
Submitted:
07 July 2023
Posted:
25 July 2023
You are already at the latest version
Abstract
Survivors of sexual and gender-based violence (SGBV) are often hindered in their quest to access quality healthcare. This could complicate the achievement of the laudable SDG Target 3.7. The study used an ethnographic approach to solicit information from health providers, adolescents, and young women (AYW) in 10 communities from Lagos and Ibadan; two major cities in Nigeria. Findings indicated that the structural system of services provided in the health services at the primary healthcare level was limited, which posed a great challenge in AYW’s utilization of services for sexual and gender-based violence (SGBV). Some of the challenges identified by health providers included non-existing counseling services, rehabilitation centers, referral problems, and a lack of training for health providers in handling victims of SGBV. The study provided the context of the health providers’ inadequacy and structural problem of health services in providing comprehensive support services to victims of SGBV like adolescents and young women in the slum setting. This poses a barrier to the utilization of services by the survivors. Necessary inclusive services that will meet the need of the victims of SGBV should be in place at primary healthcare centers close to the people in the community for accessibility.
Keywords:
Health providers
; female adolescents
; slums
; sexual and gender-based violence
; barriers
Background
Young girls around the world, especially female adolescents and young women are at risk of gender-based violence such as physical, emotional, psychological, and sexual violence, often in the hands of their intimate partners. Globally, statistics have shown that nearly one in three adolescent girls (those aged 15-19 years), or about 84 million have been victims of physical, emotional, and sexual violence perpetrated by their husbands or intimate partners. Additionally, about 15 million have experienced forced sex, and one in five women aged 20-24 were married before 18 [1].
The well-being of young people has attracted the attention of policymakers globally in recent times, particularly notable in the Sustainable Development Goals (SDGs) [2] that serve as guidance for the global development agenda. According to the Secretary General of the United Nations, “Adolescents are central to everything we want to achieve, and to the overall success of the 2030 Agenda” [3]. The age of adolescence relates to different experiences and this explains the setting of different programs and interventions targeting this group [4]. Initiatives such as the Global Strategy for Women’s Children’s and Adolescents’ Health 2016-2030 [5], and the WHO Global Accelerated Action for the Health of Adolescents (AA-HA!) [4] have called for research on adolescents’ sexual and reproductive health as well as their experiences of gender-based violence in relation to sexual behavior. Research has shown that in Sub-Saharan Africa, 33% of women aged 15-49 years have experienced gender-based violence (GBV) in their lifetime, and 20% experienced GBV in the previous year [6]. Additionally, 1 in 4 adolescent girls who have been in a relationship had experienced all forms of GBV by their partner [6].
Nigeria has made a commitment to several international initiatives such as the SDGs [2], the International Conference on Population and Development (ICPD) and ICPD Beyond 2014 Follow-Up Action [7], and the Convention on Elimination of All Forms of Discrimination Against Women (CEDAW) [8]. CEDAW in particular, focuses on the health of women and serve as a call to all state parties to eliminate discrimination against women and girls that serves as a barrier in accessing health care. This mandate represent an international bill of rights for women. Despite Nigeria’s commitment, nearly 3 in 10 women have experienced physical violence by age 15 years [9], and 9% had experienced sexual violence in the previous year [10]. Several studies reported on intimate partner violence in relation to adolescents’ health. A study from Calabar among teenage girls found that beating by sexual partners and guardians were prevalent in the study area [11], while a study from the eastern part of Nigeria also found a high prevalence of violence among adolescents, with parents and relatives being the major perpetrators [12]. A study from Lagos among adolescents found that 36% initiated sex by coercion and 64% believed sexual violence was common in the community [13]. This implies violence is present among female adolescents and young women in Nigeria.
Adolescents and young women (AYW) face countless barriers in utilizing services for their health and well-being, when they experience abuse in their intimate relationships with partners, husbands or friends. The first barrier is the culture of silence that is common among women experiencing IPV. Adolescents and young women find it difficult to speak out due to shame, stigma and the belief of keeping quiet about abuse or sexual status that is entrenched in the culture [14,15]. A second barrier in the disclosure of intimate partner violence (IPV) experiences among victims relates to a lack of confidence in the healthcare systems [16]. While, there has been an increase in youth-friendly sexual and reproductive health services that target contraceptive uptake of young people in Nigeria, GBV healthcare services remain lacking.
Extension of youth friendly services to issues of violence among young people will enhance disclosure of gender-based violence (GBV) in intimate relationships. One study has shown the feasibility of doing so. In a family planning clinic that educated about gender-based partner violence found that such interventions helped health providers’ knowledge on GBV. This enabled them to give necessary support to victims of IPV [17]. A majority of AYW confronted with all forms of violence are in dear needs of health care support in the process of recovery. Needed support from the health system for tackling all forms of IPV are; wide awareness, reporting the issue publicly, counselling of victims/survivors, and providing rehabilitation centers for both survivors and perpetrators of violence. Historically, the support services available to adolescents and young women have been informal i.e, families, friends and religious bodies [18]. Unfortunately, this support has not brought necessary changes for mitigating IPV experiences among young women.
The role of health providers
The health care services are essential in mitigating violence among women, especially among the vulnerable ones like female adolescents and young women living in the slum areas. The health care facilities remain one of the key entry points for victims/survivors of violence among AYW to provide diverse support services [19] as to seek treatment for sexual, physical, psychological and other reproductive morbidity due to a violent experience. Although in Nigeria, there have been laudable moves to increase the involvement of health providers in providing adequate services to victims and survivors of gender based violence, the necessary personnel and sustained systems are inadequate or still not in place. A manual by WHO [20] explained the need for health providers’ involvement: identifying a survivor, facilitating access to support services, contributing to preventing the recurrence of violence, integrating into health education and health promotion with clients, involvement in community awareness about human rights and documenting the magnitude of the problem for advocacy. A study argued that a healthcare system should be organized in such a way as to provide a safe environment for victims and survivors of violence. Doing so encourages them to be open to disclose their experiences so that the necessary support can be provided [21]. However, if necessary structures are not in place, this may be difficult to achieve. The political will is important to make health system responses to violence against women and girls achievable. The involvement of stakeholders in advocating for eradication of GBV can be achieved through; leadership in the health sectors, public reports of violence, media coverage, civil society advocacy, and enlightening leaders about the magnitude of IPV and its link to poor health outcomes. These elements are needed for improving the health system’s involvement and commitment [20].
A focus on the role of health system in combating violence against female adolescents and young women has been shown to be largely insufficient in previous research from Nigeria. The majority of studies that addressed specific sectors of the health system (psychology, psychiatrics, counselling and rehabilitation centres) for combating violence are found in high-income countries [16,17,22]. These networks of healthcare entities can responds to GBV experienced by young women and are important to improve the health outcomes of IPV survivors [23]. Studies on GBV from Nigeria have largely focused on issues of justice and the involvement of legal authorities, such as the police [24,25,26]. These institutions have added little in combating violence because matters around IPV are usually regarded as a family affair which can only be resolved within family and not by involving legal authorities.
Intersectionality in service care for GBV survivors
Intersectionality theory is a systemic perspective [27] to understanding how systems of power and privilege constitute people’s experiences of oppression and marginalisation. It addresses various ways of how individuals belong to multiple social positions simultaneously such as: age, gender, ethnicity, cultural background, socioeconomic class, sexual orientation, religious belief, dis/ability status and citizenship status, and how this shapes people to continuously inform positions of social power relations [28,29].
From a health system perspective, intersectionality brings attention to diversity within population groups that were homogenous, giving explanation to nuances surrounding vulnerabilities and the intricate nature of health iniquities [30]. Intersectionality is regarded as an approach to foster multifaceted analysis of power structures and relations that interact to produce and sustain inequalities in various health outcomes [27,30,31]. Talking about the power dynamics, which invariably exist at the centre of violence experience by adolescents and young women. Intersectional violence occurs in terms of place and time as systemic domination and exclusion to form a unique oppression which is typically not detected by traditional methods and modes of interpretation [29]. This focus on power dynamics first encompasses how different experiences of violence create diversity in terms of support (social and health), what is available, and social locations of privilege and disadvantage. Slum dwellers are exposed to poor healthcare services due to low socioeconomic status and environmental conditions. The adolescents and young women are disadvantaged due to location where they reside and the lack of available services. The majority of health professional services (psychologist, psychiatrist, counsellor, and rehabilitation centre) that would give support in the process of recovery from violence are not available in most or any of the primary healthcare facilities in the slums locations in urban cities. These services are essential, to mitigate experiences of IPV among AYW to prevent re-victimization and morbidity among this group. Increased risk of intimate partner violence among female adolescents and young women create differential burdens with less access to formal support services. Each of these services are important although they were less emphasized in the past, especially in the Nigerian context where these services were not sufficient or ever existed and were most needed.
Given the lack of research about health system support towards violence against adolescent and young women, the purpose of this research was to look at the barriers encounter in accessing health services, health providers’ response and challenges face in providing adequate service to victims of GBV in the slums of southwest Nigeria.
Methods
- Study design
The study used different qualitative research methods that were triangulated for cross-validation of research findings. A combination of ethnographic methods, specific observations, informal conversations, key informant interviews, In-depth interviews and focus group discussions were used in eliciting information from 10 health providers, 40 adolescent’ girls and young women. Nine sessions of focus group discussions were conducted from January 2021 to June 2021 in both locations with a minimum of 8 participants in each group. Ethnographic methods were employed to help understand the pathways of care and the daily life experiences of people who lived in the different selected communities of the study. Following-up interview conducted with survivors who attended health facilities for further and in-depth discussion. Selection of the health facilities were purposive as these facilities were situated within the communities of the study locations. We purposively interviewed health providers who were trained in youth-friendly sexual and reproductive health services (YFSRS), as they were closer to AYW and would have provider perspectives on determinants of access. These would reveal their perceptions on the specific challenges and relative disadvantages faced by both survivors and providers in each community.
- Study instruments
A semi-structured interview guide was utilized and was verified by experts from medical sociology, epidemiology. Participants were asked to share their experiences of violence with their previous or current partners, their stories of different intimate partner violence in their relationships, and barriers in reporting to health providers to seek help or support. Health providers were asked to share various interventions/support given to victims of IPV, the challenges they faced in providing adequate support to the victims/survivors and the inadequacy of health system to give support necessary to AYW survivors. Interviews were complemented by observations of primary health care centres in each facility and analysis of centre and facility protocols for violence. Two female research assistants working with local NGOs with Masters’ degrees in Sociology and Demography respectively with experience in qualitative research conducted the interviews alongside the investigator.
- Study setting, and recruitment procedure
The study was conducted in the informal settings of two major metropolitan cities of Lagos and Ibadan in Nigeria from January to June 2021. Lagos is the biggest metropolitan city with a population projected at 9 million, and Ibadan’s population was projected at 3,565,108 making it the third largest metropolitan city as of 2022 [32]. They are the major cities in Southwest of Nigeria with the largest slums settlements. In 2022, the slum population in Nigeria was estimated to be 55% of the total population [33], and the local government area (LGAs) in both locations of the study were identified as major slum areas in Southwest Nigeria. The study locations are characterized as having poor social and health infrastructures, which was more volatile to violence vices and all forms of social anomalies
- Study population
The study scope was limited to female adolescents and young women who resided in the study location and health providers who work in these study areas. The study was conducted in the selected slums communities of Agege in Lagos and Ibadan Southeast LGAs in Ibadan.
- Study population and data collection procedure
The population of the study included AYW and health providers in the study locations. The participants were female adolescents and young women living in the Ibadan Southeast and Agege and Orile-Agege local government areas (LGAs). The selection included young females who were residing in the communities for at least twelve consecutive months and who had experienced violence in the past years in intimate relationships, while health providers were selected based on those who worked in youth friendly sexual and reproductive services in the primary health care facilities situated in each community. The interviews lasted approximately 45 minutes and were audio taped in the open data kit (ODK) platform to guide against loss of interview information and were sent to the server immediately. The participants were duly informed about the purpose of the study and consent forms were signed although some declined signing because they wanted to protect their identities but gave verbal consent.
Data analysis
The objectives of the study guided the analysis of the data. The Open Data Kit (ODK) was used for collection of information through interviews and data were transcribed verbatim. The Atlas ti version 8, a computer-assisted qualitative data analysis software (CAQDAS) was used in sorting the transcripts into codes and themes. Inductive approach through thematic content analysis was developed through in-depth reading of the transcripts and iterations; codes and themes were developed. The main themes were based on the interview guide, but the sub-themes emerged directly from the participants discourse. Additionally, we used framework analysis [34] to extract factors responsible for not reporting abuse or utilizing health services for support and health providers response. The steps recommended by Gale and colleagues were followed: 1) transcription; 2) familiarization with the interview; 3) coding; 4) developing a framework; 5) applying the framework; 6) charting data into a framework matrix; and 7) interpreting the data [34]. These steps guided the analysis with inclusion of observation, informal discussions with respondents, daily debriefing of the research team and reflections after each interview. Reporting was guided by Consolidated Criteria for Reporting Qualitative Research (COREQ-32) [35]. Four categories emerged as follows; 1) factors responsible for not reporting abuse or utilizing health services for support, 2) commonly known support system available for AYW in the event of violence, 3) perceived barriers in accessing services or help by abused AYW and 4) health providers’ response, challenges and involvement on AYW recovery process.
- Ethical approval and consent to participate
Approval for the study was embedded in a larger study from Ethics Committee Northwest and Central Switzerland (ID Number: AO-2020-00028) on 14th, October 2020 and University of Ibadan Research Ethics Committee (ID: UI/EC/20/0513) on 2nd March 2021. It was conducted in accordance with the Declaration of Helsinki. Permission to carry out the study was granted by Ibadan Northeast LGA and from Agege and Orile-Agege LGAs in Lagos. Informed written consent was obtained from participants as part of the approved ethical guidance. Participants agreed to participate in the study and could stop the interview at any time. Confidentiality was assured; all the given names were pseudonyms to protect the participants. All the participants gave their consent by reading and signing the consent form and agreed verbally before conducting the interview.
Results
The results were organized from two perspectives, from the adolescents and young women level, we examined experiences of violence and barriers to reporting, while at the health care providers level, we looked at providers’ responses and challenges in treating GBV victims/survivors.
- A.
- Violence experiences and barriers in reporting
- 1)
- Factors responsible for not reporting abuse or utilizing health services for support
- Culture of silence among survivors of abuse
Given the sensitive nature of sexual violence, especially in informal communities, a culture of silence prevails, forcing the victim to remain silent about the incident violence. Health care providers confirmed the cultural norm that no one should know about the sexual status of victims. This is usually done to protect the identity of the victim and, in some cases, the perpetrator if they are close relatives or personality with power and influence in the community. Likewise, the tendency of married women to conceal their victim status because they are trying to protect their homes and project a perfect image of the home has also exacerbated the culture of silence. A medical doctor in Sango, Lagos, explained that many women did not report abuses against them because of the fear of reprisals for reporting. Another health worker in Dopemu, Lagos reported that it was against the cultural practices to report abuse because the girl (victim) would be the laughing stock eventually if any report is made.
…..constant abuse, but It’s very rare cases where people come and report, so even there’s no forensic evidence, and the fact that, the community they live in, when you report abuse or rape, how are other people going to perceive you? I think it is a cultural issue for the community, the lack of voices. Moreover, people do not believe in the justice system. (Medical doctor, Sango Lagos)
A health care worker further elaborated……
[..] Culturally, it is not so much acceptable, they will believe that, “let us just cover it” so that at the end of the day, they will not be abusing the girl. Socially, they may be embarrassed so they will want to keep it [...]. (KII Health worker, Dopemu Lagos)
- Stigma; being judged, blame syndrome, discourage reporting
The fear of stigmatization was another major discouragement for reporting of abuse by victims. Health workers in Lagos and Ibadan reported that some parents would even discourage their children, who had been victims of abuse from reporting. They feared the reactions of neighbours who might begin to spread the news of the abuse to the utmost embarrassment of the victims
[…] Most of the concern they face is parent discouraging them in reporting, then fear of stigma, fear of being shouted at too, fear of – “I don’t know what-- people around, when they broadcast this issue now, I don’t know what my friends will see me as […]. (KII Health worker, Powerline Lagos).
People will blame them that before they started the relationship, why do not they seek counsel, so if they will have to report. [..]’ ‘[..] Because they are scared of what people are going to say, they are scared of being stigmatized. And again, due to the threat from the perpetrator […]’ (FGD Dopemu, Lagos)
- Fear of re-victimization from perpetrator and lack of confident in justice
Another reason for not reporting IPV is the re-victimization of victims by perpetrators of violence. Since some AYW who are married and have children still want to retain their marriage, the fear of separation and the responsibility of having to take care of the children alone, keep them from reporting violence.
[…] the perpetrators ran away to another environment immediately they commit the crime, they returned to the community with the hope that people would have forgotten the incident. I witnessed a case where a girl was raped of recent the perpetrators were caught and sent to prison, they have been released now. (IDI AYW, Soretire Lagos)
[…] when a woman is going through unpleasant things in her relationship and does not want her home to be separated if she wants to talk about her husband outside, she will say pleasant things even among her family members. A woman whose husband beats in the morning and she visits her family and she was asked how her husband is doing, hope he has stopped beating you? …She will say ‘we had our bath together this morning, he fetched water for me, I was in the kitchen, he bathed and took the child to school” -because she does not want her home to be scattered….so, she will have to bear it […]. (IDI AYW, Oniyanrin Ibadan)
- 2)
- Barriers in accessing support services and help for abuse/victims
- Finances; lack of money by AYW and family:
Finances, is one of the major barriers to accessing health services in the communities studied. Given the socio-economic background of the location of study, most of the respondents reported that cost of services served as a major barrier to accessing support services by victims of abuse. Participants reported that whether victims decided to use the medical facilities or the services of the police, none was available for free as they all cost some money which therefore served as a major barrier to the type of support services they may get. AYW are either trainee, in school or out of school, most whom depend on their partners or parents for their livelihood. This limits the support they received, especially in terms of health services.
[…] most of them go to pharmacist and go to the hospital. If they have money, they will visit the hospital and the one that does not use hospital finds alternative (R2…FGD Oniyarin Ibadan)
[…] I think is that there is no way one will go to the hospital and they will not request for money, so if the person is capable and has the money she will go there (R8…FGD Oniyarin Ibadan)
…..the police cannot render any help, there is no police you go to that you will not spend money so there is no help police can render when it is not that we took a matter there, if she need support from police they cannot help her. And if it is government owned hospital, if anything happens to someone or the child even if you go there and they treat you they will end up collect some change (money) they cannot say someone should go free, so that is how it is (R 5 FGD, Ogunpa Ibadan)
- See below in the result section: Figure 1
- Preferred type of services by adolescents and young women in the community
Most of the participants indicated that they prefer to go to a private hospital if they have the money to do so, as a result of the convenience and promptness of their services.
[…] When it comes to rape, they go to private hospitals but not for beating. However, if is forced sex from their sexual partner, some people have nurses they confide in who comes to treat them at home. (Resp. 4, FGD AYW Sango Lagos)
[…] I heard the sound of bottle on my head that day. As I looked back I saw the person I was dating around this area, he lives around here. I suffered that day as blood was gushing out of my body, the cloth I wore turnedto blood all of a sudden… it was Group Medical (hospital) that admitted me […]’. (IDI AYW, Oniyarin Ibadan).
When it comesto pregnancy they go to the hospitals, it could be some government, or private depending on how much they can afford, but for beatings it usually chemist, and rape is definitely private or a nurse. (IDI AYW, Dopemu Lagos)
- 3)
- Support system available for adolescents and young women in the event of violence
In two of the ten communities surveyed, there are other support services that have been organized by community groups and health care providers.
[….] we have another support service within the community group. Which is actually a community group, it was founded by the Chamen’s foundation. It comprises of the police, health workers, community people like the Alfa, imams and pastor they form a social community network that fight against abuse. (Health provider, Sango Lagos)
[…] I have also seen a scenario by—a girl came to us and she told us that she was still a virgin though but she wants to do family planning because she knows that she can be raped at any time and she does not want to be pregnant because she understands the environment that she lives in. Even her grandmother consented to it because I was like—so the grandmother gave us the consent that she is actually right. So environment too. (Health provider, Powerline Lagos)
[….] Like I said the other time, okay I have remembered “The child Protection Committee” that has been set up within the community. We do not have it in every community but we have it in few communities like KwaKwa Uku community and few other communities also. Child Protection Association so it is like a link within the community to fight such things (Health Counsellor, Agege Lagos).
B. Providers responses and challenges in treating gender-based violence victims/survivors
1). Health providers’ response and involvement in adolescents and young women’s health decision
- Health care providers’ attitude to AYW and prompt intervention
The attitudes of health workers reportedly varied by the type of facility used by the victims Participants reported that in most secondary or tertiary hospital, health care providers were willing to find out what was responsible for the pain and offer a solution or make referrals. This was unlike private hospitals where health workers did not care about what happened to the victim rather than given treatments. Ironically, most victims of violence who are more financially stable preferred to patronized these private hospitals.
[…] Adolescents that will go to hospitals go to private hospitals, they cannot go to general hospitals because they will counselthem there and they are not comfortable with it. General hospitals will want to get to the root of the matter, for example, maybe you go there and tell them your husband beat you and from there they will start probing wanting to know what is going on within the person’s family unlike private hospitals. They are just after their money, just pay them and they will treat you without story, they are less concerned about what is happening to you, just give them their money and you are good to go […]. (Resp. 3, FGD AYW Sango Lagos)
[…] They come to us. We have a contact with Lagos State where we can contact them and get in touch. We have some NGO’s that we work together like Hello Lagos. Hello Lagos has their branch at LASUTH, also at Agege too. So when such case is been found, it’s either I report to Hello Lagos LASUTH or I put to my office directly and they take it up, you know, ask the girl to come, fix her up. Then go through the protocol, then to Lagos State Domestic Violence Respond Squad […]. (Health provider, Powerline Lagos)
- Support by health providers for victims that utilizes service
In most cases, health care providers first offered counseling and then referred them to places where they could get treatment and care, and in cases of very severe violence, they were referred to places where they could actually get justice.
‘[…] Like the one I referred to the other time the girl, seventeen years old was actually with her estranged boyfriend and she was stabbed with bottles on her hand and she had a baby and the baby was subtly taken away from her and all those stuffs. The mother came in and I had to refer the mother to the hmmmm-there is a center in the maternity that deals with violence […]’. (Health Counsellor, Agege Lagos).
‘[….] So whenever she comes for clinic, she does not interact, laugh nor smiles. Then one day, I called her, and asked her what the problem is, it was there she narrated the story that the mother in-law is not treating her well and her parent had warned her never to come back home. UCH organized one program/project on adolescents’ pregnancy. I had to inform them; they went to the place and settle the matter because I noticed she is already becoming depressed […]’. (Matron Ayeye, Ibadan).
‘[…] Unless only if the victim is injured, we take it up just to save the life of the girl, because sometimes if we refer them to ‘Adeoyo’ hospital, they we not go. So, we try and do some tests for them, like HIV test and give them and if there is none, we move further to pregnancy test, that is our limit, we don’t have any power other than that’. (Matron Oniyanrin Ibadan)
- Health care providers’ challenges in supporting violence victims/survivor
Health care providers were concerned about the limited support they could provide to victims and survivors, as a result of the limitations presented by available tools and professionals the government provided with in primary health care centers in the community.
[…]There are no social workers in this community, if there were, they would be confronted with such problem as the woman who said she wanted to commit suicide […]. (Matron Ayeye Ibadan)
‘[…] In every local government, I believe there is a need to have a rehabilitation center for abuse or cases of abuse. Like now, I have case of abuse and I am going to Ikeja general hospital […]’. ‘[…] the survivors of GBV you can counsel them like I said but the treatment would not be entirely 100% fixed. The treatment would not be that comprehensive within the primary health center within the locality because we do not have a particular unit of it, so, if such office that is actually responsible for just gender-based violence for young people, it would actually go a long way […]’. (Health providers, Agege Lagos).
[….] is that most of these offenders we do not take them to rehabilitation homes before they are being jailed to prison or releasing them back into the community. They need to undergo rehabilitation; we need to have rehabilitation center probably within the local government at least two or three centers within the local government (Health Counsellor, Agege Lagos).
- Health providers’ professionalism in treating victims of GBV
Health providers need to observe and monitor patients who have been victimized in order to promptly provide the necessary support. It was evident that there were no professionals health providers such as psychiatrists, psychologists and counselors in the study sites to assist abused AYW. Fortunately, primary health care facilities are closer to community members.
[….] Like the one I referred to the other time the girl, seventeen years old was actually with her estranged boyfriend and she was stabbed with bottles on her hand and she had a baby and the baby was subtly taken away from her and all those stuffs. I had to refer the mother to the hmmmm….there is a center in the maternity that deals with violence also….(Health Counsellor, Agege Lagos).
[….] The major reasons why they need to go through this support service is to get better services. Better services in terms of psycho-social support services, better services on health, better services in managing the victims and the perpetrator also. Better services to manage the girl child to be able to fit in back into the community […] (Health provider, Agege Lagos).
[…] Like I told you that, we don't have much to meet, we don't have solution, we just counsel the person to voice out to look for solution, like me now. I only advised them to please voice out to look for solution […]. (Matron Ayeye Ibadan)
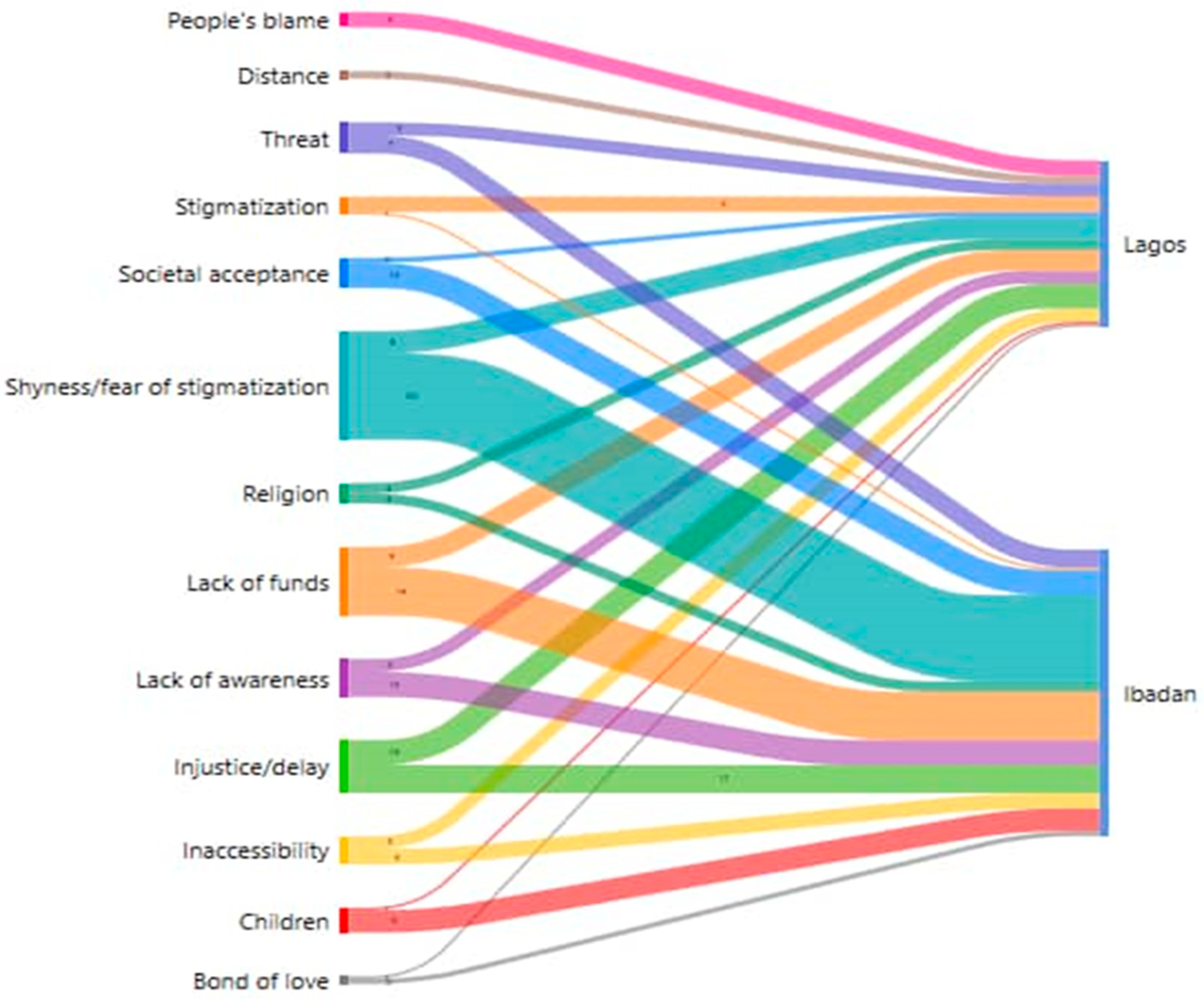
Figure 1.
Barrier in accessing health facilities for treatment of GBV.
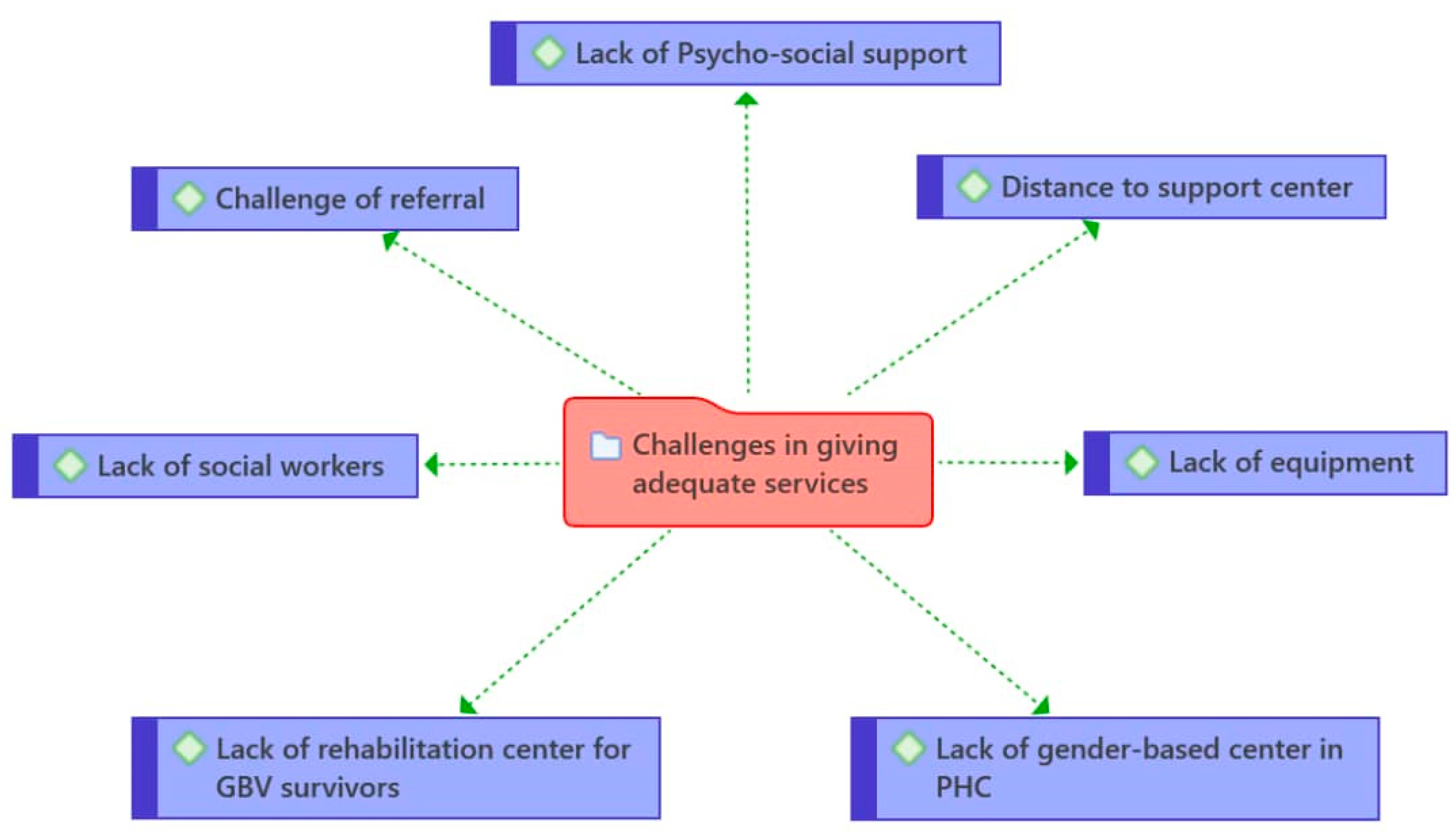
Figure 1 shows the visualization of barriers to treatment encountered by adolescents and young women and the extent by locations. Although, the two study sites are in urban cities, culture, norms and individual perspectives of the victims limit access to treatment for intimate partner violence. For example, more AYW in Ibadan than in Lagos had difficulties accessing health care facilities, due to stigma from friends, neighbors and possibly health providers. Lack of financial resources was another barrier in accessing the health system in Ibadan compared to Lagos. All of the barriers identified in Figure 1 were different in the two locations.
Discussion
This ethnography study set out to understand barriers faced by adolescents and young women in accessing health facilities for treatment on GBV, and the perspective of health providers on; access, previous support rendered by providers and challenges in giving necessary support to victims/survivors. The findings in this study showed a range of factors operating at individual and community and institutional or health system levels that influenced AYW’s decision of choices on health facilities that meet their needs. The culture of silence is one of the reasons mentioned as a barrier of not reporting, as speaking out about sexual status bring about shame, stigma, being-judged, blame syndrome, lack of support from the community members and fear of re-victimization from the perpetrators. This is consistent with previous studies on the decisions of survivors of IPV either to keep silent about their experience or to run away from the relationship [14,15]. The findings affirm the extent of interactions which are determined by the social/economic status present as a pathway of vulnerability or privilege among AYW (individuals) and institutions and structures (health providers/health facilities). The age group of AYW put them in a disadvantaged group that limited the extent of access to support services, which may not be the case for older women. For instance, AYW were seen as children who in the first place should not have a partner or experience IPV, as this limits their abilities of approaching health facilities for support. As the results showed, they would rather prefer to go to a pharmacy store or private clinic for treatment, which offers limited services.
From the providers’ perspectives, since there were no special clinics for young people experiencing intimate partner violence as there were youth-friendly sexual and reproductive health in primary healthcare services in the community. This limited the confidence of AYW in approaching the health providers and the likelihood of expectations of care. This result corroborated with a study from Switzerland on migrants who experienced GBV, [16] lacking confidence in approaching healthcare systems as major barriers in the disclosure of GBV. Incorporating GBV services in the form of YF-SRH clinics could be one of the approaches to help AYW disclose experiences of IPV in their intimate relationships, as this will give free access and trust the health system, assure confidentiality. It also gives reassurance of access to health professionals such as psychiatrists, psychologists, and counsellors for recuperating the victims/survivors. A study on implementation of family planning clinic-based partner violence supported that the system-level barrier confronted by providers limited the extent of support they could offer to victims/survivors of IPV [17].
The disadvantage in providing support to victims of violence are more pronounced in primary healthcare facilities, as most of the cases were being referred to state hospitals for proper treatment and further interventions. It was only one of the communities that had a gender-based violence office which is maternity at Sango Agege LGA. Even with that, the majority of cases on IPV were being referred to Lagos State University Teaching Hospital (LASUTH). Most of the AYW do not go to LASUTH nor University of Ibadan College Hospital (UCH) when referred due to distance and complex of structure. It was evidence that the providers were displeased with the process and inadequate support given to victims, and the concern for limited reports were due to process-related challenges. A study by Garcia and others [21] seems to be divergent according to the findings, as most of the primary healthcare centers in the study communities were not well structured to offer GBV services in such a way that will make AYW disclose on IPV experiences, as these were not within their reach. Of course, this is compounded in slum locations as those in the city are likely to enjoy state facilities compared to those in the disadvantaged regions like in our study area. The role of health providers cannot be overemphasized in mitigating the experiences of IPV among AYW in the informal setting. Nonetheless, the WHO manual on Health Systems Response [20] on IPV does not categorize facility locations, therefore this needs a second look and political will from the state party to provide the availability of access to health professionals especially at the grassroots level, where many vulnerable AYW reside.
In this study, the use of intersectionality theory allowed us to see from diverse angles beyond individual factors (AYW and health providers), and how this shapes poor health outcome in the slum communities. The homogeneity of experiences is prevented due to locations (poor access among AYW) as these may not be the same with those in the city closer to tertiary health institutions. The study revealed multiple communities and structures of power that interacted in health systems, which produced multiple levels of disadvantage and privilege among AYW. It exposed the link between primary and tertiary healthcare services in the slum locations, the barriers due to access-(age, norms, value, community perceptions and health systems) and political will for availability of health professionals’ services on GBV at the local government level that will remove health inequalities [36]. The significance of this study, first are the low reports of experiences of IPV victims, are due to inadequate support from the primary healthcare system in the community in terms of professionals (psychiatrists, psychologists, counsellors) beyond doctors and nurses diagnostic treatments. The cultural norms of silence, not revealing the sexual status which prevent victims/survivors of reporting IPV experiences. This is due to awareness of the IPV impact and no evidence of justice, which make perpetrators walk freely after the incident of violence in the community. The trauma of violence does not vanish from the memories easily among the survivors, routine counselling and professionals support for the survivors along this journey will help avoid re-victimization.
- Strengths and limitations
The strengths of this study were to see how victims/survivors of IPV encountered barriers in accessing support from health system and the available support received. The institutional structure and cultural barriers encountered in accessing the facilities, and the reporting and adequate care received from health professionals were completely absent in the study locations. This study also revealed the need for health professionals i.e. the psychiatrists, psychologists and counsellors beyond doctors’ and nurses treatments are needed to enhance full support for the survivors. However, some limitations need to be discussed. First, our findings are based on self-reports from the survivors and health providers and we cannot control the level of bias as AYW with negative experiences of IPV may have great challenge to share or discuss them. This were encountered during our data collection, the emotional trauma of bringing back old painful experiences of IPV. Second, our study was not able to interview health professionals except for doctors and nurses, as these other professionals were not present in the facilities within communities of our study locations. We also did not ask the participants on their needs for health professionals in the process of recovery or if a lack of health professionals stood as a barrier in utilizing health services. Our results should be interpreted with care, as this is only applicable to the locations of the study and should not be generalized, but to show a pathway in which AYW could utilize health facilities, and the provision of all the necessary arms of the health system are in place in primary health centres.
- Implications for policy
Health providers need retraining on how to handle AYW who are victims of abuse or intimate partner violence and prompt interventions are required by providers to mitigate their pain. In addition, psychologists, psychiatrists, periodic counselling for survivors and rehabilitation centers for survivors, and for men/perpetrators, were not well positioned to provide support to victims of violence in the health system. A support system for GBV victims/survivor is either inadequately developed or was not available in primary health care centres we investigated. While conducting an intensive study across all of Nigeria is infeasible, we believe that the overarching findings are transferable [37] to other settings as well. Hence, the need for appropriate intervention to make health system accessible and available for support to eliminate violence among female adolescents and young women.
Conclusion
As demonstrated by this research, adolescent and young women in an informal areas are particularly vulnerable to the horrific effects of intimate partner violence. As illustrated here, a culture of silence and the lack of adequate social policies contribute. Further, a lack of training and lack of a broader network of providers who can support the victims of IPV are the consequence of policy priorities and decisions that can be changed. Education and empowerment of adolescents and young women are fundamental in disclosure of IPV. Health providers should be trained to identify and support survivors and strategies to address violence should be integrated into services, like youth-friendly SRH, as a way forward to eliminate IPV or repeat victimization among young people. Decentralization of gender-based unit at primary healthcare level give AYW access to report and get necessary care for IPV. Beyond a reactionary, curative approach, health providers need to play a preventive role through education, advocacy, and coordination of interventions at the community level.
Author Contributions
Olutoyin O. Ikuteyijo collected, analyzed and interpreted the interview transcripts and wrote the first draft. Akanni I. Akinyemi supervised the data collection and reviewed the manuscript. SM supervised the interpretation of data, Andrea Kaiser-Grolimund and Michael D. Fetters critically reviewed the manuscript. All authors read and agreed to the published version of the manuscript.
Funding
This study was part of the larger study on adolescent violence experience in the slums area in Nigeria funded by BOTNAR Foundation and the European Union’s Horizon 2020 research and innovation program under the Marie Sklodowska-Curie grant agreement No. 801076, through the SSPH+ Global PhD Fellowship in Public Health Sciences (GlobalP3HS) of the Swiss School of Public Health. The sponsors had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Acknowledgments
We thank the health directors from Ibadan Northeast and Agege LGAs for giving us the opportunity to speak to the Matrons, Doctors and Health Counselors in the Primary Health Care facilities. We also thank the female adolescents and young women for their insights into their personal experiences on IPV. We thank Damilola Amire, Dimeji Ogunoye, Dayo Ayodele, Bisola Ekanem and Oluwakemi Olateju who supported in data collection. We also thank Karen Maigetter for taking time to edit the manuscript.
Availability of data and materials
The dataset presented in this article are not publicly available, because it contains information that could compromise the privacy of the interviewees and a breach of agreement. Request to access the dataset can be directed to the corresponding author.
Conflicts of Interest
The authors declare they have no conflict of interest.
Appendix A
Figure A1.
References
- United Nations, UN special representative of the Secretary-General on violence against children. Accessed October 2022, https://violenceagainstchildren.un.org/content/girls. 2021.
- United Nations, Transforming our world: the 2030 Agenda for Sustainable Development. Department of Economic and Social Affairs Sustainable Development. Accessed October, 2022 https://sdgs.un.org/2030agenda. 2015.
- United Nations, Global Strategy for Women’s, Children’s and Adolescents’ Health (2016-20230). Accessed October, 2022 https://globalstrategy.everywomaneverychild.org/pdf/EWEC_globalstrategyreport_200915_FINAL_WEB.pdf. 2015.
- World Health Organization (WHO), Global accelerated action for the health of adolescents ( AA-HA!): guidance to support country implementation. Accessed October, 2022 https://www.who.int/publications/i/item/9789241512343. 2017.
- World Health Organisation (WHO), Global Strategy for Women’s, Children’s and Adolescent’s Health 2016-2030. Accessed October, 2022 https://globalstrategy.everywomaneverychild.org/. 2015.
- World Bank, Violence against women and girls – what the data tell us. https://genderdata.worldbank.org/data-stories/overview-of-gender-based-violence/. 2022.
- UNFPA, ICPD Beyound 2014, High-Level Global Commitments: Implementing the Population and Development Agenda. Accessed October, 2022 https://www.unfpa.org/sites/default/files/pub-pdf/ICPD_UNGASS_REPORT_for_website.pdf. 2016.
- United Nations, Convention on the elimination of All Forms of Discrimination against Women New York, 18 20 December 1979. United Nations Human Rights office of the high commissioner. Accessed October, 2022 https://www.ohchr.org/en/instruments-mechanisms/instruments/convention-elimination-all-forms-discrimination-against-women. 1979. 18 December.
- ICF, N.P.C.N.a. Nigeria Demographic and Health Survey 2018. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF. 2019.
- ICF, N.P.C.N.a. Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF. 2013.
- Egbe IB, A.O., Itita EV, Patrick AE, Bassey OU. Sexual Behaviour and Domestic Violence among Teenage Girls in Yakurr Local Government Area, Cross River State, Nigeria. Acad. J. Interdiscip. Stud. 2020, 9.
- Okey-Orji S, A.E. Prevalence and Perpetrators of Domestic Violence against Adolescents in Rivers State. Arch. Bus. Res. 2020, 8, 1–14. [Google Scholar] [CrossRef]
- Odeyemi K, O.T., Ogunnowo B, Onajole A., Sexual Violence Among Out-of-School Female Adolescents in Lagos, Nigeria. SAGE Open 2016, 6.
- Adegbite, O. and A. Ajuwon, Intimate partner violence among women of child bearing age in Alimosho LGA of Lagos State, Nigeria. African Journal of Biomedical Research 2015, 18, 135–146.
- Herrero-Arias, R., et al., Keeping silent or running away. The voices of Vietnamese women survivors of Intimate Partner Violence. Glob Health Action, 2021, 14, 1863128. [CrossRef]
- Rodella Sapia, M.D., et al., Understanding access to professional healthcare among asylum seekers facing gender-based violence: a qualitative study from a stakeholder perspective. BMC Int Health Hum Rights, 2020, 20, 25. [CrossRef]
- Miller, E., et al., Implementation of a Family Planning Clinic-Based Partner Violence and Reproductive Coercion Intervention: Provider and Patient Perspectives. Perspect Sex Reprod Health, 2017, 49, 85-93. [CrossRef]
- Le Roux, E., et al., Getting dirty: Working with faith leaders to prevent and respond to gender-based violence. The Review of Faith & International Affairs. 2016, 16, 22–35.
- UN Women, Handbook for national action plans on violence against women. Accessed October 2022 https://www.unwomen.org/sites/default/files/Headquarters/Attachments/Sections/Library/Publications/2012/7/HandbookNationalActionPlansOnVAW-en%20pdf.pdf. 2012.
- World Health Organization, Strengthening health systems to respond to women subjected to intimate partner violence or sexual violence: A manual for health managers. Access August 2022 https://apps.who.int/iris/handle/10665/259489. 2017.
- García-Moreno, C., et al., Addressing violence against women: a call to action. Lancet, 2015, 385, 1685-95. [CrossRef]
- Briones-Vozmediano, E., et al., Professionals' perceptions of support resources for battered immigrant women: chronicle of an anticipated failure. J Interpers Violence, 2014, 29, 1006-27. [CrossRef]
- Ogbe, E., et al., The potential role of network-oriented interventions for survivors of sexual and gender-based violence among asylum seekers in Belgium. BMC public health. 2021, 21, 1–15.
- Fawole, O.I., A.J. Ajuwon, and K.O. Osungbade, Evaluation of interventions to prevent gender-based violence among young female apprentices in Ibadan, Nigeria. Health Education, 2005.
- Wada, O.Z., et al., Gender-Based violence during COVID-19 lockdown: case study of a community in Lagos, Nigeria. African Health Sciences 2022, 22, 79–87. [CrossRef]
- Azuh, D.E., et al., KNOWLEDGE AND PREDICAMENTS OF GENDER-BASED VIOLENCE IN SOUTHWEST NIGERIA. Proceedings of ADVED, 2021. 2021(7th).
- Crenshaw, K. Mapping the Margins: Intersectionality, Identity Politics, and Violence Against Women of Color. Stanford Law Review. 1991, 46, 1241–1299. [Google Scholar]
- Sokoloff, N.J. and I. Dupont, Domestic violence at the intersections of race, class, and gender: Challenges and contributions to understanding violence against marginalized women in diverse communities. Violence against women 2005, 11, 38–64. [CrossRef] [PubMed]
- Grzanka, P.R. From buzzword to critical psychology: An invitation to take intersectionality seriously. Women & Therapy 2020, 43, 244–261. [Google Scholar]
- Kapilashrami, A. and O. Hankivsky, Intersectionality and why it matters to global health. Lancet 2018, 391, 2589–2591. [CrossRef] [PubMed]
- Kapilashrami, A. What is intersectionality and what promise does it hold for advancing a rights-based sexual and reproductive health agenda? BMJ Sex Reprod Health, 2019.
- Worldometer, Elaboration of data by United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects:The 2019 Revision. Accessed October, 2022 https://www.worldometers.info/world-population/nigeria-population/. 2019.
- UN-HABITAT, Population living in slums (% of urban population)-Nigeria. United Nations Human settlements programme. Accessed October 2022 https://data.worldbank.org/indicator/EN.POP.SLUM.UR.ZS?locations=NG. 2016.
- Gale, N.K., et al., Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol 2013, 13, 117. [CrossRef] [PubMed]
- Tong, A., P. Sainsbury, and J. Craig, Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care 2007, 19, 349–357. [CrossRef] [PubMed]
- Kapilashrami, A. and S. Marsden. Examining intersectional inequalities in access to health (enabling) resources in disadvantaged communities in Scotland: advancing the participatory paradigm. Int J Equity Health 2018, 17, 83. [CrossRef] [PubMed]
- Fetters, M.D. The mixed methods research workbook: Activities for designing, implementing, and publishing projects. 2020: SAGE Publication.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



