
Submitted:
07 August 2023
Posted:
07 August 2023
You are already at the latest version
Abstract
High prevalence of allergic disorders in Indian pediatric patients demands early diagnosis of allergens so that appropriate allergen avoidance methods, pharmacotherapy or immunotherapy can be provided in time to avoid the worsening of symptoms due to triggers. In this context, identification of the most prevalent aeroallergens in a given area is critical for diagnosis and treatment of various allergic reactions especially in case of rhino-conjunctivitis and asthma. The specific diagnosis of IgE mediated allergy is usually based on the correlation between the clinical history and signs and symptoms endorsed by the diagnostic tests. Skin prick tests are the gold standard however has some limitation. In view of this, the aim of this study was to assess the significance of ImmunoCAP assay for assessing serum specific IgE levels, available in India, against skin prick test by standardized allergens, for the diagnosis of allergic sensitization. A single-center observational study was conducted at tertiary care corporate hospitals in North India from 2017-2020. Patients with self-reported allergic symptoms or whose symptoms were suspected for allergies were tested for the type of sensitization using skin prick test (SPT) after their consents followed by ImmunoCAP based quantification of serum specific IgE levels. A total of 256 (95.9%) pediatric patients were analyzed in the study and were analysed. The patients were most commonly (30% patients) sensitized to D. farinae (173 [67.6%]), D. pteronyssinus (174 [68.0%]), Acarus siro (93 [36.3%]), Lepidoglyphus destructor (96 [37.5%]), Plantago lanceolata (Engl.). The ROC curve of Bermuda grass shows that the AUC of serum-specific IgE is larger than that of SPT (1.000 / 0.881). The receiver operating characteristic (ROC) analysis of serum-specific IgE reference method resulted in the largest AUC of all the allergens taken into consideration (0.711 / 1.000) compared to those of SPT (0.589 / 1.000). These results revealed that serum-specific IgE is more reliable method over prick test for accessing the sensitivity of patient for various allergens. This study may be helpful in performing early diagnosis of allergies as well as in taking appropriate preventive measures for managing life threatening allergic reactions
Keywords:
Pediatric Allergy. Specific IgE
; Skin prick test
; allergens
Introduction
Allergy is not a disease itself, but a mechanism leading to disease. An allergic disorder is a medical condition that involves hypersensitivity reactions where the immune system is activated due to the presence of harmless allergens commonly found in the environment [Mallol J et al 2013]. Plasma cells produced normal to copious titer of Immunoglobulin E (IgE) in response to the antigen present [Oettgen 2016] are drive Type 1st/2nd hypersensitivity reactions. Allergies can be seen in almost every organ and often start in the first three months of life. Skin and mucous membranes barriers are the most common organs which are involved in the hypersensitivity reactions in the body. In clinical practice, allergies are manifested in various different conditions such as anaphylaxis, urticaria, angioedema, rhino-conjunctivitis, asthma, serum sickness, vasculitis, hypersensitive pneumonitis, atopic dermatitis, contact dermatitis, granulomatous reactions, food or drug induced hypersensitivity reactions etc. [Ring J 2014]. Symptoms including headache, common cold, and sinus problems are commonly observed among allergic patients while symptoms like constipation, indigestion, diarrhea, and bloating are less prevalent [Joseph et al 2016].
The specific diagnosis of IgE mediated allergy is usually based on the correlation between the clinical history, signs & symptoms endorsed by the diagnostic tests. Skin prick tests are the gold standard for demonstrating an IgE mediated mechanisms which are associated with the allergic symptoms but its efficacy totally depends on the use of standardized skin prick test solutions. In our country, there is lack of availability of standardized allergens. In this context, we explored various standardized allergens and assessed serum specific IgE levels of those allergens by using globally approved ImmunoCAP method. Pediatric patients reporting to outpatient department pediatric / allergy clinic of tertiary care corporate hospital from North India were included in this observational study. The main aim of this study was to compare the efficacy of the ImmunoCAP method the skin prick test and assessed serum specific IgE levels against various allergens, for the diagnosis of allergic sensitization. This study potentially indicated that an allergen specific serum IgE level is more reliable marker over conventional prick test for allergic manifestation in pediatric allergies. This study can help in early diagnosis of allergic disorders which is paramount for taking appropriate preventive measures for preventing deleterious health risk.
Material and Methods
This is a single-center, observational study done at a tertiary care corporate hospital in North India from 2017 - 2020 to evaluate the efficacy of serum specific IgE levels compared to skin prick test for allergic sensitization. The eligible patients with self-reported allergic symptoms or whose symptoms were suspected for allergies were tested for the type of sensitization using skin prick test (SPT) after their consents. During SPT, a drop of commercially available allergen solution was to be introduced into the epidermis of the patients by pricking the skin with a 1mm guarded lancet at an angle of 45 degrees and observed for the appearance of wheal and redness within 15 minutes [Kumar R 2016]. Both histamine positive control and negative saline control were tested. Afterwards, the wheal diameter was to be recorded for the positive control, negative control, and allergen. The results were discussed with the patients and their guardians and appropriate treatment advice and tests were done after their consents. Few patients also got serum specific IgE levels done. Patients were then followed up in the OPD. The treatment plan for the patients was to be per the diagnosis of the allergy symptoms and was discontinued after the allergy resolved. Patients with confirmed allergy by positive SPT at the first screening visit were included. Patients with an uncertain diagnosis of allergy by the doctor or presence of any systemic disease which would interfere with evaluation were excluded from the study. Informed consent was taken from the patients prior to enrollment in the study. Fifty AllergoSPT Prick test solution (including powdered gluten) were used for testing allergy which were available in standard concentrations as: Grass pollens – 50000 BU/ml; Weed pollens – 50000 BU/ml; Mite solution – 50000 BU/ml ; Mould solutions – 10000 BU/ml; Cat dander – 50000 BU/ml; Cow dander – 10000 BU/ml; Orange – 1000 PNU/ml; Banana – 500 PNU/ml, Aniseed – 25000 PNU/ml; Spinach – 1000 PNU/ml; Asparagus – 2500 PNU/ml; Rest all food items – 5000 PNU/ml; Histamine (positive control) – 1.7 mg/ml; and Physiological saline which served as negative control. Immunocap method (Thermo Fisher Scientific/Phadia, Uppsala, Sweden) was used to quantify Serum-specific IgE. Sample size was estimated based on the number of subjects visiting the Allergy and Pediatric clinic in the outpatient department of Fortis hospital, Mohali, Punjab.
Statistical Analysis
The population size for the entire study period was 765; Response rate- 50% Confidence level- 95% Margin of error- 5%. Sample size estimation was done via Raosoft, Inc., at a 95% confidence interval with 5% margin of error by taking response rate of 50%. The study analysis was comprised of 256 subjects who actively took part in the study.
Results
A total of 267 patients were enrolled for this study annually. Of them, 256 (95.9%) patients completed the study and were analysed. Eleven patients (4.1%) withdrew from the study as they could be followed up (Table 1) during study.
Sensitization to Allergens
By wheal diameter ≥3 mm, the patients were most commonly (≥30% patients) sensitized to D. farinae (173 [67.6%]), D. pteronyssinus (174 [68.0%]), Acarus siro (93 [36.3%]), Lepidoglyphus destructor (96 [37.5%), Plantago lanceolata (Engl. Plantain; 81 [31.6%]), and Artemisia vulgaris (Mugwort; 81 [31.6%]; (Table 2).
Serum-specific IgE Analysis
As per the serum-specific IgE test, the patients were most commonly (>10% patients) sensitized to D. farinae (36 [14.1%]) and D. pteronyssinus (32 [12.5%]). Most of the patients had serum-specific IgE values >20 IU/mL (32 [12.5%]; (Table 3). However, the proportion of patients with sensitivity towards allergens was much higher in the case of SPT analysis (Table 4).
Comparison of Serum-specific IgE Test with Skin Prick Test in the Diagnosis of Allergy
Compititive analysis revealed that the sensitivities for mites and mould were excellent (55% to 88%). In contrast, the sensitivities for the pollen (grasses) were poorer (13% to 35%), however, their specificities were excellent (75% to 92%). For mites, the specificities ranged from 35% to 45% only. The PPV was more than 65% for all recorded allergens and NPV was highest for Alternaria alternata (mould) and recorded more than 53% for other allergens (Table 5). There were significant correlations between the SPT and serum-specific IgE result in the reported allergens. A good correlation (r=0.51 to 0.75) were shown for Alternaria alternata and Holcus lanatus while a fair correlation (r=0.26 to 0.50) were shown for D. farinae, D. pteronyssinus, and Bermuda grass (Table 6).
Discussion
Identification of the most prevalent aeroallergens in each area has a very important role in diagnosis and treatment of allergic symptoms especially rhino-conjunctivitis and asthma. The skin prick test is the recommended investigation for identifying the offending allergen. In our study, we used skin prick allergen solutions with international standardization and all the skin reactions with wheal diameter of 3mm or more were taken as positive. In our study, by wheal diameter ≥3 mm, the most common allergen was D. farinae (173 [67.6%]), D. pteronyssinus (174 [68.0%]) mites, Alternaria alternata mould (70 [27.3%]), Plantago lanceolata (Engl. Plantain; 81 [31.6%]) and Artemisia vulgaris weed pollens (Mugwort; 81 [31.6%], Cyanodon dactylon grass pollen (74 [28.9%]) and, corn (68 [26.6%]). A few patients were observed for specific IgE analysis. Among these, most of the patients had levels between 2-20 kU/L.The ROC analysis of serum-specific IgE reference method resulted in the largest AUC of all the allergens taken into consideration (0.711 – 1.000) compared to those of SPT (0.589 – 1.000). Therefore, serum-specific IgE reference method stands at top in terms of sensitivity and specificity (allergy prediction).The high prevalence of allergic disorders in Indian pediatric patients reinforces the need for early diagnosis so that appropriate allergen avoidance methods, pharmacotherapy or immunotherapy can be provided in time to avoid the worsening of symptoms due to triggers. The only limitation of this study was that the Serum specific IgE levels could not be tested in all patients due to financial constraints. Also, the effect of pharmacotherapy or immunotherapy was incomplete for the patients which could have provided complete data (from diagnosis till treatment) to tackle an allergic disorder. We used SPT and serum-specific IgE as reference methods in our study. SPT was taken as Gold standard. To investigate the rationale of the two reference tests used by detecting the optimal diagnostic concentration, we carried out receiver operating characteristic (ROC) analysis against the allergens taken into consideration. This analysis was performed to confirm whether the positive SPT results are valid for the diagnosis of IgE-mediated allergies. Area under the ROC curve is directly proportional to the accuracy of the diagnostic tests taken into account. The diagnostic test is said to be more accurate when there is more area under the ROC curve represented by the test [Wagner et al 2019]15. The ROC curve given below showed that both the tests ie, SPT and serum-specific IgE could be used as reference tests for diagnostic purposes.
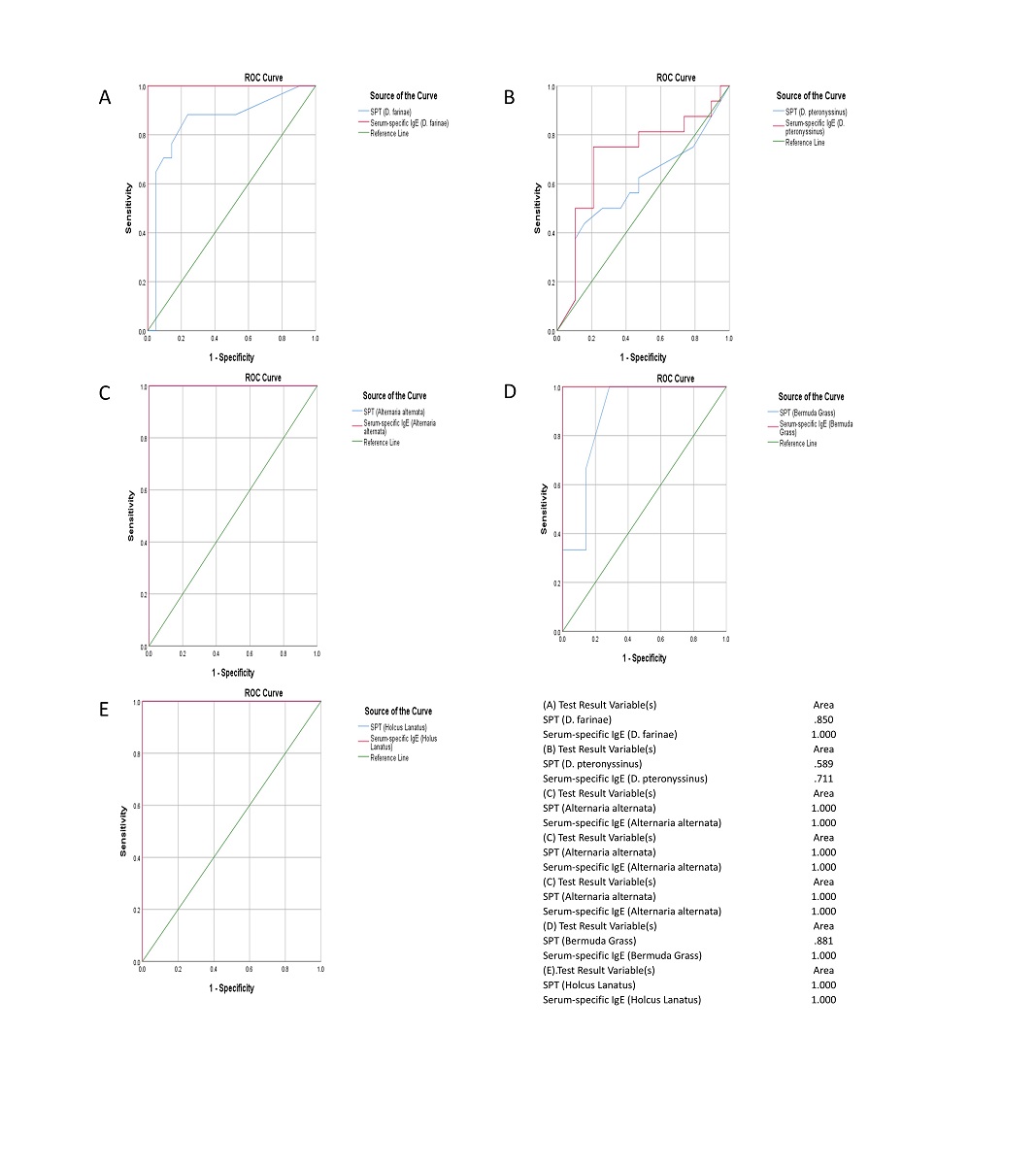
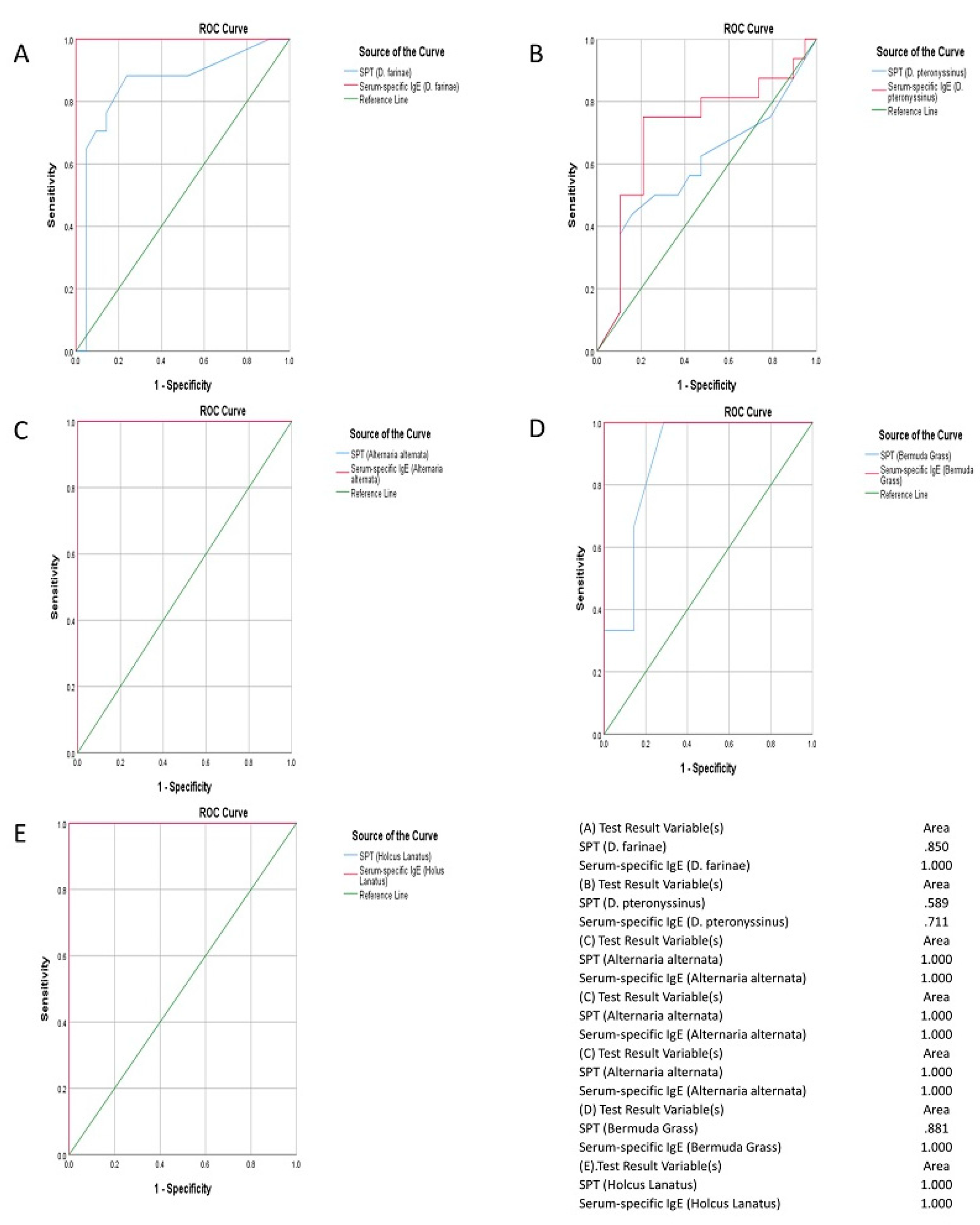
Figure 1.
(A) D. farinae (Mite) The results of ROC curve of D. farinae (Mite) depicts that AUC of serum-specific IgE is larger than that of SPT (1.000 vs. 0.850). (B) D. pteronyssinus (Mite) The results of ROC curve of D. pteronyssinus (Mite) depicts that AUC of serum-specific IgE is larger than that of SPT (1.000 vs. 0.589). (C) Alternaria alternata (Mould) The results of ROC curve of Alternaria alternata (Mould) illustrates that AUC of both the reference methods used are similar in proportion (1.000 vs. 1.000). (D) Bermuda Grass (Pollen [grasses]) The results of ROC curve of bermuda grass shows that AUC of serum-specific IgE is larger than that of SPT (1.000 vs. 0.881). (E) Holcus lanatus (Pollen [grasses]) The results of ROC curve of Holcus lanatus (grass pollen) illustrates that AUC of both the reference methods used are similar in proportion (1.000 vs. 1.000).
Figure 1.
(A) D. farinae (Mite) The results of ROC curve of D. farinae (Mite) depicts that AUC of serum-specific IgE is larger than that of SPT (1.000 vs. 0.850). (B) D. pteronyssinus (Mite) The results of ROC curve of D. pteronyssinus (Mite) depicts that AUC of serum-specific IgE is larger than that of SPT (1.000 vs. 0.589). (C) Alternaria alternata (Mould) The results of ROC curve of Alternaria alternata (Mould) illustrates that AUC of both the reference methods used are similar in proportion (1.000 vs. 1.000). (D) Bermuda Grass (Pollen [grasses]) The results of ROC curve of bermuda grass shows that AUC of serum-specific IgE is larger than that of SPT (1.000 vs. 0.881). (E) Holcus lanatus (Pollen [grasses]) The results of ROC curve of Holcus lanatus (grass pollen) illustrates that AUC of both the reference methods used are similar in proportion (1.000 vs. 1.000).
Conflict of Interest
No conflicts to disclose.
References
- Mallol, J.; Crane, J.; von Mutius, E.; et al. The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three: a global synthesis. Allergologia et immunopathologia. 2013, 41, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Oettgen, H.C. Fifty years later: emerging functions of IgE antibodies in host defense, immune regulation, and allergic diseases. Journal of Allergy and Clinical Immunology. 2016, 137, 1631–1645. [Google Scholar] [CrossRef]
- Ring, J. What is Allergy. Global Atlas of Allergy 2014, 1, 2–3. [Google Scholar]
- Joseph, N.; Palagani, R.; Shradha, N.H.; et al. Prevalence, severity and risk factors of allergic disorders among people in south India. African health sciences 2016, 16, 201–209. [Google Scholar] [CrossRef]
- Kang, S.Y.; Song, W.J.; Cho, S.H.; Chang, Y.S. Time trends of the prevalence of allergic diseases in Korea: a systematic literature review. Asia Pacific Allergy. 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Dara, P.K.; Kumari, P.; Meena, H.; Sharma, B.S. Prevalence of various oculo-respiratory allergic conditions and their comorbid association: A cross-sectional observational study in children (6–18 years) from Jaipur. Indian Journal of Allergy, Asthma and Immunology. 2018, 32, 15. [Google Scholar] [CrossRef]
- Jaggi, V.; Dalal, A.; Ramesh, B.R.; et al. Coexistence of allergic rhinitis and asthma in Indian patients: The CARAS survey. Lung India: Official Organ of Indian Chest Society. 2019, 36, 411. [Google Scholar] [CrossRef]
- Kumar, R. Allergy Testing. Manual of Workshop on Respiratory Allergy: Diagnosis and Management 2016, 4, 59–108. [Google Scholar]
- Nagaraju, K. Approach to an Allergic Child. Manual of Pediatric Allergy (second edition) 2021, 1, 1–7. [Google Scholar]
- Simpson, C.R.; Newton, J.; Hippisley-Cox, J.; Sheikh, A. Incidence and prevalence of multiple allergic disorders recorded in a national primary care database. J R Soc Med. 2008, 101, 558–563. [Google Scholar] [CrossRef]
- Ghaffari, J.; Khademloo, M.; Saffar, M.; Raflei, A.; Masiha, F. Hypersensitivity to house dust mite and cockroach is the most common allergy in north of Iran. Iran J Immunol 2010, 7, 234–239. [Google Scholar]
- Almogren, A. Airway allergy and skin reactivity to aeroallergens in Riyadh. Saudi Med J 2009, 3, 392–396. [Google Scholar]
- Madden, K.J.; Forrester, T.E.; Hambleton, I.R.; et al. Skin test reactivity to aeroallergens in Jamaicans: Relationship to Asthma. West Indian Med J 2006, 55, 142–147. [Google Scholar] [CrossRef]
- Kumar, R.; Sharan, N.; Kumar, M.; Bisht, I.; Gaur, S.N. Pattern of skin sensitivity to various aeroallergens in patients of bronchial asthma and/or allergic rhinitis in India. Ind J Allergy Asthma Immunol 2012, 26, 66–72. [Google Scholar]
- Wagner, N.; Rudert, M. Sensitivity and specificity of standardised allergen extracts in skin prick test for diagnoses of IgE-mediated respiratory allergies. Clin Transl Allergy 2019, 9, 8. [Google Scholar] [CrossRef]
- Boechat, J.L.; Moore, D.; Cortes, V.; et al. Prevalence, clinical features and severity of allergic rhinitis in elderly: preliminary results. World Allergy Organization Journal. BioMed Central. 2015, 8, A276. [Google Scholar] [CrossRef]
- Pawankar, R. Allergic diseases and asthma: a global public health concern and a call to action. World Allergy Organization Journal. 2014, 7, 12. [Google Scholar] [CrossRef]
- Singh, S.; Sharma, B.B.; Salvi, S.; et al. Allergic rhinitis, rhinoconjunctivitis, and eczema: prevalence and associated factors in children. The Clinical Respiratoy Journal. 2018, 12, 547–556. [Google Scholar] [CrossRef]
- Veerapaneni, V.; Jayaraj, B.S.; Lokesh, K.S.; et al. Prevalence of allergic rhinitis, atopic dermatitis and asthma among school children in Hyderabad, India. Journal of Allergy and Clinical Immunology. 2017, 139, AB205. [Google Scholar] [CrossRef]
- Yoo, B.; Park, Y.; Park, K.; Kim, H. A 9-year trend in the prevalence of allergic disease based on national health insurance data. Journal of Preventive Medicine and Public Health. 2015, 48, 301. [Google Scholar] [CrossRef]
- Bousquet, J.; Heinzerling, L.; Bachert, C.; et al. Global Allergy and Asthma European Network; Allergic Rhinitis and its impact on Asthma. Practical guide to skin prick tests in allergy to aeroallergens. Allergy. 2012, 67, 18–24. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Patients analyzed.
| Number of Patients, n (%) | |
|---|---|
| Patients enrolled in the study | 267 |
| Year 2017 | 80 (29.9) |
| Year 2018 | 106 (39.7) |
| Year 2019 | 66 (24.7) |
| Year 2020 | 15 (5.6) |
| Patients completed the study | 256 (95.9) |
| Patients analysed in the study | 256 (95.9) |
| Patients withdrawn from the study | 11 (4.1) |
| Reason for withdrawal | - |
| Lost to follow-up | 11 (4.1) |
| Investigator-executed withdrawal | 0 |
Table 2.
Number (%) of Patients Sensitized to Allergens (by Wheal Diameter ≥3 mm).
| SPT positive allergens | Number of Patients, n (%) (N=256) |
|---|---|
| Mites | - |
| D. farinae | 173 (67.6) |
| D. pteronyssinus | 174 (68.0) |
| Acarus siro | 93 (36.3) |
| Lepidoglyphus destructor | 96 (37.5) |
| Mould | - |
| Aspergillus fumigatus | 66 (25.8) |
| Alternaria alternata (Alternaria tenuis) | 70 (27.3) |
| Helminthosporium halodes | 46 (18.0) |
| Penicillum notatum | 29 (11.3) |
| Cladosporium herbarum | 54 (21.1) |
| Rhizopus nigricans | 37 (14.5) |
| Fusarium moniliforme | 31 (12.1) |
| Botrytis cinerea | 46 (18.0) |
| Pollen (Grasses) | - |
| Bermuda Grass (Cynodon dactylon) | 74 (28.9) |
| Barley (Hordeum vulgare) | 8 (3.1) |
| Orchard Grass (Dactylis glomerata) | 51 (19.9) |
| Timothy Grass (Phleum pratense) | 65 (25.4) |
| Rye grass (Lolium perenne) | 57 (22.3) |
| Kentucky Blue Grass (Poa pratensis) | 52 (20.3) |
| Rye (Secale cereale) | 51 (19.9) |
| Wheat (Triticum sativum) | 34 (13.3) |
| Zea mays (Corn) | 32 (12.5) |
| Holcus lanatus (Velvet grass) | 14 (5.5) |
| Pollen (Weeds) | - |
| Lambs Quarter (Chenopodium album) | 65 (25.4) |
| Ragweed (Ambrosia artemisiifolia) | 58 (22.7) |
| Engl. Plantain (Plantago lanceolata) | 81 (31.6) |
| Nettle (Urtica dioica) | 44 (17.2) |
| Mugwort (Artemisia vulgaris) | 81 (31.6) |
| Taraxacum vulgare (Dandelion) | 12 (4.7) |
| Pollen (Trees) | - |
| Locust Black (Robinia pseudoacacia) | 50 (19.5) |
| Mountaineous Pollen (Trees) | - |
| Alder (Alnus glutinosa) | 35 (13.7) |
| Birch (Betula alba) | 46 (18.0) |
| Poplar (Populus alba) | 50 (19.5) |
| Salix capera (Willow) | 14 (5.5) |
| Quercus robur (Oak) | 12 (4.7) |
| Cottonwood (Populas deltoids) | 1 (0.4) |
| Animal Epithelia | - |
| Cow Epithhelia | 29 (11.3) |
| Cat Epithelia | 21 (8.2) |
| Fruits | - |
| Banana | 39 (15.2) |
| Orange | 45 (17.6) |
| Food - Flours & Seeds | - |
| Corn | 68 (26.6) |
| Wheat | 51 (19.9) |
| Gluten | 27 (10.5) |
| Food - Nuts | - |
| Ground nut | 37 (14.5) |
| Walnut | 41 (16.0) |
| Hazelnut | 1 (0.4) |
| Vegetables | - |
| Spinach | 9 (3.5) |
| Asparagus | 13 (5.1) |
| Spices and Pulses | - |
| Aniseed | 7 (2.7) |
| Milk/Egg | - |
| Milk | 34 (13.3) |
| Egg | 31 (12.1) |
Table 3.
Serum-specific IgE Analysis.
| SIgE values (IU/mL) | Number of Patients, n (%) (N = 256) |
| 0.1-2 | 22 (8.6) |
| 2-20 | 23 (9.0) |
| >20 | 32 (12.5) |
Table 4.
Number (%) of Patients with Serum-specific IgE Test.
| Allergens | Number of Patients, n (%) (N=256) |
|
|---|---|---|
| SPT | Serum-specific IgE | |
| Mites | - | - |
| D. farinae | 173 (67.6) | 36 (14.1) |
| D. pteronyssinus | 174 (68.0) | 32 (12.5) |
| Mould | - | - |
| Aspergillus fumigatus | 66 (25.8) | 12 (4.7) |
| Alternaria alternata (Alternaria tenuis) | 70 (27.3) | 11 (4.3) |
| Cladosporium herbarum | 54 (21.1) | 6 (2.3) |
| Pollen (Grasses) | - | - |
| Bermuda Grass (Cynodon dactylon) | 74 (28.9) | 8 (3.1) |
| Timothy Grass (Phleum pratense) | 65 (25.4) | 5 (2.0) |
| Rye grass (Lolium perenne) | 57 (22.3) | 1 (0.4) |
| Rye (Secale cereale) | 51 (19.9) | 4 (1.6) |
| Holcus lanatus (Velvet grass) | 14 (5.5) | 6 (2.3) |
| Pollen (Weeds) | - | - |
| Lambs Quarter (Chenopodium album) | 65 (25.4) | 4 (1.6) |
| Ragweed (Ambrosia artemisiifolia) | 58 (22.7) | 2 (0.8) |
| Engl. Plantain (Plantago lanceolata) | 81 (31.6) | 7 (2.7) |
| Nettle (Urtica dioica) | 44 (17.2) | 1 (0.4) |
| Mugwort (Artemisia vulgaris) | 81 (31.6) | 10 (3.9) |
| Mountaineous Pollen (Trees) | - | - |
| Alder (Alnus glutinosa) | 35 (13.7) | 1 (0.4) |
| Birch (Betula alba) | 46 (18.0) | 1 (0.4) |
| Quercus robur (Oak) | 12 (4.7) | 2 (0.8) |
| Animal Epithelia | - | - |
| Cat Epithelia | 21 (8.2) | 1 (0.4) |
| Fruits | - | - |
| Orange | 45 (17.6) | 1 (0.4) |
| Food - Flours & Seeds | - | - |
| Corn | 68 (26.6) | 1 (0.4) |
| Wheat | 51 (19.9) | 2 (0.8) |
| Gluten | 27 (10.5) | 3 (1.2) |
| Food – Nuts | - | - |
| Hazelnut | 1 (0.4) | 1 (0.4) |
| Spices and Pulses | - | - |
| Aniseed | 7 (2.7) | 1 (0.4) |
| Milk/Egg | - | - |
| Milk | 34 (13.3) | 3 (1.2) |
Table 5.
Sensitivity and Specificity of Serum-specific IgE versus SPT. PPV = positive predictive values; NPV = negative predictive values; CI = confidence interval.
Table 5.
Sensitivity and Specificity of Serum-specific IgE versus SPT. PPV = positive predictive values; NPV = negative predictive values; CI = confidence interval.
| Type of allergen | Sensitivity (95% CI) |
Specificity (95% CI) |
PPV (%) |
NPV (%) |
|---|---|---|---|---|
| D. farinae (Mite) | 88.0% | 44.8% | 68.1% | 53.2% |
| D. pteronyssinus (Mite) | 87.6% | 35.7% | 73.7% | 56.9% |
| Alternaria alternate (Mould) | 55.0% | 18.4% | 64.8% | 96.4% |
| Bermuda Grass (Pollen [grasses]) | 34.7% | 74.6% | 81.3% | 56.3% |
| Holcus lanatus (Pollen [grasses]) | 13.2% | 91.8% | 66.6% | 72.9% |
Table 6.
Correlation between SPT and Serum-specific IgE among the Study Subjects (* pearson correlation: r = 0 – 0.25 (poor or no correlation); r = 0.26 – 0.50 (fair correlation); r = 0.51 – 0.75 (good correlation) and r = 0.71 – 1.0 (excellent correlation).
Table 6.
Correlation between SPT and Serum-specific IgE among the Study Subjects (* pearson correlation: r = 0 – 0.25 (poor or no correlation); r = 0.26 – 0.50 (fair correlation); r = 0.51 – 0.75 (good correlation) and r = 0.71 – 1.0 (excellent correlation).
| Type of allergen | p-value * | r* |
|---|---|---|
| D. farinae (Mite) | 0.001 | 0.412 |
| D. pteronyssinus (Mite) | 0.001 | 0.398 |
| Alternaria alternate (Mould) | 0.001 | 0.560 |
| Bermuda Grass (Pollen [grasses]) | 0.001 | 0.457 |
| Holcus lanatus (Pollen [grasses]) | 0.001 | 0.531 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



