
Submitted:
24 July 2023
Posted:
25 July 2023
You are already at the latest version
Abstract
Attack on health has become a significant concern for non-belligerents of war, including healthcare personnel and facilities as witnessed in the ongoing Sudan conflict. About 1.5 billion people living in fragile and conflict-affected settings (FCAS) have a heightened need for essential health services. Conflicts often lead to the disruption of building blocks of health systems, lack of access to health facilities, failure of essential medical supply chains, the collapse of political, social and economic systems, migration of health care workers, and upsurges in illness. While health indicators often decline in conflict, health can also bring peace and harmony among communities. Investment in health systems and health diplomacy is a neutral starting point for bringing peace and mitigating conflicts. The international commitment towards Sustainable Development Goals (SDGs) provides the impetus to emphasize the relationship between health and peace with the amalgamation of SDG 3, SDG 16, and SDG 17. The inspection of how health should be used as a ‘tool for peace’ and not as leverage during the war must be reiterated by international institutions.
Keywords:
health diplomacy
; sustainable development goals
; peace
; Sudan
; fragile
; conflict-affected countries
; healthcare
1. Introduction
As an area of study and practice, health diplomacy has gained prominence over the years and highlights the interplay between health and international relations. The field has become essential over the years due to the emergence and reemergence of diseases and global health challenges. The vulnerabilities in a health system that have been exposed due to globalization must be addressed before a new pandemic or other crises arise. Health is no longer a concern to be addressed by a particular nation but for the whole world to collectively work together and tackle. With the heightened need for health discussions in the area of high political endeavour (national and international security), health diplomacy has become critical in policy deliberations [1]. This becomes especially important in the case of fragile and conflict settings where “over 80 per cent of major infectious diseases and epidemics occur” [2].
The threat and impact of a conflict's indiscriminate nature on people's well-being is multifold. A conflict usually comes with a dearth in the supply of essential goods and services and with people fighting for them to survive the volatile conditions. A functioning healthcare system that delivers health goods, services, and infrastructure is one of the critical elements that people require to support themselves. However, its importance in a conflict has made it a vulnerable point for belligerents to attack and leverage on it. The attacks on healthcare centres and professionals prevent critical supplies, including medicines, surgical equipment, and trained staff. The combined effect of poor public health and conflicts also deprives the effective functioning of other services. While such attacks have immediate ramifications in the form of a lack of availability of treatment for the victims of the attack, in the long run, the destroyed health infrastructure deprives people of good health and could compound into an economic downturn [3]. Thus, it has become imperative to understand how a resilient health system can be built that can withstand the negative externalities of a conflict.
The need for resilient health systems to ensure the continuity of essential health services led to the World Health Organization (WHO) health systems building block framework designed to strengthen its constituents. The framework conceptualizes six building blocks for the health system, which are: (i) service delivery; (ii) health workforce; (iii) information; (iv) medical products, vaccines, and technologies; (v) financing and (vi) leadership and governance [4]. These blocks are expected to address concerns such as quality and safety, access, and scope of health systems to improve efficiency and ensure health equity. These blocks further create a common and shared understanding of factors needed to build a resilient health system. However, the major hurdle for countries to accomplish this is the complex and volatile environment in which health systems function, especially in conflict settings.
As the world has become more interconnected in the last few decades, the conflict in one region has repercussions across the world. This calls for collective action from the international community to enhance cooperation to maintain peace and harmony around the world using various policy tools such as health diplomacy. Thus, this paper attempts to understand how health diplomacy can enable the building of such resilient health systems in conflict settings. We critically analyse how health was affected in different conflict settings and later highlight the importance of the current situation in Sudan. Subsequently, we discuss how health diplomacy has been used in other conflict regions and how a few hurdles are required to be parred to build resilient health systems to achieve the Sustainable Development Goals (SDGs) of health, peace, and partnership (SDG 3,16, and 17).
2. Attack on Health in Conflict Settings
The functioning of an essential sector such as health has time and again been witnessed to be in jeopardy in a conflict region. With health being imperative for the stability and security of a nation’s well-being, it is an essential sector for belligerents to use as a war tactic. The attack on health in conflict settings can be majorly subdivided into five categories: the attack on i) health facilities, ii) health professionals and support staff, iii) patients, iv) medical transport, and v) health facilities [5]. Attacks on health facilities mainly include damage to physical facilities such as clinics, hospitals, laboratories, and drugstores. The violence against healthcare professionals and support staff undertaking medical functions includes killing, kidnapping and detention from performing their duties. During an attack, the patients and the wounded could also be targeted with disruption of treatments and denial of medical assistance.
Further, the attacks directed towards medical transport, such as strikes on ambulances and trucks, aircraft or vessels ferrying medical supplies, have large repercussions. Violence against health also includes misusing health and medical facilities for storing arms or using these infrastructures as a shield against offensives. Such instances lead to the compromise of neutrality of these structures otherwise held [6,7]. The figure S1 in the supplement depicts the distribution of attacks on health facilities, health transport, and health workers in conflict-affected states in 2022 [8]. The tables S1 and S2 in the supplement provide the number of hospital beds (per 10,000 population) and nurses and midwifery personnel (per 10,000) that are available in these areas [9,10]. The data suggests that healthcare facilities and workers have been primary victims of the attack on health. There are also a low proportion of hospital beds and nurses due to the volatile and uncertain working environment in conflict settings. These inadequacies of health facilities and services have pushed these countries to become ‘medical desserts’ [11].
Healthcare in conflicts has been under the continuous threat of sabotage irrespective of who the belligerents of a particular conflict are. Kosovo witnessed prolonged violence against health, where professionals were attacked before, during, and after the conflict. Before the beginning of the widespread attacks, the Albanian doctors were said to be systematically tormented by the Serbs as their medical training was eliminated and, in some cases, were subject to mass firings [12]. The war crimes associated with the conflicts also record the Serb policemen and soldiers disguising themselves as health professionals to create fear among ethnic Albanians. It was also observed that anti-aircraft weapons were installed in medical facilities while its basements were used as armouries. Even after the conflict ceased, the deep-rooted divide between ethnic Serbs and Albanians remained in Kosovo, where these populations continue to receive health care from practitioners from their respective ethnicities. The two groups of practitioners have little to no contact between them, with a constant fear of new tensions stemming [13].
Other examples also include Afghanistan, which has undergone several transitions due to the powerplay of multiple superpowers. In the past two decades, the central conflict was against terrorism, where heavily equipped and battle-trained soldiers from multiple countries and Afghan allies were up against several rebel groups such as the Taliban. In the ensuing war, the rebel groups used ambulances to attack the opposite camps and civilian sites in major cities, such as the 2011 Kandahar bombings [14]. The protracted conflict against the elusive rebel fighters also adversely impacted the already damaged healthcare facilities. The presence of Taliban fighters within the civilian society forced multiple raids on clinics with the hope of finding traces. The Government and international allies also ordered the functioning healthcare staff to report about the Taliban movements. However, this move was counterproductive as doctors and medical staff were kidnapped to treat the wounded. During Hamid Karzai’s Government, multiple instances were reported where healthcare professionals were threatened and forced to shut their clinics [15]. This dented the effectiveness of using humanitarian assistance to win the legitimacy of the Government among the Afghans.
The Democratic Republic of Congo (DRC) also accounts for violence against health by armed groups to further their political agenda. The Masisi region witnessed government attacks on measles vaccination camps where the members of the rebel group, Democratic Forces for the Liberation of Rwanda, had assembled. The government attacks were carried out despite permissions and security assurances taken by the Médecins Sans Frontières (MSF), the camp’s organiser. Following this, the region witnessed widespread violence, where entire villages were forcibly evacuated and set on fire [16]. This situation provides an example of how a health objective was used as bait to advance political and military goals.
Another example which helps to understand threats of attacks on healthcare in conflict is from Somalia. During the 2007 Ethiopian occupation of the city of Mogadishu, it was alleged that Ethiopia indulged in intentional damage to hospitals. The attacks were carried out under the pretext of these facilities treating insurgents [17]. The Ethiopian Army also placed roadblocks and conducted extensive checks restricting medical activities. However, interviews with the hospital staff later claimed that the Ethiopian officers wanted to use the hospitals as a vantage point [18].
Having been aware of the significant challenges of healthcare systems and workers, the international community has enacted multiple laws for their protection. According to the existing protection laws, medical personnel assigned exclusively to medical duties must be respected and protected as stated in Rule 28 of International Humanitarian Law (IHL), Article 24 of the Geneva Convention, and Article 15 of the Additional Protocols [19,20,21]. Medical units, including hospitals and related facilities, are to receive protection under all circumstances as per Article 19 of the Geneva Convention, Article 12 of Additional Protocol I, and Article 11 of Additional Protocol II [22,23,24]. Further, it requires the belligerents to ensure the medical units are not situated near any kind of offensives during a conflict.
However, hospital buildings have been used to store weapons and facilitate attacks, compromising healthcare neutrality. Such instances were reported in Palestine, where Israel claimed to have bombed medical facilities in Gaza because they housed militants and arms [25]. While there was an international condemnation criticising Israel Defence Force (IDF) for their indiscriminate attacks, the officials on their part claimed that groups like Hamas purposefully chose civilian institutions for military operations as they provide a “shield” from IDF [26]. A press release by the UN in 2014 on this issue stated that rockets and other weapons were being stored in schools and hospitals in Gaza [27]. Thus, the laws that intend to protect healthcare workers and units are challenged in such scenarios as the facilities were utilised beyond their humanitarian duties.
3. International measures against attack on health
In 2016, the former president of the International Committee of the Red Cross (ICRC), Peter Maurer voiced his concern about the 2400 attacks on healthcare personnel and facilities in 3 years spread across conflict regions such as Afghanistan, Central African Republic, South Sudan, Syria, Ukraine and Yemen [28]. The need for reforms in regulations for insulating healthcare conflict settings was also recognized by the UNSC in 2016, which unanimously adopted Resolution 2286, that strongly condemned attacks on wounded and sick medical personnel and facilities [29]. The council emphasized that all parties involved in the armed conflict must adhere to the International Humanitarian Law (IHL) to facilitate medical personnel's safe and unrestricted passage. The Council urged its member states to conduct independent investigations on violations of IHL related to the protection of personnel engaged in medical duties and called to act following domestic and international law to help reinforce preventive measures and ensure accountability by the state.
The adoption of the resolution provided the impetus to establish a Surveillance System for Attacks on Health (SSA) by the WHO in 2017. Despite these developments, since 2016, there have been a combined 4787 violent attacks on healthcare personnel, patients, hospitals, transport, and supplies, with 1150 deaths and 2873 injuries across 18 countries and territories [30] (Figure 1). According to a study report by Syrian American Medical Society, Syria alone claimed that the rates of attacks after the resolution’s passing have increased by 89 per cent [31]. Further, the report stated that the increased attacks in Syria could be linked to the Russian intervention in Syria and the Syrian government’s offensive in Aleppo. Additionally, an issue of concern was that out of 168 documented attacks on healthcare between June and December of 2016, 164 were recorded to be committed by the Syrian government and its allies [32]. Thus, while the resolutions and regulations by the international community have been in place, giving the responsibility to member states to investigate violence against health has turned out to be ineffective.
While Non-Governmental Organizations (NGOs) and international societies are continuously involved in providing humanitarian aid and support in conflict settings, they must also examine the possibility of providing dedicated psychological support for medical staff engaged in these areas. The trauma of war could adversely affect doctors and humanitarian support providers, especially if they belong to different countries or strata, making psychological support a dire need. The global health and humanitarian assistance stakeholders must play a significant role in setting the agenda and promoting norms through humanitarian diplomacy to safeguard healthcare workers' lives and prevent damage to healthcare settings [33].
4. Healthcare in Threat – Sudan
On 15 April 2023, Khartoum, the capital of Sudan, came into the headlines due to an uprising of an internal conflict within the military-run government. The current clashes have erupted between General Abdel Fattah al-Burhan of the Sudanese Armed Forces (SAF) and General Mohamed Hamdan Dagalo, also known as Hemedti of the Rapid Support Forces (RSF). Despite previously working together for the successful ousting of the former dictatorial president Omar al-Bashir in 2019 and a subsequent coup in 2021, the emergence of a power struggle between the two leaders is a consequence of a proposal to integrate the RSF into the military with an ambiguity in the leadership [34,35,36].
The clash of generals has threatened civilians, with big explosions reported on military buildings and Air Force headquarters close to residential areas, schools and hospitals [37]. The attack has displaced 3 million people and over 700,000 fleeing to neighbouring countries [38]. The Sudanese health minister stated that more than 3000 casualties and 6000 injuries have been reported, and almost 50 per cent of the hospitals in the capital are non-functional as the battle continues [39]. Attack on health has become a major concern with the safety of non-belligerents of war, such as medical personnel, aid providers, and facilities in the current conflict settings.
Despite the capital and several regions reiterating the need to safeguard healthcare facilities from violent and armed attacks, there have been cases of intentional military strikes against health facilities, looting and hijacking of ambulances, in addition to forceful occupation [40]. Furthermore, the International Federation of Red Cross and Red Crescent Societies (IFRC) has claimed that it is impossible to provide any kind of humanitarian assistance to the affected areas, especially around Khartoum [41]. As per the WHO, several hospitals face a shortage of medical supplies and associated life-saving commodities. This irregular violence towards the healthcare systems could widen the pre-existing gap between the need and capacity for health-related services [42].
The country has witnessed multiple armed conflicts since its independence in 1956, mostly after 1989 when the coup d’état led by Colonel Omar al-Bashir overthrew the elected government [43]. Under his rule, Sudan has since witnessed some of the most blood-stained armed conflicts, such as the war in Darfur, where the Sudanese Government is alleged of involving in ethnic cleansing [44]. Between 1989 and 2022, the total number of deaths due to violence is estimated to be 98508, of which 51978 were caused by state-based actions, 23970 by non-state violence, and 22560 were one-sided acts [45]. The current conflict and the ‘attack on health’ exposes the vulnerabilities and difficulty in building a robust health system in a country that has indulged in numerous violent movements and uncertainties.
Since the adoption of Resolution 2286 in 2016, there have been 112 violent attacks on the health of which the highest cases in a month being reported in the ongoing April 2023 conflict in Sudan [30]. While inspecting the number of attacks, it is also imperative to understand the types of violence on health workers and patients (Figure 2). The status of the overlapping effects suggests that the instances of psychological violence, assault, obstruction, individual weapons, and violent searches have been a prominent type of violence on medical personnel, aid, and patients.
The data provides the grim status of how the attack on healthcare has emerged as one of the sought tactics by the parties in conflict settings and challenge the medical neutrality principle adopted from the IHL [46]. Health facilities were previously deemed as one of the “safe zones” amidst conflict settings for civilians and military alike. However, the notion has evolved with the changing nature of warfare, such as attacking healthcare facilities for leveraging negotiation processes between the parties [47,48]. While military strikes have an immediate impact on components of health systems such as hospitals, medical transport, aid supplies, and personnel, it also affects other determinants such as supply chains, water resource, and electricity. This attack on infrastructure could interrupt the ability to deliver preventive and routine care for civilians and critical patients [49]. Hence, failure to protect healthcare personnel and facilities might instil fear of safety, leading to the mass migration that the international community would have to address [50].
5. Role of Health Diplomacy in Conflict Settings
Health, peace, and conflicts are interlinked aspects. Conflicts incite damage to the combatants and civilians due to the disruption of essential supply chains and the breakdown of social order, which could lead to the collapse of the health systems [51]. However, health can also be employed to restore and preserve peace in societies. In this regard, using health as a tool for peace closely interlinks it with the state’s foreign policy. Historically, the health of a particular population was affected by the government’s decision about war, explorations, and trade, but its foreign policy has had multisectoral impacts. The role of public health in this regard has played a significant role where mutual benefits are observed. While the diplomatic relations of extending health paves the way for improving health services, it also helps in furthering the foreign policy agenda, such as garnering support at the global level. An example of a state leveraging health was seen during the 1960s when China sent doctors to Africa to improve the accessibility and availability of healthcare while also ensuring its interests in securing food and energy security [52].
Another instance is Cuba sending its medical staff and medical diplomats to around 70 countries for medical training. As part of their missions, these personnel were involved in recovery and rescue operations during natural disasters and disease outbreaks [53]. Cuba also set up one of the world’s largest medical schools, the Latin American School of Medicine, which has an enrolment of students hailing from 110 countries [54]. The medical diplomacy of Cuba to help restore peace and extend aid for the development of medical resources resulted in the expansion of its geopolitical influence. Further, Cuba re-established diplomatic ties with its Central American neighbours.
The United States’ mission to train healthcare professionals such as physicians, nurses, and laboratory technicians in the states like Afghanistan, Iraq, and Syria is also a step towards health diplomacy in conflict settings [55]. Thus, diplomacy has become a collaborative tool that countries can use to reap the benefits of better health systems and improved diplomatic relations. The tool allows the correction of political or diplomatic failures in conflict-prone areas where the resources for better health conditions are sparsely available. Whilst training professionals and building conflict-resilient health systems are medium and long-term objectives. The short-term measures mainly comprise rendering critical services like shelter, rescue operations, surgeries, and treatment of infectious diseases.
Health diplomacy has taken place in multiple ways in which NGOs, coalitions of national governments and international organizations have played a vital role in responding to attacks on health. The MSF, founded in France in 1971, is one of the foremost organisations working towards delivering emergency medical and humanitarian aid in conflict zones [56]. The MSF is known for maintaining neutrality in conflicts by focusing on providing medical care by deploying doctors and other healthcare staff. Another organisation active in conflict zones is the International Committee of the Red Cross (ICRC) focuses on humanitarian protection and assistance for victims of war and conflicts[57]. The organization primarily promotes IHL, facilitates operations, and creates awareness among war and conflict victims [58].
Despite laws and resolutions condemning the attacks on health, there is a tendency for continued violence. A noteworthy issue concerning such attacks is that they tend to be under and unreported, which demands robust mechanisms and strategies to hold the perpetrators accountable. The Safeguarding Health in Conflict Coalition is one such organisation that has come up for monitoring threats and reporting attacks on health [59]. The WHO is regarded as the lead responsibility for global health concerns. To address the issue of attacks on healthcare, Resolution 65.20 was passed, in which the WHO was requested to provide leadership in collecting data about attacks on healthcare in conflicts, including conflicts. Hence, the WHO established the Attacks on Health Care initiative in 2012 to collect systematic evidence on attacks on health and promote practices for protecting healthcare from future attacks [60].
WHO has further introduced the Global Health for Peace Initiative, which aims to build on global policies to make the health sector a fundamental contributor to peace and deliver a combined outcome of peace and health outcomes. The WHO, by using its legitimacy and neutrality, aims to create a system based on humanitarian principles, which could deliver equity of services by overcoming all kinds of discrimination that are one of the root causes to trigger conflict. This health-for-peace approach has been implemented in Africa, where the programme focuses on building sustainable health systems. The WHO aims to achieve this through an adaptive approach focusing on the participation of all communities, thereby enabling a trust-building situation between civilians, healthcare staff and external health intervention missions [61]. For instance, the WHO in Somalia uses the UN Peacebuilding funds to improve adolescents' psychosocial and mental heaths, as most are born and grow up in conflicts [62]. Similarly, in Cameroon, WHO aims to reduce community violence by deploying skilled community health workers to improve access and quality of community health centres, focusing on mental health [63].
Health diplomacy has evolved to be recognised as a valuable component within the soft power tools countries possess. Although the term is relatively new, the practice of health diplomacy has found be conducted in multiple venues, such as health-related negotiations in global forums, where it has played a crucial role in agreements, treaties and conventions related to not just health but broader agendas, such as human rights and security related discussions of United Nations General Assembly. One such instance is the 1980s when the International Physicians for the Prevention of Nuclear War (IPPNW) launched a campaign against the nuclear arms race. Its members claimed they were reacting as physicians who wanted to use their expertise to prevent a widespread health disaster threat posed due to nuclear weapons [64]. This is an example where health was used to advocate global peace. For their efforts in raising awareness about a potential health disaster, the group was awarded by Nobel Peace Prize in 1985 [65].
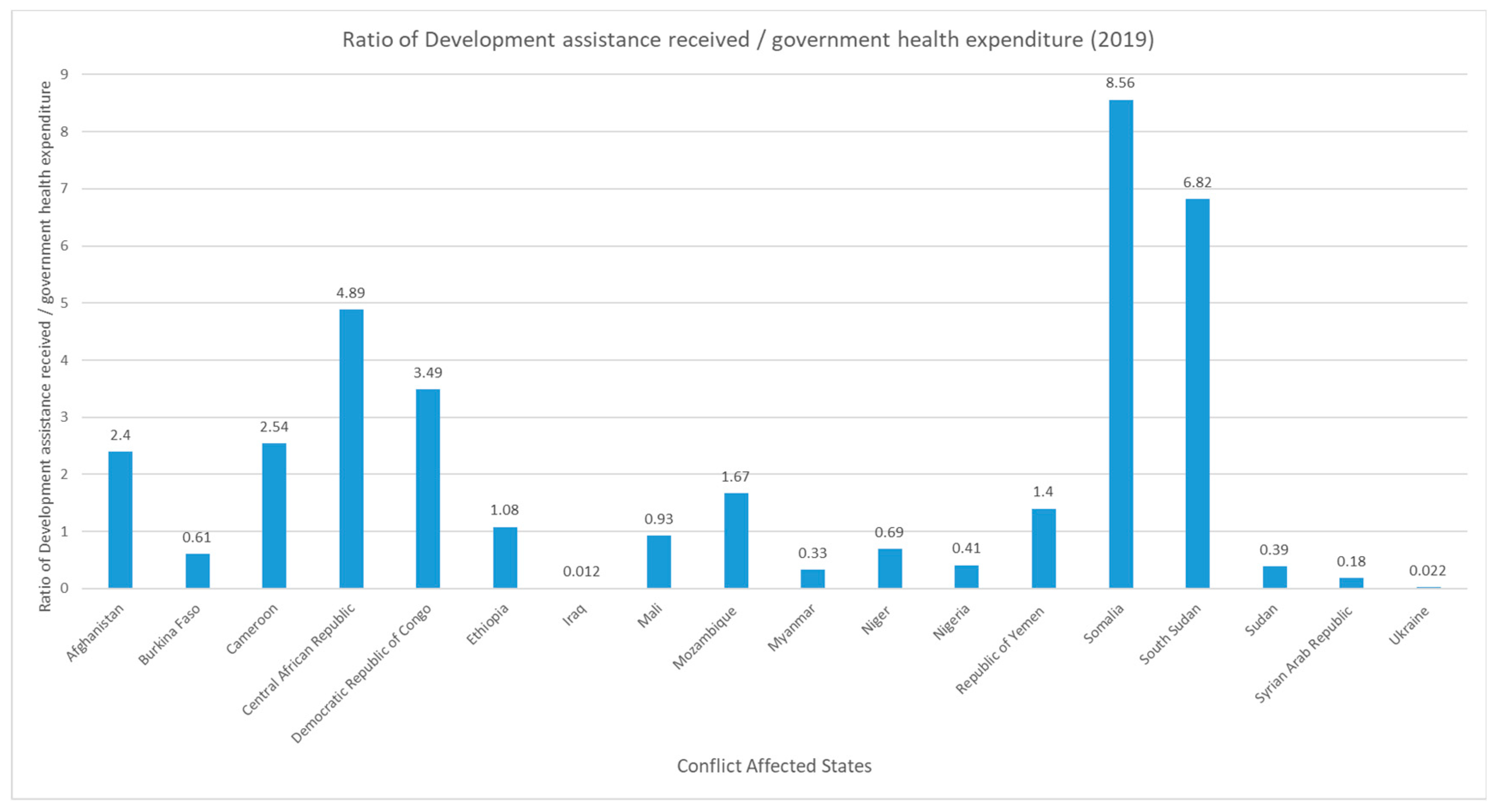
The growing links between health and foreign policy are evident from the development assistance for health. The disparities related to health are viewed as a concern for national security with economic implications. The international community has recognized the importance of providing development assistance funds for maintaining a functioning healthcare system in a conflict setting and providing a helping hand to the non-belligerents. Figure 3 provides the ratio of the development assistance funds to conflict-ridden countries and the government health expenditure in 2019. This ratio indicates the conflict-affected states' dependency on health development assistance funds. Countries like Somalia, South Sudan, and Central African Republic (CAR) that have financial and political constraints to spend on health have received assistance larger than what the government spent out of its account on health. In this manner, the international community intends to help the conflict-affected regions with vulnerable healthcare systems.
These health initiatives have contributed to peace by developing training modules for health facilities and capacity building, which, to an extent, have prevented youths from participating in activities that could drive them towards violence. The initiatives employ the health-development-peace nexus, which contributes towards achieving SDGs of health (SDG3), peace (SDG16), and strengthening partnerships (SDG17). Health diplomacy can be used to strengthen public health systems, especially in conflict settings, which are vulnerable to shocks from the conflicts, in addition to the disease burdens [67]. Thus, a cohesive approach comprising the required disease-specific and region-specific measures for building a resilient health system is essential to achieve the SDGs. Health emergencies exacerbate health and socioeconomic inequalities, whose impacts could be further compounded by conflicts. The conflict settings are prone to concerns such as high numbers of refugees and internal displacement, making the health system fragile and susceptible to disease outbreaks. Therefore, tailored support is required by the conflict-affected areas where health and social protection measures are placed to enhance the resilience of the health systems at the subnational and national levels.
6. Challenges for Health Diplomacy
Health diplomacy provides an avenue to develop intersectoral cooperation, which could bring benefits in the form of building capacities and institutions [68]. However, building a robust health diplomacy depends on the leadership, as their commitments to health issues would require higher positioning in both developmental and political agenda. Health diplomacy can raise health as not just a national issue but a global and transboundary concern [69]. However, it is essential to note that peace and health share a complex bidirectional relationship. In this regard, it is crucial to understand that providing basic social needs is pivotal. The state of accessibility of healthcare to specific groups, either on ethnic, religious, or social grounds, could lead to sentiments of exclusion. This perception of unequal treatment can pave the way for grievances which, if left unattended, could boil into protests and eventually into violence.
While it is true that the effects of health diplomacy have led to unprecedented diplomatic and foreign policy successes, in addition to effectively catering to public health needs, certain instances have led to ramifications leading to a decline in international relations [70]. The US launched the President’s Emergency Plan for AIDS Relief (PEPfAR) to finance the treatment and prevention of HIV/AIDS in resource-limited and conflict-ridden countries. While the initiative proved to be successful as it saved a record number of lives and improved maternal and child healthcare [71]. The program also faced opposition due to the fiscal threats to the treatment programmes. Further, the programme faced a setback in Sub-Saharan Africa due to the suspicion of hidden agendas such as the controversial intervention of male circumcision [72,73]. Hence, while health diplomacy in various forms is crucial for bridging health and peace, it is important to deliberate its components, such as access to medicine, enhancing capacity, and healthily enabling resilient systems to avoid counter-reactions.
The world has seen a steady increase in the number of diplomatic missions in the post-World War era, with states requiring aid for restoration and rebuilding [74]. These missions, hence, have developed as one of the central means through which the states lead international relations. The donor states have used it to boost their economic and political interests while maintaining power and goodwill. While diplomatic missions continue to function as a focal instrument of foreign policy, the emergence of new challenges has allowed to expand areas, such as public health, where diplomacy can be employed.
The threat emanating from health crises and conflicts demands a holistic approach towards building resilience in health systems directly linked to governance and the overall environment [75]. One of the approaches is to enhance inter and cross-sector coordination by linking various other sectors in the economy, which helps improve the capacity to absorb shocks to the system and provide rapid responses. For instance, the public-private partnership is one way to arrange to transport critical medicine supplies and human resources to needy areas. While building a shock-proof system is the main objective, one should also ensure that it is designed to be rebuilt quickly, even after suffering damages due to violence [76]. Additionally, while external support helps mitigate the emergency, the capacity building of care providers at the local level should be prioritised. International organisations can facilitate workshops for the local healthcare staff to prepare them to plan and respond during a crisis [77]. This would ensure continuity in medical care even if foreign states end their missions. However, the success of this approach depends on the level of engagement with the local communities and the development of their trust. A community-based approach has proved efficient in building resilient health systems in multiple West African countries during the Ebola outbreaks [78]. Thus, resilient health systems can be realised by integrating cross-cutting actions such as improving health systems and emergency management to absorb and develop conceptual and operational resources and assistance to countries.
The objectives of Global Health Diplomacy (GHD) can be effectively achieved only when factors when the issue is addressed from a multidimensional approach. Geopolitical factors are one of the primary determinants that influence the delivery of health internationally [79]. The components related to government, its policies, interests, and relationship with other states are determining factors that enable understanding health as policy outcomes at the national, regional, and international levels [80]. Additionally, climate change, population increase and disasters, both natural and man-made, are complex issues that impact geopolitical factors, which in turn affect health [81]. Thus, there is a need for attention to the state’s internal and external vulnerabilities while analyzing the patterns of aid extended to the states in need.
One of the possible policy avenues to counter the range of determinants is adopting an approach to Health in all policies (HiAP), as policy in all sectors affects health outcomes and vice versa82. The approach employs an inter-sectoral relationship by collaborating with all sectors of the economy to develop robust and healthy public policies [83]. The COVID-19 pandemic provides instances to understand the interplay between a state's health, security, and economic policies. While the pandemic posed a health disaster, other issues, such as the superpower tussle, conflicts in Africa and the Middle East, and the re-emergence of the threat of Weapons of Mass Destruction (WMD), intensified the situation [84]. It is amidst this that a few states went ahead with vaccine diplomacy, which can be understood as a diplomatic tool that is part of GHD based on vaccines [85]. The idea was lauded for its potential as a lifesaver and a tool to resolve conflicts. India, China, and Russia were at the forefront of furthering vaccine diplomacy [86]. While India was regarded to be the global vaccine hub, China was able to promote partnerships with over 20 developing states and marketize its vaccines to impact global health governance significantly [87]. The vaccine diplomacy by these states was viewed to significantly impact global health governance.
While the pandemic exposed the states' fragility, it highlighted the importance of investing in a resilient health system [88]. Resilience is the need of the hour, especially in the states that are infested by conflicts, to ensure security, economic and political stability. Hence, GHD finds itself as one of the avenues that could help achieve the economic, health and political outcomes focused on in SDGs.
7. Conclusion and Future Directions
Peace and tranquillity are undoubtedly essential components for ensuring the population’s welfare. The international commitment towards SDGs provides the impetus to revisit the relationship between health and peace. As highlighted by researchers, the amalgamation of SDG 3 (on attaining healthy lives and promoting well-being), SDG 16 (towards peace, justice, and building strong institutions) and SDG 17 (partnership for goals) is imperative in any conflict setting [89,90]. In a globalized world, conflict in one region will affect other parts of the world, making a global response necessary. The inspection of how health should be used as a ‘tool for peace’ and not as leverage during the war must be reiterated by international institutions.
Proposals for ceasefires, mediating dialogues between the battling parties, negotiating for unimpeded provision of reliefs to civilians, and close coordination with embassies for the safety of international citizens and local institutions for civilians must be prioritized. However, this cannot be ensured just by influencing fighting parties but also needs to consider all the stakeholders, including marginalised and deprived groups, to facilitate a lasting reform. The lack of commitment by states to laws of war jeopardises the efforts made by IHL, Geneva Conventions and Additional Protocols committed to protecting healthcare personnel and facilities [91].
As the international community prepares solutions for the current issue, a systemic approach must also be formulated. Establishing a robust accountability mechanism for compliance with UN Resolution 2286 and data transparency are key aspects for global leaders to ensure resilient insulation against attacks on health. As such, the States carry out investigations of such incidents, but an independent mechanism comprising the state, international institutions and NGOs can be facilitated for investigating, which also increases the credibility of the findings due to the involvement of multiple stakeholders. The SSA launched by WHO has provided a platform for finding out attacks on health; however, the mechanism should be further extended with adequate coordination and customisation with local, national, and regional stakeholders.
Healthcare facilities face varying difficulties in conflict settings which could differ according to their region. The increasing trend of attacks on health indicates that it is being weaponised and used as a war tactic. Hospitals and healthcare facilities that were always considered a place for people to heal and feel protected have now been transformed into epicentre for either an offensive or defensive strategy in a conflict. Thus, while the war continues in Sudan, a collective action plan and preparedness mechanisms must be made for the crisis at hand and the future.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, S.P., H.B, A.I, K.K.B; Methodology, S.P., A.I, K.K.B; Formal Analysis, S.P, A.I, K.K.B, V.D; Investigation, S.P., A.I, K.K.B, V.D; Data Curation, A.I, K.K.B, V.D; Writing – Original Draft Preparation, A.I, K.K.B, V.K.C; Writing – Review & Editing, S.P, H.B, A.I, K.K.B, V.D, V.K.C; Visualization, A.I, K.K.B, V.D; Supervision, H.B, S.P.
Funding
This research received no external funding.
Data Availability Statement
All data underlying the results are available as part of the article and no additional source data are required.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fidler, D.P. Health as Foreign Policy: Harnessing Globalization for Health. Health Promot. Int. 2006, 21 (suppl_1), 51–58. [Google Scholar] [CrossRef]
- Quality of Care in Fragile, Conflict-Affected and Vulnerable Settings: Taking Action; World Health Organization, Series Ed.; World Health Organization: Geneva, 2020. Available online: https://www.who.int/publications-detail-redirect/9789240015203 (accessed on 17 July 2023).
- Devadas, S.; Elbadawi, I.; Norman, V. Loayza. Growth After War in Syria, 2019. Available online: https://erf.org.eg/publications/growth-after-war-in-syria/ (accessed on 18 July 2023).
- World Health Organization. Everybody’s Business -- Strengthening Health Systems to Improve Health Outcomes : WHO’s Framework for Action. 2007, 44.
- International Committee of the Red Cross. Health Care in Danger: Making the Case; Publication; International Committee of the Red Cross: Geneva, Switzerland, 2011; Available online: https://www.icrc.org/en/publication/4072-health-care-danger-making-case (accessed on 18 July 2023).
- International Committee of the Red Cross. Respecting and protecting health care in armed conflicts and in situations not covered by international humanitarian law - Factsheet. International Committee of the Red Cross. Available online: https://www.icrc.org/en/document/respecting-and-protecting-health-care-armed-conflicts-and-situations-not-covered (accessed on 18 July 2023).
- Faith Everett. Under threat: healthcare in conflict zones. The Health Policy Partnership. Available online: https://www.healthpolicypartnership.com/under-threat-healthcare-in-conflict-zones/ (accessed on 18 July 2023).
- IGNORING RED LINES Violence Against Health Care in Con_ict 2022; Safeguarding Health in Conflict Coalition and Insecurity Insight, 2022.
- WHO. Global Health Workforce Statistics Database. Available online: https://www.who.int/data/gho/data/themes/topics/health-workforce (accessed on 18 July 2023).
- WHO. Hospital Beds (per 10 000 Population). Available online: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/hospital-beds-(per-10-000-population) (accessed on 18 July 2023).
- Brînzac, M.G.; Kuhlmann, E.; Dussault, G.; Ungureanu, M.I.; Cherecheș, R.M.; Baba, C.O. Defining Medical Deserts—an International Consensus-Building Exercise. Eur. J. Public Health 2023, ckad107. [Google Scholar] [CrossRef]
- Physicians for Human Rights. WAR CRIMES IN KOSOVO A Population-Based Assessment of Human Rights Violations Against Kosovar Albanians; Physicians for Human Rights: Boston, 1999; pp. 93–110. [Google Scholar]
- Physicians For Human Rights. The Legacy of Oppression and Conflict on Health in Kosovo; June 16, 2009; US, 2009, pp. 22–34. Available online: https://phr.org/our-work/resources/perilous-medicine/ (accessed on 17 July 2023).
- Taliban rue ambulance attack. The New Humanitarian. Available online: https://www.thenewhumanitarian.org/news/2011/04/12/taliban-rue-ambulance-attack (accessed on 17 July 2023).
- Fiona Terry. Violence against health care: insights from Afghanistan, Somalia, and the Democratic Republic of the Congo. International Review of the Red Cross. Available online: http://international-review.icrc.org/articles/violence-against-health-care-insights-afghanistan-somalia-and-democratic-republic-congo (accessed on 17 July 2023).
- MSF. MSF vaccination used as bait in unacceptable attack on civilians. Médecins Sans Frontières (MSF) International. Available online: https://www.msf.org/msf-vaccination-used-bait-unacceptable-attack-civilians (accessed on 17 July 2023).
- MSF. After a week of intense fighting in Somalia, MSF is extremely concerned about the security of medical staff and safety of patients. Médecins Sans Frontières (MSF) International. Available online: https://www.msf.org/after-week-intense-fighting-somalia-msf-extremely-concerned-about-security-medical-staff-and-safety (accessed on 17 July 2023).
- Shell-Shocked: Civilians under Siege in Mogadishu - Somalia; 2007; pp 51–57. Available online: https://reliefweb.int/report/somalia/shell-shocked-civilians-under-siege-mogadishu (accessed on 17 July 2023).
- International Humanitarian Law Databases - Medical Units. International Committee of the Red Cross. Available online: https://ihl-databases.icrc.org/en/customary-ihl/v1/rule28 (accessed on 17 July 2023).
- Convention (I) for the Amelioration of the Condition of the Wounded and Sick in Armed Forces in the Field. Geneva, 12 August 1949. Available online: https://ihl-databases.icrc.org/en/ihl-treaties/gci-1949/, https://ihl-databases.icrc.org/en/ihl-treaties/gci-1949/article-15 (accessed on 17 July 2023).
- Article 15 - Search for casualties. Evacuation. International Humanitarian Law Databases. Available online: https://ihl-databases.icrc.org/en/ihl-treaties/gci-1949/, https://ihl-databases.icrc.org/en/ihl-treaties/gci-1949/article-15 (accessed on 17 July 2023).
- Geneva Convention relative to the Protection of Civilian Persons in Time of War. The Office of the High Commissioner for Human Rights. Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/geneva-convention-relative-protection-civilian-persons-time-war (accessed on 17 July 2023).
- Protocol Additional to the Geneva Conventions of 12 August 1949, and relating to the Protection of Victims of International Armed Conflicts (Protocol 1). The Office of the High Commissioner for Human Rights. Available online: https://www.ohchr.org/en/instruments-mechanisms/instruments/protocol-additional-geneva-conventions-12-august-1949-and (accessed on 17 July 2023).
- Article 11 - Protection of medical units and transports. International Humanitarian Law Databases. Available online: https://ihl-databases.icrc.org/en/ihl-treaties/apii-1977/, https://ihl-databases.icrc.org/en/ihl-treaties/apii-1977/article-11 (accessed on 17 July 2023).
- Asi, Y.M.; Tanous, O.; Wispelwey, B.; AlKhaldi, M. Are There ‘Two Sides’ to Attacks on Healthcare? Evidence from Palestine. Eur. J. Public Health 2021, 31, 927–928 Available online:. [Google Scholar] [CrossRef]
- Terrence McCoy. Why Hamas stores its weapons inside hospitals, mosques and schools. The Washington Post. Available online: https://www.washingtonpost.com/news/morning-mix/wp/2014/07/31/why-hamas-stores-its-weapons-inside-hospitals-mosques-and-schools/ (accessed on 17 July 2023).
- UNRWA. UNRWA condemns placement of rockets, for a second time, in one of its schools. United Nations Relief and Works Agency for Palestine Refugees in the Near East. Available online: https://www.unrwa.org/newsroom/press-releases/unrwa-condemns-placement-rockets-second-time-one-its-schools (accessed on 17 July 2023).
- Even wars have limits: Health-care workers and facilities must be protected. International Committee of the Red Cross. Available online: https://www.icrc.org/en/document/hcid-statement (accessed on 17 July 2023).
- United Nations. Security Council Adopts Resolution 2286 (2016), Strongly Condemning Attacks against Medical Facilities, Personnel in Conflict Situations. UN Press. Available online: https://press.un.org/en/2016/sc12347.doc.htm (accessed on 17 July 2023).
- SSA Home. SURVEILLANCE SYSTEM FOR ATTACKS ON HEALTH CARE (SSA). Available online: https://extranet.who.int/ssa/Index.aspx (accessed on 17 July 2023).
- Hakki, L.; Stover, E.; Haar, R.J. Breaking the Silence: Advocacy and Accountability for Attacks on Hospitals in Armed Conflict. Int. Rev. Red Cross 2020, 102, 1201–1226. [Google Scholar] [CrossRef]
- The Failure of UN Security Council Resolution 2286 in Preventing Attacks on Healthcare in Syria. Syrian American Medical Society Foundation. Available online: https://www.sams-usa.net/reports/failure-un-security-council-resolution-2286-preventing-attacks-healthcare-syria/ (accessed on 17 July 2023).
- Chattu, V.K.; Jean-Louis, G.; Zeller, J.L.; Pandi-Perumal, S.R. Aiding Universal Health Coverage through Humanitarian Outreach Services and Global Health Diplomacy in Resource-Poor Settings. J. Natl. Med. Assoc. 2021, 113, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Omar Al-Bashir: Sudan’s Ousted President. BBC News. December 5, 2011. Available online: https://www.bbc.com/news/world-africa-16010445 (accessed on 17 July 2023).
- Salih, Z.M.; Beaumont, P.; Sudan’s Army Seizes Power in Coup and Detains Prime Minister. The Guardian. October 25, 2021. Available online: https://www.theguardian.com/world/2021/oct/25/sudan-coup-fears-amid-claims-military-have-arrested-senior-government-officials (accessed on 17 July 2023).
- Sudan unrest: What are the Rapid Support Forces? | News | Al Jazeera. Available online: https://www.aljazeera.com/news/2023/4/16/sudan-unrest-what-is-the-rapid-support-forces (accessed on 17 July 2023).
- Jake Horton; Kayleen Devlin. Sudan: Fighting between Rival Forces Hits Residential Areas. BBC News. April 17, 2023. Available online: https://www.bbc.com/news/world-africa-65299756 (accessed on 17 July 2023).
- Samy Magdy. UN says Sudan conflict has displaced over 3 million people. PBS NewsHour. Available online: https://www.pbs.org/newshour/world/un-says-raging-conflict-in-sudan-has-displaced-over-3-million-people (accessed on 17 July 2023).
- Reuters Staff. More than 3,000 People Killed, 6,000 Injured in Sudan Conflict - Health Minister. Reuters. June 17, 2023. Available online: https://www.reuters.com/article/sudan-politics-casualties-idINC6N37W000 (accessed on 17 July 2023).
- Harriet Barber. Sudan hospitals and ambulances attacked during fighting between army and RSF. The Telegraph. Available online: https://www.telegraph.co.uk/global-health/terror-and-security/sudan-fighting-khartoum-world-health-organisation-hospitals/ (accessed on 17 July 2023).
- Emma Farge; Gabrielle Tétrault-Farber. “Almost impossible” to provide aid in Sudanese capital, IFRC says. Reuters. Available online: https://www.reuters.com/world/africa/ifrc-says-almost-impossible-provide-aid-around-sudanese-capital-2023-04-18/ (accessed on 17 July 2023).
- Scott Gates; Håvard Mokleiv Nygård; Karim Bahgat. Patterns of Attacks on Medical Personnel and Facilities: SDG 3 meets SDG 16 – Peace Research Institute Oslo. The Peace Research Institute Oslo (PRIO). Available online: https://www.prio.org/publications/10785 (accessed on 17 July 2023).
- Reuters Staff. FACTBOX - Sudan’s President Omar Hassan al-Bashir. Reuters. July 14, 2008. Available online: https://www.reuters.com/article/uk-warcrimes-sudan-bashir-profile-idUKL1435274220080714 (accessed on 17 July 2023).
- Lefkow, L. Darfur Destroyed. Hum. Rights Watch 2004.
- UCDP - Uppsala Conflict Data Program. Available online: https://ucdp.uu.se/country/625 (accessed on 17 July 2023).
- Rule 25. Medical Personnel. Customary IHL Database. Available online: https://ihl-databases.icrc.org/en/customary-ihl/v1/rule25 (accessed on 17 July 2023).
- Druce, P.; Bogatyreva, E.; Siem, F.F.; Gates, S.; Kaade, H.; Sundby, J.; Rostrup, M.; Andersen, C.; Rustad, S.C.A.; Tchie, A.; Mood, R.; Nygård, H.M.; Urdal, H.; Winkler, A.S. Approaches to Protect and Maintain Health Care Services in Armed Conflict – Meeting SDGs 3 and 16. Confl. Health 2019, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Leebaw, B. The Politics of Impartial Activism: Humanitarianism and Human Rights. Perspect. Polit. 2007, 5, 223–239. [Google Scholar] [CrossRef]
- Siem, F.F. Leaving them behind: healthcare services in situations of armed conflict. Tidsskr. Den Nor. Laegeforening Tidsskr. Prakt. Med. Ny Raekke 2017, 137. [Google Scholar] [CrossRef] [PubMed]
- The Humanitarian-Development-Peace Initiative. World Bank. Available online: https://www.worldbank.org/en/topic/fragilityconflictviolence/brief/the-humanitarian-development-peace-initiative (accessed on 17 July 2023).
- Abuelaish, I.; Goodstadt, M.S.; Mouhaffel, R. Interdependence between Health and Peace: A Call for a New Paradigm. Health Promot. Int. 2020, 35, 1590–1600. [Google Scholar] [CrossRef]
- Killeen, O.J.; Davis, A.; Tucker, J.D.; Mason Meier, B. Chinese Global Health Diplomacy in Africa: Opportunities and Challenges. Glob. Health Gov. Sch. J. New Health Secur. Paradigm 2018, 12, 4–29. [Google Scholar]
- Feinsilver, J.M. Fifty Years of Cuba’s Medical Diplomacy: From Idealism to Pragmatism. Cuban Stud. 2010, 41, 85–104. [Google Scholar] [CrossRef] [PubMed]
- Jiwa, A. The Latin American School of Medicine (Elam): Admissions, Academics and Attitudes. Int. J. Cuban Stud. 2017, 9, 142–154. [Google Scholar] [CrossRef]
- Feldbaum, H.; Lee, K.; Michaud, J. Global Health and Foreign Policy. Epidemiol. Rev. 2010, 32, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Médecins Sans Frontières. About us: What is MSF? What we do? Our history. Médecins Sans Frontières(MSF)/Doctors Without Borders. Available online: https://msfsouthasia.org/our-history/ (accessed on 18 July 2023).
- International Committee of the Red Cross. History of the ICRC. ICRC. Available online: https://www.icrc.org/en/document/history-icrc (accessed on 18 July 2023).
- International Committee of the Red Cross. Partnership is key to ending violence against health care. ICRC. Available online: https://www.icrc.org/en/document/partnership-key-ending-violence-against-health-care (accessed on 18 July 2023).
- Safeguarding Health in Conflict. About the Coalition. Safeguarding Health in Conflict Coalition. Available online: https://www.safeguardinghealth.org/about-coalition (accessed on 18 July 2023).
- World Health Organization. Attacks on Health Care Initiative. What is the Atacks on Health Care Initiative. Available online: https://www.who.int/news-room/questions-and-answers/item/attacks-on-health-care-initiative (accessed on 17 July 2023).
- WHO. Global Health and Peace Initiative (GHPI) - Fifth Draft of the Roadmap; World Health Organization (WHO). 2023, pp. 2–4. Available online: https://www.who.int/initiatives/who-health-and-peace-initiative (accessed on 17 July 2023).
- WHO EMRO. Somalia implements ground-breaking project aimed at improving psychosocial support and mental health care for young people affected by conflict through a socially-inclusive integrated approach for peace-building. World Health Organization - Regional Office for the Eastern Mediterranean. Available online: http://www.emro.who.int/somalia/news/somalia-implements-ground-breaking-project-aimed-at-improving-psychosocial-support-and-mental-health-care-for-young-people-affected-by-conflict-through-a-socially-inclusive-integrated-app.html (accessed on 18 July 2023).
- Coninx, R.; Ousman, K.; Mathilde, B.; Kim, H.-T. How Health Can Make a Contribution to Peace in Africa: WHO’s Global Health for Peace Initiative (GHPI). BMJ Glob. Health 2022, 7 (Suppl 8), e009342. [Google Scholar] [CrossRef] [PubMed]
- Castillo, F.M. The International Physicians for the Prevention of Nuclear War: Transnational Midwife of World Peace. Med. War 1990, 6, 250–268. [Google Scholar] [CrossRef]
- Official Statement of the Nobel Committee Upon Awarding the 1985 Nobel Peace Prize to IPPNW. International Physicians for the Prevention of Nuclear War. Available online: https://www.ippnw.org/1985/12/10/1985-nobel-peace-prize/' (accessed on 18 July 2023).
- Institute for Health Metrics and Evaluation (IHME). Development Assistance for Health Database 1990-2020, 2021. [CrossRef]
- WHO EMRO. Global health security is integral to foreign policy. World Health Organization - Regional Office for the Eastern Mediterranean. Available online: http://www.emro.who.int/health-topics/health-diplomacy/foreign-policy.html (accessed on 18 July 2023).
- WHO EMRO. Global health needs global health diplomacy. World Health Organization - Regional Office for the Eastern Mediterranean. Available online: http://www.emro.who.int/health-topics/health-diplomacy/about-health-diplomacy.html (accessed on 18 July 2023).
- WHO EMRO. Health challenges. World Health Organization - Regional Office for the Eastern Mediterranean. Available online: http://www.emro.who.int/health-topics/health-diplomacy/health-challenges.html (accessed on 18 July 2023).
- Tom Daschle; Bill Frist. The Case for Strategic Health Diplomacy: A Study of PEPFAR.; Bipartisan Policy Center, 2015, pp. 10–12. Available online: https://bipartisanpolicy.org/report/the-case-for-strategic-health-diplomacy-a-study-of-pepfar/ (accessed on 17 July 2023).
- PEPFAR Organization and Implementation. In Evaluation of PEPFAR.; National Academies Press (US), 2013.
- Lyman, P.N.; Wittels, S.B. No Good Deed Goes Unpunished: The Unintended Consequences of Washington’s HIV/AIDS Programs. Foreign Aff. 2010, 89, 74–84. [Google Scholar]
- Quigley, M.A.; Weiss, H.A.; Hayes, R.J. Male Circumcision as a Measure to Control HIV Infection and Other Sexually Transmitted Diseases. Curr. Opin. Infect. Dis. 2001, 14, 71–75. [Google Scholar] [CrossRef]
- Bagozzi, B.E.; Landis, S.T. The Stabilizing Effects of International Politics on Bilateral Trade Flows. Foreign Policy Anal. 2015, 11, 151–171. [Google Scholar] [CrossRef]
- Blanchet, K.; Nam, S.L.; Ramalingam, B.; Pozo-Martin, F. Governance and Capacity to Manage Resilience of Health Systems: Towards a New Conceptual Framework. Int. J. Health Policy Manag. 2017, 6, 431–435. [Google Scholar] [CrossRef]
- Yassmin Moor. Cash and vouchers can improve health outcomes – but you must understand the challenges first. The CALP Network. Available online: https://www.calpnetwork.org/blog/cva-can-improve-health-outcomes/ (accessed on 18 July 2023).
- Goodman, C.; Opwora, A.; Kabare, M.; Molyneux, S. Health Facility Committees and Facility Management - Exploring the Nature and Depth of Their Roles in Coast Province, Kenya. BMC Health Serv. Res. 2011, 11, 229. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, S.; Al-Dahir, S.; Al Mulla, T.; Lami, F.; Hossain, S.M.M.; Baqui, A.; Burnham, G. Resilience of Health Systems in Conflict Affected Governorates of Iraq, 2014–2018. Confl. Health 2021, 15, 76. [Google Scholar] [CrossRef]
- Persaud, A.; Day, G.; Gupta, S.; Ventriglio, A.; Ruiz, R.; Chumakov, E.; Desai, G.; Castaldelli-Maia, J.; Torales, J.; Juan Tolentino, E.; Bhui, K.; Bhugra, D. Geopolitical Factors and Mental Health I. Int. J. Soc. Psychiatry 2018, 64, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Persaud, A.; Bhat, P.S.; Ventriglio, A.; Bhugra, D. Geopolitical Determinants of Health. Ind. Psychiatry J. 2018, 27, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Khanal, S.; Ramadani, L.; Boeckmann, M. Health Equity in Climate Change and Health Policies: A Systematic Review. Sustainability 2023, 15, 10653. [Google Scholar] [CrossRef]
- Baum, F.; Lawless, A.; Delany, T.; Macdougall, C.; Williams, C.; Broderick, D.; Wildgoose, D.; Harris, E.; Mcdermott, D.; Kickbusch, I.; Popay, J.; Marmot, M. Evaluation of Health in All Policies: Concept, Theory and Application. Health Promot. Int. 2014, 29 (suppl 1), i130–i142. [Google Scholar] [CrossRef]
- Green, L.; Ashton, K.; Bellis, M.A.; Clemens, T.; Douglas, M. ‘Health in All Policies’—A Key Driver for Health and Well-Being in a Post-COVID-19 Pandemic World. Int. J. Environ. Res. Public. Health 2021, 18, 9468. [Google Scholar] [CrossRef]
- Kim, Y.; Park, Y. International Health Cooperation in the Post-Pandemic Era: Possibilities for and Limitations of Middle Powers in International Cooperation. Soc. Sci. 2022, 11, 259. [Google Scholar] [CrossRef]
- Giusti, S.; Tafuro Ambrosetti, E. Making the Best Out of a Crisis: Russia’s Health Diplomacy during COVID-19. Soc. Sci. 2022, 11, 53. [Google Scholar] [CrossRef]
- Suzuki, M.; Yang, S. Political Economy of Vaccine Diplomacy: Explaining Varying Strategies of China, India, and Russia’s COVID-19 Vaccine Diplomacy. Rev. Int. Polit. Econ. 2023, 30, 865–890. [Google Scholar] [CrossRef]
- Sharun, K.; Dhama, K. India’s Role in COVID-19 Vaccine Diplomacy. J. Travel Med. 2021, 28, taab064. [Google Scholar] [CrossRef]
- Greer, S.L.; Falkenbach, M.; Siciliani, L.; McKee, M.; Wismar, M.; Figueras, J. From Health in All Policies to Health for All Policies. Lancet Public Health 2022, 7, e718–e720. [Google Scholar] [CrossRef] [PubMed]
- Chattu, V.K.; Knight, W.A. Global Health Diplomacy as a Tool of Peace. Peace Rev. 2019, 31, 148–157. [Google Scholar] [CrossRef]
- Egbende, L.; Helldén, D.; Mbunga, B.; Schedwin, M.; Kazenza, B.; Viberg, N.; Wanyenze, R.; Ali, M.M.; Alfvén, T. Interactions between Health and the Sustainable Development Goals: The Case of the Democratic Republic of Congo. Sustainability 2023, 15, 1259. [Google Scholar] [CrossRef]
- António Guterres. International Laws Protecting Civilians in Armed Conflict Not Being Upheld, Secretary-General Warns Security Council, Urging Deadly Cycle Be Broken. UN Press. Available online: https://press.un.org/en/2023/sc15292.doc.htm (accessed on 18 July 2023).
Figure 1.
Countries and territories with reported attacks on health workers and infrastructures (2016-2023). Source: Surveillance System for Attacks on Health Care (SSA) [30]
Figure 1.
Countries and territories with reported attacks on health workers and infrastructures (2016-2023). Source: Surveillance System for Attacks on Health Care (SSA) [30]
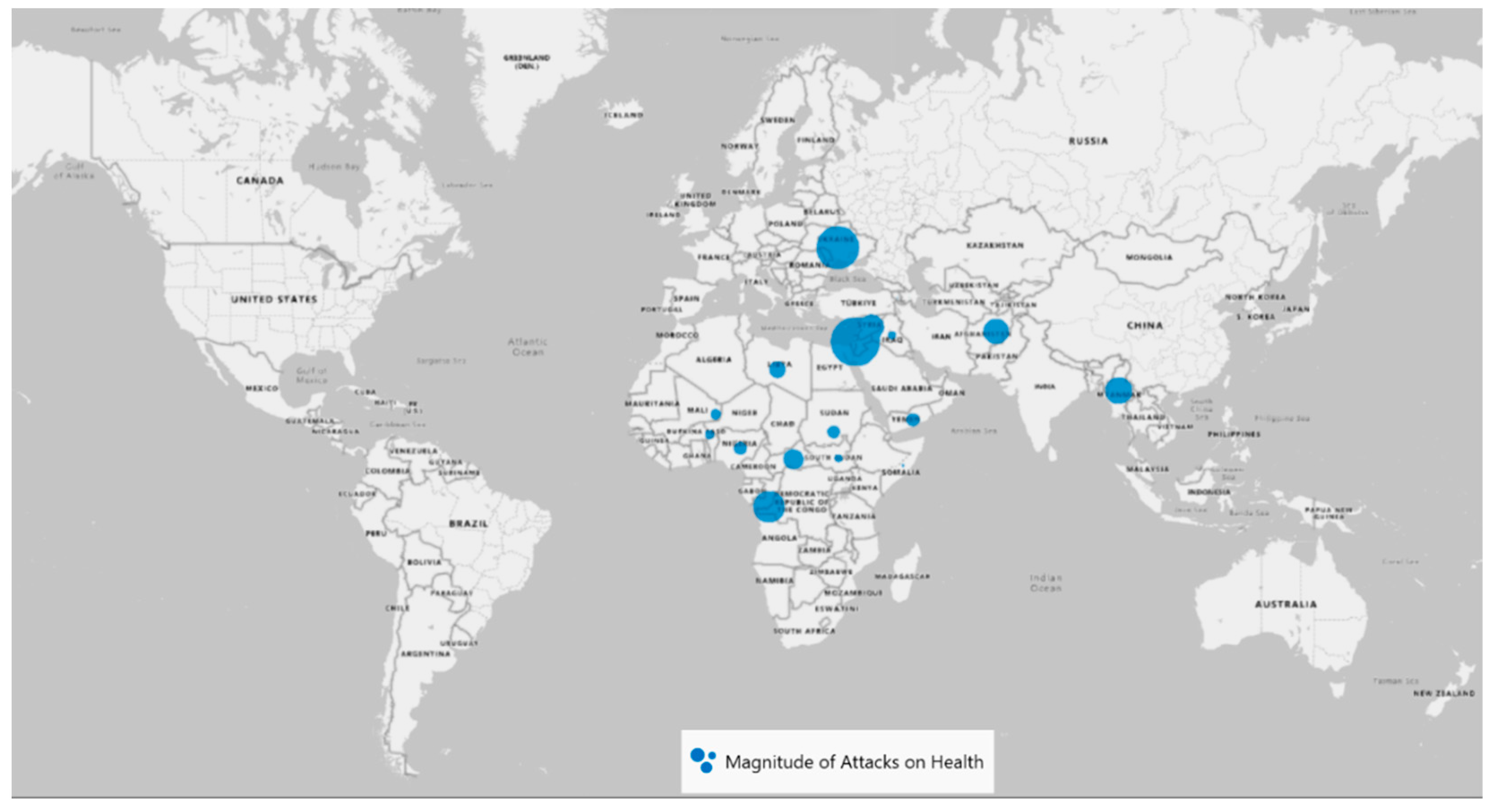
Figure 2.
Number of Attacks by type in Sudan (2016-2023). Source: Surveillance System for Attacks on Health Care(SSA) [30].
Figure 2.
Number of Attacks by type in Sudan (2016-2023). Source: Surveillance System for Attacks on Health Care(SSA) [30].
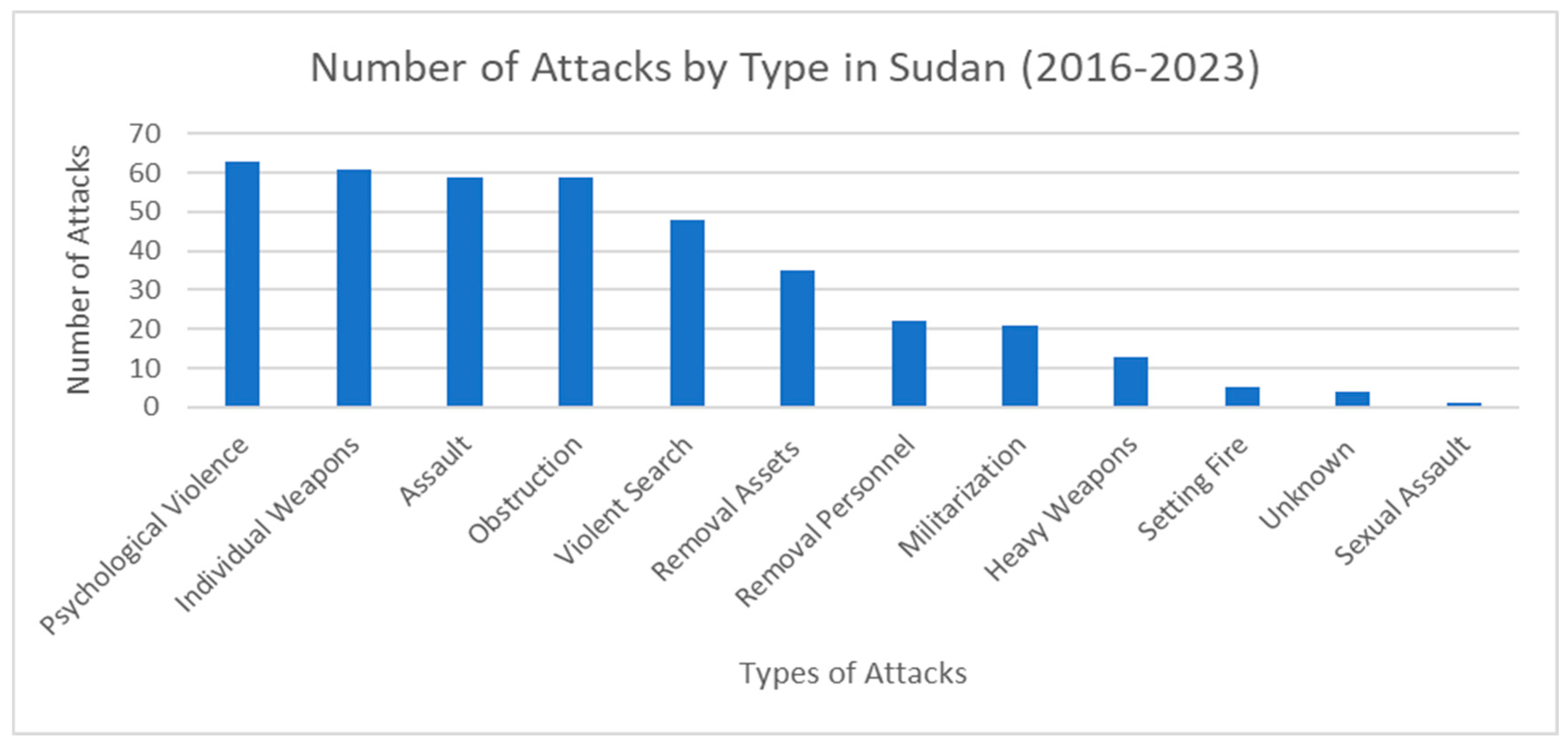
Figure 3.
Ratio of development assistance received / government health expenditure (2019). Source: Institute for Health Metrics and Evaluation [66].
Figure 3.
Ratio of development assistance received / government health expenditure (2019). Source: Institute for Health Metrics and Evaluation [66].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



