
Submitted:
01 August 2023
Posted:
02 August 2023
You are already at the latest version
Abstract
Background and Objectives: Treatment of visceral artery pseudoaneurysms (VAP) is always indicated regardless of their diameters, as their risk of rupture is significantly higher than that of visceral artery aneurysms. The invasiveness of surgery and its associated complications have led to a shift in favour of radiological interventions as the initial treatment of choice. However, there are still some unanswered questions on endovascular treatment of VAP regarding the optimal endovascular technique and the efficacy and safety outcomes. The purpose of this multicenter study was to retrospectively evaluate the effectiveness and safety of endovascular treatment of visceral pseudoaneurysms using Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs).
Materials and Methods: Consecutive patients who underwent endovascular embolization with EVOH-based NALEAs for visceral artery pseudoaneurysms between January 2018 and June 2023 were retrospectively evaluated.
Results: 38 embolizations were performed. Technical success was achieved in all patients. The clinical success rate was high (92.1% overall), with no significant differences between ruptured and unruptured VAPs (p=0.679). 7 patients (18.4%) experienced procedure-related complications, related to a case of non-target embolization, four splenic abscesses due to end-organ infarction and two femoral pseudoaneurysms. The rates of procedure-related complications, end-organ infarction, and vascular access-site complications did not significantly differ between ruptured and unruptured VAPs (p>0.05).
Conclusions: Both ruptured and unruptured visceral pseudoaneurysms can be effectively and safely treated with NALEA-based endovascular embolization. We suggest considering the use of NALEAs, particularly in specific clinical cases that highlight their advantages, including patients with coagulopathy, fragile vessels, and embolization targets that are located at a considerable distance from the microcatheter tip and are otherwise difficult to reach.
Keywords:
pseudoaneurysm
; visceral pseudoaneurysms
; TAE
; embolization
; endovascular treatment
; percutaneous
; embolic agents
; EVOH
; NALEA
; Onyx
1. Introduction
Visceral artery pseudoaneurysms (VAPs) are critical vascular abnormalities originating from the splanchnic circulation, often attributed to inflammatory, infectious, traumatic, iatrogenic, and neoplastic etiologies [1,2]. Distinguishing them from true aneurysms, pseudoaneurysms arise from the disruption of the intimal and medial layers of the arterial wall, lacking an epithelized wall structure [3]. Pseudoaneurysms pose a significant risk to patient health and survival [1,2].
Accurate pre-procedural imaging is crucial to assess the anatomy of the pseudoaneurysm, its relationship with surrounding structures, and to plan the endovascular intervention [4,5]. It should be noted that there are no studies specifically designed to identify the best imaging work-up for VAP. However, some reviews suggest that CT-angiography (CTA) is preferred over other imaging methods, both in an emergency and in an election fashion, because of its high accuracy, low invasiveness, and ease of performance [6,7,8,9]. Ultrasonography frequently serves as the primary diagnostic modality, capable of incidentally identifying sizeable pseudoaneurysms that are superficially located or within solid organs such as the liver and spleen [4,10]. The utilization of MR-angiography (MRA) for VAP detection is infrequent due to limitations such as inapplicability in hemodynamically unstable patients, extended scan durations, elevated costs, and lower spatial resolution compared to CTA. Nonetheless, the absence of ionizing radiation and the availability of non-contrast techniques confer certain advantages to MRA [4,6,11]. In exceptional cases, digital subtraction angiography (DSA) may be warranted in the identification of a VAP when there is a strong clinical suspicion and non-invasive imaging modalities such as CTA yield unremarkable findings [12].
Treatment of VAPs is always indicated regardless of its diameters, as their risk of rupture is significantly higher than that of visceral artery aneurysms (VAAs) [13,14,15]. VAPs ruptured at a substantially greater incidence than VAAs (76.3% vs. 3.1%), according to an investigation on 233 individuals by Pitton et al. [16]. Visceral pseudoaneurysms with and without rupture did not differ significantly in size, and the rupture event is not reliably predicted by diameter [16]. Compared to 30% of VAAs, 80% of VAPs were symptomatic upon presentation according to a series by Tulsyan et al. [17]. Therefore, treatment of VAPs is recommended as soon as possible [15].
Traditionally, surgical intervention has been the primary approach for addressing pseudoaneurysms [13,15]. Nevertheless, the invasiveness of surgery and its associated complications have led to a shift in favor of radiological interventions as the initial treatment of choice. Radiological interventions offer the advantages of minimally invasive procedures, demonstrating notable success rates and minimal complication rates [10,13,15,18,19]. Endovascular treatment has become the preferred method for the management of VAPs in many cases, as it allows the pseudoaneurysm to be excluded from the arterial circulation, thus preventing its rupture and associated complications [15].
However, there are still some unanswered questions and ongoing research in this field. Firstly, there is a lack of consensus regarding the optimal endovascular technique (e.g., coil embolization, liquid embolic agents, stent grafts) as it depends on various factors, including the size, location, and morphology of the pseudoaneurysm, as well as the patient's overall health condition [12]. Further studies are needed to evaluate the efficacy of different techniques and identify patient-specific factors that influence treatment selection. Secondly, there is a need for further investigation into the potential complications associated with endovascular repair of VAPs, such as stent graft migration, infection, endoleaks, visceral ischemia, and long-term vascular complications [15]. Understanding these risks and implementing strategies to minimize adverse events are essential for optimizing patient outcomes. Thirdly, a paucity of studies focused exclusively on reporting data regarding pseudoaneurysms, and the available studies exhibited limited sample sizes [13,20].
In this context, the purpose of the study was to retrospectively evaluate the efficacy and safety of endovascular treatment of visceral pseudoaneurysms using Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs). Data were collected exclusively on patients with VAPs, discarding cases of endovascular treatment of VAAs.
2. Materials and Methods
2.1. Study design
Consecutive patients who underwent endovascular embolization for visceral artery pseudoaneurysms between January 2018 and June 2023 were retrospectively evaluated.
Inclusion criteria were: I) transcatheter arterial embolization of visceral artery pseudoaneurysm; II) 18 years of age or older; III) evaluation in a multidisciplinary team composed by surgeons, interventional radiologists and anesthesiologists. The following exclusion criteria were applied: I) pregnant or nursing females; II) individuals with a platelet (PLT) count lower than 20,000 per microliter of blood, as per the recommendations of the Society of Interventional Radiology (SIR), who also declined blood component transfusion [21]; III) International Normalized Ratio (INR) levels incompatible with femoral (>1.8) or radial (>2.2) artery access for low bleeding risk operations that require arterial access [21]; IV) documented hypersensitivity to suitable embolic agents; V) patients presenting at an emergency room of another hospital and subsequently transferred to our facilities.
Given the retrospective nature of the study, no ethical committee permission was required. The research adhered to the principles outlined in the Declaration of Helsinki. Prior to the endovascular procedure, written informed consent was obtained from each patient.
2.2. Treatment
The diagnostic workup included performing CT-angiography, which was necessary to make diagnosis and plan endovascular intervention. Occasionally, critically ill patients with an already known diagnosis of VAP (e.g., by ultrasound examination) were transferred directly to the angiography room. A 24-hour interventional radiology service was available at participating centers (Dulbecco University Hospital, Catanzaro, Italy; Circolo Hospital, Varese, Italy; Maggiore della Carità University Hospital, Novara, Italy; Mater Domini University Hospital, Catanzaro, Italy; Pugliese-Ciaccio Hospital, Catanzaro, Italy; San Timoteo Hospital, Termoli, Italy), so the first treatment option for VAPs was always endovascular embolization. An absolute contraindication for percutaneous interventions arises when preserving adequate blood flow to the target organ is of utmost importance and would be potentially compromised by the implementation of endovascular techniques, therefore a surgical approach is indicated (e.g., hepatic artery nourishing a compromised liver and covered stent delivery not feasible) [22]. Patients symptomatic or with evidence at CTA of ruptured VAPs were treated on an urgent basis. Asymptomatic patients with unbroken VAPs were treated as early as possible in the daytime [15].
In all patients undergoing angiography, a transfemoral retrograde approach was employed as first-choice vascular access. This approach offers the advantage of using a wide range of catheters with various shapes and sizes, enabling selective access to the splanchnic vessels. Following catheterization, angiography was performed by injecting iodinated contrast medium through the catheter to visualize the target vessel and identify any associated pathology. Subsequently, embolization materials or covered stent were delivered through the catheter under fluoroscopic guidance to address the pseudoaneurysm. Prior to embolization, ensuring the accurate positioning of the catheter tip is crucial to avoid unintentional non-target embolization. The endovascular procedure was conducted in specialized catheterization laboratories by a skilled interventional radiologist. The selection of the embolic agent was based on the personal preferences of the operator. Non-adhesive liquid embolic agents (NALEAs) were prepared following the provided instructions and administered under fluoroscopic guidance using a microcatheter compatible with dimethyl sulfoxide (DMSO). To prevent EVOH (ethylene vinyl alcohol) copolymer precipitation, the dead space of the microcatheter, including the luer-lock hub at its proximal end, was filled with DMSO. The microcatheter was strictly single-use and not subjected to DMSO rinsing after the injection. By adhering to a controlled injection rate, ensuring it remains below the recommended threshold of 0.3 mL/min, the potential for reflux has been minimized. This, in turn, has reduced the risk of unintended embolization in non-target areas, thereby enhancing the precision and control over the delivery of embolic agents [23,24,25]. Evaluation of technical success and identification of any non-target embolization were carried out through postembolization angiography. Follow-up consisted of clinical examination at 1 and 6 months, and of CTA at 6 months after embolization.
2.3. Outcomes and Definitions
The primary efficacy endpoint was to report the clinical success rate of endovascular treatment of VAPs using EVOH Copolymer-Based NALEAs. The secondary efficacy endpoint was to investigate the differences in technical success, clinical success, reintervention, and 30-day bleeding-related mortality rates between ruptured (rVAP) and unruptured (urVAP) VAPs. The primary safety endpoint of this study was determined to be the disparity in procedure-related complication rates between the two groups (ruptured vs. unruptured VAPs). End-organ infarction rate was evaluated as secondary safety endpoints.
SIR reporting standards were used [26]. Technical success was defined by the effective exclusion of the VAP from circulation. Time-to-embolization (TTE) was calculated as the time elapsed between diagnosis and successful embolization. VAP was defined as ruptured if active contrast extravasation was noted on CTA or angiography. Procedure-related complication rate included vascular access site complication (VASC) rate. The subgroup with coagulopathy was characterized using the criteria established by Loffroy et al., where coagulopathy was defined as having an International Normalized Ratio (INR) greater than 1.5, a partial thromboplastin time exceeding 45 seconds, or a platelet count below 80,000/mm3 [27]. Procedure-related complications were classified according to the 2017 SIR classification [28], the 2003 SIR classification [29], and the CIRSE classification [30].
2.4. Statistical analysis
The data were recorded and organized in a Microsoft Excel spreadsheet (Microsoft Inc, Redmond, Wash), while statistical analyses were conducted based on the intention-to-treat principle using SPSS software (version 22 for Windows; SPSS Inc, Chicago IL, USA) and R/R Studio software. The Modified Intention-To-Treat population, consisting of all randomized patients who underwent at least one embolization procedure, was utilized for the subsequent analyses [31,32]. Kolmogorov-Smirnov and Shapiro-Wilk tests were performed to verify the normality assumption of data. Categorical data are presented as frequencies (% value) [33]. Continuous data with a normal distribution are expressed as mean ± standard deviation, whereas continuous data that do not follow a normal distribution are presented as median (first to third quartile) [34,35]. Statistical differences in continuous data with a normal distribution were assessed using the unpaired Student t-test, while categorical data and continuous data without a normal distribution were evaluated using the Chi-squared/Fisher's exact tests and the Mann-Whitney test, respectively [36,37,38]. A P-value of less than 0.05 was considered statistically significant for all the aforementioned tests.
Figure 1.
In Figure A, CT angiography reveals spontaneous retroperitoneal bleeding attributed to a ruptured pseudoaneurysm (indicated by the arrow) originating from a renal tumor. Figure B shows digital subtraction angiography, which confirms the presence of a ruptured pseudoaneurysm arising from a feeding artery of the tumor. Lastly, Figure C displays digital subtraction angiography, illustrating the successful embolization achieved using an EVOH copolymer cast (indicated by the arrowhead). (From Minici et al. doi: 10.3390/medicina59040710, by MDPI, Basel, Switzerland, licensed under CC BY 4.0).
Figure 1.
In Figure A, CT angiography reveals spontaneous retroperitoneal bleeding attributed to a ruptured pseudoaneurysm (indicated by the arrow) originating from a renal tumor. Figure B shows digital subtraction angiography, which confirms the presence of a ruptured pseudoaneurysm arising from a feeding artery of the tumor. Lastly, Figure C displays digital subtraction angiography, illustrating the successful embolization achieved using an EVOH copolymer cast (indicated by the arrowhead). (From Minici et al. doi: 10.3390/medicina59040710, by MDPI, Basel, Switzerland, licensed under CC BY 4.0).
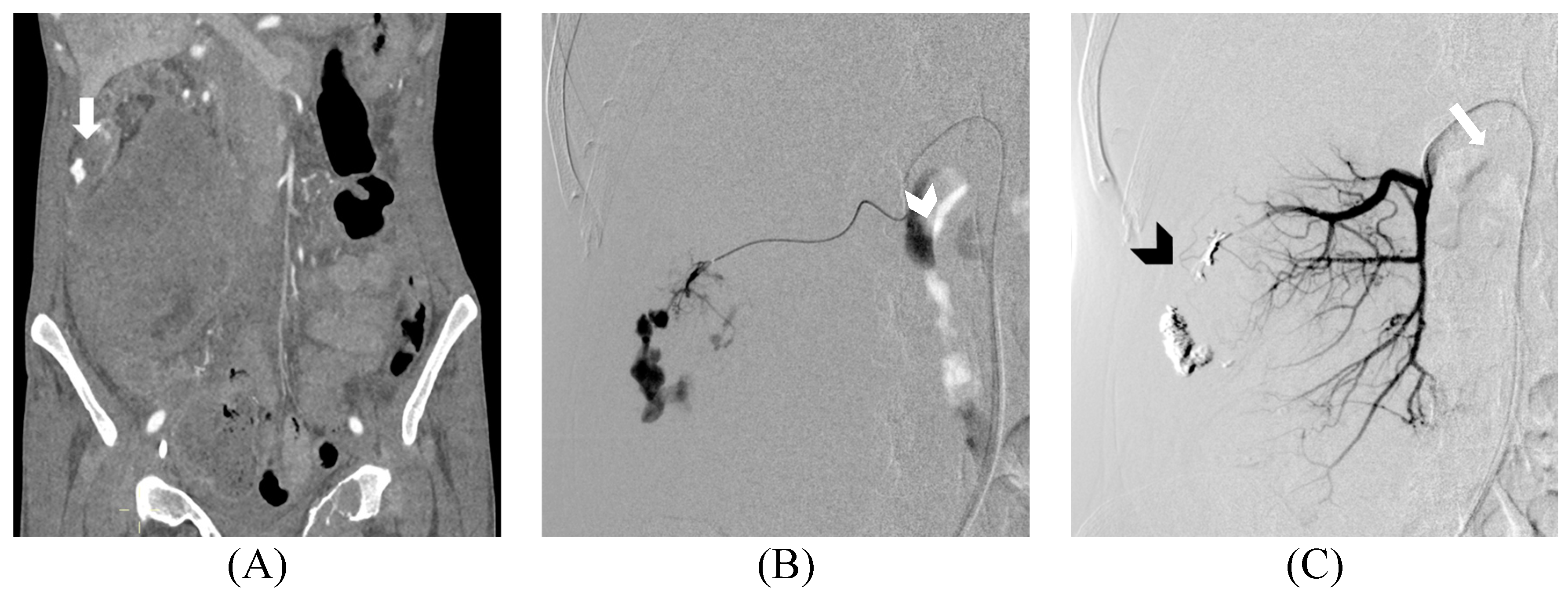
Figure 2.
Ruptured Hepatocellular Carcinoma (HCC) within the hepatic parenchyma is depicted in the images. In the contrast-enhanced CT, arterial phase, there is evidence of a 1 cm pseudoaneurysm within an HCC nodule (A). On the MRI T1 Fast Field Echo In-Phase sequence, hyperintense material (blood) is observed within a large HCC nodule of the right lobe (B). Gd-BOPTA enhanced MRI in the arterial phase confirms the presence of an intranodular contrast blush (C). Superselective digital subtraction angiography of the S7 hepatic artery branch shows contrast leakage into the ruptured HCC (D). Successful embolization of the HCC nodule (indicated by the arrow) and the parent artery (indicated by the arrowhead) was achieved using EVOH copolymer (E and F). (From Minici et al. doi: 10.3390/medicina59040710, by MDPI, Basel, Switzerland, licensed under CC BY 4.0).
Figure 2.
Ruptured Hepatocellular Carcinoma (HCC) within the hepatic parenchyma is depicted in the images. In the contrast-enhanced CT, arterial phase, there is evidence of a 1 cm pseudoaneurysm within an HCC nodule (A). On the MRI T1 Fast Field Echo In-Phase sequence, hyperintense material (blood) is observed within a large HCC nodule of the right lobe (B). Gd-BOPTA enhanced MRI in the arterial phase confirms the presence of an intranodular contrast blush (C). Superselective digital subtraction angiography of the S7 hepatic artery branch shows contrast leakage into the ruptured HCC (D). Successful embolization of the HCC nodule (indicated by the arrow) and the parent artery (indicated by the arrowhead) was achieved using EVOH copolymer (E and F). (From Minici et al. doi: 10.3390/medicina59040710, by MDPI, Basel, Switzerland, licensed under CC BY 4.0).
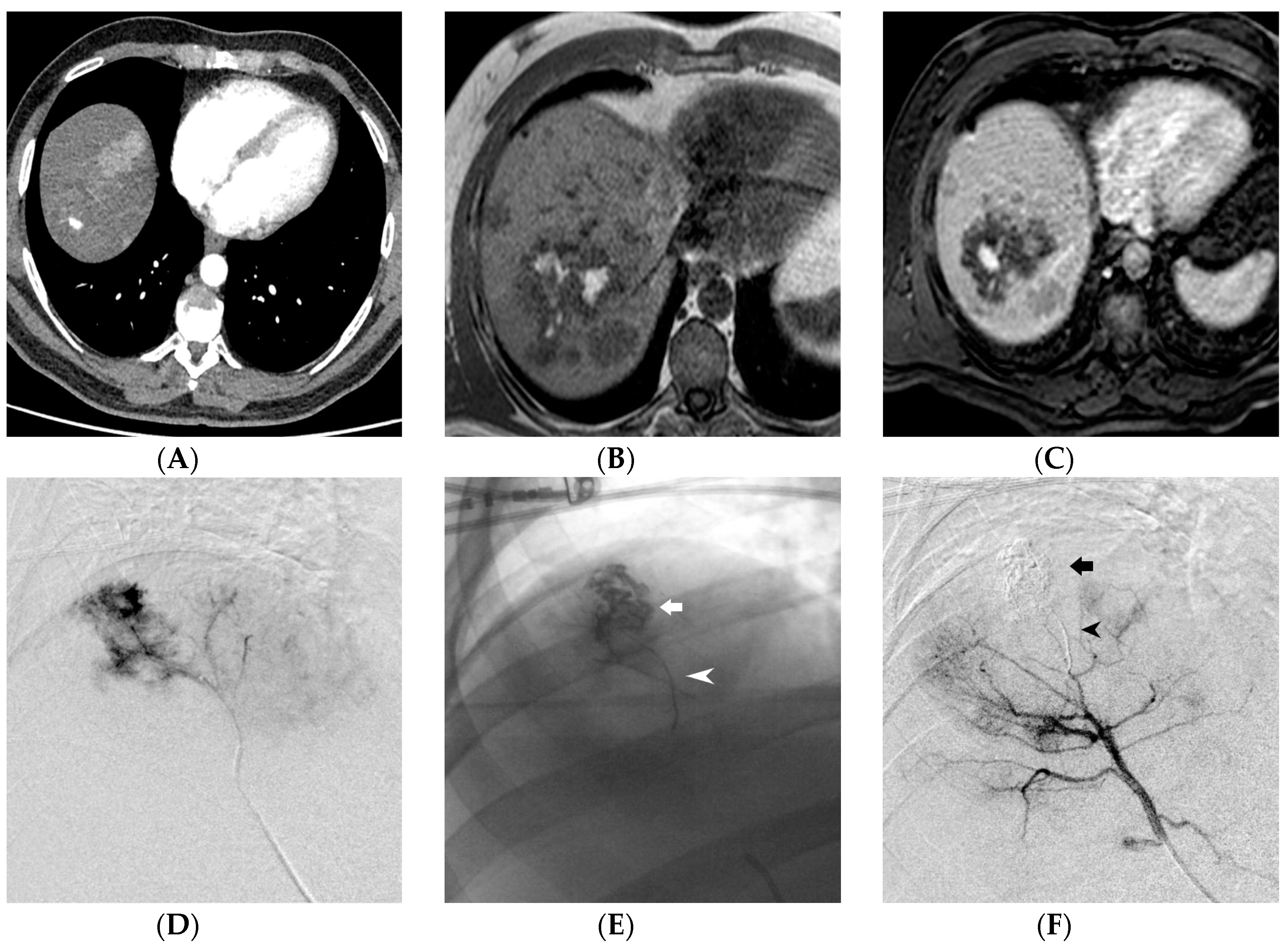
Figure 3.
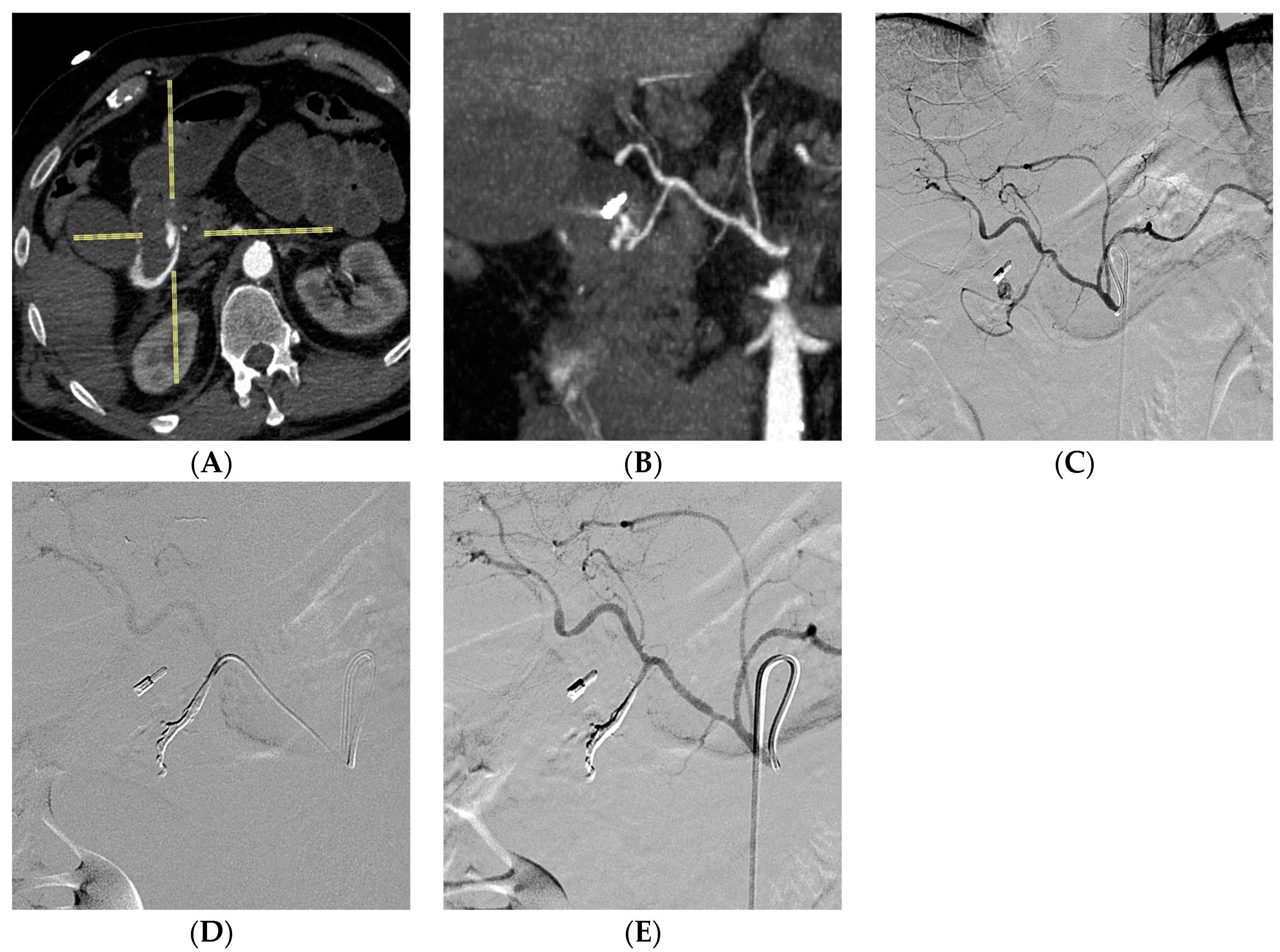
A young woman with a history of NSAID overuse experienced a sudden onset of hematemesis. During endoscopy, duodenal bleeding was observed but proved unresponsive to treatment. Advanced imaging techniques, including axial CT scans (A) and MPR coronal reconstruction (B), revealed the presence of a pseudoaneurysm in the gastroduodenal artery. The celiac trunk was subsequently catheterized, confirming the presence of the pseudoaneurysm (arrow) close to the clip previously placed by the endoscopist at the site of bleeding (C). To address the condition, a superselective catheterization of the gastroduodenal artery was performed using a DMSO-compatible microcatheter, followed by effective embolization using EVOH copolymer (D). The completion angiography confirmed the successful embolization, with the EVOH copolymer cast distributed along the gastroduodenal artery, ensuring no unintended embolizations to non-target areas (E).
Figure 3.
A young woman with a history of NSAID overuse experienced a sudden onset of hematemesis. During endoscopy, duodenal bleeding was observed but proved unresponsive to treatment. Advanced imaging techniques, including axial CT scans (A) and MPR coronal reconstruction (B), revealed the presence of a pseudoaneurysm in the gastroduodenal artery. The celiac trunk was subsequently catheterized, confirming the presence of the pseudoaneurysm (arrow) close to the clip previously placed by the endoscopist at the site of bleeding (C). To address the condition, a superselective catheterization of the gastroduodenal artery was performed using a DMSO-compatible microcatheter, followed by effective embolization using EVOH copolymer (D). The completion angiography confirmed the successful embolization, with the EVOH copolymer cast distributed along the gastroduodenal artery, ensuring no unintended embolizations to non-target areas (E).
3. Results
Endovascular embolization with EVOH-based NALEAs was performed in 38 patients with VAPs. The population was divided into two groups based on whether the pseudoaneurysm ruptured (namely rVAP group, 17 subjects) or was intact (namely urVAP group, 21 subjects). urVAP and rVAP groups did not differ statistically in age, gender, BMI, renal and coagulation function, baseline hemoglobin, antiplatelet and anticoagulant therapy, and CTA execution. Individuals with rVAP showed more frequent symptoms and hemodynamic instability than individuals with urVAP. Interestingly, rVAP group had a significantly shorter maximum pseudoaneurysm diameter than urVAP group (3.3 vs. 4.4 cm; p=0.005). Demographic and clinical data are reported in Table 1.
The most common etiologies were trauma, iatrogenic causes (e.g., biopsy, PCNL, surgery), and medical conditions (e.g., pancreatitis, cholecystitis, cancer, abscess). The distribution of pseudoaneurysm locations did not significantly differ between the groups (p=0.830). The most common sites were splenic, hepatic, and renal. The majority of patients with unruptured pseudoaneurysms underwent treatment as soon as possible, while patients with ruptured pseudoaneurysms had more urgent treatment (p<0.001). The distribution of EVOH viscosity did not show significant differences between the groups (p=0.449). There were no significant differences in time and radiation-related variables (CT-to-groin time, procedure time, CT-to-embolization time, fluoroscopy time, cumulative air kerma (CAK), and dose area product (DAP)) between the groups. Procedure data are summarized in Table 2.
The technical success rate was 100% for all patients, indicating that the endovascular treatment was successful in achieving the desired outcome. The clinical success rate, indicating resolution of symptoms, was high in both groups (92.1% overall), with no significant differences between the unruptured and ruptured groups (p=0.679). The incidence of rebleeding was low in both groups, with no significant differences observed (p=0.819). The need for blood transfusion was significantly higher in the rVAP group compared to the urVAP group (p<0.001). The occurrence of non-target embolization was low overall (2.6%), related to only one case of non-occluding reflux in the right hepatic artery without clinical sequelae. 7 patients (18.4%) experienced procedure-related complications, related to a case of non-target embolization, four splenic abscesses due to end-organ infarction (2 cases managed with antibiotic therapy, while the other two with percutaneous drainage), a case of femoral pseudoaneurysm treated with US-guided thrombin injection and another case of femoral pseudoaneurysm managed with prolonged groin compression. The rates of procedure-related complications, end-organ infarction, and vascular access-site complications did not significantly differ between the unruptured and ruptured VAP groups (p>0.05). The mortality rate due to bleeding within 30 days was low overall (linked to a single case of multiple organ dysfunction syndrome in a patient with major trauma), with no significant differences between the urVAP and rVAP groups (p=0.362). Details are reported in Table 3.
4. Discussion
Visceral pseudoaneurysms form a heterogeneous category due to their occurrence in diverse arterial locations and their association with a range of etiologies [15,22]. The etiology of VAP recognizes a few main causes, including trauma, iatrogenic procedures (e.g., biopsies, percutaneous nephrolithotomy, surgery, radiation therapy, etc.), and medical conditions (e.g., acute pancreatitis, tumors, abscesses, etc.) [13,14]. The majority of the studies available in the literature include a mixed population comprising both VAAs and VAPs, thus introducing an additional source of data heterogeneity given their distinct pathological conditions [13]. Besides, the assessment of outcomes in endovascular treatment is further complicated by the presence of studies in which various endovascular techniques were employed, but the outcomes were not differentiated based on the specific technique used [22,39,40]. It would be desirable to have outcome data specific to each technique in order to conduct comparative evaluations among homogeneous patient groups according to the site and etiology of the VAP.
Endovascular treatment aims to effectively exclude the VAP from the systemic circulation [6]. Nagaraja et al. conducted one of the few comparative assessments between surgery and angioembolization for the treatment of hepatic artery pseudoaneurysms, concluding that both techniques are effective. However, they found that endovascular treatment offers faster hemostasis, reduced transfusion requirements, and shorter hospital stays [41]. The choice of endovascular technique and embolic agent relies on several factors, including the size of the pseudoaneurysm sac and neck, the expendability of the parent artery, the presence of terminal or collateral circulation, the feasibility of superselective catheterization of the pseudoaneurysm considering vessel tortuosity and hostile anatomy, the availability of adequate landing zones for a covered stent, the patient's coagulation status, and the operator's preferences [12,42,43].
Deliberate parent artery sacrifice is generally considered in cases of end-arteries (e.g., intraparenchymal renal pseudoaneurysm) or when the presence of collateral circulations minimizes the risk of end-organ ischemia. Fascinatingly, the study conducted by Nagaraja et al. provided evidence that the occlusion of the common hepatic artery is generally well-tolerated when treating VAP in patients with preserved liver function. This favorable tolerance is attributed to the phenomenon of flow reversal in the gastroduodenal artery and the hypertrophy of branches originating from the inferior phrenic artery [41,44]. In the presence of collateral circulation (e.g., splenic, hepatic and gastroduodenal VAPs), the sandwich embolization of afferent and efferent vessels is essential to achieve effective embolization, thus preventing backdoor bleeding [6]. Conversely, in the case of end-arteries (e.g., renal circulation), proximal embolization of the afferent artery alone proved to be effective [45,46]. Liquid embolics may allow to avoid direct negotiation of the pseudoaneurysm sac; however, they are associated with a risk of non-target embolization. In such situations, in addition to adjusting the density of the liquid embolic, it is possible to employ the sandwich technique by pre-embolizing the outflow with coils to minimize the risk of unintentional leakage of the liquid embolic [6,19,47,48].
When intentional parent artery sacrifice is not indicated, it is necessary to exclude the VAP from the circulation while preserving the patency of the parent artery [6,12]. The task can be accomplished through selective embolization of the pseudoaneurysm sac using coils, vascular plugs, or liquid embolics such as NALEA or n-butyl cyanoacrylate (NBCA) [49]. Unlike coils, liquid embolics can avoid exerting radial force on the sac, but they carry a higher risk of reflux and non-target embolization [19,47]. In some cases of wide neck, stent-assisted or balloon-remodelling techniques can be employed to provide a scaffold for safer delivery of the embolic agent [4,6]. Finally, in the presence of adequate landing zones, the pseudoaneurysm can be excluded while preserving patency of the parent artery through the deployment of a covered stent [50,51]. The successful placement of stent grafts is often impeded by the small size or tortuous nature of numerous visceral arteries, leading to a restricted range of stent graft options available [52]. Recently, the use of multi-layered flow-diverting stents has emerged in the treatment of true visceral aneurysms due to their ability to induce flow stagnation and subsequent thrombosis within the sac while preserving the patency of the parent artery and any collateral branches originating from the segment covered by the stent [53]. However, evidence regarding their use in visceral pseudoaneurysms is limited, as thrombosis requires time to occur, whereas the risk of imminent rupture remains substantial [12,54,55].
This study aims to mitigate the data heterogeneity prevalent in the literature by presenting the outcomes of endovascular treatment specifically for VAPs managed by embolization with EVOH-copolymer based NALEAs. The efficacy endpoints in the present series are comparable to those in other research, although the frequent case mix in previous reports (i.e., VAAs/VAPs, endovascular/surgical treatments, parent artery sacrifice/preservation, various embolic agents) makes comparative evaluation difficult. Evidence on endovascular treatment of VAPs using EVOH Copolymer-Based NALEAs is poor and often limited to mixed reports involving visceral true aneurysms and pseudoaneurysms [56]. Ghoneim et al. reported the outcomes of the endovascular management of 15 renal arterial pseudoaneurysms following partial nephrectomy. They achieved an 80% clinical success rate with coils embolization technique [20]. In their mixed cohort of 33 VAAs/VAPs, Regus et al. treated with coils embolization technique 2 splenic artery VAPs, 2 hepatic artery VAPs and 2 pancreaticoduodenal artery VAPs, achieving a 100% technical success rate. Interestingly, the average diameter of ruptured VAPs was found to be 2 cm, whereas non-ruptured VAPs measured 3.5 cm on average [14]. In a recent investigation by Zabicki et al. on 15 pancreatitis-related pseudoaneurysms, coil embolization was conducted in five patients, while one patient received treatment with a stent graft. Liquid embolic agents were utilized in seven cases, with thrombin injection being employed in five patients and Squid in two patients. A combination of techniques was employed in two patients. A technical success rate of 93.3% and a reintervention rate of 6.7% were noted [39]. Balderi et al. examined the short- and medium-term outcomes of endovascular repair of 31 VAAs/VAPs using coils (84%), multilayer stents (9.5%), and a combination of coils with either vascular plug or covered stent (6.5%). Successful immediate exclusion of VAAs/VAPs was achieved in all instances, indicating a 100% technical success rate. However, one patient with a coeliac axis pseudoaneurysm succumbed to renewed hemorrhage and passed away 10 days following the procedure, resulting in a 3% 30-day bleeding-related mortality rate [40]. Fankhauser presented the results of percutaneous endovascular treatment in a large cohort of patients with visceral artery aneurysms (66 cases, 36%) and pseudoaneurysms (119 cases, 64%). In the majority of cases, specifically 144 instances (78%), the exclusive interventional approach involved the utilization of endovascular coiling. Furthermore, in 10 cases (5%), the sole technique employed was the placement of a covered stent to exclude the vascular lesion from circulation. A 98% technical success rate, a 97% clinical success rate, and a 3.4% 30-day bleeding-related mortality rate were noticed [22]. In their investigation on endovascular treatment of 22 VAAs and 7 VAPs, Laganà et al. reported a 100% technical success rate and a 10.3% reintervention rate [57]. Recently, Gong et al. reported a 40% mortality rate for pseudoaneurysms; all patients who died had ruptured VAPs. This finding differs from other evidence probably because of the extremely small sample size (i.e., only 5 VAPs included in the study) [52]. Roberts et al. treated 48 patients with hemorrhaging coeliac or mesenteric artery aneurysms (6%) and pseudoaneurysms (94%); they highlighted a 91.7% technical success rate and a 6.25% 30-day bleeding-related mortality, thus demonstrating the efficacy of endovascular treatment even in cases of bleeding ruptured VAPs [58]. Therefore, endovascular treatment of both ruptured and non-ruptured visceral pseudoaneurysms using EVOH-copolymer-based non-adhesive liquid embolic agents (NALEAs) has comparable efficacy to other embolic agents, as demonstrated by literature review, and can be a valuable tool, especially in certain clinical scenarios where the unique characteristics of NALEAs offer particular advantages.
Firstly, the unique flow characteristics resembling molten magma facilitate the transportation of the embolic agent through narrow arteries, enabling successful embolization of targets located at considerable distances from the microcatheter tip [59,60]. In contrast, the efficacy of coil embolization is diminished when dealing with small-caliber vessels that are challenging to catheterize, and it is less effective in controlling backdoor bleeding stemmed from collateral circulation if the efferent vessels is not embolized [61,62]. Secondly, EVOH-based NALEAs ensure a secure, swift, and efficient embolization process through polymerization, thereby accomplishing mechanical embolization without necessitating coagulation activation. This property is particularly advantageous in patients with coagulation disorders, as supported by previous studies [59,60,63]. Intriguingly, coil embolization exhibits reduced efficacy in individuals with coagulopathy, while liquid embolics do not appear to encounter this limitation [27,64,65,66,67,68,69]. Thirdly, in the study conducted by Khalil et al., it was recommended that EVOH be prioritized for embolization procedures involving compromised blood vessels. This preference stems from the fact that EVOH is capable of deployment without exerting radial pressure on the vessel walls, in contrast to coils and vascular plugs that have the potential to cause rupture in fragile vessels [23].
Repeated endovascular treatment, surgery, percutaneous or endoscopic embolization are the main options if the first-line endovascular therapy fails [58]. If the endovascular management is the first-line therapy, surgery will be needed in less than 5% of cases [58]. Roberts et al. reported a 17% reintervention rate [58]. The underlying causes for the endovascular treatment failure were diverse, yet they predominantly fell into two discernible categories: either the radiological access to the VAP was unsuccessful or the initial attempts at hemorrhage control failed. In instances where radiological access proved unsuccessful, alternative methods such as percutaneous embolization or surgical repair were employed to attain effective control. Conversely, in cases where initial attempts at hemorrhage control failed, it was deemed reasonable to make repeated efforts utilizing the endovascular management, as this approach yielded satisfactory results in half of such instances. A major cause of bleeding control failure is ineffective hemostasis with coils [58]. In our study we observed a very low reintervention rate, may be due to the effectiveness of NALEAs in patients with coagulopathy.
In this study, endovascular embolization using EVOH-copolymer-based NALEAs has been proven to be a safe treatment for both ruptured and unruptured pseudoaneurysms. Other reports on endovascular management of VAPs have shown comparable data. Ghoneim et al. reported a 13.3% procedure-related complication rate in their series on endovascular management with coils embolization of 15 renal arterial pseudoaneurysms following partial nephrectomy [20]. In their cohort of 7 VAPs treated with coils embolization technique (5 patients) or surgery (2 patients), Regus et al. recorded a 14.3% procedure-related complication rate due to a case of bleeding [14]. In a recent investigation by Zabicki et al. on 15 pancreatitis-related pseudoaneurysms treated various techniques including coils embolization, stent graft, and liquid embolic agents, a 13.3% procedure-related complication rate was noted (two cases of splenic ischemia requiring splenectomy) [39]. End-organ ischemia is one of the most feared complications. Balderi et al. observed splenic ischemia in 50% of patients treated for splenic VAAs/VAPs and renal infarction in 75% of patients with renal artery VAPs. However, the evidence agrees that the practical consequences of end-organ ischemia are often minimal; in the series by Balderi et al. only 1 case (3.2%) required surgical treatment (splenectomy) [40]. Similarly, Fankhauser et al. showed 25 cases (13.5%) of splenic or hepatic infarction, but only one case required hepaticojejunostomy for bile duct ischemia; furthermore, a 7.3% VASC rate was noticed [22]. In their investigation on endovascular treatment of 22 VAAs and 7 VAPs, Laganà et al. reported a 27.6% procedure-related complication rate with 7 cases of splenic infarction out of 8 cases of complications [57]. Roberts et al. demonstrated the safety of endovascular treatment even in cases of bleeding ruptured VAPs, highlighting a 6.1% procedure-related complication rate [58]. Furthermore, the safety results of our report, including vascular access site complications, align with previous studies conducted on endovascular treatments and transcatheter arterial embolization [70,71,72,73,74,75,76,77,78,79,80,81,82]. Finally, this retrospective multicenter study provides further evidence supporting the safety and efficacy of endovascular embolization using EVOH-copolymer-based non-adhesive liquid embolic agents (NALEAs) for the management of visceral pseudoaneurysms. These findings also extend to patients with ruptured visceral pseudoaneurysms, highlighting the suitability of this treatment approach in such cases.
However, it is important to acknowledge several limitations associated with EVOH-based non-adhesive liquid embolic agents (NALEAs). Firstly, it is necessary to shake the mixture containing EVOH and tantalum powder vigorously for a duration of 20 minutes to make the embolic agent for use. Consequently, this may limit its application in time-sensitive scenarios [72,83,84]. At our institute, we have successfully tackled this concern by instructing staff to initiate shaking of the vials with a Vortex shaking mixer upon activating the catheterization lab for an angioembolization. Secondly, dimethyl sulfoxide (DMSO) requires the use of a DMSO-compatible microcatheter and exhibits toxicity towards blood vessels, resulting in vasospasm, pain, and the occurrence of atypical reflexes like the trigeminocardiac reflex [48,85,86,87,88]. Thirdly, the addition of tantalum powder to EVOH-based NALEAs enhances radiopacity, facilitating visibility during the embolization procedure; however, it can introduce beam hardening artifacts in subsequent CT examinations. To address this issue, both Onyx and Squid offer reduced tantalum formulations known as Onyx L and Squid LD, respectively, which minimize the occurrence of beam hardening artifacts [89,90].
Some limitations of the study should be noted. The extensive length of the follow-up period instills confidence that our investigation has captured the majority of recurrences or treatment-related complications. However, it is important to acknowledge that the possibility of unreported complications, recurrences, or even fatalities cannot be completely ruled out. Notably, Guillon et al. observed no cases of long-term recurrence in their own study [91]. The implementation of a multicenter registry would allow to collect data prospectively and to be able to carry out comparative evaluations for homogeneous groups taking into account etiology, comorbidities, endovascular technique and embolic agent used. The retrospective nature of the analysis weakens the study also because some cases may have been missed, although we believe this hypothesis unlikely given the research carried out using the radiological electronic database present in all participating centers.
5. Conclusions
In conclusion, this is the first multicenter investigation evaluating the feasibility of endovascular embolization of visceral pseudoaneurysms using EVOH-copolymer-based non-adhesive liquid embolic agents (NALEAs). Our data demonstrate that both ruptured and unruptured visceral pseudoaneurysms can be effectively and safely treated with NALEA-based endovascular embolization, with outcomes similar to those of other embolic agents. We suggest considering the use of NALEAs, particularly in specific clinical cases that highlight their advantages. These cases may include patients with coagulopathy, particularly fragile vessels, and embolization targets that are located at a considerable distance from the microcatheter tip and are otherwise difficult to reach. Nevertheless, further larger comparative studies with long-term follow-ups would be desirable to confirm these preliminary data.
Author Contributions
Conceptualization, R.M. and D.L.; methodology, G.G. and A.S.; software, M.V.; validation, R.M., D.L., F.F., M.V., F.P., A.C., G.G., M.S., A.S., D.C., N.I., Raffaele Serra, Rita Santoro, P.G., L.B. and MGJRT; formal analysis, A.C. and F.P.; investigation, Raffaele Serra, D.C. and N.I.; resources, P.G.; data curation, D.L.; writing—original draft preparation, R.M., D.L., F.F., M.V., F.P., A.C., G.G., M.S., A.S., D.C., N.I., Raffaele Serra, Rita Santoro, P.G., L.B. and MGJRT; writing—review and editing, L.B. and MGJRT; visualization, R.M., D.L., F.F., M.V., F.P., A.C., G.G., M.S., A.S., D.C., N.I., Raffaele Serra, Rita Santoro, P.G., L.B. and MGJRT; supervision, D.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the retrospective nature of the investigation.
Informed Consent Statement
Informed consent was obtained from all patients undergoing endovascular treatment.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy issues.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
APTT: activated partial thromboplastin time; CKD: chronic kidney disease; CTA: CT-angiography; DAP: dose-area product; DSA: digital subtraction angiography; eGFR: estimated Glomerular Filtration Rate; EVOH: ethylene-vinyl alcohol; ICU: intensive care unit; INR: international normalized ratio; MRA: MR-angiography; NALEA: non-adhesive liquid embolic agent; NBCA: N-butyl cyanoacrylate; PCNL: percutaneous nephrolithotomy; PRBC: packed red blood cells; PT: prothrombin time; PVA: polyvinyl alcohol; SIR: Society of Interventional Radiology; TAE: transcatheter arterial embolization; TTE: time-to-embolization; US: ultrasound; VAA: visceral artery aneurysm; VAP: visceral artery pseudoaneurysm; VASCs: vascular access site complications; XA: x-ray angiography.
References
- Gabelmann A, Görich J, Merkle EM. Endovascular treatment of visceral artery aneurysms. J Endovasc Ther 2002;9:38–47. [CrossRef]
- Belli A-M, Markose G, Morgan R. The role of interventional radiology in the management of abdominal visceral artery aneurysms. Cardiovasc Intervent Radiol 2012;35:234–43. [CrossRef]
- Lu M, Weiss C, Fishman EK, Johnson PT, Verde F. Review of visceral aneurysms and pseudoaneurysms. J Comput Assist Tomogr 2015;39:1–6. [CrossRef]
- Saad NEA, Saad WEA, Davies MG, Waldman DL, Fultz PJ, Rubens DJ. Pseudoaneurysms and the role of minimally invasive techniques in their management. Radiographics 2005;25 Suppl 1:S173-189. [CrossRef]
- Shuaib W, Tiwana MH, Vijayasarathi A, Sadiq MF, Anderson S, Amin N, et al. Imaging of vascular pseudoaneurysms in the thorax and abdomen. Clin Imaging 2015;39:352–62. [CrossRef]
- Jesinger RA, Thoreson AA, Lamba R. Abdominal and pelvic aneurysms and pseudoaneurysms: imaging review with clinical, radiologic, and treatment correlation. Radiographics 2013;33:E71-96. [CrossRef]
- Saba L, Anzidei M, Lucatelli P, Mallarini G. The multidetector computed tomography angiography (MDCTA) in the diagnosis of splenic artery aneurysm and pseudoaneurysm. Acta Radiol 2011;52:488–98. [CrossRef]
- Corvino F, Giurazza F, Ierardi AM, Lucatelli P, Basile A, Corvino A, et al. Splenic Artery Pseudoaneurysms: The Role of ce-CT for Diagnosis and Treatment Planning. Diagnostics (Basel) 2022;12:1012. [CrossRef]
- Hagspiel KD, Flors L, Hanley M, Norton PT. Computed tomography angiography and magnetic resonance angiography imaging of the mesenteric vasculature. Tech Vasc Interv Radiol 2015;18:2–13. [CrossRef]
- Keeling AN, McGrath FP, Lee MJ. Interventional radiology in the diagnosis, management, and follow-up of pseudoaneurysms. Cardiovasc Intervent Radiol 2009;32:2–18. [CrossRef]
- Sueyoshi E, Sakamoto I, Nakashima K, Minami K, Hayashi K. Visceral and peripheral arterial pseudoaneurysms. AJR Am J Roentgenol 2005;185:741–9. [CrossRef]
- Madhusudhan KS, Venkatesh HA, Gamanagatti S, Garg P, Srivastava DN. Interventional Radiology in the Management of Visceral Artery Pseudoaneurysms: A Review of Techniques and Embolic Materials. Korean J Radiol 2016;17:351–63. [CrossRef]
- Barrionuevo P, Malas MB, Nejim B, Haddad A, Morrow A, Ponce O, et al. A systematic review and meta-analysis of the management of visceral artery aneurysms. J Vasc Surg 2019;70:1694–9. [CrossRef]
- Regus S, Lang W. Rupture Risk and Etiology of Visceral Artery Aneurysms and Pseudoaneurysms: A Single-Center Experience. Vasc Endovascular Surg 2016;50:10–5. [CrossRef]
- Chaer RA, Abularrage CJ, Coleman DM, Eslami MH, Kashyap VS, Rockman C, et al. The Society for Vascular Surgery clinical practice guidelines on the management of visceral aneurysms. Journal of Vascular Surgery 2020;72:3S-39S. [CrossRef]
- Pitton MB, Dappa E, Jungmann F, Kloeckner R, Schotten S, Wirth GM, et al. Visceral artery aneurysms: Incidence, management, and outcome analysis in a tertiary care center over one decade. Eur Radiol 2015;25:2004–14. [CrossRef]
- Tulsyan N, Kashyap VS, Greenberg RK, Sarac TP, Clair DG, Pierce G, et al. The endovascular management of visceral artery aneurysms and pseudoaneurysms. J Vasc Surg 2007;45:276–83; discussion 283. [CrossRef]
- Bergert H, Hinterseher I, Kersting S, Leonhardt J, Bloomenthal A, Saeger HD. Management and outcome of hemorrhage due to arterial pseudoaneurysms in pancreatitis. Surgery 2005;137:323–8. [CrossRef]
- Chadha M, Ahuja C. Visceral artery aneurysms: diagnosis and percutaneous management. Semin Intervent Radiol 2009;26:196–206. [CrossRef]
- Ghoneim TP, Thornton RH, Solomon SB, Adamy A, Favaretto RL, Russo P. Selective arterial embolization for pseudoaneurysms and arteriovenous fistula of renal artery branches following partial nephrectomy. J Urol 2011;185:2061–5. [CrossRef]
- Patel IJ, Rahim S, Davidson JC, Hanks SE, Tam AL, Walker TG, et al. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions—Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. Journal of Vascular and Interventional Radiology 2019;30:1168-1184.e1. [CrossRef]
- Fankhauser GT, Stone WM, Naidu SG, Oderich GS, Ricotta JJ, Bjarnason H, et al. The minimally invasive management of visceral artery aneurysms and pseudoaneurysms. J Vasc Surg 2011;53:966–70. [CrossRef]
- Khalil A, Fartoukh M, Bazot M, Parrot A, Marsault C, Carette M-F. Systemic arterial embolization in patients with hemoptysis: initial experience with ethylene vinyl alcohol copolymer in 15 cases. AJR Am J Roentgenol 2010;194:W104-110. [CrossRef]
- Rennert J, Herold T, Schreyer AG, Banas B, Jung EM, Feuerbach S, et al. [Evaluation of a liquid embolization agent (Onyx) for transcatheter embolization for renal vascular lesions]. Rofo 2009;181:996–1001. [CrossRef]
- Urbano J, Manuel Cabrera J, Franco A, Alonso-Burgos A. Selective arterial embolization with ethylene-vinyl alcohol copolymer for control of massive lower gastrointestinal bleeding: feasibility and initial experience. J Vasc Interv Radiol 2014;25:839–46. [CrossRef]
- Dariushnia SR, Redstone EA, Heran MKS, Cramer HR, Ganguli S, Gomes AS, et al. Society of Interventional Radiology Quality Improvement Standards for Percutaneous Transcatheter Embolization. Journal of Vascular and Interventional Radiology 2021;32:476.e1-476.e33. [CrossRef]
- Loffroy R, Guiu B, D’Athis P, Mezzetta L, Gagnaire A, Jouve J-L, et al. Arterial embolotherapy for endoscopically unmanageable acute gastroduodenal hemorrhage: predictors of early rebleeding. Clin Gastroenterol Hepatol 2009;7:515–23. [CrossRef]
- Khalilzadeh O, Baerlocher MO, Shyn PB, Connolly BL, Devane AM, Morris CS, et al. Proposal of a New Adverse Event Classification by the Society of Interventional Radiology Standards of Practice Committee. Journal of Vascular and Interventional Radiology 2017;28:1432-1437.e3. [CrossRef]
- Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of Interventional Radiology Clinical Practice Guidelines. Journal of Vascular and Interventional Radiology 2003;14:S199–202. [CrossRef]
- Filippiadis DK, Binkert C, Pellerin O, Hoffmann RT, Krajina A, Pereira PL. Cirse Quality Assurance Document and Standards for Classification of Complications: The Cirse Classification System. Cardiovasc Intervent Radiol 2017;40:1141–6. [CrossRef]
- Minici R, Ammendola M, Manti F, Siciliano MA, Minici M, Komaei I, et al. Safety and Efficacy of Degradable Starch Microspheres Transcatheter Arterial Chemoembolization (DSM-TACE) in the Downstaging of Intermediate-Stage Hepatocellular Carcinoma (HCC) in Patients With a Child-Pugh Score of 8-9. Front Pharmacol 2021;12:634087. [CrossRef]
- Minici R, Ammendola M, Manti F, Siciliano MA, Giglio E, Minici M, et al. Safety and Efficacy of Degradable Starch Microspheres Transcatheter Arterial Chemoembolization as a Bridging Therapy in Patients with Early Stage Hepatocellular Carcinoma and Child-Pugh Stage B Eligible for Liver Transplant. Front Pharmacol 2021;12:634084. [CrossRef]
- Costa D, Ielapi N, Minici R, Peluso A, Bracale UM, Andreucci M, et al. Risk Factors for Bleeding Varicose Veins in Patients with Chronic Venous Disease. Medicina 2023;59:1034. [CrossRef]
- Minici R, Mercurio M, Iannò B, Galasso O, Gasparini G, Laganà D. Advantages of the Use of Axial Traction Magnetic Resonance Imaging (MRI) of the Shoulder in Patients with Suspected Rota-Tor Cuff Tears: An Exploratory Pilot Study. Healthcare 2023;11:724. [CrossRef]
- Ammendola M, Filice F, Battaglia C, Romano R, Manti F, Minici R, et al. Left hemicolectomy and low anterior resection in colorectal cancer patients: Knight-griffen vs. transanal purse-string suture anastomosis with no-coil placement. Front Surg 2023;10:1093347. [CrossRef]
- Rossi R, Talarico M, Schepis F, Coppi F, Sgura FA, Monopoli DE, et al. Effects of sildenafil on right ventricle remodelling in Portopulmonary hypertension. Pulm Pharmacol Ther 2021;70:102071. [CrossRef]
- Rossi R, Talarico M, Pascale A, Pascale V, Minici R, Boriani G. Low Levels of Vitamin D and Silent Myocardial Ischemia in Type 2 Diabetes: Clinical Correlations and Prognostic Significance. Diagnostics (Basel) 2022;12:2572. [CrossRef]
- Cernigliaro M, Stanca C, Galbiati A, Spinetta M, Coda C, Negroni D, et al. Innovation in Acute Ischemic Stroke Patients over 80 y/o—A Retrospective Monocentric Study on Mechanical Thrombectomy of Consecutive Patients: Is Age an Adequate Selection Criterion? Journal of Clinical Medicine 2023;12:3688. [CrossRef]
- Zabicki B, Limphaibool N, Holstad MJV, Juszkat R. Endovascular management of pancreatitis-related pseudoaneurysms: A review of techniques. PLoS One 2018;13:e0191998. [CrossRef]
- Balderi A, Antonietti A, Ferro L, Peano E, Pedrazzini F, Fonio P, et al. Endovascular treatment of visceral artery aneurysms and pseudoaneurysms: our experience. Radiol Med 2012;117:815–30. [CrossRef]
- Nagaraja R, Govindasamy M, Varma V, Yadav A, Mehta N, Kumaran V, et al. Hepatic artery pseudoaneurysms: a single-center experience. Ann Vasc Surg 2013;27:743–9. [CrossRef]
- Leyon JJ, Littlehales T, Rangarajan B, Hoey ET, Ganeshan A. Endovascular embolization: review of currently available embolization agents. Curr Probl Diagn Radiol 2014;43:35–53. [CrossRef]
- Minici R, Paone S, Talarico M, Zappia L, Abdalla K, Petullà M, et al. Percutaneous treatment of vascular access-site complications: a ten years’ experience in two centres. CVIR Endovasc 2020;3:29. [CrossRef]
- Rappaport AM, Schneiderman JH. The function of the hepatic artery. Rev Physiol Biochem Pharmacol 1976;76:129–75. [CrossRef]
- Li L, Zhang Y, Chen Y, Zhu K-S, Chen D-J, Zeng X-Q, et al. A multicentre retrospective study of transcatheter angiographic embolization in the treatment of delayed haemorrhage after percutaneous nephrolithotomy. Eur Radiol 2015;25:1140–7. [CrossRef]
- Spiliopoulos S, Sabharwal T, Karnabatidis D, Brountzos E, Katsanos K, Krokidis M, et al. Endovascular treatment of visceral aneurysms and pseudoaneurysms: long-term outcomes from a multicenter European study. Cardiovasc Intervent Radiol 2012;35:1315–25. [CrossRef]
- Song H-H, Won Y-D, Kim Y-J. Transcatheter N-butyl cyanoacrylate embolization of pseudoaneurysms. J Vasc Interv Radiol 2010;21:1508–11. [CrossRef]
- Vaidya S, Tozer KR, Chen J. An overview of embolic agents. Semin Intervent Radiol 2008;25:204–15. [CrossRef]
- Loffroy R, Rao P, Ota S, De Lin M, Kwak B-K, Krause D, et al. Packing technique for endovascular coil embolisation of peripheral arterial pseudo-aneurysms with preservation of the parent artery: safety, efficacy and outcomes. Eur J Vasc Endovasc Surg 2010;40:209–15. [CrossRef]
- Kulkarni CB, Moorthy S, Pullara SK, Kannan RR. Endovascular Treatment of Aneurysm of Splenic Artery Arising from Splenomesentric Trunk Using Stent Graft. Korean J Radiol 2013;14:931–4. [CrossRef]
- Künzle S, Glenck M, Puippe G, Schadde E, Mayer D, Pfammatter T. Stent-graft repairs of visceral and renal artery aneurysms are effective and result in long-term patency. J Vasc Interv Radiol 2013;24:989–96. [CrossRef]
- Gong T, Tsauo J, Ding M, Jin L, Duan F, Yu Y, et al. Transcatheter arterial embolization for cancer-related non-variceal upper gastrointestinal bleeding: A multicenter retrospective study of 107 patients. Diagnostic and Interventional Imaging 2023;104:60–6. [CrossRef]
- Sfyroeras GS, Dalainas I, Giannakopoulos TG, Antonopoulos K, Kakisis JD, Liapis CD. Flow-diverting stents for the treatment of arterial aneurysms. J Vasc Surg 2012;56:839–46. [CrossRef]
- Hardman RL, Taussky P, Kim R, O’Hara RG. Post-Transplant Hepatic Artery Pseudoaneurysm Treated with the Pipeline Flow-Diverting Stent. Cardiovasc Intervent Radiol 2015;38:1043–6. [CrossRef]
- Rabuffi P, Bruni A, Antonuccio EGM, Ambrogi C, Vagnarelli S. Treatment of visceral artery aneurysms and pseudoaneurysms with the use of cerebral flow diverting stents: initial experience. CVIR Endovasc 2020;3:48. [CrossRef]
- Venturini M, Piacentino F, Coppola A, Bettoni V, Macchi E, De Marchi G, et al. Visceral Artery Aneurysms Embolization and Other Interventional Options: State of the Art and New Perspectives. J Clin Med 2021;10:2520. [CrossRef]
- Laganà D, Carrafiello G, Mangini M, Dionigi G, Caronno R, Castelli P, et al. Multimodal approach to endovascular treatment of visceral artery aneurysms and pseudoaneurysms. Eur J Radiol 2006;59:104–11. [CrossRef]
- Roberts KJ, McCulloch N, Forde C, Mahon B, Mangat K, Olliff SP, et al. Emergency treatment of haemorrhaging coeliac or mesenteric artery aneurysms and pseudoaneurysms in the era of endovascular management. Eur J Vasc Endovasc Surg 2015;49:382–9. [CrossRef]
- Piacentino F, Fontana F, Curti M, Macchi E, Coppola A, Ossola C, et al. Non-Adhesive Liquid Embolic Agents in Extra-Cranial District: State of the Art and Review of the Literature. J Clin Med 2021;10:4841. [CrossRef]
- López-Martínez L, Molina-Nuevo JD, Pedrosa-Jiménez MJ, Juliá-Mollá E. Spontaneous Haematomas in Anticoagulated Covid-19 Patients: Diagnosis and Treatment by Embolization. Cardiovasc Intervent Radiol 2022;45:1001–6. [CrossRef]
- van Vugt R, Bosscha K, van Munster IP, de Jager CPC, Rutten MJCM. Embolization as treatment of choice for bleeding peptic ulcers in high-risk patients. Dig Surg 2009;26:37–42. [CrossRef]
- Aina R, Oliva VL, Therasse E, Perreault P, Bui BT, Dufresne MP, et al. Arterial embolotherapy for upper gastrointestinal hemorrhage: outcome assessment. J Vasc Interv Radiol 2001;12:195–200. [CrossRef]
- Minici R, Venturini M, Fontana F, Guzzardi G, Pingitore A, Piacentino F, et al. Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study. Medicina 2023;59:710. [CrossRef]
- Tipaldi MA, Orgera G, Krokidis M, Rebonato A, Maiettini D, Vagnarelli S, et al. Trans Arterial Embolization of Non-variceal Upper Gastrointestinal Bleeding: Is the Use of Ethylene-Vinyl Alcohol Copolymer as Safe as Coils? Cardiovasc Intervent Radiol 2018;41:1340–5. [CrossRef]
- Huang Y-S, Chang C-C, Liou J-M, Jaw F-S, Liu K-L. Transcatheter arterial embolization with N-butyl cyanoacrylate for nonvariceal upper gastrointestinal bleeding in hemodynamically unstable patients: results and predictors of clinical outcomes. J Vasc Interv Radiol 2014;25:1850–7. [CrossRef]
- Yonemitsu T, Kawai N, Sato M, Sonomura T, Takasaka I, Nakai M, et al. Comparison of hemostatic durability between N-butyl cyanoacrylate and gelatin sponge particles in transcatheter arterial embolization for acute arterial hemorrhage in a coagulopathic condition in a swine model. Cardiovasc Intervent Radiol 2010;33:1192–7. [CrossRef]
- Minici R, Fontana F, Venturini M, Guzzardi G, Siciliano A, Piacentino F, et al. Transcatheter Arterial Embolization (TAE) in the Management of Bleeding in the COVID-19 Patient. Medicina 2023;59:1062. [CrossRef]
- Abdulmalak G, Chevallier O, Falvo N, Di Marco L, Bertaut A, Moulin B, et al. Safety and efficacy of transcatheter embolization with Glubran®2 cyanoacrylate glue for acute arterial bleeding: a single-center experience with 104 patients. Abdom Radiol (NY) 2018;43:723–33. [CrossRef]
- Yonemitsu T, Kawai N, Sato M, Tanihata H, Takasaka I, Nakai M, et al. Evaluation of transcatheter arterial embolization with gelatin sponge particles, microcoils, and n-butyl cyanoacrylate for acute arterial bleeding in a coagulopathic condition. J Vasc Interv Radiol 2009;20:1176–87. [CrossRef]
- Sapoval M, Vidal V, Déan C, Del Giudice C, Tradi F, Chevallier O, et al. Safety and Efficacy of Peripheral Embolization with EASYX Liquid Embolic Agent: A Multicenter Prospective Study. J Vasc Interv Radiol 2021;32:1136–43. [CrossRef]
- Minici R, Ammendola M, Talarico M, Luposella M, Minici M, Ciranni S, et al. Endovascular recanalization of chronic total occlusions of the native superficial femoral artery after failed femoropopliteal bypass in patients with critical limb ischemia. CVIR Endovasc 2021;4:68. [CrossRef]
- Né R, Chevallier O, Falvo N, Facy O, Berthod P-E, Galland C, et al. Embolization with ethylene vinyl alcohol copolymer (Onyx®) for peripheral hemostatic and non-hemostatic applications: a feasibility and safety study. Quant Imaging Med Surg 2018;8:280–90. [CrossRef]
- Minici R, Serra R, Giurdanella M, Talarico M, Siciliano MA, Carrafiello G, et al. Efficacy and Safety of Distal Radial Access for Transcatheter Arterial Chemoembolization (TACE) of the Liver. Journal of Personalized Medicine 2023;13:640. [CrossRef]
- Kim PH, Tsauo J, Shin JH, Yun S-C. Transcatheter Arterial Embolization of Gastrointestinal Bleeding with N-Butyl Cyanoacrylate: A Systematic Review and Meta-Analysis of Safety and Efficacy. J Vasc Interv Radiol 2017;28:522-531.e5. [CrossRef]
- Minici R, Serra R, Ierardi AM, Petullà M, Bracale UM, Carrafiello G, et al. Thoracic endovascular repair for blunt traumatic thoracic aortic injury: Long-term results. Vascular 2022:17085381221127740. [CrossRef]
- Bracale UM, Peluso A, Panagrosso M, Cecere F, Del Guercio L, Minici R, et al. Ankle-Brachial Index evaluation in totally percutaneous approach vs. femoral artery cutdown for endovascular aortic repair of abdominal aortic aneurysms. Chirurgia 2022;35. [CrossRef]
- Minici R, Serra R, De Rosi N, Ciranni S, Talarico M, Petullà M, et al. Endovascular treatment of femoro-popliteal occlusions with retrograde tibial access after failure of the antegrade approach. Catheter Cardiovasc Interv 2023. [CrossRef]
- Regine R, Palmieri F, De Siero M, Rescigno A, Sica V, Cantarela R, et al. Embolization of traumatic and non-traumatic peripheral vascular lesions with Onyx. Interv Med Appl Sci 2015;7:22–9. [CrossRef]
- Minici R, Serra R, Maglia C, Guzzardi G, Spinetta M, Fontana F, et al. Efficacy and Safety of Axiostat® Hemostatic Dressing in Aiding Manual Compression Closure of the Femoral Arterial Access Site in Patients Undergoing Endovascular Treatments: A Preliminary Clinical Experience in Two Centers. Journal of Personalized Medicine 2023;13:812. [CrossRef]
- Sun CJ, Wang CE, Wang YH, Xie LL, Liu TH, Ren WC. Transcatheter arterial embolization of acute gastrointestinal tumor hemorrhage with Onyx. Indian J Cancer 2015;51 Suppl 2:e56-59. [CrossRef]
- Minici R, Fontana F, Venturini M, Guzzardi G, Piacentino F, Spinetta M, et al. A Multicenter Retrospective Cohort Study Evaluating the Clinical Outcomes of Patients with Coagulopathy Undergoing Transcatheter Arterial Embolization (TAE) for Acute Non-Neurovascular Bleeding. Medicina 2023;59:1333. [CrossRef]
- Minici R, Guzzardi G, Venturini M, Fontana F, Coppola A, Spinetta M, et al. Transcatheter Arterial Embolization (TAE) of Cancer-Related Bleeding. Medicina 2023;59:1323. [CrossRef]
- Khalil A, Parrot A, Fartoukh M, Djibre M, Tassart M, Carette M-F. Pulmonary artery occlusion with ethylene vinyl alcohol copolymer in patients with hemoptysis: initial experience in 12 cases. AJR Am J Roentgenol 2012;198:207–12. [CrossRef]
- Loffroy R, Midulla M, Falvo N, Chevallier O. Ethylene Vinyl Alcohol Copolymer as First Hemostatic Liquid Embolic Agent for Non-variceal Upper Gastrointestinal Bleeding Patients: Pros and Cons. Cardiovasc Intervent Radiol 2018;41:1808–9. [CrossRef]
- Kolber MK, Shukla PA, Kumar A, Silberzweig JE. Ethylene Vinyl Alcohol Copolymer (Onyx) Embolization for Acute Hemorrhage: A Systematic Review of Peripheral Applications. Journal of Vascular and Interventional Radiology 2015;26:809–15. [CrossRef]
- Loffroy R, Favelier S, Genson P-Y, Guiu B. Onyx for embolization of life-threatening hemoptysis: a promising but luxury embolic agent! Cardiovasc Intervent Radiol 2012;35:221; author reply 222. [CrossRef]
- Lv X, Li Y, Jiang C, Wu Z. The Incidence of Trigeminocardiac Reflex in Endovascular Treatment of Dural Arteriovenous Fistula with Onyx. Interv Neuroradiol 2010;16:59–63. [CrossRef]
- Simon SD, Reig AS, Archer KJ, Mericle RA. Biomechanical attributes of microcatheters used in liquid embolization of intracranial aneurysms. Journal of NeuroInterventional Surgery 2012;4:211–4. [CrossRef]
- Pop R, Mertz L, Ilyes A, Mihoc D, Richter JS, Manisor M, et al. Beam hardening artifacts of liquid embolic agents: comparison between Squid and Onyx. Journal of NeuroInterventional Surgery 2019;11:706–9. [CrossRef]
- Larzon T, Mathisen SR. Internal sealing of acute aortic bleeding with a catheter-delivered liquid to solid embolic agent (Onyx). Vascular 2010;18:106–10. [CrossRef]
- Guillon R, Garcier JM, Abergel A, Mofid R, Garcia V, Chahid T, et al. Management of splenic artery aneurysms and false aneurysms with endovascular treatment in 12 patients. Cardiovasc Intervent Radiol 2003;26:256–60. [CrossRef]

Table 1.
Baseline demographic and clinical variables of the sample: descriptive analyses according to ruptured or unruptured status of the pseudoaneurysm.
Table 1.
Baseline demographic and clinical variables of the sample: descriptive analyses according to ruptured or unruptured status of the pseudoaneurysm.
| Variables | All patients (n=38) | |||
|---|---|---|---|---|
| Unruptured VAP (n=21) | Ruptured VAP (n=17) | P value | ||
| Age (years) | 55.7 (±23.9) | 53.7 (±25.5) | 58.2 (±22.3) | 0.547 |
| Sex (M/F) | 11 (28.9%) / 27 (71.1%) | 7 (33.3%) / 14 (66.7%) | 4 (23.5%) / 13 (76.5%) | 0.721 |
| BMI | 25.7 (±4) | 25.8 (±4) | 25.6 (±4.1) | 0.918 |
| eGFR (mL/min) | 71.4 (±22.2) | 75.8 (±19.8) | 66.1 (±24.5) | 0.290 |
| INR | 1.26 (±0.3) | 1.26 (±0.3) | 1.25 (±0.3) | 0.965 |
| aPTT (s) | 40.2 (±5.5) | 40 (±5.5) | 40.5 (±5.4) | 0.768 |
| Platelet count (No. x103/μL) | 341 (±91.8) | 335.4 (±98.2) | 348 (±85.6) | 0.692 |
| Coagulopathy | 9 (23.7%) | 6 (28.6%) | 3 (17.6%) | 0.476 |
| Baseline Hemoglobin (g/dl) | 7.7 (±0.8) | 7.4 (±0.5) | 8 (±1) | 0.093 |
| Antiplatelet therapy | 9 (23.7%) | 5 (23.8%) | 4 (23.5%) | 1 |
| Anticoagulant therapy | 11 (28.9%) | 5 (23.8%) | 6 (35.3%) | 0.491 |
| Hemodynamic instability | 7 (18.4%) | 0 (0%) | 7 (41.2%) | 0.002 |
| Symptomatic Pseudoaneurysm | 24 (63.2%) | 7 (33.3%) | 17 (100%) | <0.001 |
| CT-angiography execution | 37 (97.4%) | 21 (100%) | 16 (94.1%) | 0.447 |
| VAP max diameter (cm) | 3.9 (±1.2) | 4.4 (±1.2) | 3.3 (±0.9) | 0.005 |
Table 2.
Procedure data.
| Variables | All patients (n=38) | |||
|---|---|---|---|---|
| Unruptured VAP (n=21) | Ruptured VAP (n=17) | P value | ||
Etiology
|
16 (42.1%) 9 (23.7%) 12 (31.6%) 1 (2.6%) |
8 (38.1%) 6 (28.6%) 6 (28.6%) 1 (4.8%) |
8 (47.1%) 3 (17.6%) 6 (35.3%) 0 (0%) |
0.660 |
Site of the pseudoaneurysm
|
13 (34.2%) 7 (18.4%) 1 (2.6%) 4 (10.5%) 3 (7.9%) 4 (10.5%) 6 (15.8%) |
7 (33.3%) 4 (19%) 0 (0%) 3 (14.3%) 1 (4.8%) 2 (9.5%) 4 (19%) |
6 (35.3%) 3 (17.6%) 1 (5.9%) 1 (5.9%) 2 (11.8%) 2 (11.8%) 2 (11.8%) |
0.830 |
Endovascular treatment timing
|
14 (36.8%) 24 (63.2%) |
14 (66.7%) 7 (33.3%) |
0 (0%) 17 (100%) |
<0.001 |
|
18 (47.4%) 20 (52.6%) |
11 (52.4%) 10 (47.6%) |
7 (41.2%) 10 (58.8%) |
0.532 |
EVOH viscosity (centiStokes)
|
2 (5.3%) 6 (15.8%) 7 (18.4%) 23 (60.5%) |
1 (4.8%) 4 (19%) 2 (9.5%) 14 (66.7%) |
1 (5.9%) 2 (11.8%) 5 (29.4%) 9 (52.9%) |
0.449 |
| Intraoperative contrast medium (mL) | 33.6 (±12) | 30.9 (±11.9) | 36.9 (±11.6) | 0.100 |
| Volume of contrast to creatinine clearance ratio | 0.58 (±0.54) | 0.45 (±0.29) | 0.74 (±0.73) | 0.064 |
Vascular access site
|
34 (89.5%) 2 (5.3%) 2 (5.3%) |
18 (85.7%) 1 (4.8%) 2 (9.5%) |
16 (94.1%) 1 (5.9%) 0 (0%) |
0.424 |
Sheath diameter
|
7 (18.4%) 27 (71.1%) 4 (10.5%) |
4 (19%) 16 (76.2%) 1 (4.8%) |
3 (17.6%) 11 (64.7%) 3 (17.6%) |
0.435 |
| CT-to-groin time (min) | 143.8 (±179) | 199.2 (±225.9) | 75.3 (±35.6) | 0.150 |
| Procedure time (min) | 39.7 (±10.3) | 41 (±11.6) | 38.1 (±8.5) | 0.444 |
| CT-to-embolization time (min) | 186.4 (±182.4) | 245.9 (±229) | 112.8 (±31.5) | 0.177 |
| Fluoroscopy time (min) | 14.6 (±5.9) | 15.1 (±6) | 14 (±5.8) | 0.744 |
| Cumulative air kerma (mGy) | 218 (±68.2) | 206.3 (±68.1) | 232.3 (±67.6) | 0.246 |
| Dose area product (DAP) (Gy/cm2) | 34.7 (±10.1) | 33.7 (±10) | 35.9 (±10.3) | 0.537 |
Table 3.
Outcomes data.
| Variables | All patients (n=38) | |||
|---|---|---|---|---|
| Unruptured VAP (n=21) | Ruptured VAP (n=17) | P value | ||
| Technical success | 38 (100%) | 21 (100%) | 17 (100%) | 1 |
| Clinical success | 35 (92.1%) | 19 (90.5%) | 16 (94.1%) | 0.679 |
| Rebleeding | 5 (13.2%) | 3 (14.3%) | 2 (11.8%) | 0.819 |
Repeated XA
|
33 (86.8%) 2 (5.3%) 3 (7.9%) |
18 (85.7%) 1 (4.8%) 2 (9.5%) |
15 (88.2%) 1 (5.9%) 1 (5.9%) |
0.911 |
Imaging follow-up modality
|
34 (89.5%) 1 (2.6%) 3 (7.9%) |
18 (85.7%) 0 (0%) 3 (14.3%) |
16 (94.1%) 1 (5.9%) 0 (0%) |
0.154 |
Vascular access site hemostasis
|
19 (50%) 19 (50%) |
11 (52.4%) 10 (47.6%) |
8 (47.1%) 9 (52.9%) |
0.744 |
| Units of packed red blood cells transfused per patient | 1.6 (±2.1) | 0.6 (±0.7) | 2.9 (±2.5) | <0.001 |
| Non-target embolization | 1 (2.6%) | 1 (4.8%) | 0 (0%) | 0.362 |
| Procedure-related complication Rate | 7 (18.4%) | 4 (19%) | 3 (17.6%) | 0.912 |
| End-organ infarction Rate | 4 (10.5%) | 2 (9.5%) | 2 (11.8%) | 0.823 |
| Vascular access-site complication (VASC) Rate | 2 (5.3%) | 1 (4.8%) | 1 (5.9%) | 0.878 |
Procedure-related Complications (SIR classification)
|
31 (81.6%) 7 (18.4%) 0 (0%) |
17 (81%) 4 (19%) 0 (0%) |
14 (82.4%) 3 (17.6%) 0 (0%) |
0.912 |
Procedure-related Complications (CIRSE classification)
|
31 (81.6%) 1 (2.6%) 6 (15.8%) |
17 (81%) 1 (4.8%) 3 (14.3%) |
14 (82.4%) 0 (0%) 3 (17.6%) |
0.644 |
| 30-day bleeding-related mortality | 1 (2.6%) | 1 (4.8%) | 0 (0%) | 0.362 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



