
Submitted:
26 July 2023
Posted:
27 July 2023
You are already at the latest version
Abstract
Introduction: Obstructive sleep apnea (OSA) is the most common sleep-breathing disorder. OSA is associated with cardiovascular diseases such as coronary artery disease (CAD) and arrhythmias with an increased risk of sudden cardiac death. Some changes in ECG markers are seen as an indicator of arrhythmogenicity, especially ventricular arrhythmias. The goal of this study was to investigate if OSA patients with CAD have QT dispersion and T peak to T end (TpTe) changes as a surrogate of arrhythmogenicity.
Methods: We studied 75 patients with CAD who underwent polysomnographic studies. Patients were categorized into mild, moderate, and severe OSA according to the Apnea hypopnea index (AHI). Baseline ECG and echocardiography for assessing LV function and valvular heart disease were done for all of them.
Results: Results showed that in patients with moderate and severe sleep apnea QT dispersion was higher in a group with more involvement of coronary artery disease, reduced ejection fraction, and a history of old MI. However, we didn’t find any significant statistical relationship between OSA and TpTe marker.
Conclusion: Our results showed a positive relation between ECG arrhythmic indices such as QT dispersion and OSA severity in patients with CAD.
Keywords:
Obstructive sleep apnea
; Coronary artery disease
; QT dispersion
; T peak to T end
; multivessel coronary disease
; cardiomyopathy
1. Introduction
Obstructive sleep apnea (OSA) is the most common breathing-related sleep disorder worldwide [1] characterized by snoring and collapsing of upper airways during sleep which leads to partial (hypopnea) or complete (apnea) hindrance of airway flow despite efforts to breathe. Apnea hypopnea index (AHI) is an index used to diagnose and classify OSA into mild, moderate, and severe. AHI includes the total number of apnea and hypopnea per hour of sleep [2].
OSA now is an independent risk factor for cardiac disease especially coronary artery disease and arrhythmia. OSA has also a role in the pathogenesis of systemic hypertension, especially in multidrug-resistant hypertension [3]. Cardiovascular morbidity and mortality have been shown to be higher in OSA patients. Etiologies such as sympathetic overactivity, vascular endothelial dysfunction, abnormalities in coagulation pathways, and metabolic dysregulation are to be mentioned in the pathogenesis of OSA-related cardiac disorders. [4]
OSA has a close association with cardiac arrhythmias including both supraventricular such as atrial fibrillation (AF) and ventricular arrhythmias such as ventricular tachycardia and fibrillation (VT, VF) and also sudden cardiac death (SCD). Transient nocturnal arrhythmias have also been higher in these patients. [5] Measured corrected QT interval (QTc) and QT dispersion are known to be risk factors for cardiac arrhythmogenicity. Tpeak to Tend interval (Tpe) and Tp dispersion (Tpe-D) are markers of arrhythmia susceptibility. Furthermore, the Tpe/QT ratio is reported to predict a cardiac arrhythmia risk. [6]
OSA patients have higher major cardiovascular risk factors such as systemic hypertension, diabetes mellitus, smoking, previous myocardial infarction, obesity, and premature coronary artery disease.[7] Furthermore, patients with OSA have an increased prevalence of other respiratory disorders including chronic obstructive pulmonary disease, asthma, interstitial lung disease, and Pulmonary thromboembolism which may further exacerbate the respiratory condition. [8] QT dispersion is defined as the difference between the maximum and minimum QT intervals that can be measured on the 12-lead ECG. T peak to T end is defined as the measurement of T-peak as the maximum absolute T-wave deflection from the isoelectric line, and the T-end as the intersection of the isoelectric line and the tangent to the downslope of the T-wave. [9] The goal of this study was to investigate if OSA patients with CAD have QT dispersion and T peak to T end (TpTe) changes as a surrogate of arrhythmogenicity.
2. Material and methods
In this retrospective study, we enrolled 75 patients who were undergone coronary arteriography for acute coronary syndrome (ACS) with documented CAD artery disease based on angiography from 2018 up to 2019. This study was done under the approval of Shahid Beheshti Medical University Research Committee (IRB: IR.SBMU.MSP.REC.1397.32).
2.1. Inclusion and exclusions criteria:
We included patients with coronary lesions with more than 50 % stenosis who underwent percutaneous coronary intervention (PCI) for clinical indication. The range for age was 40 to 70 years old and BMI was 25 to 35. All of the study populations were stable at the time of the study.
Excluded were patients who presented with acute coronary syndrome or sleep apnea diagnosis was not documented by a sleep study. Patients with < 50% coronary stenosis were also excluded. Excluded were also patients who didn’t cooperate, who were treated with medications that could change QT intervals such as antiarrhythmics and anti-psychotics, and patients with disorders that prolong or shorten QT intervals such as atrial fibrillation or bundle blocks. Patients with pacemaker or ICD, liver disease, renal disease, history of cerebrovascular accidents, and other sleep disorders were also excluded. Any electrolyte abnormalities were also excluded.
We categorized patients based on coronary involvement, Left ventricular ejection fraction, and history of previous myocardial infarction (MI). All of the patients underwent polysomnography in the sleep laboratory about 1 month after their coronary angiogram regardless of any sleep breathing disorders or complaints.
2.2. Sleep apnea diagnosis:
Sleep apnea was diagnosed based on the clinical history and Epworth sleep questionnaire and polysomnography criterion. After eight hours of polysomnography, we used the Apnea-Hypopnea Index (AHI) to sub-classifying patients into different categories: 5 to 15 episodes per hour of apnea or hypopnea were categorized as mild, 15 to 30 episodes per hour of apnea or hypopnea as moderate and more than 30 episodes per hour of apnea or hypopnea as severe
Apnea defines as the absence of nasal airflow for > 10 seconds while hypopnea defines as a reduction of O2 saturation level of 3% or more for > 10 seconds with polysomnographic arousal. All patients with a history of hypertension were treated and were in a normal range during our study. All diabetic patients were euglycemic. Patients who used oral agents only for glycemic control were included. Echocardiography was done for all patients for assessing LV global function and any valvular heart disease. All patients were instructed to abstain from caffeine, alcohol, and tobacco for 48 hours before their sleep study.
2.3. QT dispersion and TpTe measurements:
Participants rested in the supine position in a calm room with constant room light and temperature. Standard ECG was obtained from all patients before the sleep study. All ECG measurements included QT intervals and QTmax and QTmin are defined as the longest and shortest QT interval in the ECG. QT dispersion was defined as the difference between QTmax and QTmin. The TpTe interval was defined as the time from the peak of the T wave to the cutting point of the tangent to the downward slope of the T wave and the isoelectric line. Both of them were measured by the ruler as previous literature describes. [10] U waves were excluded. Leads in which QT and TpTe were low amplitude or with excessive noise were excluded. All patients with wide QRS complexes were excluded.
2.4. Statistical analysis:
Statistical analyses were done using IBM SPSS version 25. P-values less than 5 % were significant. This study was supervised by the Ethics Committee at Shahid Beheshti University of medical sciences.
3. Results
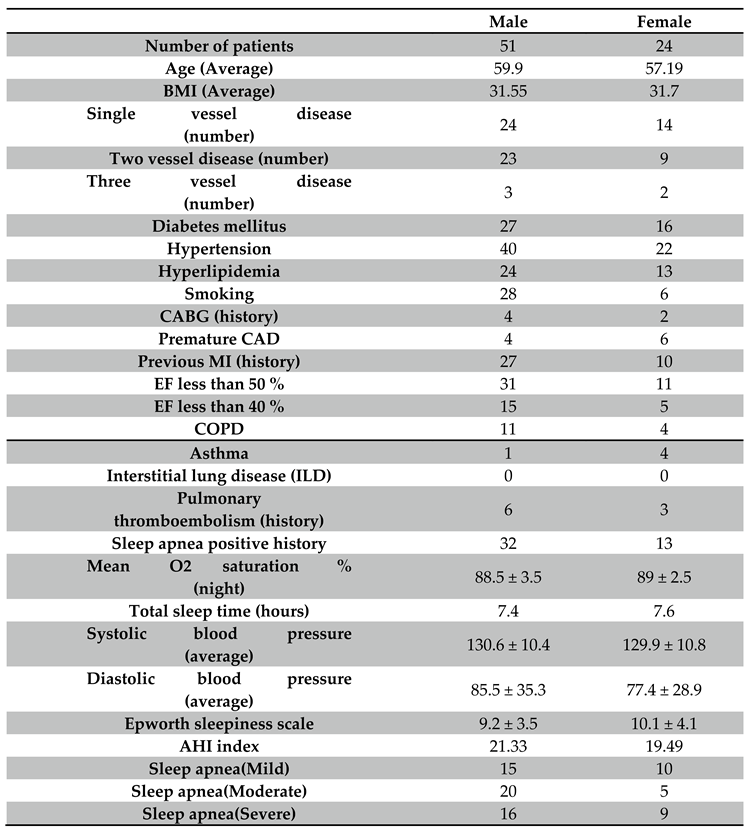
We studied 75 patients with CAD and OSA. Demographic data are as follows and can be seen in Table 1. The mean age of the study group was 59.19 for males and 57.19 for females. The average BMI for males and females was 31.55 and 31.7 respectively. There is no significant difference in age and BMI between males and females. We analyzed QT dispersion and TpTe in patients with mild, moderate, and severe OSA in groups with different coronary involvement, Ejection fraction, and previous MI.
3.1. Comparison of QT dispersion and TpTe in OSA patients with CAD severity:
In patients with mild OSA, there are no significant changes in QT dispersion in patients with different coronary territories. (P-value: 0.69) and the mean of QT dispersion also didn’t differ within these groups. TpTe also did not show any significant differences between these groups (P-value: 0.91). In patients with moderate OSA however, QT dispersion was significantly higher in patients with more coronary involvement (P-value: 0.045) but TpTe didn’t differ with the severity of vascular involvement (P-value: 0.9). However, in patients with severe and moderate OSA,
3.2. Comparing QT dispersion and TpTe in OSA patients with an ejection fraction of less than or over 40 %:
In patients with mild OSA, the mean of QT dispersion was higher in EF less than 40 % but the p-value was not significant (0.47). Also, TpTe was not significant between the groups (P-value: 0.37). In patients with moderate OSA, QT dispersion was statistically different between these groups (P-value: 0.012). The mean of QT dispersion was 67.8 inpatient with low EF vs 50.0 in patients with high EF respectively. TpTe didn’t differ (the mean of TpTe was higher in EF less than 40 % (89.4 vs 94.28). In patients with severe OSA, QT dispersion was also higher among patients with EF less than 40 % (0.048 vs 0.211) but TpTe didn’t differ significantly between these groups (mean of TpTe in patients with EF less than 40 % was 113.33 vs 130.0 with EF >40%). Figure 1
Comparison of QT dispersion and TpTe in OSA patients in previous MI history: In patients with mild OSA, QT dispersion and TpTe didn’t differ between groups with a history of previous MI. In patients with moderate OSA, QT dispersion was statistically higher in groups with previous MI history (P-value: 0.005) but TpTe didn’t differ (P-value: 0.18). In patients with severe OSA, QT dispersion was higher (P-value: 0.05)v but TpTe values didn’t differ in these groups (0.86). Figure 2 and Figure 3.
4. Discussion
OSA causes transient respiratory airway collapse which leads to transient hypoxemia and cardiac electrical instability [11]. These effects may progress to supraventricular and ventricular arrhythmia and finally to sudden cardiac death. Ventricular repolarization and arrhythmogenesis can be assessed by several electrocardiographic parameters including QT interval, QT dispersion, and TpTe. [12] Kilicaslan examined 23 patients with moderate to severe OSA without any cardiac abnormality and 23 patients within the control group. Only TpTe was longer in the OSA group but QT and QTc were not.[12] . However, they did not include any patients with cardiac disease. TpTe is used as an indicator of trans-mural dispersion in ventricular repolarization. Prolonged TpTe may predict ventricular arrhythmias and mortality. [13]. Alonso Fernandez et al. reported more daytime and especially nocturnal PVCs and bigeminies in patients with OSA but VT and AF were not found. Again they did not study patients with cardiac disease. [14] Yamashita et al. showed QT dispersion increased in patients with old MI and also increased in hypertension and OSA which may affect some bias in the study. [15] however, they didn’t specify any relation between CAD severity and OSA. Dursunoglu et al. studied QT dispersion changes in 96 patients without any previous cardiac and respiratory disorders. QTc was higher in patients with more AHI but patients with CAD were excluded. [16] Some studies also discussed the effect of obesity in QT interval, QT dispersion, and other ECG parameters but Pontiroli et al. didn’t find this relationship. [17] Kilicaslan et al. reported increased QT dispersion and TpTe in patients with moderate to severe OSA with CPAP therapy significantly reducing these parameters with a reduction in ventricular bigeminies and tachyarrhythmia. [12] Tasci et al. measured Pro-BNP as an indicating marker for congestive heart failure in patients with OSA [18]. They showed that Pro-BNP increased in patients with heart failure and OSA and effective CPAP therapy would reduce this level. [18] Jarrah et al. assessed 398 patients who underwent coronary angiography for one year and classified them into high-risk and low-risk for OSA based on a questionnaire. They found important relationship between coronary artery stenosis and OSA. [20] However, severity was classified only based on symptoms and not based on polysomnography. Konishi et al. studied 21 patients with OSA and 30 patients within the control group by OFDI-PCI. They found non-significant more severe stenosis with fibrous cap in the OSA group but the p-value did not reach statistical significance and they did not evaluate QTd or TpTe. [21] Silveria et al. found no relation between OSA and coronary angiographic findings based on the Gensini score in 80 patients. [22]. Mustafa Umut et al. did their study on patients with mild to moderate risk for CAD and based on the severity of OSA, they divided them into three categories. They found that patients with more severe findings in polysomnography had more calcified plaques found on CT angiography. [23] In this study, only patients with CAD risk factors were included and they didn’t include any patients with documented CAD. Based on our experiences, the risk of arrhythmias is higher in patients with prolonged QT and QT dispersions. We suggest that the above indices be followed closely in patients that may represent a group of patients at higher risk for cardiac events.
5. Conclusion
In our study, we evaluated 75 patients with documented CAD based on angiographic findings who underwent PCI. Moderate to severe OSA patients had higher QTd, especially in more severe cAD patients based on angiography, low EF, and history of previous MI. No significant differences were seen in these groups for TpTe interval. Our results suggest that OSA is an independent risk factor for QT changes, especially in precordial leads which would result in a higher possibility of arrhythmogenicity.
Shortcoming and future directions
We did not follow our patient over a longer period in order to evaluate our results in regard to sudden death. Furthermore, the effect of treatment was not studied. Larger clinical trials are warranted to confirm our results. Enrolling patients with acute coronary syndrome can further expand our knowledge about the importance of these indices for the occurrence of cardiac events.
Contribution
Each other had almost equal contribution in designing, writing and editing this manuscript.
Acknowledgments
The authors would like to acknowledge the support of Labbafinezhad medical center.
Statement of Conflict of Interest
There is no conflict of interest.
References
- Young T, Palta M, Dempsey J, Skatrud J, Weber S and Badr S. The occurrence of sleep disordered breathing among middle-aged adults.N Engl J Med. 1993;328:1230–1235. [CrossRef]
- Grimm W and Becker HF. Obesity, sleep apnea syndrome, and rhythmogenic risk. Herz. 2006 May;31(3):213-8.
- Kanagala R, Murali NS, Friedman PA, Ammash NM, Gersh BJ, Ballman KV, Shamsuzzaman AS and Somers VK. Obstructive sleep apnea and the recurrence of atrial fibrillation. Circulation 2003;107:2589–94.
- Gami AS, Olson EJ, Shen WK, Wright RS, Ballman KV, Hodge DO, Herges RM, Howard DE and Somers VK. Obstructive sleep apnea and the risk of sudden cardiac death: a longitudinal study of 10,701 adults. J Am CollCardiol 2013;62:610–16.
- Lattimore JDL, Celermajer DS and Wilcox I. Obstuctive sleep apnea and cardiovascular disease. J Am CollCardiol. 2003;41:1429–1437.
- Shahar E, Whitney CW, Redline S, Lee ET, Newman AB, Nieto FJ, O’Connor GT, Boland LL, Schwartz JE and Samet JM. Sleep-disordered breathing and cardiovascular disease: cross-sectional results of the Sleep Heart Health Study. Am J RespirCrit Care Med. 2001;163:19– 25.
- Caples SM, Wolk R, and Somers VK, “InGuence of cardiac function and failure on sleep- disordered breathing: evidence for a causative role,” Journal of Applied Physiology, vol. 99, no. 6, pp. 2433–2439, 2005.
- Kaneko Y, Floras JS, Usui K, Plante J, Tkacova R, Kubo T, Ando S and Bradley TD. “Cardiovascular effects of continuous positive airway pressure in patients with heart failure and obstructive sleep apneas,” New England Journal ofMedicine, vol. 348, no. 13, pp. 1233–1241, 2003. [CrossRef]
- Bazett HC. An analysis of the time-relations of electrocardiograms. Ann Noninvasive Electrocardiol 1997; 2: 177-94.
- Eslami V, Safi M, Taherkhani M, Adibi A and Movahed MR. Evaluation of QT, QT Dispersion, and T-Wave Peak to End Time Changes After Primary Percutaneous Coronary Intervention in patients presenting with acute ST-Elevation myocardial infarction. J INVASIVE CARDIOL 2013;25(5):232-234.
- Nakamura T, Chin K, Hosokawa R, Takahashi K, Sumi K, Ohi M and Mishima M. Corrected QT dispersionand cardiac sympathetic function in patients with obstructive sleep apnea-hypopnea syndrome. Chest. 2004;125:2107– 2114.
- Kilicaslan F, Tokatli A, Ozdag F, Uzun M, Uz O, Isilak Z, Yiginer O, Yalcin M, Guney MS and Cebeci BS. “Tp-e interval, Tpe/QT ratio, and Tp-e/QTc ratio are prolonged in patients with moderate and severe obstructive sleep apnea,” Pacing and Clinical Electrophysiology, vol. 35, no. 8, pp. 966–972, 2012. [CrossRef]
- Topilski I, Rogowski O, Rosso R, Justo D, Copperman Y, Glikson M, Belhassen B, Hochenberg M and Viskin S. The morphology of the QT interval predicts torsade de pointes during acquired bradyarrhythmias. J Am Coll Cardiol. 2007 Jan 23;49(3):320-8. [CrossRef]
- Alonso-Fernández A, García-Río F, Racionero MA, Pino JM, Ortuño F, Martínez I and Villamor J.Cardiac rhythm disturbances and ST segment depression episodes in patients with obstuctive sleep apnea-hypopnea syndrome and its mechanisms. Chest. 2005;127:15–22.
- Yamashita J, Nomura M, Uehara K, Nakaya Y, Uemura E, Iga A, Sawa Y, Nishikado A, Saito K and Ito S.. Influence of sleep apnea on autonomic nervous activity and QT dispersion in patients with essential hypertension and old myocardial infarction. J Electrocardiology. 2004;37:31–40. [CrossRef]
- Dursunoglu D, Dursunoglu N, Evrengül H, Ozkurt S, Kiliç M, Fisekci F, Kuru O and Delen O. QT interval dispersion in obstructive sleep apnea syndrome patients without hypertension. EurRespir J. 2005;25:677–681.
- Pontiroli AE, Pizzocri P, Saibene A, Girola A, Koprivec D and Fragasso G Left ventricular hypertrophy and QT interval is obesity and in hypertension: effects of weight loss and of normalization of blood pressure. Int J Obesity. 2004;28:118–123.
- Tasci S, Manka R, Scholtyssek S, Lentini S, Troatz C, Stoffel-Wagner B and Lüderitz B. “NT-pro-BNP inobstructive sleep apnea syndrome is decreased by nasal continuous positive airway pressure,” Clinical Research inCardiology, vol. 95, no. 1, pp. 23–30, 2006.
- Strehmel R, Valo M, and Teupe C. “Natriuretic peptide and high-sensitive troponin t concentrations correlate with effectiveness of short-term cpap in patients with obstructive sleep apnea and coronary artery disease,” Clinical MedicineInsights: Circulatory, Respiratory and Pulmonary Medicine, vol. 10, pp. 33–39, 2016. [CrossRef]
- Jarrah MI, Yassin AM, Ibdah RK, Ibnian AM, Eyadeh AA and Khassawneh BY. “Screening for obstructive sleep apnea amongpatients undergoing coronary catheterization in Jordan” Vascular Health and Risk Management 2019:15 109–113.
- Konishi T, Kashiwagi Y, Funayama N, Yamamoto T, Murakami H, Hotta D and Tanaka S. “Obstructive sleep apnea is associated with increased coronary plaque instability: an optical frequency domain imaging study” Heart and Vessels (2019) 34:1266–1279.
- Rivera-Pérez SJ, Martinez D, Araujo GN, Goncalves SC, Lazzaretti LK, Wainstein RV, Wainstein MV and Ribeiro JP. “Severity of obstructive sleep apnea and extension of coronary artery disease” Sleep and Breathing (2019) 23:747–752.
- Umut Somuncu M, Bulut U, Karakurt H, Utkusavas A, Akbay E and Kartal Kilinc F. “The Relationship Between Obstructive Sleep Apnea and Coronary Plaque: A Coronary Computed Tomographic Angiography Study” Acta Cardiol Sin 2019;35:325_334.
Figure 1.
Mean QTd in moderate obstructive sleep apnea (OSA) based on Multi-vessel coronary disease (SVD=Single vessel disease, 2VD= 2 vessel disease, 3VD=3 vessel disease) , ejection fraction(EF) and history myocardial infarction (MI).
Figure 1.
Mean QTd in moderate obstructive sleep apnea (OSA) based on Multi-vessel coronary disease (SVD=Single vessel disease, 2VD= 2 vessel disease, 3VD=3 vessel disease) , ejection fraction(EF) and history myocardial infarction (MI).
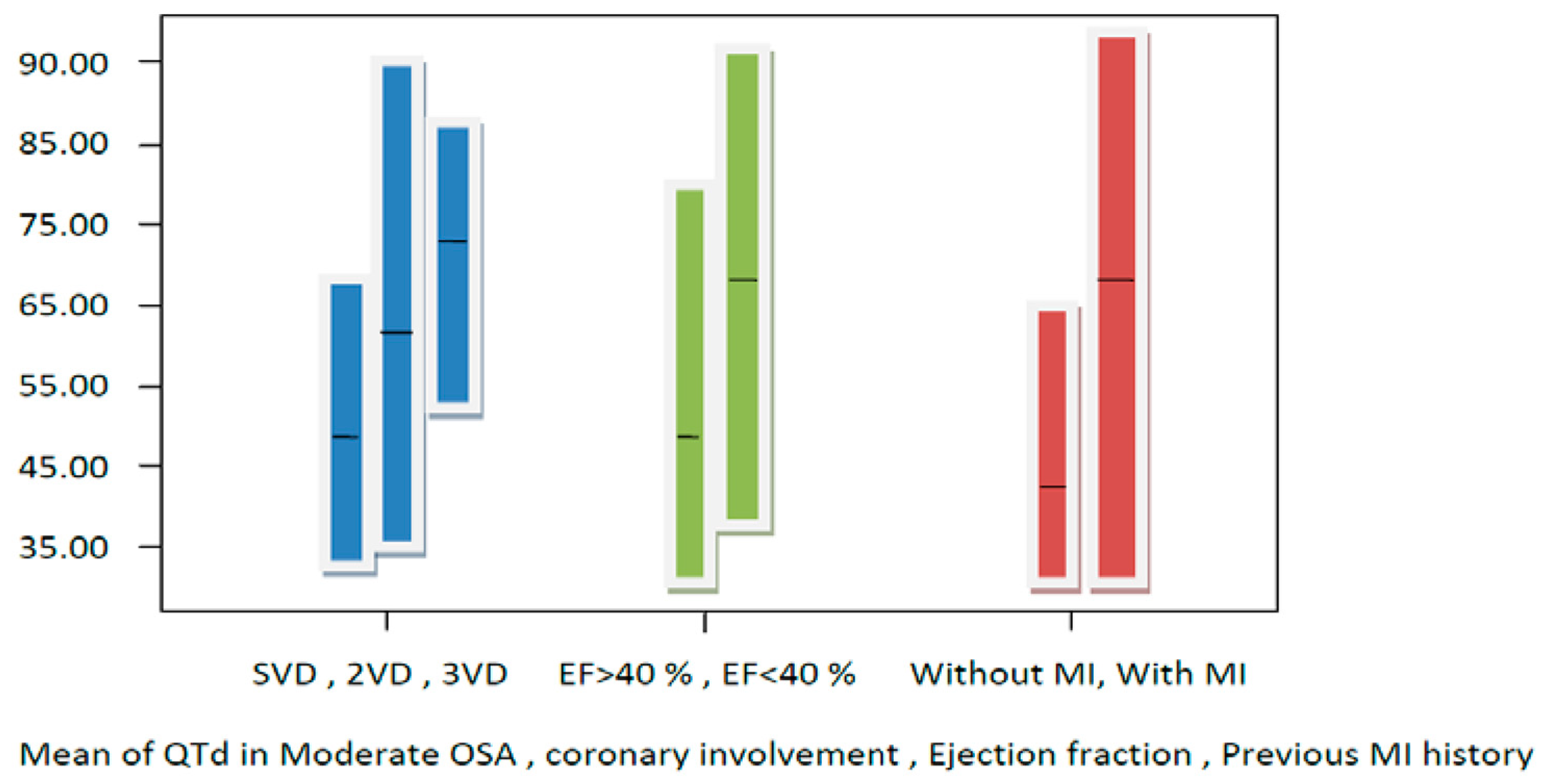
Figure 2.
Mean QTd in severe obstructive sleep apnea (OSA) based on Multi-vessel coronary disease (SVD=Single vessel disease, 2VD= 2 vessel disease, 3VD=3 vessel disease) , ejection fraction(EF) and history myocardial infarction (MI).
Figure 2.
Mean QTd in severe obstructive sleep apnea (OSA) based on Multi-vessel coronary disease (SVD=Single vessel disease, 2VD= 2 vessel disease, 3VD=3 vessel disease) , ejection fraction(EF) and history myocardial infarction (MI).
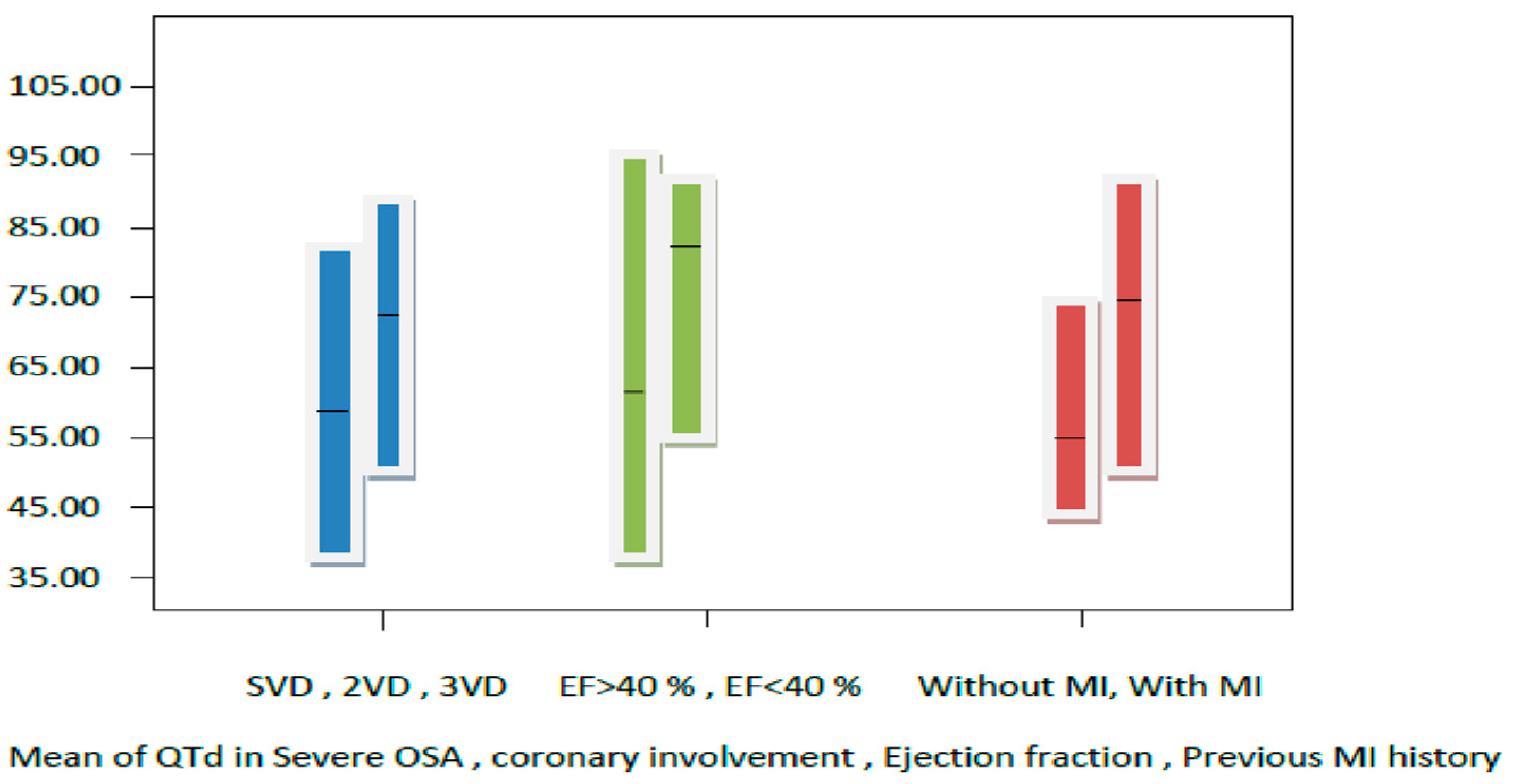
Figure 3.
comparison of QTd and TpTe in severe/moderate and mild obstructive sleep apnea (OSA) patients based on coronary involvement , ejection fraction(EF) and history of myocardial infarction (MI).
Figure 3.
comparison of QTd and TpTe in severe/moderate and mild obstructive sleep apnea (OSA) patients based on coronary involvement , ejection fraction(EF) and history of myocardial infarction (MI).
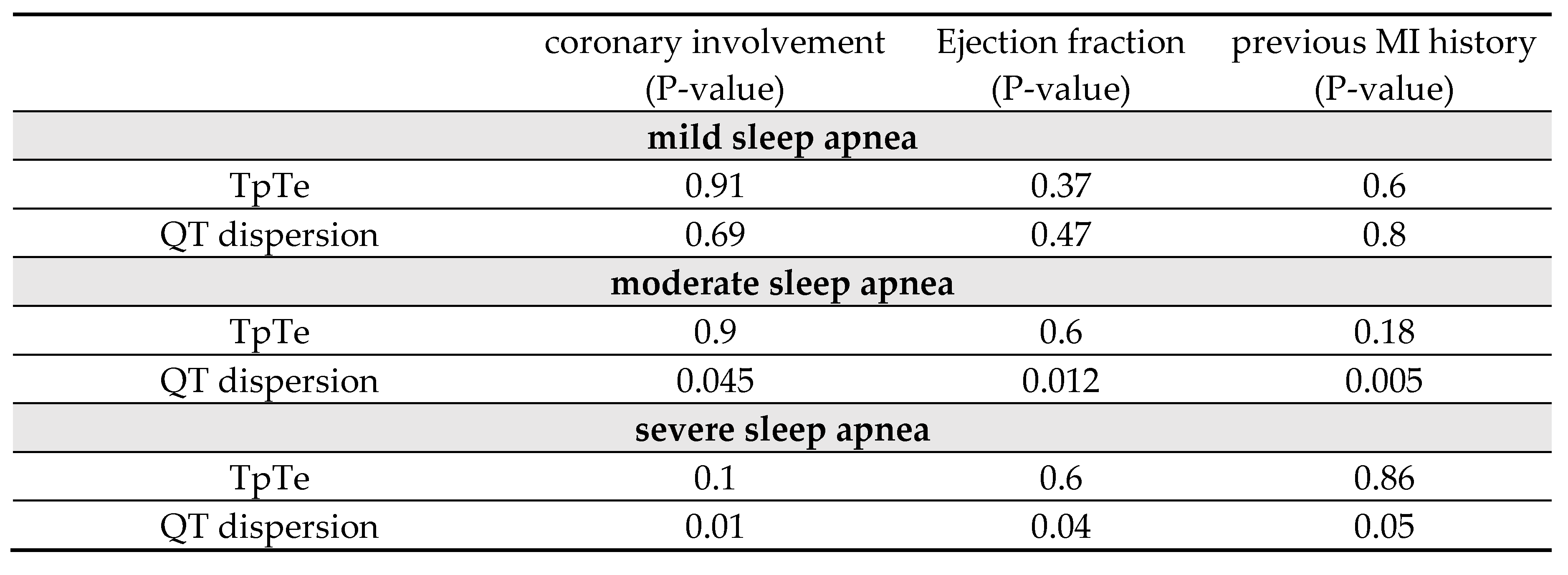

Table 1.
Baseline characteristics.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



