
Submitted:
18 July 2023
Posted:
19 July 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background:
COVID-19 vaccines have been a game changer in the pandemic, their extensive use was favorable compared to the burden of COVID-19 complications. Despite the low incidence of complications, it was important to analyze them carefully to understand the underlying mechanisms and predisposing factors. For instance, myopericarditis especially from mRNA vaccines, and its relatively higher prevalence in young adults and adolescents has raised a public concern about the use of this vaccine in this group. We aimed through this review to compare the age likelihood of ADEM from COVID-19 vaccines, with that reported in myopericarditis cases; secondary outcome parameters included the gender and number of doses needed to induce COVID-19 vaccines related ADEM.
Methodology:
A literature search has been conducted on relevant databases to retrieve all case reports/series and systematic reviews describing ADEM with possible linkage to COVID-19. Exclusion criteria included any report not including the desired outcome parameters. Our results were then qualitatively compared with a similar systematic review reporting myopericarditis from COVID-19 vaccines.
Results:
In 38 cases with ADEM, mean age was 49±16 compared to 25±14 in myopericarditis, females were more likely to be affected, and while most of myopericarditis cases develop after the second dose, most of ADEM cases develop after the first dose (76%). Moreover, age>56 years was more predictive of negative outcome after ADEM in the form of death or permanent vegetative state.
Conclusion:
The discrepancy in age, gender and number of doses needed to induce complications between ADEM and myopericarditis, signify that the tissue affected is the major orchestrator of the age, gender, and dose characteristics, and not the type of vaccines. A leakier blood brain barrier with aging, might allow easier passage of autoantibodies and cytokines into the brain while lack of inhibitory immune checkpoints in the myocardium in young age might explain the higher prevalence of those cases in young adults and adolescents.
Keywords:
ADEM
; COVID-19 VACCINES
; MYOPERICARDITIS
; IMMUNE CHECK POINTS
Background:
There has been a dilemma in the diversified sequelae of post-COVID-19 (coronavirus disease 2019) mRNA (messenger Ribonucleic acid) vaccinations. Although most of the outcomes are satisfactory, and vaccination benefits outweighs the risk, there have been some case reports that intrigued further analysis. A study conducted by Minghui Li et al assessed the incidence rate of myocarditis and pericarditis following COVID-19 vaccination in the United States in perspective to age group and vaccine type.(1) It was found that the rates of myocardial affection are more prevalent in adolescents and young adults than in older age groups while using the mRNA vaccines. As the reporting odds ratio (ROR) of BNT162b2 (Pfizer-Biontech) and mRNA-1273 (Moderna) vaccine subtypes were higher than the ROR of viral vector vaccines of Ad26.COV2. S (Janssen), 5.3, 2.91 and 1.39 respectively. Another study supports the outcomes of mRNA vaccination post-COVID-19 in youths. A retrospective study was implemented by Dongngan T. Truong et al, and the results of the collected data on patients <21 years old following mRNA vaccination were significant.(2) The incidence of suspected myocarditis in younger patients was noticeable.
The affection of young age by postvaccine myocarditis, has not only be observed with mRNA vaccines; as myocardial and pericardial complications can also occur in young age groups following the smallpox vaccine, not only after the COVID-19 mRNA vaccine. This can be supported by an observational cohort study conducted by Engler et al, where the outcomes of smallpox vaccines were elaborated.(3) 348 individuals out of over 5000 case reports that showed side effects post smallpox vaccination, manifested with cardiological adversities such as myocarditis and pericarditis: 276 and 72 cases respectively. The median age of the myopericarditis cases was 24 years old, emphasizing the prevalence of myocarditis post-vaccination in the younger segment of the age spectrum, irrespective to vaccination subtype.
This young age trend for postvaccine myocarditis, regardless of the type of vaccine, is poorly understood.
In contrast, postvaccine acute disseminated encephalomyelitis (ADEM), tend to occur in a relatively older age. A report by Huynh and colleagues illustrated a case of 61-year-old male with ADEM following influenza vaccine, while Nakamura et al documented two adult cases aged 62 and 70 with post-influenza vaccine ADEM (4,5). The rest of systematic reviews were mainly focused on postvaccine neurologic sequelae overall and not specifically targeting the specific age of ADEM following different types of vaccines. In addition most of the studies assessing postvaccine ADEM, cannot be reliably cited as the involved vaccines are exclusive childhood compulsory vaccines, thus they cannot reflect the true age trend of postvaccine ADEM. (6,7)
It seems, from the above that age likelihood of postvaccine tissue affection, might be related to the tissue characteristics rather than to the vaccine type. For this purpose, we dedicate this systematic review, to study the age likelihood of acute disseminated encephalomyelitis (ADEM), post-COVID-19 vaccination specifically post-mRNA COVID-19 vaccines. We hypothesize that we might find a discrepancy between the mean age of ADEM cases reported after COVID-19 vaccines compared to myocarditis seen after the same vaccines. The latter finding might consolidate our initial impression that tissue characteristics might be closely tied to the age predilection of postvaccination immune sequelae in the respective tissue.
Methodology:
Inclusion and Exclusion Criteria for Literature Search
A literature search was implemented on PubMed, Scopus, Google scholar and Web of science to identify studies using the following key words ADEM and COVID-19 vaccination. The bibliography of any identified study was clearly inspected to find any report that could have been missed during the initial computer run.
Inclusion criteria included any age, developing ADEM after COVID-19 vaccination, accepted type of studies were systematic reviews, case reports, and case series.
Studies not fulfilling the outcome parameters targeted by the study were excluded.
Outcome Parameters:
Three of the authors examined each study for the following outcome parameters: age, gender, type, and dose of the vaccine incriminated, the time interval between the vaccination and the development of ADEM, the main neurologic presentation, the treatment lines used, and the outcome of the case.
Statistical Analysis:
Data collected were analysed using Excel and MedCalc statistical software. Numerical data were represented using mean and standard deviation when normally distributed and using median, minimum, and maximum when non-normally distributed. Non-recovery was defined as persistence of neurologic abnormalities, vegetative state or death in our collected cases, this categorical division was essential to perform a Receiver Operating Characteristic analysis (ROC) to determine the cut-off age predicting non-recovery from ADEM developing from COVID-19 vaccines. The latter was represented using an interactive dot diagram.
Results:
A systematic review has been identified (8) including 20 studies, out of which 19 were eligible to be included in our review: (9,10,19–27,11–18) (Figure 1)
In addition to the 19 studies included, our literature search has identified nine other studies: (28–35). Thus, a total of 28 studies were analysed comprising a total of 38 cases. (Table 1). Most of the cases were attributed to the adenoviral vector vaccines (63%).
ADEM occurred following the first dose of vaccination (76%), with a median interval of 14 after vaccination (Table 2).
The oldest age seen in ADEM cases following vaccination was seen in patients receiving mRNA vaccines (57±19) compared to a mean of 48±14 following adenoviral vector vaccines.
Complete recovery was observed in 37% of patients, while non-recovery (defined as residual motor deficit or the development of vegetative state) or death was observed in a total of 45% of cases (Table 2).
Receiver operating characteristic analysis illustrated as an interactive dot diagram showed that an age>56, predicts non-recovery in ADEM cases following post-COVID-19 vaccines. (Figure 2)
Treatment received were mainly steroids (oral and pulse intravenous), intravenous immunoglobulins, plasma exchange. While only three cases received rituximab (8%), and one received eculizumab and another one receives cyclophosphamide (3%) (Table 1)
Table 1 illustrates the details of each case in the included cases and case reports.
Discussion:
Our review describes the demographic, and clinical characteristics of a rare complication of COVID-19 vaccines. It is the second systematic review of reported cases in this context, after Nabizadeh et al study(8), however with a different aim. The aim of our systematic review was mainly to study the differences of age predisposition, type of vaccine and number of doses between myocarditis and ADEM following COVID-19 vaccines. Several major differences were observed, notably the number of literature reports, which points to a relatively higher incidence of myocarditis as our group could only find 28 reports with a total of 38 cases compared to thousands of cases of myopericarditis in the literature; this can make the comparison between the two complications flawful, as the scarcity of ADEM reports is not very helpful to draw solid conclusions.
However, we still decided to compare the aforementioned outcome parameters across the two complications. We took Goyal et al study as a reference for myopericarditis cases as it shares the different outcome parameters intended in our study, and it is not a VAERS based study; thus, its results can be qualitatively compared to the results of our research. (36)
Age of clustered ADEM cases was 49±16 compared to 25±14 in myopericarditis cases. The young age of myopericarditis especially from mRNA vaccines, lead to fears among parents, planning to vaccinate their children using these vaccines, and led to an overall impression that mRNA vaccines might be associated with increased complications’ rate at the young age. Our study contradicts this false belief, as it clearly shows that ADEM occurring from mRNA vaccines is likely to occur in older age groups compared to myocarditis and to ADEM cases from other COVID-19 vaccines. Nevertheless, older age was also predictive of worst outcomes in our collected cases (Figure 2), patients older than 56 were more prone to develop residual neurologic deficit, vegetative state, or death. This might also mean that age likelihood and other demographic characteristics of any vaccine complication are related to the type of the complication and tissue involved rather than the vaccine type.
One of the theories that can explain the young age of myocarditis from COVID-19 and other vaccines (such as vaccinia virus vaccine used for smallpox) is the mechanism of immune inhibition inside the myocardium. The heart muscle harbours a strict system for immune surveillance, that can prevent any immune-mediated damage, this immune surveillance is particularly important in the heart as the regenerative capacity of myocardial cells is absent.
Two main mechanisms of peripheral tolerance protect myocytes from T cell damage namely cytotoxic T-lymphocyte-associated protein-4 (CTLA4), and Programmed cell protein death-1 (PD1). CTLA4 and PD1 block T cell activation by binding to CD-28 receptors on the surface of T cells, thereby preventing any viral antigen from its activation. (37) The myocardial protection from autoimmunity, offered by inhibitory immune checkpoints, such as PD1, is upregulated by aging, which might mean that the susceptibility of myocardium to immune-mediated inflammation, should decrease with aging. (38) On another note, antibodies implicated in CNS autoimmune inflammation, must gain access to the CNS via the blood brain barrier, olfactory route, or blood-cerebrospinal fluid barrier, or sometimes produced locally witing the CNS itself. The latter mechanism has been particularly of focus in multiple sclerosis, as Quintana and colleagues proved the present of myelin reactive antibodies that are locally produced in the brain. There also hypotheses that post-infectious ADEM, which is intriguingly common in the pediatric age group, involves the local production of antibodies in the CNS against viral antigen entering the CNS through the olfactory route. But, for antibodies, to gain access to the CNS, this implies a leakier BBB Blood brain barrier) or BCSFB (Blood cerebrospinal fluid barrier), this can be understandable in post-infectious ADEM, where implicated micro-organisms weaken the tight junctions of the BBB, and this allows access of cross-reactive antibodies to the brain (39); but this cannot be the case in post-vaccination ADEM, as no offending organism is present to play this synergistic getaway role. An explanation for antibody access to the CNS in post-vaccination ADEM, is aging. If aging protects the myocardium against autoimmunity, it plays an inverse role in the CNS by rendering the BBB and BCSFB more permeable to antibodies and to external antigens. (40)
Back to the findings, of our study, which also showed that ADEM mainly occurs after the first dose of vaccination, this is different than the immune-priming pattern seen in myocarditis from COVID-19 vaccines, as they need two doses usually to produce this complication.
This pattern might be consistent with a cytokine rather than immune-mediated damage. Wu et al described a subtype of ADEM known as acute necrotizing encephalitis which involves a personal susceptibility to CNS damage due to hypercytokinemia. (41)
Finally, yet importantly female patients were more likely to develop ADEM following COVID-19 vaccination compared to male patients. A study by Falahi et al, examined COVID-19 outcomes across both genders, and showed that female patients have a higher susceptibility to cytokine storm, and suggested that estrogen upregulates pro-inflammatory molecules, leading to an augmented inflammatory response in females. This might consolidate the impression taken from dose pattern of post-COVID-19 vaccination ADEM, that it is mainly mediated via hypercytokinemia rather than auto-antibodies. (42)
Figure 3 summarizes the differences outlined above between ADEM and myopericarditis developing following COVID-19 vaccines in view of our findings compared to the findings of Goyal et study. (36)
Conclusion:
This review compares the demographic, vaccine types and dose characteristics of post-COVID-19 vaccines ADEM and Post-COVID-19 vaccines myopericarditis. Older age, predominance of female gender, and first dose implication all characterize ADEM compared to myopericarditis. And despite the rarity of these complications, they open new horizons in understanding post-vaccination complications and their underlying mechanisms. They might signify that aging can be protective against autoimmunity in the myocardium, but the same aging can jeopardize the BBB, rendering it more susceptible to delivery of antibodies and cytokines to the CNS. More studies at the molecular level, should be implemented to confirm these findings and to prove that vaccine complications are not only determined by the vaccine type but also by the type of the target tissue. The findings highlighted by our study, can wipe out the public-based impression that mRNA vaccines are linked to higher complications in younger individuals, and can help in combating vaccine hesitancy especially towards a vaccine mechanism that might be very promising in the future for other infectious and non-infectious disorders.
Risk of Bias assessment has been performed and illustrated in Figure 4:
Author Contributions
Conceptualization, AA, NK, HG.; methodology, AA, AK, AB, LM, HG, YH, HH, RS, NK.; software, AA, AK, AB, LM, HG, YH, HH, RS, NK ; investigation, AA, AK, AB, LM, HG, YH, HH, RS, NK; resources, AA, AK, AB, LM, HG, YH, HH, RS, NK, data curation, AA, AK, AB, LM, HG, YH, HH, RS, NK; writing—original draft preparation, AA, AK, AB, LM, HG, YH, HH, RS, NK; writing—review and editing, AA, AK, AB, LM, HG, YH, HH, RS, NK; supervision, AA, NK, HG; project administration, AA, NK, HG; funding acquisition, (none). All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
not applicable as this study is a systematic review of the reported cases.
Informed Consent Statement
not applicable as this study is a systematic review of the reported cases.
Data Availability Statement
Data is made available upon request to the corresponding author.
Acknowledgments
I wanted, as a first author, to dedicate this work to anyone who is considered as a “black sheep” in his workplace, college or school environment, just because he is beautifully different. We all, through different stages of our life, have gone through similar, difficult times, where we felt alone and non-appreciated, but you should know that your personal worth is unrelated to others’ perception.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| Ad26.COV2. | Janssen vaccine |
| ADEM | Acute Disseminated Encephalomyelitis |
| BBB | Blood brain Barrier |
| BBIBP-CorV | Sinopharm |
| BCSFB | Blood cerebrospinal fluid barrier |
| BNT162b2 | Pfizer Biontech vaccine |
| CD | Cluster of differentiation |
| CNS | Central nervous system |
| CoronaVac | Sinovac |
| Covax | Coronavirus vaccine initiative |
| COVID-19 | Coronavirus Disease 2019 |
| CTLA4 | cytotoxic T-lymphocyte-associated protein-4 |
| DCL | Disturbed Conscious level |
| Gam-COVID-Vac | Sputnik Vaccine |
| GCS | Glasgow Coma Scale |
| IV | Intravenous |
| LL | Lower Limb |
| MP | Methylprednisolone |
| mRNA | Messenger Ribonucleic acid |
| mRNA | Messenger Ribonucleic acid |
| mRNA-1273 | Moderna Spikevax vaccine |
| NR | Not reported |
| PD-1 | Programmed Death ligand 1 |
| PP | Plasmapheresis |
| VAERS | Vaccine adverse events Reporting system |
References
- Li, M.; Yuan, J.; Lv, G.; Brown, J.; Jiang, X.; Lu, Z.K. Myocarditis and Pericarditis following COVID-19 Vaccination: Inequalities in Age and Vaccine Types. J Pers Med 2021, 11, 1106. Available online: https://www.mdpi.com/2075-4426/11/11/1106. [CrossRef]
- Truong, D.T.; Dionne, A.; Muniz, J.C.; McHugh, K.E.; Portman, M.A.; Lambert, L.M.; et al. Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults: Suspected Myocarditis After COVID-19 Vaccination. Circulation 2022, 145, 345–356. [Google Scholar] [CrossRef]
- Engler, R.J.M.; Nelson, M.R.; Collins Jr, L.C.; Spooner, C.; Hemann, B.A.; Gibbs, B.T.; et al. A Prospective Study of the Incidence of Myocarditis/Pericarditis and New Onset Cardiac Symptoms following Smallpox and Influenza Vaccination. Horwitz MS, editor. PLoS ONE 2015, 10, e0118283. Available online: https://dx.plos.org/10.1371/journal.pone.0118283. [CrossRef] [PubMed]
- Nakamura, N.; Nokura, K.; Zettsu, T.; Koga, H.; Tachi, M.; Terada, M.; et al. Neurologic Complications Associated with Influenza Vaccination: Two Adult Cases. Intern Med 2003, 42, 191–194. Available online: http://www.jstage.jst.go.jp/article/internalmedicine1992/42/2/42_2_191/_article. [CrossRef] [PubMed]
- Huynh, W.; Cordato, D.J.; Kehdi, E.; Masters, L.T.; Dedousis, C. Post-vaccination encephalomyelitis: Literature review and illustrative case. J Clin Neurosci 2008, 15, 1315–1322. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0967586808001896. [CrossRef]
- Sejvar, J.J. Neurologic Adverse Events Associated With Smallpox Vaccination in the United States, 2002-2004. JAMA 2005, 294, 2744. Available online: http://jama.jamanetwork.com/article.aspx?doi=10.1001/jama.294.21.2744. [CrossRef]
- Williams, S.E.; Pahud, B.A.; Vellozzi, C.; Donofrio, P.D.; Dekker, C.L.; Halsey, N.; et al. Causality assessment of serious neurologic adverse events following 2009 H1N1 vaccination. Vaccine 2011, 29, 8302–8308. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21893148. [CrossRef]
- Nabizadeh, F.; Noori, M.; Rahmani, S.; Hosseini, H. Acute disseminated encephalomyelitis (ADEM) following COVID-19 vaccination: A systematic review. J Clin Neurosci 2023, 111, 57–70. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0967586823000668. [CrossRef]
- Miyamoto, K.; Koh, J.; Takahashi, M.; Niwa, M.; Ito, H. A case of anti-MOG antibody-positive ADEM following COVID-19 mRNA vaccination. Neurol Sci 2022, 43, 3513–3514. Available online: https://link.springer.com/10.1007/s10072-022-06019-6. [CrossRef]
- Ballout, A.A.; Babaie, A.; Kolesnik, M.; Li, J.Y.; Hameed, N.; Waldman, G.; et al. A Single-Health System Case Series of New-Onset CNS Inflammatory Disorders Temporally Associated With mRNA-Based SARS-CoV-2 Vaccines. Front Neurol 2022, 13, 796882. Available online: http://www.ncbi.nlm.nih.gov/pubmed/35280277. [CrossRef] [PubMed]
- Al-Quliti, K.; Qureshi, A.; Quadri, M.; Abdulhameed, B.; Alanazi, A.; Alhujeily, R. Acute Demyelinating Encephalomyelitis Post-COVID-19 Vaccination: A Case Report and Literature Review. Diseases 2022, 10, 13. Available online: https://www.mdpi.com/2079-9721/10/1/13. [CrossRef]
- Yazdanpanah, F.; Iranpour, P.; Haseli, S.; Poursadeghfard, M.; Yarmahmoodi, F. Acute disseminated encephalomyelitis (ADEM) after SARS- CoV-2 vaccination: A case report. Radiol case reports 2022, 17, 1789–1793. Available online: http://www.ncbi.nlm.nih.gov/pubmed/35355527. [CrossRef]
- Permezel, F.; Borojevic, B.; Lau, S.; de Boer, H.H. Acute disseminated encephalomyelitis (ADEM) following recent Oxford/AstraZeneca COVID-19 vaccination. Forensic Sci Med Pathol 2022, 18, 74–79. Available online: https://link.springer.com/10.1007/s12024-021-00440-7. [CrossRef] [PubMed]
- Vogrig, A.; Janes, F.; Gigli, G.L.; Curcio, F.; Del Negro, I.; D’Agostini, S.; et al. Acute disseminated encephalomyelitis after SARS-CoV-2 vaccination. Clin Neurol Neurosurg 2021, 208, 106839. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0303846721003681. [CrossRef]
- Ahmad, H.R.; Timmermans, V.M.; Dakakni, T. Acute Disseminated Encephalomyelitis After SARS-CoV-2 Vaccination. Am J Case Rep 2022, 23, e936574. Available online: https://www.amjcaserep.com/abstract/index/idArt/936574. [CrossRef] [PubMed]
- Cao, L.; Ren, L. Acute disseminated encephalomyelitis after severe acute respiratory syndrome coronavirus 2 vaccination: A case report. Acta Neurol Belg 2022, 122, 793–795. Available online: https://link.springer.com/10.1007/s13760-021-01608-2. [CrossRef] [PubMed]
- Simone, A.M.; Monti, G.; Amidei, S.; Costa, M.; Vaghi, L.; Devetak, M.; et al. Acute disseminated encephalomyelitis associated with anti-myelin oligodendrocyte glycoprotein (MOG-IGG) antibody in a patient with recent vaccination against SARS-CoV-2. J Neurol Sci 2021, 429, 118167. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0022510X21008637. [CrossRef]
- Lazaro, L.G.; Perea Cossio, J.E.; Luis, M.B.; Tamagnini, F.; Paguay Mejia, D.A.; Solarz, H.; et al. Acute disseminated encephalomyelitis following vaccination against SARS-CoV-2: A case report. Brain, Behav Immun - Heal 2022, 20, 100439. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2666354622000291. [CrossRef]
- Kania, K.; Ambrosius, W.; Tokarz Kupczyk, E.; Kozubski, W. Acute disseminated encephalomyelitis in a patient vaccinated against SARS-CoV-2. Ann Clin Transl Neurol 2021, 8, 2000–2003. Available online: https://onlinelibrary.wiley.com/doi/10.1002/acn3.51447. [CrossRef]
- Nagaratnam, S.A.; Ferdi, A.C.; Leaney, J.; Lee, R.L.K.; Hwang, Y.T.; Heard, R. Acute disseminated encephalomyelitis with bilateral optic neuritis following ChAdOx1 COVID-19 vaccination. BMC Neurol 2022, 22, 54. Available online: https://bmcneurol.biomedcentral.com/articles/10.1186/s12883-022-02575-8. [CrossRef]
- Ozgen Kenangil, G.; Ari, B.C.; Guler, C.; Demir, M.K. Acute disseminated encephalomyelitis-like presentation after an inactivated coronavirus vaccine. Acta Neurol Belg 2021, 121, 1089–1091. Available online: http://www.ncbi.nlm.nih.gov/pubmed/34018145. [CrossRef]
- Rinaldi, V.; Bellucci, G.; Romano, A.; Bozzao, A.; Salvetti, M. ADEM after ChAdOx1 nCoV-19 vaccine: A case report. Mult Scler J 2022, 28, 1151–1154. Available online: http://journals.sagepub.com/doi/10.1177/13524585211040222. [CrossRef] [PubMed]
- Mumoli, L.; Vescio, V.; Pirritano, D.; Russo, E.; Bosco, D. ADEM anti-MOG antibody-positive after SARS-CoV2 vaccination. Neurol Sci 2022, 43, 763–766. Available online: https://link.springer.com/10.1007/s10072-021-05761-7. [CrossRef]
- Shimizu, M.; Ogaki, K.; Nakamura, R.; Kado, E.; Nakajima, S.; Kurita, N.; et al. An 88-year-old woman with acute disseminated encephalomyelitis following messenger ribonucleic acid-based COVID-19 vaccination. eNeurologicalSci 2021, 25, 100381. Available online: http://www.ncbi.nlm.nih.gov/pubmed/34841097. [CrossRef]
- Ancau, M.; Liesche-Starnecker, F.; Niederschweiberer, J.; Krieg, S.M.; Zimmer, C.; Lingg, C.; et al. Case Series: Acute Hemorrhagic Encephalomyelitis After SARS-CoV-2 Vaccination. Front Neurol 2022, 12. Available online: https://www.frontiersin.org/articles/10.3389/fneur.2021.820049/full. [CrossRef] [PubMed]
- Maramattom, B.V.; Lotlikar, R.S.; Sukumaran, S. Central nervous system adverse events after ChAdOx1 vaccination. Neurol Sci 2022, 43, 3503–3507. Available online: http://www.ncbi.nlm.nih.gov/pubmed/35275317. [CrossRef] [PubMed]
- Netravathi, M.; Dhamija, K.; Gupta, M.; Tamborska, A.; Nalini, A.; Holla, V.V.; et al. COVID-19 vaccine associated demyelination & its association with MOG antibody. Mult Scler Relat Disord 2022, 60, 103739. Available online: https://linkinghub.elsevier.com/retrieve/pii/S2211034822002541. [CrossRef]
- Mousa, H.; Patel, T.H.; Meadows, I.; Ozdemir, B. Acute Disseminated Encephalomyelitis (ADEM) After Consecutive Exposures to Mycoplasma and COVID Vaccine: A Case Report. Cureus 2022. Available online: https://www.cureus.com/articles/93548-acute-disseminated-encephalomyelitis-adem-after-consecutive-exposures-to-mycoplasma-and-covid-vaccine-a-case-report. [CrossRef]
- Sazgarnejad, S.; Kordipour, V. Acute disseminated encephalomyelitis following inactivated COVID-19 vaccine: A case report Case presentation: 2022;1–9.
- Gustavsen, S.; Nordling, M.M.; Weglewski, A. Acute disseminated encephalomyelitis following the COVID-19 vaccine Ad26.COV2.S, a case report. Bull Natl Res Cent 2023, 47, 5. Available online: https://bnrc.springeropen.com/articles/10.1186/s42269-023-00981-7. [CrossRef]
- Bastide, L.; Perrotta, G.; Lolli, V.; Mathey, C.; Vierasu, O.I.; Goldman, S.; et al. Atypical acute disseminated encephalomyelitis with systemic inflammation after a first dose of AztraZaneca COVID-19 vaccine. A case report. Front Neurol. 2022, 13. [Google Scholar] [CrossRef]
- Nimkar, S.V.; Yelne, P.; Gaidhane, S.A.; Kumar, S.; Acharya, S.; Gemnani, R.R. Fatal Acute Disseminated Encephalomyelitis Post-COVID-19 Vaccination: A Rare Case Report. Cureus 2022. Available online: https://www.cureus.com/articles/126502-fatal-acute-disseminated-encephalomyelitis-post-covid-19-vaccination-a-rare-case-report. [CrossRef]
- Garg, A.; Batra, P.K.; Gupta, P. Post COVID-19 Vaccination Acute Disseminated Encephalomyelitis: A Case Report. Curr Med Imaging Rev 2023, 19, 91–95. Available online: https://www.eurekaselect.com/204488/article. [CrossRef]
- Raknuzzaman. Post Covid19 Vaccination Acute Disseminated Encephalomyelitis: A Case Report in Bangladesh. Int J Med Sci Clin Res Stud.
- Lohmann, L.; Glaser, F.; Möddel, G.; Lünemann, J.D.; Wiendl, H.; Klotz, L. Severe disease exacerbation after mRNA COVID-19 vaccination unmasks suspected multiple sclerosis as neuromyelitis optica spectrum disorder: A case report. BMC Neurol 2022, 22, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Ray, I.; Mascarenhas, D.; Kunal, S.; Sachdeva, R.A.; Ish, P. Myocarditis post-SARS-CoV-2 vaccination: A systematic review. QJM Int. J. Med. 2023, 116, 7–25. [Google Scholar] [CrossRef] [PubMed]
- Grabie, N.; Lichtman, A.H.; Padera, R. T cell checkpoint regulators in the heart. Cardiovasc Res. 2019, 115, 869–877. [Google Scholar] [CrossRef]
- Platt, M.P.; Agalliu, D.; Cutforth, T. Hello from the Other Side: How Autoantibodies Circumvent the Blood–Brain Barrier in Autoimmune Encephalitis. Front Immunol 2017, 8. Available online: http://journal.frontiersin.org/article/10.3389/fimmu.2017.00442/full. [CrossRef]
- Spindler, K.R.; Hsu, T.-H. Viral disruption of the blood-brain barrier. Trends Microbiol 2012, 20, 282–290. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22564250. [CrossRef]
- No Title.
- Wu, X.; Wu, W.; Pan, W.; Wu, L.; Liu, K.; Zhang, H.-L. Acute necrotizing encephalopathy: An underrecognized clinicoradiologic disorder. Mediators Inflamm 2015, 2015, 792578. Available online: http://www.ncbi.nlm.nih.gov/pubmed/25873770. [CrossRef]
- Falahi, S.; Kenarkoohi, A. Sex and gender differences in the outcome of patients with COVID-19. J Med Virol 2021, 93, 151–152. Available online: https://onlinelibrary.wiley.com/doi/10.1002/jmv.26243. [CrossRef]
Figure 1.
PRISMA 2020 flow diagram for our systematic review to show study selection process.
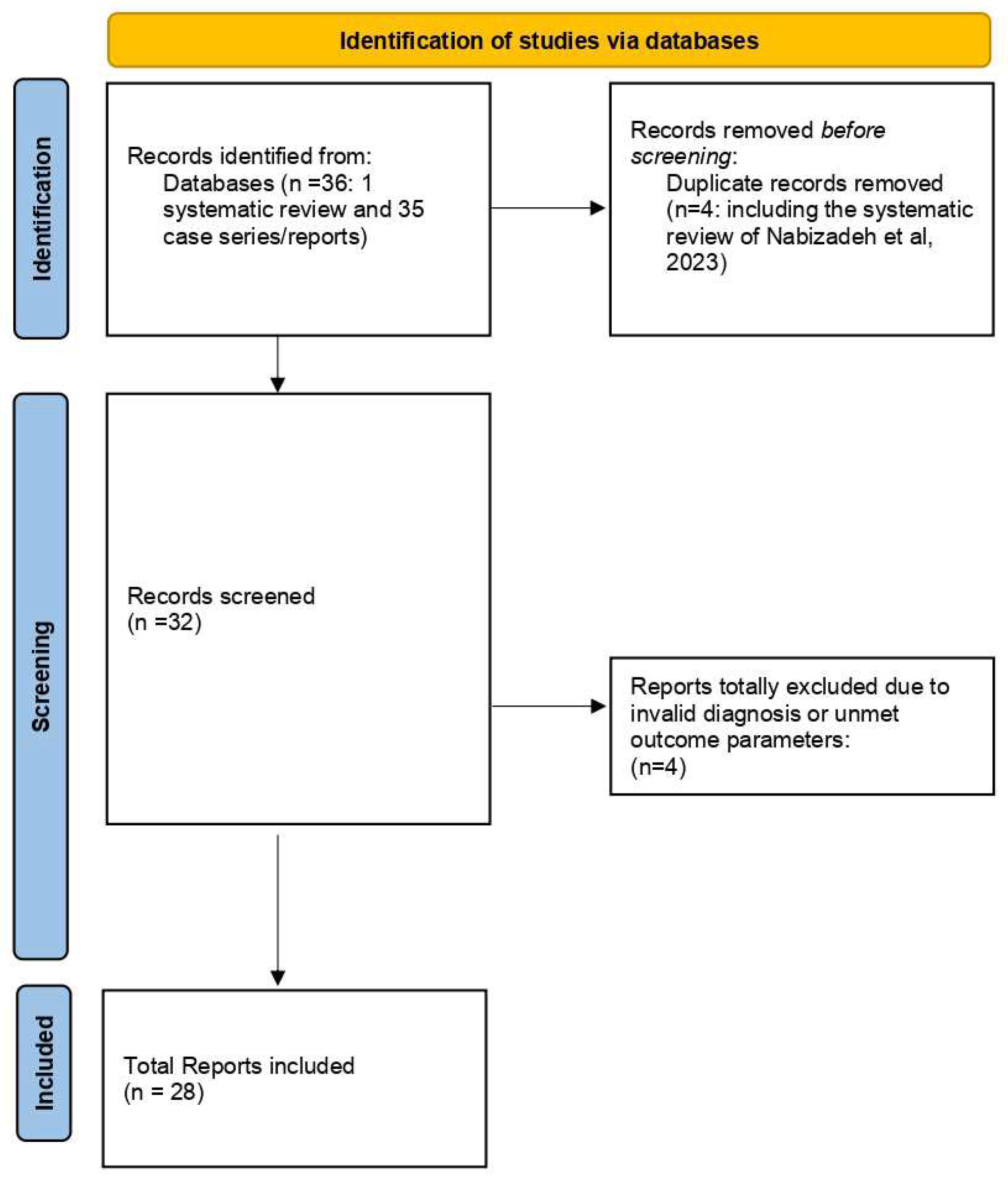
Figure 2.
Interactive dot diagram for illustration of the diagnostic accuracy of age in predicting non-recovery after ADEM post COVID-19 vaccines.
Figure 2.
Interactive dot diagram for illustration of the diagnostic accuracy of age in predicting non-recovery after ADEM post COVID-19 vaccines.
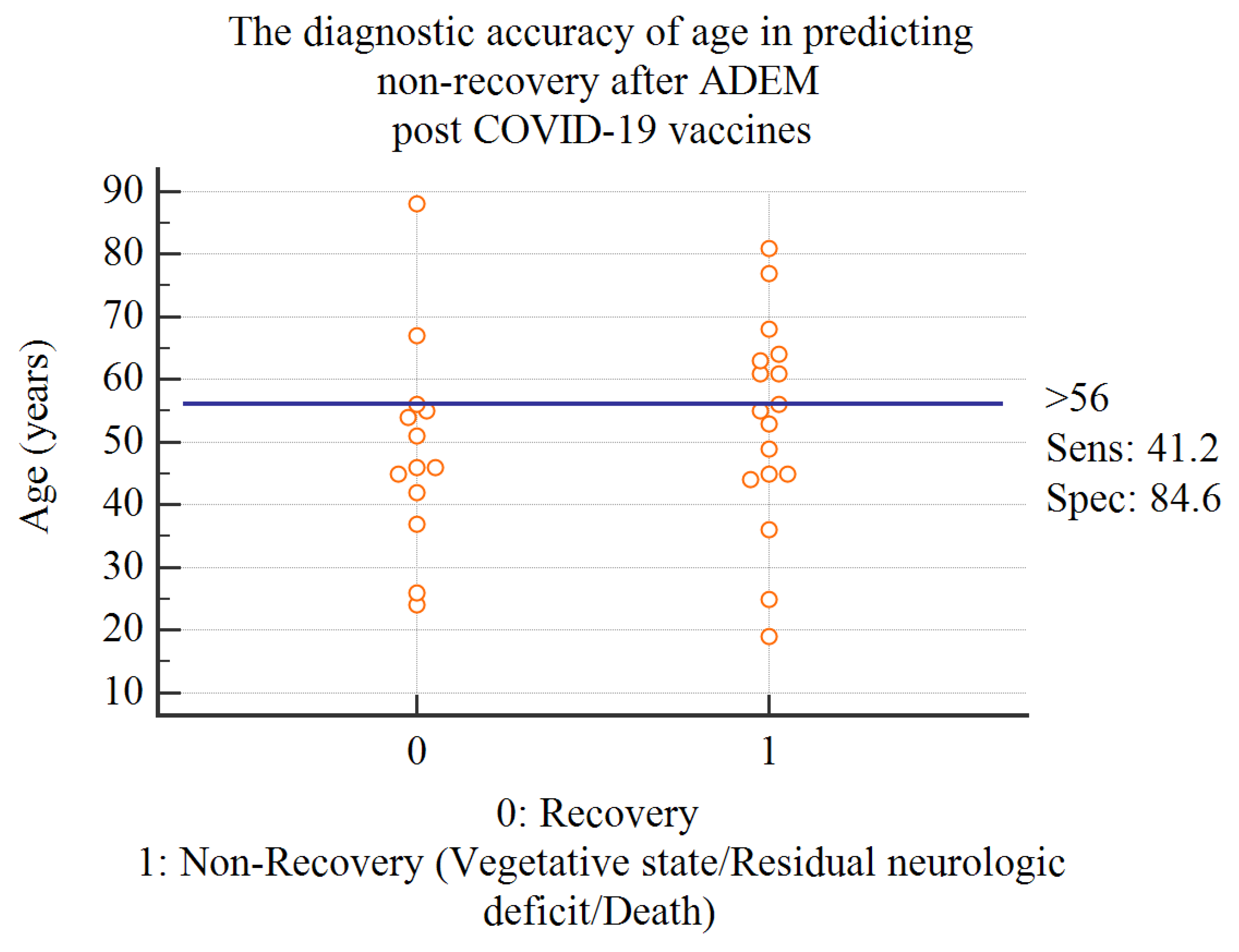
Figure 3.
Summary of Differences between myopericarditis and ADEM cases post-COVID-19 vaccines.
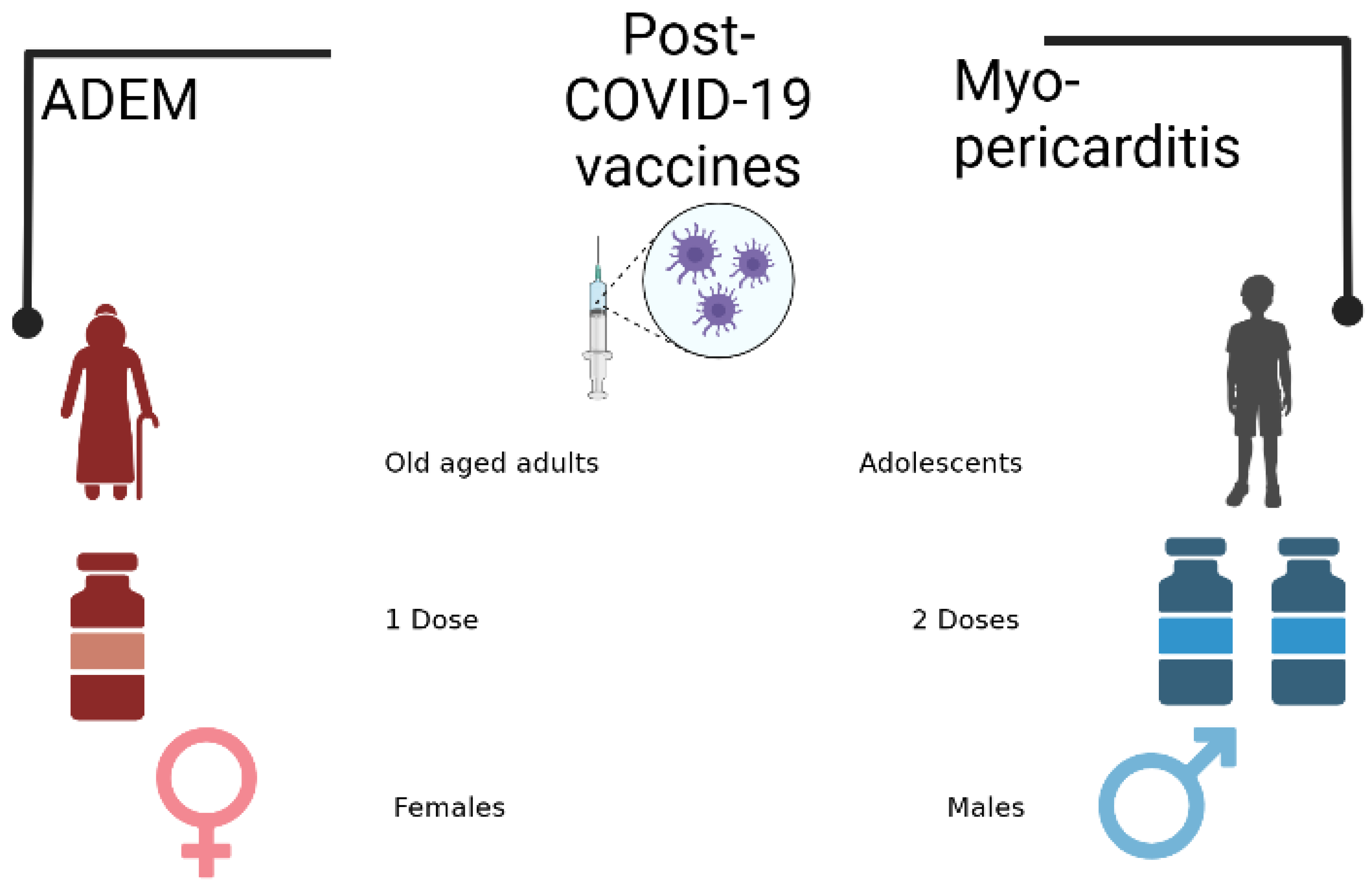
Figure 4.
Bias Assessment in included studies.
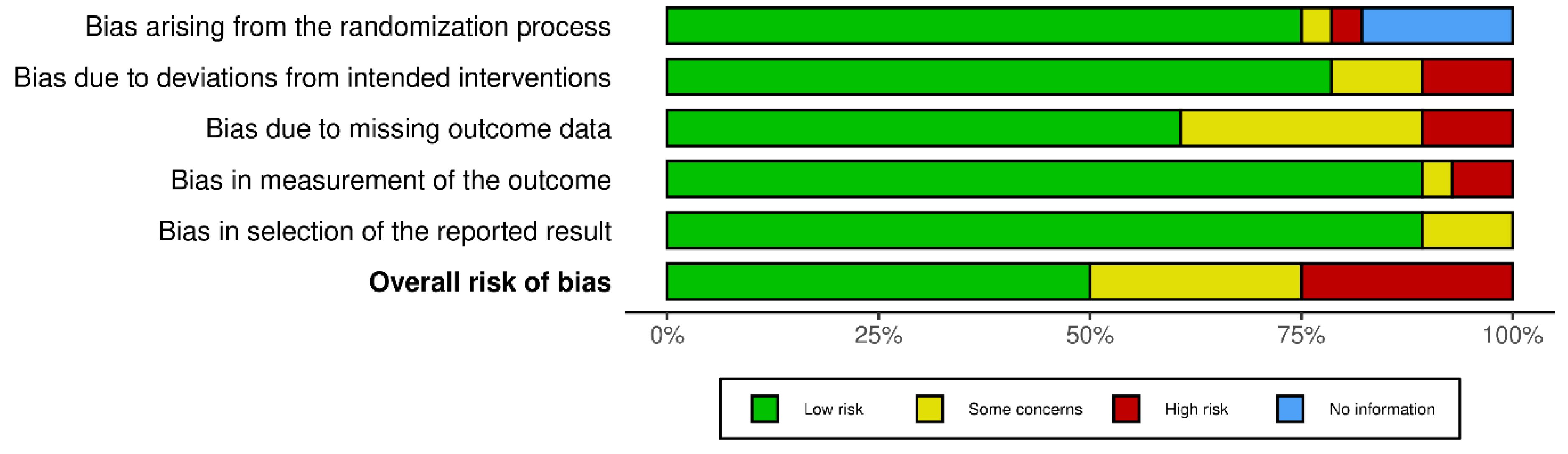

Table 1.
Details of the included cases.
| Report | Age | Main Vaccine Mechanism | Subtype of Vaccine | Interval between Vaccine and Sequelae (days) | Dose Number |
Gender | Clinical Picture | Treatment Received | Recovery/Residual Lesion |
|---|---|---|---|---|---|---|---|---|---|
| (Raknuzzaman n.d, 2021) | 55 | 1 | mRNA (unspecified subtype) | 21 | NR | 2 | Headache, somnolence, fluctuating alertness, and orientation consistent with delirium and convulsions | MP then oral steroids | full recovery |
| (Mousa et al. 2022) | 44 | 1 | mRNA (unspecified subtype) | 6 | 1 | 1 | Blurred vision, DCL, lower limb weakness, impaired sensation, urine retention. | IV, oral steroids and plasmapheresis | Bilateral optic atrophy |
| (Shimizu et al. 2021) | 88 | 1 | BNT162b2 | 29 | 2 | 1 | impaired consciousness and gaze-evoked nystagmus | Improved on pulse IV methylprednisolone for 3 days | Progressive improvement on day 31 and day 66 |
| (Kits et al. 2022) | 53 | 1 | BNT162b2 | 2 | 2 | 2 | Confusion and unconsciousness (GCS of 7), agitation, snoring, anisocoria, and reduced voluntary movements in the left arm and leg | MP, IVIG, PP | Remained in vegetative state |
| (Ahmad, Timmermans, and Dakakni 2022) | 61 | 1 | BNT162b2 | 70 | 1 | 1 | Generalized weakness and altered mental status | steroids and IVIG | Required tracheostomy and gastrostomy tube due to generalized weakness |
| (Miyamoto et al. 2022) | 54 | 1 | BNT162b2 | 12 | 2 | 1 | Fever, urine retention, headache, DCL, facial palsy. | MP, IVIG, PP | Well recovered |
| (Lohmann et al. 2022) | 68 | 1 | BNT162b2 | 23 | 1 | 1 | Exacerbating of preexisting paraparesis. | Improved on IV steroids and plasmapheresis. Also received eculizumab. | Residual paraparesis |
| (Vogrig et al. 2021) | 56 | 1 | BNT162b2 | 14 | 1 | 1 | unsteadiness of gait, predominantly on the left side, followed by clumsiness of left arm. | Steroids | Improvement in gait stability, being able to walk without aid. Mild dysmetria and intention tremor of the left upper limb were still present |
| (Kania et al. 2021) | 19 | 1 | mRNA-1273 | 14 | 1 | 1 | Severe headache, fever (37.5°C), back and neck pain, nausea and vomiting and urinary retention | MP | Residual mild headache |
| (Ballout et al. 2022) | 81 | 1 | mRNA-1273 | 13 | 1 | 2 | Coma | MP, IVIG, PP | Death |
| (Garg, Batra, and Gupta 2023) | 67 | 2 | ChAdOX1 nCoV-19 | 14 | nr | 1 | symptoms of encephalopathy | The patient was given steroids, and a good response was reported. | good response was reported |
| (Nimkar et al. 2022) | 77 | 2 | ChAdOx1 nCov-19 | 15 | 1 | 1 | Altered sensorium for four hours, aphasia for four hours, and loss of consciousness within one hour. Altered mental status for 15 days | MP | vegetative state |
| (Bastide et al. 2022) | 49 | 2 | ChAdOx1 nCoV-19 | 7 | 1 | 1 | flu-like symptoms with fever, fatigue, neck pain, paraesthesia in both legs, up to the chest, Lhermitte's phenomenon and sphincter dysfunction. | MP then readmission/ PP, rituximab | 3 relapses, residual paraparesis |
| (Nagaratnam et al. 2022) | 36 | 2 | ChAdOx1 nCoV-19 | 14 | 1 | 1 | Reduced visual acuity, headache, fatigue, painful eye movement | Significant improvement on IV and oral steroids. | Mild impairment of visual acuity, one relapse |
| (Maramattom, Lotlikar, and Sukumaran 2022) |
64 | 2 | ChAdOx1 nCoV-19 | 20 | 2 | 2 | leg stiffness hand parathesia | IVIG | Mild residual paresis |
| 46 | 2 | ChAdOx1 nCoV-19 | 4 | 1 | 2 | LL weakness | IVIG, MP | Improvement | |
| 42 | 2 | ChAdOx1 nCoV-19 | 5 | 1 | 1 | headache/photophobia | spontaneous improvement | ||
| (Al-Quliti et al. 2022) | 56 | 2 | ChAdOx1 nCoV-19 | 10 | 1 | 1 | LL weakness | MP | Complete resolution |
| (Ancau et al. 2022) |
61 | 2 | ChAdOx1 nCoV-19 | 2 | 1 | 2 | Coma | MP | vegetative state |
| 25 | 2 | ChAdOx1 nCoV-19 | 9 | 1 | 1 | Ascending weakness and numbness | MP/plasma exchange | Persistent hemiplegia | |
| 55 | 2 | ChAdOx1 nCoV-19 | 9 | 1 | 1 | Tetraparesis | Steroids | Death | |
| (Mumoli et al. 2022) | 45 | 2 | ChAdOx1 nCoV-19 | 7 | 1 | 2 | Paraparesis and urine retention | MP | Persistence of urine retention |
| (Rinaldi et al. 2022) | 45 | 2 | ChAdOx1 nCoV-19 | 12 | 1 | 2 | Numbness, decreased visual acuity | - | Complete recovery |
| (Permezel et al. 2022) | 63 | 2 | ChAdOx1 nCoV-19 | 12 | 1 | 2 | Coma | MP-PP | Death |
| (Netravathi et al. 2022) | 54 | 2 | ChAdOx1 nCoV-19 | 14 | 1 | 1 | Quadriparesis | MP+PP | NR |
| 35 | 2 | ChAdOx1 nCoV-19 | 9 | 1 | 1 | Paraparesis and sensory disturbances | MP | NR | |
| 33 | 2 | ChAdOx1 nCoV-19 | 14 | 1 | 1 | Persistent sensory disturbances below midthoracic level | MP+PP | NR | |
| 60 | 2 | ChAdOx1 nCoV-19 | 14 | 2 | 2 | Sensory disturbances, left hemiparesis, memory and behaviour disturbances | MP | NR | |
| 45 | 2 | ChAdOx1 nCoV-19 | 10 | 1 | 2 | Urine retention, altered sensorium | MP+PP | NR | |
| 52 | 2 | ChAdOx1 nCoV-19 | 35 | 1 | 1 | Slurred speech, swallowing difficulties, paresis involving right side | MP+ rituximab | NR | |
| 20 | 2 | ChAdOx1 nCoV-19 of the COVAX initiative | 1 | 1 | 1 | Paraparesis and altered sensorium | MP+PP | NR | |
| (Gustavsen, Nordling, and Weglewski 2023) | 31 | 2 | Ad26.COV2. | 28 | 1 | 1 | right-sided weakness and numbness during a three-week period. | MP | complete clinical recovery at the four-month follow-up. |
| (Lazaro et al. 2022) | 26 | 2 | Gam-COVID-Vac (sputnik) | 28 | 1 | 1 | Disorientation/gait imbalance | MP | Complete resolution |
| (Simone et al. 2021) | 51 | 2 | Adenoviral vector vaccine (unspecified) | - | nr | 1 | Paraparesis and urine retention | MP, | Improved |
| (Sazgarnejad and Kordipour 2022) | 45 | 3 | BBIBP-CorV | 28 | 1 | 2 | Acute disorientation and fever | No significant improvement on pulse corticosteroids and plasmapheresis. Also received cyclophosphamide and rituximab. | Residual aphasia and paresis |
| (Cao and Ren 2022) | 24 | 3 | BBIBP-CorV | 14 | 1 | 1 | Memory decline | IVIG | Complete resolution |
| (Yazdanpanah et al. 2022) | 37 | 3 | BBIBP-CorV | 30 | 1 | 2 | Tetraparesis | MP, PP | Improvement of motor function |
| (Ozgen Kenangil et al. 2021) | 46 | 3 | CoronaVac | 30 | 2 | 1 | Seizure | Steroids | Persistence of abnormal MRI |
In gender: 1=Female; 2=Male; And in vaccine main type; 1=mRNA; 2=Adenoviral vector; 3=Inactivated.
Table 2.
Summary statistics of ADEM developing following COVID-19 vaccination.
| Age in patient receiving mRNA vaccines. Mean±SD |
57±19 |
| Age in patients receiving adenoviral vaccines. Mean±SD |
48±14 |
| Age in patients receiving inactivated vaccines. Mean±SD |
38±10 |
| Age in overall patients Mean±SD |
49±16 |
| Sex distribution in the collected cases n (%) |
Female 25(66) |
| Male 13(34) | |
| Major vaccine type distribution in the collected cases n (%) |
mRNA 10(26) |
| Adenoviral vector 24 (63) | |
| Inactivated 4 (11) | |
| Dose distribution in the collected cases n (%) |
1st dose 29 (76) |
| 2nd dose 6 (16) | |
| NR 3 (8) | |
| Interval between vaccination and ADEM Median (min-max) |
14 |
| Major outcome of collected cases n (%) | Complete clinical recovery 14 (37) |
| Residual Neurologic deficit 10 (26) | |
| Vegetative state 4 (11) | |
| Death 3 (8) | |
| NR 7 (18) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



