
Submitted:
02 August 2023
Posted:
03 August 2023
You are already at the latest version
Abstract
Cesarean section is a challenge intervention in patients treated with dual antiplatelet therapy. We present case of 32 years old pregnant woman experiencing large acute myocardial infarction (MI) of anterolateral wall complicated by cardiogenic shock in the 38th week of pregnancy treated with drug-eluting stent implantation and dual antiplatelet therapy (DAPT) consisting of aspirin and ticagrelor. Less than 24 hours after MI delivery started, urgent Caesarean section was indicated. As multiplate aggregometry testing showed a relatively insufficient level of ticagrelor platelet inhibition and a moderate level of aspirin platelet inhibition, Caesarean section was performed without discontinuation of ticagrelor, which was decided due to the need for emergency surgery. Local hemostatic measures including administration of tranexamic acid were applied. The patient did not experience excessive bleeding. A healthy male baby was born. To the best of our knowledge, this is the first reported case of surgery in pregnant women treated with DAPT without ticagrelor discontinuation.
Keywords:
ticagrelor
; pregnancy
; myocardial infarction
; aggregometry
1. Introduction
Although acute MI in pregnancy is a rare disorder, coronary artery disease accounts for more than 20% of maternal cardiac deaths. Considering the raising age of women getting pregnant, acute coronary syndrome might become more common [1].
Currently, the management of antiplatelet therapy in urgent surgeries is not extensively covered in clinical guidelines. Usually, in high-ischemic-risk-patient aspirin should not be discontinued regardless of the hemorrhagic risk of the surgery, whereas P2Y12 antagonists (ticagrelor, prasugrel, and clopidogrel) administration should be discontinued when possible [1,2]. Here we present complex case of pregnant woman experiencing MI with ST segment elevation (STEMI) and treated with DAPT consisting of aspirin and ticagrelor, without discontinuation of ticagrelor prior to Caesarean delivery.
2. Case report
A 32-year-old female patient in the 38th week of gestation was admitted to Reanimation Ambulance of the Emergency Centre in a state of cardiogenic shock and clinical signs of STEMI of anterolateral wall. On admission, the patient was found to be dyspneic, hypotensive (arterial tension: 85/65mmHg both-sided), and tachycardic (heart frequency: 115 per minute). Medical history was taken – she was a former smoker and hypertensive two years preceding pregnancy. Hereditary factors were considered to have strongly contributed to her state as the patient's pregnant sister had a sudden death at the age of 35 in the 9th month of pregnancy while her other sister had sudden death at the age of 38. In addition, the patient's father died of MI at the age of 55.
Electrocardiography testing was performed with the results showing ST elevation in leads D1, aVL, and V2-V6 and ST depression in leads D2, D3, and aVF, as displayed in Figure 1.
Echocardiography testing showed a slightly enlarged left ventricle (5.7cm in diastole and 3.7cm in sistole), hypokinetic medial segments of interventricular septum, anterior and lateral walls and akinetic apical segments. Total left ventricle ejection fraction (EF) was 30%. Laboratory analysis showed: Troponin T 98 ng/L (normal value up to 14 ng/L) at first measure, reaching maximum value of 10000 ng/L, with creatine kinase (CK) 7263 U/L (normal value up to 150 U/L).
The obstetric examination showed aligned cervix with 2 cm to 3 cm dilation and regular heartbeats in the neonate. DAPT consisting of aspirin 300 mg and ticagrelor 180 mg, with the support of inotropic drugs, was administered. Angiography disclosed a 90% diameter stenosis in the proximal segment of the left anterior descendent coronary artery (LAD) and left coronary sinus aneurysm. Due to high thrombus burden, bolus eptifibatide was administered. (Figure 2a)
After diagnosing single-vessel disease, drug-eluting stent (DES, type: Premier® 3.0x28mm) was implanted in the osteo-proximal part of LAD (Figure 2b).
Shortly after percutaneous coronary intervention (PCI) with DES implantation, the patient was temporarily stabilized with reduced signs of left-sided heart failure (HF), but deteriorated next day. Further obstetric examination showed: cervix dilation 4cm, vertex presentation engaged, regular heartbeats of baby, a normal and adequate volume of amniotic fluid and placenta on the back wall. Doppler obstetric ultrasound showed normal blood flow through the umbilical cord. Due to significant cervix dilation and persisting signs of HF, urgent Caesarian section was indicated.
As a part of the perioperative assessment, laboratory analyses including aggregometry testing were performed. Impedance aggregometry testing (Multiplate® platelet function analyzer) revealed a relatively insufficient level of ticagrelor platelet inhibition (area under the curve: 591 AU*min) in adenosine diphosphate (ADP) high sensitive test (ADP + prostaglandin E), while moderate level of aspirin-induced platelet inhibition was detected (area under the curve: 404 AU*min) using arachidonic acid (ASPI) test. Thrombin receptor activating peptide (TRAP) test which represents baseline platelets aggregation showed expected values of 1399 AU*min. ADP high sensitive, ASPI, and TRAP test results can be seen in Figure 3.
Based on these aggregometry results, it was decided that the bleeding risk was minimal, with the high ischemic risk and therefore, DAPT was not interrupted prior to delivery. Caesarian section was performed with intraoperative blood salvage, transfusion of red cell concentrates (due to a preoperative hemoglobin value of 7.5 g/dl) and local hemostatic measures (application of six ampules of tranexamic acid via surgical incision (3000mg) and two ampules in the front abdominal wall muscles (1000mg)). Due to uterine hypotonia, one ampule of Prostaglandin M 15 (250µg) was injected in the myometrium. The procedure ha passed without complications and a male baby of 2700 g weight was born with an estimated standardized assessment for infants after delivery (APGAR) score of 8.
In the subsequent treatment course, the patient had the following findings: blood in lochia secretion and mild epistaxis, paroxysmal atrial fibrillation, parietal left ventricular thrombus, bilateral bronchopneumonia, and pleural effusions. She also had anemia (without meeting the criteria of major bleeding) and psycho-organic syndrome.
Taking into consideration epistaxis and blood in lochia secretion, it was decided to replace ticagrelor with clopidogrel. However, after receiving a loading dose of 600 mg of clopidogrel in two divided doses, aggregometry testing showed even more significantly pronounced clopidogrel resistance. Therefore, clopidogrel was discontinued and ticagrelor reintroduced. In the following course, aggregometry testing showed adequate response to ticagrelor, as shown in table 1.
Following detailed thrombophilia testing showed transitory positive lupus anticoagulant LA1/LA2: 1,74…1,65…1,43 (normal range 1,1 – 1,4), a transitory decrease of protein C global (0,45…0,73, ...1,10 µmol/l; normal levels of protein C 3,9-5,9 µmol/l), transitory elevated factor VIII (>145 %) and elevated homocysteine (17.4 µmol/l; normal range 0-14 µmol/l). On genetic examination, we detected MTHFR C677T heterozygote mutation, PAI-1 4G/5G heterozygote mutation with normal FII 20210: GG normal and normal FV Leiden. The antithrombin levels were normal.
Anti-cardiolipin antibodies showed normal values.
Analysis of lipidogram revealed elevated Lipoprotein (a) (0.64 g/L, normal range: 0-0,3 g/L) and normal value of Apolipoprotein A-I had normal value (1.01 g/L; normal range: 1.08-2.25 g/L). High-density lipoprotein (HDL) cholesterol was decreased (0.78 mmol/L, normal value above 1.3 mmol/L), whereas the total cholesterol level (4.22 mmol/L, normal value up to 5.2 mmol/L) and low-density lipoprotein (LDL) cholesterol level (2.64 mmol/L, normal value up to 3.4 mmol/L) were in normal range. Triglycerides were elevated, ranged from 3.29 to 1.75 mmol/L (normal values up to 1.7 mmol/L).
After leaving the intensive care unit, the patient's antithrombotic therapy included aspirin (100mg), ticagrelor (90mg twice daily), and enoxaparin 0.6 ml subcutaneously. On discharge, enoxaparin was replaced with warfarin.
Three years after the surgery mother and the baby was in stable condition.
3. Discussion
Pharmacological treatment of acute MI in pregnancy represents a clinical challenge in which both pregnant women and the baby's safety must be considered. Low-dose aspirin is considered generally safe, whereas information on P2Y12 antagonists is insufficient [1]. However, taking into account the hypercoagulable nature of the pregnancy [3,4] and the platelet aggregation changes [5,6], individualized approaches may prove especially useful. In the current literature, only two case reports of the use of ticagrelor in pregnant women with MI were described. In the first case, ticagrelor was discontinued two weeks before delivery [7], whereas in the second case, ticagrelor was stopped five days prior to the procedure, with tirofiban infusion antiplatelet therapy bridging [8]. Similar cases describing prasugrel use in pregnancy and its discontinuation prior to delivery are described in the literature [9,10]. Also, clopidogrel was discontinued in most cases available in literature 5 to 7 days prior to delivery or earlier [11,12,13]. We were able to identify two cases when the Caesarean section was performed without clopidogrel discontinuation. In the first case platelet transfusion was administered and no aggregometry testing was performed [14]. In the other case, clopidogrel was withheld on the morning of the Caesarean section that was urgent and platelet function testing was not reported [15].
Our patient required an emergency Caesarean section. Based on the aggregometry results and our previous experience with platelet function testing, the decision was made to perform the procedure without discontinuation of ticagrelor. However, we emphasize the importance of using systemic and local hemostatic preventive measures – intraoperative blood salvage with local use of tranexamic acid.
According to the manufacturer, normal values for multiplate ADP high sensitivity test (Multiplate®; Roche Diagnostics, Basel, Switzerland) range from 430 AU*min to 1000 AU*min. Although current guidelines recommend discontinuation of ticagrelor at least five days prior to surgery [1,16], a recent retrospective study showed five days to be possibly longer than necessary – i.e., there was no significant increase of the major bleeding risk in acute coronary syndrome patients operated 72-120 hours after ticagrelor discontinuation as compared to those operated more than 120 hours after the discontinuation [17].
C. J. Malm et al. performed a prospective observational study in ticagrelor-treated cardiac surgery patients. The authors found the optimal cut-off value for ADP-induced aggregation to be 220 AU*min. According to their study, 61% of patients developed severe bleeding when ADP-induced aggregation was below the cut-off value, compared to only 14% of patients when aggregation was at or above the cut-off value [18]. Ranucci et al. suggested a cut-off of 310 AU*min for the Multiplate ADP test to support a clinical decision to postpone elective surgery [19]. Similar to the aforementioned results, Sebastian Woźniak et al. found that in patients undergoing coronary artery bypass graft surgery, the results of ADP test (multiple electrode platelet aggregometry) of less than 260 AU*min strongly predicted serious bleeding complications after coronary artery bypass graft surgery [20]. With the value of 591 AU*min for ADP-induced aggregation in our patient, her results were well above the aforementioned cut-off values.
A large meta-analysis in 4213 patients showed that the use of platelet reactivity testing after PCI and consequent appropriate intensification of antiplatelet therapy reduces cardiovascular mortality and stent thrombosis following PCI [21,22].
Since systemic use of antifibrinolytics may increase the ischemic risk but decrease major bleeding [23], we opted for local use of tranexamic acid. According to guide of Italian group of experts, aspirin should be continued even if the risk of bleeding is high, whereas the approach with P2Y12 antagonists differs based on the type of surgery. Although the Caesarian section was not described, the authors of the guideline suggested that individual bleeding and ischemic risk assessment should be performed. A multidisciplinary approach is to be taken to tailor adequate antiplatelet therapy in high-risk patients needing the surgery [2].
4. Conclusions
To the best of our knowledge, this is the first case of pregnancy-associated MI treated with DAPT without ticagrelor discontinuation prior to delivery. In surgeries, aspirin is regarded as relatively safe and possibly useful drug when used in small doses. On the other hand, evidence supporting decisions on ticagrelor and other P2Y12 antagonists in urgent surgeries is lacking. Therefore, laboratory monitoring of platelet aggregation may provide invaluable insight into the overall bleeding and ischemic risk. However, the use of antiplatelet therapy in pregnancy and delivery requires significant pharmacotherapeutic considerations, and multidisciplinary approach should always be applied.
Author Contributions
Conceptualization, N.A. and D.M.; Investigation N.A, D.M., P.M., D.O. and S.K.; Data curation, N.G., T.I.M., N.S., L.B. and Z.L.; Writing—original draft preparation, N.A and D.M.; Writing—review and editing, P.M., D.O. and L.B.; Visualization S.K., N.S. and Z.L.; Supervision, N.A. and D.M. Project administration, D.M. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Regitz-Zagrosek, V.; Roos-Hesselink, J.W.; Bauersachs, J.; Blomström-Lundqvist, C.; Cífková, R.; De Bonis, M.; Iung, B.; Johnson, M.R.; Kintscher, U.; Kranke, P.; et al. 2018 ESC Guidelines for the management of cardiovascular diseases during pregnancy. Eur Heart J. 2018, 39(34), 3165–241. [Google Scholar] [CrossRef] [PubMed]
- Rossini, R.; Musumeci, G.; Visconti, L.O.; Bramucci, E.; Castiglioni, B.; De Servi, S.; Lettieri, C.; Lettino, M.; Piccaluga, E.; Savonitto, S.; et al. Perioperative management of antiplatelet therapy in patients with coronary stents undergoing cardiac and non-cardiac surgery: a consensus document from Italian cardiological, surgical and anaesthesiological societies. EuroIntervention. 2014, 10(1), 38–46. [Google Scholar] [CrossRef] [PubMed]
- Battinelli, EM.; Marshall, A.; Connors, J.M. The role of thrombophilia in pregnancy. Thrombosis. 2013, 2013, 516420. [Google Scholar] [CrossRef] [PubMed]
- Ormesher, L.; Simcox, L.; Tower, C.; Greer, I.A. Management of inherited thrombophilia in pregnancy. Women's Health (Lond Engl). 2016; 12(4): 433–41. [CrossRef]
- Juan, P.; Stefano, G.; Antonella, S.; Albana, C. Platelets in pregnancy. J Prenat Med. 2011, 5(4), 90–2. [Google Scholar] [PubMed]
- Burke, N.; Flood, K.; Murray, A.; Cotter, B.; Dempsey, M.; Fay, L.; Dicker, P.; Geary, M.P.; Kenny, D.; Malone, F.D. Platelet reactivity changes significantly throughout all trimesters of pregnancy compared with the nonpregnant state: a prospective study. BJOG. 2013, 120(13), 1599–604. [Google Scholar] [CrossRef] [PubMed]
- Verbruggen, M.; Mannaerts, D.; Muys, J.; Jacquemyn, Y. Use of ticagrelor in human pregnancy, the first experience. BMJ Case Rep. 2015; 2015, bcr2015212217. [CrossRef]
- Argentiero, D.; Savonitto, S.; D'Andrea, P.; Iacovelli, F. Ticagrelor and tirofiban in pregnancy and delivery: beyond labels. J Thromb Thrombolysis. 2020; 49(1), 145–8. [CrossRef]
- Tello-Montoliu, A.; Seecheran, N.A.; Angiolillo, D.J. Successful pregnancy and delivery on prasugrel treatment: considerations for the use of dual antiplatelet therapy during pregnancy in clinical practice. J Thromb Thrombolysis. 2013; 36(3), 348–51. [CrossRef]
- Pop, R.; Cebula, H.; Lambert, A.; Mihoc, D.; Manisor, M.; Cindea, C.; Hasiu, A.; Deruelle, P.; Chibbaro, S.; Mertz, L.; et al. Treatment with flow diverter stent during pregnancy. Neuroradiology. 2020, 62(11), 1507–10. [Google Scholar] [CrossRef] [PubMed]
- Reilly, C.R.; Cuesta-Fernandez, A.; Kayaleh, O.R. Successful gestation and delivery using clopidogrel for secondary stroke prophylaxis: a case report and literature review. Arch Gynecol Obstet. 2014; 290(3), 591–4. [CrossRef]
- De Santis, M.; De Luca, C.; Mappa, I.; Cesari, E.; Mazza, A.; Quattrocchi, T.; Caruso, A. Clopidogrel treatment during pregnancy: a case report and a review of literature. Intern Med. 2011, 50(16), 1769–73. [Google Scholar] [CrossRef] [PubMed]
- Klinzing, P.; Markert, U.R.; Liesaus, K.; Peiker, G. Case report: successful pregnancy and delivery after myocardial infarction and essential thrombocythemia treated with clopidogrel. Clin Exp Obstet Gynecol. 2001, 28(4), 215–6. [Google Scholar] [PubMed]
- Santiago-Díaz, P.; Arrebola-Moreno, A.L.; Ramírez-Hernández, J.A.; Melgares-Moreno, R. Platelet antiaggregants in pregnancy. Rev Esp Cardiol (Engl Ed). 2009, 62(10), 1197–8. [CrossRef]
- Al-Aqeedi, R.F.; Al-Nabti. A.D. Drug-eluting stent implantation for acute myocardial infarction during pregnancy with use of glycoprotein IIb/IIIa inhibitor, aspirin and clopidogrel. J Invasive Cardiol. 2008, 20(5), E146-9.
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L,; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS. Eur Heart J. 2018, 39(3), 213–60. 3. [CrossRef]
- Hansson, E.C.; Malm, C.J.; Hesse, C.; Hornestam, B.; Dellborg, M.; Rexius, H.; Jeppsson, A. Platelet function recovery after ticagrelor withdrawal in patients awaiting urgent coronary surgery. Eur J Cardiothorac Surg. 2017, 51(4), 633–7. [Google Scholar] [CrossRef] [PubMed]
- Malm, C.J.; Hansson, E.C.; Åkesson, J.; Andersson, M.; Hesse, C.; Shams Hakimi, C.; Jeppsson, A. Preoperative platelet function predicts perioperative bleeding complications in ticagrelor-treated cardiac surgery patients: a prospective observational study. Br J Anaesth. 2016, 117(3), 309–15. [Google Scholar] [CrossRef] [PubMed]
- Ranucci, M.; Baryshnikova, E.; Soro, G.; Ballotta, A.; De Benedetti, D.; Conti, D. Multiple electrode whole-blood aggregometry and bleeding in cardiac surgery patients receiving thienopyridines. Ann Thorac Surg. 2011, 91(1), 123–9. [Google Scholar] [CrossRef] [PubMed]
- Woźniak, S.; Woźniak, K.; Hryniewiecki, T.; Kruk, M.; Różański, J.; Kuśmierczyk, M. The predictive value of multiple electrode platelet aggregometry for postoperative bleeding complications in patients undergoing coronary artery bypass graft surgery. Kardiochir Torakochirurgia Pol. 2016; 13(1), 3–9. [CrossRef]
- Aradi, D.; Komócsi, A.; Price, M.J.; Cuisset, T.; Ari, H.; Hazarbasanov, D.; Trenk, D.; Sibbing, D.; Valgimigli, M.; Bonello, L. Efficacy and safety of intensified antiplatelet therapy on the basis of platelet reactivity testing in patients after percutaneous coronary intervention: systematic review and meta-analysis. Int J Cardiol. 2013, 167(5), 2140–8. [Google Scholar] [CrossRef] [PubMed]
- Lenk, E.; Spannagl, M. Platelet function testing-guided antiplatelet therapy. EJIFCC. 2013, 24(3), 90–6. [Google Scholar] [PubMed]
- Mazzeffi, M.A.; Lee, K.; Taylor, B.; Tanaka, K.A. Perioperative management and monitoring of antiplatelet agents: a focused review on aspirin and P2Y12 inhibitors. Korean J Anesthesiol. 2017, 70(4), 379–89. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
ECG on admission.
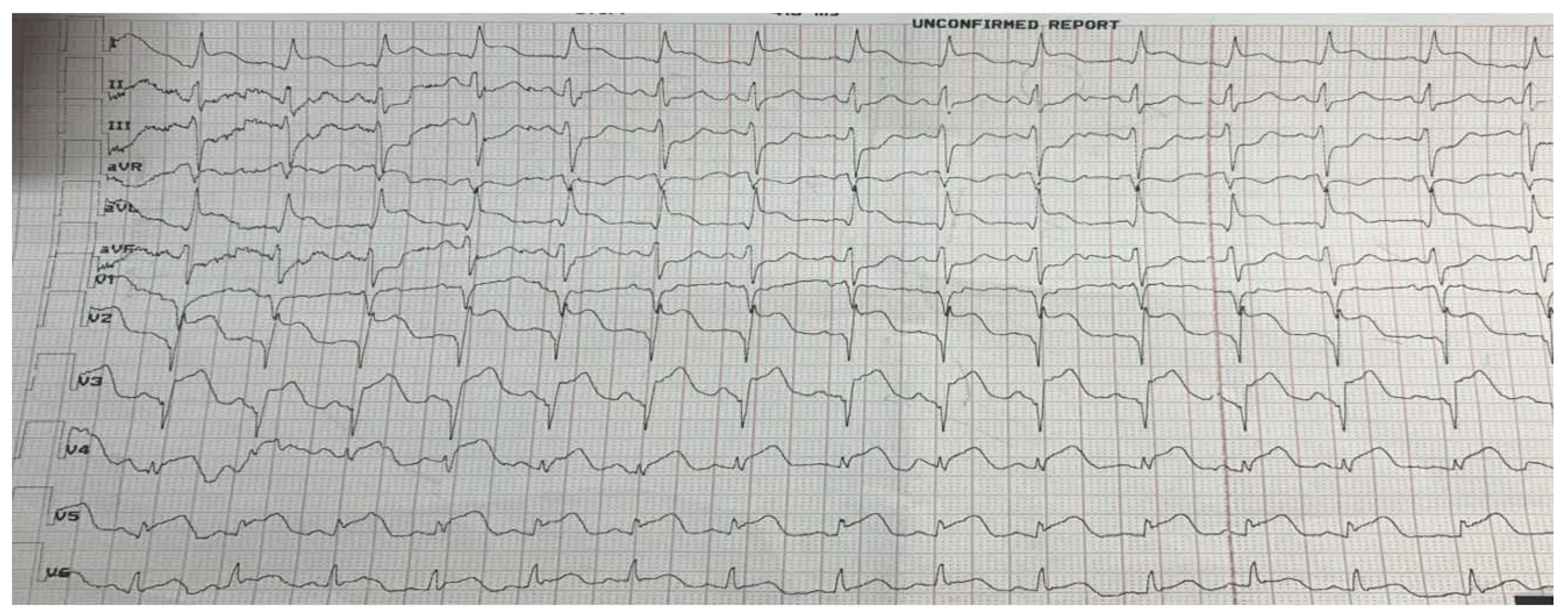
Figure 2.
Coronary angiography: (a) stenosis of the proximal segment of left anterior descendent coronary artery (arrow). (b) recovery of coronary flow after stent implantation (arrow).
Figure 2.
Coronary angiography: (a) stenosis of the proximal segment of left anterior descendent coronary artery (arrow). (b) recovery of coronary flow after stent implantation (arrow).
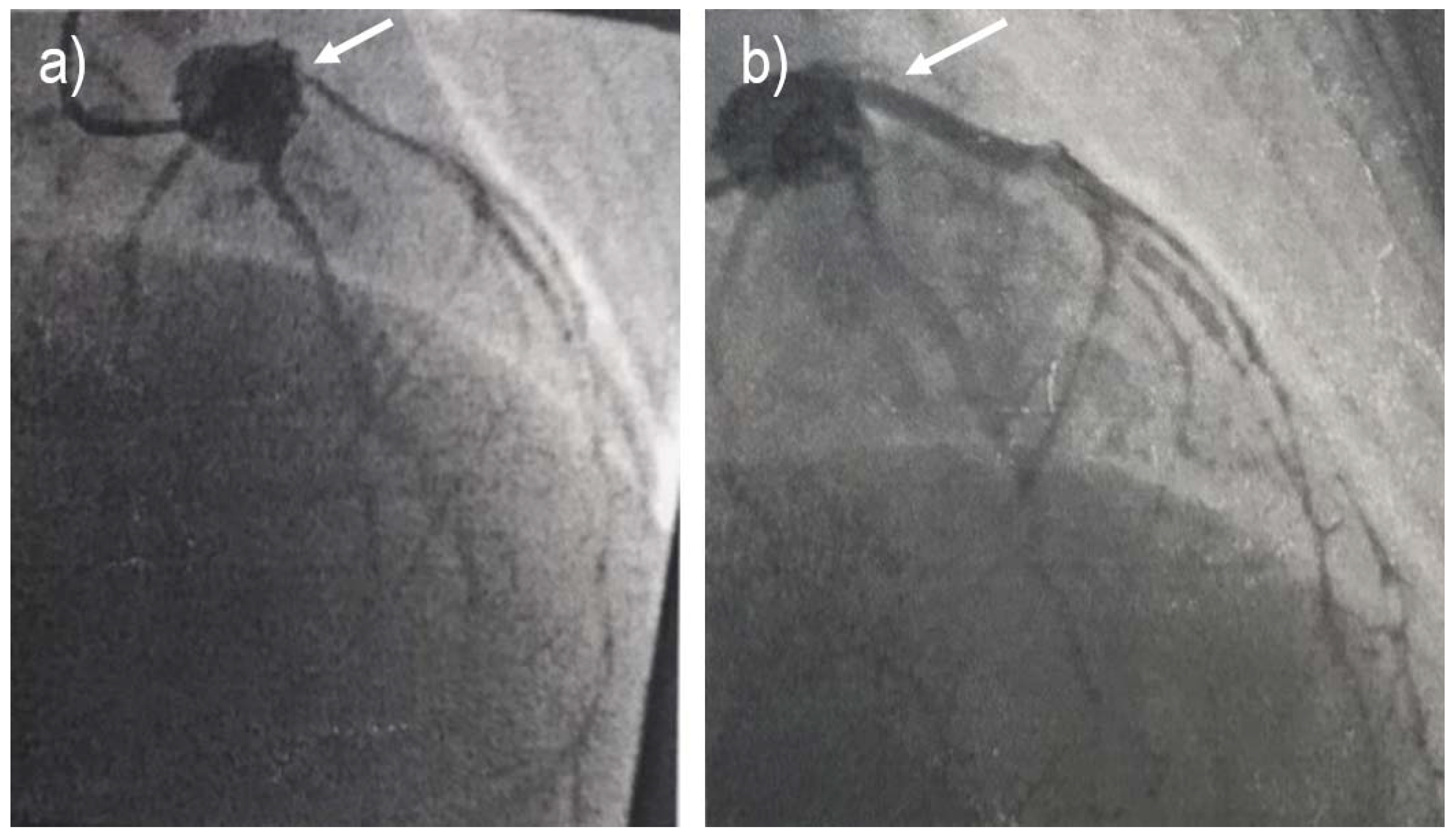
Figure 3.
Impedance aggregometry testing results.
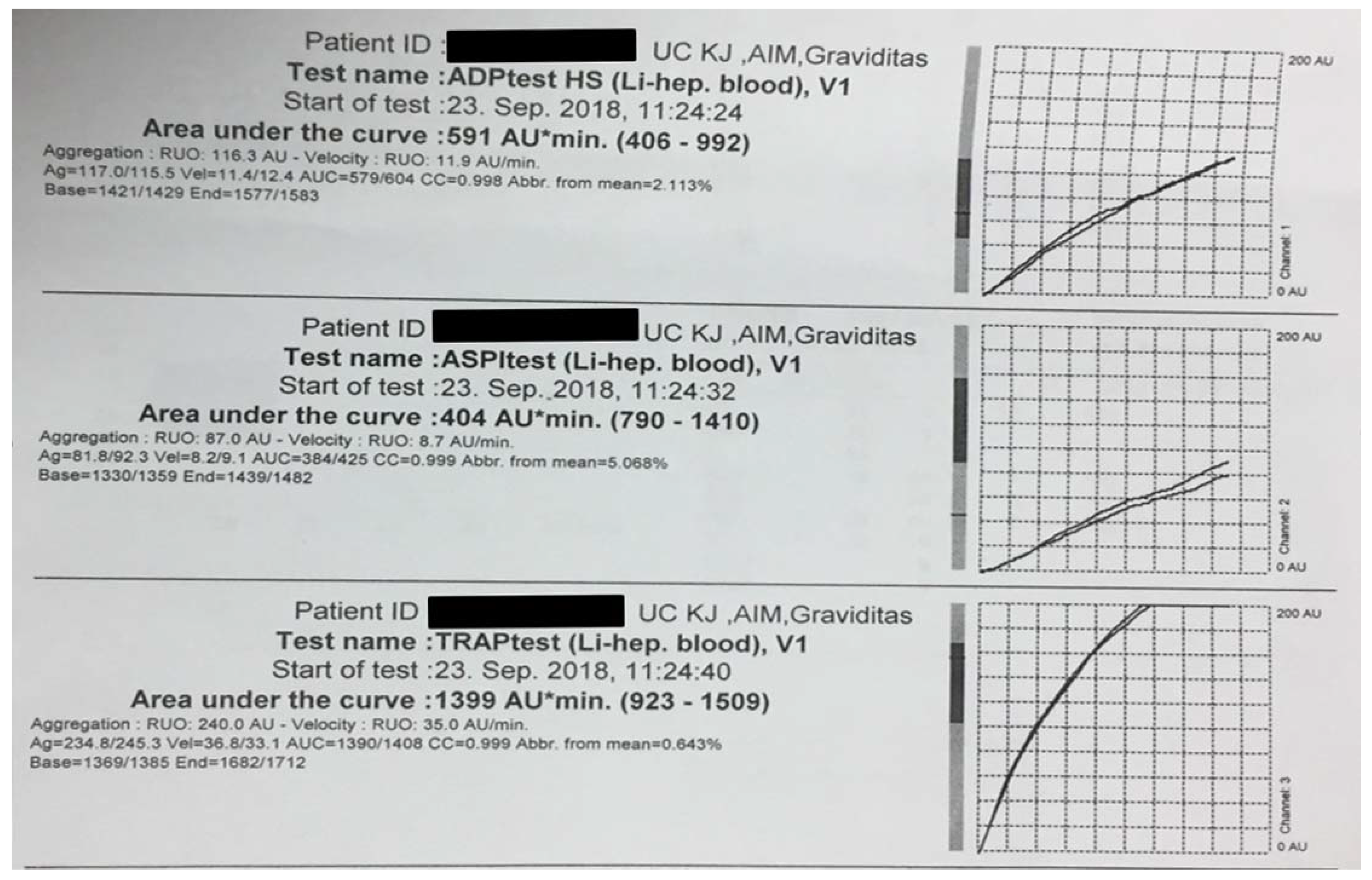

Table 1.
Aggregometry findings during hospital stay.
| Hospitalization day | ADP inhibitor drug | ADP test HS (AU*min) |
ASPI test (AU*min) |
TRAP test (AU*min) |
| Day 1 | ticagrelor | 591 | 404 | 1399 |
| Day 2 | clopidogrel | 1081 | 889 | 1984 |
| Day 3 | clopidogrel | 1263 | 1109 | 1718 |
| Day 4 | ticagrelor | 567 | 1320 | 1807 |
| Day 5 | ticagrelor | 535 | 646 | 1679 |
| Day 6 | ticagrelor | 373 | 373 | 1761 |
| Day 9 | ticagrelor | 315 | 512 | 1352 |
ADP - adenosine diphosphate; HS – high sensitive; AU – area under the curve; ASPI – arachidonic acid; TRAP - Thrombin receptor activating peptide.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



