
Submitted:
19 July 2023
Posted:
21 July 2023
You are already at the latest version
Abstract
It is currently unknown whether thrombin generation is associated with venous thromboembolism (VTE) recurrence, major bleeding, and mortality in the elderly. Therefore, our aim was to prospectively study the association between thrombin generation and VTE recurrence, major bleeding and mortality in elderly patients with acute VTE. Consecutive patients aged ≥65years with acute VTE were followed for 2 years starting from 1 year after the index VTE. Primary outcomes were VTE recurrence, major bleeding and mortality. Thrombin generation was assessed in 565 patients 1 year after the index VTE. At this time, 59% of patients were still anticoagulated. Thrombin generation was discriminatory for VTE recurrence, but not for major bleeding and mortality in non-anticoagulated patients. Moreover, peak ratio (adjusted subhazard ratio 4.09, 95% CI, 1.12-14.92) and normalized peak ratio (adjusted subhazard ratio 2.18, 95% CI, 1.28-3.73) in presence/absence of thrombomodulin were associated with VTE recurrence, but not with major bleeding and mortality after adjustment for potential confounding factors. In elderly patients, thrombin generation was associated with VTE recurrence, but not with major bleeding and/or mortality. Therefore, our study suggests the potential usefulness of thrombin generation measurement after anticoagulation completion for VTE to help identifying among elderly patients those at higher risk of VTE recurrence.
Keywords:
Thrombin generation
; venous thromboembolism
; elderly
; bleeding
; mortality
1. Introduction
Venous thromboembolism (VTE), comprising deep vein thrombosis (DVT) and pulmonary embolism (PE), constitutes a worldwide major health issue, and a leading cause of death [1]. VTE incidence increases with age due to the accumulation of risk factors and comorbidities predisposing to thrombosis [2,3,4,5,6]. Incidence rate is about 1/10,000 annually before age 40 years, rises after age 45, and approaches 5–6/1,000 annually by age 80 [7]. In older patients, VTE results in higher mortality, but the rate of recurrence is no higher than in younger patients [4]. The morbidity burden of VTE on the older patient appears to be larger, with a higher increase in the incidence of PE compared with DVT with aging [7].
The recurrence rate of VTE is principally determined by the circumstances in which the index VTE occurs and varies between <3% and >8% annually after a first event [8]. The risk is greatest in patients whose first episode was associated with cancer, and lowest in those whose first episode was associated with a transient risk factor [8,9,10,11].
Because older patients are more likely to have comorbidities, they are not only at increased risk of VTE, but also of bleeding [6]. Therefore, managing anticoagulation in the elderly is often challenging. Since the risk of VTE recurrence is highest in the first 6 to 12 months after discontinuation of treatment for the initial event, and gradually decreases thereafter [4], the benefit of prolonged anticoagulation may be outweighed by the risk of clinically significant bleeding [12,13,14,15,16,17]. Consequently, identification of older patients who might benefit from indefinite anticoagulant treatment is paramount. In order to facilitate the identification of these patients, the benefit/risk ratio should be carefully evaluated by considering clinical and laboratory information. Of these, D-dimer has been proposed over the past twenty years as one of the laboratory tests that can be used to evaluate the risk of VTE recurrence after cessation of anticoagulation [18,19,20]. Recently, a higher-than-expected recurrence rate has been observed in patients who discontinued anticoagulation in response to negative D-dimer results, particularly in men [21]. Another study showed that the long-term risk of recurrence in patients with a first unprovoked VTE and negative D-dimer results is not low enough to warrant discontinuation of anticoagulation in men but can be envisaged in women [22]. Thus, the validation of alternative test to D-dimer is justified.
Thrombin activity may be recorded by continuously measuring the cleavage of a fluorescent substrate, yielding a thrombin generation (TG) curve [23]. From this curve, several parameters can be extracted, including thrombin burst time, maximum amount of thrombin generated, TG rate or total amount of thrombin generated. The TG assay proved to be a reliable predictor of recurrent VTE [24,25] and can therefore be used individually or in conjunction with D-dimer [26] to determine the risk of recurrence and the appropriate length of anticoagulation therapy. In a prospectively conducted cohort study including patients with a first unprovoked VTE, Hron et al. [27] reported that TG assessed after the cessation of anticoagulation can identify patients at a lower risk for recurrent VTE. In addition, a numerical simulation model showed that the TG assay was associated with the risk of first VTE [28]. TG increases with age [29,30] and TG parameters are associated with the risk of first venous thrombosis in the older adults [31]. However, it is unknown if TG is associated with recurrent VTE, major bleeding and mortality in the elderly.
Here, in a prospective cohort of VTE patients aged ≥65 years, we studied whether TG 1 year after index VTE is associated with VTE recurrence, major bleeding, and mortality for 2 years starting from 1 year after the index VTE.
2. Materials and Methods
2.1. Cohort Sample
The study was performed between 09/2009 and 12/2013 as part of the SWIss venous Thromboembolism COhort (SWITCO65+), a multicenter prospective cohort study to evaluate medical outcomes and quality of life of elderly patients with acute symptomatic VTE at the 5 university hospitals and 4 non-university hospitals in Switzerland [32,33]. Consecutive patients aged ≥65 years with acute VTE were followed for 2 years starting from 1 year after the index VTE. The patients had to give separate written consents for the clinical part of the study and for the future use of the blood samples. The study and biobank protocols were approved by the ethics committees of all participating hospitals [32,33]. The blood samples were collected between 09/2009 and 03/2012, and the patients were followed up until 12/2013. An outline of the study methods has been published [32,33].
2.2. Data Collection
For all registered patients, study nurses prospectively collected baseline information (Table 1). The follow-up consisted of one telephone interview and two face-to-face assessments during the first year of study participation, followed by semiannual contacts, alternating face-to-face assessments and telephone calls, and periodic revisions of the patient's hospital chart. At each visit/contact, study nurses interviewed patients to get information on the date and type of clinical events (recurrent VTE, bleeding, or death). If a clinical event had happened, this information was supplemented by reviewing medical records and interviewing patients' primary care physicians and family members [33].
2.3. Blood Samples
Venous blood was collected into 0.106 M trisodium citrate S-Monovette (Sarstedt, Nümbrecht, Germany) one year after the index VTE. The samples were handled in accordance with the guideline of the ISTH Scientific and Standardization Committee subcommittee [34,35]. The resulting platelet-free plasma was stored in small aliquots at -80°C within one hour of blood collection [32].
2.4. Thrombin Generation Assay
TG measurements were performed 1 year after the index VTE with the calibrated automated thrombogram (CAT) assay (Stago, Asnières-sur-Seine, France) as previously described [36]. Two experimental settings were used.
In the first setting (referred later on as CATlow tissue factor [TF]), 74 μL PFP was added to 20 μL of a mixture of 1 pmol L-1 TF and 4 µmol L-1 phospholipids (PPP reagent LOW, Stago), and of recombinant human thrombomodulin (Sekisui, Alveo AG, Switzerland) or 6 µL of HN-buffer (Hepes 20 mM, NaCl 140 mM, pH 7.4 + 5 mg mL-1 BSA), in a 96-well round bottom microtiter plate (Immulon2HB, Thermo Fischer Scientific, Reinach, Switzerland). The concentration of thrombomodulin was tested in a preliminary assay and selected by the ability to decrease by 50% the peak of thrombin.
For the second setting (referred later on as CAThigh TF), 74 μL PFP was added to 20 μL of a mixture of TF and phospholipids (7:3 mixture PPP reagent HIGH and MP reagent, Stago, Asnières-sur-Seine, France) and 6 µL of recombinant human activated protein C (APC) (Enzyme Research, Swansea, United Kingdom) or HN-buffer, in a 96-well round bottom microtiter plate. The concentration of APC was tested in a preliminary assay and selected by the ability to decrease by 90% the endogenous thrombin potential (ETP) [29].
The reaction was initiated with 20 μL of a mixture of fluorogenic substrate and CaCl2 (Fluobuffer, Stago, Asnières-sur-Seine, France) and fluorescence measured using a fluorescence plate reader (Fluoroskan Ascent, Thermo Labsystems, Helsinki, Finland). All experiences were carried out in duplicate at 37°C for each assay. In addition, the same reference plasma (Cryocheck Reference Control Normal, PrecisionBiologic, Dartmouth, Canada) was tested in all experiments in order to correct day-to-day variations. TG curves were generated using the Thrombinoscope software version 5.0.0.742 (Thrombinoscope BV, Maastricht, The Netherlands). Lag time, peak height, time to peak, ETP and the ETP ratio obtained in presence/absence of thrombomodulin (TM) or APC was calculated. Results from the reference plasma were used to calculate the normalized peak ratio as follows [37,38]: Patient peak+TM/Patient peak-TM)/Reference peak+TM/Reference peak-TM) and Patient peak+APC/Patient peak-APC)/Reference peak+APC/Reference peak-APC). Results from the control plasma were also used to calculate the normalized ETP ratio as follows [37,38]: Patient ETP+TM/Patient ETP-TM)/Reference ETP+TM/Reference ETP-TM) and Patient ETP+APC/Patient ETP-APC)/Reference ETP+APC/Reference ETP-APC).
2.5. Outcome Variables
The primary outcomes of the study were symptomatic VTE recurrence, major bleeding, and overall mortality between 12 months and 36 months after the index VTE. We adjudicated outcomes by interviewing the patient or patient representative, interviewing the patient's treating physician and reviewing hospital records [33].
Recurrent VTE was defined as fatal or new nonfatal PE or new DVT [39]. The diagnosis of recurrent VTE during follow-up was made on the basis of the following criteria: for DVT, on the basis of abnormal ultrasound findings; and for PE, on the basis of CT or angiography displaying new intraluminal defects, or on the basis of ventilation-perfusion lung scans exhibiting a high-probability pattern with new perfusion defects. A new proximal DVT, on the basis of abnormal ultrasound findings, associated with one or more new PE symptom(s) was also regarded as recurrent PE.
Major bleeding was defined as fatal bleeding, symptomatic bleeding at critical sites, or clinically overt bleeding accompanied by a decrease in hemoglobin level of at least 20 g L-1, or resulting in the transfusion of two or more units of packed red blood cells [40].
2.6. Statistical Analysis
Patient characteristics were compared between groups using the Chi-squared test for categorical variables and the non-parametric Mann-Whitney U test for continuous variables.
We calculated the incidence rates of a first VTE recurrence, first major bleed, or death at 2 years, starting 1 year after the index VTE, by level of the different TG parameters separately for anticoagulated and non-anticoagulated patients.
We did a complete case analysis for the different TG parameters, only patients with available values were analyzed.
The discriminative power of peak height or ETP in predicting VTE recurrence, major bleeding and mortality was determined by calculating the Harrell’s C concordance statistic. Associations between TG parameters, analyzed as continuous variables and the time to a first VTE recurrence and major bleeding were assessed by the use of competing risk regression accounting for non-PE-related and non-bleeding-related death, respectively, as a competing event [41]. The method yields subhazard ratios (SHR) with their corresponding 95% confidence intervals (CI). For mortality, an ordinary Cox regression with robust standard errors was calculated. We adjusted the model for previously published predictors of VTE recurrence or major bleeding [39,40,42,43,44,45,46,47,48,49,50,51]. For overall mortality, analyses were adjusted for age, gender, cancer, provoked VTE, prior VTE, overt PE, renal disease, history of major bleeding, heart failure, chronic lung disease, elevated heart rate, low blood pressure, low oxygen and periods of anticoagulation as a time-varying covariate [48,52]. The missing values in the adjustment variables were imputed a normal or an absence status.
3. Results
3.1. Study Sample
A total of 1863 were screened. We excluded 462 who had at least one of the following exclusion criteria: thrombosis at different site than lower limb (n = 21), catheter-related thrombosis (n = 7), insufficient ability to speak German or French (n = 51), follow-up not possible (n = 192), inability to provide informed consent (n = 285), leaving a sample of 1,401 eligible patients. After the exclusion of 398 patients who refused to provide informed consent, our initial study sample comprised 1,003 patients (54 % of screened patients) [33]. Of the 1003 enrolled patients aged ≥65 years with acute VTE, we excluded 438 patients, yielding a study sample of 565 patients (Figure 1). Of 438 excluded patients, 430 patients had no blood analyses 1 year after the index VTE, including TG.
Patient characteristics of the study cohort are reported in Table 1. Overall, 239 patients (42%) were females, and the median age was 74 years (interquartile range [IQR] 69–79 years). All patients but 1 were Caucasians. Three hundred and seventeen patients (56%) presented with an index PE.
Sixty-four patients (11%) had cancer-related VTE, 114 (20%) had provoked VTE and 387 (68%) had an unprovoked index VTE. Hundred and seventy-two patients (30%) had experienced prior VTE. Patients still under anticoagulation 1 year after the index VTE were more inclined to have PE only as index VTE, and, if DVT was the index VTE, they were more likely to have a proximal DVT. They were also more prone to have cancer-related VTE and unprovoked VTE. Finally, these patients were also less immobilized and had less major surgery during the last 3 months. However, they were less likely to have heart failure. Characteristics of tested and non-tested patients for TG are provided in Table S1. Untested patients were slightly older and showed more morbidity and more cancer-associated and provoked VTE than tested patients.
3.2. Thrombin Generation Parameters in Study Samples
TG was assessed in 565 patients 1 year after the index VTE (Figures S1 and S2). Among the 565 studied patients, 232 were not under anticoagulation and 333 patients were under anticoagulation. The group of patients not under anticoagulation has been studied in more details. In subgroups of patients, thrombomodulin resistance (n = 222) and normalized TG (n = 122) assays were performed in addition.
TG parameters with 1 pM TF in the absence of TM were comparable in patients with and without recurrent VTE in both anticoagulated and non-anticoagulated patients. (Figure S3). However, both peak ratio (patients with VTE recurrence, median 0.54, IQR 0.26-1.11 versus patients without VTE recurrence, median 0.46, IQR 0.23-0.88, P < 0.05) and normalized peak ratio (patients with VTE recurrence, median 0.99, IQR 0.46-2.87 versus patients without VTE recurrence, median 0.85, IQR 0.36-1.70, P < 0.05) with/without TM where slightly but significantly higher in patients with recurrent VTE and not under anticoagulation (P < 0.05) (Figure 2). When TG was measured with 13.6 pM TF, only time to peak was prolonged in the group of patients not under anticoagulation and with recurrent VTE (Figure S4-S5).
Peak (patients with major bleeding, median 123.2 nM, IQR 38.8-268.3 versus patients without major bleeding, median 148.6 nM, IQR 76.3-280.5, P < 0.05) and ETP (patients with major bleeding, median 1068 nM.min, IQR 669-2012 versus patients without major bleeding, median 1325 nM.min, IQR 791-2015, P < 0.05) measured using 1 pM TF were lower in non-anticoagulated patients who presented major bleeding during the follow-up period (Figure 3). However, ETP in presence of TM with 1 pM TF was higher in anticoagulated patients who had major bleeding during follow-up (Figure S6-S8).
Lag time and time to peak with 1 pM and 13.6 pM TF in non-anticoagulated patients who died during follow-up were longer than in patients who did not die during this period (Figure S9-S11). In addition, ETP with APC as well as normalized and non-normalized ETP ratio with/without APC using 13.6 pM TF were lower in non-anticoagulated patients who died than in non-anticoagulated patients who did not die during the follow-up period (Figure S12).
3.3. Incidence Rates of VTE Recurrence, Major Bleeding, and Mortality, and Thrombin Generation
During the 2-year follow-up, incidence rates (IR) of VTE recurrence and major bleeding were higher in non-anticoagulated patients with either peak ratio or normalized peak ratio (normalized peak ratio: VTE recurrence: ≤median, IR=4.5; 95% CI, 1.7-12.0; >median IR=19.4; 11.3-33.4; major bleeding: ≤median, IR=0; >median IR=4.0; 95% CI, 1.3-12.5), or ETP ratio or normalized ETP ratio with/without TM values above median than in those with peak and ETP ratio below median (normalized ETP ratio: VTE recurrence: ≤median, IR=7.1 ; 95% CI, 3.2-15.7; >median IR=15.5, 95% CI, 8.6-27.9; major bleeding: ≤median, IR=1.1, 95% CI, 0.2-8.1; >median IR=2.6, 95% CI, 0.6-10.3) (Table 2).
The mortality rate was higher in non-anticoagulated patients with peak ratio or normalized peak ratio, or high ETP ratio with/without TM than in those with peak and ETP ratio below median (Table 2). However, it was comparable in non-anticoagulated patients with low and high normalized ETP ratio in presence or absence of TM (Table 2).
3.4. Discriminative Power of Thrombin Generation Parameters for Outcomes
To assess the discriminative power of TG parameters, C-statistic values (95% CI) were calculated for TG parameters where TM was involved in non-anticoagulated patients 1 year after index VTE (Table 3). Peak ratio with/without TM (C-statistic 0.70, 95% CI [0.59 to 0.81]) and ETP with/without TM (C-statistic 0.70, 95% CI [0.60 to 0.80]) normalized with reference plasma were discriminatory for VTE recurrence, but not for major bleeding and overall mortality from 1 year to 3 years following index VTE. (Table 3).
3.5. Association between Thrombin Generation Parameters and Outcomes
We investigated the association of various TG parameters measured in non-anticoagulated patients 1 year after the index VTE with VTE recurrence, major bleeding and mortality from 1 to 3 years following the index VTE (Table 4).
Peak ratio in presence/absence of TM was associated with VTE recurrence (SHR: 4.09, 95% CI
[1.12-14.92] after adjustment for potential confounding factors for the risk of VTE recurrence). This
association remained when peak ratio was normalized with reference plasma (SHR: 2.18, 95% CI
[1.28-3.73] after adjustment for potential confounding factors for the risk of VTE recurrence).
However, peak ratio in presence/absence of TM was not associated with major bleeding and overall
mortality. ETP ratio in presence/absence along with ETP ratio with/without APC normalized with
reference plasma was not associated with VTE recurrence, major bleeding and mortality.
4. Discussion
We prospectively followed 565 elderly patients for 2 years starting from 1 year after the index VTE. Of these, 59% were still anticoagulated 1 year after the index VTE. Anticoagulated patients were more likely to experience prior VTE and unprovoked VTE than patients who were no longer anticoagulated 12 months after the initial VTE (prior VTE: 43% versus 13%; unprovoked VTE 75% versus 59%). We observed that several TG parameters were not only different for primary outcomes, but also discriminatory for VTE recurrence in non-anticoagulated patients and associated with it after adjustment for potential confounding factors.
TG has been used alone [24,25] or in conjunction with D-dimer [26] to evaluate the recurrence of VTE and to determine the length of secondary thromboprophylaxis. Several aspects of the design of our study differs from those of previous ones involving TG measurement to assess VTE recurrence [24,25,26,27,69], namely: (1) TG measured 1 year after the index VTE; (2) TG assessed in both anticoagulated and non-anticoagulated patients; (3) 2-year follow-up starting 1 year after the initial VTE; (4) inclusion of patients with provoked and cancer-related VTE; (5) cohort of elderly patients.
Our data showed that both peak ratio and peak ratio normalized with reference plasma with/without TM were higher in non-anticoagulated patients with recurrent VTE than in those without recurrent VTE. Time to peak at 13.6 pM TF was prolonged in non-anticoagulated patients with recurrent VTE. Peak along with ETP ratio with/without TM showed a trend for a discriminatory power for VTE recurrence, whereas both peak and ETP ratio with/without TM normalized with reference plasma showed a significant discriminatory power for VTE recurrence. These parameters were did not display a discriminatory power for both major bleeding and mortality. In addition, peak ratio in presence/absence of TM was associated with VTE recurrence after adjustment for potential confounding factors for the risk of VTE recurrence. This association remained when peak ratio was normalized with reference plasma. However, peak ratio in presence/absence of TM was not associated with major bleeding and overall mortality. These data point to the importance of these TG parameters not only in the general but also in the elderly population. To our knowledge, the association between TG parameters and VTE recurrence has not been previously demonstrated in the elderly. Notably, normalized peak and ETP ratio were more discriminatory than those that were not normalized, demonstrating the importance of the use of a reference plasma for TG measurement.
Non-anticoagulated patients who developed a major bleeding event during the follow-up period had lower peak and ETP at 1 pM TF than those who did not. Further validation of this parameter may help identifying an elderly population, in whom an extension of the anticoagulation might be potentially harmful. Peak and ETP with TM were higher in anticoagulated patients who had a major bleeding event than in those who did not, pointing to a potential usefulness of TG to monitor elderly patients under anticoagulation. Importantly, TG measurement has not been previously reported for major bleeding assessment in this age-group with VTE. However, we were unable to demonstrate and association between TG parameters and major bleeding.
Lag time and time to peak with 1 and 13.6 pM TF were longer, and ETP measured with APC and ETP ratio obtained in presence/absence of APC with 13.6 pM TF were lower in non-anticoagulated patients who died during the follow up than in those who did not. However, normalized ETP ratio obtained in presence/absence of APC was not associated with overall mortality. ETP measured in presence of APC and ETP obtained in presence/absence of APC at 13.6 pM TF were lower in anticoagulated patients who died than in non-anticoagulated patients who did not. These last data indicate that it might be valuable to measure TG in anticoagulated patients using a high concentration of TF. Further studies in a larger population would be necessary to confirm this approach. A few studies have examined the association between TG and mortality. The PROSPER study, which enrolled only older adults, demonstrated positive associations of vascular mortality with lag time and peak height and of total mortality with lag time [70]. After adjustment for interleukin-6 and C-reactive protein levels, however, the associations were no longer statistically significant, pointing to inflammation as a contributor to increased TG in this population. A smaller study showed that increased ETP and peak height (with 5 pM TF), independent of age, sex, and cardiovascular risk factors, were associated with an enhanced risk of cardiovascular death in patients with acute coronary syndrome [71]. In a recent large adult population-based study, an association was found between lag time with 1 pM TF and overall mortality and a relation, between elevated ETP with 5 pM TF and increased risk of death [72]. Although our study showed no significant differences and associations in peak or ETP regarding overall mortality, a significantly higher APC resistance in non-anticoagulated alive patients shows a promising further research topic. Tissue factor pathway inhibitor is found to be one of the major determinants to prolong lag time and reduce ETP in presence of APC and ETP ratio with/without APC lowering the APC resistance in TG [29], and known to be elevated in presence of co-morbidities such as obesity and diabetes mellitus [73], which may lead to higher mortality rate. However, our findings cannot be explained by this fact entirely as the distribution of these co-morbidities was comparable in both alive and dead non-anticoagulated patients of this cohort. Hence another determinant of this study finding should be considered.
Our study has some limitations. First, the study included 565 patients and 59% of them were still anticoagulated at the time of TG measurement. Second, TM resistance assay was only performed in 222 non-anticoagulated patients and normalized TG, in only 122 non-anticoagulated patients. The reason for creating this subgroups of patients was that there was not enough plasma materials for a complete analysis in some patients. This is because the initial analysis planed only TG testing without TM resistance and normalized TG assays. Third, all the patients but one were Caucasians; therefore, our findings may not be extrapolable to other ethnicities. Fourth, a significant number of patients had comorbidities including cancer (11%). Therefore, mortality from comorbid disease tends to be higher than the rate of VTE recurrence, because patients with limited life expectancy often do not have time to develop recurrent VTE. Fifth, the treatment of VTE has evolved since the establishment of this cohort: direct oral anticoagulants are used instead of VKAs for the vast majority of patients. Therefore, it is not clear whether the findings can be generalized to patients treated with direct oral anticoagulants. Sixth, protein C and S could not be measured in patients under anticoagulation, because most of them were receiving VKA.
In conclusion, we demonstrated that several TG parameters were discriminatory for VTE recurrencein non-anticoagulated elderly patients and associated with them, but not for the other primary outcomes (major bleeding and overall mortality. Therefore, our study suggests the potential usefulness of TG measurement after anticoagulation completion for VTE to help identifying among elderly patients those at higher risk of VTE recurrence. The addition of TG testing may also help to improve the performance of validated assessment measures of the risk of thrombosis. These findings will set the basis a larger prospective study.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1. Patient characteristics by thrombin generation testing status one year after index venous thromboembolism (VTE), Figure S1. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation 12 months after the index venous thromboembolism using 1pM tissue factor without thrombomodulin (TM), Figure S2 Thrombin generation in patients under anticoagulation and not under anticoagulation 12 months after the index venous thromboembolism using 13.6 pM tissue factor without activated protein C (APC), Figure S3. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation after index venous thromboembolism (VTE) using 1 pM tissue factor without thrombomodulin, Figure S4. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation after index venous thromboembolim (VTE) using 13.6 pM tissue factor without activated protein C, Figure S5. Peak and endogenous thrombin potential (ETP) in patients under anticoagulation and not under anticoagulation after index venous thromboembolim (VTE) using 13.6 pM tissue factor with activated protein C (APC), Figure S6. Peak and endogenous thrombin potential (ETP) in patients under anticoagulation and not under anticoagulation after index venous thromboembolism using 1 pM tissue factor with thrombomodulin (TM), Figure S7. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation after index venous thromboembolim using 13.6 pM tissue factor without activated protein C (APC), Figure S8. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation after index venous thromboembolim using 13.6 pM tissue factor with activated protein C (APC), Figure S9. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation after index venous thromboembolim using 1 pM tissue factor without thrombomodulin (TM), Figure S10. Peak and ETP in patients under anticoagulation and not under anticoagulation after index venous thromboembolim using 1 pM tissue factor, Figure S11. Thrombin generation parameters in patients under anticoagulation and not under anticoagulation after index venous thromboembolism using 13.6 pM tissue factor without activated protein C, Figure S12. Peak and endogenous thrombin potential (ETP) in patients under anticoagulation and not under anticoagulation after index venous thromboembolism using 13.6 pM tissue factor with activated protein C (APC).
Author Contributions
Conceptualization, A.A.S.; methodology, K.V.B., S.C., C.Q., A.A.S.; software, K.V.B., S.C., O.S.; validation, K.V.B., O.S., A.A.S.; formal analysis, K.V.B., S.R., S.C., C.Q., O.S. and A.A.S.; investigation, K.V.B., S.R., S.C., O.S., M.M., M.R., D.S., J.H.B., B:F., J.O., N.K., C.M.M., M.H., M.B., M.A., L.M., O.H., N.R., D:A. and A.A.S.; data curation, K.V.B., S.C., O.S., A.A.S.; writing—original draft preparation, K.V.B., S.R. and A.A.S.; writing—review and editing, K.V.B., S.R., S.C., O.S., M.M., M.R., D.S., J.H.B., B:F., J.O., N.K., C.M.M., M.H., M.B., M.A., L.M., O.H., N.R., D:A. and A.A.S.; visualization, K.V.B. and A.A.S.; supervision, A.A.S.; project administration, K.V.B, S.C., C.Q. and A.A.S.; funding acquisition, D.A. and A.A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by grants of the Swiss National Science Foundation grant number 33CSCO-122659/139 470 to D.A. and grant number 310030_153436 to A.A.S.
Institutional Review Board Statement
The protocol of the study is registered at clinicaltrials.gov (NCT00973596). The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by Swiss Ethics Committee.
Informed Consent Statement
Patient consent was waived according to the Swiss Ethics Committee, as the further use of health-related datasets and samples is permissible without the consent of the participants if all criteria of Articles 34 and 37–40 of the Swiss Human Research Act are fulfilled, as was the case for this study.
Data Availability Statement
There were no publicly archived datasets analyzed or generated during the study.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M. Epidemiology and risk factors for venous thrombosis. Seminars in hematology 2007, 44, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Deitelzweig, S.B.; Johnson, B.H.; Lin, J.; Schulman, K.L. Prevalence of clinical venous thromboembolism in the USA: current trends and future projections. American journal of hematology 2011, 86, 217–220. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A. Predicting the risk of venous thromboembolism recurrence. American journal of hematology 2012, 87 Suppl 1, S63–67. [Google Scholar] [CrossRef]
- Spencer, F.A.; Gore, J.M.; Lessard, D.; Emery, C.; Pacifico, L.; Reed, G.; Gurwitz, J.H.; Goldberg, R.J. Venous thromboembolism in the elderly. A community-based perspective. Thrombosis and haemostasis 2008, 100, 780–788. [Google Scholar]
- Spencer, F.A.; Gurwitz, J.H.; Schulman, S.; Linkins, L.A.; Crowther, M.A.; Ginsberg, J.S.; Lee, A.Y.; Saczynski, J.S.; Anand, S.; Lessard, D.; et al. Venous thromboembolism in older adults: A community-based study. The American journal of medicine 2014, 127, 530–537. [Google Scholar] [CrossRef]
- Silverstein, M.D.; Heit, J.A.; Mohr, D.N.; Petterson, T.M.; O'Fallon, W.M.; Melton, L.J. , 3rd. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Archives of internal medicine 1998, 158, 585–593. [Google Scholar] [CrossRef]
- Ainle, F.N. , Kevane, B. Which patients are at high risk of recurrent venous thromboembolism (deep vein thrombosis and pulmonary embolism)? Blood Adv 2020, 4, 5595–5606. [Google Scholar] [CrossRef]
- Abdulla, A. , Davis, W.M.; Ratnaweera, N.; Szefer, E.; Ballantyne Scott, B.; Lee, A.Y.Y. A Meta-Analysis of Case Fatality Rates of Recurrent Venous Thromboembolism and Major Bleeding in Patients with Cancer. Thrombosis and haemostasis 2020, 120, 702–713. [Google Scholar]
- Iorio, A.; Kearon, C.; Filippucci, E.; Marcucci, M.; Macura, A.; Pengo, V.; Siragusa, S.; Palareti, G. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: a systematic review. Archives of internal medicine 2010, 170, 1710–1716. [Google Scholar] [CrossRef]
- Khan, F.; Rahman, A.; Carrier, M.; Kearon, C.; Weitz, J.I.; Schulman, S.; Couturaud, F.; Eichinger, S.; Kyrle, P.A.; Becattini, C.; et al. Long term risk of symptomatic recurrent venous thromboembolism after discontinuation of anticoagulant treatment for first unprovoked venous thromboembolism event: systematic review and meta-analysis. Bmj 2019, 366, l4363. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Prandoni, P.; Santamaria, M.G.; Bagatella, P.; Iorio, A.; Bazzan, M.; Moia, M.; Guazzaloca, G.; Bertoldi, A.; Tomasi, C.; et al. Three months versus one year of oral anticoagulant therapy for idiopathic deep venous thrombosis. Warfarin Optimal Duration Italian Trial Investigators. The New England journal of medicine 2001, 345, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Gent, M.; Hirsh, J.; Weitz, J.; Kovacs, M.J.; Anderson, D.R.; Turpie, A.G.; Green, D.; Ginsberg, J.S.; Wells, P.; et al. A comparison of three months of anticoagulation with extended anticoagulation for a first episode of idiopathic venous thromboembolism. The New England journal of medicine 1999, 340, 901–907. [Google Scholar] [CrossRef]
- Kearon, C.; Ginsberg, J.S.; Kovacs, M.J.; Anderson, D.R.; Wells, P.; Julian, J.A. , MacKinnon, B.; Weitz, J.I.; Crowther, M.A.; Dolan, S.; et al. Comparison of low-intensity warfarin therapy with conventional-intensity warfarin therapy for long-term prevention of recurrent venous thromboembolism. The New England journal of medicine 2003, 349, 631–639. [Google Scholar] [CrossRef]
- Palareti, G.; Leali, N.; Coccheri, S.; Poggi, M.; Manotti, C.; D'Angelo, A.; Pengo, V.; Erba, N.; Moia, M.; Ciavarella, N.; et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Italian Study on Complications of Oral Anticoagulant Therapy. Lancet 1996, 348, 423–428. [Google Scholar] [CrossRef]
- Pinede, L.; Ninet, J.; Duhaut, P.; Chabaud, S.; Demolombe-Rague, S.; Durieu, I.; Nony, P.; Sanson, C.; Boissel, J.P.; Investigators of the "Duree Optimale du Traitement AntiVitamines KS. Comparison of 3 and 6 months of oral anticoagulant therapy after a first episode of proximal deep vein thrombosis or pulmonary embolism and comparison of 6 and 12 weeks of therapy after isolated calf deep vein thrombosis. Circulation 2001, 103, 2453–2460. [Google Scholar] [CrossRef]
- Schulman, S.; Rhedin, A.S.; Lindmarker, P.; Carlsson, A.; Larfars, G.; Nicol, P.; Loogna, E.; Svensson, E.; Ljungberg, B.; Walter, H. A comparison of six weeks with six months of oral anticoagulant therapy after a first episode of venous thromboembolism. Duration of Anticoagulation Trial Study Group. The New England journal of medicine 1995, 332, 1661–1665. [Google Scholar] [CrossRef]
- Cosmi, B.; Legnani, C.; Tosetto, A.; Pengo, V.; Ghirarduzzi, A.; Testa, S.; Prisco, D.; Poli, D.; Tripodi, A.; Marongiu, F.; et al. Usefulness of repeated D-dimer testing after stopping anticoagulation for a first episode of unprovoked venous thromboembolism: the PROLONG II prospective study. Blood 2010, 115, 481–488. [Google Scholar] [CrossRef]
- Douketis, J.; Tosetto, A.; Marcucci, M.; Baglin, T.; Cushman, M.; Eichinger, S.; Palareti, G.; Poli, D.; Tait, R.C.; Iorio, A. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Annals of internal medicine 2010, 153, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Palareti, G.; Cosmi, B.; Legnani, C.; Tosetto, A.; Brusi, C.; Iorio, A.; Pengo, V.; Ghirarduzzi, A.; Pattacini, C. ; Testa S; et al: D-dimer testing to determine the duration of anticoagulation therapy. The New England journal of medicine 2006, 355, 1780–1789. [Google Scholar] [CrossRef]
- Kearon, C. Natural history of venous thromboembolism. Seminars in vascular medicine 2001, 1, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Parpia, S.; Spencer, F.A.; Schulman, S.; Stevens, S.M.; Shah, V.; Bauer, K.A.; Douketis, J.D.; Lentz, S.R.; Kessler, C.M.; et al. Long-term risk of recurrence in patients with a first unprovoked venous thromboembolism managed according to d-dimer results; A cohort study. Journal of thrombosis and haemostasis : JTH 2019, 17, 1144–1152. [Google Scholar] [CrossRef] [PubMed]
- Hemker, H.C.; Al Dieri, R.; De Smedt, E.; Beguin, S. Thrombin generation, a function test of the haemostatic-thrombotic system. Thrombosis and haemostasis 2006, 96, 553–561. [Google Scholar]
- Tripodi, A.; Legnani, C.; Chantarangkul, V.; Cosmi, B.; Palareti, G.; Mannucci, P.M. High thrombin generation measured in the presence of thrombomodulin is associated with an increased risk of recurrent venous thromboembolism. Journal of thrombosis and haemostasis : JTH 2008, 6, 1327–1333. [Google Scholar] [CrossRef]
- van Hylckama Vlieg, A.; Baglin, C.A.; Luddington, R.; MacDonald, S.; Rosendaal, F.R.; Baglin, T.P. The risk of a first and a recurrent venous thrombosis associated with an elevated D-dimer level and an elevated thrombin potential: results of the THE-VTE study. Journal of thrombosis and haemostasis : JTH 2015, 13, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Eichinger, S.; Hron, G.; Kollars, M.; Kyrle, P.A. Prediction of recurrent venous thromboembolism by endogenous thrombin potential and D-dimer. Clinical chemistry 2008, 54, 2042–2048. [Google Scholar] [CrossRef]
- Hron, G.; Kollars, M.; Binder, B.R.; Eichinger, S.; Kyrle, P.A. Identification of patients at low risk for recurrent venous thromboembolism by measuring thrombin generation. Jama 2006, 296, 397–402. [Google Scholar] [CrossRef]
- Brummel-Ziedins, K.E.; Vossen, C.Y.; Butenas, S.; Mann, K.G.; Rosendaal, F.R. Thrombin generation profiles in deep venous thrombosis. Journal of thrombosis and haemostasis : JTH 2005, 3, 2497–2505. [Google Scholar] [CrossRef]
- Dielis, A.W.; Castoldi, E.; Spronk, H.M.; van Oerle, R.; Hamulyak, K.; Ten Cate, H.; Rosing, J. Coagulation factors and the protein C system as determinants of thrombin generation in a normal population. Journal of thrombosis and haemostasis : JTH 2008, 6, 125–131. [Google Scholar] [CrossRef]
- Haidl, H.; Cimenti, C.; Leschnik, B.; Zach, D.; Muntean, W. Age-dependency of thrombin generation measured by means of calibrated automated thrombography (CAT). Thrombosis and haemostasis 2006, 95, 772–775. [Google Scholar] [CrossRef]
- Wang, H.; Rosendaal, F.R.; Cushman, M.; van Hylckama Vlieg, A. D-dimer, thrombin generation, and risk of a first venous thrombosis in the elderly. Research and practice in thrombosis and haemostasis 2021, 5, e12536. [Google Scholar] [CrossRef]
- Mean, M.; Aujesky, D.; Lammle, B.; Gerschheimer, C.; Trelle, S.; Angelillo-Scherrer, A. Design and establishment of a biobank in a multicenter prospective cohort study of elderly patients with venous thromboembolism (SWITCO65+). Journal of thrombosis and thrombolysis 2013, 36, 484–491. [Google Scholar] [CrossRef]
- Mean, M.; Righini, M.; Jaeger, K.; Beer, H.J.; Frauchiger, B.; Osterwalder, J.; Kucher, N.; Lammle, B.; Cornuz, J.; Angelillo-Scherrer, A.; et al. The Swiss cohort of elderly patients with venous thromboembolism (SWITCO65+): rationale and methodology. Journal of thrombosis and thrombolysis 2013, 36, 475–483. [Google Scholar] [CrossRef]
- Calzavarini, S.; Brodard, J.; Quarroz, C.; Maire, L.; Nutzi, R.; Jankovic, J.; Rotondo, L.C.; Giabbani, E.; Fiedler, G.M.; Nagler, M.; et al. Thrombin generation measurement using the ST Genesia Thrombin Generation System in a cohort of healthy adults: Normal values and variability. Research and practice in thrombosis and haemostasis 2019, 3, 758–768. [Google Scholar] [CrossRef] [PubMed]
- Dargaud, Y.; Wolberg, A.S.; Gray, E.; Negrier, C.; Hemker, H.C.; Subcommittee on Factor Viii FIX, Rare Coagulation D. Proposal for standardized preanalytical and analytical conditions for measuring thrombin generation in hemophilia: communication from the SSC of the ISTH. Journal of thrombosis and haemostasis : JTH 2017, 15, 1704–1707. [Google Scholar] [CrossRef]
- Brodard, J.; Calzavarini, S.; Quarroz, C.; Berzigotti, A.; De Gottardi, A.; Angelillo-Scherrer, A. Resistance to thrombomodulin correlates with liver stiffness in chronic liver disease a prospective single-center cohort study. Thrombosis research 2021, 207, 40–49. [Google Scholar] [CrossRef]
- Tripodi, A. Detection of procoagulant imbalance. Modified endogenous thrombin potential with results expressed as ratio of values with-to-without thrombomodulin. Thrombosis and haemostasis 2017, 117, 830–836. [Google Scholar] [PubMed]
- Hemker, H.C.; Giesen, P.; Al Dieri, R.; Regnault, V.; de Smedt, E.; Wagenvoord, R.; Lecompte, T.; Beguin, S. Calibrated automated thrombin generation measurement in clotting plasma. Pathophysiology of haemostasis and thrombosis 2003, 33, 4–15. [Google Scholar] [CrossRef] [PubMed]
- Prandoni, P.; Noventa, F.; Ghirarduzzi, A.; Pengo, V.; Bernardi, E.; Pesavento, R.; Iotti, M.; Tormene, D.; Simioni, P.; Pagnan, A. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica 2007, 92, 199–205. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C.; Subcommittee on Control of Anticoagulation of the S, Standardization Committee of the International Society on T, Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. Journal of thrombosis and haemostasis : JTH 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Fine, J.P.; Gray, R.J. A proportional Hazards Model for the Subdistribution of a Competing Risk. Journal of the American Statistical Association 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Agnelli, G.; Prandoni, P.; Becattini, C.; Silingardi; M. ; Taliani, M.R.; Miccio, M.; Imberti, D.; Poggio, R.; Ageno, W.; Pogliani, E; et al. Extended oral anticoagulant therapy after a first episode of pulmonary embolism. Annals of internal medicine 2003, 139, 19–25. [Google Scholar] [CrossRef]
- Boutitie, F.; Pinede, L.; Schulman, S.; Agnelli, G.; Raskob, G.; Julian, J.; Hirsh, J.; Kearon, C. Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants' data from seven trials. Bmj 2011, 342, d3036. [Google Scholar] [CrossRef] [PubMed]
- Christiansen, S.C.; Lijfering, W.M.; Helmerhorst, F.M.; Rosendaal, F.R.; Cannegieter, S. C: Sex difference in risk of recurrent venous thrombosis and the risk profile for a second event. Journal of thrombosis and haemostasis : JTH 2010, 8, 2159–2168. [Google Scholar] [CrossRef]
- Hansson, P.O.; Sorbo, J.; Eriksson, H. Recurrent venous thromboembolism after deep vein thrombosis: incidence and risk factors. Archives of internal medicine 2000, 160, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Mohr, D.N.; Silverstein, M.D.; Petterson, T.M.; O'Fallon, W.M.; Melton, L.J. , 3rd. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Archives of internal medicine 2000, 160, 761–768. [Google Scholar] [CrossRef]
- Huang, W.; Goldberg, R.J.; Anderson, F.A.; Cohen, A.T.; Spencer, F.A. Occurrence and predictors of recurrence after a first episode of acute venous thromboembolism: population-based Worcester Venous Thromboembolism Study. Journal of thrombosis and thrombolysis 2016, 41, 525–538. [Google Scholar] [CrossRef] [PubMed]
- Insam, C.; Mean, M.; Limacher, A.; Angelillo-Scherrer, A.; Aschwanden, M.; Banyai, M.; Beer, J.H.; Bounameaux, H.; Egloff, M.; Frauchiger, B.; et al. Anticoagulation Management Practices and Outcomes in Elderly Patients with Acute Venous Thromboembolism: A Clinical Research Study. PloS one 2016, 11, e0148348. [Google Scholar] [CrossRef]
- Lopez-Jimenez, L.; Montero, M.; Gonzalez-Fajardo, J.A.; Arcelus, J.I.; Suarez, C.; Lobo, J.L.; Monreal, M.; RIETE Investigators. Venous thromboembolism in very elderly patients: findings from a prospective registry (RIETE). Haematologica 2006, 91, 1046–1051. [Google Scholar]
- Prandoni, P.; Lensing, A.W.; Piccioli, A.; Bernardi, E.; Simioni, P.; Girolami, B.; Marchiori, A.; Sabbion, P.; Prins, M.H.; Noventa, F.; et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood 2002, 100, 3484–3488. [Google Scholar] [CrossRef]
- Wattanakit, K.; Cushman, M.; Stehman-Breen, C.; Heckbert, S.R.; Folsom, A.R. Chronic kidney disease increases risk for venous thromboembolism. Journal of the American Society of Nephrology : JASN 2008, 19, 135–140. [Google Scholar] [CrossRef]
- Gussoni, G.; Frasson, S.; La Regina, M.; Di Micco, P.; Monreal, M.; RIETE Investigators. Three-month mortality rate and clinical predictors in patients with venous thromboembolism and cancer. Findings from the RIETE registry. Thrombosis research 2013, 131, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Beyth, R.J.; Quinn, L.M.; Landefeld, C.S. Prospective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarin. The American journal of medicine 1998, 105, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Fang, M.C.; Go, A.S.; Chang, Y.; Borowsky, L.H.; Pomernacki, N.K.; Udaltsova, N.; Singer, D.E. A new risk scheme to predict warfarin-associated hemorrhage: The ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) Study. Journal of the American College of Cardiology 2011, 58, 395–401. [Google Scholar] [CrossRef]
- Gage, B.F.; Yan, Y.; Milligan, P.E.; Waterman, A.D.; Culverhouse, R.; Rich, M.W.; Radford, M.J. Clinical classification schemes for predicting hemorrhage: results from the National Registry of Atrial Fibrillation (NRAF). American heart journal 2006, 151, 713–719. [Google Scholar] [CrossRef]
- Hutten, B.A.; Prins, M.H.; Gent, M.; Ginsberg, J.; Tijssen, J.G.; Buller, H.R. ; Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both malignancy and achieved international normalized ratio: a retrospective analysis. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2000, 18, 3078–3083. [Google Scholar] [CrossRef] [PubMed]
- Kuijer, P.M.; Hutten, B.A.; Prins, M.H.; Buller, H.R. Prediction of the risk of bleeding during anticoagulant treatment for venous thromboembolism. Archives of internal medicine 1999, 159, 457–460. [Google Scholar] [CrossRef]
- Landefeld, C.S.; Goldman, L. Major bleeding in outpatients treated with warfarin: incidence and prediction by factors known at the start of outpatient therapy. The American journal of medicine 1989, 87, 144–152. [Google Scholar] [CrossRef]
- Lip, G.Y.; Frison, L.; Halperin, J.L.; Lane, D.A. Comparative validation of a novel risk score for predicting bleeding risk in anticoagulated patients with atrial fibrillation: the HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile INR, Elderly, Drugs/Alcohol Concomitantly) score. Journal of the American College of Cardiology 2011, 57, 173–180. [Google Scholar]
- Nieto, J.A.; Bruscas, M.J.; Ruiz-Ribo, D.; Trujillo-Santos, J.; Valle, R.; Ruiz-Gimenez, N.; Monreal, M.; RIETE Investigators. Acute venous thromboembolism in patients with recent major bleeding. The influence of the site of bleeding and the time elapsed on outcome. Journal of thrombosis and haemostasis : JTH 2006, 4, 2367–2372. [Google Scholar] [CrossRef]
- Olesen, J.B.; Lip, G.Y.; Hansen, P.R.; Lindhardsen, J.; Ahlehoff, O.; Andersson, C.; Weeke, P.; Hansen, M.L.; Gislason, G.H.; Torp-Pedersen, C. Bleeding risk in 'real world' patients with atrial fibrillation: comparison of two established bleeding prediction schemes in a nationwide cohort. Journal of thrombosis and haemostasis : JTH 2011, 9, 1460–1467. [Google Scholar] [CrossRef]
- Pisters, R.; Lane, D.A.; Nieuwlaat, R.; de Vos, C.B.; Crijns, H.J.; Lip, G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest 2010, 138, 1093–1100. [Google Scholar] [CrossRef]
- Prandoni, P.; Lensing, A.W.; Cogo, A.; Cuppini, S.; Villalta, S.; Carta, M.; Cattelan, A.M.; Polistena, P.; Bernardi, E.; Prins, M.H. The long-term clinical course of acute deep venous thrombosis. Annals of internal medicine 1996, 125, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Gimenez, N.; Suarez, C.; Gonzalez, R.; Nieto, J.A.; Todoli, J.A.; Samperiz, A.L.; Monreal, M.; RIETE Investigators. Predictive variables for major bleeding events in patients presenting with documented acute venous thromboembolism. Findings from the RIETE Registry. Thrombosis and haemostasis 2008, 100, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Shireman, T.I.; Mahnken, J.D.; Howard, P.A.; Kresowik, T.F.; Hou, Q.; Ellerbeck, E.F. Development of a contemporary bleeding risk model for elderly warfarin recipients. Chest 2006, 130, 1390–1396. [Google Scholar] [CrossRef] [PubMed]
- Torn, M.; Bollen, W.L.; van der Meer, F.J.; van der Wall, E.E.; Rosendaal, F.R. Risks of oral anticoagulant therapy with increasing age. Archives of internal medicine 2005, 165, 1527–1532. [Google Scholar] [CrossRef]
- van der Meer, F.J.; Rosendaal, F.R.; Vandenbroucke, J.P.; Briet, E. Bleeding complications in oral anticoagulant therapy. An analysis of risk factors. Archives of internal medicine 1993, 153, 1557–1562. [Google Scholar] [CrossRef]
- White, R.H.; Beyth; R. J.; Zhou, H.; Romano, P.S. Major bleeding after hospitalization for deep-venous thrombosis. The American journal of medicine 1999, 107, 414–424. [Google Scholar] [CrossRef]
- Chaireti, R.; Jennersjo, C.; Lindahl, T.L. Is thrombin generation at the time of an acute thromboembolic episode a predictor of recurrence? The LInkoping Study on Thrombosis (LIST)--a 7-year follow-up. Thrombosis research 2013, 131, 135–139. [Google Scholar] [CrossRef]
- Loeffen, R.; van Oerle, R.; Leers, M.P.; Kragten, J.A.; Crijns, H.; Spronk, H.M.; Ten Cate, H. Factor XIa and Thrombin Generation Are Elevated in Patients with Acute Coronary Syndrome and Predict Recurrent Cardiovascular Events. PloS one 2016, 11, e0158355. [Google Scholar] [CrossRef]
- Attanasio, M.; Marcucci, R.; Gori, A.M.; Paniccia, R.; Valente, S.; Balzi, D.; Barchielli, A.; Carrabba, N.; Valenti, R.; Antoniucci, D.; et al. Residual thrombin potential predicts cardiovascular death in acute coronary syndrome patients undergoing percutaneous coronary intervention. Thrombosis research 2016, 147, 52–57. [Google Scholar] [CrossRef] [PubMed]
- van Paridon, P.C.S.; Panova-Noeva, M.; van Oerle, R.; Schultz, A.; Hermanns, I.M.; Prochaska, J.H.; Arnold, N.; Binder, H.; Schmidtmann, I.; Beutel, M.E.; et al. Thrombin generation in cardiovascular disease and mortality - results from the Gutenberg Health Study. Haematologica 2020, 105, 2327–2334. [Google Scholar] [CrossRef] [PubMed]
- Vambergue, A.; Rugeri, L.; Gaveriaux, V.; Devos, P.; Martin, A.; Fermon, C.; Fontaine, P.; Jude, B. Factor VII, tissue factor pathway inhibitor, and monocyte tissue factor in diabetes mellitus: influence of type of diabetes, obesity index, and age. Thrombosis research 2001, 101, 367–375. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram of patients included in the study. VTE, venous thromboembolism.
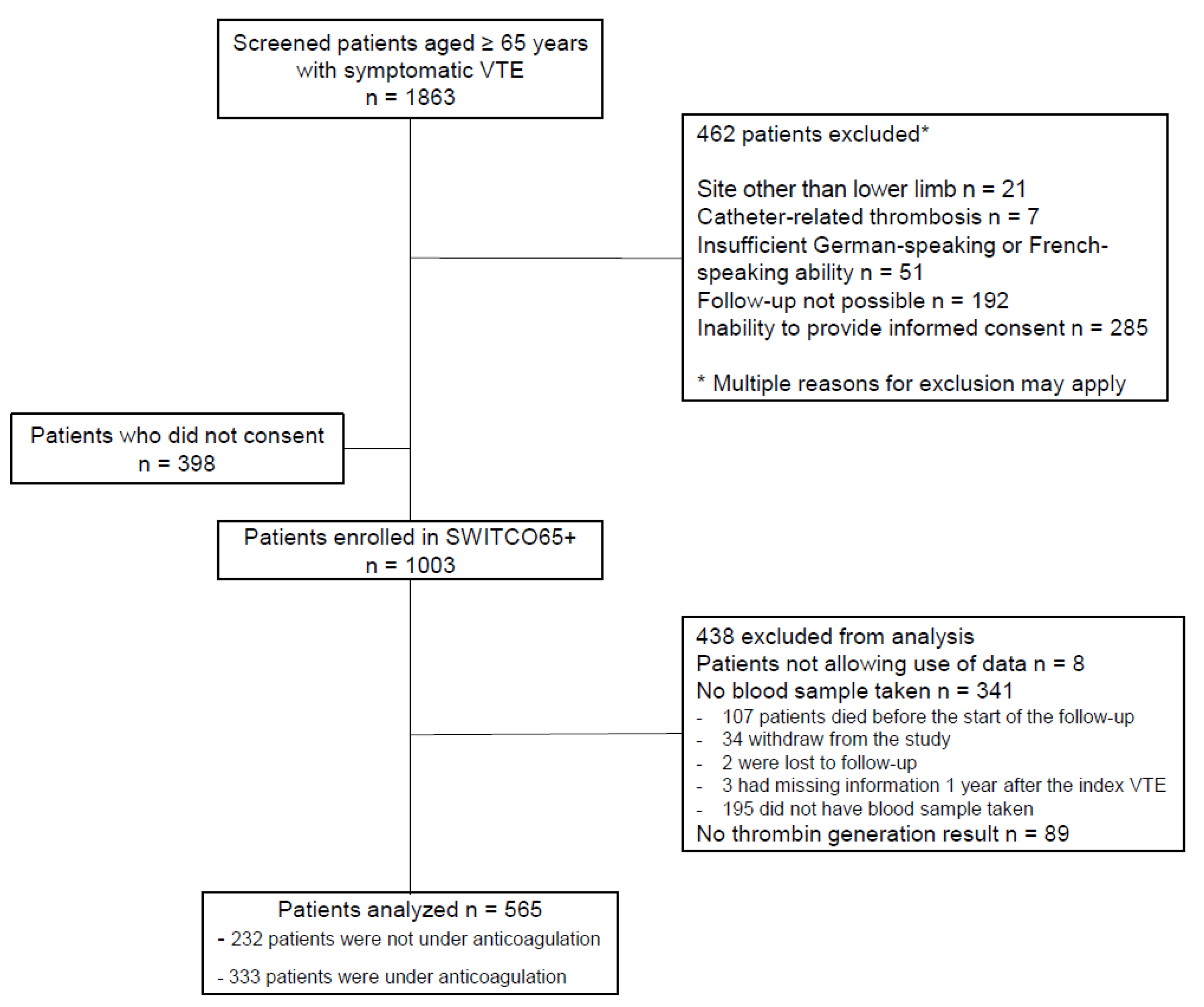
Figure 2.
Thrombin generation parameters in patients under anticoagulation and not under anticoagulation 12 months after the index venous thromboembolism (VTE) at 1 pM TF with and without thrombomodulin (TM). A, Peak and endogenous thrombin potential (ETP) with TM. B, Peak and ETP ratio with/without TM. C, Peak and ETP ratio with/without TM normalized with reference plasma. The grey boxes indicate patients with VTE recurrence and the white boxes, those without VTE recurrence up to 24 months following the index VTE. Box-plots of thrombin generation parameters are presented as median with interquartile range (5-95%). Groups were compared using Mann-Whitney U test. ns, not significant; *, P < 0.05.
Figure 2.
Thrombin generation parameters in patients under anticoagulation and not under anticoagulation 12 months after the index venous thromboembolism (VTE) at 1 pM TF with and without thrombomodulin (TM). A, Peak and endogenous thrombin potential (ETP) with TM. B, Peak and ETP ratio with/without TM. C, Peak and ETP ratio with/without TM normalized with reference plasma. The grey boxes indicate patients with VTE recurrence and the white boxes, those without VTE recurrence up to 24 months following the index VTE. Box-plots of thrombin generation parameters are presented as median with interquartile range (5-95%). Groups were compared using Mann-Whitney U test. ns, not significant; *, P < 0.05.
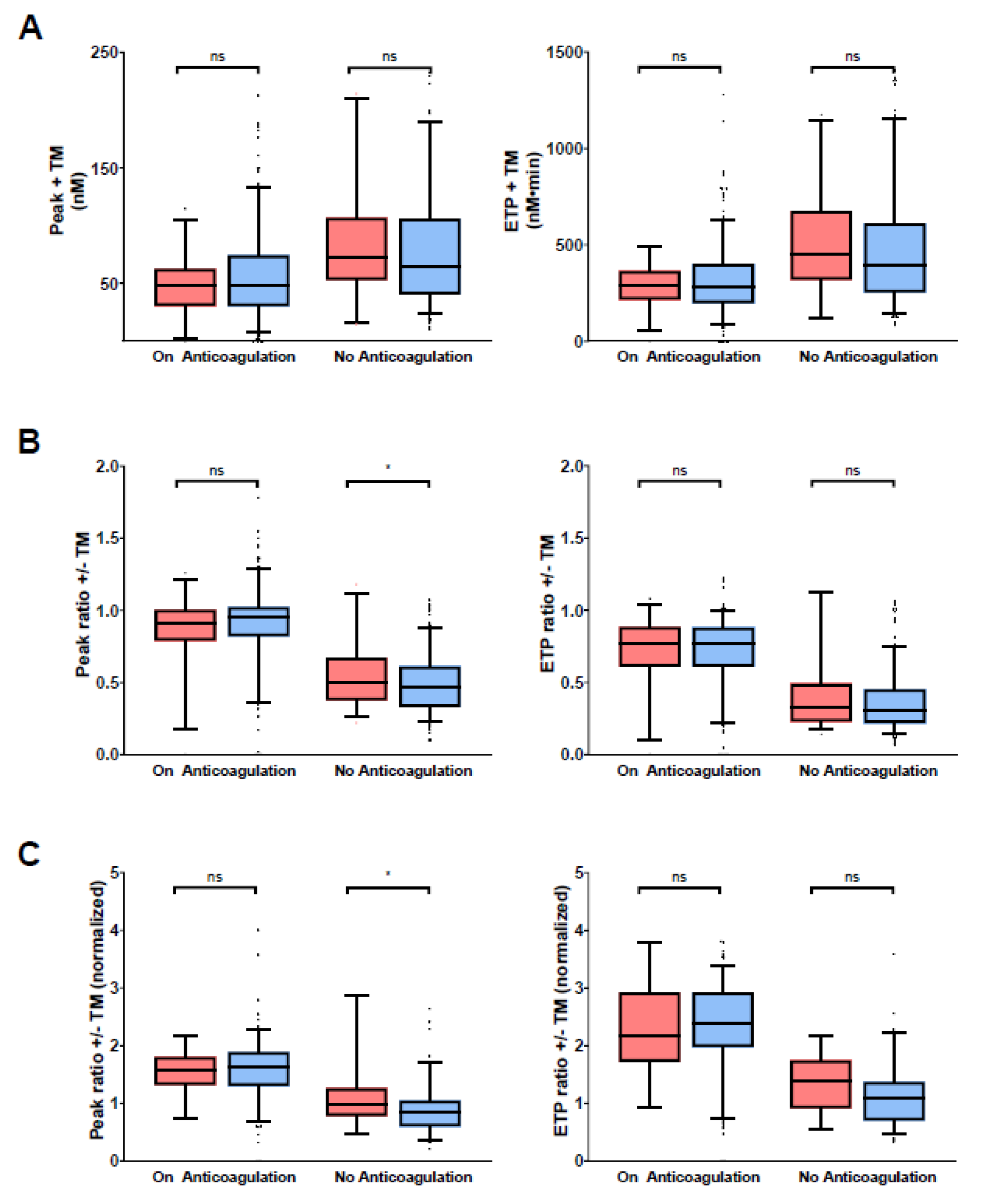
Figure 3.
Thrombin generation parameters in patients under anticoagulation and not under anticoagulation 12 months after index venous thromboembolism (VTE) at 1 pM TF without thrombomodulin (TM). The grey boxes indicate patients who had a major bleeding event and the white boxes, those without major bleeding up to 24 months following the index VTE. Box-plots of thrombin generation parameters are presented as median with interquartile range (5-95%) are indicated. Groups were compared using the Mann-Whitney U test. ETP, endogenous potential; ns, not significant; *P < 0.05; **P < 0.01.
Figure 3.
Thrombin generation parameters in patients under anticoagulation and not under anticoagulation 12 months after index venous thromboembolism (VTE) at 1 pM TF without thrombomodulin (TM). The grey boxes indicate patients who had a major bleeding event and the white boxes, those without major bleeding up to 24 months following the index VTE. Box-plots of thrombin generation parameters are presented as median with interquartile range (5-95%) are indicated. Groups were compared using the Mann-Whitney U test. ETP, endogenous potential; ns, not significant; *P < 0.05; **P < 0.01.
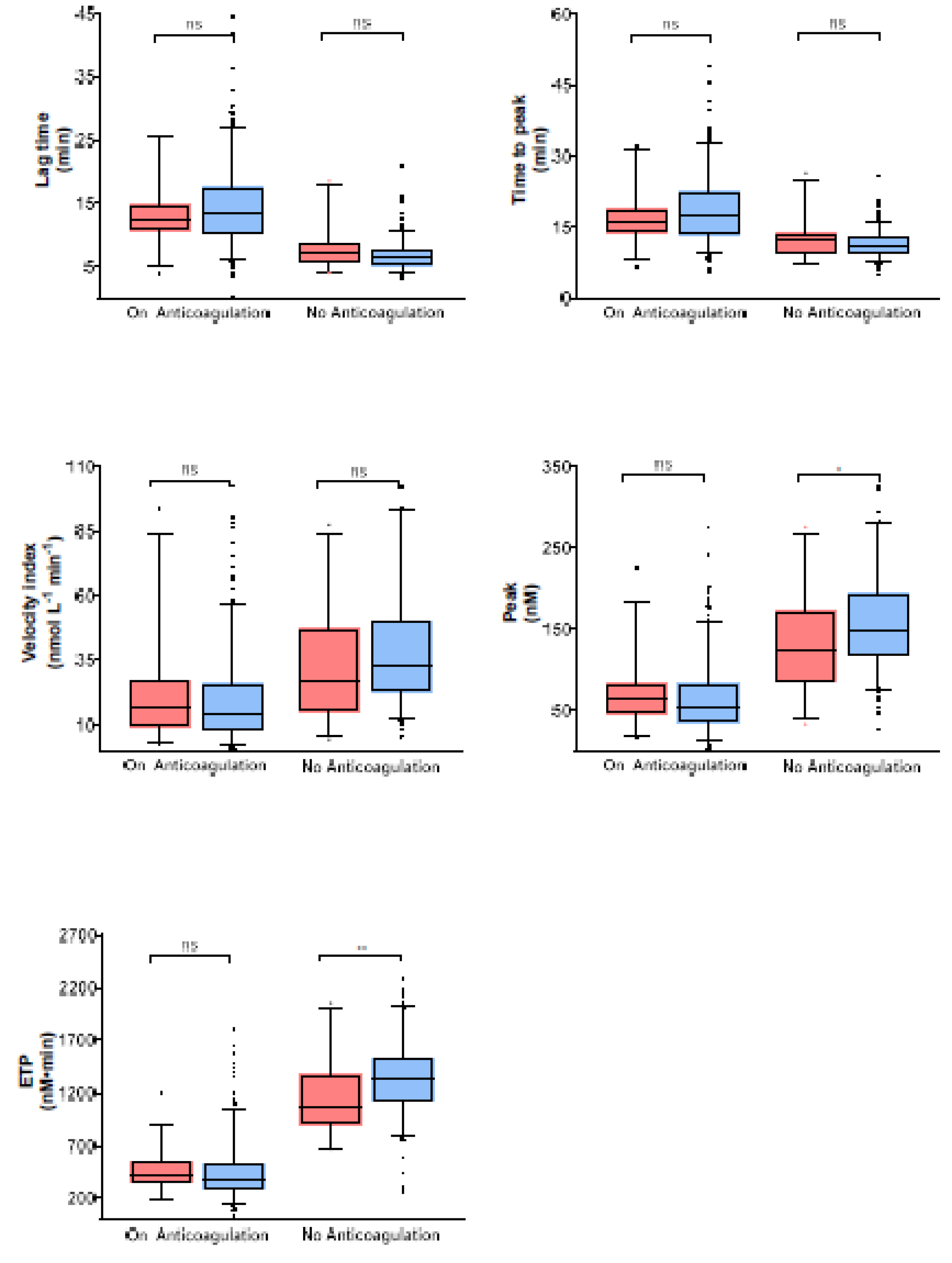

Table 1.
Patient characteristics by anticoagulation status one year after index venous thromboembolism (VTE).
Table 1.
Patient characteristics by anticoagulation status one year after index venous thromboembolism (VTE).
| Characteristic | Alln (%) or Median (IQ-Range) | Not under Anticoagulation One Year after Index VTE n (%) or Median (IQ-Range) |
Under Anticoagulation one Year after Index VTE n (%) or Median (IQ-Range) |
p-Value | |||
|---|---|---|---|---|---|---|---|
| Total number of patients | 565 | 232 | 333 | ||||
| Patient age (years) | 74.0 (69.0;79.0) | 74.0 (68.0;78.0) | 75.0 (69.0;80.0) | 0.262 | |||
| Female sex1 | 239 (42) | 107 (46) | 132 (40) | 0.141 | |||
| Patient race | |||||||
| Caucasian | 564 (100) | 231 (100) | 333 (100) | ||||
| African | 1 (0) | 1 (0) | 0 (0) | ||||
| Index VTE event | <0.001 | ||||||
| PE only | 317 (56) | 111 (48) | 206 (62) | ||||
| DVT only | 175 (31) | 98 (42) | 77 (23) | ||||
| PE and DVT | 73 (13) | 23 (10) | 50 (15) | ||||
| Index DVT type2 | <0.001 | ||||||
| proximal DVT only | 101 (18) | 47 (20) | 54 (16) | ||||
| distal DVT only | 58 (10) | 42 (18) | 16 (5) | ||||
| proximal and distal DVT | 89 (16) | 32 (14) | 57 (17) | ||||
| Type of index VTE | <0.001 | ||||||
| cancer-related VTE | 64 (11) | 27 (12) | 37 (11) | ||||
| provoked index VTE | 114 (20) | 69 (30) | 45 (14) | ||||
| unprovoked index VTE | 387 (68) | 136 (59) | 251 (75) | ||||
| Current oestrogen therapy during the last 3 months | 19 (3) | 9 (4) | 10 (3) | 0.638 | |||
| Immobilization during the last 3 months | 96 (17) | 60 (26) | 36 (11) | <0.001 | |||
| Major surgery during the last 3 months | 81 (14) | 53 (23) | 28 (8) | <0.001 | |||
| Prior VTE | 172 (30) | 29 (13) | 143 (43) | <0.001 | |||
| PTS2 | 295 (52) | 123 (53) | 172 (52) | 0.665 | |||
| History of major bleeding2 | 44 (8) | 18 (8) | 26 (8) | 1.000 | |||
| Chronic liver disease | 8 (1) | 4 (2) | 4 (1) | 0.722 | |||
| Chronic renal disease | 101 (18) | 34 (15) | 67 (20) | 0.118 | |||
| Chronic or acute heart failure | 67 (12) | 17 (7) | 50 (15) | 0.005 | |||
| Anemia2 | 189 (33) | 88 (38) | 101 (30) | 0.020 | |||
| Concomitant antiplatelet therapy | 177 (31) | 66 (28) | 111 (33) | 0.232 | |||
| Concomitant antiplatelet/NSAID therapy | 207 (37) | 77 (33) | 130 (39) | 0.183 | |||
| Heart rate of ≥ 110 beats min-1 2 | 47 (8) | 15 (6) | 32 (10) | 0.218 | |||
| Systolic BP of < 100 mmHg2 | 12 (2) | 3 (1) | 9 (3) | 0.376 | |||
| Arterial oxygen saturation of < 90%2 | 54 (10) | 16 (7) | 38 (11) | 0.233 | |||
| D-dimer at the time of the index VTE2 | 2482 (1599;3757) | 2407 (1687;3758) | 2513 (1554;3757) | 0.967 | |||
| D-dimer 1 year after the index VTE2 | 630 (393;1125) | 945 (567;1537) | 503 (327;807) | <0.001 | |||
| Overall anticoagulation duration (days) | 645 (213;976) | 192 (145;281) | 900 (709;1210) | <0.001 | |||
| Anticoagulation duration until 1 year after the index VTE (days) | 354 (194;365) | 186 (121;212) | 363 (357;371) | <0.001 | |||
| Anticoagulation duration from 1 year after the index VTE (days) | 338 (0;686) | 0 (0;0) | 535 (351; 865) | <0.001 | |||
Abbreviations: BP, blood pressure; BMI, body mass index; DVT, deep vein thrombosis; IQR, interquartile range; NSAID, mon-steroidal anti-inflammatory drug; PE, pulmonary embolism; PTS, post-thrombotic syndrome. 1Assigned at birth; 2values were missing for presence of PTS (2%), anemia (7%), heart rate of ≥ 110 beats min-1 (3%), systolic BP of < 100 mmHg (2%), arterial oxygen saturation of < 90% (23%), D-dimer at the time of the index VTE (8%), D-dimer 12 months after the index VTE (1%).
Table 2.
Incidence rate of VTE recurrence, major bleeding, or overall mortality per 100 person-years - from 12 months until 36 months after index venous thromboembolism (VTE) in non-anticoagulated patients. This is a table. Tables should be placed in the main text near to the first time they are cited.
Table 2.
Incidence rate of VTE recurrence, major bleeding, or overall mortality per 100 person-years - from 12 months until 36 months after index venous thromboembolism (VTE) in non-anticoagulated patients. This is a table. Tables should be placed in the main text near to the first time they are cited.
| No of Patients | No of Events/Person-Years | Incidence Rate (95%-CI) | ||
|---|---|---|---|---|
| Peak ratio obtained in presence/absence of TM | ||||
| VTE recurrence | ||||
| All | 222 | 32 / 322.3 | 9.9 (7.0 to 14.0) | |
| ≤ median | 111 | 12 / 172.0 | 7.0 (4.0 to 12.3) | |
| > median | 111 | 20 / 150.3 | 13.3 (8.6 to 20.6) | |
| Major bleeding | ||||
| All | 222 | 11 / 342.2 | 3.2 (1.8 to 5.8) | |
| ≤ median | 111 | 2 / 182.0 | 1.1 (0.3 to 4.4) | |
| > median | 111 | 9 / 160.3 | 5.6 (2.9 to 10.8) | |
| Overall mortality | ||||
| All | 222 | 13 / 348.5 | 3.7 (2.2 to 6.4) | |
| ≤ median | 111 | 4 / 182.8 | 2.2 (0.8 to 5.8) | |
| > median | 111 | 9 / 165.8 | 5.4 (2.8 to 10.4) | |
| Normalized peak ratio in presence/absence of TM | ||||
| VTE recurrence | ||||
| All | 122 | 17 / 156.1 | 10.9 (6.8 to 17.5) | |
| ≤ median | 61 | 4 / 89.1 | 4.5 (1.7 to 12.0) | |
| > median | 61 | 13 / 67.0 | 19.4 (11.3 to 33.4) | |
| Major bleeding | ||||
| All | 122 | 3 / 165.6 | 1.8 (0.6 to 5.6) | |
| ≤ median | 61 | 0 / 91.2 | 0.0 (-) | |
| > median | 61 | 3 / 74.4 | 4.0 (1.3 to 12.5) | |
| Overall mortality | ||||
| All | 122 | 4 / 167.0 | 2.4 (0.9 to 6.4) | |
| ≤ median | 61 | 1 / 91.2 | 1.1 (0.2 to 7.8) | |
| > median | 61 | 3 / 75.8 | 4.0 (1.3 to 12.3) | |
| ETP ratio obtained in presence/absence of TM | ||||
| VTE recurrence | ||||
| All | 221 | 31 / 321.5 | 9.6 (6.8 to 13.7) | |
| ≤ median | 111 | 12 / 174.5 | 6.9 (3.9 to 12.1) | |
| > median | 110 | 19 / 147.0 | 12.9 (8.2 to 20.3) | |
| Major bleeding | ||||
| All | 221 | 11 / 340.2 | 3.2 (1.8 to 5.8) | |
| ≤ median | 111 | 4 / 182.9 | 2.2 (0.8 to 5.8) | |
| > median | 110 | 7 / 157.4 | 4.4 (2.1 to 9.3) | |
| Overall mortality | ||||
| All | 221 | 3.8 (2.2 to 6.5) | ||
| ≤ median | 111 | 2.7 (1.1 to 6.5) | ||
| > median | 110 | 8 / 161.0 | 5.0 (2.5 to 9.9) | |
| Normalized ETP ratio obtained in presence/absence of TM | ||||
| VTE recurrence | ||||
| All | 122 | 17 / 156.1 | 10.9 (6.8 to 17.5) | |
| ≤ median | 61 | 6 / 84.9 | 7.1 (3.2 to 15.7) | |
| > median | 61 | 11 / 71.2 | 15.5 (8.6 to 27.9) | |
| Major bleeding | ||||
| All | 122 | 3 / 165.6 | 1.8 (0.6 to 5.6) | |
| ≤ median | 61 | 1 / 87.8 | 1.1 (0.2 to 8.1) | |
| > median | 61 | 2 / 77.8 | 2.6 (0.6 to 10.3) | |
| Overall mortality | ||||
| All | 122 | 4 / 167.0 | 2.4 (0.9 to 6.4) | |
| ≤ median | 61 | 2 / 87.8 | 2.3 (0.6 to 9.1) | |
| > median | 61 | 2 / 79.1 | 2.5 (0.6 to 10.1) |
Table 3.
Discriminative power of thrombin generation parameters involving thrombomodulin (TM) for outcomes – from 1 year to 3 years following the index VTE in not anticoagulated patients This is a table. Tables should be placed in the main text near to the first time they are cited.
Table 3.
Discriminative power of thrombin generation parameters involving thrombomodulin (TM) for outcomes – from 1 year to 3 years following the index VTE in not anticoagulated patients This is a table. Tables should be placed in the main text near to the first time they are cited.
| Thrombin Generation Parameters Measured one Year after the Index VTE | No. of Events/no. of Patients |
C-Statistics (95% Confidence Interval) |
|---|---|---|
|
Peak ratio obtained in presence/absence of TM VTE recurrence Major bleeding Overall mortality |
32/222 11/222 13/222 |
0.60 (0.51 to 0.69) 0.65 (0.50 to 0.80) 0.59 (0.45 to 0.73) |
|
Normalized peak ratio obtained in presence/absence of TM VTE recurrence Major bleeding Overall mortality |
17/122 3/122 4/122 |
0.70 (0.59 to 0.81) 0.65 (0.55 to 0.75) 0.63 (0.36 to 0.89) |
|
ETP ratio obtained in presence/absence of TM VTE recurrence Major bleeding Overall mortality |
31/221 11/221 13/221 |
0.59 (0.50 to 0.69) 0.63 (0.48 to 0.77) 0.44 (0.32 to 0.56) |
|
Normalized ETP ratio obtained in presence/absence of TM VTE recurrence Major bleeding Overall mortality |
17/122 3/122 4/122 |
0.70 (0.60 to 0.80) 0.48 (0.37 to 0.58) 0.66 (0.46 to 0.87) |
Table 4.
Association between thrombin generation parameters and venous thromboembolism (VTE) recurrence, major bleeding and overall mortality – from 1 year to 3 years following the index VTE in not anticoagulated patientsThis is a table. Tables should be placed in the main text near to the first time they are cited.
Table 4.
Association between thrombin generation parameters and venous thromboembolism (VTE) recurrence, major bleeding and overall mortality – from 1 year to 3 years following the index VTE in not anticoagulated patientsThis is a table. Tables should be placed in the main text near to the first time they are cited.
| n/N (%) | Crude Subhazard Ratio (95% Confidence Interval) |
Adjusted Subhazard Ratio (95% Confidence Interval) |
|||
|---|---|---|---|---|---|
| Peak ratio obtained in presence/absence of TM | |||||
| VTE recurrence | 32/222 (14.4) | 3.94 (1.00 to 15.49) | 4.09 (1.12 to 14.92) | ||
| Major bleeding | 11/222 (5.0) | 5.01 (0.67 to 37.24) | 5.65 (0.83 to 38.71) | ||
| Overall mortality | 13/222 (5.9) | 1.89 (0.33 to 10.75) | 2.93 (0.39 to 21.71) | ||
| Normalized peak ratio obtained in presence/absence of TM | |||||
| VTE recurrence | 17/122 (13.9) | 2.21 (1.30 to 3.77) | 2.18 (1.28 to 3.73) | ||
| Major bleeding | 3/122 (2.5) | 1.35 (0.84 to 2.18) | - | ||
| Overall mortality | 4/122 (3.3) | 1.36 (0.50 to 3.67) | - | ||
| ETP ratio obtained in presence/absence of TM | |||||
| VTE recurrence | 31/221 (14.0) | 3.10 (0.86 to 11.24) | 2.88 (0.82 to 10.09) | ||
| Major bleeding | 11/221 (5.0) | 3.38 (0.40 to 28.79) | 3.02 (0.38 to 23.97) | ||
| Overall mortality | 13/221 (5.9) | 0.80 (0.16 to 3.97) | 0.80 (0.10 to 6.55) | ||
| Normalized ETP ratio obtained in presence/absence of APC | |||||
| VTE recurrence | 17/122 (13.9) | 1.82 (1.01 to 3.29) | 1.80 (0.99 to 3.27) | ||
| Major bleeding | 3/122 (2.5) | 0.81 (0.54 to 1.23) | - | ||
| Overall mortality | 4/122 (3.3) | 1.58 (0.71 to 3.50) | - | ||
Abbreviations: APC, activated protein C; ETP, endogenous thrombin potential; TM, thrombomodulin. Adjustments: VTE recurrence was adjusted for age, cancer, provoked VTE, prior VTE, overt pulmonary embolism, renal disease and periods of anticoagulation (oral or parenteral anticoagulation) as a time-varying covariable [42,43,44,45,46,47,48,49,50,51]. Major bleeding was adjusted for age, cancer, provoked VTE, prior VTE, overt pulmonary embolism, renal disease, history of major bleeding, anemia, antiplatelet therapy and periods of anticoagulation as time-varying covariate [53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68]. Mortality was adjusted for age, gender, cancer, provoked VTE, prior VTE, overt pulmonary embolism, renal disease, history of major bleeding, heart failure, chronic lung disease, high pulse, low blood pressure, low oxygen, and periods of anticoagulation as a time-varying covariate [48,52].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



