
Submitted:
02 August 2023
Posted:
03 August 2023
You are already at the latest version
Abstract
Diseases caused by arboviruses are on the increase worldwide. In addition to arthropod bites, most arboviruses can be transmitted via accessory routes. Products of human origin (labile blood products, solid organs, hematopoietic stem cells, tissues) present a risk of contamination for the recipient if the donation is made when the donor is viremic. This narrative review describes the risks of acquiring certain arboviral diseases from human products, mainly solid organs and hematopoietic stem cells, in the French context. Mainland France and its overseas territories are exposed to a complex array of imported and endemic arboviruses, which differ according to their respective location. The main risks considered in this study are infections by West Nile virus, dengue virus and tick-borne encephalitis virus. The ancillary risks represented by Usutu virus infection, chikungunya and Zika are also addressed more briefly. For each disease, the guidelines issued by the French High Council of Public Health, which is responsible for issuing guidelines to mitigate the risks associated with products of human origin and for supporting public health policy decisions, are briefly outlined. The aim of this review is also to contribute to the standardization of recommendations at international level in areas with the same viral epidemiology.
Keywords:
safety of products of human origin
; solid organ transplantation
; hematopoietic stem-cell transplantation
; West Nile virus
; dengue virus
; tick-borne encephalitis virus
; Usutu virus
; Chikungunya virus
; Zika virus
; mainland and overseas France
1. Overall Presentation of the Main Risks of Arboviral Diseases in Graft Recipients with Special Reference to the French Context
Arboviruses represent a vast group of viruses that are transmitted by arthropods, which includes, for human diseases, hematophagous mosquitoes, phlebotomine sand flies and ticks. Arboviral diseases are endemic to all continents except Antarctica. By definition, arthropod bites by breeding females constitute the major mode of transmission of arboviruses to human beings. However, other pathogen-specific modes of transmission have been identified, including milk or milk-derived foods from infected animals or women, transplacental transmission during pregnancy, sexual transmission from infected persons or healthcare-associated transmission resulting from the administration of products originating from infected donor (blood, organs, tissues and cells). Table 1 shows the main arboviruses for which transmission via blood transfusion or grafts have been demonstrated or suspected.
This review is specifically dedicated to the main risks generated by arboviral diseases potentially transmitted by solid organ and hematopoietic stem cell grafts in humans with special reference to the French context. Indeed, as shown in Figure 1, France has a great geographical and complex administrative diversity, with 18 administrative regions divided, for most of them, in smaller areas named Departments (n = 101). In terms of arboviral risk, that situation leads to the circulation of a wide variety of vector species across space and time [1]. French territories are exposed to a variety of epidemiological situations. In mainland France, these include the absence of arbovirus circulation in certain areas, the circulation of endemic pathogens in animal cycles with occasional human spillovers [for example West Nile virus (WNV), Usutu virus (USUV) or tick-borne encephalitis virus), and in recent years the indigenous circulation of 'tropical' arboviruses [dengue virus (DENV), chikungunya virus (CHIKV) and Zika virus (ZIKV)] in southern regions. In the overseas territories, dengue fever is endemic and epidemic in most tropical areas (Caribbean islands, French Guiana, islands in the south-west Indian Ocean, Pacific territories) and Zika and Chikungunya have caused epidemics in all regions (except in the south-west Indian Ocean for Zika). Global warming is also a major factor affecting the distribution and vectorial capacity of arbovirus vectors [2], particularly in temperate zones that were previously protected from this risk.
Together with different national Agencies such as (i) “Santé publique France” (SpF) (French public health agency) associated to different regional agencies for public health, (ii) the French Blood product agencies, namely “Etablissement français du sang” (EFS) and “Centre de transfusion sanguine des armées” (CTSA)], (iii) the “Agence de la biomedicine” (ABM) (French Agency of Biomedicine) , the “Agence nationale de sécurité du médicament et des produits de santé” (ANSM) (National Agency for the Safety of Medicines and Health Products), and (iv) the “Centre national de reference (CNR) des arbovirus” (French national center for arboviruses), the “Haut conseil de la santé publique” (HCSP) (French High Council for Public Health) is in charge of defining recommendations in terms of safety of products of human origin at the national level, including blood, solid organs, cells and tissues. The aim of the current report is to focus on the arboviral diseases that are most frequently involved in solid organ transplantation (SOT) and hematopoietic stem-cell transplantation (HSCT) in France. For each of these diseases, we will study the risks associated with SOT and HSCT with a rapid review of published cases of transmission at the international level, the epidemiological context in mainland and overseas France and the specific prophylactic recommendations issued by the HCSP for recipients of solid organs and hematopoietic stem cells, in accordance with those of the European center for disease prevention and control (ECDC). Arboviral infections occurring in transplant recipients after mosquito bite, which accounts for most of the cases of arboviral infections in these patients, are excluded from the field of the review.
2. West Nile Virus (WNV)
WNV is a single-stranded RNA virus belonging to the Flaviviridae family. The main characteristics of WNV infection are shown in Table 1. The reservoir of the virus is constituted by wild birds that get infected mainly via mosquito bites (enzootic cycle). Infected mosquitoes (mostly Culex) can contaminate humans and other mammals, including horses; however, humans and horses are an epidemiological dead end since the viral load in blood is not high enough to infect new mosquitoes [3]. Five distinct lineages have been identified, three of them having been linked to significant outbreaks in humans. First isolated in 1937 in Uganda from a febrile patient, WNV has been shown to circulate for several decades in Africa, Europe, Middle-East (and notably Israel), in certain parts of Asia and even in Australia (lineage 1b also known as Kunjin virus) [4]. Since the end of the 1990s, the circulation of WNV re-increased in Europe, Northern Africa and Middle-East. In 1999, WNV was imported for the first time to the American continent causing an outbreak of severe encephalitis in New York City [5]. Within 3 years, WNV disseminated throughout North America.
Of note, it was only after the virus became endemic in the USA that human-to-human transmission of WNV via contaminated blood or solid organs was recognized. The first donor-derived WNV infections were reported in 2002 [6,7,8]. Since then, about 40 patients have been shown to be contaminated via blood products, including 38 in the USA −mostly in 2002 before the implementation of nucleic acid testing (NAT) in blood donors [6,9]− and 2 in Greece [10]. Among these, 29 presented a symptomatic infection, including 26 neuroinvasive diseases and 3 febrile infections; two recipients remained asymptomatic while no clinical data were available in the remaining 9 cases. As for SOT-derived WNV infections, 9 cases of transmission from deceased donors have been documented (Table 2), mostly in the USA [7,8,11,12] and in Italy [13,14]. As shown in Table 2, 9 donors, who had been contaminated pre-mortem either by blood transfusion or by mosquito bite, were the source of these contaminations. Twenty-six (26) subjects received organs from these 9 donors: 14 developed a neuroinvasive disease (including 6 fatal cases), 1 developed fever, 9 stayed asymptomatic despite documented infection, and 2 were not infected. Interestingly, 5 donors were diagnosed by WNV PCR test in blood while 4 exhibited only IgM specific antibodies (Table 2), which demonstrates that both tests are effective for donors' screening. No case of WNV transmission has been reported so far in HCST recipients. Blood- and transplant-transmitted WNV infections significantly decreased after blood and organ donors’ screening, especially after introduction of more sensitive NAT during the periods of WNV circulation.
In mainland France, WNV infections have been identified mainly in the Southern part of the country. The first human cases were reported in 1962-1963 in Camargue area and the first horse cases were reported only in the 2000s. The cases reported in mainland France in humans, horses and birds during the last 20 years are shown in Figure 2. Three epidemic peaks were observed in 2003-2004, 2015 and 2018. During the 2022 season, 6 human cases and 9 horse cases were observed (Figure 2). The low number of avian cases in France is probably due to the absence of systematic viral investigations in birds. Lineage 1a was predominant up to 2017 but lineage 2, originating from North Africa and Italy, is becoming endemic in the Mediterranean basin, possibly as a result of climate change [15].
In 2022 and 2023, the French HCSP updated its recommendations on the safety of blood-derived products, SOT and HSCT about the risk of WNV transmission [16,17,18]. Its main recommendations are as follows:
the human cases of WNV infection diagnosed on the French territory must be informed as a notifiable disease to SpF [19];
- –
- regarding blood products, all platelet concentrates and a part of the fresh frozen plasma must be secured by using a pathogen reduction method (Intercept blood System®, amotosalen/UVA); in case of identification of a new confirmed autochthonous case, an individual NAT screening (ID-NAT) must be implemented without delay for all blood donations collected in the impacted Department ; the blood products already collected in this area must be tested by ID-NAT if blood samples are still available with the exception of those treated by the Intercept® process. Blood donors having stayed (at least one night) in an affected area must be deferred until 28 days after their return or tested by ID-NAT. Candidate for donation reporting diagnosis of WNV infection must be deferred 122 days after the end of symptoms;
- –
- as for SOT and HSCT, in case of identification of a new autochthonous case, donors living or having stayed in the Region or Department concerned must be tested by WNV NAT and IgM/IgG serology must be performed, ideally before transplantation. The decision to use or not the organs or cells from donors tested positive either by NAT or IgM serology is submitted to the benefit-risk balance, with the recommendation of delaying the grafts that are not urgently needed;
- –
- a list of countries at risk for WNV during the period of circulation of the virus (namely June to November) is updated each year [20]. Candidates for blood, organ or cell donations originating from or having traveled in these countries must be either tested for WNV (NAT for blood and NAT + serology for grafts) or their donation postponed for 28 days after returning from the risk area;
- –
- in parallel, a surveillance of the circulation of WNV is recommended in horses and birds, notably when an epidemic episode is identified at the European level.
By now, no case of WNV infection has been identified on the French territory after blood transfusion, SOT or HSCT. However, discussions are in progress for a more efficient organization of this surveillance, notably in collaboration with other European countries, in order to share epidemiological information in real time at the international level with blood and graft agencies and to improve the veterinary monitoring.
3. Dengue Virus
Dengue virus (DENV) is a single-stranded RNA virus belonging to the Flaviviridae family that exhibits four serotypes numbered from 1 to 4. The main characteristics of DENV infection are shown in Table 1. Originally, the virus reservoir was wild non-human primates infected by mosquito bites in forests (sylvatic cycle). Infected mosquitoes of the Stegomyia subgenus of Aedes (mainly Aedes aegypti and Aedes albopictus) are capable of biting and infecting humans, but uninfected mosquitoes can also be infected while blood feeding in viremic humans. The resulting 'human-mosquito-human' urban cycle is extremely rapid and efficient, and is now responsible for the vast majority of human cases. The current global burden of dengue fever is considerable: 2.5 billion people in over 100 countries are exposed; 50 to 100 million DENV infections occur each year, with around 20,000 fatal cases [21]. Although frequently asymptomatic or presenting as a self-limited mild fever, dengue fever may be life-threatening mainly linked to capillary leak syndrome that can lead to shock and death, particularly in children from low-resource backgrounds. DENV circulates mainly in intertropical regions, but over the past 10 years it has spread dramatically to temperate regions, due to increased human and commercial exchanges, with a probable contribution from global warming, which has extended both the potential Aedes breeding areas and the mosquito activity period [22].
Despite the wide distribution of this “old” infection and the fact that the virus can be present for about one week in the blood of infected patients, the risk of dengue fever as a transfusion- or graft-transmitted disease emerged only recently [23].The first documented case of post-transfusion dengue was observed in Hong-Kong in 2002 but was published only in 2008 [24]. Between 2002 and 2019, a total of 7 papers reported on 15 cases of possible transmission of DENV to 15 recipients, with different levels of accountability [24,25,26,27,28,29,30]. All types of blood products were involved, with a majority of packed red cells. In terms of severity, 6 patients developed hemorrhagic dengue fever, 6 developed mild dengue fever, 2 remained asymptomatic, and the last case was not documented. In the two fatal cases, dengue fever was not deemed to be the cause of the death. Sabino et al. [29] showed that the risk of transmission was independent of the viral load measured in the blood product and much lower than that observed after mosquito bite. As for transplant-derived DENV infections, 10 cases of transmission from infected donors have been documented, involving 8 organ donors and 2 donors of bone marrow [31,32,33,34,35,36,37,38,39]. As shown in Table 3, 13 recipients were involved with a strong or very strong (same viral sequence between donor and receiver) accountability in 10 of them. The outcome was favorable in 10 of the 13 cases; at least one death could be attributed to the DENV infection (Table 3). A virological diagnosis was available in 7 of the 10 donors: 4 were positive for a direct test (NAT and/or NS1 antigen), 2 exhibited anti-DENV IgM antibodies and 1 was positive for both direct (NAT) and indirect (IgM) markers. DENV transmission was also observed after cornea graft [40]. The donor, a 76-year-old Indian, was deceased in a picture of hemorrhagic fever; although the donation was recused, the corneoscleral tissue was cultivated, leading to the identification by NAT of the presence of DENV RNA that was further typed 3.
In France, the epidemiological situation of dengue fever is particularly complex (Figure 1). In French West Indies, the 4 serotypes of DENV have been circulating since the end of the 1990s and caused several outbreaks, such as those observed in 2010 and 2013 [41]. In French Guiana, DENV serotypes 1-3 circulate actively. In these American French territories, Aedes aegypti is the main vector. In Indian Ocean Reunion island, a dengue fever epidemic broke out in 2018 (the former DENV outbreak lasted from 1978); initially, the main circulating serotype was DENV-2; however, since 2019, DENV-1 and DENV-3 serotypes have been increasingly common, and in 2020 the most frequently isolated serotype was DENV-1. Aedes albopictus is the most common vector. In French Polynesia, DENV is also endemic with co-circulation of the 4 serotypes; Aedes aegypti and Aedes polynesiensis are both responsible for transmission of different arboviruses including DENV [42]. In mainland France, the first autochthonous cases of dengue fever occurred in 2010 [43]. From 2010 to 2019, 11 clusters totaling 32 subjects were recorded. In 2022, 19 clusters of 48 subjects were identified in 6 different Departments. DENV-1 was identified in 10 cases and DENV-2 in 6 cases. When known, the index case was returning from an endemic area and was bitten by Aedes albopictus mosquitoes that transmitted the virus in the vicinity. Currently, control strategies include systematic inquiries in the cluster areas, vector control operations, door-to-door information of local residents, and briefing of general practitioners for tracking mild cases. Despite these, it is more and more likely that the virus becomes endemic in mosquitoes.
The French HCSP recommended the following rules for the safety of blood products, SOT and HSCT regarding the transmission of DENV:
- –
- When a case or a cluster of dengue fever is identified in an endemic area, ID-NAT screening must be performed for blood donations at the Department level. When positive, the products must be discarded and the donor is deferred 28 days from the date of the end of the symptoms. For donors of solid organs and bone marrow present in the cluster areas or having stayed there, PCR and IgM/IgG serology must be performed close to the time of the donation. In case of positivity of one of these markers, it is recommended for living donors to postpone the graft or to use another donor if available; in deceased donors, it is recommended to discard the organs, except in case of vital emergency for the recipient for which a benefit-risk evaluation must be performed; if organs are transplanted, a specific follow-up of the recipient is required [44].
- –
- In clusters of autochthonous dengue in mainland France, blood collections must be postponed in the area, donors living or having stayed in this area must be discarded from blood donation for 28 days and blood products already collected in this area and not treated by the Intercept® process must be placed in quarantine in order to be tested by ID-NAT; by contrast, due to the very low risk of selecting a positive donor of solid organ or bone marrow, no specific information is done in this context [45].
4. Tick-Borne Encephalitis Virus
Tick-borne encephalitis virus (TBEV) is a single-stranded RNA virus belonging to the Flaviviridae family; within the TBEV viral species, three main subtypes are defined by the International Committee on Taxonomy of Viruses: the European TBEV (TBEV-EU), the Siberian TBEV (TBEV-Sib), and the Far Eastern TBEV (TBEV-FE). The main characteristics of TBEV infection are shown in Table 1. Ticks belonging to Ixodes ricinus and Ixodes persulcatus species are considered as the main natural vectors, but Dermacentor reticulatus was recently shown to be also an effective vector of TBEV [46]. The geographical distribution of TBEV is Europe and Asia (Figure 3) [47]. According to the stages of development of the tick, the natural reservoir of TBEV is mainly constituted by small rodents, birds and wild ungulates (mainly cervids) that are present in the natural environment of endemic areas (mainly forests and grassland areas with sufficient rainfall) [48]. Ticks can also get the virus transtadially (from larva to nymph to adult ticks), transovarially (from adult female tick to eggs), or when cofeeding on animals. Humans and domestic mammals, including dogs, goats, sheep and cows, may be contaminated by tick bites. Besides tick bites, humans can be infected by alimentary route via unpasteurized milk or milk products from animal origin (for reviews, see [49,50]).
Data on transmission of TBEV by products of human origin are scarce [50]. In 1989, Wahlberg et al. [51] reported in Finland one case of transmission of TBEV by blood transfusion to two recipients (year not mentioned between 1959 and 1987). The donor was sampled a few hours before the onset of clinical symptoms. The first recipient exhibited symptoms the day after transfusion while the second one showed a typical biphasic infection with fever the day after transfusion and a neurological episode 14 days later. TBEV infection was confirmed in both patients. No further case of TBEV transmission via blood products was recorded. As for SOT, Lipowski et al. [52] reported in 2017 in Poland three fatal cases of TBEV infection in recipients (liver and 2 kidneys) from a donor deceased following car-crash and living in a region endemic for TBEV. Symptoms appeared between 17 and 49 days post transplantation and presented as sepsis and meningitis in the liver recipient and encephalitis in the kidney recipients. All three patients died. By contrast to natural tick-borne encephalitis, the infection course was monophasic in the three cases and no abnormality was observed in the cerebrospinal fluid (CSF) for 2 of the 3 patients, which could have resulted from immune suppression. The diagnosis was performed retrospectively, based on next generation sequencing that showed the presence of TBEV genome in brain or CSF of the three recipients. Sequences of TBEV were also detected by RT-PCR in the brain (donor and two recipients) or CSF (one recipient), with similar sequences for the 4 patients.
In mainland France, TBEV infection is mostly limited to three administrative regions of the East of the country (Grand-Est, Bourgogne-Franche-Comté and Auvergne-Rhône-Alpes) (Figure 1 and Figure 3). In April 2020, an outbreak of encephalitis and meningoencephalitis occurred in the Ain Department (Auvergne-Rhône-Alpes region) where TBEV had never been detected before. Following a public health alert, 43 patients with encephalitis, meningoencephalitis, or flu-like symptoms were recorded; all of them but one had eaten fresh goat cheese made of raw milk originating from a single local producer. The alimentary transmission was evidenced by the presence of TBEV in a batch of cheese and goat milk [53]. Since June 2020, TBEV infection has become a notifiable disease in France [54]. From May 2021 to May 2023, 71 cases of TBEV infection were notified to SpF; 61 of them were autochthonous (including 17 in Departments where the virus had never been detected before) whereas 10 were acquired in other European countries. The latter observations are indicative of an increase in reported cases of TBEV infections in France since a few years, as also observed in all Europe [48], with many drivers that could explain this expansion including climate warming, modifications in human habits and ecosystem changes [55].
The French HCSP recommended the following rules for the safety of blood products, SOT and HSCT regarding the transmission of TBEV [56]:
- –
- for blood products, donors having experienced a tick bite in the 28 days preceding the donation in an area known to be at risk for TBEV (in or out of France) during the period of virus circulation (March to November) must be excluded for 28 days after the tick bite’s date. In addition, blood collection is interrupted in areas where a source of foodborne outbreak of TBEV is recognized, with quarantine of blood products already collected and not secured by the Intercept® process, until tested negative by TBEV NAT;
- –
- for SOT and HSCT, living donors staying or traveling in at-risk areas for TBEV must be made aware of the risks of tick bites and of the consumption of unpasteurized milk and milk products from March to November to avoid contamination. All living donors should be questioned for a possible recent tick bite in a zone at risk for TBEV when completing the pre-donation check-up list. In case of positive answer to this question, living donors must be tested for TBEV (NAT and IgM/IgG serology) prior to the gift; if at least one of these tests is positive, it is recommended to postpone the graft or to select another donor if available. For deceased donors recently exposed to a tick bite, when this information can be recorded from his/her relatives or after skin inspection, as it may be difficult to obtain virological tests prior to the transplantation, it is recommended to inform the recipient(s) and their medical team of the potential risk of TBEV infection and to perform specific virological tests in case of fever or neurological symptoms in the two months following the transplantation.
5. Other Arboviruses Circulating in France
5.1. Usutu Virus
Usutu virus (USUV) is a single-stranded RNA virus belonging to the Flaviviridae family. This emerging arbovirus was first isolated in 1959 in Eswatini (ex-Swaziland). Restricted for a long time to sub-Saharan Africa, USUV was introduced to Europe in 1996 with approximately one hundred cases reported so far in this area [57]. As shown in Table 1, its characteristics are very close to that of WNV: similar reservoirs (wild birds), similar vectors, humans and other mammals (including horses and wild boars) as dead-end hosts, similar clinical pictures. It was first isolated in Southern France (Occitanie region) in birds in 2015 [58] and in humans in 2016 [59]. The second French case occurred in 2022 in the Aquitaine region; because former vaccination against yellow fever and dengue infection in this patient, the diagnosis of USUV infection was made possible only by seroneutralisation assay. So far USUV was not shown to be transmitted via products of human origin. However, following its spread in many European countries via different lineages, attention should be paid to this risk in the future [60].
5.2. Chikungunya Virus
Chikungunya virus (CHIKV) is a single-stranded RNA virus belonging to the Togaviridae family and Alphavirus genus. As shown in Table 1, CHIKV is transmitted by Aedes mosquitoes and is responsible for a high percentage of symptomatic forms mainly represented by joint pains that can evolve to chronic rheumatism. First isolated in 1952 in Tanzania in a patient suffering of arthralgia (the name “chikungunya” derives from a word in the Kimakonde language meaning “to be bent with pain”), the virus was rapidly shown to circulate in other regions of Africa and Asia. Different lineages have been described according to their geographical origin: West African (WA), East, Central and South African (ECSA) and Asian lineages. In 2004, an “epidemic lineage” derived from ESCA strains and named Indian Ocean lineage (IOL) emerged in Kenya; due to mutations of envelope proteins that facilitate its adaptation to Aedes albopictus, this lineage disseminated to South-East Asia, Indian subcontinent, territories of Indian Ocean and Pacific Ocean, and Europe [61,62]. In parallel, strains derived from the original ESCA lineage and the Asian lineage disseminated to the American continent with Aedes aegypti as main vector. CHIKV is genetically close to other viruses of the Alphavirus genus such as O’Nyong Nyong, Ross River and Mayaro viruses.
As with DENV, the initial sylvatic cycle involved forest mosquitoes and non-human primates, but the 'human-aedes-human' urban cycle is now responsible for the majority of epidemic cases in humans. Human-to-human transmission of CHIKV is exceptional, with a few cases of infection in utero or during childbirth [63]. The virus has never been isolated from sperm or human milk. Despite the probable exposure of recipients to infected products, products of human origin have never been found to be responsible for human contamination.
In France, different outbreaks of CHIKV infections were recorded:
- –
- –
- The French Territories in the Americas experienced also an important CHIKV outbreak in 2013-2014 with respectively 72500, 81200 and 15000 cases in Martinique, Guadeloupe, and French Guiana. No significant re-emergence of the virus was further observed.
- –
- In French Polynesia, a CHIKV outbreak developed in 2014-2015.
- –
Despite the absence of demonstrated transmission of CHIKV by blood products, CHIKV NAT was implemented in the overseas territories and also in the mainland departments experiencing cases of autochthonous infections. Persons returning from regions where the virus circulates are excluded from blood donation for 28 days. The same nonspecific measures as for dengue fever are recommended for CHIKV infection (see above). For donors of SOT and HSCT present or having stayed in these areas, NAT and IgM/IgG serology must be performed close to the time of the donation. In case of positivity of one of these markers, it is recommended for living donors to postpone the graft or to select another donor if available. For HSCT, if it is not possible to postpone or find another donor, a risk-based approach and a specific follow-up of the recipient are required. In deceased donors, it is recommended to discard the organs, except in case of vital emergency in the recipient for whom a benefit-risk evaluation must be performed; if the organs are used, a specific follow-up of the recipient is required [69]. These guidelines are founded only on the precautionary principle since it has been assessed that transplant recipients who developed CHIKV infection after mosquito bite did not present with severe infection [70,71].
5.3. Zika Virus
After first isolation of Zika virus (ZIKV) in a monkey in the Zika forest, Ouganda, in 1947, and in Aedes africanus mosquito, which suggested its arboviral origin, the first case of human infection was reported in 1952 [72]. Again, the epidemiological cycle of Zika changed from its original sylvatic cycle to a predominantly "human-aedes-human" urban cycle. As shown in Table 1, ZIKV is transmitted by various vectors, including Aedes aegypti and Aedes albopictus. ZIKV raised relatively little medical attention until the report of an outbreak in Micronesia in 2007 [73], and of a second one in French Polynesia in October 2013 [74], which allowed to describe the usual mild clinical presentation of the disease when symptomatic. The second outbreak allowed also to identify an increased risk of perinatal transmission [75] and of Guillain-Barré syndrome [76,77]. Then CHIKV reached New Caledonia in January 2014 and South America and Caribbean in 2015-2016 [78,79]. The latter outbreak, which led to the issue of a Public Health Emergency of International Concern by the World Health Organization (WHO) in February 2016, was a significant shift in the epidemiology of Zika infection: (i) there was a huge extension to vast territories of the American continent; (ii) after a first report in 2011 [80], the sexual transmission of the virus via semen was confirmed [81]; (iii) the vertical transmission was shown to happen frequently and description of severe disease in the newborn was reported, with a notably high proportion of microcephaly and other malformations [82,83,84]. ZIKV is a genetically versatile virus with two major lineages: the African lineage that was predominant up to the 1970s and that was mostly transmitted to humans via a sylvatic cycle, and the Asian lineage that adapted notably to Aedes aegypti and was responsible for large outbreaks via an urban cycle in the South-East Asia, the Pacific Territories and the American continent [85,86].
In terms of blood safety, ZIKV was shown to be able to persist in some cases for up to two months after the onset of symptoms in serum or plasma [87]. To date, four cases of transfusion-borne ZIKV infection have been reported [88,89,90], all of them in Brazil: three occurred after the transfusion of platelets and one after the transfusion of packed red cells. Of the three living transfusion recipients, none displayed any clinical sign of ZIKV infection. After implementation of NAT for preventing the transfusion of blood products contaminated by circulating arboviruses (DENV, CHIKV and ZIKV) in French Polynesia between 2012 and 2018, it was shown that this measure excluded five blood donations reactive for DENV RNA, 34 for CHIKV and 42 for ZIKV. As Zika screening could not have been implemented before the third month of the outbreak, 36 blood products from ZIKV-infected donors were transfused to 26 recipients, which resulted in no transfusion-transmitted ZIKV infection [91]. Altogether, these data illustrate that, if ZIKV could be transmitted very unfrequently via labile blood products, the clinical consequences remain limited. As for solid organs, bone marrow and tissues, no case of ZIKV infection has been yet reported.
As described above, the outbreaks of Zika having occurred in the French overseas territories (French Polynesia in 2013, New Caledonia in 2014, and French territories in the Americas in 2015-2016) contributed largely to the description of the clinical and epidemiological characteristics of this emerging disease. Interestingly, the first episode of Zika in Europe was reported in Southern France (Provence-Alpes-Côte d’Azur region) in 2019 [92,93]. The index patient exhibited fever, rash, and fatigue and was tested positive for ZIKV by NAT in blood two days after the onset of symptoms; IgM antibodies were also positive together with ZIKV-specific neutralizing antibodies in a blood sample collected 12 days after symptom onset. The door-to-door campaign conducted in the vicinity of the index case led to identify two more healthy patients who had developed fever and rash 8 days before the onset of the rash in the index case and who lived within 90 meters from the index case; both of them were also tested positive for ZIKV IgM and IgG and were confirmed positive to ZIKV by seroneutralisation. None of the 3 patients or their partners reported a recent travel to a ZIKV-endemic area. No further case of autochthonous Zika was reported in mainland France during the following years.
Since February 2016, Zika has become a notifiable disease in France [94].ZIKV NAT was implemented for blood donors in the oversea territories where the virus circulated largely (New Caledonia, French Polynesia, and French America Departments). Persons returning from regions where the virus circulates are excluded for 28 days from blood donation. During the outbreaks, the same nonspecific measures as for dengue fever are recommended for CHIKV infection (see above). Despite the absence of reported cases of ZIKV transmission in SOT or HSCT, similar specific measures to those recommended for CHIKV infection are recommended (see above). Following the autochthonous episode notified in mainland France in 2019, due to the limited size of the outbreak (3 cases) without further development, the HCSP required no specific measure for both blood safety, and organ and cell grafts [95].
6. Concludings Remarks
This review provides an overview of the main arboviral risks observed in mainland and overseas France, with a particular focus on the safety of SOT and HCST. With global climate change, the dramatic expansion of the range of certain competent vectors, the growing internationalization of exchanges of people and goods, and the increased demands in terms of the quality of products of human origin, the viral risks multiply, adding difficulty to the selection of donors of solid organs or hematopoietic stem-cells. At the same time, the need for products of human origin is increasing as a result of advances in medical care for many chronic diseases, and the multiplication of donor selection criteria, particularly from a virological point of view, may limit the availability of organs and cells, requiring a careful assessment of the benefit-risk ratio in each individual situation. This overview illustrates some of the diversity of arboviral risk within a single country. In France, the role of the HCSP, in collaboration with other national agencies and the National reference center for arboviruses, is to define clear, pragmatic selection rules that need to be constantly updated as outbreaks occur in different regions, with the aim to propose adequate testing of donors and to help the clinicians to make informed choices with regard to the selection of donors and follow-up of recipients. After each new viral episode, the current recommendations need to be checked to ensure they are still relevant; in addition, when the circulation of a viral agent ceases, certain measures need to be scaled back, which is not always easy to make health authorities understand. As arboviral diseases are mainly zoonoses, a "One Health" approach is imperative. Finally, international cooperation (WHO and ECDC in particular) is desirable in order to standardize recommendations between countries, as viruses, birds and even insects know no borders, and the diversity of recommendations can be detrimental to exchanges of products of human origin between foreign partners involved in transplantation. We hope that this review will contribute to this joint effort.
Acknowledgments
The authors acknowledge all the experts who participated to the discussion and reading/writing of the advices cited in this review with a special attention to Benoit Averland, Nathalie Boulanger, Dominique Challine, Benoit Clavier, Bernard Clero, Catherine Faucher, Florence Fouque, Eliane Garrabé, Yves Hansmann, Edmond-Luc Henry, Sabine Henry, Alexandra Kerléguer, Jean-Jacques Lataillade, Didier Lecointe, Alexandra Mailles, Anne Mendes, Pascal Morel, Elisabeth Nicand, Harold Noël, Pascale Richard, Claire Rieux, Anne-Marie Roque-Afonso, Isabelle Sainte-Marie, Renaud Verdon, and Aliénor Xhaard.
Conflicts of Interest
The authors declare that they have no competing interest regarding the subject of this review.
References
- Devillers J, David JP, Barrès B; et al. Integrated plan of insecticide resistance surveillance in mosquito vectors in France. Insects. 2023, 14, 457. [Google Scholar] [CrossRef] [PubMed]
- Robert MA, Stewart-Ibarra AM, Estallo EL. Climate change and viral emergence: Evidence from Aedes-borne arboviruses. Curr. Opin. Virol. 2020, 40, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Chancey C, Grinev A, Volkova E, Rios M. The global ecology and epidemiology of West Nile virus. Biomed. Res. Int. 2015, 2015, 376230. [Google Scholar] [CrossRef]
- Petersen LR, Brault AC, Nasci RS. West Nile virus: Review of the literature. JAMA. 2013, 310, 308–315. [Google Scholar] [CrossRef]
- Nash D, Mostashari F, Fine A; et al. The outbreak of West Nile virus infection in the New York City area in 1999. N Engl J Med. 2001, 344, 1807–1814. [Google Scholar] [CrossRef]
- Pealer LN, Marfin AA, Petersen LR; et al. Transmission of West Nile virus through blood transfusion in the United States in 2002. N Engl J Med. 2003, 349, 1236. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Update: Investigations of West Nile virus infections in recipients of organ transplantation and blood transfusion–Michigan, 2002. Morb Mortal Wkly Rep. 2002, 51, 879. [Google Scholar]
- Iwamoto M, Jernigan DB, Guasch A; et al. Transmission of West Nile virus from an organ donor to four transplant recipients. N. Engl. J. Med. 2003, 348, 2196. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Fatal West Nile virus infection after probable transfusion-associated transmission--Colorado, 2012. Morb Mortal Wkly Rep. 2013, 62, 622–624. [Google Scholar]
- Pervanidou D, Detsis M, Danis K; et al. West Nile virus outbreak in humans, Greece, 2012: Third consecutive year of local transmission. Euro Surveill. 2014, 19, 20758. [Google Scholar] [CrossRef]
- Winston DJ, Vikram HR, Rabe IB; et al. Donor-derived West Nile virus infection in solid organ transplant recipients: Report of four additional cases and review of clinical, diagnostic, and therapeutic features. Transplantation. 2014, 97, 881–889. [Google Scholar] [CrossRef]
- Anesi JA, Silveira FP; AST Infectious Diseases Community of Practice. Arenaviruses and West Nile Virus in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13576. [Google Scholar] [CrossRef]
- Morelli MC, Sambri V, Grazi GL; et al. Absence of neuroinvasive disease in a liver transplant recipient who acquired West Nile virus (WNV) infection from the organ donor and who received WNV antibodies prophylactically. Clin. Infect. Dis. 2010, 51, e34–7. [Google Scholar] [CrossRef]
- Inojosa WO, Scotton PG, Fuser R; et al. West Nile virus transmission through organ transplantation in north-eastern Italy: A case report and implications for pre-procurement screening. Infection. 2012, 40, 557–562. [Google Scholar] [CrossRef]
- Barzon L, Montarsi F, Quaranta E; et al. Early start of seasonal transmission and co-circulation of West Nile virus lineage 2 and a newly introduced lineage 1 strain, northern Italy, June 2022. Euro Surveill. 2022, 27, 2200548. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Avis du 7 novembre 2022 sur la sécurisation des produits du corps humain dans un contexte de circulation du virus West Nile en France métropolitaine. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=1259.
- Haut Conseil de la Santé Publique. Statement on measures of security for human body products owing to a human case report of West Nile virus (WNV) infection in mainland France outside the seasonal alert period. 13th January 2023. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=1270.
- Haut Conseil de la Santé Publique. Avis du 28 mars 2023 sur la sécurisation des éléments et produits issus du corps humain en prévision de la circulation du virus West Nile en France métropolitaine. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=1284.
- Haut Conseil de la Santé Publique. Avis du 7 février 2020 relatif à l’inscription à la liste des maladies à déclaration obligatoire de l’infection due au virus West-Nile. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=843.
- Haut Conseil de la Santé Publique. Liste des pays à risque de transmission du virus West Nile (WNV) pour les produits du corps humain, saison 2023. Avis du 24 mai 2023. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=1307.
- Bhatt S, Gething PW, Brady OJ; et al. The global distribution and burden of dengue. Nature. 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Gwee XWS, Chua PEY, Pang J. Global dengue importation: A systematic review. BMC Infect. Dis. 2021, 21, 1078. [Google Scholar] [CrossRef]
- Pozzetto B, Memmi M, Garraud O. Is. transfusion-transmitted dengue fever a potential public health threat? World J. Virol. 2015, 4, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Chuang VWM, Wong TY, Leung YH; et al. Review of dengue fever cases in Hong Kong during 1998 to 2005. Hong Kong Med J. 2008, 14, 170–177. [Google Scholar]
- Tambyah PA, Koay ESC, Poon MLM, Lin RVTP, Ong BKC, Transfusion-Transmitted Dengue Infection Study Group. Dengue hemorrhagic fever transmitted by blood transfusion. N. Engl. J. Med. 2008, 359, 1526–1527. [Google Scholar] [CrossRef]
- Stramer SL, Linnen JM, Carrick JM; et al. Dengue viremia in blood donors identified by RNA and detection of dengue transfusion transmission during the 2007 dengue outbreak in Puerto Rico. Transfusion. 2012, 52, 1657–1666. [Google Scholar] [CrossRef] [PubMed]
- Matos D, Tomashek KM, Perez-Padilla J; et al. Probable and possible transfusion-transmitted dengue associated with NS1 antigen-negative but RNA confirmed-positive red blood cells. Transfusion. 2016, 56, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Oh HB, Muthu V, Daruwalla ZJ, Lee SY, Koay ES, Tambyah PA. Bitten by a bug or a bag? Transfusion-transmitted dengue: A rare complication in the bleeding surgical patient. Transfusion. 2015, 55, 1655–1661. [Google Scholar] [CrossRef]
- Sabino EC, Loureiro P, Lopes ME; et al. Transfusion-transmitted dengue and associated clinical symptoms during the 2012 epidemic in Brazil. J Infect Dis. 2016, 213, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Levi JE, Nishiya A, Félix AC, Salles NA; et al. Real-time symptomatic case of transfusion-transmitted dengue. Transfusion. 2015, 55, 961–964. [Google Scholar] [CrossRef]
- Rigau-Pérez JG, Vorndam AV, Clark GG. The dengue and dengue hemorrhagic fever epidemic in Puerto Rico, 1994-1995. Am J Trop Med Hyg. 2001, 64, 67–74. [Google Scholar] [CrossRef]
- Tan FL-S, Loh DLSK, Prabhakaran K, Tambyah PA, Yap H-K. Dengue haemorrhagic fever after living donor renal transplantation. Nephrol. Dial. Transplant. 2005, 20, 447–448. [Google Scholar] [CrossRef]
- Tangnararatchakit K, Tirapanich W, Tapaneya-Olarn W; et al. Severe nonfebrile dengue infection in an adolescent after postoperative kidney transplantation: A case report. Transplant. Proc. 2012, 44, 303–306. [Google Scholar] [CrossRef]
- Saigal S, Choudhary NS, Saraf N, Kataria S, Mohanka R, Soin AS. Transmission of dengue virus from a donor to a recipient after living donor liver transplantation. Liver Transpl. 2013, 19, 1413–1414. [Google Scholar] [CrossRef]
- Punzel M, Korukluoğlu G, Caglayik DY; et al. Dengue virus transmission by blood stem cell donor after travel to Sri Lanka; Germany, 2013. Emerg Infect Dis. 2014, 20, 1366–1369. [Google Scholar] [CrossRef]
- Gupta RK, Gupta G, Chorasiya VK; et al. Dengue virus transmission from living donor to recipient in liver transplantation: A case report. J. Clin. Exp. Hepatol. 2016, 6, 59–61. [Google Scholar] [CrossRef] [PubMed]
- Rosso F, Pineda JC, Sanz AM, Cedano JA, Caicedo LA. Transmission of dengue virus from deceased donors to solid organ transplant recipients: Case report and literature review. Braz. J. Infect. 2018, 22, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Shaji Mathew J, Menon VP, Menon VP; et al. Dengue virus transmission from live donor liver graft. Am. J. Transplant. 2019, 19, 1838–1846. [Google Scholar] [CrossRef]
- Lecadieu A, Teysseyre L, Larsen K; et al. Case report: Transmission of dengue virus from a deceased donor to a kidney transplant recipient previously infected by dengue virus. Am. J. Trop. Med. Hyg. 2021, 104, 2199–2201. [Google Scholar] [CrossRef] [PubMed]
- Janani MK, Durgadevi P, Padmapriya J, Malathi J, Kulandai LT, Rao Madhavan HN. First report on detection of dengue virus in the donor cornea. Cornea. 2018, 37, 1586–1589. [Google Scholar] [CrossRef] [PubMed]
- L’Azou M, Jean-Marie J, Bessaud M; et al. Dengue seroprevalence in the French West Indies: A prospective study in adult blood donors. Am. J. Trop. Med. Hyg. 2015, 92, 1137–1140. [Google Scholar] [CrossRef] [PubMed]
- Richard V, Cao-Lormeau VM. Mosquito vectors of arboviruses in French Polynesia. New Microbes New Infect. 2019, 31, 100569. [Google Scholar] [CrossRef]
- La Ruche G, Souarès Y, Armengaud A; et al. First two autochthonous dengue virus infections in metropolitan France, September 2010. Euro Surveill. 2010, 15, 19676. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Avis du 28 novembre 2020 relatif à l’actualisation des mesures de prévention vis-à-vis du virus de la dengue à appliquer aux produits issus du corps humain dans les Antilles françaises. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=953.
- Haut Conseil de la Santé Publique. Avis du 19 octobre 2022 sur les mesures de prévention pour la sécurité infectieuse transfusionnelle et de la greffe à la suite de cas de dengue autochtones dans le sud de la France. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=1258.
- Ličková M, Fumačová Havlíková S, Sláviková M, Slovák M, Drexler JF, Klempa B. Dermacentor reticulatus is a vector of tick-borne encephalitis virus. Ticks Tick. Borne Dis. 2020, 11, 101414. [Google Scholar] [CrossRef]
- Kunze M, Banović P, Bogovič P; et al. Recommendations to improve tick-borne encephalitis surveillance and vaccine uptake in Europe. Microorganisms. 2022, 10, 1283. [Google Scholar] [CrossRef]
- Michelitsch A, Wernike K, Klaus C, Dobler G, Beer M. Exploring the reservoir hosts of tick-borne encephalitis virus. Viruses. 2019, 11, 669. [Google Scholar] [CrossRef] [PubMed]
- Ličková M, Fumačová Havlíková S, Sláviková M, Klempa B. Alimentary infections by tick-borne encephalitis virus. Viruses. 2021, 14, 56. [Google Scholar] [CrossRef]
- Martello E, Gillingham EL, Phalkey R; et al. Systematic review on the non-vectorial transmission of tick-borne encephalitis virus (TBEv). Ticks Tick. Borne Dis. 2022, 13, 102028. [Google Scholar] [CrossRef] [PubMed]
- Wahlberg P, Saikku P, Brummer-Korvenkontio M. Tick-borne viral encephalitis in Finland. The clinical features of Kumlinge disease during 1959-1987. J Intern Med. 1989, 225, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Lipowski D, Popiel M, Perlejewski K; et al. A cluster of fatal tick-borne encephalitis virus infection in organ transplant setting. J. Infect. Dis. 2017, 215, 896–901. [Google Scholar] [CrossRef]
- Gonzalez G, Bournez L, Moraes RA; et al. A One-health approach to investigating an outbreak of alimentary tick-borne encephalitis in a non-endemic area in France (Ain, Eastern France): A longitudinal serological study in livestock, detection in ticks, and the first tick-borne encephalitis virus isolation and molecular characterisation. Front. Microbiol. 2022, 13, 863725. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Inscription de l’encéphalite à tiques sur la liste des maladies à déclaration obligatoire. 5 juin 2020. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=856.
- Saegerman C, Humblet MF, Leandri M; et al. First Expert Elicitation of knowledge on possible drivers of observed increasing human cases of tick-borne encephalitis in Europe. Viruses. 2023, 15, 791. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Avis du 23 juillet 2020 relatif aux risques transfusionnels et de contamination des greffons induits par le virus de l’encéphalite à tiques (TBEV) ; précautions à prendre lors de foyers infectieux. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=895.
- Vilibic-Cavlek T, Petrovic T, Savic V; et al. Epidemiology of Usutu virus: The European scenario. Pathogens. 2020, 9, 699. [Google Scholar] [CrossRef]
- Lecollinet S, Blanchard Y, Manson C; et al. Dual emergence of Usutu virus in common blackbirds, Eastern France, 2015. Emerg Infect Dis. 2016, 22, 2225. [Google Scholar] [CrossRef]
- Simonin Y, Sillam, O, Carles MJ; et al. Human Usutu virus infection with atypical neurologic presentation, Montpellier, France, 2016. Emerg Infect Dis. 2018, 24, 875–878. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Avis du 28 avril 2023 sur la sécurisation des produits issus du corps humain en prévision de cas d’infection à virus West Nile. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=1284.
- Desdouits M, Kamgang B, Berthet N; et al. Genetic characterization of chikungunya virus in the Central African Republic. Infect. Genet. Evol. 2015, 33, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Sharif N, Sarkar MK, Ferdous RN; et al. Molecular epidemiology, evolution and reemergence of Chikungunya virus in South Asia. Front. Microbiol. 2021, 12, 689979. [Google Scholar] [CrossRef]
- Fritel X, Rollot O, Gerardin P; et al. Chikungunya virus infection during pregnancy, Reunion, France, 2006. Emerg Infect Dis. 2010, 16, 418–425. [Google Scholar] [CrossRef]
- Josseran L, Paquet C, Zehgnoun A; et al. Chikungunya disease outbreak, Reunion Island. Emerg. Infect. Dis. 2006, 12, 1994–1995. [Google Scholar] [CrossRef] [PubMed]
- Borgherini G, Poubeau P, Staikowsky F; et al. Outbreak of chikungunya on Reunion Island: Early clinical and laboratory features in 157 adult patients. Clin. Infect. Dis. 2007, 44, 1401–1407. [Google Scholar] [CrossRef]
- Grandadam M, Caro V, Plumet S; et al. Chikungunya virus, southeastern France. Emerg. Infect. Dis. 2011, 17, 910–913. [Google Scholar] [CrossRef]
- Rezza G, Nicoletti L, Angelini R; et al. Infection with Chikungunya virus in Italy: An outbreak in a temperate region. Lancet. 2007, 370, 1840–1846. [Google Scholar] [CrossRef]
- Watson, R. Chikungunya fever is transmitted locally in Europe for first time. Br. Med. J. 2007, 335, 532–533. [Google Scholar] [CrossRef]
- Haut Conseil de la Santé Publique. Dengue et chikungunya : Mesures pour la sécurité transfusionnelle et des greffes. 14 juin 2019. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=722.
- Pierrotti LC, Lopes MIBF, Nascimento APD; et al. Chikungunya in kidney transplant recipients: A series of cases. Int. J. Infect. Dis. 2017, 64, 96–99. [Google Scholar] [CrossRef]
- Rosso F, Rodríguez S, Cedano JA, Mora BL, Moncada PA, Velez JD. Chikungunya in solid organ transplant recipients, a case series and literature review. Transpl. Infect. Dis. 2018, 20, e12978. [Google Scholar] [CrossRef]
- Smithburn, KC. Neutralizing antibodies against certain recently isolated viruses in the sera of human beings residing in East Africa. Immunol. 1952, 69, 22334. [Google Scholar] [CrossRef]
- Duffy MR, Chen TH, Hancock WT; et al. Zika virus outbreak on Yap Island, Federated States of Micronesia. N. Eng. J. Med. 2009, 360, 2536–2543. [Google Scholar] [CrossRef] [PubMed]
- Musso D, Nilles EJ, Cao-Lormeau VM. Rapid spread of emerging Zika virus in the Pacific area. Clin. Microbiol. lnfect. 2014, 20, O595–O596. [Google Scholar] [CrossRef]
- Besnard M, Lastere S, Teissier A, Cao-Lormeau V, Musso D. Evidence of perinatal transmission of Zika virus. French Polynesia. December 2013 and February 2014. Euro Surveil. 2014, 9, 20751. [Google Scholar] [CrossRef]
- Petersen LR, Jamieson DJ, Honein MA. Zika virus. N. Engl. J. Med. 2016, 375, 294–295. [Google Scholar] [CrossRef]
- Cao-Lormeau VM, Blake A, Mons S; et al. Guillain-Barre syndrome outbreak associated with Zika virus infection in French Polynesia: A case-control study. Lancet. 2016, 387, 1531–1539. [Google Scholar] [CrossRef]
- Campos GS, Bandeira AC, Sardi Sl. Zika vírus outbreak, Bahia, Brazil. Emerg. Infect. Dis. 2015, 21, 1005–1006. [Google Scholar]
- Faria NR, Azevedo R, Kraemer MUG; et al. Zika virus in the Americas: Early epidemiological and genetic findings. Science. 2016, 352, 345–349. [Google Scholar] [CrossRef]
- Foy BD, Kobylinski KC. Chilson Foy JL; et al. Probable non-vector- borne transmission of Zika virus, Colorado, USA. Emerg. Infect. Dis. 2011, 17, 880–882. [Google Scholar] [CrossRef]
- Moreira J, Peixoto TM, Siqueira AM, Lamas CC. Sexually acquired Zika virus: A systematic review. Clin. Microbiol. Infect. 2017, 23, 296–305. [Google Scholar] [CrossRef]
- Funk AL, Hoen B, Vingdassalom I; et al. Reassessment of the risk of birth defects due to Zika virus in Guadeloupe, 2016. PLoS Negl Trop Dis. 2021, 15, e0009048. [Google Scholar] [CrossRef]
- Moore CA, Staples JE, Dobyns WB; et al. Characterizing the pattern of anomalies in congenital Zika syndrome for pediatric clinicians. JAMA Pediatr. 2017, 171, 288–295. [Google Scholar] [CrossRef]
- Hoen B, Schaub B, Funk AL; et al. Pregnancy outcomes after ZIKV infection in French Territories in the Americas. N. Engl. J. Med. 2018, 378, 985–94. [Google Scholar] [CrossRef] [PubMed]
- Nielsen-Saines K, Brasil P, Kerin T; et al. Delayed childhood neurodevelopment and neurosensory alterations in the second year of life in a prospective cohort of ZIKV-exposed children. Nat. Med. 2019, 25, 1213–1217. [Google Scholar] [CrossRef] [PubMed]
- Simonin Y, van Riel D, van de Perre P, Rockx B, Salinas S. Differential virulence between Asian and African lineages of Zika virus. PloS Negl. Trop. Dis. 2017, 11, e0005821. [CrossRef]
- Lustig Y, Mendelson E, Paran N, Melamed S, Schwartz E. Detection of Zika virus RNA in whole blood of imported Zika virus disease cases up to 2 months after symptom onset, Israel, December 2015 to April 2016. Euro Surveill 2016, 21, 30269. [Google Scholar] [CrossRef]
- Herriman, R. Transfusion-associated Zika virus reported in Brazil. Outbreak news today. December 18, 2015. http://outbreaknewstoday.com/transfusion-associated-zika-virus-reported-in-brazil-76935/.
- Barjas-Castro ML, Angerami RN, Cunha MS; et al. Probable transfusion-transmitted Zika virus in Brazil. Transfusion 2016, 56, 1684–1688. [Google Scholar] [CrossRef]
- Motta IJ, Spencer BR, Cordeiro da Silva SG; et al. Evidence for transmission of Zika virus by platelet transfusion. N. Engl. J. Med. 2016, 375, 1101–1103. [Google Scholar] [CrossRef]
- Beau F, Lastère S, Mallet HP, Mauguin S, Broult J, Laperche S. Impact on blood safety of the last arboviruses outbreaks in French Polynesia (2012-2018). Transfus Clin Biol. 2020, 27, 4–9. [Google Scholar] [CrossRef]
- Giron S, Franke F, Decoppet A; et al. Vector-borne transmission of Zika virus in Europe, southern France, August 2019. Euro Surveill. 2019, 24, 1900655. [Google Scholar] [CrossRef]
- Brady OG, Hay S. The first local cases of Zika virus in Europe. Lancet. 2019, 394, 1991–1992. [Google Scholar] [CrossRef] [PubMed]
- Haut Conseil de la Santé Publique. Infection par le virus Zika : Inscription sur la liste des maladies à déclaration obligatoire. 2 février 2016. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=539.
- Haut Conseil de la Santé Publique. Mesures de prévention pour la sécurité infectieuse transfusionnelle et de la greffe résultant de la circulation de virus Zika à la suite de cas autochtones en France métropolitaine. 22 novembre 2019. https://www.hcsp.fr/explore.cgi/avisrapportsdomaine?clefr=752.
Figure 1.
Location of French overseas territories and administrative regions. Ultramarine departments are shown in blue. Ultramarine collectivities and territories are shown in magenta (French Austral and Antarctic Territories not shown). The embedded map shows the 18 French administrative regions.
Figure 1.
Location of French overseas territories and administrative regions. Ultramarine departments are shown in blue. Ultramarine collectivities and territories are shown in magenta (French Austral and Antarctic Territories not shown). The embedded map shows the 18 French administrative regions.
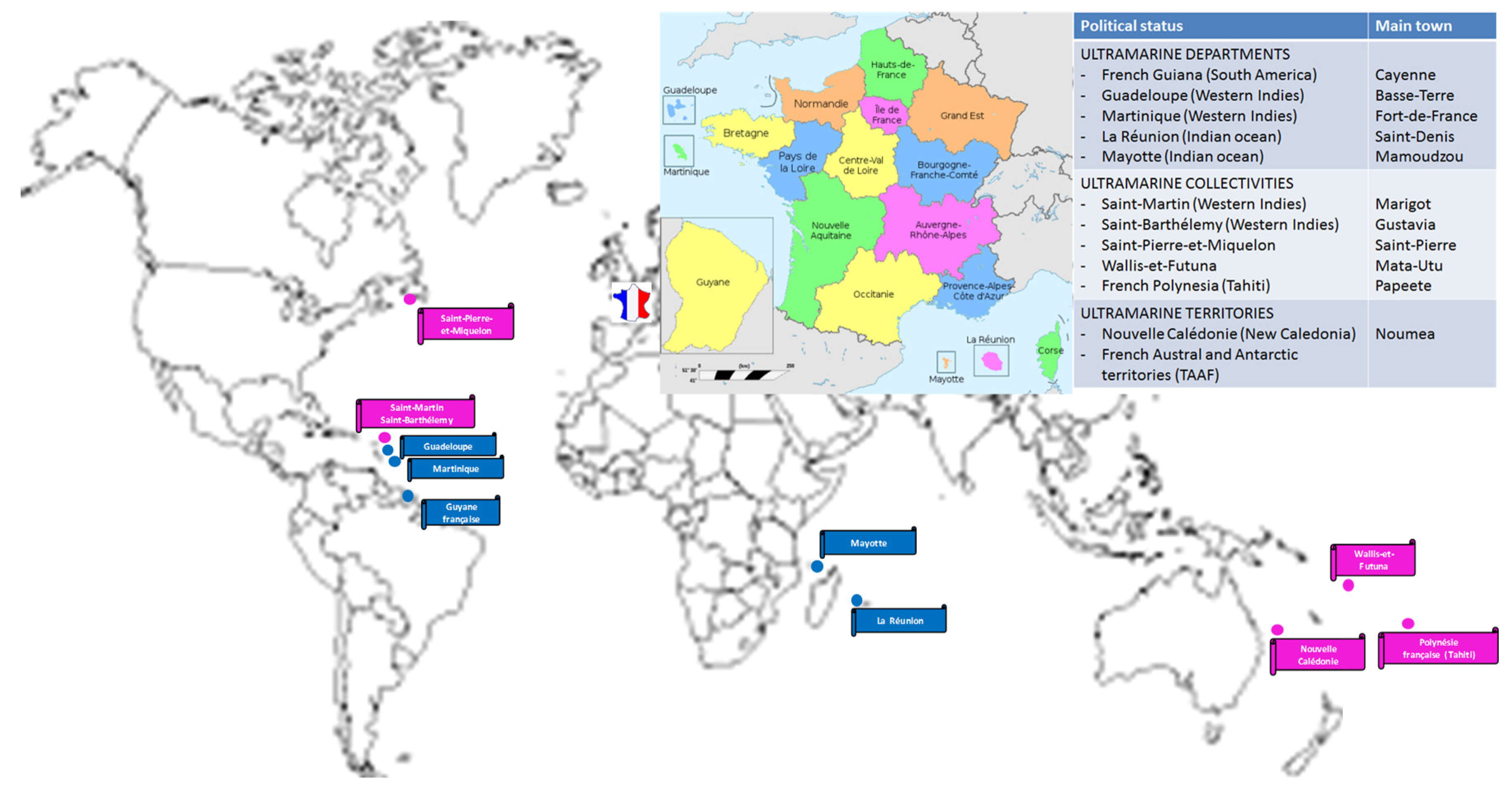
Figure 2.
Number of annual cases of West Nile virus infection identified in humans, horses and birds in mainland France, 2001-2022. (source: Santé publique France).
Figure 2.
Number of annual cases of West Nile virus infection identified in humans, horses and birds in mainland France, 2001-2022. (source: Santé publique France).
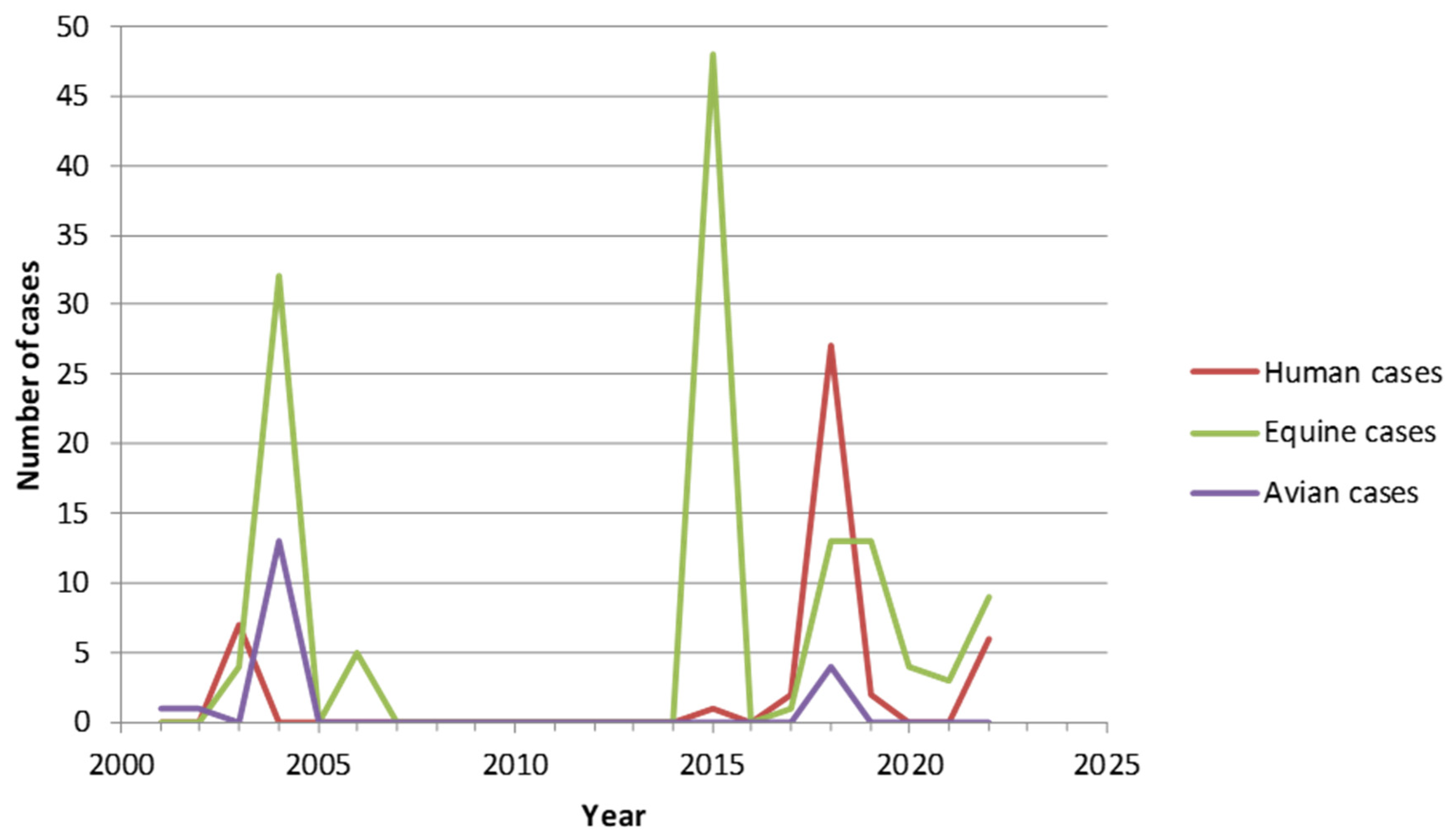
Figure 3.
Worldwide distribution of tick-borne encephalitis virus (TBEV). Source: CDC, March 7 2022 (available at: https://www.cdc.gov/tick-borne-encephalitis/geographic-distribution/index.html#:~:text=Highly%20endemic%20regions%20include%20Carinthia,%2C%20Tyrol%2C%20and%20Vorarlberg%20Provinces.&text=Almost%20all%20of%20the%20country,some%20small%20geographically%20dispersed%20areas).
Figure 3.
Worldwide distribution of tick-borne encephalitis virus (TBEV). Source: CDC, March 7 2022 (available at: https://www.cdc.gov/tick-borne-encephalitis/geographic-distribution/index.html#:~:text=Highly%20endemic%20regions%20include%20Carinthia,%2C%20Tyrol%2C%20and%20Vorarlberg%20Provinces.&text=Almost%20all%20of%20the%20country,some%20small%20geographically%20dispersed%20areas).


Table 1.
Main arboviruses presenting a potential or demonstrated risk of inter-human transmission by blood transfusion or transplantation.
Table 1.
Main arboviruses presenting a potential or demonstrated risk of inter-human transmission by blood transfusion or transplantation.
|
Virological Data Family / Genus |
Vectors | Usual Vertebrate Hosts | Geographic Distribution |
Incubation (days) |
Percent of Asymptomatic Forms |
Main Clinical Symptoms |
Current Vaccine Prophylaxis |
Documented Transmission by Blood or Grafts |
|
Flaviviridae / Flavivirus (ssRNA, Enveloped) |
||||||||
| - West Nile virus (WNV) - Usutu virus (USUV) - Saint-Louis encephalitis virus (SLEV) - Tick-borne encephalitis virus (TBEV) - Dengue virus (DENV, serotypes 1 to 4) |
Mosquitoes (genus Culex but also Aedes albopictus) Mosquitoes (genus Culex but also Aedes) Mosquitoes (genus Culex) Ticks (genus Ixodes) Mosquitoes (Aedes aegypti and Aedes albopictus) |
Birds Birds Birds Rodents Dears Humans Non-human primates |
Asia, Africa, Europe, Americas Africa, Israel, Europe Americas Europe, Asia World (mainly intertropical regions) |
2-14 3-6 4-21 2-28 2-14 |
80 Frequent > 99 80 50-75 |
Fever, Encephalitis Fever, Rash, Encephalitis, Meningo-encephalitis Fever, Encephalitis Fever, Encephalitis Fever, Hemorrhagic dengue, Shock |
No No No Yes Yes |
Yes (numerous cases) No No Yes Yes (numerous cases) |
| - Zika virus (ZIKV) – Yellow fever virus (YFV) Togaviridae / Alphavirus (ssRNA, enveloped) - Chikungunya virus (CHIKV) - Ross River virus (RRV) |
Different mosquitoes (genus Aedes, Anopheles, Mansonia) Mosquitoes (Aedes aegypti) Mosquitoes (Aedes aegypti and Aedes albopictus) Different mosquitoes (genus Culex, Aedes, Anopheles, Mansonia) |
Humans Non-human primates Humans Non-human primates Humans Non-human primates Kangaroos and wallabies |
Africa, Oceania, India, South-East Asia, Western Indies, Central and South America, Europe Africa Central and South America Africa, Asia, Indian and Pacific oceans, Europe, Western Indies, Americas Oceania, South Pacific |
3-12 3-6 1-12 5-15 |
30-80 55 15 50-75 |
Fever, Rash, Conjunctivitis, Arthralgia, Myalgia, Guillain-Barre syndrome, Microcephaly Fever, Jaundice Hemorrhagic fever Shock Fever, Fatigue, Arthralgia Fever, Rash, Arthralgia |
No Yes No No |
Yes No No Yes |
|
+Reoviridae / Coltivirus (dsRNA, naked) - Colorado tick fever virus (CTFV) |
Ticks (Dermacentor andersoni) |
Humans |
Western USA and Canada |
3-6 |
Low |
Fever, Encephalitis |
No |
Yes |
ssRNA: single-stranded RNA; dsRNA: double-stranded RNA.
Table 2.
Reported cases of transmission of West Nile virus following solid organ transplantation.
|
Year/Location |
Donor | Recipient(s) | |||||||
| Infection route | Serum testing | Organ | OSPT1 | Serum testing | CSF testing | Treatment | Symptoms | Outcome | |
| 2002 / USA | Blood transfusion | NAT2+ | Kidney Kidney Heart Liver |
13 17 8 7 |
IgM+ IgM- NAT+ IgM+ |
IgM+ IgM- IgM+ Non tested |
None None None None |
Neuroinvasive disease Neuroinvasive disease Neuroinvasive disease Fever |
Survived Died3 Survived Survived |
| 2005 / USA | Probable mosquito bite | NAT – IgM+ IgG+ |
Liver Lung Kidney Kidney |
13 17 AS4 AS |
IgM+ IgM+;IgG+ NAT+;IgM-;IgG+ NAT-; IgM-;IgG- |
NAT+;IgM+ NAT+;IgM+ Not tested Not tested |
Immunotherapy Immunotherapy Immunotherapy Immunotherapy |
Neuroinvasive disease Neuroinvasive disease Asymptomatic Not infected |
Coma Coma Survived Survived |
| 2008 / USA | Blood transfusion | NAT-;IgM+ | Heart | 8 | IgM+ | IgM+ | Supportive care | Neuroinvasive disease | Survived |
| 2009 / USA | Probable mosquito bite | NAT+;IgM- | Liver | 15 | NAT-; IgM+;IgG- |
IgM+ | Immunotherapy |
Neuroinvasive disease | Survived |
|
2009 / USA |
Mosquito bite |
NAT+;IgM+;IgG equivocal |
Kidney Kidney Liver |
NA5 AS AS |
NA NA NA |
NA NA NA |
NA NA NA |
Neuroinvasive disease Asymptomatic Asymptomatic |
Survived Survived Survived |
|
2009 / Italy |
Mosquito bite |
NAT+ |
Liver |
AS |
NAT+; IgM+ |
Not tested |
Immunotherapy |
Asymptomatic |
Survived |
| 2010 / USA | Mosquito bite | NAT+;IgM-;IgG+ | Kidney Kidney Liver |
8 AS AS |
IgM+;IgG+ NAT+;IgM+;IgG+ NAT-; IgM-;IgG+ |
NAT-;IgM+ Not tested Not tested |
Supportive care None None |
Neuroinvasive disease Asymptomatic Asymptomatic |
Died Survived Survived |
| 2011 / Italy | Mosquito bite | NAT-;IgM+;IgG+ | Kidney Kidney Liver Lung Heart |
10 10 AS AS AS |
NAT+;IgM+;IgG+ NAT+;IgM+;IgG+ NAT-;IgM+;IgG+ NAT+;IgM+;IgG+ NAT-; IgM-;IgG- |
NAT+;IgM+;IgG+ NAT+;IgM+;IgG+ Not tested Not tested Not tested |
Immunotherapy None None None None |
Neuroinvasive disease Neuroinvasive disease Asymptomatic Asymptomatic Not infected |
Coma Survived Survived Survived Survived |
| 2011 / USA | Increased WNV activity in the donor region | NAT-;IgM+;IgG+ (NAT+ in lymph nodes and spleen) |
Kidney Kidney Lungs Liver |
10 17 20 AS7 |
NAT+ NAT+;IgM+ NAT+ NAT-;IgM-;IgG+ |
NAT+;IgM- NAT+;IgM- NAT+;IgM+ NAT+;IgM- |
Immunotherapy + IFNα2b6 Immunotherapy + IFNα2b Immunotherapy + IFNα2b Immunotherapy + oral ribavirin |
Neuroinvasive disease Neuroinvasive disease Neuroinvasive disease No sign of WNV infection |
Died Survived Survived Survived |
1 OSPT: Onset of symptoms post transplantation. 2 NAT: Nucleic acid testing. 3 NAT positive in brain at autopsy. 4 AS: Asymptomatic. 5 Not available. 6 IFN α2b: Interferon α2b. 7 The patient developed symptoms at day 18 post-transplantation, but not in link with a WNV infection.
Table 3.
Published cases of possible transplantation-associated infection by dengue virus (DENV). NS1 Ag: NS1 antigen of DENV.
Table 3.
Published cases of possible transplantation-associated infection by dengue virus (DENV). NS1 Ag: NS1 antigen of DENV.
|
Country (reference) |
Period | Donor | Recipient(s) | Accountability | ||||||
| Sex/Age/Status | Viral diagnosis | Clinical picture | Graft | Sex/Age | Viral diagnosis | Clinical picture | Evolution | |||
| (31) | 1994 | ?/?/Alive | Not tested | Fever 2 days after gift | Bone marrow | ?/6 | Not tested | Not reported | Deceased | Low |
| Singapore
(32) |
Not reported | F/ ?/Alive | Not tested | Fever | Kidney | M/23 | PCR+ (DENV-1) | Hemorrhagic dengue | Survived | Intermediate |
| Thailand
(33) |
Not reported | F/ ?/Alive | Positive serology without details | Fever one month before gift | Kidney | F/16 | NS1 Ag + PCR+ (DENV-1) Culture + |
Hemorrhagic dengue | Survived | Low |
| India
(34) |
Not reported | M/19/Alive | NS1 Ag + PCR+ (type?) |
Not reported | Liver | M/38 | NS1Ag + PCR+ (type?) |
Fever + hepatitis | Survived | Strong |
| Germany
(35) |
2013 | F/24/Alive | IgM -/IgG - NS1 Ag + PCR+ (DENV-1) |
Fever one day before gift, 8 days after return from Sri Lanka | Bone marrow | M/51 | IgM +/IgG + NS1 Ag + PCR+ (DENV-1) |
Leukemia worsening Enterocolitis Veno-occlusive disease |
Death not dependent of dengue | Very strong (same sequence) |
| India
(36) |
Not reported | M/29/Alive | NS1 Ag + | Fever 3 days after gift | Liver | M/40 | NS1 Ag + | Fever | Survived | Strong |
| Columbia
(37) |
2007 | M/40/Deceased | IgM +/IgG + | Fever | Liver | M/53 | IgM +/IgG - PCR + (DENV-3) |
Fever + transient encephalopathy + hepatitis | Survived | Strong |
| Heart | M/41 | IgM -/IgG - PCR + (DENV-3) |
Hemorrhagic dengue + shock | Survived | Strong | |||||
| 2010 | M/32/Deceased | IgM -/IgG + NS1+ |
Asymptomatic | Kidney | F/31 | IgM -/IgG - NS1 Ag + PCR + (DENV-4) |
Hemorrhagic dengue | Survived | Strong | |
| Kidney | F/48 | IgM +/IgG - NS1 Ag -, PCR - |
Fever | Survived | Strong | |||||
| India
(38) |
2016 | 58/M/Alive | IgM +/IgG + NS1 Ag - PCR + (DENV-1) |
Fever 6 days after gift Encephalopathy |
Liver | M/58 | IgM -/IgG - NS1 Ag + PCR+ (DENV-1) |
Fever + encephalopathy + liver and kidney failure | Deceased | Very strong (same sequence) |
| La Reunion,
France (39) |
2020 | 62/M/Deceased | IgM +/IgG + PCR - |
Asymptomatic | Kidney Kidney |
M/58 M/61 |
PCR+ (DENV-1) IgM +/IgG + PCR+ (DENV-1) IgM +/IgG + |
Pancytopenia + hepatic cytolysis + hemorrhagic shock Intraabdominal collection operated infected by S. epidermidis Thrombopenia + hepatic cytolysis |
Survived Survived |
Strong Strong |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



