
Submitted:
02 August 2023
Posted:
03 August 2023
You are already at the latest version
Abstract
Aging involves several changes depending on genetic and behavioural factors, such as lifestyle and number and quality of social relationships, which in turn can be influenced by empathy. Here, the change in the perceived social support across the life span as a function of empathy was investigated, considering the mediating role of the empathy, after controlling for gender and education. 441 people (18-91 years old) filled in the Italian short version of the Interpersonal Support Evaluation List (ISEL-12) and the Social Support Questionnaire (SSQ6) as well as the Empathy Questionnaire (EQ) and the Reading the Mind in the Eyes test (RMET). The mediation analyses with ISEL-12 showed that age and the EQ fully mediated the relationship between age and Appraisal, Belonging and Tangible scores. Further, the EQ fully mediated only the relationship between age and SSQ6-People. These results showed that empathic skills play a key role in the relationships between age and social support. This suggests: empathy can trigger social support and ultimately well-being if stimulated across the lifespan, especially since young age; this would help to form the socio-emotional competence across the years, as a sort of cushion that can be useful in the elderly to fulfil active aging.
Keywords:
well-being
; affective support
; community engagement
; ageing
; mental health
; socio-emotional skills
1. Introduction
Social support is defined as the provision of emotional, instrumental, or informational assistance or guidance [1]. Above all, it involves the perception that one is cared for, esteemed, and part of a mutually supportive social network, and consequently produce several positive effects on mental and physical health [2]. For example, perceived social support moderates the appraisal of threatening situations and enhances self-confidence to cope with new challenges [3,4,5]. Furthermore, the perception of support is a better predictor of health outcomes than the actual receipt of support [6,7,8]. When an individual is able to perceive the existence of a social support, he/she feels a sense of belonging, increasing the capability to recognize the self-worth [9,10]. Social support is considered as one of the five critical factors necessary for successful aging along with diet, education, physical and cognitive exercise [11,12].
Social support changes as age increases [13]. Within the theoretical frame of the socioemotional selectivity theory (SST) [14,15,16,17,18], age differences in goals and in time horizons influence social preferences and the composition of social networks, as well as cognitive processing. When social interactions as well as the composition of social networks change, especially older people choose to spend more of their time with close others. The decreasing of relationships with age led to wonder about older adults being lonely and depressed [19]. However, other studies reported that this change in social networks reflects a proactive pruning process whereby older people increasingly invest their limited time in relationships with close others [20]. Specifically, older individuals maintain their most meaningful, core relationships and let go the less satisfying, peripheral social partners. It has been reported that when asked to older people to imagine they have a half hour of free time, they choose to spend time with a close social partner rather than a novel one, differently younger individuals do not show this preference. Not only the number of relationships changes, but also the quality of social contacts, indeed, relationship quality improves over time with children, spouses, and other meaningful partners, presumably as a reflection of both experience and motivation [18].
Undoubtedly, supportive social relationships have positive effects on physical and mental health [20]. Several studies demonstrated as partners, children, family, friends, neighbours, colleagues as well as community members may represent an important source of support in life periods characterized by poor health and stress [22,23,24,25]. However, social networks are not static across lifespan [26]. Wrzus and colleagues [27] performed a meta-analysis on 277 studies finding that: i) social network increased from adolescence until young adulthood and then decreased; ii) both the personal and friendship networks decreased throughout adulthood; iii) the family network was always stable in size; iv) other specific networks including colleagues and neighbors were crucial only in determined ages. Summing up, individuals from young adults draw support very different than those in middle or late adulthood.
Age also affects empathy. As defined by Baron-Cohen and Wheelwright [28], empathy is an important ability that allows us to tune into how someone else is feeling, or what they might be thinking. Empathy allows us to understand the intentions of others, to predict their behavior, and to experience an emotion triggered by their emotion. In short, empathy plays a central role in social interactions (e.g. pro-social behavior, inhibition of aggressive behavior and of externalizing problem behavior) allowing us to interact effectively in the social world [27]. Interestingly, empathy was found slightly higher in women than men [28,29]. Of particular interest is the fact that older adults experience some reduction of empathy [30,31,32] associated with greater risk for loneliness and depression, and poorer personal life satisfaction [30,33,34]. Chen and colleagues [35] found that older adults reported lower trait empathic concern and personal distress than the younger group.
Moreover, empathy can be conceptually divided into a cognitive and an emotional component [36,37,38,39,40]: the cognitive component helps us to identify his or her emotions at the cognitive level and thus implies the ability to take another person's perspective, while emotional empathy refers to our ability to experience an emotion similar to that of another person, even though the event that caused the emotion did not directly happen to us [38,41]. In this conceptual perspective, some studies focused on age-related psychological differences in empathy suggesting that older adults have lower cognitive empathy and preserved or increased emotional empathy [36,42]. Previous studies have shown how cognitive empathy also varies as a consequence of age, since older people (usually older than 64 years) obtain lower scores on cognitive empathy in comparison with younger people (with age ranges between 17 to 56 years) when using performance tests [36,42,43,44]. Studies of empathy development show that emotional and cognitive empathy have different developmental trajectories; cognitive empathy develops more slowly and steadily in life span and therefore may rely more strongly on learning experiences, while emotional empathy remains relatively stable throughout development [45,46,47,48]. Labouvie-Vief [49] proposed that the cognitive empathy and age relationship would exhibit an inverted-U-shaped curve, which was later confirmed by O’Brien et al. [50] and by Gutierrez-Cobo et al. [51]. However, other studies revealed that older adults show increased prosocial behavior in the form of monetary donation in response to an empathic context.
It is also true that the lack of consistent results may be due to the differences in methods to measure empathy, sample sizes as well as the unequal numbers of men and women. In particularly, depending on the tests used, different facets of empathy can be assessed; in fact, sometimes even the very form of measurement is used to define the type of empathy [52,53]. There are many measures of empathy, but the most commonly used empathy tests are the Reading the Mind in the Eyes (RMET) [54]; test, which primarily measures cognitive empathy capacity, and the Empathy Quotient (EQ) [28], which provides an overall empathy score without dividing between affective and cognitive empathy [36,55].
Empathy is one of the factors underlying social support: individuals with a high capacity for empathy may more actively understand the care and support of others [56]. In this vein, people with high empathy have a stronger ability to actively obtain support and can more actively understand the care and support from others. Emotionally competent individuals have sensitivity to care and support from the outside world. On the contrary, people with low empathy may not care about others’ support and concern for them. This may further affect their attitude towards others. People with high empathy are more likely to perceive support and then exhibit higher prosocial behavioral tendencies [57].
Therefore, considering the relationship between age, empathy and social support, in the present study the idea was to assess if the cognitive or emotional empathy mediates the relationships between age and interpersonal support defined as ‘appraisal’, ‘belonging’ and ‘tangible’, on the one hand, and social support defined in terms of number of people and level of satisfaction, on the other hand. After controlling for gender and educational level, the hypothesis was formulated as follows: the empathy partially mediates the relationships between age and social support and social network.
2. Method
2.1. Participants
The eligible study sample was composed by individuals without neurological or psychiatric disorders. To exclude the presence of cognitive decline in participants older than 45 years, the Mini-Mental State Exam (MMSE) [58,59] was administered. Additionally, the history or the presence of neurological or psychiatric diseases were investigated by an informal interview carried out before the test phase. Seventeen participants were excluded because they reported having cerebral ischemia or head trauma or for having scored below the cutoff of the MMSE (cut-off = 23) [60]. A final sample of 441 participants took part in the study (mean age = 42.51, SD = 16.93; age range 18-91 years; 220 males and 221 females). Participants had a full-time education, ranging from 5 to 18 years (mean = 13.52 years, S.D. = 3.06 years). The study was approved by the Local Ethical Committee, in accordance with the Declaration of Helsinki. Each participant signed the consent form.
2.2. Instruments
2.2.1. Social Support Measures
Interpersonal Support Evaluation List shortened version -12 items (ISEL-12) [61,62,63]. It is a 12-item scale investigating three types of social support (appraisal, belonging, and tangible). Specifically, the appraisal sub-scale corresponds to the perceived availability of someone with whom to discuss issues of personal importance; the belonging sub-scale measures the perception that there is a group which one can identify and socialize with; the tangible sub-scale investigates the perceived availability of material aid. Participants respond on a four-point Liker scale ranging from 1 (definitively false) to 4 (definitively true); on each subscale the score ranges from 0 to 12. Higher scores correspond to a high perception of social support received.
Social Support Questionnaire 6 (SSQ6) [64]. It is a 6-item questionnaire developed to measure both the social support network and the satisfaction of the social support received. Each item solicits a two-part answer: Part 1 asks participants to list up to nine people that fit the description stated in the question (e.g., “Whom can you really count on to help you feel better when you are feeling generally down-in-the-dumps?”) and are available to provide support, and Part 2 asks participants to indicate for each of the person indicated in the first part, the level of satisfaction using a 6-point Likert scale, ranging from ‘1 - very dissatisfied’ to ‘6 - very satisfied’. The score reflecting the number of people ranges from 6 to 54, whereas the score related to satisfaction ranges from 6 to 36.
2.2.2. Empathy Measures
Empathy Quotient (EQ) [28]. It is a 60-item questionnaire: 40 items measure empathy and 20 are filler items. EQ assesses empathy in adults. According to Baron-Cohen and Wheelwright [28] the items are not separated into cognitive and emotional empathy as the two components are often not easily distinguishable as they co-exist. Each item is a first-person statement on a 4-point Likert Scale (ranging from Strongly Agree to Strongly Disagree). Baron-Cohen and Wheelwright [28] established a cut-off of 30 to screen for autism spectrum disorders. The instrument is scored on a scale of 0 (the least empathetic possible) to 80 (the most empathetic possible).
Reading the Mind in the Eyes test (RMET) [54,65]. It is composed by 36 photographs of the eye region of 19 actors and 17 actresses surrounded by four single-word describing mental state descriptors (e.g., bored, angry). One of these descriptors fitted with the mental state depicted in the photo, and the others were uncorrected. Participants had to choose the correct mental state for each photo. It is based on a four-alternative forced-choice paradigm, with 25% correct guess rate. The test score was the number of descriptors correctly identified (Maximum score: 36).
2.3. Procedure
Participants were tested individually in a quiet room with artificial lighting and seated on a height-adjustable chair filling in questionnaires after having answered to a socio-demographic-anamnestic interview and performed the MMSE.
3. Statistical Analysis and results
Analyses were carried out using IBM SPSS Statistics software v.24 (2016). Data were first transformed in z scores and checked for the presence of potential univariate outliers considering a cut-off of ±4 z-scores as the reference values for samples larger than 100 [66,67]. In total, 6 outliers were detected and excluded from subsequent analyses. The new sample consists in 435 participants. Then, data were tested for normality using the Kolmogorov-Smirnov Test showing that all variables of interest were not normally distributed: ZAge = .124 , p < .0001; ZEducational level = .257, p < .0001; ZISEL12-Appraisal = .085, p < .0001; ZISEL12-Belonging = .124, p < .0001; ZISEL12-Tangible = .138, p < .0001; ZSSQ6-People = .077, p < .0001; ZSSQ6-Satisfaction = .489, p < .0001. Therefore, the Spearman’s Rho correlation analysis was carried out (see Table 1). In general, age correlated negatively to empathy quotient (r = -.170, p < .01), ISEL12-Belonging (r = -.111, p < .05) and ISEL12-Tangible (r = -.160, p < .01), whereas empathy quotient correlated positively to all scores of ISEL-12 (Appraisal: r = .305, p < .01; Belonging: r = .312, p < .01; Tangible: r = .242, p < .01) and SSQ6 (People: r = .136, p < .01; Satisfaction: r = .168, p < .01) (See Table 2 for details). Given that gender and educational level were not correlated to the outcomes, the mediation analyses were carried out without controlling for the covariates. In addition, because RMET did not correlate with any measure of social support, mediation analyses were not conducted.
|
Mean (SD) |
1-Age | 2-Gender | 3-Edu. | 4-EQ | 5-RMET | 6-ISEL-12-A | 7-ISEL-12-B | 8-ISEL-12-T | 9-SSQ6-P | 10-SSQ6-S | |
| 1 | 42.17 (16.75) |
1 | |||||||||
| 2 | --- | -.017 | 1 | ||||||||
| 3 | 7.45 (3.02) | -.194** | .014 | 1 | |||||||
| 4 | 44.24 (12.04) | -.170** | .161** | .066 | 1 | ||||||
| 5 | 21.94 (5.10)- | -.186** | .088 | -.038 | .068 | 1 | |||||
| 6 | 12.61 (2.81) | -.093 | .093 | .007 | .305** | .024 | 1 | ||||
| 7 | 12.63 (2.32) | -.160** | -.035 | -.021 | .312** | .023 | .502** | 1 | |||
| 8 | 13.13 (2.23) | -.111* | -.027 | -.020 | .242** | -.015 | .565** | .586** | 1 | ||
| 9 | 22.42 (10.81) | .011 | .028 | -.017 | .136** | .017 | .253** | .090 | .143** | 1 | |
| 10 | 7.45 (7.49) | .089 | .076 | -.008 | .168** | .091 | .265** | .241** | .225** | .193** | 1 |
Note: ** p ﹤ .01 (two-tailed); * p ﹤ .05 (two-tailed); Edu = Educational Level; EQ = Empathy Quotient; RMET=Eyes test; ISEL-12-A = ISEL-12-Appraisal; ISEL-12-B = ISEL-12-Belonging; IESL-12-T = ISEL-12-Tangible; SSQ6-6 = SSQ6-People; SSQ6-S = SSQ6-Satisfaction.
The hypothesis that the empathy quotient mediates the association between age and social support was investigated using the PROCESS macro for SPSS (version 3.5) [68]. Five mediation models were carried out, one for each social support score (See Figure 1), using age as focal predictor and empathy quotient as mediator. 5000 bootstrap samples were used. Bootstrapping is a non-parametric method which bypasses the issue of non-normality distribution [69].
----- Insert Figure 1 approximately here -----
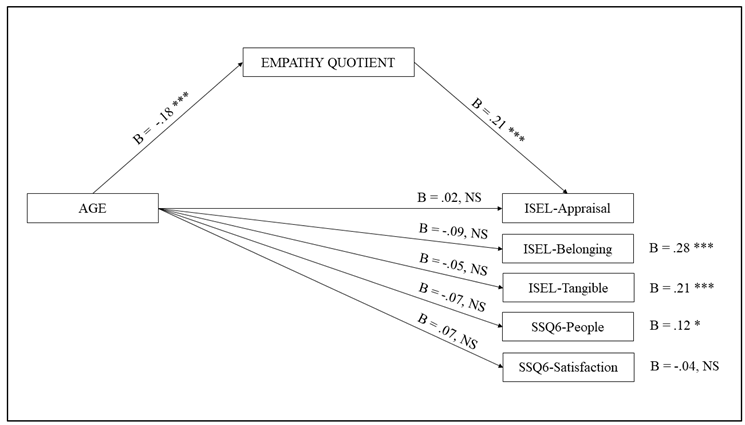
Note: *** p ﹤ .001; ** p ﹤ .01; * p ﹤ .05.
As regards the first model, using ISEL-12-Appraisal as the outcome, the direct effect of age was not significant (b = .02, p = .68). Age negatively predicted the empathy quotient (b = -.18, p < .001), which in turn positively predicted the outcome (b = .21, p < .001). Therefore, the indirect effect was significant (indirect effect = -.0373, 95 % BootLLCI = -.0637 - BootULCI = -.0163).
As regards the second model, using ISEL-12-Belonging as the outcome, the direct effect of age was not significant (b = -.09, p = .06). Age negatively predicted the empathy quotient (b = -.18, p < .001), which in turn positively predicted the outcome (b = .28, p < .001). Therefore, the indirect effect was significant (indirect effect = -.0506, 95 % BootLLCI = -.0824 - BootULCI = -.0231).
As regards the third model, using ISEL-12-Tangible as the outcome, the direct effect of age was not significant (b = -.05, p = .28). Age negatively predicted the empathy quotient (b = -.18, p < .001), which in turn positively predicted the outcome (b = .21, p < .001). Therefore, the indirect effect was significant (indirect effect = -.0381, 95 % BootLLCI = -.0651 - BootULCI = -.0162).
As regards the fourth model, using SSQ6-People as the outcome, the direct effect of age was not significant (b = .07, p = .16). Age negatively predicted the empathy quotient (b = -.18, p < .001), which in turn positively predicted the outcome (b = .12, p < .05). Therefore, the indirect effect was significant (indirect effect = -.0217, 95 % BootLLCI = -.0462 - BootULCI = -.0044).
As regards the fifth model, using SSQ6-Satisfaction as the outcome, the direct effect of age was not significant (b = -.07, p = .14). Age negatively predicted the empathy quotient (b = -.18, p < .001), which in turn did not predict the outcome (b = -.04, p = .40). Therefore, the indirect effect was not significant (indirect effect = -.0074, 95 % BootLLCI = -.0067 - BootULCI = .0249).
4. Discussion
In the present study, we found that the three types of social support (Appraisal, Belonging, and Tangible), as measured by the ISEL-12, and the social support network, as measured by SSQ6, are fully mediated by the empathy quotient and the empathy quotient changes as subjects’ age increases. Several studies demonstrate that empathy in aging is a crucial capacity because it predicts loneliness, people with poor empathy experience greater levels of loneliness [36,57,70]. In general, empathy affects the quality of older adults’ relationships [34,70], and the life satisfaction [70], which relate to increased morbidity in the elderly [71]. In addition, loss of empathy has been considered as a key symptom in patients with Alzheimer’s disease and frontotemporal dementia, and some have suggested that these measures might also help distinguish between the two conditions [72,73,74,75,76,77]. Gouveia et al. [78] found a decline in the EQ’s emotional and social subscales in elderly people.
Another aspect should be considered when measuring empathy is related to the instrument used. For example, in our study we used, on the one hand, the Reading the Mind in the Eyes Test (RMET) [54], which primarily measures cognitive empathy capacity by inferring complex emotions and other mental states from photographs of the eye region of human faces, and, on the other hand, the Empathy Quotient (EQ) [28], which is a self-report questionnaire that provides an overall empathy score without dividing between affective and cognitive empathy [55]. By using RMET and EQ, results are often inconsistent. For example, some studies have reported that older adults have lower cognitive empathy than younger adult [29,30,31,32,79]; one study found no difference between young and old participants [35], whereas another study showed that older adults are characterized by higher levers of empathy [50]. Consistent with Schieman and Co-authors [79], our data showed that both test correlate negatively with age indicating lower empathic ability as age increases.
In the empathy literature, data on the consistency between the two tests are also discordant, in fact while some studies found a relationship between RMET and EQ [80,81], other did not [65,82]. It has been also noted that the interpretation of performance during the eyes test is complicated by its dependence on verbal ability [80,83] and the influence of education, race, and ethnicity [84]. This may explain why our data find that only the EQ correlates positively with the measures of social support we used. Furthermore, both the EQ and the measures of social support used in our work, unlike the RMET, are self-report questionnaires that may suffer from the social desirability bias, being influenced by demand characteristics, as individuals may want to appear empathetic or self-sufficient because these latter are believed to be desirable characteristics.
In the present study, in agreement with some data from the literature [30,31,32], we found that at increasing age decrease the cognitive and emotional empathy and that empathy is crucial for people to be satisfied with the social support they receive and perceive. On the other hand, older people may generally need more than younger people to receive help from others to make up for the physical and psychological difficulties inherent in age, but the fact that the empathic capacity decrease plays against a large e dense social support network. In particular, age does not have a direct effect on perceived social support but it correlates negatively with empathy i. e., older subjects are less empathic than younger subjects and in turn lower empathic abilities mediate the perception of less social support.
Thus, it can be hypothesized that the changes found in the literature [36,42] in the quality and quantity of social interactions and in the composition of social networks were due to an effect mediated by the decreased ability to decode and to understand the intentions of others, to predict their behavior, and to experience an emotion triggered by their emotion. In fact, it is conceivable that elderly people are still able to fully empathize with people they are closest to and have known for a long time (such as family members), but have more difficulty with new people, with the consequence that they prefer to spend their free time with family members rather than forming new relationships [17,20]. An alternative hypothesis comes from the study by Richter and coworkers [85] who found that older adults show better performance on tasks that were relevant to them, suggesting that, in general, older adults perform lower than younger adults on tests of empathic accuracy, except when the information is emotionally relevant to them. However, a confirmation of reduced empathy in ageing also comes from two neuroimaging studies [35,86]. These studies showed that, despite conflicting behavioral results in terms of empathy, older adults show reduced activity in regions typically associated with empathy in younger adults (e.g., anterior cingulate and insula).
In a review [36] concerning the psychological and neural mechanisms of empathy in ageing emerged that older adults have lower cognitive empathy (to understand others’ thoughts and feelings) than younger adults, but similar and in some cases even higher levels of emotional empathy (to feel emotions that are like others’ or feel compassion for them). This is in line with reduced activity in a key brain area associated with cognitive empathy, and also supports our results. Indeed, we found that only one test (EQ) correlates with all aspects of social support (appraisal, belonging and tangible) as well as with the satisfaction of the social support received probably because EQ measured both cognitive and emotional empathy with respect to RMTE.
From a certain point of view it may seem a contradiction that as I get older, at the time when I most need to receive social support I lose the ability to be empathic on a cognitive level, and this has a negative effect on the possibility of receiving support. It is also possible that young people’s self-assessment of support is superficial and not significantly linked to tangible support; however, the fact that the EQ also mediates the tangible dimension would seem to refute this interpretation.
Our results emphasize the importance of working on psychological and cognitive well-being by using training that facilitates cognitive empathy, because increasing this capacity maintains the social network and support received. Empathy is an innate quality, but it is also malleable and can be enhanced by strategic educational interventions [87,88]. Many methods were found to be effective in developing greater levels of empathy, e.g., the use of video recordings [89,90], service to disadvantaged communities [91], reflective writing [92,93], and in our view could easily be used in education to increase empathy in young adults by creating an empathic cognitive reserve that would counteract its decline with age.
This is particularly important because, it is now well established, that some social and environmental variables can have positive and protective effects on the mental and physical health of elderly people [94]; in fact, e.g., Ricciardi and collaborators [95] find that older people who had higher levels of perceived social support experienced fewer symptoms of geriatric depression. Continuing to be an active and positive part of the social context brings the elderly person a number of primary and secondary benefits and through targeted interventions this is possible. The pandemic taught us that it is possible to be part of a social network even at a distance and showed us how those who managed to maintain social relationships even during the period of home restriction suffered less from the negative consequences of isolation and reduced the psychological phenomena of unease and fear that the condition experienced at that time had brought. Therefore, every intervention aimed at reducing mental health vulnerability is mandatory.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Finfgeld-Connett, D. Clarification of social support. J Nurs Scholarsh. 2005, 37, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E. Social support: A review. In Oxford library of psychology; Friedman, H.S., Ed.; The Oxford handbook of health psychology Oxford University Press, 2011; pp. 189–214. [Google Scholar]
- Alemán-Ruíz, I.; Calvo-Francés, F. Validation of the Interpersonal Support Links Scale VIDA. Anales de Psicología, 2017, 33, 168–179. [Google Scholar] [CrossRef]
- Stallman, H. Embedding resilience within the tertiary curriculum: a feasibility study. Higher Education Research & Development 2011, 30, 121–133. [Google Scholar]
- Xerri, M.J.; Radford, K.; Shacklock, K. Student engagement in academic activities: a social support perspective. Higher Education 2018, 75, 589–605. [Google Scholar] [CrossRef]
- Helgeson, V.S. Two important distinctions in social support: kind of support and perceived versus received. Journal of Applied Social Psychology 1993, 23, 825–845. [Google Scholar] [CrossRef]
- Norris, F.H.; Kaniasty, K. Received and perceived social support in times of stress: a test of the social support deterioration deterrence model. Journal of Personality and Social Psychology 1996, 71, 498–511. [Google Scholar] [CrossRef]
- Wethington, E.; Kessler, R.C. Perceived support, received support, and adjustment to stressful life events. Journal of Health and Social Behavior 1986, 27, 78–89. [Google Scholar] [CrossRef]
- Cohen, S.; Gottlieb, B.H.; Underwood, L.G. Social relationships and health. In Social support and health; Cohen, S., Underwood, L.G., Gottlieb, B.H., Eds.; Oxford University Press: New York, 2000; pp. 3–25. [Google Scholar]
- Lau, E.Y.H.; Chan, K.K.S.; Lam, C.B. Social Support and Adjustment Outcomes of First-Year University Students in Hong Kong: Self-Esteem as a Mediator. Journal of College Student Development 2018, 59(1), 129–134. [Google Scholar] [CrossRef]
- Schulz, R.; Heckhausen, J. A life span model of successful aging. American Psychologist 1996, 51, 702–714. [Google Scholar] [CrossRef]
- Piccardi, L.; Pecchinenda, A.; Palmiero, M.; Giancola, M.; Boccia, M.; Giannini, A.M.; Guariglia, C. Successful ageing through physical activity. In Frontiers in Human Neuroscience; Department of Psychology, Sapienza University of Rome: Rome, Italy.
- Vaux, A. Variations in social support associated with Gender, Ethnicity, and Age. Journal of Social Issues 1985, 41, 89–110. [Google Scholar] [CrossRef]
- Carstensen, L.L. Socioemotional selectivity theory: Social activity in life-span context. Annual Review of Gerontology and Geriatrics 1991, 11, 195–217. [Google Scholar]
- Carstensen, L.L. Motivation for social contact across the life span: A theory of socioemotional selectivity. In Nebraska symposium on motivation; Jacobs, J.E., Ed.; University of Nebraska Press: Lincoln, 1993; pp. 209–254. [Google Scholar]
- Carstensen, L.L.; Isaacowitz, D.; Charles, S.T. Taking time seriously: A theory of socioemotional selectivity. American Psychologist 1999, 54, 165–181. [Google Scholar] [CrossRef]
- Carstensen, L.L. The influence of a sense of time on human development. Science 2006, 312, 1913–1915. [Google Scholar] [CrossRef]
- English, T. ; Carstensen. L.L. Socioemotional Selectivity Theory. in: Pachana, N. (eds) Encyclopedia of Geropsychology. Springer: Singapore, 2016. [Google Scholar] [CrossRef]
- Pecchinenda, A.; Yankouskaya, A.; Boccia, M.; Piccardi, L.; Guariglia, C.; Giannini, A.M. Exploring the relationship between perceived loneliness and subjective cognitive decline in older individuals. In Aging and Mental Health; Department of Psychology, Sapienza University of Rome: Rome, Italy, 0015. [Google Scholar]
- Lang, F.R.; Carstensen, L.L. Time counts: Future time perspective, goals, and social relationships. Psychology and Aging 2002, 17, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Karb, R.A.; Elliott, M.R.; Dowd, J.B.; Morenoff, J.D. Neighborhood-level stressors, social support, and diurnal patterns of cortisol: the Chicago Community Adult Health Study. Soc. Sci. Med. 2012, 75, 1038–1047. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.; Subramanian, S.V.; Kawachi, I.; Molnar, B.E. Is blood thicker than water? Social support, depression and the modifying role of ethnicity/nativity status. J Epidemiol Community Health 2011, 65, 51–6. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.H. The effects of positive and negative support from children on widowed older adults' psychological adjustment: a longitudinal analysis. Gerontologist. 2010, 50, 471–81. [Google Scholar] [CrossRef]
- Wolff, J.L.; Kasper, J.D. Caregivers of frail elders: updating a national profile. Gerontologist. 2006, 46, 344–56. [Google Scholar] [CrossRef]
- Bert, F.; Lo Moro, G.; Corradi, A.; Acampora, A.; Agodi, A.; Brunelli, L.; Chironna, M.; Cocchio, S.; Cofini, V.; D'Errico, M.M.; Marzuillo, C.; Pasquarella, C.; Pavia, M.; Restivo, V.; Gualano, M.R.; Leombruni, P.; Siliquini, R.; Collaborating Group. Prevalence of depressive symptoms among Italian medical students: The multicentre cross-sectional "PRIMES" study. PLoS One 2020, 15, e0231845. [Google Scholar] [CrossRef]
- Walen, H.R.; Lachman, M.E. Social support and strain from partner, family, and friends: Costs and benefits for men and women in adulthood. Journal of Social and Personal Relationships 2000, 17, 5–30. [Google Scholar] [CrossRef]
- Wrzus, C.; Hänel, M.; Wagner, J.; Neyer, F.J. Social network changes and life events across the life span: a meta-analysis. Psychol Bull. 2013, 139, 53–80. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S. The Empathy Quotient (EQ): an investigation of adults with Asperger syndrome or high functioning autism and normal sex differences. J. Autism Dev. Disord. 2004, 4, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Guariglia, P.; Piccardi, L.; Giaimo, F.; Alaimo, S.; Miccichè, G.; Antonucci, G. The eyes test is influenced more by artistic inclination and less by sex. Front Hum Neurosci 2015, 22, 292. [Google Scholar] [CrossRef]
- Beadle, J.N.; Paradiso, S.; Kovach, C.; Polgreen, L.; Denburg, N.L.; Tranel, D. Effects of age-related differences in empathy on social economic decision-making. Int Psychogeriatr 2012, 24, 822–33. [Google Scholar] [CrossRef] [PubMed]
- Beadle, J.N.; Sheehan, A.H.; Dahlben, B.; Gutchess, A.H. Aging, empathy, and prosociality. J Gerontol B Psychol Sci Soc Sci 2013, 70, 215–24. [Google Scholar] [CrossRef] [PubMed]
- Bailey, P.E.; Henry, J.D.; Von Hippel, W. Empathy and social functioning in late adulthood. Aging Ment Health 2008, 12, 499–503. [Google Scholar] [CrossRef]
- Davis, M.H.; Oathout, H.A. Maintenance of satisfaction in romantic relationships: empathy and relational competence. J Pers Soc Psychol 1987, 53, 397–410. [Google Scholar] [CrossRef]
- Tully, E.C.; Ames, A.M. , Garcia, S.E.; Donohue, M.R. Quadratic associations between empathy and depression as moderated by emotion dysregulation. J Psychol 2016, 150, 15–35. [Google Scholar] [CrossRef]
- Chen, Y.C.; Chen, C.C.; Decety, J.; Cheng, Y. Aging is associated with changes in the neural circuits underlying empathy. Neurobiol Aging 2014, 35, 827–36. [Google Scholar] [CrossRef]
- Beadle, J.N.; de la Vega, C.E. Impact of Aging on Empathy: Review of Psychological and Neural Mechanisms. Front. Psychiatry 2019, 10, 331. [Google Scholar] [CrossRef]
- Dziobek, I.; Rogers, K.; Fleck, S.; Bahnemann, M.; Heekeren, H.R.; Wolf, O.T.; et al. Dissociation of cognitive and emotional empathy in adults with asperger syndrome using the multifaceted empathy test (MET). J Autism Dev Disord 2008, 38, 464–73. [Google Scholar] [CrossRef] [PubMed]
- Shamay-Tsoory, S.G.; Aharon-Peretz, J.; Perry, D. Two systems for empathy: a double dissociation between emotional and cognitive empathy in in- ferior frontal gyrus versus ventromedial prefrontal lesions. Brain 2009, 132, 617–27. [Google Scholar] [CrossRef] [PubMed]
- Shamay-Tsoory, S.G. The neural bases for empathy. Neuroscientist 2011, 17, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Abramson, L.; Uzefovsky, F.; Toccaceli, V.; Knafo-Noam, A. The genetic and environmental origins of emotional and cognitive empathy: Review and meta-analyses of twin studies. Neurosci Biobehav Rev. 2020, 114, 113–133. [Google Scholar] [CrossRef]
- Uzefovsky, F.; Knafo-Noam, A. Empathy development throughout the lifespan. In Social Cognition: Frontiers in Developmental Science Series; Sommerville, J., Decety, J., Eds.; Psychology Press | Taylor and Francis Group: NY, USA, 2016; pp. 71–97. [Google Scholar]
- Henry, J.D.; Phillips, L.H.; Ruffman, T.; Bailey, P.E. A meta-analytic review of age differences in theory of mind. Psychol Aging 2013, 28, 826. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.L.; Rourke, N.O.; Thornton, W.L. Age differences in cognitive and affective theory of mind : Concurrent contributions of neurocognitive performance, sex, and pulse pressure. Journals of Gerontology: Psychological Sciences 2017, 72, 71–81. [Google Scholar] [CrossRef]
- Warrier, V.; Grasby, K.; Uzefovsky, F.; Toro, R.; Smith, P.; Chakrabarti, B.; Khadake, J.; Mawbey-Adamson, E.; Litterman, N.; Hottenga, J.J.; Lubke, G.; Boomsma, D.I.; Martin, N.G.; Hatemi, P.K.; Medland, S.E.; Hinds, D.A.; Bourgeron, T.; S Baron-Cohen, S. Genome-wide meta-analysis of cognitive empathy: heritability, and correlates with sex, neuropsychiatric conditions and cognition. Mol Psychiatry 2018, 23, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Knafo, A.; Zahn-Waxler, C.; Van Hulle, C.; Robinson, J.L.; Rhee, S.H. The developmental origins of a disposition toward empathy: genetic and environmental contributions. Emotion 2008, 8, 737–752. [Google Scholar] [CrossRef]
- Roth-Hanania, R.; Davidov, M.; Zahn-Waxler, C. Empathy development from 8 to 16 months: early signs of concern for others. Infant Behav. Dev. 2011, 34, 447–458. [Google Scholar] [CrossRef]
- Van der Graaff, J.; Branje, S.; De Wied, M.; Hawk, S.; Van Lier, P.; Meeus, W. Perspective taking and empathic concern in adolescence: gender differences in developmental changes. Dev. Psychol. 2014, 50, 881–888. [Google Scholar] [CrossRef]
- Tousignant, B.; Eug. ne, F.; Jackson, P.L. A developmental perspective on the neural bases of human empathy. Infant Behave. Dev. 2017, 48, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Labouvie-Vief, G. Cognition and equilibrium regulation in de- velopment and aging. Restorative Neurology and Neuroscience 2009, 27, 551–565. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, E.; Konrath, S.H.; Grühn, D.; Hagen, A.L. Empathic concern and perspective taking: Linear and quadratic effects of age across the adult life span. Journals of Gerontology - Series B Psychological Sciences and Social Sciences 2013, 68, 168–175. [Google Scholar] [CrossRef]
- Gutiérrez-Cobo, M.; Cabello, R.; Megías-Robles, A.; Gómez-Leal, R.; Baron-Cohen, S.; Fernández-Berrocal, P. Does our cognitive empathy diminish with age? The moderator role of educational level. International Psychogeriatrics 2023, 35, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Cuff, B.; Brown, S.J.; Taylor, L.; Howat, D. Empathy: a review of the concept. Emot. Rev. 2016, 8, 144–153. [Google Scholar] [CrossRef]
- Teding van Berkhout, E.; Malouff, J.M. The efficacy of empathy training: a meta-analysis of randomized controlled trials. J. Couns. Psychol. 2016, 63, 32–41. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The ‘‘Reading the mind in the eyes’’ test revised version: a study with normal adults and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef]
- Schmidt, I.; Rutanen, T.; Luciani, R.S.; Jola, C. Feeling for the Other With Ease: Prospective Actors Show High Levels of Emotion Recognition and Report Above Average Empathic Concern, but Do Not Experience Strong Distress. Front Psychol. 2021, 12, 543846. [Google Scholar] [CrossRef]
- Betzler, M. The relational value of empathy. Int. J. Philos. Stud. 2019, 27, 136–161. [Google Scholar] [CrossRef]
- Hu, T.; Zheng, X.; Huang, M. Absence and presence of human interaction: the relationship between loneliness and empathy. Front. Psychol. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘‘Mini-mental state’’. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Frisoni, G.B.; Rozzini, R.; Bianchetti, A.; Trabucchi, M. Principal lifetime occupation and MMSE score in elderly persons. Journal of Gerontology 1993, 48, S310–S314. [Google Scholar] [CrossRef]
- Magni, E.; Binetti, G.; Bianchetti, A.; Rozzini, R.; Trabucchi, M. Mini-mental state examination: a normative study in Italian elderly population. European Journal of Neurology 1996, 3, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Hoberman, H. Positive events and social supports as buffers of life change stress. Journal of Applied Social Psychology 1983, 13, 99–125. [Google Scholar] [CrossRef]
- Cohen, S.; Mermelstein, R.; Kamarck, T.; Hoberman, H.M. Measuring the functional components of social support. In Social support: Theory, research, and applications; Sarason, I.G., Sarason, B.R., Eds.; Springer: Dordrecht, Holland, 1985; pp. 73–94. [Google Scholar]
- Cohen, S. ISEL-12: Basic psychometric information. 2015. [Google Scholar]
- Sarason, I.G.; Sarason, B.R.; Shearin, E.N.; Pierce, G.R. A Brief Measure of Social Support: Practical and Theoretical Implications. Journal of Social and Personal Relationships 1987, 4, 497–510. [Google Scholar] [CrossRef]
- Vellante, M.; Baron-Cohen, S.; Melis, M.; Marrone, M.; Petretto, D.R.; Masala, C.; Preti, A. The ‘‘reading the mind in the eyes’’ test: systematic review of psychometric properties and a validation study in Italy. Cogn. Neuropsychiatry 2013. 18, 326–354. [CrossRef]
- Mertler, C.A.; Vannatta, R.A. Advanced and multivariate statistical methods: Practical application and interpretation (3.Basm). 2005 CA: Pyrczak Publishing.
- Giancola, M. Who complies with prevention guidelines during the fourth wave of COVID-19 in Italy? An empirical study. Personality and Individual Differences 2022, 199, 111845. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, 2017. [Google Scholar]
- Bollen, K.A.; Stine, R. Direct and indirect effects: Classical and bootstrap estimates of variability. Sociological Methodology 1990, 20, 115–140. [Google Scholar] [CrossRef]
- Beadle, J.N. , Brown, V.; Keady, B.; Tranel, D.; Paradiso, S. Trait empathy as a predictor of individual differences in perceived loneliness. Psychol. Rep. 2012, 110, 3–15. [Google Scholar] [CrossRef]
- Cacioppo. S.; Capitanio, J.P.; Cacioppo, J.T. Toward a neurology of loneliness. Psychol. Bull. 2014, 140, 1464–504. [Google Scholar] [CrossRef]
- Caminiti, S.P.; Canessa, N.; Cerami, C.; Dodich, A.; Crespi, C.; Iannaccone, S.; Marcone, A.; Falini, A.; Cappa, S.F. Affective mentalizing and brain activity at rest in the behavioral variant of frontotemporal dementia. Neuroimage Clin 2015, 9, 484–97. [Google Scholar] [CrossRef] [PubMed]
- Cerami, C.; Dodich, A.; Canessa, N.; Crespi, C.; Marcone, A.; Cortese, F.; et al. Neural correlates of empathic impairment in the behavioral variant of frontotemporal dementia. Alzheimers Dement. 2014, 10, 827–34. [Google Scholar] [CrossRef] [PubMed]
- Dermody, N.; Wong, S.; Ahmed, R.; Piguet, O.; Hodges, J.R.; Irish, M. Uncovering the neural bases of cognitive and affective empathy deficits in Alzheimer’s disease and the behavioral-variant of frontotemporal dementia. J. Alzheimers Dis. 2016, 53, 801–16. [Google Scholar] [CrossRef] [PubMed]
- Eslinger, P.J.; Moore, P.; Anderson, C.; Grossman, M. Social cognition, executive functioning, and neuroimaging correlates of empathic deficits in frontotemporal dementia. Neuropsychiatry Clin. Neurosci. 2011, 23, 74–82. [Google Scholar] [CrossRef]
- Lee, G.J.; Lu, P.H.; Mather, M.J.; Shapira, J.; Jimenez, E.; Leow, A.D.; Thompson, P.M.; Mendez, M.F. Neuroanatomical correlates of emotional blunting in behavioral variant frontotemporal dementia and early-onset Alzheimer’s disease. J Alzheimers Dis. 2014, 41, 793–800. [Google Scholar] [CrossRef]
- Oliver, L.D.; Mitchell, D.G.; Dziobek, I.; MacKinley, J.; Coleman, K.; Rankin, K.P.; et al. Parsing cognitive and emotional empathy deficits for negative and positive stimuli in frontotemporal dementia. Neuropsychologia 2015, 67, 14–26. [Google Scholar] [CrossRef]
- Gouveia, V.V.; Milfont, T.L.; Gouveia, R.S.; Neto, J.R. , and Galvão, L. Brazilian-portuguese empathy quotient: evidences of its construct validity and reliability. Span. J. Psychol. 2012, 15, 777–782. [Google Scholar] [CrossRef]
- Schieman, S.; Van Gundy, K. The personal and social links between age and self-reported empathy. Soc. Psychol. Q 2000, 63, 152–74. [Google Scholar] [CrossRef]
- Lawrence, E.J.; Shaw, P.; Baker, D.; Baron-Cohen, S.; David, A.S. Measuring empathy: Reliability and validity of the Empathy Quotient. Psychological Medicine 2004, 34, 911–920. [Google Scholar] [CrossRef]
- Voracek, M.; Dressler, S.G. Lack of correlation between digit ratio (2D:4D) and Baron-Cohen’s “Reading the Mind in the Eyes” test, empathy, systemising, and autism-spectrum quotients in a general population sample. Personality and Individual Differences 2006, 41, 1481–1491. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Bowen, D.C.; Holt, R.J.; Allison, C.; Auyeung, B.; Lombardo, M.V.; Smith, P.; Lai, M.C. The “reading the mind in the eyes” test: Complete absence of typical sex difference in 400 men and women with autism. PLOS ONE 2015, 10, e0136521–10. [Google Scholar] [CrossRef] [PubMed]
- Olderbak, S.; Wilhelm, O.; Olaru, G.; Geiger, M.; Brenneman, M.W.; Roberts, R.D. A psychometric analysis of the reading the mind in the eyes test: Toward a brief form for research and applied settings. Frontiers in Psychology 2015, 6, 1503. [Google Scholar] [CrossRef] [PubMed]
- Dodell-Feder, D.; Ressler, K.J.; Germine, L.T. Social cognition or social class and culture? On the interpretation of differences in social cognitive performance. Psychological Medicine 2020, 50, 133–145. [Google Scholar] [CrossRef]
- Richter, D.; Kunzmann, U. Age differences in three facets of empathy: performance-based evidence. Psychol. Aging 2011, 26, 60–70. [Google Scholar] [CrossRef] [PubMed]
- Riva, F.; Tschernegg, M.; Chiesa, P.A.; Wagner, I.C.; Kronbichler, M.; Lamm, C.; Silani, G. Age-related differences in the neural correlates of empathy for pleasant and unpleasant touch in a female sample. Neurobiol. Aging 2018, 65, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Stepien, K.A.; Baernstein, A. Educating for empathy: a review. J. Gen. Intern. Med. 2006, 21, 524–530. [Google Scholar] [CrossRef]
- Kelm, Z.; Womer, J.; Walter, J.K.; Feudtner, C. Interventions to cultivate physician empathy: a systematic review. BMC Med. Educ. 2014, 14, 219–230. [Google Scholar] [CrossRef]
- Kataoka, H.; Iwase, T.; Ogawa, H.; et al. Can communication skills training improve empathy? A six-year longitudinal study of medical students in Japan. Med Teach. 2018, 22, 1–6. [Google Scholar] [CrossRef]
- Shaw, D.J.; Czekòova´, K.; Spilakova´, B.; Salazar, M.; Rezač, P.; Kurečkova´, V.; Zamecmik, P.; Brazdil, M. A neuroscientific evaluation of driver rehabilitation: Functional neuroimaging demonstrates the effectiveness of empathy induction in altering brain responses during social information processing. PLoS ONE 2020, 15, e0232222. [Google Scholar] [CrossRef]
- Fritz, C.; Naylor, K.; Watkins, Y.; Britt, T.; Hinton, L.; Curry, G.; Randal, F.; Lam, H.; Kim, K. Are we missing the mark? The implementation of community based participatory education in cancer disparities curriculum development. J. Racial Ethn Health Disparities. 2015, 2, 237–243. [Google Scholar] [CrossRef]
- Brown, K.M.; Bright, L.M. Teaching caring and competence: student transformation during an older adult focused service-learning course. Nurse Educ Pract. 2017, 27, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Moniz, T.; Artnfield, S.; Miller, K.; Lingard, L.; Watling, C.; Regehr, G. Considerations in the use of reflective writing for student assessment: issues of reliability and validity. Med Educ. 2015, 49, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in Older Adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef] [PubMed]
- Ricciardi, E.; Spano, G.; Tinella, L.; Lopez, A.; Clemente, C.; Bosco, A.; Caffò, A.O. Perceived Social Support Mediates the Relationship between Use of Greenspace and Geriatric Depression: A Cross-Sectional Study in a Sample of South-Italian Older Adults. Int. J. Environ. Res. Public Health 2023, 20, 5540. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



