
Submitted:
17 July 2023
Posted:
19 July 2023
You are already at the latest version
Abstract
After the first release of synthalin B (dodecamethylenbiguanide) in 1928 and its later retraction in the 1940s in Germany and the retraction of phenformin (N-Phenethylbiguanide) because of the letal complication of acidosiss,metformin (1-1-dimethylbiguanide) was first released in France in 1959 and then in the USA in 1995 for oral treatment of diabetes type 2.
Acute gastrointestinal side effects often lead to dose reduction and strongly limit adherence to therapy.Main long-term consequences are deficency of vitamin B12 and of iron and sometimes also acidosis development.
Intravenously injected F18-labelled glucose in metformin-treated type 2 diabetics accumulates in the the small and even more in the large intestine.The densitometry picture observed in metformin-treated diabetics is similar to that observed in patients after bowel-cleansing or chronically taking different types of laxatives where the accumulated radioactivity can even reach values observed in colon cancer.
The glucose-lowering mechanism of action of metformin is therefore not only due to inhibition of glucose uptake in the small intestine but also to „attraction“ of glucose from the hepatocyte to the intestine,possibly through its secretion into the bile.Metformin is not different from the other biguanides ,synthalin B and phenformin.The mechanism of action,and the side effects are comparable to those of laxatives.
Keywords:
guanidene
; metformin
; diabetes mellitus type 2
; vomit
; diarrhea acidosis loss of body weight laxatives
; malabsorption
; anemia
; dehydration
; kidney injury
Introduction
Metformin (1,1-dimethylbiguanide) is a water-solule strong basic compound (1) belonging to the group of the biguanides.It has a molecular weight of 129,16,while metformin hydrochloride (Glucophage) has a m.w. of 165,62. Since 1957, when the „second life“ of the biguanides started (2) to reach nowdays about 200 million doses/day worldwide for treatment of overweight persons with diabetes type II alone or in combination with other orally administered antidiabetic compounds or with insulin (3).Many elderly diabetics type 2 suffer from hypertension and also take diuretics and other antihypertensive medication in addition to metformin (4).
1. History of Biguanide: From the First Animal Experiments to the Use of Synthetic Compounds for Oral Use in Overweight Type 2 Diabetics
After Minkowski in 1889 presented his observation that the pancreas is the source of a substance which regulates the glucose serum level (5), Falkenberg in 1891 reported his observation on the thyroidectomized dogs.Of 16 dogs, which died as a consequence of the operation, 11 presented glycosuria and two of the long-term survivors (several months) were diagnosed by Falkenberg (6) to suffer from what he called diabetes (in both cases parathyroid glands were found in place at autopsy).Glycosuria under such conditions was confirmed by Hirsch 1906 (7).
While looking for the substance responsible for tetanic symptoms observed in parathyreodectomized animals Fühner H (8) found that the substance guanidine, a product of protein metabolism, eliminated in the urine (9,10), causes muscle contraction by directly acting on the nerval plate (8). On the other hand,it was also found that a thyreoparathyreodectomy in dogs also causes hypoglycemia and depletion of glycogen deposits in the liver and no glycosuria (11).Extirpation of three parathyroid glands caused a reduction of absorption of dextrose given by mouth or subcutaneously.Normalisation of calcium serum level by administration of calcium lactate resulted in normalisation of blood sugar content (12), while it had been shown that ammonia elimination into the urine was increased (13). At the same time Burns and Sharpe demonstrated a marked increase of guanidine in the urine and blood of parathyreidectomized dogs and in the urine of children with idiopathic tetany (14).On the basis of the assumption that parathyroids are involved in glucose metabolism,Watanabe first studied the effect of subcutaneous guanidine administration on rabbit blood sugar levels and on urinary excretion of glucose and of ammonia (15-18).He administered guanidine hydrochloride subcutaneously into rabbits which were kept without food and water after administration and several blood glucose tests were performed after the start of the experiments.A decrease of glucose serum level was observed, wich was paralleled by a deterioration of general conditions until death occurred.
Frank,Nothemann and Wagner in 1926 (19) first studied the hypoglycemic effect of guanidine on rabbits and realized that it worked like a poison after subcutaneous administration and that, before death, the animals developed hyperglycemia.Authors then tested herring-sperm extracted- and then synthetically produced- guanidine. They called it Agmatin (aminobuthylenguanidine, derived from the amino acid arginine). In the attempt to dissociate the toxic from the hypoglycemic effect, they found that a non-toxic dose of this compound was able to induce a decrease of glycemia .A further modification to aminopenthylguanidine was able to induce a decrease of blood glucose similar to that observed after insulin administration. In an attempt to increase the glucose-lowering effect, structural modifications were performed and synthalin A and B were generated. Subcutaneous injection of the substances in pancreatectomized dogs was able to reduce blood sugar concentration in a dose-dependent manner before toxicity symptoms became evident.The speed of the hypoglycemic effec was slower than that observed after insulin injection.A small increase of the dosis given orally was sufficient to achieve an effect similar to that observed after the subcutaneous administration .“Die Versuche über die wir bis jetzt berichtet haben,sind fast sämtlich mittels subcutaner Einverleibung ausgeführt. Es stellte sich bald heraus,dass die orale Darreichung diesen Stoffen nichts von ihrer Wirksamkeit nimmt“ (19 p. 2102).Die Tatsache der oralen Wirksamkeit eines antidiabetischen Agens ist praktisch so bedeutsam,daß sie zur Anwendung des aktivsten Körpers der ganzen Reihe, des Synthalins, auf den Menschen verlocken mußte.Die Übertragung in die menschliche Therapie durfte aber nur sehr vorsichtig vorgenommen werden; denn unsere Körper stellen kein hypoglykämisierendes Prinzip in schärfster Reinheit dar wie das Insulin, sondern es haftet ihnen noch ein Rest der Toxizität der Guanidine an, anscheinend nicht mehr die Erzeugung allgemeiner Übererregbarkeit des Nervensystems, die den methylierten Derivaten des Guanidins das Tetaniegift vermuten läßt, sondern eine andere, uns ebenfalls bereits von der chronischen Guanidinvergiftung der Katze her bekannte Wirkung, die sich in Freßunlust, Neigung zu Erbrechen, verbunden mit der Mattigkeit der Tiere äußert“.
After the maximal toxic dosis in rabbits and dogs was found, first clinical attemps in diabetic persons were mature.The effect of orally administered synthalin was compared to that of subcutaneously administered insulin, namlely on the effect of peripheral glucose consumption and on glucose storage as glycogen.“II. Wir versuchten experimentell festzustelle einerseits ,ob die Substanz die Verwertung des Zuckers in den Verbrauchsorganen begünstigt und andererseits seine Speicherung als Glykogen fördert, das heißt also, ob sich die Wirkung unseres Präparates mit denen des Insulins vergleichen lassen“ (19 p.2012)
To demonstrate the first effect, insulin was injected into the arteria femoralis of a pancreatectomized dog and a decrease of venous blood glucose level compared to the arterial level was determined.A similar effect was reported after intraarterial injection of synthalin.While a higher venous glucose level could be observed three hours and 50 minutes after the intraarterial injection, a continous increase of the difference between the venous and the arterial glycemia up to 22 mg, two hours and 45 minuntes after the injection, was observed. It took two hours before the biginning of the decrease of glucose blood levels could be observed in this dog.The authors hypothesized an extrahepatic consumption of glucose as observed after injection of insulin.Contrary to what could be observed after administration of insulin, however, only trace amounts of hepatic glycogen were found in the pancreatectomized fasting dog when non-toxic amounts of synthalin were injected(19)….Sie erlauben aber trotzdem mit Sicherheit den Schluss,daß es auch mit unserer Substanz möglich ist,einen Glykogenansatz bei pankreasdiabetischen Hunden zu erzielen,da wir aus den Untersuchungen Minkowskis wissen,daß das Glykogen der Leber diabetischer Hunde nach kurzer Zeit regelmäßig bis auf minimalste Spuren verschwindet und auch nach Verfütterung von sehr großen Traubenzuckermengen-170 g-nur ganz geringe Glykogenmengen-im Höchstfalle waren es 0,14%-nachzuweisen sind“ (19,p 2013).
After the successful animal experiments were considered concluded, first diabetes patients were treated with synthalin.Therapy was started with different dosages in insulin-dependent patients , insulin dosages could be reduced and glycosuria disappeared.After two, three days however, therapy had to be temporarily interrupted (24-36 hours) because of gastrointestinal side effects:nausea,vomiting,diarrhea,gastric pain.The therapy was more successful if accompained by a diet.“Die Pause ist aber notwendig, da das Präparat Nebenwirkungen besitzt, die sich bei den von uns jetzt gewählten Schemata fast gar nicht mehr, bei Überdosierung aber sehr schnell bemerkbar machen können. Sie bestehen in Appetitlosigkeit, Drücken in der Magengegend, Unbehagen im Leibe und beschleugneter Peristaltik und können sich bei starker Überdosierung zu Übelkeit, Nausea und schließlich zu Erbrechen und gelegentlich zu Durchfällen steigern“ (19,p.2106)
Under these conditions, authors calculated that 1 mg synthalin administered orally generated the same effect as one unit insulin (20) in the reduction of the amount of glucose eliminated in the urine.Furthermore, authors found that synthalin was able to reduce the serum glucose level below the glucosuric concentration,to abolish acidotic episodes and to reduce the symptoms of the disease, namely polyuria and polydypsia.Comparable results were obtained by oral and subcutaneous application of the substance.
In a comment to the presentation of his coworkers, professor Minkowski(21) certified that the data generated in his own department were valid. Based on previous experiences from the use of similar compounds,he however also expressed some caveats as to the insulin-like effects attributed to previously used substances,they could be due either to the calorie- restricted diet alone or to the impairment of the proper intestinal glucose handling .He meant that it was justified to define synthalin as“ insulin-like substance“.It however should not be considered as an insulin „substitute“ as the effect was not as strong and rapid as that of insulin (20).
He added to his judgment that it was too early to definitively decide about the grade of efficacy for the treatment of mild diabetes and for the possibility to develop substances with less side effects. He also prophetically supposed that in short time there would be many experiences from several sites. He expressed the wish that such trials and their reporting would be performed with necessary, strong scientific rigor.He prophetically wished that previously reported similar insulin-like effects of natural anti-diabetic substances should be studied again under the actual conditions as reported by his coworkers(19).
After the first supporting experiences were published (22-26), Frank, Nothmann and Wagner published their next experience with the „new“ bigunanide,synthalin B (dodecamethylendiguanidin).This was a further molecular development in the attempt to reduce the gastrointestinal side effects observed whith synthalin(27). Initially, the substance induced diarrhea,which was more frequent than under synthalin but less strong and more temporary.Indication for this therapy was considered to be diabetes of the older patient normally reluctant to take the prescribed diet ,while treatment of choice for the joung diabetic patient remained insulin administration (27).Synthalin B was approved in Germany and also made available for further studies in England (28) and in the United States of America (29). These experiences delivered some support but also confirmed the high frequency of gastrointestinal side effects (28,29).The data were summarized and also critically commented in an article in Nature in January 1928 (29) .It was underlined that synthalin, in spite of the advantages of the oral administration and of its more prolonged action, is not comparable to insulin because its action is slower in onset and because of the unpleasent side effects „suggesting intestinal irritation“(29).The author repeated the judgment of the late Minkowski 1926 that synthalin was not „ a substitute for insulin“ BUT THE FIRST RESULTS OBTAINED WITH THAT SUBSTANCE WOULD ENCOURAGE the continuation of the search for better compounds with insulin-like effects (29). In spite of these positive experiences the search for new guanidine-compounds continued (30) and synthalin remained as an oral ANTIDIABETIC DRUG on the german market until 1940. Then retraction from the maket occurred because of the seldom but fatal acidosis .Other compounds were developed and used for treatment of obese type 2 diabetics (30-33) until retraction for the same reason was determined. Metformin, a „new“ biguanide was first described by Sterne 1957 (2 ) and first approved in France 1959.It was used in the UK where the lowering effect on body weight was described when compared to the opposite result obtained with chlorpropamide after twelve months of treatment in obese diabetics (34).By that time „some non-tissue-forming catabolic process“ should be hypothesized if reduction in food intake was not the explanation for the tendency of weight loss in obese diabetics ( 34,35).After the positive trial results were published (36-38 )metformin was approved as one more oral antidiabetic drug in the United States in 1995 ( DeFronzo 36-38 ) and defined 1996 as the „cousin“ of phenformin by Campbell and collagues (39).
United Kingdom Prospective Diabetes Study (UKPDS) and Metformin
After several reports claimimg positive effects of orally administered drugs including metformin alone or in combination with other oral substances (39 ) but also with insulin (40 ) were published, „new medications for attempting to nearly normalize blood glucose levels could not have arrived at a better time“ ( 41) the enthusiasm about metformin,the first drug that did not induce increase of body weight, did not induce increase of insulin serum level, built up continuously although the true mechanism of action of this compound, which was poorly absorbed (30% eliminated with the stool) and quickly eliminated unchanged via urine was only speculative.In addition, dose-dependent gastrointestinal side effects caused the drug to be withdrawn in up to 50 % of the study patients (42-45).
The results of the large UKPDS-trial,which was started 1977 in England, contributed to the enormous „popularity“ of the substance (46,47).The UKPDS-reported positive results in the reduction of microvascular consequences of type 2 diabetes in the subgroup of overweight diabetics treated with metformin.They represented,in spite of several critical comments (48-51)especially about the statistical significance of the obtained results, the definitive establishment of long-term oral therapy alone and/or in combination with insulin (52) and other oral antidiabetic drugs (53).
UKPDS: Some Details About the Metformin Response (46,47)
One thousend seven hundred and four overweight patients with newly diagnosed diabetes mellitus type 2 in 15 centers in the UK were randomized in 4 groups: 1.simple diet high in carbohydrates and fibers and low in saturated fats with calory restriction (411=24%),2.chlorpropamide group (265=16%),3.glibenclamide group (277=16%),4.insulin group (409=24%).A comparison of the results of the 411 overweight patients under conventional treatment (simple energy restricted diet) and of the 342 overweight patients treated on energy restricted diet with metformin was performed after a 10.7 years of median duration (46,47).Furthermore, a comparison of the results observed in the metformin group (34=20%) was performed with those observed in the 951 patients of the three groups of patients under intensive therapy with chlorpropamide,glibenclamide or insulin (46).
In addition, results obtained in a group of patients,both normal weight and overweight,who 1990 were found to have a fasting plasma glucose between 6.1 and 15.0 mmol/L without symptoms of hyperglycemia (48), despite maximum sulphonylurea dose, were then divided into a group continuing solphonylurea alone (268 patients) and a second group on sulphonylurea and metformin (269 patients) .If those patients on sulphonylurea alone developed marked hyperglycemina metformin was added.
If the patients on the combination therapy developed marked hyperglycemia, therapy was changed to insulin.The finding of increased mortality in the group of metformin- and sulphonylurea- therapy-patients suggested a comparison of the two groups.
The results in terms of mortality of combination of the two drugs (sulphonylurea and metformin) were also compared with the other therapy groups.
Metformin was started with a dose of 850 mg/day which was then increased to twice daily; then two tablets in the morning and one in the evening meal were given.When symptoms of diarrhea,nausea or other gastrointestinal disturbances occurred, the daily dose was reduced to that which did not cause such side effects.
When marked hyperglycemia developed, glibenclamide was added to metformin. When the combination also failed to reach the goal of a fasting plasma glucose under 6.0 mmol/L ,therapy was switched to insulin.
The study was closed 1997 after 20 years with a median follow-up of 10.7 years for the original groups and of 4 years for the two groups which were randomized 1990 (after 7.1 years from the first randomisation) when metformin was added to sulphonylurea.Authors stated that the data obtained „suggest“ that metformin added to diet-treated overweight patients with diabetes type 2 reduced the risk of diabetes -related endpoints,diabetes-related death and all-cause mortality.On the contrary, addition of metformin to sulphonylurea increased risk of death and all-cause mortality (within the 4 years after randomisation!) both in non-overweight and overweight patients.The surprising finding, however, was also that metformin did not reduce cancer-related mortality (18/341 compared to the diet-alone group (21/411),even more surprising was the finding that the number of cancer related-deaths in the combination therapy group was more than double (14/268) than in the sulphonylurea only group (6/269).Authors also commented the positive findings in the metformin-diet-treated overweight patients compared to the diet-only group in spite of comparable HbA1c-improvement that „the additional effect of metformin on risk reduction of all the endpoints attributed to the hyperglycemia is not explicable by the improvement of the glycemic control“.
In addition,although the serum levels of total cholesterol,LDL-cholesterol and HDL-cholesterol were added to the patient‘s basic characteristics and further measurements were performed at each visit 3,6,12 months and every year thereafter, no significant role was attributable to their changes even in those patients who were unresponsive to high dose of insulin( ).Unfortunately the relvance of this finding was not discussed in consideration of the mounting literature output claiming the central role of serum lipids in the food and in the blood for artherosclerosis and microvascular and macrovascular endpoints (49-51).
A possible role of cigarette smoke and of consumption of alcoholic beverages on some cardivascular endpoints (e.g stroke) and cancer development, was not discussed.
In fact,although the approximative numbers of patients reporting cigarette smoke and intake of alcoholic beverages (without quantitative mention) were given under the patient characteristics at baseline, there was no request of this attitude in the questionary presented at each control visit (at least not reported in the publications) and no separate analysis of such relevant risky behaviour was performed for the dead patients.
The overwehlming role of cigarette smoke not only on cancer development but also as a risk factor for development of coronary heart disease (52) was already known in the early 1950ties from the Framingham study in the USA (53) confirmed later (54,55) and from the investigations of Doll in the UK (56-58) .But also within the seven countries study (59) as supported by Grombaek et al.(60) the negative role of heavy consumption of alcoholic beverages on survival was underlined (61)
An oral therapy was too appealing for the increasing number of patients with increasing body mass index (BMI) and diabetes type 2. Although the effect of this therapy on the macrovascular consequences attributed to diabetes,stroke,fatal or non fatal myocardial infarction ,peripheral arterial obstructive disease was quite low (30% risk reduction compared to diet-only), not-significant compared to the other treatment groups, an optimistic „suggestion“ was made without discussing that cigarette smoke was the leading cause of cardivascular disease and death, followed by cancer-related deaths (52,61).The optimistic consequences drawn from the study were also criticised (especially from the statistically point of view) by different diabetologists (62-66).
Ten years later It was confirmed that metformin reduces glucose serum level, it also reduceses the serum level of insulin.This especially during the early and temporary (up to 1 year after therapy begin) decrease of body weight in obese patients with type 2 diabetes (67).
Pharmakocinetic and Pharmacodynamic of Metformin
After oral administration of metformin hydrochloride, about 60% of the compound is absorbed in the first part of the small intestine ,taken up by the liver and from that organ released into the systemic circulation and eliminated unchanged through the kidney by glomerular filtration but also by tubular secretion and can be found to fast 100% in the urine (68). After intravenous administration, Pentikäinen found some C14-labelled metformin in the saliva but not in the faeces(69).After oral administration of C14-metformin the bioavalibility in three of healthy volunteers was 61% and 51% of the administered dose was found at 48 hours.The recovery in the feces of one volunteer from whom the stool was collected for one week was 29.4% and 90.5 % together with the activity recovered in the urine.Metformin was not bound to proteins neither in vivo nor in vitro (69).
C11-metformin (9.5 microSv/MBq=ca.1.1 microgram), first injected intravenously, allowed to study its biodistribution in humans (70) by the PET-scan technique.Most of the activity was found in the liver,the kidney and the urinary bladder.Activity peaked immediately after injection and most of the compound was cleared from the blood 20 minutes after injection.In the kidney there was a quick intense activity (80% of the injected activity) with an equally rapid decrease with a reversibility velocity similar to that of the liver but faster.In the liver the peak of the activity was of course lower (15% of that in the kidney) because of the much larger volume of the cellular distribution (Fig 1 upper panel).
After rapid ingestion of the strong basic compound C11-metformin (18.1micro Sv/MBq,half-life= 20.4 minutes) dissolved in water containing 100mM (NH4)2-HPO4 [pH=5], consecutive whole-body scans were performed.Dosimetry calculations were performed for the stomach content,small intestine,liver, kidney and bladder content.It was demonstrated that hepatic metformin uptake is very rapid and fully reversible but the accumulation of the activity is higher than after the intravenous administration, as ,although slower, the tracer delivery comes from the portal blood through the liver first.Two hours after the oral ingestion of the tracer the bulk of the radioactivity is still in the intestine (Fig.1 lower panel) and no further observation of the fate of the radioactive metfomin was possible.
It is understandable that the study performed by Pentikäinen and collagues with 14C-labelled metformin could only be repeated by the addition of „cold“ metformin tot he 11C-labelled compound.This would most probably accelerate the intestinal passage as most of the conventional drug- containing tablets also contain polyethylenglycol (3-6.000) as additive,which is also a laxative.
Although an active transport of metformin through the membrane of the hepatocyte has been exstensevly discussed by Gromensen et al (70),it has to be mentioned that hepatic densitometry pictures similar to those observed after intravenous and oral administration of C11-metformin can be observed also after the injection of C11-nicotine (71) or even of C11-Donepezil,a high-affinity antagonist of acetylcholinesterase normally used as drug in the treatment of patients with Parkinson´s disease (72,73), it can not be ruled out that there is a diffusion into the space of Disse through the fenestrae of the sinusoidal endothelial cells (74,75) and that the compound is then whashed out from the interstitium back into the heptic vein.It may be therefore more approriate to speak about hepatic metformin „extraction“ ( 76) than about uptake.
The kidney to blood activity ratio was identical independently of the administration route of the radioactive metformin . Some discrete uptake of the tracer was found in the salivary glands and discrete uptake was found also in the intestine.No activity was found in the gallbladder.Significant amounts of the tracer passed to the small intestine 10 minutes after ingestion.
Despite the increasing popularity, the mechanism of action of metformin (gluco-phage of Sterne) has remained elusive until nowadays.
Especially after the report of Bonora et al. (77) and of Sum et al (78) on the lack of metabolic changes after intravenous administration of metformin hydrochloride, attention concentrated mostly on pharmacokinetic studies performed after oral administration of immediate- or retarded release-metformin formulations and of different dosages at different time of the day.
Bonora and collegues (77) found no significant change in fasting plasma level of glucose,insulin,C-peptide, glucagon and growth hormone after intravenous injection of 1g metformin as bolus in 15 non-diabetic subjects (4 males and 11 females) after a 12-hours overnight fast.Blood was drawn 15 minutes and up to 30 minutes after injection of metformin hydrochloride dissolved in 10 ml distilled water.The finding ended the discussion about a possible direct effect of metformin on insulin production in the pancreas.Sum et al.(78) performed double-blind randomized crossover study in nine type 2 diabetic patients (6 female and 3 male,HbA1c 8,8 vs 8,6)) on oral metformin therapy (Glucophage,Lypha).
After a 10 hour fasting period and having omitted the morning metformin dose,D-glucose,[3-H3]-glucose and metformin/Nacl were injected intravenously.Metformin was continously infused to achieve a serum concentration at lower therapeutic level and then (after the first 120 minutes) increased to reach a high therapeutic range of 5-7 mg/L . Glucose was infused to reach and then maintain a concentration of 5 mmol/L.Blood samples were collected at 10-minute intervals.Urine samples were also collected.After the first increase of metformin serum level from 1.64 to 6.57 at the end of the second step a continuous decrease of metformin level was measured under NaCl infusion.
The study was repeated between 10 and 20 days after the first study and no difference was found between the two study days in fasting glucose-,and insulin-plasma-levels and in metformin concentration.No difference between control and metformin studies in hepatic glucose disposal,peripheral glucose disposal,glucose oxidation and blood lactate concentrations was found.These results demonstrated that there was no acute effect of increasing metformin serum concentration in type 2 diabetics on hepatic glucose production or peripheral glucose disposal.
Pharmacokinetics and pharmakodynamics of metformin were then studied in NIDDM and healthy subjects both in male and female taking single- or multiple-daily -dose (78).No statistically significant difference was found between healthy subiects and NIDDM-patients in the pharmacokinetic parameters after a single dose of 850 mg of metformin hydrochloride between the 11 males and the 7 females studied.
No single dose (850-2.550 mg) of metformin significantly decreased the postprandial glucose serum concentration.When the single dose was augmented the clearance/bioavailability ratio increased in both partecipant groups, mainly due to decrease of bioavailability than to increased clearance which was lower when 1.700 or 2550 mg than 850 mg were administered in NIDDM and was significantly lower in healthy persons.It was confirmed that bioavailability decreased with increase of the administered dose.In fact it was previously reported that bioavailability decreased from 86% to 42% when the dose was increased from 250 mg to 2.5 gm .As an explanation for this phenomenon it was hypothesized that metformin permeability is limited as a non lipophilic compound,this is confirmed by the 30-60% bioavailability in absence of hepatic extraction and by the fact that bioavailability of metformin of intermediate release formulations is lower than that of immediate release formulations.
In addition it was found that intake of food decreases the absorption of metformin by about 25%.While multiple doses of metformin decreased glucose fasting serum concentration and also postprandial glucose level in diabetic partecipants, no effect on glucose serum level was detected in healthy subjects.Ths is not due to different pharmacokinetics of metformin in each group and can only be observed also in non diabetics if the serum glucose level has been artificially raised.
Furthermore, the glucose-lowering effect of metformin in NIDDM was correlated to the level of severity of fasting hyperglycemia and significant reduction of preprandial insulin plasma level was observable after multiple doses of metformin hydrochloride.Interestingly a statistically significant decrease of postprandial (0-2 hours post meals) insulin concentrantions was observable in healthy subjects after metformin administration (4-6 hours) both of different single doses (850-2550 mg) and multiple doses.
It was justified to conclude that the preprandial glucose-lowering effect of metformin in NIDDM-subjects and the early postprandial in healthy subjects is not dependent on stimulation of insulin production.
Besides the previously hypothesized fact that a clear effect of metformin on lowering glucose concentration can only be found when administered orally by reducing glucose absorption (79) in the intestine ,additional effects like inhibition of hepatic glucose production, improved glucose uptake and utilisation were mentioned toghether with weight reduction and reduction of plasma lipid levels and prevention of some vascular complications (80).
Short- and Long-Term Side Effects and Adherence to Metformin Therapy
a)Short-term side effects of metformin therapy.
As described by Frank and colleagues (19) at the first use ,synthalin administration causes nausea,loss of appetite,increased intestinal movements,gastric pain,vomiting and also diarrhea.For this reason they developed a therapeutic procedure consisting of increasing the dosis for the first 3-4 days followed by an interruption of drug administration of 1-2 days.It is therefore understandable that many diabetics,especially the older ones can not tolerate the medication,dizziness,tiredness abdominal cramps, asthenia,myalgia and an altered metallic taste (81-84) as confirmed to be more frequent in patients treated with metformin than in the placebo treated control diabetics.This has been attributed in part to the intestinal disturbance of the bile salt metabolism by metformin (85-88) which is eliminated to more than 30% of the oral dose with the stool.The increase of bile salt elimination in the stool has been observed also in patients with chronic constipation treated with elobixibat, a laxative approved in Japan for treatment of chronic constipation (89),probably similar to what has been discussed recently for other antihyperglycemic drugs (90).
Metformin can cause, besides the above mentioned side effects, also flatulence,abdominal bloating,heartburn,headache,agitation,chills.
After the first reports of lactic acidosis (38,40),similar to the previously used guanidines (91-94),at time of release by the Food and Drug Administration (FDA) such a life-threatening complication has been published only sporadically and has been considered to happen significantly more seldom compared to tolbutamide .It has been described
especially in diabetics with reduced kidney function (95-97) and in emergency conditions such as severe COVID-19-infection (98-103) in hospitalized diabetics.
The above-mentioned intestinal effects and side effects of metformin not only can cause the complete withdrawal from metformin intake but also the long-term more or less complete adherence to the therapy (104-110).Furthermore,although the significant loss of body weight observed especially at the beginning of metformin therapy (46), can be seen as an achievement as it is known that overweight ,obese elderly diabetics do not tolerate diet restrictions.It should however be seen as a possible acute consequence of the gastrointestinal side effect of the drug.In fact there could not only be a negative effect of the metformin on food- but also on fluid-intake with consequent dehydration , tissue hypoperfusion,hypoxia and tissue damage.The following kidney injury could conditionate lactate overproduction and lead to acute lactic acidosis,the symptoms of which may be similar to the side effects of metformin with the main distinctive characteristic of dehydration,namely tissue hypotension.
b)Long-term side effects of metformin therapy.
In their 10-year follow-up report, after the end of the UKPDS, Holman and coworkers (67) describe that the metformin group-patients were followed 17.7 years with 8.8 years of post-trial follow-up.Overall mortality was 44% (51.5% cardiovascular cause of death and 24.2 the cause of death was cancer).Baseline differences in surrogate marker glycated hemoglobin disappeared after the first year of intensive-therapy.Although there was no difference in levels of blood pressure and plasma creatinine was not significantly different within the two groups,the plasma creatinine levels in the metformin group were 15% higher then those in the conventional therapy group. As about 10% of the patients were treated with diuretics because of hypertension,(110) both metformin and diuretics can eventually increase dehydration,which also naturally develops with increasing age in elderly persons.
Metformin treatment in type 2 diabetics is associated with early anemia development, which is most probably due,but not solely, to Vitamin B12 absorption inhibition (111-116).Vitamin B12 absorption inhibition could also explain development of peripheral neuropathy in elderly diabetics treated with metformin (117).
Anemia and iron deficiency under long-term metformin treatment (> 5 years) has been descibed by Ahmed and collagues (118)
Mechanisms of Action of Metformin Therapy: Direct or Indirect?
The mechanism of action of metformin in lowering glucose serum level has been discussed, for seven decades since its introduction as therapeutic option in overweight type 2 diabetics (3,119-123) and is still under discussion as reported in the most recent publications (110).
In experiments performed in metformin treated fa/fa rats Penicaud et al.(124)demonstrated that there was no glucose utilization in insulin-dependent organs and it was even decreased in skeletal muscle.Authors found an increased glucose utilization in the stomach and small intestine of the metformin-treated rats.The experiments made clear that metformin does not exert its hypoglycemic action through an increased insulin secretion but it rather causes an increased glucose elimination (124).Bailey also underlined glucose utilization in the intestine even in the fasted state using glucose from the vascular compartment(87).
Besides the inhibitory effect of glucose absorbtion in the small intestine a reduction of the glucose production in the liver is still under discussion.This is however difficult to understand as intravenously injected metformin does not have any effect on glycemia (77,78).
A further indirect mechanism of the glucose -lowering effect of orally administered metformin has been postulated,namely through the increase of the incretin GLP-1- production in the small intestine mediated by bile salts (125).On the other hand if it has been demonstrated ex vivo in the perfused rat ileum that carbohydrate luminal perfusion increases the release of glucagon-like peptide-1 into the mesenteric vene (126) and a similar increase could be detected in the portal blood of diabetic and non-diabetic cirrhotic patients after introduction of a study meal (69 gramms carbohidrates) into the small intestine and no significant difference in the peripheral insulin serum level was found (127) between diabetic and non-diabetic patients. As GLP-1 should reduce glycemia by stimulating insulin production in the pancreas only in hyperglycema,increased insulin serum level under metformin therapy should be the precondition for the indirect hypoglycemic effect .Insulin serum concentration under metformin therapy however does not increase,either it remains unchanged or it is decreased (46).The administration of GLP-1 RA exanatide in type 2 diabetics seems on the contrary to use a mechanism similar to that of metformin by inducing a significant reduction of body weight in a short-term treatment (128).
Kim and coworkers described accumulation of injected F18-FDG in the lumen of patients suffering of non-inflammatory diarrhea or constipation and for the first time intravenously injected, radioactive glucose in the stool(129).Gontier and collague studied localisation of F18-FDG injected in diabetics type 2 and found a significant increase of the radioactively-labelled glucose in the wall, but also in the lumen of the small bowel and of the colon in patients treated with metformin compared to that of non-metformin treated diabetics,which was not different from that of non-diabetics controls (130).Author stated that „the digestive tract is the only tissue responsible for a large glucose utilisation enhancement“.
Morita and coworkers by using positron emission tomography (PET)-MRI, recently found that the maximum standardized uptake value (SUVmax) of F18-FDG in the intestine (jejunum,ileum and right or left hemicolon) of metformin treated diabetics was higher than that of the control group.More importantly the study permitted to differentiate the SUVmax of the intestinal wall from that of the intestinal lumen.The SUVmax of the intraluminal space in metformin-treated diabetics was greater than that of controls (Figure 2).On the contrary the SUVmax of the intestinal wall was similar in both groups (131).An increased accumulation of the injected tracer seems to be appreciable (Figure 3) also in the liver of metformin-treated diabetics up to 48 hours after interruption of the oral uptake of the drug (132,133).
Accumulation of F18-FDG in the large intestine (Figure 4) has been found also in persons who regularly use laxatives (136-137).SUVmax can even reach levels,which simulate those of colorectal neoplasms (Figure 5) in patients with chronic constipation (138).
It seems justified to conclude that metformin not only induces glucose „ malabsorption“ as descried by Bechtold et al 1969 (111),it also may „attract“ glucose from the intestinal vasculature into the lumen of the small bowel which is then transported and concentrated in as stool of the large intestine. Under the influence of intestinal metformin, the reduced glucose uptake from the intestine into the portal blood could also be compensated by an increase of an insulin-mediated uptake (139-141) of glucose from the systemic circulation into the liver , from there into the bile (142) and into the small bowel. Through the effect of metformine radioactive glucose then reachs the large intestine there achieving the concentration necessary to be captured by the dosimetry scan (whole-body PET-scan).
The reduction of intestinal absorption of glucose (143) of other nutrients (144,145) and of some drugs (146) by metformin resembles that of „irritant laxatives“ (147,148) which produce peristalsis and not only reduce absorption of glucose and other food components (149-151) and but it also induces loss of water .The latter may explain dehydration and increase of creatinine serum level as described in metformin treated overweight type 2 diabetics. It may even worsen the latent hypoperfusion of peripheral tissues, eventually explaining excess of production of lactate,hyperferritinemia, increase of hepcidin serum level and hyposideremic anemia as an acute-phase- response to tissue damage (152,153).
Figure 1.
Scans of C11-metformin administered to humans intravenously and orally (lower and lower panel respectively) taken at different time after administartion .Gormensen LC et al.(70,with permission).
Figure 1.
Scans of C11-metformin administered to humans intravenously and orally (lower and lower panel respectively) taken at different time after administartion .Gormensen LC et al.(70,with permission).
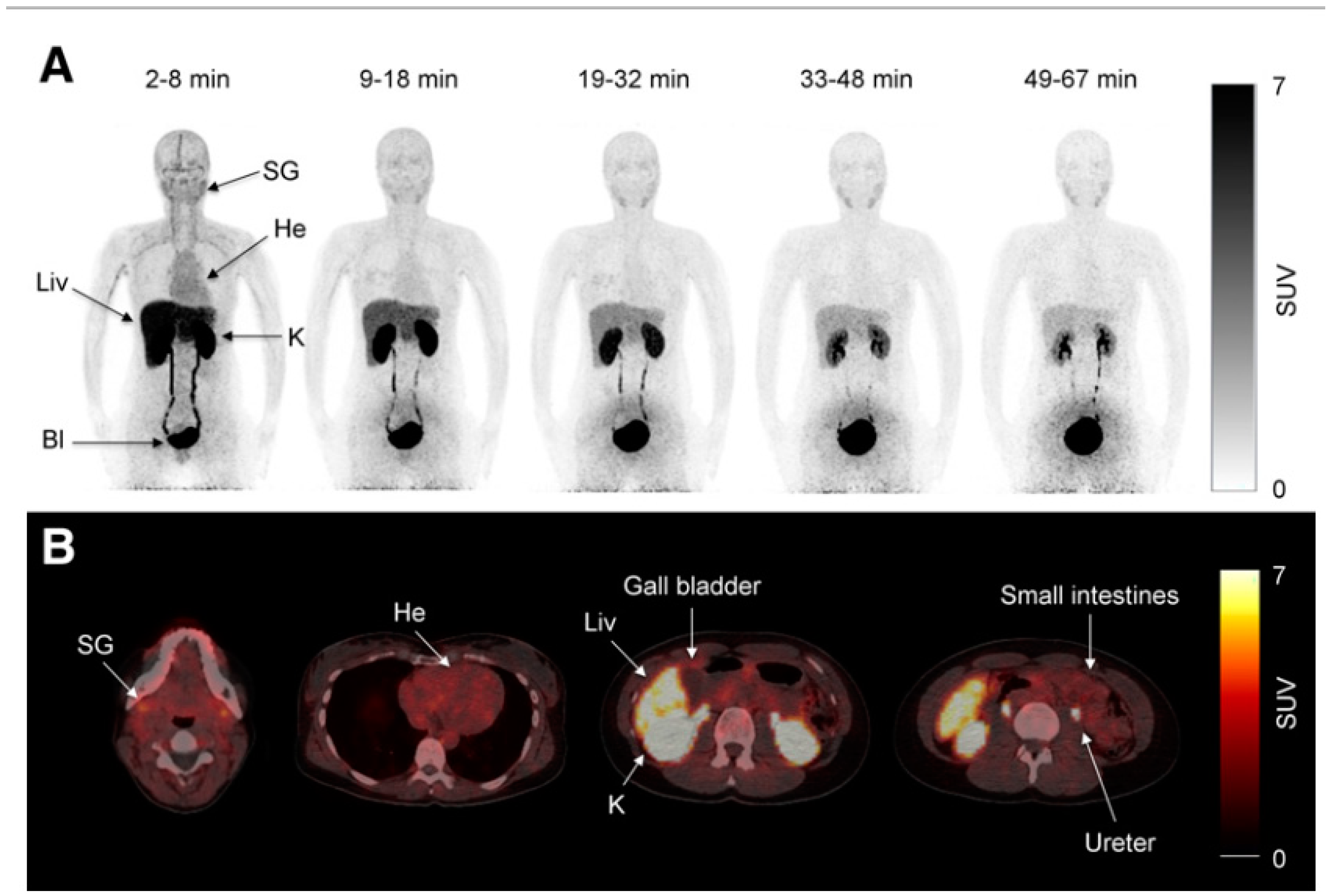
Figure 2.
PET-images taken 60 minutes after intravenuous administration of F18-FDG in a diabetic patient treated with metformin (A) and in a control patient(B).In A radiactivity has accumulated in the last portion of the ileum and in the colon (right hemicolon stronger than left hemicolon).The indication for the study was gall bladder cancer as confirmed by the accumulation oft he tracer in the gall bladder(arrow).From Morita Y et al.(131).
Figure 2.
PET-images taken 60 minutes after intravenuous administration of F18-FDG in a diabetic patient treated with metformin (A) and in a control patient(B).In A radiactivity has accumulated in the last portion of the ileum and in the colon (right hemicolon stronger than left hemicolon).The indication for the study was gall bladder cancer as confirmed by the accumulation oft he tracer in the gall bladder(arrow).From Morita Y et al.(131).
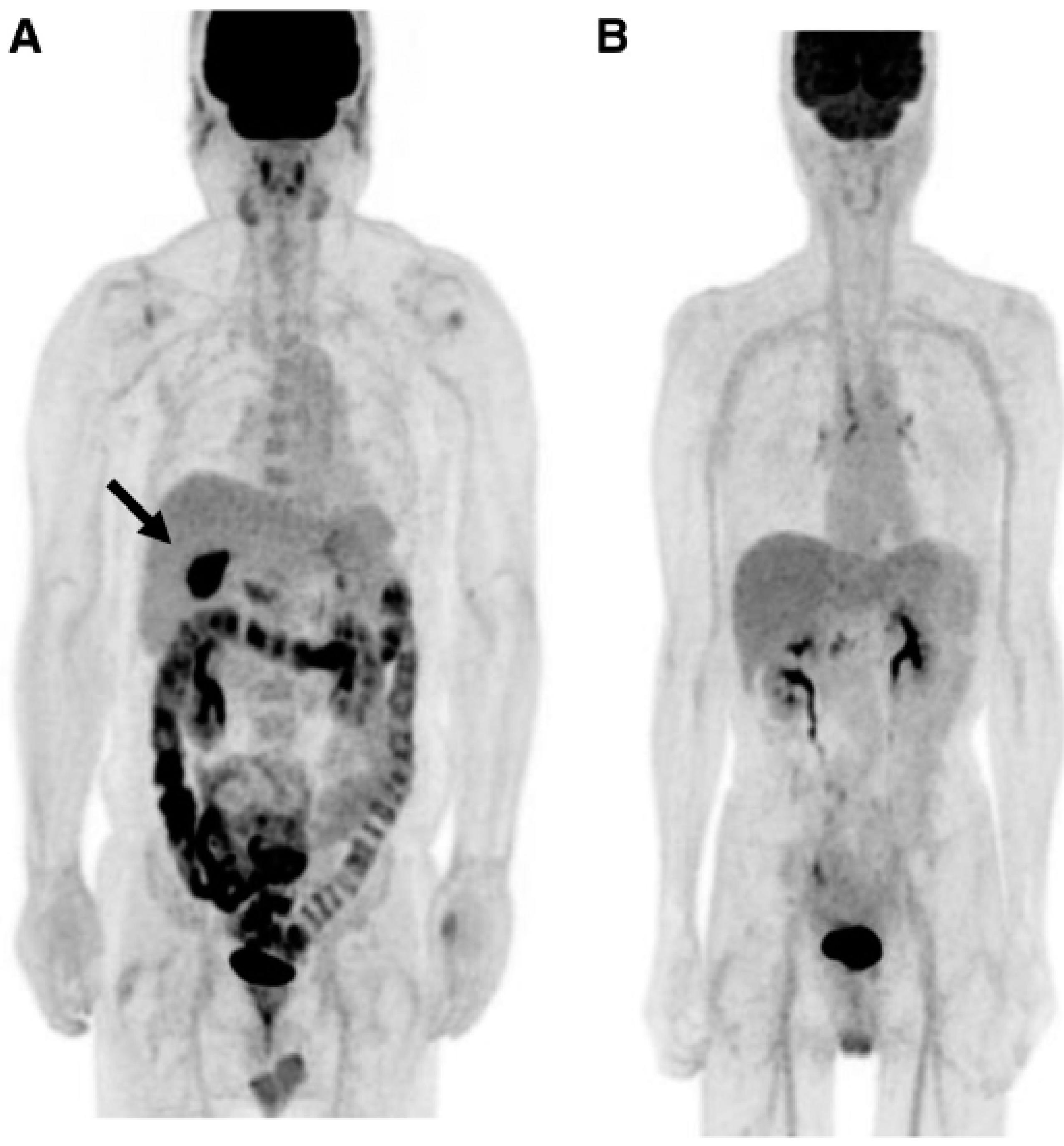
Figure 3.
PET-scan performed in diabetics at different time after interruption of metformin therapy.In patient 4 interruption time was shorter than 48 hours and shows strong accumulation of the tracer in the colon. From Schreuder N et al.(133).
Figure 3.
PET-scan performed in diabetics at different time after interruption of metformin therapy.In patient 4 interruption time was shorter than 48 hours and shows strong accumulation of the tracer in the colon. From Schreuder N et al.(133).
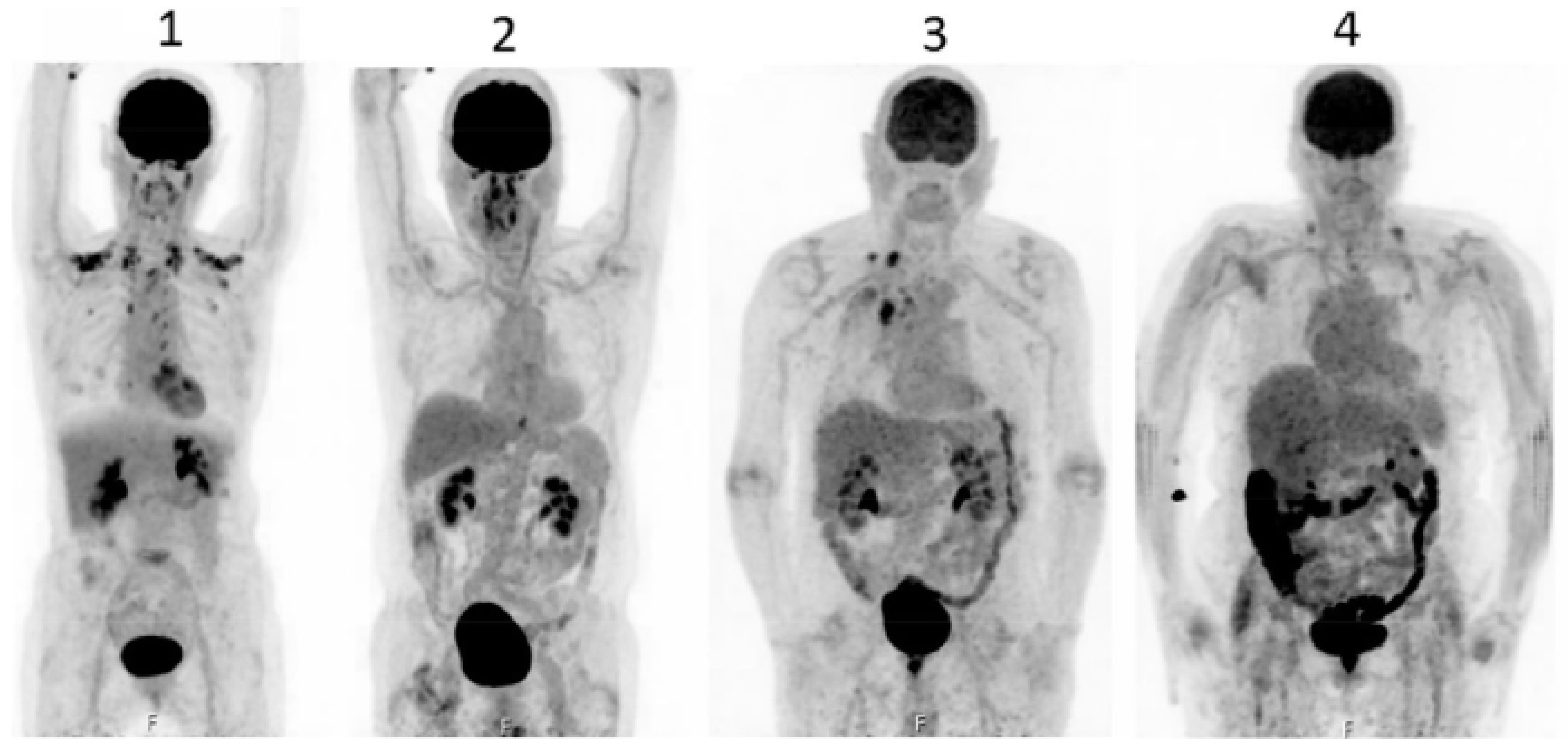
Figure 4.
PET-pictures of early scans (upper row) and of late FDG-scans(lower raw) after oral administration of laxatives. The arrows in the upper row of PET-scans shows the different patterns of accumulation of the tracers in the large intestine.From Chen Y-K et al.(137, with permission).
Figure 4.
PET-pictures of early scans (upper row) and of late FDG-scans(lower raw) after oral administration of laxatives. The arrows in the upper row of PET-scans shows the different patterns of accumulation of the tracers in the large intestine.From Chen Y-K et al.(137, with permission).
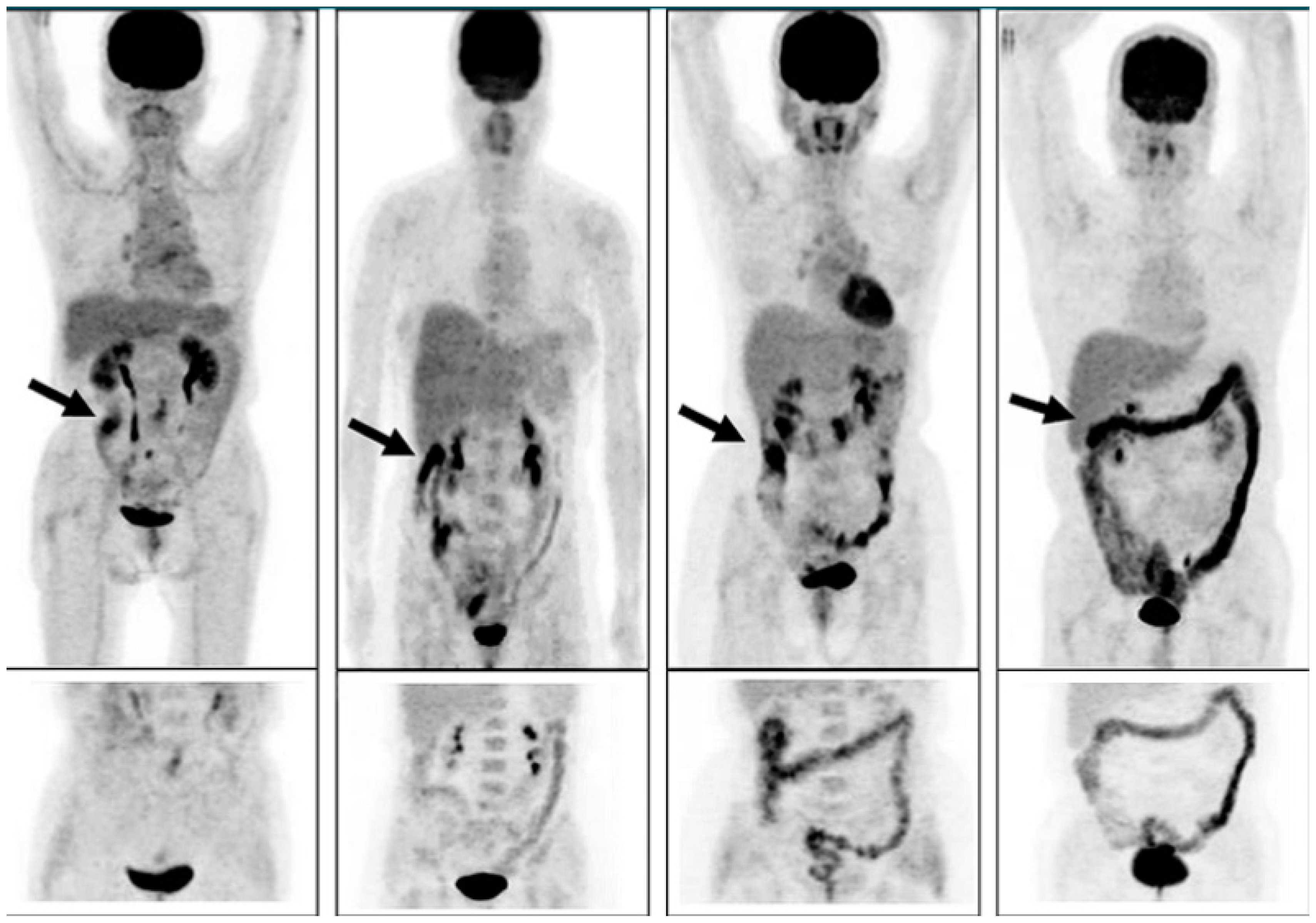
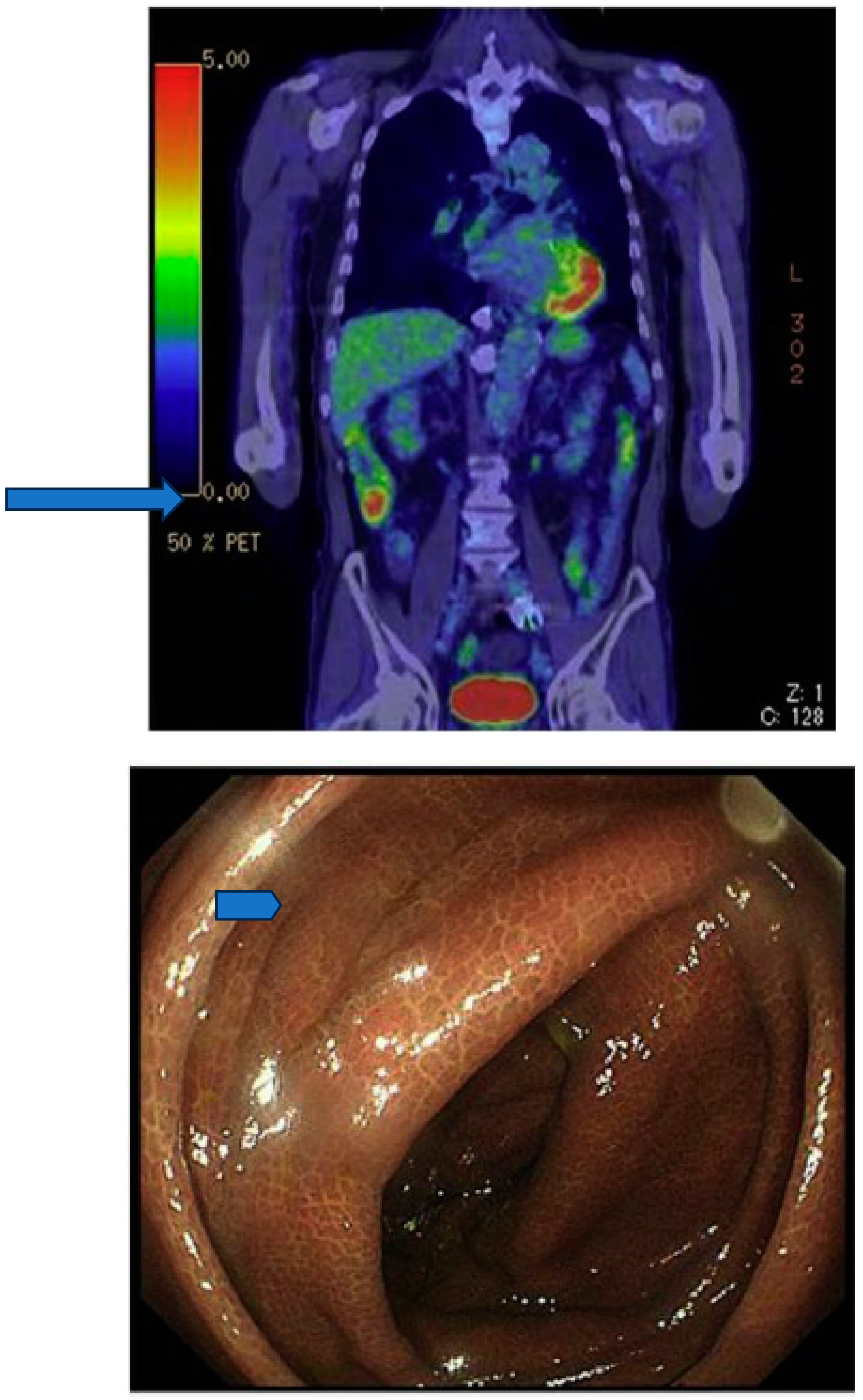
Figure 5.
Accumulation of F18-FDG(after intravenous administration) in the coecum and ascending colon (upper panel,long arrow) of a patient suffering from a mild diabetes (HbA1c=6.8%) and from chronic constipation treated with anthraquinone laxatives as demonstrated by the presence of melanosis coli at colonoscopy performed to exclude colon cancer (lower panel,short arrow).From Katsumata R (138).
Figure 5.
Accumulation of F18-FDG(after intravenous administration) in the coecum and ascending colon (upper panel,long arrow) of a patient suffering from a mild diabetes (HbA1c=6.8%) and from chronic constipation treated with anthraquinone laxatives as demonstrated by the presence of melanosis coli at colonoscopy performed to exclude colon cancer (lower panel,short arrow).From Katsumata R (138).
Concluions
Metformin,the latest and most often prescribed biguanide to overweight mostly older type 2 diabetics does not seem to differ from the previous biguanides used as oral antidiabetics.The mechanisms of serum glucose-lowering effect and the acute-and long-term consequences are similar to those of conventional laxatives.Dehydration,pre-renal kidney injury and even acidosis are the most serious and, for older multimorbide patients,life-threatning consequences of protracted metformin therapy.
References
- 1. Foretz M,Viollet B.:Le nouvelles promesses de la metformine.Vers une meilleure comprehension de ses mechanismes d‘action.Medicine/sciences 2014;30 (1):82-92.DOI10.1051/medsci/20143001010. [CrossRef]
- Sterne J.:Du nouveau dans les antidiabetiques.La NNdimethylamino guanyl guanidine(NNDG).Maroc Med 1957;36:1295-1296.
- Bailey CJ.The origin of type 2 diabetes medications.Br J Diabetes.2022;22:112-120.
- Staub H:Übersichten.40 Jahre insulin und intermediärer Stoffwechsel.Kli Wschr 1965;42(2): 61-69.
- Minkowski O,Verhandlungen des I.internationalen Physiologenkongresses.Basel 1889.Zentbl.Physiol.1889;312-313.
- Falkenberg M .Verhandlungen des X.Congresses für Innere Medizin.Wiesbaden 1891 S.502.
- Hirsch R.:Glykosurie nach Schilddrüsenextirpation by Hunden.Z.exp.Path.u.Therap.1906;3:393-400.
- Fühner H Über den Angriffsort der peripheren Guanidinwirkung.Zugleich eine Erwiederung.Archiv f.experiment.Pathol.u.Pharmakol.1909;65:402-427.
- Koch WF.On the occurrence of methyl Guanidine in the urine of parathyroidectomized animals.J Biol Chem 1912;12(3):313-315. [CrossRef]
- Koch WF.Toxic bases in the urine of parathyroidectomized dogs. J Biol Chem 1913;15:43-64. [CrossRef]
- Underhill FP,Blatherwick NR.Studies in carbohydrate metabolism.VI.The influence of Thyreoparathyroidectomy upon the sugar content of the blood and the gycogen content oft he liver.J Biol Chem 1914;118 (1):87-90.
- Underhill FP,Blatherwick NR.Studies in Carbohydrate Metabolism.VII.The influence of subcutaneous injections of dextrose and of calcium lactate upon the blood sugar content and upon tetany after thyreoparathyroidectomy.J Biol Chem 1914;119(1):119-126. [CrossRef]
- Underhill FP,Saiki T.The influence of complete thyroidectomy and thyroid feeding upon certain phases of intermediary metabolism. BiolChem.1908;5:225—241. [CrossRef]
- Burns D,Sharpe JS.THE PARATHYROIDS-TETANIA PARATHYREOPRIVA,IST NATURE,CAUSE,AND RELATIONS TO IDIOPATHIC TETANY.PART V: GUANIDIN AND METHYL-GUANIDINE IN THE BLOOD AND URINE IN TETANIA PARATHYREOPRIVA AND IN THE URINE IN IDIOPATHIC TETANY.Quart.J Exp Physiol 1916;10:345-354. [CrossRef]
- Watanabe CK.Studies in the metabolic changes induced by administration of guanidine bases.I.Influence of injected guanidine hydrochloride upon blood sugar content.J Biol Chem 1918;33:253-265.
- Watanabe CK.:Studies in the metabolic changes induced by administration of guanidine bases.II.The influence of guanidine upon urinary ammonia and acid excretion.J Biol Chem 1918;34(1)51-63.
- Watanabe CK.Studies in the metabolic changes induced by administration of guanidine bases.IV.Th influence of the administration of calcium upon blood sugar content in rabbits with guanidine hypoglycemia.J Biol Chem 1918;34(19:73-76.
- Watanabe CK.:Studies in the metabolic changes induced by the administration of guanidine bases.V.The change of phosphate and calcium content in serum in guanidine tetany and the relation between the calcium content and sugar in the blood.J Biol Chem 1918; 34(1):531-546. [CrossRef]
- Frank E,Northmann M,Wagner A.:Über Synthetisch Dargestellte Körper mit insulinartiger Wirkung auf den Normalen und diabetischen Organismus.Kli Wochenschr. 1926;45:2100-2107.
- Banting FC,Best CH.The internal secretion oft he pancreas.J Lab clin.Med.1922;7(5):251-266.
- Minkowski O.:Synthetische Insulinähnlich Wirkende Substanzen.Bemerkungen zu den vorstehenden Mitteilungen von Frank,Nothmann und Wagner.Klin Wochenschr.1926;45:2107.
- Calvert EGB.:Observations on the treatment of Diabetes By Synthalin.Lancet 1927;5430(2):649-651.DOI:10.1016/S0140-6736(01)31246-1. [CrossRef]
- Anonimus.:Synthalin in the treatment of Diabetes.Preliminary reports to the medical research council.Lancet 1927;5427 (2)517-521.DOI:10.1016/S0140-6736(01)31155-8. [CrossRef]
- Bodo R Marks A .:The relation of SYNTHALIN TO CARBOHYDRATE METABOLISM.J Physiol 1928;65:83-99. [CrossRef]
- Ringer AI,Bilon S,Harris MM,Landy A.:SYNTHALIN.its use in the treatment of Diabetes.Arch Int Med.1928;41(4):453-471.
- Staub H,Küng O.:Zum SANTHALINMECHANISMUS.Klin Woch.1928;7(29):1365-1366.
- Frank E,Nothmann M,Wagner A.:Über die Experimentelle und Klinische Wirkung des Dodekamethylendiguanids (Synthalin B).Klin Woch.1928;42:1996-2000. [CrossRef]
- Bischoff F,Sahyun M,Long L.:GUANIDINE STRUCTURE AND HYPOGLYCEMIA.J Biol Chem 1929;81:325-349.
- Anonymus.Insulin and Synthalin.Nature 1928;3039(121):151-153.
- Bloom A,Richards JG.:PHENFORMIN AS ADJUVANT ORAL THERAPY IN DIABETES.Br Med J 1961; 1796-1799. [CrossRef]
- Goldner M.:Oral Hypoglycemic Agents Past and Present.Archiv Int Med.1958;102:830-840.
- Williams RH,Tanner DC,Odell WD.Hypoglycemic Actions of Phenethyl-Amyl-,and Isoamyl-Diguanide.Diabetes 1958;7(2):87-92. [CrossRef]
- Beaser S.:THERAPY OF DIABETES MELLITUS WITH COMBINATIONS OF DRUGS GIVEN ORALLY.N Engl J Med 1958;259 (25):1207-1210. [CrossRef]
- Clarke BF,Duncan UP:Comparison of chlorpropamide and metformin tretment on weight and blood glucose response and uncontrolled obese diabetics.Lancet 1968;1:123-126.
- Beaser SB.:Oral Treatment of Diabetes Mellitus.JAMA 1964;187(12):887-893. [CrossRef]
- DeFronzo R,Goodmann A.:Efficacy of metformin in patients with non-insulin-dependent diabetes mellitus.NEngl J Med 1995;333(9):541-549. [CrossRef]
- Stumvoll M,Nurjahan N,Perriello G,Dailey G,Gerich JE.:Metabolic effects of metformin in non-insulin-dependent diabetes Mellitus.N Engl J Med 1995;333:550-554. [CrossRef]
- Guriguian J,Green L,Misbin RJ,Stadel B,Fleming GA.:Efficacy of Metformn in non-insulin-dependent diabetes mellitus.N Engl J Med 1996;334(4):269.
- Misbin RI,Green L,Stadel BV,Gueriguian JL,Gubbi A,Fleming GA.N Engl J Med 1998;338:265-266.
- Campbell RK,White JR,Saulie BA.:Metformin: A new Oral Biguanide.CLINICAL THERAPEUTICS 1996;18(3):360-370. [CrossRef]
- Ungar G,Freedman L,Shapiro S.:Pharmacological Studies of a new Oral Hypoglicemic Drug.Proc.Soc.Exp.Biol.Med 1957;100:190-192. [CrossRef]
- Dandona P,Fonseca V,Mier A,Beckett A.:Diarrhea and Metformin in Diabetic Clinic.Diabetes Care 1983;6(5):472-474. [CrossRef]
- Bailey CJ,Turner RC.:Metformin.N Engl J Med 1996;334(9):574-579.
- Inzucchi SE,Lipska KJ,Mayo H,Bailey CJ,McGuire DK.Metformin in patients with type 2 diabetes and kidney disease: a systematic review. JAMA 2014;312:2668-2675. [CrossRef]
- .46.UKPDS (33).Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33).Lancet 1998;352:837-853. [CrossRef]
- UKPDS(34).Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes(UKPDS 34) Lancet 1998;352:854-865. [CrossRef]
- Beaser SB.The Clinical Characteristics of Early Diabetes Mellitus.New Engl J Med 1948;239 (21):765-769. [CrossRef]
- Keys A,Menotti A,Karvonen MJ,Arvanis C,Blackburn H,Buzina R,Djorjevic BS,Dontas AS,Fidanza F,Keys MH,Kromhout D,Nedeljkovic S,Punsar S,Seccareccia F,Thoshima H.:The diet and 15-year death rate in the seven countries study.Am J Epidemiol.1986;124(6):903-915. [CrossRef]
- Dawber TR,Moore E,Mann GV:II.Corornary heart Disease in the Framingham study.Am J Publ Health.1957;47:4-24. [CrossRef]
- Huijbregets P,Feskens E,Raesanen L,Fidanza F,Nissinen A, Menotti A, Kromhout D.:Dietary pattern and 20 year Mortality in elderly men in Finland,Italy,and the Nederlands:longitudinal cohort study.BMJ 1997;315:13-17. [CrossRef]
- Sheps MC.:SHALL WE COUNT THE LIVING OR THE DEAD?N Engl J Med 1958;259 (25):1210-1214.
- Doyle JT,Dawber TR,Kannel WB,Heslin SA,Kahn HA:Cigarette smoking and coronary hearth disease.Combined experience oft he Albany and Framingham Studies.N Engl J Med 1962;266(16):796-801. [CrossRef]
- Doll R,Hill AB.:Lung cancer and other causes of death in relation to smoking.A second report on mortality of british doctors.BMJ 1956; 2(5001) :1070-1081. DOI: 10.1136/bmj.2.5001.1071. [CrossRef]
- Garcia MJ, McNamara PM, Gordon T, Kannell WB. Morbidity and mortality in diabetics in the Framingham population. Sixteen year follow-up study. Diabetes. 1974;23:105–111. [CrossRef]
- Freund K,Belanger AJ,DÀgostino RB,Kanner WB.:The health Risk of Smoking.The framingham Study:34 years of follow-up.AEP 1992;3(4):417-424.
- Doll R,Peto R.:Mortality in relation to smoking:20 years observations on male british doctors BMJ 1976;2:1525-1536. [CrossRef]
- Doll RD,Peto R,Hall E,Wheatley K,Gray R::Mortality in relation to consumption of alcohol:13 years observation of male british doctors.BMJ 1994;309:911-918. [CrossRef]
- Farchi G,Fidanza F,Menotti S,Menotti A.:Alcohol and Mortality in the italian rural cohorts of the seven countries study.Int J Epidemiol 1992;21(1):74-81. [CrossRef]
- Gronbaek M, Dies A,Sorensen TIA,Becker U,Borch-Johnsen K,Müller C,Schnohr P,Jensen G.:Influence of sex,age,body mass index,and smoking on alcohol intake and mortality.BMJ 1994,308:302-305. [CrossRef]
- Chyou P-H,Burchfiel CM,Yano K,Sharp DS,Rodriguez BL,Curb D,Nomura AMY.:Obesity,Alcohol Consumption,Smoking,and Mortality.AEP 1997;7(4):311-317. [CrossRef]
- Grunberg NE.Cigarette smoking and body weight:information may be hazardous to your health.Tabacco Control 1997;6:80. [CrossRef]
- Hermann LS.:Combination THERAPY WITH INSULIN AND METFORMIN.ENDOCRINE PRACTICE 1998;4(6):404-412. [CrossRef]
- Bailey CJ,Grant PJ,Evans M,Fine Olivarius N,Andreasen AH,Fowler PSB,Good CB,Turner RC,Holman R,Stratton I,Kerner W.:CORRESPONDENCE:The UK Prospective Diabetes Study. Lancet 1998;352:1932-1934.
- Ewart RM.:The UKPDS:what was the question?The Lancet 1999;353:1882. [CrossRef]
- Amiel SA.:Hypoglycaemia avoidance-technology and knowledge.The Lancet 1998;352:502-503. [CrossRef]
- Nathan DM.:Some answers,more controversy,from UKPDS.COMMENTARY.The Lancet 1998;352:832-833.
- Holman RR,Paul SK,Bethel MA,Matthews DR,Neil AW..10-Year Follow-up of intensive Glucose Control in Type 2 Diabetes.N Engl J Med 2008;359:1577-1589. [CrossRef]
- Sambol NC,Chiang J,O´Conner M,Liu CY,Lin ET,Goodman AM,Benet LZ,Karam JH.Pharmacokinetics and Pharmacodynamics of Metformin in Healthy Subjects and Patients with Non-Insulin-Dependent Diabetes Mellitus.J clin Pharmacol. 1996;36:1012-1021. [CrossRef]
- Pentikäinen PJ,Neuvonen PJ,Penttilä A.Pharmacokinetics of Metformin After intravenous and Oral Administration to Man.Eur J Clin Pharmacol 1979;16:185-202. [CrossRef]
- Gormensen LC,Sundelin EI,Jensen JB,Vendelbo MH,Jakobsen S,Munk OL,Christensen MMH,Broesen K,Froekiaer J, Jessen N.In vivo Imaging of Human C11-Metformin in Peripheral Organs:Dosimetry,Biodistribution,and Kinetic Analyses.J Nucl Med 2016;57(12):1920-1926.
- Garg,PK,Lokitz SJ,Nazih R,Garg S.Biodistribtution and Radiation Dosimetry of C11-Nicotine from Whole-Body PET Imaging in Humans.J Nucl Med 2017;58:473-478.
- Gierloeff T,Jakobsen S,Nahimi A,Munk OL, Bender D,Alstrup AKO,Vase KH,Hansen SB,Brooks DJ,Berghammer P.In Vivo Imaging of Human Acetylcholinesterase Density in Peripheral Organs using C11-Donezepezil:Dosimetry,Biodistribution,and Kinetic Analyses.J Nucl Med 2014;55:1818-1824. [CrossRef]
- Gierloeff T,Fedorova T,Knudsen K,Munk OL,Nahimi A,Jacobsen S,Danielsen EH,Terkelsen AJ,Hansen J,Pavese N,Brooks DJ,Borghammer P.Imaging acetylcholinesterase density in peripheral organs in Parkinson‘s diesease with C11-donepezil PET.BRAIN 2015;138:653-663. [CrossRef]
- Wisse E,De Zanger RB,Van Der Smissen CP,McCuskey RS.The Liver Sieve:Considerations Concerning the Structure and Function of Endothelial Fenestrae,the Sinusoidal Wall and the Space of Disse.Hepatology 1985;5(4):683-692. [CrossRef]
- Le Couteur DG,Fraser R,Hilmer S,Rivory LP,McLean AJ.The Hepatic Sinusoid in Aging and Cirrhosis.Effects on Hepatic Substrate Disposition and Drug Clearance.Clin Pharmacokinet.2005;44(2):187:200. [CrossRef]
- Chou C-H.Uptake and Dispersion of Metformin in the Isolated Perfused Rat Liver.J Pharm Pharmacol 2000;52:1011-1016. [CrossRef]
- Bonora E,Cigolini M,Bosello O,Zancanaro C,Capretti L,Zavaroni I,Coscelli CButturini U.:Lack of effect of intravenous metformin on plasma concentrations of glucose,insulin,C-peptide,glucagon and growth hormone in non-diabetic subjects.Curr.Med.Res.Opin.1984;9:47-51. [CrossRef]
- Sum CF,Webster JM,Johnson AB,Catalano C,Cooper BG,Taylor R.:The effect of intravenous Metformin on Glucose Metabolism During Hyperglicemia in Type 2 Diabetes.DIABETIC MEDICINE 1992;9:61-65. [CrossRef]
- Ong CR,Molyneaux LM,Binfotech MIC,Twigg SM, Yue DK.:Long-Term Efficacy of Metformin Therapy in Nonobese Individuals With Type 2 Diabetes.Diabetes Care.2006;29(11):2361-2364. [CrossRef]
- Goldberg RB,Orchard TJ,Crandall JP,Boyko EJ, Budoff M, Dabelea D,Gadde KM, Knowler WC, Lee CG, Nathan DM.:Diabetes prevention Program Research Group.Effects of long-term metformin and life-style interventions on cardiovascular events in the Diabetes Prevention Program and ist outcome study.Circulation 2022;145:1632-1641.DOI:10.1161/CIRCULATIONAHA.121.056756. [CrossRef]
- Vidon N,Chaussade S,Noel M,Franchisseur C,Huchet B,Bernier JJ..Metformin in the digestive tract.Diabetes Research and Clinical Practice.1988;4:223-229. [CrossRef]
- McCreight LJ,Bailey CJ,Pearson ER.:Metformin and the gastrointestinal tract.Diabetologia 2016;59:426-435. [CrossRef]
- Fatima M, Sadeeqa S,Nazir SUR.:Metformin and ist gastrointestinal problems:A review.Biomedical Research 2018;29(11):2285-2289.aw.
- Ghosal S,Ghosal S.:The Side Effects of Metformin-A Review.J Diabetes Metab.Disorders 2019.DOI:10.24966/DMD-201X/100030. [CrossRef]
- Caspary WF,Creutzfeldt W.:Inhibition of Bile salt absorption by blood sugar lowering biguanides.Diabetologia 1975;11:113-117. [CrossRef]
- Scarpello JHB,Hodgson E,Howlett HCS..Effect of Metformin on Bile salt Circulation and Intestinal Motility in Type 2 Diabetes Mellitus.Diabetic Medicine 1998;15:651-656.
- Sansome DJ,Xie C,Veedfald S, Horowitz M, Rayner CK,Wu T.:Mechanisms of glucose-lowering by metformin in type 2 diabetes:Role of bile acids.Diabetes Obes Metab.2019;.DOI:10.1111/dom.13869. [CrossRef]
- Metry M,Krug SA,Karra VK,Kane MA,Fink JC,Shu Y,Wang H,Polii JE.:Differential effects of metformin-mediated BSEP repression on pravastatin and bile acid pharmacokinetics in humans: A randomized controlled trial.Clin Transl Sci.2022;15:2468-2478. [CrossRef]
- Nakajima A,Ishizaki S, Matsuda K,Kurosu S,Taniguchi S,Gilberg PG,Mattsson JP,Hasumuma T,Camillen M.:Impact of elobixibat on serum and fecal bile acid levels and constipation symptoms in patients with chronic constipation.Journal of Gastroenterology and Hepatology 2022;37:883-890. [CrossRef]
- Spiller R.Inhibiting glucoe absorption to treat constipation.Lancet Gastroenterol Hepatol 2018.DOI:10.1016/S2468-1253 (18)30214-0. [CrossRef]
- Unger RH,Madison LL,Carter NW.:Tolbutamide-Phenformin in Ketoacidosis-Resistant Patients.JAMA 1960;174(17):2132-2136. [CrossRef]
- Bloom A,RicharsJG.Phenformin as adjuvant oral therapy in Diabetes.Br Med J 1961;1(5242): 1796-1799. [CrossRef]
- Cornfield J.:The university Group Diabetes Program.A Further Statistical Analysis of the Mortality Findings.JAMA 1971;217(12):1676-1687. [CrossRef]
- Palmer JP.Farewell to Phenformin for treating diabetes Mellitus.Ann Int Med 1975;83(4):567-568. [CrossRef]
- Fitzgerald E,Mathieu S,Ball A.:Metformin associated lactic acidosis.BMJ 2009;339:1254-1257.
- Blough B,Moreland A,Mora A.:Metformin-induced lactic acidosis with emphasis on the anoin gap.Proc(Bayl Univ Med Cent) 2015;28(1):31-33. [CrossRef]
- DeFronzo R,Fleming A,Chen K, Bicsak TA.:Metformin-associated lactic acidosis:current perspectives on causes and risk.Metabolism Clinical and Experimental 2016;65:20-29. [CrossRef]
- Gong O,Zhang P,Wang J,Ma J,An Y,Chen Y,Zhang B,Feng X,Li H,Chen X.:Da Qing Diabetes Prevention Study Group.Morbidity and Mortality after lifestyle intervention for people with impaired glucose tolerance:30-year results of the Da Oing Diabetes Prevention Outcome Study.Lancet Diabetes Endocrinol.2019;7:452-461.DOI:10.1016/S2213-8587(19)30093-2. [CrossRef]
- Faggian G,Cesaro A,Faggian R,Del Piano C,Vitagliano A,Del Piano D,Salzano M,Diglio A,Faggian A.Insufficienza renale acuta,acidosi lattica e metforrmina:due casi clinici e review della letteratura.Giornale Italiano di Nefrologia. 2023;3(3): ISSN 1724-5990.
- Cheng X,Liu MY-M,Li H, Zhang X,Lei F, Quin JJ,Chen Z,Deng KQ,Lin L,Chen M-MSong X, Xia M et al.Metformin is associated with higher incidence of acidosis,but not mortality,in individuals with COVID-19 and pre-existing type 2 diabetes.Cell Metabolism 2020;32:537-547.
- Vordoni A,Theofilis P,Vlachopanos G,Koukoulaki M,Kalaitzidis RG.Metfromin-associated lactic acidosis and acute kidney injury in the era of COVID-19.Frontiers in Bioscience Scholar 2021;13 (2):202-207.DOI:10.52586/S563. [CrossRef]
- Takayama K,Obata Y,Maruo Y,Yamaguchi H,Kosugi M,Irie Y,Hazama Y,Yasuda T.Metformin-associated Lactic Acidosis with Hypoglycemia during Covid-19 Pandemic.Intern Med 2022;61:2333-23337.DOI:10.2169/internalmedicine.9179-21. [CrossRef]
- Baley CJ,Gwilt M.Diabetes,Metformin and Clinical Course of COVID-19:Outcomes, Mechanisms and Suggestions on the Therapeutic Use of Metformin.Front Pharmacol 2022;13:78459.DOI:10.3369/iphar.2022.784459.
- Donelly LA,Morris AD,Pearson ER.:Adherence in patients transferred from immediate release metformin to a sustained release formulation:a population based study.Diabetes,Obesity and Metabolism.2009;11:338-342. [CrossRef]
- Rashid M,Warraich NY,Laique T,Shujaat K,Zawar S,Munir A.:Reasons of NON-Compliance to metformin among type 2 dibetics attending diabetic clinic in Lahore.Journal of Akhtar Saeed Medical and Dental College 2019;01(3):111-116.
- Christofides EA.:Practical Insight Into Improving Adherence to Metformin Therapy in Patients With Type 2 Diabetes.CLINICAL.DIABETES JOURNALS.ORG.2019;37 (3):234-241.DOI:10.2337/cd18-0063. [CrossRef]
- Walker EA,Gonzalez JS,Tripputi MT,Dagogo-Jack S,Matulik MJ,Montez MG,Tadros S,Edelstein SL.:Long-term metformin adherence in the Diabetes Prevention Program Outcomes Study.BMJ Open Diab Res Care 2020;8:e001537.DOI:10.1136/bmjdrc-2020-001537. [CrossRef]
- Syafhan NF,Donnelly R,Harper R,Harding J,Mulligan C,Hogg A,Scott M,Fleming G,Scullin C,Hawwa AF,Chen G,Pearson C,McEnlay JC.:Adherence to Metformin in adults with type 2 diabetes:a combined method approach.Journal of Pharmaceutical Policy and Practice 2022;15:61.DOI:10.1186/s40545-022-00457-5. [CrossRef]
- McGovern A,Tippu Z,Hinton W,Munro N, Whyte M,de Lusignan S.:A comparison of adherence and persistence by medication class in type 2 diabetes:A systematic review and meta-analysis.Diabetes Obes Metab.2018;20(4):1040-1043.
- Foret M,Guigas B,Viollet B.Metfrormin:update on mechanisms of action and repurposing potential.Nature rev endocrinol 2023.DOI:10.1038/s41574-023-00833-4. [CrossRef]
- Berchtold P,Bolli P,Arbenz U,Keiser G.:Intestinale Absorptionsstörung infolge Metforminbehandlung(Zur Frage der Wirkungsweise der Biguanide).Diabetologia 1969;5:405-412.
- Tomkin GH,Hadden DR,Weaver JA,Montgomery DAD..Vitamin-B12 Status of Patients on long-term Metformin Therapy.BMJ 1971;2:685-687.
- Kim J,Ahn CW,Fang S,Lee HS,Park JS.Association between metformin dose and vitamin B12 deficiency in patients with type 2 diabetes.Medicine 2019;98:46(e17918).
- Jager J,Kooy A, Lehret Ph, Wulfele‘MG, Kolk J,Bets D, Verbung J, Donker AJM,Stehouver CDA.:Long term treatment with metformin in patients with type 2 diabetes and risk of vitamin B-12 deficiency:randomized placebo controlled trial.BMJ 2010;340:c2181.DOI:10.1136/bmj.c2181. [CrossRef]
- Farland MZ,McPheeters CM, Renwick RC,Barlow PB,Williams JD,Keeble DS,Franks AS.:Comparison of patients receiving Long-Term Metformin Therapy and Vitamin B12 Monitoring.Journal of Pharmacy Technology.2015;31(4):184-189.
- Donnelly L,Dennis JM,Coleman RI,Sattar N,Hattersley AT,Holman RR,Pearson ER.:Risk of anemia with metformin Use in Type 2 diabetes:A MASTERMIND Study. Diabetes Care 2020;43:2493-2499.
- Serra MC,Kancherla V,Khakharia A,Allen LL,Phillips LS,Rhee MK,Wilson PWF,Vaughan CP.:Long-term metformin treatment and risk of peripheral neuropathy in older Veterans.Diabetes Research and Clinical Practice 2020;170:108486..DOI:10.1016/j.diabres.2020.108486. [CrossRef]
- Ahmed HH,Fadl NN,Kotob SE.Impact of long term Metformin therapy on hepcidin and Iron status in type II Diabetic Patients.IJPCR 2015;7 (3):185-193.
- 119. Bischoff F,Long L.STUDIES IN CARBOHYDRATE METABOLISM FOLLOWING GUANIDINE DEGLYCOGENATION.J Nutr 1930;3(2):201-216. doi.org/10.1093/jn/3.2.201. [CrossRef]
- Wilcock C,Bailey CJ.:Reconsideration of inhibitory effect of metformin on intestinal glucose absorption.J.Pharm.Pharmacol.1991;43:120-121. [CrossRef]
- Bailey CJ.Metformin and intestinal glucose handling.Diabetes Metab Rev 1995;11 Suppl 1:S23-32.
- Wu T, Xie C,Wu H, Jones KI,Horowitz M,Rayner CK.:Metformin reduces the rate of the small intestinal glucose absorption in type 2 diabetes.Diabetes,Obesity and Metab 2017;119(2):290-293.DOI.10.1111/dom.12812. [CrossRef]
- Horakova O,Kroupova P,Bardova K,Buresova J,Janowska P,Kopecky J,Rossmeisl M.:Metformin acutely lowers blood glucose levels by inhibition of intestinal glucose transport.Scientific Reports 2019;9:6156.DOI:10.1038/s41598-019-42531-0. [CrossRef]
- Penicaud L,Hitier Y,Ferre P,Girard J.Hypoglycemic effect of metformin in genetically obese(fa/fa) rats results from an increased utilization of blood glucose by intestine.Biochem J.1989;262:881-885. [CrossRef]
- Bronden A,Alber A,Rohde U,Rehfeld JF,Holst JJ,Vilsboell T,Knop FK.:Single-dose Metformin enhances Bile-Acid-induced Glucagon-like Peptide-1 Secretion in Patients with type-2 Diabetes.J Clin Endocrinol Metab 2017;102(11):4153-4162. [CrossRef]
- Ritzel U,Fromme A,Otteleben M,Leonhardt U,Ramadori G.Release of glucagon-like peptide-1(GLP-1) by carbohydrates in the perfused rat ileum.Acta Diabetol 1997;34:18-21. [CrossRef]
- Raddatz D,Nolte W,Roßbach C,Leonhardt U,Buchwald A,Scholz KH,Ramadori G.Measuring the effect of a Study Meal on Portal Concentrations of Glucagon-Like Peptide-1 (GLP-1) in Non Diabetic and Diabetic Patients with Liver Cirrhosis:Transjugular Intrahepatic Portosystemic Stent Shunt(TIPSS) as a New Method for Metabolic Measurement.Exp Clin Endocrinol Diabetes 2008;116:461-467. [CrossRef]
- Li B, Hu Y,Wang G, liu L.The effect of exenatide on fasting bile acids in newly diagnosed type 2 diabetes mellitus patients, a pilot study.BMC Pharmacology and toxicology 2020;21:44.DOI:10.1186/s40360-020-00422-5. [CrossRef]
- 129.Kim S,Chung JK,Kim BT, Relationship between gastrointestinal F-18-fluorodoxyglucose accumulation and gastrointestinal symptoms in whole-body PET.Clin Positron Imaging 1999;2:273-279. [CrossRef]
- Gontier E,Fourme E,Wartski M,Blondet C Bonardel G,Le Stanc E,Mantzarides M,Foehrenbach H,Pecking A-P,Alberini J-L.High and typical F18-FDG bowel uptake in patients treated with metformin.Eur J Med Mol Imaging 2008;35:95-99. [CrossRef]
- Morita Y,Nogami M,Sakaguchi K,Okada Y,Hirota Y,Sugawara K,Tamori Y,Zeng F,Murokami T,Ogawa W.:Enhanced Release of Glucose Into Intraluminal Space of the Intestine Associated With Metformin Treatment as Revealed by [18F]Fluorodeoxyglucose PET-MRI.Diabetes Care 2020;43:1796-1802.DOI:10.2337/dc20-0093. [CrossRef]
- Özülkur T,Özülkur F,Mert M,Özpacaci T.Clearance of high intestinal F18-FDG uptake associated with metformin after stopping the drug.Eur J Nucl Med Mol Imaging 2010;37:1011-1017.
- Schreuder N,Klarenbeek H,Vendel BN,Jager PL,Kosterink JGW,van Puijenbroek EP.Discontinuation of metformin to prevent metformin-induced high colonic FDG uptake:is 48 h sufficient?.Annals of Neclear Medicine 2020;34:833-839. [CrossRef]
- Vangu MDT,Momodu JI.F-18 FDG PET/CT Imaging in Normal Variants,Pitfalls and Artifacts in the Abdomen and Pelvis.Front. Nucl. Med.1:826109.DOI:10.3389/fnume.2021.826109. [CrossRef]
- Soyka JD,Strobel K,Veit-Haibach P,Schaefer NG,Schmid DT,Tschopp A,Hany TF.Influence of Bowel Preparation Before F18-FDG PET/CT on Physiologic F-18-FDG Activity in the Intestine.J Nucl Med 2010;51:507-510. [CrossRef]
- Tu DG,Chen C-R,Wang Y-W,Tu C-W,Huang YC.Bowel-cleansing methods affecting PET-CT Image interpretation.Nucl Med Commun 2011;32:570-574. [CrossRef]
- Chen Y-K,Chen J-H,Tsui C-C,Chou H-H,Cheng R-H,Chiu J-S.Use of Laxative-augmented Contrast Medium in the Evaluation of Colorectal Foci at FDG PET.Radiology 2011;259 (2):525-533. [CrossRef]
- Katsumata R,Manabe N,Ayaki M,Tanikawa T,Fujita M,Ono Y, Fujiwara H,Suehiro M,Monobe Y,Kato K,Kawamoto H,Haruma K.Increased Colonic Fluorodeoxyglucose Uptake in Melanosis Coli-A Case Series of Three Patients.Gastro Hep Advances 2022;1:125-128. [CrossRef]
- Soskin S,Allweiss MD,Cohn DJ.INFLUENCE OF THE PANCREAS AND THE LIVER UPON THE DEXTROSE TOLERANCE CURVE.Am J Physiol-Legacycontent 1934;109(1):155-165.DOI:10.1152/ajphysiog.1934.109.1.155.
- Madison LL.Role of insulin in the hepatic Handling of glucose.Arch Int Med 1969;123:284-292. [CrossRef]
- Balks H-J,Jungermann K.Regulation of peripheral insulin/glucagon levels by rat liver.Eur J Biochem 1984;141:645-650. [CrossRef]
- Guzelian Ph,Boyer JL.Glucose Reabsorption from Bile.J Clin Invest 1974;53:526-535.
- Ikeda T,Iwata K,Murakami H.Inhibition Effect of Metformin on Intestinal Glucose Absorption in the perfused Rat Intestine.Biochem Pharmacology 2000;59:887-890. [CrossRef]
- Albai O,Timar B,Paun DL,Sima A,Roma D,Timar R.:Metformin Treatment:A potential Cause of Megaloblastic Anemia in Patients with Type 2 Diabetes Mellitus.Diabetes,Metabolic Syndrome and Obesity:Targets and Therapy 2020;13:3873-3878.
- Infante M,Leoni M,Caprio M,Fabbri A.:Long-term Metformin therapy and Vitamin B12 deficiency:An association to bear in mind.World Journal Diabetes 2021;12(7):916-931.
- Wijnen JCF,Van De Riet IR,Lijfering WM,Van Der Meer FJM.Metformin use decreases the anticoagulant effect of phenprocoumon.J Thromb Haemost 2014;12:887-890. [CrossRef]
- Baker EH,Sandle GI.Complications of Laxative Abuse.Ann Rev Med 1996;47:127-134. [CrossRef]
- Hart SL,McColl I.The effect of the laxative oxyphenisatin on the intestinal absorption of glucose in rat and man.Br J Pharmac Chemother 1968;32:683-686. [CrossRef]
- Nilsson SE,Takkinen S,Johansson B,Dotevall G,Melander a,Berg S,McClearn G.Laxatie treatment elevates plasma homocysteine:a study on a population-based Swedish sample of old people.Eur J Clin Pharmacol 2004;60:45-49. [CrossRef]
- Sturtzel B,DIETRICH A,Wagner KH,Gisinger C,Elmafda I.The status of vitamins B6,B12,Folate,and of HOmocysteine in Geriatric home residents receiving laxatives or dietary fiber.The Journal of Nutrition Health.2010;14(3):219-223. [CrossRef]
- Sugimoto H,Yamada U.Iron deficiency anemia induced by magnesium overuse:a case report.BioPsychoSocial Medicine 2019;13:18.DOI:10.1186/s13030-019-0159-y. [CrossRef]
- Naz N,Malik IA,Sheikh N,Ahmad S,Kahn S,Blaschke M,Schultze F,Ramadori G.Ferroportin-1 is a nuclear negative acute-phase protein in rat liver:a comparison with other iro-transport proteins.Lab Invest 2012;92:842-856. [CrossRef]
- Ahmad S,Moriconi F,Naz N,Sultan S,Sheikh N,Ramadori G,Malik IA.Ferritin L and Ferritin H are differentially located within hepatic and extra hepatic organs under physiological and acute-phase conditions.Int J Clin Exp Pathol 2013;6(4):622-629.
- 83.Tan J,Wang Y,Liu S,Shi Q,Zhou X,Zhou Y, Yang X, Chen P,Li s.:Long-Acting Metformin Vs Metformin Immediate Release in Patients With Type 2 Diabetes:A Systematic Review.Frontiers in Pharmacology 2021;12.DOI:10.3389/fphar.2021.669814. [CrossRef]
- 67.Chalmers J,Cooper ME.:UKPDS and the Legacy Effect.N Engl J Med.2008;359:1618-1620. [CrossRef]
- 100.Tang Y,Weiss T,Liu J,Rajpathak S,Khunti K.:Metformin adherence and discontinuation among patients with type 2 diabetes:A retrospective cohort study.Journal of Clinical and Translational Endocrinology 2020;20:100235.DOI:10.1016/j.jcte.2020.100225. [CrossRef]
- 108.Wamil M,Coleman RL,Adler AI,McMurray JJV,Holman RR.Increased risk of Incident heart Failure and death is asociated with insulin Resistance in people with newly diagnosed Type 2 Diabetes:UKPDS 89.Diabetes Care 2021;44:1877-1884. [CrossRef]
- 118.Love KM,Barrett EJ,Horton WB.Metforrmin‘s impact on the Microvascular Response to Insulin.Endocrinology 2022;;162(11).DOI:10.1210/endocr/bqac162. [CrossRef]
- 80.Spiller R:Inhibiting glucose absorption to treat constipation.Lancet Gastroenterol Hepatol 2018;.DOI:10.1016/S2468-1253(18)30214-0. [CrossRef]
- Kuriyama S,Ohmori K,Miura Ch,Suzuki Y,Nakaya N,Fujita K,Sato Y, Tsubono Y,Tsuji I,Fukao A, Hisamichi S.:Body Mass Index and Mortality in Japan:The Miyagi Cohort Study.J Epidemiol 2004;14 (Supl1):S-33-38. [CrossRef]
- Gerstein HC.:Shouln‘t Preventing Type 2 Diabetes Also Prevent Ist long-term Consequences?.Circulation 22022;145:1642-1644.DOI:10.1161/CIRCULATIONAHA.122.060026. [CrossRef]
- Rehee E-J.:Extra-Glycemic Effects of Anti-Diabetic Medications:Two Birds with One Stone?.Endocrinol Metab 2022;37:415-429.DOI:10.3803/EnM.2022.304. [CrossRef]
- Campbell JE,Drucker DJ.Pharmacology,Physiology,and Mechanisms of Incretin Hormon Action.Cell Metabolism.2013;17:819-836.
- 35.Palmer JP.:Farewell to Phenformin for treating Diabetes Mellitus.Ann Int Med 1975;83(4):567-568. [CrossRef]
- 34.Clarke BF,Duncan LJP.Comparison of chlorpropamide and metformin treatment on weight and blood-glucose response and uncontrolled obese diabetics.Lancet 1968;1:123-126. [CrossRef]
- 40.Hermann LS,Schersten B,Bitzen P-O,Kjellström T,Lindgärde F,Melander A.:Therapeutic Comparison of Metformin and Sulfonylurea,Alone and in Various Combinations.A double-blind controlled study. Diabetes Care 1994;17(10):1100-1109. [CrossRef]
- .Heyden S,Cassel JC,Bartel A,Tyroler HA,Hames CG,Ga C,Cornoni JC.Body Weight and Cigarette Smoking As Risk Factors.Arch Intern Med 1971;128:915-919. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



