Submitted:
14 July 2023
Posted:
17 July 2023
You are already at the latest version
Abstract
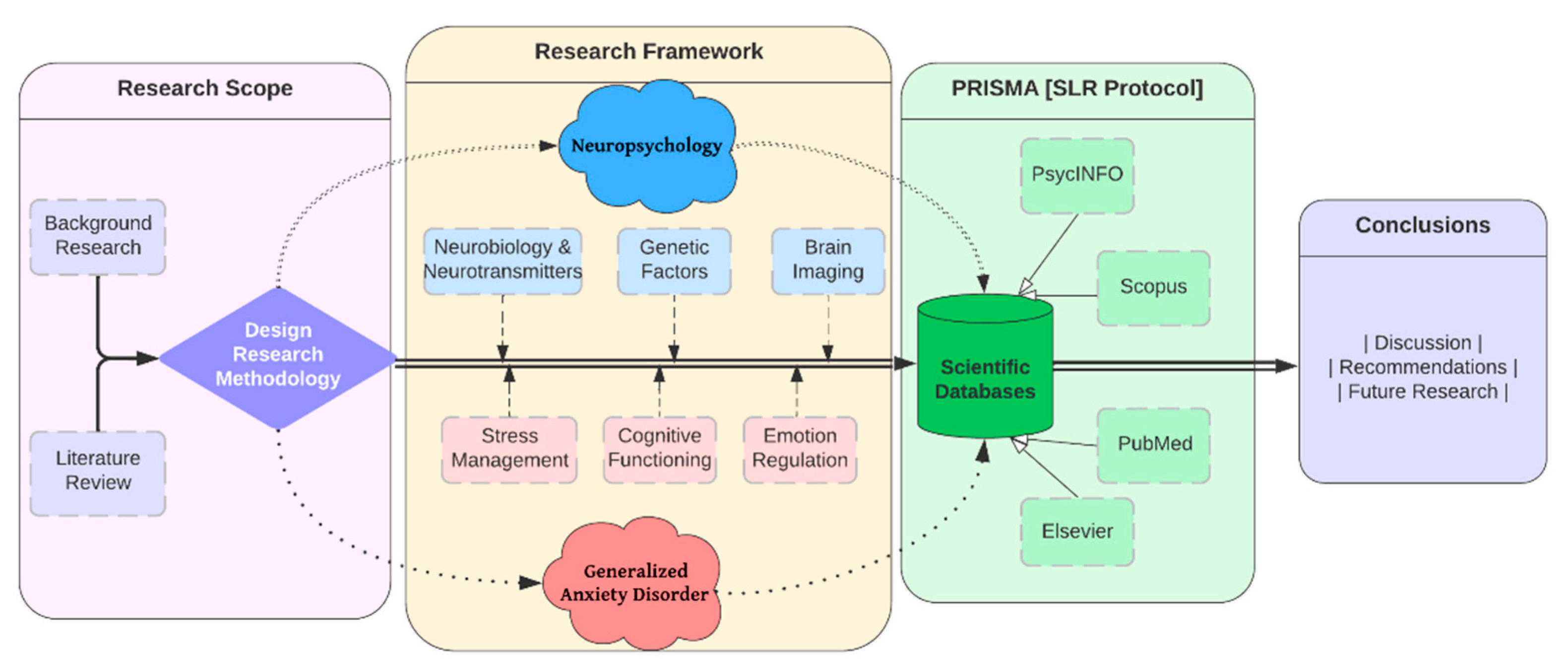
The purpose of this systematic review is to examine the various articles published in the field of neuropsychology of anxiety research in terms of publication type and volume, methodology, and subject matter. The significance of this topic derives from the clinical and functional consequences of cognitive symptoms. Generalized anxiety disorder refers to the cluster of clinical symptoms characterized by predominant anxious anticipation and difficulty controlling worry. In order for the review to be systematic and reproducible, a search of the PsycINFO, Scopus, PubMed, Elsevier databases and an analysis using the PRISMA method are suggested. After analyzing the research data, empirical studies evaluating the clinical neuropsychology of generalized anxiety disorder are discussed.
Keywords:
Neuropsychology
; Anxiety Disorders
; Clinical Setting
; Generalized Disorder
; Prisma
; Systematic Review
1. Introduction
In the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), generalized anxiety disorder is categorized as an anxiety disorder. Its primary clinical manifestations are anxious anticipation and difficulty controlling anxiety. One of the possible associated symptoms is inability to cope with situations or a loss of memory.
In clinical practice, patients with generalized anxiety disorder manifest cognitive complaints and a lack of confidence in their cognitive performance, which frequently impairs their ability to function at work. Similarly, recent research evaluating a potential metacognitive dysfunction in a large sample of patients with anxiety disorders reveals that they have decreased confidence in their cognitive functions and increased self-awareness regarding them [1].
In the scientific literature, cognitive symptoms of psychiatric disorders such as schizophrenia, depression, and bipolar disorder are defined in detail, and specific neuropsychological tests have been developed for their evaluation [2]. However, cognitive symptoms of anxiety disorders are considerably less well-defined. In the literature, neuropsychological findings for these disorders are less consistent. The study of cognitive symptoms in patients with generalized anxiety disorder is of interest because they have a substantial effect on the subject's functional adaptation. Consequently, the purpose of this review is to validate the primary literature from the last ten years that addresses neuropsychological functioning [3] in the various cognitive domains in individuals with generalized anxiety disorder [4].
The following are the fixed objectives that emerge from the general and that will direct this review:
[RQ1] The estimation of the number and nature of publications in the field of clinical neuropsychology of anxiety.
[RQ2] An examination of the methodology utilized in the unearthed investigations.
[RQ3] Determining the cognitive manifestations of generalized anxiety disorder.
2. Literature Review
Generalized Anxiety Disorder (GAD) is a prevalent chronic disorder characterized by long-lasting, non-specific anxiety. Neuropsychology of GAD typically investigates the interactions between neurological function and behavior in a clinical setting. It can provide valuable insight into how the brain contributes to the symptoms and experience of GAD. GAD is believed to be caused by dysregulation in the body's fear-response systems, which are primarily located in the amygdala and hippocampus. Changes in the function of these regions can result in heightened fear and anxiety responses. Moreover, neurotransmitter imbalances such as serotonin, dopamine, and GABA (gamma-Aminobutyric acid) can contribute to GAD. GABA, the principal inhibitory neurotransmitter in the brain, reduces neuronal excitability and promotes calm and relaxation. People with GAD frequently have decreased GABA levels, increasing anxiety and fear responses [5].
Cognitive Function: Individuals with GAD tend to exhibit heightened sensitivity to hazards and negative stimuli, frequently exaggerating the probability and severity of adverse outcomes. This results in a pattern of anxiety, ruminating, and avoidance behaviors. Neuropsychological evaluations frequently disclose attentional biases toward threatening stimuli, difficulties with cognitive flexibility, and impaired attention and memory functioning, particularly under stressful or threatening conditions [2].
Brain Imaging: Brain imaging investigations using fMRI (functional Magnetic Resonance Imaging) and PET (Positron Emission Tomography) have uncovered structural and functional abnormalities in GAD patients. For instance, increased activity has been observed in the amygdala and insula, which are involved in processing emotions and interpreting physical sensations. In addition, people with GAD have decreased connectivity between the prefrontal cortex and amygdala, which is believed to help regulate emotional responses [6].
Genetic Factors: Although not a direct focus of neuropsychology, it is essential to note that genetic factors play an important role in GAD, with estimates of heritability ranging from 30% to 50%.
Understanding the neuropsychological basis of GAD can inform and direct treatment in a clinical setting. For instance, cognitive-behavioral therapies (CBT) can assist individuals with GAD in challenging and altering maladaptive thought patterns and developing more adaptive coping strategies. In addition, medications that target the neurotransmitters implicated in GAD, such as selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), and benzodiazepines, can effectively reduce symptoms. Emerging evidence suggests that neuromodulation techniques such as transcranial magnetic stimulation (TMS) may also be advantageous for generalized anxiety disorder [7].
Individuals with Generalized Anxiety Disorder (GAD) must effectively manage their tension. Chronic stress can exacerbate symptoms and precipitate intense bouts of concern and anxiety. Here are some tension management strategies for GAD:
Cognitive Behavioral Therapy: CBT is a form of therapy that teaches individuals how their beliefs and actions affect their emotions and well-being. It teaches individuals to recognize, challenge, and alter stressful thought and behavior patterns. CBT is among the most effective treatment methods for GAD.
Mindfulness and Relaxation Techniques: Mindfulness, meditation, yoga, and deep-breathing exercises can help individuals become more aware of their body and stress response, as well as facilitate relaxation. By focusing on the present, individuals can reduce their propensity to fret about the future or ruminate on the past, both of which are typical GAD symptoms [8].
Regular Physical Activity: Regular physical activity has been shown to reduce anxiety and boost mood. Physical activity increases the production of endorphins, the body's natural mood enhancers, and can serve as a beneficial diversion [9].
A well-balanced diet can substantially affect an individual's disposition and energy level. Caffeine and alcohol, which can provoke or exacerbate anxiety, should be consumed in moderation, and adequate essential nutrients should be consumed to promote overall health. Poor sleep hygiene can aggravate anxiety and tension. Good sleep practices, such as establishing a regular sleep schedule, creating a restful environment, and avoiding stimuli (such as screens or caffeine) close to bedtime, can improve sleep quality.
Medication: If lifestyle modifications and therapy are insufficient, medication may be considered. Antidepressants, such as SSRIs and SNRIs, and anxiolytics, such as benzodiazepines, can aid in symptom management. However, medication should always be taken under the supervision of a medical professional due to the possibility of adverse effects and dependence [10].
Assisting Networks: Maintaining connections with supportive and empathetic friends, family members, or support organizations can reduce feelings of stress and anxiety.
Stressors Should Be Avoided Whenever Possible: If certain situations or individuals cause significant tension and can be avoided in a healthy manner, it may be best to do so.
Time Management: Feeling overburdened with duties and responsibilities is one of the leading causes of stress. Effective time management can foster a sense of control and alleviate tension.
A mental health professional will collaborate with the individual to establish a comprehensive treatment plan that takes into account the individual's specific symptoms, stressors, and lifestyle in a clinical setting. The objective is to discover a balanced, long-term strategy for stress management.
Emotion regulation is the effective management and response to emotional experiences. It is necessary for the development and maintenance of mental health and for the rational decision-making [11]. Difficulties in emotion regulation can exacerbate symptoms and contribute to distress in individuals with Generalized Anxiety Disorder (GAD). Consequently, increasing emotion regulation skills is frequently a primary treatment objective for GAD. In the context of GAD, the following emotion regulation strategies are frequently employed:
Cognitive Behavioral Therapy: CBT is among the most effective treatment methods for GAD. It entails recognizing and altering unproductive thought patterns that contribute to emotional distress. For example, catastrophizing, or consistently imagining the worst possible consequence in any given situation, is a common cognitive distortion in GAD. Individuals can reduce anxiety and enhance their ability to manage negative emotions by challenging these thoughts.
Mindfulness-Based Interventions: Mindfulness, a type of meditation in which you focus on being intensely aware of what you are sensing and experiencing in the present moment, without interpretation or judgment, can assist people in observing and comprehending their emotions without acting impulsively. Individuals can better regulate their emotional responses by increasing their emotional awareness and learning to tolerate distress without acting upon it.
DBT is a form of cognitive behavioral therapy (CBT) that emphasizes the development of emotion regulation skills. This approach involves learning strategies for recognizing and naming emotions, decreasing susceptibility to emotional dysregulation, increasing positive emotional experiences, managing negative emotions without making matters worse, and enhancing resilience [12].
ACT: Acceptance and Commitment Therapy ACT focuses on assisting individuals to embrace their emotions as they are, as opposed to attempting to alter or avoid them. The objective is to cultivate psychological flexibility – the capacity to maintain contact with the present moment and act in accordance with one's values, even when experiencing challenging emotions [13].
Exposure Treatment: In this therapy, individuals are progressively and repeatedly exposed to their anxiety-provoking thoughts, situations, or objects. The objective is to diminish the anxiety response over time, resulting in improved emotional control.
Relaxation Techniques: Breathing deeply, progressively relaxing your muscles, and visualizing can help reduce the physiological arousal associated with anxiety, promoting improved emotional regulation.
When necessary, pharmacological treatments such as SSRIs, SNRIs, and benzodiazepines can be considered an adjunct to psychotherapy for the management of GAD symptoms. However, these should always be administered under the supervision of a medical expert. In clinical settings, a combination of these techniques, tailored to the individual's unique requirements and challenges, is frequently employed. The ultimate objective is to enable those with GAD to comprehend, experience, and navigate their emotions in a healthier, more adaptive manner [14].
3. Materials and Methods
This section will indicate the review protocol used to carry out this systematic review, detailing all sources of information, years covered, eligibility criteria and other guidelines used. To carry out this systematic review, only the articles published in the PsycINFO database have been used, using the procedure of PRISMA system reviews. A systematic review of the literature of the last ten years has been carried out, which allows us to appreciate the evolution in this field of research until today. Therefore, the inclusion criteria used have been, articles only in English published from 2013 to the present day, 2023 on the neuropsychology of anxiety disorder. Articles that include a study of anxiety in children under 18 years of age have been excluded, since I have focused my systematic review on that. Likewise, articles that investigate this in only one of the two sexes have been omitted. The critical words in the scan have been "anxiety disorders", "anxiety" and "generalized anxiety disorder" joined by OR to obtain different documents that contain one of those terms.
Figure 1.
Flowchart of Research Framework.
4. Results
In this section includes the results acquired in the systematic review. A systematic review is an overview of primary research on a specific research question that systematically identifies, selects, evaluates, and synthesizes all relevant high-quality research evidence. A systematic review employs transparent methods to reduce bias and generate more reliable findings for decision-making purposes.
PRISMA, or Preferred Reporting Items for Systematic Reviews and Meta-Analyses, is a minimum standard for reporting in systematic reviews and meta-analyses that is supported by empirical evidence. It seeks to assist authors in reporting systematic reviews and meta-analyses more effectively. Here are the essential stages for conducting a systematic review in accordance with PRISMA standards.
Articles are organized according to the following criteria:
4.1. Information sources and search strategies
Regarding Figure 2, we begin with 311 637 articles before applying any restriction. To begin the selection of articles, the following limitations were applied: articles published in the last ten years (2013-2023), only English-language articles were selected, the age of the investigations had to be at least 18 years (adulthood) to avoid cognitive changes associated with the neurodevelopmental process, and a subject limiter was applied. In the main title, "anxiety disorders" or "anxiety" should appear. After applying the limiters depicted in Figure 2, 117 articles are obtained. After discarding the articles with little overlap for the present systematic review, we were left with 33 articles, of which 18 were chosen for full-text evaluation. After evaluating the full-text articles, references were eliminated, and 13 full-text articles that met all inclusion criteria were recovered.
4.2. Empirical studies
The studies addressing the empirical studies can be seen in Table 1, which contains the number of subjects included in each article, the conclusions reached, and the number of adult patients with a clinical diagnosis of generalized anxiety disorder who were evaluated using a neuropsychological test of any cognitive domain and compared with a healthy control group.
According to research [1], anxiety disorders such as GAD are associated with significant levels of fatigue. Anxiety can cause both mental and physical exhaustion, and persistent fatigue may result from chronic anxiety. Also well-established is the link between anxiety and subjective memory complaints. Anxious individuals may perceive their memory to be impaired, despite the absence of objective memory impairments. This is likely due to the fact that anxiety can impair attention and focus, which are essential for encoding and retrieving memories. Anxiety can consume cognitive resources, leaving less capacity for other cognitive tasks such as memory.
Despite the fact that the severity of symptoms such as depression, insomnia, and pain may not always correlate directly with the level of anxiety, they are frequently co-occurring with anxiety disorders. It is also important to note that these relationships can be complex and influenced in both directions. For example, while anxiety can cause sleep difficulties, sleep difficulties can also exacerbate anxiety. In terms of clinical implications, these results highlight the need for a comprehensive assessment and treatment strategy for individuals with anxiety disorders. Not only should the anxiety itself be treated (via cognitive-behavioral therapy or appropriate medication, for example), but also associated symptoms such as fatigue and subjective memory complaints. Occasionally, strategies to improve sleep, manage pain, or deal with depressive symptoms may also be advantageous.
Individuals with anxiety disorders [15], such as Generalized Anxiety Disorder (GAD), frequently experience cognitive and emotional difficulties. Here is additional information on each of your mentioned points:
High levels of anxiety are associated with slower reaction times. This may be due to the fact that anxious people are frequently preoccupied with worry or fear, which can distract them from the task at hand and slow their responses.
Inability to Recruit Cognitive Resources: Anxiety can impair the ability to recruit and utilize cognitive resources, especially those associated with attention, memory, and executive functions. This can make it challenging for anxious individuals to concentrate, remember information, or perform complex cognitive tasks.
Intrusive Ideas and Weak Control: Anxiety disorders frequently exhibit intrusive thoughts, or unwanted thoughts that appear involuntarily. These thoughts are difficult to control, resulting in increased anxiety and fear.
Emotion Regulation Difficulties: Individuals with anxiety frequently struggle to regulate their emotions. This suggests that they may struggle to manage or control their emotional responses to various situations, resulting in increased anxiety and distress.
Attempts to Confront Fearful Stimuli: Exposure to fearful or anxiety-provoking stimuli frequently elicits a powerful anxiety response. Anxious individuals may require considerable effort to confront these stimuli and manage their fear response.
Continuous Threat-Related Thoughts: Anxiety disorders are frequently accompanied by continuous threat-related thoughts. This can cause them to become distracted from their work and exacerbate their anxiety symptoms.
These factors can significantly impair the daily functioning and quality of life of an individual. The good news is that there are effective treatments for anxiety disorders. These typically involve cognitive-behavioral techniques, which assist individuals in challenging and altering maladaptive thought patterns, developing better emotion regulation skills, and gradually confronting and reducing their fears. In some instances, medication may be advantageous. Consult a mental health professional for a comprehensive evaluation and appropriate treatment if you or someone you know is experiencing these symptoms.
The dorsal part of the dorsolateral prefrontal cortex (dIPFC) plays a crucial role in cognitive control functions such as working memory (WM), attention regulation, and decision-making [16]. Low levels of cognitive control and WM are frequently associated with high levels of trait anxiety, which is the stable tendency to attend to, experience, and report negative emotions such as fears, worries, and anxiety in a variety of situations. In that study [16] researchers manipulated perceived threat in order to examine its effect on cognitive control in people with high trait anxiety. The reported findings of performance deficits under threat conditions in anxious individuals suggest that these individuals may struggle to recruit the necessary cognitive resources when they perceive danger or threat. This may contribute to difficulties with attention regulation and working memory, thereby exacerbating the common cycle of anxiety disorders.
If cognitive control and WM deficits are indeed stable traits in anxious individuals, this could have several implications. These deficits may predict future symptom severity or treatment outcomes, as you mentioned. Those with greater cognitive control or WM deficits at baseline, for instance, may experience worsening symptoms over time or be less responsive to certain treatments. This can inform therapeutic strategies by highlighting the need to enhance cognitive control and working memory (WM) functions in individuals with high trait anxiety. Cognitive remediation therapy and cognitive training are therapeutic techniques. Understanding these deficiencies can also lead to the development of novel therapeutic interventions aimed at enhancing the cognitive control and WM functions of this population [27].
Despite the fact that these hypotheses are testable, additional research is required to confirm these associations and explore the complex relationship between cognitive control, working memory, trait anxiety, and perceived threat. It is also essential to keep in mind that anxiety disorders, like all mental health conditions, are complex and multifaceted, with a wide variety of contributing factors that must be considered in each individual case.
The dual-process psychotherapeutic model [17] suggests that Generalized Anxiety Disorder (GAD) treatment may involve two parallel processes:
Reducing Threat Reactivity: First, the cingulate cortex and amygdala, two brain regions that play a central role in responding to threatening stimuli, are inhibited in their reactivity. The cingulate cortex detects and monitors threats, while the amygdala initiates the fear response. These regions may be hyperactive or hypersensitive in individuals with GAD, resulting in an exaggerated fear response to non-threatening stimuli. Therapeutic interventions, such as cognitive-behavioral therapy, can aid in reducing this overreactivity, allowing individuals to respond more proportionally to actual threats [28].
Boosting Responses to Positive Stimuli: The second process involves boosting (potentiating) the insular response to positive emotional stimuli, such as smiling faces. The insula is a region of the brain that processes emotions and physical sensations. Positive stimuli may be overlooked or under-reacted to in those with GAD, resulting in a negative bias in perception and memory. By enhancing the insular response to positive stimuli, therapeutic interventions can assist in counteracting this bias and enhancing mood and well-being. By combining these two processes, therapy can help individuals with GAD rebalance their emotional processing by decreasing their overreaction to threats and increasing their response to positive stimuli. This can result in a decrease in symptoms and enhancements to overall functioning and quality of life [29].
These findings demonstrate the value of neuropsychotherapy, in which knowledge of brain function can inform therapeutic strategies [30]. However, it is essential to recognize that these are complex processes that are influenced by a variety of variables. This model requires further refinement and investigation to fully comprehend its implications. Different anxiety-related disorders [21] may exhibit distinct patterns of social cognitive deficits, according to the study's findings. Social cognition refers to the cognitive processes underlying social interactions, such as understanding the perspectives and emotions of others, attributing causes to social events, and predicting and interpreting social behavior. In this situation:
PTSD (Post-Traumatic Stress Disorder): Mentalization (also known as Theory of Mind) is the capacity to understand and infer the mental states of others, whereas emotion recognition is the capacity to correctly identify and interpret the emotional expressions of others. The findings suggest that individuals with PTSD may demonstrate deficits in mentalization (also known as Theory of Mind) and emotion recognition. These deficits may be attributable to the traumatic experiences that characterize PTSD, which can lead to alterations in social cognition-related brain regions, such as the amygdala, prefrontal cortex, and anterior cingulate cortex [31].
Other Anxiety Disorders: Individuals with alternative anxiety disorders may be more susceptible to attributional biases. This refers to the propensity to interpret or attribute erroneously the causes of social events. For instance, they may excessively attribute negative outcomes to themselves (self-blame bias) or to stable and global causes (catastrophic thinking). These biases can exacerbate anxiety and contribute to the disorder's maintenance.
Understanding these distinct patterns of social cognitive deficits can facilitate the creation of targeted therapeutic interventions. For instance, therapies for PTSD may focus on enhancing emotion recognition and mentalization skills, whereas therapies for other anxiety disorders may target attributional biases. Cognitive-behavioral therapies are frequently effective in this regard, as they can assist individuals in recognizing and challenging maladaptive thought patterns and in developing more adaptive cognitive strategies.
As with all psychological research, it is probable that these findings represent tendencies rather than hard and fast rules. Individual experiences of PTSD and other anxiety disorders can vary considerably, and each person's social cognitive abilities will be influenced by a variety of factors, such as their personal history, comorbid conditions, and cognitive strengths and weaknesses. To continue exploring these patterns and their implications for treatment, additional research is required.
Also, according to research [25] demonstrates a complex relationship between anxiety, cognitive functioning (primarily executive functions and memory), worry, and the effectiveness of specific treatments:
Executive Functions: Neurocognitive assessment as examined by neuropsychological tests as the Wisconsin Card Sorting Test (WCST) which is a test of set-shifting, can demonstrate adaptability in the face of shifting reinforcement schedules. This aspect of executive function involves cognitive processes of a higher order that are primarily governed by the frontal lobes. Research indicates that elevated anxiety levels, particularly in younger individuals, can result in diminished WCST performance, indicating potential deficits in executive function [32].
Memory: Anxiety can impair memory functions, specifically immediate recall. Anxiety can impair the encoding, storage, and retrieval of information, which significantly impairs the ability to recall recently learned material.
Chronic worry, a defining feature of Generalized Anxiety Disorder, can consume significant cognitive resources, leaving less capacity for other cognitive processes. The linguistic processing associated with ruminative worry—constantly considering and verbalizing potential threats or negative outcomes—can interfere with tasks requiring sustained attention, working memory, and other executive functions [33].
Antidepressant medications, which are commonly used to treat anxiety disorders, can have a variety of cognitive effects. Despite the fact that they frequently alleviate anxiety symptoms, some research indicates that they may impair performance on tasks requiring sustained attention, or the capacity to maintain consistent behavioral responses during continuous and repetitive activity. This may manifest as a diminished capacity to maintain vigilance for extended periods.
These points illustrate the multifaceted effects of anxiety on cognitive processes as well as the complex ways in which treatments may influence these relationships. However, these effects can vary considerably from person to person, and many people with anxiety disorders or who are taking antidepressants are able to perform well on cognitive tasks. In addition, it is crucial to keep in mind that cognitive-behavioral therapies can assist individuals in managing anxiety and enhancing cognitive control, thereby potentially compensating for some of these cognitive difficulties [34].
Individuals with Generalized Anxiety Disorder (GAD) may have deficits in reinforcement-based decision-making, which involves making choices based on an understanding of potential rewards (positive reinforcement) and punishments (negative reinforcement), according to the findings of research [26]. This decision-making frequently involves complex cognitive processes, such as assessing the likelihood of outcomes, weighing the potential benefits and costs, and revising beliefs in light of new information. The prefrontal cortex and striatum, which are involved in reward processing, decision-making, and executive function, are typically involved in these tasks. Several factors may contribute to such decision-making impairments in the context of GAD:
Enhanced Concentration on Potential Dangers: Individuals with GAD exaggerate the probability and severity of potential threats. When making decisions, they may place disproportionate importance on potential negative outcomes, even if they are unlikely or relatively minor. This could lead to overly cautious decision-making or avoidance.
Chronic worry and ruminating can deplete cognitive resources, thereby limiting the capacity for other cognitive processes. This could hinder the intricate cognitive tasks required for decision-making.
Reduced Punishment Signal Sensitivity: A lower correlation between punishment and responses suggests that individuals with GAD may be less responsive to punishment signals when making decisions. They may need to modify their decisions in response to negative outcomes, which could result in repeated errors or suboptimal decisions.
Fear of Uncertainty: People with GAD frequently have a high intolerance for uncertainty, which hinders their ability to make decisions in ambiguous situations [35,36,37,38].
These results highlight the numerous ways in which anxiety can impact cognitive functioning and daily life. It is important to note, however, that these impairments are not inevitable: cognitive-behavioral therapy (CBT) can assist individuals in managing their anxiety, enhancing their tolerance for uncertainty, and developing more effective decision-making strategies [39]. Additional research can provide a nuanced understanding of these processes and aid in the development of more targeted interventions.
5. Discussion and Conclusions
Following an analysis of the publications in the results section, the review concludes with a discussion of the extracted results and their conclusion. The majority of analyzed studies conclude that patients with generalized anxiety disorder have impaired cognitive performance in the following functions: selective attention, working memory, cognitive inhibition, decision making (error prediction), and social cognition [40]. Emotional stimuli (primarily threatening or anxious) have an effect on performance in tasks requiring attention, working memory, and cognitive inhibition [41]. Subjects with generalized anxiety disorder have difficulty identifying and processing emotions, and their heightened sensitivity to harmful stimuli tends to be generalized. The conclusion of a meta-analysis evaluating the social cognition of individuals with anxiety disorders is that they frequently exhibit attributional biases [21]. The cognitive difficulties of subjects with generalized anxiety disorder are not limited to the difficulty of concentration, as the state of anticipation and the inability to control anxiety also interfere with the performance of certain cognitive tasks. This disorder is characterized by an abundance of negative thoughts, which can be attributed to hyperactivity in the corticothalamostriatal circuit of the dorsolateral prefrontal cortex.
When exposed to a working memory task, patients with obsessive-compulsive disorder exhibit alterations in frontoparietal function, which increase as the task's difficulty increases. During task performance, there is hyperactivity of the left lateral frontal cortex and left medial parietal cortex relative to controls, along with hyperconnectivity between the frontal lobes and amygdala. Similarly, hyperactivity and hyperconnectivity of limbic regions have been linked to decision-making difficulties in those with generalized anxiety disorder. After psychotherapeutic intervention, cognitive performance improves in patients with generalized anxiety disorder. Compared to the control group, subjects with generalized anxiety disorder are characterized by the presence of depressive symptoms [23].
As previously stated, only patients over the age of 28 have been included in this systematic review to avoid cognitive changes associated with the typical neurodevelopmental process of aging.
Generalized Anxiety Disorder (GAD) and neuropsychology intersect in a number of promising ways for future research, diagnosis, and treatment. Future research may result in a more in-depth comprehension of the neurobiological mechanisms underlying GAD. This may entail a more in-depth investigation of neural circuitry, neurotransmitter systems, and genetic factors. The development of brain imaging and genomics technologies can significantly facilitate these investigations. By understanding individual differences in the neurobiology of GAD, it is possible to develop personalized treatment approaches. For instance, specific pharmacological treatments could be tailored based on an individual's neurochemical profile, or cognitive-behavioral therapy (CBT) techniques could be modified based on an individual's cognitive functioning or brain activity patterns.
Early Identification and Intervention: If specific neuropsychological markers or symptoms of GAD can be identified, it may be possible to intervene earlier in at-risk individuals, potentially preventing the disorder's onset or lessening its severity. For instance, children or adolescents exhibiting particular brain activity patterns or cognitive biases could benefit from early intervention programs.
Neuromodulation Techniques: Treatments involving direct modification of brain activity, such as transcranial magnetic stimulation (TMS), deep brain stimulation (DBS), and neurofeedback, could be explored and refined further for the treatment of GAD. These treatments have shown promise, but additional research is necessary to determine their efficacy and safety [42].
Therapy with Virtual Reality (VR) and Augmented Reality (AR): Virtual reality (VR) and augmented reality (AR) can provide immersive environments for exposure therapy, mindfulness training, and other therapeutic methods. These tools may be especially useful for GAD patients who struggle to confront anxiety-inducing real-world situations [43].
Artificial Intelligence and Machine Learning: Complex datasets (including neuroimaging, genetic, and clinical data) could be analyzed using machine learning algorithms, potentially revealing new insights about GAD and improving prediction, diagnosis, and treatment.
Integration with Other Academic Subjects: The neuropsychology of GAD is isolated. Integrating neuropsychological perspectives with those of other disciplines, such as psychopharmacology, social psychology, and developmental psychology, could result in a more comprehensive understanding of GAD.
The potential future ramifications are expansive and intriguing. It is important to note, however, that advancements in these areas will necessitate careful ethical considerations, rigorous scientific testing, and a commitment to translating research findings into clinical practice for the benefit of individuals with GAD.
Author Contributions
Conceptualization, E.G. and P.O.; methodology, E.G. and P.O.; formal analysis, E.G. and P.O.; investigation, P.O.; resources, E.G. and P.O.; writing—original draft preparation, E.G. and P.O.; writing—review and editing, E.G.; visualization, E.G.; supervision, E.G.; project administration, E.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aasvik, J. K., Woodhouse, A., Jacobsen, H. B., Borchgrevink, P. C., Stiles, T. C., & Landrø, N. I. (2015). Subjective memory complaints among patients on sick leave are associated with symptoms of fatigue and anxiety. Frontiers in Psychology, 6. [CrossRef]
- Gkintoni, E., Pallis, E., Bitsios, P., Giakoumaki, S. (2017). “Neurocognitive performance, psychopathology and social functioning in individuals at high-genetic risk for schizophrenia and psychotic bipolar disorder”. International Journal of Affective Disorders 208, 512-520. [CrossRef]
- Timulak, L. (2017). Generalized anxiety disorder. Transforming Generalized Anxiety, 8–28. [CrossRef]
- Generalized Anxiety Disorder. (2022). Child and Adolescent Psychopathology for School Psychology. [CrossRef]
- Del Giudice, M. (2018). Generalized Anxiety Disorder. Evolutionary Psychopathology, 319–322. [CrossRef]
- De la Peña-Arteaga, V., Fernández-Rodríguez, M., Silva Moreira, P., Abreu, T., Portugal-Nunes, C., Soriano-Mas, C., Picó-Pérez, M., Sousa, N., Ferreira, S., & Morgado, P. (2022). An fMRI study of cognitive regulation of reward processing in generalized anxiety disorder (GAD). Psychiatry Research: Neuroimaging, 324, 111493. [CrossRef]
- Newman, M. G., Zainal, N. H., & Hoyer, J. (2020). Cognitive-Behavioral Therapy (CBT) for Generalized Anxiety Disorder (GAD). Generalized Anxiety Disorder and Worrying, 203–230. Portico. [CrossRef]
- Wang, X., Thiel, L., & Graff, N. de. (2022). Mindfulness and Relaxation Techniques for Stroke Survivors with Aphasia: A Feasibility and Acceptability Study. Healthcare, 10(8), 1409. [CrossRef]
- Rippe, J. M. (2020). Promoting Regular Physical Activity. Increasing Physical Activity, 173–188. [CrossRef]
- Substance/Medication-Induced Anxiety Disorder. (2017). The SAGE Encyclopedia of Abnormal and Clinical Psychology. [CrossRef]
- Gkintoni, E., Halkiopoulos, C., Antonopoulou, H. (2022). Neuroleadership an Asset in Educational Settings: An Overview. Emerging Science Journal. Emerging Science Journal, 6(4), 893–904. [CrossRef]
- Chapman, A. L., & Owens, L. (2020). Mechanisms of change in dialectical behavior therapy. The Handbook of Dialectical Behavior Therapy, 51–69. [CrossRef]
- Whittingham, K., & Coyne, L. W. (2019). Integrating Acceptance and Commitment Therapy with other interventions. Acceptance and Commitment Therapy, 377–402. [CrossRef]
- Portman, M. E. (2009). Pharmacotherapy for Generalized Anxiety Disorder. Generalized Anxiety Disorder Across the Lifespan, 65–84. [CrossRef]
- Balderston, N. L., Vytal, K. E., O’Connell, K., Torrisi, S., Letkiewicz, A., Ernst, M., & Grillon, C. (2016). Anxiety Patients Show Reduced Working Memory Related dlPFC Activation During Safety and Threat. Depression and Anxiety, 34(1), 25–36. Portico. [CrossRef]
- Fitzgerald, J. M., Phan, K. L., Kennedy, A. E., Shankman, S. A., Langenecker, S. A., & Klumpp, H. (2017). Prefrontal and amygdala engagement during emotional reactivity and regulation in generalized anxiety disorder. Journal of Affective Disorders, 218, 398–406. [CrossRef]
- Fonzo, G. A., Ramsawh, H. J., Flagan, T. M., Sullivan, S. G., Simmons, A. N., Paulus, M. P., & Stein, M. B. (2014). Cognitive-behavioral therapy for generalized anxiety disorder is associated with attenuation of limbic activation to threat-related facial emotions. Journal of Affective Disorders, 169, 76–85. [CrossRef]
- Gordeev, S. A., Posokhov, S. I., Kovrov, G. V., & Katenko, S. V. (2013). Psychophysiological characteristics of panic disorder and generalized anxiety disorder. Zhurnal nevrologii i psikhiatrii imeni SS Korsakova, 113(5), 11-14.
- Hallion, L. S., Tolin, D. F., Assaf, M., Goethe, J., & Diefenbach, G. J. (2017). Cognitive Control in Generalized Anxiety Disorder: Relation of Inhibition Impairments to Worry and Anxiety Severity. Cognitive Therapy and Research, 41(4), 610–618. [CrossRef]
- Khdour, H. Y., Abushalbaq, O. M., Mughrabi, I. T., Imam, A. F., Gluck, M. A., Herzallah, M. M., & Moustafa, A. A. (2016). Generalized Anxiety Disorder and Social Anxiety Disorder, but Not Panic Anxiety Disorder, Are Associated with Higher Sensitivity to Learning from Negative Feedback: Behavioral and Computational Investigation. Frontiers in Integrative Neuroscience, 10. [CrossRef]
- Plana, I., Lavoie, M.-A., Battaglia, M., & Achim, A. M. (2014). A meta-analysis and scoping review of social cognition performance in social phobia, posttraumatic stress disorder and other anxiety disorders. Journal of Anxiety Disorders, 28(2), 169–177. [CrossRef]
- Moon, C.-M., & Jeong, G.-W. (2015). Functional neuroanatomy on the working memory under emotional distraction in patients with generalized anxiety disorder. Psychiatry and Clinical Neurosciences, 69(10), 609–619. Portico. [CrossRef]
- Renna, M. E., Seeley, S. H., Heimberg, R. G., Etkin, A., Fresco, D. M., & Mennin, D. S. (2017). Increased Attention Regulation from Emotion Regulation Therapy for Generalized Anxiety Disorder. Cognitive Therapy and Research, 42(2), 121–134. [CrossRef]
- Stefanopoulou, E., Hirsch, C. R., Hayes, S., Adlam, A., & Coker, S. (2014). Are attentional control resources reduced by worry in generalized anxiety disorder? Journal of Abnormal Psychology, 123(2), 330–335. [CrossRef]
- Tempesta, D., Mazza, M., Serroni, N., Moschetta, F. S., Di Giannantonio, M., Ferrara, M., & De Berardis, D. (2013). Neuropsychological functioning in young subjects with generalized anxiety disorder with and without pharmacotherapy. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 45, 236–241. [CrossRef]
- White, S. F., Geraci, M., Lewis, E., Leshin, J., Teng, C., Averbeck, B., Meffert, H., Ernst, M., Blair, J. R., Grillon, C., & Blair, K. S. (2017). Prediction Error Representation in Individuals With Generalized Anxiety Disorder During Passive Avoidance. American Journal of Psychiatry, 174(2), 110–117. S. (. [CrossRef]
- Patel, N., Stoodley, C., Pine, D. S., Grillon, C., & Ernst, M. (2017). Interaction of induced anxiety and verbal working memory: influence of trait anxiety. Learning & Memory, 24(9), 407–413. [CrossRef]
- Gorka, S. M., Lieberman, L., Shankman, S. A., & Phan, K. L. (2017). Association between neural reactivity and startle reactivity to uncertain threat in two independent samples. Psychophysiology, 54(5), 652–662. [CrossRef]
- Cunningham, W. A., & Kirkland, T. (2013). The joyful, yet balanced, amygdala: moderated responses to positive but not negative stimuli in trait happiness. Social Cognitive and Affective Neuroscience, 9(6), 760–766. [CrossRef]
- Ward, T., Delrue, N., & Plagnol, A. (2017). Neuropsychotherapy as an integrative framework in counselling psychology:The example of trauma. Counselling Psychology Review, 32(4), 18–28. [CrossRef]
- Gkintoni, E., Boutsinas, B., Kourkoutas, E. (2022). Developmental Trauma and Neurocognition in Young Adults. 14th Annual International Conference on Education and New Learning Technologies, 4th – 6th July, Mallorca, Spain. [CrossRef]
- Carruthers, S., Gurvich, C., Sumner, P., Tan, E., Thomas, E., & Rossell, S. (2018). T75. GENERAL AND EXECUTIVE COGNITIVE PROFILES: GENERAL COGNITIONS INFLUENCE ON WCST PERFORMANCE. Schizophrenia Bulletin, 44(suppl_1), S143–S143. [CrossRef]
- Wells, A. (n.d.). The Metacognitive Model of Worry and Generalised Anxiety Disorder. Worry and Its Psychological Disorders, 177–199. [CrossRef]
- Anderson, I. M., & Palm, M. E. (n.d.). Pharmacological Treatments for Worry: Focus on Generalised Anxiety Disorder. Worry and Its Psychological Disorders, 305–334. [CrossRef]
- Berg, C. (2021). The Fundamental Nature of Anxiety. Fear, Punishment Anxiety and the Wolfenden Report, 83–100. [CrossRef]
- Bashford-Largo, J., Aloi, J., Zhang, R., Bajaj, S., Carollo, E., Elowsky, J., Schwartz, A., Dobbertin, M., Blair, R. J. R., & Blair, K. S. (2021). Reduced neural differentiation of rewards and punishment during passive avoidance learning in adolescents with generalized anxiety disorder. Depression and Anxiety, 38(8), 794–803. Portico. [CrossRef]
- Taylor, S. (2019). Treating anxiety sensitivity in adults with anxiety and related disorders. The Clinician’s Guide to Anxiety Sensitivity Treatment and Assessment, 55–75. [CrossRef]
- McHugh, R. K. (2019). Assessing anxiety sensitivity. The Clinician’s Guide to Anxiety Sensitivity Treatment and Assessment, 9–29. [CrossRef]
- Halkiopoulos, C., Antonopoulou, H., Gkintoni, E., & Aroutzidis, A. (2022). Neuromarketing as an Indicator of Cognitive Consumer Behavior in Decision-Making Process of Tourism destination—An Overview. Springer Proceedings in Business and Economics, 679–697. [CrossRef]
- Fung, K., Alden, L. E., & Sernasie, C. (2021). Social anxiety and the acquisition of anxiety towards self-attributes. Cognition and Emotion, 35(4), 680–689. [CrossRef]
- Antonopoulou, H., Halkiopoulos, C., Gkintoni, E., Katsibelis, A. (2022). Application of Gamification Tools for Identification of Neurocognitive and Social Function in Distance Learning Education. International Journal of Learning, Teaching and Educational Research, 21(5), 367–400. [CrossRef]
- Nakamae, T. (2017). Neuromodulation for Obsessive-Compulsive Disorder. Anxiety Disorder Research, 9(1), 50–56. [CrossRef]
- WANG, G.-X., & LI, L. (2013). Virtual Reality Exposure Therapy of Anxiety Disorders. Advances in Psychological Science, 20(8), 1277–1286. [CrossRef]
Figure 2.
This is a figure. Schemes follow the same formatting.
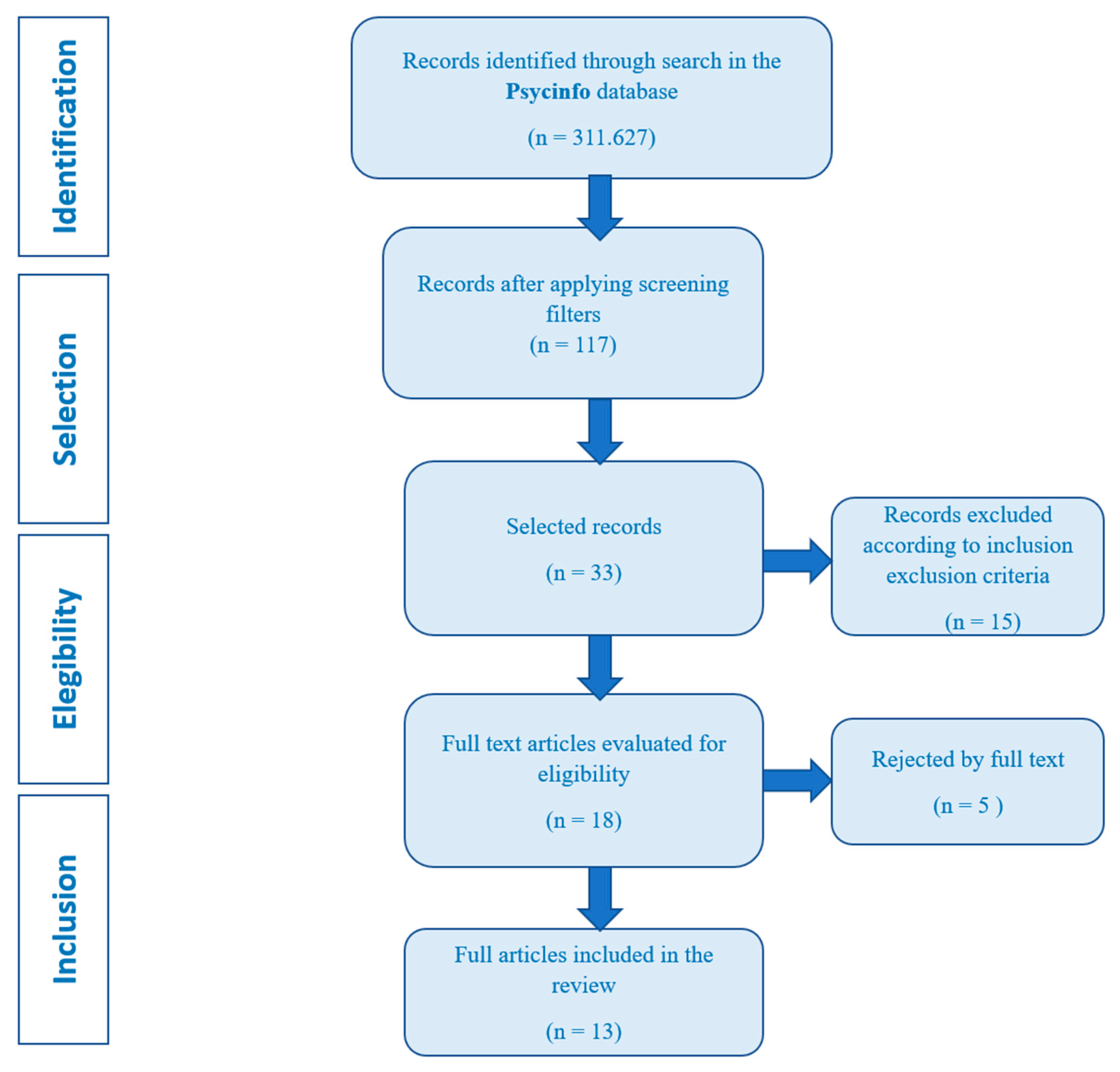

Table 1.
Empirical studies (author, sample, instrument, conclusions).
| Author (year) | Type of study | Sample | Instrument | Conclusions |
|---|---|---|---|---|
| Aasvik et al. (2015) [1] | Quantitative | 167 patients | Clinical assessment: clinical questionnaires to measure memory complaints (EMQ-R), chronic pain (SF-8), depression and anxiety (HADS), fatigue (CFQ) and insomnia (ISI) | Significant levels of fatigue and anxiety while those of depression, insomnia and intensity of pain are not. Subjective memory complaints may reflect concerns about one's own memory performance, so it is an expression of anxiety, becoming anxious when asked to remember something. Anxiety consumes attention. |
| Balderston et al. (2017) [15] | Quantitative | 69 participants from the Washington DC metropolitan area |
Participants completed measures of anxiety: Beck Anxiety Inventory (BAI), State/Trait Anxiety Scale, Beck Depression Inventory (BDI) and Wechsler Abbreviated Scale of Intelligence (WASI) |
There is a deterioration in performance in patients with anxiety, slower reaction time, difficulty recruiting some regions in cognitive tasks, there are intrusive thoughts and low control over them, low regulation of emotions, they have to make efforts to face fearful stimuli, continuous thoughts related to threats during tasks. |
| Fitzgerald et al. (2017) [16] |
Qualitative | 69 individuals |
A block-design Emotion Regulation Task (ERT) |
Individuals with trait anxiety exhibit deficits in cognitive control mediated by the dIPFC; in this study, they experimentally manipulate threat, and it is found that patients with anxiety demonstrated performance deficits. These results suggest that poor cognitive control is a stable trait in patients with anxiety. Furthermore, these results generate a testable hypothesis that WM deficits may predict the future severity of symptoms or the outcome of treatment. |
| Fonzo et al. (2014) [17] | Quantitative | 32 individuals (21 adults with a principal diagnosis of a generalized anxiety disorder and 11 non-anxious healthy controls) | PSWQ, 10 sessions of weekly cognitive-behavioral therapy, the Emotion Face Assessment Task | It provides evidence for a dual-process psychotherapeutic model of changes in neural systems in generalized anxiety disorder in which cingulo-amygdala reactivity to threat signals is attenuated while insular responses to positive facial emotions are potentiated. |
| Gordeev et al. (2013) [18] | Quantitative | 95 patients (34 patients with panic disorder, 32 patients with generalized anxiety disorder and 29 healthy) | Clinical-neurological, psychometric, neuropsychological, and neurophysiological methods | Patients with generalized anxiety disorder differed from patients with panic disorder by a higher level of anxiety, a greater degree of depression, and more reported disorders of short-term memory and directed attention. They also had lower P300 amplitudes but in panic patients they were higher. |
| Hallion et al. (2017) [19] | Quantitative | 56 participants (35 of them had generalized anxiety disorder, the other 21 had no history of mental health, treatment, or mental disorders) | Has been used: MINI, CSR, CGI, SIGH-A, PSWQ, SIGH-D | Generalized anxiety states predicted impaired 'cool' inhibition and impaired cognitive inhibition, although not for the worry trait. Anxiety affects cognitive efficiency by requiring more effort (reflected in part by slower response times) to maintain adequate overall performance (reflected in task accuracy), and that this increased effort is partly attributable to the presence of worry, which competes for attentional resources. |
| Khdour et al. (2016) [20] | Quantitative | 73 participants from clinics associated with the universities of Cairo and Ain Shams. | The North American Adult Reading Test (NAART), the Wechsler Adult Intelligence Scale-Revised (WAIS-R), Digit Span test and the Hamilton Anxiety Rating Scale (HAM-A). | Patients with generalized anxiety learned better from negative feedback. There is a cognitive dissociation between the subtypes of anxiety spectrum disorders, which could underlie a difference in the neural circuitry involved in these disorders. Enhanced learning from negative feedback in people with generalized anxiety is not attributed to group differences in speed of learning or the ability to explore available outcomes. |
| Plana et al. (2014) [21] | Quantitative | 1417 anxious patients and 1321 non-clinical controls. | 40 studies evaluating mentalization, emotion recognition, social perception/knowledge, or attributional style in anxiety disorders | The results indicate different patterns of deterioration of social cognition: people with post-traumatic stress disorder show deficits in mentalization and emotion recognition while other anxiety disorders showed attributional biases. |
| Moon et al. (2015) [22] | Quantitative | 36 right-hand subjects (18 patients with generalized anxiety disorder and 18 healthy controls) | The subjects underwent structured clinical interviews for DSM-IV diagnosis 18 and various psychiatric rating scale: HAMD 17, GAD-7, STAI-I, STAIII, ASI-R | Patients with generalized anxiety disorder showed significant differences on all questionnaires compared to healthy controls.Therefore, this finding suggests that patients with generalized anxiety tend to respond to anxiety-related situations with fear, lower accuracy, and a combination of cognitive deficits. with low attention. |
| Renna et al. (2018) [23] | Qualitative | 17 participants from two different clinics in the northeastern of United States | Structured Clinical Interview for the DSM-IV and the Anxiety Disorders Interview Schedule for DSM-IV | Patients with generalized anxiety disorder present a deficit in attention regulation. They found that a greater ability to sustain attention may be an indicator of clinical improvement. Worry is the hallmark of generalized anxiety, and it inhibits the ability to divert attention because of this, they pay more attention to the threat. There is a decrease in social skills (due to lack of maintenance of attention). |
| Stefanopoulou et al. (2014) [24] | Quantitative | 17 participants after their first session of cognitive-behavioral treatment or on a waitlist from National Health Service clinical psychology clinics in the UK. | Penn State Worry Questionnaire, BDI-II, N-Back Task, Random Generation Key-Pressing Task, Mood ratings, thought valence ratings, filler task and WTAR. | People with generalized anxiety disorder have fewer residual attentional control resources available during the worry process. Fewer resources were available to perform concurrent thinking tasks when individuals with anxiety were thinking about personally relevant topics. Verbal preoccupation takes less attentional control, suggesting that negative biases use resources. |
| Tempesta et al. (2013) [25] | Quantitative | Forty subjects between 20 and 35 years of age with a first episode of generalized anxiety from the Psychiatry Service for Diagnosis and Treatment, Hospital G. | STAI, the Beck Depression Inventory (BDI), PSQI, TAS-20 | Executive functions, as measured by the WCST, were affected in young subjects, immediate recall is also affected. Worry can interfere with the execution of some cognitive functions since it dedicates attentional resources to ruminant linguistic processing of threatening stimuli. Antidepressant treatment affects performance on sustained attention tasks, reducing the ability to remain alert for a long period of time. |
| White et al. (2017) [26] |
Quantitative | 78 participants 18-50 years of age (46 had generalized anxiety disorder and 32 were healthy subjects). | A passive avoidance task | Individuals with generalized anxiety disorder showed impaired reinforcement-based decision making. Lower correlation on the test between punishment and responses. They showed impaired reinforcement-based and worry about possible future consequences, such as illness or losing a job. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



