Submitted:
19 July 2023
Posted:
20 July 2023
You are already at the latest version
Abstract
Health issues of children with intellectual disabilities (ID) have gained significant attention as a key focus of China health goals. This study aimed to compare the differences in displacement skills and problem behaviors among children with varying degrees and types of ID, while also exploring their relationship. The study included 90 participants who were children with ID and had completed TGMD-2 displacement skills and Strengths and Difficulties Questionnaire (SDQ) assessments. Covariance, partial correlation, and multiple linear regression analyses were conducted to examine the differences and correlations between these factors. The findings revealed that higher severity of intellectual disability was associated with lower scores in locomotor skills and increased manifestation of problem behaviors. Notably, there were significant variations in locomotor skills and problem behaviors among children with different types of intellectual disabilities. There is a positive correlation between locomotor skills and problem behaviors in children with intellectual disabilities, where locomotor skills can predict the occurrence of problem behaviors. In Conclusion, the research confirms that the development of locomotor skills can have a positive impact on the accompanying problem behaviors of children with developmental disabilities.
Keywords:
Intellectual Disabilities
; Children
; Displacement Skills
; Problem Behaviors
1. Introduction
Intellectual disabilities, commonly referred to as intellectual impairments, are categorized into four levels of severity: mild, moderate, severe, and profound, based on the degree of cognitive impairment [1]. Additionally, depending on the accompanying physical and neurological impairments, these disabilities can be further classified into specific types, including Pure Intellectual Disability(Pure-ID), Down Syndrome (DS), Cerebral Palsy (CP), and Autism Spectrum Disorders (ASD) [2]. Global data indicates that ID are neurodevelopmental disorders that affect approximately 3% of children and adolescents [3]. Individuals with ID often face a range of behavioral challenges, such as varying levels of hyperactivity, maladaptive emotions, inappropriate social interactions, and aggressive tendencies, which hinder their ability to engage in prosocial behavior [4]. In comparison to typically developing children, those with ID generally exhibit higher levels of problem behavior [5], coupled with lower levels of physical fitness encompassing speed, agility, strength, flexibility, balance, coordination, reaction time, cardiovascular endurance, and muscle endurance [6]. Problematic behaviors associated with ID significantly contribute to the manifestation of antisocial behavior and social rejection during adolescence and adulthood [7].
Gross motor displacement skills refer to the body's ability to move and change position in space [8]. These skills are crucial indicators for assessing gross motor movements, which, in turn, have a positive impact on physical health and cognitive development [9,10]. The development of fundamental motor skills during childhood significantly influences cognitive functions and the maturation of the motor nervous system [11]. However, children with ID experience delayed development of basic motor skills compared to their typically developing peers [12]. Research indicates that the degree of ID affects motor performance [13], with children with mild ID displaying better motor skills than those with severe ID [14]. Additionally, there is a correlation between intellectual level and motor coordination ability, as children with marginal, mild, and moderate ID score lower on displacement skills compared to typically developing children [15,16]. A study discovered a correlation between the severity of intellectual disability in children and their level of physical activity [17], as well as the severity of their learning disabilities [18]. However, there is limited research available regarding the variations in displacement skill levels among different degrees of disability. Scholars have conducted research on the developmental characteristics of gross motor movements in children with ASD [19] and DS [20], shedding light on the development of basic Displacement skills in children with various ID. However, there have been no reports comparing the levels of displacement skills among children with specific ID, DS, and ASD. It is essential to recognize the significance of developing displacement skills in children with ID as it positively contributes to their cognitive functions, physical health, motor coordination, and overall physical activity levels.
During the mid-1990s, the American Psychiatric Association defined problem behavior as behaviors exhibited by individuals that deviate from prevailing social norms and age-appropriate expectations, persisting over an extended duration and influencing the individual's own life or the lives of others to varying degrees [21]. Research consistently demonstrates that children with ID exhibit higher levels of problem behavior compared to typically developing children [22]. Common behaviors include excessive emotional reactivity [23], while psychiatric disorders, oppositional behavior, and antisocial behavior tend to be more pronounced [24]. Children with ID often experience specific cognitive deficits [25], accompanied by sensory integration dysfunction, which is more prevalent in this population than in typically developing children [26]. Moreover, sensory integration is intricately linked to both physical fitness and problem behavior [27]. Studies also indicate a strong correlation between lower physical fitness levels and increased rates of problem behavior in children [28]. Additionally, there is a close relationship between basic motor skills, health status, and problem behavior in this population [29]. However, existing literature does not report a direct link between displacement skills and problem behavior in children with ID. Further investigation is necessary to determine potential variations in displacement skills and problem behavior characteristics among different types of ID (e.g., specific ID, DS, ASD, etc.). Moreover, it is crucial to assess whether displacement skills in children with varying degrees and types of ID have predictive value for problem behavior.
Consequently, this study aims to investigate the characteristics and associations between displacement skills and levels of problem behavior in children with diverse degrees and types of ID.
2. Methods
2.1. Participants
Through the selection of 90 children with intellectual disabilities who successfully completed the assessments, participants were chosen from two specialized educational institutions, consisting of 70 males and 20 females (Figure 1). These participants had an average age of (9.13±1.73) years, an average height of (135.30±12.37) cm, and an average weight of (34.18±11.90) kg. Their classification was based on their intelligence quotient (IQ) and social adaptability, resulting in four disability levels: mild (50~69), moderate (IQ=35~49), severe (IQ=20~34), and profound (IQ<20). Their IQ was evaluated using the Wechsler Intelligence Scale [1]. Additionally, considering the accompanying physical and neurological impairments associated with intellectual disabilities, they can also be classified into various types, including Pure-ID, DS, and ASD [2]. By reviewing the academic records of these 90 participants, the severity of intellectual disability was categorized into three levels: moderate (n=36), severe (n=35), and profound (n=19). The types of intellectual disabilities included Pure-ID (n=21), DS (n=12), and ASD (n=57), totaling three distinct categories.
2.2. Materials
2.2.1. Body morphology
The height and weight of the participants were measured using the In Body J30 pediatric body composition analyzer, manufactured by Bio space, a Korean company. Participants were instructed to stand barefoot on the device with relaxed bodies, hold the sensors with both hands, and gaze straight ahead while removing their shoes and socks during the test.
2.2.2. Displacement Skills
Test of Gross Motor Development-Ⅱ (TGMD-2) was used to evaluate the displacement ability of children with ID [8]. The test assesses six movements, including running (8 points), sliding forward (8 points), jumping sideways (6 points), one-legged jump (10 points), standing long jump (8 points), and side sliding (8 points). Each movement is scored as either 1 point for "compliance" or 0 points for "non-compliance". The test is conducted twice, and the maximum score is 48 points. The TGMD-2 has been cross-culturally validated and demonstrated good reliability and validity [33]. This study found that the gross motor displacement skills had a Cronbach's α coefficient of 0.859, indicating good internal consistency.
2.2.3. Problematic Behaviors
The Strengths and Difficulties Questionnaire (SDQ) is a reliable tool developed by Goodman R to assess the psychological well-being of special children and adolescents. It consists of 25 items across five dimensions [30]. The difficulty score is evaluated through 20 items and includes four dimensions: emotional, conduct, hyperactivity, and peer problems, which assess negative emotions and problematic behaviors of the subjects. The strengths section includes five items that evaluate positive behaviors of the subjects in the prosocial behavior dimension [31]. The SDQ questionnaire is a valid tool for assessing problem behaviors in children with ID in clinical diagnosis [32].
2.3. Procedure
The data for this study was obtained from a research project conducted by the National Research Center for Early Childhood Physical Education Development at Chengdu University. Approval for the project was granted by the Ethics Committee of Sichuan Normal University, and the study was carried out from March to May 2022, encompassing all the tests.
The testing involved the distribution of questionnaires and on-site assessments. The study examined the growth records of 90 participants within the past three years, excluding those without growth records from the screening process. The test subjects were children with intellectual disabilities, and their participation required parental consent, with parents present throughout the entire process. To ensure participant privacy, each individual was assigned a unique code instead of using their names for testing and evaluation purposes.
The study included students with ID from special schools who had lower cognitive comprehension abilities. Prior to testing, teachers, parents, and examinees received 3-5 instructions and demonstrations. For severely disabled children who could not comprehend during testing, teachers and parents guided and motivated them to complete the demonstration again. The test was scored by a primary examiner and an assistant who had not engaged in any physical activity before the test and met the physical requirements. The scoring criteria were standardized, and the entire test process was videotaped. The test exercises were conducted in the following order: running, forward sliding step, stepping jump, single-leg jump, standing long jump, and lateral sliding step.
The SDQ parent version is a questionnaire that the homeroom teacher of the corresponding class distributes to evaluate children. The teacher provides training to the main investigator and explains the requirements for filling out the questionnaire. Parents fill out the questionnaire on site, and it is immediately collected upon completion. The investigators then conduct a unified count and sorting of the questionnaires. If parents encounter difficulties while completing the questionnaire, the investigators provide one-on-one assistance. To ensure the questionnaire's authenticity and validity, the investigators conduct follow-up phone calls or require parents to fill out the questionnaire again if there are issues such as missing or multiple answers.
2.4. Data Analysis
The data were analyzed using SPSS 22.0 and expressed as mean ± standard deviation(M±SD). Multivariate covariance analysis was used to examine the differences in displacement skill and problem behavior in relation to the degree and type of ID in the subjects. The effect of variance analysis was evaluated using the local Eta square test (η2), with the correlation coefficient standards for small, medium, and large effect sizes being 0.01, 0.06, and 0.14 [34]. Partial correlation analysis was used to test the correlation between displacement skill and problem behavior, with the correlation coefficient standards for weak, moderate, and high effect sizes being 0.1, 0.3, and 0.5 [13]. Multivariate linear regression analysis was conducted to investigate the impact of displacement skills on problem behavior in children with varying degrees of ID. Subject gender, age, and body weight were used as controls, ID degree was the independent variable, problem behavior was the dependent variable, and the degree of influence was evaluated using the standardized coefficient β. The model interpretation rate was measured using the change in R2. The significance level for the differences in the data analysis results was set as follows: P<0.01 for extremely significant, 0.01<P<0.05 for significant, and 0.05<P<0.1 for marginally significant.
3. Results
3.1. Analysis of displacement skills and problem behaviors in children with different levels of ID.
3.1.1. Displacement Skills
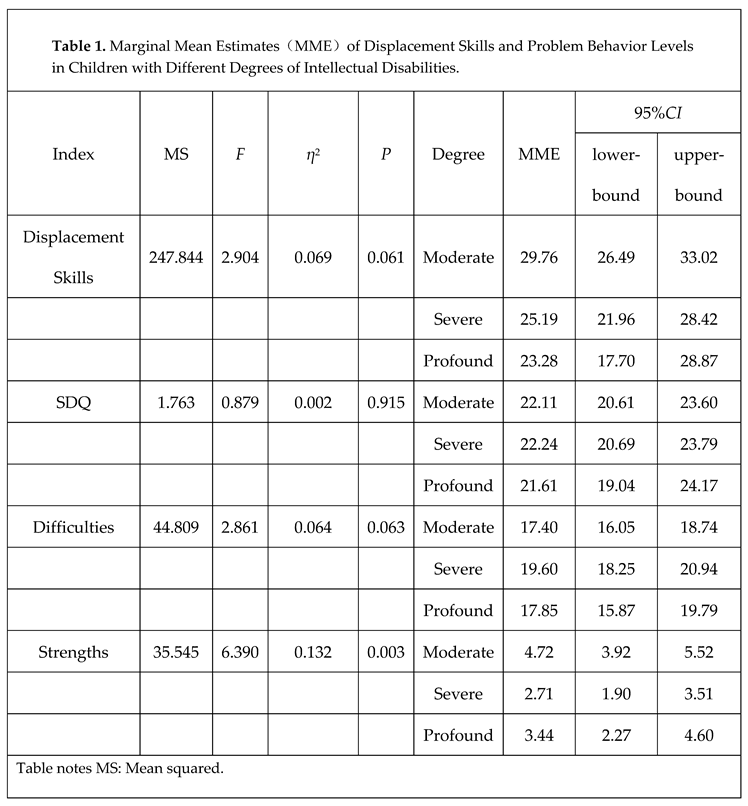
Covariance analysis was used to calculate the mean scores of displacement skills in children with varying degrees of ID. The subjects' gender, age, and body weight were controlled for in the analysis to ensure accuracy. The results presented in Table 1 suggest a marginally significant difference in displacement skill mean scores among children with varying degrees of ID [F(247.844)=2.904, η2=0.069, P<0.1]. Specifically, children with moderate ID exhibit significantly higher displacement skill scores than those with severe ID (P<0.05), and slightly higher scores than those with profound ID (P<0.1). However, no significant difference in displacement skills is observed between children with severe and profound ID (P>0.1). Additionally, the score for displacement skills decreases as the degree of ID becomes more severe, with the order being moderate (29.76)>severe (25.19)>profound (23.28).
3.1.2. Problem Behaviors
Covariance analysis was used to calculate the mean scores of total SDQ, difficulty scores, and strength scores in children with varying degrees of ID, while controlling for gender, age, and body weight. The results presented in Table 1 show that there is no significant difference in the mean scores of total SDQ among children with different degrees of ID [F(1.763)=0.089, η2=0.002, P=0.915], and no significant difference in pairwise comparisons (P>0.1).
A marginally significant difference in the mean difficulty scores among children with varying degrees of ID is observed [F(44.81)=2.861, η2=0.064, P<0.1]. Specifically, children with moderate ID exhibit significantly lower mean difficulty scores than those with severe ID (P<0.05), while no significant difference in pairwise comparisons is observed between the other groups (P>0.1). Moreover, the severity of ID is positively correlated with the mean difficulty scores, with the order being moderate (17.40)<profound (17.84)<severe (19.60).
The mean scores of strengths in children with varying levels of ID showed significant differences [F(35.545)=6.390, η2=0.132, P<0.01]. Specifically, children with moderate ID scored significantly higher in strengths compared to those with severe disabilities (P<0.01) and slightly higher than those with profound disabilities (P<0.1). As the severity of ID decreased, the scores of strengths increased. Notably, children with moderate disabilities (4.72) outperformed those with profound disabilities (3.44) and severe disabilities (2.71).
3.2. Analysis of displacement skills and problem behaviors in children with different types of ID.
3.2.1. Displacement Skills
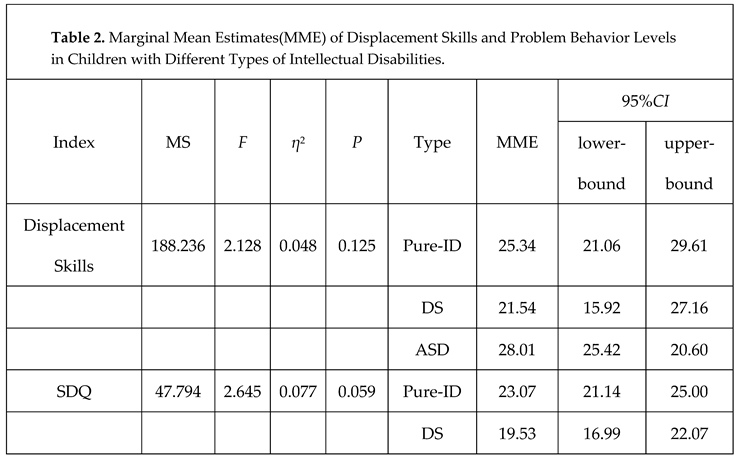
The study utilized covariance analysis to investigate the mean displacement skill scores of children with varying ID. Gender, age, and body weight were controlled for in the analysis. Table 2 presents the results, which indicate no significant differences in mean displacement skill scores among children with different types of ID [F(188.236)=2.128, η2=0.048, P>0.1]. However, children with ASD exhibited significantly higher displacement skill scores than those with DS (P<0.05). No significant differences were observed in the other pairwise comparisons (P>0.1). The abilities of spatial displacement among children with various types of ID demonstrate distinct variations, with ASD (28.01) surpassing Pure-ID (25.34) and DS (21.54).
3.2.2. Problem Behaviors
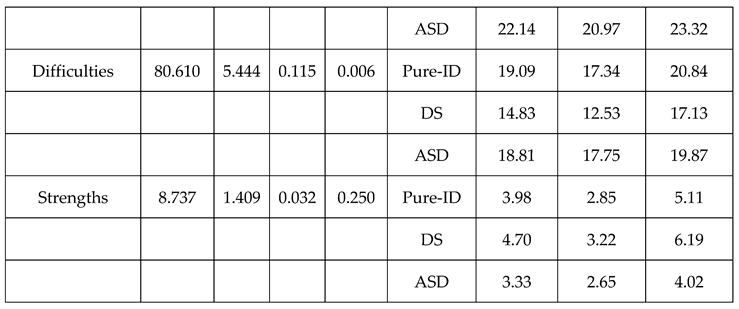
The study utilized covariance analysis to investigate the mean total SDQ scores, as well as the mean difficulty and strength subscale scores, of children with varying types of ID. Gender, age, and body weight were controlled for in the analysis. The results, presented in Table 2, indicate marginally significant differences in mean total SDQ scores among children with different types of ID [F(47.794)=2.645, η2=0.059, P<0.1]. Specifically, children with Pure-ID exhibited significantly higher mean total SDQ scores than those with DS (P<0.05), while children with ASD had slightly higher mean total SDQ scores than those with DS (P<0.1). No significant differences in mean total SDQ scores were observed between children with Pure-ID and those with ASD (P>0.1). The overall scores of the Strengths and Difficulties Questionnaire (SDQ) among children with varying types of ID demonstrate distinct variations, with Pure-ID (23.07) surpassing ASD (22.14) and DS (19.53).
The study revealed highly significant differences in mean difficulty scores among children with varying types of ID [F(80.610)=5.444, η2=0.115, P<0.01]. Children with Pure-ID and ASD exhibited significantly higher mean difficulty scores than those with DS (P<0.01), while no significant differences in mean difficulty scores were observed between children with Pure-ID and those with ASD (P>0.1). The scores of difficulties among children with various types of ID display distinct disparities, with Pure-ID (19.09) surpassing ASD (18.81) and DS (14.83).
No significant differences were found in mean strength scores among children with varying types of ID [F(8.737)=1.409, η2=0.032, P>0.1]. Post-hoc pairwise comparisons also did not reveal any significant differences (P>0.1).
3.2.3. Correlation analysis of displacement skills and problematic behaviors in children with ID
A partial correlation analysis was conducted to examine the relationship between displacement skills and problem behaviors among children with ID. Gender, age, and body weight were controlled for in the analysis. The results, presented in Table 3, revealed a highly significant positive correlation between displacement skills and the total score of the Strengths and Difficulties Questionnaire (SDQ) among children with moderate ID (r=0.486, P<0.01). Additionally, a significant positive correlation was found between displacement skills and the difficulties score (r=0.442, P<0.05). However, no significant correlation was observed between displacement skills and the strengths score (P>0.1). Among children with severe ID, displacement skills showed a marginally significant positive correlation with the total score of the SDQ (r=0.339, P<0.1). However, no significant correlation was found between displacement skills and the difficulties or strengths scores (P>0.1). Finally, for children with profound ID, no significant correlation was observed between displacement skills and the scores of SDQ, difficulties, or strengths (P>0.1).
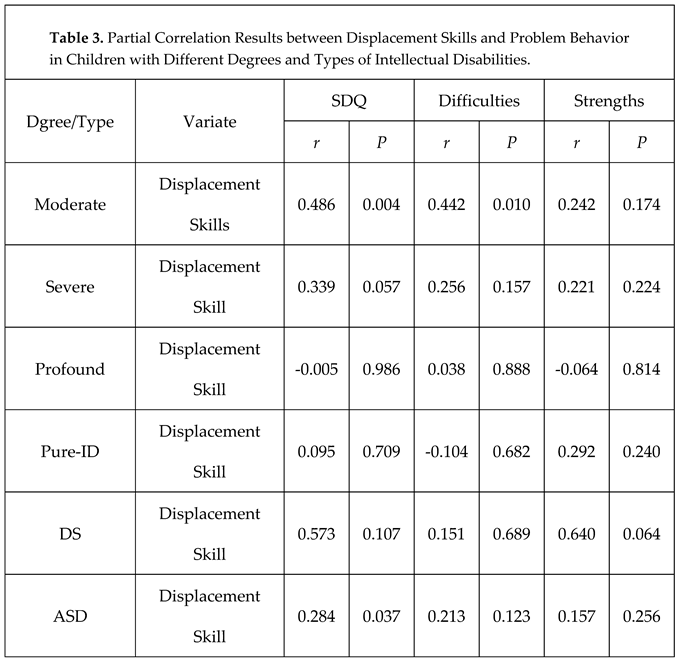
Among children with Pure-ID, no significant correlation was found between displacement skills and the scores of SDQ, difficulties, or strengths (P>0.1). In children with DS, displacement skills showed a marginally significant positive correlation with the strengths score (r=0.640, P<0.1), but no significant correlation was observed between displacement skills and the SDQ or difficulties score (P>0.1). For children with ASD, displacement skills were significantly and positively correlated with the SDQ score (r=0.284, P<0.05). However, no significant correlation was found between displacement skills and the difficulties or strengths score (P>0.1).
3.2.4. Multivariate linear regression analysis of the impact of displacement skills on problematic behaviors in children with ID
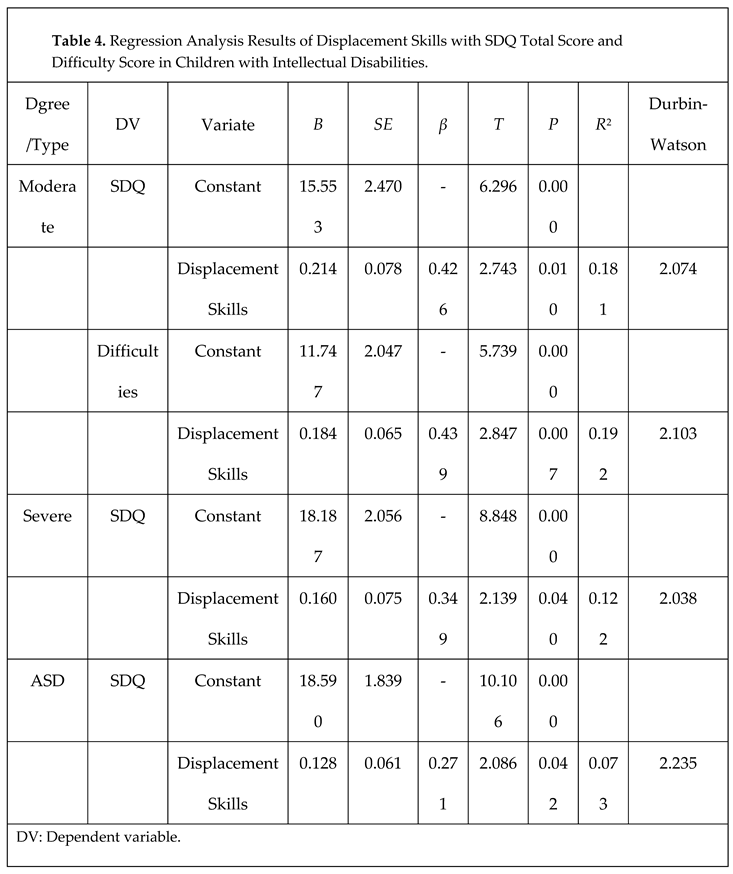
After examining the relationship between displacement skills and SDQ total score and difficulty score in children with mild ID, marginal correlation in children with severe ID, and significant correlation in children with ASD, we conducted further investigation to explore the impact of displacement skills on problem behavior scores. To achieve this, displacement skills were used as independent variables, and SDQ total score and difficulty score were used as dependent variables, while controlling for gender, age, and body mass index. Multiple linear regression analysis was employed, and control variables were gradually removed until the retained regression analysis results showed the impact of displacement skills on problem behavior. The results indicated that displacement skills predicted SDQ total score (β=0.426, P=0.01) and difficulty score (β=0.439, P<0.01) in children with moderate ID, with a coefficient of determination of R2=0.181 and R2=0.192, respectively (Table 4).
The score of displacement skills had a significant impact on SDQ total score in children with severe ID (β=0.349, P<0.05), with a coefficient of determination of R2=0.122 (Table 4). However, the correlation between the score of displacement skills and SDQ total score and difficulty score in children with profound ID was not significant, and therefore did not meet the conditions for regression analysis.
Displacement skills had a significant impact on SDQ score in children with ASD (β=0.271, P<0.05), with a coefficient of determination of R2=0.073 (Table 4). However, there was no significant correlation between the score of displacement skills and SDQ total score and difficulty score in children with Pure-ID and DS, and therefore, regression analysis was not appropriate.
4. Discussion
4.1. Children with varying degrees of ID exhibit differences in their displacement skills and problem behaviors
Children with ID typically attend regular schools where they receive conventional education, as they have limited intellectual function and impaired cognitive functions [35]. Their basic motor skills, specifically their displacement skills, are lower than those of typically developing children [36]. However, there are individual differences in the difficulty of accepting the same action [2], and as the severity of the disability increases, the learning, imitation, and understanding abilities decrease, and the performance of movement coordination worsens [36]. This study focused on intellectually disabled children in special education schools, with varying degrees of ID, including moderate, severe, and extremely severe. The findings revealed differences in displacement skills among children with different levels of ID, primarily between children with mild to moderate ID and those with severe or extremely severe ID. Children with mild to moderate ID demonstrated better displacement skills than those with severe or extremely severe ID. Additionally, children with moderate ID exhibited higher displacement skill levels than those with severe or extremely severe ID. The more severe the ID, the poorer the performance of displacement skills. These results are consistent with the findings of Zhang Lei's research [36].
Children with varying degrees of ID did not show significant differences in their total SDQ score. However, significant differences were found in the difficulty scores of assessing negative emotions and problematic behaviors among children with different degrees of ID. Specifically, children with moderate ID had significantly lower difficulty scores than those with severe ID. Additionally, significant differences existed in the strength scores of assessing prosocial behavior among children with different ID, with children with moderate ID having higher strength scores than those with extremely severe or severe ID. These findings not only explain the lack of significant difference in the total SDQ score but also reveal that as the degree of ID increases, the score for problematic behavior increases while the score for prosocial behavior decreases. Conversely, for children with milder degrees of ID, the score for prosocial behavior increases while the score for problematic behavior decreases. These results are consistent with Kostikj's research, which found that problematic behavior in children with ID is related to the severity of their disability [24].
In summary, children with moderate ID exhibit milder motor impairments, stronger prosocial behaviors, greater adaptability, more advanced displacement skills, and less problematic behavior compared to their counterparts with severe and extremely severe ID.
4.2. Children with different types of ID exhibit differences in their displacement skills and problem behaviors
Research indicates that ID can be categorized into three types: ID without co-occurring physical impairments or autistic behavior, ID accompanied by physical impairments (such as DS, the most prevalent type of ID in China, which is accompanied by physical impairments), and ID co-occurring with ASD [37]. While several scholars have studied large motor development in children with ASD [19,38] and DS [20], no studies have reported differences in levels of displacement skills among children with ID without co-occurring physical impairments or autistic behavior, DS, and ASD.
The study discovered that individuals with ID, DS, and ASD share similar overall characteristics in spatial skills. Nonetheless, when comparing the groups, those with ASD demonstrated better spatial skills than those with DS. Additionally, individuals with ASD scored higher than those with ID and DS. It is important to note that ID, DS, and ASD are all disorders of the brain and nervous system that share similarities in cognition, emotions, and psychological disorders [2]. Regarding physical disabilities, limb impairment stands out as a prominent feature of DS, resulting in diminished body control [39]. Conversely, children with ASD generally display less severe physical impairments when compared to individuals with Pure-ID and DS [40]. Furthermore, children with Pure-ID tend to exhibit more positive emotional expressions. This, to some extent, elucidates why children with ASD outperform their counterparts with Pure-ID and DS in terms of spatial displacement skills.
The study revealed that individuals with different types of ID exhibit varying overall SDQ scores. Specifically, those with ID and ASD had higher overall SDQ scores than those with DS. Further analysis showed significant differences in the scores of difficulties in assessing negative emotions and problem behaviors among children with different types of disorders. Those with ID and ASD had significantly higher scores of difficulties than those with DS. However, there were no significant differences in the scores of strengths in assessing prosocial behavior among children with different types of disorders. This suggests that the differences in overall SDQ scores among those with ID, DS, and ASD mainly appeared in the scores of difficulties in assessing negative emotions and problem behaviors. Regarding psychological disorders, individuals with DS experience severe physical impairments, while those with ID exhibit more expressive behavior and emotions, leading to more physical activity [37]. Children with ASD typically exhibit more severe symptoms than those with ID and have mental developmental delays, difficulty adapting to the environment, and communicating with others [41]. This partially accounts for why children with ID have more problem behaviors than those with ASD and DS.
In summary, individuals with ID without comorbidities and those with DS face physical limitations, whereas individuals with ASD exhibit superior spatial skills compared to those with ID without comorbidities and DS. Additionally, challenging behaviors are less prevalent among individuals with ASD than those with ID without comorbidities and DS. Among these populations, individuals with DS exhibit the lowest performance in spatial skills, while those with ID without comorbidities exhibit the highest occurrence of challenging behaviors.
4.3. The relationship between displacement skills and problem behavior in children with ID
Research suggests that physical fitness and cognitive development are closely linked to the development of large motor skills [36]. Children with ID often experience cognitive deficits, which can lead to challenging behaviors such as slow movements, emotional instability, hyperactivity, and impulsivity [2]. Additionally, these children may exhibit slower rates of growth and development compared to their typically developing peers, and their occurrence of challenging behaviors is much higher than that of healthy children [29]. However, there is currently no literature reporting a direct correlation between displacement skills and challenging behaviors in children with ID. It is important to note that limitations may arise when comparing and discussing the results of similar studies.
This study has found a correlation between displacement skills and behavioral problems in children with varying levels of ID. Specifically, displacement skill scores and SDQ total scores, as well as difficulty scores, are positively correlated with moderate ID in children. For severe ID, displacement skill scores are slightly positively correlated with SDQ total scores. However, there is no correlation between displacement skills and behavioral problems in children with profound ID. Regression analysis results indicate that displacement skills in children with moderate ID can predict SDQ total scores and difficulty scores to a certain extent, with predictive power of 18.1% and 19.2%, respectively. A one-unit change in displacement skill score results in a change of 0.426 standard deviations for SDQ total scores and a change of 0.439 standard deviations for difficulty scores. Children with severe ID also exhibit predictive ability on SDQ total scores through displacement skills, with a predictive accuracy of 12.2%. A one-unit change in displacement skill score results in a change of 0.349 standard deviations for SDQ total scores. This suggests that displacement skills have a higher predictive ability on behavioral problems in children with moderate ID than in their severe counterparts. According to a study by Dekker and colleagues, children with moderate ID may have an easier time learning displacement skill than those with severe ID, as the latter are more limited by their cognitive development [42]. Therefore, children with moderate ID may be more likely to utilize displacement skills to regulate their behavioral problems.
The study found a positive correlation between the displacement skills score of children with ASD and problem behavior, as measured by the total score of SDQ. In contrast, a marginal correlation was observed between the displacement skills score and the strengths score of children with DS. No correlation was detected between the displacement skills score of children with Pure-ID and the total score, difficulties, and strengths score of SDQ. Regression analysis revealed that the displacement skills score of children with ASD can predict SDQ score, with a predictive explanatory power of 7.3%. Specifically, a one-unit change in the displacement skills score corresponds to a 0.271 standard deviation change in the SDQ total score. It is worth noting that children with ASD exhibit significant differences in behavior, emotion, language, and socialization when compared to those with Pure-ID and DS [43]. Specifically, children with ASD typically experience less severe physical impairments and demonstrate superior motor performance when compared to those with Pure-ID and DS [2]. As a result, the displacement skills score of children with ASD may have a direct impact on the total score of SDQ, albeit with a relatively low predictive explanatory power of 7.3%.
In brief, a correlation exists between displacement skills and problem behavior in children with ID. The former can directly affect the latter, and the displacement skills score can predict problem behavior. Specifically, the displacement skills scores of children with moderate ID, severe ID, and ASD can influence the total score of SDQ to some degree. Furthermore, the displacement skills score of children with moderate ID can impact the difficulties score of negative emotions and problem behavior directly.
5. Conclusion
1) After children with different levels of ID are analyzed, it is found that those with moderate ID display higher levels of displacement skills and strength scores, but lower difficulty scores, compared to those with severe and profound ID.
2) Among children with varying degrees of ID, those with ASD exhibit higher levels of adaptive skills compared to those with Pure-ID and the DS. Children with Pure-ID exhibit the most significant behavioral symptoms.
3) A correlation exists between adaptive skills and challenging behavior in children with ID. Adaptive skill scores have a predictive role in challenging behavior, especially in children with moderate ID. The adaptive skills of children with moderate ID significantly affect their overall score and difficulty score on the SDQ. Likewise, the adaptive skills of children with severe ID significantly affect their overall score on the SDQ,suggesting that the development of displacement skills in children with ID can have a positive impact on their accompanying problem behavior.
Author Contributions
Conceptualization, Renren Zhang, Yu Su; Methodlogy, Yu Su, Renren Zhang; Fomal analysis, Yu Su; Data curation, Yu Su, Guoyi Zheng, Yi He,Qin Wu; Writing-original draft, Yu Su; Writing-review and editing: Yu Su, Guoyi Zheng; Funding acquisition, Renren Zhang. All authors have read and agreed to the published version of the manuscript.
Funding
The data for this study was obtained from a research project (Project ID: YETY2019A01) conducted by the National Research Center for Early Childhood Physical Education Development at Chengdu University.
Institutional Review Board Statement
Approval for the project was granted by the Ethics Committee of Sichuan Normal University (Approval ID: 2022LSTY01).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request to the corresponding author.
Acknowledgments
We gratefully acknowledge the support of the organizations, professionals, and people with intellectual disabilities in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Matson, J.L.; Dixon, D.R.; Matson, M.L.; Logan, J.R. Classifying mental retardation and specific strength and deficit areas in severe and profoundly mentally retarded persons with the MESSIER. Res. Dev. Disabil. 2005, 26, 41–45. [Google Scholar] [CrossRef]
- Yuzhao, Z.; Yang, C. A Study on the Design Strategies for School Space of Special Needs Based on the Characteristics of Mentally Retarded Students. Architectural Journal. 2017, (05), 98–103. [Google Scholar]
- Leite, A.J.d.C.; Pinto, I.P.; Leijsten, N.; Ruiterkamp-Versteeg, M.; Pfundt, R.; de Leeuw, N.; da Cruz, A.D.; Minasi, L.B. Diagnostic yield of patients with undiagnosed intellectual disability, global developmental delay and multiples congenital anomalies using karyotype, microarray analysis, whole exome sequencing from Central Brazil. PLOS ONE 2022, 17, e0266493. [Google Scholar] [CrossRef]
- Wagemaker, E.; Hofmann, V.; Müller, C.M. Prosocial behavior in students with intellectual disabilities: Individual level predictors and the role of the classroom peer context. PLOS ONE 2023, 18, e0281598. [Google Scholar] [CrossRef]
- Taanila, A.; Ebeling, H.; Heikura, U. Behavioral problems of 8-year-old children with and without intellectual disability. Journal of Pediatric Neurology. 2013, 1, 15–24. [Google Scholar]
- Wouters, M.; Evenhuis, H.M.; Hilgenkamp, T.I.M. Physical fitness of children and adolescents with moderate to severe intellectual disabilities. Disabil. Rehabilitation 2019, 42, 2542–2552. [Google Scholar] [CrossRef] [PubMed]
- van Lier, P.A.C.; Vitaro, F.; Barker, E.D.; Brendgen, M.; Tremblay, R.E.; Boivin, M. Peer Victimization, Poor Academic Achievement, and the Link Between Childhood Externalizing and Internalizing Problems. Child Dev. 2012, 83, 1775–1788. [Google Scholar] [CrossRef]
- Ulrich, D.A.; Sanford, C.B. Test of gross motor development; Pro-ed: Austin, TX, 1985. [Google Scholar]
- Ricci, L.A. Exploration of reading interest and emergent literacy skills of children with down syndrome. International Journal of Special Education 2021, 26. [Google Scholar]
- Barnett, L.M.; Beurden, E.V.; Morgan, P.J.; Lyndon, O.B.; John, R.B. Childhood Motor Skill Proficiency as a Predictor of Adolescent Physical Activity. Journal of Adolescent Health. 2008, 44, 252–259. [Google Scholar] [CrossRef]
- Goodwhy, J.D.; Ozmun, J.C.; Gallahue, D.L. Under-standing Motor Development:Infants, Children, Adolescent, Adults; Jones & Bartlett Learning: Burlington, USA, 2019; p. 5. [Google Scholar]
- Gkotzia, E.; Venetsanou, F.; Kambas, A. EPJ Motor proficiency of children with autism spectrum disorders and intellectual disabilities: a review. 2017, 9, 46–69. [Google Scholar]
- Lei, Z.; Dandan, W.; Xueping, W. Influence of Fundamental Motor Skills on Moderate to Vigorous Physical Activity in Children with Intellectual Disabilities: Difference in Severity. China Sport Science and Technology. 2023, 59, 27–35. [Google Scholar]
- Vuijk, P.J.; Hartman, E.; Scherder, E.; Visscher, C. Motor performance of children with mild intellectual disability and borderline intellectual functioning. J. Intellect. Disabil. Res. 2010, 54, 955–965. [Google Scholar] [CrossRef]
- Marieke, W.; Suzanne, H.; Esther, H.; Chris, V. Are gross motor skills and sports participation related in children with intellectual disabilities? Research in Developmental Disabilities. 2011, 32, 1147–1153. [Google Scholar]
- Hartman, E.; Houwen, S.; Scherder, E.; Visscher, C. On the relationship between motor performance and executive functioning in children with intellectual disabilities. J. Intellect. Disabil. Res. 2010, 54, 468–477. [Google Scholar] [CrossRef]
- Eguia, K.F.; Capio, C.M.; Simons, J. Object control skills influence the physical activity of children with intellectual disability in a developing country: The Philippines. J. Intellect. Dev. Disabil. 2015, 40, 265–274. [Google Scholar] [CrossRef]
- Nonis, K.P.; Jernice, T.S.Y. The gross motor skills of children with mild learning disabilities. International Journal of Special Education 2014, 29. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed.; American Psychiatric Publishing: Arlington, 2013; pp. 936–937. [Google Scholar]
- Alesi, M.; Battaglia, G.; Pepi, A.; Bianco, A.; Palma, A. Gross motor proficiency and intellectual functioning: A comparison among children with Down syndrome, children with borderline intellectual functioning, and typically developing children. Medicine. 2018, 97, e12737. [Google Scholar] [CrossRef] [PubMed]
- Bell, C.C. DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. JAMA: The Journal of the American Medical Association 1994, 272, 828–829. [Google Scholar] [CrossRef]
- Kaptein, S.; Jansen, D.E.M.C.; Vogels, A.G.C.; Reijneveld, S.A. Mental health problems in children with intellectual disability: use of the Strengths and Difficulties Questionnaire. J. Intellect. Disabil. Res. 2007, 52, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Dovgan, K.; Mazurek, M.O.; Hansen, J. Measurement invariance of the child behavior checklist in children with autism spectrum disorder with and without intellectual disability: Follow-up study. Res. Autism Spectr. Disord. 2019, 58, 19–29. [Google Scholar] [CrossRef]
- Kostikj-Ivanovikj, V. Behavioral Problems In Children With Mild And Moderate Intellectual Disability. 2015. [Google Scholar] [CrossRef]
- Cavadini, T.; Courbois, Y.; Gentaz, E. Eye-tracking-based experimental paradigm to assess social-emotional abilities in young individuals with profound intellectual and multiple disabilities. PLOS ONE 2022, 17, e0266176. [Google Scholar] [CrossRef]
- Silverstein, M.J.; Faraone, S.V.; Leon, T.L.; Biederman, J.; Spencer, T.J.; Adler, L.A. The Relationship Between Executive Function Deficits and DSM-5-Defined ADHD Symptoms. J. Atten. Disord. 2020, 24, 41–51. [Google Scholar] [CrossRef]
- Ren, G.; Wang, Y. A survey of children's behavioral problems and Sensory processing disorders in urban areas of Beijing. Chinese Mental Health Journal 1997, 11, 34–36. [Google Scholar]
- Liao, P.; Vajdic, C.; Trollor, J.; Reppermund, S. Prevalence and incidence of physical health conditions in people with intellectual disability – a systematic review. PLOS ONE 2021, 16, e0256294. [Google Scholar] [CrossRef]
- Ayres, A. Jensory integration and learning disorders; Western Psychological Services: Los Angels, 1972; Volume 36, pp. 258–259. [Google Scholar]
- Goodman, R. The strengths and difficulties questionnaire: a research note. Journal of Child Psychology and Psychiatry and Allied Disciplines. 1997, 38, 581–586. [Google Scholar] [CrossRef]
- Goodman, R.; Meltzer, H.; Bailey, V. The strengths and difficulties questionnaire: A pilot study on the validity of the self-report version. Eur. Child Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.A.; Hastings, R.P.; Totsika, V. Clinical utility of the parent-reported Strengths and Difficulties Questionnaire as a screen for emotional and behavioral difficulties in children and adolescents with intellectual disability. The British journal of psychiatry: the journal of mental science. 2020, 218, 323–325. [Google Scholar] [CrossRef]
- Ulrich, D.A. Test of Gross Motor Development (Second Edition) Examiner’s Manual; pro-ed Publishers: Austin, TX, 2000; p. 3. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Taylor and Francis, 2013; pp. 5–13. [Google Scholar]
- Lixia, Q.; Xiaoying, J. An Investigation Report on Current Situation of the Development of Mainstreaming in China. Chinese Journal of Special Education. 2004, (05), 1–5. [Google Scholar]
- Lei, Z.; Dandan, W.; Xueping, W. Characteristics and Differences of Fundamental Movement Skills in Children and Youth with Different Severity of Intellectual Disability. Journal of Capital University of Physical Education and Sports. 2022, 34(02), 161–169. [Google Scholar]
- Chunling, L.; Hongying, M. Development and education of children with intellectual disabilities; Peking University Press: Beijing, 2011; pp. 26-28, 68-72. [Google Scholar]
- Jeoung, B. Motor proficiency differences among students with intellectual disabilities, autism, and developmental disability. J. Exerc. Rehabilitation 2018, 14, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Ilker, Y.; Nevin, E.; Ferman, K.; Bulent, A.; Erdal, Z.; Zafer, C. The Effects of Water Exercises and Swimming on Physical Fitness of Children with Mental Retardation. Journal of Human Kinetics. 2009, 21, 105–111. [Google Scholar]
- Nianli, Z. Development and education of children with autism spectrum disorders; Peking University Press: Beijing, 2011; pp. 10-13, 29. [Google Scholar]
- Green, D.; Charman, T.; Pickles, A.; Chandler, S.; Loucas, T.; Simonoff, E.; Baird, G. Impairment in movement skills of children with autistic spectrum disorders. Dev. Med. Child Neurol. 2009, 51, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Dekker, M.C.; Koot, H.M. DSM-IV Disorders in Children With Borderline to Moderate Intellectual Disability. I: Prevalence and Impact. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 915–922. [Google Scholar] [CrossRef] [PubMed]
- Ting, Z.; Junming, F. The Medical Foundation of Special Education; Peking University Press: Beijing, 2011; p. 202. [Google Scholar]
Figure 1.
Recruitment process of participants.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



