
Submitted:
18 July 2023
Posted:
19 July 2023
You are already at the latest version
Abstract
For a subject suffering from complex post-traumatic stress disorder, a psychological intervention program was designed, monitored in real-time during psychotherapy, and evaluated quantitatively and qualitatively after psychotherapy. One male subject participated in this program under consent. The proposed intervention program was designed using cognitive behavioral therapy and stabilization treatments for body-based sensory processes in four sessions of 90 min each. During psychotherapy, a wearable heart sensor and a communication application were utilized to determine the subject’s current psychological state. After the intervention, the effect of the proposed program was analyzed qualitatively and quantitatively using the Impact of Event Scale–Revised (IES-R-K), Athens insomnia scale (AIS), and heart rate variability (HRV). After the intervention program was conducted, the subject reconstructed his traumatic events and trained himself with certain psychological techniques to decrease his negative thoughts and emotions induced by his previous traumatic events. The IES-R-K and AIS ten months after the last session were changed positively by approximately 25% compared with the subject’s state before the first session. During psychotherapy, the HRV exhibited a significant correlation with the subject’s emotional state. The proposed intervention program induced a positive change in the subject. Although the HRV was well utilized in this investigation, more sophisticated statistical analysis will be required for clinical trials.
Keywords:
real time
; heart rate variability
; psychological intervention program
; complex posttraumatic stress disorder
1. Introduction
Experiencing a situation in which one's life is threatened, or witnessing a scenario in which others’ lives are in danger, are considered traumatic events. Some traumatic events are one-time or short-term events, such as traffic accidents or assaults. Other traumatic events may occur repeatedly over a long period of time, such as child abuse and domestic violence. A one-time or simple traumatic event is called simple trauma, while recurring and persistent traumatic is long-term trauma [1,2,3].
Individuals who experience long-term trauma are more impulsive and have more difficulty in emotional regulation than those who experience simple trauma [1,4]. Repressed hostility may appear as somatization symptoms or, in extreme cases, may be accompanied by dissociative identity disorder. Chronic complex trauma influences the severity of symptoms and the personality structure. This is not clearly explained by post-traumatic stress disorder (PTSD). In other words, symptoms due to complex trauma are characterized by the individual experiencing difficulties in self-organization (DSO), such as problems with emotional regulation, having a negative self-concept, and difficulties with interpersonal relationships, along with re-experiencing the trauma and demonstrating avoidance and hyper-arousal, which are major symptoms of PTSD. This syndrome is called complex post-traumatic stress disorder (CPTSD) [1,5].
Previous studies have involved separately diagnosing complex PTSD to elucidate the psychopathology and enable more effective treatments of subjects who have experienced repeated and chronically extreme traumatic events [1,4,6,7,8,9,10]. CPTSD is listed separately from PTSD in the International Classification of Diseases 11th Revision (ICD-11); however, it is not separately listed in the Diagnostic and Statistical Manual of Mental Disorders 5th Revision (DSM-5). Studies comparing CPTSD and PTSD have been undertaken and have produced evidence for intervention methods through worldwide clinical trials.
In Republic of Korea, the Daegu subway disaster in 2003 drew attention to PTSD, and the National Trauma Center was established in 2018 after the Sewol ferry disaster in 2014. However, there was no discrimination between the PTSD intervention and the CPTSD intervention. Ahn introduced CPTSD in 2007 [11] emphasizing requirement of the intervention for CPTSD only. Lee reported psychotherapy and treatment of CPTSD in 2020 [6]. Nowadays, studies on the CPTSD intervention have increased in Korea. Those recent studies have some limitations in that the existing psychological treatment applied to CPTSD as it is and treatment based on CPTSD symptoms was not performed [12].
CPTSD requires psychological stabilization through physical stabilization and setting treatment goals for cognitive intervention. This condition induces emotional changes through cognitive distortion owing to the subject’s experience of long-term trauma [8,13]. Because these emotional changes cause the subject to re-experience negative feelings and to dissociate symptoms from sensing, psychological stabilization by means of physical stabilization is required. CPTSD caused by continuous exposure to abuse and violence in interpersonal relationships negatively affects the subject’s daily life through generating negative concepts about oneself and others and causing a distorted understanding in relational contexts. To review and restructure damaged interpersonal relationships, physical intervention as well as cognitive intervention should be set as goals for effective treatment.
To modulate the abnormal coping mechanisms of the brain caused by CPTSD, the intervention program designed in this study applies principles of bottom-up intervention, top-down intervention, and integration intervention. The bottom-up approach is intended to change the lower part of the brain through experience from five sensors so that it eventually affects the upper part of the brain, such as the prefrontal cortex (PFC), which is responsible for cognition. The top-down approach is intended to change the bodily and emotional responses (the lower part of the brain) through reconstructing cognition (the upper part of the brain). In other words, the top-down approach is applied to the cerebral neocortex. It addresses cognition by finding meaning and understanding to facilitate control of the affective disorder and bodily sensory experiences and to increase linguistic self-esteem [13]. The proposed intervention program consists of the bottom-up approach and the top-down approach to treat CPTSD symptoms, which helps to stabilize the arousal state of the autonomic nervous system (ANS) and restructure negative cognition and thinking.
In psychology, the effectiveness of an intervention program is typically evaluated based on the subject’s subjective response to scaled questionnaires. Although the clinical scale has been widely utilized for validity and reliability, there is some limitation in consistency with this approach because it is a subject-self-reporting method. In biomedical engineering and digital healthcare fields, heart rate variability (HRV), which is a quantitative measure of the variation in intervals between heartbeats, has been broadly utilized to quantify the state of the subject [14,15]. In psychology, it has been increasingly employed to assess the effect of psychotherapy [16,17]. However, HRV has rarely been utilized for CPTSD.
The HRV serves as a sensitive indicator of the functionality of the autonomic nervous system (ANS) [18,19,20]. This system's parasympathetic and sympathetic branches modulate the heart rate via influences on the sinoatrial node pacemaker [21]. The high-frequency (HF) peak of HRV, derived from the spectral analysis of interbeat intervals, is believed to represent parasympathetic or vagal tone, though there is some debate regarding the sensitivity and specificity of commonly utilized HRV measures [22,23]. Reduced HRV, which is often observed in posttraumatic stress disorder (PTSD), implies autonomic inflexibility potentially resulting from sympathetic overactivity, parasympathetic deficiency [20,21,24,25], or the exacerbation of common cardiovascular issues associated with PTSD [26]. Lower HRV values have also been noted in various psychiatric disorders including schizophrenia, depression, bipolar disorder, and panic disorder [27,28,29,30], linking decreased HRV to pathophysiology, psychopathology, and increased mortality [21,31].
Therefore, this study investigated the relationship between HRV and the psychological status of one subject who suffers from CPTSD. The principal hypothesis is to check subject’s HRV in real time could help psychotherapist to figure out subject’s psychological status. During the intervention program, we monitored subject’s HRV in real time using a wearable heart rate sensor (H10, Polar, Finland) and a communication application (Elite HRV, Elite HRV Inc., U.S.A.). After the intervention program, using the recorded interbeat intervals, statistical relation between interventional events during the program and change ratio of the HRV was analyzed to inspect our hypothesis.
2. Materials and Methods
2.1. Proposed intervention program for CPTSD
The proposed intervention program for CPTSD in this study was designed using the imagery and cognitive interventions of cognitive behavioral therapy (CBT) [12] and stabilization treatments for body-based sensory processes. In addition, the phase-based approach, which is the recommendation of the International Society for Traumatic Stress Studies (ISTSS) for CPTSD treatment [32], was reflected. Each stage was structured as follows: Phase 1 was bottom-up stabilization training, Phase 2 was trauma treatment, and cognitive (bottom-up), somatosensory and imagery (top-down) techniques were applied, and Phase 3 was the process of integration. Our program consisted of four sessions of 90 min each. The proposed program consisted of complex PTSD core traumatic events and symptom differentiation, cognitive restructuring and self-management training, and a stabilization technique.
Session 1 introduced the program, checked the symptoms and the trauma events of participants, and implemented stabilization techniques. Session 2 checked CPTSD education and cognitive distortion correction. Session 3 covered how to use the sense of preference to improve adaptation to daily life. Session 4 discussed ways to check and maintain changes. Bottom-up stabilization training was conducted every session so that the participants could acquire self-stabilization skills. When invasion occurs due to the trauma memory processing, the first stage stabilization technique was implemented so that the treatment stage could interact organically. This is in accordance with the recommendations of ISTSS [32].
To increase the content validity and effectiveness of this program, it was cross-checked by a mental health social worker supervisor, a disaster mental health specialist, and an eye movement desensitization and reprocessing movement specialist. The researcher who conducted this program is a psychotherapist with 14 years of experience in neuro-linguistic programming developed based on CBT, 4 years of firefighter psychotherapy experience, and 13 years of experience as a couple and family therapy specialist.
A simple time-series design method for this investigation was used to evaluate the effect of the proposed intervention program for CPTSD. A total of four sessions were conducted from November 5, 2020 to November 25, 2020. A preliminary survey was performed on November 5, 2020 before the main intervention program. An end-up survey was conducted on November 25, 2020 immediately after the last session. A follow-up survey was performed on September 23, 2021, almost ten months after the last session. During each session, the subject wore a heart rate sensor to measure HRV with the communication application.
2.2. Subject
The protocol of this study was approved by the Institutional Review Board of the University of Ulsan (1040968-A-2020-016). All methods were performed in accordance with the relevant guidelines and regulations. The trial conformed to the tenets of the Declaration of Helsinki. The subject provides written informed consent for the publication of their case details.
The subject of this study was a 25-year-old male. He graduated from high school and was unmarried. Although he had close friends, they had some conflicts. His current level of physical health and overall life satisfaction were low. Prior to participating in this program, he had engaged in 12 psychotherapy sessions with the topic of family and interpersonal conflict and trauma based on the CBT and the Object Relations Psychology Model. He stated that previous psychotherapy was helpful in fostering his self-understanding and interpersonal coping. He complained difficulties in interpersonal relationships, nightmares, and negative emotions due to school and family violence he had repeatedly experienced since childhood. However, when participating in this study, the subject self-reported re-experiencing, avoidance, sensing threat, affect dysregulation, negative self-concept, relationship disturbances, etc. These symptoms are well known as major features of CPTSD [33]. In Korean societies, any diagnostic criteria to discriminate CPTSD symptoms from PTSD has not yet developed [12]. To secure the CPTSD representativeness of the participant, authors requested an expert having a doctorate degree in educational psychology and a counseling expert certificate from the Korean Counseling Association (KCA) to compare and analyze the CPTSD diagnosis criteria. After the delicate evaluation based on MMPI-2, interview data, voice-record, and transcripts, the expert endorsed the participant would be a presentative case of the CPTSD.
2.3. Data analysis
2.3.1. Quantitative analysis
A The preliminary survey, end-up survey, and follow-up survey were estimated using a questionnaire. The questionnaire consisted of the Impact of Event Scale – Revised (IES-R-K), which was first developed by Weiss and Marmar in 1997 [34] and was enhanced by Eun et al. in 2005 [35]. It additionally included the Athens Insomnia Scale (AIS) developed by Soldatos et al. in 2000 [36]. IES-R-K is a self-reporting scale for trauma-related symptoms. It consists of 22 questions. This scale is composed of five points (0 to 4), with 0 being “not at all” and 4 being “a lot.” On this scale, a total score of 24 or higher indicates “the need for clinical consideration for PTSD,” a score of 33 to 36 is a “potential PTSD level,” and a score of 37 or higher is clinically considered “the extent that the immune system is not functioning properly.” On this scale, when it was higher than 17-18, it was considered to have partial PTSD symptoms, and when it was 24-25 or higher, it was considered to have full PTSD symptoms [35]. The full PTSD could be classified in detail: a score of 25-39 is moderate PTSD, 40-59 is severe PTSD, and 60 or higher is very severe PTSD [37]. AIS consists of eight questions as a measure to evaluate the quantity and quality of sleep. This scale has four points (0 to 3), with 0 being “no problem at all” and 3 being “very serious.” This scale is used to make a clinical judgment on the degree of sleep disorder with the sum of scores. If the total score is less than 4, it is deemed “maintaining a good sleep state.” If it is between 4 and 5, it is “suspicious insomnia,” and if it is 6 or more, it is considered that an “insomnia test is required.”
The subject wore the heart rate sensor, which measured the peak-to-peak interval (r-r ' interval) during each intervention session with the Bluetooth-based communication application. The sensor was worn on the subject’s chest according to the manufacturer guidelines [38]. During psychotherapy, the application obtained the subject’s heart rate information and calculated the HRV in real time. After psychotherapy, the HRV was calculated using Open Source Python Toolbox for HRV [39,40]. Among various factors of HRV, the root mean square of successive RR interval differences (RMSSD), standard deviation of NN intervals (SDNN), absolute power of very low frequency band (VLF, 0.00 – 0.04 Hz), absolute power of low frequency band (LF, 0.04 – 0.15 Hz), absolute power of high frequency band (HF, 0.15 – 0.40 Hz) and ratio of LF-to-HF power (Ratio) were calculated and compared [39,40,41]. Calculation equations of the RMSSSD and SDNN are as follows [41]:
where N is the number of measured values, RR is the time between two detected heartbeats, and NN is the time between two filtered heartbeats. The initial 3-min data for each session were discarded as artifacts. HRV indexes neurocardiac function and is generated by heart-brain interactions and dynamic non-linear ANS processes [41]. HRV is an emergent property of interdependent regulatory systems which operate on different time scales to help us adapt to environmental and psychological challenges [41]. Higher values of RMSSD and SDNN signified higher top-down self-regulation (the ability to regulate behavioral, cognitive, and emotional processes) [42].
2.3.2. Qualitative analysis
In qualitative analysis, the case analysis method was used [43]. This method could understand the process in which a case develops in a unique and complex way in a specific situation or context by collecting in-depth data including rich information sources appearing in the context. The psychotherapist encouraged the subject to express his emotions, thoughts, and attitudes, especially during visual observation of the subject’s symptom changes in the intervention session. Each session was voice-recorded under the subject’s consent, including this self-expression process. Dramatic emotion changes, self-reporting of traumatic events, and treatment with stabilization techniques were noted. The observation notes and transcript of the recorded session were analyzed. Our qualitative analysis was cross-checked three times by every three experts officially qualified as a mental health social worker supervisor, a disaster mental health specialist, or an expert belonging to the KCA. By these nine cross-checkings, authors’ analysis and three experts’ analysis consented over 90%.
3. Results
3.1. Therapeutic intervention and symptom change during proposed program
To analyze the effectiveness of the therapeutic intervention on the symptoms of the subject in every session, observation notes (dramatic changes in positive and negative emotions of the subject, self-reporting of his traumatic events, treatment with stabilization techniques) and the transcripts were qualitatively analyzed. The qualitative analysis was compared with the calculated HRV in each session. Its comparison is outlined below.
3.1.1. Session one: Exploring traumatic event and CPTSD symptoms, creating safety zone and training stabilization
In the first session, traumatic events and CPTSD symptoms were first explored. After that, the stabilization treatment to establish a safety zone for relieving and self-managing of the subject’s symptoms was performed. Figure 1 shows 5-min RMSSD and SDNN in the first session. At 15 min from the start of the first session, the subject self-reported his core traumatic event (The “T” remark). The abrupt negative emotional change (The “N” remark) and abrupt drop in the RMSSD near the 15-min point appears related to this self-reporting. However, the SDNN near the 15-min point is increased in contrast to the RMSSD.
In the first session, the subject self-narrated his traumatic events at approximately minute 14 and minute 51 from the session start: “Hits for no reason...all my friends know.” “I’m still scared when I run into kids who look like mutts on the way. When I think of their faces, I get angry...scared.” The subject expressed negative emotions, such as shame and neglect, while recalling the above key traumatic events. The subject self-reported symptoms of CPTSD caused by these events, such as re-experience, avoidance, negative self-concept, and interpersonal difficulties. To address the core symptoms, a total of four safety-zone-making and stabilization techniques were performed from minute 35 to minute 52. When the subject recalled the traumatic event, he self-reported discomfort as “8” on the scale before the stabilization technique was implemented. After the stabilization technique was performed, he self-reported “4” for his discomfort level.
3.1.2. Session two: Cognitive reconstruction
In The second session was the stage of restructuring the subject’s distorted cognition by finding the core beliefs that have a significant impact on his core being. He identified his traumatic events with his other experiences. He self-narrated his traumatic events: “Sometimes I thought I might be mentally sick. When I see someone whom I don’t like, I just want to kill them...so I thought I had a mental disease.” “I’m just walking around...a random assault could happen to me.” [What is the random assault?] “It’s when suddenly, for no reason, someone just beats, assaults, and robs me.” [Is that the same as your experience when a friend slapped the back of your head on the bus in high school?] “Isn’t it the same thing?” [Can you tell me what you read in the newspaper about the random assault?] “It was an assault and threats with a knife.”
This is a typical symptom of CPTSD victims: a negative self-concept and cognitive distortion that cause the emotional changes. After the initial stabilization technique was implemented at the start of the session (approximately 5 min from the beginning), the subject self-reported his interpersonal experience until the middle of the second session. During this self-reporting period, the subject exhibited depression and an abrupt decrease of the SDNN (Figure 2).
Immediately after the subject’s self-narration of traumatic events at approximately 4 min, both the SDNN and RMSSD increase in Figure 3, which suggests that the self-narration induces the subject’s psychological change. At approximately 74 min, the preferred sense of the subject among the five senses was explored. Based on the explored preferred sense, the second stabilization technique was performed. Psychological stability was self-reported as “2” in terms of the discomfort level, and an increase in the SDNN and RMSSD is observed in Figure 2.
The stabilization technique, a bottom-up process, produced an immediate response to HRV changes compared to the top-down process, such as the cognitive intervention method. Since the cognitive changes of those who experience CPTSD are chronic symptoms, the process of changing distorted cognition and thinking is likely a more difficult process. Therefore, during the top-down process, a dramatic change in HRV was not observed, unlike in the bottom-up intervention.
3.1.3. Session three: Sensory reconstruction and identifying resources
In the third session, the subject clearly revealed his negative self-concept, which was not integrated within himself. At the start of this session, a rapid decline in both the SDNN and RMSSD is observed in Figure 3. At this point, the subject self-reported his unacceptable experience. In the transcript, this was described as follows: “Embarrassment is seven points. … Injustice is ten points. It’s really terrifying. It’s unfair I had to go through this experience.” “Just think about it for a moment...I wouldn’t have gone this far...I’m so sorry for him....It’s confusing. I’m sorry and I’m annoyed.... However, it was not that I was 100% kind, and he did that kind of thing afterward [after recalling the traumatic event].” “The maximum points, ten points (of discomfort)....Does this make sense? [a sigh and a deep breath...hesitating to talk].”
Since he had self-reported his negative self-experience at the beginning of the session, he self-narrated his traumatic symptoms up to the middle of the session. He scored his traumatic events as ten points, the maximum points. Although he reported negative events, as in Session 2, the previous session, he deconstructed and reconstructed his traumatic events in talking with the psychotherapist, which resulted in a symptom change. This process is a typical top-down one. In the process of discussing the traumatic events, the story is reassembled, which helps the CPTSD victim to have a new point of view toward the traumatic events. Here, it is suggested that the increasing trend of both the SDNN and RMSSD from approximately minute 18 to minute 50 in Figure 3 is related to these verbal reports.
In this session, the stabilization technique, which involved exploring resources, was performed. First, the subject was to hug himself, identify an external resource (someone beside himself), and then experience the acceptance by the external resource. Next, the stabilization technique based on the subject’s preferred sense was performed similar to the second session. The subject rated his experience, ranging from ten points to six points after the second stabilization and to three points after the third stabilization.
3.1.4. Session four: Confirming one’s own change, exploring self-management plan, and projecting one’s one future (going into the world)
In the last session, the subject confirmed his own changes and explored self-management methods. These results appear related to the abrupt positive emotion changes at approximately minute 5 and minute 42 in Figure 4. The HRV at both moments exhibits increasing tendencies, except the SDNN at 5 min. The subject described his positive emotion accordingly: [What kind of person do you think you are?] “I think I am growing a bit....I could say it is unnecessary to be upset. Let’s talk just about this situation.”
The stabilization technique in the last session utilized a timeline based on the subject’s preferred sense. As the intervention program progressed, the subject integrated his separate sense of self. He practiced maintaining these changes in the future. He talked about a problem centered on himself as the victim at approximately minute 45 (Figure 4). This re-experience is a phenomenon that can happen to those who have experienced CPTSD. Therefore, through a future projection technique, the subject’s coping methods were checked in a future situation. After the projection process, breathing training and imagery training work were conducted. During these sessions, the subject experienced positive sensations of the five senses through Light Stream Mediation. Through a body scanning technique, he verbally reported a “warm and cozy sensation.” The HRV in Figure 4 increased as well.
During the future projection process, the subject assessed himself accordingly: “Compared to five years ago, I am doing better....First of all, I’m getting older and getting to know the world more. I grew up.” [Are you punishing yourself like you did before?] “I don’t think so.” [What do you want to say to yourself in five years?] “Something cool. My future is wonderful. I would like to inherit something valuable.”
3.2. Statistical analysis of relation between the interventional event and the HRV change ratio
During all four sessions, the subject self-reported his traumatic event five times. Among the five trauma tellings, abrupt negative emotion changes within five minutes of the trauma tellings were observed four times. In the case of the only trauma telling not related to abrupt negative emotion change, the psychotherapist performed the stabilizing technique right after the trauma telling. Among the ten stabilizing techniques used in all four sessions, abrupt positive emotion change within five minutes was observed once. The trauma telling appears to alter the subject's psychological status.
To statistically evaluate the relations between the interventional events (the trauma telling, stabilization technique, positive emotion change, and negative emotion change) and the subject's psychological and physical status, change ratios of the calculated HRV factors (RMSSD, SDNN, VLF, LF, HF, and Ratio) were analyzed. The change ratios of the HRV factors were used for the statistical analysis instead of their absolute values because their change trends are more meaningful than their absolute values. The HRV factors in this investigation were calculated using the measured heart beat intervals for the latest five minutes. The RMSSD at minute 18 was calculated using the recorded heart beat intervals from minute 13 to minute 18. If the subject started to self-report his traumatic event at minute 14, it could affect the HRV factors at minute 18 or minute 23. To calculate the change ratio of the HRV factors, the difference from the former five-minute HRV factors to the present five-minute HRV factors was divided by the present five-minute HRV factors. To check the effect of the trauma telling at minute 14, the change ratio from the HRV factors at minute 13 to the HRV factors at minute 18 was calculated and noted as "Time 0". To track the slow effect of the trauma telling at minute 14, the change ratio from the HRV factors at minute 18 to the HRV factors at minute 23 was computed and remarked as "5 Min. later".
In summary, the "Time 0" change ratio was calculated as follows:
, and the “5 Min. later” was computed as follows:
where HRV-5 is the HRV factors calculated with the heart beat intervals from minute -10 to minute -5, HRV0 is from -5 to 0, and HRV5 is from 0 to 5.
First of all, with respect to the cases marked as no interventional event, change ratios of the HRV factors were calculated. In all four sessions, the time-zero HRV change ratios of the non-noteworthy events were counted as 39. The five-min-later HRV change ratios were 23. The standard deviations of the RMSSD and SDNN were under 0.327, which were much smaller than the others'. The standard deviation range of the other HRV factors ranged from 0.489 to 1.803, and their average was 0.934. The average change ratio of the RMSSD and SDNN were -0.3% and -10.2% at time 0 and 1.1% and -11.9% five minutes later, respectively. The RMSSD showed almost no change during the ordinary status, but the SDNN showed a gradual decrease of around 10%.
Figure 5 exhibits the change ratio of the HRV factors when the subject told his traumatic event at time 0. In all four sessions, the trauma telling happened five times. The RMSSD and SDNN only showed reliable standard deviations. The SDNN increased by 10% at time 0 of the trauma telling and then decreased by 10% five minutes later. In relation to the average SDNN change ratio of the ordinary status (around -10%), it appears that parasympathetic change occurred due to the trauma telling and then returned to the ordinary status. Considering the above-mentioned relation between the trauma telling and the abrupt negative emotional change, the SDNN change ratio according to the trauma telling is explainable. Even though the standard deviation of the RMSSD is the least among all the HRV factors, its change ratio (under 10%) is negligible comparing with its change ratio at the ordinary status (around 0%).
The change ratio of the HRV factors when the psychotherapist performed the stabilizing technique at time 0 was as shown in Figure 6. In all four sessions, the stabilizing technique was performed ten times. The RMSSD and SDNN only showed reliable standard deviations. The SDNN increased by about 23% at time 0 and then exhibited almost no change five minutes later. It is supposed that the stabilizing technique facilitated autonomic flexibility. Even though the standard deviation of the RMSSD is the least among all the HRV factors, its change ratio (under 10%) is negligible comparing with its change ratio at the ordinary status (around 0%).
Figure 7 showed the change ratio of the HRV factors when the subject's abrupt positive emotion change was observed at time 0. In all four sessions, the positive emotion change was observed four times. The RMSSD and SDNN only showed reliable standard deviations. The RMSSD at time 0 only increased by about 25%. The SDNN at time 0 decreased about 4.4%. Only at the positive emotional change in all the sessions, the RMSSD changed by over 10%. Considering these things, the 25% RMSSD increase at time 0 looked no consistency to represent subject's status at that time.
The change ratio of the HRV factors when the subject's abrupt negative emotion change was observed at time 0 was as shown in Figure 8. In all four sessions, the negative emotion change was observed eight times. The RMSSD and SDNN only showed reliable standard deviations. The SDNN increased by about 4.5% at time 0 and then decreased by about 17% five minutes later since the negative emotion change. Considering the average SDNN change ratio of the ordinary status (around -10%), the 4.5% increase was a significant change, and the 17% SDNN decrease looked closer to the ordinary status. It is supposed that the abrupt negative emotion change affected the SDNN to increase at time 0. Even though the standard deviation of the RMSSD is the least among all the HRV factors, its change ratio (under 10%) is negligible comparing with its change ratio at the ordinary status (around 0%).
The results revealed that trauma telling had a significant impact on the subject's psychological status, as evidenced by the observed abrupt negative emotion changes within five minutes of the trauma tellings and 10% SDNN increasement at the time of the trauma tellings. This suggests that reliving the traumatic event through self-reporting can flex subject’s ANS as well as induce subject’s emotional distress. The abrupt negative emotion changes followed by the trauma-tellings increased the SDNN about 10.5%, which is about two times than the average SDNN increasement (4.5%) at the observed time of all the abrupt emotion change. The abrupt emotion change followed by the trauma telling looked to regulate subject’s ANS more.
The occurrence of abrupt negative emotion changes had a notable impact on the SDNN, which increased by approximately 4.5% on the average at the time of the negative emotion change. However, this increase was followed by a decrease of approximately 17% five minutes later, indicating a return to the subject's ordinary state. Furthermore, the stabilizing technique performed by the psychotherapist showed promising results in promoting autonomic flexibility. The change ratios of the HRV factors demonstrated an increase in SDNN by approximately 23% at the time of intervention, indicating a positive effect on the subject's physiological response. This suggests that the stabilizing technique may help the subject regulate their autonomic nervous system and achieve a more balanced state.
Additionally, the occurrence of abrupt positive emotion changes was observed to have confused influence on the HRV factors. While the RMSSD showed a considerable increase of around 25% at the time of positive emotion change, the other HRV factors exhibited decreases of under 10%. This indicates that the HRV factors may not be highly sensitive to transient positive emotional fluctuations. Therefore, relying solely on the RMSSD as a real-time indicator during psychological counseling may not be reliable.
Overall, the findings highlight the importance of considering different interventional events and their corresponding effects on subject's psychological and physiological status. While trauma telling and stabilizing techniques showed significant associations with emotional and autonomic responses, the impact of positive emotion changes was less pronounced, and the use of RMSSD as a real-time indicator may be limited. These findings contribute to our understanding of the complex dynamics between interventional events and the subject's well-being, emphasizing the need for comprehensive assessments in psychological counseling settings.
3.3. Change in the IES-R-K and AIS scale before, after, and 10 months after the proposed program
Table 1 shows the scale change in the IES-R-K and AIS before, after, and 10 months after the proposed program. The IES-R-K showed 60 points in the pre-survey, 43 points in the post-survey, and 40 points follow-up survey, indicating that the level was lowered from the very serious level before the program to the serious level after the program. The IES-R-K changed to 43 points at the post-survey, which is at a low level among severe (40-59 points), and the status was maintained until the follow-up survey (40 points). As for the difference by subfactor of the IES-R-K, re-experiencing decreased the most from 23 to 15 points, followed by avoidance from 24 to 17 points, sleep and dissociation from 14 to 10 points, and hyperarousal decreased from 21 to 20 points. The AIS change supposed to show the quality of sleep improved from 10 points in the pre-survey, to 7 points in the post-survey, and finally to 6 points in the follow-up survey.
4. Discussion and Conclusions
In this paper, a practical intervention program was proposed to help a subject lead a normal daily life through cognitively restructuring of their CPTSD symptoms by applying cognitive and physical interventions. Through this research, the following findings were made. First, using real-time HRV, the psychotherapist could easily check the subject’s current state. Second, the HRV showed a significant relationship with the intervention techniques. Therefore, HRV can be utilized to check a subject’s current state and to choose personalized intervention techniques among many other psychotherapy methods, such as the bottom-up method and the top-down method. This approach may overcome the limitations of subject self-reporting. This real-time HRV-assisted psychotherapy approach can be utilized much more frequently in online therapy, especially during pandemic periods.
Despite these positive findings, this research has some limitations. Only one subject participated in this study; therefore, it was impossible to statistically analyze the results. In addition, the relationship between the subject’s psychological state and the HRV should be more finely analyzed. More refined tracking of this program’s effect is required. Currently, we are planning a more sophisticated investigation for CPTSD patients.
Author Contributions
Conceptualization, B. I. and K.-i. K.; methodology, B. I., J. K., T. K. and K.-i. K.; software, B. I., J. K., and T. K.; validation, K.-i. L. and K.-i. K.; writing—original draft preparation, B. I. and K.-i. K.; writing—review and editing, K.-i. L. and K.-i. K.; visualization, K.-i. K..; supervision, X.X.; project administration, K.-i. L. and K.-i. K.; funding acquisition, K.-i. K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the 2022 Research Fund of University of Ulsan, Ulsan, Republic of Korea.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of University of Ulsan, Ulsan, Republic of Korea (IRB approval number: 1040968-A-2020-016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Herman, J.L. Complex PTSD: A syndrome in survivors of prolonged and repeated trauma. Journal of Traumatic Stress 1992, 5, 377–391. [Google Scholar] [CrossRef]
- Terr, L.C. Childhood Traumas - an Outline and Overview. Am J Psychiat 1991, 148, 10–20. [Google Scholar] [CrossRef]
- Kolk, B.v.d.; Pelcovitz, D. CLINICAL APPLICATIONS OF THE STRUCTURED INTERVIEW FOR DISORDERS OF EXTREME STRESS (SIDES). Clinical Quarterly 1999, 8, 21–26. [Google Scholar]
- Courtois, C.A. Complex trauma, complex reactions: Assessment and treatment. Psychotherapy: Theory, Research, Practice, Training 2004, 41, 412–425. [Google Scholar] [CrossRef]
- Herman, J.L. Trauma and recovery, 2015 edition. ed.; BasicBooks: New York, 2015; pp. ix, 326 pages. [Google Scholar]
- Lee, J. Psychotherapy of Complex PTSD: Focus on a Phase-Based Approach. The Korean Journal of Psychology: General 2020, 39, 307–333. [Google Scholar] [CrossRef]
- Kim, H.K. Differences in the Symptoms of Complex PTSD and PTSD in North Korean Defectors by Trauma Type. 2014, 4, 65–92. [Google Scholar]
- van der Kolk, B.A.; Courtois, C.A. Editorial comments: Complex developmental trauma. Journal of Traumatic Stress 2005, 18, 385–388. [Google Scholar] [CrossRef]
- Pelcovitz, D.; van der Kolk, B.; Roth, S.; Mandel, F.; Kaplan, S.; Resick, P. Development of a criteria set and a structured interview for disorders of extreme stress (SIDES). Journal of Traumatic Stress 1997, 10, 3–16. [Google Scholar] [CrossRef]
- Resnick, H.S.; Kilpatrick, D.G.; Dansky, B.S.; Saunders, B.E.; Best, C.L. Prevalence of civilian trauma and posttraumatic stress disorder in a representative national sample of women. Journal of Consulting and Clinical Psychology 1993, 61, 984–991. [Google Scholar] [CrossRef]
- Ahn, H.-n. An Empirical Review of Complex Trauma. The Korean Journal of Psychology: General 2007, 26, 105–119. [Google Scholar]
- Joo, H. Development of a trauma case formulation framework (TCFF): The case formulation approach for trauma-focused psychotherapy. Korean Journal Of Counseling And Psychotherapy 2016, 28, 89–125. [Google Scholar] [CrossRef]
- Ogden, P.; Minton, K.; Pain, C. Trauma and the body : a sensorimotor approach to psychotherapy, 1st ed.; W.W. Norton: New York, 2006; pp. xxxiv, 345 p. [Google Scholar]
- Kim, C.; Woo, J. Comparison of Smart Watch Based Pulse Rate Variability with Heart Rate Variability. Journal of Biomedical Engineering Research 2018, 39, 87–93. [Google Scholar] [CrossRef]
- Kim, H.; Na, Y.; Woo, J. Study on Listening Efforts Based on Heart Rate Variability. Journal of Biomedical Engineering Research 2019, 40, 75–80. [Google Scholar] [CrossRef]
- Kim, W. Heart Rate Variability in Stressful Events and Mental Disorder. Stress 2008, 16, 161–166. [Google Scholar]
- Lee, C.; Kim, M.-K.; Choi, S.-W.; Park, H.-i.; Seok, J.-H. Characteristics in Heart Rate Variability Associated with Early Life Stress in Patients with Major Depressive Disorder. Mood Emot 2017, 15, 117–122. [Google Scholar]
- Bilchick, K.C.; Berger, R.D. Heart rate variability. J Cardiovasc Electrophysiol 2006, 17, 691–694. [Google Scholar] [CrossRef]
- Minassian, A.; Geyer, M.A.; Baker, D.G.; Nievergelt, C.M.; O'Connor, D.T.; Risbrough, V.B.; Marine Resiliency Study, T. Heart rate variability characteristics in a large group of active-duty marines and relationship to posttraumatic stress. Psychosom Med 2014, 76, 292–301. [Google Scholar] [CrossRef]
- Minassian, A.; Maihofer, A.X.; Baker, D.G.; Nievergelt, C.M.; Geyer, M.A.; Risbrough, V.B.; Marine Resiliency Study, T. Association of Predeployment Heart Rate Variability With Risk of Postdeployment Posttraumatic Stress Disorder in Active-Duty Marines. JAMA Psychiatry 2015, 72, 979–986. [Google Scholar] [CrossRef]
- Malik, M.; Camm, A.J. Heart rate variability; Futura Pub. Co.: Armonk, NY, 1995; pp. xiv, 543 p. [Google Scholar]
- Berntson, G.G.; Bigger, J.T., Jr.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef]
- Eckberg, D.L. Sympathovagal balance: a critical appraisal. Circulation 1997, 96, 3224–3232. [Google Scholar] [CrossRef]
- Lee, E.A.; Theus, S.A. Lower heart rate variability associated with military sexual trauma rape and posttraumatic stress disorder. Biol Res Nurs 2012, 14, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.J.; Lampert, R.; Goldberg, J.; Veledar, E.; Bremner, J.D.; Vaccarino, V. Posttraumatic stress disorder and impaired autonomic modulation in male twins. Biol Psychiatry 2013, 73, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, H.; Greenman, P.S.; Tasse, V. Post-Traumatic Stress Disorder among Cardiac Patients: Prevalence, Risk Factors, and Considerations for Assessment and Treatment. Behav Sci (Basel) 2014, 5, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Carney, R.M.; Freedland, K.E. Depression following myocardial infarction. Gen Hosp Psychiatry 2005, 27, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Cohen, H.; Benjamin, J.; Geva, A.B.; Matar, M.A.; Kaplan, Z.; Kotler, M. Autonomic dysregulation in panic disorder and in post-traumatic stress disorder: application of power spectrum analysis of heart rate variability at rest and in response to recollection of trauma or panic attacks. Psychiatry Res 2000, 96, 1–13. [Google Scholar] [CrossRef]
- Henry, B.L.; Minassian, A.; Paulus, M.P.; Geyer, M.A.; Perry, W. Heart rate variability in bipolar mania and schizophrenia. J Psychiatr Res 2010, 44, 168–176. [Google Scholar] [CrossRef]
- Malaspina, D.; Bruder, G.; Dalack, G.W.; Storer, S.; Van Kammen, M.; Amador, X.; Glassman, A.; Gorman, J. Diminished cardiac vagal tone in schizophrenia: associations to brain laterality and age of onset. Biol Psychiatry 1997, 41, 612–617. [Google Scholar] [CrossRef]
- Thayer, J.F.; Lane, R.D. Claude Bernard and the heart-brain connection: further elaboration of a model of neurovisceral integration. Neurosci Biobehav Rev 2009, 33, 81–88. [Google Scholar] [CrossRef]
- Cloitre, M.; Courtois, C.A.; Ford, J.D.; Green, B.L.; Alexander, P.; Briere, J.; Herman, J.L.; Lanius, R.; Stolbach, B.C.; Spinazzola, J.; et al. The ISTSS Expert Consensus Treatment Guidelines for Complex PTSD in Adults. Available online: https://istss.org/ISTSS_Main/media/Documents/ISTSS-Expert-Concesnsus-Guidelines-for-Complex-PTSD-Updated-060315.pdf (accessed on 6 February 2023).
- Kim, S.H.Y., K. L. A Validation Study of the Korean Version of the Complex Trauma Inventory. Journal of Rehabilitation Psychology 2020, 27, 27–48. [Google Scholar] [CrossRef]
- Wilson, J.P.; Keane, T.M. Assessing psychological trauma and PTSD; Guilford Press: New York, 1997; p. xiv, 577 p. [Google Scholar]
- Eun, H.-J.; Kwon, T.-W.; Lee, S.-M.; Kim, T.-H.; Choi, M.-R.; Cho, S.J. A Study on Reliability and Validity of the Korean Version of Impact of Event Scale-Revised. JOURNAL OF THE KOREAN NEUROPSYCHIATRIC ASSOCIATION 2005, 44, 303–310. [Google Scholar]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. J Psychosom Res 2000, 48, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.S.; Marmar, C.R. The Impact of Event Scale—Revised. In Assessing psychological trauma and PTSD.; The Guilford Press: New York, NY, US, 1997; pp. 399–411. [Google Scholar]
- Polar. Polar H10 User Manual. Available online: https://support.polar.com/e_manuals/h10-heart-rate-sensor/polar-h10-user-manual-english/manual.pdf (accessed on 6 February 2023).
- Gomes, P.; Margaritoff, P.; Silva, H. pyHRV: Development and evaluation of an open-source python toolbox for heart rate variability (HRV); 2019; pp. 822–828. [Google Scholar]
- Gomes, P. pyHRV - OpenSource Python Toolbox for Heart Rate Variability. Available online: https://pyhrv.readthedocs.io/en/latest/index.html (accessed on 6 February 2023).
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed]
- Holzman, J.B.; Bridgett, D.J. Heart rate variability indices as bio-markers of top-down self-regulatory mechanisms: A meta-analytic review. Neurosci Biobehav Rev 2017, 74, 233–255. [Google Scholar] [CrossRef] [PubMed]
- Stake, R.E. Qualitative Case Studies. In The Sage handbook of qualitative research, 3rd ed.; Sage Publications Ltd: Thousand Oaks, CA, 2005; pp. 443–466. [Google Scholar]
Figure 1.
Every five-min SDNN and RMSSD in the first session. The 3-min data from the session start were removed for being considered the stabilization time. In the period from minute 43 to minute 48 from the session start, the sensor was so loose that the data were measured notably high. The “X” mark denotes that period. The “T” mark is trauma self-narrating. The “N” mark is negative emotion changing abruptly. The “S” mark is stabilization technique. In this session, first trauma self-narrating and the negative emotion changing happened at around minute 15 simultaneously. At around minute 52, second trauma self-narrating and the last stabilization technique performed together.
Figure 1.
Every five-min SDNN and RMSSD in the first session. The 3-min data from the session start were removed for being considered the stabilization time. In the period from minute 43 to minute 48 from the session start, the sensor was so loose that the data were measured notably high. The “X” mark denotes that period. The “T” mark is trauma self-narrating. The “N” mark is negative emotion changing abruptly. The “S” mark is stabilization technique. In this session, first trauma self-narrating and the negative emotion changing happened at around minute 15 simultaneously. At around minute 52, second trauma self-narrating and the last stabilization technique performed together.
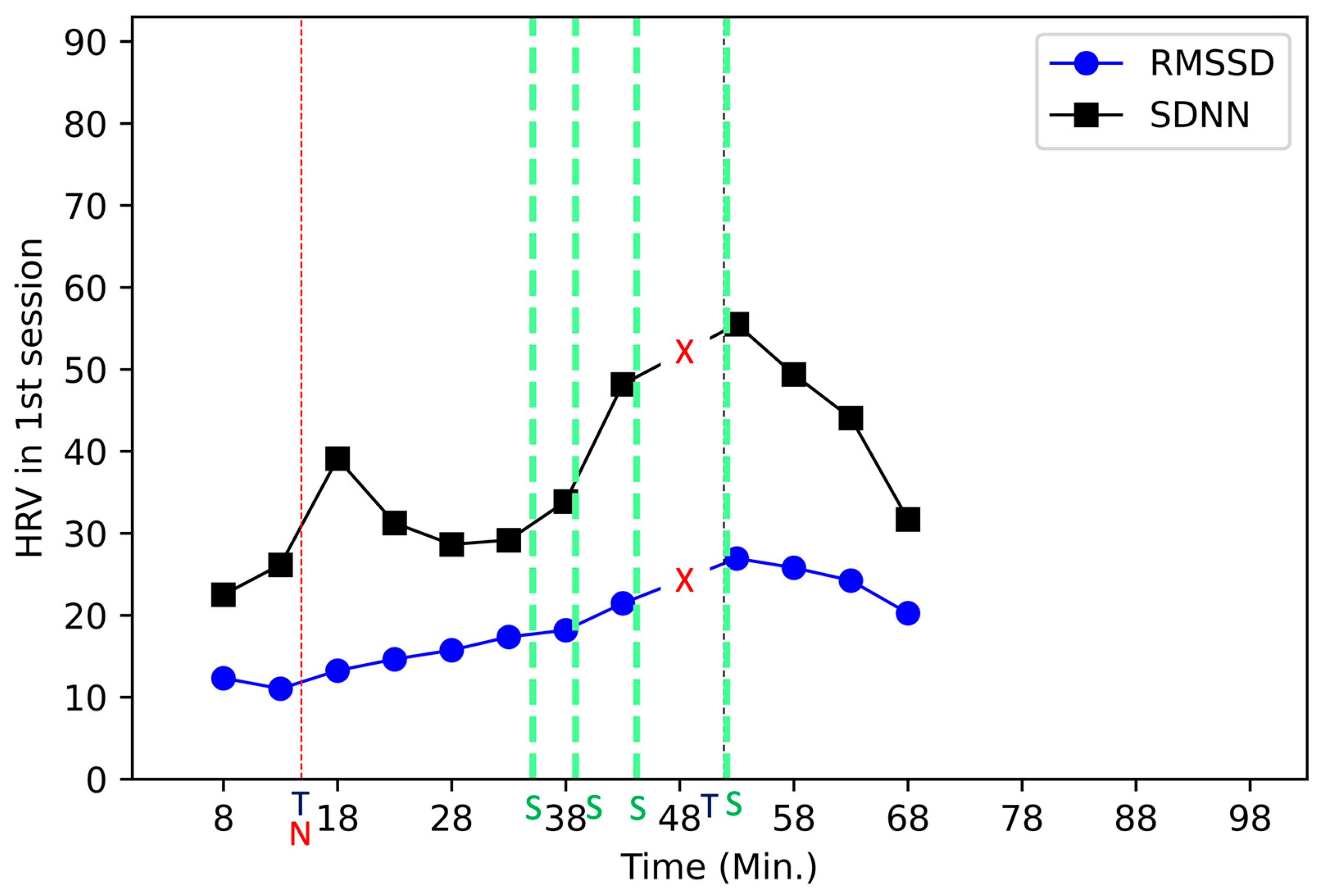
Figure 2.
Each 5-min SDNN and RMSSD in the second session. The 3-min data from the session start are omitted as part of the stabilizing time. The “S” mark is stabilization technique. The “N” mark is negative emotion changing abruptly. The “T” mark is trauma self-narrating.
Figure 2.
Each 5-min SDNN and RMSSD in the second session. The 3-min data from the session start are omitted as part of the stabilizing time. The “S” mark is stabilization technique. The “N” mark is negative emotion changing abruptly. The “T” mark is trauma self-narrating.
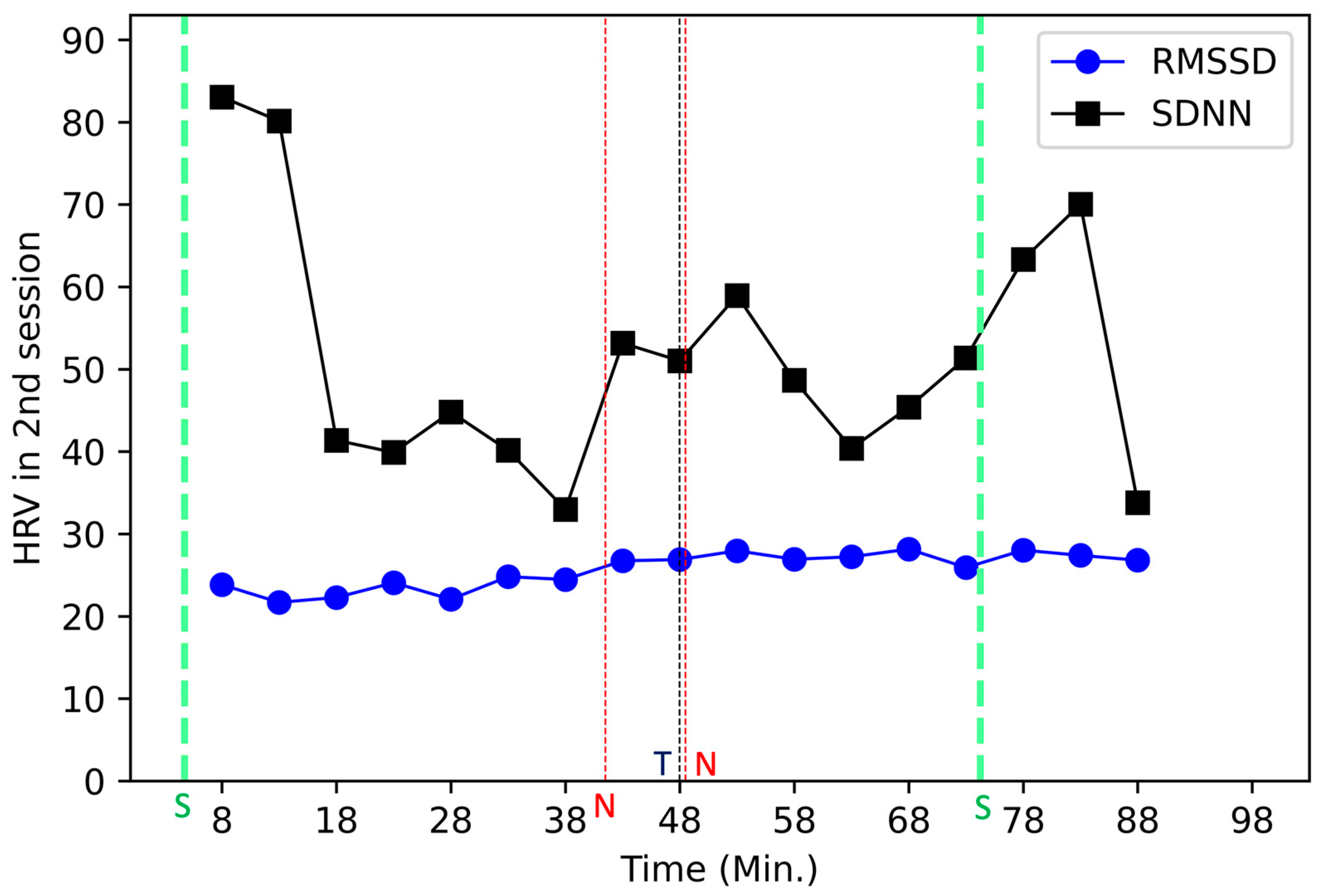
Figure 3.
Each 5-min SDNN and RMSSD in the third session. The 3-min data from the session start were omitted as being part of the stabilizing time. The “N” mark is negative emotion changing abruptly. The “P” mark is positive emotion changing abruptly. The “S” mark is stabilization technique. The “T” mark is trauma self-narrating. In this session, at around minute 49, the trauma self-narrating and the negative emotion changing happened simultaneously.
Figure 3.
Each 5-min SDNN and RMSSD in the third session. The 3-min data from the session start were omitted as being part of the stabilizing time. The “N” mark is negative emotion changing abruptly. The “P” mark is positive emotion changing abruptly. The “S” mark is stabilization technique. The “T” mark is trauma self-narrating. In this session, at around minute 49, the trauma self-narrating and the negative emotion changing happened simultaneously.
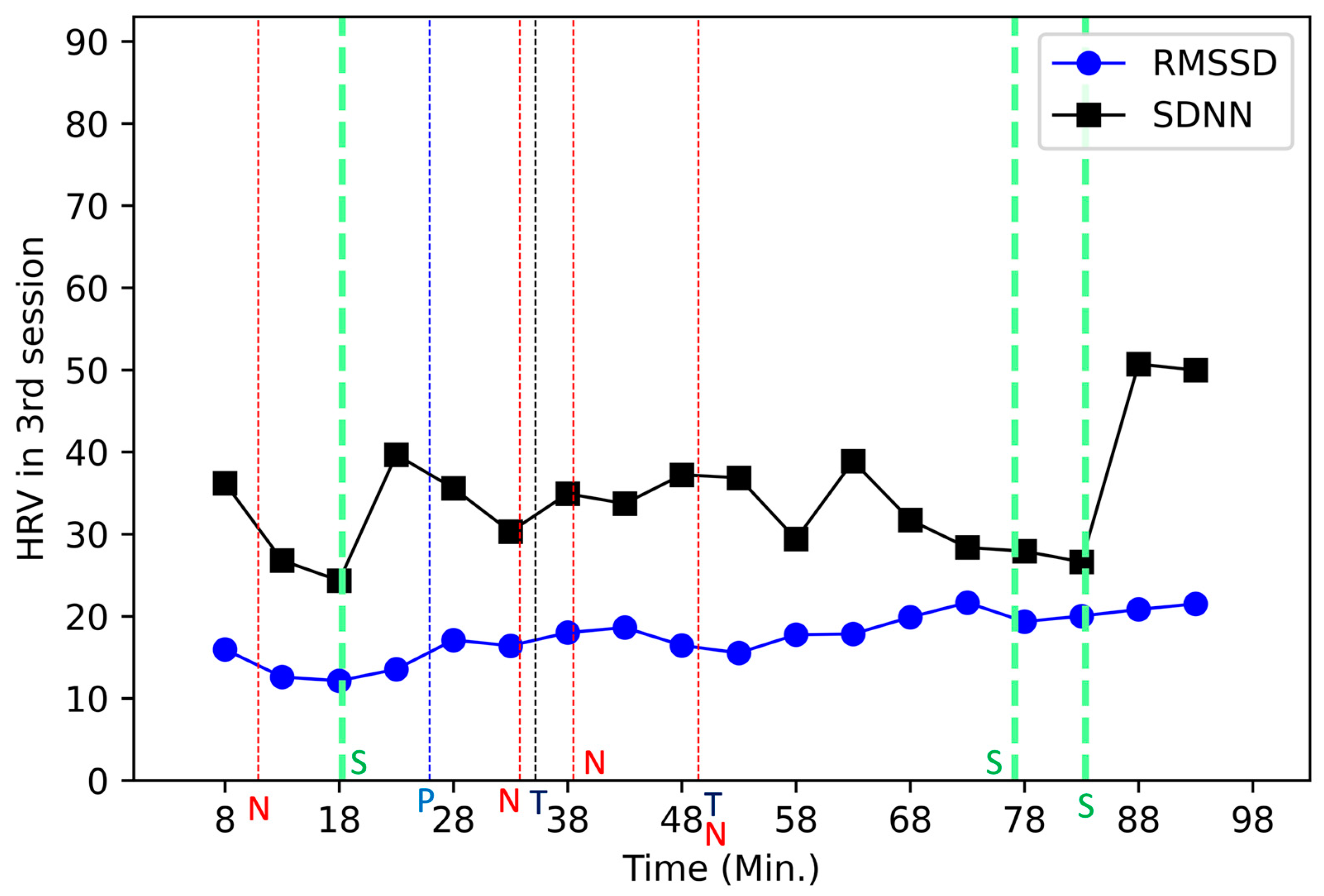
Figure 4.
Each 5-min SDNN and RMSSD in the fourth session. The 3-min data from the session start are omitted as being part of the stabilization period. The “P” mark is positive emotion changing abruptly. The “N” mark is negative emotion changing abruptly. The “S” mark is stabilization technique.
Figure 4.
Each 5-min SDNN and RMSSD in the fourth session. The 3-min data from the session start are omitted as being part of the stabilization period. The “P” mark is positive emotion changing abruptly. The “N” mark is negative emotion changing abruptly. The “S” mark is stabilization technique.
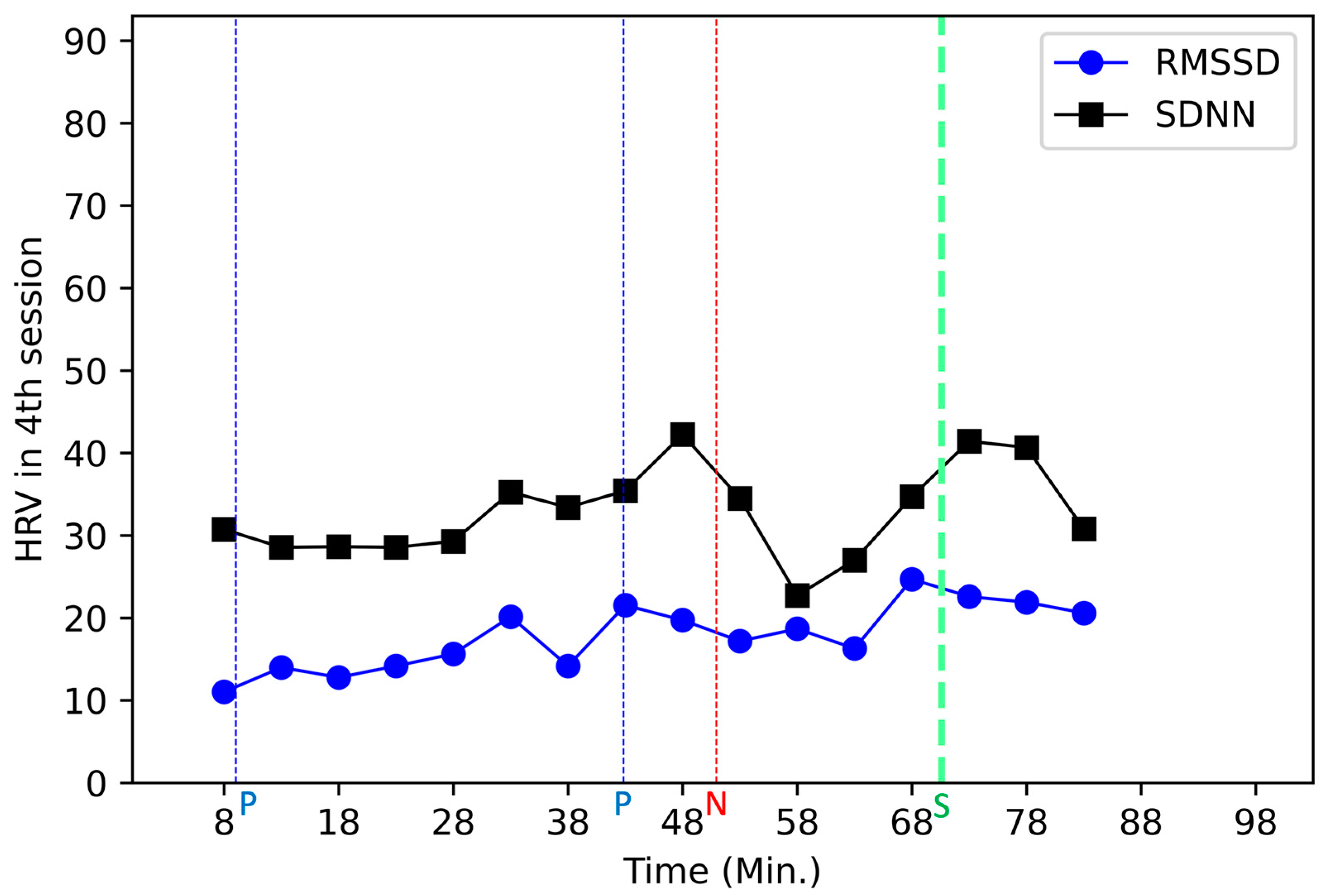
Figure 5.
Change ratio of the HRV when the subject telling his trauma at time 0. During all the 4 sessions, the subject told his trauma 5 times.
Figure 5.
Change ratio of the HRV when the subject telling his trauma at time 0. During all the 4 sessions, the subject told his trauma 5 times.
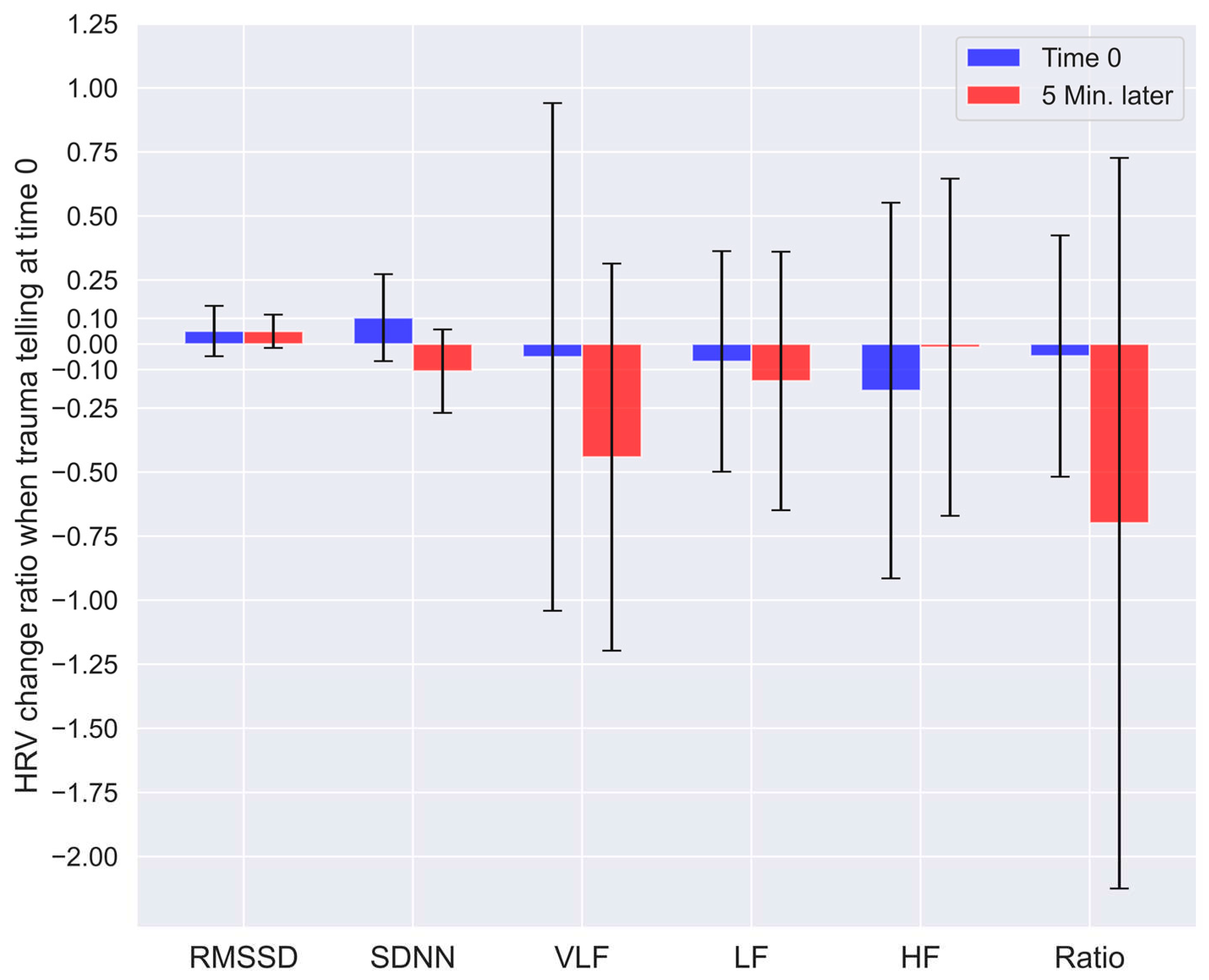
Figure 6.
Change ratio of the HRV when the stabilizing technique was performed at time 0. During all the 4 sessions, 10 times of the stabilizing technique were taken. The “*” mark indicates that the p value is under 0.05.
Figure 6.
Change ratio of the HRV when the stabilizing technique was performed at time 0. During all the 4 sessions, 10 times of the stabilizing technique were taken. The “*” mark indicates that the p value is under 0.05.
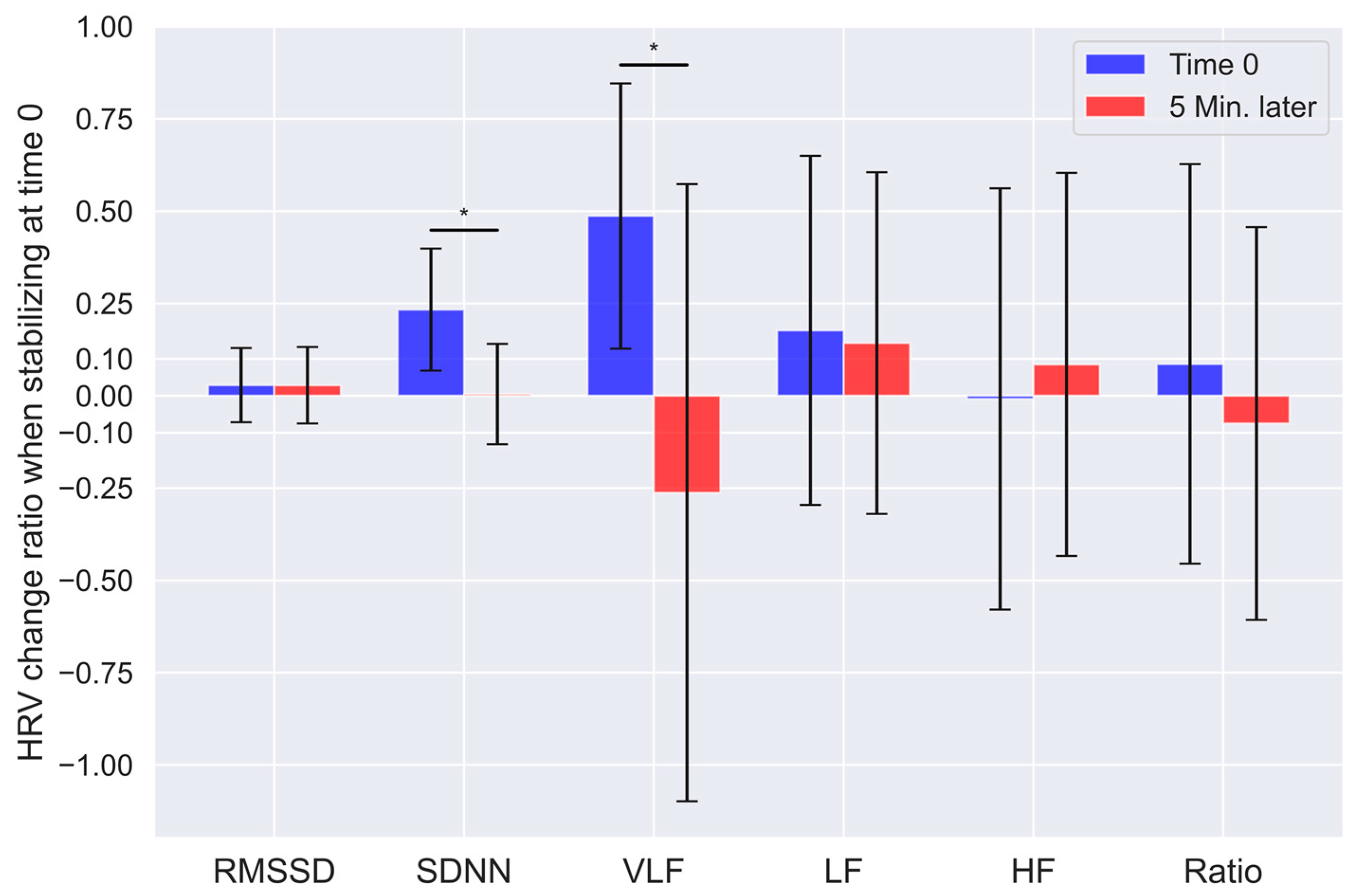
Figure 7.
Change ratio of the HRV when subject’s positive emotion change was observed at time 0. During all the 4 sessions, 3 times of the positive emotion change were observed. The “**” mark indicates that the p value is between 0.001 and 0.05.
Figure 7.
Change ratio of the HRV when subject’s positive emotion change was observed at time 0. During all the 4 sessions, 3 times of the positive emotion change were observed. The “**” mark indicates that the p value is between 0.001 and 0.05.
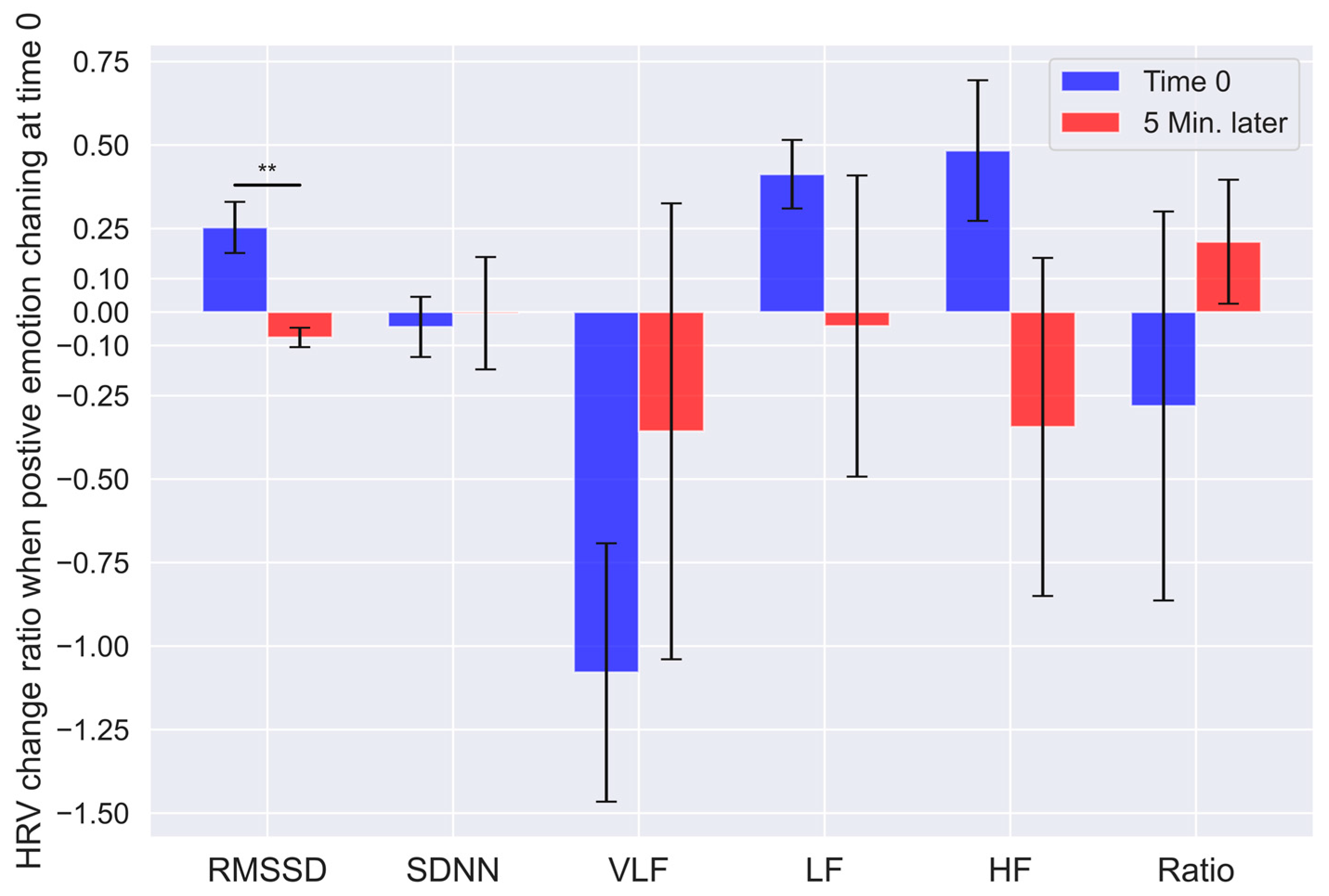
Figure 8.
Change ratio of the HRV when subject’s negative emotion change was observed at time 0. During all the 4 sessions, 8 times of the negative emotion change were observed. The “*” mark indicates that the p value is under 0.05.
Figure 8.
Change ratio of the HRV when subject’s negative emotion change was observed at time 0. During all the 4 sessions, 8 times of the negative emotion change were observed. The “*” mark indicates that the p value is under 0.05.
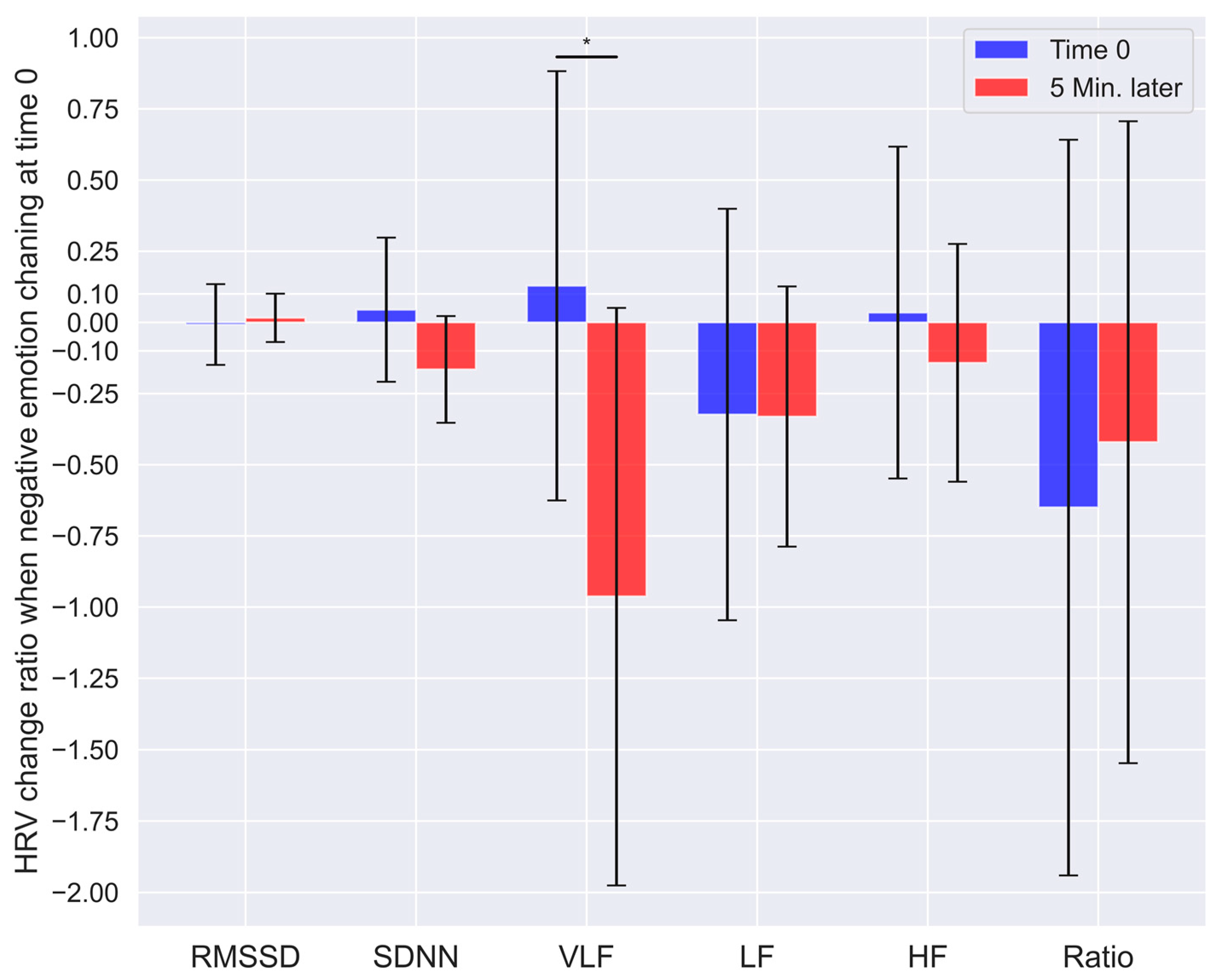

Table 1.
The scale change in the IES-R-K and AIS before, after, and 10 months after the proposed program. Lower score is more positive.
Table 1.
The scale change in the IES-R-K and AIS before, after, and 10 months after the proposed program. Lower score is more positive.
| Before | After | 10 moths after | ||
| IES-R-K (Full score: 88) |
Re-experiencing | 23 | 10 | 15 |
| Hyperarousal | 21 | 19 | 20 | |
| Sleep, emotion, dissociation |
14 | 15 | 10 | |
| Avoidance | 24 | 17 | 17 | |
| Summation | 60 | 43 | 40 | |
| AIS (Full score: 24) |
10 | 7 | 6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



