
Submitted:
31 July 2023
Posted:
02 August 2023
You are already at the latest version
Abstract
High-flow Nasal Cannula (HFNC) oxygen therapy is gaining traction globally as a treatment for respiratory failure. There are several physiological benefits and there may be a growing patient preference for HFNC. In this narrative review, we aim to outline the basic mechanisms of HFNC, who can use it and review the literature regarding its utility both in the critical care setting, as well as in the home setting for chronic hypercapnic respiratory failure with an emphasis on Chronic Obstructive Pulmonary Disease (COPD). The role of non-pharmacological interventions like non-invasive ventilation (NIV) and HFNC in the prevention of hospital readmissions following acute exacerbations of COPD (AECOPD) is an area of increasing importance because randomised controlled trials and systematic reviews have found measures like nurse-led predischarge bundles to be clinically ineffective and to have a high cost per quality adjusted life year. This review therefore considers the evidence of NIV vs HFNC in the context of AECOPD and the application of HFNC at home in the prevention of AECOPD. We also look at applications of HFNC in specific settings, such as in the peri-operative period, emergency department, acute (mainly Critical Care) setting including in immunocompromised patients and palliative care.
Keywords:
HFNC
; COPD
; NIV
; respiratory failure
; respiratory support
; critical care
; LTOT
Introduction
High flow nasal cannulae (HFNC) oxygen therapy is being used globally in a wide variety of settings as a treatment for both acute and chronic respiratory failure. In the acute setting, it can be used an intermediate step in between oxygen (O2) delivery via simple facemask and non-invasive ventilation (NIV). HFNC can comfortably deliver high flows of O2 with rates of 20-70L/minute with fraction of inspired O2 (FiO2) ranging from 0.2-1.0[1]. There are differential physiological benefits at different rates of HFNC delivery. In the intermediate range of around 20-45L/min, there is improvement in work of breathing, respiratory rate and dead space washout, while at the higher range of around 60-70L/min increases airway pressure, end-expiratory lung volume and oxygenation[2]. There are several physiological benefits of HFNC: improved mucociliary clearance, dead space washout and improved pulmonary mechanics[3]. These lead to improved clinical parameters: reduced respiratory rate and work of breathing. This then improves patient comfort (Figure 1).
Set-Up and Delivery
While HFNC is still predominantly used in the critical care setting, it is easy to set up on medium to high dependency wards and even at home. There are four essential components of the HFNC circuit: flow generator (air/oxygen blender, turbine, or Venturi mask), active heated humidifier unit, heated tubing, and chamber kit and lastly the nasal cannula interface. There are a range of sizes of the nasal cannulae to account for anatomical differences in facial structure. In the hospital setting the device would have to be set up with an oxygen source and a high-pressure air source. Devices have been adapted to use a turbine instead in a domiciliary setting. The flow rate, FiO2 and temperature can all be set and adjusted to optimise patient comfort. The ranges and upper limits of all these factors are device dependent. Flow rates can typically be up-titrated to 60-70L/min. This should match the patient’s inspiratory flow rate[3,4]. This avoids inhalation of excess ambient air, hence maintaining a stable FiO2 to the alveoli without dilution[3,4]. However, dilution may be unavoidable for patients in acute respiratory distress with higher flow rates up to and over 100L/min, where maximal flow rate achievable on the device should be selected[3]. FiO2 can be adjusted between 60-100% through the oxygen inlet port. The in-built oxygen sensors can analyse the FiO2 of the inspired gas therefore minimise discrepancies between the setting and the FiO2 delivered to the patient[3]. Most manufacturers recommend setting the temperature to around 37oC to achieve a relative humidity of 100%[5], thereby maximising patient comfort. Devices will typically be able to set temperatures between 31-39oC, with setting below the patient’s core body temperature depending on patient preference[3]. Currently, Airvo2 humidification equipment and Optiflow interface system (Fisher and Paykel, Maidenhead, UK) are two of the most frequently used HFNC devices in the UK. Nishimura et al provide further head-to-head device descriptions in the 2019 review[6].
Physiological Effects of HFNC
There are many physiological benefits of HFNC. Firstly, HFNC improves dead space washout. The anatomical dead space is segments of the respiratory tract where air is conducted to alveoli but there is no exchange of O2 and CO2 across the alveolar membrane. In COPD, increase in dead space leads to impaired ventilation. Delivery of high flow gas has shown to improve ventilation and exercise tolerance[7]. HFNC is delivered via nasal cannulae, creating an oxygen reservoir by allowing continuous flushing of exhaled gases in the upper airways[8]. Therefore, as the flow is increased, the dead space washout improves, thereby improving gas exchange and decreasing the PaCO2[3,9]. In normal ventilation, around 30% of the tidal volume is wasted due to dead space. Thus the dead space washout effect is particularly beneficial, especially as compared to NIV, which increases anatomical dead space with use of the tight fitting face mask[9].
Secondly, HFNC improves work of breathing and pulmonary mechanics. Work of breathing is defined as the energy expended to produce a constant tidal volume (TV) over a unit time. This is dependent on lung compliance and airway resistance. Clinically, increased work of breathing translates to signs such as nasal flaring and use of abdominal muscles. In respiratory distress, HFNC reduces the respiratory rate[10]. HFNC also improves thoracoabdominal synchrony as compared to conventional oxygen therapy in patients with mild to moderate respiratory distress[11]. Therefore, in theory, HFNC reduces work of breathing. Clinically, HFNC has been shown to decrease work of breathing head-to-head against conventional oxygen therapy[12]. The electrical activity of the diaphragm significantly decreased during post-extubation phase in acute exacerbation of COPD with HFNC vs conventional oxygen therapy[13]. Another study assessed diaphragm activation using ultrasound in patients recovering from acute hypercapnic respiratory failure treated with NIV. The study showed that after NIV interruption, diaphragm activation increased with conventional oxygen therapy but not with HFNC[14]. This positive effect on work of breathing may render HFNC sufficient in hypercapnic patients to avoid escalation to NIV[9]. Although HFNC reduces minute ventilation by reducing the respiratory rate, it improves tidal volume as compared to LTOT in healthy volunteers, stable COPD and in patients in critical care[15]. Therefore, due to dead space washout, alveolar recruitment and improvement in tidal volume, HFNC improves the overall efficiency of ventilation[9].
Thirdly, HFNC improves mucociliary clearance. The respiratory epithelium is very sensitive to changes in airway temperature and pressure. It functions best at core body temperature and 100% relative humidity[3]. A fall in temperature can affect the consistency of respiratory secretions, reduces cilia beating thereby reducing the speed of mucociliary clearance[3,5]. Administration of conventional oxygen therapy, a cool dry gas, alters the physical and biochemical properties of respiratory mucus can precipitate bronchoconstriction. This is worse in patients with established airway disease such as COPD. Reduced mucociliary clearance increases chances of mucus plugging, worsening infections and eventual lung function decline[3,16]. Effective tracheobronchial secretion clearance occurs when the inhaled air is fully saturated and conditioned to 37°C in patients with obstructive airways disease[17]. Therefore, the heated humidification built into HFNC circuits improves improved patient comfort and concordance through better mucociliary clearance and maintaining comfortable levels of moisture in the airways.
Clinical Applications
There are many established clinical applications of HFNC, as well as possible applications in the future based on physiological effects (Table 1).
It is commonly used in the treatment of hypoxaemic respiratory failure; which is caused by a ventilation/perfusion mismatch, hypoventilation, limitation of diffusion, right-to-left shunt and reduced inspired oxygen tension[3]. Conventional oxygen therapy can be administered via nasal cannulae, with flow rates up to 5-6L/min, via simple facemask up to about 10L/min and via non-rebreathe mask with rates of 15-20L/min. While oxygen is the treatment, conventional oxygen therapy is often not sufficient to keep up with the demands of patients in hypoxaemic respiratory failure, who have flow rates up to about 60L/min[3]. Prolonged treatment with conventional oxygen therapy without humidification can also lead to adverse effects such as dry mouth, increased upper airway secretions and epistaxis[3,18].
As previously mentioned, HFNC is effective in managing acute exacerbations of COPD by improving washout of dead space, therefore ameliorating gas exchange and leading to a reduction in PaCO2.
Although not widely used clinically, HFNC may be effective in the management of cardiogenic pulmonary oedema. Guidelines advocate the use of positive airway pressure to improve oxygenation and decrease cardiac afterload. Studies have shown that HFNC can achieve the same physiological effects with less discomfort for the patient[19, 20]. More randomised controlled trials (RCTs) looking specifically at patients with cardiogenic pulmonary oedema as the cause for hypoxaemic respiratory failure are needed in order to adopt HFNC as part of its management guideline.
HFNC is also a useful support device to allow patients to eat, drink and talk while taking breaks from positive airway pressure, which is commonly used to treat many causes of respiratory failure in a variety of hospital settings[3].
HFNC may go on to play a bigger role in both the short- and long-term management of suppurative diseases such as cystic fibrosis and bronchiectasis by increasing the mucociliary clearance[9]. More studies are required to compare the head-to-head effectiveness of HFNC against established treatments.
HFNC in the peri-operative setting
HFNC has several roles in different aspects of the perioperative period. HFNC is a promising tool in preoxygenation in patients, especially in those with difficult anticipated intubation or during awake fibre-optic intubation[2,21]. Moreover, patients with hypoxaemic respiratory failure due to COPD or other underlying illnesses (idiopathic pulmonary fibrosis, severe obesity, neuromuscular disorders or pregnancy) are more prone to severe oxygen desaturation. This is because the oxygen stores are depleted by increased oxygen consumption[21]. NIV can be used for pre-oxygenation as it reduces alveolar collapse and the likelihood of atelectasis, which lead to hypoventilation, thereby increasing the ventilation/perfusion mismatch[21]. However, NIV cannot be used during laryngoscopy, therefore cannot prevent desaturation during tracheal intubation[21]. HFNC has an advantage over NIV in laryngoscopy as it is delivered purely via nasal cannulae[21]. HFNC increases apnoea time with adequate oxygenation without hypercapnia[21, 22,23]. Evidence shows that in patients with moderate to severe hypoxaemia (PaO2/FiO2 ≤ 200mmHg), desaturation to <80% occurred significantly less frequently after preoxygenation with NIV as compared with HFNC (24% vs. 35%, p=0.046)[2,24]. Another study showed that the combination of both NIV and HFNC significantly reduced significant desaturation during intubation as compared to NIV alone[25]. Based on this, Ricard et al suggest that preoxygenation with HFNC may be considered in patients with a PaO2:FiO2 ratio (P/F ratio) between 200-300mmHg, while at lower P/F ratios, NIV may be superior[2].
The role of HFNC post-surgery is more complicated and requires further evaluation. Generally, surgical patients are classed as low risk of needing reintubation due to generally shorter periods of mechanical ventilation[2]. There are other factors that may render surgical patients as higher risk, such as anaesthetic factors and surgical complications[2]. There is evidence to suggest that HFNC post-extubation in low-risk patients, including complex surgical patients with >12hrs mechanical ventilation, reduces reintubation rate as compared to conventional oxygen therapy[2,21,26]. HFNC was also shown to be non-inferior to NIV[26]. However, the data was very heterogenous[2,21]. Other studies have not found such differences in uncomplicated post-abdominal surgery patients[2,27]. Zhu et al conducted a meta-analysis, which confirmed that HFNC was superior to conventional oxygen therapy in management of post-extubation respiratory failure and avoiding reintubation following planned extubation[28].
HFNC is also useful in specific respiratory procedures such as elective and emergency bronchoscopy, especially in patients with pre-existing chronic respiratory disease. HFNC has been shown to improve oxygen throughout the procedure as compared with conventional oxygen therapy[3,29]. The use of HFNC in acute hypoxaemic respiratory failure should be closely monitored to avoid delay to intubation when it is required[2]. The ROX index can be used to serially assess the need to either escalate oxygen therapy or to intubate promptly in patients with hypoxaemic respiratory failure[2].
Use of HFNC in COVID-19
HFNC was widely used in acute hypoxaemic respiratory failure due to coronavirus disease 2019, although the data is limited. The RECOVERY-RS trial found no significant difference between an initial strategy of HFNC compared with conventional oxygen therapy[30]. However, a retrospective study in patients not mechanically ventilated within 6 hours of admission in the five hospitals of the Johns Hopkins Health System, USA, found that HFNC was associated with a significantly reduced hazard of death[31].
HFNC in the Emergency Department
Respiratory failure is a very common presentation to the emergency department, where it may be postulated that HFNC could have an important role in its treatment. However, Tinelli et al’s 2019 systematic review looked at four RCTs comparing HFNO to conventional oxygen therapy exclusively in ED, where HFNC did not improve intubation requirement, treatment failure, hospitalisation or mortality[32]. In one RCT looking at HFNC vs NIV, there was no difference in intubation requirement, treatment failure, tolerance or dyspnoea[32]. This could be due to the underlying reason for respiratory failure and rate of deterioration, as well as type of and familiarity with equipment. The data looking at use of HFNC in the emergency department is very limited and much more work needs to be done to determine its effectiveness.
HFNC vs NIV in the acute setting
HFNC and NIV are both established forms of treatment in acute respiratory failure. There are an increasing number of head-to-head studies looking at the effectiveness of HFNC compared to NIV. Lee et al conducted a systematic review of twelve studies comparing HFNC vs NIV (and conventional oxygen therapy) in terms of oxygenation, breathing mechanics, escalation of oxygen therapy, mortality and patient comfort[33]. HFNC was inferior to NIV for oxygenation[33]. HFNC did not significantly reduce respiratory rate in two studies[33,34,35]. In Frat et al’s 2015 study, there was significantly reduced respiratory rate after 1hr of HFNC therapy but not after 6hrs HFNC therapy[33,36]. They also showed that HFNC significantly reduced intubation rate in those with baseline PaO2:FiO2 ≤200mmHg (P/F ratio) as compared to NIV (35% intubation rate in HFNC with 95%CI 25-46% vs 58% in NIV with 95%CI 47-68%, p=0.009) but not above this P/F ratio threshold[33,36]. Frat et al showed that both 90-day mortality and ICU mortality were significantly reduced in those who received HFNC as compared to those who received NIV[33,36]. Several studies showed that HFNC was significantly more comfortable than conventional oxygen therapy[33]. In a few studies looking at comfort head-to-head HFNC vs NIV, dyspnoea significantly improved with HFNC[33,36], although some studies did not find the difference to be statistically significant[33].
Sun et al performed an observational cohort study of 82 COPD patients with acute hypercapnic respiratory failure in 2019, comparing HFNC and NIV as the initial treatment on intensive care[37]. This showed no significant difference in treatment failure, intubation rates, length of ICU stay or 28-day mortality between the two groups[37]. However, there were significantly fewer nursing airway care interventions, increased device application time and significantly fewer episodes of skin breakdown in the HFNC group as compared to the NIV group[37].
Feng et al more recently conducted a systematic review including eight studies, looking specifically at HFNC vs NIV in AECOPD patients post-extubation[38]. Their primary outcome was reintubation rate. They found that in those with hypercapnia, there was no statistically significant benefit of HFNC over NIV[38]. However, in those without hypercapnic respiratory failure, there was a statistically higher reintubation rate in the HFNC group as compared to NIV[38]. Feng et al looked at mortality, ICU length of stay, complication rates and a handful of other assorted outcomes as secondary outcomes[38]. There was no significant difference in mortality or length of stay in ICU in the HFNC group as compared to NIV, regardless of hypercapnia[38]. However, HFNC significantly reduced complication rates (nasal facial skin breakdown, aspiration and flatulence during treatment) in AECOPD patients post-extubation in all patients[38]. There was no significant difference in heart rate, PaCO2 post extubation, pH or P/F ratio in any of the patients regardless of hypercapnia[38]. However, there was significantly reduced RR in patients with hypercapnia but not in the non-hypercapnic group[38].
Overall, the literature suggests that HFNC is non-inferior to NIV in management of acute hypercapnic failure with regards to intubation rates, escalation of oxygen therapy, length of stay in ICU and mortality. However, HFNC appears to be superior in terms of patient comfort and reduces complications of therapy. Further RCTs with large sample sizes are required to explore the direct comparison of HFNC vs NIV, especially with the advancement of both the nasal cannulae and high flow oxygen delivery systems.
HFNC in immunocompromised patients
There is unclear evidence regarding whether HFNC is beneficial in the management of acute hypoxaemic respiratory failure in immunocompromised patients. This is due to the heterogeneity of the patient population and cause of immunosuppression. This may be iatrogenic, for example due to steroids or chemotherapy medications. It could also be due to the underlying disease, for example a haematological malignancy or a primary immunodeficiency[3]. Ricard et al reviewed several studies and concluded that evidence suggested that HFNC may reduce intubation rate as compared to HFNC in immunocompromised patients[2]. Azoulay et al showed that there were no significant differences in 28- or 90-day mortality, ICU stay, intubation rates or breathlessness between those treated with HFNC versus those treated with conventional oxygen therapy via facemask[3,39]. The multivariate analysis did confirm that there was a trend towards lower intubation rates in the HFNC group[2,39]. The results could partly be due to overall lower survival rates in immunocompromised patients as compared to immunocompetent patients[3,40]. Causes of lower survival rates could be due to the propensity of immunocompromised patients to develop multi-system complications of their underlying disease or pharmacological therapies. Utilisation of HFNC in immunocompromised patients should occur with the input of a multidisciplinary team in order to simultaneously optimise management of co-morbidities, correct the acute respiratory failure and to enable prompt recognition and treatment of any complications[3].
HFNC at home
Advanced COPD leads to significantly compromised exercise tolerance and progressive inability to carry out activities of daily living. They are prone to exacerbations, associated with hospitalisation and increased mortality. After smoking cessation and pulmonary rehabilitation programmes, long-term oxygen therapy (LTOT) is beneficial for longer-term survival of COPD patients with severe resting hypoxaemia. Established criteria exist for starting LTOT: PaO2<7.3kPa on room air or PaO2<8.0kPa with one of secondary polycythaemia (haematocrit >55%), right heart failure or cor pulmonale[41].
HFNC is an emerging treatment in the management of chronic hypercapnic COPD. Storgaard et al compared LTOT+HFNC with LTOT alone in 200 patients[42]. They showed that HFNC significantly reduced AECOPD rates as compared to LTOT alone (3.12 vs 4.95 exacerbations/patient/year, p<0.001) but there was no significant difference in annual hospital admission rate[42]. The HFNC group had significantly fewer exacerbations in the study year as compared to the previous year (p<0.001)[42]. Dyspnoea as calculated by the mMRC score was significantly better at 3 months and onwards in the HFNC group as compared to the LTOT group[42]. Quality of life (QoL) as calculated using the St George’s Respiratory Questionnaire (SGRQ) was better at 6 and 12 months in the HFNC group[35]. PaCO2 gradually decreased and was significantly lower in the HFNC group at 12 months[42]. 6 minute walk test (6MWT) distances were significantly better in the HFNC group at 12 months[42]. Although not statistically significant, there was a trend towards increased FEV1 in the HFNC group as compared to LTOT at 6 and 12 months[42]. There was no difference in the FVC%, FEV1/FVC, PaO2, saO2 or pH between the two groups at 6 or 12 months[42]. Interestingly, there was an increase in BMI in the HFNC group as compared to the LTOT group[42].
Nagata et al performed a multicentre crossover trial in 2018, where patients with stable hypercapnic respiratory failure with GOLD classification 2-4 (2013 guidelines)[43] already receiving LTOT for at least one month received LTOT for 6 weeks, followed by LTOT+HFNC for 6 weeks and vice versa[44]. The study recruited from nine hospitals in Japan. The total SGRQ-C (compact SGRQ) score as well as all its individual components (symptoms, activity, impact) reflecting QoL significantly improved in those receiving HFNC. Furthermore, PaCO2, pH and ptCO2 significantly improved in the HFNC group[44]. There was no significant difference in 6MWT (distance, SpO2 decline %, Borg scale for dyspnoea), pulmonary function tests (vital capacity, FVC, FEV1, FEV1/FVC, DLCO, RV, FRC, TLC) or physical activity (calorie consumption, step count, activity time)[44]. They also studied the impact of HFNC on health economics by studying quality adjusted life years (QALYs) using the five-level version of the EuroQol five-dimensional questionnaire (EQ-5D-5L) score[44,45]. They found that there was no statistically significant difference in QALYs between HFNC+LTOT compared with LTOT alone[44], although when using the visual analogue scale version of the same scoring system, there was a statistical difference[44]. They found that the net difference equated to a benefit of 15,780 Japanese Yen (US$158.70) per patient per year[44].
Bonnevie et al conducted a systematic review and meta-analysis, which concluded that HFNC improved PaCO2, acute exacerbation and QoL in patients with stable hypercapnic COPD both short-term and long-term[46]. Although the improvement in PaCO2 reached statistical significance, it remains unclear whether if it was a clinically important difference.
Nagata et al carried out conducted an RCT with ninety-three patients in 2022[47]. They showed that HFNC+LTOT significantly reduced number of moderate/severe exacerbations as compared to LTOT alone[47]. However, there was no statistically significant difference between HFNC+LTOT vs LTOT alone when looking at severe-only exacerbations[47]. HFNC also prolonged time to first moderate or severe exacerbation of COPD as compared to LTOT[47]. They further analysed QoL using the SGRQ-C (compact version of SGRQ) looking at total score, symptoms score, activity score and impact score. Only the total score at 24 weeks and the impact score at 12 weeks were significantly improved in the HFNC group, although the trend showed generally improved QoL across the board at 52 weeks[47]. They did not find any statistically significant differences between the two groups in terms of dyspnoea as per the mMRC score, pH, PaO2, PaCO2, FVC, FEV1 DLCO, 6MWT distance or all-cause mortality at 52 weeks. Resting SpO2 was significantly higher only at 52 weeks in the HFNC group[47].
Horvath et al suggests that a subset of patients with chronic hypercapnic COPD who failed to benefit from NIV may have long-term reductions in PaCO2 with HFNC, although the clinical significance remains unclear due to data limitations[48].
McKinstry et al focused on measuring transcutaneous carbon dioxide (ptCO2 ) in stable hypercapnic COPD patients using NIV vs HFNC. They found that NIV was significantly better at reducing ptCO2 at 60 minutes than HFNC (mean -5.3 SD 5mmHg vs mean -2.5 SD 3.5mmHg respectively, p=0.021)[49]. However, there was no statistically significant difference between NIV and HFNC for ptCO2 reductions ≥4mmHg and ≥8mmHg[49]. HFNC was associated with significantly increased comfort, fit and ease of application[49].
Huang et al reviewed four RCTs, which looked at PaCO2 (primary outcome) and PaO2 (secondary outcome) in patients with hypercapnic COPD using HFNC vs conventional oxygen therapy, which included both domiciliary and acute settings[50]. There was no significant difference in either outcome between the groups[50]. However, the heterogeneity of the population (inclusion of both hypercapnic AECOPD and stable hypercapnic COPD patients) makes the interpretation difficult.
Overall, the limited literature suggests that home HFNC is beneficial in the management of stable hypercapnic COPD as it reduces moderate/severe exacerbations, is more comfortable and improves quality of life. Further studies are needed to look more closely at the longer-term effects of home HFNC on exercise tolerance, hospitalisations/admission free survival and mortality.
HFNC in the palliative care setting
There is limited evidence on the efficacy of HFNC in symptom control in cancer patients. Epstein et al evaluated the potential of HFNC as a management strategy for breathlessness in cancer patients’ breathlessness[51]. Most patients remained stable or improved, while a minority of the patients worsened[51,52].The role of HFNC in managing breathlessness in those with established treatment limitations remains unclear[3,53]. Further work is needed to evaluate the effectiveness of HFNC in management of acute respiratory failure with do not intubate/do not resuscitate orders as compared to NIV, conventional oxygen therapy and use of opioid medication[3,53]. HFNC could be used as an adjunct to pharmacological therapy and other therapies in the management of patients with respiratory failure where mechanical ventilation has failed or is clinically inappropriate[3,54]. Isolated cases have shown great potential of HFNC in ameliorating symptom management in patients with life-limiting illnesses[55]. There is scant evidence to suggest that HFNC was comparable with NIV with regards to improving dyspnoea, O 2 saturation and respiratory rate in patients with advanced cancer[56]. More work needs to be done comparing HFNC with conventional oxygen therapy, NIV and medications in dying patients to further understand when to commence HFNC and how to adjust it, much like any other ventilation intervention in the palliative care setting[57].
Conclusion
HFNC has many clinical advantages over other therapies such as NIV, with patients preferring it because it is lighter and more comfortable to use and they can continue to talk, eat and drink while using HFNC. There are many potential applications of HFNC in the future for a wide variety of respiratory conditions.
The vast majority of the studies of HFNC in the acute setting is in critical care. More work needs to be done to look at the feasibility and effectiveness of HFNC in medical wards, where the nursing skill mix and nurse-to-patient ratios differ greatly from critical care. HFNC has the potential to be a simpler means of respiratory support due to ease of application of the device and the need for fewer nursing airway care interventions.
Following acute hospital admissions for exacerbations of COPD, a multitude of readmission prevention strategies exist, like smoking cessation, optimisation of inhaled therapies, exercise programmes, telemonitoring with remote interventions, specialist nurse surveillance and discharge bundles. Despite this, there is an unmet need in reducing hospital readmission and mortality. There is an increasing drive to incorporate respiratory support devices to improve outcomes. A randomised controlled trial has demonstrated that home mechanical ventilation (domiciliary NIV) added to home oxygen therapy can improve admission-free survival and quality of life[58]. With domiciliary NIV, there are on-going issues with patient tolerance/compliance due to issues around synchronisation, leaks and discomfort with the mask. HFNC has the potential to be equally efficacious with greater compliance, thereby improving quality of life and reducing the number of hospital admissions[42,47].
Further studies are needed, particularly in post-acute hospital admission and stable hypercapnic COPD patients, to assess the effects on acute exacerbation rate, quality of life and admission-free survival. This may be enhanced with the utilisation of telemonitoring in improving compliance[59].
List of Abbreviations
| HFNC | High-flow Nasal Cannula oxygen therapy |
| COPD | Chronic Obstructive Pulmonary Disease |
| AECOPD | Acute Exacerbation of Chronic Obstructive Pulmonary Disease |
| NIV | Non-invasive ventilation |
| FiO2 | Fraction of inspired O2 |
| PaO2 | Partial pressure of Oxygen in Arterial Blood |
| PaCO2 | Partial pressure of Carbon Dioxide in Arterial Blood |
| ptCO2 | Transcutaneous carbon dioxide monitoring |
| TV | Tidal Volume |
| P/F | PaO2: FiO2 |
| ICU | Intensive Care Unit |
| RECOVERY-RS | Randomised Evaluation of Covid-19 Therapy – Respiratory Support |
| LTOT | Long-term oxygen therapy |
| mMRC score | Modified Medical Research Council dyspnoea score |
| HRQoL | Health Related Quality of Life |
| EQ-5D-5L | European quality of life five dimensional questionnaire five level score |
| SGRQ | St George’s Respiratory Questionnaire |
| 6MWT | 6-Minute Walk Test |
| QALY | Quality Adjusted Life Year |
References
- Delorme, M.; Bouchard, P.A.; Simon, M.; Simard, S.; Lellouche, F. Effects of High-Flow Nasal Cannula on the Work of Breathing in Patients Recovering From Acute Respiratory Failure*. Critical Care Medicine. 2017, 45, 1981–1988. [Google Scholar] [CrossRef] [PubMed]
- Ricard, J.D.; Roca, O.; Lemiale, V.; Corley, A.; Braunlich, J.; Jones, P.; et al. Use of nasal high flow oxygen during acute respiratory failure. Intensive Care Medicine. 2020, 46, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, R.F.; Hart, N.; Kaltsakas, G. High-flow therapy: physiological effects and clinical applications. Breathe. 2020, 16, 200224. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, J.E.; Williams, A.B.; Gerard, C.; Hockey, H. Evaluation of a Humidified Nasal High-Flow Oxygen System, Using Oxygraphy, Capnography and Measurement of Upper Airway Pressures. Anaesthesia and Intensive Care. 2011, 39, 1103–1110. [Google Scholar] [CrossRef]
- Williams, R.; Rankin, N.; Smith, T.; Galler, D.; Seakins, P. Relationship between the humidity and temperature of inspired gas and the function of the airway mucosa. Critical Care Medicine. 1996, 24, 1920–1929. [Google Scholar] [CrossRef]
- Nishimura, M. High-Flow Nasal Cannula Oxygen Therapy Devices. Respiratory Care. 2019, 64, 735–742. [Google Scholar] [CrossRef]
- Cirio, S.; Piran, M.; Vitacca, M.; Piaggi, G.; Ceriana, P.; Prazzoli, M.; et al. Effects of heated and humidified high flow gases during high-intensity constant-load exercise on severe COPD patients with ventilatory limitation. Respiratory Medicine. 2016, 118, 128–132. [Google Scholar] [CrossRef]
- Möller, W.; Celik, G.; Feng, S.; Bartenstein, P.; Meyer, G.; Eickelberg, O.; et al. Nasal high flow clears anatomical dead space in upper airway models. Journal of Applied Physiology. 2015, 118, 1525–1532. [Google Scholar] [CrossRef]
- Spicuzza, L.; Schisano, M. High-flow nasal cannula oxygen therapy as an emerging option for respiratory failure: the present and the future. Therapeutic Advances in Chronic Disease. 2020, 11, 204062232092010. [Google Scholar] [CrossRef]
- Sztrymf, B.; Messika, J.; Mayot, T.; Lenglet, H.; Dreyfuss, D.; Ricard, J.D. Impact of high-flow nasal cannula oxygen therapy on intensive care unit patients with acute respiratory failure: A prospective observational study. Journal of Critical Care. 2012, 27, 324–e9. [Google Scholar] [CrossRef]
- Itagaki, T.; Okuda, N.; Tsunano, Y.; Kohata, H.; Nakataki, E.; Onodera, M.; et al. Effect of high-flow nasal cannula on thoraco-abdominal synchrony in adult critically ill patients. Respiratory Care. 2014, 59, 70–74. [Google Scholar] [CrossRef]
- Pisani, L.; Astuto, M.; Prediletto, I.; Longhini, F. High flow through nasal cannula in exacerbated COPD patients: a systematic review. Pulmonology. 2019, 25, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Di mussi, R.; Spadaro, S.; Stripoli, T.; Volta, C.A.; Trerotoli, P.; Pierucci, P.; et al. High-flow nasal cannula oxygen therapy decreases postextubation neuroventilatory drive and work of breathing in patients with chronic obstructive pulmonary disease. Critical Care. 2018, 22. [Google Scholar] [CrossRef]
- Longhini, F.; Pisani, L.; Lungu, R.; Comellini, V.; Bruni, A.; Garofalo, E.; et al. High-Flow Oxygen Therapy After Noninvasive Ventilation Interruption in Patients Recovering From Hypercapnic Acute Respiratory Failure. Critical Care Medicine. 2019, 47, e506–11. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.F.; Spooner, A.J.; Dunster, K.R.; Anstey, C.M.; Corley, A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue carbon dioxide while increasing tidal and end-expiratory lung volumes: a randomised crossover trial. Thorax. 2016, 71, 759–761. [Google Scholar] [CrossRef] [PubMed]
- Vestbo, J.; Prescott, E.; Lange, P. Association of chronic mucus hypersecretion with FEV1 decline and chronic obstructive pulmonary disease morbidity. Copenhagen City Heart Study Group. American Journal of Respiratory and Critical Care Medicine. 1996, 153, 1530–1535. [Google Scholar]
- Hasani, A.; Chapman, T.; McCool, D.; Smith, R.; Dilworth, J.; Agnew, J. Domiciliary humidification improves lung mucociliary clearance in patients with bronchiectasis. Chronic Respiratory Disease. 2008, 5, 81–86. [Google Scholar] [CrossRef]
- Roca, O.; Riera, J.; Torres, F.; Masclans, J. High-flow oxygen therapy in acute respiratory failure. Respiratory Care. 2010, 55, 408–413. [Google Scholar]
- Roca, O.; Pérez-Terán, P.; Masclans, J.R.; Pérez, L.; Galve, E.; Evangelista, A.; et al. Patients with New York Heart Association class III heart failure may benefit with high flow nasal cannula supportive therapy: High flow nasal cannula in heart failure. Journal of Critical Care. 2013, 28, 741–746. [Google Scholar] [CrossRef]
- Makdee, O.; Monsomboon, A.; Surabenjawong, U.; Praphruetkit, N.; Chaisirin, W.; Chakorn, T.; et al. High-Flow Nasal Cannula Versus Conventional Oxygen Therapy in Emergency Department Patients With Cardiogenic Pulmonary Edema: A Randomized Controlled Trial. Annals of Emergency Medicine. 2017, 70, 465–472. [Google Scholar] [CrossRef]
- Cortegiani, A.; Accurso, G.; Mercadante, S.; Giarratano, A.; Gregoretti, C. High flow nasal therapy in perioperative medicine: from operating room to general ward. BMC Anesthesiology. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Badiger, S.; John, M.; Fearnley, R.A.; Ahmad, I. Optimizing oxygenation and intubation conditions during awake fibre-optic intubation using a high-flow nasal oxygen-delivery system. British Journal of Anaesthesia. 2015, 115, 629–632. [Google Scholar] [CrossRef] [PubMed]
- Renda, T.; Corrado, A.; Iskandar, G.; Pelaia, G.; Abdalla, K.; Navalesi, P. High-flow nasal oxygen therapy in intensive care and anaesthesia. British Journal of Anaesthesia. 2018, 120, 18–27. [Google Scholar] [CrossRef]
- Frat, J.P.; Ricard, J.D.; Quenot, J.P.; Pichon, N.; Demoule, A.; Forel, J.M.; et al. Non-invasive ventilation versus high-flow nasal cannula oxygen therapy with apnoeic oxygenation for preoxygenation before intubation of patients with acute hypoxaemic respiratory failure: a randomised, multicentre, open-label trial. The Lancet Respiratory Medicine. 2019, 7, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Jaber, S.; Monnin, M.; Girard, M.; Conseil, M.; Cisse, M.; Carr, J.; et al. Apnoeic oxygenation via high-flow nasal cannula oxygen combined with non-invasive ventilation preoxygenation for intubation in hypoxaemic patients in the intensive care unit: the single-centre, blinded, randomised controlled OPTINIV trial. Intensive Care Medicine. 2016, 42, 1877–1887. [Google Scholar] [CrossRef]
- Hernández, G.; Vaquero, C.; González, P.; Subira, C.; Frutos-Vivar, F.; Rialp, G.; et al. Effect of Postextubation High-Flow Nasal Cannula vs Conventional Oxygen Therapy on Reintubation in Low-Risk Patients: A Randomized Clinical Trial. JAMA. 2016, 315, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Futier, E.; Paugam-Burtz, C.; Godet, T.; Khoy-Ear, L.; Rozencwajg, S.; Delay, J.M.; et al. Effect of early postextubation high-flow nasal cannula vs conventional oxygen therapy on hypoxaemia in patients after major abdominal surgery: a French multicentre randomised controlled trial (OPERA). Intensive Care Medicine. 2016, 42, 1888–1898. [Google Scholar] [CrossRef]
- Zhu, Y.; Yin, H.; Zhang, R.; Ye, X.; Wei, J. High-flow nasal cannula oxygen therapy versus conventional oxygen therapy in patients after planned extubation: a systematic review and meta-analysis. Critical Care. 2019, 23. [Google Scholar] [CrossRef]
- Douglas, N.; Ng, I.; Nazeem, F.; Lee, K.; Mezzavia, P.; Krieser, R.; et al. A randomised controlled trial comparing high-flow nasal oxygen with standard management for conscious sedation during bronchoscopy. Anaesthesia. 2017, 73, 169–176. [Google Scholar] [CrossRef]
- Perkins, G.D.; Ji, C.; Connolly, B.A.; Couper, K.; Lall, R.; Baillie, J.K.; et al. Effect of Noninvasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19. JAMA. 2022, 327, 546. [Google Scholar] [CrossRef]
- Burnim, M.S.; Wang, K.; Checkley, W.; Nolley, E.P.; Xu, Y.; Garibaldi, B.T. The Effectiveness of High-Flow Nasal Cannula in Coronavirus Disease 2019 Pneumonia. Critical Care Medicine Publish Ahead of Print. 2021. [Google Scholar]
- Tinelli, V.; Cabrini, L.; Fominskiy, E.; Franchini, S.; Ferrante, L.; Ball, L.; et al. High Flow Nasal Cannula Oxygen vs. Conventional Oxygen Therapy and Noninvasive Ventilation in Emergency Department Patients: A Systematic Review and Meta-Analysis. The Journal of Emergency Medicine. 2019, 57, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Mankodi, D.; Shaharyar, S.; Ravindranathan, S.; Danckers, M.; Herscovici, P.; et al. High flow nasal cannula versus conventional oxygen therapy and non-invasive ventilation in adults with acute hypoxemic respiratory failure: A systematic review. Respiratory Medicine. 2016, 121, 100–108. [Google Scholar] [CrossRef]
- Schwabbauer, N.; Berg, B.; Blumenstock, G.; Haap, M.; Hetzel, J.; Riessen, R. Nasal high–flow oxygen therapy in patients with hypoxic respiratory failure: effect on functional and subjective respiratory parameters compared to conventional oxygen therapy and non-invasive ventilation (NIV). BMC Anesthesiology. 2014, 14. [Google Scholar] [CrossRef]
- Vargas, F.; Saint-Leger, M.; Boyer, A.; Bui, N.H.; Hilbert, G. Physiologic Effects of High-Flow Nasal Cannula Oxygen in Critical Care Subjects. Respiratory Care. 2015, 60, 1369–1376. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; et al. High-Flow Oxygen through Nasal Cannula in Acute Hypoxemic Respiratory Failure. New England Journal of Medicine. 2015, 372, 2185–2196. [Google Scholar] [CrossRef]
- Sun, J.; Li, Y.; Ling, B.; Zhu, Q.; Hu, Y.; Tan, D.; et al. High flow nasal cannula oxygen therapy versus non-invasive ventilation for chronic obstructive pulmonary disease with acute-moderate hypercapnic respiratory failure: an observational cohort study. International Journal of Chronic Obstructive Pulmonary Disease. 2019, 14, 1229–1237. [Google Scholar] [CrossRef]
- Feng, Z.; Zhang, L.; Yu, H.; Su, X.; Tiankui Shuai Zhu, L.; et al. High-Flow Nasal Cannula Oxygen Therapy versus Non-Invasive Ventilation for AECOPD Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. International Journal of Chronic Obstructive Pulmonary Disease. 2022, 17, 1987–1999. [Google Scholar] [CrossRef]
- Azoulay, E.; Lemiale, V.; Mokart, D.; Nseir, S.; Argaud, L.; Pène, F.; et al. Effect of High-Flow Nasal Oxygen vs Standard Oxygen on 28-Day Mortality in Immunocompromised Patients With Acute Respiratory Failure. JAMA. 2018, 320, 2099. [Google Scholar] [CrossRef]
- Frat, J.P.; Ragot, S.; Girault, C.; Perbet, S.; Prat, G.; Boulain, T.; et al. Effect of non-invasive oxygenation strategies in immunocompromised patients with severe acute respiratory failure: a post-hoc analysis of a randomised trial. The Lancet Respiratory Medicine. 2016, 4, 646–652. [Google Scholar] [CrossRef]
- Hardinge, M.; Annandale, J.; Bourne, S.; Cooper, B.; Evans, A.; Freeman, D.; et al. British Thoracic Society guidelines for home oxygen use in adults: accredited by, N. I.C.E. Thorax. 2015, 70 (Suppl 1), i1–43. [Google Scholar] [CrossRef]
- Storgaard, L.H.; Hockey, H.; Laursen, B.S.; Weinreich, U.M. Long-term effects of oxygen-enriched high-flow nasal cannula treatment in COPD patients with chronic hypoxemic respiratory failure. International Journal of Chronic Obstructive Pulmonary Disease. 2018, 13, 1195–1205. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American journal of respiratory and critical care medicine 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Nagata, K.; Kikuchi, T.; Horie, T.; Shiraki, A.; Kitajima, T.; Kadowaki, T.; et al. Domiciliary High-Flow Nasal Cannula Oxygen Therapy for Patients with Stable Hypercapnic Chronic Obstructive Pulmonary Disease. A Multicenter Randomized Crossover Trial. Annals of the American Thoracic Society. 2018, 15, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.F.; Kind, P.; Parkin, D.; et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality of Life Research. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [PubMed]
- Bonnevie, T.; Elkins, M.; Paumier, C.; Medrinal, C.; Combret, Y.; Patout, M.; et al. Nasal High Flow for Stable Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. COPD: Journal of Chronic Obstructive Pulmonary Disease. 2019, 16, 368–377. [Google Scholar] [CrossRef]
- Nagata, K.; Horie, T.; Chohnabayashi, N., Jinta; et al. Home High-Flow Nasal Cannula Oxygen Therapy for Stable Hypercapnic COPD: A Randomized Clinical Trial. American Journal of Respiratory and Critical Care Medicine. 2022, 206, 1326–1335. [Google Scholar] [CrossRef]
- Horvath, C.; Baty, F.; Kähler, C.J. Long term home high flow nasal cannula therapy in hypercapnic and hypoxic patients after non-invasive ventilation failure – a retrospective analysis. European Respiratory Journal. 2019.
- McKinstry, S.; Singer, J.; Baarsma, J.P.; Weatherall, M.; Beasley, R.; Fingleton, J. Nasal high-flow therapy compared with non-invasive ventilation in COPD patients with chronic respiratory failure: A randomized controlled cross-over trial. Respirology. 2019. [CrossRef]
- Huang, H.W.; Sun, X.M.; Shi, Z.H.; Chen, G.Q.; Chen, L.; Friedrich, J.O.; et al. Effect of High-Flow Nasal Cannula Oxygen Therapy Versus Conventional Oxygen Therapy and Noninvasive Ventilation on Reintubation Rate in Adult Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Intensive Care Medicine. 2017, 33, 609–623. [Google Scholar] [CrossRef]
- Epstein, A.J.; Hartridge-Lambert, S.K.; Ramaker, J.S.; Voigt, L.; Portlock, C.S. Humidified High-Flow Nasal Oxygen Utilization in Patients with Cancer at Memorial Sloan-Kettering Cancer Center. Journal of Palliative Medicine. 2011, 14, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Ambrosino, N.; Fracchia, C. Strategies to relieve dyspnoea in patients with advanced chronic respiratory diseases. A narrative review. Pulmonology. 2019, 25, 289–298. [Google Scholar] [PubMed]
- Wilson, M.T.; Mittal, A.; Dobler, C.C.;Curtis, J.R.; et al. High-Flow Nasal Cannula Oxygen in Patients with Acute Respiratory Failure and Do-Not-Intubate or Do-Not-Resuscitate Orders: A Systematic Review. Journal of Hospital Medicine. 2020, 15, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Messika, J.; Ben Ahmed, K.; Gaudry, S.; Miguel-Montanes, R.; Rafat, C.; Sztrymf, B.; et al. Use of High-Flow Nasal Cannula Oxygen Therapy in Subjects With ARDS: A 1-Year Observational Study. Respiratory Care. 2014, 60, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Y.; Steele, P.; Dabscheck, E.; Smallwood, N. Nasal High Flow Therapy For Symptom Management in People Receiving Palliative Care. Journal of Pain and Symptom Management. 2021. [CrossRef]
- Hui, D.; Morgado, M.; Chisholm, G.; Withers, L.; Nguyen, Q.; Finch, C.; et al. High-Flow Oxygen and Bilevel Positive Airway Pressure for Persistent Dyspnea in Patients With Advanced Cancer: A Phase II Randomized Trial. Journal of Pain and Symptom Management. 2013, 46, 463–473. [Google Scholar] [CrossRef]
- Shah, N.; Mehta, Z.; Mehta, Y. High-Flow Nasal Cannula Oxygen Therapy in Palliative Care #330. Journal of Palliative Medicine. 2017, 20, 679–680. [Google Scholar]
- Murphy, P.B.; Rehal, S.; Arbane, G.; Bourke, S.; Calverley, P.M.A.; Crook, A.M.; et al. Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation. JAMA [Internet]. 2017, 317, 2177. Available online: https://jamanetwork.com/journals/jama/fullarticle/2627985. [CrossRef]
- Gassama, A.; Mukherjee, D.; Ahmed, U.; Coelho, S.; Daniels, M.; Mukherjee, R. The Effect of Telemonitoring (TM) on Improving Adherence with Continuous Positive Airway Pressure (CPAP) in Obstructive Sleep Apnoea (OSA): A Service Improvement Project (SIP). Healthcare. 2022, 10, 465. [Google Scholar] [CrossRef]
Figure 1.
Schematic Representation of the physiological effects of HFNC in respiratory failure. Abbreviations: L/min litres per minute, FiO2 fraction of inspired oxygen, PEEP positive end expiratory pressure, EELV end expiratory lung volume, PaO2 partial pressure of oxygen in arterial blood, PaCO2 partial pressure of carbon dioxide in arterial blood, WoB work of breathing, RR respiratory rate.
Figure 1.
Schematic Representation of the physiological effects of HFNC in respiratory failure. Abbreviations: L/min litres per minute, FiO2 fraction of inspired oxygen, PEEP positive end expiratory pressure, EELV end expiratory lung volume, PaO2 partial pressure of oxygen in arterial blood, PaCO2 partial pressure of carbon dioxide in arterial blood, WoB work of breathing, RR respiratory rate.
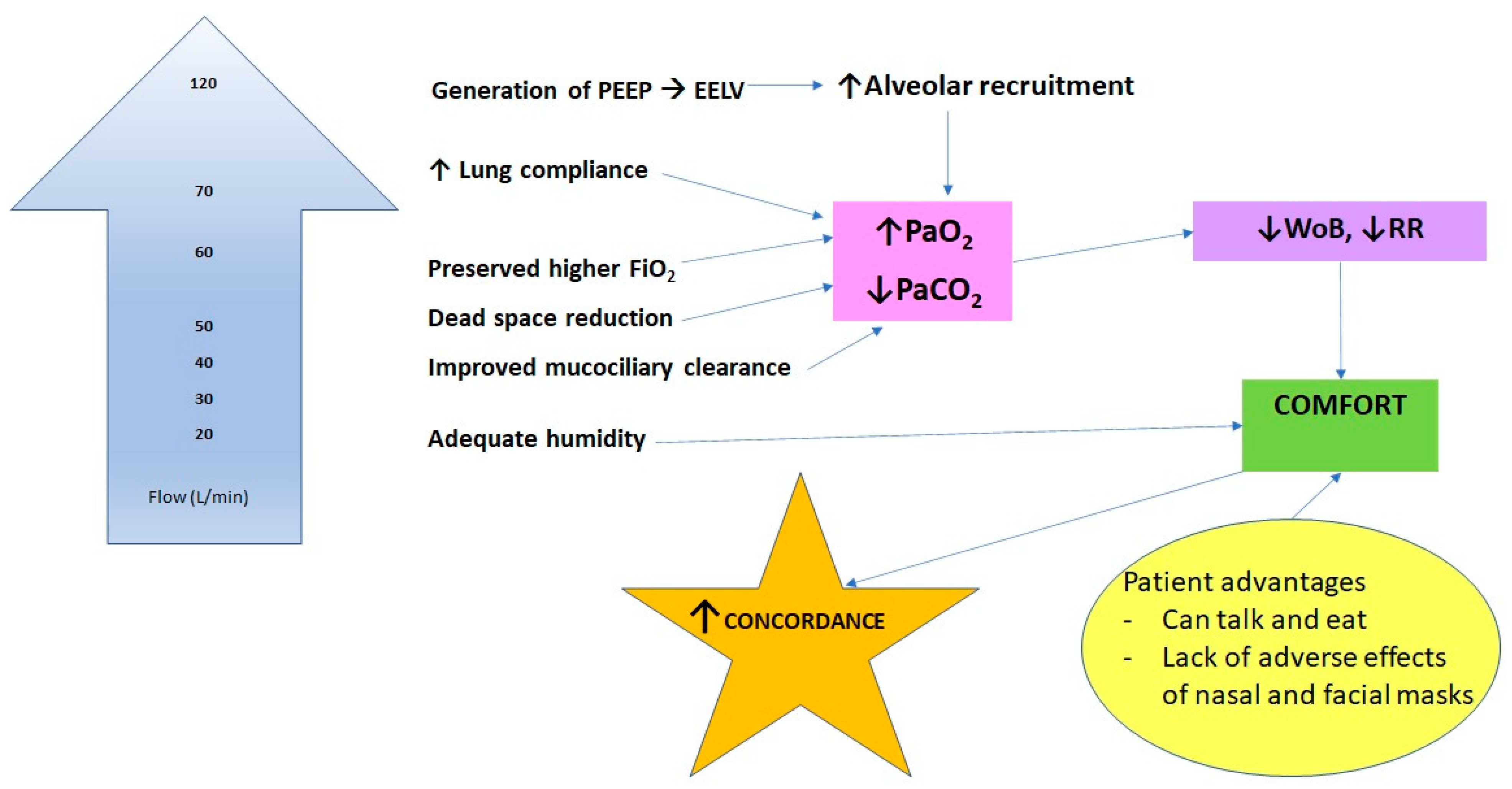

Table 1.
Summary of established and potential applications of HFNC in suitable settings and physiological effects. Abbreviations: ED emergency department, ICU intensive care unit, HDU high dependency unit.
Table 1.
Summary of established and potential applications of HFNC in suitable settings and physiological effects. Abbreviations: ED emergency department, ICU intensive care unit, HDU high dependency unit.
| Clinical Application | Setting of Application | Physiological Effects |
|---|---|---|
| Acute respiratory failure | ED, ICU, hospital ward | Maintains higher FiO2, improves lung compliance, improves alveolar recruitment, increases PaO2, decreases PaCO2, reduces WoB, improves patient comfort |
| Acute exacerbation of COPD | ED, ICU, HDU, hospital ward | Increases dead space wash out, leading to improved gas exchange and reduction in PaCO2 |
| Stable hypercapnic COPD | Home | Reduces exacerbations and PaCO2, leading to improved quality of life |
| Support during exercise in COPD | Home, pulmonary rehabilitation | Improves oxygenation, leading to less dyspnoea, leading to increased exercise tolerance |
| Cardiogenic pulmonary oedema | ED, ICU, HDU, hospital ward | Improves oxygenation, decreases afterload |
| Prevention of reintubation | Theatres, ICU, HDU, hospital ward | Improves gas exchange similar to NIV |
| Preoxygenation during airway procedures | Theatres | Increased apnoea time |
| Breaks from positive airway pressure | ICU, hospital ward | Patients can eat and talk |
| Immunocompromised patients | ED, ICU, hospital ward | Improves gas exchange similar to NIV |
| Palliative patients | ED, hospital ward, ICU/HDU if clinically appropriate, home, hospice | Decreases breathlessness |
| Bronchiectasis and cystic fibrosis | ICU, hospital ward, home | Improves mucociliary clearance, leading to improved ventilation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



