
Submitted:
17 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Background: Best Possible Medication History (BPMH) collected by clinical pharmacists is crucial for effective medication review but, in Italy, it is often left to the nursing staff. This study aims to compare the quality and accuracy of a clinical pharmacist-documented BPMH with the current standard practice of ward staff-collected BPMH at an Italian perioperative surgical setting. Methods: A 20-week prospective observational non-profit study was conducted in a major University hospital. The study comprised a feasibility, an observational, and an interventional phase. During the feasibility phase, 10 items for obtaining a correct BPMH were identified. The control group consisted of retrospectively analyzed BPMHs collected by the ward staff during the observational phase, while interventions included BPMHs collected by the clinical pharmacist during the third phase. Omissions between the two groups were compared. Results: 14 (2%) omissions were found in the intervention group, compared with 400 (57.4%) found in the controls (p<0.05); data collection was more complete when collected by pharmacists compared to the current modalities (98.0% versus 42.6%; p<0.05). Conclusions: The involvement of a pharmacist significantly reduced the number of omissions in perioperative surgical-collected BPMHs. This intervention holds the potential to decrease the risk of medication errors associated with inaccurate or incomplete BPMHs prior to surgical hospitalization.
Keywords:
clinical pharmacist
; pharmacist intervention
; perioperative
; surgical setting
; potentially inappropriate medication
; best possible medication history
1. Introduction
Medication review is defined as a clinical intervention, frequently performed by pharmacists, aimed to improve medication safety and health outcomes by ensuring optimal medication use [1]. It consists of two consecutive phases: the identification of the best possible medication history (BPMH) and the medication reconciliation. In particular, BPMH allows to collect complete and accurate information about the patient and his/her medications. In addition, the reconciliation examines the patient’s clinical conditions during therapeutic transitions [2]. BPMH is a process of medical information gathering, essential to ensure the prescribing appropriateness. Clinical pharmacists can assist or play a key role, especially as part of interdisciplinary teams, in improving medication use, advising providers to respond to gaps in treatment/care needs, diminishing inappropriate prescribing practices and improving therapeutics safety. Furthermore, an imprecise BPMH process could lead to an increase of errors during the medication reconciliation phase, resulting in an increase of Adverse Drug Reactions (ADRs) and Potentially Inappropriate Prescriptions (PIPs) which can determine patient’s unfavourable clinical outcomes, such as prolonged hospitalization time [3].
In Italy, given the not-yet official recognition of the clinical pharmacist’s role, medication review activities are not restricted to the pharmacist’s responsibility but often delegated to other health professionals, such as clinicians and nurses. Furthermore, in 2014 the Italian Ministry of Health issued a specific recommendation on the implementation of medication review activities to prevent the risk of inadequate prescriptions, with explicit reference to the active involvement of the pharmacist in all stages of the process [4]. Despite this, the Italian situation remains extremely heterogeneous, with some hospitals independently promoting clinical pharmacy activities, usually dedicated to frail patients exposed to polypharmacy [5].
Although the surgical setting is not a common area of intervention for the clinical pharmacist, a few studies have shown the positive impact of the clinical pharmacist in reducing omissions, incompleteness and the risk of adverse events related to patient’s therapy [3]. A 2.7-fold increase in the risk of experiencing postoperative complications has been revealed in surgical patients treated with preadmission medications compared to those not taking preadmission medications [6]. This underlines the importance of preventing unintentional interruptions to prescribed therapies unrelated to surgery during the perioperative period. Most of the patients undergoing major surgery are exposed to the associated significant cardio-respiratory stress. Accordingly, any sudden or prolonged withdrawal of the current drug therapy in these patients could add significant risk to their surgery and complicated outcome, especially considering that they are often elderly and potentially treated with an average six preadmission medications. No research to date has evaluated the impact of preadmission medication errors in surgical patients in Italy.
Even if routine internal and external audits have shown that more than 90% of the patients have a BPMH documented within 24 hours of admission to our University Hospital by the ward staff, the accuracy of BPMH documentation by a pharmacist in a ’real world' scenery and related issues determining medication discrepancies is still not well defined in Italian healthcare.
The Padua University Hospital is a 1600-bed tertiary referral hospital which provides emergency medicine, general medicine, oncology, cardiology, respiratory, general surgery, orthopaedic surgery, cardiothoracic surgery, rehabilitation, geriatrics, mental health and palliative care services. The hospital also provides specialist services such as heart, liver and lung transplantation, as well as caring for paediatrics patients with acute, chronic and rare diseases. The pharmacy department oversees all clinical and surgical areas throughout the hospital and thus care for complex patients with extensive medication use.
In this study we aimed to investigate the potential role of the clinical pharmacist in the perioperative surgical ambulatory of our University Hospital by measuring the impact of the quality and accuracy of pharmacist-documented BPMH compared with the current standard BPMH in charge by the ward staff.
2. Materials and Methods
2.1. Study Design
A prospective observational non-profit study was undertaken at major public University hospital in Padova, Italy, over a 20-week period (March to July 2021) and performed in three phases (see Figure 1):
i. The first one, a feasibility phase, focused on the identification of the specific and tailorized information necessary to obtain a correct BPMH during March 2021. A total of 10 items related to the patient's therapy were selected. These include, in addition to the number of drugs taken and polypharmacotherapy, essential information for proper BPMH such as the name of the drugs and active ingredients prescribed; pharmaceutical form, and dosage; initiation and duration of therapy; completeness of information on integrative therapies and homeopathic medicines and dietary/herbal supplements.
ii. The second observational phase involved systematic data collection on the activity of ward staff (e.g., nurses) in gathering medication history during April-May 2021.
iii. The third interventional phase examined the impact of BPMH collection carried out by the clinical pharmacist in optimizing the prescription appropriateness during June-July 2021.
The consecutive research phases were useful for determining the percentage of omissions found in the BPMH collection conducted by the nursing staff (e.g., the current practice, used as a control group) to those subsequently obtained by the clinical pharmacist (intervention group). In both cases, health care professionals collected all patient’s data at the time of the preoperative anaesthesiology visit through direct interview with the patient and/or his/her caregiver as well as referring to online medical records and, if available, to general practitioner documentation of the patient’s clinical history.
The clinical pharmacy service involved one dedicated hospital pharmacy resident, supervised by an attending clinical pharmacist, in this project. The role of the clinical pharmacist related with patient admissions comprised the following: acquiring a BPMH, performing the medication reconciliation, reviewing medication orders, pharmaceutical compounding and managing medications’ supply. The clinical pharmacist reviewed the patients within 24 to 72 hours from admission, (e.g., patients hospitalized over the weekend were reviewed on Monday).
The primary outcome of the study was to measure the rate of total omissions in the two groups.
Both the present manuscript and all parts of the study were checked and submitted according to the checklist for Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [7].
2.2. Ethics Approval
This study was conducted in accordance with Good Clinical Practice (GCP) recommendations, using the guidance documents and practices outlined by the International Conference on Harmonization, and the European directives 2011/20/CE and ISO 4155, and in agreement with the Italian regulation. All patients gave written informed consent to take part in the study, and the protocol was approved by the Padova Province Local Ethical Committee (authorization number: 5136/AO/21).
2.3. Inclusion and Exclusion Criteria
All patients with a scheduled surgery in 2021, admitted to the pre-operative outpatient clinic of the General Surgery Department of the University Hospital of Padua were recruited. Patients unable to sign a consent form or with less than three drugs in their BPMH were excluded from the analysis.
2.4. Statistical Analysis
The sample size of the study was calculated referring to the data already available in the literature on this topic [3]. G Power software (version 3.1.9.7) was used to better estimate the proportion of patients to include into the two groups [8]. Continuous normally and non-normally distributed variables were reported as mean ± standard deviation (SD) or median (interquartile range, IQR), respectively whereas dichotomous variables were expressed as frequencies and percentages. Statistical significance was calculated with unpaired Student's t-test for two-sample comparisons, or the non-parametric Mann–Whitney's U-test for independent variables, whereas categorical variables were compared using Pearson's chi-square test or the Fisher's exact test, using the R software [9]. The differences between groups were considered significant when P <0.05.
3. Results
We recruited a total of 140 patients, divided equally in the two groups: interventions and controls.
The two groups were comparable regarding the baseline characteristics such as median age, gender distribution, elderly patients’ percentage, comorbidities and polypharmacy. However, statistically significant differences were found in the type of surgery performed in the two groups (Table 1).
Regarding the accuracy of BPMH, statistically significant differences emerged for each item. Overall, for the 10 items considered, we found 14 (2%) omissions in the intervention group and 400 (57.4%) missing information in the controls (p<0.05), highlighting the ability of the clinical pharmacist to collect almost all data compared to the current modalities (98.0% versus 42.6%; p<0.05). Surprisingly, a marked difference was revealed in the data regarding the treatment duration and initiation, and the requisite of galenic manipulation of medicinal products before oral administration. None of these three aspects were ever considered and registered in any patient of the control group (Table 2).
4. Discussion
Many recent articles have discussed the critical importance of the pharmacist in surgical procedures, with a focus on the role in the perioperative multidisciplinary team and the impact of their collaboration on the outcome of surgical procedures. [10] As reported in the literature, an accurate medication collection process leads to more accurate reconciliation, reducing medication errors and adverse reactions due to incorrect medication prescription. [11,12]. The introduction of the clinical pharmacist into the medication process has produced positive results in decreasing the number of incomplete information and has been effective in turning drug interviews more precise, consistent and accurate. According to Nanji et al., 5.3% of medication administration during 277 surgeries were incorrect, and 79.3% were avoidable. [13]
Only few studies, however, have investigated the possible role of the clinical pharmacist in a pre-surgical setting, such as the one we performed [14,15,16]. Although, especially for scheduled surgeries, interaction with the patient (or his or her caregivers) is highly sought after to achieve effective BPMH: in fact, transitions of care are critical moments for patient safety and a more effective medication reconciliation and information collection accuracy verification process is needed to prevent potential errors. Complete and accurate documentation of a patient's medications is critical for communication among health care providers, especially at the time of surgery, to clearly identify which medications have been discontinued due to surgery or replaced over a period of time due to surgical risks.
The role of the pharmacist during surgical procedures is indisputably necessary for efficient healthcare delivery and positive patient outcomes. Indeed, the perioperative pharmacist has advanced therapeutic knowledge and experience to ensure the appropriate use of drugs and patient outcomes during the preoperative, intraoperative and postoperative phases for all surgical patients. [17] During the preoperative period, the pharmacist ensures fluid status optimization, appropriate analgesia administration, antimicrobial prophylaxis, and venous thromboembolism prophylaxis. At the intraoperative stage, the pharmacist ensures that antimicrobial prophylaxis, fluid resuscitation and anaesthetic plans are redosed. Opioid doses are then adjusted based on the patient's tolerance and adverse effects. during the postoperative period, the patient receives medication monitoring, withdrawal of strong opioids and counselling. [17] Furthermore, the pharmacist is able to understand and participate in the analysis of the main causes of surgical complications: in fact, our study demonstrated the possibility of decreasing the risk of medication errors due to incorrect medication prescription or an inaccurate, incomplete or absent medical history prior to hospitalisation. [18] In addition to the reduction in drug therapy’s errors, a higher percentage of patients in the intervention arm obtained accurate information on how to use the pharmaceutical form, or the homeopathic medicine or other dietary supplements. In the control arm, on the other hand, more than 400 omissions were recorded, most of which related to the active ingredient taken, the duration of home therapy and the taking split-crushed tablets. This difference in terms of omissions could be attributed to various reasons. These include information paucity of patient medication history, inaccuracies of primary care physicians' referral letters, outdated drug history obtained from the general practitioner, and lack of time to collect a detailed medication history. [19] The high frequency of medication omissions at the time of data gathering has been revealed by several previous studies [20,21,22].
As demonstrated by Nguyen et al., the introduction of the clinical pharmacist in a perioperative environment determined an improvement in the BPMH, decreasing the average error rate from 5.25 to 0.21 errors per patient in the intervention arm (reconciliation performed by pharmacist). [3] In addition, the introduction of a pharmacist in the surgical department helped to lower the amount of incompleteness by more than 96%.
Stratifying by clinical setting, 27% of patients enrolled in the present study (19/70) had a tumor of the gastrointestinal tract, closely related to the scheduled surgery; the median age was 64 (IQR 48-80) and of these, 41% (11 patients) were taking more than 5 drugs per day. As shown by recent epidemiological studies, 50 percent of elderly cancer patients (over 60 years of age) take more than 5 medications per day. [23] Polypharmacotherapy is therefore a fairly common condition in these individuals and is a high-risk factor for ADRs, for the risk of interactions and for potentially inappropriate medication use.
Furthermore, cancer patients are managed across the entire health care spectrum, both in acute hospital care and in home chemotherapy programs and other community settings. This complex system of interdependencies has a high potential for miscommunication, especially in changing hospital settings. [24] This is an area of interest for pharmacists, who possess the skills needed to optimize the transition of patient care across these settings by identifying errors and other medication-related problems. [24] The collaboration between pharmacists and surgeons has the potential to make a significant contribution, including improving the quality of care, containing costs for patients and, above all, reducing mortality. [25]
4.1. Strengths and Weaknesses (Study Limitations)
In the light of the findings obtained from our study, we are confident that the role of a pharmacist-led data collection service could be developed and implemented. As pioneered in an Australian hospital, a collaborative model between clinical pharmacists and physicians regarding data collection, medication reconciliation, and pharmacotherapy records management for in-patients was successfully introduced. [21] The service was positively received, and the pharmacist's recording and reconciliation of medical records led to a statistically significant reduction in medication errors of over 80% versus the comparison arm without pharmacist intervention. [19] We therefore believe that in the future a similar model could be structured for the Italian hospital reality: the pharmacist should no longer deal only with the management of the medication itself, but working in collaboration with the multidisciplinary clinical team either in the emergency department or on the wards would enable pharmacists to strengthen their role in the clinical setting to improve data collection and the main stages of therapeutic reconciliation, ensuring a higher quality of care of patients.
The present study has some limitations: primarily, we collected data only from a limited number of surgical units, excluding other departments such as the emergency surgery. The impact of the pharmacist in other perioperative sceneries needs to be investigated and will be the subject of further research. Another limitation concerns clinical outcomes: we analysed process endpoints such as the number of incomplete information, but we did not evaluate efficacy or safety endpoints. Future analyses on a larger cohort will be aimed at assessing the proportion of patients who experienced one or more medication errors, the type of medication errors related to drug prescribing or administration, and number and consequences of ADRs associated with medication errors to investigate the impact of hospitalization length, the number of drugs prescribed at hospital discharge and the number of drug interactions.
4.2. Further Research
The evidence from this analysis will be useful for planning the implementation of the whole medication review process, including the reconciliation phase in our specific clinical setting in order to highlight the potential contribution of the clinical pharmacist, as a part of a multidisciplinary team. The development of a new professional role may also provide a further opportunity for clinical pharmacists working in the Italian National Health System, advancing their professional practice in hospital pharmacy. Finally, a mutual collaboration between the pharmacist, the physicians and the nurses not only will allow a direct interaction with patients and their caregivers but also will strengthen the pharmacist's role in the ward team leading to an improved quality of patient care.
5. Conclusions
A new organisational model, in which the clinical pharmacist is involved in the perioperative surgical setting, has demonstrated a marked improvement in the collection of BPMH over the previous standard of care. Further research into aspects related to therapeutic reconciliation and the implantation of the service in other settings will be necessary to increase the visibility of the clinical pharmacist in a country where this figure is not yet fully recognised.
Author Contributions
Conceptualization, F.V. and M.C.G.; methodology, F.F.F., D.M.; validation, F.V., and M.C.G.; formal analysis, D.M.; investigation, L.Co.; data curation, L.Co., L.P.; writing—original draft preparation, L.P., F.F.F.; writing—review and editing, D.M. and L.Ca.; visualization, all authors; supervision, F.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding..
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Padova Province Local Ethical Committee (authorization number: 5136/AO/21)
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Data are available from the authors upon requested to the corresponding author.
Acknowledgments
none.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gillespie U, Alassaad A, Henrohn D, et al. A comprehensive pharmacist intervention to reduce morbidity in patients 80 years or older: a randomized controlled trial. Arch Intern Med. 2009;169(9):894-900. [CrossRef]
- Hohl CM, Partovi N, Ghement I, et al. Impact of early in-hospital medication review by clinical pharmacists on health services utilization. PLoS One. 2017;12(2):e0170495. Published 2017 Feb 13. [CrossRef]
- Nguyen AD, Lam A, Banakh I, Lam S, Crofts T. Improved Medication Management With Introduction of a Perioperative and Prescribing Pharmacist Service. J Pharm Pract. 2020;33(3):299-305. [CrossRef]
- Italian Ministry of Health, Recommendation No. 17 - Reconciliation of drug therapy. December 2014 (Ministero della Salute, Raccomandazione n. 17 - Riconciliazione della terapia farmacologica. Dicembre 2014), https://www.salute.gov.it/imgs/C_17_pubblicazioni_2354_allegato.pdf.
- Chiarelli MT, Antoniazzi S, Cortesi L, et al. Pharmacist-driven medication recognition/ reconciliation in older medical patients. Eur J Intern Med. 2021;83:39-44. [CrossRef]
- Kennedy JM, van Rij AM, Spears GF, Pettigrew RA, Tucker IG. Polypharmacy in a general surgical unit and consequences of drug withdrawal. Br J Clin Pharmacol. 2000;49(4):353-362. [CrossRef]
- von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495-1499. [CrossRef]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175-191. [CrossRef]
- R Core Team (2021) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/.
- Wireko AA, Ohenewaa Tenkorang P, Tope Adebusoye F, et al. The importance of pharmacists in modern day surgery - editorial. Int J Surg. 2023;109(2):88-90. Published 2023 Feb 1. [CrossRef]
- Abdulghani KH, Aseeri MA, Mahmoud A, Abulezz R. The impact of pharmacist-led medication reconciliation during admission at tertiary care hospital. Int J Clin Pharm. 2018;40(1):196-201. [CrossRef]
- van den Bemt PM, van der Schrieck-de Loos EM, van der Linden C, Theeuwes AM, Pol AG; Dutch CBO WHO High 5s Study Group. Effect of medication reconciliation on unintentional medication discrepancies in acute hospital admissions of elderly adults: a multicenter study. J Am Geriatr Soc. 2013;61(8):1262-1268. [CrossRef]
- Nanji KC, Patel A, Shaikh S, Seger DL, Bates DW. Evaluation of Perioperative Medication Errors and Adverse Drug Events. Anesthesiology. 2016;124(1):25-34. [CrossRef]
- Renaudin A, Leguelinel-Blache G, Choukroun C, et al. (2020) Impact of a preoperative pharmaceutical consultation in scheduled orthopedic surgery on admission: a prospective observational study. BMC Health Serv Res. 2020 Aug 13;20(1):747. [CrossRef] [PubMed] [PubMed Central]
- Vallecillo T, Slimano F, Moussouni M, et al. (2022) Development and validation of a ready-to-use score to prioritise medication reconciliation at patient admission in an orthopaedic and trauma department. Eur J Hosp Pharm. 2022 Sep;29(5):264-270. Epub 2020 Dec 8. [CrossRef] [PubMed] [PubMed Central]
- Cheng HT, Zhao M, Liu HT, Shen GL, Zhao T, Feng ZE (2022) The prevalence of chronic medication therapy problems and pharmacists' interventions among hospitalized perioperative patients: a retrospective observational study. BMC Health Serv Res. 2022 Dec 6;22(1):1483. [CrossRef] [PubMed] [PubMed Central]
- Patel GP, Hyland SJ, Birrer KL, et al. (2020) Perioperative clinical pharmacy practice: Responsibilities and scope within the surgical care continuum. JACCP Journal of the American College of Clinical Pharmacy, 3(2), 501-519. [CrossRef]
- Lovely JK, Hyland SJ, Smith AN, Nelson G, Ljungqvist O, Parrish RH 2nd. Clinical pharmacist perspectives for optimizing pharmacotherapy within Enhanced Recovery After Surgery (ERAS®) programs. Int J Surg. 2019;63:58-62. [CrossRef]
- Khalil V, deClifford JM, Lam S, Subramaniam A (2016) Implementation and evaluation of a collaborative clinical pharmacist's medications reconciliation and charting service for admitted medical inpatients in a metropolitan hospital. J Clin Pharm Ther. 2016 Dec;41(6):662-666. Epub 2016 Aug 31. [CrossRef] [PubMed]
- deClifford JM, Lam SH, Leung BK (2009) Evaluation of a pharmacist-initiated e-prescription transcription service for discharged patients. J Pharm Pract Res, 2009;39 (1):33–36.
- deClifford JM, Caplygin FM, Lam SS and Leung BK (2007), Impact of an Emergency Department Pharmacist on Prescribing Errors in an Australian Hospital. Journal of Pharmacy Practice and Research, 37: 284-286. [CrossRef]
- Bond CA, Raehl CL, Franke T (2002) Clinical pharmacy services, hospital pharmacy staffing and medication errors in United States hospitals. Pharmacotherapy 2002; 22: 134-47.
- Hurria A, Browner IS, Cohen HJ, et al. (2012) Senior adult oncology. J Natl Compr Canc Netw. 2012 Feb;10(2):162-209. [CrossRef] [PubMed] [PubMed Central]
- Coutsouvelis J, Siderov J, Tey A, et al. (2020) The impact of pharmacist-led strategies implemented to reduce errors related to cancer therapies: a systematic review. Journal of Pharmacy Practice and Research, 50.
- Neville HL, Chevalier B, Daley C, et al. Clinical benefits and economic impact of post-surgical care provided by pharmacists in a Canadian hospital. Int J Pharm Pract. 2014;22(3):216-222. [CrossRef]
Figure 1.
Graphical representation of the study phases.
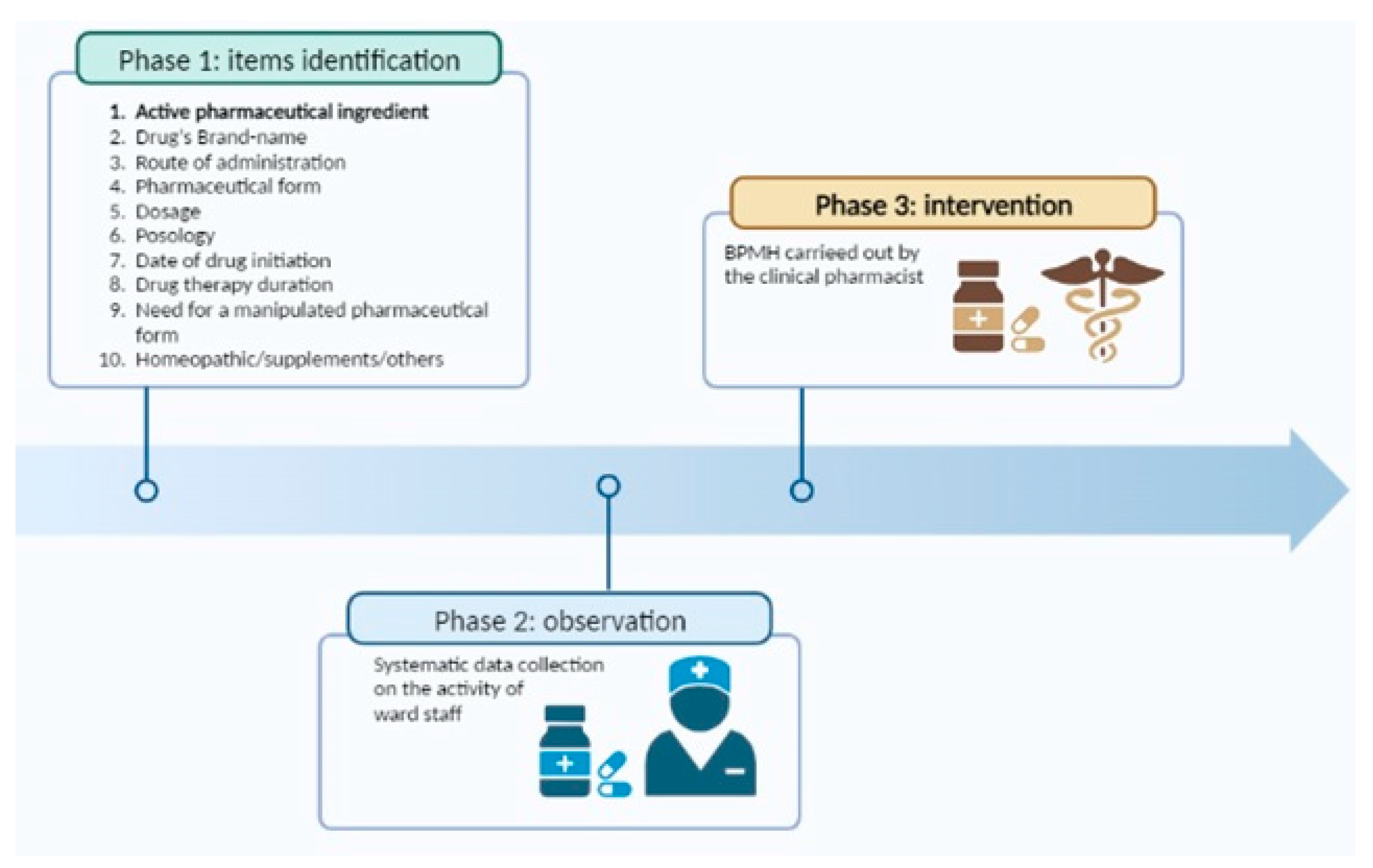

Table 1.
Baseline patients’ characteristics.
| Variables | All patients (N=140) |
Control Group (N=70) |
Intervention Group (N=70) |
p |
|---|---|---|---|---|
| Male, n (%) | 75 (53.6) | 37 (52.8) | 38 (54.3) | 0.862 |
| Age, median (IQR) | 61 (55-73) | 60 (55-74) | 64 (56-75) | 0.760 |
| Comorbidities, median (IQR) | 3 (2-5) | 3 (2.5-4) | 3 (2-5) | 0.804 |
| Patients aged ≥ 65 years (%) | 67 (47.8) | 34 (48.6) | 33 (47.1) | 0.863 |
| Polypharmacy, median (IQR) | 4(2-5) | 4(2-5) | 4(2.25-6) | 0.308 |
| Patients in polypharmacotherapy (drugs taken ≥3; %) | 96 (68.6) | 44 (62.8) | 52 (74.3) | 0.145 |
| Type of surgery | <0.05 | |||
| General surgery (%) | 73 (52.1) | 70 (100.0) | 3 (4.3) | -- |
| Gastric surgery (%) | 62 (44.8) | 0 (0.0) | 62 (88.6) | -- |
| Others (%) | 5 (3.1) | 0 (0.0) | 5 (7.1) | -- |
Table 2.
Comparative analysis of information accuracy on drug therapy of pre-surgical patients collected during the feasibility phase and the intervention period.
Table 2.
Comparative analysis of information accuracy on drug therapy of pre-surgical patients collected during the feasibility phase and the intervention period.
| Information reported in the BPMH | Control Group (N=70) |
Intervention Group (N=70) |
p |
|---|---|---|---|
| Active pharmaceutical ingredient (%) | 21 (30.0) | 68 (97.1) | <0.05 |
| Brand name (%) | 53 (75.7) | 69 (98.6) | <0.05 |
| Route of administration (%) | 44 (62.9) | 70 (100) | <0.05 |
| Pharmaceutical form (%) | 53 (75.7) | 70 (100) | <0.05 |
| Dosage (%) | 55 (78.6) | 68 (97.1) | <0.05 |
| Posology (%) | 49 (70.0) | 70 (100) | <0.05 |
| Date of drug initiation (%) | 0 (0.0) | 64 (91.4) | N.A. |
| Drug therapy duration (%) | 0 (0.0) | 67 (95.7) | N.A. |
| Need for a manipulated pharmaceutical form (%) | 0 (0.0) | 70 (100) | N.A. |
| Homeopathic/supplements/others (%) | 25 (35.7) | 70 (100) | <0.05 |
| Total omissions (%) | 400/700 (57.1) | 14/700 (2.0) | <0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



