
Submitted:
02 August 2023
Posted:
04 August 2023
You are already at the latest version
Abstract
A patient in her early 20s presented with constant and progressive lower abdominal and back pain, mainly on the right side of the abdomen, purulent vaginal discharge and pyrexia. Radio-logical assessment revealed a possible tuboovarian abscess and incidental diagnosis of ipsilateral renal agenesis. The patient was treated for pelvic inflammatory disease (PID), however after antibiotic administration and since the symptoms were not resolving, an abdominal MRI was requested which revealed a uterus didelphys with two cervices, an obstructed haemivagina and evidence of haematocolpos. The diagnosis of OHVIRA syndrome was confirmed and the patient underwent an excision of the vaginal septum, drainage of the haematopyocolpos and laparoscopic drainage of the tuboovarian abscess. She achieved a good recovery.
Keywords:
OHVIRA syndrome 1
; differential diagnosis 2
; tuboovarian abscess 3
; congenital syndrome 4
; pelvic inflammatory disease 5
Figure 1.
Axial T2 weighted MR image demonstrates a uterus didelphys (two uterine cavities indicated by white arrows). A 21-year-old woman presented with lower abdominal and back pain, mainly located on the right side. The pain was constant and progressively worse over a six-day period. She also reported episodes of vomiting over the last two days, constipation, and loss of appetite. Additionally, she had a previous assessment in A+E five days prior to this admission, where she was diagnosed with a chest infection and was treated with Co-amoxiclav. Her previous medical history and family history was unremarkable, she had never had any previous surgeries, had never conceived and was not allergic to any medication. Initially, she was assessed by members of the A+E team and was referred to the surgical team to exclude appendicitis or mesenteric adenitis. On examination, the abdomen was soft with voluntary guarding on the right iliac fossa. She was pyrexial (T:38.1oC), tachycardic (HR:129bpm), tachypnoeic (RR:19), with normal blood pressure (BP:119/80mmHg) and oxygen saturation (SO2:98%). Biochemical and haematological investigations revealed elevated CRP (>320mg/L), white cell count (WCC:16x 109 /L) and platelets (405x 109 /L). Liver and kidney function were normal. Venous blood gas indicated a pH of 7.35 and lactate of 1.3mmol/L. The urine sample indicated the presence of leucocytes, protein and blood. The urine pregnancy test was negative. The patient underwent a CT abdomen/pelvis after the initial surgical review. It revealed a large complex pelvic collection, measuring 7x6x10cm, arising from the right adnexa, with the inflammatory process extending into the uterus. The CT also suggested incidental right renal agenesis, of which the patient was not aware of. The findings were suggestive of a tuboovarian abscess (TOA) and the patient was started on intravenous ceftriaxone and metronidazole as per the unit’s protocol. Due to the CT scan findings, the patient was then referred to the Gynaecology team. Her gynaecological history indicated a menarche at 10 years of age. Her periods were regular, but she reported significant dysmenorrhea and heavy menstrual bleeding. Clinical examination including speculum exam revealed that the cervix was difficult to visualise, since it was deviated to the left. A purulent foul-smelling discharge was also noted as well as a fullness on the anterior fornix, but no signs of significant tenderness were present at the time of the examination. After the gynaecological assessment, a pelvic ultrasound was requested to further characterize the pelvic mass. The TVUSS was performed approximately 24 hours after the CT, while the patient remained febrile. Sonographic assessment revealed the collection, previously attributed to the TOA, but the additional finding of a uterus didelphys with two cervices were also noted. The combination of renal agenesis and uterine abnormality raised the possibility of a Müllerian abnormality; thus, an abdomen/pelvis MRI with contrast was requested in order to confirm the diagnosis. The MRI report confirmed that there is a double uterus and cervix and further added that there is a longitudinal vaginal septum.
Figure 1.
Axial T2 weighted MR image demonstrates a uterus didelphys (two uterine cavities indicated by white arrows). A 21-year-old woman presented with lower abdominal and back pain, mainly located on the right side. The pain was constant and progressively worse over a six-day period. She also reported episodes of vomiting over the last two days, constipation, and loss of appetite. Additionally, she had a previous assessment in A+E five days prior to this admission, where she was diagnosed with a chest infection and was treated with Co-amoxiclav. Her previous medical history and family history was unremarkable, she had never had any previous surgeries, had never conceived and was not allergic to any medication. Initially, she was assessed by members of the A+E team and was referred to the surgical team to exclude appendicitis or mesenteric adenitis. On examination, the abdomen was soft with voluntary guarding on the right iliac fossa. She was pyrexial (T:38.1oC), tachycardic (HR:129bpm), tachypnoeic (RR:19), with normal blood pressure (BP:119/80mmHg) and oxygen saturation (SO2:98%). Biochemical and haematological investigations revealed elevated CRP (>320mg/L), white cell count (WCC:16x 109 /L) and platelets (405x 109 /L). Liver and kidney function were normal. Venous blood gas indicated a pH of 7.35 and lactate of 1.3mmol/L. The urine sample indicated the presence of leucocytes, protein and blood. The urine pregnancy test was negative. The patient underwent a CT abdomen/pelvis after the initial surgical review. It revealed a large complex pelvic collection, measuring 7x6x10cm, arising from the right adnexa, with the inflammatory process extending into the uterus. The CT also suggested incidental right renal agenesis, of which the patient was not aware of. The findings were suggestive of a tuboovarian abscess (TOA) and the patient was started on intravenous ceftriaxone and metronidazole as per the unit’s protocol. Due to the CT scan findings, the patient was then referred to the Gynaecology team. Her gynaecological history indicated a menarche at 10 years of age. Her periods were regular, but she reported significant dysmenorrhea and heavy menstrual bleeding. Clinical examination including speculum exam revealed that the cervix was difficult to visualise, since it was deviated to the left. A purulent foul-smelling discharge was also noted as well as a fullness on the anterior fornix, but no signs of significant tenderness were present at the time of the examination. After the gynaecological assessment, a pelvic ultrasound was requested to further characterize the pelvic mass. The TVUSS was performed approximately 24 hours after the CT, while the patient remained febrile. Sonographic assessment revealed the collection, previously attributed to the TOA, but the additional finding of a uterus didelphys with two cervices were also noted. The combination of renal agenesis and uterine abnormality raised the possibility of a Müllerian abnormality; thus, an abdomen/pelvis MRI with contrast was requested in order to confirm the diagnosis. The MRI report confirmed that there is a double uterus and cervix and further added that there is a longitudinal vaginal septum.
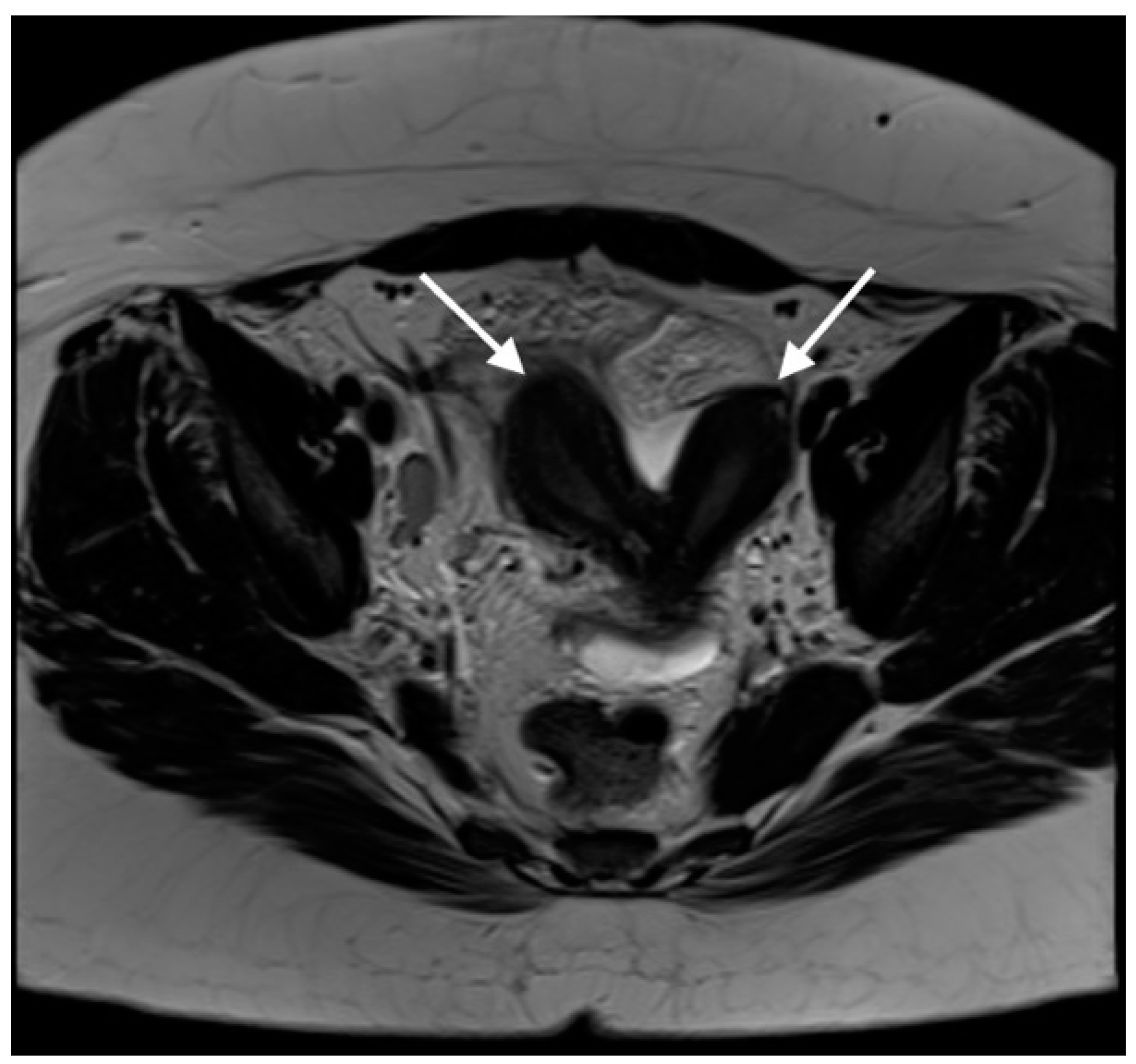
Figure 2.
Sagittal T2 weighted MR image showing a vaginal septum with a haematopyocolpos of the obstructed hemivagina and a tubo-ovarian abscess (red arrow indicates the obstructed haematopyocolpos and white arrow shows the tubo-ovarian abscess). The presence of a gas fluid level within its lumen, was indicative of a concurrent infection. The patient was initially treated with intravenous antibiotics against the provisional diagnosis of PID. After three days of treatment, she continued to have episodes of pyrexia, the CRP remained high (242mg/L), and there were persistently high WCC (16.5x 109 /L) and platelets (500x 109 /L). On the third day after admission, the diagnosis of OHVIRA syndrome was finalised and the decision was taken to take the patient for a surgical intervention to drain the haematocolpos and perform a laparoscopic exploration, to which the patient consented. The next day the patient underwent an examination under anaesthesia, vaginal septectomy and drainage of the haematopyocolpos. Intraoperative hysteroscopy confirmed the presence of a uterus didelphys bicollis. The cervix of the affected cavity was dilated to encourage continuous drainage. Subsequently, on laparoscopy significant pelvic adhesions were noted, involving the bowel being adherent to the uterus, and a large right-sided tubo-ovarian abscess. Laparoscopic adhesiolysis was performed as well as drainage of the abscess. A pelvic drain was left in situ at the end of the procedure. She remained an inpatient for four days after surgery. The drain was removed three days after the operation. She was continued on intravenous antibiotics for a further three days before they were converted to oral. She stopped spiking a temperature post-operatively and her pulse normalised two days after the operation. Her CRP dropped to 51mg/L and WCC to 9.5x 109 /L on the day of discharge. She was followed up in the Gynaecology Clinic with repeat imaging that confirmed the resolution of the tubo-ovarian abscess. She was carefully debriefed about the implications of having a uterus didelphys and a single kidney in pregnancy and was further signposted to written information provided by the British Society of Paediatric and Adolescent Gynaecology.
Figure 2.
Sagittal T2 weighted MR image showing a vaginal septum with a haematopyocolpos of the obstructed hemivagina and a tubo-ovarian abscess (red arrow indicates the obstructed haematopyocolpos and white arrow shows the tubo-ovarian abscess). The presence of a gas fluid level within its lumen, was indicative of a concurrent infection. The patient was initially treated with intravenous antibiotics against the provisional diagnosis of PID. After three days of treatment, she continued to have episodes of pyrexia, the CRP remained high (242mg/L), and there were persistently high WCC (16.5x 109 /L) and platelets (500x 109 /L). On the third day after admission, the diagnosis of OHVIRA syndrome was finalised and the decision was taken to take the patient for a surgical intervention to drain the haematocolpos and perform a laparoscopic exploration, to which the patient consented. The next day the patient underwent an examination under anaesthesia, vaginal septectomy and drainage of the haematopyocolpos. Intraoperative hysteroscopy confirmed the presence of a uterus didelphys bicollis. The cervix of the affected cavity was dilated to encourage continuous drainage. Subsequently, on laparoscopy significant pelvic adhesions were noted, involving the bowel being adherent to the uterus, and a large right-sided tubo-ovarian abscess. Laparoscopic adhesiolysis was performed as well as drainage of the abscess. A pelvic drain was left in situ at the end of the procedure. She remained an inpatient for four days after surgery. The drain was removed three days after the operation. She was continued on intravenous antibiotics for a further three days before they were converted to oral. She stopped spiking a temperature post-operatively and her pulse normalised two days after the operation. Her CRP dropped to 51mg/L and WCC to 9.5x 109 /L on the day of discharge. She was followed up in the Gynaecology Clinic with repeat imaging that confirmed the resolution of the tubo-ovarian abscess. She was carefully debriefed about the implications of having a uterus didelphys and a single kidney in pregnancy and was further signposted to written information provided by the British Society of Paediatric and Adolescent Gynaecology.
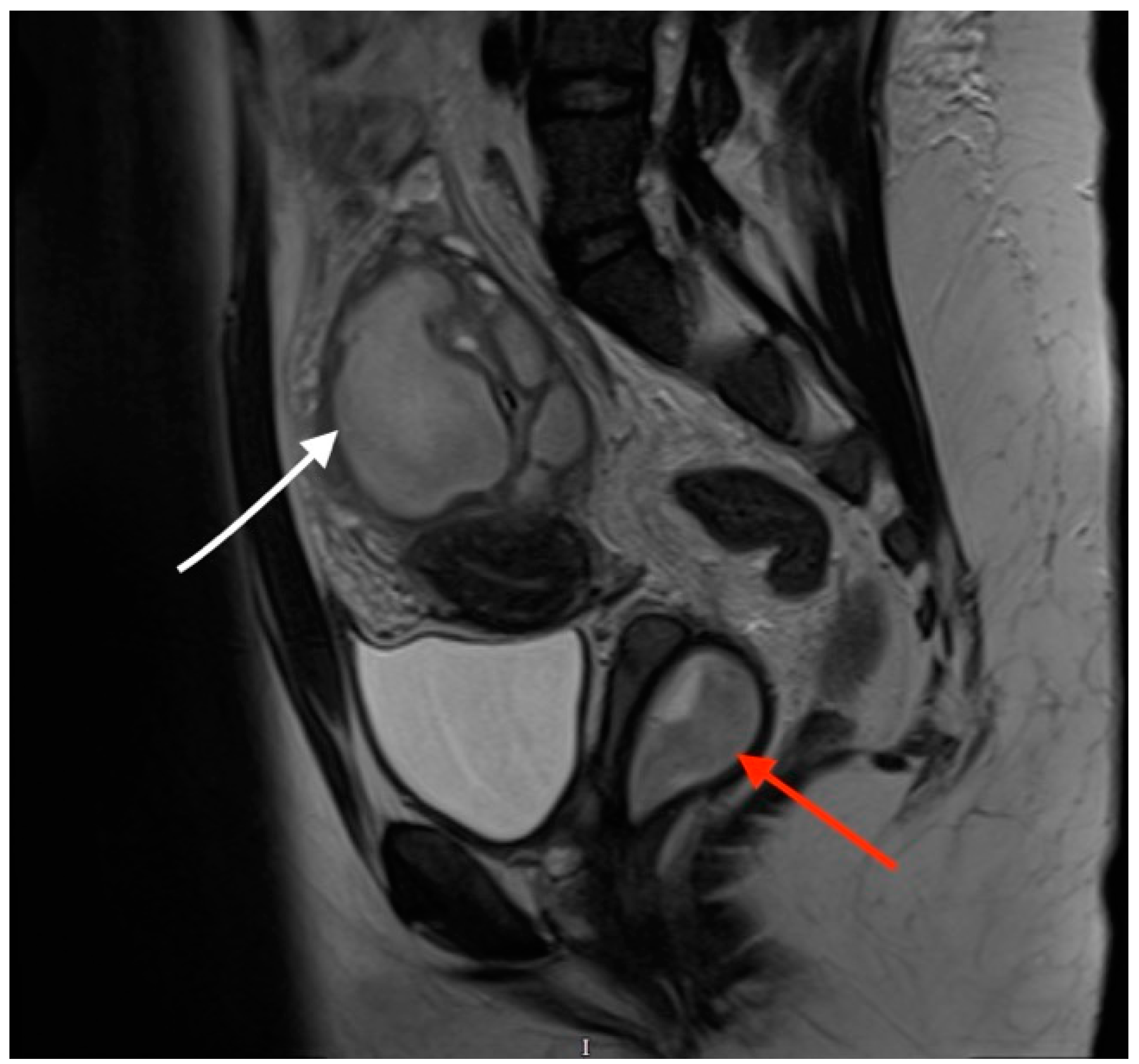
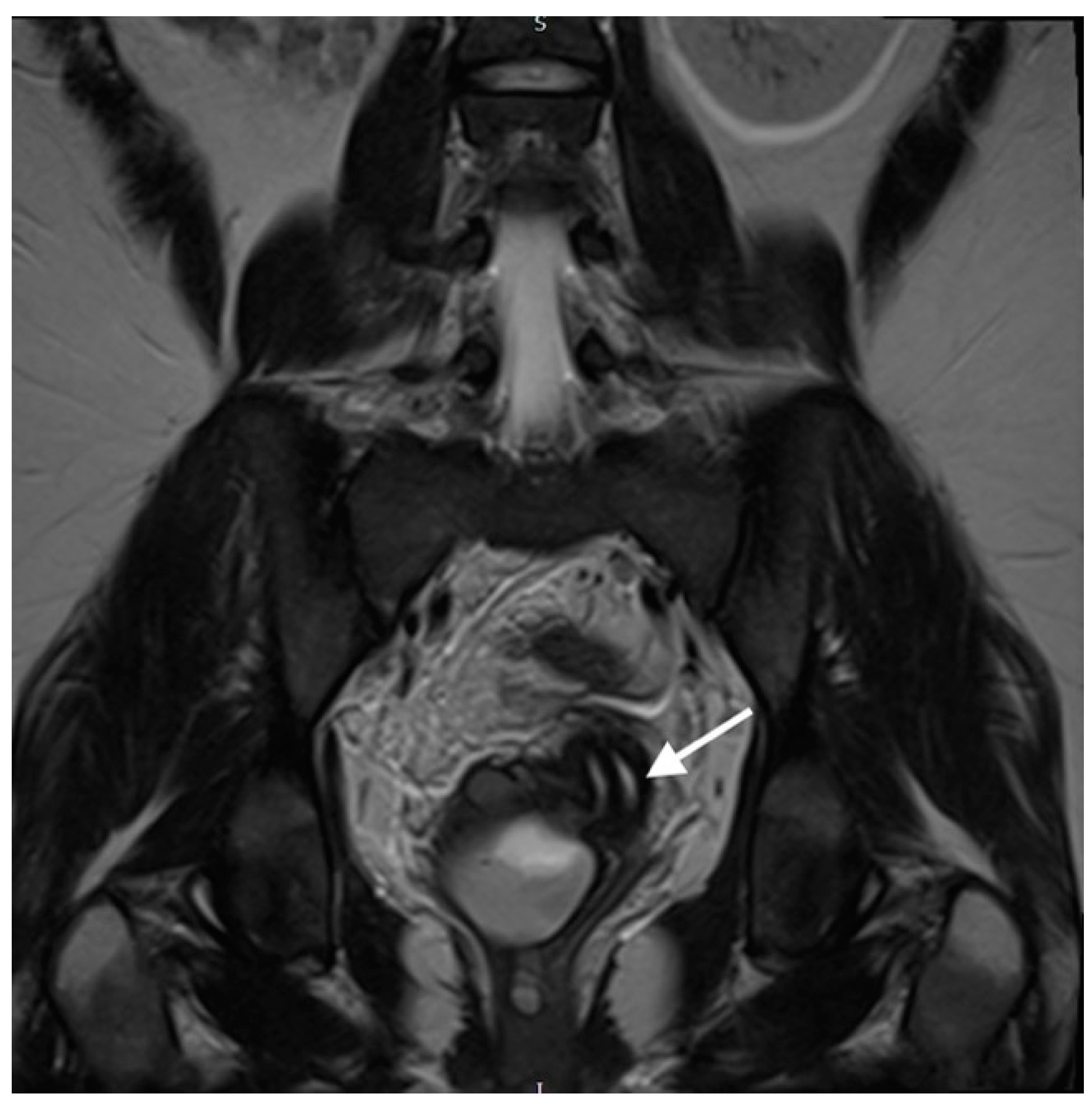
Figure 3.
Coronal T2 weighted MR image shows 2 cervical canals (white arrow indicates the two cervical canals. The right-sided cervix leads to the obstructed haematopyocolpos). OHVIRA syndrome, also known as Herlyn–Werner–Wunderlich syndrome, is a rare uterine and renal congenital abnormality which is characterized by an obstructed hemivagina and ipsilateral renal agenesis [1]. The exact prevalence of the syndrome has not been yet estimated, but it has been reported that it accounts for 0,16%-10% of Mullerian abnormalities, the incidence of which is 2-3% of the population [2]. Assessment by pelvic ultrasound in combination with MRI help to establish an accurate clinical diagnosis [3]. In the majority of cases, pubertal women are more likely to be identified with the syndrome, since the onset of menstrual periods might lead to hematometra and/or delayed menarche. However, in cases of partial obstruction, the diagnosis can be elusive, often taking years to be established, leading at times to women presenting in adulthood with symptoms resembling pelvic infection and endometriosis [4]. Septectomy remains the treatment of choice and should be performed in all affected patients. Knowledge of this rare condition and maintaining high levels of suspicion is critical in these cases [5,6]. Its complex embryological origin makes OHVIRA syndrome a complicated, heterogeneous condition that can be challenging to diagnose. The common triad of congenital variations (uterus didelphys, obstructed hemivagina and renal agenesis on the same side of the vaginal abnormality) is not always present, as reports have indicated that there can also be a septate uterus in up to 22% of cases [7] The renal anomalies can also include an ectopic ureter or a dysplastic kidney [8,9]. Variants of the syndrome have also been reported, where there is a fenestration in the vaginal septum that results in a partial obstruction [6], or cases when the septum is very thin and menstrual contents cause it to perforate leading to communication between the two vaginas [10]. Patients with this type of vaginal variation, such as in our case report, will have normal menses through the patent hemivagina and will typically have a delayed diagnosis much later during their reproductive years. Whereas the classic clinical presentation is that of a prepubertal girl around menarche presenting with pelvic pain, and a vaginal bulge is present on examination, indicating haematocolpos, cases that present in adulthood can be misdiagnosed with more common conditions such as pelvic infection, tuboovarian abscess, or endometriosis.In adulthood, patients will usually present with progressive dysmenorrhea and lower abdominal pain and will also possibly report urinary retention and offensive vaginal discharge [11]. On an acute basis, they might present with symptoms of an acute pelvic infection, secondary to pyocolpos, leading to a pyometra and tubo-ovarian abscess. These cases can closely resemble the symptoms of PID, and clinicians will need a high index of suspicion as the patients will not respond to antibiotics. Furthermore, endometriosis, in the form of ovarian or deep infiltrating endometriosis, can be found in 17-36% of these patients [12,13], with the most likely pathogenesis being the inability of the obstructed hemivagina to distend due to the thick septum resulting in retrograde menstruation [14]. Studies indicate that the age of diagnosis of pelvic endometriosis usually comes much earlier than the diagnosis of OHVIRA syndrome [15] and clinicians should be aware that patients with Mullerian anomalies can develop severe endometriosis, particularly in cases with an obstructed outflow tract [16]. Thus, in adolescent girls diagnosed with pelvic endometriosis, due to symptoms of dysmenorrhea with an onset close to menarche, an obstructive genital abnormality should be considered as a potential diagnosis [17]. Studies have shown that over 30% of female patients with a unilateral renal agenesis or multicystic dysplastic kidney have an associated uterine anomaly, so such a finding should always trigger further imaging of the uterus either by ultrasound or MRI.[18] Screening young women, before menarche if possible, with such renal abnormalties for Mullerian anomalies would potentially prevent not only acute presentations, such as the one we describe in this case, but also long-term complications associated with untreated obstructive malformations. Clear guidelines are currently scarce to guide this type of screening and are needed to ensure adequate communication between sonographers, paediatricians, and gynaecologists to diagnose this syndrome early [18]. They would also help to promote age-specific treatment of the vaginal obstruction [19]. Studies on long-term reproductive outcomes in patients with OHVIRA syndrome indicate that a delayed diagnosis is associated with high rates of PID, pelvic adhesions and endometriosis, although thankfully not subfertility [7,20]. Pregnancies are, in up to 80% of cases, on the contralateral side to the obstructed hemivagina, but they have also been reported on the same side [7]. High rates of preeclampsia (14%), preterm delivery (36%), high frequency (38%) of breech presentation and caesarean section rate (67%) are common obstetric complications found in patients with OHVIRA syndrome and patients should be appropriately counselled [7,20,21]. The treatment as described in this case involves a simple correction of the vaginal obstruction by means of a vaginal septectomy. This will relieve the menstrual flow and spontaneously drain the haematocolpos, haematometra and haematosalpinx. Some authors advocate that the septectomy should be followed by the complete resection of the vaginal septum and vaginal remodelling depending on the thickness of the septum either as a single or two-stage procedure [22]. In any case, a simple septectomy is highly effective to relieve dysmenorrhea and can also achieve resolution of endometriosis if present [23]. Early diagnosis of the condition can prevent aggressive interventions with long-term reproductive implications,such as salpingectomy and hemihysterectomy. that are used to treat delayed complications of the obstruction such as tuboovarian abscess and pyometra [7,22].
Figure 3.
Coronal T2 weighted MR image shows 2 cervical canals (white arrow indicates the two cervical canals. The right-sided cervix leads to the obstructed haematopyocolpos). OHVIRA syndrome, also known as Herlyn–Werner–Wunderlich syndrome, is a rare uterine and renal congenital abnormality which is characterized by an obstructed hemivagina and ipsilateral renal agenesis [1]. The exact prevalence of the syndrome has not been yet estimated, but it has been reported that it accounts for 0,16%-10% of Mullerian abnormalities, the incidence of which is 2-3% of the population [2]. Assessment by pelvic ultrasound in combination with MRI help to establish an accurate clinical diagnosis [3]. In the majority of cases, pubertal women are more likely to be identified with the syndrome, since the onset of menstrual periods might lead to hematometra and/or delayed menarche. However, in cases of partial obstruction, the diagnosis can be elusive, often taking years to be established, leading at times to women presenting in adulthood with symptoms resembling pelvic infection and endometriosis [4]. Septectomy remains the treatment of choice and should be performed in all affected patients. Knowledge of this rare condition and maintaining high levels of suspicion is critical in these cases [5,6]. Its complex embryological origin makes OHVIRA syndrome a complicated, heterogeneous condition that can be challenging to diagnose. The common triad of congenital variations (uterus didelphys, obstructed hemivagina and renal agenesis on the same side of the vaginal abnormality) is not always present, as reports have indicated that there can also be a septate uterus in up to 22% of cases [7] The renal anomalies can also include an ectopic ureter or a dysplastic kidney [8,9]. Variants of the syndrome have also been reported, where there is a fenestration in the vaginal septum that results in a partial obstruction [6], or cases when the septum is very thin and menstrual contents cause it to perforate leading to communication between the two vaginas [10]. Patients with this type of vaginal variation, such as in our case report, will have normal menses through the patent hemivagina and will typically have a delayed diagnosis much later during their reproductive years. Whereas the classic clinical presentation is that of a prepubertal girl around menarche presenting with pelvic pain, and a vaginal bulge is present on examination, indicating haematocolpos, cases that present in adulthood can be misdiagnosed with more common conditions such as pelvic infection, tuboovarian abscess, or endometriosis.In adulthood, patients will usually present with progressive dysmenorrhea and lower abdominal pain and will also possibly report urinary retention and offensive vaginal discharge [11]. On an acute basis, they might present with symptoms of an acute pelvic infection, secondary to pyocolpos, leading to a pyometra and tubo-ovarian abscess. These cases can closely resemble the symptoms of PID, and clinicians will need a high index of suspicion as the patients will not respond to antibiotics. Furthermore, endometriosis, in the form of ovarian or deep infiltrating endometriosis, can be found in 17-36% of these patients [12,13], with the most likely pathogenesis being the inability of the obstructed hemivagina to distend due to the thick septum resulting in retrograde menstruation [14]. Studies indicate that the age of diagnosis of pelvic endometriosis usually comes much earlier than the diagnosis of OHVIRA syndrome [15] and clinicians should be aware that patients with Mullerian anomalies can develop severe endometriosis, particularly in cases with an obstructed outflow tract [16]. Thus, in adolescent girls diagnosed with pelvic endometriosis, due to symptoms of dysmenorrhea with an onset close to menarche, an obstructive genital abnormality should be considered as a potential diagnosis [17]. Studies have shown that over 30% of female patients with a unilateral renal agenesis or multicystic dysplastic kidney have an associated uterine anomaly, so such a finding should always trigger further imaging of the uterus either by ultrasound or MRI.[18] Screening young women, before menarche if possible, with such renal abnormalties for Mullerian anomalies would potentially prevent not only acute presentations, such as the one we describe in this case, but also long-term complications associated with untreated obstructive malformations. Clear guidelines are currently scarce to guide this type of screening and are needed to ensure adequate communication between sonographers, paediatricians, and gynaecologists to diagnose this syndrome early [18]. They would also help to promote age-specific treatment of the vaginal obstruction [19]. Studies on long-term reproductive outcomes in patients with OHVIRA syndrome indicate that a delayed diagnosis is associated with high rates of PID, pelvic adhesions and endometriosis, although thankfully not subfertility [7,20]. Pregnancies are, in up to 80% of cases, on the contralateral side to the obstructed hemivagina, but they have also been reported on the same side [7]. High rates of preeclampsia (14%), preterm delivery (36%), high frequency (38%) of breech presentation and caesarean section rate (67%) are common obstetric complications found in patients with OHVIRA syndrome and patients should be appropriately counselled [7,20,21]. The treatment as described in this case involves a simple correction of the vaginal obstruction by means of a vaginal septectomy. This will relieve the menstrual flow and spontaneously drain the haematocolpos, haematometra and haematosalpinx. Some authors advocate that the septectomy should be followed by the complete resection of the vaginal septum and vaginal remodelling depending on the thickness of the septum either as a single or two-stage procedure [22]. In any case, a simple septectomy is highly effective to relieve dysmenorrhea and can also achieve resolution of endometriosis if present [23]. Early diagnosis of the condition can prevent aggressive interventions with long-term reproductive implications,such as salpingectomy and hemihysterectomy. that are used to treat delayed complications of the obstruction such as tuboovarian abscess and pyometra [7,22].
Author Contributions
A.L.G. wrote the initial draft and performed the literature review. F.A. conceptualised the case report and made editorial amendments. D.W. reviewed all images and helped with the figure legends. T.D. supervised the project and made substantial editorial amendments. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
All data generated or analysed during this study are included in the article.
Acknowledgments
The authors thank the patient for their cooperation.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| PID | Pelvic inflammatory disease |
| TOA | Tuboovarian abscess |
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| CRP | C-reactive protein |
| WCC | White cell count |
| T | Temperature |
| RR | Respiratory rate |
| HR | Heart rate mg/L: milligrams per litre mmol/L: millimole per litre |
| SO2 | saturation of oxygen |
References
- Yang, M.; Wen, S.; Liu, X.; He, D.; Wei, G.; Wu, S.; Huang, Y.; Ni, Y.; Shi, Y.; Hua, Y. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA): Early diagnosis, treatment and outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 261, 12–16. [Google Scholar] [CrossRef]
- Dural, O.; Tas, I.S.; Ugurlucan, F.G.; Yasa, C.; Evruke, I.; Bakir, B.; et al. Unique Diagnosis of Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) at the Time of FirstTrimester Ultrasound Imaging. Journal of pediatric and adolescent gynecology 2020, 33, 748–51. [Google Scholar] [CrossRef] [PubMed]
- Robbins, J.B.; Broadwell, C.; Chow, L.C.; Parry, J.P.; Sadowski, E.A. Müllerian duct anomalies: embryological development, classification, and MRI assessment. J. Magn. Reson. Imaging. 2015, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Wen, S.; Liu, X.; He, D.; Wei, G.; Wu, S.; Huang, Y.; Ni, Y.; Shi, Y.; Hua, Y. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA): Early diagnosis, treatment and outcomes. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 261, 12–16. [Google Scholar] [CrossRef]
- González Ruiz, Y.; Delgado Alvira, R.; Siles Hinojosa, A.; Izquierdo Hernández, B.; Rihuete Heras, M.Á. Diagnosis of OHVIRA syndrome in prepuberty: Is it possible? An Pediatría (English Ed [Internet]. 2019, 90, 244–245. [Google Scholar] [CrossRef]
- Fedele, L.; Motta, F.; Frontino, G.; Restelli, E.; Bianchi, S. Double uterus with obstructed hemivagina and ipsilateral renal agenesis: pelvic anatomic variants in 87 cases. Hum. Reprod. 2013, 28, 1580–1583. [Google Scholar] [CrossRef] [PubMed]
- Haddad, B.; Barranger, E.; Paniel, B.J. Blind hemivagina: long-term follow-up and reproductive performance in 42 cases. Hum. Reprod. 1999, 1962–1964. [Google Scholar] [CrossRef]
- Acien, P.; Susarte, F.; Romero, J.; et al. Complex genital malformation: ectopic ureter ending in a supposed mesonephric duct in a woman with renal agenesis and ipsilateral blind hemivagina. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 117, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, Y.; Nakada, S.; Hitomi, K.; Hanaki, S.; Doi, K.; Goto, T.; et al. Urological anomalies associated with obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome, a case series. J Pediatr Surg Case Reports [Internet]. 2020, 52, 101358. [Google Scholar] [CrossRef]
- Santos, X.M.; Dietrich, J.E. Obstructed hemivagina with ipsilateral renal anomaly. J. Pediatr. Adolesc. Gynecol. 2016, 29, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.; Abdi, S. Diverse Presentations of OHVIRA Syndrome: A Case Series. Clin Pediatr (Phila). 2021, 6–8. [Google Scholar] [CrossRef]
- Fedele, L.; Bianchi, S.; Di Nola, G.; Franchi, D.; Candiani, G.B. Endometriosis and nonobstructive Mullerian anomalies. Obstet. Gynecol. 1992, 79, 515–517. [Google Scholar] [PubMed]
- Tong, J.; Zhu, L.; Chen, N.; Lang, J. Endometriosis in association with Herlyn-WernerWunderlich syndrome. Fertil. Steril. 2014, 790–794. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, J.S.; Wakim, N.G.; Schikler, K.N.; Yussman, M.A. Endometriosis in association with uterine anomaly. Am. J. Obstet. Gynecol. 1986, 39–43. [Google Scholar] [CrossRef]
- Audebert, A. Caractéristiques de l'endométriose de l'adolescente: à propos d'une série de 40 cas [Characteristics of adolescent endometriosis: apropos of a series of 40 cases]. Gynecol Obstet Fertil. 2000, 450–454, French. [Google Scholar]
- Kudela, G.; Wiernik, A.; Drosdzol-Cop, A.; Machnikowska-Sokołowska, M.; Gawlik, A.; HylaKlekot, L.; Gruszczyńska, K.; Koszutski, T. Multiple variants of obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome - one clinical center case series and the systematic review of 734 cases. J. Pediatr. Urol. 2021, 653.e1–653.e9. [Google Scholar] [CrossRef]
- Yang, M.; Wen, S.; Liu, X.; He, D.; Wei, G.; Wu, S.; et al. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA): Early diagnosis, treatment and outcomes. Eur J Obstet Gynecol Reprod Biol [Internet]. 2021, 261, 12–16. Available from: https://pubmed.ncbi.nlm.nih.gov/33873082/. [CrossRef]
- Friedman, M.A.; Aguilar, L.; Heyward, Q.; Wheeler, C.; Caldamone, A. Screening for Mullerian anomalies in patients with unilateral renal agenesis: Leveraging early detection to prevent complications. J. Pediatr. Urol. 2018, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Zarfati, A.; Lucchetti, M.C. OHVIRA (obstructed hemivagina and ipsilateral renal anomaly or Herlyn-Werner-Wunderlich syndrome): Is it time for age-specific management? J. Pediatr. Surg. 2022, S0022-3468(22)00274-3. [Google Scholar] [CrossRef]
- Heinonen, P.K. Pregnancies in women with uterine malformation, treated obstruction of hemivagina and ipsilateral renal agenesis. Arch. Gynecol. Obstet. 2013, 975–978. [Google Scholar] [CrossRef]
- Candiani, G.B.; Fedele, L.; Candiani, M. Double uterus, blind hemivagina, and ipsilateral renal agenesis: 36 cases and long-term follow-up. Obstet Gynecol. 1997, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Skinner, B.; Quint, E.H. Obstructive Reproductive Tract Anomalies: A Review of Surgical Management. J. Minim. Invasive Gynecol. 2017, 901–908. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, J.E.; Millar, D.M.; Quint, E.H. Obstructive reproductive tract anomalies. J. Pediatr. Adolesc. Gynecol. 2014, 396–402. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



