin sensitization, nausea, elevated liver enzymes, anemia |
| Talaporfin sodium (Laserphyrin, AptocineTM, LS11, PhotoIon®) | Lysosomes | 664 | 12 – 26 h | 15 days | ND | Systemic | Skin sensitization | |
| Temoporfin [m-THPC; m-tetrahydroxyphenylchlorin] (Foscan®, liquid formulation; Foslip®, liposomal formulation) | Strong: golgi apparatus, Endoplasmic reticulum Weak: mitochondria, lysosomes | 652 | 48 – 110 h | 15 days | 150 : 14 | Systemic | Skin sensitization | |
| Boronated protoporphyrin [BOPP] | Lysosomes | 630 | 24 h | 4 – 6 weeks | 400 : 1 | Systemic | Skin sensitization, thrombocytopenia | |
| Benzoporphyrin derivative [BPD] | Lysosomes | 680-690 | 15 – 30 min. | 1 – 5 days | ND | Systemic | Vascular damage |
aTime frame between drug and light administration; bTumor tissue : normal tissue fluorescence ratio (T:N); cOptimal excitation wavelength; ND, not determined.
Table 2.
Summary of clinical studies using first-generation photosensitizers (PS) for glioma PDT.
| Study Groupa (n, number of GBM patients in study) |
Mean Age | PSb | Dosec | Routed | Time prior to Photoillumin-ation | Photoillumi-nation Methode | Laser / Light Wavelengthf (nm) |
Photoillumination Energy (ED unless otherwise specified) |
Reported survivalg | Survival Statistics | Adverse Events | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Perria et al. (1980) | GBM | 2 | n/a | HpD | 5 mg/kg | IV | n/a | n/a | 628 | 720 – 2400 J/cm2 | MS | 6.9 mo | n/a | |
| Laws et al. (1981) | rMG | 5 | 14-75 | HpD | 5 mg/kg | IV | 48 – 72 h | Interstitial | 630 | 30 – 60 mW/cm2 § | TTP | 1-6 mo | Increased skin photosenstivity | |
| McCulloch et al. (1984) | GBM | 9 | n/a | HpD | 5 mg/kg | IV | n/a | n/a | 627.8 (>1 laser) | n/a | OS | GBM (n=3) | 17-42 mo | Increase in P/O cerebral edema |
| Muller & Wilson (1985)h | GBM rGBM |
1 2 |
53 32,44 |
HpD | 2.5 mg/kg 2 mg/kg |
IV | 24 h | Cavitary (balloon) | 630 | 8 – 68 J/cm2 | n/a | None | ||
| Kaye et al. (1987)i | GBM rGBM |
13 6 |
45*** 40*** |
HpD | 5 mg/kg | IV | 24 h | Interstitial | AI (9) GMVL (14) |
70 – 120 J/cm2 120 – 230 J/cm2 |
PFS | GBM rGBM |
3-13 mo 12-16 wk |
No AEs |
| Kostron et al. (1987)j | GBM rGBM (1x) rGBM (mult) |
6 5 3 |
63.3 50.8 57.0 |
HpD | 1.0 mg/cm3 | IV IA Direct tumor |
3 d | LED (n = 9) Cavitary (n = 5) |
620-640 632 |
422 J/cm2 § < 1600 J/cm2 § |
MS/OS | GBM rGBM (1x) rGBM (mult) |
12 mo 2-7 mo 5 mo |
IA/Direct tolerated without skin phototoxicity |
| Muller & Wilson (1987)h |
[HpD] GBM rGBM [DHE] GBM rGBM |
1 1 7 7 |
52 32 58.3 39.4 |
HpD (8) DHE (24) Total dose |
2.14 mg/kg 2.08 mg/kg 150 mg |
IV | 18 – 24 h | Cavitary | 630 | HpD: 32 J/cm2 DHE: 23 J/cm2 |
MS | [HpD] GBM rGBM [DHE] GBM rGBM |
2.9 mo 5.8 mo 1.1-13.6 mo 0.2-10.7 mo |
Skin photosensitivity (n = 3) |
| Kostron et al. (1988)j | GBM rGBM (1x) rGBM (mult) |
8 9 3 |
55** | HpD | 1 mg/cm3 | IV, IA and/or Direct | 3 d | LED Cavitary |
590-750 632 |
422 J/cm2 § 60 – 200 J/cm2 |
OS | GBM rGBM (1x) rGBM (mult) |
0.5-19 m 3-14 mo 1-6 mo |
Skin phototoxicity (IA/IV only) |
| HPD only (n=9), [HPD + single dose radiation of 4 Gy fast electrons] (n=10), [HPD + single dose radiation + conventional radiotherapy] (n=4); 3 cases of recurrence and subsequent re-treatment. | ||||||||||||||
| Kostron et al. (1990)j | GBM rGBM |
9 18 |
n/a | HpD | n/a | IV, IA and/or Direct | n/a | Interstitial | 630 | 40 – 220 J/cm2 | OS | GBM rGBM |
0.5-29 mo 4-13 mo |
Increased phototoxicity of the skin |
| Muller & Wilson (1990)h | GBM rGBM |
9 14 |
48 | HpD DHE |
5 mg/kg 2 mg/kg |
IV | 18 – 24 h | Cavitary | 630 | 24 J/cm2 | MS | GBM + rGBM | 6.3 mo | Increased skin photosensitivity |
| Powers et al. (1991) | rGBM rMG |
1 5 |
42-61 | HPE | 2.0 mg/kg | IV | 24 h | Interstitial | 630 | 1000 J§§ | TTP | rGBM rMG |
2-27 wk 6-45 wk |
Edema, increased intracranial pressure and skin photosensitivity |
| Origitano et al. (1993) |
rGBM | 8 | 42.2 | PNa | 2.0 mg/kg | IV | 48 – 72 h | Cavitary Interstitial + post-resection cavitary |
630 630 |
50 J/cm2 100 J/cm per fiber |
TTP | 5-22 mo | Increased skin photosensitivity | |
| Muller & Wilson (1995)h | rGBM | 32 | 41** | HpD PNa HPE |
5 mg/kg 2 mg/kg 2 mg/kg |
IV IV IV |
12 – 36 h | Cavitary | 630 | 38 J/cm2 | MS | [Stratify by light dose] Energy: > 1700 J < 1700 J |
28 wk 29 wk |
Edema, increased skin photosensitivity |
| Popovic et al. (1995)i | GBM rGBM |
38 40 |
n/a | HpD | 2.0-2.5 mg/kg | IV | 24 h | Cavitary | AI (1986-1987) GMVL (1987-1994) |
240 – 260 J/cm2 (initial pts: 70) |
MS | GBM rGBM |
24 mo 9 mo |
n/a |
| Muller & Wilson (1997)h | GBM rGBM |
11 32 |
40 58 |
PNa | 2 mg/kg | IV | 12 – 36 h | Cavitary | 630 | GBM: 30 J/cm2 * rGBM: 43 J/cm2 * |
MS | GBM rGBM |
37 wk 30 wk |
Increased P/O cerebral edema |
| Muller et al. (2001) [Phase II]h | rGBM (ED ≤ 50) (ED ≥ 50) |
37 (22) (15) |
41** | PNa | 2 mg/kg | IV | 12 – 36 h | Cavitary | 630 | 8 – 110 J/cm2 | MS | rGBM (ED ≤ 50) (ED ≥ 50) |
avg 29 wk (29 wk) (34 wk) |
Increased P/O cerebral edema |
| Muller et al. (2001) [Phase III]h |
GBM High light rGBM Low light High light |
20 26 26 |
54 48 52 |
PNa | 2 mg/kg | IV | 12 – 36 h | Cavitary | 630 | 30 – 50 J/cm2 (low) 110 – 130 J/cm2 (high) |
MS |
GBM High rGBM Low High |
92 wk 29 wk 51 wk |
n/a |
| Schmidt et al. (2004) | Recurrent brain tumors (including GBM) |
NS | n/a | PNa | 0.75 mg/kg 1.20 mg/kg 1.60 mg/kg 2.00 mg/kg |
IV | 18 – 24 h | Laser/LED + Cavitary balloon | Laser: 630 LED: 20 – 25 |
100 J/cm2 | Not specified | No neurotoxicity | ||
| Stylli et al. (2004)i | GBM rGBM |
31 27 |
44*** | HpD | 5 mg/kg | IV | 24 h | Cavitary | AI (1986-1987) GMVL (1987-1994) KTP (1994-2000) |
240 J/cm2 §§ | MS | GBM/rGBM | 24 mo | n/a |
| Stylli et al. (2005)i | GBM rGBM |
31 55 |
47* 42* |
HpD | 5 mg/kg | IV | 24 h | Cavitary | AI (1986-1987) GMVL (1987-1994) KTP (1994-2000) |
240 J/cm2 §§ | MS | GBM rGBM |
14.3 mo 13.5 mo |
Increased cerebral edema (n = 3) |
| Muller et al. (2006)h | GBM rGBM |
12 37 |
59 41 |
PNa | 2 mg/kg | IV | 12 – 36 h | Cavitary (balloon or continuous filling with Intralipid) +/- interstitial |
AI KTP |
58 J/cm2 §§§ | MS | GBM rGBM |
33 wk 29 wk |
Skin photosensitivity |
| Kaneko (2008) | GBM | 26 | HPE | 3 mg/kg | IV | 2 d | Interstitial | 640 | 180 J/cm | n/a | n/a | |||
aStudy group: GBM, newly diagnosed GBM; rGBM, recurrent GBM; rGBM (1x), first recurrence of GBM; rGBM (mult), multiple recurrences of GBM; MG, malignant glioma; rMG, recurrent malignant glioma; ED, energy density. bPhotosensitizer: HpD, Hematoporphyrin derivative; DHE, dihematoporphyrin ether; PNa, porfimer sodium; HPE, Hematoporphyrin ether; NS, not specified. cDosage units: mg/kg of body weight, mg/cm3 of tumor. dPS administration route: IV, intravenous administration; IA, intra-arterial administration; Direct, direct tumor injection. ePhoto-illumination Method: I/O, intra-operative; P/O, post-operative. fLaser / Light wavelength: AI, Argon Ion Dye pumped laser (630 nm); GMVL, Gold Metal Vapour laser (627.8 nm); KTP, Potassium titanyl phosphate pumped dye laser (532 nm transduced to 628 nm via dye module). gReported survival: MS, median overall survival; OS, overall survival; TTP, time to progression; mo, months; wk, weeks. hLongitudinal reporting of St. Michael’s Hospital patient series. iLongitudinal reporting of the Royal Melbourne Hospital patient series. jLongitudinal reporting of the University of Innsbruck patient series. n/a: not available, AEs: adverse events. §Power density. §§Median total dose. §§§Mean total dose. *median. **mean age of entire study. ***median age of entire study.
Table 3.
Summary of clinical studies using second-generation photosensitizers (PS) for glioma PDT.
| Study Groupa (n, number of patients with disease & treatment) |
Mean Age | PSb | Dosec | Routed | Time prior to Photoillumination | Photoillumination Methode | Laser / Light Wavelengthf (nm) |
Photoillumination Energyg (ED unless otherwise specified) |
Reported survivalh | Survival Statistics | Adverse Events | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kostron et al. (1998) | GBM rGBM |
2 8 |
61-72 34-72 |
mTHPCx | 0.15 mg/kg | IV | 4 d | Interstitial I/O cavitary |
KTP 652 |
300 mW/cm2 § 20 J/cm2 |
TTP MS |
rGBM rGBM |
4 mo 6 mo |
Phototoxicity |
| Rosenthall et al. (2001/2003)i | GBM rGBM |
7 9 |
51* | BOPP | 0.25-8.0 mg/kg | IV | 24 h | I/O fiber diffuser for focused surface irradiation | 630 | 25 J/cm2 | MS | GBM rGBM |
5 mo 11 mo |
n/a |
| Schmidt et al. (2004) | Recurrent brain tumors (including GBM) |
NS | n/a | BPD | 0.25 mg/kg | IV | 3–6 h | Laser fiber optic catheter/balloon LED balloon |
680 | 1,800 J§§ (at 100 J/cm2) |
Not specified | No cytotoxic effects | ||
| Kostron et al. (2006) | GBM | 26 | n/a | mTHPCx | 0.15 mg/kg | IV | 4 d | I/O cavitary I/O fiber diffuser |
KTP 652 |
300 mW/cm2 § 20 J/cm2 |
MS | GBM | 15 mo | Increased skin sensitivity |
| Beck et al. (2007) | rGBM | 10 | 51.7 | 5-ALA | 20 mg/kg | Oral | 1 h | I/O fiber diffuser for focused surface irradiation | 633 | 100 J/cm2 | MS | 15 m | n/a | |
| Elijamel et al. (2007) | GBM, PDT(+) GBM, PDT(-) |
13 14 |
59.6 60.1 |
5-ALA -- |
20 mg/kg -- |
Oral -- |
3 h -- |
P/O cavitary balloon | 630 | 100 J/cm2 | PFS MS |
GBM | 8.6 mo 52.8 wk |
Deep venous thrombosis (n=2) |
| Stepp et al. (2005) | GBM | 5 | n/a | 5-ALA | 20 mg/kg | Oral | 3 h | I/O fiber diffuser for focused surface irradiation | 633 | 100 – 200 J/cm2 | n/a | n/a | ||
| Stepp et al. (2007) | GBM (a) GBM (b) GBM (c) |
5 8 7 |
n/a | 5-ALA | 20 mg/kg | Oral | 3 h | I/O fiber diffuser for focused surface irradiation | 633 | (a) 100 J/cm2 (b) 150 J/cm2 (c) 200 J/cm2 |
n/a | No AEs | ||
| Akimoto et al. (2012) | GBM rGBM |
6 8 |
49-82 41-61 |
TS | 40 mg/m2 | IV | 24 h | I/O fiber diffuser for focused surface irradiation (1.0 cm diameter) |
664 | 27 J/cm2 | PFS | GBM | 24.8 mo | Increased photosenstivity |
| Lyons et al. (2012) | Total (GBM) PDT(+) PDT(-) [a], [b] [c], [d] |
73 30 43 17, 13 18, 25 |
59** | 5-ALA | 20 mg/kg | Oral | 3 h | [a] IORT, I/O cavitary, MSR [b] I/O cavitary, MSR [c] IORT, MSR [d] MSR only |
630 | 100 J/cm2 | PFS MS |
[a] [b] PDT+ PDT- |
79 wk 39.7 wk 62.9 wk 20.6 wk |
n/a |
| Johansson et al. (2013) | GBM rGBM |
1 4 |
42 56 |
5-ALA | 20-30 mg/kg | Oral | 5–8 h | Interstitial | 635 | 720 J/cm2 | TTP | 3-36 mo | n/a | |
| Muragaki et al. (2013) | GBM | 13 | 47.1** | TS | 40 mg/m2 | IV | 22–27 h | I/O fiber diffuser for focused surface irradiation (1.5 cm diameter) |
664 | 27 J/cm2 | PFS MS |
12 mo 27.9 mo |
Increased photosensitivity | |
| Schwartz et al. (2015) | GBM | 15 | n/a | 5-ALA | 20 mg/kg 30 mg/kg |
Oral | n/a | Interstitial | 633 | 12.96 J §§ | PFS MS |
16 m 34 m |
Transient aphasia, pulmonary embolism | |
| Vanaclocha et al. (2015) | GBM | 20 | 49*** | DHE mTHPCx |
2 mg/kg 0.15 mg/kg |
IV | 48 h 96 h |
I/O cavitary | 630 652 |
75 J/cm2 20 J/cm2 |
PFS MS MS (from 1st diagnosis) |
10 mo 9 mo 17 mo |
Skin photosensitivity Dermatitis |
|
| Nitta et al. (2018) | GBM | 11 | 54 | TS | 40 mg/m2 | IV | 22–26 h | I/O fiber diffuser for focused surface irradiation (1.5 cm diameter) | 664 | 27 J/cm2 | PFS MS |
19.6 mo 27.5 mo |
Asymptomatic transient peripheral edema | |
| Shimizu et al. (2018) | GBM rGBM |
7 7 |
45-74 40-69 |
TS | 40 mg/m2 | IV | 22– 26 h | I/O fiber diffuser for focused surface irradiation (1.5 cm diameter) | 664 | 100 J/cm2 | n/a | Pulmonary embolism (if vessels are not shielded) |
||
| Lietke et al. (2021) | rGBM | 37 | 49.4* | 5-ALA | 20 mg/kg | Oral | 3 – 5 h | Interstitial | 635 | 8,883 J §§ | TTP MS (from 1st diagnosis) |
Study combines GBM & AA | 7.1 mo 39.7 mo |
Transient worsening of pre-existing neurological deficits |
| Vermandel et al. (2021) | GBM | 10 | 57.1* | 5-ALA | 20 mg/kg | Oral | 6 h | I/O cavitary | 635 | 200 J/cm2 | PFS MS |
17.1 mo 23.1 mo |
No AEs | |
| Kobayashi et al. (2022) | GBM | 43 | 46.7** | TS | 40 mg/m2 | IV | 22 – 26 h | I/O fiber diffuser for surface irradiation (1.5 cm diameter) |
664 | 27 J/cm2 | PFS MS |
6.3 mo 15.4 mo |
No AEs | |
| Kozlikina et al. (2022) | GBM | CR | 29 | 5-ALA + Ce6 | 20 mg/kg 1 mg/kg |
Oral IV |
4 – 4.5 h 3 – 3.5 h |
I/O fiber | 660 | 60 J/cm2 §§§ | n/a | n/a | ||
aStudy group: GBM, newly diagnosed GBM; rGBM, recurrent GBM; rGBM (1x), first recurrence of GBM; rGBM (mult), multiple recurrences of GBM; NS, not specified. bPhotosensitizer: DHE, porfimer sodium; 5-ALA, 5-aminolevulinic acid; TS, Talaporfin sodium; mTHPC, Temoporfin, BOPP, boronated porphyrin; BPD, benzoporphyrin derivative; Ce6, chlorin e6. Approval: unless otherwise noted (x), approved for worldwide use, xEU approval only. cDosage units: mg/kg of body weight, μg/g of tumor, mg/cm3 of tumor, mg/m2 of body surface area. dPS administration route: IV, intravenous administration; IA, intra-arterial administration; Direct, direct tumor injection. ePhotoillumination Method: iPDT, interstitial PDT; I/O, intra-operative; P/O, post-operative; IORT, intraoperative radiotherapy; MSR, maximum safe resection. fLaser / Light wavelength: KTP, Potassium titanyl phosphate pumped dye laser. gED, energy density. hReported Survival: MS, median overall survival; PFS, progression free survival (median); TTP, time to progression (median). iSurvival data reported in 2003. n/a: not available, AEs: adverse events, CR: case report. §Power density. §§Median dose. §§§Total dose. *median. **mean age of entire study. ***median age of entire study.
Table 4.
Ongoing PDT clinical trials recruiting for malignant glioma patients.
| Study Name | Clinical Trial Phase (Study ID) |
Type of Cancer | Drug | Principal Investigator |
|---|---|---|---|---|
| Photodynamic Therapy (PDT) for malignant brain tumor in children | Phase I/II (UMIN000030883) |
Brain Tumor (Pediatric) |
Talaporfin sodium (Leserphyrin) |
Kawamata Takakazu (Tokyo Women’s Medical University Hospital) |
| Clinical Safety Study on 5-Aminolevulinic Acid (5-ALA) in Children and Adolescents With Supratentorial Brain Tumors | Phase II (NCT04738162) |
Brain Tumor (Pediatric) |
5-ALA (Gliolan) |
Walter Stummer (University Hospital, Münster) |
| Stereotactical Photodynamic Therapy With 5-aminolevulinic Acid (Gliolan®) in Recurrent Glioblastoma | Phase II (NCT04469699) |
GBM | 5-ALA (Gliolan) |
Walter Stummer (University Hospital, Münster) |
| PD L 506 for Stereotactic Interstitial Photodynamic Therapy of Newly Diagnosed Supratentorial IDH Wild-type Glioblastoma | Phase II (NCT03897491) |
GBM | 5-ALA (PD L 506) |
Niklas Thon (Klinikum der Universität München) |
| Dose Finding for Intraoperative Photodynamic Therapy of Glioblastoma | Phase II (NCT04391062) |
GBM | 5-ALA (Gliolan) |
Nicholas Reyns (University Hospital, Lille) |
| Study to Evaluate 5-ALA Combined With CV01 Delivery of Ultrasound in Recurrent High Grade Glioma | Phase I (NCT05362409) |
High Grade Glioma | 5-ALA (Gliolan) |
Alpheus Medical (Wash. Univ. St. Louis, Dent Institute, Northwell Health) |
*Note: This table includes information on clinical trials as of January 10th, 2023. Data was gathered by searching the National Institutes of Health’s (NIH) clinical trials database (https://clinicaltrials.gov/) as well as the World Health Organization’s (WHO) International Clinical Trials Registry Platform (ICTRP; https://trialsearch.who.int/). Search criteria included “photodynamic therapy” for “glioma” and/or “brain tumor” patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



