
Submitted:
20 July 2023
Posted:
24 July 2023
You are already at the latest version
Abstract
Congenital diseases of the large intestine have scarcely been reported and mostly include fistula, atresia, or colonic duplication. Cases of partial colonic agenesis have rarely been described. The purpose of this study was to report a cohort of dogs and cats diagnosed with partial colonic agenesis. The colon was measured during colonoscopy or contrast-radiography and compared to the average length described in the literature. Six dogs and 17 cats were retrospectively included. Depending on the case, partial colonic agenesis could represent an incidental finding or the likeliest cause of clinical signs. Diarrhea was reported in most cases, and no specific clinical or biological abnormality was observed. Median age of presentation was variable and long asymptomatic periods were common. Abdominal ultrasound was useful and identified a short colon in 14/17 cats but only in one dog. Endoscopy was useful to confirm the diagnosis and to identify associated lesions and complications. Among others, colonic stenosis was reported in 8/9 cases that had lifelong clinical signs and the shortest colon length. This anatomical abnormality could promote chronic inflammation that might generate fibrosis and ultimately stenosis.
Keywords:
Congenital
; Colonic Agenesis
; Stenosis
; Canine
; Feline
1. Introduction
The colon is the terminal part of the digestive tract; it begins at the ileocolic sphincter and ends at the rectum. It is composed of the ascending, transverse and descending parts, demarcated by connecting flexures [1]. Its main roles are absorption and secretion of water and electrolytes, storage of feces, immune surveillance, and it is the site of microbial fermentation [2]. Colonic diseases are relatively frequent disorders in dogs and cats. In young animals, the main etiologies are infectious (parasites), alimentary (food intolerance, fiber responsive colopathy) or breed-related (granulomatous colitis). Congenital colopathies are rare and mostly include fistula [3,4], atresia [5] or colon duplication [6]. The normal length of the colon varies between 60 to 75 cm in dogs (ranges 25-90) [7,8] and is approximately 30 cm in healthy cats (27-37 cm) [9]. It may depend on the size of the animal and is usually considered to contribute to 20-25% of the total intestinal length [1,2,9]. Very few data about congenital partial colonic agenesis exist in the literature. Previous studies have described isolated case reports of short colon in a foal [10] and in few dogs and cats [11,12].
The objective of this study was to retrospectively describe a population of dogs and cats diagnosed with congenital partial colonic agenesis.
2. Materials and Methods
Medical records of all cats and dogs diagnosed with partial colonic agenesis between January 2016 and May 2022 at the Veterinary Teaching Hospital of Alfort, Paris, France, were retrospectively searched from the database. Inclusion criteria was presence of a short colon diagnosed using contrast radiography, ultrasonography, endoscopy, or a combination of these modalities.
Partial colonic agenesis was defined as a colon length below 20 cm for cats, measured during colonoscopy or on positive contrast abdominal radiographs. In dogs, there is an extreme variability in body weight and size that affects the colon length with values ranging from 30 cm in dogs weighing 5 kg to 99 cm in dogs weighing 60 kg [13,14]. As such, a threshold of 25 cm was defined for smaller dogs (between 8 and 14 kg, 2 cases) and 45 cm for larger dogs (between 15 and 30 kg, 3 cases). We did not record dogs heavier than 30 kg in this study. Two cases with an extremely short colon on abdominal ultrasound did not have endoscopy performed yet were also included (one cat and one dog). Information was collected regarding signalment, clinical signs, age at presentation, clinical signs duration, diagnostic tests, treatments, and outcome. Hematologic data (scil Vet abc, IDEXX ProCyte Dx), serum biochemical analysis (Scil VetScan, IDEXX catalyst), electrolytes, B9 and B12 vitamin profile and stool analysis from patients at presentation or at the referring veterinarian were assessed. Abdominal ultrasonography, abdominal radiographs and endoscopic images were reviewed. Abdominal ultrasonography was performed with an Affinity 70, Phillips Medical System, using both microconvex and linear probes. Normal ranges for ultrasonographic measures were defined according to the current literature [15,16,17] ; among others, colonic wall was considered thickened above 1.5 mm for dogs and cats and lymph nodes were considered enlarged over 5 mm for dogs and 4 mm for cats. Subjective assessment based on lymph nodes echogenicity and shape was also taken into consideration for equivocal cases. Endoscopic evaluation was performed with an Olympus Evis Exera III Gif-h190 gastrointestinal videoscope and according to the WSAVA endoscopic recommendations [18]. At least 6 colonic biopsies were performed. Histological specimen were also evaluated according to the WSAVA criteria [18]. Medical treatment and outcomes were compared when available. The ratio between the duration of clinical signs (in months) and the age (in months) was calculated. A ratio over 0.75 was considered consistent with clinical signs lasting since the adoption (referred thereafter as group A), whereas a ratio below 0.5 was considered to represent emerging clinical signs (referred thereafter as group B). Cases for which no primary colonic lesion but the partial colonic agenesis was detected were described together as subgroup C (see below).
Data were expressed by standard descriptive statistics and presented as mean or median and range (minimum-maximum). The student’s t-test was used to compare age between group A and B. Categorial variables were compared among groups using the chi-squared test. Each of which initially included variables that were significant at P < .05 in simple logistic regression. Statistical analyses were performed using available statistical software (BiostatGV).
3. Results
3.1. Epidemiological and Clinical Data
A total of 23 cases, 17 cats and 6 dogs, were included in the study. Among the cats, there were 7 females and 10 males and among the dogs, there were 4 females and 2 males. Males and females comprised 12 and 11 of the 23 cases, respectively, and no sex predilection was identified. Two French bulldogs and two boxers were present among the 6 dogs. The other breeds were one border collie and one whippet. Domestic short hair (DSH) was the most common breed in cats (5/17). Most cats were purebred and included Bengals (3/17) and one of each breed: Siberian, Savanah, exotic shorthair, Persian, Birman, Scottish, Burmese, Abyssinian and Chartreux.

Table 1.
Cases included and epidemiological data.
| Number | Species | Breed | Age (months) | Sexes | Weight (kg) |
|---|---|---|---|---|---|
| 1 | Cat | Bengal | 16 | Female | 2.26 |
| 2 | Cat | Savannah | 13 | Female | 2.3 |
| 3 | Cat | Exotic Shorthair | 48 | Male | 3.2 |
| 4 | Cat | DSH | 160 | Male | 4.2 |
| 5 | Cat | Bengal | 120 | Male | 3.6 |
| 6 | Cat | DSH | 11 | Male | 2.2 |
| 7 | Cat | Persian | 120 | Male | 4.3 |
| 8 | Cat | DSH | 12 | Male | 2.7 |
| 9 | Cat | DSH | 130 | Male | 5.1 |
| 10 | Cat | Siberian | 12 | Male | 3.7 |
| 11 | Cat | Scottish | 6.5 | Male | 2.3 |
| 12 | Cat | Chartreux | 192 | Male | 6.3 |
| 13 | Cat | Birman | 96 | Female | 2.25 |
| 14 | Cat | Burmese | 156 | Female | 1.9 |
| 15 | Cat | Abyssinian | 81 | Female | 3.6 |
| 16 | Cat | DSH | 103 | Female | 3.3 |
| 17 | Cat | Bengal | 18 | Female | 2.6 |
| 18 | Dog | Colley | 96 | Male | 26.5 |
| 19 | Dog | Boxer | 4 | Female | 15 |
| 20 | Dog | French Bulldog | 16 | Female | 9.7 |
| 21 | Dog | Whippet | 108 | Male | 10.8 |
| 22 | Dog | French bulldog | 60 | Female | 8.5 |
| 23 | Dog | Boxer | 52 | Female | 30.5 |
The median age was 81 months/6.7 years in cats and 56 months/4.7 years in dogs. The age distribution was bimodal: one group with clinical signs lasting since the adoption (group A) and one group with a progressive or acute onset during adulthood (group B). In group A, the mean age at presentation was 48.8 months/4 years with a median of 17 months/1.4 years and a range of [4–160] months. This group included 11/17 cats and 1/6 dogs. In group B, the mean age was 95 months/7.9 years with a median of 103 months (range, [12–192] months). Mean and median duration of clinical signs in this group were 14.5 months and 12 months (range, [4–48] months), respectively. This group included 5/6 dogs and 6/17 cats. Age was not significantly different between group A and B (Figure 1) (Student’s t test).
The most common clinical signs were diarrhea (21 of 23 cases/91.3%) and weight loss/failure to grow (11 of 23 cases/47.8%). Table 2 summarizes the clinical signs. Table 3 and Table 4 summarize the clinical signs in groups A and B. All clinical signs were present in both groups except for dysorexia or polyphagia, which were only found in group B. Mucoid stools and dyschezia were more common in group A (both clinical signs had a prevalence of 41% and 9% in group A and B, respectively).
On physical examination, a low body condition score was the most common abnormality. It was slightly low (BCS of 3/9) in 7 of 23 cases (30%) and markedly low in 2 cases (BCS of 2/9, 8.7%). It was normal in 12 of 23 cases (52.2%, BCS 4-5/9) and increased in 2 (8.8%, BCS 6-7/9). Thickened intestinal loops were noticed on abdominal palpation in 3 of 23 cases and one case had a painful abdominal palpation. One case was presented with lethargy, hyperthermia and dehydration. In most cases, the physical examination was unremarkable (17 of 23 cases, 73.9%).
3.2. Diagnostic Tests
3.2.1. Biological
Cell blood count was performed in 21 of 23 cases and revealed slight anemia (PCV 26%) in 3 cases; neutrophilic leucocytosis in two cases; mild eosinophilia in 5 cases, monocytosis in 4 cases, basophilia in one case and lymphocytosis in one case.
Biochemistry was performed in 20 of 23 cases and revealed slight hyperuremia in one case (0.88 g/L; reference range [0.4-0.8] g/L); increased ALT in one dog (700 U/L; reference range [15–123] U/L); increased ALP in one dog (410 U/L; reference range [22–187] U/L); increased AST in one cat (62 U/L; reference range [0–45] U/L); decreased albumin in 3 cases (18-25 g/L; reference range [26–35] g/L); hypoglobulinemia in one case and hyperglobulinemia in two cases.
Electrolytes were measures in 16 cases. It revealed hyponatremia (135 mmol/L; reference range [150–165] mmol/L) in one of 16 cases and hypokalaemia (3.2-3.4 mmol/L; reference range [3.6-5.5] mmol/L) in two of 16 cases.
The TLI were measured in 8 cases and was normal in all but one cat.
Cobalaminemia was measured in 18 cases. It was decreased in 3 cases and increased in 8 cases. Folic acids were measured in 7 cases, increased in 4 and decreased in 1 case.
Fecal analysis was negative in all cases where it was tested but with positive tritrichomonas PCR in one case.
In group A, hypercobalaminemia was present in 5 of 10 cases; hyperfolatemia was present in 2 of 5 cases; hypocobalaminemia in 1 of 10 cases, hypofolatemia in 1 of 5 cases and hyperglobulinemia in one of 10 cases. The 5 cases with eosinophilia were all in group A.
An additional diagnosis other than partial colonic agenesis was established in all cases in group B (see below) and biological abnormalities in this group were most likely associated with the identified comorbidity.
3.2.2. Abdominal Ultrasound
Abdominal ultrasound was performed in 22 cases. Peritoneal effusion was present in 7 of 22 cases and was associated with hypoalbuminemia in one case. A partial colonic agenesis was suspected on abdominal ultrasound in 15 cases (14 cats and 1 dog).
Colonic wall thickness was increased in 17 of 22 cases. In group A, it was increased in 9 of 11 cases. In group B, it was increased in 8 of 11 cases. It was focal in 4 cases and diffuse in 13 cases. Table 5 summarizes the subjective severity of colonic wall thickening and its distribution depending on groups. Loss of colonic wall layering was observed in 4 cases.
The ileocolic junction was visualized in 20/22 cases and did not show any abnormality. One case (canine) had a thickened cecal wall.
Ileocolic or colic lymphadenomegaly was seen in 14 cases (7 in group A and 7 in group B).
Other ultrasound abnormalities included gall bladder wall thickening (3 cases), hypoechogenic liver (3 cases), gastric wall thickening (2 cases) and small intestinal wall thickening (8 cases). These other abdominal ultrasound abnormalities were more common in group B (12/16 in group B).
3.2.3. Abdominal Radiographs
Abdominal radiographs were acquired in 5 cases (4 cats and one dog). In two cats, the descending colon showed an abrupt ending with a total length approximately half as long as expected. No ascending nor transverse colon could be identified in these 2 cases (Figure 2). In the dog, the cecum appeared mispositioned in the left cranial abdominal quadrant and seemed associated with a focal area of colonic lumen narrowing 22 cm orally to the anus (Figure 3). Positive contrast colonography were performed in 3 cases (three cats) and allowed the diagnosis of partial colonic agenesis in all of them (Figure 4).
3.2.4. Endoscopic Findings
Colonic length was available in 19 cases. In cats, colonic length ranged from 8 to 20 cm with a median of 18 cm. Four cats had a marked colon shortening with lengths ranging from 8 to 12 cm whereas 10 had only mild partial shortening with values ranging from 18 to 20 cm. In dogs of 10 kg or less (2 cases), colonic length ranged from 22 to 23 cm. In dogs over 15 kg (3 cases), it ranged from 40 to 45 cm.
Endoscopic abnormalities are presented in Table 6 and included: gaping, atone and opened ileocolic junction in 8 cases (4 in group A and 4 in group B, Figure 5), absence of cecum in one case, colonic stenosis of variable degree in 12 cases (2 in group B and 10 in group A, Figure 6), erosive or marked macroscopic signs of colopathy in 5 cases (5 in group B and 3 in group A), non-specific slight to moderate signs of colopathy in 8 cases (3 in group B and 5 in group A) and unremarkable colon in two cases (one in group A and B).
3.2.5. Histology
Histology was available in 20 cases (Table 7). It revealed a lymphoplasmacytic infiltrate in 19 cases, mild to moderate in 16 cases (6 in group A and 10 in group B) and marked in 3 cases (2 in group A and one in group B). A neutrophilic infiltrate was present in 9 cases (5 in group A and 4 in group B); erosion or ulcers were found in 6 cases (3 in group A and 3 in group B) and fibrosis was seen in 6 cases (4 in group A and 2 in group B). Two cases showed a significant eosinophilic infiltrate (group B).
3.2.6. Diagnosis
A concurrent diagnosis was established in all the cases in group B and comprised 1 low grade intestinal T-cell lymphoma in a cat (LGITL), 1 protein-losing-enteropathy in a dog (PLE), and 4 granulomatous colitis. In the 5 remaining cases, a non-specific, mild to moderate lymphoplasmacytic infiltrate was present and was considered secondary to an inflammatory bowel disease (IBD) based on an exclusion diet.
One dog in group A had a diagnosis of granulomatous colitis, 1 cat had trichomoniasis and 1 cat had a granulomatous infiltrate with high suspicion of feline infectious peritonitis.
Seven other cases had a lymphoplasmacytic infiltrate of variable severity associated with fibrosis in 4/7 cases, neutrophilic infiltrate in 5/7 cases, mucosal erosion or ulcers in 3/7 cases and necrosis in 3/7 cases. In these 7 cases, no other diagnosis was found and since the clinical signs lasted since adoption, they were categorized as “sub group C” (Figure 7). All were cats and all but one developed a stenosis.
The last 2 cases were cats that did not have histological analysis performed due to owner’s decline and could not be assigned to a specific diagnosis group. However, they had lifelong clinical signs, marked shortening of the colon with stenosis and they both improved with lactulose and hyper digestible diet or interventional treatment (colonic stenting) without relapse. Hence, the clinical signs were attributed to the stenosis and the partial colonic agenesis, and these cats were also included in the subgroup C.
Cats of this sub-group had a significantly shorter colon than the other cats (p = 0.04, Student test, median length 13 cm vs 18 cm, range [8–20]cm vs [15–20]cm).
3.2.7. Management and Outcome
Treatment was based on the different lesions previously listed or on the nature of the mucosal infiltrate. The data are presented in Table 8.
Diet change and symptomatic treatments led in all cases to no or only slight and transient improvement.
Stenosis was managed by partial colectomy (two cases), bougienage (two cases) or endoluminal stenting (one case). Neutrophilic or ulcerative/erosive cases were managed by antibiotics (amoxicillin/clavulanic acid in two cases, metronidazole in 6 cases, marbofloxacin in 2 cases, enrofloxacin in 2 cases, and tylosin in 1 case). Antibiotics were also used in a case of cholecystitis and suspected acquired dysbiosis.
Prednisolone was prescribed in cases of lymphoplasmacytic infiltrate and ranged from 0.5 mg/kg/d to 2 mg/kg/day. Budesonide was used in one case. Other treatment included chlorambucil (one case), ciclosporin (one case) and were all in group B, depending on additional diagnosis.
Six cases were lost to follow-ups. Three cases were included during the redaction of the manuscript and had no follow-up data. Two cases died of unrelated causes and one died because of persistent marked diarrhea and hypovolemic shock. One case relapsed after 6 months of normal stools and was diagnosed with colonic adenocarcinoma (ADK). In the remaining cases, the 4 cases with suspected granulomatous colitis on histology improved with fluoroquinolone antibiotherapy. Two cases with a diagnosis of IBD and PLE improved with immunosuppressive treatment and one case with LGITL improved with cytotoxic treatment.
In sub-group C (7 cases), 4 were lost to follow-ups, 2 did not have follow-up at the time of redaction yet, and 1 died of post-operative complications after a colectomy for colonic stenosis.
Two cases showed marked stenosis and had no histological analysis performed. One improved with endoluminal stent and prednisolone and the other one with lactulose, metronidazole and a hyper digestible diet.
One case underwent necropsy which confirmed partial colonic agenesis (Figure 8). No other malformation was found on the digestive tract.
4. Discussion
To the authors’ knowledge, this is the first study describing congenital partial colonic agenesis in a cohort of dogs and cats. In this study, there was no sex predisposition and too few cases to detect breed overrepresentation. However, cats included in the Group C were mostly purebreed cats.
In terms of frequency, clinical signs included diarrhea, hematochezia, weight loss or failure to thrive, vomiting, mucoid stools, dyschezia and dysorexia. No clinical signs nor specific associations of clinical signs were found to be specific in the diagnosis of a partial colonic agenesis. Likewise, CBC, biochemistry and electrolytes were non-specific. Mild anemia, monocytosis and mild neutrophilia were occasionally present and likely secondary to chronic inflammation. Five cases had mild eosinophilia that was not explained by parasitism or by an eosinophilic infiltrate in the colon. Biochemical abnormalities were seldom. Apart from 1 dog that had panhypoproteinemia due to PLE, all biochemical abnormalities remained mild and were considered non-specific (chronic inflammation, dehydration, suspected reactive hepatitis) in the context of gastro-intestinal disease. Cobalamin and folic acid abnormalities were variable and could not be predictive of a partial colonic agenesis or of any group. No association was found between hypocobalaminemia and ileocolic valve malformation. One cat had low TLI consistent with exocrine pancreatic insufficiency (EPI). In this case, EPI did not seem to explain the dyschezia [19], therefore motivating colonoscopy that led to the diagnosis of partial colonic agenesis.
Abdominal ultrasonography seems to be a useful tool in the diagnosis of partial colonic agenesis, leading to the diagnosis in 14 of 17 cats. However, diagnosis of partial colonic agenesis was more challenging in dogs because abdominal ultrasonography identified it in only 1 case, suggesting a lack of sensitivity of this modality for diagnosing this disease in dogs. This apparent discrepancy can be explained by the position of the ileocecocolic junction is an indicator of the colon size and that it can be challenging to localize in dogs. The ileocolic junction and the cecum are typically located to the right of the midline, along with the duodenum [20]. This localization might be modified in case of partial colonic agenesis. On canine abdominal ultrasound, the junction can be challenging to identify because the cecum is most commonly gas-filled. On the contrary, in cats, it can be more easily recognized [15]. Thus, an abnormal position of the ileocolic junction in association with a subjective short colon length might be more easily recognized in feline cases and increases the suspicion of partial colonic agenesis. Unfortunately, due to the retrospective nature of the study, the imaging criteria that led the radiologist to suspect a short colon were not available. Thickening of the colonic wall and local adenomegaly were seen in 17 and 14 cases of 22, respectively, but are unspecific findings in cases of colic diarrhea. Few cases had other abdominal ultrasound abnormalities outside of the colon or associated lymph nodes and were more common in group B (12/16 in group B). They may thus by secondary to a concomitant disease.
Abdominal radiography was performed in few cases and raised the suspicion of partial colonic agenesis in only half of them. This difference might be due to the difficulty in identifying the oral part of the colon on abdominal radiograph because its filling with air or stool is variable. Positive colonography has not been investigated extensively in this study. However, as the ileocolic junction was clearly identified in the 2 cases with colonography, it might be a useful and easily accessible tool to diagnose partial colonic agenesis in small animals.
Colonoscopy allowed the diagnosis in most cases. Partial colonic agenesis was associated with other anatomical malformation in 8 cases and included absence of the cecum or abnormal ileocolic junction (Image 3). Focal stenosis was also identified in 12 cases. Marked macroscopic signs of active colonic disease were identified in 5 cases and corresponded to a diagnosis of granulomatous inflammation or IBD. In most cases however, the colic mucosa was macroscopically normal or only slightly modified, especially in group A.
Two different subtypes of presentation were identified in this study: 1 with clinical signs that lasted since a young age or adoption, and 1 with clinical signs that developed during adulthood. In cases where clinical signs developed in adult individuals, a concomitant affection was present in all cases and included IBD, PLE, LGITL, and granulomatous colitis. It is likely that these diseases were responsible for the clinical signs and that the partial colonic agenesis was an incidental finding. However, it might also have been a predisposing factor to the development of these diseases. Indeed, in these 11 cases, an infectious origin was suspected or confirmed in 4 cases (granulomatous infiltrate). A partial colonic agenesis might then have increased to sensitivity of the colon to infectious agent.
In cases where clinical signs started young or at adoption, an infectious agent was found in 3 cases and included 1 trichomonosis and 2 granulomatous infiltrates. In the 9 remaining cases (subgroup C), 7 were submitted to a histologic analysis that showed variable degree of lymphoplasmacytic inflammation. Eight out of these 9 cases developed a colic stenosis. This complication has previously been described in 1 case report of short colon [12]. In this case, the cat had chronic and progressive signs of diarrhea and developed dyschezia. Colonoscopy identified stenosis with mild to moderate lymphoplasmacytic infiltration and fibrosis, as well as absence of an ileocolic papilla. It is then possible that, in these individuals, partial colonic agenesis might have led to a persistent colic inflammation which predisposed to secondary fibrosis and stenosis. In dogs and cats, rectal strictures can indeed be secondary to diarrhea and the associated colonic inflammation [21] and in humans, stenosis is a well-known complications of Crohn’s disease with fibrosis and inflammation involved in the pathogenesis [22]. Furthermore, in the subgroup C, the length of the colon was significantly shorter than in the other cats of the cohort. However, overlap exists, and it remains unclear why some individuals might develop severe clinical signs whereas some remained free of clinical signs for several years. In cats and dogs who underwent small intestinal resection, secondary morphological modifications allow an increase of the villous mucosal surface area following the length reduction [23,24]. It seems to be also the case when the resection affects the colon with an adaptative response and villi elongation in the small intestine after sub-total colectomy in dogs [25]. In all our cases with clinical signs since adoption (with the exclusion of infectious cases) the histological analysis revealed only mild to moderate lymphoplasmacytic infiltration. It is then possible that a histological compensatory adaptation was lacking in this group and could explain the early presentation. Comparison with asymptomatic cases of partial colonic agenesis would be required to answer this question.
The outcomes were highly variable in our cases. Because many of them were lost to follow-up, it is difficult to draw conclusions on the potential benefits of the treatments initiated (Table 8). However, in some cases, management of the clinical signs seemed to be more difficult than in animals exhibiting a colopathy without partial colonic agenesis.
Partial colonic agenesis might be part of a wider syndrome of short bowel. Indeed, congenital short bowel is described [26] and was associated with marked weight loss and intermittent diarrhea. In our study, the small intestinal length could not be evaluated. However, weight loss, when present, was usually mild as most BCS were higher than 3/9. Furthermore, 1 case underwent necropsy that did not show any small intestinal shortening.
Congenital partial colonic agenesis is described in humans. It is a rare condition, more common in males and in which the colon is partially or completely replaced by a dilated pouch. It is however often associated with anorectal malformations [27] and usually terminates in a fistulous communication with the genitourinary tract [28].
This study has some limitation. Firstly, a precise reference range of the normal colonic length according to the animal weight is lacking in the literature. It may vary according to the animal’s size and may differ if the measure has been performed on dead or alive individuals. Secondly, because of its retrospective nature, diagnostic criteria were not standardised and varied. Many of our cases were lost to follow-up and treatment efficiency could not be assessed precisely. Reviewing the abdominal ultrasounds was retrospectively performed on fixed images which might have troubled the identification of abnormalities. In addition, at the time of presentation, no specific attention was focused on the research of a shorten colon and subtle indicator might thus have been missed. Finally, Fluorescence in situ Hybridation (FISH) analysis could have been done to exclude invasive bacteria within the colonic mucosa.
5. Conclusions
In conclusion, partial colonic agenesis is a congenital abnormality that is occasionally seen in dogs and cats with diarrhea. The age at presentation varies widely, and animals can remain asymptomatic during extended periods of time. Abdominal ultrasonography seems to be a more useful modality to identify this abnormality in cats than in dogs. Colonoscopy is needed to confirm the diagnosis, precisely perform colonic measurement, identify other abnormalities, and perform biopsy sampling required for histopathology. Congenital colonic agenesis might predispose animals to a self-perpetuating inflammation that could ultimately lead to fibrosis and stenosis. After exclusion of the alimentary and infectious causes, early colonoscopy or contrast radiography might be indicated to exclude this disease in young animals with persistent diarrhea. Partial colonic agenesis should be included in the differentials in any dog and cat presenting clinical signs of colonic disease.
Author Contributions
Conceptualization, R.P. and F.V.; imaging reviewing G.L. and M.J.; writing—original draft preparation, R.P.; writing—review and editing, G.L., M.J. and F.V.; supervision, F.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to its retrospective nature.
Informed Consent Statement
Not applicable.
Acknowledgement
The authors would like to thank the Anatomic Pathology and Surgery services for their contribution in the diagnosis and management of many included cases.
Conflicts of Interest
The authors declare no conflict of interest.
References
- John Hermanson, Alexander de Lahunta. Miller’s Anatomy of the Dog - 5th Edition. Elsevier., https://www.elsevier.com/books/millers-anatomy-of-the-dog/hermanson/978-0-323-54601-0 (2018, accessed 1 March 2022).
- Washabau R. Large Intestine. Canine and Feline Gastroenterology 2013; 729–777. [CrossRef]
- Fruehwald C, Ellison G. Successful Surgical Correction of Congenital Colonic Duplication and Anogenital Cleft in a Cat. J Am Anim Hosp Assoc 2020; 56: 170–174. [CrossRef]
- Lecoindre A, Saade D, Barthez P, et al. Congenital duodenocolic fistula in a dog. J Small Anim Pract 2018; 59: 311–314. [CrossRef]
- van der Gaag I, Tibboel D. Intestinal atresia and stenosis in animals: a report of 34 cases. Vet Pathol 1980; 17: 565–574. [CrossRef]
- de Battisti A, Harran N, Chanoit G, et al. Use of negative contrast computed tomography for diagnosis of a colonic duplication in a dog. J Small Anim Pract 2013; 54: 547–550. [CrossRef]
- Edward James Hall. Chapter 277: Diseases of the Large Intestine. In: Textbook of Veterinary Internal Medicine, 8th edition, https://expertconsult.inkling.com/read/ettinger-textbook-veterinary-internal-medicine-8e/chapter-277/chapter-277-diseases-of-the (2016, accessed 1 March 2022).
- Kararli TT. Comparison of the gastrointestinal anatomy, physiology, and biochemistry of humans and commonly used laboratory animals. Biopharmaceutics & Drug Disposition 1995; 16: 351–380. [CrossRef]
- Sturgess CP, Canfield PJ, Gruffydd-Jones TJ, et al. A gross and microscopical morphometric evaluation of feline large intestinal anatomy. J Comp Pathol 2001; 124: 255–264. [CrossRef]
- Koenig JB, Rodriguez A, Colquhoun JK, et al. Congenital colonic malformation (‘short colon’) in a 4-month-old standardbred foal. Can Vet J 2007; 48: 420–422.
- Fluke MH, Hawkins EC, Elliott GS, et al. Short colon in two cats and a dog. J Am Vet Med Assoc 1989; 195: 87–90.
- Schlesinger DP, Philibert D, Breur GJ. Agenesis of the cecum and the ascending and transverse colon in a 12-yer-old cat. Can Vet J 1992; 33: 544–546.
- Deschamps C, Humbert D, Zentek J, et al. From Chihuahua to Saint-Bernard: how did digestion and microbiota evolve with dog sizes. Int J Biol Sci 2022; 18: 5086–5102. [CrossRef]
- Weber MP, Biourge VC, Nguyen PG. Digestive sensitivity varies according to size of dogs: a review. J Anim Physiol Anim Nutr (Berl) 2017; 101: 1–9. [CrossRef]
- Penninck D., D’anjou M.-A. Gastrointestinal tract chapter 8. In: Atlas of small animal ultrasonography 2nd edition. 2015, pp. 259–308.
- Di Donato P, Penninck D, Pietra M, et al. Ultrasonographic measurement of the relative thickness of intestinal wall layers in clinically healthy cats. Journal of Feline Medicine and Surgery 2014; 16: 333–339. [CrossRef]
- Gladwin NE, Penninck DG, Webster CRL. Ultrasonographic evaluation of the thickness of the wall layers in the intestinal tract of dogs. American Journal of Veterinary Research 2014; 75: 349–353. [CrossRef]
- Group TWIGS, Washabau R j., Day M j., et al. Endoscopic, Biopsy, and Histopathologic Guidelines for the Evaluation of Gastrointestinal Inflammation in Companion Animals. Journal of Veterinary Internal Medicine 2010; 24: 10–26. [CrossRef]
- Xenoulis PG, Zoran DL, Fosgate GT, et al. Feline Exocrine Pancreatic Insufficiency: A Retrospective Study of 150 Cases. J Vet Intern Med 2016; 30: 1790–1797. [CrossRef]
- Evans H. E., De Lahunta A. The digestive apparatus and abdomen - chapter 7. In: Miller’s Anatomy of the Dog 4th Edition. St. Louis, Missouri, USA., 2013, pp. 322–327.
- Lamoureux A, Maurey C, Freiche V. Treatment of inflammatory rectal strictures by digital bougienage: a retrospective study of nine cases. J Small Anim Pract 2017; 58: 293–297. [CrossRef]
- Brochard C, Siproudhis L, Wallenhorst T, et al. Anorectal stricture in 102 patients with Crohn’s disease: natural history in the era of biologics. Aliment Pharmacol Ther 2014; 40: 796–803. [CrossRef]
- Kouti V, Papazoglou L, Rallis T. Short-Bowel Syndrome in Dogs and Cats. Compendium (Yardley, PA); 28.
- Vanderhoof JA, Langnas AN, Pinch LW, et al. Short bowel syndrome. J Pediatr Gastroenterol Nutr 1992; 14: 359–370.
- Jimba Y, Nagao J, Sumiyama Y. Changes in gastrointestinal motility after subtotal colectomy in dogs. Surg Today 2002; 32: 1048–1057. [CrossRef]
- Clancy CS, Jensen KA, Van Wettere AJ. Congenital Short-Bowel Syndrome in an Adult Dog. Vet Pathol 2018; 55: 462–465. [CrossRef]
- Wakhlu AK, Wakhlu A, Pandey A, et al. Congenital short colon. World J Surg 1996; 20: 107–114. [CrossRef]
- Chadha R, Khan NA. Congenital Pouch Colon. J Indian Assoc Pediatr Surg 2017; 22: 69–78.
Figure 1.
Age at presentation according to the group (A: animals with clinical signs lasting since the adoption and B: animals with a progressive or acute onset of clinical signs during adulthood).
Figure 1.
Age at presentation according to the group (A: animals with clinical signs lasting since the adoption and B: animals with a progressive or acute onset of clinical signs during adulthood).
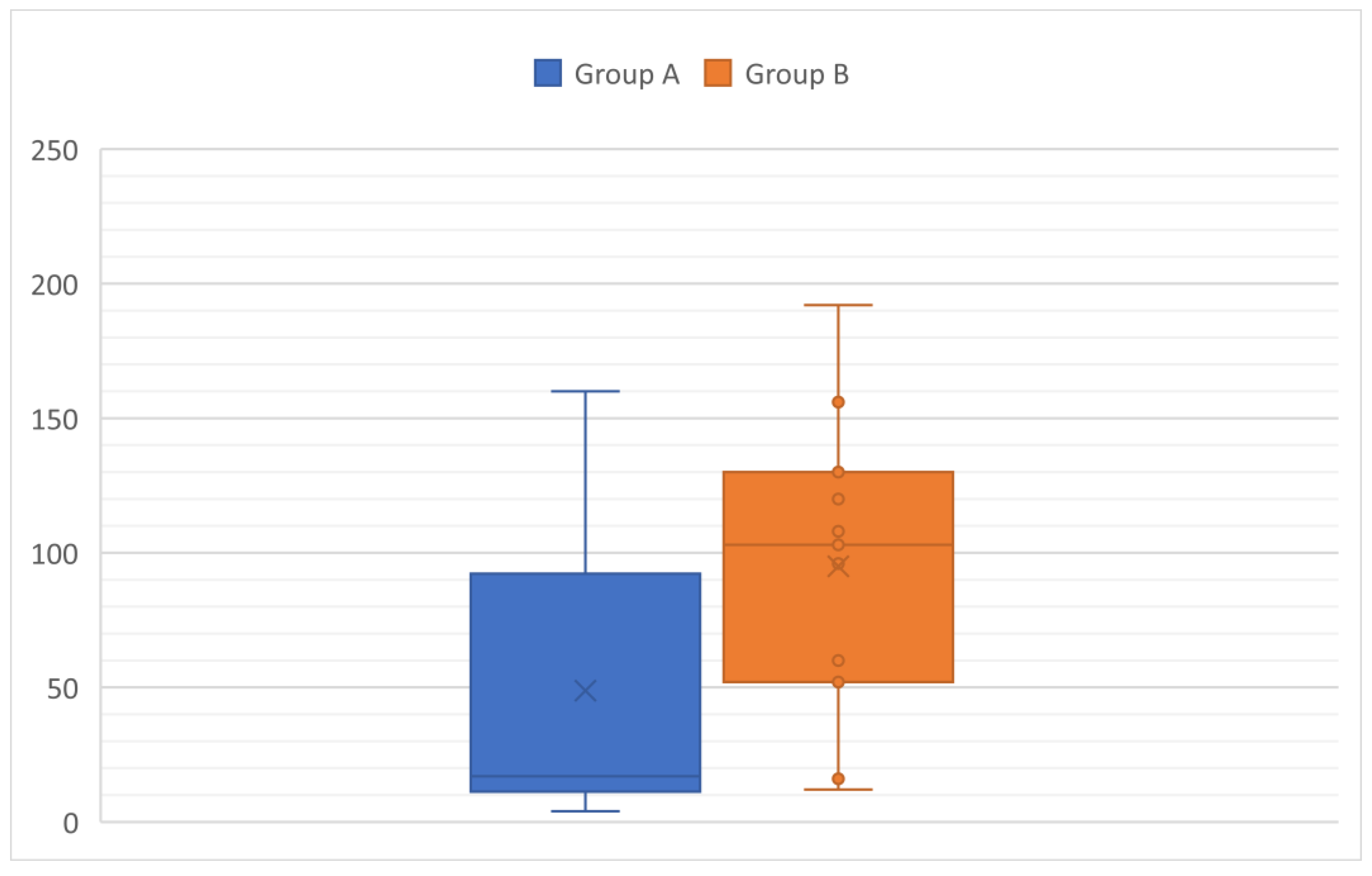
Figure 2.
A. Right lateral radiograph and B. Ventro-dorsal radiograph of the abdomen of case 11, a 6 months old Scottish cat. The descending colon is shorter than expected and abruptly end in the mid left abdomen (white arrow heads). No other parts of the colon are identified.
Figure 2.
A. Right lateral radiograph and B. Ventro-dorsal radiograph of the abdomen of case 11, a 6 months old Scottish cat. The descending colon is shorter than expected and abruptly end in the mid left abdomen (white arrow heads). No other parts of the colon are identified.
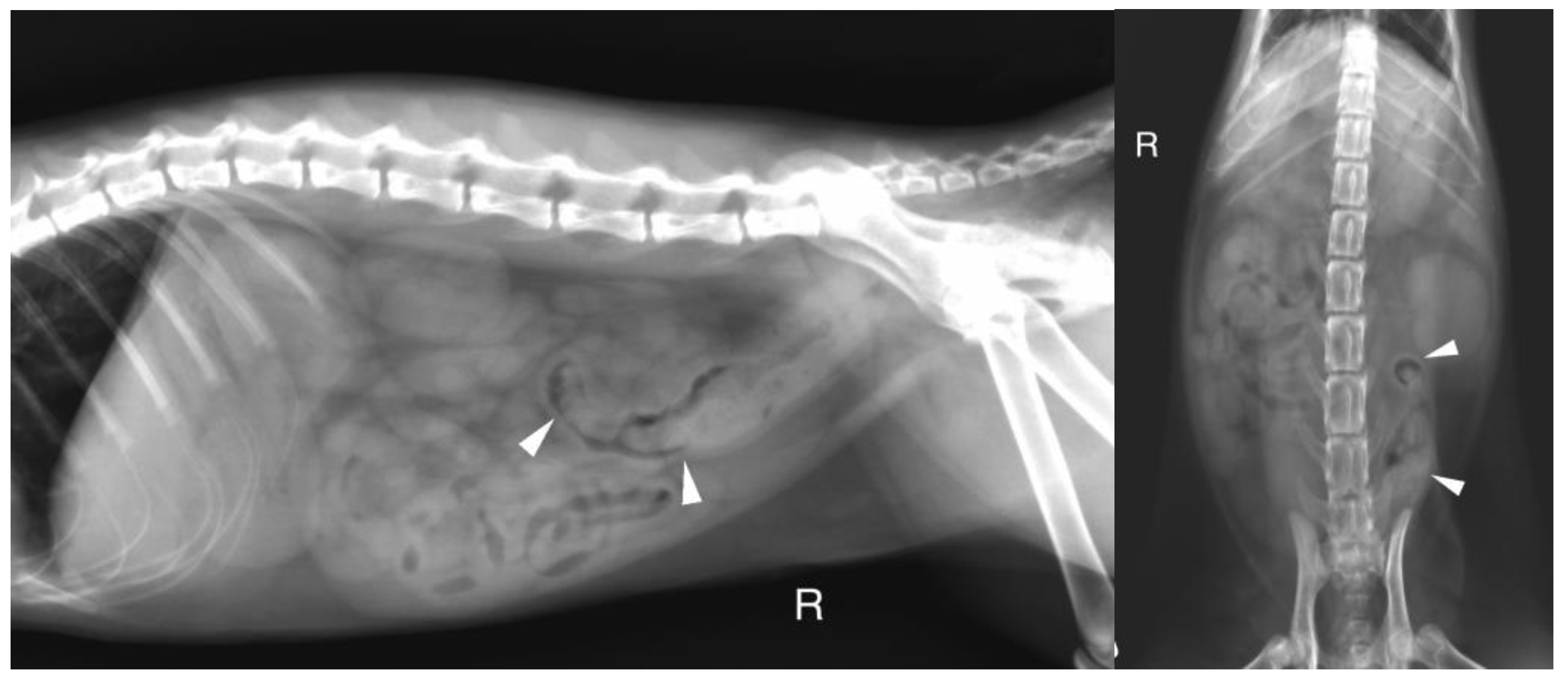
Figure 3.
A. Right lateral radiograph and B. Ventro-dorsal radiograph of the abdomen of case 18, an 8 years-old Colley dog. The cecum is malpositioned in the left cranial and dorsal abdomen (white arrow heads), in continuity with the descending colon on the lateral view (black arrows). A focal narrowing of the aboral part of the descending colon is observed before it enters the pelvis (black arrow heads).
Figure 3.
A. Right lateral radiograph and B. Ventro-dorsal radiograph of the abdomen of case 18, an 8 years-old Colley dog. The cecum is malpositioned in the left cranial and dorsal abdomen (white arrow heads), in continuity with the descending colon on the lateral view (black arrows). A focal narrowing of the aboral part of the descending colon is observed before it enters the pelvis (black arrow heads).
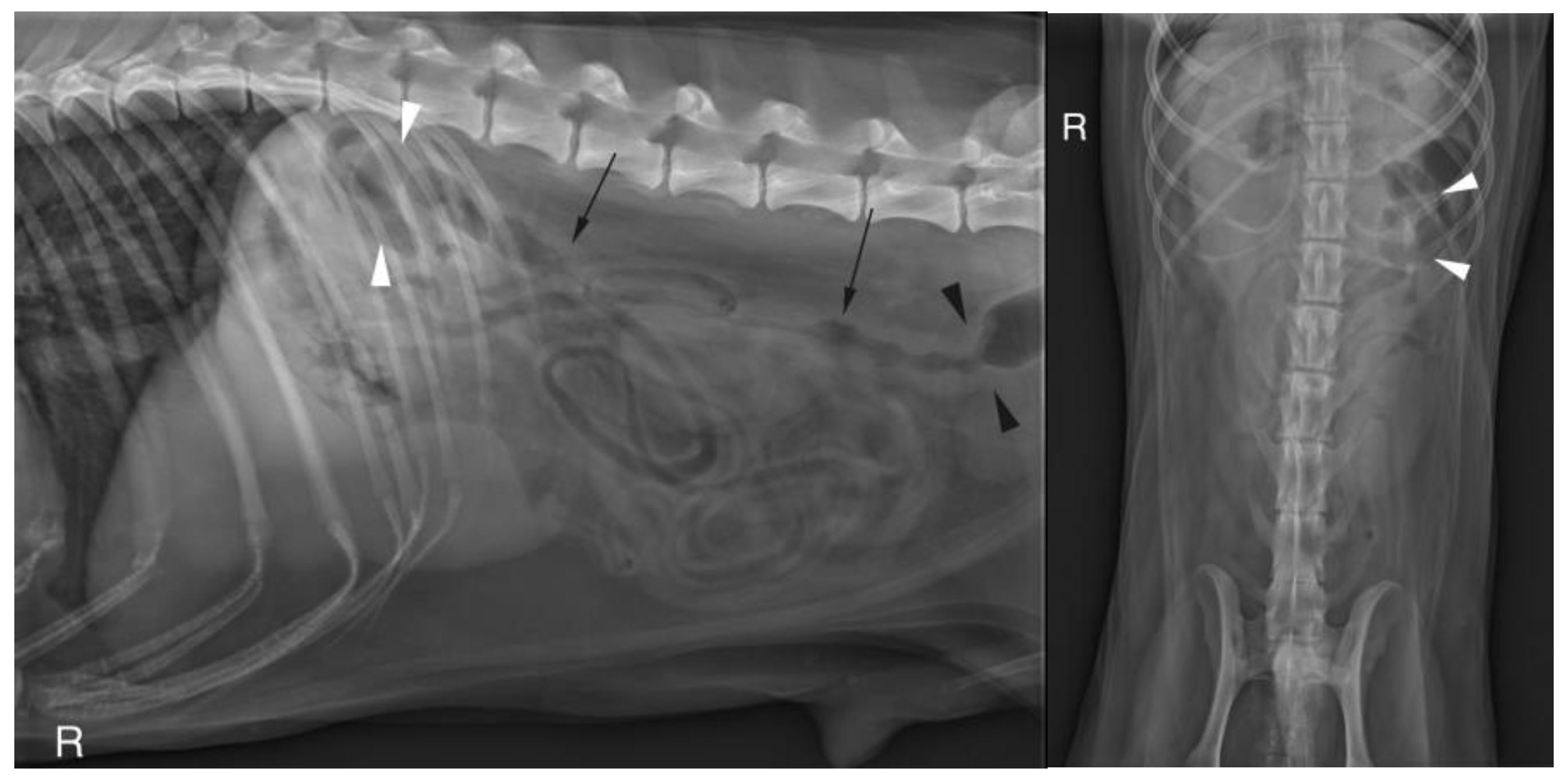
Figure 4.
A. Right lateral radiograph and B. Ventro-dorsal radiograph of the abdomen of the same cat as on image 2, during positive retrograde colonography. The descending colon is shorter than expected (white arrow heads), the ileocolic junction is identified as a narrowing of the colonic lumen orally (asterisk). Contrast medium is also visible within the small intestine (black arrows). The cecum is not identified.
Figure 4.
A. Right lateral radiograph and B. Ventro-dorsal radiograph of the abdomen of the same cat as on image 2, during positive retrograde colonography. The descending colon is shorter than expected (white arrow heads), the ileocolic junction is identified as a narrowing of the colonic lumen orally (asterisk). Contrast medium is also visible within the small intestine (black arrows). The cecum is not identified.
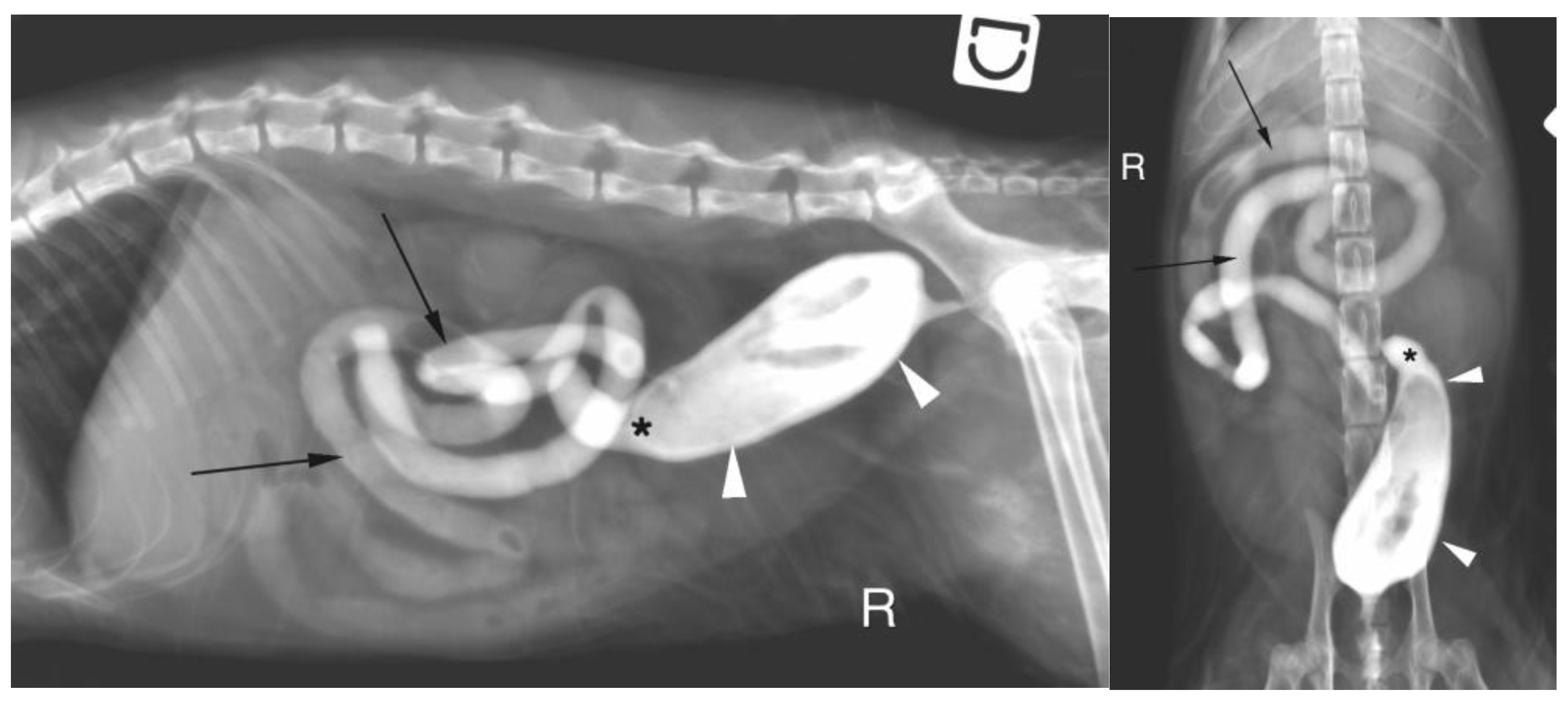
Figure 5.
Abnormal ileocolic junction in a cat (Case 10).
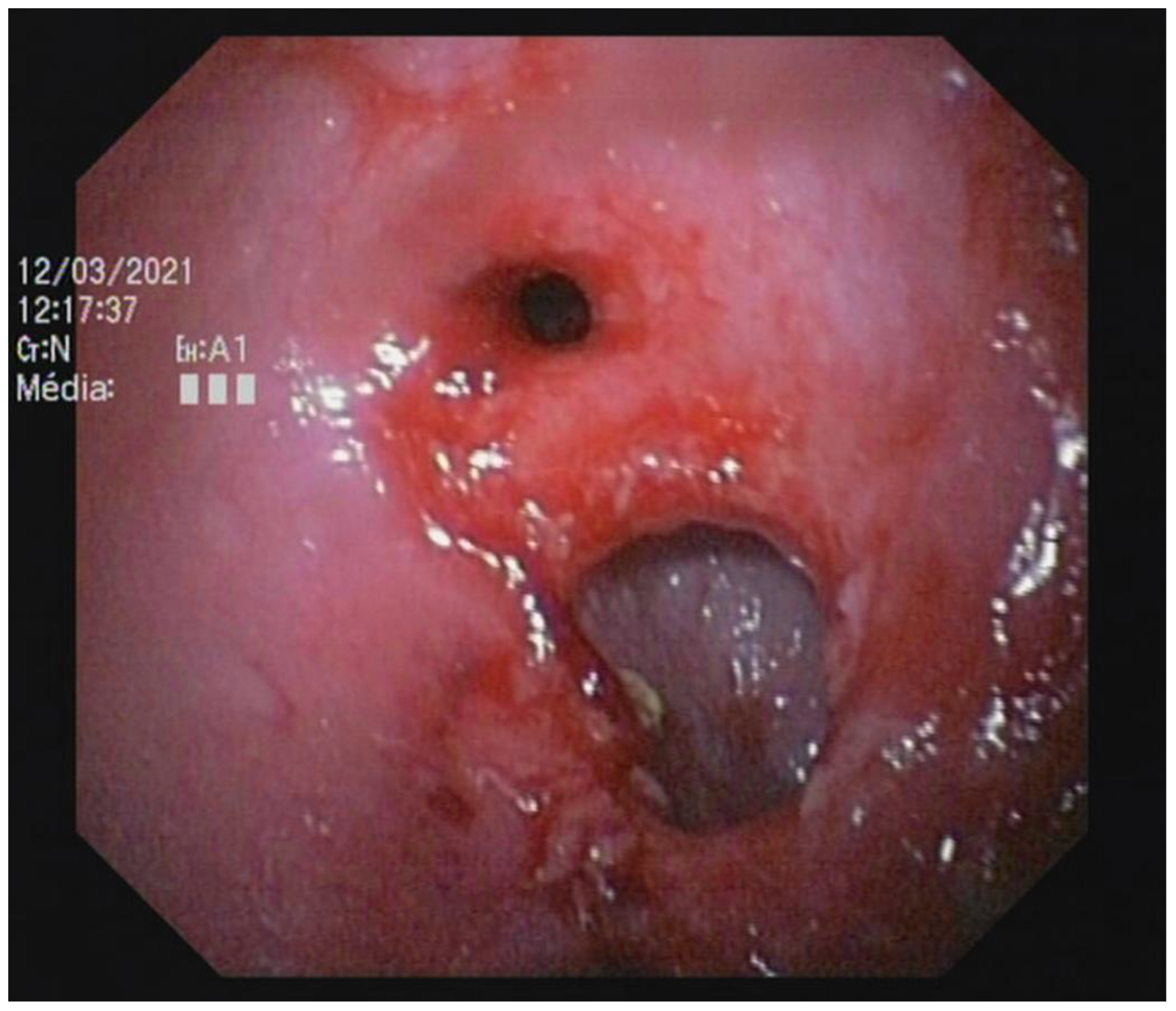
Figure 6.
Focal colonic stenosis in a cat (Case 15).
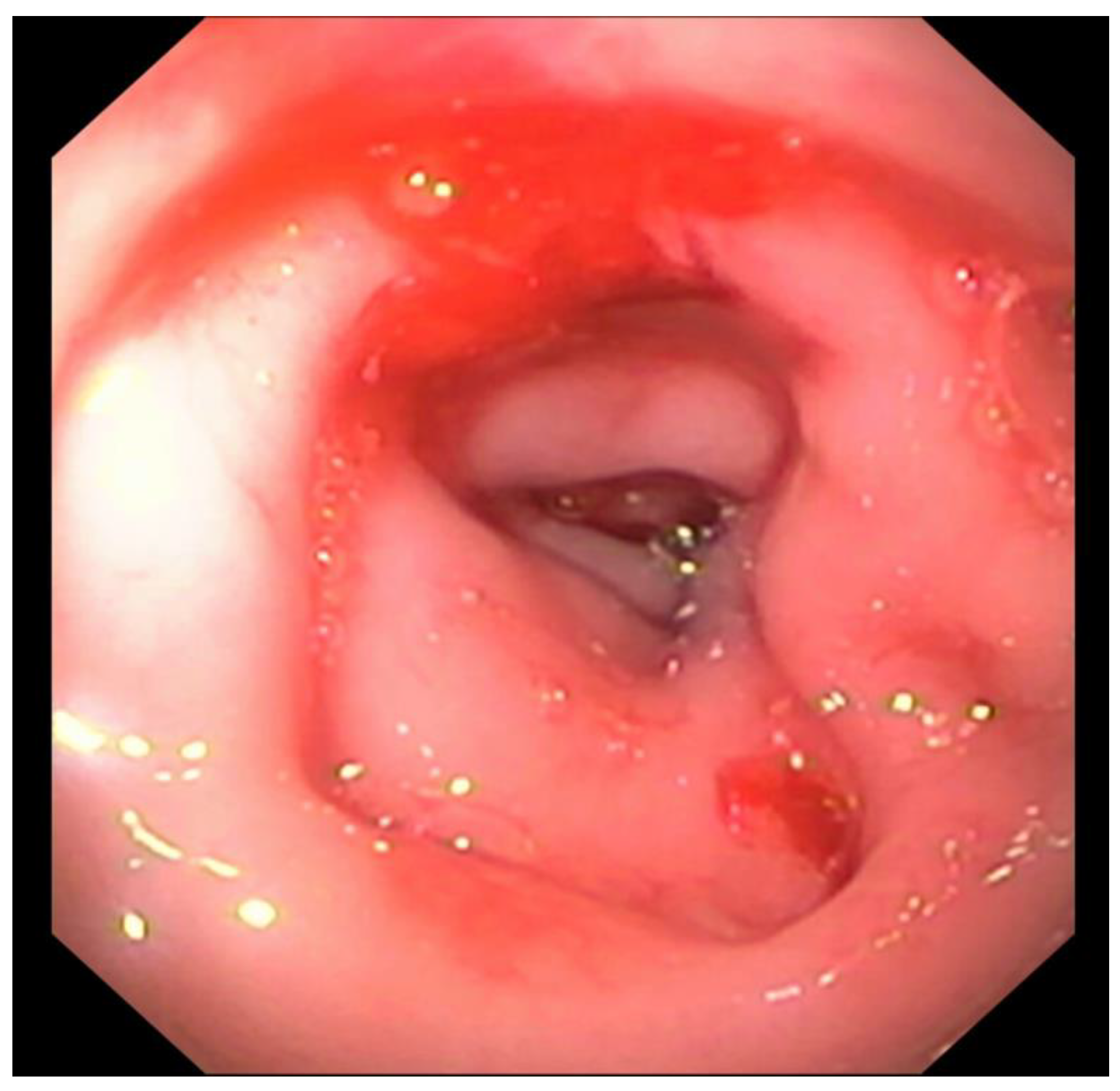
Figure 7.
Diagnosis repartition (FIP: Feline Infectious Peritonitis, LGITL: Low Grade Intestinal T-cell Lymphoma, PLE: Protein-Losing-Enteropathy, y-o: years-old, LP: lymphoplasmacytic).
Figure 7.
Diagnosis repartition (FIP: Feline Infectious Peritonitis, LGITL: Low Grade Intestinal T-cell Lymphoma, PLE: Protein-Losing-Enteropathy, y-o: years-old, LP: lymphoplasmacytic).
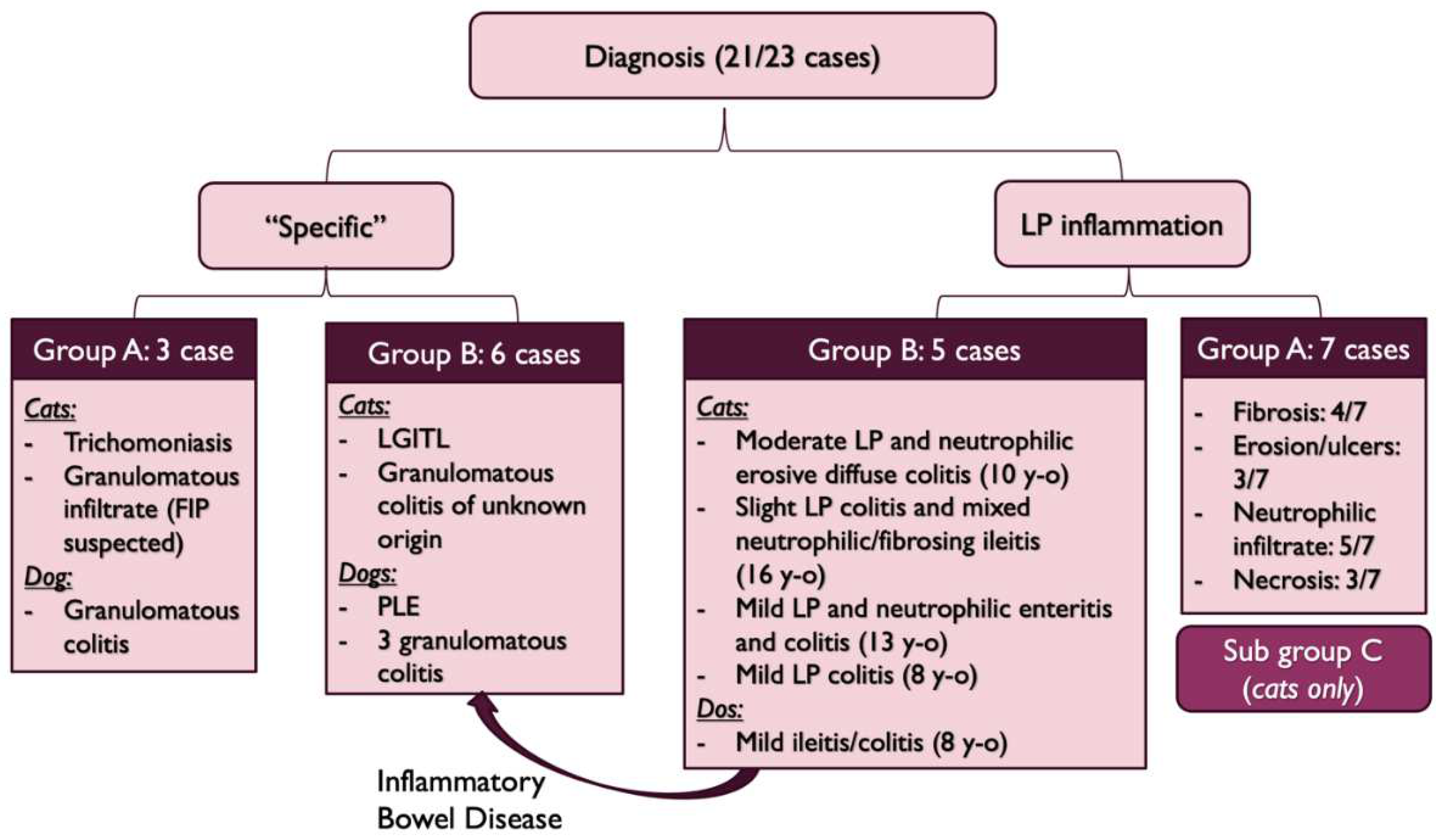
Figure 8.
Colectomy in a cat with partial colonic agenesis: the total length was estimated to 8 cm.

Table 2.
Clinical signs in both groups (y = yes; n = no).
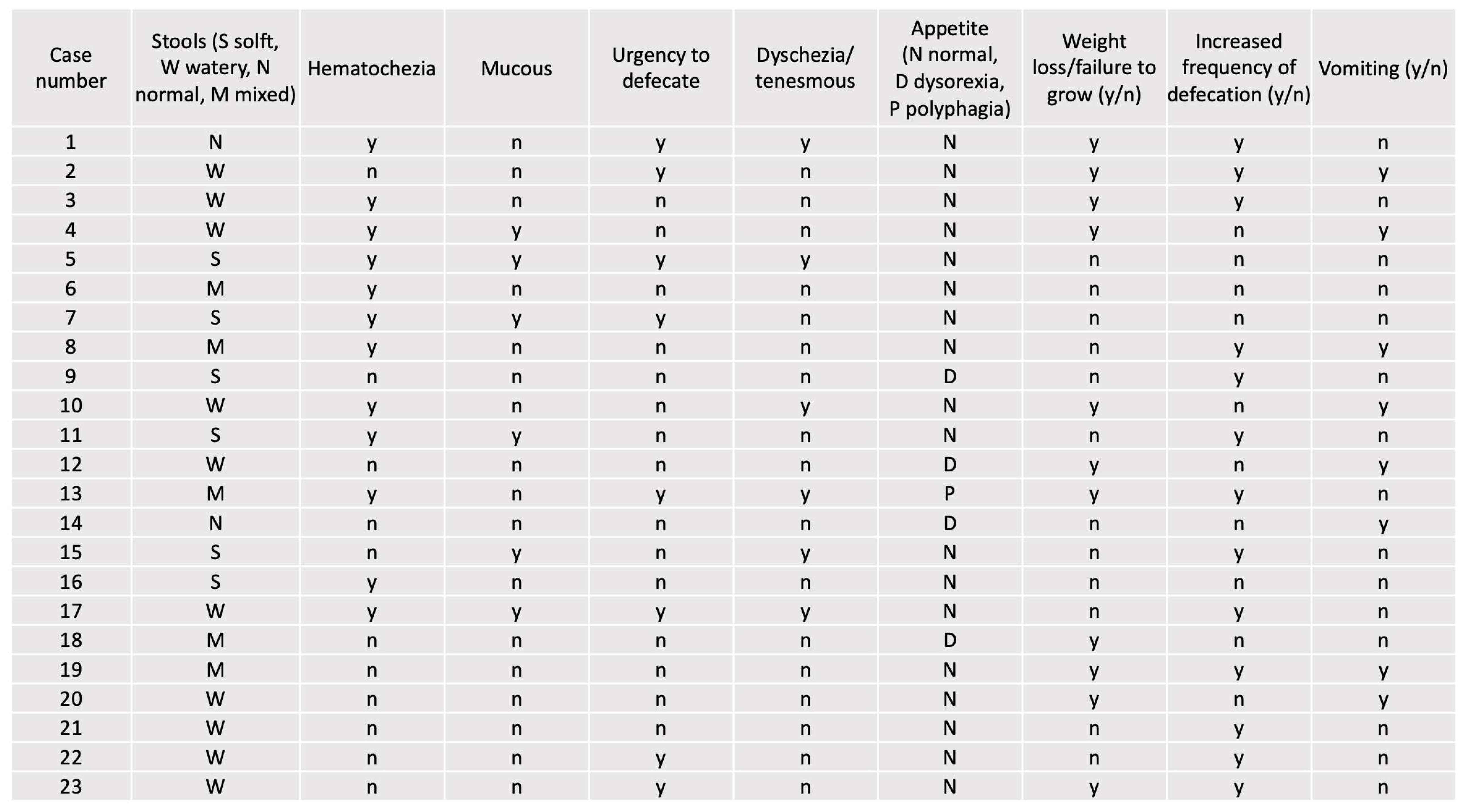 |
Table 3.
Clinical signs in group A (y = yes; n = no).
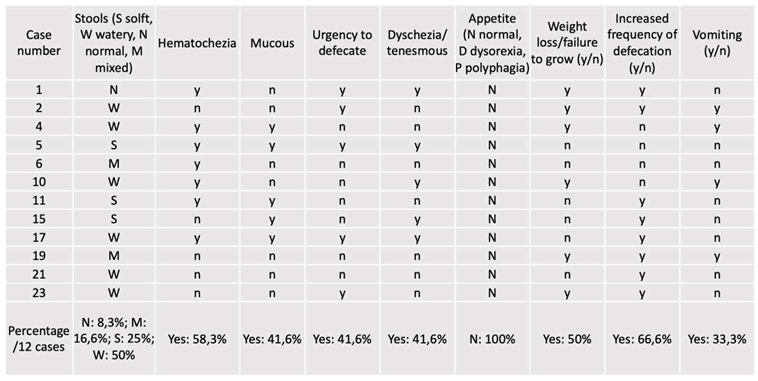 |
Table 4.
Clinical signs in group B (y = yes; n = no).
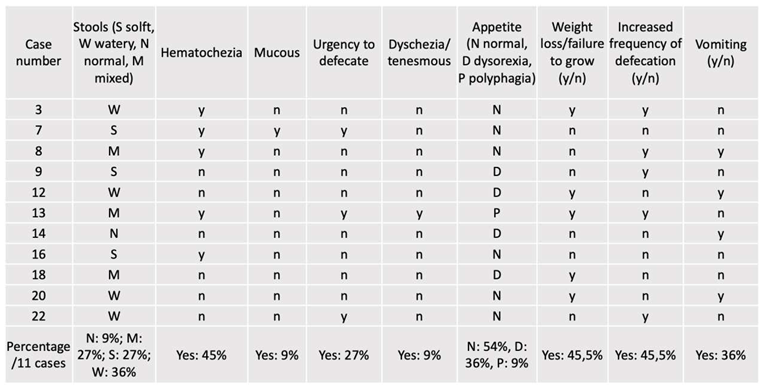 |
Table 5.
Severity of colonic wall thickening at diagnosis (abdominal ultrasound).
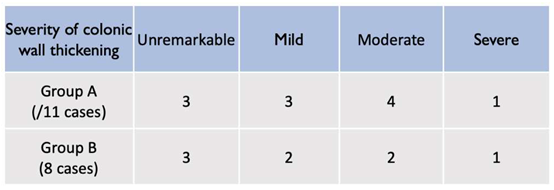 |
Table 6.
Endoscopic findings according to the presentation.
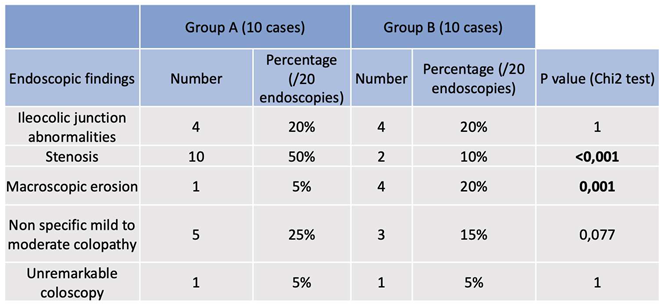 |
Table 7.
Histologic findings according to the presentation (LP: lymphoplasmacytic) (established according to the WSAVA criteria [18].
Table 7.
Histologic findings according to the presentation (LP: lymphoplasmacytic) (established according to the WSAVA criteria [18].
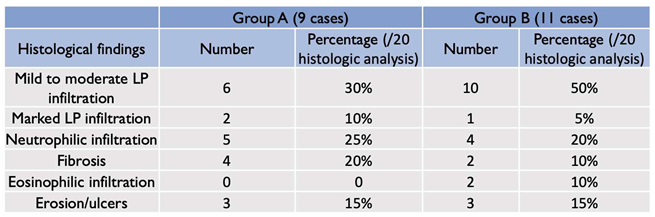 |
Table 8.
Diagnosis, treatments and outcomes (LP: lymphoplasmacytic, FIP: Feline Infectious Peritonitis, IBD: Inflammatory Bowel Disease, PLE: Protein-Losing-Enteropathy, LGITL: Low Grade Intestinal T-cell Lymphoma, D: dog, C: cat). Cases are referenced according to Table 1.
Table 8.
Diagnosis, treatments and outcomes (LP: lymphoplasmacytic, FIP: Feline Infectious Peritonitis, IBD: Inflammatory Bowel Disease, PLE: Protein-Losing-Enteropathy, LGITL: Low Grade Intestinal T-cell Lymphoma, D: dog, C: cat). Cases are referenced according to Table 1.
| Group | Case Number | Diagnosis | Treatment | Outcome |
|---|---|---|---|---|
| 1 | Sub group C and stenosis (C) | Colectomy | Died in the post operative period | |
| A | 2 | Sub group C and stenosis (C) | Bougienage, amoxicillin/clavulanic acid, metronidazole, prednisolone 0.5 mg/kg/d, probiotics, pancreatic enzymes supplementation, cobalamine, diosmectite, hyperdigestible diet | Lost to follow-ups |
| 3 | Tritrichomonosis (C) | Ronidazole | Lost to follow-ups | |
| 4 | Sub group C and stenosis (C) | Metronidazole, prednisolone 0.7 mg/kg/d, hyperdigestible diet | Lost to follow-ups | |
| 6 | Sub group C and stenosis (C) | Colonic stent and bougienage, titanoreine, prednisolone 1 mg/kg/d, metronidazole, pancreatic enzymes, hyperdigestible diet, diosmectite | Marked improvement | |
| 7 | Sub group C with variable degree of LP inflammation (C) | Prendnisolone 0.5 mg/kg/d | Lost to follow up | |
| 10 | Short colon with stenosis. Granulomatous infiltrate (FIP suspected) (C) | Colectomy then prednisolone 1.5 mg/kg, smectite if needed, metronidazole and GS 441524 | Mild improvement | |
| 11 | Sub group C and stenosis (C) | Metronidazole, Lactulose and a/d food | Marked improvement | |
| 13 | Sub group C and stenosis (C) | Metronidazole, prednisolone 0.7 mg/kg/d, hyperdigestible diet | Lost to follow-ups | |
| 15 | Sub group C and stenosis (C) | Prednisolone 0.75 mg/kg/d, marbofloxacin, fiber, hyperdigestible diet | Recent inclusion | |
| 17 | Sub group C and stenosis (C) | Fiber enriched diet, metronidazole, prednisolone 1 mg/kg/d | Recent inclusion | |
| 19 | Granulomatous colitis (D) | Marbofloxacin | Improvement | |
| B | 5 | IBD (C) | Prednisolone 0.5 mg/kg and amoxicillin/clavulanic acid (antibiogram) 3 weeks | Lost to follow up |
| 8 | Granulomatous inflammation of unknown origin (C) | Prednisolonone 2 mg/kg/d, smectite, TMPS, | Died within 2 weeks of hypovolemic shock | |
| 9 | LGITL in ileum (C) | Prednisolonone 2 mg/kg/d, chlorambucil 20 mg/m2 every 2 weeks | Marked improvement | |
| 12 | LP colitis (C) | Prednisolone 0.5 mg/kg and hyperdigestible diet | Marked improvement | |
| 14 | IBD with cholecystitis (C) | Marbofloxacin, amoxicillin/clavulanic acid, prednisolone 0.65 mg/kg/d after cholelithiasis removal. | Marked improvement | |
| 16 | IBD with stenotic areas (C) | Prednisolone, marbofloxacine, hyperdigestible diet | Recent inclusion | |
| 18 | IBD with stenotic areas (D) | Smectite, homemade eviction diet, fortiflora, tylosine, prednisolone 0.5 mg/kg/d 15 days. | Marked improvement. Colonic ADK diagnosed 6 months after | |
| 20 | Granulomatous colitis (D) | Enrofloxacine, fenebendazole, diosmectite | Died of septic choc after aspiration pneumonia | |
| 21 | Granulomatous colitis (D) | Marbofloxacine 4 mg/kg for 6 weeks | Marked improvement | |
| 22 | PLE (D) | Prednisolone 2 mg/kg/d, cobalamine, ciclosporine 5 mg/kg/d, clopidogrel, metronidazole, ULF diet | Improvement with normal stools | |
| 23 | Granulomatous colitis (D) | Enrofloxacine, hyperdigestible diet, diosmectite | Marked improvement |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



