
Submitted:
04 August 2023
Posted:
04 August 2023
You are already at the latest version
Abstract
A surgical technique aimed at rerouting aqueous humor (AH) outflow from the anterior chamber to the suprachoroidal space (SCS) without performing surgical cyclodialysis was developed to decrease intraocular pressure (IOP) in glaucoma patients. The surgical outcomes of the technique were retrospectively analyzed in fifty-eight patients. At 6, 12, and 24 months, the mean IOP decreased from 27.8±8.3 to 14.95.0 mmHg, median 15.0 (25th percentile (p25 )13.0; 75th percentile (p75) 18.0), and 15.23.3 mmHg; hypotensive medication use reduced from median (p25; p75) 3 (2; 3) to 0 (0; 2), 0 (0; 2), and 0 (0; 1.5), and complete success was achieved in 62.8%, 51.2%, and 32.5% cases, with partial success in 28.4%, 44.2%, and 62.5% cases, respectively. Eight cases (13.8%) presented unsatisfactory outcomes. Intra- and postoperative complications were few and manageable. No bleb formation was observed in any of the cases. In 50% of cases, conjunctival lymphatic vessels (CLVs) developed following surgery in superior quadrants. The technique is safe and effective in providing a long-term decrease in IOP and hypotensive medication use. It was hypothesized in this study that the IOP decrease occurred as a result of enhanced AH outflow from the SCS to CLVs through intrascleral microchannels connecting the SCS to CLVs.
Keywords:
glaucoma
; open-angle glaucoma
; collagen implant
; glaucoma surgery
; bleb less glaucoma surgery
; bleb independent glaucoma surgery
; suprachoroidal space
; uveolymphatic aqueous humor outflow
; conjunctival lymphatic vessels
; conjunctival lymphatics
1. Introduction
Glaucoma is a neurodegenerative ocular disease. The imbalance between aqueous humor (AH) production and outflow results in increased intraocular pressure (IOP). AH outflows from the anterior chamber (AC) via trabecular (traditional) and non-trabecular (non-traditional) pathways [1].
Penetrating and non-penetrating filtering glaucoma surgeries performed for the management of open-angle glaucoma (OAG) aim to create an artificial pathway for AH outflow. Penetrating glaucoma surgeries are effective for a long-term decrease in IOP but may produce various complications [2,3]. Non-penetrating glaucoma surgeries are safer; however, they produce a short-term hypotensive effect, and Nd:YAG laser goniopuncture is a mandatory step to maintain the hypotensive effect [4,5]. Both classes of glaucoma surgeries are bleb dependent. The AH, after leaving the AC, accumulates in a subconjunctival space (bleb), from where it may percolate into the cut ends of the Schlemm’s canal, outflows to the suprachoroidal space (SCS), or become absorbed into the conjunctival blood vessels or lymphatics [6,7]; or, if the bleb is thin-walled, it passes directly across the conjunctiva into the tear layer [8,9]. Fibrosis occurring at the operation site is the main reason for bleb failure. Recently, antimetabolites have been used both intra- and postoperatively to prevent the occurrence of fibrosis; however, their use has increased the risk of the development of certain complications, such as bleb leakage, blebitis, and endophthalmitis [10].
The non-trabecular (non-traditional) outflow pathway has good potential to decrease IOP. Various surgical techniques and modifications of the existing techniques in the field have been proposed in the literature, and different devices are used in clinical practice, to date, to enhance AH outflow via this pathway. However, the surgical outcomes of these techniques and devices are unpredictable [11,12,13,14,15,16]. In most of these techniques, performing surgical cyclodialysis is mandatory.
We developed a surgical technique aimed at rerouting AH outflow from the AC to the SCS without performing surgical cyclodialysis to decrease IOP in glaucoma patients, and, in a pilot study, we reported the short-term surgical outcomes demonstrating a decrease in IOP without the formation of a bleb and the development of conjunctival lymphatic vessels (CLVs) in 40% of the examined cases [17,18]. In this paper, we report the medium- and long-term surgical outcomes of the technique we employed.
2. Materials and Methods
In this non-randomized and non-comparative interventional case series, a total of ninety-eight patients were operated upon. Of these, fifty-eight patients fulfilled the inclusion criteria. Glaucoma surgery was performed as a standalone procedure in 18 eyes (31%) and in combination with cataract surgery in 40 eyes (69%). One surgeon (VK) performed all the operations between 1 January 2020 and 31 December 2021.
Inclusion criteria were OAG, decompensated IOP following previous glaucoma surgeries, medically uncontrolled IOP, OAG in pseudophakic eyes, and a minimum postoperative follow-up period of 25 weeks.
Exclusion criteria were angle closure glaucoma, secondary glaucoma, intraocular lens (IOL) dislocation with decompensated IOP, patients on anticoagulants, and patients with micro-perforations of the trabecular meshwork (TM) that occurred during surgery.
Prior to surgery, all patients underwent a comprehensive ophthalmological examination. Visual acuity (VA) was assessed using Snellen’s chart. The VA values were converted to a logarithm of the minimum angle of resolution (logMAR). Tonometry was performed with an iCare tonometer (ic100, Icare Finland Oy, Vantaa, Finland) [19]. The median values of three consecutive measurements were considered [20]. The IOP values were adjusted for corneal thickness using the pachymeter application of spectral domain optical coherence tomography (OCT) (SOCT Copernicus Revo 80, OPTOPOL Technology Sp.z.o.o., Zawiercie, Poland). The patients’ field of vision was tested on a perimeter Perigraph Perikom (Spetsmedpribor Co. Ltd., Moscow, Russia). An OCT glaucoma analysis was conducted provided the native lens condition permitted this.
Preoperatively, the patient’s ocular hypotensive medications were not washed out. Antibacterial (sol. Levofloxacin 0.5%, 1–2 drops, 3 times per day) and anti-inflammatory (sol. Bromfenac 0.09% once per day) medications were prescribed to patients for a period of three days prior to surgery.
2.1. Surgical Technique
The details of the surgical technique we employed are described elsewhere [18]. The aim of the technique to reroute AH outflow from the AC to the SCS without performing surgical cyclodialysis was achieved, first, by creating an intrascleral reservoir (ISR) to receive and accumulate AH from the AC. From the ISR, a suprachoroidal tunnel was created and a collagen implant (CI) was inserted into it, leaving one end in the ISR. The CI acted as a spacer for the ISR and suprachoroidal tunnel and as a conduit for AH flow from the ISR to the SCS. The Schlemm’s canal was deroofed without creating a window in the trabeculo-Descemete’s membrane, and a part of the juxtacanalicular connective tissue (JCT) was removed. Postoperatively, if the IOP was observed to be elevated, Nd:YAG laser trabeculotomy was performed at the surgery site to allow for resistance-free AH flow from the AC to the ISR and SCS. This was performed no earlier than postoperative days 7–10, allowing enough time for the conjunctiva to heal, thus preventing AH flow from the ISR to the subconjunctival space. Sclerectomy was performed in the posterior section of the ISR to prevent the occurrence of choroidal effusion and to expose more uveal tissue for the resorption of AH.
The ophthalmic CI (MakMedi, Moscow, Russia) used in this case series was composed of collagen material obtained from farm animals. These implants are hydrophilic implants and are biologically inert. When immersed in fluid, the implants swell and thicken. The frontal dimensions practically remain unchanged. With time, the implants are slowly resorbed by tissue fluids. They are commercially available and are permitted for use in human beings. For our purposes, we selected implants measuring 0.1*2*5 mm.
All surgeries were performed on an ambulatory basis. Following the surgery, a monocular eye pad was applied on the operated eye. Postoperatively, a standard postoperative protocol was followed by the patients. Five hours after the surgery, the patients removed their eye pads and begun the eye drop instillation process: dexamethasone (0.1% solution) eye drops were used three times per day for the first week, which was then reduced to one drop per week, and the instillation of levofloxacin eye drops (0.5% solution) was continued three times per day for one additional week. In the case of suture irritation, the patients were advised to apply an antibiotic ointment (Ofloxacin ointment 0.3%) until the sutures were removed. The patients continued with the instillation of hypotensive medications. All patients attended the out-patient department the day after surgery. In cases where a patient’s IOP was higher than the target IOP, he/she was advised to continue with the instillation of hypotensive medications, and if the IOP was lower than the target IOP, the patients were advised to terminate the instillation of eye drops. Conjunctival sutures were removed 7–10 days following surgery. On this day, if the IOP remained elevated, Nd:YAG laser trabeculotomy was performed and the patient was instructed to stop instillation of antiglaucoma medications. All patients were evaluated on days 1 and 7 and then at 1, 3, 6, 9, 12, 18, and 24 months. If laser trabeculotomy was performed, the first postoperative day was the day following the Nd:YAG laser trabeculotomy; otherwise, the first day was the subsequent day, after the surgery. The postoperative assessment included VA assessment, tonometry, slit lamp examination, direct ophthalmoscopy, and gonioscopy. Wherever possible, the results were documented using a digital photo slit lamp. In each follow-up session, the surgical site and adjunct areas were evaluated using OCT.
A slit lamp-mounted Nd:YAG laser (OptoYAG, Optotek medical, Slovenia) and a single-mirror laser gonio lens (OLSLTF, Latina SLT Gonio Laser Lens, Ocular instruments, Bellevue, WA, USA) were used to perform Nd:YAG laser trabeculotomy. Usually, 3 or 5 millijoules of energy was selected and one or more openings were created in the trabecular meshwork (TM). In a successful trabeculotomy case, the pulsatile movement of AH passing through it was detected.
OCT images taken prior to and following the surgery were acquired by using the commercially available SOCT Copernicus Revo 80, using the technique described earlier [18] and were evaluated as per Kawana K. et al. [21]. In Figure 1, the OCT evaluation of the surgery and adjunct sites is presented.
The outcome measures were IOP change, the use of hypotensive medication(s), complications, and the need for a second surgery.
Eyes with mild OAG had a target IOP of at least 20% reduction from the baseline or IOP ≤ 21 mmHg (whichever was lower); eyes with moderate and severe OAGs had a target IOP of at least 30% reduction from the baseline or ≤ 18 mmHg (whichever was lower) [22,23].
Complete success was assigned to a case if, at the last follow-up visit, the target IOP was achieved without the use of additional glaucoma medications. In the case of a qualified success, the target IOP was achieved with or without the use of glaucoma medications. Cases with partial success were those that achieved target IOPs with the use of additional hypotensive medications. A case was judged as a failure case if his/her IOP level was measured above the upper limit or below the lower limit during two consecutive visits and if further glaucoma interventions were required. In cases with preoperative medically controlled IOPs, the IOP reduction was assessed by the percentage reduction in the IOP value. IOP reduction had to be greater than 20% for it to be considered a success. Fixed-combination glaucoma medications were counted as two separate medications.
2.2. Statistics
The Shapiro–Wilk test was used to determine the distribution of continuous variables. Categorical variables were described as the frequency with percentage. Continuous and discrete variables were described as means with standard deviations (SDs) or median with percentiles (p25; p75). A paired Student’s T-test was applied to calculate the significance between two paired groups for parametric variables, and a Wilcoxon rank sum test was used for non-parametric variables. VA and medications were examined using Friedman and Wilcoxon signed-rank tests. The success of the treatment was expressed by the Kaplan–Meier curve, and p-values below 0.05 were considered statistically significant. SPSS Statistics (IBM SPSS Statistics, Armonk, New York, USA) 28.0.0.0 software for Windows 7 and the Excel application of Microsoft Office 365 (Microsoft Corporation, Redmond, WA, USA) were used for statistical processing purposes.
3. Results
The demographic and clinical data of 58 patients who satisfied the inclusion criteria are presented in Table 1.
A scatterplot showing the distribution of preoperative IOPs is presented in Figure 2.
3.1. IOP change
Following surgery at 6, 12, 18, and 24 months, the baseline IOP mean ± SD (95% confidence interval) decreased to 14.9 ± 5.0 (13.5–16.3), median 15.0 (13.0; 18.0), 16.5 ± 6.2 (14.1–18.8), and 15.2 ± 3.3 (13.5–16.9) mm Hg, respectively. The IOP change, percentage reduction in IOP from preoperative values, and p values at follow-up visits are presented in Table 2 and are illustrated in Figure 3 and Figure 4.
The distribution of patients as a percentage reduction in IOP at different follow-up visits is presented in Table 3. As can be observed from the table, most patients presented a decrease in IOP values by more than 40%.
3.2. Change in use of hypotensive medications
The median value of hypotensive medications used by patients preoperatively was 3 (2; 3). The use of hypotensive medications at 6, 12, and 24 months was 0 (0; 2), 0 (0; 2), and 1 (0; 1,25), respectively. The change in the use of hypotensive medications following surgery is presented in Figure 5. As can be observed from the diagram, additional hypotensive medication was required by patients after a period of 18 and 24 months.
3.3. Visual acuity
Average VA improved in all cases in whom a combined surgery was performed (Figure 6), whereas it remained unchanged in cases where glaucoma surgery was performed as a standalone procedure.
3.4. Success
At 6, 12, 18, and 24 months, complete success was achieved in 62.8% (32/51), 51.2% (22/43), 46.7% (14/30), and 32.5% (6/16) of cases, respectively, and partial success was achieved in 28.4% (14/51), 44.2% (19/43), 50% (15/30), and 62.5% (10/16) of cases, respectively. Eight cases (13.8%) did not achieve target IOP values, of which five cases were declared as failures at 6 months, another 2 cases at 12 months, and another 1 case at 18 months. In four cases, the reason for this was the blockage of the trabeculotomy opening by iris tissue. Four additional cases presented advanced stage glaucoma, of which three cases previously failed filtering surgeries.
Kaplan–Meier curve showing success of treatment is presented in Figure 7.
3.5. Observations during surgery
In all 16 cases, having previously undergone filtration surgeries, the surgery was attempted close to the previous surgery area, and certain difficulties in performing the dissection of the conjunctival and scleral flaps were faced by the surgeons because of existing fibrosis. However, no difficulties or complications were encountered during the operation while creating a supraciliary tunnel and inserting the CI into it. No complication related to glaucoma surgery was noticed in any of the other cases.
3.6. Observations in the postoperative period
Postoperatively, one case was reported with a spontaneous retinal hemorrhage not related to surgery, which resolved after one month. There was no evidence of cases of hypotony or shallow AC during the follow-up period. The blockage of the trabeculotomy by iris tissue (Figure 8 A, B) leading to an elevated IOP was observed in four cases; in two cases, the IOP was medically controlled; and, in another case, a repeat trabeculotomy performed close to the blockage site lowered the IOP below the target level, and it remained at this level for the rest of the follow-up period. In the fourth case, a second surgery was required.
3.7. Nd:YAG laser trabeculotomy
Nd:YAG laser trabeculotomy was requierd in 67.2% cases (39/58). Some oozing of blood from Schlemm’s canal immediately after the trabeculotomy was performed was observed in two cases (Figure 8C). The blood resolved spontaneously within one week.
The distribution of patients according to the time that passed between the surgery and laser trabeculotomy is presented in Table 4. Most of the trabeculotomies were performed within one month following surgery—in 84.6% of cases (33 out of 39 eyes).
Trabeculotomy was performed once on 30 eyes. Nine eyes (23%) required more than one trabeculotomy procedure. Of these, in six eyes, the trabeculotomy was performed twice to achieve the target-level IOP, reaching the target level in only two eyes. Four additional eyes required additional hypotensive medications. In another two eyes, trabeculotomies were performed three times, and in one eye, four times, all in vain. A second trabeculotomy was required in four eyes within a period of one month, in one eye after four months, and in another eye after seven months.
3.7.1. IOP decrease after Nd:YAG laser trabeculotomy
In 76.9% of eyes (30/39) IOP values were less than 15 mmHg after laser trabeculotomy (Table 5).
During the Nd:YAG laser trabeculotomy procedure, the following events were observed: difficulty in identifying the surgery site—four cases; pulsatile AH flow after trabeculotomy—12 cases; and blood oozing from trabeculotomy—two cases. After trabeculotomy, in one case, the Tindal phenomenon was observed, requiring the instillation of anti-inflammatory medication for 3–4 days. In four cases, the blockage of the trabeculotomy by iris tissue leading to IOP elevation was observed. To prevent this complication from occurring, in cases that underwent combined procedures, a peripheral iridotomy using a 100 µm tip of a Fugo plasma blade was performed at the end of cataract surgery. In standalone cases prior to surgery, Nd:YAG laser iridotomy was performed in the out-patient department.
3.8. Filtration bleb
Some tissue reaction to surgical trauma was noticed at the surgery site on the day after surgery. The OCT of the surgery site demonstrated the absence of blebs in all cases except one, where a bleb lasted for a period of one month.
3.9. CLVs development
The postoperative development of lymphatic vessels in the conjunctiva was observed in 50% of cases (29/58). Biomicroscopically, these vessels had uneven calibers and were visible in the form of a plexus or solitary vessels running parallel to the limbus or perpendicular to it. The lymphatic nature was confirmed by OCT [21]. Sausage-type vessels with valve like structures (VLS) in their lumens were evident.
The time of CLVs development differed from case to case. In six eyes, CLVs developed the following day after Nd:YAG laser trabeculotomy was performed, in seven eyes after one week, and in 14 eyes after one month. In summary, in 93.1% eyes (27 out of 29 eyes), CLVs developed within one month. In two eyes, CLVs developed late, at six months in one eye and at nine months in another eye.
The CLVs lasted for different periods of time. The time of CLV development and the duration of CLV visibility via biomicroscopy are presented in Table 6. On OCT, CLVs with VLS in their lumens were diagnosed in most cases—in 82.8% eyes (48/58).
No relationship was established between Nd:YAG laser trabeculotomy and the development of CLVs. CLVs were observed to develop irrespective of Nd:YAG laser trabeculotomy (Figures 9,10). Of thirty-nine eyes that underwent Nd:YAG laser trabeculotomy, CLVs developed in 46.1% eyes (18/39 eyes), whereas in eyes without laser trabeculotomy, they developed in 52.6% eyes (10/19 eyes), suggesting that the role of laser trabeculotomy was limited to provide AH resistance-free flow from the AC to the SCS.
Figure 9.
Slit lamp view of the surgery site and superior quadrants in a patient’s left eye in whom CLVs developed immediately after Nd:YAG laser trabeculotomy. (A) 10 minutes after Nd:YAG laser trabeculotomy, surgery site and nearby areas free from CLVs; some swelling at the surgery site persists. (B) 10 minutes after Nd:YAG laser trabeculotomy, slit lamp view of the superior temporal quadrant showing a CLVs plexus (black arrows). (C) 30 minutes after the procedure, slit lamp view of the superior temporal quadrant after massaging the area with the lid margin; a well-developed CLVs plexus is observed far from the surgery site. CLV=conjunctival lymphatic vessel; Nd:YAG laser = neodymium yttrium aluminum garnet laser.
Figure 9.
Slit lamp view of the surgery site and superior quadrants in a patient’s left eye in whom CLVs developed immediately after Nd:YAG laser trabeculotomy. (A) 10 minutes after Nd:YAG laser trabeculotomy, surgery site and nearby areas free from CLVs; some swelling at the surgery site persists. (B) 10 minutes after Nd:YAG laser trabeculotomy, slit lamp view of the superior temporal quadrant showing a CLVs plexus (black arrows). (C) 30 minutes after the procedure, slit lamp view of the superior temporal quadrant after massaging the area with the lid margin; a well-developed CLVs plexus is observed far from the surgery site. CLV=conjunctival lymphatic vessel; Nd:YAG laser = neodymium yttrium aluminum garnet laser.
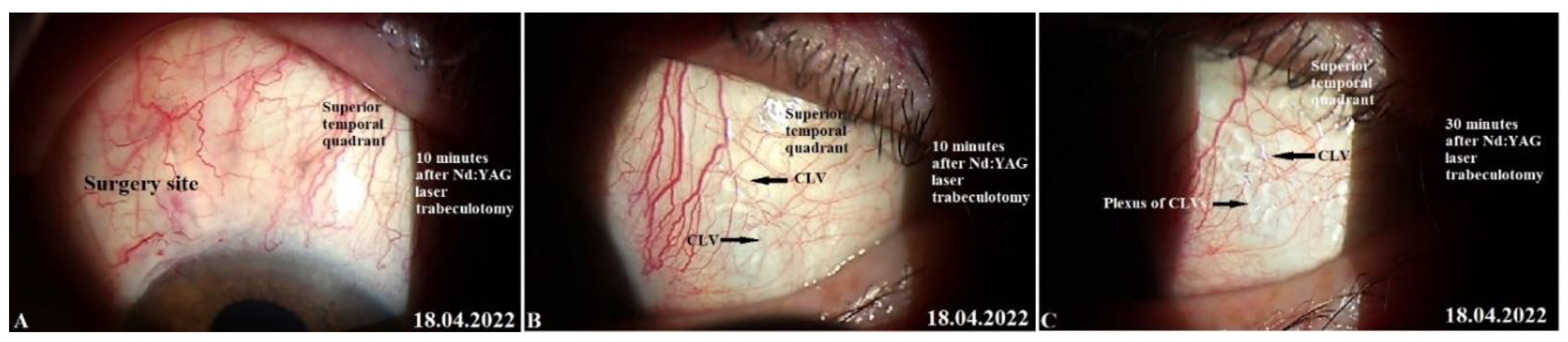
Figure 10.
Slit lamp view of the right eye of a patient in whom CLVs developed without Nd:YAG laser trabeculotomy. (A) Slit lamp view of the superior temporal quadrant of the eyeball on day 21 after surgery showing a plexus of CLVs located away from the surgery site (arrow with black borders). (B) The same view with a red-free filter. (C) Same site as in A and B, an Enface image (OCT angio) demonstrating sausage-shaped lymphatic vessels with uneven calibers (arrows with black borders). CLV = conjunctival lymphatic vessel.
Figure 10.
Slit lamp view of the right eye of a patient in whom CLVs developed without Nd:YAG laser trabeculotomy. (A) Slit lamp view of the superior temporal quadrant of the eyeball on day 21 after surgery showing a plexus of CLVs located away from the surgery site (arrow with black borders). (B) The same view with a red-free filter. (C) Same site as in A and B, an Enface image (OCT angio) demonstrating sausage-shaped lymphatic vessels with uneven calibers (arrows with black borders). CLV = conjunctival lymphatic vessel.

Interesting facts were uncovered when the site of CLV development was analyzed as per the operated eye. The results are presented in Table 7. In cases where surgery was performed on the right eye, CLVs developed more commonly in the nasal quadrant, and in cases where surgery was performed on the left eye, CLVs developed more commonly in the temporal quadrant. Out of 17 cases where glaucoma surgery was performed in the right eyes of patients, in 16 cases (94.1%), CLVs developed in the nasal quadrant. Of these, in five eyes, CLVs developed in both quadrants. The quantitative analysis of CLVs identified on OCT presented the same pattern—in the superior nasal quadrant, they were identified in 20 out of 24 eyes (83.3%). Nearly the same pattern of CLV development was noticed in the left eyes of patients. In cases where surgery was performed on the left eyes (12 eyes), CLVs were predominant in the temporal area in nine eyes (75.0%). The same was true for OCT—CLVs were identified in the temporal area (60.7%) in 17 out of 28 eyes.
In all except one case, CLVs developed in an area located away from the surgery site. CLVs developed from the sclera, indicating the existence of intrascleral microchannels located across the sclera connecting the SCS to the CLVs (Figure 9C). Clinically, we observed a few patients in whom CLVs first appeared in one quadrant; with time, they disappeared, but new CLVs developed in another quadrant (pl. refer to case 2).
To define the relationship between CLV development and the decrease in IOP, all cases were divided into two subgroups: subgroup I included cases with CLVs identified via a slit lamp and subgroup II included cases without CLV identification. In each subgroup, the success rate was analyzed. The results are presented in Table 8. The number of cases in both subgroups was equal. The analysis showed that the rate of complete success was higher in subgroup II, achieving 75.9% versus 37.9% in subgroup I (p=0.000368). The qualified success rate was equal in both subgroups. The instillation of hypotensive medications to achieve target IOP values was required by more patients in subgroup I—by 44.8% patients versus 13.8% patients in subgroup II (p=5.13X10-5). There was no difference in failure rates in both subgroups. These results suggest that the development of CLVs after surgery has a poor prognostic value for IOP control. If the fluid flow from the SCS to CLVs through intrascleral microchannels is smooth and resistance-free, no CLV development is evident. However, if any resistance exists in the flow, the fluid accumulates in lymphatics, resulting in their engorgement and longer visibility period.
Below, we present a few clinical cases to demonstrate the effectiveness and safety of the proposed technique, the role of Nd:YAG laser trabeculotomy, the impact of CLVs development on IOP decrease, and the possible mechanism of the hypotensive effect produced by the technique without forming a filtration bleb.
3.10. Case reports
Case 1. Patient K, a 78-year-old female patient with advanced stage glaucoma in her right eye and moderate-stage glaucoma in her left eye underwent combined surgery in both eyes. Glaucoma was diagnosed five years ago and, since then, the patient has been on four classes of hypotensive medications in both eyes (analog of prostaglandins F2α, beta blocker, carbonic anhydrase inhibitor, and selective α 2-adrenomimetic). Her IOP prior to surgery was 27.0 mmHg in both eyes. The patient had a history of intravitreal injections of antiVEGF (sol. Lucentis—three injections) for wet macular degeneration in her right eye. Her preoperative best-corrected visual acuity (logMAR) was 0.1 in both eyes.
Right-eye surgery. On 14 April 2020, under retrobulbar anesthesia (2% solution of lidocaine hydrochloride), the patient underwent a combined procedure. Prior to surgery, no washout of hypotensive medications was performed. First, phacoemulsification with an implantation of a foldable acrylic IOL in the capsular bag was performed, followed by glaucoma surgery, as previously described. Intraoperatively, no complications were encountered. Postoperatively, the patient followed a standard protocol. On day 16, conjunctival sutures were removed. On day 21, the patient’s IOP on hypotensive medications was 23 mmHg and she underwent Nd:YAG laser trabeculotomy in the operated area.
IOP change. Immediately following the laser trabeculotomy procedure, some swelling was observed at the surgery site (not a bleb according to OCT), and to avoid the blockage of the trabeculotomy opening by iris tissue, the instillation of 1% pilocarpine eye drops twice daily was advised for three days, and the patient was advised to cease the instillation of other hypotensive medications. On the following follow-up visit on day 10, after the trabeculotomy, no filtration bleb was observed at the surgery site, and the patient’s IOP was 13 mmHg off medications. The patient was further followed up at predetermined intervals up to 2.5 years. At 3, 6, 12, 15, and 30 months, the patient’s IOP was 9, 13, 11, 16, and 9 mmHg, respectively, off medication. The absence of bleb was confirmed by OCT at all follow-up visits.
CLVs development. The following day after the trabeculotomy, a well-developed plexus of CLVs was identified biomicroscopically in the superior nasal quadrant. With the passage of time, these vessels reduced in number and size (Figure 11, Figure 12 and Figure 13). At the last follow-up visit, at 2.5 years, no CLVs were identified biomicroscopically. However, on OCT, CLVs were identifiable in the nasal and temporal quadrants until the last follow-up visit.
Left-eye surgery. On 23 September 2020, the patient underwent an identical-to-right-eye combined procedure on her left eye. No preoperative hypotensive medication washout was performed. First, phacoemulsification with the implantation of a foldable acrylic IOL in the capsular bag was performed, followed by glaucoma surgery. Surgery was uneventful. Postoperatively, on day 7, conjunctival sutures were removed. On days 1, 6, and 13, the patient’s IOP values on two classes of medications were 18, 13, and 25 mmHg, respectively. On day 13, the patient underwent Nd:YAG laser trabeculotomy at the surgery site.
IOP change. Immediately after the trabeculotomy, some swelling appeared at the surgery site (absence of bleb confirmed by OCT), and the IOP decreased to 11 mmHg. The patient was advised to discontinue the installation of hypotensive medication and was followed up for a period of 24 months with an interval of 3 months between visits. At 6, 12, 18, and 24 months, the patient’s IOP values were 15, 14, 10, and 10 mmHg, respectively, off medication.
CLVs development. The day after the laser trabeculotomy, a plexus of CLVs with uneven calibers and filled with transparent fluid was observed in the superior temporal quadrant (Figure 14A). During the subsequent follow-up visit, one week after the trabeculotomy (on 13 October 2020), CLVs were reduced in size and number (Figure 14B). By month 14, only an isolated CLV could be observed in the temporal quadrant (Fig.14C). The surgery site and superior nasal and temporal quadrants, which were investigated by OCT, showed CLVs with VLSs in their lumens (Figure 15A-C). At the final follow-up visit, CLVs were not visible biomicroscopically (Figure 16A-C).
By reporting this case, the role of Nd:YAG laser trabeculotomy in providing the resistance-free flow of AH from the AC to the SCS was emphasized in our study. The patient underwent combined surgery in both eyes, and laser trabeculotomies were performed after surgery on both eyes. Prior to the trabeculotomy, sufficient time was allowed for the conjunctiva to heal, thus preventing AH flow to the subconjunctival space, which was shown by OCT. Until the last follow-up visit, the patient presented a significant decrease in IOP without a filtering bleb. Postoperatively, CLVs, which were identified biomicroscopically, developed in both eyes. Notably, once the proper AH flow from the SCSs to CLVs was established, these vessels reduced in size and number, leaving a few (identified on OCT) to maintain the flow.
Case 2. Patient R., an 80-year-old male patient, was operated upon on his left eye for an underlying visually significant cataract and advanced-stage glaucoma. The patient had glaucoma in both his eyes, which was diagnosed seven years prior and, since then, he was on two classes of hypotensive medications (a combination of a carbonic anhydrase inhibitor and a beta blocker). Two years ago, the patient underwent cataract surgery in his right eye. Preoperatively, IOP levels on medications were 19 and 31 mmHg in his right and left eye, respectively. Best-corrected visual acuity (logMAR) values were 0.3 and 0.4 in his right and left eye, respectively.
Left-eye surgery. On 26 April 2021, the patient underwent a combined procedure under retrobulbar anesthesia (2% solution of lidocaine hydrochloride). Prior to surgery, no washout of hypotensive medications was performed. First, phacoemulsification with an implantation of a foldable acrylic IOL in the capsular bag was performed. Intraoperatively, no complications occurred. Postoperatively, the patient followed the standard protocol and continued the instillation of hypotensive medication. Conjunctival sutures were removed on day 10. His IOP was 10 mmHg on this day, and he was advised to discontinue the instillation of hypotensive medication. The patient was followed up at predetermined intervals up to 12 months. As his IOP was below the target level at all visits, no YAG laser trabeculotomy was performed.
IOP change. At 1, 3, 6, and 12 months, the patient’s IOP levels were 14, 10, 10, and 7 mmHg, respectively, off medication. Postoperative logMAR VA improved to 0 and remained at this value until the final follow-up visit.
CLVs development. At one week after surgery (on 13 May 2022), slit lamp biomicroscopy revealed an absence of bleb and CLVs. On OCT, the absence of bleb at the surgery site was confirmed, and CLVs were identified in the superior nasal and temporal quadrants and at the surgery site (Figure 17 A-F).
The patient was then consulted after another 2 weeks on 25 May 2022. On biomicroscopy, two CLVs were observed in the superior temporal quadrant (Figure 18 A-C); the lymphatics arose directly from the sclera located at a considerable distance from the surgery site and became more prominent when the upper eye lid closed over them (see Supplementary Materials Video S1_Case 2_month 1 after surgery: CLVs in superior temporal quadrant).
The patient’s subsequent consultation was on 22 June 2022 (1.5 months after surgery). The slit lamp showed that remnants of CLVs could be identified in the superior temporal quadrant. On OCT, CLVs were identifiable in the superior temporal quadrant and at the surgery site (Figure 19 A-D).
The patient’s last follow-up visit was at 12 months (on 21 April 2023). On biomicroscopy, no bleb was noticed at the surgery site and, notably, no CLVs were observed in the superior temporal quadrant; instead, close to the insertion of the internal rectus muscle and in the superior nasal quadrant, a plexus of CLVs was observed. Massaging the conjunctiva over the plexus by moving the lid margin over it caused the vessels to become engorged (Figure 20 A-C). Pl. refer to Supplementary Materials video S2_Case 2_month 12 after surgery: CLVs in superior nasal quadrant.
By reporting this case, we aimed to emphasize the effectiveness of the proposed technique in decreasing the IOP level without performing Nd:YAG laser trabeculotomy. The deroofing of the SC and the thinning of its inner wall by removing a part of the JCT was sufficient for AH outflow from the AC to decrease IOP significantly. Furthermore, OCT investigations of the surgery site at different follow-up visits confirmed that the IOP decrease occurred without the formation of a filtering bleb. This indirectly indicated that the proposed technique rerouted the AH flow from the AC to the SCS without leaking into the subconjunctival space. This case also emphasized that the development of CLVs occurs irrespective of laser trabeculotomy. The deroofed SC and its thinned inner wall allowed enough AH to flow from the AC to the SCS to initiate its outflow across the sclera to CLVs. AH flowed across the sclera through some pores or microchannels. Our clinical observations in this case demonstrated that some of the AH flowed from SCSs to CLVs. Another important observation we made in this case was that CLVs first appeared in the superior temporal quadrant and lasted for a period of 12 months. Towards the end of this observation period, another CLV plexus developed in the superior nasal quadrant. This meant that as soon as the existing lymphatic pathway became unfunctional for some reason, the CLVs developed in another area where a functional natural outflow pathway from SCSs to CLVs remained. For practical purposes, this case emphasized that it is paramount to preserve the lymphatics while performing glaucoma surgery.
Case 3. Patient A. was a 69-year-old female patient who underwent a combined procedure for an intumescent cataract and advanced-stage OAG in her left eye, which was followed up for a period of 1.5 years. Glaucoma was diagnosed eight years prior and, since then, the patient was on hypotensive medications. Prior to surgery, the IOP in her right eye on one class of hypotensive medication (analog of prostaglandins) was 25 mmHg and on three classes of hypotensive medication (analog of prostaglandins, beta blockers, and carbonic anhydrase inhibitors) was 30 mmHg in her left eye. The preoperative best-corrected logMar VA values were 0 and 2 in her right and left eye, respectively. On 13 February 2021, the patient underwent surgery in her left eye under retrobulbar anesthesia (2% solution of lidocaine hydrochloride). Prior to surgery, no washout of hypotensive medications was performed. First, phacoemulsification with an implantation of a foldable acrylic IOL in the capsular bag was performed, followed by glaucoma surgery, as previously described. Surgery was uneventful, and no intraoperative complications were observed. Postoperatively, the patient followed a standard protocol and continued the instillation of two classes of hypotensive medications. On day 12, conjunctival sutures were removed (Fig.21A).
IOP changes. On day 12, the patient’s IOP on medication was 18 mmHg. On the same day, sutures were removed and Nd:YAG laser trabeculotomy was performed. Immediately after the trabeculotomy, the patient’s IOP decreased to 16 mmHg and the patient was advised to stop the instillation of hypotensive medications. On the following two follow-up visits, the patient had elevated IOP levels up to 26 mmHg. Repeat-laser trabeculotomy was attempted two more times with an interval of 7 days. After the third trabeculotomy attempt, the patient’s IOP decreased to 7 mmHg off medication. The IOP remained below the target level until 3 months, when an increase in the IOP to 31 mmHg was noticed. A 4th YAG trabeculotomy was attempted to decrease the IOP; however, this failed. The patient was advised to restart the instillation of hypotensive medications. At 6, 9, 12, and 15 months, the patient’s IOP levels were 34, 24, 24, and 27 mmHg, respectively, on three classes of hypotensive medications. A repeat glaucoma surgery was advised. On 29 May 2022, a diode laser cyclophotodestruction procedure was performed.
CLVs development. Immediately after the first Nd:YAG laser trabeculotomy, some conjunctival swelling appeared at the surgery site (Figure 21B). After 1 week, the slit lamp images showed overfilled CLVs with uneven calibers in the form of a plexus, which became visible at the surgery site (Figure 21C). Their course from the surgery site could be detected towards the superior temporal quadrant (Figure 21D). CLVs remained visible biomicroscopically up to months 2 after the trabeculotomy. With time, their number and size decreased considerably (Figure 21E, F). At 7 months, the CLVs completely disappeared (Fig.21G). At each follow-up visit, the patient’s surgery site and nearby quadrants were evaluated by OCT (Figure 22A-D). CLVs with VLSs were present in the conjunctiva over the surgery site and in both superior quadrants at all follow-up visits.
This study demonstrated the activation of AH flow from SCSs to CLVs after Nd:YAG laser trabeculotomy was performed. Similar to the previous cases, outflow activation occurred without the formation of a filtering bleb (the absence of bleb was confirmed by OCT). The appearance of engorged CLVs with uneven calibers over the surgery site and in the superior temporal quadrant within a period of 7 days after laser trabeculotomy indicated that, with the proposed technique, the functional status of conjunctival lymphatics played a considerable role in IOP regulation. Overfilled engorged CLVs pointed out the possible resistance in the fluid pathway or the non-satisfactory functional status of the conjunctival lymphatic system. This case emphasizes the necessity for early surgical intervention in glaucoma patients when conjunctival lymphatics are still active and functional.
4. Discussion
AH is produced by ciliary processes. From there, it flows into the AC. From the AC, aqueous outflows mainly occur via two pathways. Eighty percent of AH outflows through the trabecular (traditional) pathway. Through this pathway, AH flows into the SC via TM, and from there it flows into the systemic circulation through collecting channels. The resistance at the TM and SC regulates the degree of AH outflow to maintain IOP levels. In glaucomatous eyes, outflow resistance is often significantly increased, leading to ocular hypertension and optic nerve damage [24,25].
In the non-trabecular (non-traditional) outflow pathway, AH flows through the posterior aspect of the uveal meshwork, passing through the ciliary muscle, and entering the SCS. Fluid movement from the AC to the SCS results from fluid flow rather than diffusion [26]. The non-trabecular outflow is controlled by the resistance imparted by the muscle bundles and connective tissues of the ciliary body. The percentage AH outflow via this pathway in young, healthy individuals comprises approximately 50% of the total outflow. A decrease in the outflow rate can be observed in glaucomatous eyes. AH drains from SCSs via three possible routes [27,28,29,30]. In the first route, AH flows across the sclera to be collected and drained by orbital vessels and extraocular lymph vessels. This route has been termed the uveoscleral route [27]. The flow through the uveoscleral route depends upon scleral permeability, which in turn depends upon the IOP level. At higher IOP levels, scleral permeability is reduced. The second route is the uveovortex route. Through this route, AH is resorbed into the choroidal vessels and then into vortex veins [28]. The uveovortical route depends upon the colloidal osmotic gradient of the choroidal vasculature [1]. The third route—the uveolymphatic route—was discovered by Yucel et al. [29,30]. The authors identified lymphatics in the ciliary body. They opined that fluid and solutes flow at least partially through this pathway. The existence of lymphatic channels in the uveal tract has been supported by other studies [31,32,33,34].
After traditional glaucoma surgeries have been performed, AH accumulates in a subconjunctival space, which is termed the “filtration bleb”. The long-term survival rate of bleb is paramount to achieve a long-term hypotensive effect. Various modifications in surgical techniques, the use of different devices, and the peri- and postoperative use of antimetabolites have been proposed in the literature to achieve the long-term survival of filtration blebs [35,36,37]. The use of antimetabolites is not free from complications. Their use causes a long-term reduction in conjunctival and lymphatic vessels in the bleb and surrounding tissue, which may hamper the immunologic response against microbial flora on the conjunctival surface and may also play a key role in immunopathologic mechanisms resulting in blebitis [38].
From blebs, AH filters through conjunctival vessels and lymphatics [6,7,39,40,41,42,43]. Benedikt O. [44,45] investigated AH drainage from a bleb using fluorescence photography after an intracameral injection of fluorescein. From his observations, he claimed that if the tension was too low at the surgery site, in most cases, a filtering bleb would form. If the IOP was at a physiological level (i.e., higher than the episcleral vein pressure), new vessels could develop and drain the AH by bulk flow from the scleral fistula, which meant that there would be a good pressure-regulating effect without a filtering bleb.
Mini-invasive glaucoma surgeries (MIGSs) have been developed in the field to overcome the drawbacks of filtering glaucoma surgeries. These surgeries restore or enhance AH outflow through natural outflow pathways. At present, most of the surgical techniques developed in this direction aim at activating or enhancing AH outflow through the trabecular outflow pathway. Various procedures have been proposed in the literature to bypass the resistance at the inner wall of Schlemm’s canal [46,47,48,49]. These techniques have limited success, as they mostly address the resistance at the distal end of the trabecular outflow pathway, leaving resistance proximal to the posterior wall of the Schlemm’s canal unattended [50,51,52].
Owing to the large surface area of a choroid with its high resorptive capacity and large area of sclera overlying the choroid with its pores and preformed microchannels, which are capable of draining fluid directly into scleral veins, the non-trabecular pathway has tremendous potential to decrease IOP levels [53,54]. This pathway has a system of interconnected spaces, namely, intertrabecular fissures of the uveal layers of the trabecular reticulum, spaces between the bundles of ciliary muscle myocytes, SCSs with a valve-like suprachoroidal system, and paravasal spaces of transscleral vessels, which ensure the continuous movement of fluid from the AC along the vascular tract to the posterior parts of the eyeball [55]. Previously, surgeons accessed this route by performing surgical cyclodialysis. In cyclodialysis, the attachment of the ciliary body to the scleral spur is disrupted, providing AH resistance-free access to the SCS. This procedure decreases IOP significantly; however, its results are unpredictable. Its success rate solely depends upon the patency of the cyclodialysis tunnel. The detachment of the ciliary body from the scleral spur is traumatic, and cyclodialysis clefts have the tendency to close on their own due to the associated inflammation. Various modifications of the cyclodialysis procedure with implantations of different kinds of drainage devices and implants have been proposed in the research and are being used with variable successes [14,16,56,57,58,59,60,61,62,63,64]. CyPASS, a device inserted in the cyclodialysis tunnel ab interno [65], showed promising results regarding IOP decrease; however, the long-term observations demonstrated a progressive loss of endothelial cells. As a result, this device was withdrawn from the market by the manufacturer [15]. Its implantation in a heterogenous clinical population resulted in a high incidence of sudden IOP peaks with a low success rate [66]. Several other devices have been proposed but are still under study [67,68].
Different techniques have been popularized to reroute AH flow from the AC to the SCS without performing surgical cyclodialysis and bypassing ciliary muscle resistance [11,69]. Jordon et al. [11] proposed the insertion of a silicone tube as an intrascleral connection from the AC to the SCS and reported satisfactory surgical outcomes in 31 eyes of 31 patients with uncontrollable refractory glaucoma. At year one, 60% of the eyes were classified as achieving success, and at year 1.5, 40% of the eyes had controlled IOP levels. As per the authors, the intrascleral course of the tube minimized the risk of conjunctival erosion and associated infections, and there was no need to perform cyclodialysis. Identical to the technique described by Jordon et al., [11] Unal M. et al. [69] proposed a technique in which a suprachoroidal silicone tube shunt was implanted after making a 1.5 mm deep sclerotomy adjacent to the scleral flap opening; the posterior end of the silicone tube was placed posteriorly in the SCS, and the anterior end was placed into the AC. The authors evaluated the efficacy and safety in 24 eyes and reported satisfactory qualified success rates of 95.8% in the first week and 87.5% in the first, third, sixth, and twelfth months. Complications were minimal and included early hypotony in six eyes, a fibrin reaction in the anterior chamber in three patients, and intracameral bleeding in two patients. No infection, choroidal, or retinal detachment was observed. Failure was observed in seven eyes, of which three underwent reoperations for glaucoma.
The non-conventional outflow pathway has been exploited by surgeons to enhance the hypotensive effect of other glaucoma surgical procedures. Dada et al. [70] combined trabeculectomy with a limited deep sclerectomy and cyclodialysis in two pseudophakic patients who developed secondary glaucomas after vitreo-retinal surgery with silicone oil insertions. In this technique, the authors used excised scleral tissue obtained after performing a deep sclerectomy as a spacer to maintain the patency of the cyclodialysis cleft.
The intrascleral implantation of biocompatible CI was recommended to enhance the success rate of the deep sclerectomy and to reduce the effect of fibrosis at the surgery site [71,72,73]. These implants acted as spacers in the scleral bed and also acted similar to a sponge, transporting the liquid by capillary action. Shaarawy T. et al. [71] conducted a comparative study between deep sclerectomies with and without CI and reported satisfactory long-term results. As per their conclusions, deep sclerectomy augmented with the suprachoroidal implantation of a CI was more effective in the long-term lowering of IOP than with intrascleral CI [74]. Pershin K.B. et al. [75] also compared the results of non-penetrating deep sclerectomy and the implantation of CI in the surgical treatment of glaucoma and observed that, except for the lower rate of goniopuncture among patients with suprachoroidal implantations, i.e., a collagen glaucoma implant ("Xenoplast", Dubna-Biofarm, Russia), the results were comparable with those from patients in whom implants were placed intrasclerally.
Szurman P. et al. [76] modified the canaloplasty technique to facilitate the surgical procedure and potentially maximize the IOP-lowering effect by altering both the trabecular and non-trabecular aqueous outflow rates. The authors reduced full-thickness deep scleral layers to the choroid, opening the SCS. A retrospective analysis of the surgical outcomes of 78 operated eyes showed a significant decrease in mean IOP values from 19.1 mmHg on 3 topical medications to 13.5 mmHg on 1 topical medication at twelve months. More than fifty percent of patients were free from the instillation of hypotensive medication.
In the present study, the mid- and long-term results of a technique to enhance AH outflow from the AC to the SCS without performing cyclodialysis are presented. By the technique described above, AH, after leaving the AC, accumulated in the ISR and, maintaining a physiological pressure, entered the SCS, from where it outflowed through uveoscleral, uveovortex, and uveolymphatic routes. Clinical observations and the results of OCT investigations achieved in this study, namely, a decrease in IOP without forming a filtering bleb, the activation of fluid flow from SCSs to CLVs, and CLV development, indicate that some of the AH flow from SCS occurred via intrascleral microchannels to CLVs. This route may be termed as the SCS–intrascleral microchannels–CLVs route.
In the literature, we did not observe CLV developments following the enhancement of AH flow to SCSs. To the best of our knowledge, this is the second report to mention the development of CLVs. Previously, we reported the results of a pilot study consisting of 38 patients in whom glaucoma surgery was performed using the technique mentioned above [18]. In that study, at six and twelve months, a significant decrease in IOP levels without forming a filtering bleb and a reduction in the use of additional hypotensive medications were achieved. СLVs developed in more than thirty-nine percent of cases (15 eyes out of 38). In the present study, these cases were followed up further, and new cases, if they fulfilled the inclusion criteria, were added. The development of CLVs in this case study was observed in 50% of cases (29/58). CLVs had characteristic lymphatic vessel appearances—they had uneven calibers, a sausage-shaped pattern, appeared in the form of plexus or solitary vessels running parallel to the limbus, perpendicular to it, or in a free manner, and had VLSs in their lumens in OCT scans. CLV identification by OCT in more than 82% of cases demonstrated that AH flowed from SCS across the sclera to CLVs. Based on the clinical observations, a relationship between the duration of biomicroscopic CLV appearance and a decrease in IOP levels was established. It was concluded that longer CLVs identified biomicroscopically produced a poor prognosis for IOP control. Pronounced CLVs for a longer period of time indicated the possible resistance to fluid flow in the path ahead. The biomicroscopic appearance of CLVs may be an indication for initiating some kind of medical treatment to enhance conjunctival lymphatic outflow to control IOP levels and preserve visual functions.
Ocular lymphoangiogenesis may explain some observations made in this study for sites of CLVs development, depending on the eye operated on. As presented in Table 7, CLVs developed predominantly in the nasal quadrants in the right eyes and in temporal quadrants in the left eyes. Ocular lymphoangiogenesis determined that limbal and conjunctival lymphatic networks are progressively formed from a primary lymphatic vessel that grows from the nasal-side medial canthus region at birth. This primary lymphatic vessel immediately branches out, invades the limbus and conjunctiva, and bidirectionally encircles the cornea. As a result, the distribution of ocular lymphatics is significantly polarized toward the nasal side, and limbal lymphatics are directly connected to conjunctival lymphatics. New lymphatic sprouts are produced mainly from nasal side limbal lymphatics, presenting the nasal side of the eye as more responsive to fluid drainage and inflammatory stimuli [77]. Further research is needed to explore the practical implications of the observations made in the present study.
The clinical observations and results of this study permit us to conclude that CLVs play an important role in IOP decrease following surgery. CLVs health, the patency of the conjunctival lymphatic system, is paramount to attain the success of any glaucoma surgery. Any resistance in lymphatic flow results in the failure of the procedure. Hence, it is wise to save the lymphatics, not only at the time of surgery, but also before surgery. The instillation of hypotensive medications with preservatives has an adverse effect on the ocular surface and the status of conjunctival lymphatics [39,78,79]. The earlier the surgery is attempted, the higher the chances of lymphatics being functional and the higher the chances of long-term surgical success rates.
The analysis showed that the main reason for failure in this study was the blockage of the trabeculotomy opening by iris tissue leading to the elevation of IOP levels. The blockage of the trabeculotomy opening by iris tissue is a well-known complication of Nd:YAG laser goniopuncture [80]. To overcome this complication, we further modified the technique by performing a high-frequency peripheral iridotomy at the time of surgery.
The mechanism of IOP decrease by the proposed technique may be explained as follows. AH bypasses resistance at the TM and the ciliary muscle and travels as bulk flow from the AC to the ISR through the trabeculotomy opening or percolates through the thinned inner wall of the SC. The healed-up conjunctiva prevents any flow to the subconjunctival space. In the ISR, AH accumulates temporarily and after creating pressure at the physiological level (i.e., above the episcleral vein pressure), it encounters the interstitial spaces of the uvea. The pressure in the ISR acts as a trigger for the development of newly incorporated veins and lymphatic vessels without forming a filtering bleb. Surplus AH overfills the interstitial spaces and lymphatics. From the ISR, the AH enters SCSs to be absorbed by the vortex vessels or flows across the sclera via scleral pores or through intrascleral channels to be collected by orbital vessels or to drain into CLVs. When a balance is achieved between AH inflow from the AC to the ISR and SCS and AH outflow from SCS, the CLVs decrease in size and number, leaving a few to maintain the fluid flow.
The proposed technique presented certain advantages. All of the surgical steps were performed without perforating the eyeball; hence, all of the complications related to the sudden decrease in IOP were either minimized or completely avoided. The decrease in IOP occurred without the formation of a bleb; therefore, complications related to blebs were negligible and completely avoided. The use of antimetabolites became irrelevant, and all adverse effects related to their use were avoided. The conjunctiva was intentionally permitted enough time to heal, preventing any flow to the subconjunctival space. The enhancement of AH outflow from SCS to CLVs occurred via the natural outflow pathway.
Some of the drawbacks of this technique are its ab-externo approach, the need for extensive tissue dissection resulting in increased surgical trauma, the prolongation of surgery time, two-stage surgery, and the need for the close monitoring of patients in the early post-operative period. There was a possibility of trabeculotomy blockage by iris tissue, resulting in an elevation of IOP levels. A pre- peri-, or postoperative peripheral iridotomy, adjacent to the area of the proposed intervention, helped to avoid this complication.
Randomized, controlled, and comparative studies with longer follow-up visits and larger groups are required to further confirm the efficacy and safety of this technique.
5. Conclusions
The results of this interventional case series enabled us to conclude that the proposed technique is easy to learn, safe to perform, and effective in decreasing IOP levels and reducing hypotensive medication use in glaucoma patients. IOP was decreased by enhanced AH outflow from SCS to the circulatory system and extraocular lymphatics. Some of the AH outflowed from SCS to CLVs through scleral pores or intrascleral channels. The health of conjunctival lymphatics was paramount to achieve success in the surgical management of glaucoma. For predictable hypotensive outcomes, every precaution should be taken in glaucoma surgery to preserve lymphatics.
6. Patents
Patent of the Russian Federation for invention № 2766730 dated March 15, 2022.
Patent of the Russian Federation for invention № 2782126 dated October 21, 2022.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org. Video S1_Case 2_ 1 month after surgery, CLVs in superior temporal quadrant. Video S2_Case 2_12 months after surgery, CLVs in superior nasal quadrant.
Author Contributions
Conceptualization, V.K., A.I.B., A.S.S.S.; data curation, V.K., K.A.A.Z., A.I.B., A.S.S.S., and Z.S.R.; investigation, V.K., K.A.A.Z., A.I.B., Z.S.R., and A.S.S.S.; methodology, V.K., A.I.B., and A.S.S.S.; project administration, V.K., M.A.F, and G.N.D.; supervision, V.K., G.N.D., and M.A.F.; validation, A.I.B. and G.N.D.; writing—original draft, V.K.; writing—review and editing, V.K.; funding acquisition, not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the Medical Institute of RUDN University (protocol code 16 dated 17 November 2016).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to case histories of patients.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Johnson, M.; McLaren, J.W.; Overby, D.R. Unconventional aqueous humor outflow: A review. Exp. Eye Res. 2017, 158, 94–111. [CrossRef]
- Gedde, S.J.; Singh, K.; Schiffman, J.C.; Feuer, W.J.; Tube Versus Trabeculectomy Study Group. The Tube Versus Trabeculectomy Study: Interpretation of results and application to clinical practice. Curr. Opin. Ophthalmol. 2012, 23, 118–126. [CrossRef]
- Khaw, P.T.; Chiang, M.; Shah, P.; Sii, F.; Lockwood, A.; Khalili, A. Enhanced Trabeculectomy: The Moorfields Safer Surgery System. Dev. Ophthalmol. 2017, 59, 15–35. [CrossRef]
- Rulli, E.; Biagioli, E.; Riva, I.; Gambirasio, G.; De Simone, I.; Floriani, I.; Quaranta, L. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: A systematic review and meta-analysis. JAMA Ophthalmol. 2013, 131, 1573–1582. [CrossRef]
- Volkova, N.V.; Shchuko, A.G.; Iureva, T.N.; Yakimov, A.P.; Akulenko, M.V. [Nd: YAG laser goniopuncture as a mandatory adjuvant procedure after non-penetrating deep sclerectomy (long-term observation results)]. Vestn. Oftalmol. 2019, 135, 93–101. (In Russian). [CrossRef]
- Akiyama, G.; Saraswathy, S.; Bogarin, T.; Pan, X.; Barron, E.; Wong, T.T.; Kaneko, M.K.; Kato, Y.; Hong, Y.; Huang, A.S. Functional, structural, and molecular identification of lymphatic outflow from subconjunctival blebs. Exp Eye Res. 2020 Jul;196:108049. [CrossRef]
- Lee J.Y., Heilweil G., Le P., Saraswathy S., Hong Y.K., Girkin C.A., Huang A.S. Structural Confirmation of Lymphatic Outflow from Subconjunctival Blebs of Live Human Subjects. Ophthalmol Sci. 2021 Dec;1(4):100080. [CrossRef]
- Kazakova, D.; Roters, S.; Schnyder, C.C.; Achache, F.; Jonescu-Cuypers, C.; Mermoud, A.; Krieglstein, G. Ultrasound biomicroscopy images: long-term results after deep sclerectomy with collagen implant. Graefes Arch Clin Exp Ophthalmol. 2002; 240(11):918-23. [CrossRef]
- Aptel, F.; Dumas, S.; Denis, P. Ultrasound biomicroscopy and optical coherence tomography imaging of filtering blebs after deep sclerectomy with new collagen implant. Eur J Ophthalmol. 2009; 19:223–230. [CrossRef]
- Borgohain, M.; Sarma, P.; Tayab, S.; Sangma, C.A.; Paul, S. Smaller-incision Revision of Trabeculectomy With Mitomycin: Long-term Outcomes and Complications. J. Glaucoma 2019; 28: e107. [CrossRef]
- 11. Jordan, J,F,; Engels, B.F.; Dinslage, S.; Dietlein, T.S.; Ayertey, H.D.; Roters, S.; Esser, P.; Konen, W.; Krieglstein, G.K. A novel approach to suprachoroidal drainage for the surgical treatment of intractable glaucoma. J Glaucoma. 2006 Jun;15(3):200-5. [CrossRef]
- Vinod, K. Suprachoroidal shunts. Curr Opin Ophthalmol. 2018 Mar;29(2):155-161. [CrossRef]
- Szurman, P.; Januschowski, K.; Boden, K.T.; Seuthe, A.M. Suprachoroidal drainage with collagen sheet implant- a novel technique for non-penetrating glaucoma surgery. Graefes Arch Clin Exp Ophthalmol. 2018 Feb;256(2):381-385. [CrossRef]
- König, S.; Hirneiß, C.W. [STARflo-a suprachoroidal drainage implant in glaucoma surgery]. Ophthalmologe. 2018 Aug;115(8):670-675. [CrossRef]
- Garcia-Feijoo J. CyPass stent withdrawal: The end of suprachoroidal MIGS? Arch Soc Esp Oftalmol (Engl Ed). 2019 Jan;94(1):1-3. [CrossRef]
- Frolov, M.A.; Ryabey, A.V.; Frolov, A.M. [Results of surgical treatment of glaucoma using sinustrabeculectomy modified for drainage of anterior chamber and suprachoroidal space by autosclera]. Vestn Oftalmol. 2020;136(3):46-50. (in Russian). [CrossRef]
- Kumar, V. [RU]; Frolov, M.A.; [RU]; Dushina, G.N.;[RU]; Shradka, A.S.S. [JO]; Abu Zaalan, K.A. [RU]; Bezzabotnov, A.I. [RU] (2022). A combined method for activating various mechanisms of intraocular fluid outflow in glaucoma. (Patent of the Russian Federation for invention No. 2766730). Russian Federation. Rospatent.; Federal Service for Intellectual Property. The date of registration in the State Register of Inventions of the Russian Federation is March 15, 2022. https://ru.espacenet.com/publicationDetails/biblio?FT=D&date=20220315&DB=&locale=en_RU&CC=RU&NR=2766730C1&KC=C1&ND=5 (accessed on 13.06.2023).
- Kumar, V.; Abu Zaalan, K.A.; Bezzabotnov, A.I.; Dushina, G.N.; Shradqa, A.S.S.; Rustamova, Z.S.; Frolov, M.A. Bleb-independent glaucoma surgery to activate the uveolymphatic route of non-trabecular aqueous humor outflow: short-term clinical and OCT results. Vision. 2022;6 (1),4. [CrossRef]
- Realini, T.; McMillan, B.; Gross, R.L.; Devience, E.; Balasubramani, G.K. Assessing the Reliability of Intraocular Pressure Measurements Using Rebound Tonometry. J. Glaucoma 2021, 30, 629–633. [CrossRef]
- Kato, Y.; Nakakura, S.; Matsuo, N.; Yoshitomi, K.; Handa, M.; Tabuchi, H.; Yoshiaki, K. Agreement among Goldmann applanation tonometer, iCare, and Icare PRO rebound tonometers, non-contact tonometer, and Tonopen XL in healthy elderly subjects. Int. Ophthalmol. 2018, 38, 687–696. [CrossRef]
- Kawana, K.; Kiuchi, T.; Yasuno, Y.; Oshika, T. Evaluation of trabeculectomy blebs using 3-dimensional cornea and anterior segment optical coherence tomography. Ophthalmology. 2009, 116, 848–855. [CrossRef]
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; et al. Laser in Glaucoma and Ocular Hypertension (LiGHT) trial. A multicentre, randomised controlled trial: design and methodology. Br J Ophthalmol. 2018;102(5):593e598.
- Gazzard, G.; Konstantakopoulou, E.; Garway-Heath, D.; et al. Selective laser trabeculoplasty versus drops for newly diagnosed ocular hypertension and glaucoma: the LiGHT RCT. Health Technol Assess. 2019;23(31):1e102.
- Carreon, T.; Merwe, E.; Fellman, R.L.; Johnstone, M.; Bhattacharya, S.K. Aqueous outflow—A continuum from trabecular meshwork to episcleral veins. Prog. Retin. Eye Res. 2017, 57, 108–133. [CrossRef]
- Sanchez, I.; Martin, R. Advances in diagnostic applications for monitoring intraocular pressure in glaucoma: a review. J Optom. 2019;12(4):211–221.
- Pederson, J.E.; Toris, C.B. Uveoscleral outflow: diffusion or flow? Invest Ophthalmol Vis Sci. 1987 Jun;28(6):1022-4.
- Bill, A. The aqueous humor drainage mechanism in the cynomolgus monkey (Macaca irus) with evidence for unconventional routes. Investigative Ophthalmology. 1965; 4:911–919.
- Pederson, J.E.; Gaasterland, D.E.; et al. Uveoscleral aqueous outflow in the rhesus monkey: importance of uveal reabsorption. Investigative Ophthalmology and Visual Science. 1977; 16:1008–1017.
- Yücel, Y.H.; Johnston, M.G.; Ly, T.; Patel, M.; Drake, B.; Gümüş, E.; Fraenkl, S.A.; Moore, S.; Tobbia, D.; Armstrong, D.; Horvath, E.; Gupta N. Identification of lymphatics in the ciliary body of the human eye: A novel “uveolymphatic” outflow pathway. Exp. Eye Res. 2009, 89, 810–819. [CrossRef]
- Yucel, Y.; Gupta, N. Lymphatic drainage from the eye: A new target for therapy. Prog. Brain Res. 2015, 220, 185–198. [CrossRef]
- Kim, M.; Johnston, M.G.; Gupta, N.; Moore, S.; Yücel, Y.H. A model to measure lymphatic drainage from the eye. Exp Eye Res. 2011 Nov;93(5):586-91. [CrossRef]
- Khan, A.M.; Kagan, D.B.; Gupta, N.; Navajas, E.V.; Jin, Y.P.; Yücel, Y.H. Ciliary body lymphangiogenesis in uveal melanoma with and without extraocular extension. Ophthalmology 2013;120:306 –10. [CrossRef]
- Chernykh, V.V.; Bgatova, N.P. [Lymphatic structures of the eye and uveolymphatic (metabolic) pathway of intraocular fluid outflow. Part 1]. Natsional’nyi zhurnal glaukoma. 2018; 17(1):3-13. (in Russian).
- Dubin, A.; Freeman, K.S.; Charles, J .; Ammar, D.A.; Ehrhart, E.J. Pilot study supporting the existence of novel lymphatic channels within the canine anterior uveal tract using Lyve-1 and CD31. Vet Ophthalmol. 2021 Jul;24(4):354-360.. [CrossRef]
- Leung, D.Y.; Tham, C.C. Management of bleb complications after trabeculectomy. Semin Ophthalmol. 2013 May;28(3):144-56. [CrossRef]
- Broadway, D.C.; Bloom, P.A.; Bunce, C.; Thiagarajan, M.; Khaw, P.T. Needle revision of failing and failed trabeculectomy blebs with adjunctive 5-fluorouracil: survival analysis. Ophthalmology. 2004 Apr;111(4):665-73. Erratum in: Ophthalmology. 2005 Jan;112(1):66. [CrossRef]
- Coote, MA.; Gupta, V.; Vasudevan, S.; Crowston, J.G. Posterior revision for failed blebs: long-term outcomes. J Glaucoma. 2011 Aug;20(6):377-82. [CrossRef]
- Bouhenni, R.A.; Jadaan, I.A.; Rassavong, H.; Shahwan, S.A.; Katan, H.A.; Dunmire, J.; Krasniqi, M.; Edward, D.P. Lymphatic and blood vessel density in human conjunctiva after glaucoma filtration surgery. J. Glaucoma 2016, 25, e35–e38. [CrossRef]
- Singh, D.J. Conjunctival lymphatic system. Cataract Refract Surg. 2003 Apr;29(4):632-3. [CrossRef]
- Khoo, Y.J.; Abdullah, A.A.H.; Yu, D.Y.; Morgan, W.H. Use of trypan blue to assess lymphatic function following trabeculectomy. Clin Exp Ophthalmol. 2019 Sep;47(7):892-897. Epub 2019 May 27. PMID: 31074572. [CrossRef]
- Subileau, M.; Vittet, D. Lymphatics in Eye Fluid Homeostasis: Minor Contributors or Significant Actors? Biology (Basel). 2021 Jun 25;10(7):582. [CrossRef]
- Ng, H-K.; Yu, P.; Yu, D-Y.; Morgan, W. Prominent lymphatic vessel in a functioning bleb after repeat XEN gel stent implantation surgery in pseudoexfoliative glaucoma: a case report. Asian Journal of Ophthalmology, 2021; 18(1): 92-97. [CrossRef]
- Lee, J.Y.; Strohmaier, C.A.; Akiyama, G.; Saraswathy, S.; Yoo, C.; Kim, Y.Y.; Hong, Y.K.; Huang, A.S. Bleb-related Porcine Lymphatic Outflow is Greater from Subconjunctival compared to Subtenon Blebs. J Curr Glaucoma Pract. 2022 Sep-Dec;16(3):144-151. [CrossRef]
- Benedikt, O. [Demonstration of aqueous outflow patterns of normal and glaucomatous human eyes through the injection of fluorescein solution in the anterior chamber (author's transl)]. Albrecht Von Graefes Arch. Klin. Exp. Ophthalmol. 1976, 199, 45–67. (In German). [CrossRef]
- Benedikt, O. [The effect of filtering operations]. Klin. Monbl. Augenheilkd. 1977, 170, 10–19. (In German).
- Dubey, S.; Bansal, T.; Garg, P.; Hegde, A.; Das, R.; Rekha, P.D. Outcomes of ab-interno irrigating goniectomy with trabectome in primary and secondary glaucoma from a single center in India. Indian J Ophthalmol. 2022 Oct;70(10):3569-3574. [CrossRef]
- Grover, D.S.; Godfrey, D.G.; Smith, O.; Feuer, W.J.; Montes de Oca, I.; Fellman, R.L. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: technique report and preliminary results. Ophthalmology. 2014 Apr;121(4):855-61. [CrossRef]
- Barkander, A.; Economou, M.A.; Jóhannesson, G. Kahook Dual-Blade Goniotomy with and without Phacoemulsification in Medically Uncontrolled Glaucoma. Clin Ophthalmol. 2023 May 12;17:1385-1394. [CrossRef]
- Feltgen, N.; Mueller, H.; Ott, B.; Frenz, M.; Funk, J. Endoscopically controlled erbium:YAG goniopuncture versus trabeculectomy: effect on intraocular pressure in combination with cataract surgery. Graefes Arch Clin Exp Ophthalmol. 2003 Feb;241(2):94-100. [CrossRef]
- Lavia, C.; Dallorto, L.; Maule, M.; Ceccarelli, M.; Fea, AM. Minimally invasive glaucoma surgeries (MIGS) for open angle glaucoma: A systematic review and meta-analysis. PLoS One. 2017 Aug 29;12(8):e0183142. [CrossRef]
- Ahmed, I.I.K.; Fea, A.; Au, L.; Ang, R.E.; Harasymowycz, P.; Jampel, H.D.; Samuelson, T.W.; Chang, D.F.; Rhee, D.J. A Prospective Randomized Trial Comparing Hydrus and iStent Microinvasive Glaucoma Surgery Implants for Standalone Treatment of Open-Angle Glaucoma: The COMPARE Study. Ophthalmology 2020 Jan;127(1):52-61. Clinical Trial. [CrossRef]
- Otárola, F.; Pooley, F. Minimally invasive glaucoma surgery (MIGS) devices: risks.; benefits and suitability. Community Eye Health. 2021;34(112):59-60.
- Krohn, J.; Bertelsen, T. Light microscopy of uveoscleral drainage routes after gelatine injections into the suprachoroidal space. Acta Ophthalmol Scand. 1998;76(5):521-7. [CrossRef]
- Figus, M.; Posarelli, C.; Passani, A.; Albert, TG.; Oddone, F.; Sframeli, A.T.; Nardi, M. The supraciliary space as a suitable pathway for glaucoma surgery: Ho-hum or home run? Surv Ophthalmol. 2017 Nov-Dec;62(6):828-837. [CrossRef]
- Karlova, E.V. [Morphological studies of the ciliary part of the uveoscleral outflow pathway]. Bulletin of the Orenburg State University. 2011 14(133): 178-183 (in Russian).
- Jordan, J.F.; Dietlein, T.S.; Dinslage, S.; Lüke, C.; Konen, W.; Krieglstein, G.K. Cyclodialysis ab interno as a surgical approach to intractable glaucoma. Graefes Arch Clin Exp Ophthalmol. 2007 Aug;245(8):1071-6. [CrossRef]
- Dada, T.; Sharma, R.; Sinha, G.; Angmo, D.; Temkar, S. Cyclodialysis-enhanced trabeculectomy with triple Ologen implantation. Eur J Ophthalmol. 2016 Jan-Feb;26(1):95-7. [CrossRef]
- Gupta, S.; Gupta, V. Trabeculectomy Augmented With Cyclodialysis: A Surgical Option for Refractory Glaucomas. J Glaucoma. 2016 Jul;25(7):e726. [CrossRef]
- Emami-Naeini, P.; You, G. Medical and Surgical Applications for the Suprachoroidal Space. Int Ophthalmol Clin. 2019;59(1):195-207. [CrossRef]
- Kumar, V.; Frolov, M.A.; Dushina, G.N.; Shradqa, A.S.; Bezzabotnov, A.I.; Abu Zaalan, K.A. Reverse meridional cyclodialysis ab interno in management of open angle glaucoma — a preliminary report. Bulletin of RSMU. 2019; (6): 92–8. [CrossRef]
- Shradqa, A.S.; Kumar, V.; Frolov, M.A.; Dushina, G.N.; Bezzabotnov, A.I.; Abu Zaalan, K.A. [Cyclodialysis ab externo with implantation of a collagen implant in surgical management of glaucoma]. Bulletin of RSMU. 2019; 5: 92–8. (In Russian). [CrossRef]
- Kumar, V.; Shradqa, A.S.S.; Abu Zaalan, K.A [Variant of Micro-Invasive Glaucoma Surgery: Calibrated Reverse Meridional Cyclodialysis ab interno Involving Implantation of a Non-Absorbable Collagen Implant]. Ophthalmology in Russia. 2021;18(1):61-69. (In Russian). [CrossRef]
- Kumar, V.; Frolov, M.A.; Dushina, G.N.; Shradqa, A.S.; Bezzabotnov, A.I. [Reverse meridional cyclodialysis ab interno with implantation of a metallic implant in patients with glaucoma of different etiology]. Vestnik Oftalmologii. 2019;135(3):10-19. (In Russian).
- Kumar, V.; Shradqa, A.; Frolov, M.; Dushina, G.; Bezzabotnov, A. Valve cyclodialysis with implantation of a non-absorbable collagen implant in the cyclodialysis tunnel in surgical management of open-angle glaucoma: long-term results. Acta Ophthalmologica. 2022; 100 (S267). [CrossRef]
- Erb, C. [Suprachoroidal minimally invasive glaucoma surgery: Procedures and clinical outcome]. Ophthalmologe. 2018 May;115(5):370-380. (In German). [CrossRef]
- Kuusniemi, A.M.; Lindbohm, N.; Allinen, P.; Harju, M. Intraocular Pressure Peaks After Suprachoroidal Stent Implantation. J Glaucoma. 2020 Nov;29(11):1050-1055. [CrossRef]
- Grierson, I.; Minckler, D.; Rippy, M.K.; Marshall, A.J.; Collignon, N.; Bianco, J.; Detry, B.; Johnstone, M.A. A novel suprachoroidal microinvasive glaucoma implant: in vivo biocompatibility and biointegration. BMC Biomed Eng. 2020 Oct 14;2:10. [CrossRef]
- Denis, P.; Hirneiß, C.; Durr, G.M.; Reddy, K.P.; Kamarthy, A.; Calvo, E.; Hussain, Z.; Ahmed, I.K. Two-year outcomes of the MINIject drainage system for uncontrolled glaucoma from the STAR-I first-in-human trial. Br J Ophthalmol. 2022 Jan;106(1):65-70. [CrossRef]
- Unal, M.; Kocak Altintas, A.G.; Koklu, G.; Tuna, T. Early results of suprachoroidal drainage tube implantation for the surgical treatment of glaucoma. J Glaucoma. 2011 Jun-Jul;20(5):307-14. [CrossRef]
- Dada, T.; Shakrawal, J.; Ramesh, P.; Sethi, A. Trabeculectomy Augmented with Limited Deep Sclerectomy and Cyclodialysis with Use of Scleral Tissue as a Spacer. J Ophthalmic Vis Res. 2022 Nov 29;17(4):596-600. [CrossRef]
- Shaarawy, T.; Nguyen, C.; Schnyder, C.; Mermoud, A. Comparative study between deep sclerectomy with and without collagen implant: long term follow up. Br. J. Ophthalmol. 2004; 88: 95–98. [CrossRef]
- Demailly, P.; Jeanteur-Lunel, M.N.; Berkani, M.; Ecoffet, M.; Kopel, J.; Kretz, G.; Lavat, P. [Non-penetrating deep sclerectomy combined with a collagen implant in primary open-angle glaucoma. Medium-term retrospective results]. J. Fr. Ophtalmol. 1996; 19: 659–666. (In French).
- Anisimova, N.S.; Arbisser, L.B.; Anisimov, S.I.; Arutyunyan, L.L.; Shilova, N.F.; Bashaeva, G.; Kirtaev, R.V.; Anisimova, S.Y. Five-year results of non-penetrating deep sclerectomy with demineralized cancellous bone xenogenically derived collagen glaucoma implant. Int. Ophthalmol. 2021;41:2041–2052. [CrossRef]
- Mitwally, R.; Aref, A.; Shaarawy, T. Deep sclerectomy with intrascleral versus suprachoroidal collagen implant: A Randomized Control Trial. J Glaucoma 2021;30:124–128. [CrossRef]
- Pershin, K.B.; Pashinova, N.F.; Tsygankov, A.Yu.; Kosova, I.V.; Solovyova, G.M. [Non-penetrating deep sclerectomy and implantation of collagen drainage in the surgical treatment of glaucoma]. National Journal glaucoma. 2022;21(2):42-50. (In Russian). [CrossRef]
- Szurman, P.; Januschowski, K.; Boden, K.T.; Szurman, G.B. A modified scleral dissection technique with suprachoroidal drainage for canaloplasty. Graefes Arch Clin Exp Ophthalmol. 2016;254 (2):351–54. [CrossRef]
- Wu, Y.; Seong, Y.J.; Li, K.; Choi, D.; Park, E.; Daghlian, G.H.; Jung, E.; Bui, K.; Zhao, L.; Madhavan, S.; Daghlian, S.; Daghlian, P.; Chin, D.; Cho, I.T.; Wong, A.K.; Heur, M.; Zhang-Nunes, S.; Tan, J.C.; Ema, M.; Wong, T.T.; Huang, A.S.; Hong, Y.K. Organogenesis and distribution of the ocular lymphatic vessels in the anterior eye. JCI Insight. 2020 Jul 9;5(13):e135121. [CrossRef]
- Andole, S.; Senthil, S. Ocular Surface Disease and Anti-Glaucoma Medications: Various features, Diagnosis, and Management Guidelines. Semin Ophthalmol. 2023 Feb;38(2):158-166. [CrossRef]
- Fineide, F.; Lagali, N.; Adil, M.Y.; Arita, R.; Kolko, M.; Vehof, J.; Utheim, T.P. Topical glaucoma medications - Clinical implications for the ocular surface. Ocul Surf. 2022 Oct;26:19-49. [CrossRef]
- Marja-Liisa, Vuori. Complications of Neodymium: YAG laser goniopuncture after deep Sclerectomy. Acta Ophthalmol. Scand. 2003: 81: 573– 576. [CrossRef]
Figure 1.
OCT evaluation of the surgery and adjunct sites. (A) OCT scan of the surgery site, showing the ISR with collagen implant, covered by a superficial scleral flap (SSF) and conjunctiva (CO). No filtration bleb cavity can be observed over the implant and in the nearby area. A conjunctival lymphatic vessel (CLV) can be observed running horizontally over the surgery site. (B) OCT scan of conjunctiva adjacent to the surgery site showing a CLV with valve like structures (VLS) in its lumen. CO = conjunctiva; CLV = conjunctival lymphatic vessel; SSF = superficial scleral flap; VLS = valve-like structure.
Figure 1.
OCT evaluation of the surgery and adjunct sites. (A) OCT scan of the surgery site, showing the ISR with collagen implant, covered by a superficial scleral flap (SSF) and conjunctiva (CO). No filtration bleb cavity can be observed over the implant and in the nearby area. A conjunctival lymphatic vessel (CLV) can be observed running horizontally over the surgery site. (B) OCT scan of conjunctiva adjacent to the surgery site showing a CLV with valve like structures (VLS) in its lumen. CO = conjunctiva; CLV = conjunctival lymphatic vessel; SSF = superficial scleral flap; VLS = valve-like structure.
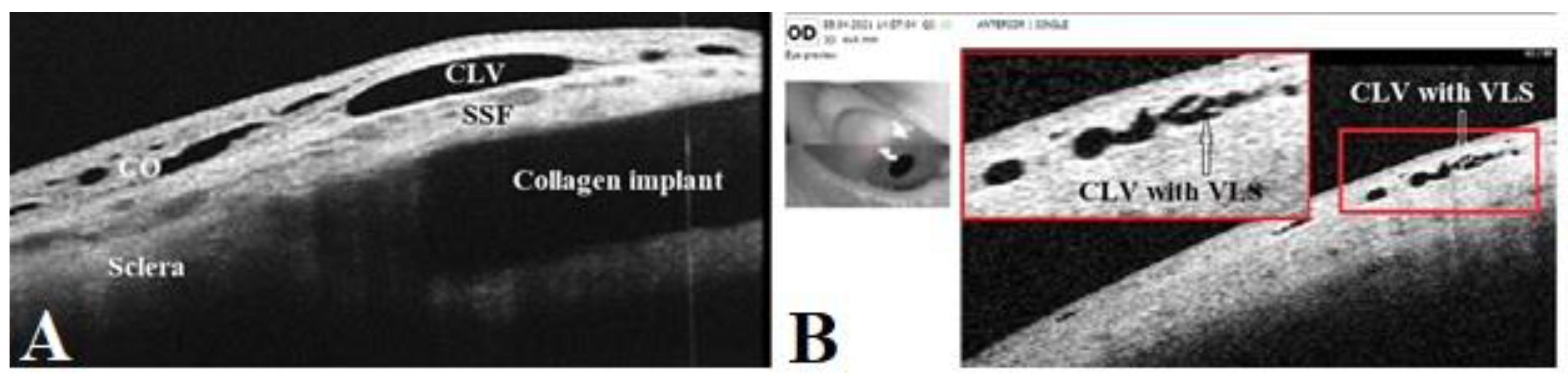
Figure 2.
Scatterplot showing the distribution of preoperative IOPs (n=58 patients). The solid red horizontal line represents an IOP of 18 mmHg.
Figure 2.
Scatterplot showing the distribution of preoperative IOPs (n=58 patients). The solid red horizontal line represents an IOP of 18 mmHg.
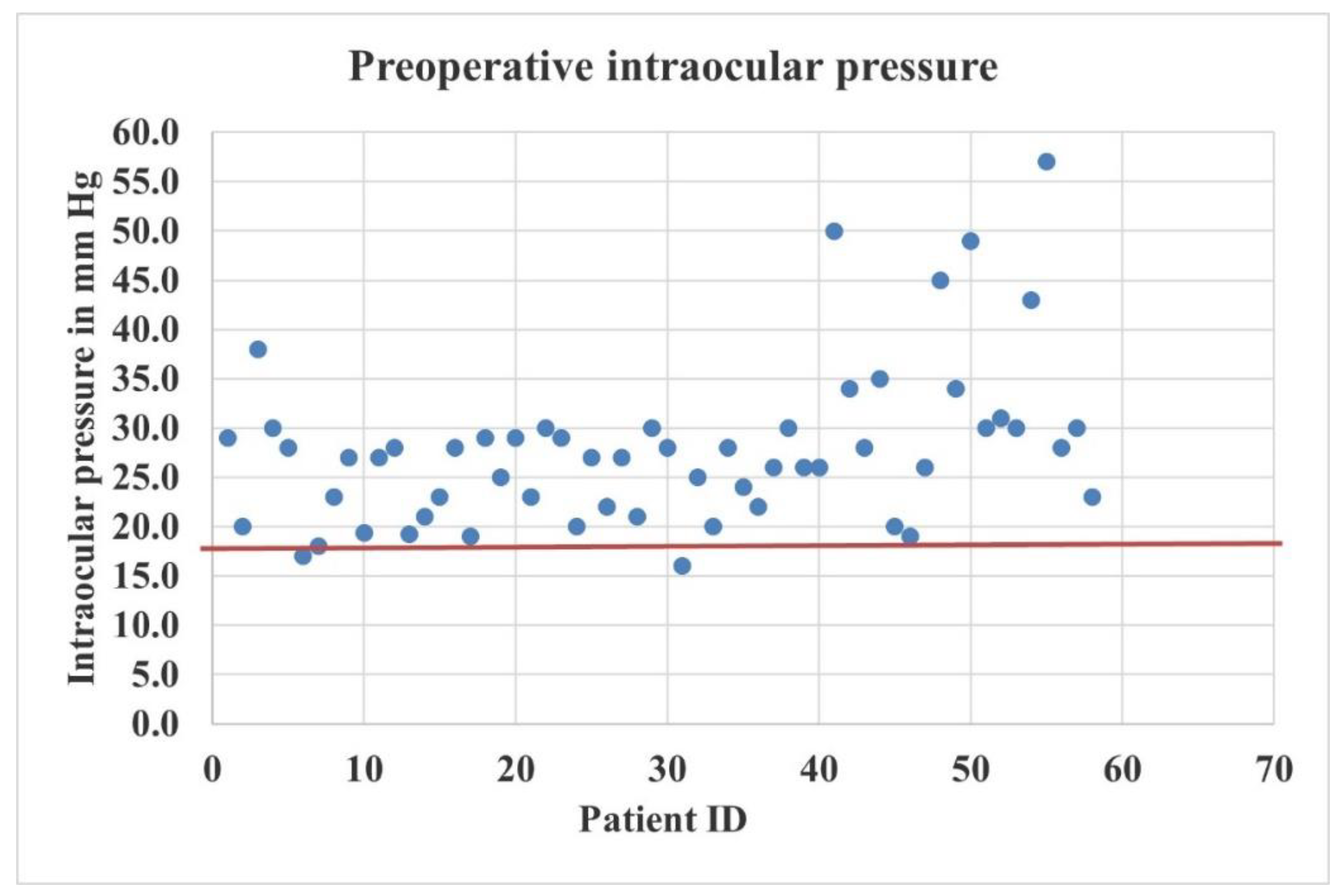
Figure 3.
Box-and-whisker plot showing IOP changes following surgery. The colored boxes represent the 25th and 75th percentiles; the solid horizontal lines in the colored boxes represent the median; X represents the mean; vertical solid black lines extend the interquartile range 1.5 times; and the dots represent outliers.
Figure 3.
Box-and-whisker plot showing IOP changes following surgery. The colored boxes represent the 25th and 75th percentiles; the solid horizontal lines in the colored boxes represent the median; X represents the mean; vertical solid black lines extend the interquartile range 1.5 times; and the dots represent outliers.
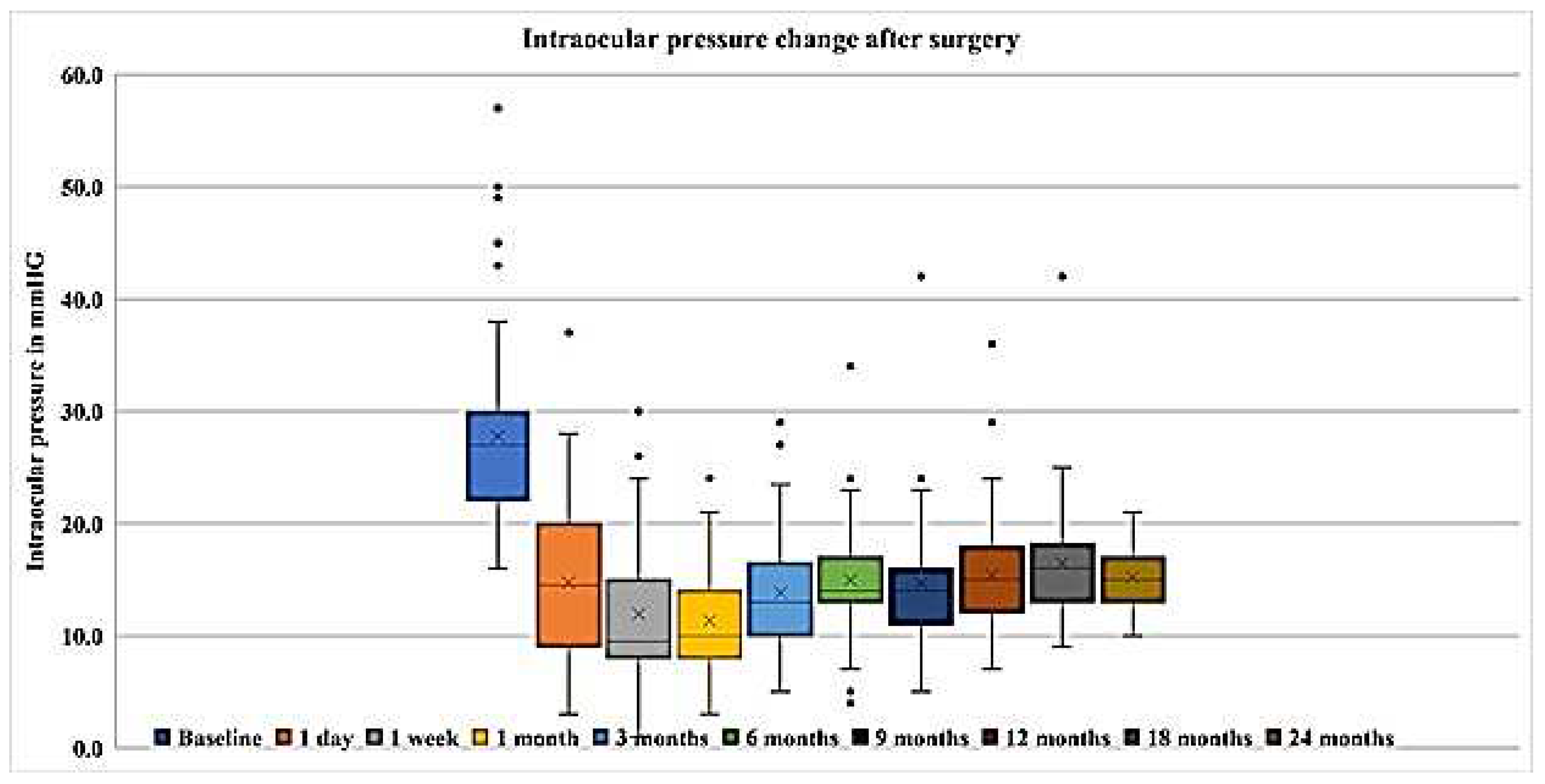
Figure 4.
Scatter plots of IOPs at different follow-up visits. The solid horizontal lines represent the target IOP =18 mmHg.
Figure 4.
Scatter plots of IOPs at different follow-up visits. The solid horizontal lines represent the target IOP =18 mmHg.
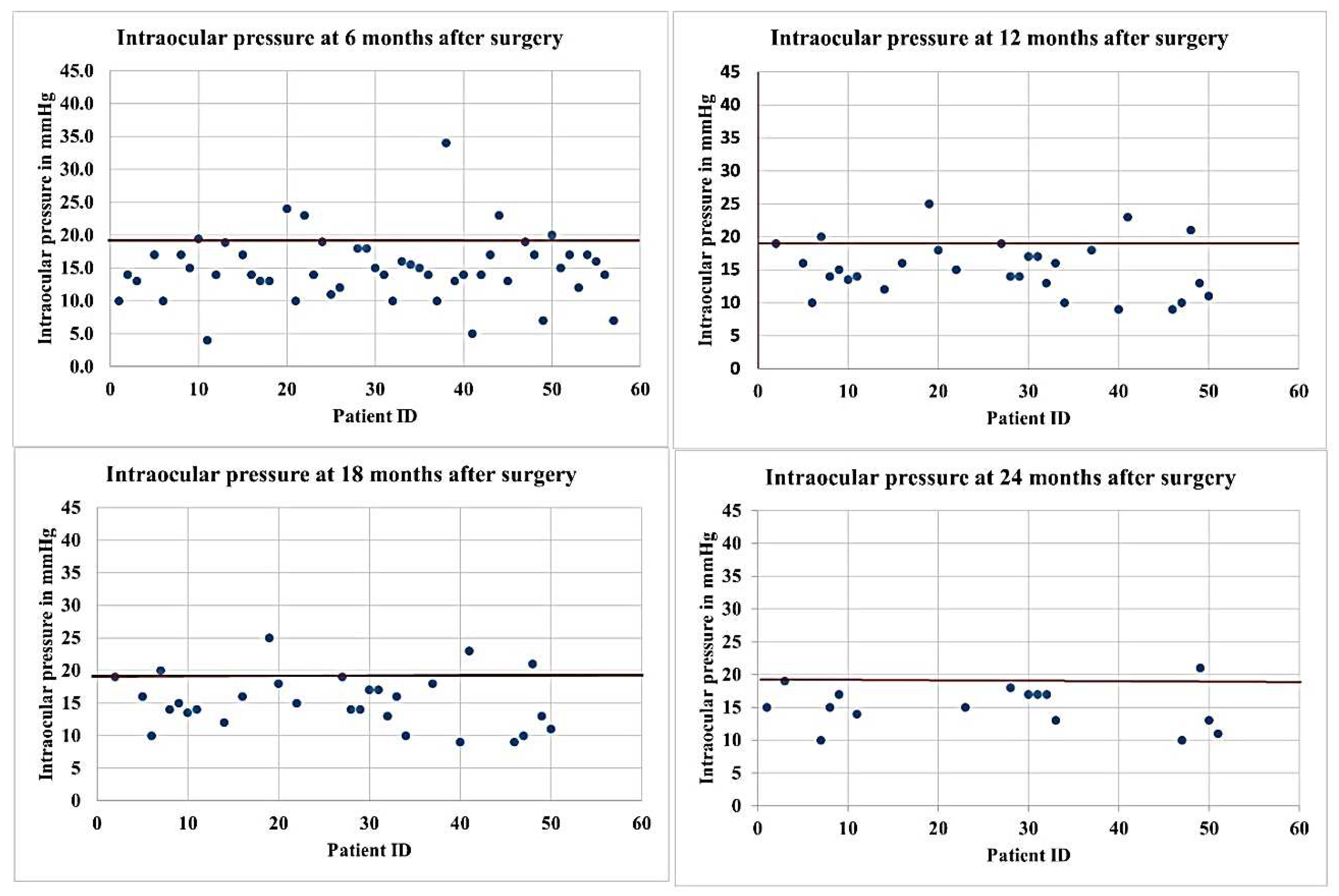
Figure 5.
Bar diagram showing the median values of hypotensive medications used after surgery at different follow-up times.
Figure 5.
Bar diagram showing the median values of hypotensive medications used after surgery at different follow-up times.
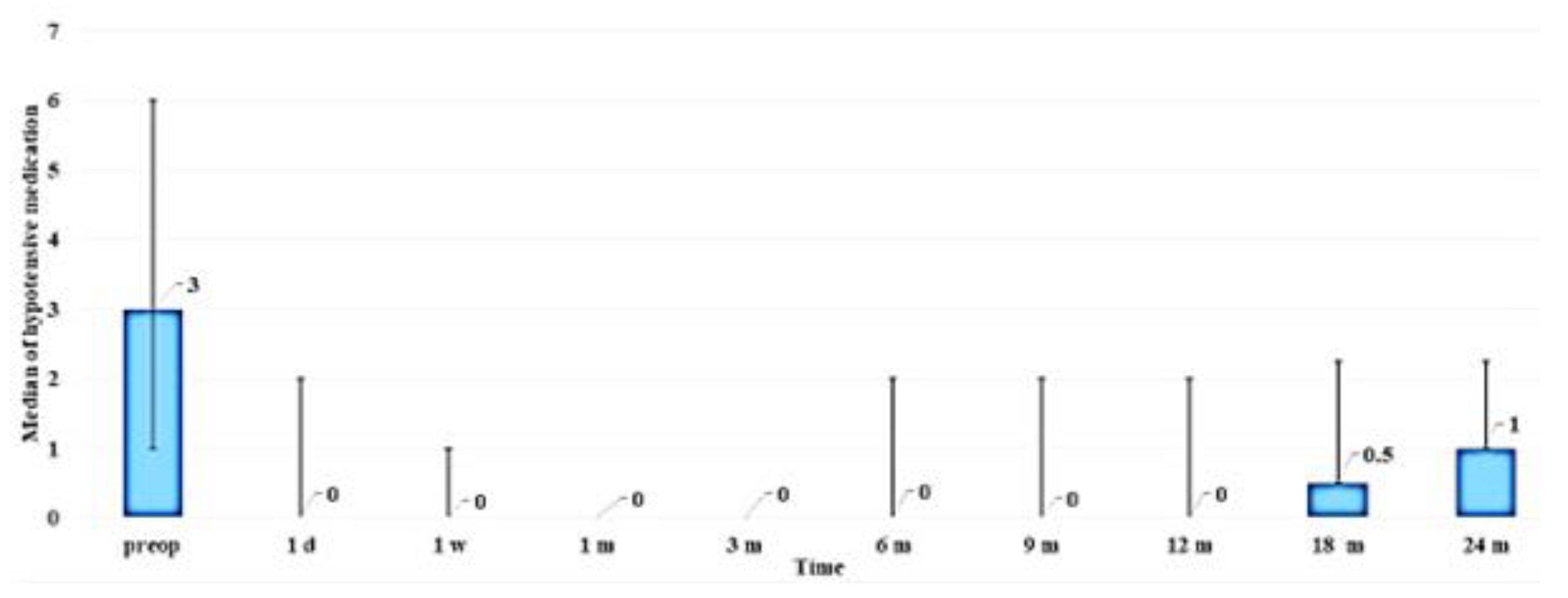
Figure 6.
Preoperative versus postoperative logMAR VA (median) values for patients having undergone combined procedures (blue solid horizontal line showing the median VA and blue solid vertical lines showing p25 and p75) and glaucoma surgery as a standalone procedure (red solid horizontal line showing median VA and red broken vertical lines showing p25 and p75).
Figure 6.
Preoperative versus postoperative logMAR VA (median) values for patients having undergone combined procedures (blue solid horizontal line showing the median VA and blue solid vertical lines showing p25 and p75) and glaucoma surgery as a standalone procedure (red solid horizontal line showing median VA and red broken vertical lines showing p25 and p75).
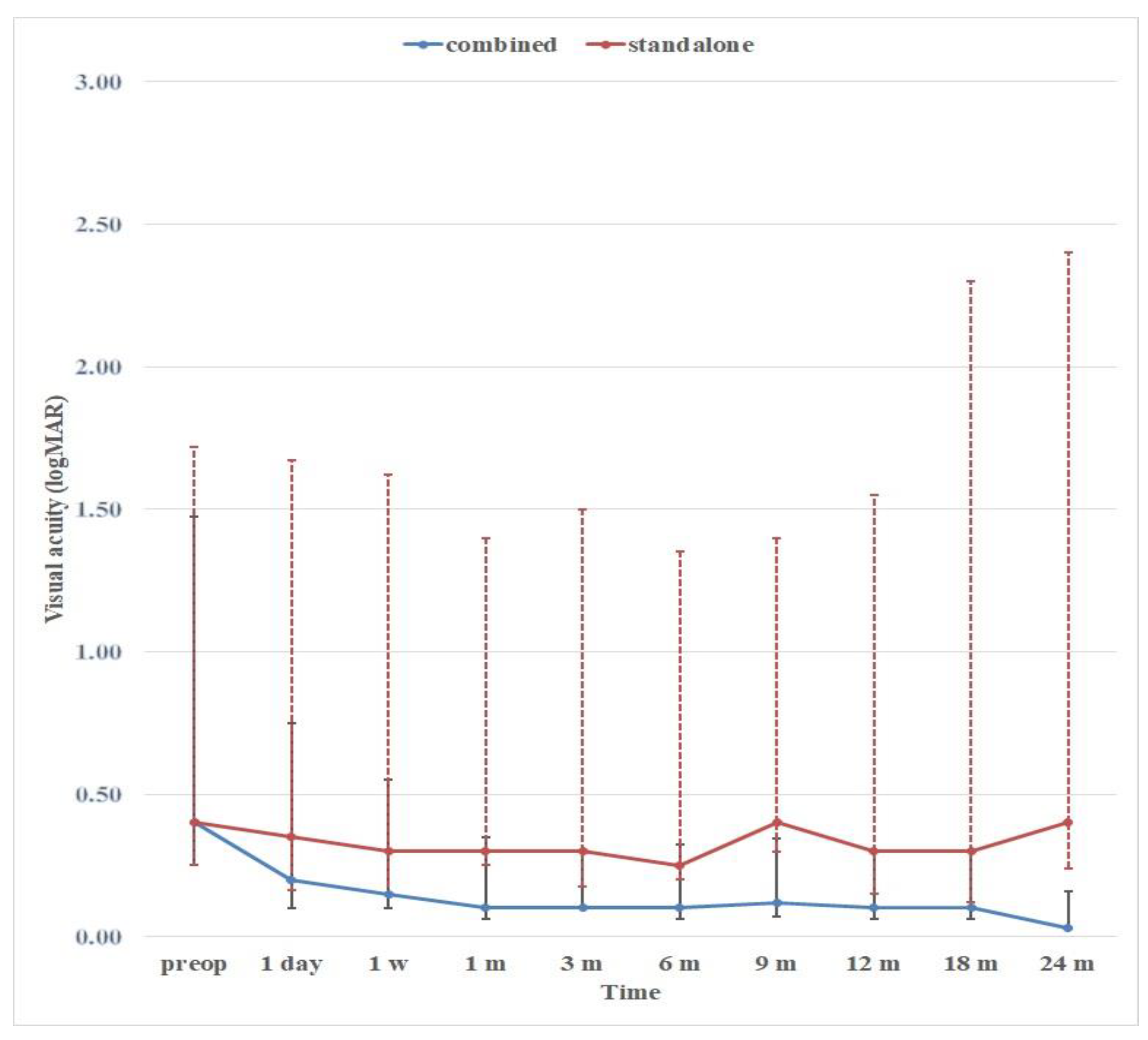
Figure 7.
Kaplan–Meier survival curve after surgery.
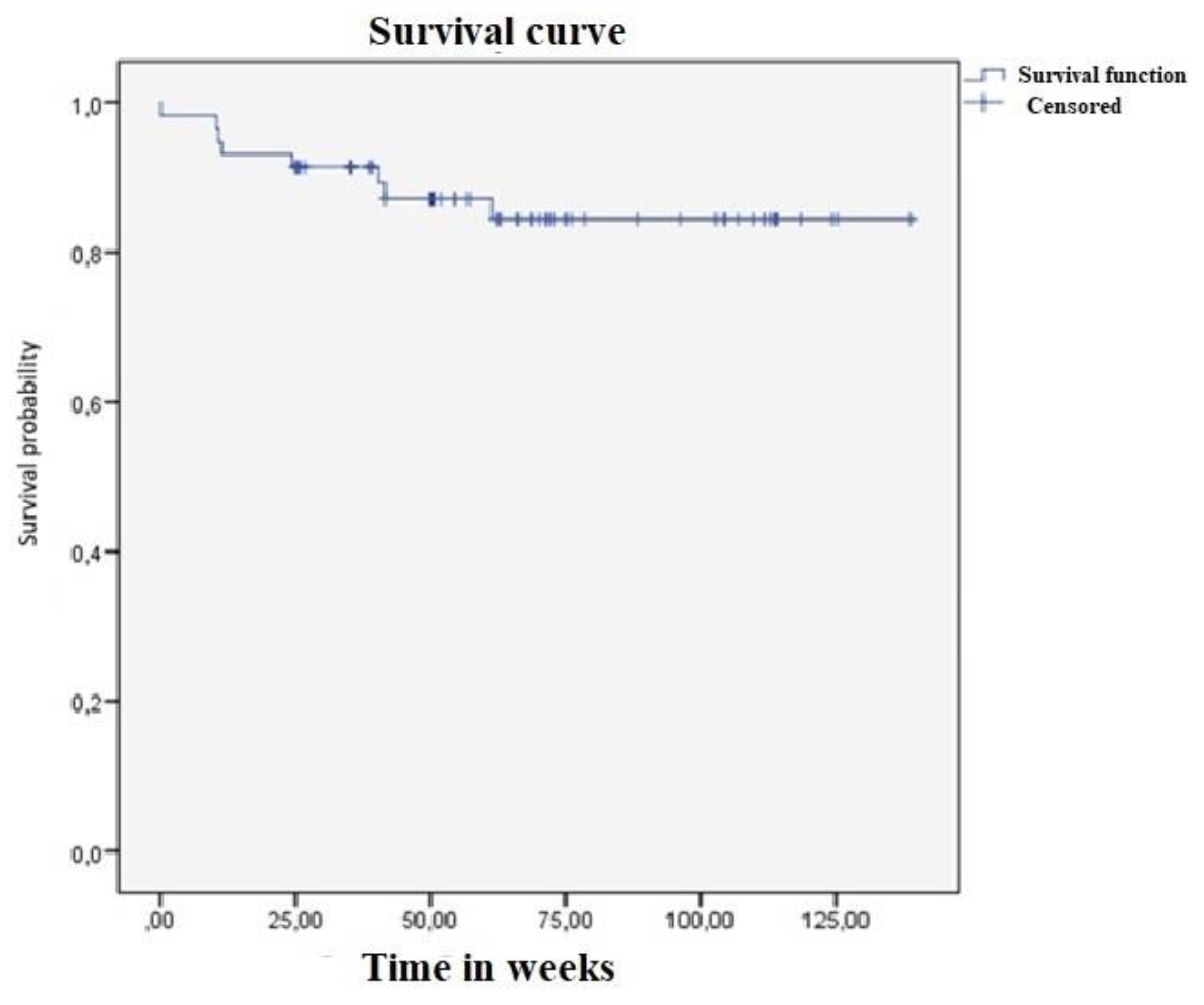
Figure 8.
Complications after receiving Nd:YAG laser trabeculotomy. (A) Trabeculotomy blockage by pigment. (B) Blockage by iris tissue. (C) Bleeding from Schlemm’s canal.
Figure 8.
Complications after receiving Nd:YAG laser trabeculotomy. (A) Trabeculotomy blockage by pigment. (B) Blockage by iris tissue. (C) Bleeding from Schlemm’s canal.
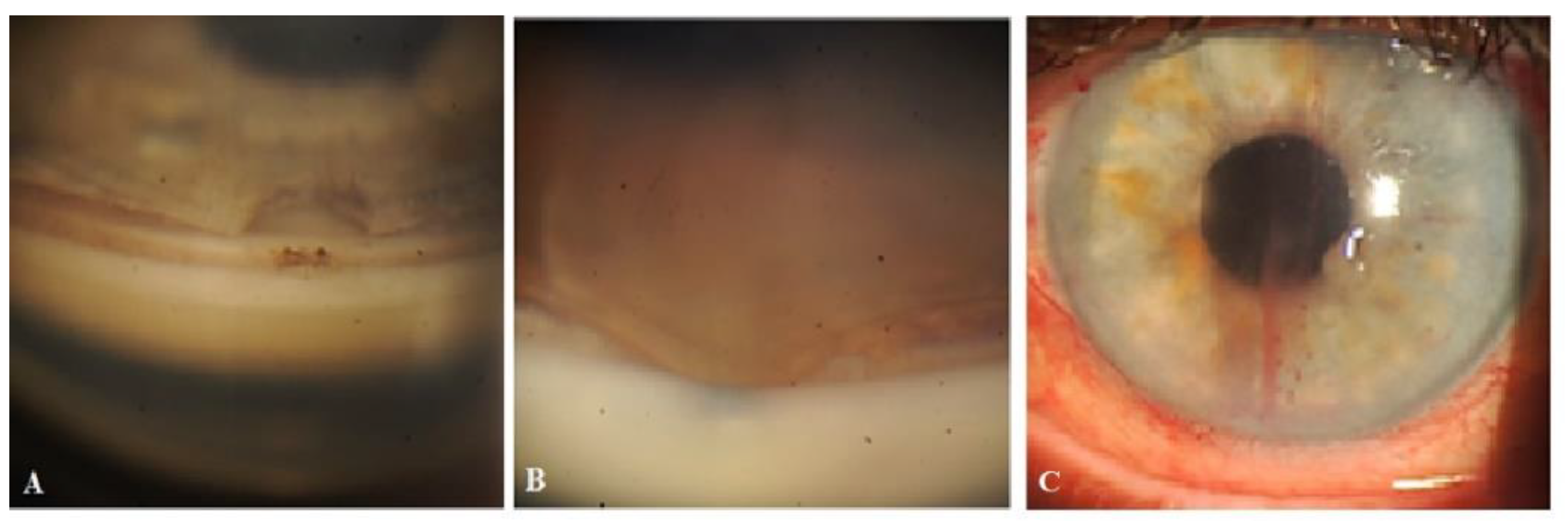
Figure 11.
Case 1 (right eye). Follow-up visit at 12 months. OCT scans of the superior nasal quadrant (A), surgery site (B), and superior temporal quadrant (C) showing a CLV with a VLS in its lumen (white arrow). Enlarged scans of the area of interest are displayed nearby, enclosed by a red boundary. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
Figure 11.
Case 1 (right eye). Follow-up visit at 12 months. OCT scans of the superior nasal quadrant (A), surgery site (B), and superior temporal quadrant (C) showing a CLV with a VLS in its lumen (white arrow). Enlarged scans of the area of interest are displayed nearby, enclosed by a red boundary. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
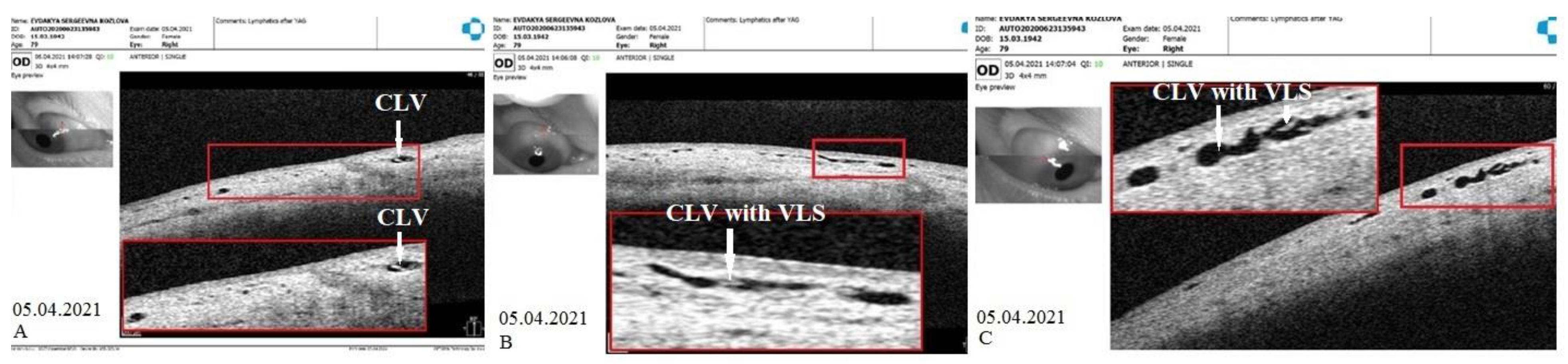
Figure 12.
Case 1 (right eye). Follow-up visit at 15 months. (A) Slit lamp view of the superior nasal quadrant showing a few CLVs, which are located far from the surgery site and which arose directly from sclera (arrow with sky-blue border). (B) Slit lamp image of the superior temporal quadrant and surgery site showing the absence of bleb and CLV (arrow with green border). (C) OCT scan of the superior nasal quadrant showing a CLV with a VLS in its lumen (white arrows); an enlarged scan of the area of interest is displayed nearby, enclosed by a red boundary. CLV = conjunctival lymphatic vessel; VLS = valve-like structures.
Figure 12.
Case 1 (right eye). Follow-up visit at 15 months. (A) Slit lamp view of the superior nasal quadrant showing a few CLVs, which are located far from the surgery site and which arose directly from sclera (arrow with sky-blue border). (B) Slit lamp image of the superior temporal quadrant and surgery site showing the absence of bleb and CLV (arrow with green border). (C) OCT scan of the superior nasal quadrant showing a CLV with a VLS in its lumen (white arrows); an enlarged scan of the area of interest is displayed nearby, enclosed by a red boundary. CLV = conjunctival lymphatic vessel; VLS = valve-like structures.
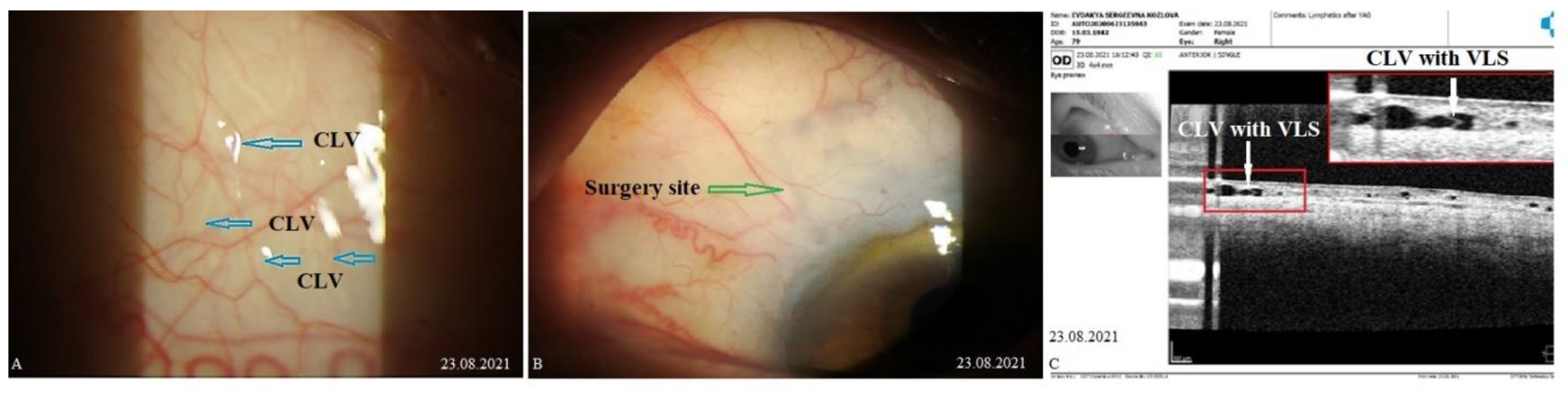
Figure 13.
Case 1 (right eye). Follow-up visit at 18 months. OCT horizontal scan of the superior temporal quadrant showing a CLV with a VLS (white arrows). An enlarged image of the area of interest is presented. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
Figure 13.
Case 1 (right eye). Follow-up visit at 18 months. OCT horizontal scan of the superior temporal quadrant showing a CLV with a VLS (white arrows). An enlarged image of the area of interest is presented. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
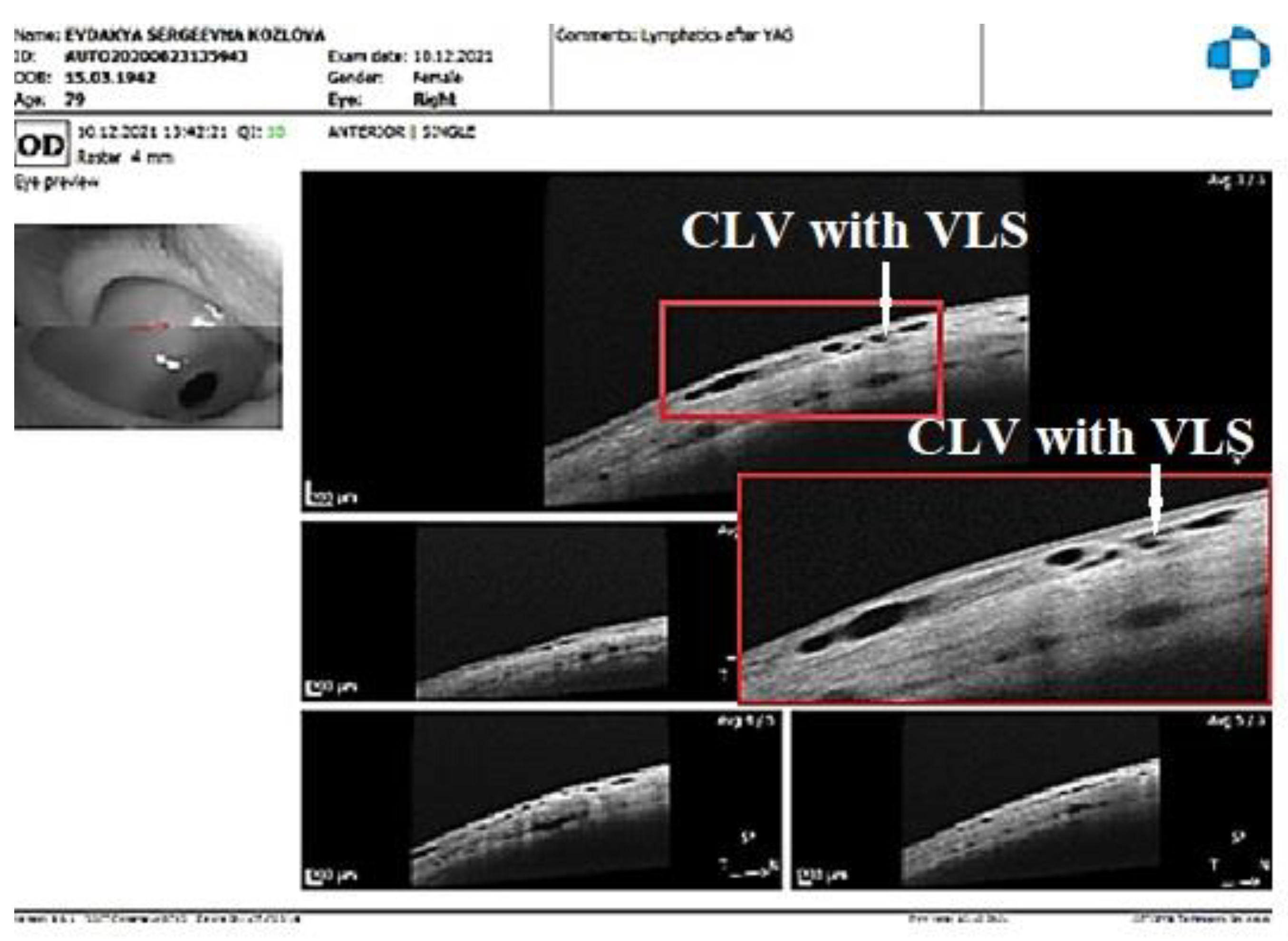
Figure 14.
Case 1 (left eye). CLV development after surgery. (A) Slit lamp view of the superior temporal quadrant on the day after laser trabeculotomy; a plexus of engorged CLVs with uneven calibers and filled with transparent fluid; some of these vessels originated from the surgery site and most of them run parallel to the limbus. (B) Slit lamp view of the superior temporal quadrant after 1 week; the size and number of vessels are considerably reduced, and they are less engorged. (C) slit lamp view of the superior temporal quadrant at follow-up visit at 14 months; an isolated CLV originating directly from the sclera located far from the surgery site; at the surgery site, there is no bleb or CLV. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
Figure 14.
Case 1 (left eye). CLV development after surgery. (A) Slit lamp view of the superior temporal quadrant on the day after laser trabeculotomy; a plexus of engorged CLVs with uneven calibers and filled with transparent fluid; some of these vessels originated from the surgery site and most of them run parallel to the limbus. (B) Slit lamp view of the superior temporal quadrant after 1 week; the size and number of vessels are considerably reduced, and they are less engorged. (C) slit lamp view of the superior temporal quadrant at follow-up visit at 14 months; an isolated CLV originating directly from the sclera located far from the surgery site; at the surgery site, there is no bleb or CLV. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
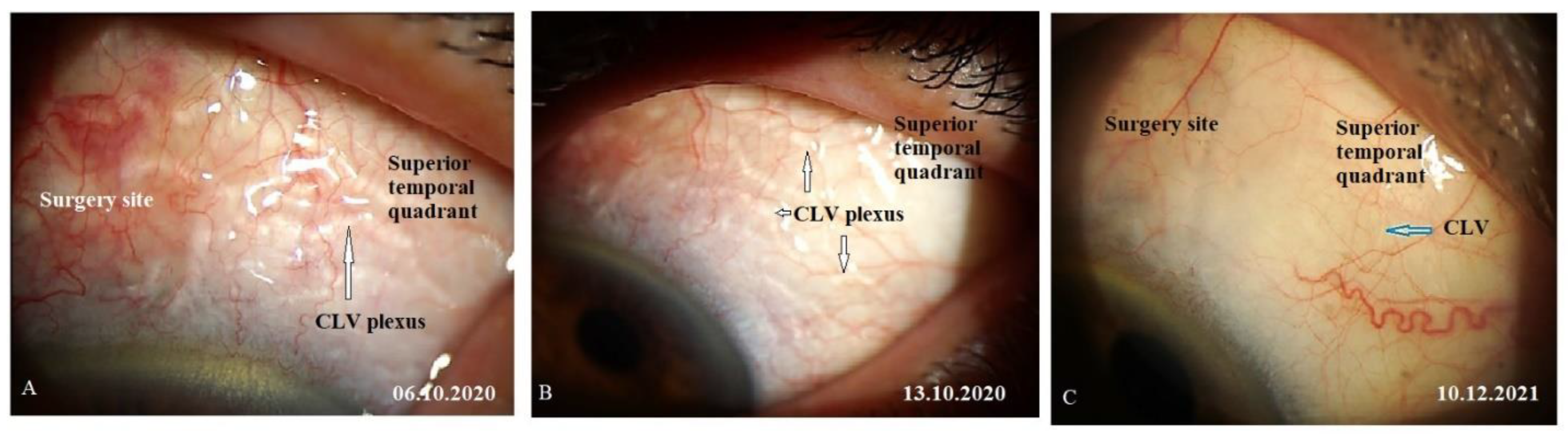
Figure 15.
Case 1 (left eye). CLV dynamics upon OCT investigation at different follow-up visits. (A) OCT scan of the superior temporal quadrant 2 weeks after laser trabeculotomy showing well-developed CLVs with VLSs in their lumens. (B) OCT scan of the same area as A, a CLV with a VLS at 4 weeks reduced in size; and (C) OCT scan of the same areas in A and B, at 6 months showing a CLV with a VLS in the lumen. The vessel is nearly non-identifiable. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.
Figure 15.
Case 1 (left eye). CLV dynamics upon OCT investigation at different follow-up visits. (A) OCT scan of the superior temporal quadrant 2 weeks after laser trabeculotomy showing well-developed CLVs with VLSs in their lumens. (B) OCT scan of the same area as A, a CLV with a VLS at 4 weeks reduced in size; and (C) OCT scan of the same areas in A and B, at 6 months showing a CLV with a VLS in the lumen. The vessel is nearly non-identifiable. CLV = conjunctival lymphatic vessel; VLS = valve-like structure.

Figure 16.
Case 1 (left eye). Slit lamp images of late follow-up visits. (A) Follow-up visit at 14 months and slit lamp view of the superior temporal quadrant and surgery site showing the absence of bleb and a few questionable isolated CLVs (arrow with red border). (B) Slit lamp view of the superior temporal quadrant at 18 months and a few collapsed CLVs (arrow with blue border); and (C) slit lamp view at 24 months after surgery. No bleb is observed at the surgery site (arrow with green border), and there is an isolated CLV in the temporal quadrant (arrow with sky-blue border). CLV = conjunctival lymphatic vessel.
Figure 16.
Case 1 (left eye). Slit lamp images of late follow-up visits. (A) Follow-up visit at 14 months and slit lamp view of the superior temporal quadrant and surgery site showing the absence of bleb and a few questionable isolated CLVs (arrow with red border). (B) Slit lamp view of the superior temporal quadrant at 18 months and a few collapsed CLVs (arrow with blue border); and (C) slit lamp view at 24 months after surgery. No bleb is observed at the surgery site (arrow with green border), and there is an isolated CLV in the temporal quadrant (arrow with sky-blue border). CLV = conjunctival lymphatic vessel.
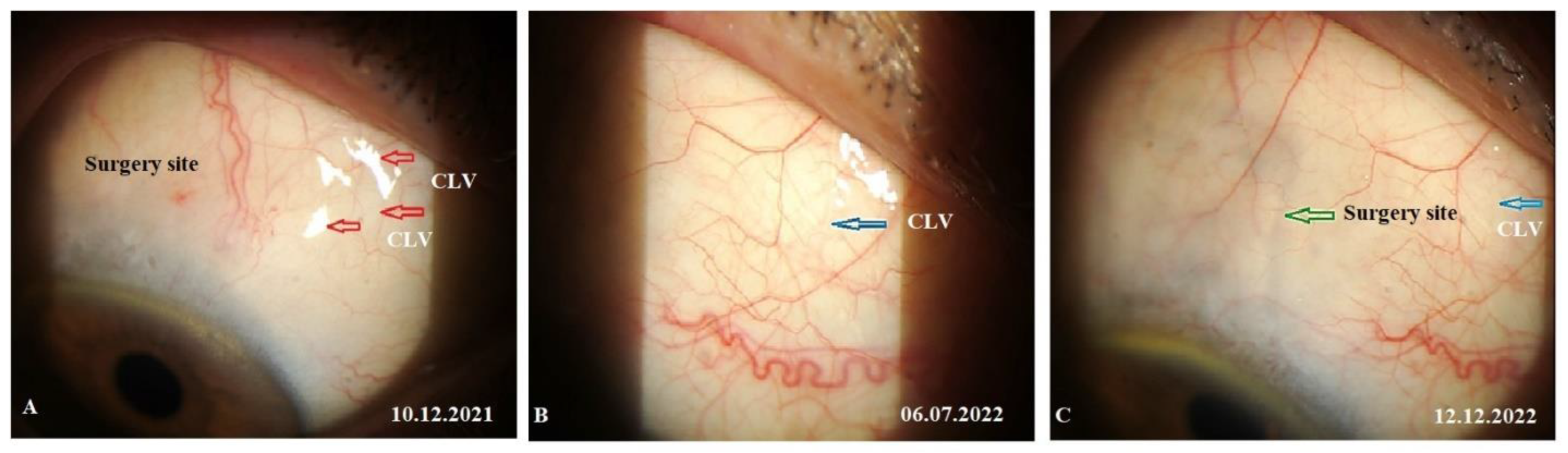
Figure 17.
Case 2 (left eye). OCT evaluation of the surgery site and superior quadrants 1 week after surgery (on 13 May 2022): horizontal (A) and vertical (B) scans of the superior nasal quadrant showing a CLV on the horizontal scan (arrow with white border); horizontal (C) and vertical (D) scans of the surgery site showing CLVs (arrows with white borders); and horizontal (E) and vertical (F) scans of the superior temporal quadrant showing CLVs (arrow with white border) with VLSs in their lumens. CLV = conjunctival lymphatic vessel.
Figure 17.
Case 2 (left eye). OCT evaluation of the surgery site and superior quadrants 1 week after surgery (on 13 May 2022): horizontal (A) and vertical (B) scans of the superior nasal quadrant showing a CLV on the horizontal scan (arrow with white border); horizontal (C) and vertical (D) scans of the surgery site showing CLVs (arrows with white borders); and horizontal (E) and vertical (F) scans of the superior temporal quadrant showing CLVs (arrow with white border) with VLSs in their lumens. CLV = conjunctival lymphatic vessel.
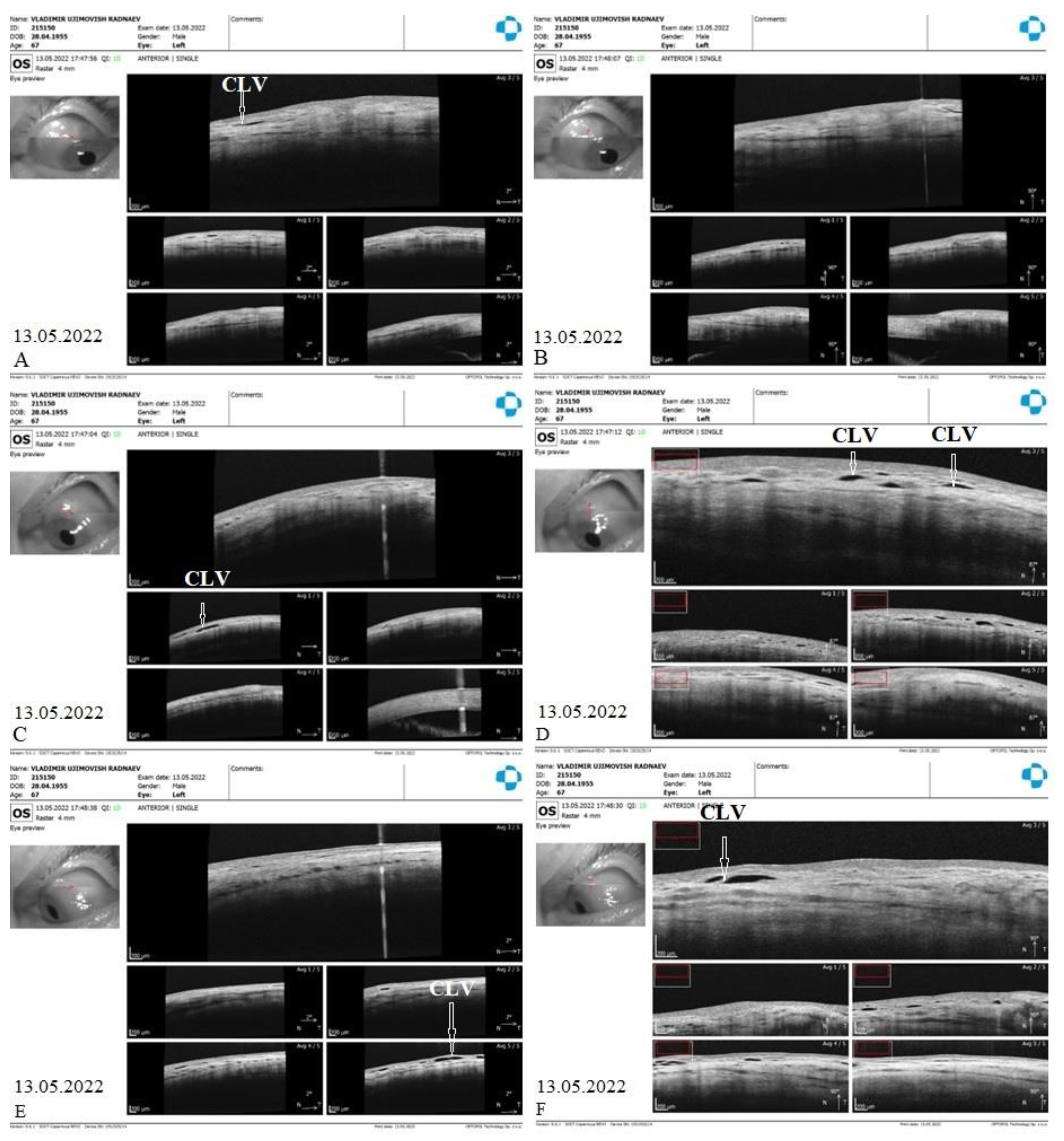
Figure 18.
Case 2 (left eye). Slit lamp view (red free filter) at 1 month (on 25 May 2022) after surgery. (A) Slit lamp view of the superior nasal quadrant, showing the absence of any CLVs. (B) Slit lamp view of the surgery site demonstrating the absence of bleb and CLVs (arrow with black border). (C) Slit lamp view of the superior temporal quadrant showing a CLV plexus (arrow with black border); CLVs have no connection to the surgery site, they arise directly from the sclera located at a considerable distance from the surgery site. CLV = conjunctival lymphatic vessel.
Figure 18.
Case 2 (left eye). Slit lamp view (red free filter) at 1 month (on 25 May 2022) after surgery. (A) Slit lamp view of the superior nasal quadrant, showing the absence of any CLVs. (B) Slit lamp view of the surgery site demonstrating the absence of bleb and CLVs (arrow with black border). (C) Slit lamp view of the superior temporal quadrant showing a CLV plexus (arrow with black border); CLVs have no connection to the surgery site, they arise directly from the sclera located at a considerable distance from the surgery site. CLV = conjunctival lymphatic vessel.
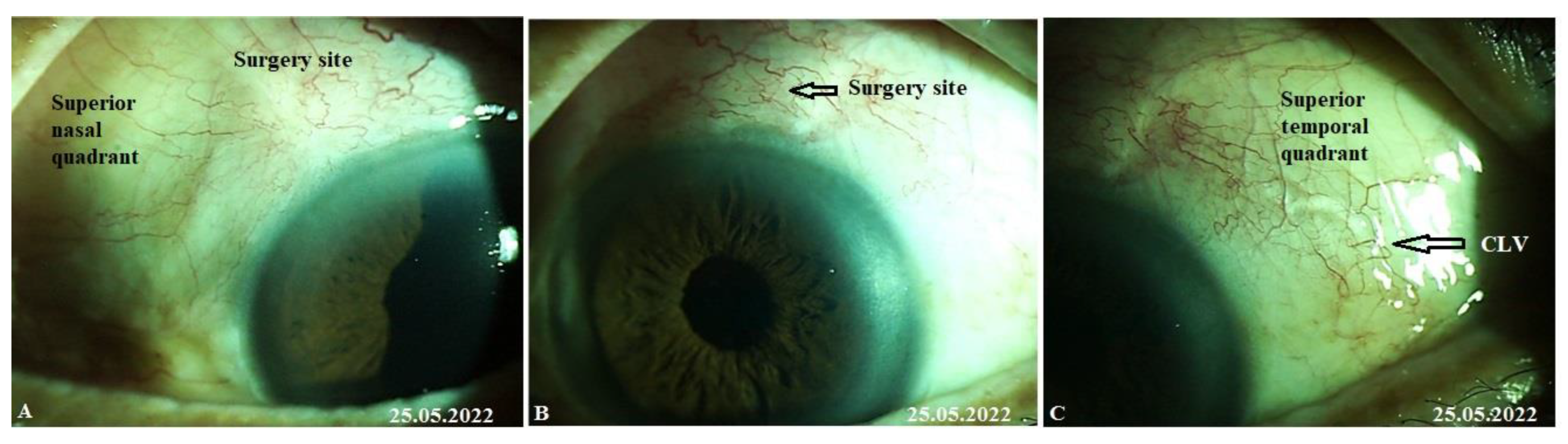
Figure 19.
Case 2 (left eye). OCT investigation at 1.5 months after surgery (on 22 June 2022). OCT raster scans of the superior temporal quadrant (A, B) and surgery site (C, D) demonstrating CLVs (arrows with white borders); in scan C, a collagen implant (CI) can also be observed in the ISR and there is no bleb above it. Scans of the superior nasal quadrant are not included as they lack any useful information. CLV= conjunctival lymphatic vessel; CI = collagen implant.
Figure 19.
Case 2 (left eye). OCT investigation at 1.5 months after surgery (on 22 June 2022). OCT raster scans of the superior temporal quadrant (A, B) and surgery site (C, D) demonstrating CLVs (arrows with white borders); in scan C, a collagen implant (CI) can also be observed in the ISR and there is no bleb above it. Scans of the superior nasal quadrant are not included as they lack any useful information. CLV= conjunctival lymphatic vessel; CI = collagen implant.
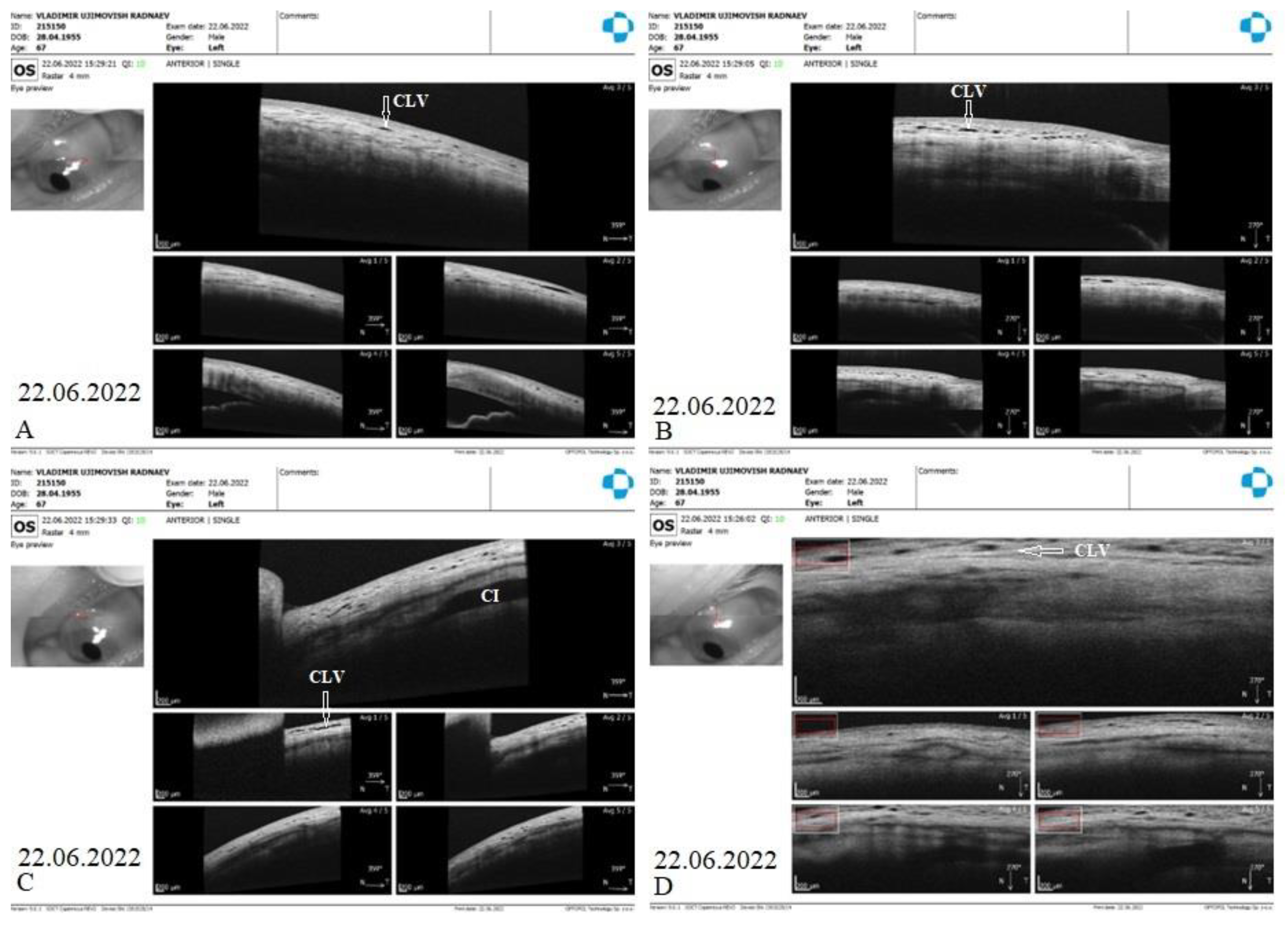
Figure 20.
Case 2 (left eye). Slit lamp views at 12 months after surgery (on 21 April 2023). (A) Slit lamp view of the superior nasal quadrant showing a well-developed CLV plexus (black horizontal arrow); the vessels became engorged after a gentle massage moving the eyelid over them (pl. refer to video S2_Case 2_month 12 after surgery), CLVs show no connection with the surgery site; they arise directly from the sclera located at a considerable distance from surgery site. (B) Slit lamp view of the surgery site demonstrating the absence of filtration blebs and CLVs. (C) Slit lamp view of the superior temporal quadrant showing remnants of previously developed CLV plexus (black arrow). CLV = conjunctival lymphatic vessel.
Figure 20.
Case 2 (left eye). Slit lamp views at 12 months after surgery (on 21 April 2023). (A) Slit lamp view of the superior nasal quadrant showing a well-developed CLV plexus (black horizontal arrow); the vessels became engorged after a gentle massage moving the eyelid over them (pl. refer to video S2_Case 2_month 12 after surgery), CLVs show no connection with the surgery site; they arise directly from the sclera located at a considerable distance from surgery site. (B) Slit lamp view of the surgery site demonstrating the absence of filtration blebs and CLVs. (C) Slit lamp view of the superior temporal quadrant showing remnants of previously developed CLV plexus (black arrow). CLV = conjunctival lymphatic vessel.
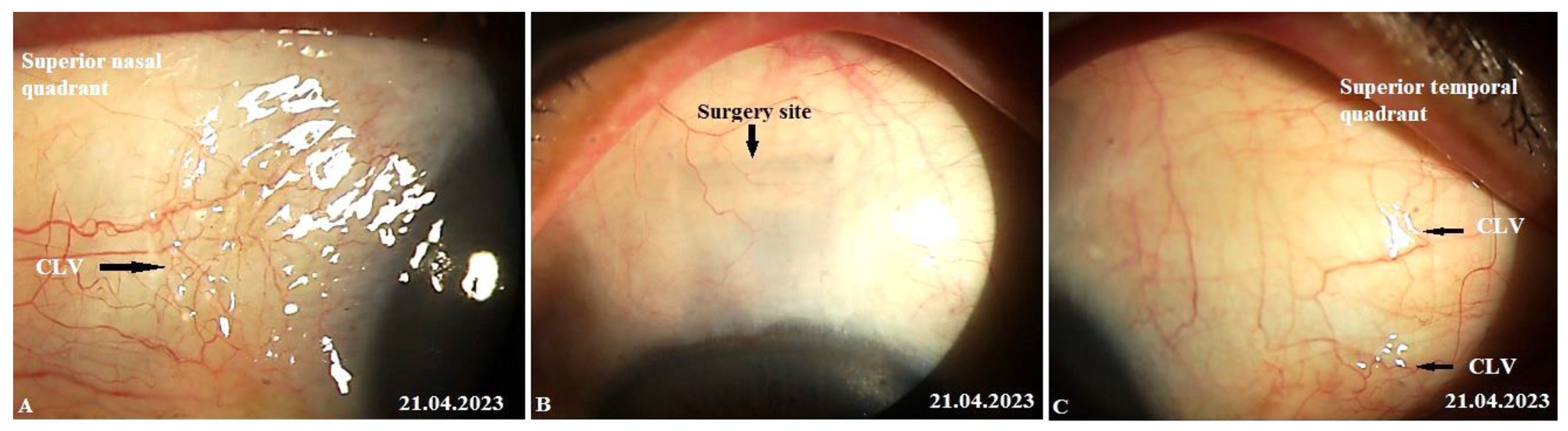
Figure 21.
Case 3 (left eye). Postoperative follow-up visits. (A) Slit lamp view of the surgery site before sutures were removed. There is no bleb at the surgery site. (B) Slit lamp view of the surgery site after sutures were removed and Nd:YAG laser trabeculotomy was performed, resulting in conjunctival swelling at the surgery site. OCT confirmed the absence of blebs. (C–D) Slit lamp view of the surgery site and superior temporal quadrant 12 days after trabeculotomy on 09 March 2021, a plexus of engorged transparent vessels with uneven calibers overfilled with transparent fluid was observed at the surgery site (arrows with white borders); its course could be detected towards the superior temporal quadrant, and no CLVs were visible in the superior nasal quadrant. (E–F) Slit lamp view of the superior temporal quadrant after another 2 weeks on 23 March 2021; the CLV plexus disappeared from the surgery site leaving few CLVs in the superior temporal quadrant (arrows with black borders) with reduced sizes. (G) Slit lamp view of the surgery site and superior nasal and temporal quadrants 15 months after postoperative follow-up visit. No blebs or CLVs could be detected. CLV = conjunctival lymphatic vessel.
Figure 21.
Case 3 (left eye). Postoperative follow-up visits. (A) Slit lamp view of the surgery site before sutures were removed. There is no bleb at the surgery site. (B) Slit lamp view of the surgery site after sutures were removed and Nd:YAG laser trabeculotomy was performed, resulting in conjunctival swelling at the surgery site. OCT confirmed the absence of blebs. (C–D) Slit lamp view of the surgery site and superior temporal quadrant 12 days after trabeculotomy on 09 March 2021, a plexus of engorged transparent vessels with uneven calibers overfilled with transparent fluid was observed at the surgery site (arrows with white borders); its course could be detected towards the superior temporal quadrant, and no CLVs were visible in the superior nasal quadrant. (E–F) Slit lamp view of the superior temporal quadrant after another 2 weeks on 23 March 2021; the CLV plexus disappeared from the surgery site leaving few CLVs in the superior temporal quadrant (arrows with black borders) with reduced sizes. (G) Slit lamp view of the surgery site and superior nasal and temporal quadrants 15 months after postoperative follow-up visit. No blebs or CLVs could be detected. CLV = conjunctival lymphatic vessel.
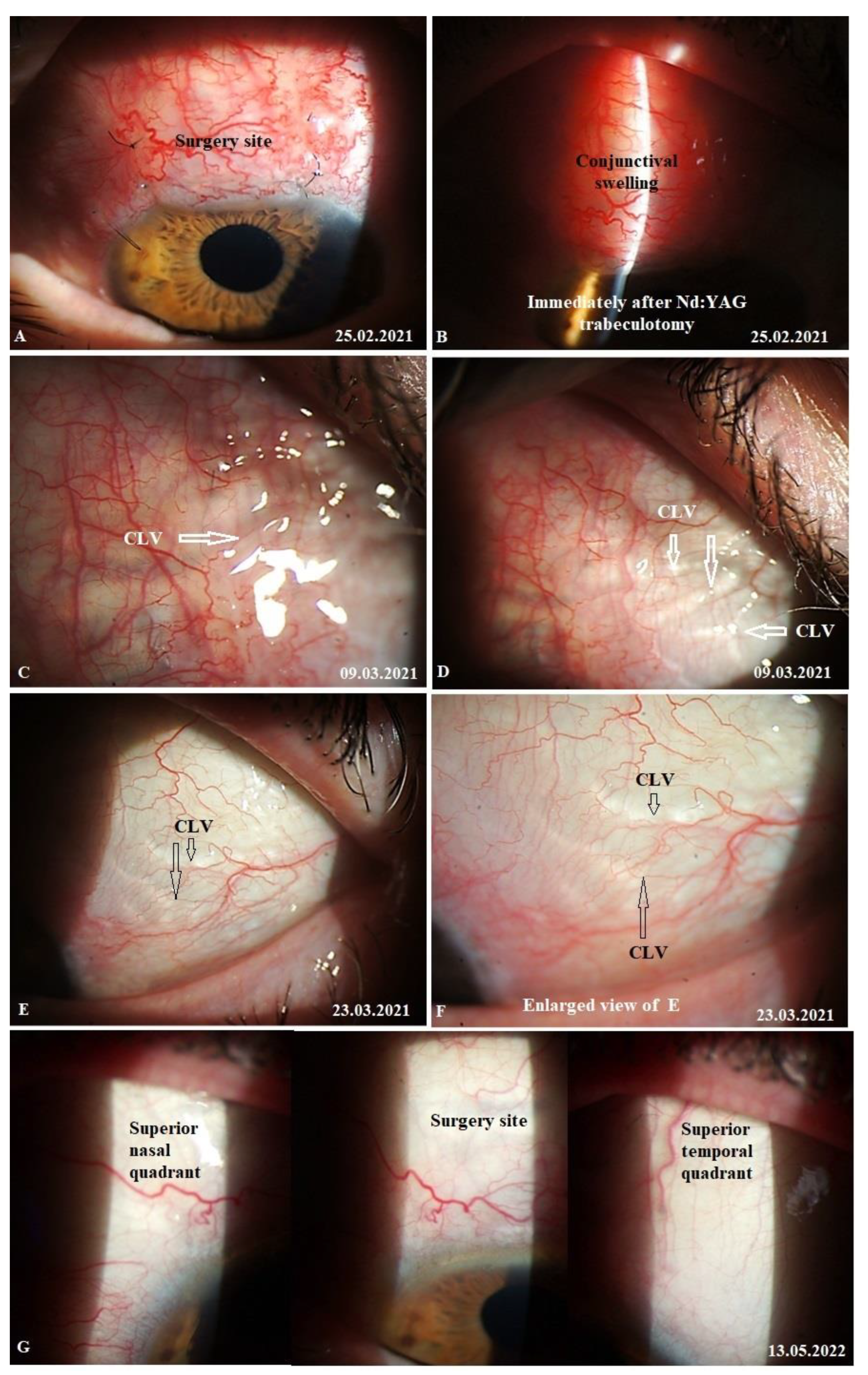
Figure 22.
D). Case 3 (left eye). OCT investigation at 12 months after surgery (on 16 February 2022). OCT raster scans of conjunctiva in superior nasal (A: horizontal scan, B: vertical scan) and temporal quadrants (E: horizontal scan, F: vertical scan) and at the surgery sites (C: horizontal scan, D: vertical scan); few CLVs with valve-like structures in their lumens could be identified in all investigated areas. CLV = conjunctival lymphatic vessel.
Figure 22.
D). Case 3 (left eye). OCT investigation at 12 months after surgery (on 16 February 2022). OCT raster scans of conjunctiva in superior nasal (A: horizontal scan, B: vertical scan) and temporal quadrants (E: horizontal scan, F: vertical scan) and at the surgery sites (C: horizontal scan, D: vertical scan); few CLVs with valve-like structures in their lumens could be identified in all investigated areas. CLV = conjunctival lymphatic vessel.
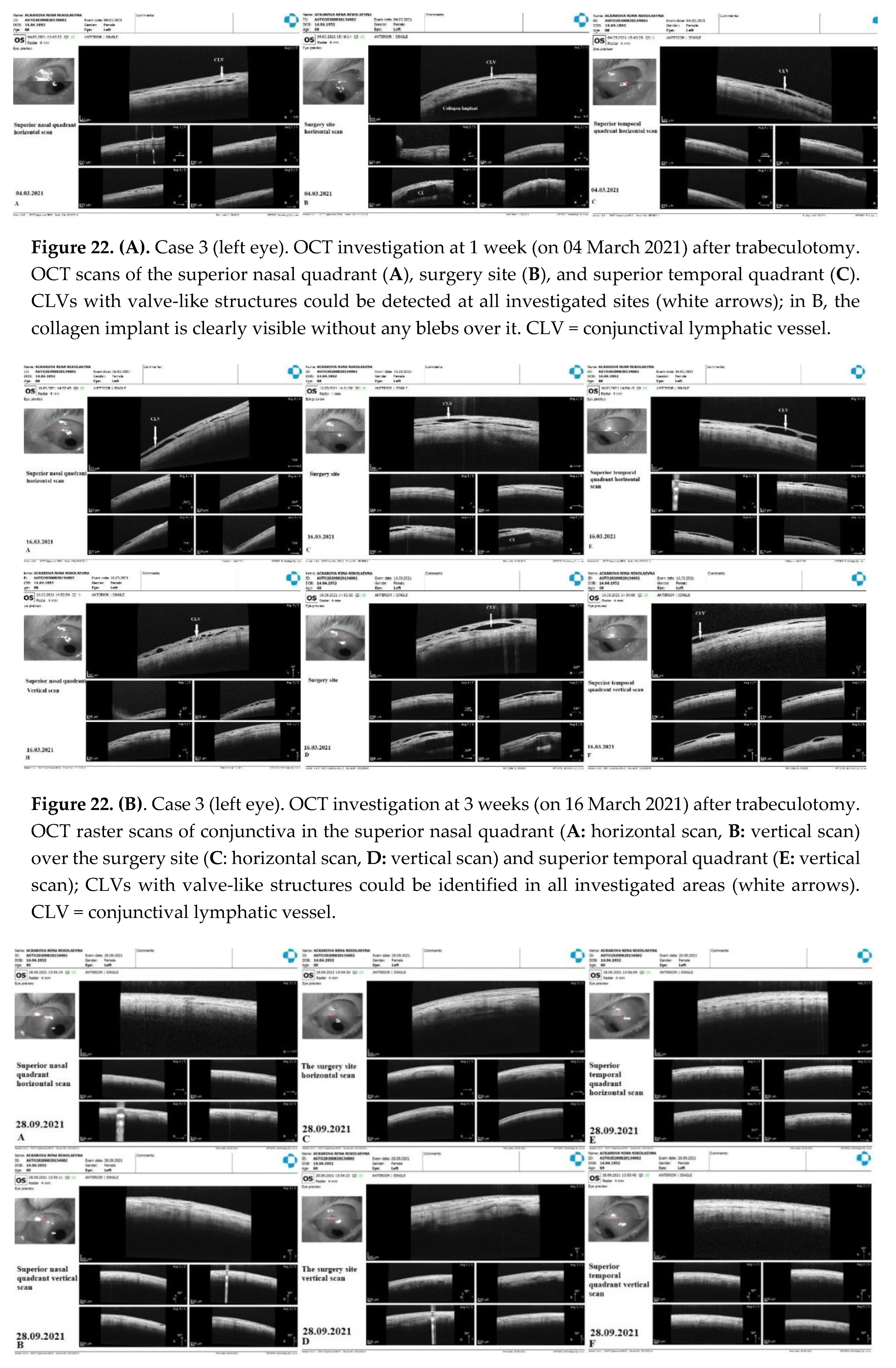
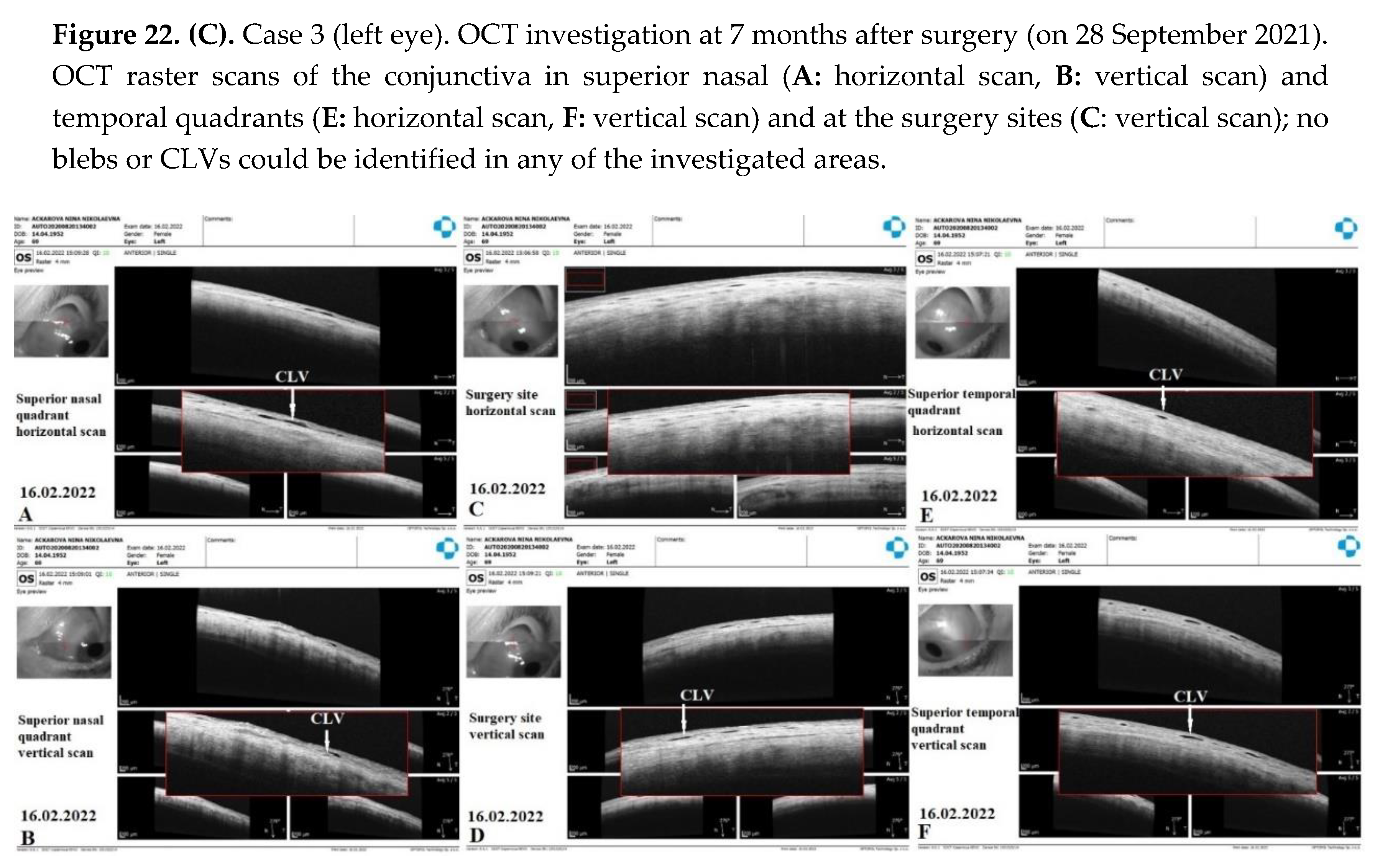

Table 1.
Demographic and clinical data of 58 patients included in the study.
| Variables | Number of patients (%) |
|---|---|
| Eyes n | |
| Right | 28 (48.3) |
| Left | 30 (51.7) |
| Sex | |
| Male | 18 (31.1) |
| Female | 40 (68.9) |
| Mean age (SD) [95% CI] years | 75.5 (7.7) [73.5 – 77.5] |
| The median postoperative observation period (p25; p75) in weeks | 76.3 (63.1; 111.8) |
| Type of glaucoma | |
| Primary open angle | 42 (72.4) |
| Previously operated open-angle glaucoma | 16 (27.6) |
| Glaucoma surgery performed one time | 11 |
| Glaucoma surgery performed two times | 4 |
| Glaucoma surgery performed more than three times | 1 |
| Type of glaucoma surgery performed (number of eyes) | |
| Trabeculectomy | 6 |
| Segmental dilation of Schlemm’s canal using stainless steel expander | 7 |
| Laser iridotomy | 2 |
| Cyclodialysis ab externo with implantation of a collagen implant in the tunnel | 6 |
| Non-penetrating deep sclerectomy | 1 |
| Severity of glaucoma | |
| Moderate | 21 (36.2) |
| Severe | 37 (63.8) |
| Median preoperative IOP in mm Hg (p25; p75) | 27.0 (23.5; 28.0) |
| Median preoperative hypotensive medication use (p25; p75) | 3 (2;3) |
| Number of patients who used 2 classes of hypotensive medications | 21 (36.2) |
| Number of patients who used 3 classes of hypotensive medications | 26 (44.8) |
| Number of patients who used 4 classes of hypotensive medications | 10 (17.2) |
| Number of patients who used 5 classes of hypotensive medications | 1 (1.7) |
| Lens condition | |
| Visually significant cataract | 40 (68.9) |
| Pseudophakia | 15 (25.9) |
| Comorbidities | |
| Macular degeneration | 3 (5.2) |
| Pseudo-exfoliative syndrome | 24 (41.4) |
| High myopia | 3 (5.2) |
| Diabetes mellitus | 5 (8.6) |
CI = confidence interval; IOP = intraocular pressure; n = number of cases; p25 = 25th percentile; p75 = 75th percentile; and SD = standard deviation.
Table 2.
IOP changes.
| Follow-up period | n | IOP in mmHg median (p25; p75); mean (SD) |
% reduction in IOP | p-value |
|---|---|---|---|---|
| Baseline | 58 | 27.0 (21.0; 30) | - | - |
| 1 day | 58 | 14.7 (7.1) | 45.6 | 2.6x10-12 |
| 1 week | 56 | 9.0 (7.2; 13.0) | 66.7 | <0.001 |
| 1 month | 57 | 11.3 (4.3) | 58.1 | 1.5x10-22 |
| 3 months | 49 | 12.5 (10; 16.0) | 53.7 | <0.001 |
| 6 months | 51 | 14.9 (5.0) | 44.8 | 2.1x10-13 |
| 12 months | 43 | 15.0 (13.0; 18.0) | 44.4 | <0.001 |
| 18 months | 30 | 16.5 (6.2) | 38.9 | 1.1x10-10 |
| 24 months | 16 | 15.2 (3.3) | 43.7 | 1.7x10-06 |
IOP =intraocular pressure; n =number of cases; p25 =25th percentile; p75 =75th percentile; and SD =standard deviation.
Table 3.
Patient distribution as a percentage reduction in IOP at different follow-up visits.
| Reduction in IOP % | Follow-up visits, n (%) | ||||||
|---|---|---|---|---|---|---|---|
| 1 m | 3 m | 6 m | 9 m | 12 m | 18 m | 24 m | |
| ≤ 20 | 1 (1.7) | 5 (10.2) | 8 (15.7) | 5 (11.4) | 7 (16.3) | 5 (16.7) | 1 (6.3) |
| >20 and ≤30 | 2 (3.5) | 6 (12.2) | 5 (9.8) | 7 (15.9) | 4 (9.3) | 5 (16.7) | 3 (18.7) |
| >30 and ≤40 | 6 (10.5) | 4 (8.2) | 8 (15.7) | 6 (13.6) | 10 (23.3) | 9 (30.0) | 5 (31.3) |
| >40 | 48 (84.3) | 34 (69.4) | 30 (58.8) | 26 (59.1) | 22 (51.1) | 11 (36.6) | 7 (43.7) |
| n | 57 | 49 | 51 | 44 | 43 | 30 | 16 |
where IOP=intraocular pressure; n=number of patients; m=months.
Table 4.
Period between surgery and Nd:YAG laser trabeculotomy.
| Period | Number of cases |
|---|---|
| Laser trabeculotomy not performed | 19 |
| ≤10 days | 20 |
| 11–30 days | 13 |
| 1–3 months | 4 |
| 3–6 months | 2 |
| Total | 58 |
Table 5.
IOP decrease after Nd:YAG laser trabeculotomy operation.
| IOP (mmHg) | Number of cases before trabeculotomy | Number of cases after trabeculotomy |
|---|---|---|
| ≤ 10.0 | 0 | 17 |
| 10.1 – 15 | 0 | 13 |
| 15.1 – 20 | 7 | 5 |
| 20.1 – 25 | 6 | 4 |
| 25.1 – 30 | 19 | 0 |
| 30.1 – 35 | 4 | 0 |
| 35.1 – 40 | 1 | 0 |
| ≥ 40 | 2 | 0 |
| Total | 39 | 39 |
Table 6.
Time of CLV development and duration of CLV visibility based on slit lamp examination in twenty-nine eyes.
Table 6.
Time of CLV development and duration of CLV visibility based on slit lamp examination in twenty-nine eyes.
| CLVs details | Follow-up visits, number of eyes | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 1 D | 1 W | 1 M | 3 M | 6 M | 9 M | 12 M | 18 M | 24 M | |
| Time of CLVs development | 6 | 7 | 14 | 1 | 0 | 1 | 0 | 0 | 0 |
| CLVs remained identifiable | 3 | 2 | 11 | 5 | 1 | 2 | 1 | 0 | 4 |
D=day; W=week; M=months; and CLVs=conjunctival lymphatic vessels.
Table 7.
CLVs development as per the operated eye.
| CLVs observed at | Surgery performed on the right eye, number of eyes | Surgery performed on the left eye, number of eyes | ||
|---|---|---|---|---|
| Slit lamp exam. | OCT exam. | Slit lamp exam. | OCT exam. | |
| Surgery site | 1 | 2 | 1 | 1 |
| Superior nasal quadrant | 9 | 4 | 1 | 1 |
| Superior temporal quadrant | 0 | 1 | 4 | 0 |
| Surgery site and superior nasal quadrant | 2 | 6 | 1 | 5 |
| Surgery site and superior temporal quadrant | 0 | 1 | 2 | 2 |
| Superior nasal and temporal quadrants | 3 | 1 | 2 | 1 |
| Surgery site and superior nasal and temporal quadrants | 2 | 9 | 1 | 14 |
| Total | 17 | 24 | 12 | 24 |
CLVs = conjunctival lymphatic vessels; OCT = optical coherence tomography.
Table 8.
CLV development and success rate.
| Success rate | Subgroup I* (n=29), number of cases (%) | Subgroup II** (n=29), number of cases (%) | p-value |
|---|---|---|---|
| Complete success | 11 (37.9) | 22 (75.9) | 0.000368 |
| Qualified success | 24 (82.7) | 26 (89.7) | 0.5939 |
| Partial success | 13 (44.8) | 4 (13.8) | 5.13X 10-5 |
| Failure | 5 (17.3) | 3 (10.3) | 0.1827 |
*Cases with CLVs development; ** cases without CLVs development.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



