
Submitted:
03 August 2023
Posted:
07 August 2023
You are already at the latest version
Abstract
Cardiovascular diseases (CVDs) represent the leading cause of global mortality with 1,7 million deaths a year. One of the alternative systems to drug therapy to minimize the risk of CVDs is represented by alpha-linolenic acid (ALA), an essential fatty acid of the Omega-3 series, known for its cholesterol-lowering effect. The main purpose of this review is to analyze the effects of ALA and investigate the relevant n-6/n-3 ratio in order to maintain functionally beneficial effects. Concerning the lipid-lowering preventive effects, ALA may favorably affect the values of LDL-C and triglycerides in either adult and pediatric populations and it has a positive and protective effect against hypertension, suggesting that ALA is an useful diet-related antihypertensive compound. According to the 2009 EFSA statement, dietary ALA may contribute to reducing the risk of CVDs, thanks to anti-hypertensive, anti-atherosclerotic and cardio-protective effects.
Keywords:
alpha-linolenic acid
; hempseed oil
; cardiovascular events
; LDL-cholesterol
; TCcholesterol
; cardioprotective effect
; heart disorders
; linoleic acid
1. Introduction
Cardiovascular diseases (CVDs) represent the primary cause of global mortality, as they are responsible for about 1,7 million deaths a year, and the major contributor to reduced quality of life [1,2].
CVDs include ischemic heart disease (IHD), stroke, heart failure, peripheral arterial disease, and several other cardiac and vascular conditions. As of 2023, the American Heart Association identifies CVDs as the leading cause of death in the United States, accounting for 928.741 deaths in 2020. Between 2018 and 2019, direct and indirect costs of total CVD were $407.3 billion ($251.4 billion in direct costs and $155.9 billion in lost productivity/mortality) [3].
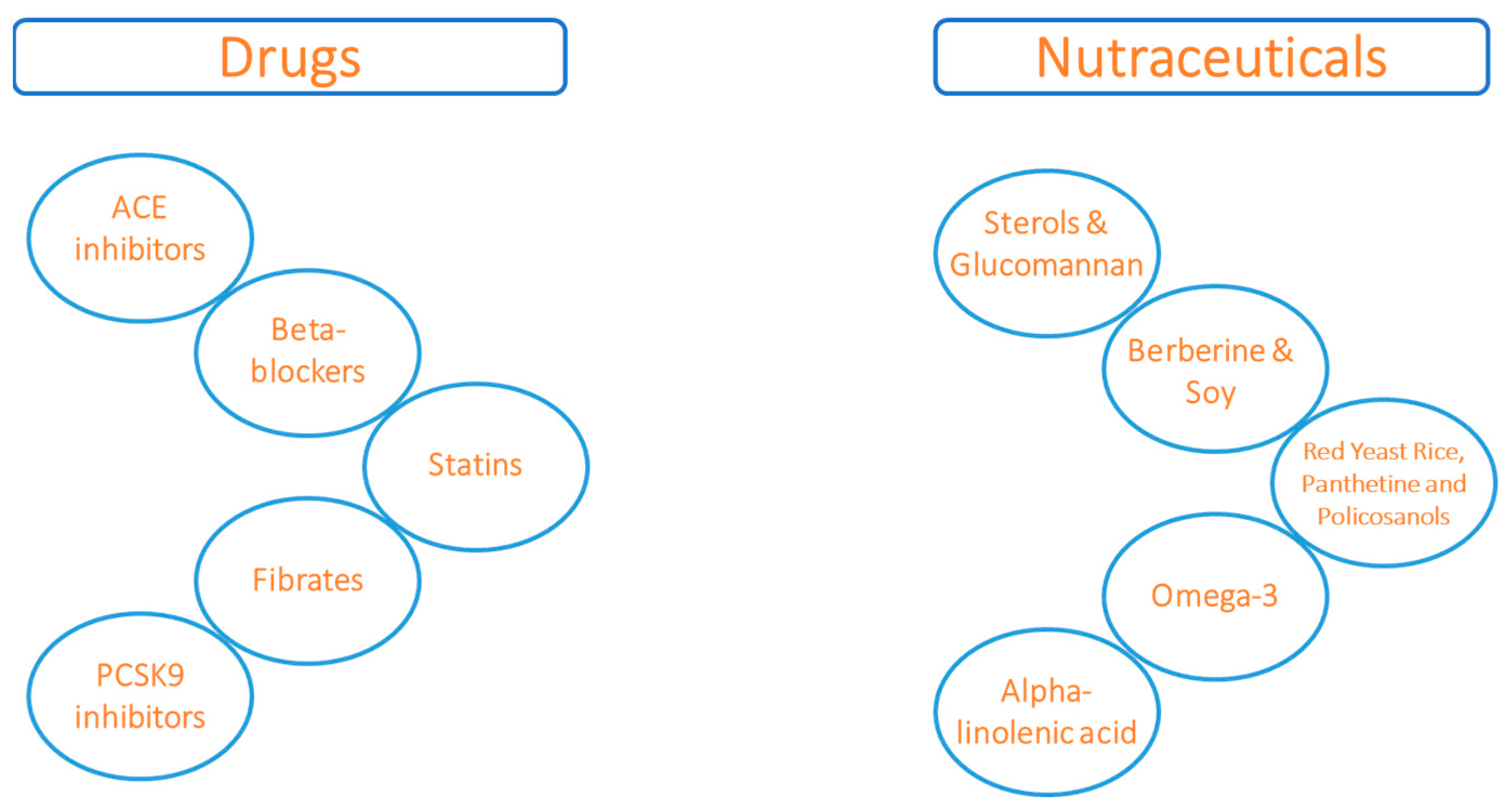
In addition to conventional pharmacological therapy (ACE inhibitors, beta-blockers, statins, fibrates and PCSK9 inhibitors), nutraceutical solutions have been proposed in recent years as contributing factors to reduce cardiovascular risk [4,5]. Accordingly, nutraceuticals may act on the reduction of lipid risk markers, including Total Cholesterol (TC), Low-Density Lipoprotein (LDL-C), and triglycerides (TG) and can be divided on the basis of their mechanism of action.
For instance, sterols and glucomannan may reduce LDL-C by decreasing the intestinal absorption of endogenous cholesterol, competing in the formation of solubilized micelles [6,7], which interact with the membrane and are the substrate of the Niemann-Pick C1-Like 1 (NPC1L1) transporter that facilitates the transport of sterols from the intestinal lumen. Red yeast rice, garlic, panthetine, and policosanols (mimicking statin action) inhibit hepatic cholesterol synthesis. These types of nutraceuticals have a reversible inhibitory action on 3-Hydroxy-3-Methyl-Glutaryl-CoA (HMG-CoA) reductase, the key enzyme in the synthesis of endogenous cholesterol. Food supplements usually derived from red yeast rice contain a concentration of monacolins up to 1,9% [8].
Berberine acts directly on the expression of the LDL receptor (LDL-R) an up-regulation of the receptors through a post-transcriptional mechanism that stabilizes their mRNA.
Recent studies have underlined that it reduces the intestinal absorption of cholesterol, increasing fecal excretion and promoting its hepatic turnover and the formation of bile acids [9].
Similarly, plant-derived polyunsaturated fatty acids (PUFAs) may share analogous functional effects. The human body possesses the capacity to endogenously synthesize the amount of required fatty acids, except for linoleic acid (LA), the precursor of the Omega-6 fatty acids, and alpha-linolenic acid (ALA), the precursor of the Omega-3 fatty acids. Since these compounds must be introduced with diet, they are called essential fatty acids (EFAs).
LA and ALA are in competition, as they are metabolized by the enzyme delta-6-desaturase. This has been suggested to be important for health, as a high intake of LA may reduce the amount of the enzyme available for ALA metabolism, so increasing the risk of heart disease through mechanisms mainly associated with pro-inflammatory conditions [12,13,14]. Evidence supporting this theory shows that over the past 150 years, Omega-6 intakes through today’s diet have increased, while Omega-3 intakes have decreased in parallel with the increase in heart disease. Thus, the concept of an “ideal” ratio of n-6/n-3 in the diet was developed and is between 10:1 and 5:1[15,16]. Within this context, while the functional effects of LA are well-known [17,18,19,20,21], ALA, present in hempseed oil (HSO), walnuts, olive and flaxseed oils, has less known, but still relevant, functional effects. Nuts and seeds are important sources of ALA and other micronutrients, such as sterols, fibers and polyphenolic compounds. These nutrients are effective in protecting against cardiovascular, inflammatory, and chronic diseases [22,23,24]. Regarding the ALA content of nuts and seeds, 28 g of hempseed, or walnuts exceeds the Adequate Intake for ALA, which is 1.1 g/day for women, and 1.6 g/day for men [25,26]. Oils rich in ALA, such as flaxseed and hempseed ones, are effective in analyzing the effects of ALA. Flaxseed, hempseed and canola oil are the main sources of ALA; soybean oil is often considered to be a low to moderate source of this nutrient, as studies of its fatty acid composition have shown ALA concentrations ranging from 2.7% to 7.8% [27,28]. These dietary sources of ALA may also be relevant during pregnancy and breastfeeding women, not only because of their rich nutritional composition, but also because of the well-founded need to avoid complex mixtures of herbal supplements that may jeopardize the health of both mother and child. In addition, plant sources of omega-3 PUFAs could be considered an effective option for women who cannot tolerate fatty fish and for those who suffer from nausea, common manifestation during pregnancy [29,30]. Exclusively vegan diets should be evaluated carefully because of the risk of n-3 PUFA deficiency. In addition to lower intakes of total and saturated fats, another characteristic of exclusively vegan diets is a higher proportional intake of n-6 PUFAs compared to vegetarian diets [31,32]. For these reasons, recommendations for vegan diets that include adequate amounts of ALA are of paramount importance for the maintenance of long-term health [33].
Therefore, the main purpose of this narrative review is to analyze the effects of ALA and investigate the relevant n-6/n-3 ratio in order to maintain functionally favorable effects [34,35,36].
Functional Effects of ALA
We selected different studies about ALA and its effects on the cardiovascular system and categorized them by effects, on risk factors for CVD, and direct cardioprotection, respectively.
Risk Factors for Cardiovascular Disease
The most important claim declared by EFSA concerning ALA is related to the influence on blood cholesterol concentrations (EFSA 2009; 7(9):1252) [37]. Specifically, the claim indicates that ALA contributes to the maintenance of normal blood cholesterol levels. (Figure 1)
(A cause-effect relationship between the dietary intake of ALA and the reduction of plasma concentrations of TC and LDL-C has been recognized. Studies issued after the EFSA statement further suggest that ALA has anti-proliferative [38], anti-hypertensive [39,40,41], anti-atherosclerotic [42], cardioprotective effects [42,43,44,45,46], and it successfully improves the composition of the red cell membrane in children with hyperlipidemia [47], possibly reducing the risk of cardiovascular events in adulthood. In a pilot study by Del Bo’ et al [47], a randomized clinical trial (RCT), 8 week-long, dietary intervention study aimed to evaluate the impact of HSO supplementation on the lipid profile and fatty acid composition of red blood cells (RBCs) in children and adolescents with primary hyperlipidemia. The 36 study subjects aged 6 to 16 years were divided into 2 different groups: the control group and the HSO one, receiving 3 g of HSO with 1.4 g of linoleic acid (LA) and 0.7 g/day of ALA. Both groups received specific dietary guidelines. Blood samples were kept for each subject, before and after administration with HSO, in order to analyze the lipid profile, composition of RBCs, and omega-3 index After an eight-week supplementation with HSO, there were significant reductions in the RBC content of total saturated and monounsaturated FAs (−5.02 ± 7.94% and − 2.12 ± 2.23%, respectively). Conversely, the levels of total n-3 and n-6 PUFAs increased (+1.57 ± 1.96% and + 5.39 ± 7.18%, respectively), as did the Omega-3 index (+1.18 ± 1.42%). This study confirms that diet represents the first line of therapy for primary hyperlipidemia.
In the clinical study by Yue et al of 2021 [48], the effect of ALA intake on blood lipid profiles was examined, especially on triglycerides (TG), TC, HDL-C, LDL-C, VLDL-C, and the ratio of TC to HDL-C. 1305 subjects were enrolled in the ALA group and 1325 in the control one were identified. Compared with the control group, dietary intake of ALA significantly reduced the concentrations of TG (WMD −0.101 mmol/L; 95% CI: −0.158 to −0.044 mmol/L; P = 0.001), TC (WMD −0.140 mmol/L; 95% CI: −0.224 to −0.056 mmol/L; P = 0.001), LDL-C (WMD −0.131 mmol/L; 95% CI: −0.191 to −0.071 mmol/L; P < 0.001), VLDL-C (WMD −0.121 mmol/L; 95% CI: −0.170 to −0.073 mmol/L; P < 0.001), TC/HDL-C ratio WMD −0.165 mmol/L; 95% CI: −0.317 to −0.013 mmol/L; P = 0.033) and LDL-C/HDL-C ratio (WMD −0.158 mmol/L; 95% CI: −0.291 to −0.025 mmol/L; P = 0.02). ALA has no effect on HDL-C (WMD 0.008 mmol/L; 95% CI: −0.018 to 0.034 mmol/L; P = 0.541). Dose-response analysis showed that 1 g/day increase in ALA was associated with reductions in TG of 0.0016 mmol/L 0.0071 mmol/L, 0.0015 and 0.0061 mmol/L reduction in TG (95% CI: −0.0029 to −0.0002 mmol/L), TC (95% CI: −0.0085 to −0.0058 mmol/L), HDL-C (95% CI: −0.0020 to −0.0011 mmol/L) and LDL-C (95% CI: −0.0073 to −0.0049 mmol/L) levels, respectively. The effects of ALA intake on TG, TC, and LDL-C concentrations were pronounced in patients with hyperlipidemia or hyperglycemia compared to healthy subjects. Dietary ALA intervention improved blood lipid profiles by reducing levels of TG, TC, LDL-C and VLDL-C. These results show that increasing ALA intake could potentially prevent the risk of CVDs.
In a meta-analysis of controlled trials conducted by Khalesi et al [49] the intake of ALA-rich sesame fractions is associated with a reduction of TG. As a result, the consumption of sesame did not significantly change the TC (-0.32 mmol/L, 95% CI: -0.75 to 0.11; p=0.14, I2 =96 %), LDL-C (-0.15 mmol/L, 95 % CI: -0.50 to 0.19; p = 0.39, I2 = 96 %) or HDL-C levels (0.01 mmol/L, 95% CI:-0.00 to 0.02; p= 0.16, I2 = 0 %). However, a significant reduction was observed in serum TG levels (-0.24 mmol/L, 95 % CI: -0.32 to -0.15; p <0.001, I2 = 84 %) after consumption of sesame. Although the consumption of sesame rich in ALA seems to significantly reduce blood TG levels, there is not enough evidence to support its hypocholesterolemic effects.
Importantly, the positive effects of ALA can also be extended to non-lipid outcomes as well. Experiments show that ALA stimulates nitric oxide (NO) production [50,51], and increases action mediated by prostanoids, with effects on platelet aggregation and coagulation. Therefore, it reduces the probability of thrombotic events, regulates the heart rhythm and decreases the onset of arrhythmias and inflammation, with a direct action on prostaglandins [39,52]. Recent evidence agrees that the intake of PUFAs has cardioprotective effect, through mild lowering blood pressure (BP). Cicero et al [39] evaluated the long-term effect of a PUFA intake on the BP of 111 subjects with hypertriglyceridemia. Subjects were treated with 2 g PUFA/day to improve lipid profile. Following 12 months of treatment, the systolic blood pressure (SBP) exhibited a mean reduction of 2.7 ± 2.5 mmHg (p = 0.001), and the diastolic blood pressure (DBP) decreased by 1.3 ± 3.3 mmHg (p < 0.001). Additionally, the basal heart rate decreased by 4.0 ± 4.4 bpm (p < 0.001). Both the reductions in SBP and DBP were significantly correlated with the baseline SBP (p < 0.001) and DBP (p < 0.001), respectively. In this retrospective study, PUFA supplementation for 1 year led to a significant reduction in SBP, DBP, pulse pressure (PP), and basal heart rate in hypertriglyceridemic patients with normal-high blood pressure.
Additionally, a series of studies aimed to understand how the intake of ALA in the diet was useful in tracing BP and in increasing the aortic thickness of the intima and media tunica in Small Gestational Age (SGA) infants [39,40]. In this study of 2015 by Skilton et al [40], 1009 participants were recruited at 6 months and were followed until age 19 years. The purpose of this study is to evaluate a possible association between dietary ALA intake, low BP and aortic intima-media thickness in children born with SGA. Blood pressure and food records were assessed at each visit. A total of 1009 participants had at least one blood pressure measure and complete birth weight and gestational age data, including 115 (11%) SGA. These children had greater systolic and PP from age 14 years onwards. In those born with SGA, SBP was 2.1 mmHg lower ([95% CI 0.8-3.3]; P=.001) and PP 1.4 mmHg lower ([95% CI 0.3-2.4]; P=.01), per exponential increase in ALA intake. It can be concluded from the study that ALA supplementation during childhood improves cardiovascular health of children with SGA.
Flaxseed and HSO contain Omega-3 fatty acids, lignans, and fiber, which together may be beneficial for patients with CVDs. Hypertension is often associated with peripheral artery disease. Rodriguez-Leyva and colleagues [41], aimed to investigate the effects of daily flaxseed intake on SBP and DBP in patients with peripheral artery disease. In this prospective, double-blinded, placebo-controlled, randomized trial, 110 patients consumed a variety of food containing 30 g of ALA or placebo daily for 6 months. Plasma levels of Omega-3 ALA increased 2- to 50-fold in the flaxseed-fed group but did not increase significantly in the placebo group. SBP was ≈ 10 mmHg lower, and DBP was ≈ 7 mmHg lower in the flaxseed group compared with placebo at 6 months. Enrolled patients with an SBP ≥ 140 mmHg at baseline achieved a significant reduction of 15 mmHg in SBP and 7 mmHg in DBP with flaxseed supplementation. These results confirmed that ALA is one of the most powerful antihypertensive agents achieved by a dietary intervention.
A very important study that examined changes in atherosclerosis markers was the MARGARIN trial [53], conducted on 110 subjects with a high risk of IHD. The experimental group received margarine (80% fat, of which 60% as PUFAs) containing either 15% or 0.3% of total fat as ALA for two years. Results showed that the intake of ALA reduced C-reactive protein, a marker of inflammation, but the present study found no effect on markers of atherosclerosis.
Cardioprotective Effect
The 2020-2025 American Dietary Guidelines showed that there is strong evidence to demonstrate that replacing Saturated Fatty Acids (SFAs) with PUFAs reduces the risk of IHD events and CVD mortality [54]. In high-risk patients, ALA prevents coronary heart disease (CHD), considered one of the major causes of death worldwide [41,42,43,45,55,56].
The aim of the study by Vedtofte et al [55] was to examine the association between ALA intake and the risk of CHD. Data from eight American and European prospective cohort studies including 148.675 women and 80.368 men were used. During 4-10 years of follow-up, 4.493 CHD events and 1.751 CHD deaths occurred. Among men, the researchers found an inverse association between ALA intake and CHD events and deaths. Each additional gram of ALA was associated with a 15% lower risk of CHD events (HR: 0.85; 95% CI: 0.72, 1.01) and a 23% lower risk of CHD deaths (HR: 0.77; 95% CI: 0.58, 1.01). The Cardiovascular Health Study [31] was designed to examine the associations of dietary ALA with the risk of mortality, CHD and stroke among older adults who participated in the study, a cohort study of 2709 adults aged ≥ 65 years. After adjustment for age, sex, race, enrollment site, education, smoking status, diabetes, Body Mass Index (BMI), alcohol consumption, treated hypertension and total energy intake, higher dietary ALA intake was found to be associated with a lower risk of total and non-cardiovascular mortality. When the highest quintile of dietary ALA was compared with the lowest quintile, the HR for total and non-cardiovascular mortality was found to be 0.73 (95% CI: 0.61, 0.88) and 0.64 (95% CI: 0.52, 0.80), respectively. In conclusion, this study suggests that dietary ALA is associated with a lower risk of total and non-cardiovascular mortality in older adults.
In a 2012 meta-analysis of observational studies by Pan et al [42], increasing dietary ALA was associated with a moderately lower risk of total CVD (RR: 0.90; 95% CI: 0.81, 0.99). 27 studies were analyzed, including 251.049 individuals and 15.327 CVD events. The association between ALA intake and reduced risk of CVD was significant in 13 comparisons, but 17 comparisons show similar but non-significant trends Therefore, considering observational studies, higher ALA intake is associated with a moderately lower risk of CVD.
In the study by Zelniker et al of 2021 [57], patients with acute coronary syndrome, after intake of n-3 PUFAs, were associated with a lower risk of cardiovascular death (OR: 0.82; 95% CI: 0.68, 0.98 per 1-SD increment), whereas an attenuated relation was observed after administration of ALA (OR: 0.92; 95% CI: 0.74, 1.14).
In the European Prospective Investigation into Cancer and Nutrition (EPIC) study [58] which included 22.043 subjects in Greece, there were 275 deaths after 44 months. These individuals consumed a traditional Mediterranean diet rich in ALA, there was a significant reduction in total mortality, death from CHD of 25% and 33%, respectively. In 1302 individuals with known CHD, there was a reduction in total mortality and CHD of 27% and 31%, respectively [59].
The Lyon Diet Heart Study [60] was an effective study in demonstrating the efficacy of a Mediterranean-style diet supplemented with ALA on composite measures of IHD recurrence after a first MI. Subjects in the experimental group were instructed to follow a Mediterranean diet and were given a canola oil-based margarine containing 4.8% ALA. After 46 months of this diet, these subjects have 50-70% lower risk of recurrent IHD [61]. Only ALA was significantly associated with improved prognosis (RR for the composite of cardiac death and nonfatal acute MI: 0.20; 95% CI: 0.05, 0.84) when plasma fatty acids were analyzed as crude estimates of dietary data.
Another systematic review and meta-analysis of cohort studies by Jingkai et al [56] examined an overall association between ALA intake and CHD risk, assessing dose-response relationships. 14 studies of 13 cohorts were identified and included in the meta-analysis. The pooled results showed that higher ALA intake was associated with a modestly reduced risk of combined CHD (risk ratios (RR)=0.91; 95 % CI: 0.85, 0.97) and fatal CHD (RR=0.85; 95 % CI: 0.75, 0.96). Compared with individuals with lower ALA intake, only subjects with ALA intake < 1.4 g/d showed a reduced risk of composite CHD. ALA intake was linearly associated with fatal CHD, and each 1 g/d increase in ALA intake was associated with a 12% reduction in the risk of fatal CHD (95 % CI: -0.21, -0.04).
To better understand the role of ALA, Sala-Vila et al [62] prospectively evaluated the association between dietary ALA and fatal CVD in participants of the PREvèncion with DIeta MEDiterranea (PREDIMED) study (n=7202). These results showed that dietary ALA at > 0.7% of daily energy intake was associated with a 28% reduced risk of all-cause mortality. Participants (n=7447) at high CVD risk in a treatment arm receiving 30 g/day of mixed nuts (15 g walnuts, 7.5 g hazelnuts, and 7.5 g almonds) had a reduced incidence of cardiovascular events (HR: 0.72; 95% IC: 0.54, 0.95) with 4.8 daily grams of ALA consumption compared to the control group. In the intervention group, dietary ALA increased by 0.43 g/day and plasma ALA increased by 0.30% - 0.44% in a random subsample [63]. In addition,, several studies have examined the association between ALA intake and CHD risk and evaluated a possible dose-response relationship. Results showed that higher intakes of ALA were associated with a modestly reduced risk of composite coronary disease (RR=0.91; CI 95 % 0.85, 0.97) and fatal coronary disease (RR=0.85; 95 %; CI 0.75, 0.96). Subjects who consumed ALA < 1.4 g/day had a significant risk reduction, in contrast to those who did not include ALA in their diet [64].
Regarding ALA and its association with cardiovascular risk, there is the hypothesis that ALA may influence cardiovascular risk through effects on arrhythmogenesis and lethal ventricular arrhythmia. Intravenous infusions of ALA reduced the risk of ventricular fibrillation during coronary artery ischemia in different animals, and dietary ALA is associated with a reduced risk of abnormal repolarization in men and women [65]. In addition, after intake, ALA can be converted to EPA and DHA, both of which have antiarrhythmic effects. Other plausible pathways by which ALA may exert beneficial effects on coronary and CVD risk include endothelial function, inflammation, and thrombosis. With respect to CVD, only one large trial has evaluated ALA supplementation for cardiovascular outcomes, including arrhythmias. In the AlphaOmega trial [66], ALA was associated with a significant reduction in arrhythmia-related events compared with placebo or Eicosapentaenoic acid (EPA) and Docosahexaenoic acid (DHA) in post hoc analyses in the subgroup of patients with diabetes, who are particularly prone to ventricular arrhythmias and sudden death after myocardial infarction (MI), (HR: 0.39; 95% CI: 0.17, 0.88). In addition, the results of the study by Kromhout et al [67] suggest and antiarrhythmic effect of ALA intake, but further clinical trials are needed to confirm this. Meta-analyses of observational studies have shown that increasing dietary ALA is associated with a 10% lower risk of total CVD and a 20% lower risk of fatal CHD.
2. Discussion
This narrative review describes the functional effects of ALA in preventing risk factors for cardiovascular diseases, and its direct cardioprotective effects.
Regarding the lipid-lowering preventive effects, this review shows that ALA may favorably affect the levels of LDL-C and TGs in both adult and pediatric populations [47,48, 49]. Dietary ALA intake has a significant effect on the plasma values of LDL-C, TC, and TG levels, as well as on the improvement of erythrocyte membrane composition. However, the reduction of cholesterol and triglyceride levels may also depend on the plant source of ALA used. For example, HSO allows for a significant reduction of LDL-C, TC, and RBC, while sesame seeds are effective in reducing triglyceride levels, but not other cholesterol-rich fractions.
A beneficial and protective effect against hypertension has been reported in three studies [39,40,41]. All of them confirm that daily consumption of ALA reduces SBP and DBP, possibly through the release of NO, a potent vasodilator. The results were also confirmed in subjects with borderline BP values, suggesting that ALA is an effective dietary antihypertensive compound.
With regard to cardioprotective effects, the studies and meta-analyses [41,42,43,45,55,56,57,58,59,60,61,62,63,64] reported by us, show controversial results. While some studies confirm an important association between daily ALA intake and a significant reduction in CVD risk, others indicate that there is no strong correlation. A dose-dependent dietary intake of ALA appears to be associated with a reduced risk of CVD. Some studies confirm that adherence to the Mediterranean diet, with the addition of ALA following the correct intakes, has positive and beneficial effects on significantly reducing IHD, cardiac death and nonfatal acute MI. Although some studies are significant and vouch for the effectiveness of ALA, further clinical trials are needed to confirm an between ALA intake, at different doses and CVD events. Eating more ALA, for example, by eating more hempseed or flaxseed oil, probably makes little or no difference in all-cause or cardiovascular death or coronary events, but slightly reduces CVD, coronary mortality, and heart arrhythmias. The effects of ALA on stroke are unclear, because the evidence was low quality
Three studies [65,66,67] investigated the association between ALA intake and its antiarrhythmic effect, caused, probably, by its direct action on anti-inflammatory eicosanoids. In fact, due to the action of these metabolites, the regulation of heart rhythm is also affected. The anti-inflammatory properties of essential fatty acids, including ALA, are well known. Some of these trials verified that ALA intake was associated with a significant reduction in arrythmia and subsequently MI, while others need further clinical evidence to confirm the efficacy.
ALA has the potential to provide novel and promising research perspectives, which are indirectly related to CVD prevention. A growing body of evidence [68,69,70,71,72,73,74] suggests that ALA intake may be a co-adjuvant intervention to modulate the progression of inflammatory and cancer-related conditions. The effects of n-3 PUFAs on CLSC (cancer stem-like cell) may be an important target for cancer therapy and will be an interesting challenge for future studies, In any case, the antitumor activity of omega-3 PUFAs shown through multiple mechanisms, suggests that they may have an important therapeutic role in the management of CSC (cancer stem cell). At this stage, further large observational and prospective studies are needed to confirm these effective and innovative properties of ALA and to develop RCTs.
3. Conclusions
Based on the studies and research presented herein, increasing ALA in the daily diet within the recommended n-6/n-3 ratio is safe. Thus, in addition to serving as an essential fatty acid and a precursor to more bioactive long-chain Omega-3 fatty acid derivatives, ALA has significant functional properties similar to those associated with nutraceuticals. As stated in the 2009 EFSA report, the inclusion of dietary ALA may play a role in reducing the risk of cardiovascular events (CHD and IHD) due to its ant-hypertensive, anti-atherosclerotic, and cardio-protective effects. Recently, there has been promising evidence of its potential anti-inflammatory and anti-proliferative properties, which may extend beyond cardiovascular diseases to include inflammatory and oncological conditions. However, further validation through high-quality studies is required to definitively establish these effects.
4. Patents
Author Contributions
Conceptualization, C.B. and A.M..; writing—original draft preparation, C.B.; writing—review and editing, A.M., G.P.M., M.A,. V.D. and C.A; supervision, A.M and C.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research was partially funded by a contribution from the Italian Ministry of Health (IRCCS grant).
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data sharing not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [PubMed]
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; et al. Heart disease and stroke statistics – 2023 update: a report from the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhang, J.; Shi, Y.; Grimsgaard, S.; Alraek, T.; Fønnebø, V. Chinese red yeast rice (Monascus purpureus) for primary hyperlipidemia: a meta-analysis of randomized controlled trials. Chin. Med. 2006, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Santini, A.; Novellino, E. Nutraceuticals in hypercholesterolaemia: an overview. Br. J. Pharmacol. 2016, 174, 1450–1463. [Google Scholar] [CrossRef] [PubMed]
- Ras, R.T.; Hiemstra, H.; Lin, Y.; Vermeer, M.A.; Duchateau, G.S.; Trautwein, E.A. Consumption of plant sterol-enriched foods and effects on plasma plant sterol concentrations – A meta-analysis of randomized controlled studies. Atherosclerosis 2013, 230, 336–346. [Google Scholar] [CrossRef]
- Ferguson, J.J.; Stojanovski, E.; MacDonald-Wicks, L.; Garg, M.L. Fat type in phytosterol products influence their cholesterol-lowering potential: A systematic review and meta-analysis of RCTs. Prog. Lipid Res. 2016, 64, 16–29. [Google Scholar] [CrossRef]
- Gordon, R.Y.; Cooperman, T.; Obermeyer, W.; Becker, D.J. Marked variability of monacolin levels in commercial red yeast rice products: buyer beware! Arch Intern Med 2010, 170, 1722–1727. [Google Scholar] [CrossRef]
- Li, X.-Y.; Zhao, Z.-X.; Huang, M.; Feng, R.; He, C.-Y.; Ma, C.; Luo, S.-H.; Fu, J.; Wen, B.-Y.; Ren, L.; et al. Effect of Berberine on promoting the excretion of cholesterol in high-fat diet-induced hyperlipidemic hamsters. J. Transl. Med. 2015, 13, 278. [Google Scholar] [CrossRef]
- Cho, S.-J.; Juillerat, M.A.; Lee, C.-H. Cholesterol Lowering Mechanism of Soybean Protein Hydrolysate. J. Agric. Food Chem. 2007, 55, 10599–10604. [Google Scholar] [CrossRef]
- Potter, S.M. Overview of proposed mechanisms for the hypocholesterolemic effect of soy. J. Nutr. 1995, 125, 606S–611S. [Google Scholar] [PubMed]
- Cambiagi, L.; Chakravarty, A.; Noureddine, N.; Hersberger, M. The role of Alpha-linolenic acid and its oxylipins in human cardiovascular diseases. Int J Mol Sci 2023, 24, 6110. [Google Scholar] [CrossRef] [PubMed]
- Mariamenatu, A.H.; Abdu, E.M. Overconsumption of Omega-6 Polyunsaturated Fatty Acids (PUFAs) versus Deficiency of Omega-3 PUFAs in Modern-Day Diets: The Disturbing Factor for Their “Balanced Antagonistic Metabolic Functions” in the Human Body. J. Lipids 2021, 2021, 8848161. [Google Scholar] [CrossRef] [PubMed]
- Greupner, T.; Kutzner, L.; Pagenkopf, S.; Kohrs, H.; Hanh, A.; Schebb, N.H.; Schuchardt, J.P. Effects of a low and a high dietary LA/ALA ration on long-chain PUFA concentrations in red blood cells. Food Funct 2018, 19, 4742–4754. [Google Scholar] [CrossRef] [PubMed]
- Simopoulos, A.P. The importance of the omega-6/omega-3 fatty acid ration in cardiovascular disease and other chronic diseases. Exp Biol Med 2008, 233, 674–688. [Google Scholar] [CrossRef] [PubMed]
- EFSA. Scientific Opinion on Dietary Reference Values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated fatty acids, trans fatty acids, and cholesterol. EFSA Journal 2010, 8, 1461. [Google Scholar]
- Hamilton, J.S.; Klett, E.L. Linoleic acid and the regulation of glucose homeostasis: A review of the evidence. Prostaglandins, Leukot. Essent. Fat. Acids 2021, 175, 102366. [Google Scholar] [CrossRef]
- Xu, Q.; Ma, X.; Dong, X.; Tao, Z.; Lu, L.; Zou, X. Effects of parental dietary linoleic acid on growth performance, antioxidant capacity, and lipid metabolism in domestic pigeons (Columba livia). Poult. Sci. 2020, 99, 1471–1482. [Google Scholar] [CrossRef]
- Li, X.; Yamada, H.; Morita, S.; Yamashita, Y.; Kim, Y.; Kometani, T.; Narang, N.; Furuta, T.; Kim, M. Effects of Free Linoleic Acid and Oleic Acid in Sesame Meal Extract as Pancreatic Lipase Inhibitors on Postprandial Triglyceridemia: A Randomized, Double-Blind, Placebo-Controlled, Crossover Study in Healthy Volunteers. Nutrients 2023, 15, 1748. [Google Scholar] [CrossRef]
- Ibrahim, K.S.; El-Sayed, E.M. Dietary conjugated linoleic acid and medium-chain triglycerides for obesity management. J. Biosci. 2021, 46, 12. [Google Scholar] [CrossRef]
- Marangoni, F.; Agostoni, C.; Borghi, C.; Catapano, A.L.; Cena, H.; Ghiselli, A.; La Vecchia, C.; Lercker, G.; Manzato, E.; Pirillo, A.; et al. Dietary linoleic acid and human health: Focus on cardiovascular and cardiometabolic effects. Atherosclerosis 2019, 292, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.; Mann, J.; Cummings, J.; Winter, N.; Mete, E.; Te Morenga, L. Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet 2019, 393, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Del Bo, C.; Bernardi, S.; Marino, M.; Porrini, M.; Tucci, M.; Guglielmetti, S.; Cherubini, A.; Carrieri, B.; Kirkup, B.M.; Kroon, P.A.; et al. Systematic review on polyphenol intake and health outcomes is there sufficient evidence to define a health-promoting polyphenol-rich dietary pattern? Nutrients 2019, 11, 1355. [Google Scholar] [PubMed]
- Ros, E.; Hu, F.B. Consumption of plant seeds and cardiovascular health: epidemiological and clinical trial evidence. Circulation 2013, 128, 553–565. [Google Scholar] [CrossRef] [PubMed]
- United States Department od Agriculture. USDA National Nutrient Database for Standard Reference; USDA: Washington, DC, USA, 2015. [Google Scholar]
- Institute of Medicine FaNB. Dietary reference intakes for energy, carbohydrate, fiber, fat, fatty acids, cholesterol, protein, and amino acids (macronutrients); National Academy Press: Washington, DC, USA, 2005. [Google Scholar]
- Alvares, A.Q.; Da Silva, V.A.; Góes, A.J.S.; Silva, M.S.; De Oliveira, G.G.; Bastos, I.V.G.A.; Neto, AG.D.C.; Alves, A.J. The fatty acid composition of vegetable oils and their potential use in wound care Adv Ski. Wound Care 2019, 32, 1–8. [Google Scholar] [CrossRef]
- Kim, J.; Kim, D.N.; Lee, S.H.; Yoo, S.H.; Lee, S. Correlation of fatty acid composition of vegetable oils with rheological behaviour and oil uptake. Food Chem. 2010, 118, 398–402. [Google Scholar] [CrossRef]
- Chan, R.L.; Olshan, A.F.; Savitz, D.A.; Herring, A.H.; Daniels, J.L.; Peterson, H.B.; Martin, S.L. Maternal influences on nausea and vomiting in early pregnancy. Matern. Child Heal. J. 2009, 15, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Lutomski, J.; McCarthy, F.P.; A Greene, R. Hyperemesis gravidarum: current perspectives. Int. J. Women's Heal. 2014, 6, 719–725. [Google Scholar] [CrossRef]
- Rogerson, D. Vegan diets: practical advice for athletes and exercisers. J Int Soc Sports Nutr. 2017, 14, 36. [Google Scholar] [CrossRef]
- Ellulu, M.S.; Patimah, I.; KhazáAi, H.; Rahmat, A.; Abed, Y. Obesity and inflammation: the linking mechanism and the complications. Arch. Med. Sci. 2017, 13, 851–863. [Google Scholar] [CrossRef]
- Santos, H.O.; Price, J.C.; Bueno, A.A. Beyond Fish Oil Supplementation: The Effects of Alternative Plant Sources of Omega-3 Polyunsaturated Fatty Acids upon Lipid Indexes and Cardiometabolic Biomarkers—An Overview. Nutrients 2020, 12, 3159. [Google Scholar] [CrossRef] [PubMed]
- Syren, M.-L.; Turolo, S.; Marangoni, F.; Milani, G.P.; Edefonti, A.; Montini, G.; Agostoni, C. The polyunsaturated fatty acid balance in kidney health and disease: A review. Clin. Nutr. 2018, 37, 1829–1839. [Google Scholar] [CrossRef] [PubMed]
- Marangoni, F.; Agostoni, C.; Lammardo, A.; Bonvissuto, M.; Giovannini, M.; Galli, C.; Riva, E. Polyunsaturated fatty acids in maternal plasma and in breast milk. Prostaglandins, Leukot. Essent. Fat. Acids 2002, 66, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Riva, E.; Agostoni, C. Fatty acids in pediatric nutrition. Pediatr Clin North Am 1995, 42, 861–877. [Google Scholar] [CrossRef]
- Available online: https://www.efsa.europa.eu/it/efsajournal/pub/1252.
- Yang, L.; Yuan, J.; Liu, L.; Shi, C.; Wang, L.; Tian, F.; Liu, F.; Wang, H.; Shao, C.; Zhang, Q.; et al. Alpha-linolenic acid inhibits human renal cell carcinoma cell proliferation through PPAR- γ activation and COX-2 inhibition. Oncol Lett 2016, 6, 197–202. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Derosa, G.; Di Gregori, V.; Bove, M.; Gaddi, A.V.; Borghi, C. Omega 3 Polyunsaturated Fatty Acids Supplementation and Blood Pressure Levels in Hypertriglyceridemic Patients with Untreated Normal-High Blood Pressure and With or Without Metabolic Syndrome: A Retrospective Study. Clin. Exp. Hypertens. 2010, 32, 137–144. [Google Scholar] [CrossRef]
- Skilton, M.R.; Pahkala, K.; Viikari, J.S.; Rönnemaa, T.; Simell, O.; Jula, A.; Niinikoski, H.; Celermajer, D.S.; Raitakari, O.T. The Association of Dietary Alpha-Linolenic Acid with Blood Pressure and Subclinical Atherosclerosis in People Born Small for Gestational Age: The Special Turku Coronary Risk Factor Intervention Project Study. J. Pediatr. 2015, 166, 1252–1257. [Google Scholar] [CrossRef]
- Rodriguez-Leyva, D.; Weighell, W.; Edel, A.L.; LaVallee, R.; Dibrov, E.; Pinneker, R.; Maddaford, T.G.; Ramjiawan, B.; Aliani, M.; Guzman, R.; et al. Potent Antihypertensive Action of Dietary Flaxseed in Hypertensive Patients. Hypertension 2013, 62, 1081–1089. [Google Scholar] [CrossRef]
- Pan, A.; Chen, M.; Chowdhury, R.; Wu, J.H.Y.; Sun, Q.; Campos, H.; Mozaffarian, D.; Hu, F.B. Alpha-Linolenic acid and risk of cardiovascular disease: a systematic review and meta-analysis. Am J Clin Nutr 2012, 1262–1273. [Google Scholar] [CrossRef]
- Fretts, A.M.; Mozaffarian, D.; Siscovick, D.S.; Sitlani, C.; Psaty, B.M.; Rimm, E.B.; Song, X.; McKnight, B.; Spiegelman, D.; King, I.B.; et al. Plasma phospholipid and dietary a-linolenic acid, mortality, CHD and stroke: the Cardiovascular Health Study. Br J Nutr 2014, 112, 1206–1213. [Google Scholar] [CrossRef]
- Saito, S.; Fukuhara, I.; Osaki, N.; Nakamura, H.; Katsuragi, Y. Consumption of alpha-linolenic acid-enriched diacylglycerol reduces visceral fat area in overweight and obese subjects: A randomized, double-blind controlled, parallel-group designed trial. J Oleo Sci 2016, 65, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Vedtofte, M.S.; Jakobsen, M.U.; Lauritzen, L.; Heitmann, B.L. The role of essential fatty acids in the control of coronary heart disease. Curr. Opin. Clin. Nutr. Metab. Care 2012, 15, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Rajaram, S. Health benefits of plant-derived α-linolenic acid. Am. J. Clin. Nutr. 2014, 100, 443S–448S. [Google Scholar] [CrossRef]
- Del Bo', C.; Deon, V.; Abello, F.; Massini, G.; Porrini, M.; Riso, P.; Guardamagna, O. Eight-week hempseed oil intervention improves the fatty acid composition of erythrocyte phospholipids and the omega-3 index, but does not affect the lipid profile in children and adolescents with primary hyperlipidemia. Food Res. Int. 2018, 119, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Yue, H.; Qiu, B.; Jia, M.; Liu, W.; Guo, X.-F.; Li, N.; Xu, Z.-X.; Du, F.-L.; Xu, T.; Li, D. Effects of α-linolenic acid intake on blood lipid profiles:a systematic review and meta-analysis of randomized controlled trials. Crit. Rev. Food Sci. Nutr. 2020, 61, 2894–2910. [Google Scholar] [CrossRef] [PubMed]
- Khalesi, S.; Paukste, E.; Nikbakht, E.; Khosravi-Boroujeni, H. Sesame fractions and lipid profiles: a systematic review and meta-analysis of controlled trials. Br. J. Nutr. 2016, 115, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Lowry, J.R.; Marshall, N.; Wenzel, T.J.; Murray, T.E.; Klegeris, A. The dietary fatty acids α-linolenic acid (ALA) and linoleic acid (LA) selectively inhibit microglial nitric oxide production. Mol. Cell. Neurosci. 2020, 109, 103569. [Google Scholar] [CrossRef]
- Erdinest, N.; Shohat, N.; Moallem, E.; Yahalom, C.; Mechoulam, H.; Anteby, I.; Ovadia, H.; Solomon, A. Nitric oxide secretion in human conjunctival fibroblasts is inhibited by alpha linolenic acid. J. Inflamm. 2015, 12, 59. [Google Scholar] [CrossRef] [PubMed]
- Cavina, M.; Battino, M.; Gaddi, A.V.; Savo, M.T.; Visioli, F. Supplementation with alpha-linolenic acid and inflammation: a feasibility trial. Int. J. Food Sci. Nutr. 2020, 72, 386–390. [Google Scholar] [CrossRef]
- Bemelmans, W.J.; Lenfrandt, J.D.; Feskens, E.J.; Vam Healst, P.L.; Broer, J.; Meyboom-de Jong, B.; May, J.F.; Tervaert, J.W.; Smith, A.J. Increased alpha-linolenic acid intake lowers C-reactive protein, but has no effects on markers of atherosclerosis. Eur J Clin Nutr 2004, 58, 1083–1089. [Google Scholar] [CrossRef]
- USDA and US Department of Health and Human Services (DHHS). Dietary Guidelines for Americans, 2020-2025. 9th ed. Washington (CD):USDA and US DHHS; 2020.
- Vedtofte, M.S.; Jakobsen, M.U.; Lauritzen, L.; O'Reilly, E.J.; Virtamo, J.; Knekt, P.; Colditz, G.; Hallmans, G.; Buring, J.; Steffen, L.M.; et al. Association between the intake of α-linolenic acid and the risk of CHD. Br. J. Nutr. 2014, 112, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Hou, R.; Xi, Y.; Kowalski, A.; Wang, T.; Yu, Z.; Hu, Y.; Chandrasekar, E.K.; Sun, H.; Ali, M.K. The association and dose–response relationship between dietary intake of α-linolenic acid and risk of CHD: a systematic review and meta-analysis of cohort studies. Br. J. Nutr. 2018, 119, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Zelniker, T.A.; Morrow, D.A.; Scirica, B.M.; Furtado, J.D.; Guo, J.; Mozaffarian, D.; Sabatine, M.S.; O’donoghue, M.L. Plasma Omega-3 Fatty Acids and the Risk of Cardiovascular Events in Patients After an Acute Coronary Syndrome in MERLIN-TIMI 36. J. Am. Hear. Assoc. 2021, 10, e017401. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Bamia, C.; Trichopoulos, D. Mediterranean Diet and Survival Among Patients With Coronary Heart Disease in Greece. Arch. Intern. Med. 2005, 165, 929–935. [Google Scholar] [CrossRef]
- de Lorgeril, M.; Renaud, S.; Salen, P.; Monjaud, I.; Mamelle, N.; Martin, J.; Guidollet, J.; Touboul, P.; Delaye, J. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994, 343, 1454–1459. [Google Scholar] [CrossRef]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Delaye, J.; Mamelle, N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction: final report of the Lyon Diet Heart Study. Circulation 1999, 99, 779–785. [Google Scholar] [CrossRef]
- Sala-Vila, A.; Guasch-Ferrè, M.; Hu, F.B.; Sanchez-Tainta, A.; Bullò, M.; Serra-Mir, M.; Lopez-Sabater, C.; Sorlì, J.V.; Aròs, F.; Fiol, M.; et al. Dietary alpha-linolenic acid, marine omega-3 fatty acids, and mortality in a population with high fish consumption: findings from the PREvenciòn con DIeta MEDiterranea (PREDIMED) study. J Am Heart Assoc 2016, 5, e002543. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Wei, J.; Hou, R.; Xi, Y.; Kowalski, A.; Wang, T.; Yu, Z.; Hu, Y.; Chandrasekar, E.K.; Sun, H.; Ali, M.K. The association and dose–response relationship between dietary intake of α-linolenic acid and risk of CHD: a systematic review and meta-analysis of cohort studies. Br. J. Nutr. 2018, 119, 83–89. [Google Scholar] [CrossRef]
- Djoussè, L.; Rautaharju, P.M.; Hopkins, P.N.; Whitsel, E.A.; Arnett, D.K.; Eckfeldt, J.H.; Province, M.A.; Ellison, R.C. ; and Investigators of the NHLBI Family Heart Study. Dietary linolenic acid and adjusted QT and JT intervals in the National Heart, Lung, and Blood Institute Family Heart Study. J Am Coll Cardiol 2005, 45, 1716–1722. [Google Scholar] [PubMed]
- Geleijnse, J.M.; Giltay, E.J.; Schouten, E.G.; de Goede, J.; Griep, L.M.O.; Teitsma-Jansen, A.M.; Katan, M.B.; Kromhout, D. Effect of low doses of n-3 fatty acids on cardiovascular diseases in 4,837 post-myocardial infarction patients: Design and baseline characteristics of the Alpha Omega Trial. Am. Hear. J. 2010, 159, 539–546. [Google Scholar] [CrossRef] [PubMed]
- Kromhout, D.; Geleijnse, J.M.; de Goede, J.; Griep, L.M.O.; Mulder, B.J.; de Boer, M.-J.; Deckers, J.W.; Boersma, E.; Zock, P.L.; Giltay, E.J. n-3 Fatty Acids, Ventricular Arrhythmia–Related Events, and Fatal Myocardial Infarction in Postmyocardial Infarction Patients With Diabetes. Diabetes Care 2011, 34, 2515–2520. [Google Scholar] [CrossRef] [PubMed]
- Daien, C.; Czernichow, S.; Letarouilly, J.-G.; Nguyen, Y.; Sanchez, P.; Sigaux, J.; Beauvais, C.; Desouches, S.; Le Puillandre, R.; Rigalleau, V.; et al. Dietary recommendations of the French Society for Rheumatology for patients with chronic inflammatory rheumatic diseases. Jt. Bone Spine 2021, 89, 105319. [Google Scholar] [CrossRef]
- Bernasconi, A.A.; Wiest, M.M.; Lavie, C.J.; et al. Effect of omega-3 dosage on cardiovascular outcomes: An updated meta-analysis and meta-regression of interventional trials. Mayo Clin Proc 2021, 96, 304–313. [Google Scholar] [CrossRef]
- Harris, W.S.; Bulchandani, D. Why do Omega-3 fatty acids lower serum triglycerides? Curr Opin Lipidol 2006, 17, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-B.; Nam, Y.A.; Kim, H.S.; Hayes, A.W.; Lee, B.-M. α-Linolenic acid: Nutraceutical, pharmacological and toxicological evaluation. Food Chem. Toxicol. 2014, 70, 163–178. [Google Scholar] [CrossRef]
- Stark, A.H.; Crawford, M.A.; Reifen, R. Update on alpha-linolenic acid. Nutr. Rev. 2008, 66, 326–332. [Google Scholar] [CrossRef]
- Liput, K.P.; Lepczyński, A.; Ogłuszka, M.; Nawrocka, A.; Poławska, E.; Grzesiak, A.; Ślaska, B.; Pareek, C.S.; Czarnik, U.; Pierzchała, M. Effects of Dietary n–3 and n–6 Polyunsaturated Fatty Acids in Inflammation and Cancerogenesis. Int. J. Mol. Sci. 2021, 22, 6965. [Google Scholar] [CrossRef]
- D’Angelo, S.; Motti, M.L.; Meccariello, R. Omega-3 and Omega-3 polyunsaturated fatty acids, obesity and cancer. Nutrients 2020, 12, 2751. [Google Scholar] [CrossRef]
Figure 1.
Drugs and nutraceuticals for treating heart failure and lipid risk markers.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



