
Submitted:
01 August 2023
Posted:
03 August 2023
You are already at the latest version
Abstract
Lipidomics provides comprehensive study of all lipid components in cells, serum, plasma or tissues of organisms, aiming to the discovery of diagnostic, prognostic and predictive biomarkers of diseases such as malignancies. This systematic review evaluates studies, where lipidomics applies to the diagnosis, prognosis, prediction of ovarian cancer (OC) and the discrimination between malignant and benign ovarian masses. Literature search was conducted in PubMed, Science Direct and SciFinder. Only publications written in English language after 2012 were included. From the reference lists of primary included studies, relevant citations were identified and were also added in our list. All studies included referred to the application of lipidomics in serum/plasma samples of human cases with OC, whereby few of them included also tumor tissue samples. In some of the included studies metabolomic analysis was also involved where other metabolites besides lipids were identified. Qualitative data were assessed and risk of bias was determined using the ROBINS-I tool. In total, 29 studies were included, 15 of which applied non-targeted, 7 targeted lipidomics and 7 were reviews relevant to our aim. Most studies concerned the possible application of lipidomics in OC diagnosis, exhibiting phospholipids and sphingolipids as the most significantly altered during development of the disease. In conclusion, this systematic review highlights the potential contribution of lipids as biomarkers in OC management.
Keywords:
ovarian cancer
; diagnostic
; prognostic
; predictive biomarker
; lipidomics
1. Introduction
OC is one of the most common gynecological cancers, the eighth most common in women worldwide with unfavorable prognosis due to late diagnosis in most cases. While the 5-year overall survival rate when diagnosed early (Stages I/II) is of 92%, it is only about 29% at late stages (III/IV). (1) It is difficult to detect it early because of its non-specific symptoms: Early satiety, bloating, bowel habit changes, weight loss, fatigue and urinary frequency. (2)
Even though serum Cancer Antigen 125 (CA125) is considered the “gold standard” biomarker for OC, it has low sensitivity in early stages (I-II), is elevated only in 26-50% of stage I disease and it has low specificity (sometimes even false positive) during menstruation and conditions, such as fibroids and endometriosis. Another serum biomarker that was found to be over-expressed in 93% of serous and 100% of endometrioid OC cases is HE4 (human epididymis protein 4) but, even if its specificity compared to CA125 is higher, several factors such as age, smoking and use of hormonal contraceptives provoke great variations in its levels. (3)
To date, it is well known that lipids play a critical role in proliferation, survival, death and interactions between cells due to their involvement in cell membranes, cellular signaling, cellular interactions and energy storage. Since these processes are also related to transformation, progression and metastasis of cancer, probably several lipids are mediators in oncogenic processes and could be potential cancer biomarkers. (4)
Lipidomics, first employed in 2003 (5), is a subdiscipline of metabolomics, where investigation of quantitative and qualitative profile of lipid components in biofluids, tissues, cells and organisms takes place (6). It is a rapidly evolving scientific field due to technological advances and it seems that among others it could contribute to tumor characterization, detection and classification of cancerous cells and tissues as well as differentiation between normal and neoplasmic environment. Thus, integration of lipidomics in cancer research could be applied to the discovery of new biomarkers, contributing to diagnosis, prognosis and prediction of several malignancies (4)
In the last decade, studies regarding the application of lipidomics in OC management are emerging. To date, there is no systematic review published exploring the contribution of lipidomics in OC. The systematic review by Salim et al (2020) evaluated the contribution of metabolomics in OC, where some lipids were also identified together with other small molecules. (7) For this reason, the aim of this systematic review is to evaluate literature regarding the possible application of lipidomics in diagnosis, prognosis, prediction of OC and discrimination between malignant and benign ovarian tumors.
2. Methods
2.1. Eligibility criteria
In order to focus on the applicability of lipidomics in OC management, we have included only human studies in our systematic review. Particularly, studies that deemed eligible for the review, were focused on lipidomic analyses of blood, in particular serum or plasma from pre-surgery cases, while those involved only tissues or cell lines samples were excluded. In order to investigate the most recent scientific achievements on this topic, studies curried out the last decade were included. Publications not written in English were deemed ineligible. Our review focused on non-targeted lipidomics. A supplementary analysis, consisting of 7 targeted lipidomics studies in OC, was included to confirm consistency of untargeted lipidomics.
2.2. Search strategies
Systematic search followed PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses). (8) Bibliographic search was conducted on PubMed, Science Direct and SciFinder between January 2021 and 2023. Augmentation of our search consisted of references cited in primary sources. (Figure 1) Keywords used in our research were “ovarian cancer”, “diagnostic/prognostic/predictive biomarker” and “lipidomics”. Two authors worked independently on bibliographic search. After the search of first author (VT), based on inclusion and exclusion criteria, a total of 32 studies were collected and screened. The whole process was repeated independently by a second author (OB). Communication for obtaining or confirmation of data from study authors was not conducted. The screening process is summarized in the flow diagram (Figure 1). Collection of relevant data from primary reports was conducted by the first reviewer (VT), cross-checked by the second (OB) and the whole screening process was cross-checked by 2 senior authors (ET, EG). Information and data collected included year of publication, author details, country and aim of the study, kind and size of sample, analytical methodology and technique used, findings and conclusions. The main characteristics of included non-targeted and targeted studies are summarized in Table 1 and Table 2 respectively.
2.3. Study Risk of Bias Assessment
ROBINS-I tool (Risk Of Bias In Non-randomized Studies of Interventions) (9) was used for the assessment of methodological quality of all studies, except relevant reviews. The two co-authors worked independently during this process. Each study was assigned as “low”, “moderate”, “serious”, “critical” risk of bias or “no information”. Results from methodological assessment are summarized in Table 3 and Table 4 for untargeted and targeted lipidomics respectively. In order to assess the consistency of results from untargeted lipidomic studies we conducted a supplementary analysis of 7 targeted lipidomic studies, using the ROBINS-I tool, results of which are summarized in Table 4.
2.4. Synthesis of the results
Table 1 and Table 2 display all pooled data of the studies included in our systematic review, 15 non-targeted and 7 targeted lipidomic studies.

Table 1.
Pooled data from non-targeted lipidomic studies.
| Author, Date, Country | Sample & Method | Aim of study | Study findings | Conclusions |
|---|---|---|---|---|
| Iurova et al (2022) Russia (10) | CC Total (n=41) HGSC (n=28): Stage I-II (n=5) Stage III-IV (n=23) HC (n=13) Pre-operative plasma samples HPLC-QTOF-MS |
D | Decreased plasma concentration of Plasmanyl-LPC(O-16:0), Plasmenyl-PE(P-18:0/18:2,18:0/20:3,18:0/20:4, 18:1/22:6), Plasmenyl-PC(P-16:1/18:0), LPC(14:0,17:0,18:2), PS(37:5), SM(d20:0/18:4) and CerNS(d18:1/24:0) in patients with early OC. | Lipid profiling by HPLC-MS can improve identification of early-stage OC and thus increase the efficiency of treatment |
| Salminen et al (2021) Germany, Finland (11) | CC Total (n=711) Turku (Finland): Malignant (n=197) Benign (n=114) Charite 1 (Germany): Malignant (n=51) Charite 2 (Germany): Malignant (n=104) Charite 3 (Germany): Malignant (n=147) Benign (n=98) Pre-treatment serum samples LC-QTRAP |
P | A two-lipid signature, based on the ratio of the ceramide Cer(d18:1/18:0) and the phosphatidylcholine PC-O(38:4) identified especially poor-outcome patients at the time of diagnosis, before any oncological treatment |
The two-lipid signature was able to identify EOC patients with an especially poor prognosis at the time of diagnosis, showing promise for the detection of disease relapse. |
| Wang et al (2021) China (12) | CC Total (n=340) Discovery set (n=153) EOC (n=62): Early (n=25)/Advanced (n=37) BOT (n=41) HC (n=50) Validation set (n=187): EOC (n=47) BOT (n=29) HC (n=39) Else (n=72) Serum samples UPLC-QTOF-MS |
D | Compared to HC, levels of FAs, LPCs and LPEs were significantly increased, while PCs, PC-Os, PE-Os, SMs and PIs were decreased in BOT and EOC. All of SFAs, MUFAs and PUFAs in BOT and EOC presented a considerable increase simultaneously. PC-O 36:2 (FA18:2), PC-O 38:3 (FA20:3), PC-O 38:4 (FA20:4), PE (16:0p 18:1) and PE (18:0p 22:5) presented lower levels in EEOC vs AEOC. Levels of TGs were remarkably decreased in BOT, compared with HC. Levels of Cers and FAs increased, and levels of PCs, PC-Os and PE-Os decreased in EOC, compared with HC. Cers, DGs, PCs, PEs, and TGs presented high level in EOC, while PC-Os and PE-Os presented low level in EOC, compared to BOT. Cer(d18:1/16:0), PC-O(36:2), PE(16:0p_18:1), OAHFA(18:2_24:6) were selected as the combinational diagnostic marker. |
This study provided evidence for the mechanistic understanding of OC at the level of lipid metabolism. The defined potential combinational marker would be helpful for aiding EOC diagnosis, especially for early stage EOC. |
| Buas et al (2021) USA (13) | CC Total (n=218) 1st cohort (FH) (n=100) OC (n=50) BOT (n=50) 2nd cohort (RP) (n=118) OC (n=60) BOT (n=58) Pre-operative Plasma samples Ascites samples (n=15) Direct infusion MS |
D | In both cohorts, reductions in TAG, PC, CE species, DAG, PE, LPC, LPE and SM species were observed in patients vs controls, while CER(18:0) was elevated. Differentially abundant lipid species in Early stage (I/II): TAG, DAG, PC, PE Late stage (III/IV): TAG, CE, PC, PE, LPC, LPE, SM, CER. PE, LPC, LPE exhibited significant reductions in cases vs controls. In stage-stratified analyses, certain significant class-level differences were detected only in late-stage (LPC, LPE, SM), only in early-stage (DAG, TAG) or in both subgroups (PC, PE). Results suggest that combining CA125 with specific individual lipid metabolites, such as DAG(16:1/18:1), may provide a substantial boost to specificity at 90% sensitivity, relative to CA125 alone, in separating early-stage ovarian malignancies from benign adnexal masses. Certain metabolites may exhibit changes in circulation years before an OC diagnosis: PCs (34:2, 38:3), PEs (36:3, 38:5), TAGs (46:0, 52:4/5, 54:4/5/6/7, 56:4/5/7/8), and SM 22:1 |
Potential translational utility of specific circulating lipid metabolites to aid in the clinical diagnosis and triage of women with adnexal mass. |
| Niemi et al (2018) Germany, Finland (14) | CC Total (n=604) Malignant (n=290): Charite (n=62) Finland (n=76) Charite discovery (n=152) Borderline (n=25): Charite (n=18) Finland (n=7) Benign (n=289): Charite (n=109) Finland (n=82) Charite discovery (n=98) Pre-operative serum/plasma samples Non-targeted & Targeted lipidomics UPLC-QTRAP |
D | Patients showed a consistent decrease in the concentration of most of phospholipids (PCs, LPCs, PIs), cholesteryl esters, glucosyl/galactosyl Cers, and sphingomyelins. Cers with 18:0, 20:0 and 24:1 FAs were increased, while 24:0 FA-containing Cers were decreased. TAGs with shorter FA side chains were decreased, whereas those with longer FA side chains were increased. Twenty-one of 23 lipids analyzed were decreased in all histological subtypes, and only Cer(d18:1/18:0) and TAG (18:1/18:1/20:4) were increased. It appears that borderline tumors do not cause as much of a change to the lipidome as malignant tumors. Lipids improved diagnostic value of CA125 for the detection of stage I/II |
Changes in lipid metabolism due to OC occur in early-stage disease but intensify with increasing stage. Understanding lipid metabolism in OC may lead to new therapeutic and diagnostic alternatives |
| Braicu et al (2017) Germany (15) | CC Total (n=245) Pre-operative serum samples: HGSC (n=147) Controls (n=98) Pre-operative tissue samples: HGSC (n=140) LC-QTOF-MS |
D, P | OC patients exhibit decreased serum levels of PCs, PEs, PIs, CEs, DAGs, SMs, cerebrosides (Glc/GalCers), LacCers, Gb3s, S1Ps. Cers, with 16:0, 18:0, 20:0 and 24:1 FAs were increased, while those containing 23:0 and 24:0 FAs were decreased. TAGs with short FA side chain were decreased, while long chain TAGs were the same or increased compared to controls. The predictive value of diagnosis was improved by the combination of CA125 with PEO-36:1. Lipids belonging to the CE, SM, LPC, PC, PC O and PE O lipid classes were decreased in all OC patients and progressed to lower levels especially in patients where the whole macroscopic tumor could not be removed during the surgery. Ceramides elevated in cancer patients continued to increase during disease progression. Cer(d18:1/16:0) showed significant hazard ratio both in overall and progression-free survival analyses. |
Alterations in lipid metabolism in OC could contribute to diagnosis and prognosis of the disease |
| Xie et al (2017) China (16) | Prospective study Median follow-up (37,5months) Total (n=98) Dead in 3 years (n=46) Survived after 3 years (n=52) Pretreatment plasma samples UPLC-QTOF-MS |
Pr | Poor survival with the increase of Kynurenine, Acetylcarnitine and PC(42:11) and with the decrease of LPE(22:0/0:0). The 4 potential predictive biomarkers were significantly altered in short-term mortality compared to long-term survival patients (P<0.05). PC (42:11) and LPE(22:0/0:0) were significantly altered in short-term mortality and medium survival. Patients with long-term survival showed increased plasma relative intensity of LPE (20:0/0:0) and decreased relative intensity of PC(42:11) | Plasma metabolites could be utilized to predict the overall survival and discriminate the short-term mortality and long-term survival for EOC patients |
| Li et al (2017) China (17) | Prospective study Total (n=70) EOC recurrent (n=39): ER (n=12) LR (n=27) Non recurrent (n=31): Pre-operative plasma samples UPLC-QTOF-MS |
Pr | Most of the identified lipids in EOC recurrent patients were decreased compared with the non-recurrent ones, except up-regulated PC(31:2) and PE-P(42:4). LysoPG(20:5), as a potential biomarker, could provide an AUC value of 0.736, significantly increasing the predictive power of clinical characteristics from AUC value 0.739 to 0.875. Decreased LysoPG(20:5) level was identified as the most important prognostic feature. LysoPCs were down-regulated in recurrent EOC patients compared with the non- recurrent patients. A series of PCs were down-regulated in EOC recurrent patients. Cer(d18:1/23:0), SM(d18:1/14:0), SM(d18:2/14:0) were decreased in EOC recurrent patients. PIs levels were lower in patients with recurrent EOC than in those without recurrent EOC. Decreased levels of TGs: a specific metabolic feature for early relapse. |
Plasma lipidomics study could be used for predicting EOC recurrences, as well as early and late recurrent cases. The lipid biomarker research improves the predictive power of clinical predictors, and the identified biomarkers are of great prognostic and therapeutic potential |
| Buas et al (2016) USA (18) | CC Total (n=100) Serous OC (n=50) Serous BOT (n=50) Plasma samples at the time of surgery Non-targeted & Targeted lipidomics LC-QTOF-MS |
Discr | Glycerolipids and glycerophospholipids, were found to be decreased in abundance in cases relative to controls |
Alterations in circulating plasma lipid metabolites are associated with the presence of malignant ovarian carcinoma versus benign ovarian tumor. |
| Ke et al (2016) China (19) | CC Total (n=105) Primary EOC (n=35) The same Post-operative EOC (n=35) Relapsed EOC (n=35) Controls (n=35) Plasma samples UPLC-QTOF-MS |
P,Pr | Compared with controls, significantly lower concentrations of tetracosahexaenoic acid, 2-octenoic acid, 12,13-DiHODE and 19,20-DiHDPA were observed in primary EOC. Post-operative EOC patients had increased fatty acids and decreased LPCs. Significantly increased levels of LPCs, LPEs and fatty acids were seen in EOC recurrent patients. |
There are delineated metabolic changes in response to advanced EOC, surgery and recurrence, and identified biomarkers that could facilitate both understanding and monitoring of EOC development and progression |
| Y.Zhang et al (2016) China (20) | CC Total (n=65) OC (n=27) BOT (n=27) HC (n=11) Plasma samples UPLC-QTOF-MS |
D | LPCs were up-regulated and PCs and TGs were down-regulated in OC patients compared to Benign and Healthy controls. (Potential biomarkers: 16:0 LPC, 18:1 LPC, 20:3 LPC, 20:4 LPC, 22:6 LPC, 16:0/18:1 PC, 16:0/18:2 PC, 18:0/18:2 PC, 18:0/20:5 PC, 18:2/18:2 PC, 18:2/18:2/16:0 TG) |
MS-based lipidomics is a powerful method in discovering new potential clinical biomarkers for diseases. |
| Hou et al (2016) China (21) | CCTotal (n=215) EOC (n=139) BOT (n=38) UF (n=38) Pre-operative plasma samples UPLC-QTOF-MS |
D,Pr | All the GPs were decreased in EOC patients vs controls, except PC(33:5) and PC(34:3). SPs were remarkably increased in EOC patients, except SM(d18:2/14:0). Two types of glycerolipids showed the opposite trend in EOC patients: MG were significantly increased, whereas DG were significantly decreased in EOC patients vs BOT/UF. All the PCs and pPEs were negatively associated with pathological stage, except PC(33:5), and SMs and Cers were positively associated with pathological stages, except SM(d18:2/14:0). MG was positively associated, whereas DG was negatively associated with pathological staging. PC(P-38:4), PC(35:5), PC(34:3), SM(d18:1/17:0) and SM(d18:0/16:1) together with CA125 improved the diagnostic and predictive accuracy of CA125. |
Plasma lipid profiles analyzed by UPLC- QTOF/MS could be used to discriminate EOC from controls. Promising lipid metabolites together with CA125 improved the diagnostic and predictive performance and accuracy of EOC. |
| Gaul et al (2015) USA (22) | CC Total (n=95) EOC (I/II) (n=46) HC (n=49) Serum samples Non-targeted & targeted lipidomics UPLC-HRMS |
D | 16 metabolites were found to have optimal accuracy in distinguishing between early-stage EOC and controls when used in a linear support vector machine model, most of which were lipids and fatty acids, including lysophospholipids: LPE and LPI |
The results provide the foundation of clinically significant diagnostic tests and evidence for the importance of alterations in lipid and fatty acid metabolism in the onset and progression of the disease. |
| Zhang et al (2015) China (23) | Prospective study Total (n=38) EOC (III/IV) (n=38): With recurrence (n=26) Without recurrence (n=12) Pre-treatment plasma samples UPLC-QTOF-MS |
P/Pr | Metabolites identified as potential metabolic biomarkers of EOC recurrence: L-tryptophan(AUC=0.80), LysoPC(14:0)(AUC=0.77) and LysoPE(18:2)(AUC=0.82) decreased in EOC patients with recurrence, whereas kynurenine(AUC=0.79) and bilirubin(AUC=0.76) increased. Patients with and without recurrent EOC could be distinguished using this panel of metabolites (AUC = 0.91). |
Remarkably, combining of these five biomarkers provided an AUC value of 0.91, which suggests strong potential for predicting EOC recurrence. |
| T. Zhang et al (2012) China (24) | CC Total (n=170) Training samples: EOC (n=50): BOT (n=50) External validation samples: EOC (n=30) BOT (n=40) Pre-operative plasma samples UPLC-QTOF-MS |
Discr | The plasma L-Tryptophan, LysoPC(18:3), LysoPC(14:0), and 2-Piperidinone concentrations were lower among EOC patients than those among BOT patients, either in the training set or in the external validation set |
UPLC-QTOF/MS based metabolomic platform possessed a favorable value in discriminating malignant from benign ovarian tumors. |
CC=Case-Control, HGSC=High Grade Serous Carcinoma, HC=Healthy Controls, HPLC-MS=High Performance Liquid Chromatography Mass Spectrometry, D=Diagnosis, LPC=Lyso-phosphatidyl-choline, PE=Phosphatidyl-ethanolamine, PC=Phosphatidyl-choline, SM=Sphingomyelin, CER=Ceramide, P=Prognosis, EOC=Epithelial Ovarian Cancer, BOT=Benign Ovarian Tumour, FAs=Fatty Acids, PI=Phosphatidyl-inositol, SFAs=Saturated Fatty Acids, MUFAs=Mono-unsaturated Fatty Acids, PUFAs=Poly-unsaturated Fatty Acids, EEOC=Early EOC, AEOC=Advanced EOC, TG=Triacyl-glycerol, DG=Diacyl-glycerol, OAHFA=(O-acyl)-ω-hydroxy fatty acid , LPE=Lyso-phosphatidyl-ethanolamine, ER=Early Recurrent, LR=Late Recurrent, Discr=Discrimination, Pr=Prediction, UF=Uterine Fibroid.
Table 2.
Pooled data from targeted lipidomic studies.
| Author, Date, Country | Sample & Method | Aim of study | Study findings | Conclusions |
|---|---|---|---|---|
| Hishinuma et al (2021) Japan (25) | CC Total (n=160) EOC (n=80) HC (n=80) Plasma samplesUHPLC-MS/MS |
D, Pr | Decreased concentrations of LPCs and PCs and increased concentrations of TGs were observed in EOC patients compared to HCs | Plasma metabolome analysis is useful not only for the diagnosis of EOC, but also for predicting prognosis. |
| Yagi et al (2020) USA (26) | CC Total (n=62) OC (n=20) BOT (n=20) HC (n=22) Plasma samples HPLC-MS |
D | LPE (22:6)/LPE (o-16:0) has the best sensitivity in distinguishing between control and benign, SM (d18:1/24:1)/SM (d18:1/22:0) has the best sensitivity between control and cancer, and PE (16:0/18:1)/PE (o-18:0/18:2) has the best specificity in distinguishing between benign and cancer. |
Potential of plasma phospholipids as a novel marker of OC with great sensitivity and specificity by utilizing the unique characteristics of phospholipids to further enhance the diagnostic power. |
| Zeleznik et al (2020) USA (27) | Nested CC Total (n=504) Mean follow-up (n=12,3years) Cases (n=252) Serous/PD tumors (n=176) Endometrioid/CC (n=34) Rapidly fatal tumors (n=86) Controls (n=252) Pre-diagnosis plasma samples LC-MS/MS |
A | The top three metabolites associated with risk were pseudouridine, C18:0 sphingomyelin (SM) and 4-acetamidobutanoate. Differential association by acyl carbon number and double bond content of TAGs with risk of OC overall was observed. Specifically, TAGs with higher number of acyl carbon atoms and double bonds were associated with increased risk, while TAGs with lower number of acyl carbon atoms and double bonds were associated with decreased risk. Fifty-three lipid-related metabolites (26TAGs, 7PCs, 6LPEs, 3PEs, 3LPC, 4DAGs, 2LPSs, and 2PSs) showed differences by tumor aggressiveness. |
This study suggests that TAGs may be important as a novel risk biomarker for OC, particularly for rapidly fatal tumors, with associations differing by structural features. |
| Plewa et al (2019) Poland (28) | CC Total (n=76) OC (n=26) BOT (n=25) HC (n=25) Serum samplesHPLC-TQ/MS |
D | Decreased serum levels of LPC a C16:1, PC aa C32:2, PC aa C34:4 and PC aa C 36:6 in OC patients compared to BOT and HCs | There is dominant role of lipid alterations in OC. |
| Kozar et al (2018) Slovenia (29) | CC Total (n=57) EOC (n=15) BOT (n=21) HC (n=21) Pre-treatment serum samplesHPLC-TQ/MS |
D | Five most significant markers were Cer 34:1;2 (C16), Cer 40:1;2 (C22), Cer 42:1;2 (C24), SM 36:0;2 and SM 36:1;2 (C18 and C18:1). Important increase in levels of C16-Ceramide, long chain Ceramides C22/C24 and in C18 and C18:1 Sphingomyelin levels in EOC vs Controls were observed |
Long chain ceramides and sphingomyelins may serve as a novel biomarker for EOC detection and may also offer insight into the role of sphingolipid metabolism in cell proliferation. |
| Knapp et al (2017) Poland (30) | CC Total (n=155) AOC (n=74) HC (n=81) Pre-operative Plasma samples LC-MS/MS Post-surgery Tissue samples UHPLC/MS/MS |
Pr | Significant increase (higher risk of OC) in C16-Cer (>311.88 ng/100 μl), C18:1-Cer (>4.75 ng/100 μl) and C18-Cer (>100.76 ng/100 μl) was noticed in plasma of AOC patients vs controls. Increase in C16-Cer, C18:1-Cer, C18-Cer, C24:1-Cer, C24-Cer and S1P was noticed in ovarian tissue of AOC women compared to controls. |
Some sphingolipids can be used as potential biomarkers of advanced ovarian cancer and they can play an important role in the pathogenesis of this disease. |
| Shan et al (2012) USA (31) | CC Total (n=423) EOC (n=211): Stage I/II (n=78) Stage III/IV (n=133) BOT (n=212) Pre-operative serum samplesLC-ESI-MS/MS |
D | The additional measurement of LPA, PPE, LPC (14:0, 12:0) supplements results of CA125 measurement and improves diagnostic accuracy. Measurement of phospholipids improved the identification of early-stage cases from 65% (based on CA125) to 82%, and for mucinous cases from 44% to 88%. |
Measurement of specific biologically active phospholipids improves diagnostic sensitivity and accuracy among women with suspected ovarian cancer |
PD tumors= Poorly Differentiated tumors, A=Agnostic, AOC=Advanced Ovarian Cancer.
Table 3.
Risk of bias assessment in non-targeted lipidomic studies.
| Study ID | Study Type | Pre-Intervention | At-Intervention | Post-Intervention | Total Score | ||||
|---|---|---|---|---|---|---|---|---|---|
| Confounding Bias | Selection Bias | Classification Bias | Deviation Bias | Missing Data Bias | Measurement of outcome Bias | Selective reporting Bias | Overall risk of bias judgement | ||
| Iurova et al (2022) Russia (10) | CC | S | M | L | L | L | L | L | S |
| Salminen et al (2021) Germany, Finland (11) | CC | M | M | L | L | L | M | L | M |
| Wang et al (2021) China (12) | CC | S | L | L | L | L | L | L | S |
| Buas et al (2021) USA (13) | CC | M | L | L | L | L | L | L | M |
| Niemi et al (2018) Germany, Finland (14) | CC | M | M | L | L | L | L | L | M |
| Braicu et al (2017) Germany (15) | CC | M | L | L | L | L | L | L | M |
| Xie et al (2017) China (16) | PS | M | L | L | L | L | L | L | M |
| Li et al (2017) China (17) | CC | M | L | L | L | L | L | L | M |
| Buas et al (2016) USA (18) | CC | M | M | L | L | L | L | L | M |
| Ke et al (2016) China (19) | CC | M | M | L | L | L | L | L | M |
| Y. Zhang et al (2015) China (20) | CC | S | M | L | L | L | M | L | S |
| Hou et al (2015) China (21) | CC | M | L | L | L | L | M | L | M |
| Gaul et al (2015) USA (22) | CC | S | M | L | L | L | M | L | S |
| H. Zhang et al (2014) China (23) | PS | M | L | L | L | L | L | L | M |
| T. Zhang et al (2012) China (24) | CC | M | L | L | L | L | M | L | M |
CC=Case-Control, PS=Prospective Study, M=Moderate, L=Low, S=Serious.
Table 4.
Risk of bias assessment in targeted lipidomic studies.
| Study ID | Study Type | Pre-Intervention | At-Intervention | Post-Intervention | Total Score | ||||
|---|---|---|---|---|---|---|---|---|---|
| Confounding Bias | Selection Bias | Classification Bias | Deviation Bias | Missing Data Bias | Measurement of outcome Bias | Selective reporting Bias | Overall risk of bias judgement | ||
| Hishinuma et al (2021) Japan (25) | CC | M | L | L | L | L | L | L | M |
| Yagi et al (2020) USA (26) | CC | S | L | L | L | L | S | L | S |
| Zeleznik et al (2020) USA (27) | CC | M | M | M | L | L | L | L | M |
| Plewa et al (2019) Poland (28) | CC | M | L | L | L | M | L | L | M |
| Kozar et al (2018) Slovenia (29) | CC | M | L | L | L | L | M | M | M |
| Knapp et al (2018) Poland (30) | CC | M | L | L | L | L | L | L | M |
| Shan et al (2012) USA (31) | CC | M | L | L | L | L | M | L | M |
3. Results
3.1. Study selection and characteristics
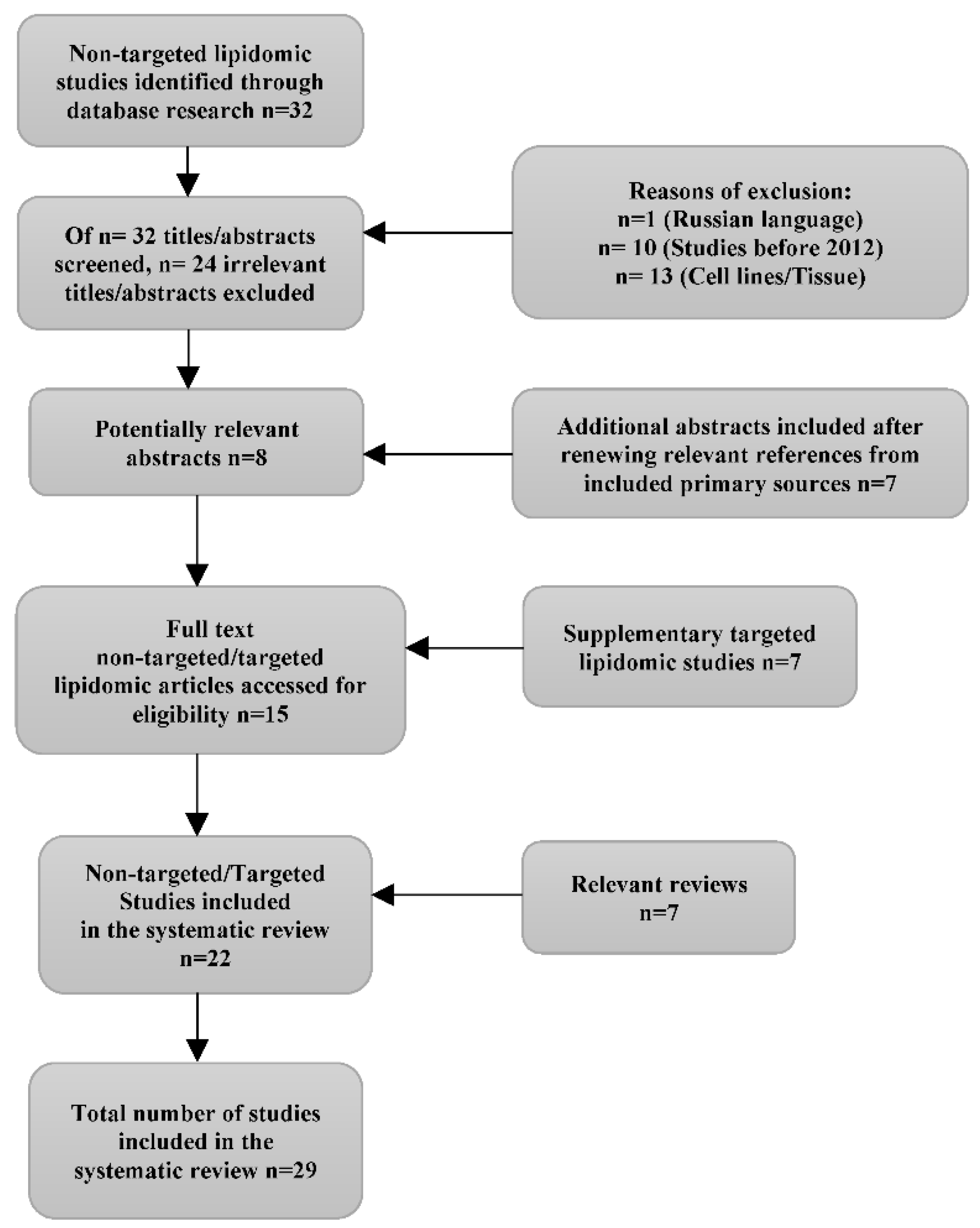
Our initial search consisted of 32 papers regarding untargeted lipidomics in OC, of which 24 were excluded due to Russian language (n=1), published before 2012 (n=10) and cell lines/tissue samples (n=13). Included studies were all relevant to lipidomic analysis of serum/plasma. Additional, 7 abstracts were included for evaluation, after careful search of primary sources citations. A supplementary analysis, consisted of 7 targeted lipidomic analyses in OC, was included in our review to enhance the validity of untargeted lipidomic analyses. Useful information from 7 relevant to our aim reviews were included for confirmation of our results. The whole screening process can be found in Figure 1.
In total, 22 studies of untargeted lipidomics (n=15) and targeted lipidomics (n=7) were included in our review consisting of 4.552 participants, 2.504 diagnosed with ovarian cancer and 2.048 serving as controls (Benign ovarian tumor/healthy controls). Ranging from 38 to 711, median sample size was 206. Most studies were conducted in China (n=8), followed by the USA (n=6). The other studies were conducted in Germany (n=3), Finland (n=2), Poland (n=2), Slovenia (n=1), Russia (n=1) and Japan (n=1). The reviews included in our study were conducted in the USA (n=3), Australia (n=2), Italy (n=1) and 1 was a cooperation of the following countries: China, USA, Austria, Poland, Finland, UK, France, Canada, Germany, Slovenia and Korea.
3.2. Risk of Bias in studies
As reflected by outcomes of ROBINS I tool assessment, the majority of included retrospective studies was open to several sources of bias since 4 out of 15 untargeted (Table 3) and 1 out of 7 targeted lipidomic studies (Table 4) were classified as being at serious risk of bias (10,12,20,22,26).
Studies of Iurova et al (10), Niemi et al (14), Hou et al (21), Zhang H. et al (23), Zhang T. et al (24) and Kozar et al (29) excluded comorbidities from their participants, such as liver, kidney and metabolic diseases and medication, attempting to reduce selection bias, while in the other studies comorbidities were not excluded or were not at all mentioned.
Any significant difference in the level of lipids between patients with OC and controls should be carefully evaluated as it is almost impossible for a non-randomized, observational study to eliminate all types of bias.
It should be noted that the small sample size in some studies conducted in Russia [Iurova et al (10)], Slovenia [Kozar et al (29)] and Poland [Plewa et al (28)] can be explained by the low prevalence of ovarian cancer in these populations. However, the smaller the sample size of a study, the lower the power of it and the smaller the size of the effect evaluated, such as differences in the level of several lipids in serum/plasma between OC patients and controls, the larger the sample size required. From the 22 studies included in our review, 9 had sample size less than 100, but even in those with more than 100 participants it is possible that they were not adequately powered, since the lack of pilot data that could guide the right choice of sample size. The largest sample size was that included in the study of Salminen et al (11), where in total 711 participants (n=499 OC patients and n=212 BOT) from 4 cohorts took part in the experimental measurements.
In “omics” evaluations, such as metabolomics and lipidomics, it is common to observe the introduction of false discovery, due to multiple scenarios being tested and the comparison of several lipids in two or more groups (OC patients, BOT and healthy controls in our review). Therefore, it is important that studies included the false discovery rate (FDR) (32). In our review, studies that used FDR were those of Wang et al (12), Buas et al (13,18), Zeleznik et al (27), Ke et al (19), Hou et al (21) and Plewa et al (28).
Studies of Wang et al (12), Buas et al (13,18), Niemi et al (14) and Zhang T. et al (24) included a discovery cohort in order to evaluate lipid differences and predictive models, this way decreasing selection bias. All other included studies cross-validated predictive models from the same cohort.
The basic target of studies included in our review was significant differences in lipidomic profile between OC patients and controls (BOT and/or healthy controls). Most studies used unsupervised principal component analysis (PCA), which is capable to reveal separation of data between groups. By this approach potential bias can be revealed (33).
Most of our studies used ultra-performance liquid chromatography-mass spectrometry (UPLC-MS) technique either for acquiring a comprehensive lipidomic profile of patients and controls’ serum/plasma or for targeting specific predefined lipids. Results could be affected by various parameters, such as type of specimen (serum or plasma), analytical protocol applied and instrumentation used for analysis, processing software and spectral libraries used for identification and statistical analysis. However, this limitation cannot be avoided in “omics” studies as harmonization in workflows is not yet put in place.
3.3. Results of syntheses
3.3.1. Diagnosis
In total, 13 out of 22 studies included in this review demonstrated the application of lipidomics in the diagnosis of OC. Eight of them concerned non-targeted lipidomics (10,12–15,20–22) and the other 5 were targeted studies (25,26,28,29,31). Data, findings and conclusions of these studies can be found in Table 1 and Table 2 for untargeted and targeted lipidomics respectively. Lipids, identified to have significantly different levels in serum/plasma between OC patients and BOT or healthy controls are summarized in Table 5 and Table 6 for untargeted and targeted lipidomic analyses. Particularly, in non-targeted lipidomic studies, up-regulation of ceramides (Cers) with 18:0, 20:0 and 24:1 fatty acyls (FAs) and triacylglycerols (TAGs) with longer FA side chains in OC patients was reported (12–15) which was also confirmed by targeted analyses (29) while down-regulation of phosphatidylcholine (PC) (12,13,15,20), sphingomyelin (SM) (10,12–15) and diacylglycerols (DGs) (13,15,21) was noted. Cers, containing 23:0 and 24:0 FAs and TAGs with short FA side chain were reported as downregulated in OC patients (14,15). In targeted lipidomic studies downregulation of lysophosphatidylcholine (LPC) was reported in EOC patients versus controls (25,28,31).
3.3.2. Prognosis
Four untargeted lipidomic studies in our review applied to prognosis of OC (11,15,19,23). Data, findings and conclusions of these studies can be found in Table 1 and lipids, identified altered in patients compared to controls, in Table 5. Analysis of Zhang H et al (23) demonstrated that LysoPC(14:0) and LysoPE(18:2) decreased in EOC patients with recurrence compared to non-recurrent, while Salminen et al (11) and Braicu et al (15) agree that upregulation of Cers could be useful in predicting OC prognosis. Moreover, Ke et al (19) reported that LPCs and LPEs were upregulated in EOC recurrent patients.
3.3.3. Prediction
From a total of 22 studies, included in this review, 5 untargeted and 2 targeted lipidomic/metabolomic analyses applied to the prediction of OC (16,17,19,21,23,25,30). Data, findings and conclusions of these studies can be found in Table 1 and Table 2 for non-targeted and targeted studies respectively and lipids, identified to be altered in patients versus controls, in Table 5 and Table 6. In untargeted analyses, Li et al (17) and H. Zhang et al (23) reported that specific LysoPC and LysoPE species decreased in EOC patients with recurrence compared to non-recurrent, while Ke et al (19) reported that some others were elevated. Furthermore, Xie et al (16) demonstrated that plasma relative intensity of LPE (20:0/0:0) was upregulated in patients with long-term survival, while relative intensity of PC (42:11) in patients with long-term survival was downregulated. Hou et al (21) and the targeted analysis of Hishinuma et al (25) reported upregulation of glycerophospholipids as a potential predictive biomarker for OC, whereas Knapp et al (30) suggested upregulation of several Cers for further investigation as biomarker for the prediction of the disease.
3.3.4. Discrimination between OC and BOT
Two untargeted lipidomic studies referred to the contribution of “omics” to discrimination between malignant and benign ovarian tumors (18,24). Data, findings and conclusions of these studies can be found in Table 1 and lipids, altered in OC versus BOT, in Table 5. Buas et al (18) reported glycerolipids and glycerophospholipids downregulated in cases versus controls to be further investigated for their possible application in discrimination between OC and BOT, while T. Zhang et al (24) refer to decreased LysoPC(18:3) and LysoPC(14:0) levels in EOC patients compared to BOT patients. Finally, Zeleznik et al (27) conducted a prospective untargeted/targeted analysis of circulating plasma metabolites (lipids included) in order to find potential correlation with OC risk. Specifically, TAGs with higher number of acyl carbon atoms and double bonds were associated with increased risk, while TAGs with lower number of acyl carbon atoms and double bonds were associated with decreased risk. Fifty-three lipid-related metabolites (26TAGs, 7PCs, 6LPEs, 3PEs, 3LPC, 4DAGs, 2LPSs, and 2PSs) showed differences by tumor aggressiveness. Data regarding this study can be found in Table 2.
Table 5.
Up/Down-regulated lipids in non-targeted lipidomic analyses.
| Non-targeted Study | Up-regulated lipids | Down-regulated lipids |
|---|---|---|
| Iurova et al (2022) | Plasmanyl-LPC(O-16:0), Plasmenyl-PE(P-18:0/18:2,18:0/20:3,18:0/20:4,18:1/22:6), Plasmenyl-PC(P-16:1/18:0), LPC (14:0,17:0,18:2), PS(37:5), SM(d20:0/18:4) and CerNS(d18:1/24:0) in patients vs controls |
|
| Salminen et al (2021) | Cer(d18:1/18:0) | PC-O(38:4) |
| Wang et al (2021) | FFAs, LPCs and LPEs in EOC/BOT vs controls. Cers in EOC vs controls |
PCs, PC-Os, PE-Os, SMs and PIs in EOC/BOT vs controls |
| Buas et al (2021) | CER(18:0) in patients vs controls | TAG, PC, CE species, DAG, PE, LPC, LPE and SM species in patients vs controls |
| Niemi et al (2018) | Cers with 18:0, 20:0 and 24:1 FAs, TAGs with longer FA side chains |
Phospholipids (PCs, LPCs, PIs), cholesteryl esters, glucosyl/galactosyl Cers, and sphingomyelins, 24:0 FA-containing Cers, TAGs with shorter FA side chains |
| Braicu et al (2017) | Cers, with 16:0, 18:0, 20:0 and 24:1 FAs. Long chain TAGs. |
PCs, PEs, PIs, CEs, DAGs, SMs, cerebrosides(Glc/GalCers), LacCers, Gb3s, S1Ps. CERs containing 23:0 and 24:0 FAs. TAGs with short FA side chain. |
| Li et al (2017) | PC(31:2) and PE-P(42:4) in EOC recurrent patients | LysoPCs, PCs, PIs in recurrent EOC patients compared with the non-recurrent patients. LysoPG(20:5), Cer(d18:1/23:0), SM(d18:1/14:0), SM(d18:2/14:0), TGs in EOC recurrent |
| Xie et al (2017) | Plasma relative intensity of LPE (20:0/0:0) in patients with long-term survival | Relative intensity of PC(42:11) in patients with long-term survival |
| Buas et al (2016) | Glycerolipids and glycerophospholipids in cases versus controls | |
| Ke et al (2016) | Fatty acids in Post-operative EOC patients. LPCs, LPEs and fatty acids in EOC recurrent patients. |
LPCs, Tetracosahexaenoic acid, 2-octenoic acid, 12,13-DiHODE and 19,20-DiHDPA of primary EOC patients compared to controls. |
| Y.Zhang et al (2016) | LPCs in patients compared to BOT and controls | PCs and TGs in patients compared to BOT and controls |
| Hou et al (2016) | All the GPs in EOC patients vs controls, except PC(33:5) and PC(34:3). MG and SPs in EOC patients, except SM(d18:2/14:0) |
DG in EOC patients vs BOT/UF |
| Gaul et al (2015) | LPE and LPI in OC patients vs controls | |
| H. Zhang et al (2015) | LysoPC(14:0) and LysoPE(18:2) decreased in EOC patients with recurrence compared to non-recurrent | |
| T. Zhang et al (2012) | LysoPC(18:3), LysoPC(14:0) levels were lower in EOC patients compared to BOT patients |
Table 6.
Up/Down-regulated lipids in targeted lipidomic analyses.
| Targeted Study | Up-regulated lipids | Down-regulated lipids |
|---|---|---|
| Hishinuma et al (2021) | TGs in EOC vs HCs | LPCs and PCs in EOC vs HCs |
| Yagi et al (2020) | ||
| Zeleznik et al (2020) | ||
| Plewa et al (2019) |
LysoPC a C16:1, PC aa C32:2, PC aa C34:4 and PC aa C 36:6 | |
| Kozar et al (2018) | C16-Ceramide, long chain Ceramides C22/C24 and C18 and C18:1 Sphingomyelin levels in EOC vs Controls |
|
| Knapp et al (2017) | C16-Cer, C18:1-Cer and C18-Cer in AOC patients compared to controls | |
| Shan et al (2012) | PPE, LPC (14:0, 12:0) in OC patients compared to controls |
4. Discussion
Known as the “silent killer”, OC is the most lethal gynecological cancer. In order to improve early detection of the disease and identify novel therapeutic targets that could improve prognosis, prediction and survival, deeper understanding of its pathogenesis is required. One of the scientific fields that could contribute to this direction is the investigation of lipid metabolism and their alterations during carcinogenesis and progression of OC by lipidomic analyses. Up today, 7 reviews regarding literature for the involvement of small molecules, lipids included, in the development of OC are published (4,6,7,34–37). The first one was that of Pyragius et al (37), where is reported that OC cells depend on lipids for their increased energy requirements during tumor growth, with phospholipids and sphingolipids to be the main lipid classes implicated in carcinogenesis. In accordance with this review in 2013, reviews of Kreitzburg et al in 2018 (35) and Pitman et al in 2021 (34) agreed and enhanced the idea that S1P pathway (Sphingosine-1-Phosphate), which involves ceramides, sphingomyelins and spingosine-1-phosphate, is implicated in oncogenic processes, such as proliferation, migration, neovascularization and metastasis. Combining these conclusions with the results of our systematic literature search, it is obvious that glycerophospholipids metabolism could be considered a key dysregulated metabolic pathway in OC.
Our systematic review is the third one regarding the implication of lipid metabolites in OC after Turkoglu et al in 2016 (36) and Salim et al in 2020 (7), in which other metabolites, apart from lipids, were also investigated by metabolomic analyses in serum, plasma, tissue or cell lines of OC cells. Many of the studies included in our review were mentioned in Turkoglu’s and Salim’s papers. The conclusion introduced by their reviews and ours is that there is great evidence that lipid aberrations contribute to OC development and offer new insights to the pathogenesis of the disease with the potential to integrate novel diagnostic, prognostic and predictive biomarkers to the “gold standard” biomarker CA125. Indeed, Niemi et al (14) reported that the combination of CA125 measurements with those of significantly altered lipids, such as LPCs and PCs, improved diagnostic capability of CA125 at early stages (I/II) of the disease. Moreover, Buas et al (18) referred to the increase in accuracy of a multivariate model, consisting of 4 lipid biomarkers, to discriminate between malignant and benign ovarian masses, after the integration of CA125 levels.
It should be noted that Perrotti et al (4) in their review in 2016 mentioned lysophosphatidic acid (LPA) to be significantly increased in OC patients compared to healthy controls, based on the study of Meleh et al (38) in 2007. As knowledge and techniques evolved, Yagi et al (39) in 2019 analyzed potential inconsistencies in the use of LPA as biomarker in OC due to the possible effect of storage time of samples (artificial LPA generation during incubation at room temperature) and concentration of ethylene-diamine-tetra-acetic acid (EDTA) during blood drawing. Thus, we should consider with skepticism the role of LPA as biomarker in OC.
The possible role of upregulated long chain ceramides and sphingomyelins as diagnostic biomarkers in OC should be more thoroughly evaluated in future studies as recorded by Salminen et al (11), Niemi et al (14), Kozar et al (29), Braicu et al (15) and Knapp et al (30). However, apart from congruent results in our review, there are also results that contradict to each other. Indeed, most of our included studies demonstrated decreased levels of LPCs in OC patients versus BOT and healthy controls, while Zhang Y. et al (20) displayed upregulation of LPCs. This could be attributed to the small sample size (only n=65 participants) or to the population included. Furthermore, Wang et al (12), while agreed with other studies that PCs are downregulated in patients versus controls and Cers upregulated, they demonstrated an increase of LPCs in patients compared to controls, which is contradictory to other studies.
The most important strength of this review is that it included all studies regarding lipidomic analyses referred to the contribution of lipidomic serum/plasma profile of patients with malignant or benign ovarian tumors and healthy controls as potential biomarker in this deadly disease. Our supplementary analysis, consisted of 7 targeted studies, and the inclusion of 7 former reviews enhanced the validity and accuracy of our review. Exclusion of studies published before 2012 could be considered a source of bias. Concomitant inclusion of serum and plasma samples could affect results. Thus, we recommend skepticism about lipid changes that take place during OC development. Eight out of 22 included studies were conducted in China, while the rest in northern America and Europe. This could be considered a confounding factor that should be more thoroughly evaluated in future studies. Studies that were identified as being at serious risk of bias (mostly due to several confounding factors) should be considered with great skepticism.
5. Conclusions and Recommendations
Several lipid classes, such as LPCs, PCs, Cers, TGs, seem to play a significant role in oncogenic processes contributing to the development of OC. Many studies aimed to elucidate and evaluate their involvement in this greatly heterogeneous disease. Most studies focused on serous subtype, as is the most common type of OC. Through literature search, it is obvious that a great effort has been made in the last decade in order to identify potential lipid biomarkers for diagnosis, prognosis and prediction of this fatal disease. Due to several confounding factors in many of our included studies, we recommend that future studies focus on more appropriate matching between patients and controls, such as number of patients and controls, age, menopausal status, comorbidities, medications, levels of CA125.
We demonstrated that the incorporation of lipid biomarkers in the existing biomarkers CA125 and HE4 increased their sensitivity and specificity in the diagnosis of the disease.
Overall, our review highlighted the importance of lipid aberration and lipid pathways alterations during the development of OC. Future untargeted and targeted lipidomic analyses, adequately designed, could elucidate oncogenic pathways involved in the pathogenesis of this malignancy of poor prognosis and improve its screening, detection and recurrence.
Author Contributions
Tzelepi Vasiliki conceived and designed the literature review, was the main contributor of preparing, gathering of data, quality assessment and writing of the paper; Gika Helen conceived and coordinated the literature review, participated in designing and construction of all tables of the review, was responsible for independently cross-checking data extraction after literature search and the revision of the manuscript; Begou Olga participated in the literature search and contributed to the construction of all tables of the review; Timotheadou Helen coordinated the writing of the paper and with Gika Helen independently cross-checked data extraction and quality assessment of the manuscript. All authors read and approved the final manuscript.
Acknowledgments
Authors would like to thank the Society for Study of Cancer Therapeutics for the support in the publication costs.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Ovarian Cancer Coalition Atlas, 2020, available at worldovariancancercoalition.org. [accessed cited 2023 Feb 3].
- NCCN (National Comprehensive Cancer Network), NCCN Clinical Practice Guidelines in Oncology, Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer, Version 1.2022, available at www.nccn.org/patients. [accessed cited 2022 Jan 5].
- Ferrarow S, Braga F, Lanzoni M, Boracchi P, Biganzoli EM, Panteghini M. Serum human epididymis protein 4 vs carbohydrate antigen 125 for ovarian cancer diagnosis: A systematic review. J Clin Pathol, 2013, 66, 273–81. [CrossRef]
- Perrotti F, Rosa C, Cicalini I, Sacchetta P, Del Boccio P, Genovesi D, et al. Advances in lipidomics for cancer biomarkers discovery. Vol. 17, Int. J. Mol. Sci., 2016, 17. [CrossRef]
- Wenk M. The Emerging Field of Lipidomics. Nature, 2005, 4, 594-610. [CrossRef]
- Yan F, Zhao H, Zeng Y. Lipidomics: a promising cancer biomarker. Clin Transl Med., 2018, 7. [CrossRef]
- Ahmed-Salim Y, Galazis N, Bracewell-Milnes T, Phelps DL, Jones BP, Chan M, et al. The application of metabolomics in ovarian cancer management: A systematic review. Int J Gynecol Cancer., 2021, 31, 647–55. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021, 372.
- Sterne JAC, Hernan MA, Reeves BC, Savovic J, Berkman ND et al Risk Of Bias In Non-randomized Studies of Interventions (ROBINS-I): detailed guidance, 2016, available from: http://www.riskofbias.info [accessed cited 2023 Mar 15].
- Iurova M V., Chagovets V V., Pavlovich S V., Starodubtseva NL, Khabas GN, Chingin KS, et al. Lipid Alterations in Early-Stage High-Grade Serous Ovarian Cancer. Front Mol Biosci., 2022, 9. [CrossRef]
- Salminen L, Braicu EI, Lääperi M, Jylhä A, Oksa S, Hietanen S, et al. A novel two-lipid signature is a strong and independent prognostic factor in ovarian cancer. Cancers, 2021, 13. [CrossRef]
- Wang Y, Wang Y, Chen C, Ren F, Cao R, Wang Y, et al. Serum lipid profiling analysis and potential marker discovery for ovarian cancer based on liquid chromatography–Mass spectrometry. J Pharm Biomed Anal., 2021, 199.
- Buas MF, Drescher CW, Urban N, Li CI, Bettcher L, Hait NC, et al. Quantitative global lipidomics analysis of patients with ovarian cancer versus benign adnexal mass. Sci Rep., 2021, 11. [CrossRef]
- Niemi RJ, Braicu EI, Kulbe H, Koistinen KM, Sehouli J, Puistola U, et al. Ovarian tumours of different histologic type and clinical stage induce similar changes in lipid metabolism. Br J Cancer., 2018, 119, 847–54. [CrossRef]
- Braicu EI, Darb-Esfahani S, Schmitt WD, Koistinen KM, Heiskanen L, Pöhö P, et al. High-grade ovarian serous carcinoma patients exhibit profound alterations in lipid metabolism Oncotarget, 2017, 8, 102912-22.
- Xie H, Hou Y, Cheng J, Openkova MS, Xia B, Wang W, et al. Metabolic profiling and novel plasma biomarkers for predicting survival in epithelial ovarian cancer. Oncotarget, 2017, 8, 32134-46. [CrossRef]
- Li j, Xie H, Li A, Cheng J, Yang K, Wang J, et al. Distinct plasma lipids profiles of recurrent ovarian cancer by liquid chromatography-mass spectrometry. Oncotarget, 2017, 8, 46834–45.
- Buas MF, Gu H, Djukovic D, Zhu J, Drescher CW, Urban N, et al. Identification of novel candidate plasma metabolite biomarkers for distinguishing serous ovarian carcinoma and benign serous ovarian tumors. Gynecol Oncol., 2016, 140, 138–44. [CrossRef]
- Ke C, Li A, Hou Y, Sun M, Yang K, Cheng J, et al. Metabolic phenotyping for monitoring ovarian cancer patients. Sci Rep., 2016, 6. [CrossRef]
- Zhang Y, Liu Y, Li L, Wei J, Xiong S, Zhao Z. High resolution mass spectrometry coupled with multivariate data analysis revealing plasma lipidomic alteration in ovarian cancer in Asian women. Talanta, 2016, 150, 88–96. [CrossRef]
- Hou Y, Li J, Xie H, Sun F, Yang K, Wang J, et al. Differential plasma lipids profiling and lipid signatures as biomarkers in the early diagnosis of ovarian carcinoma using UPLC-MS. Metabolomics, 2016, 12, 1–12. [CrossRef]
- Gaul DA, Mezencev R, Long TQ, Jones CM, Benigno BB, Gray A, et al. Highly-accurate metabolomic detection of early-stage ovarian cancer. Sci Rep., 2015, 5. [CrossRef]
- Zhang H, Ge T, Cui X, Hou Y, Ke C, Yang M, et al. Prediction of advanced ovarian cancer recurrence by plasma metabolic profiling. Mol Biosyst., 2015, 11, 516–21. [CrossRef]
- Zhang T, Wu X, Yin M, Fan L, Zhang H, Zhao F, et al. Discrimination between malignant and benign ovarian tumors by plasma metabolomic profiling using ultra performance liquid chromatography/mass spectrometry. Clinica Chimica Acta, 2012, 413, 861–8. [CrossRef]
- Hishinuma E, Shimada M, Matsukawa N, Saigusa D, Li B, Kudo K, et al. Wide-targeted metabolome analysis identifies potential biomarkers for prognosis prediction of epithelial ovarian cancer. Toxins, 2021, 13. [CrossRef]
- Yagi T, Kuschner CE, Shoaib M, Choudhary RC, Becker LB, Lee AT, et al. Relative ratios enhance the diagnostic power of phospholipids in distinguishing benign and cancerous ovarian masses. Cancers, 2020, 12. [CrossRef]
- Zeleznik OA, Heather Eliassen A, Kraft P, Poole EM, Rosner BA, Jeanfavre S, et al. A prospective analysis of circulating plasma metabolites associated with ovarian cancer risk. Cancer Res. 2020, 80, 1357–67.
- Plewa S, Horała A, Dereziński P, Nowak-Markwitz E, Matysiak J, Kokot ZJ. Wide spectrum targeted metabolomics identifies potential ovarian cancer biomarkers. Life Sci., 2019, 222, 235–44. [CrossRef]
- Kozar N, Kruusmaa K, Bitenc M, Argamasilla R, Adsuar A, Goswami N, et al. Metabolomic profiling suggests long chain ceramides and sphingomyelins as a possible diagnostic biomarker of epithelial ovarian cancer. Clinica Chimica Acta., 2018 481, 108–14. [CrossRef]
- Knapp P, Bodnar L, Błachnio-Zabielska A, Świderska M, Chabowski A. Plasma and ovarian tissue sphingolipids profiling in patients with advanced ovarian cancer. Gynecol Oncol., 2017, 147, 139–44. [CrossRef]
- Shan L, Chen YA, Davis L, Han G, Zhu W, Molina AD, et al. Measurement of Phospholipids May Improve Diagnostic Accuracy in Ovarian Cancer. PLoS One., 2012, 7. [CrossRef]
- Korthauer K, Kimes PK, Duvallet C, Reyes A, Subramanian A, Teng M, et al. A practical guide to methods controlling false discoveries in computational biology. Genome Biol., 2019, 20. [CrossRef]
- Considine EC, Thomas G, Boulesteix AL, Khashan AS, Kenny LC. Critical review of reporting of the data analysis step in metabolomics. Metabolomics, 2018,14. [CrossRef]
- Pitman MR, Oehler MK, Pitson SM. Sphingolipids as multifaceted mediators in ovarian cancer. Cellular Signalling, 2021,81. [CrossRef]
- Kreitzburg KM, van Waardenburg RCAM, Yoon KJ. Sphingolipid metabolism and drug resistance in ovarian cancer. Cancer Drug Resist. 2018, 1, 181–97. [CrossRef]
- Turkoglu O, Zeb A, Graham S, Szyperski T, Szender JB, Odunsi K, et al. Metabolomics of biomarker discovery in ovarian cancer: a systematic review of the current literature. Metabolomics, 2016, 12. [CrossRef]
- Pyragius CE, Fuller M, Ricciardelli C, Oehler MK. Aberrant lipid metabolism: An emerging diagnostic and therapeutic target in ovarian cancer. Int. J. Mol. Sci., 2013, 14, 7742–56. [CrossRef]
- Meleh M, Požlep B, Mlakar A, Meden-Vrtovec H, Zupančič-Kralj L. Determination of serum lysophosphatidic acid as a potential biomarker for ovarian cancer. J Chromatogr B Analyt Technol Biomed Life Sci. 2007, 858, 287–91. [CrossRef]
- Yagi T, Shoaib M, Kuschner C, Nishikimi M, Becker LB, Lee AT, et al. Challenges and inconsistencies in using lysophosphatidic acid as a biomarker for ovarian cancer. Cancers, 2019, 11. [CrossRef]
Figure 1.
Flow diagram of the search strategy and study selection process.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



