
Submitted:
05 August 2023
Posted:
08 August 2023
You are already at the latest version
Abstract
Asthma is a chronic respiratory disease that impairs breathing. Management of asthma presents a significant challenge due to its inherent variability; that is, its symptoms can substantially differ among individuals, thereby complicating the prediction and management of exacerbations. Furthermore, individuals with asthma often have unique triggers that precipitate symptoms or attacks. The identification of these triggers can often prove to be a challenging, and at times, an impractical attempt. To address this, our research proposes a practical, personalized alert system, predicated on individual lung function tests conducted under varying environmental conditions classified by air-quality sensors. To validate this concept, we conducted an observational pilot study involving healthy individuals. We recruited twelve healthy participants and monitored their responses across a broad spectrum of environments, characterized by varying air quality, temperature, and humidity conditions. The lung function for each participant, assessed using peak expiratory flow (PEF) values, was recorded in each of these environments. Our results highlighted substantial variability in pulmonary responses to different environments. Utilizing these insights, we proposed a personalized alarm system that provides real-time air-quality monitoring and issues alerts when environmental conditions may potentially become unfavorable. We also explored the feasibility of employing basic machine learning techniques to predict PEF values in the aforementioned environmental conditions. This proposed system has the potential to empower individuals in actively safeguarding their respiratory health and mitigating discomfort caused by environmental conditions, especially in cases of asthma patients. By enabling timely and personalized interventions, the system aims to provide individuals with the necessary tools to minimize exposure to asthma’s possible triggers.
Keywords:
respiratory health
; real-time air-quality monitoring
; lung functionality
; alert system
1. Introduction
Asthma, a chronic pulmonary disorder, afflicts approximately 374 million people globally with annual 461,000 deaths [1]. It is concerning to acknowledge that despite the highest incidence of asthma being reported in countries with high socio-demographic indices (SDIs), the maximum mortality rate due to this condition is observed in low and middle SDI countries [2]. According to the most recent report from the Global Initiative for Asthma (GINA), asthma remains insufficiently diagnosed, with its prevalence being inadequately documented in numerous middle and low-income countries [3]. A closer look at the United Arab Emirates (UAE) reveals that the disease prevalence among school-aged children is approximately between 9.8% and 11.9%, with some variability attributable to age [4]. In neighboring Saudi Arabia, the situation is similar, if not more concerning. The number of children with asthma is much higher than adults, with rates varying from 9% to 33.7% depending on the area [5]. In the broader Middle East region, asthma prevalence varies between 4.4% and 7.6% [6]. Asthma is defined by periodic episodes of wheezing, shortness of breath, and coughing, caused by the inflammation and narrowing of the respiratory tract. This chronic condition stems from the complex interaction of genetic and environmental elements, such as air pollution. Asthma places an enormous strain on patients' physical, social, emotional, and professional lives, with a significant impact on their quality of life and a marked burden on healthcare systems worldwide.
One of the significant challenges in asthma management lies in the substantial variability in individual symptoms and triggers [7]. These triggers, which differ from person to person, can include physical exercise, adverse weather conditions, exposure to cold, dry air, specific food substances, food additives, and tobacco smoke [8]. Other triggers identified include changes in air temperature, humidity, and strong odors. Recognizing and avoiding asthma triggers are pivotal in effective disease management. However, this often poses a significant challenge due to the difficulty in not only identifying these triggers but also actively avoiding them [9]. This complexity is further exacerbated by the fact that these factors can affect individuals at varying degrees [3]. Consequently, for those living with asthma, mitigating acute episodes is of paramount importance, necessitating continuous monitoring of potential triggers. Crucially, this highlights the urgent need for developing methods to predict these trigger factors early on [10]. A review of existing literature reveals that most studies primarily relied on bio-signal factors associated with asthma for prediction [11]. Meanwhile, a limited number of studies have considered environmental factors [12], and even fewer studies have incorporated both these elements in their research [13].
Asthma management has traditionally centered on medication use, patient education, and triggers avoidance, with recent trends shifting towards integrated care approaches aimed at improving asthma control and enhancing patients' quality of life [14]. Despite these strides, a prevailing challenge persists in the substantial variability of symptoms and triggers among individuals, calling for a more personalized approach to asthma management [15]. These personalized strategies have gained increased focus in modern healthcare, taking into consideration the specific asthma phenotype and endotype of each individual [16]. This personalized approach, facilitated by advanced understanding of asthma's pathophysiology, has spurred targeted biologic therapies and precision medicine [17]. Additionally, there is a growing interest in leveraging digital health interventions and smart inhaler technologies for continuous monitoring and provision of personalized feedback to patients [18]. Despite these promising advancements, the domain of personalized asthma management is still in its relative infancy and necessitates further research to refine and amplify its strategies, particularly through real-time monitoring and predictive analytics [19].
Personalized alert systems have increasingly played a vital role in chronic disease management, offering novel approaches to condition monitoring and real-time response mechanisms. In diabetes management, for instance, continuous glucose monitoring systems integrated with alert features have proven beneficial in facilitating timely intervention, thus enhancing glycemic control and reducing hypoglycemic episodes [20,21]. Similarly, in heart disease management, remote patient monitoring systems with personalized alert functions have shown potential in early detection of cardiac anomalies, reducing hospitalization rates, and improving patients' quality of life [22,23]. In the context of chronic respiratory diseases like asthma or COPD (Chronic Obstructive Pulmonary Disease), the emergence of smart inhalers and spirometers that provide real-time feedback and personalized alerts on medication usage and lung function can potentially transform disease management [24,25]. These developments signal a growing trend towards a more proactive, personalized approach to chronic disease management that emphasizes real-time monitoring, early intervention, and patient engagement.
In addition to biological factors, it is imperative to acknowledge that environmental variables have historically played a significant role in triggering asthma symptoms. Indoor allergens including dust mites, pet dander, and mold, together with particular environmental factors like humidity and temperature swings, have been connected to an increase in asthma-related hospital admissions and a decline in lung function in asthma sufferers [26,27]. Another substantial environmental risk factor that can severely affect asthma control is tobacco smoke [28]. The importance of incorporating these environmental factors into individualized asthma management strategies, which may include the use of alert systems to warn patients of poor air-quality or extreme weather conditions that may exacerbate their symptoms, is highlighted by the realization that these environmental factors have a significant impact on asthma exacerbation.
Given all the above about the inherent variability and unpredictability of asthma, there is a growing need for more personalized monitoring strategies. Current standard monitoring methods, while effective for the majority, often fail to cater to individuals with distinct symptom profiles and overlook the impact of unique triggers [29]. Addressing these issues necessitates a paradigm shift towards a more personalized strategy that accurately acknowledges unique symptom profiles and trigger patterns while considering both biological signals and environmental influences and proposing simple and practical ways to monitor them.
Our research is geared towards creating an affordable, practical, and personalized alert system to revolutionize asthma management. Based on individual pulmonary function tests and real-time environmental data, our proposed system aims to provide timely, personalized alerts according to the individual's respiratory health status. We propose that this tailored approach will gradually empower individuals to proactively monitor their respiratory health, foresee potential exacerbations, and initiate timely interventions, consequently avoiding asthma attacks and enhancing their overall quality of life. While our current study focuses on healthy individuals, we believe that the concept and scenario are applicable and beneficial for asthmatic patients [17].
2. Methodology
2.1. System Overview
Our objective in designing the personalized alert system is to safeguard individuals' respiratory wellbeing by issuing timely alerts prior to their exposure to potentially discomforting environmental conditions. This is achieved by monitoring and correlating their lung function with specific environmental data. Given the considerable variability of lung function among individuals, our goal is to create a system capable of accommodating this diversity and delivering tailored alerts that align with each individual's unique respiratory characteristics. The alert system operates by integrating data from two primary sources: individual lung function tests and real-time environmental monitoring.
For the lung function tests, we used spirometers to capture peak expiratory flow (PEF) values, recorded from Microlife PF-100 Electronic Peak Flow Digital Asthma Monitor Meter [30]. PEF values are a reliable measure of lung function, and fluctuations in these values can indicate a potential asthma attack. For environmental monitoring, we deployed two types of portable air-quality sensors, one custom-built and the other commercially available, both adept at identifying a variety of common asthma triggers, such as particulate matter, humidity, and temperature fluctuations. The custom-built sensor in this experiment has neither direct contact nor giving prescriptive actions to the study participants. It was incorporated parallelly in this pilot study for validation purposes, and to facilitate future use. When the system predicts a potential risk, it generates an alert. The alerts are designed to be unobtrusive yet attention-grabbing, delivered through the device and the associated smartphone app. The app not only notifies the individual of a potential risk but also provides initial recommendations on how to avoid it, such as staying indoors or refreshing the room air. More options can be added as needed (details are in the result section).
2.2. Air-Quality Sensors
In this study, we employed two types of sensors to gauge the quality of air within a room: a customized lab made sensor constructed using an ESP32 microcontroller, Figure 1 and Figure 2, and a commercial air-quality sensor to authenticate the readings obtained from the customized device, Figure 3. We are utilizing the customized sensor to facilitate the programming of varying alarm thresholds, which were based on data derived from the PEF reader, details are in Figure 4. Such a feature is not accessible in commercial sensors.
The sensors were designed to monitor various elements including Humidity, Temperature, Fine particulate matter with a diameter of 2.5/10 micrometers or smaller (PM2.5)/(PM10), Total Volatile Organic Compounds (TVOC), and Carbon Dioxide (CO2). In the customized device, we employed the DHT-11 sensor module to record temperature and humidity readings, while the TVOC sensor module was utilized to assess air-quality and the Carbon Dioxide (CO2) levels. The PM2.5 sensor module was used to measure dust particles. Table 1 outlines the range of recorded values, the corresponding sensor module used, and the range of sensed data. The architecture of the sensor node in terms of the required sensor array and the employed microcontroller is illustrated in Figure 2.
2.3. Lungs Function Tester
The selection of participants for our pilot study was centered on healthy young individuals who did not have a known diagnosis of asthma or any other chronic respiratory condition. We chose healthy volunteers to control for any potential confounding effects that existing respiratory conditions might have on lung function or response to environmental conditions. A total of 12 volunteers, aged between 20 and 25 years, were recruited as participants for the study, as shown in Table 2. Prior to their involvement, all participants provided informed consent for their participation in the research. The study was approved by the Ethic Committee of the University of Tabuk.
For lung function tests, we used a standard spirometer to measure Peak Expiratory Flow (PEF) values [30]. These values provide a measure of the maximum speed at which participants can exhale, offering a reliable indicator of lung function. PEF is a measure of how fast a person can exhale air after taking a deep breath, and it is influenced by various factors, including environmental conditions. Participants were instructed on the proper use of the spirometer, and measurements were taken three times for each participant in each environment, after being in the environment for 20 minutes, to ensure accuracy. The best of these three values was recorded as the participant's PEF for that specific environmental condition. Upon completion of the data collection process, participants were requested to fill out a brief survey. The survey was used to streamline data collection and minimize external factors. The survey consists of three concise questions: A) Did the participant experience breathing discomfort during the experiment? (yes/no). B) Were there any factors that may have affected the data collection? (yes/no). C) If yes, could the participant specify the factor and provide additional comments? This step was crucial to provide subjective insights that may complement the objective data collected through the PEF.
2.4. Collection of Environmental Data and PEF
In our research, we employed air-quality sensors (AQS) to measure an array of environmental parameters, encompassing levels of particulate matter, relative humidity, and ambient temperature. PEF was monitored in parallel with these air-quality metrics under four distinct environmental conditions: typical daily conditions, conditions with moderate dust/smoke enrichment, moderate temperature conditions, and moderate humidity conditions. Given the observational nature of our study, we instructed participants to measure their PEF and document the readings from the AQS in their primary living and sleeping spaces during standard conditions. An average AQS value was computed from these recorded values for analysis. Under the conditions of moderate dust/smoke enrichment, participants were instructed to record PEF and AQS measurements during their routine home incense-burning activities. For scenarios with moderate temperature, participants were asked to conduct the PEF and AQS measurements in the afternoon within a room where the air conditioning system had been turned off for the entire day. Finally, in the conditions of moderate humidity, participants recorded PEF and AQS measurements during the afternoon in a room where the air conditioner was operating in its dehumidifying, or "dry", mode without its cooling function activated.
The collected environmental data was rigorously analyzed in tandem with the participants' lung function data. We applied simple statistics to discern patterns and correlations between specific environmental conditions and changes in PEF values (details are in the results section). This approach allows us to establish a baseline of how each individual's lung function, as measured by PEF, responds to different environmental conditions. This analysis formed the basis of our proposed personalized alert system, enabling us to identify potential environmental triggers for each individual and thereby tailor the alert system to each participant's unique profile.
3. Results and Discussion
3.1. PEF in Standard Environment Condition
The collected data from the air-quality device, in conjunction with corresponding best of three PEF reading after a duration of 20 minutes spent within a standard indoor environmental condition, is demonstrated in Table 3. From the table we can conclude: First, we conducted a comparative analysis between our custom-built sensor and the commercially available counterpart. By comparing these air-quality measurements, we identified a high mean correlation coefficient of the recorded values of 95%. The noteworthy correlation coefficient signifies the reliability and accuracy of our custom device when compared against the commercial standard. This demonstrates the potential of our customized device as an affordable, yet precise open-sourced tool for monitoring air-quality and potential asthma triggers in real-time, and its potential integration into a personalized alert system for asthma management.
Second, we juxtaposed the air quality values derived from these sensors with the recorded PEF values. In other words, we evaluated the pearson correlation coefficient for each environmental variable in relation to the PEF values. Results are illustrated in Table 4. This assessment allowed us to discern which environmental factors had the greatest effect with PEF values. We found that the PM2.5 value had the strongest correlation with the PEF value. Other parameters, however, did not demonstrate a significant correlation (<0.5). These preliminary results suggest that PM2.5 levels are important to monitor, as they potentially exert a significant impact on PEF values.
Third, Table 3 confirms the healthy status of all study participants. Their PEF values were categorized following the criteria established by the Hankinson model [32]. According to this model, PEF values exceeding 80% of the predicted optimum are classified as 'normal' - a category often referred to as the 'green zone'. All participants in our study fell within this 'green zone', underscoring their healthy condition.
3.2. PEF in different Environment Condition
Table 5 showcases the average and the standard deviation (SD) values registered from the air-quality sensor across varying environmental conditions to which the study participants were experienced. For ease of understanding, we've categorized these environmental conditions into 1) Air-quality room (Good, Medium), 2) Temperature (Normal, Slightly-Hot), and 3) Humidity (Normal, Slightly-High). In the interest of safeguarding our participants, we consciously avoided subjecting them to drastic changes in environmental conditions, which could have possibly resulted in a more substantial correlation with PEF values. Despite this approach, which might be viewed as a limiting factor, our intent was to maintain the study as an initial exploration primarily aimed at understanding the overall effect of diverse environmental parameters on PEF values. The driving principle behind this decision was our objective to validate our study's concept, while ensuring that participant safety remains paramount. The table indicates that in a room with medium air-quality, there was a noticeable rise in PM2.5 levels by 67%. Similarly, in a room with a slightly elevated temperature, there was a 45% increase in the temperature recorded. Moreover, in a room with slightly high humidity, the humidity levels saw a surge of 66%.
Table 6 presents the PEF values under the different environmental conditions. This table reveals that PEF responds differently to different environmental conditions among participants. For instance, a noticeable decrease in PEF values was observed in some individuals when exposed to high levels of particulate matter PM2.5, suggestive of a potential trigger. Contrarily, variations in humidity and temperature did not evoke significant changes in PEF measurements for certain participants. Despite all participants experiencing the same environmental settings shifts, their PEF values varied, suggesting that their respiratory systems responded uniquely to these stimuli. Participants 3, and 10, for instance, demonstrated heightened sensitivity to minor changes in room air-quality in comparison to others. Consequently, it might be beneficial to establish lower thresholds for their air-quality alarms. By doing so, these individuals would receive early warnings, enabling them to vacate the room ahead of others, thereby ensuring their well-being.
The numbers underlined in the table represent participants who reported experiencing respiratory discomfort during the experiment, as per the first question of the administered survey. In response to the second and third questions of the survey, which probe for potential factors influencing data collection or any noteworthy comments, there were no significant points reported. These underlined values highlight some notable observations. Participant 10 reported experiencing respiratory discomfort, which corresponded with a significant drop in her PEF value (>0.4). Conversely, Participant 9 reported respiratory discomfort without a corresponding dip below the predetermined PEF threshold (<0.4). This is aligned with variability of normal human physiology and suggests that the threshold value for air quality alerts should be personalized and dynamically adjusted, considering each individual's unique respiratory comfort level.
3.3. Personalized Threshold Identification
In order to determine potential triggers for participant(s), we evaluated the correlation between environmental conditions and changes in PEF values. The identification of personalized triggers was based on observing substantial decreases in PEF values when individuals were exposed to specific environmental conditions, Table 6. From Table 5 and Table 6, we can conclude that when PM2.5 has increased to 67%, 2 out of the 12 participants could has more than 4% changes on their PEF values, and one of those 2 has felt uncomfortable. Setting an alarming system for these participants for instance can happen whenever PM2.5 increase up to 30-40% from the standard room value considering their sensitivity to PM2.5 value. Although some other participants reporting discomfort (the underlined value of participants 9), we did not observe significant changes in their PEF values. This observation was not the focus of this study and hence has been set aside. However, this highlights the potential influence of other factors beyond lung function that could be considered in future research.
While our initial expectation was to establish an individual threshold for each participant, limitations related to sample size and the slight variations in environmental conditions guided us to divide our participants into two groups. One group demonstrated higher sensitivity to air-quality changes, reflected in a PEF change of more than 4% (arbitrarily set), while the other group showed lesser sensitivity. Consequently, for the first, more sensitive group, we suggest setting the air-quality alert threshold to a 30-40% change in PM2.5. This would mean that if the PM2.5 value shifts by this percentage, an alert would be triggered, advising them to either leave the room or ventilate the space to improve air-quality.
Figure 4 illustrate the overall model of the proposed personalized alerting system, taking into account the insights gained from Table 3, Table 5, and Table 6. The model consists of two stages: the initial stage and the personalized stage. In the initial stage, the system prompts the user to measure PEF in various environmental conditions. The model then calculates the changes in PEF values in relation to the changes in air-quality observed in these environments. Based on this information, the model sets the alert threshold on the customized air-quality device. Once the threshold is set, the system enters the personalized stage. During this stage, the air-quality device periodically alerts the user to potential exposure to uncomfortable environmental conditions. The alerts serve as reminders for the user to take necessary precautions or adjust to ensure their comfort in response to the detected changes in air-quality.
3.4. Predicting PEF Values in Different Environmental Conditions
In this study, we also explored the application of machine learning models to predict PEF values in different environmental conditions, focusing specifically on PEF in both good AQ and medium AQ conditions. The goal was to investigate the feasibility and effectiveness of using machine learning algorithms to accurately predict PEF values in these specific environmental contexts. To achieve this, we employed feature selection methods, namely CfsSubsetEval [33] and the Best_First search method, to identify the most relevant features that have an impact on PEF values in each condition. We then tested several classifiers, including linear regression, Multilayer Perceptron, and SMOreg (support vector machine for regression) [34], to predict PEF values in both conditions, Table 7. Although the root mean squared error (RMSE) values were relatively high, likely due to the limited size of our datasets, we observed interesting patterns: 1) Predicting PEF values in good air-quality conditions proved to be challenging using the available parameters. 2) We noted the potential in predicting PEF values for medium AQ conditions using a subset of the existing features. These findings suggest that it is possible to predict PEF values, particularly for individuals who are sensitive to increases in PM2.5 levels. However, we did not investigate the prediction of PEF in high temperature or high humidity conditions due to the lack of significant changes in PEF values under these conditions, Table 6. The overall finding at this stage highlights the need for further exploration and improvement in predicting PEF values under different conditions. It's pertinent also to note that, as we are developing our own air-quality sensors, we are considering the addition of a carbon monoxide (CO) sensor in future design. Given the known impact of CO on prevalent obstructive lung diseases such as asthma and COPD, we anticipate that this inclusion could offer significant value. Specifically, we expect a high correlation between changes in CO levels and alterations in PEF.
Table 7 provides information on the performance of selected attributes and regression models for predicting PEF in different conditions. The input attributes, target attribute, attribute evaluator, and search method are specified for each case. The table also displays the selected attributes in order of relevance, along with the correlation coefficient (CC) and RMSE values obtained from linear regression, multilayer perceptron, and SMOreg model. The results highlight the effectiveness of the selected attributes and the performance of the regression models in predicting PEF in the respective conditions.
3.5. Insights and Limitation
From literature, we acknowledge the potential influence of factors such as air-quality, temperature, and humidity on individual PEF values, however, the main objective of this pilot study was to demonstrate the potential of developing personalized air-quality sensor alerts. These alerts are customized based on an individual's lung function and readings obtained from different environmental conditions. By considering these factors, the proposed model aims to provide tailored alerts to individuals, enabling them to take proactive measures in response to their unique respiratory health needs. Another aspect we explored in this research was the use of machine learning. Our preliminary experiment suggests that there is potential to predict PEF values in different environmental scenarios by increasing the number of participants and environmental conditions. Although our study had limitations due to the small sample size and limited environmental variations, the results indicate promising avenues for further research and improvement. By incorporating machine learning techniques and expanding the dataset in real-world studies, we can enhance the accuracy and applicability of PEF predictions in diverse environmental conditions.
There are several limitations in this study that we acknowledge, such as the small sample size, minor variations in environmental conditions, and the necessary time duration for each participant to stay in each environment in order to effectively measure changes in PEF. These constraints also precluded us from conducting comprehensive statistical significance tests. While acknowledging the limitations at this stage of our study, we contend that the novelty of our research is rooted in highlighting the variability of individual PEF reactions to environmental shifts. As such, it's clear that the prevailing "one-size-fits-all" model adopted by existing air-quality sensors in the market is not practically viable. Thus, our study highlights a methodology for creating a customized array of alert systems. These systems are specifically designed to adapt to each individual's unique lung functions and possess the capability to evolve and learn over time.
In the next stages of this study, we aim to address the limitations of this work by expanding our participant sample size for more diverse data and conducting a longitudinal study to better understand the real-world impacts of environmental changes on lung function over time. We will also include a broader range of environmental factors, such as pollution levels and allergens, and continue to refine our personalized alerting system, which will be tuned by Machine learning models. Ultimately, we envision testing our system through clinical trials to assess its effectiveness and make necessary adjustments for real-world implementation. Our goal remains to develop a responsive and individualized alerting system for people with varying lung functions.
While our pilot study is focused on healthy individuals, this selection is pivotal to the validation of the overall concept. From an ethical perspective, it would be unseemly to expose asthmatic individuals at high risk to known respiratory irritants within the context of this study. Instead, our approach necessitates conducting an introductory examination on healthy participants, gradually modifying the system for higher risk groups within real-world contexts after the institution of all requisite safety protocols. Furthermore, demonstrating lung function variability amongst low-risk individuals strongly suggests the potential for the alert system to be adaptable and efficacious for higher risk individuals, including asthma patients. This indication is not only plausible but offers a compelling case for the adaptability of our system. We perceive this methodological approach as a strength of our study. Given that well-controlled asthma patients generally exhibit low PEF variability, akin to healthy individuals, they will be an appropriate group for further study. Conversely, poorly controlled asthmatics at high risk usually present high PEF variability, which our proposed alert system should more likely detect [14,17,35].
4. Conclusions
This pilot study highlights the potential of personalized approaches in the management of asthma, a chronic condition that presents a significant global health challenge. We have demonstrated the feasibility of an alert system that associates individual lung functions with changes in environmental data, providing a personalized alarming system to aid proactive asthma management. Although preliminary, this result highlights its potential as a robust tool for individuals to actively monitor their respiratory health, anticipate potential respiratory discomfort, and initiate timely interventions. While we acknowledge that our study was conducted on healthy individuals, the trends and patterns observed provide us with a firm basis for predicting how such a system might benefit those living with chronic respiratory conditions like asthma. Based on the pathophysiology of asthma disease, airways and therefore PEF are highly sensitive to environmental triggers, and we speculate that using such a personalized alarm system would be a valuable tool to augment asthma management. As we advance into an era marked by a growing emphasis on personalized healthcare and digital health technologies, it is vital to continue to explore and innovate ways to make the management of conditions like asthma more tailored, proactive, and efficient. The presented alert system structure is one step towards this vision, illustrating a compelling intersection of personalized healthcare and technology.
Author Contributions
Conceptualization, All Authors; methodology, All Authors.; software, M.A., T.A., B.A.A.; validation, M.A., T.A., B.A.A. A.B., and F.A.; formal analysis, M.A., A.B., and F.A.; resources, All Authors; data curation, T.A., B.A.A.; writing—original draft preparation, M.A., F.A.; writing—review and editing, All authors; visualization, M.A., F.A., L.A.; supervision, M.A., F.A.; project administration, M.A.; funding acquisition, M.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this research work through the project number (S-1442-0049).
Institutional Review Board Statement
Ethical approval number: UT-300-141-2023.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bateman, E.D.; Hurd, S.S.; Barnes, P.J.; Bousquet, J.; Drazen, J.M.; FitzGerald, M.; Gibson, P.; Ohta, K.; O’Byrne, P.; Pedersen, S.E.; et al. Global Strategy for Asthma Management and Prevention: GINA Executive Summary. European Respiratory Journal 2008, 31, 143–178. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. The Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- 2022 GINA Main Report. Available online: https://ginasthma.org/gina-reports/ (accessed on 4 July 2023).
- Ibrahim, N.M.; Almarzouqi, F.I.; Al Melaih, F.A.; Farouk, H.; Alsayed, M.; AlJassim, F.M. Prevalence of Asthma and Allergies among Children in the United Arab Emirates: A Cross-Sectional Study. World Allergy Organization Journal 2021, 14, 100588. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, S.A.; Kobeisy, S.A.N.; AlKhater, S.A.; Alharbi, A.S.; Alqwaiee, M.M.; Alotaibi, F.N.; Alawam, K.A.; Alahmadi, T.S.; Al-Somali, F.M.; Almaghamsi, T.M.; et al. Childhood Asthma Awareness in Saudi Arabia: Five-Year Follow-Up Study. Journal of Asthma and Allergy 2020, 13, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Tarraf, H.; Aydin, O.; Mungan, D.; Albader, M.; Mahboub, B.; Doble, A.; Lahlou, A.; Tariq, L.; Aziz, F.; El Hasnaoui, A. Prevalence of Asthma among the Adult General Population of Five Middle Eastern Countries: Results of the SNAPSHOT Program. BMC Pulm Med 2018, 18, 68. [Google Scholar] [CrossRef]
- Szefler, S.J.; Chipps, B. Challenges in the Treatment of Asthma in Children and Adolescents. Annals of Allergy, Asthma & Immunology 2018, 120, 382–388. [Google Scholar] [CrossRef]
- Janssens, T.; Ritz, T. Perceived Triggers of Asthma: Key to Symptom Perception and Management. Clinical & Experimental Allergy 2013, 43, 1000–1008. [Google Scholar] [CrossRef]
- L Miller, R. Trigger Control to Enhance Asthma Management - UpToDate. Available online: https://www.uptodate.com/contents/trigger-control-to-enhance-asthma-management (accessed on 27 May 2023).
- Alharbi, E.T.; Nadeem, F.; Cherif, A. Predictive Models for Personalized Asthma Attacks Based on Patient’s Biosignals and Environmental Factors: A Systematic Review. BMC Medical Informatics and Decision Making 2021, 21, 345. [Google Scholar] [CrossRef]
- Tibble, H.; Tsanas, A.; Horne, E.; Horne, R.; Mizani, M.; Simpson, C.R.; Sheikh, A. Predicting Asthma Attacks in Primary Care: Protocol for Developing a Machine Learning-Based Prediction Model. BMJ Open 2019, 9, e028375. [Google Scholar] [CrossRef]
- Ram, S.; Zhang, W.; Williams, M.; Pengetnze, Y. Predicting Asthma-Related Emergency Department Visits Using Big Data. IEEE J Biomed Health Inform 2015, 19, 1216–1223. [Google Scholar] [CrossRef]
- Lee, C.-H.; Chen, J.C.-Y.; Tseng, V.S. A Novel Data Mining Mechanism Considering Bio-Signal and Environmental Data with Applications on Asthma Monitoring. Computer Methods and Programs in Biomedicine 2011, 101, 44–61. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.L.; Bacharier, L.B.; Bateman, E.; Boulet, L.-P.; Brightling, C.; Buhl, R.; Brusselle, G.; Cruz, A.A.; Drazen, J.M.; Duijts, L.; et al. Key Recommendations for Primary Care from the 2022 Global Initiative for Asthma (GINA) Update. npj Prim. Care Respir. Med. 2023, 33, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Papi, A.; Brightling, C.; Pedersen, S.E.; Reddel, H.K. Asthma. Lancet 2018, 391, 783–800. [Google Scholar] [CrossRef] [PubMed]
- Holguin, F.; Cardet, J.C.; Chung, K.F.; Diver, S.; Ferreira, D.S.; Fitzpatrick, A.; Gaga, M.; Kellermeyer, L.; Khurana, S.; Knight, S.; et al. Management of Severe Asthma: A European Respiratory Society/American Thoracic Society Guideline. European Respiratory Journal 2020, 55. [Google Scholar] [CrossRef]
- Singh, V.; Meena, P.; Sharma, B.B. Asthma-like Peak Flow Variability in Various Lung Diseases. Lung India 2012, 29, 15–18. [Google Scholar] [CrossRef]
- Merchant, R.K.; Inamdar, R.; Quade, R.C. Effectiveness of Population Health Management Using the Propeller Health Asthma Platform: A Randomized Clinical Trial. The Journal of Allergy and Clinical Immunology: In Practice 2016, 4, 455–463. [Google Scholar] [CrossRef]
- Fleming, L.; Murray, C.; Bansal, A.T.; Hashimoto, S.; Bisgaard, H.; Bush, A.; Frey, U.; Hedlin, G.; Singer, F.; van Aalderen, W.M.; et al. The Burden of Severe Asthma in Childhood and Adolescence: Results from the Paediatric U-BIOPRED Cohorts. Eur Respir J 2015, 46, 1322–1333. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef]
- Yoo, J.H.; Kim, J.H. Advances in Continuous Glucose Monitoring and Integrated Devices for Management of Diabetes with Insulin-Based Therapy: Improvement in Glycemic Control. Diabetes Metab J 2023, 47, 27–41. [Google Scholar] [CrossRef]
- Borrelli, N.; Grimaldi, N.; Papaccioli, G.; Fusco, F.; Palma, M.; Sarubbi, B. Telemedicine in Adult Congenital Heart Disease: Usefulness of Digital Health Technology in the Assistance of Critical Patients. Int J Environ Res Public Health 2023, 20, 5775. [Google Scholar] [CrossRef]
- Faragli, A.; Abawi, D.; Quinn, C.; Cvetkovic, M.; Schlabs, T.; Tahirovic, E.; Düngen, H.-D.; Pieske, B.; Kelle, S.; Edelmann, F.; et al. The Role of Non-Invasive Devices for the Telemonitoring of Heart Failure Patients. Heart Fail Rev 2021, 26, 1063–1080. [Google Scholar] [CrossRef] [PubMed]
- Shan, R.; Sarkar, S.; Martin, S.S. Digital Health Technology and Mobile Devices for the Management of Diabetes Mellitus: State of the Art. Diabetologia 2019, 62, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, I.; Greene, G.; MacHale, E.; Seheult, J.; Mokoka, M.; D’Arcy, S.; Taylor, T.; Murphy, D.M.; Hunt, E.; Lane, S.J.; et al. A Randomised Clinical Trial of Feedback on Inhaler Adherence and Technique in Patients with Severe Uncontrolled Asthma. Eur Respir J 2018, 51, 1701126. [Google Scholar] [CrossRef] [PubMed]
- D’Amato, G.; Holgate, S.T.; Pawankar, R.; Ledford, D.K.; Cecchi, L.; Al-Ahmad, M.; Al-Enezi, F.; Al-Muhsen, S.; Ansotegui, I.; Baena-Cagnani, C.E.; et al. Meteorological Conditions, Climate Change, New Emerging Factors, and Asthma and Related Allergic Disorders. A Statement of the World Allergy Organization. World Allergy Organ J 2015, 8, 25. [Google Scholar] [CrossRef]
- Tiesler, C.M.T.; Thiering, E.; Tischer, C.; Lehmann, I.; Schaaf, B.; von Berg, A.; Heinrich, J. Exposure to Visible Mould or Dampness at Home and Sleep Problems in Children: Results from the LISAplus Study. Environ Res 2015, 137, 357–363. [Google Scholar] [CrossRef]
- Tiotiu, A.; Ioan, I.; Wirth, N.; Romero-Fernandez, R.; González-Barcala, F.-J. The Impact of Tobacco Smoking on Adult Asthma Outcomes. Int J Environ Res Public Health 2021, 18, 992. [Google Scholar] [CrossRef]
- Bush, A.; Fleming, L. Diagnosis and Management of Asthma in Children. BMJ 2015, 350, h996. [Google Scholar] [CrossRef]
- AG, M. PF 100 - Asthma Monitor. Available online: https://www.microlife.com/consumer-products/respiratory-care/digital-peak-flow-meter/pf-100 (accessed on 27 May 2023).
- WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide. Available online: https://www.who.int/publications-detail-redirect/9789240034228 (accessed on 5 July 2023).
- Hankinson, J.L.; Odencrantz, J.R.; Fedan, K.B. Spirometric Reference Values from a Sample of the General U.S. Population. Am J Respir Crit Care Med 1999, 159, 179–187. [Google Scholar] [CrossRef]
- A, H.M. Correlation-Based Feature Subset Selection for Machine Learning. Thesis submitted in partial fulfillment of the requirements of the degree of Doctor of Philosophy at the University of Waikato 1998. [Google Scholar]
- Shevade, S.K.; Keerthi, S.S.; Bhattacharyya, C.; Murthy, K.R.K. Improvements to the SMO Algorithm for SVM Regression. IEEE Transactions on Neural Networks 2000, 11, 1188–1193. [Google Scholar] [CrossRef]
- Lewis, S.A.; Weiss, S.T.; Britton, J.R. Airway Responsiveness and Peak Flow Variability in the Diagnosis of Asthma for Epidemiological Studies. Eur Respir J 2001, 18, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Van den Bosch, O.F.C., Alvarez-Jimenez, R., de Grooth, HJ. et al. Breathing variability—implications for anaes-thesiology and intensive care. Crit Care 2021, 25, 280. [CrossRef] [PubMed]
Figure 1.
The customized Air-Quality Sensor (AQ-S). The sensor, encased in a 3D-printed cover, has been engineered for portability and scalability. The fan in the air-quality sensor is used to draw in ambient air for sampling, ensuring a continuous and representative analysis of the surrounding air-quality. Height: 2.5cm, W/L: 5cm.
Figure 1.
The customized Air-Quality Sensor (AQ-S). The sensor, encased in a 3D-printed cover, has been engineered for portability and scalability. The fan in the air-quality sensor is used to draw in ambient air for sampling, ensuring a continuous and representative analysis of the surrounding air-quality. Height: 2.5cm, W/L: 5cm.
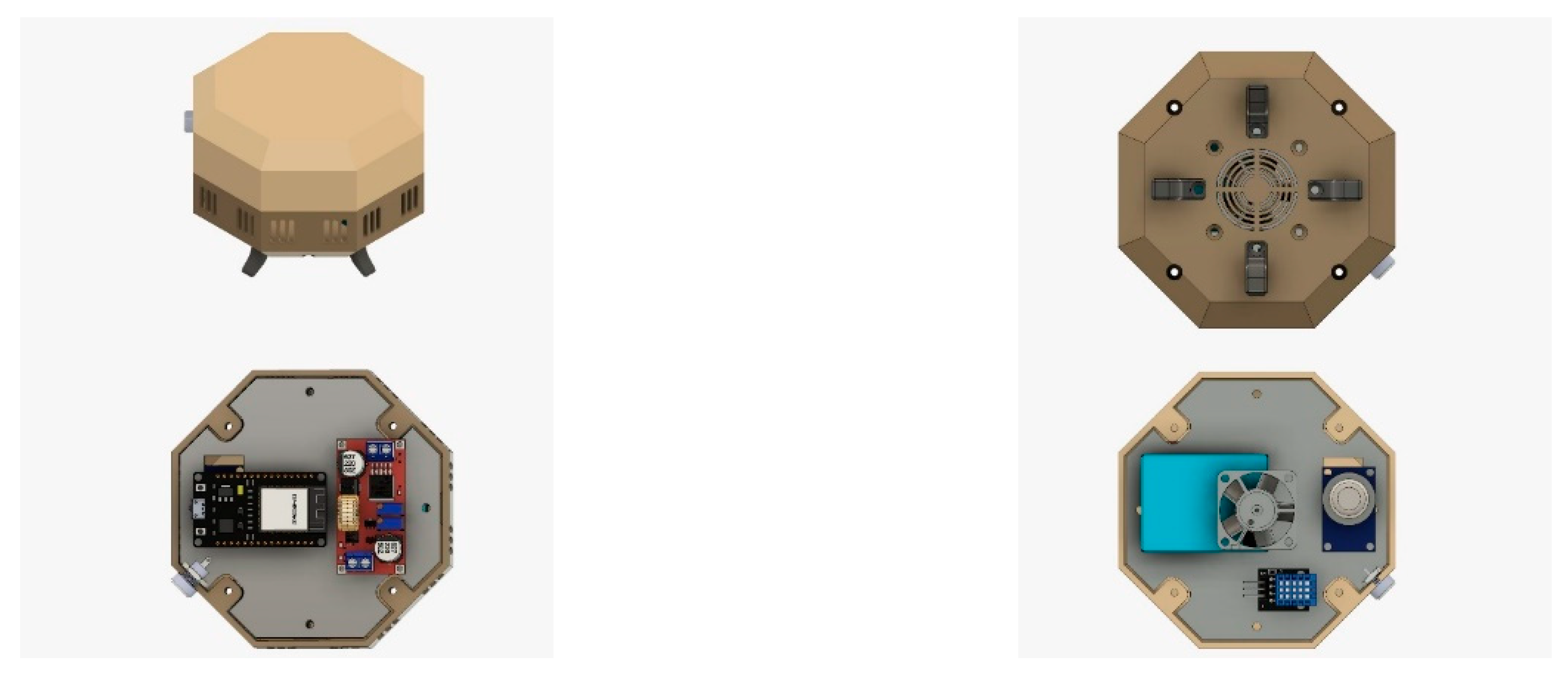
Figure 2.
Node Architecture. Details about the used array of sensors are in Table 1. The ESP32 microcontroller is employed to facilitate the processing and communication between the sensors and the user application.
Figure 2.
Node Architecture. Details about the used array of sensors are in Table 1. The ESP32 microcontroller is employed to facilitate the processing and communication between the sensors and the user application.
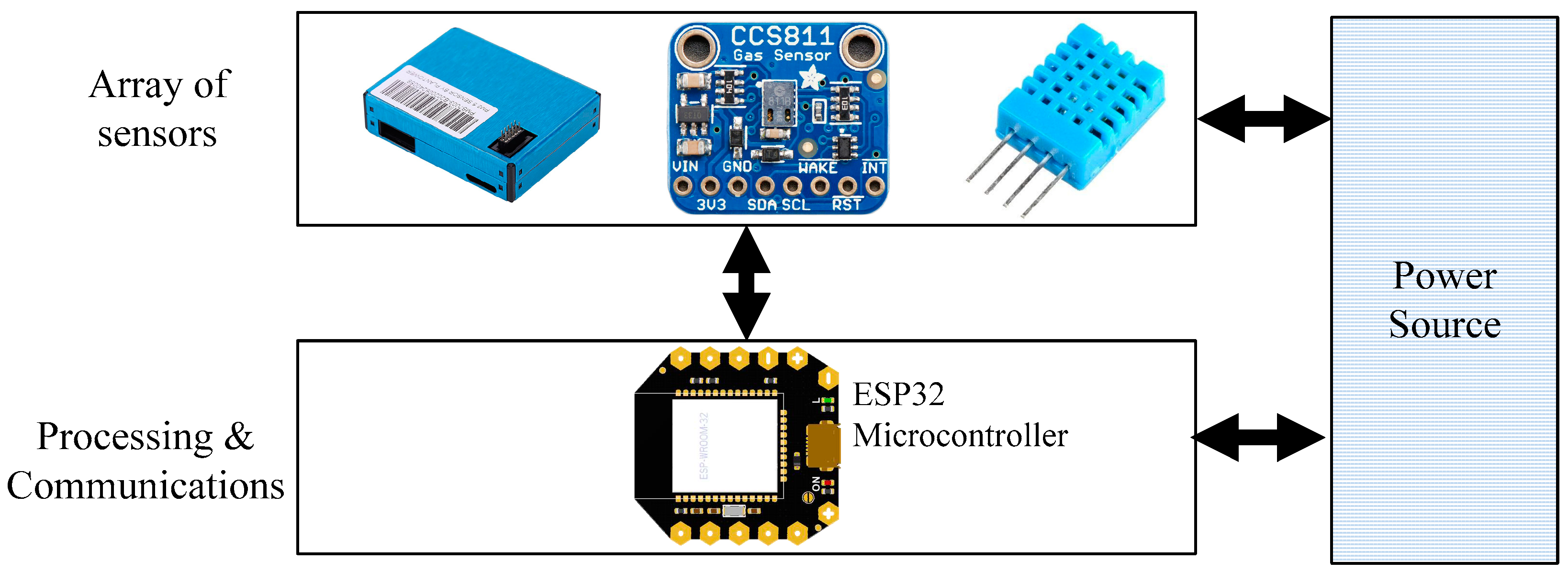
Figure 3.
Commercialized available: InkbirdPlus Air-quality Monitor.

Figure 4.
System flowchart. The variable "X" is a time-dependent measure, established through the evaluation of PEF responses to environmental alterations. As per the findings of this pilot study, the value of "X" is initially set at 0.4. However, it is anticipated that this value will be progressively adjusted to accurately reflect the lung capacity of each individual.
Figure 4.
System flowchart. The variable "X" is a time-dependent measure, established through the evaluation of PEF responses to environmental alterations. As per the findings of this pilot study, the value of "X" is initially set at 0.4. However, it is anticipated that this value will be progressively adjusted to accurately reflect the lung capacity of each individual.
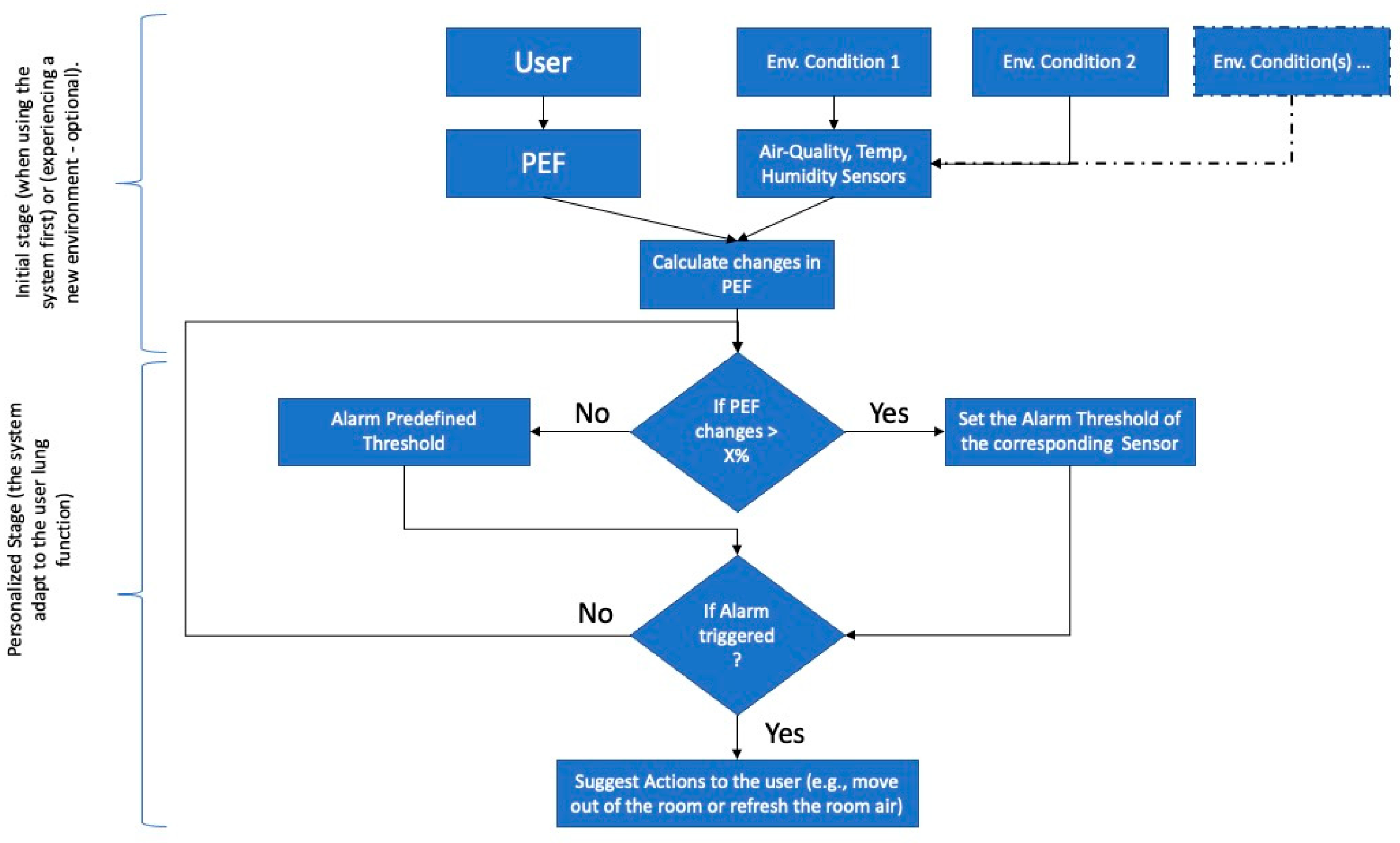

Table 1.
List of measured values along with the sensor module. The Good/Normal room air-quality is determined based on the World Health Organization (WHO) global air-quality guidelines [31].
Table 1.
List of measured values along with the sensor module. The Good/Normal room air-quality is determined based on the World Health Organization (WHO) global air-quality guidelines [31].
| Measured value | Sensor Model | Range of the customized Device | Range of InkbirdPlus (Commercial Device) |
Effect on human |
|---|---|---|---|---|
| Temperature | DHT11 | 0 – 50˚C | 0-99˚C | |
| Humidity | DHT11 | 20 – 80% | 20-99% | |
| CO2 | CCS811 module | 0 – 5,000 ppm | 350-2,000ppm | <500 (Normal); 500-1000 (Little uncomfortable); 1000-2500 (Tired); 2500-5000 (unhealthy) |
| TVOC | CCS811 module | 0 – 6,000 (PPM) | 0 – 2,000 (PPM) | <50 (Normal); 50-750 (Anxious, uncomfortable); 750-6000 (depressive, headache); >6000 (headache and other nerve problems) |
| Air-quality Sensor | PM2.5 module | 0 – 1,000 ug/m3 | 0-1,000 ug/m3) | < 12 μg/m³ (Good), 12.1 to 40.4 μg/m³ Slightly to Moderately Polluted, >40.0 μg/m³ (Seriously Polluted) |
Table 2.
Participant Demographics.
| No. | Gender | Age | Hight | Weight |
|---|---|---|---|---|
| 1 | M | 23 | 168 | 78 |
| 2 | M | 22 | 170 | 76 |
| 3 | F | 23 | 162 | 58 |
| 4 | M | 24 | 171 | 77 |
| 5 | F | 24 | 157 | 59 |
| 6 | M | 23 | 169 | 75 |
| 7 | F | 25 | 160 | 58 |
| 8 | M | 23 | 174 | 79 |
| 9 | F | 23 | 161 | 63 |
| 10 | F | 24 | 159 | 59 |
| 11 | F | 22 | 156 | 61 |
| 12 | F | 23 | 163 | 60 |
Table 3.
PEF and Air-quality Measurements in Indoor “Normal” daily Environment. The table shows two Air-quality values, the left/right is from the commercialized/customized device.
Table 3.
PEF and Air-quality Measurements in Indoor “Normal” daily Environment. The table shows two Air-quality values, the left/right is from the commercialized/customized device.
| No | PEF(L/min) | PM10 (µg/m3) | PM2.5 (µg/m3) | TVOC (µg/m3) | CO2 (ppm) | Temperature (°C) | Humidity (%) |
|---|---|---|---|---|---|---|---|
| 1 | 520 | 15/13 | 8/8 | 270/290 | 600/580 | 21/21 | 45/44 |
| 2 | 580 | 20/18 | 10/11 | 300/280 | 650/630 | 22/22 | 50/50 |
| 3 | 450 | 18/15 | 9/10 | 280/285 | 700/670 | 23/23 | 55/55 |
| 4 | 560 | 22/20 | 9/8 | 320/300 | 750/720 | 24/24 | 60/60 |
| 5 | 455 | 17/17 | 9/9 | 260/300 | 800/760 | 20/20 | 42/42 |
| 6 | 550 | 20/21 | 10/10 | 280/268 | 750/730 | 23/23 | 44/44 |
| 7 | 420 | 22/22 | 9/10 | 260/260 | 730/780 | 24/24 | 50/50 |
| 8 | 550 | 20/20 | 9/8 | 300/290 | 690/700 | 23/23 | 50/49 |
| 9 | 445 | 18/16 | 9/11 | 280/300 | 660/700 | 24/24 | 52/52 |
| 10 | 450 | 19/20 | 8/9 | 260/290 | 650/680 | 20/20 | 44/44 |
| 11 | 435 | 18/20 | 8/9 | 280/290 | 660/670 | 23/23 | 48/48 |
| 12 | 445 | 19/19 | 9/10 | 300/290 | 680/680 | 23/23 | 45/45 |
Table 4.
Statistical Evaluation of R-squared Values for Variables Relative to PEF. “*” significant correlation (>=0.3) with PEF value.
Table 4.
Statistical Evaluation of R-squared Values for Variables Relative to PEF. “*” significant correlation (>=0.3) with PEF value.
| PEF | PM10 | PM2.5 | TVOC | CO2 | Temp. | Humidity | |
|---|---|---|---|---|---|---|---|
| R-squared values | 1.00 | 0.15 | 0.52* | 0.38 | 0.05 | 0.01 | 0.03 |
Table 5.
Air-quality Measurements in the different Indoor Environments. AQ: Air-Quality, Temp: Temperature, HM: Humidity, S: Slightly.
Table 5.
Air-quality Measurements in the different Indoor Environments. AQ: Air-Quality, Temp: Temperature, HM: Humidity, S: Slightly.
| PM2.5 (µg/m3) | Temperature (°C) | Humidity (%) | ||
|---|---|---|---|---|
| Env.1: Good AQ | Avg. | 9.09 | 22.45 | 49.09 |
| SD | 1.04 | 1.51 | 5.34 | |
| Env.2: Medium AQ | Avg. | 15.26 | 22.80 | 49.00 |
| SD | 0.5 | 0.79 | 1.98 | |
| Env.3: S_Hot-Temp | Avg. | 10 | 32.00 | 54 |
| SD | 1.67 | 1.42 | 1.08 | |
| Env.4: S_High-HM | Avg. | 8.5 | 36 | 67 |
| SD | 1.3 | 1.82 | 1.34 |
Table 6.
PEF Values in Different Environmental Conditions. AQ: Air-Quality, Temp: Temperature, HM: Humidity. The column titled "Difference %" illustrates the percentage change in PEF values between conditions with good Air-quality and other environmental conditions. (A * symbol denotes a difference exceeding 4%, arbitrarily set). Underlined values represent instances where the user reported discomfort "recorded from the survey.
Table 6.
PEF Values in Different Environmental Conditions. AQ: Air-Quality, Temp: Temperature, HM: Humidity. The column titled "Difference %" illustrates the percentage change in PEF values between conditions with good Air-quality and other environmental conditions. (A * symbol denotes a difference exceeding 4%, arbitrarily set). Underlined values represent instances where the user reported discomfort "recorded from the survey.
| Good AQ | Medium AQ | Hot-Temp | High-HM | Medium AQ | Hot-Temp | High-HM | |
|---|---|---|---|---|---|---|---|
| No. | PEF(L/min) | PEF(L/min) | PEF(L/min) | PEF(L/min) | PEF(L/min) Diff % | PEF(L/min) Diff % | PEF(L/min) Diff % |
| 1 | 520 | 512 | 515 | 516 | -1.5% | -1.0% | -0.8% |
| 2 | 580 | 567 | 569 | 578 | -2.3% | -1.9% | -0.3% |
| 3 | 450 | 428* | 446 | 448 | -4.9%* | -0.9% | -0.5% |
| 4 | 560 | 549 | 555 | 558 | -2.0% | -0.9% | -0.3% |
| 5 | 455 | 461 | 450 | 455 | -1.3% | -1.2% | -0.1% |
| 6 | 550 | 539 | 545 | 546 | -2.0% | -0.9% | -0.8% |
| 7 | 420 | 411 | 416 | 418 | -2.2% | -1.0% | -0.5% |
| 8 | 550 | 538 | 548 | 547 | -2.2% | -0.3% | -0.5% |
| 9 | 445 | 435 | 444 | 444 | -2.2% | -0.2% | -0.3% |
| 10 | 450 | 430* | 449 | 446 | -4.5%* | -0.3% | -0.8% |
| 11 | 435 | 426 | 432 | 432 | -2.0% | -0.6% | -0.6% |
| 12 | 445 | 436 | 441 | 441 | -2.0% | -0.9% | -0.8% |
Table 7.
Performance of Selected Attributes and Regression Models for Predicting PEF in Different Environmental Conditions.
Table 7.
Performance of Selected Attributes and Regression Models for Predicting PEF in Different Environmental Conditions.
| Input Attributes | Target Attribute | Attribute Evaluator | CfsSubsetEva | Selected attributes (ordered) | LR* | MLP* | SMOreg | |||
|---|---|---|---|---|---|---|---|---|---|---|
| CC | RMSE | CC | RMSE | CC | RMSE | |||||
| 12 | PEF(L/min) | Search Method | BestFirst | PM2.5, Gender, Weight | 0.42 | 47.53 | 0.73 | 49.92 | 0.79 | 33.09 |
| 16 | PEF_M_AQ | Search Method | BestFirst | PEF(L/min), PM2.5_1, Condition, CO2 | 0.44 | 45.75 | 0.85 | 29.70 | 0.90 | 23.10 |
| 12 | PEF_M_AQ | Search Method | BestFirst | PEF(L/min), PM2.5_1, Condition, CO2 | 0.98 | 9.83 | 0.88 | 27.76 | 0.96 | 13.49 |
| *MLP = Multilayer Perceptron, *LR= Linear Regression | ||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



