
Submitted:
17 July 2023
Posted:
18 July 2023
You are already at the latest version
Abstract
Introduction: The identification of some prognostic markers in head and neck cancers (HNC) is necessary for the stratification of the therapeutic approach with benefits in increasing treatment response rates and limiting the toxic side effects of treatments. Neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR) and pallets-to-lymphocyte ratio (PLR) are currently validated as cheap and accessible biomarkers in different types of solid tumors.
The purpose of the study was to evaluate the possible biomarker value of NLR, PLR and MLR recorded pre-treatment (radiotherapy/chemotherapy) for prognostic purposes in HNC.
Materials and methods: The study included 190 patients with HNC included in the oncology record in the oncology outpatient clinic of the Craiova County Emergency Hospital starting from January 2002 and deceased until December 2022. Among them, 40 patients treated multimodally in the Clinic were included in the study of Oncology of the Craiova County Emergency Hospital for which the pre-treatment value (chemotherapy/radiotherapy) of NLR, PLR and MLR could be calculated. Overall survival (OS) values were correlated with NLR, PLR and MLR.
Results: Median values for NLR, PLR and MLR were 6.15 (1.24-69), 200.79 (61.3- 1775.0) and 0.53 (0.12-5.5) respectively. In the study, the mean values for NLR, PLR and MLR of 2.88, 142.97 and 0.36 respectively were obtained. Median OS in the study group was 11 months (1-120). Although a negative Pearson`s correlation, the relationship between your variables was only weak, values R =.07, p=.67; R=.02, p=.31 and R=07, p=.62 being related with NLR, PLR and MLR respectively correlation with overall survival (OS). The median values of NLR, PLR and MLR were calculated (1.53, 90.32 and 0.18 respectively) for HNC cases with pre-treatment values of NLR <2 and for HNC cases with NLR values ≥6 (23.5, 232.78 and 0.79 respectively). Median OS for cases with NLR<2 and NLR≥6 were 17.4 and 13 months, respectively.
Conclusions: The negative correlations of NLR, PLR and MLR with OS reported in the study are in accordance with the data reported in the literature for locally advanced recurrent and metastatic HNSCC cases. The comparative analysis of the data in the group with NLR<2 and NLR≥6 highlights an advantage of 4.4 months in median OS in favor of the group with low values of NLR. Being cheap and accessible, these markers could change the therapeutic approach even in centers with limited resources. The role of borderline NLR values as a prognostic factor in HNSCC must also be defined. PLR and MLR are less evaluated as biomarkers but the study demonstrates their potential to be used as prognostic biomarkers, it remains to be clarified if their inclusion in multivariable models along with NLR would bring a benefit
Keywords:
head and neck cancers
; HNC
; HNSCC
; NLR
; PLR
; MLR
; biomarkers
; prognostic
1. Introduction:
The role and value of peripheral blood biomarkers has been demonstrated in several types of cancer, especially in recent years. Neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR) and pallets-to-lymphocyte ratio (PLR) were investigated independently or in association are evaluated markers of inflammation, increased values being correlated with unfavorable prognosis. NLR, one of the most frequently evaluated biomarkers is correlated with 2 factors: acute and chronic inflammation indicated by neutrophil count and adaptive immunity correlated with the number of lymphocytes. PLR can be associated with the release of cytokines and chemokines, and MLR reflects both inflammation and the risk of cancer progression, an alteration of this ratio involving the inability of the host to block tumor proliferation [1,2,3]. One of the major advantages of using NLR, PLR and MLR as a biomarker is the simple, inexpensive evaluation method, the patient's discomfort being minimal, only peripheral blood samples being required. In contrast, the modern methods of immunohistochemistry and polymerase chain reaction (PCR) are mentioned, which involve taking samples by biopsy [4].
The heterogeneity of the response to aggressive multimodal treatment including surgery, radiotherapy, chemotherapy, target molecular therapy and immunotherapy justifies the efforts to identify prognostic and predictive biomarkers in head and neck cancers (HNC). Even if the subtype of the disease associated with Human Papilloma Virus (HPV) infection is related to a superior response to treatment and a favorable prognosis, a stratification of the treatment to limit the toxicities associated with the treatment, but also to increase the response rate is still the subject of clinical studies. Understanding the physiopatological mechanisms, the role of inflammation and the host's immune response in initiating cancer progression and metastasis, but also in modulating the response to treatment, explaining a favorable response due to the abundance of immune cells in HPV related HNC are arguments that explain the growing interest in NLR, PLR and MLR as possible biomarkers in HNC [5]. NLR is the most frequently reported biomarker, and the meta-analysis of Rodrigo et al. which includes studies related to oropharyngeal cancer identifies NLR, more precisely the increased values of this ratio as a negative prognostic factor. Even though, regardless of HPV status, high pre-treatment NLR values were associated with an unfavorable prognosis in oropharyngeal cancer. The correlation of NLR with prognosis was more significant in cases of HPV-related oropharyngeal cancer [6].
The aim of the study was to evaluate the possible biomarker value of NLR, PLR and MLR recorded pre-treatment for prognostic purposes in HNC.
1.1. NLR, PLR and MLR – from prognostic markers to future orchestrator of HNC multimodal approach?
The rapid development in recent years of genetic and molecular analysis made it possible to identify specific molecular changes that could guide oncological treatments in HNC. However, the absence of clear correlations between molecular and genetic features with a prognosis make studies on large samples and uniform characterizations of tumor specimens necessary. Excision repair cross complementing group 1 (ERCC1), a deoxyribonucleic acid (DNA) repair enzyme involved in Cisplatin resistance and HPV status are the most promising biomarkers in HNC. However, the generation of combined markers including not only imaging/radiomics features and genetic and molecular mutation, but also peripheral blood biomarkers could predict not only prognostic, but also the pattern of evolution in order to stratify treatment escalation and elective management of neck lymph-nodes [7]. The three reports including the value of neutrophils were analyzed in a systematic review of 49 relevant studies that included HNC patients. Even if an obvious heterogeneity was observed between studies, NLR, PLR and MLR were strongly correlated with prognostic. Kumarasamy et al. considers that these biomarkers could be introduced in clinical practice for the therapeutic decision [8].The study conduced in the Department of Otolaryngology, Head and Neck Surgery of Beijing Tongren Hospital included 50 laryngeal cancer patients and 40 healthy subjects as a control group and evaluated NLR, lymphocyte to monocyte ratio (LMR) and monocyte-to-white blood cell ratio (MWR) as a prognostic markers. The values calculated were higher for NLR, PLR, MWR and were lower for LMR in the group of patients with cancer than in the control group. Increased values of NLR, PLR and MWR and lower values of LMR were associated with a reduced 5 years OS, this positive correlation for NLR, PLR and MWR and negative for LMR being also identified in the case of comparative assessment of survivors and deceased patients. Age, alcohol consumption and smoking as well as TNM staging were correlated with these biomarkers, being considered that their association could confer a superior performance [9]. A significant increase in NLR and PLR with the degree of histological tumor differentiation and TNM staging was observed in a study that included 170 HNC cases and 80 cases as control group. The increased values of NLR and PLR were also higher in HNC cases compared to values obtained in healthy patients, but they were also correlated with an unfavorable prognosis. The authors recommend confirmation of the results on larger patients groups and assessment of these markers correlations with the treatment response [10,11]. An NLR value ≧3.6 is considered the cut-off value in a group of 180 patients from Taiwan diagnosed with advanced stages (stage III and IV) of nasopharyngeal cancer. NLRs higher than the maintained value are associated with reduced PFS, DFS and OS [12].
Brewczyńsk and colleagues proposed the evaluation of NLR, PLR, MLR and the SII systemic inflammation index before and after radiotherapy/chemotherapy in patients diagnosed with oropharyngeal cancers related and unrelated to HPV infection, trying to identify a correlation of these parameters with DFS and OS. In the case of HPV positive patients, a correlation with a reduced OS was identified for increased pretreatment white blood cells (WBC) (>8.33 /mm3), but also with values of NLR>2.13 and SII >448.60. Values NLR>2.29 and SII>462.58 were strongly associated with a reduced DFS. In the case of patients with HPV-unrelated disease, these correlations were not identified [13].
A meta-analysis that included 24 articles and an independent set of patients (n=540) evaluated the values and ranges of values of NLR that were correlated with OS and DFS. The study did not identify a significant cut off for OS and DFS in the range of NLR >2.2 and <6, significant differences being identified for values of NLR <2.2 and >6, higher values of NLR being associated with unfavorable prognosis [14]. Analyzing 28 cohorts including 6847 head and neck squamous cell carcinoma (HNSCC), systematic review and meta-analysis by Yang et al. concludes that increased values of pre-treatment NLR are associated with DFS, PFS, OS, but also with cancer specific survival, without a strong correlation [15].
Evaluating the prognostic value of NLR, MLR, PLR, alkaline phosphatase (ALP) and lactate dehydrogenase (LDH) pre-operatively and post-operatively, a study that included 361 cases of squamous laryngeal cancer identified the value NLR, PLR and MLR in both perioperative settings as prognostic. ALP and LDH have not demonstrated predictive power in all situations. The authors propose preoperative NLR and postoperative MLR as an independent marker of OS and PFS in laryngeal cancer [16].
The heterogeneity in the cut off values reported by different authors justifies the initiation of studies with the aim of identifying this value with a prognostic role. Using the maximum concordance index (C-index) method and internal validation via the bootstrapping method, the NLR cut off was identified on a lot of non-metastatic nasopharyngeal cancer cases treated with intensity modulated radiotherapy (IMRT) for curative purposes. The study included 463 patients and the follow-up period was 70.8 months. The value of NLR =3 was associated with the highest C index (0.548). An NLR >3 was considered an independent prognostic factor, being associated with reduced survival. The authors recommend the introduction of this prognostic factor in the evaluation of nasopharyngeal cancer [17].
The prognostic value of NLR and PLR in patients with HNSCC treated with definitive or adjuvant chemo-radiotherapy using complete blood counts (CBCs) recorded 10 days before the start of treatment were evaluated in a study that included 186 patients in relation to OS, locoregional recurrence-free survival (LRFS), DFS and acute toxicity. Most cases (45%) were cancers of the oropharynx, followed by cancers of the oral cavity, hypopharynx and larynx in proportions of 28%, 14% and 13% respectively. The study identified a relationship between NLR and OS and between LTFS and DFS. Acute grade ≥ 2 toxicity was not correlated with any of these markers. PLR was also not associated with outcomes or toxicity. The authors considered that NLR could be used as an independent predictive biomarker of mortality in patients with HNSCC treated with chemo-radiotherapy [18]. Takenada et al. analyzed 19 studies that include 3770 patients and demonstrates the prognostic value of NLR in HNSCC. The results highlighted in all studies a correlation of the NLR values higher than the cutoff with poorer disease-specific survival and OS. A meta-analysis proposed by the same authors that included 9 studies that enrolled 2327 patients also demonstrated the prognostic value of PLR in HNSCC. In this case higher PLR values were associated with unfavorable prognosis. Another study by the team from the otorhinolaryngology department in Osaka, Japan identified NLR as a predictor of response to immune checkpoint inhibitors (ICIs) treatment in HNSCC [19,20,21]. A 1.78 combined and site-specific hazard ratio for OS was identified by Mascarella et al. in a meta-analysis including 24 studies and 6479 patients for cases with higher NLR values (raging between 2.04-5). The highest hazard ratio for OS was 2.36, being associated with hypopharyngeal cancer [22]. PLR and NLR were recorded in the first 4 weeks of treatment on a group of 273 patients treated at McGill University Health Center HNSCC in a time interval of 11 years. The study evaluated PLR and NLR in relation to recurrence and mortality rates. An increased mortality (43%) and a more advanced T stage was associated with PLR >170 and NLR ≤3.0. NLR values above 4.2 were associated with a higher risk of recurrence. The study identifies the association of NLR PLR at least as precise as TNM staging in predicting survival [23].
Using the AUROC peaks method, optimal threshold for 5 years survival amd values for NLR and PLR were calculated in HNSCC cases treated with surgery. Cases without R0 resection and patients with chronic inflammatory diseases were excluded from this study. Cutoff values of 113 and 2.8 for PLR and NLR respectively were identified. It should be noted the different proportion of patients with PLR values higher than the threshold in the case of hypopharyngeal tumors (71.7%) and lower than the threshold in the case of oropharyngeal tumors (25.0%). Also, mortality at 5 years in the case of tumors with PLR values lower than the threshold was 24.6% vs 46.4% in the case of tumors with PLR ≥107. And for NLR, the same indicator was 32.3% vs 56.5% for NLR values < 3.9, respectively NLR values ≥ 3.9. For PLR, the correlation is also observed in the case of DFS and cancer specific mortality. NLR is correlated only with mortality [24]. The prognostic values (including OS and DFS) of pre-treatment lymphocyte-monocyte ratio (LMR) in HNSCC was evaluated in a systematic review and a meta-analysis that included 4260 cases from 7 cohorts. The increased value of LMR was associated with favorable prognosis. The authors mention the need for careful evaluation of the results, being a retrospective study [25]. Changes in the dynamics of LMR during radiotherapy for HNC were evaluated in relation to OS and metastasis free survival in a group of 1431 patients. The follow-up period was 9 years and during this period 44.4% of the patients died and 16.8% developed distant metastases. Higher delta-MLR variation at 2 weeks was associated with OS and metastasis free survival at 5 years of 59% and 80% rates respectively. In the case of lower delta-MLR, the same variables were associated with 73% and 87% respectively. Delta-MLR was identified as an independent prognostic factor in HNC treated with radiotherapy. The authors recommend the use of this biomarker, being cheap and accessible [26].
An analysis that included 215 cases that fulfilled the study criteria of primary adenocarcinoma and carcinoma, advanced-stage sinonasal cancers, highlighted a correlation of the pre-treatment values of NLR and PLR with OS and DFS. Cases with higher values of the two markers had shorter OS and DFS. NLR <2.6 and PLR <156.9 were associated with reduced risk of recurrence [27]. A complex score involving fibrinogen value and NLR was proposed for prognostic purposes in advanced hypopharyngeal carcinoma. All 111 patients in the study were treated with radiotherapy, bio-radiotherapy or chemo-radiotherapy. Three score values were used to divide the patients into groups, and subsequently the prognostic value of the scores was analyzed. Fibrinogen ≥341 mg/dl and NLR≥3.59, i.e. F-SCOR =2 was identified as an independent predictor of OS and PFS. In the case of patients with F-NLR score =2, OS and PFS were significantly lower than in the group with F-NLR score =0 (fibrinogen <341 mg/dl and NLR<3.59) [28]. The studies considered significant for identifying the predictive power for treatment response, but also the prognostic value of NLR, PLR and MLR were summarized in Table 1 [9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30].
2. Materials and methods:
The study included 190 patients with HNC from the oncology records in the oncology outpatient clinic of the Craiova County Emergency Hospital starting from January 2002 and deceased until December 2022. Among them, 40 patients multimodally treated in the Oncology Clinic of the County Hospital were included in the study. The possibility to calculate the pre-chemotherapy value of NLR, PLR and MLR was an inclusion criteria. Cases that benefited from other systemic oncological treatment and radiotherapy before the evaluation of these markers were excluded. Other synchronous or metachronous malignancies or autoimmune diseases treated with immunosuppressive medication were also exclusion criteria. Hypertension and type 2 diabetes mellitus were not considered exclusion criteria. However, the cases that benefited from surgical interventions for diagnostic, curative and palliative purposes were accepted. Complete blood test was recorded in the day of admission to the oncology department, being included in the evaluation of chemotherapy regimen administration eligibility. Later, the complete blood test was repeated before each cycle of chemotherapy, but the dynamic asessment of biomarkers was not proposed. The variable time interval between chemotherapy courses and the differences between the radiotherapy regimens delivered sequentially or concurrently were also considered confounding factors. We also mention that due to the long period of inclusion in the study, there was a variability in the technique and radiotherapy doses, from the Soviet Union Rokus M40 cobalt machine without imaging guidance to a 3-dimension conformal technique based on a LINAC machine. The variability in the clinical or imaging assessment of progression and the limitations due to technical reasons of the computer tomography (CT) follow up determined us not to include DFS and PFS in the analysis. All patients received chemotherapy with curative or palliative monotherapy based on platinum salts or regimens of platinum doublet or triplet combination including taxanes, 5-flurouracil or oral analog Capecitabine, the number of chemotherapy cycles varying between 1 and 12. The choice of the chemotherapy regimen was the physician's choice or was also influenced by the temporarily limited accessibility to certain chemotherapeutic agents in Romania. It should be mentioned that, being a retrospective study, in the cases that required surgery, the referral to the Oncology Clinic followed the surgical procedure. For this reason, the NLR, PLR and MLR values were recorded pre-chemotherapy/radiotherapy and not pre-treatment in all the cases. Pearson`s correlation of NLR, PLR and MLR with overall survival (OS) values were also analyzed. Evaluating the data from the meta-analysis by Cho and colleagues, we proposed in the analysis a comparison of the data for lower and higher values of NLR (<2 and ≥6 respectively) [14].
3. Results:
Of the 40 patients included in the study, 39 (97.5%) were diagnosed with head and neck squamous cell carcinoma (HNSCC). One case was diagnosed with pleomorphic sarcoma. After the initial analysis, this case was excluded from the study, only cases of HNSCC were included. The average age at the onset of the disease was 64.84 years (48-86 years). Hypertension and type 2 diabetes mellitus were reported in 8 and 2 cases, respectively. The vast majority of cases, 35 out of 39 (89.7%) included in the study are males and 4 out of 39 (10.3%) were females. All cases were diagnosed with locally advanced or metastatic stage (III and IV). The group of patients included various anatomical sites of the disease: oropharynx -11 cases (28,2%), larynx -7 cases (17,94%), oral cavity -13 cases (33,33%), nasopharynx - cases (2,55%), unknown primary -2 cases (5,1%), parathyroid – 1 case (2.55%), sinonasal– 1 case (2.55%). Mean values for NLR, PLR and MLR were 6.22 (1.24-69), 203.17 (61.3-1775.0) and 0.53 (0.12-5.5) respectively. In the study, the median values for NLR, PLR and MLR of 2.88, 142.97 and 0.36 respectively were obtained. The free online platform https://www.socscistatistics.com/ was used for the statistical analysis. In the study, the mean values for NLR, PLR and MLR of 2.88, 142.97 and 0.36 respectively were obtained. Median OS in the study group was 11 months (1-120). Although a negative Pearson`s correlation, the relationship between your variables was only weak, values R =.07, p=.67; R=.02, p=.31 and R=07, p=.62 being related with NLR, PLR and MLR respectively correlation with overall survival (OS). The mean values of NLR, PLR and MLR were calculated (1.53, 90.32 and 0.18 respectively) for HNC cases with pre-treatment values of NLR <2 and for HNC cases with NLR values ≥6 (23.5, 232.78 and 0.79 respectively). The characteristics of the patients and the heatmap including NLR, PLR MLR and OS (in months) for 39 HNSCC cases also included in Table 2 and Table 3 respectively. Median OS for cases with NLR<2 and NLR≥6 were 17.4 and 13 months, respectively [Graphic 1–4].
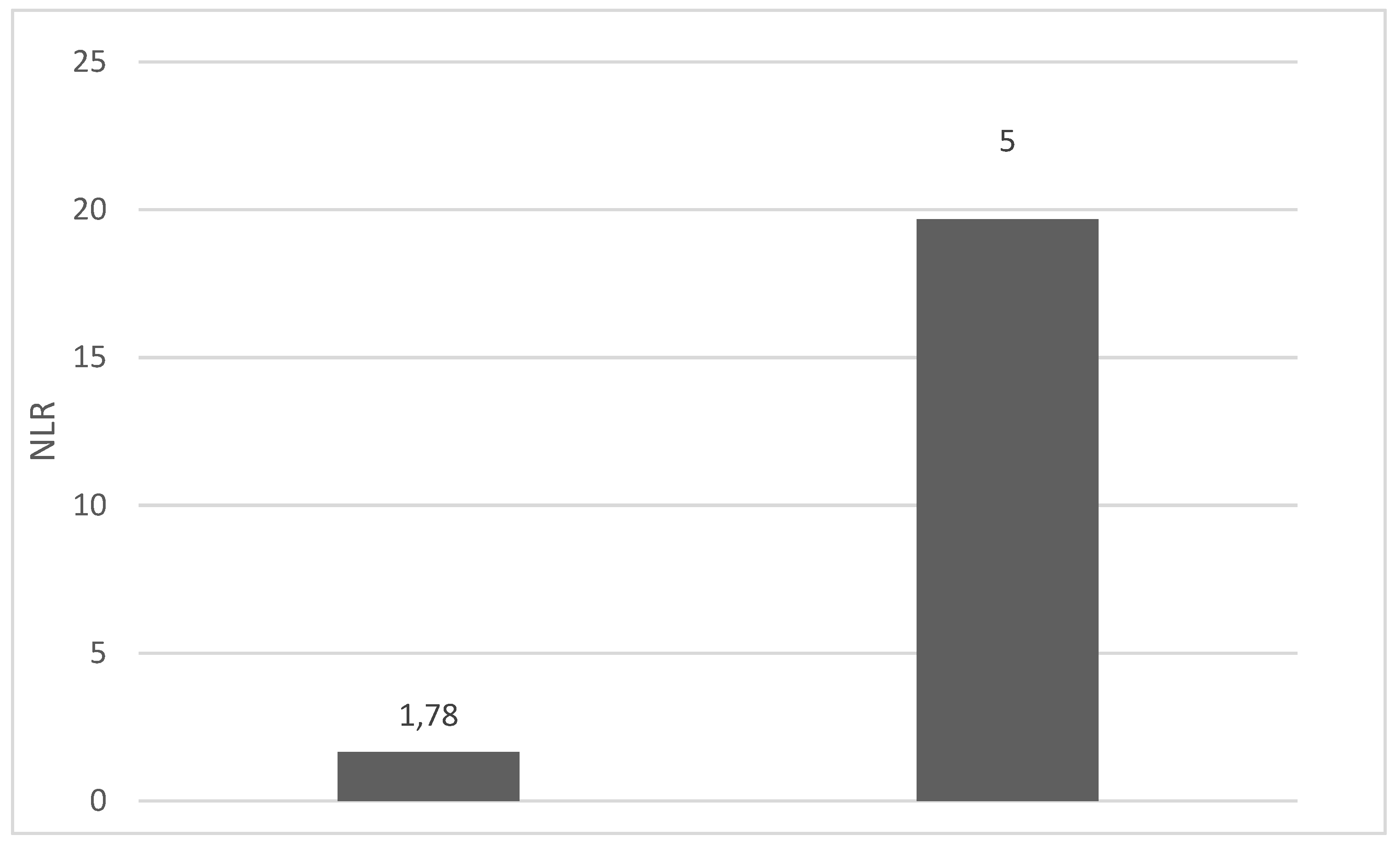
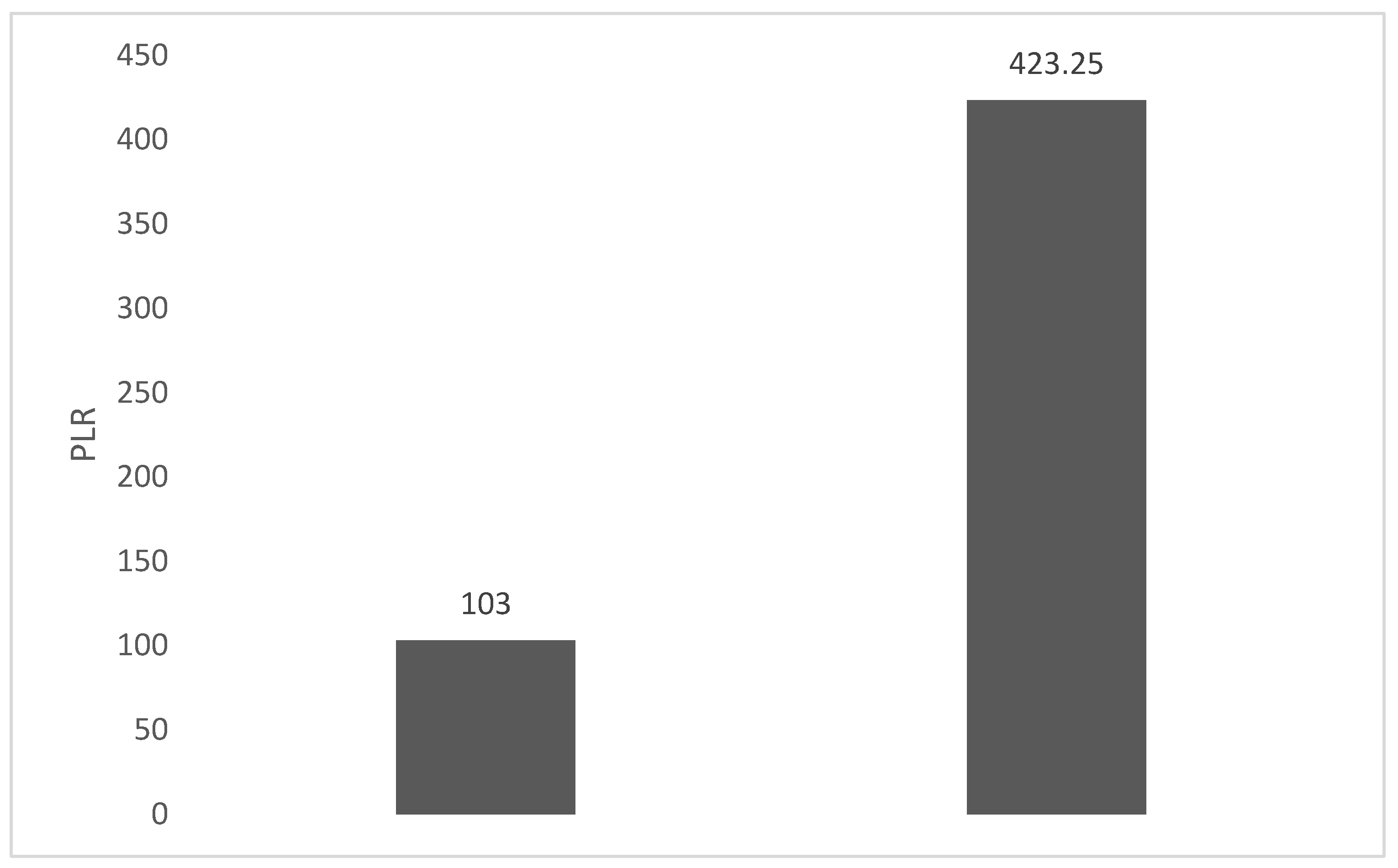
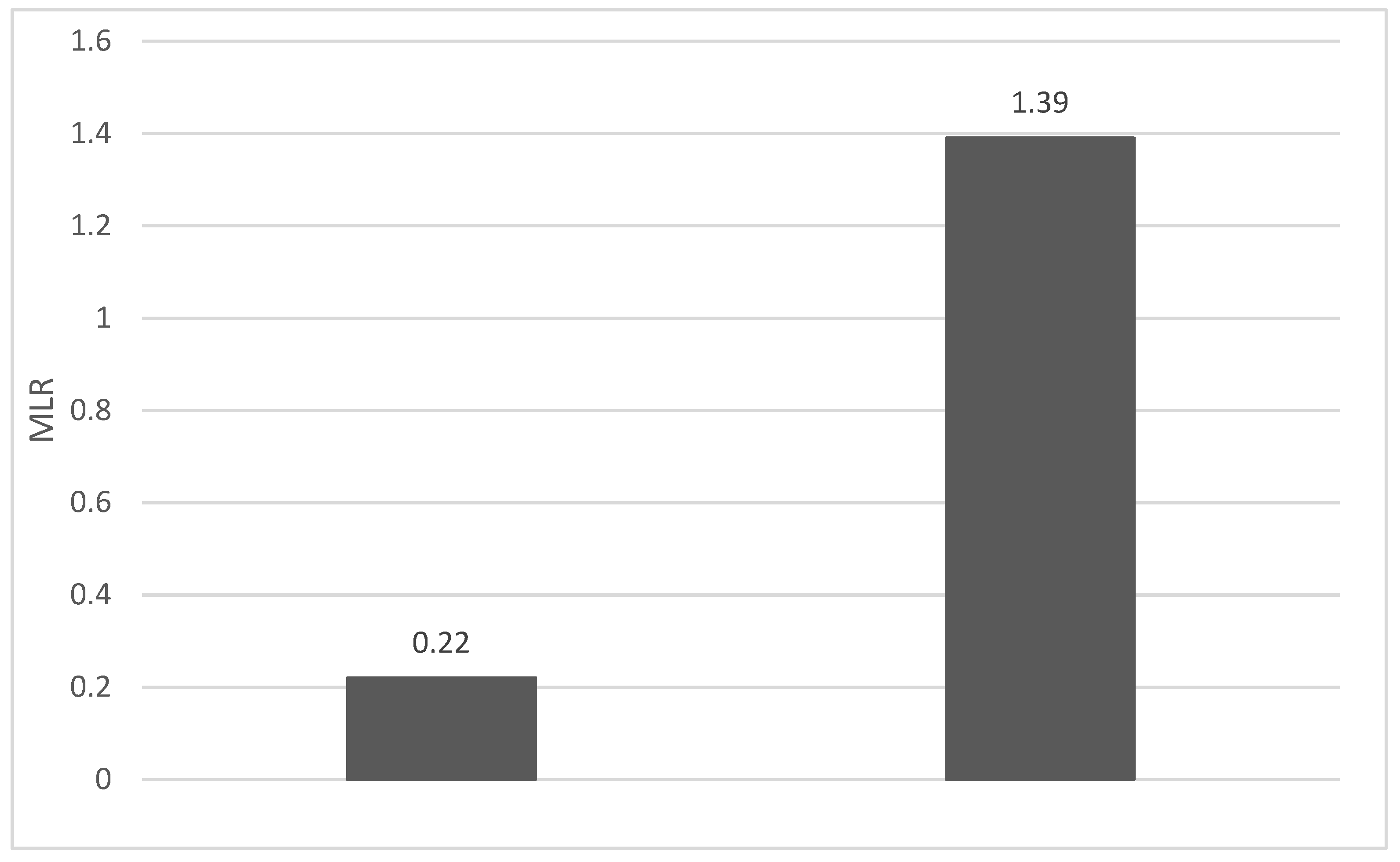
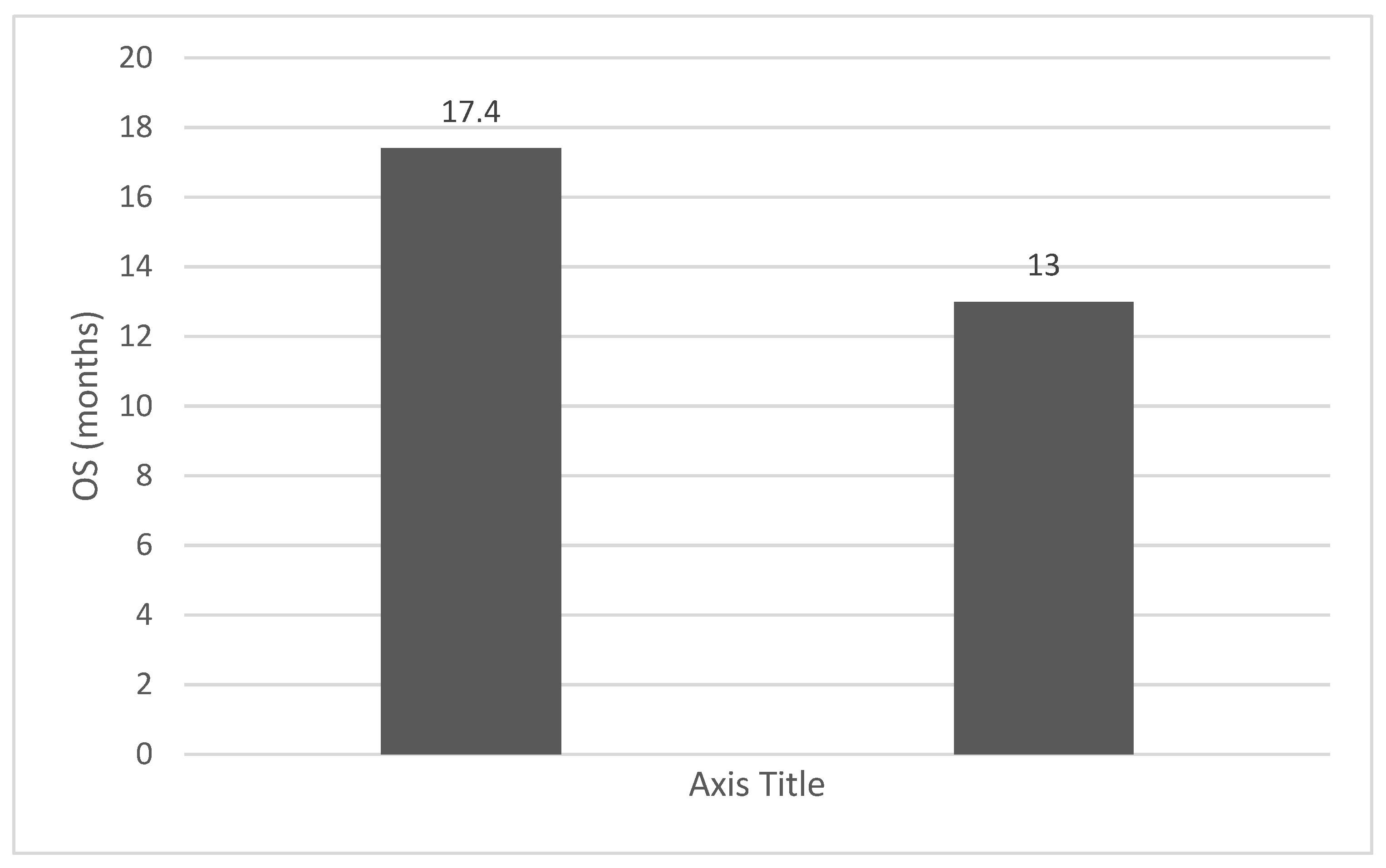

Table 1.
Patients characteristics.
| Characteristics | N (total =40) | % |
|---|---|---|
| Age at the time of diagnostic | ||
| Median (range) | 64.84 years (48-86 years). | - |
| Histology | ||
| squamous cell carcinomas (SCC) | 39 | 100 |
| Anatomical tumor site | ||
| oropharynx | 11 | 28,2 |
| oral cavity | 13 | 33,33 |
| larynx | 7 | 17,94 |
| nasopharynx | 1 | 2,55 |
| unknow priary | 2 | 5,1 |
| sinonasal | 1 | 2,55 |
| parathyroid | 1 | 2,55 |
| NLR | ||
| Mean (range) | 6.22 (1,24-69) | |
| PLR | ||
| Mean (range) | 203.17 (61.3-1775.0) | |
| MLR | ||
| Mean (range) | 0.53 (0.12-5.5) | |
| Overall survival (OS) | ||
| Median (range) | 17.92 (1-120) |
Graphic 1.
Mean NLR for patients with NLR values between 0 and 2 (left) and higher then 6 (right).
Graphic 2.
Mean PLR for patients with NLR values between 0 and 2 (left) and higher then 6 (right).
Graphic 3.
Mean MLR for patients with NLR values between 0 and 2 (left) and higher then 6 (right).
Graphic 4.
Median OS (months) for patients with NLR values between 0 and 2 (left) and higher then 6 (right).
Graphic 4.
Median OS (months) for patients with NLR values between 0 and 2 (left) and higher then 6 (right).
4. Discussions:
The importance of neutrophils and their involvement in the immune response has been evident since 1884 when the phenomenon of phagocytosis was described. These cells, the most abundant of leukocytes, have a short life span and have the role of monitoring infectious and inflammatory processes, being the main effectors of the innate immune system. Their interaction with other types of leukocytes, modulating their immune role, explains the choice of association of these ratios as possible biomarkers in autoimmune diseases, cardiovascular diseases, infections and most types of cancer [31].
Multiple factors such as age, stress, but also diseases such as diabetes, coronary disease, anemia, stroke can influence NLR, a value between 1 and 2 being considered normal. A so-called "gray zone" between 2.3-3 can serve as an early warning of some pathological conditions including psychiatric disorders, cancer, atherosclerosis, being sensitive to infections, inflammation and sepsis. Related both with cancer-specific mortality and with overall cancer mortality of patients, but also being associated with the response to immunotherapy, NLR is promoted as a cheap and accessible biomarker. A value of 3 is generally recommended as a cut-off value for prognosis and the decrease of NLR values below 7 is generally associated with a reduction in the risk of mortality in severe conditions. Zahorec considers NLR a future biomarker related to cellular immune activation, an index of stress and inflammation [32].
A meta-analysis involving 14 studies and 5,274 patients evaluated the value of NLR, PLR and MLR as prognostic markers in endometrial cancer, starting from the premise that until now conclusive positive results have only been obtained in cervical cancer, breast cancer, ovarian cancer and other types of solid tumors. NLR or PLR were correlated with disease free survival (DFS), increased values being associated with an unfavorable prognosis in endometrial cancer, but MLR was not associated with OS or DFS [33]. MLR, NLR, PLR and D-dimer were correlated with clinical outcome in lung cancer patients treated with surgery. For all these variables, lower values were identified as being associated with a better OS and PFS. In the multivariate analysis, the lower MLR value was an independent biomarker for a better OS and PFS [34]. Analyzing using Cox Regression the prognostic value of NLR and PLR on a set of 1435 cases from the University of Malaya Medical Center Breast Cancer Registry, Koh and colleagues identified both NLR and PLR as prognostic factors in breast cancer. The authors consider that additional studies are needed because this biomarker obviously brings added value if it is included in the prognostic models for breast cancer [35]. A retrospective analysis including 152 prostate cancer patients treated with radiotherapy in the Department of Radiotherapy at the Maria Sklodowska-Curie National Institute of Oncological Research (Gliwice, Poland) aimed to evaluate the prognostic value of the pretreatment values of PLR, NLR, lymphocyte to monocyte ratio (LMR), platelets (PLT), but also other biological laboratory values including red blood cells (RBC), prostate specific antigen (PSA) level, Gleason score and factors related to the patient including age, smoking status and comorbidities. NLR, PLR, leukocyte count and pre-treatment RBC were identified as independent prognostic factors [36,37].
Even if in high-income countries, especially those in Western Europe and North America, Human Papilloma Virus (HPV) involvement in the etiology of HNSCC is already common, the studies proposed in Romania by Ursu et al. demonstrates that the vast majority of analyzed cases are non-related to HPV infection. In a 26 cases evaluated for oncogenic viruses involvement in HNSCC ethiology, 23 of the cases are related to at least one of the viruses, but it should be mentioned that no case was associated with alpha or beta types of HPV infection. Only 23 cases out of 189, representing 12.2%, were identified as HPV DNA-positive in another study conducted by Ursu and colleagues in Northeastern Romania, half of the cases being oropharyngeal cancers. The authors mention that only a small subset of HNSCC cases will be associated with HPV. Even taking into account these data, the lack of fully reimbursed standard evaluation of HPV status in our country, or at least p16 from immunohistochemistry as a surrogate marker, is obviously a source of uncertainty and possible TNM staging errors for oropharynx cancers [38,39].
The limits of the study must also be mentioned, including the uncertainty induced by the presence of comorbidities in some cases that have been shown to be associated with the two faces of the immune system (innate immune response and lymphocytes mediated adaptive immunity) being correlated with other diseases [40]. Also, the variability in the chemotherapy sequences and protocols of radiotherapy and chemotherapy, the lack of complete data regarding smoker status must also be mentioned as sources of uncertainty. The heterogeneity of the reports related to the cut off value of these markers, but also the contradictory results regarding the correlation of NLR, PLR and MLR with OS in HNC not related to HPV make investigations and prospective studies on large cohorts of patients with uniform inclusion criteria necessary.
5. Conclusions:
The negative correlations of NLR, PLR and MLR with OS reported in the study are in accordance with the data reported in the literature for locally advanced recurrent and metastatic HNSCC cases. The comparative analysis of the data in the group with NLR<2 and NLR≥6 highlights an advantage of 4.4 months in median OS in favor of the group with low values of NLR. Being cheap and accessible, these markers could change the therapeutic approach even in centers with limited resources. The role of borderline NLR values as a prognostic factor in HNSCC must also be defined. PLR and MLR are less evaluated as biomarkers, but the study demonstrates their potential to be used as prognostic biomarkers, it remains to be clarified if their inclusion in multivariable models along with NLR would bring a benefit in prognostic models of HNSCC
References
- Galdiero, M.R.; Bonavita, E.; Barajon, I.; Garlanda, C.; Mantovani, A.; Jaillon, S. Tumor associated macrophages and neutrophils in cancer. Immunobiology 2013, 218, 1402–1410. [Google Scholar] [CrossRef]
- Catal O, Ozer B, Sit M, Aktas G, Erkol H. (). The role of monocyte to lymphocyt ratio in predicting me-tastasis in rectal cancer. Annals of Medical Research. 2021; 28(3), 0527–0531. Retrieved from https://www.annalsmedres.org/index.php/aomr/article/view/428.
- Kumarasamy C, Sabarimurugan S, Madurantakam RM, Lakhotiya K, Samiappan S, Baxi S, Nachimuthu R, Gothandam KM, Jayaraj R. Prognostic significance of blood inflammatory biomarkers NLR, PLR, and LMR in cancer-A protocol for systematic review and meta-analysis. Medicine (Baltimore). 2019 Jun;98(24):e14834.
- Misiewicz, A.; Dymicka-Piekarska, V. Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review. J. Inflamm. Res. 2023, ume 16, 69–81. [Google Scholar] [CrossRef]
- Kumarasamy, C.; Tiwary, V.; Sunil, K.; Suresh, D.; Shetty, S.; Muthukaliannan, G.K.; Baxi, S.; Jayaraj, R. Prognostic Utility of Platelet–Lymphocyte Ratio, Neutrophil–Lymphocyte Ratio and Monocyte–Lymphocyte Ratio in Head and Neck Cancers: A Detailed PRISMA Compliant Systematic Review and Meta-Analysis. Cancers 2021, 13, 4166. [Google Scholar] [CrossRef]
- Rodrigo, J.P.; Sánchez-Canteli, M.; Triantafyllou, A.; de Bree, R.; Mäkitie, A.A.; Franchi, A.; Hellquist, H.; Saba, N.F.; Stenman, G.; Takes, R.P.; et al. Neutrophil to Lymphocyte Ratio in Oropharyngeal Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 802. [Google Scholar] [CrossRef]
- Basheeth, N.; Patil, N. Biomarkers in Head and Neck Cancer an Update. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 1002–1011. [Google Scholar] [CrossRef]
- Hayes, M.; Lan, C.; Yan, J.; Xie, Y.; Gray, T.; Amirkhan, R.H.; E Dowell, J. ERCC1 expression and outcomes in head and neck cancer treated with concurrent cisplatin and radiation. Anticancer Res. 2011, 31. [Google Scholar]
- Li, P.; Li, H.; Ding, S.; Zhou, J. NLR, PLR, LMR and MWR as diagnostic and prognostic markers for laryngeal carcinoma. . 2022, 14, 3017–3027. [Google Scholar]
- Seetohul, Y.B.; Singh, V.; Jain, R.K.; Chaudhary, A.K. Prognostic Value of Neutrophil–Lymphocyte Ratio and Platelet–Lymphocyte Ratio in Head and Neck Malignancies. Indian J. Otolaryngol. Head Neck Surg. 2019, 72, 128–132. [Google Scholar] [CrossRef]
- Tu Xiu-Ping, Tian Tian, Chen Liang-Si, Luo Xiao-Ning, Lu Zhong-Ming, Zhang Si-Yi, Chen Shao-Hua. Prognostic values of preoperative NLR and PLR in patients with laryngeal squamous cell carcino-ma.Translational Cancer Research; Vol 7, No 2 (April 28, 2018). 28 April.
- Liao, L.-J.; Hsu, W.-L.; Wang, C.-T.; Lo, W.-C.; Cheng, P.-W.; Shueng, P.-W.; Hsieh, C.-H.; Chiu, Y.-L.; Lin, Y.-C. Prognostic impact of pre-treatment neutrophil-to-lymphocyte ratio (NLR) in nasopharyngeal carcinoma: A retrospective study of 180 Taiwanese patients. Clin. Otolaryngol. 2017, 43, 463–469. [Google Scholar] [CrossRef]
- Brewczyński, A.; Jabłońska, B.; Mazurek, A.M.; Mrochem-Kwarciak, J.; Mrowiec, S.; Śnietura, M.; Kentnowski, M.; Kołosza, Z.; Składowski, K.; Rutkowski, T. Comparison of Selected Immune and Hematological Parameters and Their Impact on Survival in Patients with HPV-Related and HPV-Unrelated Oropharyngeal Cancer. Cancers 2021, 13, 3256. [Google Scholar] [CrossRef]
- Cho, J.-K.; Kim, M.W.; Choi, I.S.; Moon, U.Y.; Kim, M.-J.; Sohn, I.; Kim, S.; Jeong, H.-S. Optimal cutoff of pretreatment neutrophil-to-lymphocyte ratio in head and neck cancer patients: a meta-analysis and validation study. BMC Cancer 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Huang, Y.; Zhou, L.; Dai, Y.; Hu, G. High pretreatment neutrophil-to-lymphocyte ratio as a predictor of poor survival prognosis in head and neck squamous cell carcinoma: Systematic review and meta-analysis. Head Neck 2018, 41, 1525–1535. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zeng, H.; Yang, J.; Lu, Y.; Zhang, D.; Wang, J.; Kuang, C.; Zhu, S.; Wang, M.; Ma, X. Survival and prognostic analysis of preoperative inflammatory markers in patients undergoing surgical resection for laryngeal squamous cell carcinoma. BMC Cancer 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Setakornnukul, J.; Chanvimalueng, W.; Patumanond, J.M.; Thephamongkhol, K.M. Cutoff point of neutrophil-to-lymphocyte ratio for predicting survival in nasopharyngeal carcinoma. Medicine 2021, 100, e27095. [Google Scholar] [CrossRef]
- Bojaxhiu, B.; Templeton, A.J.; Elicin, O.; Shelan, M.; Zaugg, K.; Walser, M.; Giger, R.; Aebersold, D.M.; Pra, A.D. Relation of baseline neutrophil-to-lymphocyte ratio to survival and toxicity in head and neck cancer patients treated with (chemo-) radiation. Radiat. Oncol. 2018, 13, 216. [Google Scholar] [CrossRef]
- Takenaka, Y.; Oya, R.; Kitamiura, T.; Ashida, N.; Shimizu, K.; Takemura, K.; Yamamoto, Y.; Uno, A. Prognostic role of neutrophil-to-lymphocyte ratio in head and neck cancer: A meta-analysis. Head Neck 2017, 40, 647–655. [Google Scholar] [CrossRef]
- Takenaka, Y.; Oya, R.; Kitamiura, T.; Ashida, N.; Shimizu, K.; Takemura, K.; Yamamoto, Y.; Uno, A. Platelet count and platelet-lymphocyte ratio as prognostic markers for head and neck squamous cell carcinoma: Meta-analysis. Head Neck 2018, 40, 2714–2723. [Google Scholar] [CrossRef]
- Takenaka, Y.; Oya, R.; Takemoto, N.; Inohara, H. Neutrophil-to-lymphocyte ratio as a prognostic marker for head and neck squamous cell carcinoma treated with immune checkpoint inhibitors: Meta-analysis. Head Neck 2022, 44, 1237–1245. [Google Scholar] [CrossRef]
- Mascarella, M.A.; Mannard, E.; Silva, S.D.; Zeitouni, A. Neutrophil-to-lymphocyte ratio in head and neck cancer prognosis: A systematic review and meta-analysis. Head Neck 2018, 40, 1091–1100. [Google Scholar] [CrossRef]
- Rassouli, A.; Saliba, J.; Castano, R.; Hier, M.; Zeitouni, A.G. Systemic inflammatory markers as independent prognosticators of head and neck squamous cell carcinoma. Head Neck 2013, 37, 103–110. [Google Scholar] [CrossRef]
- Szilasi, Z.; Jósa, V.; Zrubka, Z.; Mezei, T.; Vass, T.; Merkel, K.; Helfferich, F.; Baranyai, Z. Neutrophil-To-Lymphocyte and Platelet-To-Lymphocyte Ratios as Prognostic Markers of Survival in Patients with Head and Neck Tumours—Results of a Retrospective Multicentric Study. Int. J. Environ. Res. Public Heal. 2020, 17, 1742. [Google Scholar] [CrossRef] [PubMed]
- Tham, T.; Olson, C.; Khaymovich, J.; Herman, S.W.; Costantino, P.D. The lymphocyte-to-monocyte ratio as a prognostic indicator in head and neck cancer: a systematic review and meta-analysis. Eur. Arch. Oto-Rhino-Laryngology 2018, 275, 1663–1670. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-H.; Chou, W.-C.; Wu, Y.-Y.; Lin, C.-Y.; Chang, K.-P.; Liao, C.-T.; Ho, T.-Y.; Yeh, C.-M.; Liu, C.-J.; Hung, S.-P.; et al. Prognostic significance of dynamic changes in lymphocyte-to-monocyte ratio in patients with head and neck cancer treated with radiotherapy: results from a large cohort study. Radiother. Oncol. 2020, 154, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Turri-Zanoni, M.; Salzano, G.; Lambertoni, A.; Giovannardi, M.; Karligkiotis, A.; Battaglia, P.; Castelnuovo, P. Prognostic value of pretreatment peripheral blood markers in paranasal sinus cancer: Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratio. Head Neck 2016, 39, 730–736. [Google Scholar] [CrossRef]
- Kuwahara, T.; Takahashi, H.; Sano, D.; Matsuoka, M.; Hyakusoku, H.; Hatano, T.; Hiiragi, Y.; Oridate, N. Fibrinogen and Neutrophil-to-lymphocyte Ratio Predicts Survival in Patients with Advanced Hypopharyngeal Squamous Cell Carcinoma. Anticancer. Res. 2018, 38, 5321–5330. [Google Scholar] [CrossRef]
- Ventura, E.; Barros, J.; Salgado, I.; Millán, A.; Vilares, M.; Zagalo, C.; Gomes, P. Pretreatment Blood Markers in the Prediction of Occult Neck Metastasis: A 10-Year Retrospective Study. Cureus 2021, 13. [Google Scholar] [CrossRef]
- Hu, X.; Tian, T.; Sun, Q.; Jiang, W. Prognostic value of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in laryngeal cancer: What should we expect from a meta-analysis? Front. Oncol. 2022, 12, 945820. [Google Scholar] [CrossRef]
- Kourilovitch, M.; Galarza–Maldonado, C. Could a simple biomarker as neutrophil-to-lymphocyte ratio reflect complex processes orchestrated by neutrophils? J. Transl. Autoimmun. 2023, 6, 100159. [Google Scholar] [CrossRef]
- Zahorec, R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl. Med J. 2021, 122, 474–488. [Google Scholar] [CrossRef]
- Leng, J.; Wu, F.; Zhang, L. Prognostic Significance of Pretreatment Neutrophil-to-Lymphocyte Ratio, Platelet−to−Lymphocyte Ratio, or Monocyte-to-Lymphocyte Ratio in Endometrial Neoplasms: A Systematic Review and Meta−analysis. Front. Oncol. 2022, 12, 734948. [Google Scholar] [CrossRef]
- Wang, J.; Li, H.; Xu, R.; Lu, T.; Zhao, J.; Zhang, P.; Qu, L.; Zhang, S.; Guo, J.; Zhang, L. The MLR, NLR, PLR and D-dimer are associated with clinical outcome in lung cancer patients treated with surgery. BMC Pulm. Med. 2022, 22, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.-H.; Bhoo-Pathy, N.; Ng, K.-L.; Jabir, R.S.; Tan, G.-H.; See, M.-H.; Jamaris, S.; A Taib, N. Utility of pre-treatment neutrophil–lymphocyte ratio and platelet–lymphocyte ratio as prognostic factors in breast cancer. Br. J. Cancer 2015, 113, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Huszno, J.; Kołosza, Z.; Mrochem-Kwarciak, J.; Telka, E.; Jochymek, B.; Miszczyk, L. Role of neutrophil-lymphocyte ratio, platelet-lymphocyte ratio, lymphocyte-monocyte ratio and platelets in prognosis of patients with prostate cancer. Oncol. Lett. 2022, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Zhu, X.; Lin, Z.; Zeng, M.; Shi, P.; Cao, Y.; Chen, F. Compare the Diagnostic and Prognostic Value of MLR, NLR and PLR in CRC Patients. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef]
- Ursu, R.G.; Luchian, I.; Ghetu, N.; Costan, V.V.; Stamatin, O.; Palade, O.D.; Damian, C.; Iancu, L.S.; Porumb-Andrese, E. Emerging Oncogenic Viruses in Head and Neck Cancers from Romanian Patients. Appl. Sci. 2021, 11, 9356. [Google Scholar] [CrossRef]
- Ursu, R.G.; Danciu, M.; Spiridon, I.A.; Ridder, R.; Rehm, S.; Maffini, F.; McKay-Chopin, S.; Carreira, C.; Lucas, E.; Costan, V.-V.; et al. Role of mucosal high-risk human papillomavirus types in head and neck cancers in Romania. PLOS ONE 2018, 13, e0199663. [Google Scholar] [CrossRef]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [Google Scholar] [CrossRef]
Table 1.
NLR, PLR and MLR, predictive and prognostic biomarkers in HNC.
| Investigated ratio(s) as biomarker(s) | Anatomical site of cancer/hystology | Number of case | Results/conclusion | Cuoff value(s) | Reference |
|---|---|---|---|---|---|
| NLR, PLR, LMR, monocyte-to-white blood cell ratio (MWR) | laryngeal carcinoma | 50 | NLR, PLR, LMR, and MWR could be used as prognostic and diagnostic markers in laryngeal cancer; their combination increases the accuracy of the prediction. | Li et al., 2022 | |
| NLR, PLR | not specified | 170 hystological confirmed cases+80 case in control group | Increased NLR and PLR values is correlated with poor prognostic | Seetohul et al., 2019 | |
| NLR, PLR | laryngeal squamous cell carcinoma | 290 | preoperative NLR and PLR can be prognostic markers, the accuracy increases if they are used in combination | 2,22 for NLR and 114 for PLR | Tu et al., 2018 |
| NLR | nasopharyngeal carcinoma | 190 | A high NLR is identified as a poor prognostic factor for nasopharyngeal cancer in Taiwan | 3,6 | Liao et al., 2018 |
| NLR, PLR, MLR, systemic immune inflammation (SII) index | HPV-Related and HPV-Unrelated Oropharyngeal Cancer | 127 | Studied immune ratios could be stratification factors in both HPV− and HPV+ cases | NLR >2,13, SII >448 for OS andNLR >2.29), SII >462.58 for DFS | Brewczyński et al., 2021 |
| NLR | HNSCC | 25 studies in 24 articles, 1536 cases | pretreatment NLR values below 2 and above 6 could be more conclusive biomarkers of prognosis | NLR < 2, 2 to 6, and ≥ 6 | Cho et al., 2018 |
| NLR, PLR | HNSCC | 28 cohorts involving 6847 cases | high pretreatment NLR predicted poor OS, DFS and cancer specifical survival. PLR not associated with OS or DFS | Yang et al., 2019 | |
| NLR, MLR, PLR, alkaline phosphatase (ALP) and l actate dehydrogenase (LDH) | laryngeal squamous cell carcinoma | 361 | elevated preoperative NLR, PLR, MLR and ALP are predictors of worst survival; NLR and postoperative MLR were identified as independent prognostic markers | Chen et al., 2018 | |
| NLR | nasopharyngeal carcinoma | 463 | A value off NLR=3 is an independent poor prognostic factor | 3 | Setakornnukul et al., 2021 |
| NLR, PLR | head and neck cancer patients treated with (chemo-) radiation | 186 | Higher NLR is associated with OS but not associated with recurrence-free survival (LRFS), distant recurrence-free survival (DRFS), and acute toxicity acita de grad ≥ 2; PLR was not correlated with outcome or toxicity | Bojaxhiu et al., 2016 | |
| NLR | HNSCC | 3770 | Elevated NLR predicts worse outcomes | Takenaka et al., 2017 | |
| Platelet count and PLR | HNSCC | 8 studies including 4096 patients and 9 studies including 2327 patients | Elevated platelet count and PLR are associated with poor prognosis | Takenaka et al., 2018 | |
| NLR | HNSCC | 14 studies involving 929 | The NLR predicts treatment results in immune checkpoint inhibitors (ICIs) | Takenaka et al., 2022 | |
| NLR | HNSCC | 24 articles and 6479 cases | An elevated NLR is a predictor for a poor OS | Mascarella et al., 2018 | |
| NLR, PLR | HNSCC | 273 | PLR and NLR independent predictors of mortality and recurrence respectively | Rassouli et al., 2015 | |
| NLR, PLR | HNSCC | 156 | NLR higher than the threshold is associated with an unfavorable evolution. NLR is an independent predictor of five-year overall survival. Neither PLR nor NLR are correlated with tumor recurrence | NLR =3,9 | Szilasi et al., 2020 |
| lymphocyte-to-monocyte ratio (LMR) | HNSCC | 4260 | An elevated LMR may be a predictor of favorable prognosis | Tham et al., 2018 | |
| LMR | HNC | 1431 | Dynamic delta-LMR during radiotherapy is a simple and inexpensive marker for freedom from metastasis and OS | Lin et al. 2020 | |
| NLR,PLR | paranasal sinus | 215 | NLR and PLR are independent prognostic factors of DFS. Higher pretreatment NLR and PLR are related to poor prognosis. | NLR =2.6; PLR =156.9 | Turri-Zanoni et al., 2017 |
| Fibrinogen (F) and NLR; F-NLR score | hypopharyngeal carcinoma | 111 | F-NLR score could stratify patients into prognostic groups | Kuwahara et al., 2018 | |
| NLR, MLR | early-stage (T1-T2) oral squamous cell carcinoma (OSCC) of the tongue | 102 | NLR, MLR indepnednt predictor of o | NLR=2,96 | Ventura et al., 2021 |
| NLR, PLR | laryngeal cancer. | 5716 patients from 20 studies | higher NLR predict poor PFS and os and higher PLR predict poor OS | Hu et al., 2022 | |
| NLR, PLR, NLR/PLR relationship | Laryngeal carcimoma | 5716 patients from 20 studies | NLR is associated with poor OS, PFS, and DFS; Higher PLR is a marker of poor OS | Hu et al., 2022 |
Table 2.
Heatmap including NLR, PLR, MLR and OS data for 39 cases included in the study.
| NLR | PLR | MLR | OS (months) |
|---|---|---|---|
| 2.07 | 110.71 | 0.36 | 12 |
| 2.74 | 83.69 | 0.41 | 6 |
| 1.25 | 74.06 | 0.14 | 15 |
| 1.24 | 61.63 | 0.22 | 42 |
| 4.57 | 201.55 | 0.46 | 4 |
| 3.03 | 127.91 | 0.39 | 15 |
| 1.83 | 78.98 | 0.22 | 23 |
| 4.44 | 244.14 | 0.78 | 3 |
| 15.50 | 139.58 | 0.76 | 78 |
| 2.51 | 188.72 | 0.22 | 6 |
| 2.01 | 183.14 | 0.18 | 6 |
| 1.88 | 88.63 | 0.14 | 4 |
| 1.48 | 70.43 | 0.13 | 18 |
| 8.91 | 142.34 | 0.81 | 13 |
| 1.40 | 88.44 | 0.18 | 37 |
| 5.04 | 379.33 | 0.23 | 11 |
| 2.36 | 182.23 | 0.14 | 9 |
| 1.67 | 89.63 | 0.12 | 13 |
| 31.85 | 392.75 | 0.73 | 7 |
| 4.33 | 160.91 | 0.34 | 1 |
| 3.71 | 107.14 | 0.43 | 11 |
| 2.56 | 170.00 | 0.19 | 8 |
| 8.61 | 146.50 | 1.00 | 11 |
| 7.31 | 327.94 | 0.84 | 11 |
| 2.75 | 111.71 | 0.33 | 13 |
| 1.39 | 143.59 | 0.30 | 17 |
| 1.37 | 201.34 | 0.46 | 21 |
| 9.22 | 247.59 | 0.60 | 16 |
| 2.97 | 118.70 | 0.30 | 3 |
| 6.98 | 214.29 | 0.85 | 45 |
| 2.69 | 331.18 | 0.15 | 11 |
| 69.00 | 1775.00 | 5.50 | 1 |
| 1.63 | 117.50 | 0.25 | 3 |
| 4.10 | 155.69 | 0.45 | 3 |
| 2.78 | 87.04 | 0.37 | 120 |
| 4.74 | 174.14 | 0.50 | 69 |
| 4.96 | 131.37 | 0.56 | 3 |
| 2.34 | 137.21 | 0.30 | 8 |
| 3.56 | 136.92 | 0.38 | 17 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



