
Submitted:
21 July 2023
Posted:
25 July 2023
You are already at the latest version
Abstract
Background: Atherosclerotic plaque (AP) vulnerability can be assessed by coronary artery imaging techniques. Modern lipid-lowering therapy (LLT) has a stabilizing effect on the AP and reduces the likelihood of progression of vascular remodeling.
Methods: Databases searched comprised PubMed, and the Web of Science up to April 2023. In total, 8 relevant articles were selected, and all of them are original clinical studies.
Results Based on the results of ODISSEY-J-IVUS, there was a decrease in the percentage change in the normalized total volume of AP by 3.1% in the monotherapy group and by 4.8% in the combined LLT group (p = 0.23). According to GLACOV study normalized total atheroma volume decreased by 0.9 mm3 in the placebo group and by 5.8 mm3 in the evolocumab group (95% CI -7.3 -2.5; p<0.001). Plaque regression was observed in 64.3% of patients receiving evolocumab versus 47.3% of those on placebo. The dynamics of the minimum thickness of the fibrous cap varied within 18.0-62.67 microns while on combined LLT and 13.2-33.19 microns on monotherapy (PACMAN-AMI, Gao F). In the HUYGENS study, a lipid arc regression of 57.5° was obtained on combined LLT and by 31.4° with the statin alone.
Conclusion: significant progress in the development of cardiovascular imaging has made it possible to expand our understanding of the morphology of AP, the features of coronary vessel remodeling, and the development of acute cardiovascular complications.
Keywords:
vulnerable plaque
; intravascular imaging
; intravascular ultrasound
; optical coherent tomography
; computed tomography coronary angiography
; PCSK9 inhibitors.
Introduction
Epidemiological studies have shown that in 2019, 12.7 million new cases of cardiovascular disease (CVD) were registered in European countries, of which more than two million were in the Russian Federation [1]. One of the main risk factors for the development of CVD is hypercholesterolemia [2,3]. The prevalence of lipid disorders in Russia was studied in the ESSE-RF multicenter study, which enrolled 21,048 patients from 13 regions of the country [4]. The level of total cholesterol (TC) above 5,0 mmol/l was detected in 58.4% of the study population, without any significant differences between men and women. As far as hypercholesterolemia is currently considered as the main factor contributing to the onset and progression of atherosclerosis, the high prevalence of CVD in Russia seems to be quite understandable.
Only 2/3 of patients with acute coronary syndrome (ACS) who underwent invasive coronary angiography a few weeks or months before its onset had a hemodynamically significant narrowing of the vessel [5]. However, the likelihood of developing an ACS largely depends on the presence of unstable (vulnerable) atherosclerotic plaques (AP). It can be assessed by coronary artery imaging techniques, which provide high-resolution images. AP’s vulnerability is associated with its morphological features and severity of arterial remodeling [6], which is manifested by an increase in the outer diameter during accommodation to the growing AP to prevent narrowing of the vessel lumen. The use of modern lipid-lowering drugs has a stabilizing effect on the AP and reduces the likelihood of progression of vascular remodeling.
Objective—to study the role of cardiac imaging methods in the detection of vulnerable AP within the coronary arteries, and their stabilization using various lipid-lowering drugs.
Methods
Databases searched comprised PubMed, and the Web of Science up to April 2023, with English constraints. The search Medical Subject Headings (MeSH) were “coronary artery disease”, “vulnerable plaque”, “statin”, “Alirocumab”, “Evolocumab”, “PCSK9 inhibitor(s)”, and optical coherence tomography (OCT), and “intravascular ultrasonography (IVUS) and “computed tomography coronary angiography”.
The following criteria were used to exclude studies: published abstracts, reviews, letters to editors, case reports, and meta-analyses. In total, 8 relevant articles were selected, and all of them are original clinical studies (Table) [7,8,9,10,11,12,13,14].

Table.
inhibitors on the regression of atherosclerotic plaques.
| Study | Year | Design | Number of patients(PCSK9/ control) | Inhibitor PCSK9 | Control | Underlying disease | Follow-up duration (weeks) |
|---|---|---|---|---|---|---|---|
| IVUS | |||||||
| ODYSSEY-J | 2019 | RCCT | 93/89 | Alirocumab 75/150mg + statin (atorvastatin ≥10mg or rosuvastatin ≥5mg) | Atorvastatin ≥10mg or Rosuvastatin ≥5mg | ACS | 36 |
| GLAGVO | 2016 | RCCT | 484/484 | Evolocumab 420mg + statin | Statin + placebo | chrIHD | 78 |
| PACMAN-AMI | 2022 | RCCT | 148/152 | Alirocumab 150mg + rosuvastatin 20mg | Rosuvastatin 20mg + placebo | MI | 52 |
| OCT | |||||||
| HUYGENS | 2021 | RCCT | 80/81 | Evolocumab 420mg + atorvastatin ≥40mg | Placebo + atorvastatin ≥40mg | MIwST | 52 |
| Yanoet al. | 2019 | 18/40 | Evolocumab 140mg + rosuvastatin 5mg | Rosuvastatin 5mg | ACS | 12 | |
| ALTAIR | 2020 | RCCT | 12/12 | Alirocumab 75mg + rosuvastatin 10mg | Rosuvastatin 10mg | chrIHDor ACS | 36 |
| Gao et al. | 2021 | RCCT | 30/3 | Alirocumab 75mg + atorvastatin 20mg or rosuvastatin 10mg | Atorvastatin 20mg or Rosuvastatin 10mg | IHD orACS | 36 |
| CTCA | |||||||
| ARCHITECT | 2023 | Single group study | 104 | Alirocumab 150mg /2 weeks+ high-intensity statin therapy | - | Familial hypercholesterolemia without clinical manifestations of atherosclerotic CVD | 78 |
Stable and unstable AP
The differentiation of APs into stable and unstable is extremely important for determining the patient's prognosis and depends on the structure, size and configuration of the AP. Stable plaques are characterized by a thick, dense fibrous cap rich in collagen. They are characterized by slow growth over many years, and may not significantly affect the blood supply to organs. Distinctive features of unstable APs are a thin (<65 μm) fibrous cap, signs of acute inflammation (infiltration of the fibrous cap with inflammatory cells, mainly macrophages, activated T-cells and mast cells), the presence of a large lipid core (> 40% of the AP volume), areas of spotty-calcifications and hemorrhage into the nucleus [15].
AP destabilization develops as a result of a number of processes in the vascular wall, such as ferroptosis, necroptosis, secondary necrosis, pyroptosis, and inflammation. The combination of these processes contributes to the thinning of the fibrous cap and, under certain conditions, to its rupture, which is accompanied by the activation of the blood coagulation system and the formation of a thrombus. Depending on the size of the formed thrombus and its localization, this process is clinically manifested by unstable angina pectoris, myocardial infarction (MI), ischemic stroke, or thrombosis of the peripheral arteries. AP instability is also associated with a high risk of fatal cardiovascular events. It has been established that up to 70% of cases of acute coronary thrombosis occur against the background of unstable AP [16], and sudden coronary death develops due to the rupture of the AP followed by thrombosis in 73% of cases [17].
The Role of Imaging Methods in the Diagnostics of Vulnerable APs
Invasive coronary angiography (Figure 1) is the gold standard in the diagnostics of atherosclerotic lesions of the coronary arteries. However, this method does not allow predicting the development of acute cardiovascular events, visualizing the components of the vessel wall, and evaluating the signs of instability of AP. Besides, in some cases, it cannot provide high-quality visualization, especially in the presence of calcifications or overlapping views [18].
The invention of modern imaging techniques and its implementation into clinical practice has expanded our opportunities for diagnosing vulnerable APs. The first method, which appeared more than 30 years ago, and made it possible to study the AP parameters in vivo was intravascular ultrasound (IVUS) [19]. IVUS allows real-time assessment of the longitudinal and transverse dimensions of the vessel, the severity of its remodeling, the size and structure of the AP. While coronary angiography provides visualization of only the projection of the lumen and does not allow assessing the structure of the vascular wall, IVUS makes it possible to study the structure of the arterial wall (intima, smooth muscle and connective tissue layers). IVUS-controlled PCI reduces the likelihood of suboptimal stent deployment, incomplete atherosclerotic lesion coverage, vascular wall dissection, and increases the minimum stent lumen area compared to angiographic control. These benefits have been associated with the reduction in the frequency of ischemic events [20]. For quite a long time, IVUS had been considered to be a classic tool for assessing neointimal hyperplasia, but at the moment, the capabilities of this technology are not enough to reliably determine the individual components of the AP, which are currently considered to be the determining factors for its vulnerability. This contributed to the development of more advanced IVUS modifications using special computational algorithms that provide additional information about the vulnerability of the AP.
Optical coherence tomography (OCT) is a high-resolution imaging technique that is most commonly used to assess the AP vulnerability (Figure 2). OCT was first proposed in 1991 at the Massachusetts Institute of Technology to visualize the cross section of the retina. In 2001, OCT was applied for intracoronary imaging, and has since been widely used to assess the condition of the walls of the coronary arteries. Near-infrared light is used to obtain a cross-sectional image of the arteries.This has a higher frequency and shorter wavelength radiation compared to ultrasound, which provides a sharper resolution (about 10 times) than with IVUS. In addition, OCT makes it possible to detail the degree and thickness of calcification, determine fibrous AP and lipids in its structure, as well as to detect intimal ruptures and classify thrombi into coagulation (red) and platelet (white) thrombi based on the intensity of signal attenuation [21]. It has been shown that the sensitivity of OCT in detecting a thrombus approaches 100%, while for IVUS it is 33% [22]. The resolution of OCT makes it possible to accurately identify vulnerable APs according to the following characteristic parameters: a large necrotic nucleus, a thin fibrous capsule, neoangiogenesis, and inflammatory changes in the AP cap [23].
The use of OCT is indicated before PCI, which provides preliminary information about the type of thrombus, ulceration of the AP, superficial calcification, which can complicate the procedure. The decision on coronary intervention is made in accordance with the following OCT criteria: the minimum area of the transverse lumen of the vessel <3.5 mm2; the presence of a thrombus [24]. According to the conducted studies, OCT-controlled PCI is characterized by similar clinical and angiographic results in comparison with PCI performed using IVUS [25]. After stenting, OCT allows you to automatically measure the minimum area of the stent and the area of the lumen of the control vessel, evaluating the dilatation achieved. In addition, OCT detects dissections and perforations that occur during the stenting process [24,25]
However, OCT is characterized by low signal penetration into the tissues (to the depth of 1-3 mm), which does not allow visualizing the arterial wall to the full depth. The technique for assessing the size of the vessel during OCT is currently being improved [26]. The greatest advantage of OCT in comparison with IVUS is the ability to evaluate the stent restenosis, as mild neointimal AP is often not detected by IVUS [24]. Another advantage of OCT is the good reproducibility of measurements, which is important both in clinical practice and in scientific research. The possibility of overcoming the limitations of IVUS and OCT techniques by creating a hybrid intravascular imaging is currently being studied [27].
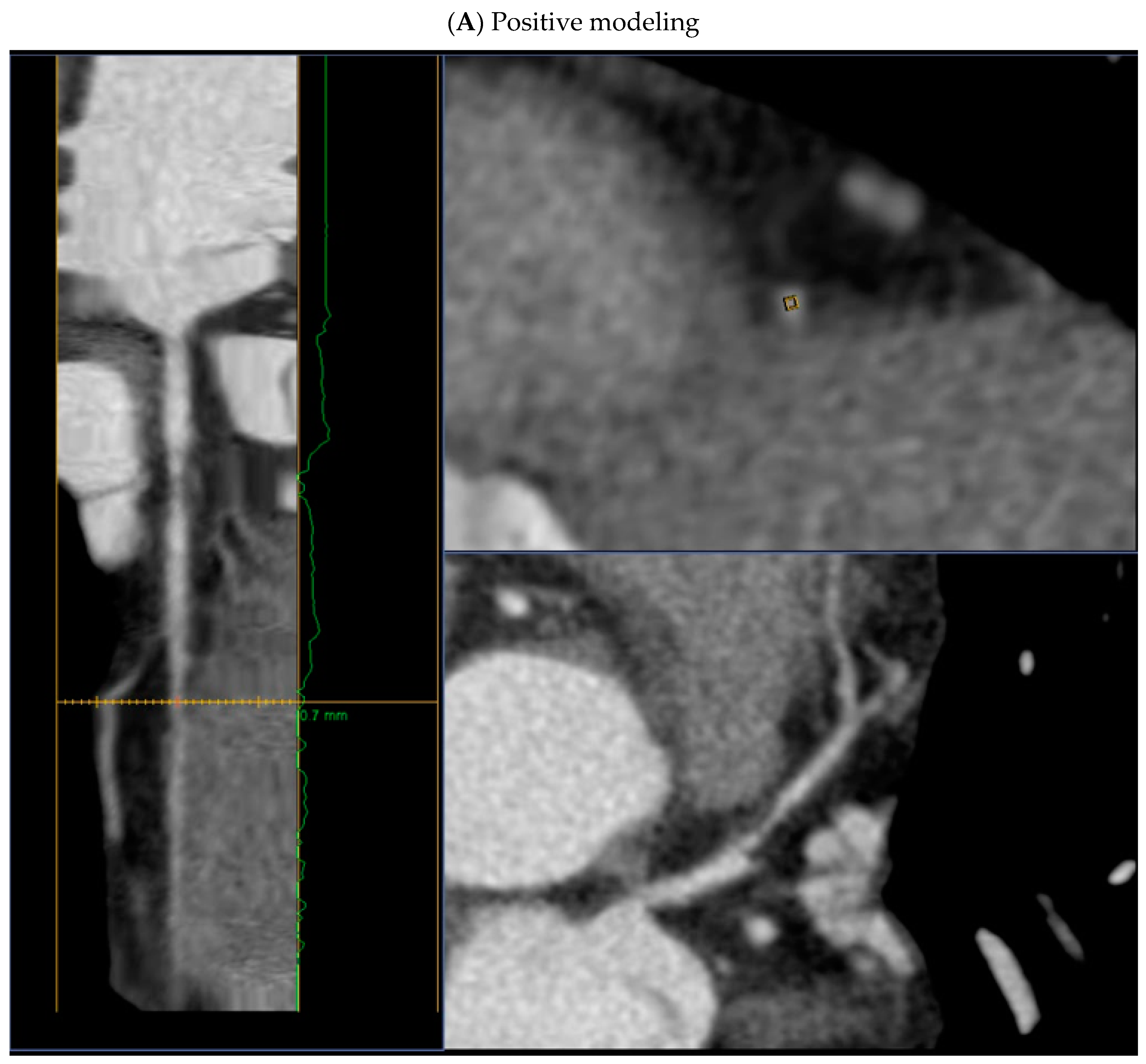
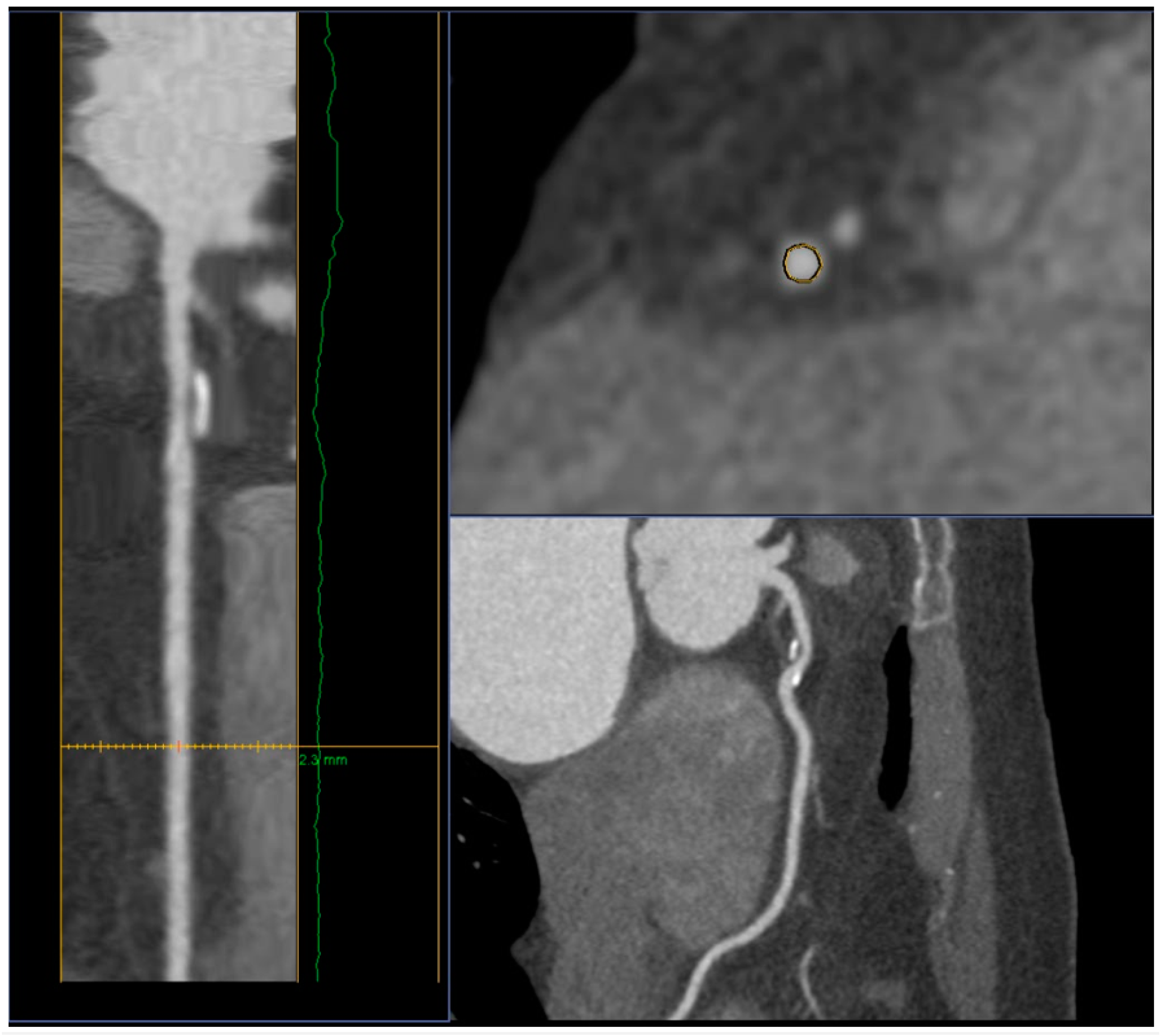
Computed tomography (CT) is the next imaging technique that allows assessing the state of the coronary bed. The CT image is a map of the x-ray density distribution of an object, expressed in the standardized Hounsfield units (HU). The advent of computed tomography coronary angiography (CTCA) (Figure 3) has provided unique opportunities for non-invasive diagnostics of coronary artery damage. In recent years, criteria for AP instability have also been recognized, which may be of great importance for further management of the patient [28] These include the following features:
- positive remodeling (foci of vascular dilatation) - increase in the total volume of the AP, leading to a relative expansion of the diameter of the coronary artery. To assess it, a quantitative indicator is used - the remodeling index (RI), which is calculated by the formula RI = D1/D2, where D1 is the diameter of the vessel at the level of the plaque, D2 is the diameter of the intact segment proximal to the plaque. Positive remodeling is considered to be an excess of the vessel diameter at the plaque level by more than 10% compared to the reference segment;
- presence of a low-density area within the plaque (less than 30 HU);
- spotty calcifications within the plaque - uneven inclusions of small calcium deposits less than 3 mm;
- napkin-ring sign - a ring-shaped increase in X-ray density along the periphery of the plaque, not exceeding 130 HU;
In addition to these features, the American Heart Association (AHA) proposed some geometric characteristics of the coronary arteries [29]:
- distance from the ostium of the vessel to the stent - the smaller the distance from the ostium to the stent, the higher the risk of developing ACS, (<39 mm for the left coronary artery and <60 mm for the right coronary artery);
- tortuosity - presence of one bend more than 90° or three bends from 45° to 90° using a 3-point angle inside the lesion;
- bifurcation lesion.
CTCA allows detecting non-calcified APs in 83% of all cases that were detected by IVUS, mixed AP - in 94%, calcified - in 95% [30].
The drawback of CTCA is unreliable detection of AP with a thin cap due to insufficient spatial resolution (about 0.3–0.5 mm). For the same reason, CTCA does not clearly distinguish plaques with an intact cap in case of patients with ACS from lesions in patients with stable angina. However, the presence of an AP with a thin cap can be detected indirectly on the basis of the presence of a napkin-ring sign in the cross section of the artery, which is visualized with the predominance of the lipid component in the AP structure, manifestations of angiogenesis, and the presence of spotty calcifications [31].
AP volume parameters obtained by CTCA have a high degree of correlation with similar parameters obtained during IVUS. Plaques with signs of positive remodeling, with low density, spotty (less than 3 mm) calcifications were significantly more often observed in patients with ACS, while patients with stable coronary artery disease (CAD) were more likely to have larger calcifications [32,33].
Thus, CTCA, despite its insufficiently high resolution, is able to provide the most important information for the stratification of cardiovascular risk. Besides, its may be useful in identifying patients with the high risk of recurrent ischemic complications after the ACS without the ST elevation due to measuring the total number of non-calcified APs associated with a poor prognosis.
Positron emission tomography (PET) refers to the methods of radionuclide diagnostics, and among numerous indications, is also the main method for molecular imaging of atherosclerosis. Fluorodeoxyglucose (FDG) visualization of unstable AP is based on the fact that increased metabolic activity within the plaque is ensured by an active macrophage response. It was observed that the severity of FDG accumulation within the AP is proportional to the number of macrophages within it, but it has no correlation with the area and/or volume of the AP. This method is quantitative, its main SUV (standardized level of radiopharmaceutical capture) indicator turned out to be highly reproducible, which allows making objective comparisons over time [34,35]. In contrast to CT, PET with FDG is able to show the inflammatory component of the plaque, and the maximum FDG uptake reflects the high level of inflammation, which makes it prone to rupture [36]. Another area of interest for FDG imaging is the assessment of inflammatory processes in the area of coronary artery stenting. To date, more than 20 radionuclides are known that allow visualization of various stages of atherogenesis in animal models or in vitro, with an emphasis on the visualization of unstable APs. [37].
The role of imaging methods in evaluating the effectiveness of lipid-lowering therapy
Statins are one of the most studied classes of drugs for primary and secondary prevention of CVD. If the target LDL level is not achieved on a maximal dose statin, it is recommended to add an inhibitor of cholesterol absorption, ezetimibe [38]. Ezetimibe monotherapy may be considered for patients with statin intolerance, but such approach has not been studied in randomized clinical trials.
Proprotein convertase subtilin/kexin type 9 (PCSK9) inhibitors are monoclonal antibodies. Their invention is closely related to the discovery of the role of the PCSK9 gene and protein in cholesterol metabolism. Binding of the PCSK9 enzyme to LDL receptor domains leads to their degradation and, accordingly, to a decrease in their distribution density, which causes a decrease in LDL metabolism and leads to hypercholesterolemia. Targeted inhibition of PCSK9 by monoclonal antibodies increases the number of active LDL receptors, followed by an increase in the uptake of LDL from the bloodstream and its decrease in plasma [39].
Currently, the intensification of lipid-lowering therapy in patients with very high cardiovascular risk is considered as an effective and justified strategy. According to the latest version of the Russian guidelines on the management of lipid disorders (2023) [38]:
- if there is a significant increase of LDL in patients with a very high risk (above 4.0 mmol/l), it is recommended to consider an initiation of a statin and ezetimibe, preferably in one tablet or capsule.
- if there is a significant increase of LDL in patients with extreme or very high risk (above 5.0 mmol/l), it is recommended to consider an initiation of a statin at the maximum tolerated dose + ezetimibe + PCSK9 inhibitor: Alirocumab, Evolocumab or Inclisiran.
Effectiveness of combined lipid-lowering therapy and its influence on features of AP’s vulnerability were evaluated in numerous studies using imaging techniques (IVUS/OCT/CTCA).
The ODYSSEY-J-IVUS study [7] comprised 206 patients with ACS within four weeks prior to enrollment with LDL level ≥ 2.59 mmol/l (≥100 mg/dL). The first group received atorvastatin ≥ 10 mg/day or rosuvastatin ≥ 5 mg/day. The second group received a combination of a statin and alirocumab (75 mg every 2 weeks), and if after 14 weeks of the study the level of LDL was ≥ 2.59 mmol/l, the dose of alirocumab was increased to 150 mg every 2 weeks. The total duration of the study was 36±2 weeks. IVUS was performed at the onset and at the end of the study. Based on the results of IVUS, there was a decrease in the percentage change in the normalized total volume of AP by 3.1% in the monotherapy group and by 4.8% in the combination therapy group (p = 0.23). The absolute change in the percentage volume of AP was 1.3% and 1.4%, respectively (p=0.79). LDL levels after 36 weeks of the study decreased by 13.4% in the monotherapy group, while in the group of combined lipid-lowering treatment - by 63.9% (p<0.0001). The safety parameters among the groups were comparable.
The GLAGOV study included 968 patients with CAD [8]. The first group received evolocumab (420 mg monthly), the second received a placebo. The total duration of the study was 78 weeks. IVUS was performed at the beginning of the study and after 78 weeks. The percentage of atheroma volume (PAV) increased by 0.05% in the placebo group and decreased by 0.95% while receiving evolocumab (95% CI, -1.8% -0.64%; p<0.001). Normalized total atheroma volume (TAV) decreased by 0.9 mm3 in the placebo group and by 5.8 mm3 in the evolocumab group (95% CI -7.3 -2.5; p<0.001). Plaque regression (for PAV) was observed in 64.3% of patients receiving evolocumab versus 47.3% of those on placebo. Besides this, lower LDL levels were achieved in the evolocumab group (93.0 vs. 36.6 mg/dL; 95% CI -59.7 -53.4; p < 0.001).
The PACMAN-AMI study [9] included 300 patients undergoing PCI due to acute myocardial infarction. Patients received alirocumab (150 mg every 2 weeks) or placebo in addition to therapy with rosuvastatin (20 mg/day). The follow-up period was 52 weeks. IVUS and OCT were performed at the beginning and end of the study. As a result, mean change in % AP volume decreased by 2.13% in the alirocumab group and by 0.92% in the placebo group (95% CI -1.78% to -0.65%; p<0.001). The mean change in the minimum fibrous cap thickness was 62.67 µm in the alirocumab group and 33.19 µm in the placebo group (95% CI 11.75–47.55; p = 0.001). Mean change in maximum lipid core burden index within 4 mm was −79.42 with alirocumab vs −37.60 with placebo (95% CI, −70.71 to −11.77; p= .006).
The Gao F. study included 61 patients with chronic CAD or ACS, and with coronary artery damage of 50-70% diameter [10], with LDL ≥ 1.81 mmol/l for patients with ACS or ≥ 2.59 mmol/l for patients without ACS. All patients received rosuvastatin ≥ 10 mg/day or atorvastatin ≥ 20 mg/day, and alirocumab (75 mg every 2 weeks) was added later on to the first group patients only. The total duration of the study was 36±2 weeks. OCT was obtained at baseline and on 36 week. As a result, a statistically significant increase in the minimum fibrous cap thickness (18.0 [10.8–29.2] µm vs 13.2 [7.4–18.6] µm) was obtained in the combination therapy group compared to the monotherapy group; p=0.029) and minimum lumen area (0.20 [0.10-0.33] mm2 vs 0.13 [0.12-0.24] mm2; p=0.006), as well as a greater decrease in the maximum lipid arc (15.1o [7.8–24.5] vs 8.4o [2.0–10.5], p=0.008). The decrease in LDL levels in the combination therapy group was significantly greater than in the monotherapy group (1.72 ± 0.51 vs. 0.96 ± 0.59, p<0.0001).
The HUYGENS study [11] included 161 patients with MI without the ST segment elevation. Evolocumab (420 mg/month) was compared with placebo. The follow-up period was 52 weeks. A series of OCT was performed during the study. In the evolocumab group, they obtained a more pronounced increase in the minimum cap thickness (+42.7 vs +21.5 μm; p=0.015), a regression of the lipid arc (-57.5o vs -31.4o; p=0.04), as well as a decrease of macrophage index (-3.17 vs -1.45 mm; p=0.04) and LDL level (28.1 vs 87.2 mg/dl; p<0.001).
The Yano study [12] included 58 patients with ACS undergoing PCI. All patients received rosuvastatin (5 mg/day), of which 18 received evolocumab (140 mg/every 2 weeks). OCT was performed at the beginning of the study, after 4 and 12 weeks of follow-up. The results showed that an increase in the thickness of the fibrous cap of the AP (177.7±33.2 µm vs 164.0±30.4 µm; p<0.001) and a decrease in the macrophage index (7.0±1.8 vs 8.0±2 .2; p=0.002) were higher in the combination therapy group.
The ALTAIR study [13] included 24 patients with chronic CAD or ACS and LDL levels >70 mg/dl. All patients received rosuvastatin (10 mg/day), of which 12 additionally received alirocumab (75 mg/every 2 weeks). The follow-up period was 36 weeks. OCT was performed on the first and final visit. In the alirocumab group, the fibrous cap thickness increased more than in the monotherapy group (190 µm [128-220] vs 90 µm [60-125]; p = 0.001), and the macrophage index was lower (-28.4% [-35, 3% to -19.0%] vs -10.2% [-25.3% to 4.3%]; p=0.033).
The last study we want to cite is the ARCHITECT study [14] which was designed as an open, multicentre, single-group study and included 104 patients with familial hypercholesterolemia without clinical manifestations of coronary atherosclerosis. In addition to high-intensity statin therapy (both with and without ezetimibe), all patients received alirocumab (150 mg/every 2 weeks). CTCA was performed at the beginning of the study and after 78 weeks of treatment. As a result, the volume of AP changed from 34.6% (32.5-36.8%) at admission to 30.4% (27.4-33.4%) on the final visit (P<0.001). The AP morphology has also been changed with an increase in the proportion of calcified (+0.3%; P<0.001) and fibrotic (+6.2%; P<0.001) plaque, while the percentage of fibrous-fatty (-3.9%; p <0.001) and necrotic (–0.6%; P<0.001) plaque decreased. Median LDL originally was 138.9 (117.5-175.3) mg/dl and was found to be 45.0 (36.0-65.0) mg/dl at the end of the study (p<0.001).
Conclusion
Significant progress in the development of cardiovascular imaging has made it possible to expand our understanding of the morphology of AP, the features of coronary vessel remodeling, and the development of acute cardiovascular complications. Combined lipid-lowering therapy seems to be the most proven option for effective treatment of vulnerable APs based on the available research studies and data .
References
- Timmis, A.; Vardas, P.; Townsend, N.; et al. European Society of Cardiology: cardiovascular disease statistics 2021. Eur Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef] [PubMed]
- Ference, B.A.; Yoo, W.; Alesh, I.; et al. Effect of long-term exposure to lower low-density lipoprotein cholesterol beginning early in life on the risk of coronary heart disease: a Mendelian randomization analysis. J Am CollCardiol 2012, 60, 2631–2639. [Google Scholar] [CrossRef] [PubMed]
- Domanski, M.J.; Tian, X.; Wu, C.O.; et al. Time course of LDL cholesterol exposure and cardiovascular disease event risk. J Am CollCardiol 2020, 76, 1507–1516. [Google Scholar] [CrossRef] [PubMed]
- Metelskaya, V.A.; Shalnova, S.A.; Deev, A.D.; et al. Analysis of the prevalence of indicators characterizing the atherogenicity of the spectrum of lipoproteins among residents of the Russian Federation (ESSE-RF study). Preventive Medicine 2016, 19, 15–23. [Google Scholar] [CrossRef]
- Shah, P.K. Mechanisms of plaque vulnerability and rupture. J Am CollCardiol. 2003, 41 (4 Suppl S), 15S–22S. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.M.; Davies, M.J. Vulnerable plaque. Relation of characteristics to degree of stenosis in human coronary arteries. Circulation. 1996, 94, 928–31. [Google Scholar] [CrossRef]
- Ako, J.; Hibi, K.; Tsujita, K.; et al. Effect of alirocumab on coronary atheroma volume in japanese patients with acute coronary syndrome - The ODYSSEY J-IVUS trial. Circ J 2019, 83, 2025–2033. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; PuriR, *!!! REPLACE !!!*; Anderson, T.; et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA. 2016, 316, 2373–2384. [Google Scholar] [CrossRef]
- Räber, L.; Ueki, Y.; Otsuka, T.; et al. Effect of alirocumab added to high-intensity statin therapy on coronary atherosclerosis in patients with acute myocardial infarction: the PACMAN-AMI randomized clinical trial. JAMA 2022, 327, 1771–1781. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Wang, Z.J.; Ma, X.T.; et al. Effect of alirocumab on coronary plaque in patients with coronary artery disease assessed by optical coherence tomography. Lipids Health Dis. 2021, 20, 106. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Kataoka, Y.; Nissen, S.E.; et al. Effect of evolocumab on coronary plaque phenotype and burden in statin-treated patients following myocardial infarction. JACC Cardiovasc Imaging 2022, 15, 1308–1321. [Google Scholar] [CrossRef] [PubMed]
- Yano, H.; Horinaka, S.; Ishimitsu, T. Effect of evolocumab therapy on coronary fibrous cap thickness assessed by optical coherence tomography in patients with acute coronary syndrome. J Cardiol 2020, 75, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Sugizaki, Y.; Otake, H.; Kawamori, H.; et al. Adding alirocumab to rosuvastatin helps reduce the vulnerability of thin-cap fibroatheroma: an ALTAIR trial report. JACC Cardiovasc Imaging 2020, 13, 1452–1454. [Google Scholar] [CrossRef] [PubMed]
- Pérez de Isla, L.; Díaz-Díaz, J.L.; Romero, M.J.; et al. Alirocumab and Coronary Atherosclerosis in Asymptomatic Patients with Familial Hypercholesterolemia: The ARCHITECT Study. Circulation. 2023, 147, 1436–1443. [Google Scholar] [CrossRef] [PubMed]
- Fishbein, M.C. The vulnerable and unstable atherosclerotic plaque. CardiovascPathol. 2010, 19, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Kolodgie, F.D.; Burke, e.t. al. Lessons from sudden coronary death: A comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.J. Anatomic features in victims of sudden coronary death: coronary artery pathology. Circulation. 1992, 85, 119–124 PMID: 1728500. [Google Scholar] [PubMed]
- Sidharta, S.L.; Baillie, T.J.; Howell, S.; et al. Evaluation of human coronary vasodilator function predicts future coronary atheroma progression. Heart 2018, 104, 1439–1446. [Google Scholar] [CrossRef]
- Malaiapan, Y.; Leung, M.; White, A.J. The role of intravascular ultrasound in percutaneous coronary intervention of complex coronary lesions. Cardiovasc Diagn Ther. 2020, 10, 1371–1388. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Mintz, G.S.; Koskinas, K.C.; et al. Intracoronary Imaging Part 1: Guidance Optimization of Coronary Interventions An Expert Consensus Document of the European Association of Percutaneous Cardiovascular Interventions /, L. Räber [et al.]. Eur. Heart J. 2018, 39, 3281–3300. [Google Scholar] [CrossRef]
- Kume, T.; Akasaka, T. ; KawamotoT; et al Assessment of coronary arterial thrombus by optical coherence tomography. Am, J. Cardiol. 2006, 97, 1713–1717. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Imanishi, T.; Takarada, S.; et al. Assessment of culprit lesion morphology in acute mycardial infarction: ability of optical coherence tomography compared with intravascular ultrasound coronary angioscopy. J. Am. Coll. Cardiol. 2007, 50, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; et al. Lessons From Sudden Coronary Death: A Comprehensive Morphological Classification Scheme for Atherosclerotic Lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef]
- Gutiérrez-Chico, J.L.; Alegría-Barrero, E.; Teijeiro-Mestre, R.; et al. Optical Coherence Tomography From Research to Practice Eur Heart, J. Cardiovasc. Imaging. 2012, 13, 370–384. [Google Scholar] [CrossRef] [PubMed]
- Kume, T. ; UemuraS Current Clinical Applications of Coronary Optical Coherence Tomography / T. Kume, S. Uemura. Cardiovasc. Interv. Ther. 2018, 33, 1–10. [Google Scholar] [CrossRef]
- Maehara, A.; Matsumura, M.; Ali, Z.A.; et al. IVUS-Guided Versus OCT-Guided Coronary Stent Implantation: A Critical Appraisal. JACC Cardiovasc Imaging. 2017, 10, 1487–1503. [Google Scholar] [CrossRef] [PubMed]
- Bourantas, C.V.; Jaffer, F.A.; Gijsen, F.J.; et al. Hybrid intravascular imaging: recent advances, technical considerations, and current applications in the study of plaque pathophysiology. Eur. Heart J. 2017, 38, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Cury, R.C.; Abbara, S.; Achenbach, S.; et al. CAD-RADS(TM) Coronary Artery Disease - Reporting and Data System. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Radiology (ACR) and the North American Society for Cardiovascular Imaging (NASCI). Endorsed by the American College of Cardiology. J Cardiovasc Comput Tomogr. 2016, 10, 269–81. [Google Scholar] [CrossRef] [PubMed]
- Han, D.; Lin, A.; Kuronuma, K.; et al. Association of Plaque Location and Vessel Geometry Determined by Coronary Computed Tomographic Angiography With Future Acute Coronary Syndrome-Causing Culprit Lesions. JAMA Cardiol. 2022, 7, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Leber, A.W.; Becker, A.; Knez, A.; et al. Accuracy of 64-Slice Computed Tomography to Classify and Quantify Plaque Volumes in the Proximal Coronary System. J Am CollCardiol. 2006, 47, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, M.; Tanaka, A.; Kitabata, H.; et al. Comparison of diagnostic accuracy between multidetectorcomputed tomography and virtual histology intravascular ultrasound for detecting optical coherence tomography-derived fibroatheroma. CardiovascIntTher. 2013, 29, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, U.; Moselewski, F.; Nieman, K.; et al. Noninvasive Assessment of Plaque Morphology and Composition in Culprit and Stable Lesions in Acute Coronary Syndrome and Stable Lesions in Stable Angina by Multidetector Computed Tomography. J Am CollCardiol. 2006, 47, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Pundziute, G.; Schuijf, J.D.; Jukema, J.W.; et al. Head-to-Head Comparison of Coronary Plaque Evaluation Between Multislice Computed Tomography and Intravascular Ultrasound Radiofrequency Data Analysis. JACC: Cardiovascular Interventions. 2008, 1, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Rudd, J.H.; Myers, K.S.; Bansilal, S.; et al. Atherosclerosis inflammation imaging with 18F-FDG PET: carotid, iliac, and femoral uptake reproducibility, quantification methods, and recommendations. J Nucl Med. 2008, 49, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; On, Y.K.; Lee, E.J.; et al. Reversal of vascular 18F-FDG uptake with plasma high-density lipoprotein elevation by atherogenic risk reduction. J Nucl Med. 2008, 49, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Rogers, I.S.; Nasir, K.; Figueroa, A.L.; et al. Feasibility of FDG imaging of the coronary arteries: comparison between acute coronary syndrome and stable angina. JACC Cardiovasc Imaging. 2010, 3, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Rudd, J.H.; Narula, J.; Strauss, H.W.; et al. Imaging atherosclerotic plaque inflammation by fluorodeoxyglucose with positron emission tomography: ready for prime time? J Am CollCardiol. 2010, 55, 2527–2535. [Google Scholar] [CrossRef] [PubMed]
- Ezhov, M.V.; Kukharchuk, V.V.; Sergienko, I.V.; et al. Disorders of lipid metabolism. Clinical Guidelines 2023. Russian Journal of Cardiology. 2023, 28, 5471. [Google Scholar] [CrossRef]
- Zyryanov, S.K.; Butranova, O.I. New opportunities for lowering lowdensity lipoprotein cholesterol: comparative characteristics of PCSK9-targeted therapy. Russian Journal of Cardiology. 2022, 27, 5271. [Google Scholar] [CrossRef]
Figure 1.
Dissection and mural thrombosis on invasive coronary angiography.
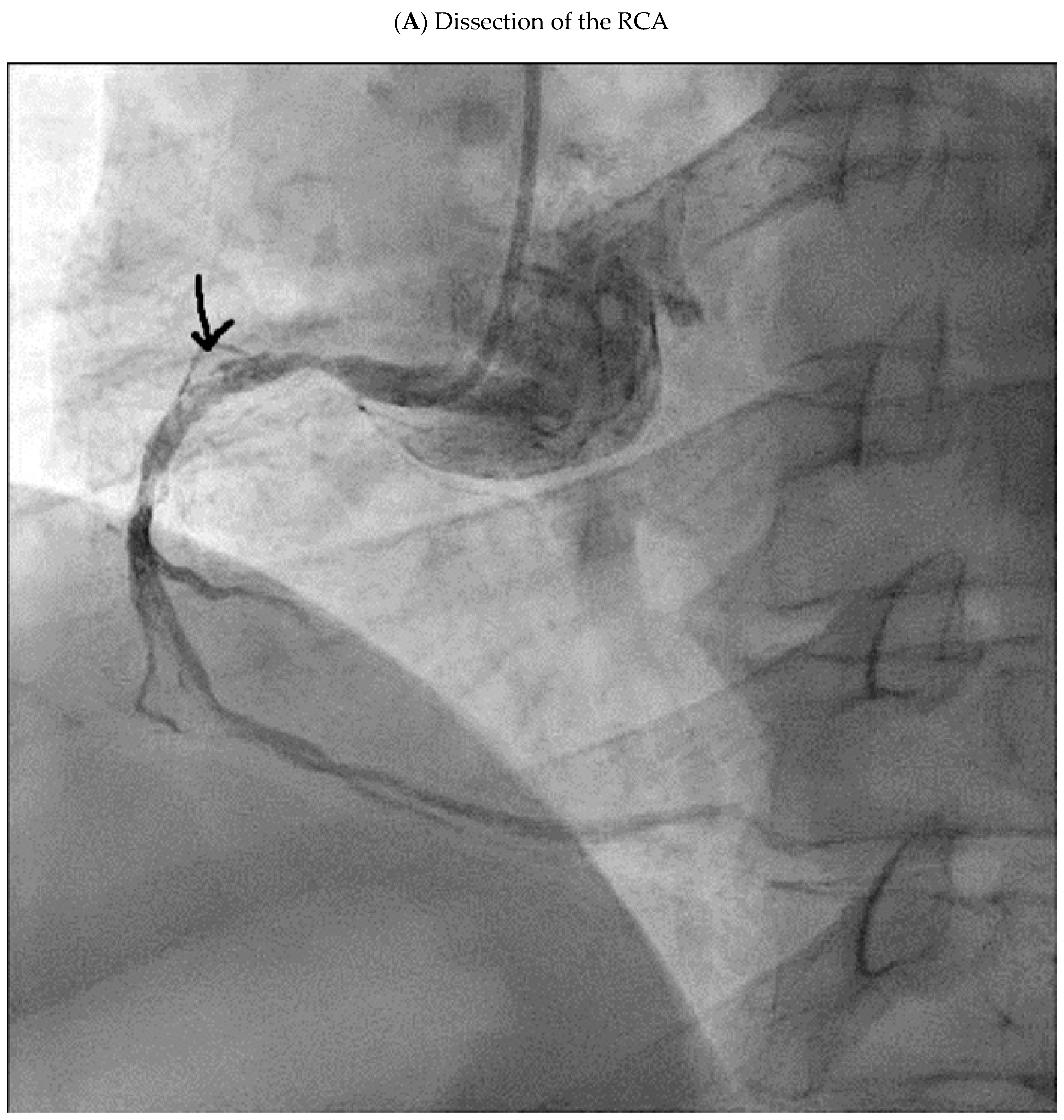
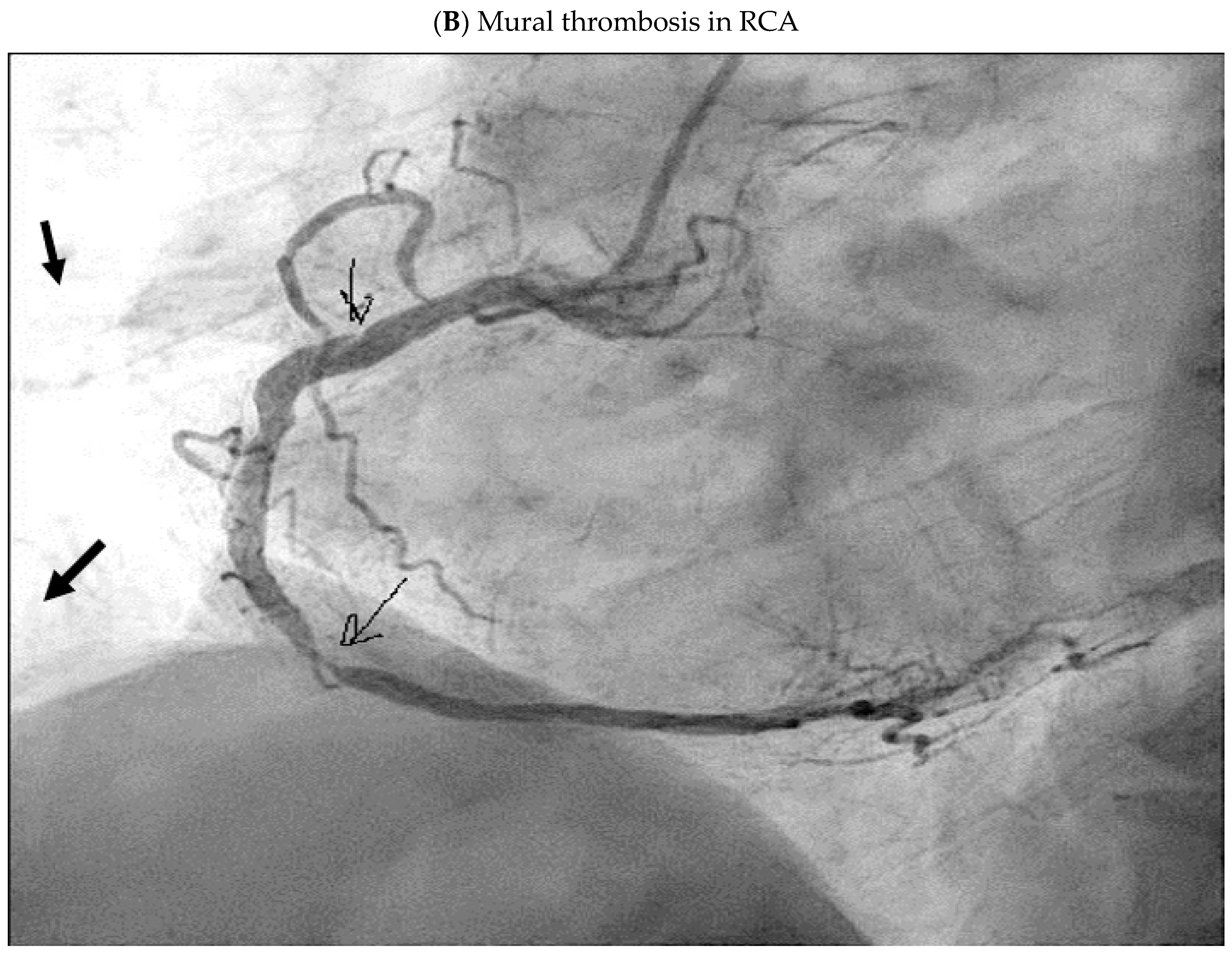
Figure 2.
А Unstable plaque on optical coherence tomography (OCT).
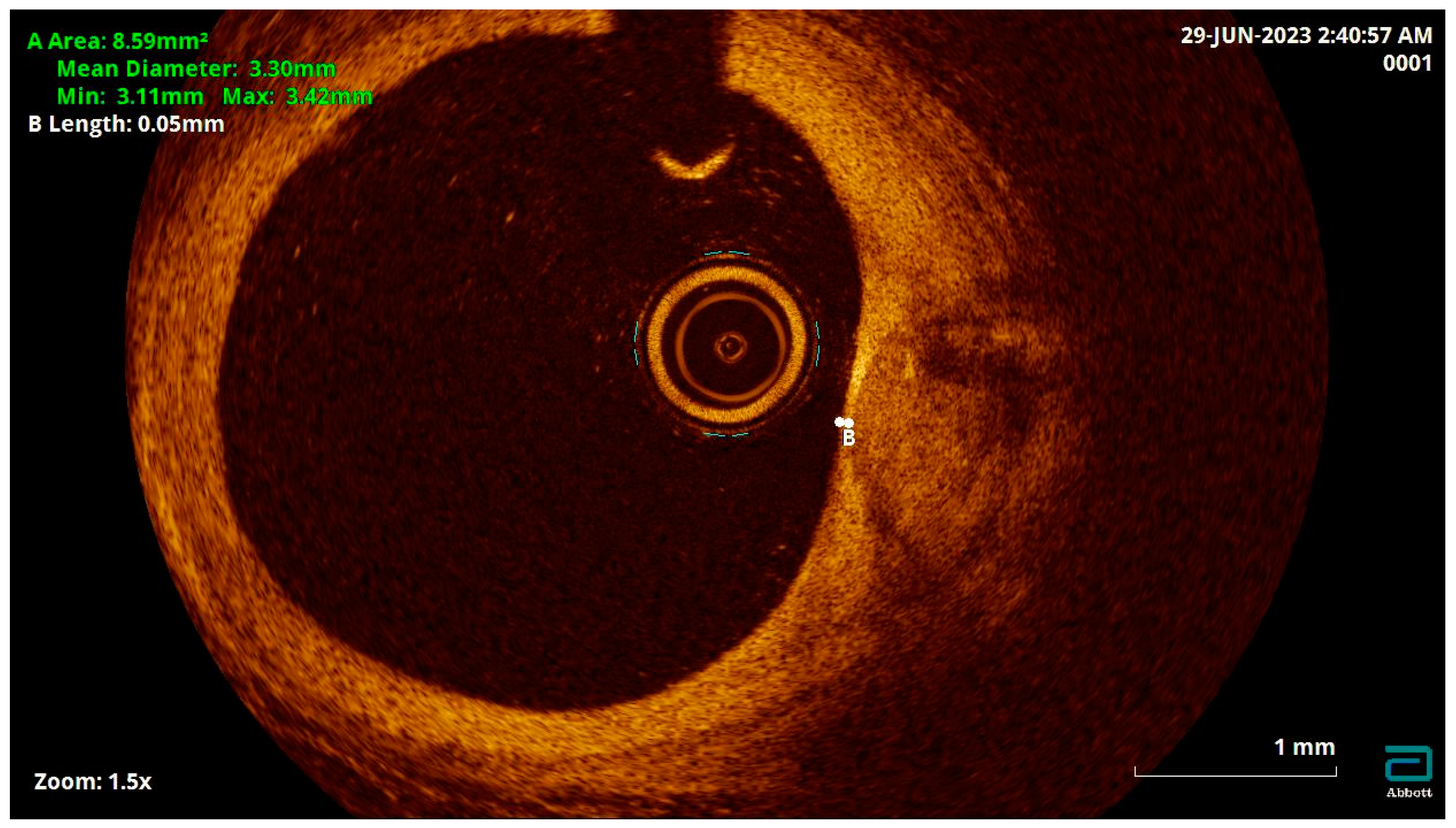
Figure 3.
Manifestations of AP instability on CTCA.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



