
Submitted:
13 July 2023
Posted:
14 July 2023
You are already at the latest version
Abstract
Colorectal cancer is a common disease, both in Chile and worldwide. The most widely used chemotherapy schemes are based on 5-fluorouracil (5FU) as the foundational drug. Genetic polymorphisms have emerged as potential predictive biomarkers of response to chemotherapy, but conclusive evidence is lacking. Additionally, the interplay between hereditary variations and acquired mutations in the EGFR pathway remains unknown. This study aimed to investigate the role of genetic variants associated with 5FU-based chemotherapy on therapeutic effectiveness, considering their interaction with the EGFR pathway mutations. In a retrospective cohort of 63 patients diagnosed with metastatic colorectal cancer, a multivariate analysis revealed that liver metastases, DPYD, ABCB1 and MTHFR polymorphisms are independent indicators of a poor prognostic, irrespective of EGFR pathway mutations. BRAF V600E wild-type status and high-risk drug-metabolism polymorphisms correlated with a poor prognosis in this Chilean cohort. Additionally, findings from the genomics of drug sensitivity (GDSC) project demonstrated that cell lines with wild-type BRAF have higher IC50 values for 5-FU compared to BRAF-mutated cell lines. In conclusion, the genetic polymorphisms DPYD rs1801265, ABCB1 rs1045642 and MTHFR rs180113 may serve as useful biomarkers for predicting a poor prognosis in patients undergoing 5-fluorouracil chemotherapy, regardless of EGFR pathway mutations.
Keywords:
colorectal cancer
; pharmacogenomics
; biomarkers
1. Introduction
Colorectal cancer (CRC) is still one of the leading causes of death in Chile and worldwide, and it is defined as malignant neoplasia that develops from the colon or rectum epithelial tissue [1,2]. A higher incidence of CRC is observed in developing countries with increasing Human Developed Index (HDI) characterized by higher prevalence of risk factors such as obesity, low physical activity, and low socioeconomic status [3]. As of 2020, the mortality rate due to colorectal cancer in Chile was 11.0 and 8.1/100,000 inhabitants, in men and women, respectively [4]. The survival rate for colorectal cancer is variable and depends on the stage diagnosed among other factors. Approximately 50% to 60% of patients diagnosed with colorectal cancer develop metastases, and 80% to 90% of these patients have unresectable metastatic liver disease [2]. Colorectal cancer recurrence after curative therapy (surgery followed by adjuvant chemotherapy) occurs in 80% and 95% of cases in the first 3 and 5 years, respectively [5,6]. The median overall survival in the metastatic setting has been estimated between 15.0 and 40.3 months and depends, among other factors, on the clinical characteristics, the tumor sidedness, and some molecular characteristics which are prognostic and eventually predictive for certain systemic therapies [7].
The treatment of metastatic CRC improved significantly with the incorporation of 5-fluorouracil (5-FU) in chemotherapy regimens in combination with leucovorin (LV) [8] and remains the backbone of most systemic treatments. Capecitabine, a prodrug of 5-fluorouracil, has similar efficacy [9]. The addition of oxaliplatin (FOLFOX regimen) to 5-FU improves the response rate and progression-free survival compared to 5-fluorouracil [10,11]. Capecitabine in combination with oxaliplatin (CAPEOX) is non-inferior to FOLFOX in first-line metastatic colorectal cancer [9]. Irinotecan (CPT-11) combined with 5-FU/LV (FOLFIRI) is another option in advanced colorectal cancer, with a different toxicity profile, but is considered equivalent to FOLFOX and [12,13]. Biological therapies, such as EGFR inhibitors (cetuximab, panitumumab), antiangiogenic agents (bevacizumab), BRAF/MEK inhibitors [14], have shown benefits in advanced metastatic disease, where these antibodies have an established role [1,2,14,15 ] whereas targeted treatment for KRASG12C-mutations is in development (e.g. sotorasib (AMG 510), adagrasib (MRTX849).
5-FU is primarily metabolized by the dihydropyridine dehydrogenase (DPD) enzyme (>80%) to 5,6-dihydro-5-FU. DPD is found primarily in liver and gastrointestinal tissue and has been identified as the main source of inter-patient variability in the pharmacokinetics of 5-FU. This variability is mainly explained by genetic polymorphisms in the DPYD gene, which encodes the DPD protein with different polymorphic variants c.1905+1 G>A, c.1679T>G, c.1236G>A/HapB3, c.1601G>A and c.2846A>T [16]. The effects of these genetic variants on DPD enzyme expression levels are well documented [17,18], as well as the effects on 5-FU metabolism [17,19]. In the DPYD gene, c.1679T>G and c.1236G>A/HapB3, DPYD*2A and c.2846A>T) are predictors of the toxicity generated by 5-fluorouracil regimens [13,18]. However, the effects of these DPYD polymorphism on the chemotherapy efficacy is controversial.
Similarly, mutations in ABCs transporters genes have been identified as significant contributors to colorectal cancer (CRC) progression and patient survival. Studies have shown that mutations in ABCB1 gene, encoding MDR1 (P-glycoprotein), can lead to multidrug resistance in CRC cells, resulting in poor response to chemotherapy [20]. Additionally, alterations in ABCC2 gene, encoding MRP2, have been associated with unfavorable clinical outcomes and reduced overall survival in CRC patients [21,22]. These findings highlight the importance of ABCs transporter mutations as prognostic factors and their role in therapeutic resistance in CRC. Further investigation into the mechanisms underlying these mutations and the development of targeted therapies is warranted to improve patient outcomes.
On the other hand, the tumor mutational status in colorectal cancer has been an important point of interest to find efficacy biomarkers. In colorectal cancer, KRAS, NRAS, BRAF and PIK3CA mutations induce a negative effect on the response to anti-EGFR therapies [23,24], specifically, only KRAS wild-type patients are candidates to anti-EGFR treatments. In addition, BRAF-mediated signaling is associated with poor prognosis; mainly, the V600E mutation in the kinase domain of the protein that generates a conformation that leads to constitutive activation [23]. BRAF V600E occurs in 8.2% of mCRC and is associated with poor survival. In BRAF V600E patients, 21.2% have poor mismatch repair (dMMR) versus 3.6% of dMMR in BRAF wild-type patients. Both markers are associated with a poor response [25]. BRAF V600E in patients with metastatic CRC is predictor of response to BRAF/MEK inhibitors and is a standard treatment [14]. Besides, PIK3CA, encoding the catalytic subunit of the phosphoinositide 3-kinase (PI3K) pathway, is frequently mutated in CRC and have a significant impact on patient survival. Dysregulation of the PI3K pathway due to PIK3CA mutations promotes tumor progression and resistance to therapy, leading to adverse patient outcomes. Various studies have reported the prevalence of PIK3CA mutations in CRC ranging from 10% to 20%, with hotspot mutations such as H1047R and E545K being the most common. These mutations result in constitutive activation of the PI3K pathway, leading to enhanced cell proliferation and survival [26]. Several studies have indicated that CRC patients harboring PIK3CA mutations have poorer overall survival compared to those without these mutations [27,28].
Both tumor mutational status and drug-metabolism polymorphisms has the potential effect on the prognosis of colorectal cancer patients. For example, EGFR mutations in exon 19 correlated with high expression of ERCC1 (oxaliplatin-related gene), low expression of TYMS (5-FU-related gene) and poor prognosis in lung cancer patients [29]. Furthermore, in vitro studies in lung cancer cells showed that EGFR exon 19 mutations increase DPD expression through the transcriptional factor SP1 [30]. This regulation of DPD may explain the limited benefit of tegafur (5-FU prodrug) in patients with EGFR exon 19 mutations.
In colorectal cancer, resistance to 5-fluorouracil chemotherapy is associated with increased expression of DPD and a possible increase in thymidylate synthase [31]. Clinical studies have shown that 5-FU and oxaliplatin-based regimens in metastatic colorectal cancer increase ERCC1 mRNA, thymidylate synthase, and DPD, and this effect is associated with decreased survival [32,33]. The only study in colorectal cancer that associates KRAS mutation and DPYD variations showed that -c.496A>C DPYD is present only in KRAS wild-type patients [34].
The effect complementary or independent of EGFR pathway mutations (EGFR, KRAS, NRAS, BRAF, PI3KCA) and the 5-Fluorouracil and Oxaliplatin -related genes polymorphisms (DPYD, TYMS, ERCC1) on the prognosis of colorectal cancer is unknown.
Therefore, this study has the objective of clarify the independence of EGFR mutations and drug-genes polymorphisms on the overall survival.
2. Results
2.1. Patient characteristics
A total of sixty-three (63) patients were included in this report. Demographic and pathology characteristics are presented in Table 1. The median age was 66.4 years (range: 30.4-81.8), and 32 patients were females (50.8%). Primary tumor origin was left in 46 (73.0%) patients and right in 15 (17.5%) patients. Monoclonal antibodies therapy (cetuximab, panitumumab and bevacizumab) was used in 14/63 patients (22.2%). A second line of treatment was used in 37/63 patients (56.8%).
2.2. Molecular profile
Table 2 shown the germline DNA variations. The genotypic frequency of TYMS del-del 3’UTR was presented in 31 of 63 patients (49.2%). The GSTP1 G/G genotype was found in 15 of 65 patients (23.8%). In the DPYD c.85T>C characterization, the genotype G/A was found in 19 patients of 63 (30.2%) and the A/A genotype was found in 37 patients of 63 (58.7%). The ABCB1 C4535T G/G was presented in 21 patients (33.3%), ABCB1 C1236T G/G was presented in 15 of 63 patients (23.8%), ABCC2 rs717620 C/C was presented in 46 of 63 patients (73.0%), MTHFR rs1801131 A/A was presented in 33 of 63 patients (52.4%) and ERCC2 rs13181 G/G was presented in 25 of 63 patients (39.7%). The mutational profile in tumor DNA is presented in the Table 3. Seven patient tumors (11.1%) had PI3KCA gene mutations. KRAS and BRAF V600E mutations were detected in 22 (34.9%) and 7 (11.1%) patients respectively.
2.3. Correlations of clinicopathological characteristics and mutation profile with overall survival
Univariate cox regression analysis shown liver metastases is related with a poor survival (HR=3.51, 95% CI 1.52-8.07) (Figure 1 and Table 4). In the tumor mutations biomarkers, BRAF V600E wild-type status correlated with better survival than BRAF V600E patients (HR=0.28, 95% CI 0.087-0.909) (Table 4), KRAS mutations had no association with overall survival and PI3KCA mutation correlated to better survival than PI3KCA wild-type (HR=0.271, 95% CI 0.84-0,876) (Table 4). In drug-metabolism polymorphisms, GSTP1 rs1695 G/G genotype was associated with a better overall survival compared with GSTP1 rs1695 G/A + A/A genotype, HR=0.484 (0.234-1.00) (Table 4). Finally, DPYD rs1801265 G/G genotype (HR= 1.819, 95% CI 1.03-3.19) (Table 4), ABCB1 rs1045642 G/G genotype (HR=1.782, 95% CI 1.03-3.19) (Table 4), MTHFR rs180113 C/C genotype (HR= 2.295, 95% CI 1.05-4.97) (Table 4), and TYMS rs151264360 del/del genotype (HR=2.169, 95%CI 1.21-3.86) (Table 4) correlated with a poor survival (Table 4). A preliminary combinatory analysis was performed to find a high-risk profile among the drug-metabolism polymorphisms. The high-risk profile was defined as the presence of at least one genotype of risk of DPYD rs1801265, ABCB1 rs1045642 and MTHFR rs180113 polymorphisms. The high-risk profile presence correlated with a poor survival (HR= 2.06, 95% CI 1.13-3.74) (Figure 2, Table 4).
Multivariate analysis included all variables with a p-value < 0.1 using a step wise procedure. The Table 5 shows the multivariate final model, where liver metastases presence (HR=3.69, 95% CI 1.49-9.09), DPYD rs1801265 G/G genotype (HR=1.88, 95% CI 0.99-3.54), ABCB1 rs1045642 G/G genotype (HR=2.62, 95% CI 1.37-4.99) and MTFHR rs180113 C/C genotype (HR= 2.63, 95% CI 1.13-6.15) were poor survival biomarkers (Table 5).
The effect of high-risk classification in drug-metabolisms polymorphisms was tested together tumor mutations status. Neither BRAF V600E mutations (Figure 3) nor KRAS mutations (Figure 4) were associated to survival in the multivariate analysis (Table 6). However, PI3KCA mutated status (Figure 5) correlated with a better survival than PI3KCA wild-type patients (HR= 0.22, 95% CI 0.05-0.95) (Table 6) in this multivariate and combinate model that considers high-risk presence and liver metastases presence.
The effect of BRAF V600E wild-type and high-risk drug-metabolism polymorphism was tested as an independent group compare with all other patients (Figure 6). The combination of these group correlated with a poor prognosis (HR = 2.71, 95% CI 1.46 – 5.01) (Table 7).
TCGA COARED cohort shown that DPYD low expression is related to better survival versus DPYD normal expression in stage III (Figure 7). The association between TYMS expression resulted not significant. However, the high expression profile of TYMS, TK1, TYMP and FOX1 is associated with a longer overall survival (Figure 8).
2.4. Drug sensitivity analysis
Cell line sensitivity to 5-fluorouracil showed that IC50 was higher in BRAF wild-type cell lines versus BRAF mutated cells lines. The comparisons between mutational status and IC50 values were not statistically significant to EGFR, KRAS and PIK3CA genes (Figure 9).
3. Discussion
This is a retrospective study of 63 patients with CRC treated with FOLFOX/CapeOx treatment as first-line in the Chilean population. The correlation of TYMS, GSTP1, DPYD, and ABCB1 gene variation and tumor mutations (KRAS, NRAS, BRAF, and PI3KCA) is poorly understood in the literature. Here, we report high-risk of genetic polymorphisms associated with the overall survival in colon cancer patients. The high-risk profile includes DPYD rs1801265, ABCB1 rs1045642 and MTHFR rs180113 polymorphisms. Our results indicated that BRAF V600E mutation was associated with better overall survival and high sensitivity to 5-fluorouracil in cell line assay. In addition, the combination of BRAF V600E wild-type and high-risk drug—metabolism polymorphisms correlated with a poor prognosis. Also, PI3KCA mutated status correlated with a better survival, however, EGFR, NRAS and KRAS status is not related with overall survival, but these results are limited to a small sample size. In the univariate and multivariate cox regression analysis, the liver metastases presences are associated with poor overall survival.
In this study, we propose a high-risk profile of genetic polymorphisms related with the drug-metabolism of chemotherapy in colon cancer. First, we found that DPYD rs1801265 (G/G) genotype is associated with poor prognosis. This result is consistence with the fact of G allele is related with a high activity of DPD enzyme, and the subsequent high elimination of 5-fluorouracil and a low antitumor activity. The impact of DPD deficiency on toxicity is well documented [17 ], as well as the effects on 5-FU metabolism [17,19]. However, the effect of DPD deficiency on efficacy outcomes is controversial. In the TCGA analysis we found that DPYD low expression is related to better overall survival compare DPYD normal expression. Second, we found that ABCB1 rs1045642 G/G genotype is associated with poor prognosis. The effect could be explained by the fact of this polymorphisms cause an increase of glycoprotein P (PgP) expression with the increase of efflux of 5-fluoruracil from tumor cells [20]. Third, MTHFR rs180113 was a risk factor associated with poor prognosis. This result is consistent with previous studies that associated C/C genotype with a low enzymatic activity and the subsequent low restitution of tetrahydrofolate and antitumor effect of 5-fluoruracil on TYMS.
Previous studies have shown that 3’UTR polymorphisms (6 bp deletion) in TYMS leads to destabilization of mRNA, reducing the translation and TS activity. On the other hand, 3’UTR with insertion of 6bp leads to stability of mRNA, increasing the TYMS transcription/activity and the poor clinical response [3]. However, other studies have showed that 3’UTR polymorphisms predict a longer diseases-progression survival and overall survival [35]. In TCGA cohort, we found that patients with a high expression of TYMS, TK1, TYMP and FOX1 genes is associated with a longer overall survival according to previous reports [36]. FOXM1 plays a key role in increase the over-expression of genes implicated in the tumoral resistance to 5-fluorouyracil treatments [37]. Probably, additional studies are necessary to confirm the effect of TYMS polymorphism and the combination or inclusion to the high-risk profile propose here.
Our findings shown that EGFR, KRAS, NRAS and PI3KCA are not a predictive factor of overall survival neither univariate nor multivariate analysis. These findings are consistent with previous studies showing controversial association of KRAS with clinical outcomes [38,39]. Previous studies have showed a small or absent effect of BRAF on the prognosis in colon cancer treated with 5-fluoruracil based chemotherapy [40]. However, the analysis of the high-risk profile of genetic polymorphism together BRAF V600E wild type showed the risk effect of those biomarkers in the cohort of Chilean patients. This observation is complementary with the results obtained from genomics drugs sensitivity of cancer (GDSC) analysis. Cell lines BRAF mutated status correlated with a higher sensitivity to 5-fluorouracil consistently with previous studies [41]. Despite the small sample size and the reference studies, the BRAF status could be consider a predictive biomarker of 5-fluoruracil treatment in colorectal cancer.
The primary objective of this study was to examine host characteristics, including germline polymorphisms in drug metabolism genes, and tumor characteristics, such as mutational profile. Following the comprehensive analysis, we found that the liver metastases status and the high-risk profile of drug-metabolism polymorphisms were associated with a poor prognosis (as indicated in Table 5) in the multivariate analysis. The effect of BRAF V600E is complementary to this high-risk profile proposed. In future studies, it is recommended to expand the sample size to validate the impact of these biomarkers in the prognosis of colorectal cancer treated with 5-fluoruracil based chemotherapy.
4. Materials and Methods
4.1. Patients and Tissue sampling
Formalin-fixed paraffin-embedded (FFPE) CRC samples (63 sixty-three) were obtained from patients at National Cancer Institute from Chile and Clinical Hospital from University of Chile. Selection criteria were older than 18 years adults and histologically diagnosed with stage IV colorectal cancer, adenocarcinoma histology and 5-fluorouracil based chemotherapy. The study was approved by the Ethics Committee of North Health Service of Metropolitan Region in accordance with Good Clinical Practice (GCP), Declaration of Helsinki and International Conference of Harmonization (ICH). All tumor samples underwent histopathological review using hematoxylin-eosin (HE) staining from FFPE blocks. Tumor samples was defined as FFPE slides containing < 10 % necrosis, and < 50 % non-neoplastic tissue. Germline samples was defined as FFPE slides containing < 10% necrosis, and < 20% tumor tissue.
In addition, TCGA Colon Cancer cohort (Pan Cancer Atlas) was included in the analysis. The expression of TYMS and DPYD mRNA data was obtained and downloaded from cBioportal. The mRNA expression used a z-score of 2 and comparing the tumor samples versus normal samples (https://www.cbioportal.org/).
4.2. Molecular testing
Extraction and purification of DNA and RNA from FFPE samples was performed using Qiagen AllPrep DNA/RNA FFPE kit according to the manufacturer’s instructions. Briefly, fresh FFPE tissue (2-4 sections of 10-20 µm) containing > 50% tumor cells were deparaffinized and incubated in a lysis buffer containing proteinase K, the mixture was centrifuged to precipitate the DNA, leaving the RNA in the supernatant. In addition, freshly cut FFPE tissue (10-20 µm sections) containing normal cells were used for similar DNA and RNA extraction. Genotyping of Drug-metabolism drug was performed using TaqMan® assay. Mutational profile of tumor DNA was performed using EntroGen® Colon Cancer mutation detection panel (CRC-RT48).
4.3. Drug sensitivity analysis
Drug sensitivity data (bulk data) for colon and rectum adenocarcinoma cell lines (COREAD) were obtained from “The Genomics Cancer Drug Sensitivity” database (https://www.cancerrxgene.org/). COREAD cell line was selected to compare the mutational profile and Ln IC50 values to 5-fluorouracil. The mutational profile includes the follow mutations: EGFR, KRAS, NRAS and BRAF. The comparison between mutated cell lines and wild-type cell lines was tested using Wilcoxon test (non-parametric).
4.4. Statistical analysis
Descriptive analysis was used to characterize the patients. Overall survival (OS) was evaluated up to 60 months of follow-up. Kaplan-Meier analysis with log-rank test and multivariate Cox regression models (step wise method) were used to evaluate the effect of mutational profile and drug-metabolism polymorphisms over therapeutic responses. The time from the start of diagnosis to death from any cause was monitored to perform the survival analysis. All analyses were performed in R software [42 ].
5. Conclusion
The genetic polymorphisms DPYD rs1801265, ABCB1 rs1045642 and MTHFR rs180113 may serve as useful biomarkers of poor prognosis independently of EGFR pathway mutations in patients undergoing 5-fluorouracil chemotherapy.
Author Contributions
Conceptualization, J.P.C., L.C., J.L.L and L.Q.; methodology, J.P.C., N.V., L.C., S.C.; software, J.P.C. and L.C.; validation, L.C., N.V., D.C. and L.Q.; formal analysis, J.P.C. and L.C.; investigation, F.R., J.L.L. and A.C.; resources, A.C., S.C.; data curation, L.C. and J.P.C.; writing—original draft preparation, L.Q., and J.P.C.; writing—review and editing, L.Q., J.P.C, N.V., L.C., A.C., F.R., J.L.L., S.C., C.G. and D.C.; project administration, N.V.; funding acquisition, L.Q. All authors have read and agreed to the published version of the manuscript.
Funding
This research and the APC were funded by FONDECYT REGULAR, grant number 1211948.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of “Servicio de Salud Metropolitano Norte” (protocol code CQF-EC-001-17, N°053/21017 approved on 06th October 2017 and protocol code CQF-EC-02-22, N°037/2022, approved on 07th October 2022).
Informed Consent Statement
Patient consent was waived due to loss of follow-up patients. The research would not be feasible without a waiver of informed consent. Also, this observational study considers a minimal risk to the patients.
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Acknowledgments
The authors wish to thank the colorectal cancer patients from the “Instituto Nacional del Cáncer”, “Hospital San José” and “Hospital Clínico de la Universidad de Chile” for their altruistic collaboration in pursuit of the common welfare.
Conflicts of Interest
The authors declare no conflict of interest.
References
- MINSAL. Guía de Práctica Clínica Cáncer Colorectal en Personas de 15 años y más. Available at: https://diprece.minsal.cl/garantias-explicitas-en-salud-auge-o-ges/guias-de-practica-clinica/cancer-colorectal-en-personas-de-15-anos-y-mas/resumen-ejecutivo/.
- National Comprehensive Cancer Network (NCCN). Colon Cancer, Version 2.2023, NCCN Clinical Practice Guidelines in Oncol-ogy. Natl Compr Cancer Netw: JNCCN. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf.
- Watanabe, T.; Wu, T.-T.; Catalano, P. J.; Ueki, T.; Satriano, R.; Haller, D. G.; Benson, A. B.; Hamilton, S. R. Molecular Predictors of Survival after Adjuvant Chemotherapy for Colon Cancer. NEJM 2001, 344 (16), 1196–1206. [CrossRef]
- International Agency for Research on Cancer (IARC). Global Cancer Observatory. Available at: https://gco.iarc.fr/.
- Sargent, D.; Sobrero, A.; Grothey, A.; O’Connell, M. J.; Buyse, M.; Andre, T.; Zheng, Y.; Green, E.; Labianca, R.; O’Callaghan, C.; Seitz, J. F.; Francini, G.; Haller, D.; Yothers, G.; Goldberg, R.; de Gramont, A. Evidence for Cure by Adjuvant Therapy in Colon Cancer: Observations Based on Individual Patient Data From 20,898 Patients on 18 Randomized Trials. J Clin Oncol 2009, 27 (6), 872–877. [CrossRef]
- Seo, S. I.; Lim, S.-B.; Yoon, Y. S.; Kim, C. W.; Yu, C. S.; Kim, T. W.; Kim, J. H.; Kim, J. C. Comparison of Recurrence Patterns between ≤5 Years and >5 Years after Curative Operations in Colorectal Cancer Patients. J Surg Oncol 2013, 108 (1), 9–13. [CrossRef]
- Lenz, H.-J.; Ou, F.-S.; Venook, A. P.; Hochster, H. S.; Niedzwiecki, D.; Goldberg, R. M.; Mayer, R. J.; Bertagnolli, M. M.; Blanke, C. D.; Zemla, T.; Qu, X.; Wirapati, P.; Tejpar, S.; Innocenti, F.; Kabbarah, O. Impact of Consensus Molecular Subtype on Survival in Pa-tients With Metastatic Colorectal Cancer: Results From CALGB/SWOG 80405 (Alliance). J Clin Oncol 2019, 37 (22), 1876–1885. [CrossRef]
- Efficacy of Intravenous Continuous Infusion of Fluorouracil Compared with Bolus Administration in Advanced Colorectal Can-cer. Meta-Analysis Group In Cancer. J Clin Oncol 1998, 16 (1), 301–308. [CrossRef]
- Mahfouf, H.; Djeddi, H.; Belhadef, S.; Bouzid, K.; Bentabak, K. Capecitabine Combined with Oxaliplatin (XELOX) as First-Line Chemotherapy in Colorectal Cancer with Liver Metastases. J Clin Oncol 2009, 27 (15_suppl), e15146–e15146. [CrossRef]
- Bleiberg, H.; de Gramont, A. Oxaliplatin plus 5-Fluorouracil: Clinical Experience in Patients with Advanced Colorectal Cancer. Semin Oncol 1998, 25 (2 Suppl 5), 32–39.
- Giacchetti, S.; Perpoint, B.; Zidani, R.; Le Bail, N.; Faggiuolo, R.; Focan, C.; Chollet, P.; Llory, J. F.; Letourneau, Y.; Coudert, B.; Bertheaut-Cvitkovic, F.; Larregain-Fournier, D.; Le Rol, A.; Walter, S.; Adam, R.; Misset, J. L.; Lévi, F. Phase III Multicenter Ran-domized Trial of Oxaliplatin Added to Chronomodulated Fluorouracil–Leucovorin as First-Line Treatment of Metastatic Colo-rectal Cancer J Clin Oncol 2000, 18 (1), 136–136. [CrossRef]
- Douillard, J.; Cunningham, D.; Roth, A.; Navarro, M.; James, R.; Karasek, P.; Jandik, P.; Iveson, T.; Carmichael, J.; Alakl, M.; Gruia, G.; Awad, L.; Rougier, P. Irinotecan Combined with Fluorouracil Compared with Fluorouracil Alone as First-Line Treatment for Metastatic Colorectal Cancer: A Multicentre Randomised Trial. The Lancet 2000, 355 (9209), 1041–1047. [CrossRef]
- Saltz, L. B.; Cox, J. V.; Blanke, C.; Rosen, L. S.; Fehrenbacher, L.; Moore, M. J.; Maroun, J. A.; Ackland, S. P.; Locker, P. K.; Pirotta, N.; Elfring, G. L.; Miller, L. L. Irinotecan plus Fluorouracil and Leucovorin for Metastatic Colorectal Cancer. NEJM 2000, 343 (13), 905–914. [CrossRef]
- Fakih, M. G.; Kopetz, S.; Kuboki, Y.; Kim, T. W.; Munster, P. N.; Krauss, J. C.; Falchook, G. S.; Han, S.-W.; Heinemann, V.; Muro, K.; Strickler, J. H.; Hong, D. S.; Denlinger, C. S.; Girotto, G.; Lee, M.-A.; Henary, H.; Tran, Q.; Park, J. K.; Ngarmchamnanrith, G.; Prenen, H.; Price, T. J. Sotorasib for Previously Treated Colorectal Cancers with KRASG12C Mutation (CodeBreaK100): A Prespecified Analysis of a Single-Arm, Phase 2 Trial. Lancet Oncol 2022, 23 (1), 115–124. [CrossRef]
- MINSAL. Guias Clínicas AUGE. Colecistectomía Preventiva en adultos de 35 a 49 años. Available at: http://www.supersalud.gob.cl/difusion/665/w3-article-600.html.
- Caudle, K. E.; Thorn, C. F.; Klein, T. E.; Swen, J. J.; McLeod, H. L.; Diasio, R. B.; Schwab, M. Clinical Pharmacogenetics Implementa-tion Consortium Guidelines for Dihydropyrimidine Dehydrogenase Genotype and Fluoropyrimidine Dosing. Clin Pharmacol Ther 2013, 94 (6), 640–645. [CrossRef]
- Hirota, T.; Date, Y.; Nishibatake, Y.; Takane, H.; Fukuoka, Y.; Taniguchi, Y.; Burioka, N.; Shimizu, E.; Nakamura, H.; Otsubo, K.; Ieiri, I. Dihydropyrimidine Dehydrogenase (DPD) Expression Is Negatively Regulated by Certain MicroRNAs in Human Lung Tissues. Lung Cancer 2012, 77 (1), 16–23. [CrossRef]
- van Kuilenburg, A. B. P.; Häusler, P.; Schalhorn, A.; Tanck, M. W. T.; Proost, J. H.; Terborg, C.; Behnke, D.; Schwabe, W.; Jabschinsky, K.; Maring, J. G. Evaluation of 5-Fluorouracil Pharmacokinetics in Cancer Patients with a c.1905+1G>A Mutation in DPYD by Means of a Bayesian Limited Sampling Strategy. Clin Pharmacokinet 2012, 51 (3), 163–174. [CrossRef]
- Panczyk, M. Pharmacogenetics Research on Chemotherapy Resistance in Colorectal Cancer over the Last 20 Years. World J Gas-troenterol 2014, 20 (29), 9775. [CrossRef]
- Zheng, Q.; Wu, H.; Yu, Q.; Kim, D. H.; Lipton, J. H.; Angelini, S.; Soverini, S.; Vivona, D.; Takahashi, N.; Cao, J. ABCB1 Polymor-phisms Predict Imatinib Response in Chronic Myeloid Leukemia Patients: A Systematic Review and Meta-Analysis. Phar-macogenomics J 2015, 15 (2), 127–134. [CrossRef]
- Leschziner, G. D.; Andrew, T.; Pirmohamed, M.; Johnson, M. R. ABCB1 Genotype and PGP Expression, Function and Therapeutic Drug Response: A Critical Review and Recommendations for Future Research. Pharmacogenomics J 2007, 7 (3), 154–179. [CrossRef]
- Kennedy, L.; Sandhu, J. K.; Harper, M.-E.; Cuperlovic-Culf, M. Role of Glutathione in Cancer: From Mechanisms to Therapies. Biomolecules 2020, 10 (10), 1429. [CrossRef]
- Davies, H.; Bignell, G. R.; Cox, C.; Stephens, P.; Edkins, S.; Clegg, S.; Teague, J.; Woffendin, H.; Garnett, M. J.; Bottomley, W.; Davis, N.; Dicks, E.; Ewing, R.; Floyd, Y.; Gray, K.; Hall, S.; Hawes, R.; Hughes, J.; Kosmidou, V.; Menzies, A.; Mould, C.; Parker, A.; Ste-vens, C.; Watt, S.; Hooper, S.; Wilson, R.; Jayatilake, H.; Gusterson, B. A.; Cooper, C.; Shipley, J.; Hargrave, D.; Pritchard-Jones, K.; Maitland, N.; Chenevix-Trench, G.; Riggins, G. J.; Bigner, D. D.; Palmieri, G.; Cossu, A.; Flanagan, A.; Nicholson, A.; Ho, J. W. C.; Leung, S. Y.; Yuen, S. T.; Weber, B. L.; Seigler, H. F.; Darrow, T. L.; Paterson, H.; Marais, R.; Marshall, C. J.; Wooster, R.; Stratton, M. R.; Futreal, P. A. Mutations of the BRAF Gene in Human Cancer. Nature 2002, 417 (6892), 949–954. [CrossRef]
- Shen, Y.; Wang, J.; Han, X.; Yang, H.; Wang, S.; Lin, D.; Shi, Y. Effectors of Epidermal Growth Factor Receptor Pathway: The Genetic Profiling of KRAS, BRAF, PIK3CA, NRAS Mutations in Colorectal Cancer Characteristics and Personalized Medicine. PLoS One 2013, 8 (12), e81628. [CrossRef]
- Venderbosch, S.; Nagtegaal, I. D.; Maughan, T. S.; Smith, C. G.; Cheadle, J. P.; Fisher, D.; Kaplan, R.; Quirke, P.; Seymour, M. T.; Richman, S. D.; Meijer, G. A.; Ylstra, B.; Heideman, D. A. M.; de Haan, A. F. J.; Punt, C. J. A.; Koopman, M. Mismatch Repair Status and BRAF Mutation Status in Metastatic Colorectal Cancer Patients: A Pooled Analysis of the CAIRO, CAIRO2, COIN, and FO-CUS Studies. Clinical Cancer Research 2014, 20 (20), 5322–5330. [CrossRef]
- Samuels, Y.; Diaz, L. A.; Schmidt-Kittler, O.; Cummins, J. M.; DeLong, L.; Cheong, I.; Rago, C.; Huso, D. L.; Lengauer, C.; Kinzler, K. W.; Vogelstein, B.; Velculescu, V. E. Mutant PIK3CA Promotes Cell Growth and Invasion of Human Cancer Cells. Cancer Cell 2005, 7 (6), 561–573. [CrossRef]
- Ganesan, P.; Janku, F.; Naing, A.; Hong, D. S.; Tsimberidou, A. M.; Falchook, G. S.; Wheler, J. J.; Piha-Paul, S. A.; Fu, S.; Stepanek, V. M.; Lee, J. J.; Luthra, R.; Overman, M. J.; Kopetz, E. S.; Wolff, R. A.; Kurzrock, R. Target-Based Therapeutic Matching in Early-Phase Clinical Trials in Patients with Advanced Colorectal Cancer and PIK3CA Mutations. Mol Cancer Ther 2013, 12 (12), 2857–2863. [CrossRef]
- Garrido-Laguna, I.; Hong, D. S.; Janku, F.; Nguyen, L. M.; Falchook, G. S.; Fu, S.; Wheler, J. J.; Luthra, R.; Naing, A.; Wang, X.; Kur-zrock, R. KRASness and PIK3CAness in Patients with Advanced Colorectal Cancer: Outcome after Treatment with Early-Phase Trials with Targeted Pathway Inhibitors. PLoS One 2012, 7 (5), e38033. [CrossRef]
- Zhang, Q.; Sun, T.; Kang, P.; Qian, K.; Deng, B.; Zhou, J.; Wang, R.; Jiang, B.; Li, K.; Liu, F.; Wu, S.; Tan, Q. Combined Analysis of Rearrangement of ALK, ROS1, Somatic Mutation of EGFR, KRAS, BRAF, PIK3CA, and MRNA Expression of ERCC1, TYMS, RRM1, TUBB3, EGFR in Patients with Non-Small Cell Lung Cancer and Their Clinical Significance. Cancer Chemother Pharmacol 2016, 77 (3), 583–593. [CrossRef]
- Tominaga, T.; Tsuchiya, T.; Mochinaga, K.; Arai, J.; Yamasaki, N.; Matsumoto, K.; Miyazaki, T.; Nagasaki, T.; Nanashima, A.; Tsukamoto, K.; Nagayasu, T. Epidermal Growth Factor Signals Regulate Dihydropyrimidine Dehydrogenase Expression in EGFR-Mutated Non-Small-Cell Lung Cancer. BMC Cancer 2016, 16 (1), 354. [CrossRef]
- Nita, M. E.; Tominaga, O.; Nagawa, H.; Tsuruo, T.; Muto, T. Dihydropyrimidine Dehydrogenase but Not Thymidylate Synthase Expression Is Associated with Resistance to 5-Fluorouracil in Colorectal Cancer. Hepatogastroenterology 1998, 45 (24), 2117–2122.
- Jensen, S. A.; Vainer, B.; Sørensen, J. B. The Prognostic Significance of Thymidylate Synthase and Dihydropyrimidine Dehydro-genase in Colorectal Cancer of 303 Patients Adjuvantly Treated with 5-Fluorouracil. Int J Cancer 2007, 120 (3), 694–701. [CrossRef]
- Kornmann, M.; Schwabe, W.; Sander, S.; Kron, M.; Sträter, J.; Polat, S.; Kettner, E.; Weiser, H. F.; Baumann, W.; Schramm, H.; Häu-sler, P.; Ott, K.; Behnke, D.; Staib, L.; Beger, H. G.; Link, K. H. Thymidylate Synthase and Dihydropyrimidine Dehydrogenase MRNA Expression Levels: Predictors for Survival in Colorectal Cancer Patients Receiving Adjuvant 5-Fluorouracil. Clin Cancer Res 2003, 9 (11), 4116–4124.
- Kleist, B.; Kempa, M.; Meurer, T.; Poetsch, M. Correlation between DPYD Gene Variation and KRAS Wild Type Status in Colorec-tal Cancer. J Clin Pathol 2016, 69 (3), 204–208. [CrossRef]
- Hitre, E.; Budai, B.; Adleff, V.; Czeglédi, F.; Horváth, Z.; Gyergyay, F.; Lövey, J.; Kovács, T.; Orosz, Z.; Láng, I.; Kásler, M.; Kralo-vánszky, J. Influence of Thymidylate Synthase Gene Polymorphisms on the Survival of Colorectal Cancer Patients Receiving Ad-juvant 5-Fluorouracil. Pharmacogenet Genomics 2005, 15 (10), 723–730. [CrossRef]
- Huang, M.-Y.; Wu, C.-H.; Huang, C.-M.; Chung, F.-Y.; Huang, C.-W.; Tsai, H.-L.; Chen, C.-F.; Lin, S.-R.; Wang, J.-Y. DPYD , TYMS , TYMP , TK1 , and TK2 Genetic Expressions as Response Markers in Locally Advanced Rectal Cancer Patients Treated with Fluoropyrimidine-Based Chemoradiotherapy. Biomed Res Int 2013, 1–10. [CrossRef]
- Varghese, V.; Magnani, L.; Harada-Shoji, N.; Mauri, F.; Szydlo, R. M.; Yao, S.; Lam, E. W.-F.; Kenny, L. M. FOXM1 Modulates 5-FU Resistance in Colorectal Cancer through Regulating TYMS Expression. Sci Rep 2019, 9 (1), 1505. [CrossRef]
- Ntavatzikos, A.; Spathis, A.; Patapis, P.; Machairas, N.; Peros, G.; Konstantoudakis, S.; Leventakou, D.; Panayiotides, I. G.; Karakitsos, P.; Koumarianou, A. Integrating TYMS , KRAS and BRAF Testing in Patients with Metastatic Colorectal Cancer. World J Gastroenterol 2017, 23 (32), 5913. [CrossRef]
- Ntavatzikos, A.; Spathis, A.; Patapis, P.; Machairas, N.; Vourli, G.; Peros, G.; Papadopoulos, I.; Panayiotides, I.; Koumarianou, A. TYMS/KRAS/BRAF Molecular Profiling Predicts Survival Following Adjuvant Chemotherapy in Colorectal Cancer. World J Gastrointest Oncol 2019, 11 (7), 551–566. [CrossRef]
- André, T.; Boni, C.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Bonetti, A.; Clingan, P.; Bridgewater, J.; Rivera, F.; de Gra-mont, A. Improved Overall Survival With Oxaliplatin, Fluorouracil, and Leucovorin As Adjuvant Treatment in Stage II or III Colon Cancer in the MOSAIC Trial. J Clin Oncol 2009, 27 (19), 3109–3116. [CrossRef]
- Shi, T.; Gao, M.; He, M.; Yue, F.; Zhao, Y.; Sun, M.; He, K.; Chen, L. 5-FU Preferably Induces Apoptosis in BRAF V600E Colorectal Cancer Cells via Downregulation of Bcl-XL. Mol Cell Biochem 2019, 461 (1–2), 151–158. [CrossRef]
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available at: https://www.R-project.org/.
Figure 1.
Kaplan Meier curve of colorectal cancer patients according to liver metastases status (without liver metastases= blue line, with liver metastases=red line).
Figure 1.
Kaplan Meier curve of colorectal cancer patients according to liver metastases status (without liver metastases= blue line, with liver metastases=red line).
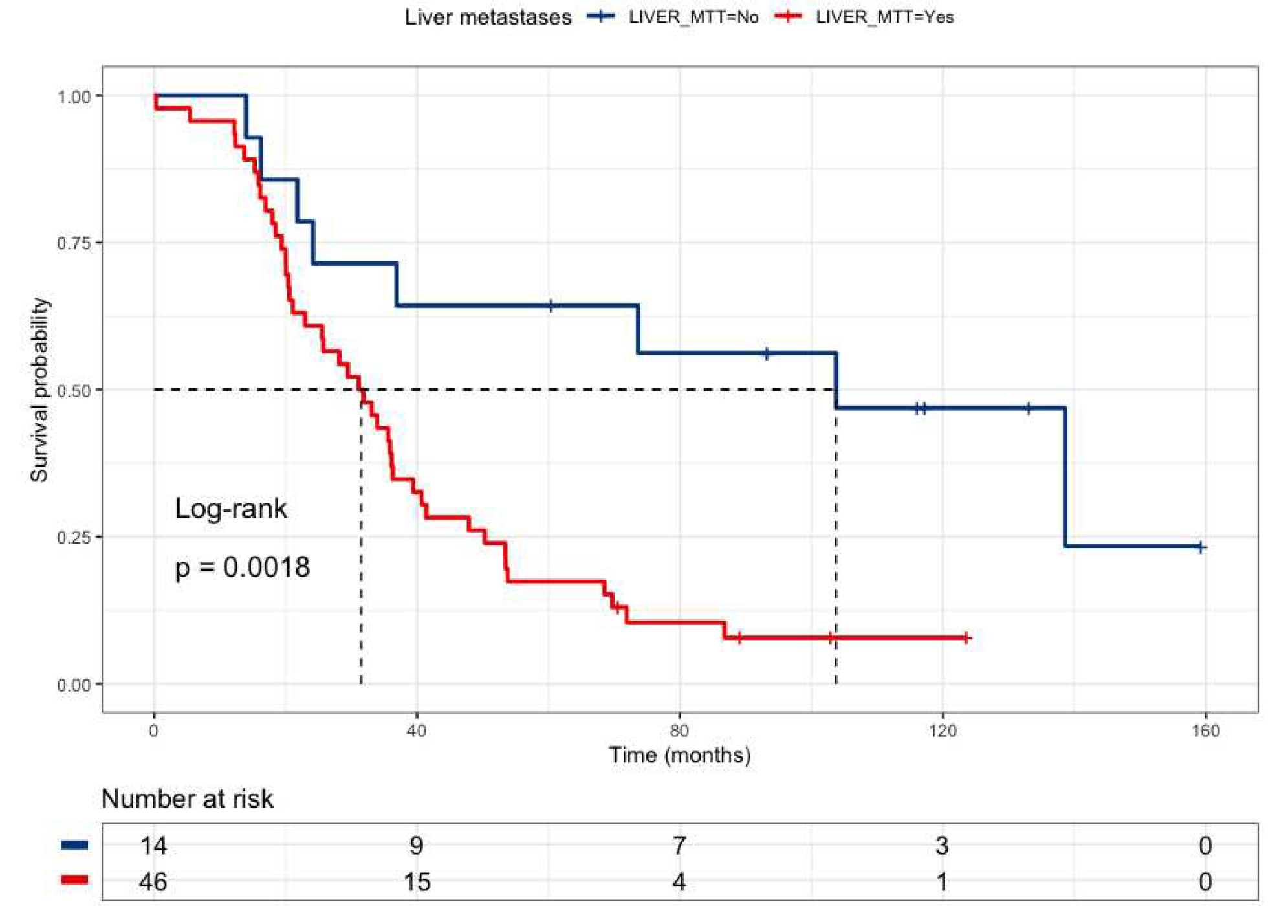
Figure 2.
Kaplan Meier curve of colorectal cancer patients according to High-Risk (DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs1801131) (Low risk= blue line, High risk=red line).
Figure 2.
Kaplan Meier curve of colorectal cancer patients according to High-Risk (DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs1801131) (Low risk= blue line, High risk=red line).
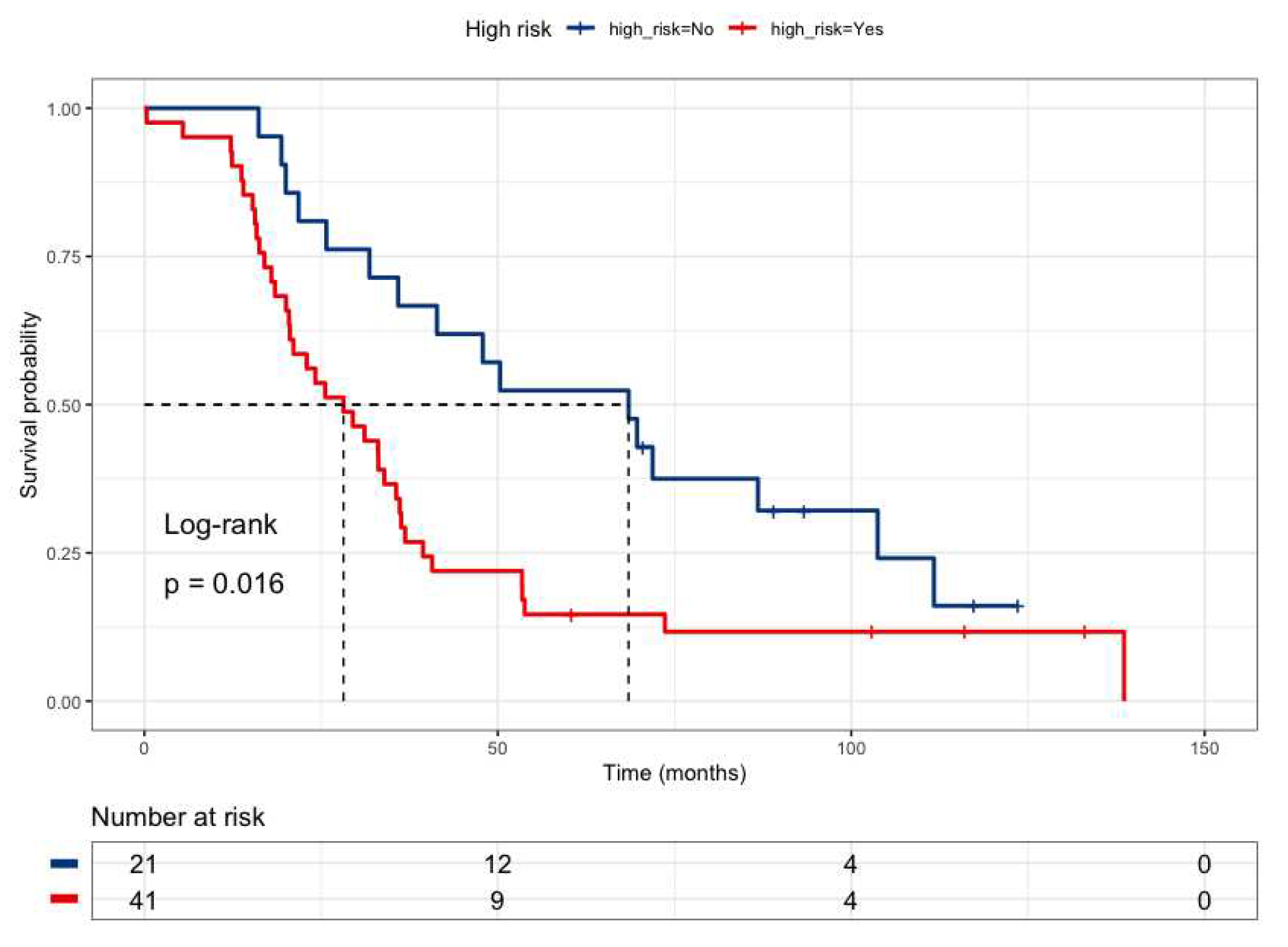
Figure 3.
Kaplan Meier curve of colorectal cancer patients according to High Risk profile and BRAF V600E mutational status (Low risk and BRAF V600E wild-type= blue line, Low risk and BRAF V600E mutated =red line, High risk and BRAF V600E wild-type= green line, High risk and BRAF V600E mutated =sky blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
Figure 3.
Kaplan Meier curve of colorectal cancer patients according to High Risk profile and BRAF V600E mutational status (Low risk and BRAF V600E wild-type= blue line, Low risk and BRAF V600E mutated =red line, High risk and BRAF V600E wild-type= green line, High risk and BRAF V600E mutated =sky blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
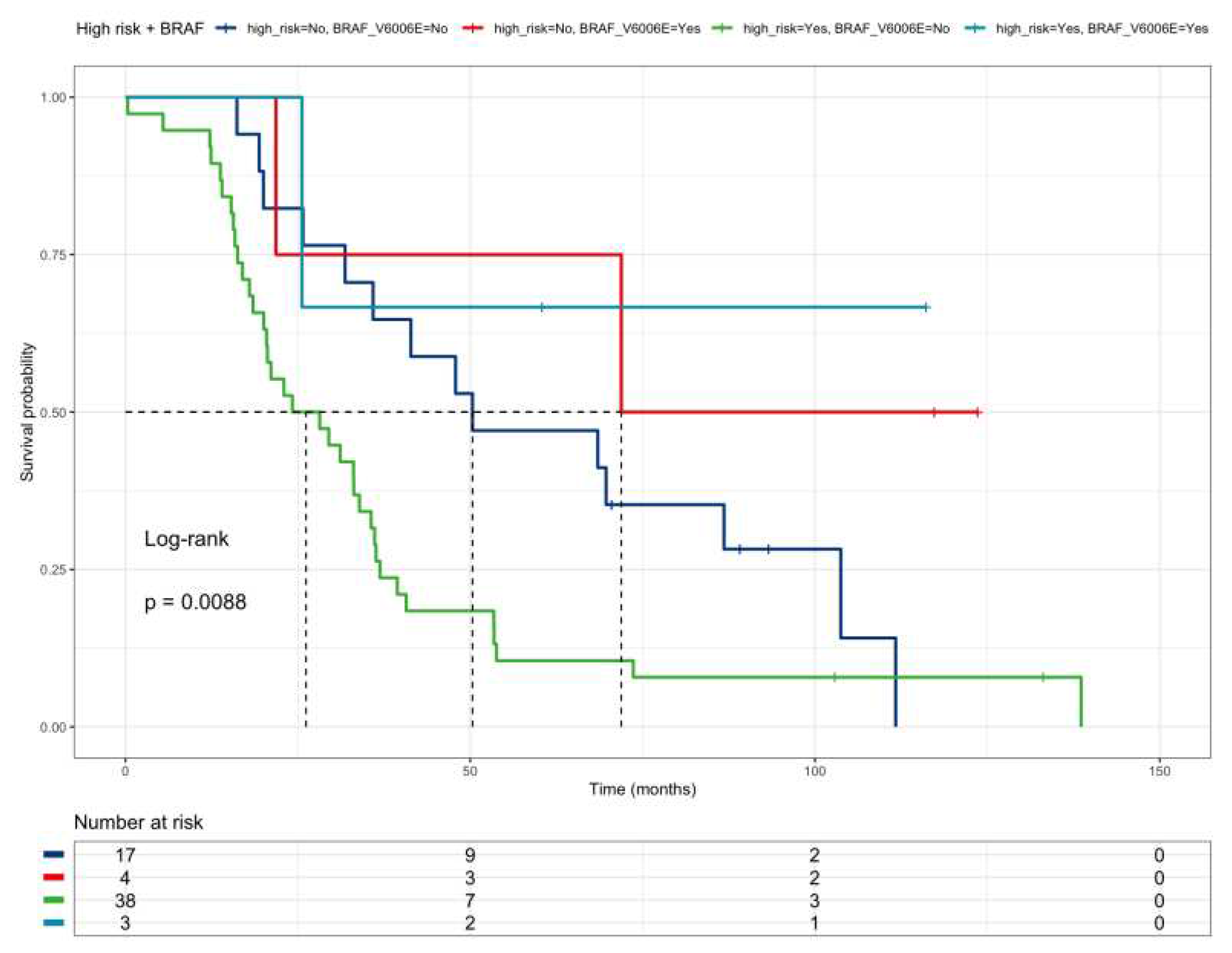
Figure 4.
Kaplan Meier curve of colorectal cancer patients according to High Risk profile and KRAS mutational status (Low risk and KRAS wild-type= blue line, Low risk and KRAS mutated =red line, High risk and KRAS wild-type= green line, High risk and KRAS mutated =sky blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
Figure 4.
Kaplan Meier curve of colorectal cancer patients according to High Risk profile and KRAS mutational status (Low risk and KRAS wild-type= blue line, Low risk and KRAS mutated =red line, High risk and KRAS wild-type= green line, High risk and KRAS mutated =sky blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
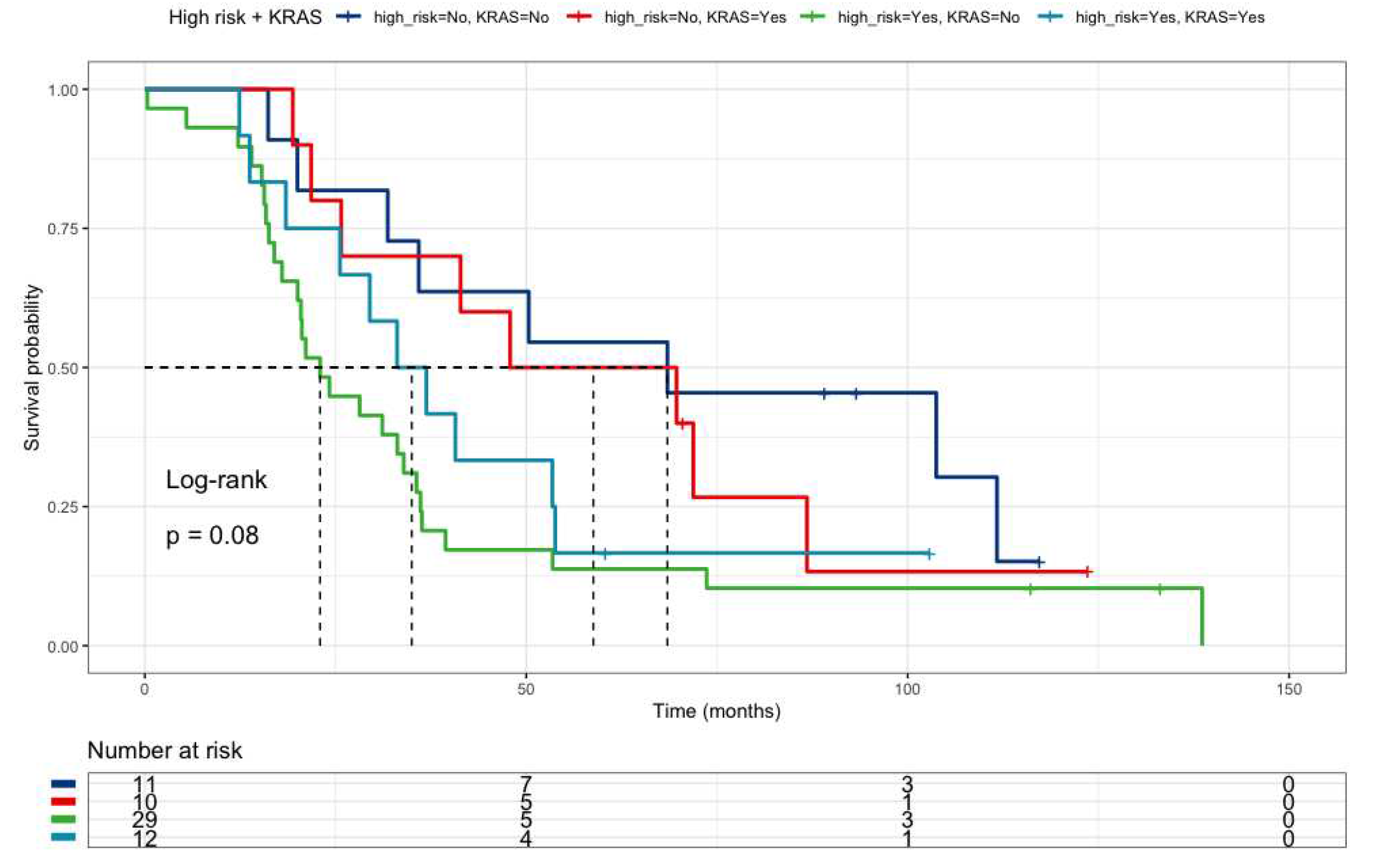
Figure 5.
Kaplan Meier curve of colorectal cancer patients according to High Risk profile and PI3KCA mutational status (Low risk and PI3KCA wild-type= blue line, Low risk and PI3KCA mutated =red line, High risk and PI3KCA wild-type= green line, High risk and PI3KCA mutated =sky blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
Figure 5.
Kaplan Meier curve of colorectal cancer patients according to High Risk profile and PI3KCA mutational status (Low risk and PI3KCA wild-type= blue line, Low risk and PI3KCA mutated =red line, High risk and PI3KCA wild-type= green line, High risk and PI3KCA mutated =sky blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
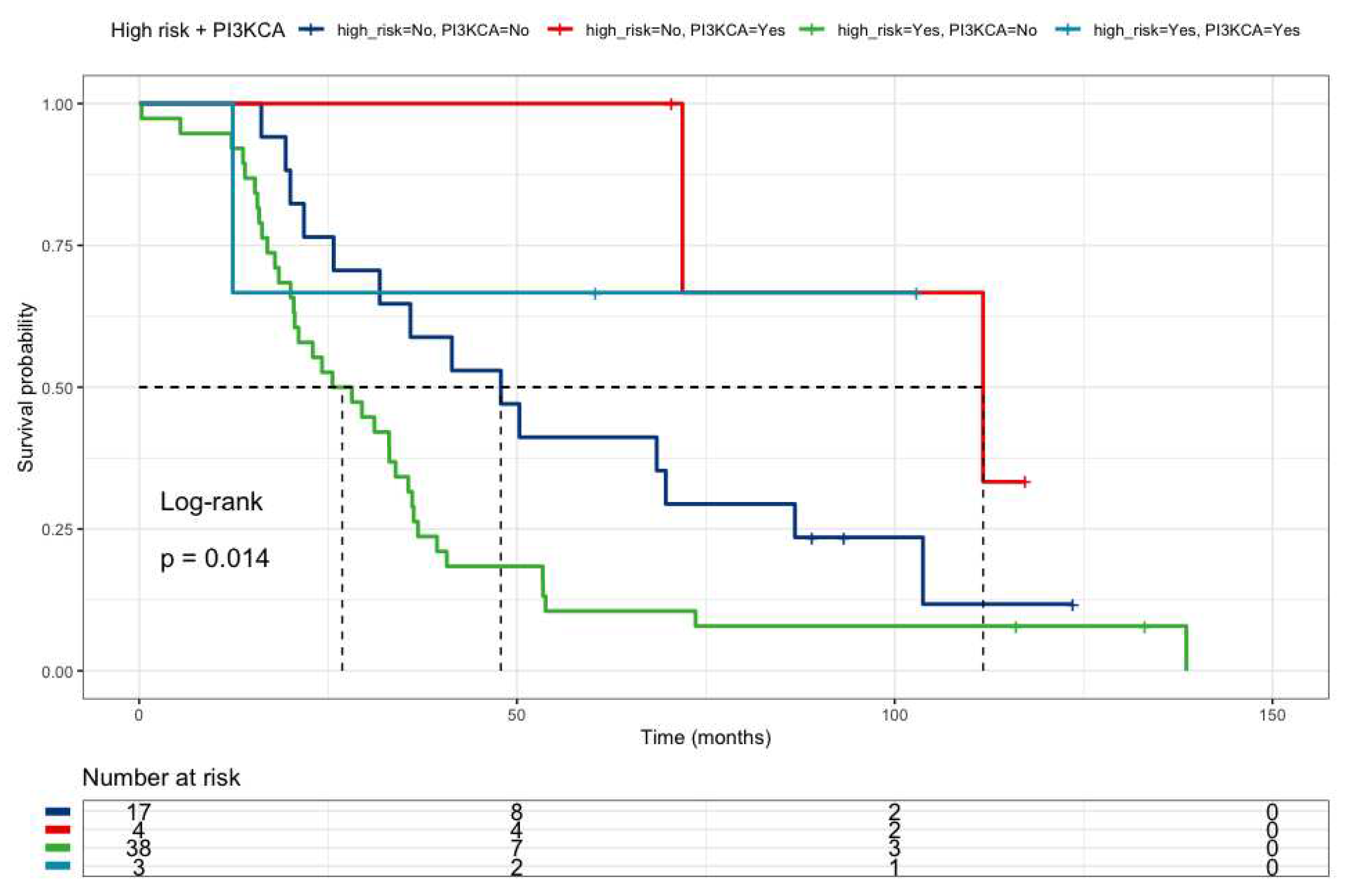
Figure 6.
Kaplan Meier curve of colorectal cancer patients comparing High Risk profile + BRAFV600E mutated patients together wild-type patients (red line) versus all the other patients (blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
Figure 6.
Kaplan Meier curve of colorectal cancer patients comparing High Risk profile + BRAFV600E mutated patients together wild-type patients (red line) versus all the other patients (blue line). *Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113.
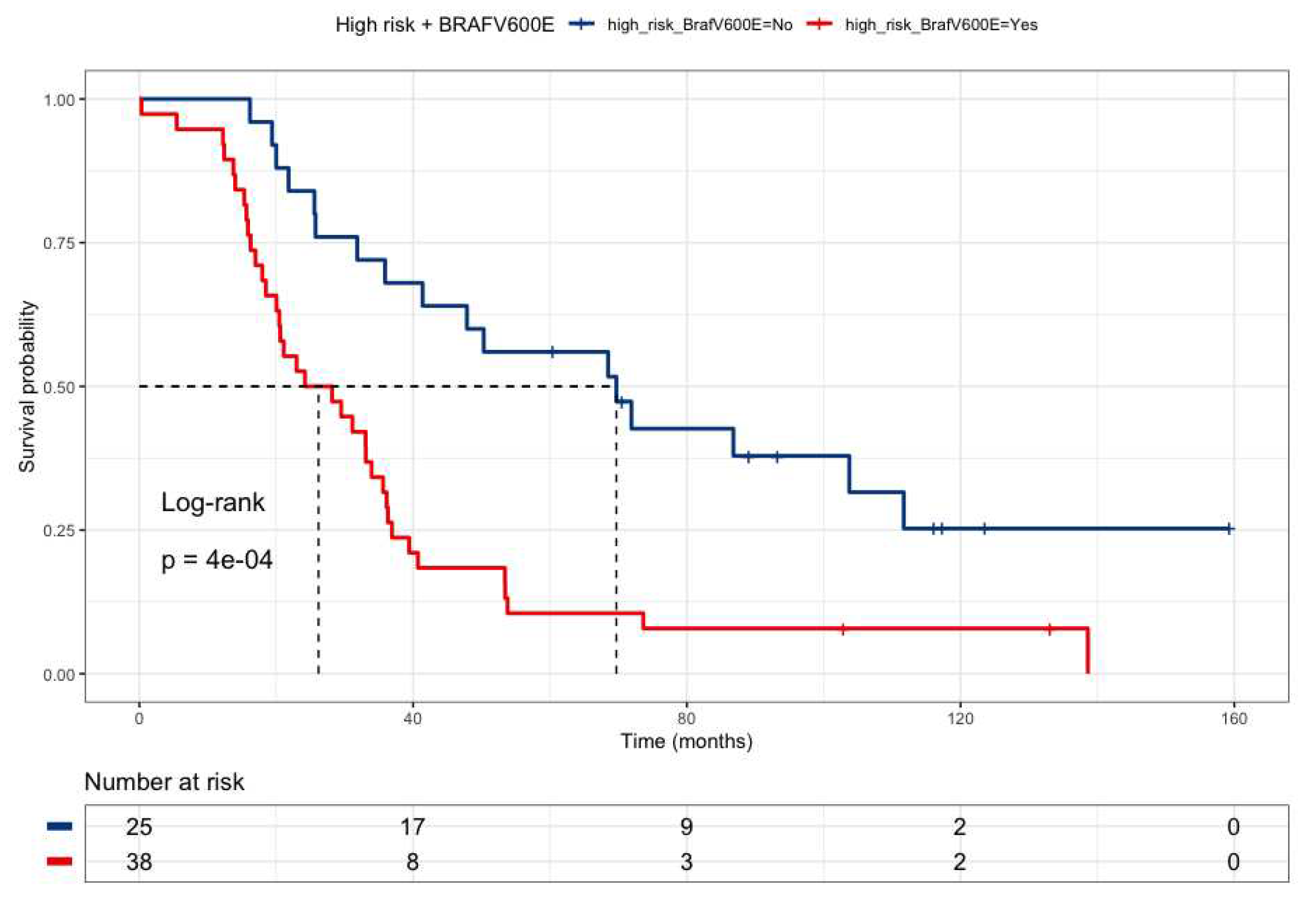
Figure 7.
Kaplan Meier curve of stage III colon cancer patients according to DPYD expression in TCGA cohort (DPD low = blue line, DPD normal = red line).
Figure 7.
Kaplan Meier curve of stage III colon cancer patients according to DPYD expression in TCGA cohort (DPD low = blue line, DPD normal = red line).
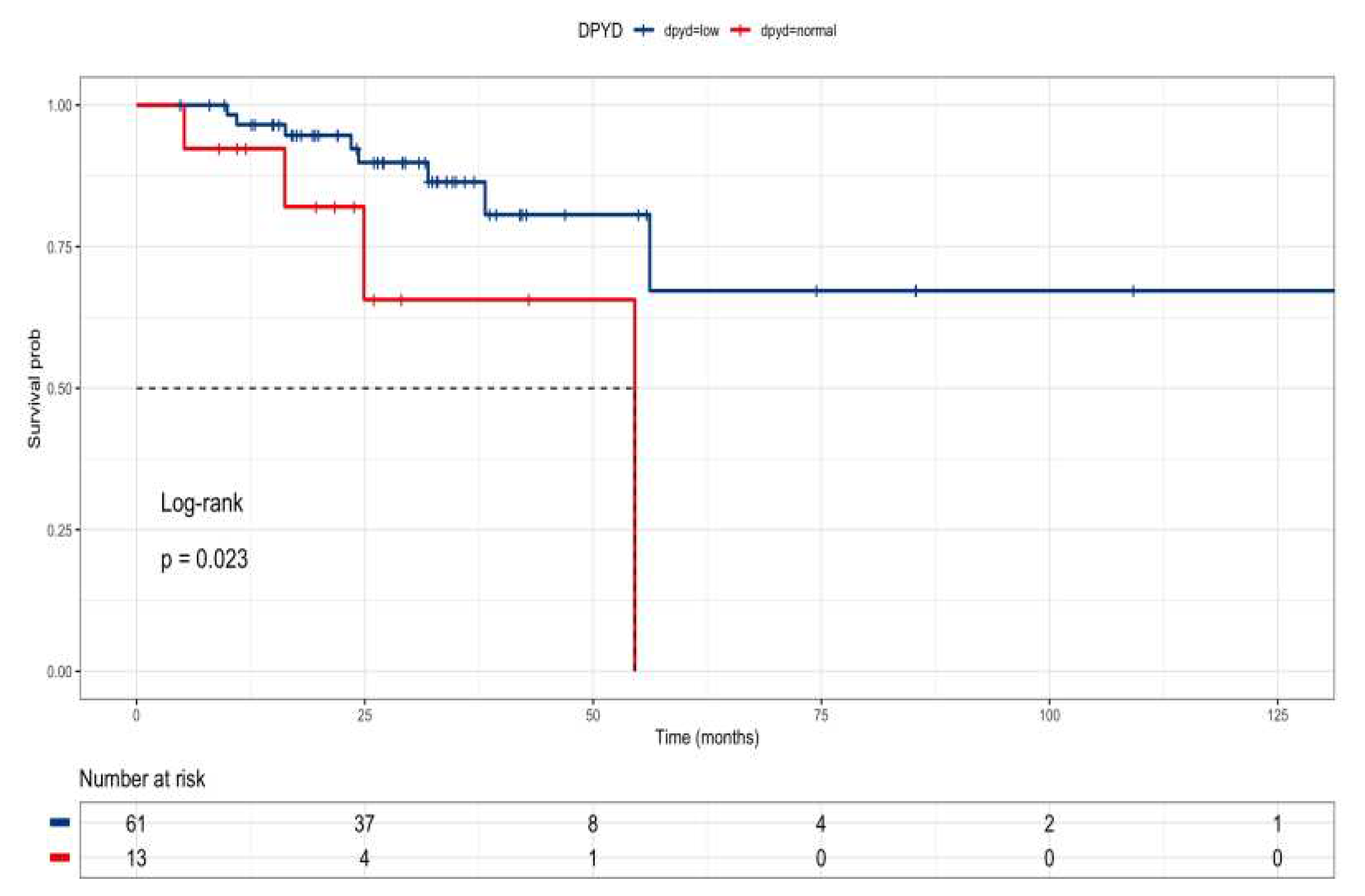
Figure 8.
Kaplan Meier curve of TCGA colon cancer patients according to TYMS, TK, TYMP and FOXM1 expression in TCGA cohort by clinical stage.
Figure 8.
Kaplan Meier curve of TCGA colon cancer patients according to TYMS, TK, TYMP and FOXM1 expression in TCGA cohort by clinical stage.
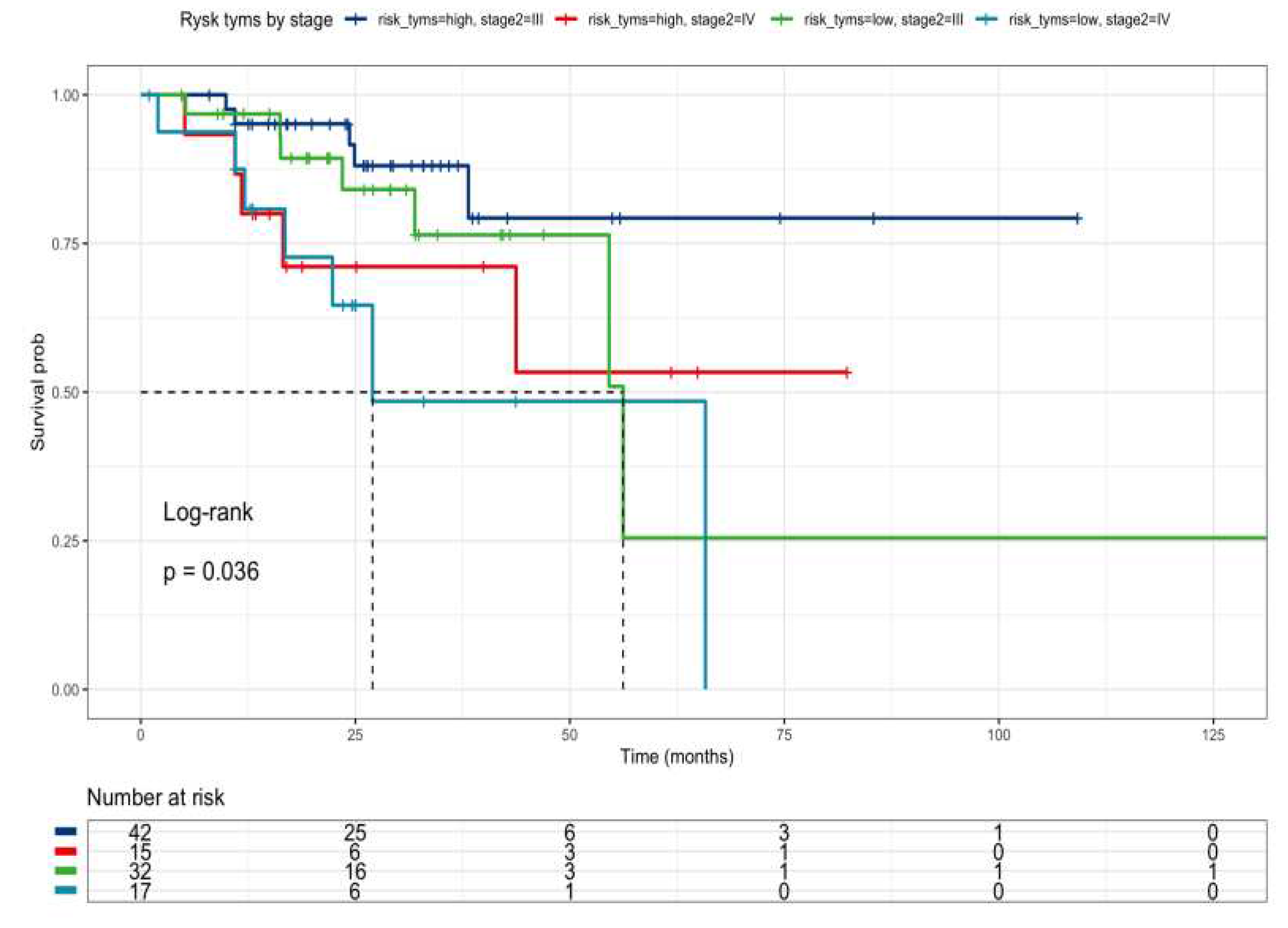
Figure 9.
Drug sensitivity analysis of COREAD (Colon and rectum adenocarcinoma) cell lines to 5-fluoruracil (GDSC2 dataset, Sanger Screening Site, n=968). The data was obtained from “The Genomics of Drug Sensitivity” (https://www.cancerrxgene.org/).
Figure 9.
Drug sensitivity analysis of COREAD (Colon and rectum adenocarcinoma) cell lines to 5-fluoruracil (GDSC2 dataset, Sanger Screening Site, n=968). The data was obtained from “The Genomics of Drug Sensitivity” (https://www.cancerrxgene.org/).
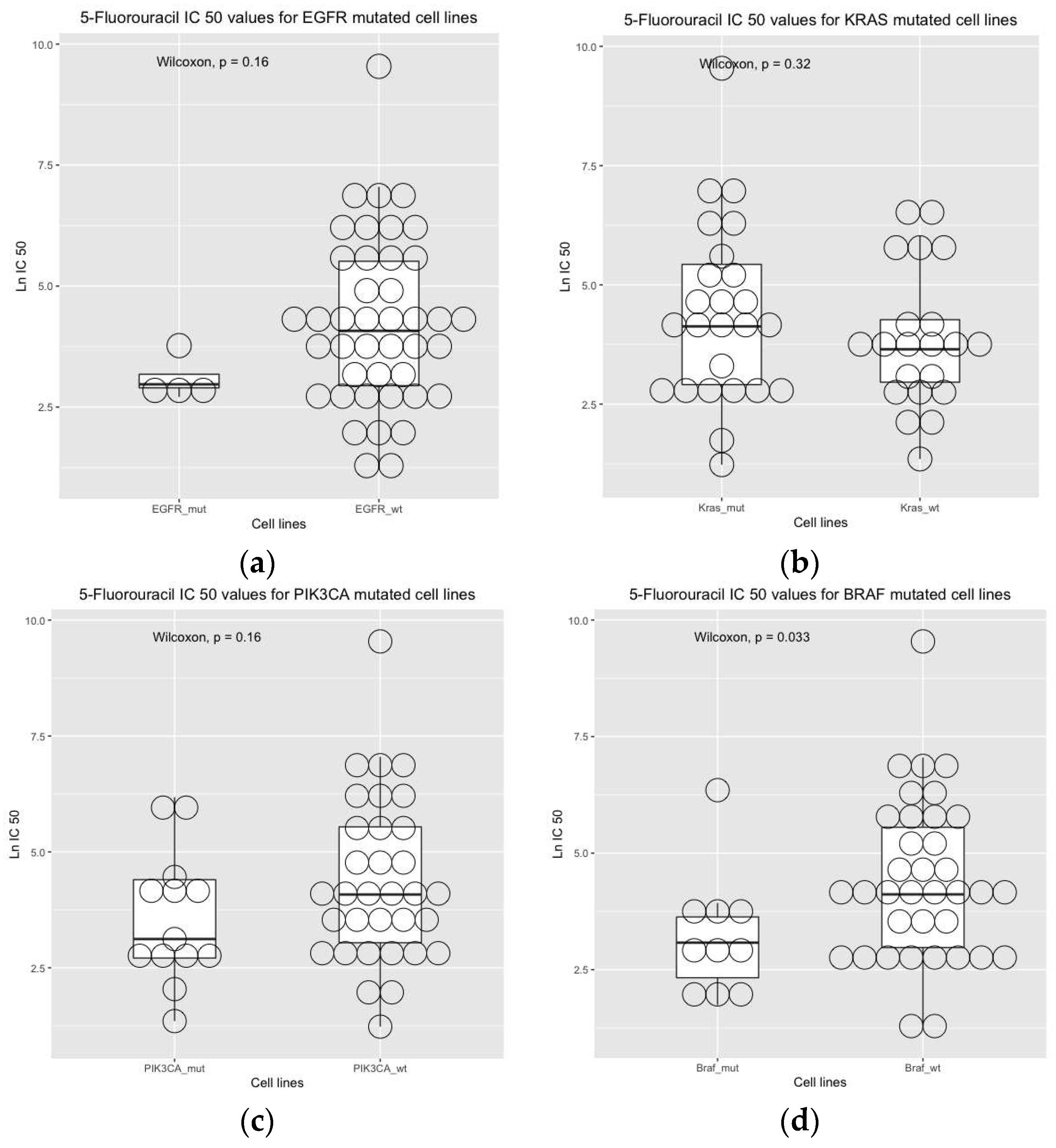

Table 1.
General characteristics of patients.
| Gender | |
| Female | 32 (50.8%) |
| Male | 31 (49.2%) |
| Age | |
| Mean (SD) | 63.3 (12.4) |
| Median [Min, Max] | 66.4 [30.4, 81.8] |
| Histology | |
| Adenocarcinoma | 57 (90.5%) |
| Adenocarcinoma Mucinous | 6 (9.5%) |
| Localization | |
| Left | 46 (73.0%) |
| Right | 15 (17.5%) |
| N.D. | 2 (3.2%) |
| Metastasectomy | |
| Yes | 27 (42.9%) |
| No | 21 (33.3%) |
| N.D. | 15 (23.8%) |
| Radiotherapy | |
| Yes | 11 (17.5%) |
| No | 52 (82.5%) |
| Monoclonal antibodies therapy | |
| Yes | 14 (22.2%) |
| No | 49 (77.8%) |
| Second line of treatment (FOLFOX or FOLFIRI) | |
| Yes | 37 (56.8%) |
| No | 26 (41.3%) |
| N.D. = No data | |
Table 2.
Genotype frequencies of patients.
| TYMS 3’UTR 6bp ins-del (rs151264360) | ||
| DEL/DEL | 31 (49.2%) | |
| INS/DEL | 32 (50.8%) | |
| GSTP1 c.313A>G (rs1695) | ||
| A/A | 20 (31.7%) | |
| G/A | 28 (44.4%) | |
| G/G | 15 (23.8%) | |
| DPYD c.1905+1 G>A (DPYD*2) (rs3918290) | ||
| G/G | 63 (100%) | |
| G/A | 0 (0%) | |
| A/A | 0 (0%) | |
| DPYD c.2846A>T (rs67376798) | ||
| A/A | 1 (1.6%) | |
| T/A | 1 (1.6%) | |
| T/T | 61 (96.8%) | |
| DPYD c.1679T>G (DPYD*13) (rs55886062) | ||
| T/T | 63 (100%) | |
| T/G | 0 (0%) | |
| G/G | 0 (0%) | |
| DPYD c.85T>C (DPYD*9) (rs1801265) | ||
| T/T | 37 (58.7%) | |
| C/T | 19 (30.2%) | |
| C/C | 6 (9.5%) | |
| N.D. | 1 (1.6%) | |
| ABCB1 c.3435C>T (rs1045642) | ||
| T/T | 9 (14.3%) | |
| C/T | 31 (49.2%) | |
| C/C | 21 (33.3%) | |
| N.D. | 2 (3.2%) | |
| ABCB1 c.1236 T>C (rs1128503) | ||
| T/T | 6 (9.5%) | |
| C/T | 41 (65.1%) | |
| C/C | 15 (23.8%) | |
| N.D | 1 (1.6%) | |
| ABCC2 c.-24C>T (rs717620) | ||
| C/C | 46 (73.0%) | |
| C/T | 11 (17.5%) | |
| T/T | 2 (3.2%) | |
| N.D. | 4 (6.3%) | |
| MTHFR c.1409A>C (rs1801131) | ||
| A/A | 33 (52.4%) | |
| A/C | 21 (33.3%) | |
| C/C | 8 (12.7%) | |
| N.D. | 1 (1.6%) | |
| ERCC2 c.2251A>C (rs13181) | ||
| A/A | 2 (3.2%) | |
| A/C | 12 (19.0%) | |
| C/C | 25 (39.7%) | |
| N.D. | 24 (38.1%) | |
| N.D. = No data (due to sample shortage) | ||
Table 3.
Molecular somatic profiles of patients.
| BRAF V600E | |
| Mutated | 7 (11.1%) |
| Wild-type | 58 (88.9%) |
| KRAS mutations* | |
| Mutated | 22 (34.9%) |
| Wild-type | 41 (65.1%) |
| NRAS mutations** | |
| Mutated | 7 (11.1%) |
| Wild-type | 56 (88.9%) |
| PI3KCA mutations*** | |
| Mutated | 7 (11.1%) |
| Wild-type | 56 (88.9%) |
| AKT1 E17K | |
| Mutated | 2 (3.2%) |
| Wild-type | 61 (96.8%) |
|
*KRAS 1213, KRAS117, KRAS61, KRAS146 and KRAS59 (Entrogen Colorectal Cancer Mutation Detection Panel) ** NRAS1213, NRAS117, NRAS61, NRAS146 and NRAS59 (Entrogen Colorectal Cancer Mutation Detection Panel) *** PI3KCA542545 and PI3KCA1047 (Entrogen Colorectal Cancer Mutation Detection Panel) | |
Table 4.
Univariate analysis (p-value < 0.1).
| HR | CI | p-value* | |
| Liver metastases | 3.51 | 1.52-8.07 | 0.003 |
| Colectomy | 0.48 | 0.214-1.08 | 0.079 |
| GSTP1 rs1695 | 0.484 | 0.234-1.00 | 0.05 |
| DPYD rs1801265 | 1.819 | 1.03-3.19 | 0.0377 |
| ABCB1 rs1045642 | 1.782 | 1.00-3.16 | 0.0483 |
| MTHFR rs180113 | 2.295 | 1.05-4.97 | 0.0352 |
| TYMS rs151264360 | 2.169 | 1.21-3.86 | 0.0087 |
| Mutated PI3KCA | 0.271 | 0.084-0.876 | 0.0292 |
| Wild-type BRAF V600E | 0.28 | 0.087-0.909 | 0.034 |
| High risk profile** | 2.06 | 1.13-3.74 | 0.018 |
| High risk profile together BRAF wild-type patients** | 2.80 | 1.55-5.06 | <0.005 |
|
* P<0.05 statistically significant (in bold) **Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113. HR = Hazzard Ratio; CI = 95% Confidence Interval | |||
Table 5.
Multivariate analysis (final model).
| HR | CI | p-value* | p-value* | |
| Liver metastases presence | 3.69 | 1.49-9.09 | 0.004 | |
| DPYD rs1801265 (G/G patients) | 1.88 | 0.99-3.54 | 0.052 | |
| ABCB1 rs1045642 (G/G patients) | 2.62 | 1.37-4.99 | 0.003 | |
| MTHFR rs180113 (C/C patients) | 2.63 | 1.13-6.15 | 0.004 | |
|
*p< 0.05 statistically significant (in bold) **Concordance of the model (C) = 0.692 HR = Hazzard Ratio; CI = Confidence Interval | ||||
Table 6.
Multivariate analysis (association between high risk profile and mutational status).
| High-risk profile and BRAF V600E mutation | HR | CI | p-value* |
| High-risk presence | 2.18 | 1.15-4.11 | 0.017 |
| Liver metastases presence | 3.34 | 1.39-8.05 | 0.006 |
| BRAF V600E mutated | 0.41 | 0.12-1.39 | 0.153 |
| High-risk profile and KRAS mutation | HR | CI | p-value |
| High-risk presence | 2.28 | 1.20-4.33 | 0.012 |
| Liver metastases presence | 4.71 | 1.91-11.6 | <0.005 |
| KRAS mutated | 0.59 | 0.31-1.11 | 0.105 |
| High-risk profile and PI3KCA mutation | HR | CI | p-value |
| High-risk presence | 2.43 | 1.26-4.66 | 0.007 |
| Liver metastases presence | 4.08 | 1.68-9.86 | 0.002 |
| PI3KCA mutated | 0.22 | 0.05-0.95 | 0.042 |
|
*p<0.05 statistically significant (in bold) **Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113. HR = Hazzard Ratio; CI = Confidence Interval | |||
Table 7.
Clinical response according to high-risk together BRAF wild-type patients versus all patients.
Table 7.
Clinical response according to high-risk together BRAF wild-type patients versus all patients.
| Group | HR | CI | p-value* |
| High-risk together BRAF wild-type patients | 2.71 | 1.46-5.01 | 0.001 |
| Liver metastases | 3.55 | 1.52-8.29 | 0.003 |
|
* P value< 0.05 statistically significant **Risk genotype profile includes DPYD rs1801265 + ABCB1 rs1045642 + MTHFR rs180113. HR = Hazzard Ratio; CI = Confidence Interval | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



