
Submitted:
06 August 2023
Posted:
08 August 2023
You are already at the latest version
Abstract
Bilateral recurrent nerve damage following total thyroidectomy in thyroid surgery represents severe complications. These complications have almost low incidence thanks also by using the Nerve Intraoperative Monitoring. The aim of this observational retrospective study is to evaluate the inception mode and the recovery time for different clinical laryngeal pictures that arise from this surgery. We enrolled 25 patients with bilateral vocal folds mobility deficit between October 2017 and October 2022, diagnosed in ENT Unit of University of Campania “L. Vanvitelli”, out of a total of 1417 patients undergoing total thyroidectomy. The 25 patients (23F,2M) aged from 24 to 78 years old (average age 51.7) presented a bilateral vocal folds motility deficit (occurring in about 0.1% of cases). All patients underwent 9 months diagnostic/therapeutic process, which started approximately 30 days after thyroid surgery. There are several outcomes of these complications with functional laryngeal defects being mainly related to respiratory and phonatory activities. These clinical manifestations evolve in different ways within a context of a wide range of possibilities, from spontaneous bilateral or monolateral recovery to functional or surgical restoration. This study allowed the acquisition of useful information about prognostic indications and an adequate therapeutic process, based on the specific clinical characteristics.
Keywords:
thyroidectomy
; bilateral vocal folds paralysis
; voice therapy
; arytenoidectomy
; NIM
1. Introduction
Laryngeal complications represent one of the most alarming sequelae following total thyroidectomy, especially in oncological disease and in relapsing of gland tumors [1,2,3]. These complications include monolateral or bilateral vocal folds immobility causing respiratory, phonatory and swallowing disorders. In particular, these symptoms are related to the position of the vocal folds following total thyroidectomy, therefore, to the residual glottal gap. The various kinds of clinical pictures are based on the vocal folds position: in “respiratory form”, dyspnea is due to the vocal folds in a median/paramedian position (Figure 1 A,B); in the “phonatory form”, dysphonia is associated with dysphagia and dyspnea during the speech and is caused by the vocal folds in an intermediate position (Figure 2) [4,5]. In the case of severe dyspnea, caused by bilateral vocal folds immobility in a median position (adduction), an hospitalization in the Intensive Care Unit, with respiratory support and/or urgent tracheotomy, is required [6]. In all other cases, an observational period of 6/12 months is recommended: in fact, vocal folds immobility is often transient, and a gradual recovery of vocal fold motility is possible [7,8,9,10,11]. In these conditions, the vocal folds dysfunction is defined as Bilateral Vocal Folds paresis (BVFp). Following the observational period, when no recovery in vocal fold motility is achieved, the vocal folds disorder is defined as Bilateral Vocal Folds Paralysis (BVFP) [12,13,14,15,16]. During this period, voice therapy might be recommended [4,5,8,17,18]; it is also suggested in the case of Unilateral Vocal Fold Paralysis (UVFP) [2,13,18,19,20,21,22,23]. However, in literature, there is no agreement about the utility of voice therapy in bilateral vocal folds dysfunction, regarding guidelines, timing and rehabilitation techniques. The low incidence of bilateral laryngeal deficit and the lack of knowledge about the reinnervation pattern currently make it hard to formulate a widely accepted standard therapy [24]. The low frequency of surgical injuries is related to the application of Nerve Intraoperative Monitoring (NIM) in thyroid surgery. The NIM system is based on a precise surface electrode position on the vocal folds that represents a precondition for functional neuromonitoring. The monitoring goals are: map the nerve; monitor manipulation technique; verify nerve integrity [25,26,27].
The aim of this study was to observe the evolution of the recurrent nerve injury following total thyroidectomy and to identify potentially useful prognostic factors able to characterize the therapeutic process, in particular:
- Vocal folds position following thyroid surgery (glottal gap);
- Timing and resolution of laryngeal defects in total or partial impairment of vocal folds motility;
- The percentage of patients with BVFP who have benefited from voice therapy;
- The percentage of patients with BVFP who underwent laryngeal surgery.
2. Materials and Methods
An observational retrospective study was conducted on 25 patients with bilateral vocal folds mobility deficit diagnosed in our ENT Unit of University of Campania “L. Vanvitelli” between October 2017 and October 2022, out of a total of 1417 patients underwent total thyroidectomy treated from Thyroid Surgery Unit of University of Campania “L. Vanvitelli”. The 25 patients (23F,2M) aged from 24 to 78 years old (average age 51.7) presented a bilateral vocal folds motility deficit following total thyroidectomy, according to literature occurring in about 0.1% of cases [1]. They were included consecutively and observed approximately 30 days following thyroid surgery (T0) and were studied over the following 9 months. All patients were assessed using the same evaluation protocol which included the administration of the following tests: Modified Medical Research Council Dyspnea Scale (MMRC Dyspnea Scale), Maximum Phonation Time (MPT), G.I.R.B.A.S Scale, Voice Handicap Index (VHI) and fiberoptic laryngoscopy, at time zero (T0) with follow-ups after 3 months (T1), 6 months (T2) and 9 months (T3). All patients underwent voice therapy using the procedures described in the following paragraph. All subjects were advised with an Informed Consent Form and Research Protocol approved by the Ethics Committee of our University Surgical Department, which was carried out in accordance with the Helsinki Declaration.
Respiratory function assessment
Respiratory capacity was assessed with a questionnaire: the Modified Medical Re-search Council (MMRC) Dyspnea Scale. The questionnaire evaluates the changes in daily activities following respiratory injury. The 0-4 grading score depends on the capacity to execute basic daily activities and more complex exercises. The use of this scale is currently recommended for the diagnosis of patients with chronic obstructive pulmonary disease (COPD) by the National Institute for Health and Care Excellence in England [28] and its modified version is a key feature of the Global Initiative for Chronic Obstructive Airways Disease recommendations on assessment [29]. The scale is also used in the classification of COPD severity [29] and to evaluate the effectiveness of pulmonary rehabilitation. [31,32]
Vocal function assessment
The assessment of vocal function was conducted with acquisition of Maximum Phonation Time (MPT) on vocal /a/ using Aerophone II, an objective measurement parameter, and using the G.I.R.B.A.S. scale, with scores from 0 (normal) to 3 (severe) on perceptual voice parameters (Grade, Instability, Roughness, Breathiness, Asthenia and Strain). Furthermore, all patients completed the VHI questionnaire for the self-evaluation of voice disorder. It also considered their impact on daily activities and it is commonly used to assess the effectiveness of voice therapy in UVFP [33].
Fiberoptic laryngoscopy
Flexible fiberoptic laryngoscopy was carried out using Richard-Wolf Endolight X300 Highlight by the same laryngologist. It was crucial to identify the exact position of the vocal folds as described by Nawka et al. and by the Italian Society of Phoniatrics and Speech Therapy (Sifel) [24,34]. In these papers, vocal folds are described as: normal moving folds, less moving vocal folds, fixed in a median position, fixed in a paramedian position, fixed in an intermediate position and fixed in a lateral position.
Voice Therapy
Voice therapy was performed twice a week for a duration of 90 days, with different purposes depending on the position of the vocal folds. Each voice therapy session lasted 30 minutes and was carried out by a speech therapist with expertise in voice disorders. All patients were asked to repeat the exercises at home for a minimum of twice a day. The planned voice therapy protocol included two stages for each of the two forms of deficit. In the first stage, the approach was conducted differently depending on the two forms, avoiding undesirable compensatory strategies and incorrect vocal behaviors. In the respiratory form, the aim of rehabilitation was the awareness and control of diaphragm breathing dynamics and its coordination with speech. In the phonatory form, voice therapy was aimed at restoring glottal competence and, at the same time, at preventing undesirable compensatory behaviors. In the second stage voice rehabilitation was conducted to achieve a necessary compromise between voice and breathing and to improve the balance between the subsystem of the phonatory mechanisms.
3. Results
The results of our observations are reported as follows:
1) In consideration of vocal folds position, we have been following, by the cohort group after thyroidectomy surgery, 25 patients with vocal folds damage (T0): 17 (68%) patients presented vocal folds fixed in paramedian position (respiratory form), and 8 (32%) patients presented vocal folds fixed in intermediate position (phonatory form) (Table 1);
2) In consideration of timing and resolution of laryngeal defects in total or partial impairment of vocal folds motility, we have observed:
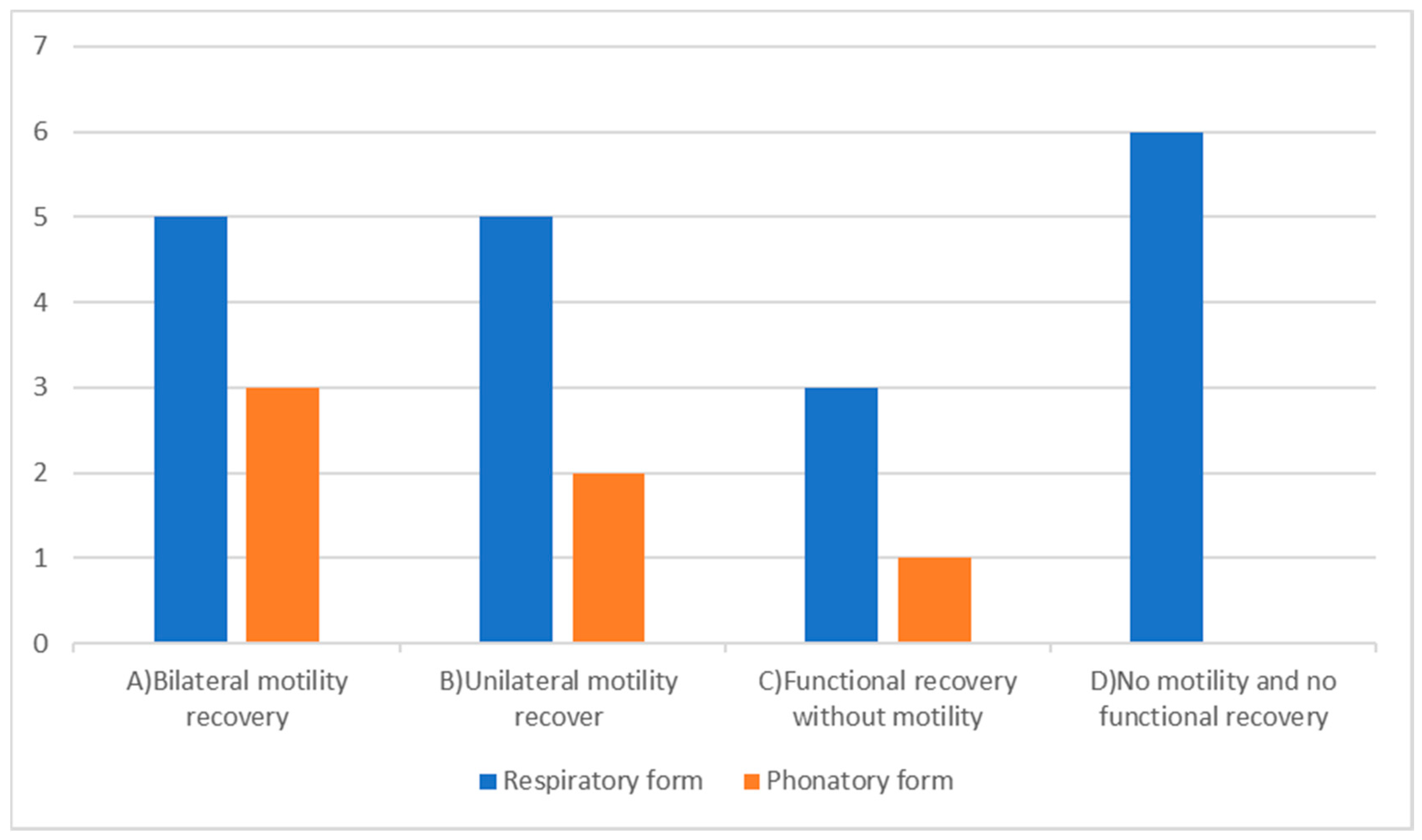
- Bilateral motility recovery occurred in 8 (32%) patients, 5 (20%) with the respiratory form and 3 (12%) with the phonatory one. The vocal fold motility restoration was achieved at a mean of 90 days (T1) after our assessment. In response to recovery patients concluded their voice therapy (Table 2-A);
- Unilateral mobility recovery occurred in 7 (28%) patients, 5 (20%) with the respiratory form and 2 (8%) with the phonatory form. The unilateral vocal fold motility restoration was obtained at a mean of 180 days (T2) after our evaluation; subjects continued voice therapy, as UVFP protocols, achieving good outcomes (Table 2-B);
3) In consideration of the percentage of patients with BVFP who have benefited from voice therapy, we have seen functional recovery without motility occurred in 4 (16%) patients, 3 (12%) with the phonatory form and 1 (4%) with the respiratory one at a mean of 90 days (T1) after our assessment (Table 2-C). After three months of continuous voice therapy, the patients, who were still having follow-up care, led a normal life with some restrictions associated with physical efforts. Functional results have been observed until T3 follow-up.
4) In consideration of the percentage of patients with BVFP who underwent laryngeal surgery, we have observed no motility and no functional recovery occurred in 6 (24%) patients, all with BVFP respiratory form. They underwent, after 270 days (T3), surgical treatment with CO2 laser arytenoidectomy at the ENT Unit of University of Campania “L. Vanvitelli” (Table 2-D).
4. Discussion
Motor bilateral injuries of the vocal folds after total thyroidectomy represent severe complications, despite their low incidence [1,2]. Different symptoms are related to these complications:
In literature, several managements of these conditions have been described [4,5,12,13,14,15,16]. However, any surgical approaches, except tracheotomy in case of acute respiratory distress, should be performed 6 – 12 months after thyroidectomy [7,8], due to the spontaneous recovery of peripheral recurrent laryngeal nerve. Furthermore, the movement disorder is transient in most cases, this is the reason why the diagnosis of vocal folds “paralysis” after thyroidectomy is considered inappropriate and it should be defined as “Bilateral Vocal Folds Paresis” (BVFp) [35]. The diversity of the various clinical pictures and the possibility of spontaneous recovery require individual therapeutic decisions. Moreover, it is necessary to consider that the symptomatology is conditioned not only by the degree of glottic insufficiency and vocal folds tension, but also by cardiopulmonary factors, age, BMI and individual tolerance of the dyspneic symptomatology [18]. In our study, we detected a higher number of respiratory forms, 17 cases (68%), approximately two-thirds of total number of patients, while the phonatory forms represented one-third of the cases, with 8 cases (32%). In the respiratory form, 17 cases, bilateral vocal folds motility recovery was observed in 5 patients (20%), monolateral mobility recovery in 5 patients (20%) and functional recovery in only one case (4%). In the remaining 6 cases (24%), about one-third of the respiratory forms, patients were underwent ENT surgery. Whereas, in phonatory form, 8 cases, bilateral vocal folds mobility recovery was observed in 3 cases (12%), monolateral recovery in 2 cases (8%) and a functional recovery in 3 cases (12%). No patient with phonatory form was underwent ENT surgery. In our experience, bilateral vocal folds motility recovery occurs in a shorter period of time if compared to monolateral recovery. Approximately one-third of patients, 8 cases (32%), showed recovery of the motility of both vocal folds within a period of 90 days (T1). Less than one-third of patients, 7 cases (28%), showed monolateral vocal fold motility recovery within a period of 180 days (T2). In these patients with monolateral recovery, the functional return after voice therapy results better in respiratory forms with a paramedian position, for more effective compense of the mobile vocal fold. In these 15 patients, the recovery of vocal folds mobility occurs within 6 months from total thyroidectomy in agreement with most of the Authors [7,8,9,10,11]. The contribution of voice therapy on the recovery of folds’ motility is not easy to prove [21]. An important data is the vocal and respiratory functional recovery in 4 (16%) patients, even though presenting BVFP (3 patients with phonatory form and 1 with respiratory one). The outcomes of their tests (MMRC Dyspnea Scale, MPT, Scale G.I.R.B.A.S. and VHI), showed a significant improvement of all parameters referred to vocal and respiratory functions and to psychological stress, despite the BVFP. Functional recovery and the role of voice therapy in our group of patients are statistically difficult to prove due to the smallness of the sample. However, our results are a starting point for subsequent investigations and evaluations of larger samples as it is poorly evaluated in literature. In particular , Pisello et al. (2005), suggested voice therapy as the only therapy to be adopted in case of phonatory form after thyroidectomy [5]. In the 2nd “Consensus Conference” of Italian Association of Endocrine Surgery Units (2009) reviewed and updated the management protocols in thyroid surgery, the authors advised voice therapy after thyroidectomy, in case of phonatory form with sufficient respiratory space [4]. Joliat et al. (2017) sustained that voice therapy is usually the first management in recurrent laryngeal nerve injury, after thyroid surgery in both cases, monolateral and bilateral damage [8]. Muller (2017) suggested supportive procedures in order to relieve symptoms in bilateral vocal folds paresis before ENT surgery; voice therapy is considered necessary in order to solve swallowing problems and to train a relaxing respiratory activity [18]. Nawka et al. have recently (2019) performed an international, retrospective, observational and multicenter study on 326 adults with permanent BVFP across various sites in Europe; among other therapeutic options, patients received voice therapy both as elective treatment and associated with ENT surgery [24]. In our experience , the functional recovery is obtained through respiratory and voice training and the achievement of new aerodynamic synchronizations, as already described in the treatment of UVFP [14,19,20,22,23]. These results indicate that the voice rehabilitation approach should be prescribed promptly after thyroid surgical healing and maintained at least for 3-6 months, especially in respiratory form with paramedian position and in phonatory form with intermediate position of vocal folds. Finally, 6 patients (24%) with BVFP respiratory form, underwent ENT surgery in particular CO2 laser arytenoidectomy (T3). For these patients who had "no mobility and no functional recovery", the failure of voice therapy induces the surgical treatment [13,15]. However, other factors may have been involved in these cases, such as:
- Severe aerodynamic incoordination due to post-polio syndrome in one case [36]. However, this patient reached a good improvement in vocal and psychological aspects, attested by results at VHI scores and by the return to work;
- Allergies and asthmatic forms [39] in two cases;
- Depression [40] in one case;
- Multiple sclerosis [41] in one case.
In conclusion, we observe various clinical pictures in the bilateral laryngeal complications following thyroid surgery characterized by different symptoms, relative to the position of the vocal folds in median, paramedian or intermediate. In accordance with literature, we observe bilateral and monolateral motility restoration within 6 months from thyroid surgery; therefore, we confirm the importance of the observation period after thyroidectomy (6-9 months) before indication to ENT surgery. The voice treatment, carried out during the period that patients must still be observed, produces a functional improvement in subjects with BVFP and reduces the percentage of patients to undergo surgery (16%). Moreover, this therapeutic process reduces the psychological stress due to the important vocal and respiratory impairment. Finally, the role of ENT surgery in patients with BVFP, in our study group, leads to support the following considerations: no patient with phonatory form needs surgery instead one-third of patients with respiratory form was subjected to surgical treatment with CO2 laser arytenoidectomy.
5. Conclusions
Following total thyroidectomy, patients may, in a minimal percentage of cases, incur in monolateral or bilateral motor injures. However the use of NIM is necessary in all patients undergoing thyroidectomy to minimize the percentage of recurrent nerve damages. Bilateral injury causes significant problems in respiratory, vocal and swal-lowing functions and, consequently, a variety of changes in an individual’s personal, social and working life. For this reason, these patients need to receive prompt support through a complete organization and treatment strategy designed to solve the various identified issues. This approach is highly effective in patients affected by post thyroidectomy BVFP, considering the diversity of the various clinical pictures, the possible comorbidities, the eventuality of the recovery of monolateral and bilateral vocal fold motility and the possibility of rehabilitation through surgery and voice therapy. All these actions reduce the possibility of medical liability, a concrete risk in post thyroidectomy.
Author Contributions
DT, LDV, SM: Partecipated substantially in conception, design; GM, GC, LD, GD: Acquisition, analysis and interpretation of data; VC, GA, AC:Drafting and editing of the manuscript. Every researcher agrees to be personally accountable for the author’s own contributions and for ensuring that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical review and approval were waived for this study due to its retrospective observatory nature.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Christou N., Mathonnet M.: Rewiew: Complications after total thyroidectomy Journal of Visceral Surgery (2013) 150, 249—256. [CrossRef]
- Chandrasekhar S.S, Randolph J.W. Seidman, M.D., Rosenfeld R. M.,Peter Angelos P., Barkmeier-Kraemer J.,Benninger M.S.,Blumin J.H., Gregory Dennis G., Hanks J., Haymart, M.R., Kloos R.T., Seals B., Schreibstein J.M.,Thomas, M.A.,Waddington C., Warren B., and Robertson P.J.: Clinical Practice Guideline: Improving Voice Outcomes after Thyroid Surgery. American Academy of Otolaryngology—Head and Neck, Surgery Foundation 2013 Otolaryngology–Head and Neck Surgery (2013)148(6S) S1– S37. [CrossRef]
- Petrosino, V., Motta, G., Tenore, G., Coletta, M., Guariglia, A., & Testa, D. (2018). The role of heavy metals and polychlorinated biphenyls (PCBs) in the oncogenesis of head and neck tumors and thyroid diseases: a pilot study. Biometals, 31(2), 285-295. [CrossRef]
- Rosato L., Miccoli P., Pinchera A., Lombardi G., Romano M., Avenia N., Bastagli A., Bellantone R., De Palma M., De Toma G., Gasparri G., Lampugnani R., Marini , Nasi P.G., Pelizzo M.R., Pezzullo L., Piccoli M, Testini M: Protocolli Gestionali Diagnostico-Terapeutico-Assistenziali in Chirurgia Tiroidea. 2ª Consensus Conference G Chir Vol. 30 - n. 3 - pp. 73-86 Marzo 2009.
- Pisello F., Geraci G., Sciumè C., Li Volsi F., Facella T., Modica G.,: Prevenzione delle complicanze in chirurgia tiroidea: la lesione del nervo laringeo ricorrente. Esperienza personale su 313 casi, Ann. Ital. Chir., LXXVI, 1, 2005.
- Ferraro F., Gambardella C., Testa D., Santini L., Marfella R., Fusco P., Lombardi CP., Polistena A., Sanguinetti A., Avenia N., Conzo G. Nasotracheal prolonged safe extubation in acute respiratory failure post-thyroidectomy: An efficacious technique to avoid tracheotomy? A retrospective analysis of a large case series. Int J Surg. 2017 May;41 Suppl 1: S48-S54. [CrossRef]
- Xuhui Chen, Ping Wan, Yabin Yu, Ming Li, Yanyan Xu, Ping Huang, and Zaoming Huang: Types and Timing of Therapy for Vocal Fold Paresis/Paralysis After Thyroidectomy: A Systematic Review and Meta-Analysis,Journal of Voice, Vol. 28, No. 6, 2014. [CrossRef]
- Joliat G.R., Guarnero V., Demartines N., Schweizer V., Matter M.:Recurrent laryngeal nerve injury after thyroid and parathyroid surgery Incidence and postoperative evolution assessment Medicine (2017) 96:17(e6674). [CrossRef]
- Hayward N.J., Grodski S., Yeung M., Johnson W.R., and Serpell J.: Recurrent laryngeal nerve injury in thyroid surgery: a review, ANZ J Surg 83 (2013) 15–21. [CrossRef]
- Higgins TS, Gupta R, Ketcham AS, Sataloff RT, Wadsworth JT, Sinacori JT. Recurrent laryngeal nerve monitoring versus identification alone on post-thyroidectomy true vocal fold palsy: a meta-analysis. Laryngoscope 2011; 121: 1009–17. [CrossRef]
- Dionigi G., Boni F., Rovera F., Rausei S., Castelnuovo P., Dionigi R. :Postoperative laryngoscopy in thyroid surgery: proper timing to detect recurrent laryngeal nerve injury, Langenbecks Arch Surg (2010) 395:327–331. [CrossRef]
- Li Y., Garrett G., Zealear D.: Current Treatment Options for Bilateral Vocal Fold Paralysis: A State-of-the-Art Review, Clinical and Experimental Otorhinolaryngology (2017) 10, 3: 203-212. [CrossRef]
- Testa D.,Guerra G., Landolfo P.G., Nunziata M.,Conzo G., Mesolella M., Motta G.: Current therapeutic prospectives in the functional rehabilitation of vocal fold paralysis after thyroidectomy: CO2 laser aritenoidectomy International Journal of Surgery (2014) 12 548-551. [CrossRef]
- Rubin A.D., Sataloff R.T.: Vocal Fold Paresis and Paralysis, Otolaryngol Clin N Am (2007) 401109–1131. [CrossRef]
- Motta S, Moscillo L, Imperiali M, Motta G.: CO2 laser treatment of bilateral vocal cord paralysis in adduction. ORL J Otorhinolaryngol Relat Spec. 2003 Nov-Dec;65(6):359-65. [CrossRef]
- Lawson G., Remacle M., Hamoir M., Jamart J: Posterior cordectomy and subtotal arytenoidectomy for the treatment of bilateral vocal fold immobility: Functional results, Journal of Voice Volume 10, Issue 3, 1996, 314-319. [CrossRef]
- Nawka T, Gugatschka M, Kölmel JC, Müller AH,Schneider-Stickler B, Yaremchuk S, Grosheva M, Hagen R, Maurer JT, Pototschnig C, Lehmann T, Volk GF, Guntinas-Lichius O: Therapy of bilateral vocal fold paralysis: real world data of an international multicenter registry, Published: April 29, 2019 https://doi.org/10.1371/journal.pone.0216096. [CrossRef]
- Muller A.H. Therapie von Rekurrensparesen, HNO June 2017, 65:621-630. [CrossRef]
- Susan Miller Voice therapy for vocal fold paralysis, Otolaryngol Clin N Am37 (2004) 105–119. [CrossRef]
- Schindler A., Bottero A., Capaccio P., Ginocchio D., Adorni F., and Ottaviani F. : Vocal Improvement After Voice Therapy in Unilateral Vocal Fold Paralysis, Journal of Voice, Vol. 22, No. 1, 2008. [CrossRef]
- Behrman A. Evidence-based treatment of paralytic dysphonia: making sense of outcomes and efficacy data. Otolaryngol Clin N Am 2004, 37 75–104. [CrossRef]
- Bartolini L., Luppi M.P., Benini M., Terenzi M. Terapia logopedica e fono chirurgia in Fonochirurgia endolaringea Quaderno monografico di aggiornamento A.O.O.I. Pacini Editore, Ospedaletto 1997, 181-197.
- Wing-Hei Viola Yu, Che-Wei Wu Speech therapy after thyroidectomy. Gland Surg 201, ;6(5):501-509. [CrossRef]
- Nawka, T., Sittel, C., Arens, C., Lang-Roth, R., Wittekindt, C., Hagen, R., Mueller, A. H., Nasr, A. I., Guntinas-Lichius, O., Fredrich, G. and Gugatschka, M. (2015), Voice and respiratory outcomes after permanent transoral surgery of bilateral vocal fold paralysis. The Laryngoscope, 125: 2749-2755. [CrossRef]
- Randolph GW. and Dralle H. with the International Intraoperative Monitoring Study Group. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope 2011; 121: S1-S16. [CrossRef]
- Dionigi G, et al. Why monitor the recurrent laryngeal nerve in thyroid surgery? J Endocrinal Invest. 2010; 33: 819-822. [CrossRef]
- Chiang FY, et al. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg. 2010 Feb; 34 (2) : 223-9. [CrossRef]
- NICE 2017: https://www.nice.org.uk/guidance/cg101/chapter/1-Guidance (23 February 2017, date last accessed).
- Gold 2011 (Global Initiative for Chronic Obstructive Airways Disease): Jones PW., Adamek L., Nadeau G. et al: Comparisons of health status scores with MRC grades in COPD: implication for the Gold 2011 classification. Eur Respir J 2013; 42:647-654. [CrossRef]
- Bestall JC., Paul EA., Garrod R., Garnham R., Jones PW., Wedzicha JA. : Usefulness of the Medical Research Council (MRC) dyspnea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax 1999; 54: 581-586. [CrossRef]
- Tonelli R., Cocconcelli E., Lanini B., Romagnoli I., Florini F., Castaniere I., Andrisani D., Cerri S., Luppi F., Fantini R., Marchioni A., Beghè B., Gigliotti F. and Clini EM.: Effectiveness of pulmonary rehabilitation in patients with interstitial lung disease of different etiology: a multicenter prospective study, Pulmonary Medicine (2017) 17:130 DOI 10.1186/s12890-017-0476-5. [CrossRef]
- Vagvolgyi A., Rozgonyi Z., Kerti M., Vadasz P., Varga J.: Effectiveness of perioperative pulmonary rehabilitation in thoracic surgery, J Thorac Dis 2017;9(6):1584-1591. [CrossRef]
- Longo L., De Vita R., Goretti P., Morelli M. : Paralisi ricorrenziali, valutazione e trattamento. L’utilizzo del VHI-test come indicatore dell’efficacia terapeutica, Prevent Res, published on line 05 Aug. 2013, P&R Public. 55. Available from: http://www.preventionandresearch.com/ . [CrossRef]
- Ricci Maccarini A., Lucchini E. : La valutazione soggettiva ed oggettiva della disfonia. Il protocollo SIFEL. Acta Phon Lat. 2002; 24(1–2):13–42.
- Salik I., Winters R. Bilateral Vocal Cord Paralysis. 2021 Jul 15. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan–. PMID: 32809687.
- Orsini M., Lopes A.J., Guimarães F.S., Freitas M.R.G., Nascimento O.J.M., de Sant’ Anna JuniorM., Filho P.M., Fiorelli S., Ferreira A.C.A.F., Pupe C., BastosV.H.V., Pessoa B., Nogueira C.B., Schmidt B.,Souza O.G., Davidovich E.R., Oliveira A.S.B., Ribeiro P. Currents issues in cardiorespiratory care of patients with post-polio syndrome. Arq Neuropsiquiatr 2016, 74(7):574-579. [CrossRef]
- Littleton S.W. Impact of obesity on respiratory function. Respirology 2012, 17, 43–49. [CrossRef]
- Ling Ching-Kai and Ling Ching-Chi Work of breathing and respiratory drive in obesity. Respirology 2012, 17, 402–411. [CrossRef]
- Heffern WA., Davis TM., Ross CJ. A case study of comorbidities: vocal cord dysfunction, asthma and panic disorder. Clin Nurs Res. 2002 Aug; 11 (3):324-40. [CrossRef]
- Sardinha A., Freire RC, Zin WA, Nardi AE Respiratory manifestation of panic disorder: causes, consequences and therapeutic implication. J Bras Pneumol. 2009 Jul; 35 (7): 698-708. [CrossRef]
- Fry DK, Pfalzer LA, Chokshi AR, Wagner MT, Jackson ES Randomizzed control trial of effects of a 10-week inspiratory muscle training program on measures of pulmonary function in person with multiple sclerosis. J Neurol Phys Ther. 2007 Dec; 31 (4):162-72. [CrossRef]
Figure 1.
A) Median position of immobile vocal folds; B) Paramedian position of immobile vocal folds.
Figure 1.
A) Median position of immobile vocal folds; B) Paramedian position of immobile vocal folds.
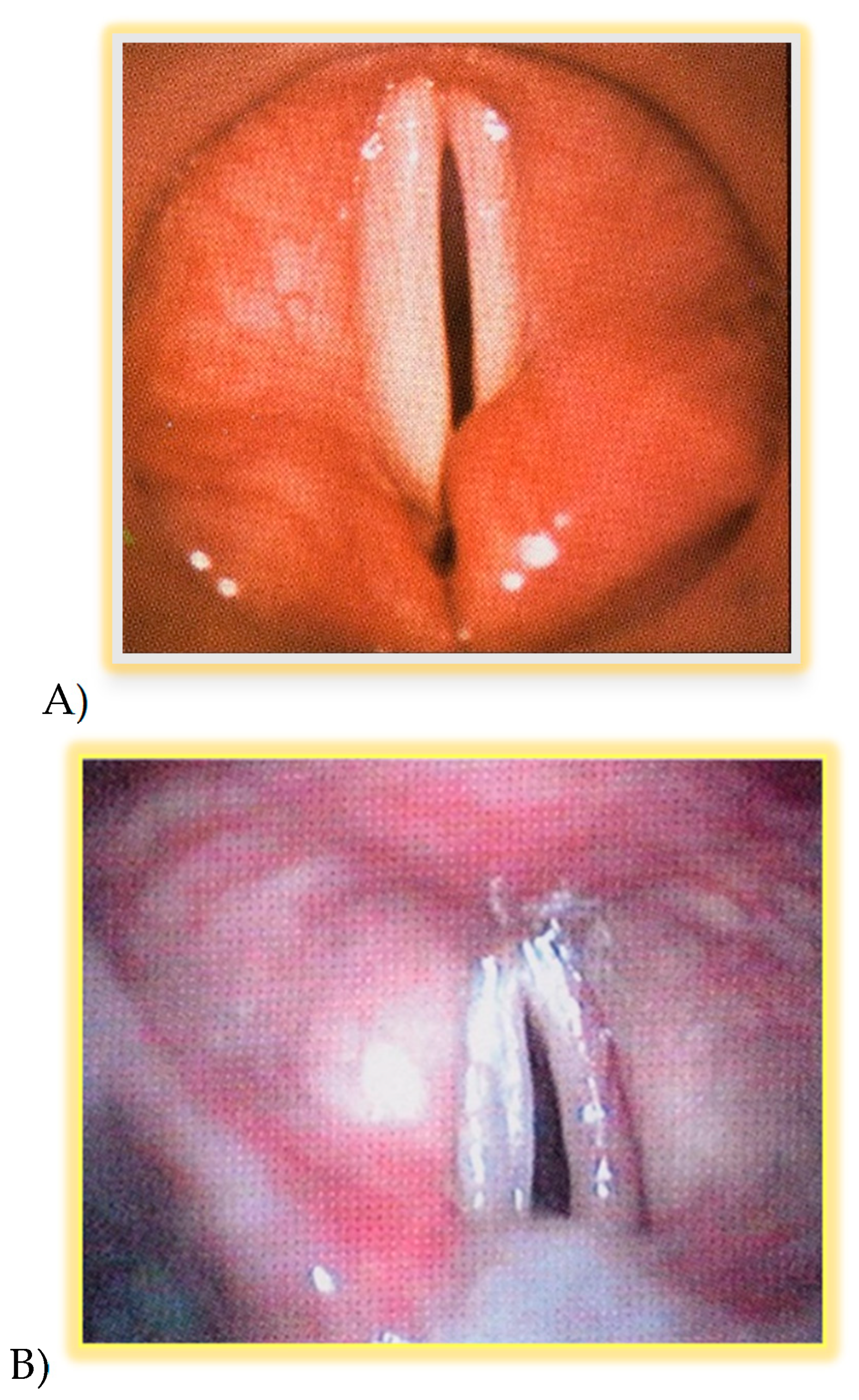
Figure 2.
Intermediate position of immobile vocal folds.
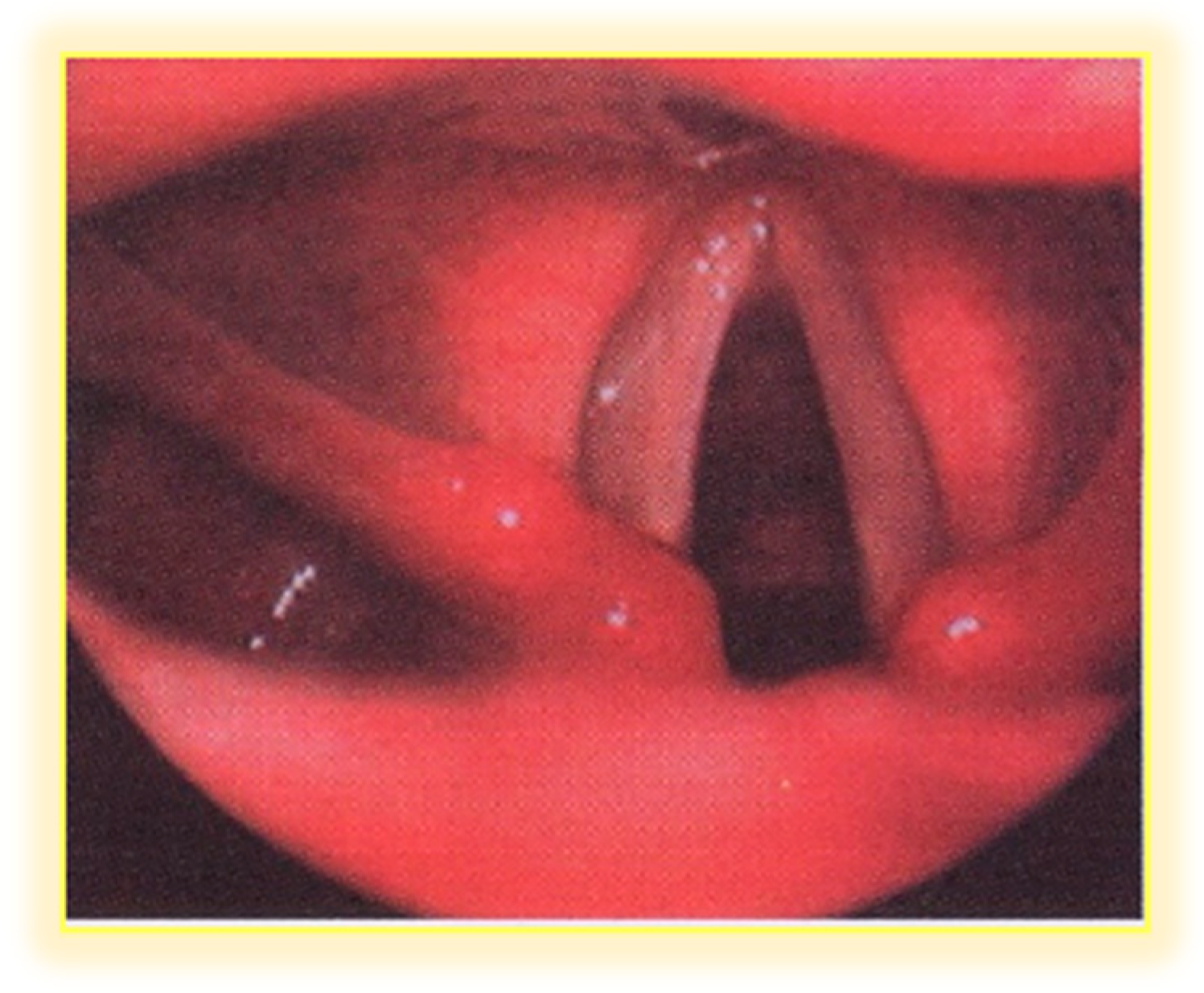

Table 1.
Vocal folds position following thyroid surgery, To. 17 (68%) patients with vocal folds fixed in paramedian position (respiratory form), and 8 (32%) with vocal folds fixed in intermediate position (phonatory form).
Table 1.
Vocal folds position following thyroid surgery, To. 17 (68%) patients with vocal folds fixed in paramedian position (respiratory form), and 8 (32%) with vocal folds fixed in intermediate position (phonatory form).
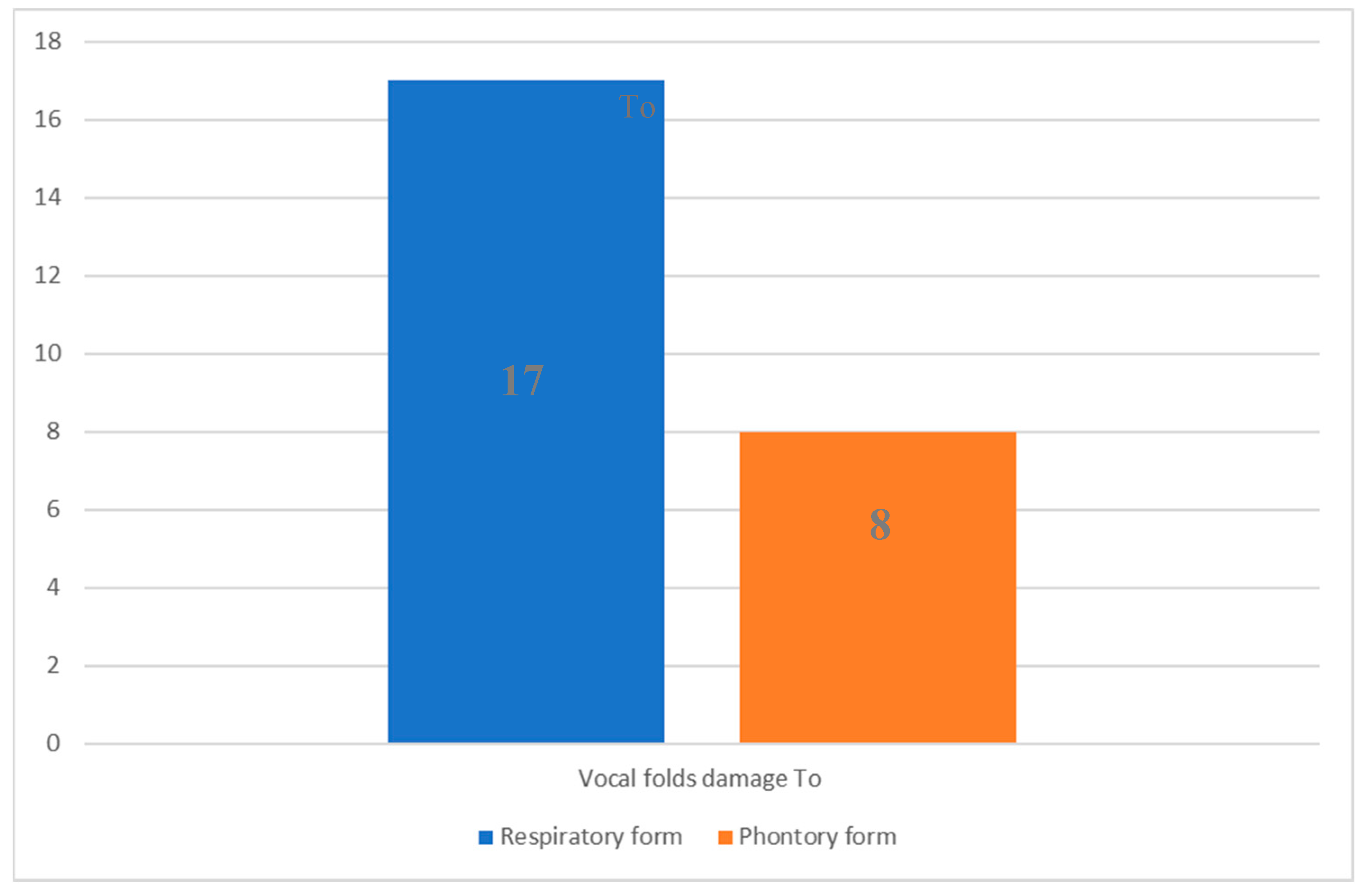
Table 2.
(A-B-C-D) Recovery of vocal folds motility in respiratory form and phonatory form. A) Bilateral motility recovery occurred in 8 (32%) patients, 5 (20%) with the respiratory form and 3 (12%) with the phonatory one, at a mean of 90 days (T1); B) Unilateral mobility recovery occurred in 7 (28%) patients, 5 (20%) with the respiratory form and 2 (8%) with the phonatory one, at a mean of 180 days (T2); C) Functional recovery without motility occurred in 4 (16%) patients, 3 (12%) with the phonatory form and 1 (4%) with the respiratory form, at a mean of 90 days (T1); D) No motility and no functional recovery occurred in 6 (24%) patients, at a mean of 270 days (T3) all with BVFP respiratory form.
Table 2.
(A-B-C-D) Recovery of vocal folds motility in respiratory form and phonatory form. A) Bilateral motility recovery occurred in 8 (32%) patients, 5 (20%) with the respiratory form and 3 (12%) with the phonatory one, at a mean of 90 days (T1); B) Unilateral mobility recovery occurred in 7 (28%) patients, 5 (20%) with the respiratory form and 2 (8%) with the phonatory one, at a mean of 180 days (T2); C) Functional recovery without motility occurred in 4 (16%) patients, 3 (12%) with the phonatory form and 1 (4%) with the respiratory form, at a mean of 90 days (T1); D) No motility and no functional recovery occurred in 6 (24%) patients, at a mean of 270 days (T3) all with BVFP respiratory form.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



