
Submitted:
04 August 2023
Posted:
08 August 2023
You are already at the latest version
Abstract
Nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH) are fast becoming the most common chronic liver disease and are often preventable with healthy dietary habits and weight management. Sugar-sweetened beverage (SSB) consumption is associated with obesity and NAFLD. However, the impact of different types of SSB, including artificially sweetened beverages (ASB), is not clear after controlling for total sugar intake and total caloric intake. In this study, we examined the association between different SSB consumption and the risk of NAFLD and NASH. A total of 3,739 US adults aged ≥20 years old who had completed 24-hour dietary recall interviews and measurements, including dietary, SSB, smoking, physical activity, and liver stiffness measurement, using the National Health and Nutrition Examination Survey 2017-2020 surveys were included in this study. Chi-square tests, t-tests, and weighted logistic regression models were utilized for analyses. The prevalence of NASH was 20.5%, and NAFLD (defined without NASH) was 32.7% of .S.U.S. adults. We observed a higher prevalence of NASH/NAFLD in men, Mexican-Americans, sugar intake from SSB, light-moderate alcohol use, individuals with lower physical activity levels, higher energy intake, obesity, and medical comorbidities. Heavy sugar consumption through SSB was significantly associated with NAFLD (aOR=1.60, 95% CI=1.05-2.45). In addition, intake of ASB only (compared to non-SSB category) was significantly associated with NAFLD (aOR=1.78, 95% CI=1.04-3.05), after adjusting for demographic, risk behaviors, and body mass index. Higher sugar intake from SSB and exclusive ASB intake are both associated with the risk of NAFLD.
Keywords:
Sugar-sweetened beverage (SSB)
; artificially sweetened beverages (ASB)
; nonalcoholic fatty liver disease (NAFLD)
; nonalcoholic steatohepatitis (NASH)
; NHANES
1. Introduction
The prevalence of Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH) has been increasing, with global prevalences of about 25% and 3-5%, respectively [1,2,3,4]. NAFLD is a chronic liver disorder that is associated with numerous metabolic disorders, such as obesity, insulin resistance, and dyslipidemia, and it is considered to be a leading cause of liver-related morbidity and mortality worldwide [4,5]. The strong association of NAFLD with the abovementioned metabolic risk factors has even prompted a trend to rename the condition altogether as metabolic dysfunction-associated steatotic liver disease (MASLD) [6]. NASH is a more severe subcategory of NAFLD that is characterized by inflammation, hepatocyte ballooning, and fibrosis, in addition to hepatic steatosis [7]. The difference between NASH and NAFLD is that NASH and NAFLD have different rates of progression for fibrosis. "These findings correspond to 1 stage of progression over 14.3 years for patients with NAFLD (95% CI, 9.1-50.0 y) and 7.1 years for patients with NASH (95% CI, 4.8-14.3 y)" [8]. NAFLD and NASH have become a significant public health concern. The underlying pathophysiology of NAFLD and NASH is complex and multifactorial, involving various genetic, metabolic, and environmental factors [4]. Several factors have been identified as potential risk factors for the development and progression of NAFLD and NASH. These include lifestyle factors, such as diet and physical activity, as well as genetic and environmental factors [5]. Individuals are more susceptible to NAFLD or NASH if they have obesity, type 2 diabetes, and high levels of triglycerides in the blood [1]. Certain populations, such as Hispanic or Asian race, post-menopausal women, and the elderly, are at higher risk of NAFLD and NASH [1]. In the U.S., Hispanic individuals have the highest prevalence of NAFLD (21%), but this prevalence varies widely among various subgroups of Hispanic populations [9]. Even though adults are more likely to have NAFLD or NASH, children are also at risk. Children with NAFLD and type 2 diabetes are more likely to have NASH, and this may be attributed to certain genes [1].
Obesity and metabolic syndrome are two of the most important risk factors for NAFLD and NASH [10,11]. Obesity is defined as a body mass index (BMI) of 30 or higher, while metabolic syndrome is a cluster of metabolic abnormalities, including abdominal obesity, insulin resistance, dyslipidemia, and hypertension [12]. The association between obesity and NAFLD/NASH is thought to be mediated by several mechanisms. One of the most important mechanisms is the effect of obesity on insulin resistance. Excess adipose tissue can lead to insulin resistance, which in turn can promote the development of NAFLD and NASH [10]. In addition, obesity is associated with chronic low-grade inflammation, which can also contribute to the development of NAFLD and NASH [11]. In the United States, obesity is associated with sedentary lifestyles and the Western diet. Western diet typically includes high levels of fructose, cholesterol, and assorted lipid species and can lead to metabolic syndrome [10,11]. The metabolic syndrome results in high levels of endotoxins in the intestines. Fatty acids, adipokines, and cytokines also result in excess adipose tissue. These factors act through multifactorial mechanisms that increase one’s risk for NAFLD [10,11,12]. Obesity-independent risk factors, such as polycystic ovarian syndrome or other hormonal abnormalities, can also contribute to NAFLD development [10,11,12]. Additionally, environmental factors, such as chronic psychosocial stress, and host factors, such as age, gender, and genetic-composition, are linked to metabolic syndrome and increased risk of NAFLD [10].
Physical inactivity has also been identified as a risk factor for NAFLD and NASH [5]. Individuals with NAFLD are recommended to participate in regular physical activity to increase metabolic control, decrease insulin resistance, and improve glucose tolerance [13]. Aerobic exercises can result in a change in energy balance, circulatory lipids, and insulin sensitivity to change the amount of liver fat [13]. Also, Romero-Gómez and colleagues noted that a ‘triple hit behavioral phenotype’ of sedentary Lifestyle, low physical activity, and poor diet to be linked to NAFLD [13].
Dietary factors have been identified as one of the primary modifiable risk factors for NAFLD and NASH. A diet high in calories, saturated and trans fats, and refined carbohydrates has been associated with an increased risk of NAFLD and NASH [13]. Gaining weight by as little as 7 to 11 pounds and consuming diets high in sugar or calories can predict NAFLD [13]. This is because a high intake of these foods results in increased fat accumulation in the liver, insulin resistance, and inflammation [14]. In contrast, studies show that a diet high in omega-2 polyunsaturated fatty acids can reduce insulin resistance and intrahepatic triglyceride content [13].
Several mechanisms have been proposed to explain the association between diet and NAFLD/NASH [13,14,21,23]. One of the most important mechanisms is the effect of diet on insulin resistance. A Western diet containing high quantities of refined carbohydrates and saturated fats can lead to insulin resistance, which in turn can promote the development of NAFLD and NASH [13,14]. In contrast, a diet rich in fiber and whole grains can improve insulin sensitivity and reduce the risk of NAFLD and NASH [14]. One of the major modifiable risk factors for NAFLD and NASH is the consumption of sugar-sweetened beverages (SSB) and artificially sweetened beverages (ASB), because they are a rapidly consumed source of calories without leading to satiety [16,19,24,41].
The consumption of SSB and ASB has increased significantly in the past few decades. SSB and ASB are widely consumed worldwide, with the global market for carbonated soft drinks alone estimated at $392.6 billion in 2020 [15,16]. SSB is defined as beverages that contain added caloric sweeteners, such as sucrose or high fructose corn syrup, while ASB is beverages that contain non-nutritive artificial sweeteners, such as aspartame, saccharin, or sucralose [16,17,24,41]. The excessive consumption of SSB has been linked to the development of obesity, type 2 diabetes, cardiovascular disease, and NAFLD, while the consumption of ASB has been associated with an increased risk of metabolic disorders, including NAFLD [16,17].
SSB and fructose consumption are found to be associated with an increased incidence of NAFLD, and new studies are concentrating on the possible associations between ASB intake and the risk of NAFLD or NASH [17,18,19,20,21,22]. One study found that a diet low in free sugar from drinks and food results in improved hepatic steatosis in adolescent boys [23]. In particular, excess intake of sugar and caramel coloring can increase insulin resistance and liver inflammation to raise one’s risk for NAFLD [17]. Another systematic review and meta-analysis of 7 observational studies reported that the connection between the consumption of ASB and NAFLD is still vague due to a lack of clinical studies on this subject [24]. A study also showed that ASB was associated with liver disease in mice, sucralose ingestion was shown to increase the expression of the efflux transporter P-glycoprotein (P-gp) and two cytochrome P-450 (CYP) isozymes in the intestine. The effect of sucralose on first-pass drug metabolism in humans, however, has not yet been determined [25]. However, some studies have reported conflicting results, with no significant association between ASB consumption and NAFLD or NASH [24,26,46,61].
Given the high prevalence of NAFLD and NASH and the potential role of SSB and ASB consumption in their development, it is important to further investigate this association. The aim of this manuscript is to examine the association between sugar intake from SSB and ASB and the risk of NAFLD and NASH.
2. Methods and Materials
2.1. Study population
A total of 3,739 National Health and Nutrition Examination Survey (NHANES) participants were selected from the cycle 2017-2020 dataset, which is a combined data set that includes the cycle 2017-2018 and partial 2019-2020 data due to uncompleted data collected for the NHANES 2019-2020 cycle. The survey was administered by the Centers for Disease Control and Prevention (CDC) every 2 years [27]. Eligible study subjects were selected based on the following steps. First, NHANES participants aged above 20 years old who participated in liver ultrasound transient elastography and 24-dietary recall interviews and had medical measurements, including alanine aminotransferase (ALT), and aspartate aminotransferase (AST), BMI were selected into this study. Then, we excluded individuals who were pregnant, on a special diet, had missing data on average alcoholic drinks intake per day, had more than 7 alcoholic drinks for females or more than 14 alcoholic drinks for males weekly, or ever had 4 or above alcoholic drinks every day, reported with liver condition, including liver fibrosis, liver cirrhosis, viral hepatitis, autoimmune hepatitis, and other liver disease, and had liver cancer. For data quality control, study subjects who had stiffness interquartile range (IQRe) ≥35% were further excluded from the current study [28]. This project was reviewed and approved by the National Center for Health Statistics (NCHS) Research Ethics Review Board (ERB). All participants have signed a written informed consent before conducting data collection [29].
2.2. Data on sweetened soda and ASB consumption and dietary patterns
Two days 24-hour recall interviews were conducted to obtain detailed food item and food components information. The first recall interview was conducted in-person in the Mobile Examination Center (MEC). A phone follow-up interview was conducted 3 to 10 days later. Each type of SSB, including soda, fruit drinks, sweetened tea and coffee, sport, and energy drinks, were identified according to the U.S. Department of Agriculture (USDA) Food codes. An average of sugar intake from SSB and from each type of SSB were also estimated. We used the cutoff point of sugar intake from SSB at 36 g for men and 25 g for women, according to the American Heart Association (AHA) recommendation for the amount of added sugar intake per day [30]. In order to explore the association between the type of SSB intake and risk of having NAFLD and NASH, we further classified our study subjects into non-SSB consumers, non-soda intake, ASB intake only, regular soda intake only, and multiple types of SSB consumers. Individuals who consumed soda with no-caloric artificial sweetener consumers only were defined as ASB intake only. Because a small size of soda consumers intake both ASB and regular soda, this population was combined with the regular soda intake only group. Individuals who consumed two or more types of SSB or ASB with any type of SSB were defined as multiple SSB consumers.
2.3. Assessment of NAFLD and NASH
Eligible vibration-controlled transient elastography (VCTE) participants in the cycle 2017-2020 were above 12 years old who were not pregnant, able to lie down on the exam table without an implanted electronic medical device or wearing a bandage on the side where measurements would be taken. VCTE was conducted to provide a controlled attenuation parameter (CAP), which estimates hepatic steatosis [31]. Individuals who had CAP <248 were defined as no fatty liver disease. The definition we used to classify non-alcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH) is CAP >248 and alanine aminotransferase (ALT) <25 U/L and aspartate aminotransferase (AST) <25 U/L, and CAP > 248 and ALT>25 U/L or AST>25 U/L, respectively [32]. In this study, NAFLD was defined as simple steatosis without NASH.
2.4. Covariates
Demographic questionnaires were used to collect data on age, gender, race, and the ratio of family income to poverty (PIR) by well-trained-interviewers using a Computer-Assisted Personal Interview (CAPI) system. A lifestyle pattern survey, including cigarettes and alcohol use, physical activity, and personal medical conditions, was administered using questionnaires at the MEC. Individuals who did not smoke at least 100 cigarettes in life (SMQ020) were defined as non-smokers. According to the question “Do you now smoke cigarettes? (SMQ040)”, former and current smokers were identified. In the alcohol use section, “Ever had a drink of any kind of alcohol (ALQ111)” and “How often drink alcoholic beverages in the past 12 months (ALQ121)” were used to recognize non-alcohol drinkers. The frequency of alcoholic beverage intake per week was calculated based on the “Average alcoholic drinks in a day during the past 12 months (ALQ130)” and “How often drank alcoholic beverages in the past 12 months (ALQ121)”. Women consumed ≤14 drinks and men consumed ≤21 drinks per week, and who never had >4 drinks every day (ALQ151) were defined as light to moderate alcohol drinkers [33]. The physical activity questionnaire was used to collect how many days in a week and how much time in a day is spent doing vigorous and moderate recreational activities, respectively. According to the questions (PAQ650, PAQ655, and PAQ660 for vigorous activities, and PAQ665, PAQ670, and PAQ675 for moderate activities), how much time spent doing vigorous and moderate recreational activities in a week was further estimated, respectively. Physical inactivity was defined if individuals had less than 150 minutes of moderate-intensity exercise or less than 75 minutes of vigorous-intensity exercise during leisure time per week [34]. Personal medical conditions were considered if participants were diagnosed with asthma, diabetes, fatty liver, chronic obstructive pulmonary disease (COPD), arthritis, hypertension, congestive heart failure, heart attack, weak/failing kidneys, angina, thyroid problem, or cancer/ malignancy. Data on total energy, total sugar, total fat, total caffeine, and total alcohol consumption were estimated from each food component by NHANES analysts based on two days of 24-hour recall interviews, which is available in the total nutrient intakes dataset [27]. An average consumption of total energy, total sugar, total fat, total caffeine, and total alcohol were calculated and considered as potential confounders in this study.
2.5. BMI and clinical measurements
Body measurements, including BMI, were collected by trained technicians in the MEC. According to the CDC recommendation for adults, overweight and obese were classified based on BMI ranging from 25 to 29.9 and ≥30 kg/m2, respectively [35]. VCTE measurements were conducted in the MEC using the FibroScan® model 502 V2 Touch equipped with a medium (M) or extra-large (XL) wand (probe) to obtain information on CAP and liver stiffness measurements (LSM). A detailed description of the protocol and procedure is available on NHANES website [31]. Data on ALT, AST, and serum creatinine is available in the standard biochemistry profile. All methods were measured on the Roche Cobas 6000 (c501 module) analyzer. The detailed description of laboratory methodologies and operating procedures was described in Laboratory Method Files [36]. Three parameters, including serum creatinine, age, and gender, were used to calculate estimated glomerular filtration rate (eGFR) levels [37].
SCr (standardized serum creatinine) = mg/dL
κ = 0.7 (females) or 0.9 (males)
α = -0.241 (females) or -0.302 (males)
min = indicates the minimum of SCr/κ or 1
max = indicates the maximum of SCr/κ or 1
age = years
2.6. Statistical analysis
Due to the complex sampling design, an appropriate sampling weight was selected and used in all analyses. Data management and all statistical analyses were performed using Stata v17 (StataCorp LLC, College Station, TX) under survey modules. Description results were presented using percentages under chi-square tests and means±standard errors under simple linear regression models for categorical variables and continuous variables, respectively. Multinomial logistic regression models were used to evaluate the association between the type of soda consumption and the risk of having NAFLD and NASH. Demographic information, including age, gender, race, and PIR were considered as potential confounders in model 1. Then, variables in Model 1 and lifestyle patterns, such as smoking, alcohol drinking, physical activity, and personal medical conditions, and dietary factors, such as total energy, total sugar, and total fat, were adjusted in Model 2. Model 3 includes variables in Model 1 and Model 2 and is additionally adjusted for BMI.
3. Results
Table 1 presents the sampling weights-adjusted distribution of demographic factors and NAFLD/NASH status. The prevalence of NASH was 20.5%, and NAFLD was 32.7% of .S.U.S. adults. People who are NAFLD/NASH are older than normal liver status (48.4±0.9, 53.6±1.1 vs. 43.9±0.9). The data showed a higher prevalence of NASH in men, and Mexican Americans and a higher prevalence of NAFLD in female Mexican Americans (all p’s≤0.002). NAFLD/NASH prevalence is similar across different ratios of family income to poverty levels.
The sampling weights-adjusted distribution of Lifestyle, dietary patterns, and SSB-related factors and biomedical examination among NAFLD/NASH status were demonstrated in Table 2. Alcohol use, physical activity level, intake, obesity, and medical comorbidities were significantly associated with NAFLD/NASH status (p<0.001). The lowest prevalence of light to moderate alcohol use was observed in individuals with NAFLD (80.8% in normal, 73.5% in NAFLD, and 80.9% in NASH, p=0.003). About 68.0% and 60.0% of individuals with NAFLD and NASH who were low physical activity, which was higher than the normal population (51.7%) (p<0.001). The highest prevalence of medical conditions was found in individuals with NAFLD (48.3% in normal, 68.0% in NAFLD, and 58.2% in NASH, p<0.001). Daily dietary patterns, including total energy, total sugar, total caffeine, and total alcohol intake, were associated with NAFLD/NASH status (all p’s <0.05). Individuals with NASH had higher total energy (2191±43 vs. 2002±31), higher total sugar (109±4.5 vs. 99±1.7), higher total caffeine (89.6±2.2 vs. 83.2±1.7), and higher total alcohol intake (8.8±1.2 vs. 6.3±0.4 ) per day than individual with normal liver status. A higher amount of sugar intake from SSB was associated with NAFLD/NASH status (p<0.001). Individuals with NASH and NAFLD had higher sugar intake from total SSB (40.7±2.9, 40.3±2.9 vs. 35.4±1.3). Regarding SSB intake, individuals who were NASH or NADFLD had higher SSB intake than individuals with normal liver status (78.1%; 74.1% vs. 70.1%, respectively). Although the type of SSB intake is not observed to be significantly statistically different by NASH/NAFLD status, individuals who are NASH or NAFLD had higher ASB intake than individuals with normal liver status (11.4%; 13.0% vs 7.3% respectively). Except for eGFR, all clinical examinations, including LSM, ALT, AST, and BMI were associated with NAFLD/NASH status (all p’s <0.001). Individuals with NASH had higher LSM (6.5±0.3 vs. 4.8±0.1), higher ALT (38.5±0.9 vs. 18.3±0.6), and higher AST (29.0±0.6 vs. 20.4±0.6) than individual with normal liver status. In addition, there is a higher prevalence of obese individuals with NASH and NAFLD than in those who were normal weight (64.5% and 49.6% vs 14.6%, respectively).
The multinomial logistic regression model between sugar intake from SSB NASH/NAFLD status is shown in Figure 1. Compared with non-SSB consumers, individuals who had ≥72 (male) and 50 (female) grams of sugar intake from total SSB had a significantly higher risk of having NAFLD (aOR=1.60, 95% CI=1.05-2.45), after adjusting for demographic, risk behaviors and BMI (model 3). Figure 2 illustrates the effect of the type of SSB consumption on the risk of having NAFLD/NASH based on the multinomial logistic regression. Significant higher risks of having NAFLD were found in individuals who consumed ASB only and multiple types of SSB when compared to non-SSB consumers before adjusted for BMI status (aOR=1.94, 95% CI=1.21-3.13 in ASB only and aOR=1.74, 95% CI=1.24-2.45 in multiple types of SSB consumers) (model 2). A 1.60-fold and 2.03-fold higher risk of having NASH was found in individuals who consumed non-soda SSB (95% CI=1.21-3.13) and regular soda only (95% CI=1.37-3.02) when compared to non-SSB consumers, respectively, after adjusting for demographic and risk behavioral factors (model 2). However, apart from the association of ASB drinkers with NAFLD, other aforementioned associations disappeared after adjusting for BMI. After additionally adjusting for BMI status in model 3, a higher risk of having NAFLD was found in individuals who consumed ASB only when compared to non-SSB consumers (aOR=1.78, 95% CI=1.04-3.05).
4. Discussion
To our knowledge, this is the first investigation of the NHANES cohort assessing the role of SSB and ASB in NAFLD. Our major findings are 1) the dose-dependent association of sugar intake from SSB with NAFLD and 2) the association of exclusive ASB consumption with NAFLD after adjusting for all covariates.
The association of SSB with NAFLD is consistent with a recent systematic review and meta-analysis by Chen et al. that found an increasing risk of NAFLD with rising levels of SSB consumption, up to 53% increased relative risk in those who drink ≥7 cups/week [19]. It is noteworthy that we found an increased risk of NASH with sugar-sweetened beverages (both non-soda and regular soda) when adjusting for demographic/socioeconomic characteristics and risk behavior (Model 2), which was mitigated after adjusting for BMI (Model 3). This suggests a possible interaction between the effects of SSB and weight gain that results in NASH rather than a direct effect of SSB on steatohepatitis. To be sure, Ma et al. did demonstrate a dose-dependent association between SSB intake and continuous ALT levels after controlling for covariates, including BMI, but while this finding was statistically significant, it was a small effect clinically [26].
Individuals with NASH or NAFLD has higher SSB and ASB consumption compared with the normal individual. Types of SSB include beverages with high levels of fructose [17]. Fructose is commonly found in fruits, fruit juices, and honey and is typically consumed as sucrose and high-fructose corn syrup [17]. Sucrose and high-fructose corn syrup are commonly found in SSB, and overconsumption of sugar from SSB is one of the major risk factors for NAFLD and NASH [38,39]. Additionally, artificial sweeteners in diet sodas are also being consumed at a fast rate in the United States. The overconsumption of artificial sweeteners can cause gut microbiome dysbiosis and release proinflammatory mediators, which can possibly increase one’s risk for NAFLD [40]. There are mixed results on the consumption of artificial sweetened beverages leading to NAFLD, but more studies are needed to support artificial sweeteners increasing NAFLD prevalence[40]. An article by Emamat and colleagues hypothesize that artificial sweeteners possibly raise the prevalence of NAFLD, but further research is needed to support this theory [41].
NAFLD is a condition when fat builds up as hepatocytes in the liver, elicited by disrupting de novo lipogenesis (DNL), fatty acid β-oxidation, fatty acid uptake, and very low-density lipoprotein (VLDL) synthesis and secretion mechanisms in the liver. In healthy people, hepatic lipogenesis is balanced with finely controlled lipid acquisition completed by DNL and fatty acid uptake and lipid disposal regulated by fatty acid b-oxidation and VLDL synthesis/secretion. In NAFLD patients, hepatic lipid acquisition exceeds lipid disposal, thus sustaining the accumulation of lipids in hepatocytes [42,43]. It is not surprising that our study demonstrated the association of SSB with NAFLD/NASH since the consumption of SSB increases DNL and fatty acid uptake mechanisms. Excessive consumption of SSB, which contains extra caloric intake, may lead to obesity with increased BMI. Thus, SSB is not significantly associated with NAFLD when the analysis is done by adjusting BMI. Unexpectedly, we revealed the association of ASB with NAFLD when those adjustments are considered for this analysis. This is a surprising finding since ASB consumption has no extra caloric content and should not alter hepatic lipogenesis. However, it has been previously reported that ASB might cause dysbiosis [44], which may explain our findings since the altered microbiota in glucose-treated mice has been linked to NAFLD progression [45]. On the other hand, a later study suggested that the ASB-mediated microbiome changes are different from SSB-mediated changes (glucose-treated) [46]. Thus, the altered microbiota in the ASB-consuming population may not completely explain our findings. Interestingly, this study identified the negative impacts of ASB on the T cell-mediated responses [46]. It has been suggested that high T cell numbers are correlated with NAFLD progression [47], despite controversy exists [48]. If ASB reduced T cell-mediated responses, which may be positively associated with the NAFLD progression, we should observe no or negative correlation of ASB with NAFLD. But we found ASB is significantly and positively associated with NAFLD. Given the complicated roles of T cells in NAFLD progression and unknown mechanisms between ASB and NAFLD progression, further studies will be needed to clarify how ASB consumption may cause the risk of developing NAFLD.
In the current study, the effect of sugar intake from SSB and type of SSB intake on the risk of having NAHS was explained by the BMI status. Therefore, we did not observe any significant contributions from sugar intake of SSB or type of SSB intake on the risk of having NASH when additionally adjusted for BMI status (model 3). Consistently, the highest proportion of obesity was estimated in individuals with NASH compared to the normal population and individuals with NAFLD.
The major ingredient in soda in the United States is predominantly high-fructose corn syrup, which contains 60-65% of fructose [51,52]. Fructose is known to be more lipogenic than glucose, and individuals with NAFLD have been shown to consume more fructose and have higher hepatic mRNA expression of fatty acid synthase on liver biopsy than non-NAFLD controls [53,54]. While our study was not designed to investigate the differences between fructose and non-fructose sugar intake, there were higher odds of NAFLD with regular soda compared to non-soda SSB consumption (aOR 2.03 versus 1.60) prior to adjusting for BMI. Nevertheless, the fact that both regular soda and non-soda SSB consumption did not have an association with NAFLD after adjusting for BMI is consistent with a prior interventional study showing equivalent hepatic triacylglycerol concentrations on magnetic resonance imaging (MRI) between individuals on isocaloric fructose versus glucose diets [55]. Our observation that non-soda SSB intake, like fructose-containing regular soda, similarly increases the risk of NAFLD before adjustment for BMI suggests the effect of SSB towards risk for NAFLD may be mediated by weight and potentially be an energy-mediated phenomenon rather than a specific effect of fructose versus glucose. Whether not there is any slight incremental benefit for fructose elimination from SSB towards NAFLD in this lens may become a difficult academic question to resolve. The more pragmatic observation may simply be that SSB in general contribute to NAFLD.
Our finding of an association between exclusive ASB consumption and NAFLD, even after adjustment of BMI status, is novel. It may be difficult to compare with other studies due to the heterogeneity of ingredients contained in ASB. Ma et al. conducted the largest known cross-sectional study in the United States assessing this association using the Framingham cohort of 2,634 patients, and while there was an association of ASB with NAFLD on imaging, the association was no longer statistically significant after adjusting for BMI [26]. The findings from Ma et al. suggest ASB may have a role in replacing SSB as long as it does not lead to weight gain. Two key differences between our study and Framingham exist: 1) we have different definitions of NAFLD, Ma et al. used computed tomography (C.T.) instead of VCTE, and 2) the Framingham cohort comprised mostly of middle-aged Americans whereas NHANES is representative of the U.S. population in general. More consistent with our findings was the observation by Naomi et al. in a European cohort that both SSB and ASB were associated with NAFLD prevalence and that the theoretical replacement of SSB with ASB was associated with higher NAFLD prevalence, which supports a class effect of ASB [56]. However, these results should be interpreted with caution in the context of our findings because 1) the United States tends to have higher fructose levels in SSB, 2) Naomi et al. determined NAFLD using the fatty liver index, which does not directly assess hepatic fat, but rather is based on anthropometrics and serologic markers [57,58].
In this study, results also showed that physical activity, total energy, total caffeine, and total alcohol intake were associated with NAFLD/NASH status, which were consistent with previous studies. Sedentary lifestyles can potentially contribute to the development of NAFLD, and an increase in daily physical activity is recommended to avoid future poor health outcomes, such as metabolic syndrome, type 2 diabetes, and NAFLD [13]. Total energy intake is another related risk factor for NAFLD. Energy restriction is a strong method to reduce one’s risk for NAFLD since excess calorie consumption often leads to obesity, which is a common risk factor for NAFLD and NASH [13]. Caffeine and alcohol intake are previously linked to NAFLD and NASH. A study by Yuan and colleagues found inverse relationships between coffee, caffeine, and alcohol, but power was low in the analysis [59]. Additionally, a systematic review of coffee consumption and the progression of NAFLD found that increased coffee consumption is inversely associated with the severity of hepatitis fibrosis, but further research is needed to fully understand coffee and caffeine’s role [60].
Our study has several strengths, first and foremost, it is a nationally representative sample of the United States. Additionally, we were able to assess hepatic fat objectively using CAP along with serum liver enzymes to accurately categorize NASH and NAFLD. The dietary assessments within the NHANES questionnaire are uniquely applicable to our study question, as they can obtain detailed reports of specific sweetened beverage intake measures from questionnaires and 2 days 24 hours recall surveys. On the other hand, our study is limited by its cross-sectional nature, limiting inference on causation. Additionally, while VCTE is an objective test, it is an imperfect test with the potential for sampling bias and inter-operator variation [28] , though we did exclude ineffective tests (IQRe≥35%). The prevalences of 32.7% and 20.5% for NAFLD and NASH, respectively, are higher because this study uses a CAP cutoff of 248 instead of 302, and AST and ALT cutoffs are both 25 rather than 25 for females and 35 for males. Also, this study includes those with diagnosed NAFLD who might be asked to reduce BMI or change their dietary intake and, consequently, may underestimate the impact of these associations. Lastly, due to the variation of ingredients of SSB and ASB between different jurisdictions, our study results may not be generalizable beyond the United States.
5. Conclusion
In conclusion, SSB was observed to have a dose-dependent effect on the risk of NAFLD, whereas ASB had a class effect on NAFLD. Future prospective studies that stratify the ingredients of both SSB and ASB may further increase our understanding of the active link between sweetened beverages and NAFLD.
Author Contributions
Conceptualization, Tung-Sung Tseng and Wei-Ting Lin; Data curation, Tung-Sung Tseng and Hui-Yi Lin; Formal analysis, Wei-Ting Lin; Methodology, Tung-Sung Tseng and Wei-Ting Lin; Software, Wei-Ting Lin; Writing – original draft, Tung-Sung Tseng, Wei-Ting Lin, Peng-Sheng Ting , Chiung-Kuei Huang and Gabrielle Gonzalez; Writing – review & editing, Tung-Sung Tseng, Wei-Ting Lin, Peng-Sheng Ting , Chiung-Kuei Huang, Po-Hung Chen, Gabrielle Gonzalez and Hui-Yi Lin.
Funding
No funding was received.
Institutional Review Board Statement
This NHANES project protocol and all procedures were approved by the Institutional Review Board for the National Center for Health Statistics (NCHS) Research Ethics Review Board (ERB).
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- American Liver, F. NASH Causes & Risk Factors. 2022.
- Kim, D.; Kim, W.R.; Kim, H.J.; Therneau, T.M. Association between noninvasive fibrosis markers and mortality among adults with nonalcoholic fatty liver disease in the United States. Hepatology (Baltimore, Md.) 2013, 57, 1357–1365. [Google Scholar] [CrossRef]
- The Nash Education, P. How Prevalent is NASH? 2022.
- National Institute of, D. ; Digestive; Kidney, D. Definitions & Facts of NAFLD & NASH. 2021.
- American Liver, F. Nonalcoholic Fatty Liver Disease (NAFLD). 2023.
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P. , et al. A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Hepatology, 2023; 10.1097/HEP.0000000000000520. [Google Scholar] [CrossRef]
- Papatheodoridi, M.; Cholongitas, E. Diagnosis of Non-alcoholic Fatty Liver Disease (NAFLD): Current Concepts. Current pharmaceutical design 2019, 24. [Google Scholar] [CrossRef]
- Singh, S.; Allen, A.M.; Wang, Z.; Prokop, L.J.; Murad, M.H.; Loomba, R. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association 2015, 13, 643–654.e649. [Google Scholar] [CrossRef]
- Duell, P.B.; Welty, F.K.; Miller, M.; Chait, A.; Hammond, G.; Ahmad, Z.; Cohen, D.E.; Horton, J.D.; Pressman, G.S.; Toth, P.P. Nonalcoholic Fatty Liver Disease and Cardiovascular Risk: A Scientific Statement From the American Heart Association. Arteriosclerosis, thrombosis, and vascular biology 2022, 42, e168–e185. [Google Scholar] [CrossRef]
- Dietrich, P.; Hellerbrand, C. Non-alcoholic fatty liver disease, obesity and the metabolic syndrome. Best Practice & Research Clinical Gastroenterology, 2014. [Google Scholar]
- Kim, H.; Lee, D.S.; An, T.H.; Park, H.-J.; Kim, W.K.; Bae, K.-H.; Oh, K.-J. Metabolic Spectrum of Liver Failure in Type 2 Diabetes and Obesity: From NAFLD to NASH to HCC. International Journal of Molecular Sciences 2021, 22, 4495–4495. [Google Scholar] [CrossRef]
- Organization, W.H. Obesity and overweight. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 5 May 2023).
- Romero-Gómez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. Journal of hepatology 2017, 67, 829–846. [Google Scholar] [CrossRef]
- Semmler, G.; Datz, C.; Reiberger, T.; Trauner, M. Diet and exercise in NAFLD/NASH: Beyond the obvious. Liver International 2021, 41, 2249–2268. [Google Scholar] [CrossRef]
- Grand Review, R. Carbonated Soft Drink Market Size, Share & Trends Analysis Report By Flavor (Cola, Citrus), By Distribution Channel (Hypermarkets, Supermarkets & Mass Merchandisers, Online Stores & D2C), And Segment Forecasts, 2021 - 2028. 2021.
- Meng, Y.; Li, S.; Khan, J.; Dai, Z.; Li, C.; Hu, X.; Shen, Q.; Xue, Y. Sugar- and Artificially Sweetened Beverages Consumption Linked to Type 2 Diabetes, Cardiovascular Diseases, and All-Cause Mortality: A Systematic Review and Dose-Response Meta-Analysis of Prospective Cohort Studies. Nutrients 2021, 13, 2636–2636. [Google Scholar] [CrossRef]
- Chhimwal, J.; Patial, V.; Padwad, Y. Beverages and Non-alcoholic fatty liver disease (NAFLD): Think before you drink. Clinical Nutrition 2021, 40, P2508–P2519. [Google Scholar] [CrossRef]
- Abid, A.; Taha, O.; Nseir, W.; Farah, R.; Grosovski, M.; Assy, N. Soft drink consumption is associated with fatty liver disease independent of metabolic syndrome. Journal of hepatology 2009, 918–924. [Google Scholar] [CrossRef]
- Chen, H.; Wang, J.; Li, Z.; Wai Kei Lam, C.; Xiao, Y.; Wu, Q.; Zhang, W. Consumption of Sugar-Sweetened Beverages Has a Dose-Dependent Effect on the Risk of Non-Alcoholic Fatty Liver Disease: An Updated Systematic Review and Dose-Response Meta-Analysis. International Journal of Environmental Research and Public Health 2019, 16, 2192–2192. [Google Scholar] [CrossRef]
- Lange, N.F.; Radu, P.; Dufour, J.F. Prevention of NAFLD-associated HCC: Role of Lifestyle and chemoprevention. Journal of hepatology 2021, 75, 1217–1227. [Google Scholar] [CrossRef]
- Vos, M.B.; Colvin, R.; Belt, P.; Molleston, J.P.; Murray, K.F.; Rosenthal, P. Correlation of vitamin E, uric acid, and diet composition with histologic features of pediatric NAFLD. Journal of Pediatric Gastroenterology 2012, 90–96. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Nitzan-Kaluski, D.; Halpern, Z.; Oren, R. Prevalence of primary non-alcoholic fatty liver disease in a population-based study and its association with biochemical and anthropometric measures. Liver International 2006, 856–863. [Google Scholar] [CrossRef]
- Schwimmer, J.; Ugalde-Nicalo, P.; Welsh, J. Effect of a Low Free Sugar Diet vs Usual Diet on Nonalcoholic Fatty Liver Disease in Adolescent Boys A Randomized Clinical Trial. Journal of the American Medical Association 2019, 321, 256–265. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Edmonds, P.J.; Cheungpasitporn, W. Associations of sugar- and artificially sweetened soda with nonalcoholic fatty liver disease: a systematic review and meta-analysis. International Journal of Medicine 2015, 109, 461–466. [Google Scholar] [CrossRef]
- Schiffman, S.S.; Rother, K.I. Sucralose, a synthetic organochlorine sweetener: overview of biological issues. Journal of Toxicology and Environmental Health 2013, 16, 399–451. [Google Scholar] [CrossRef]
- Ma, J.; Fox, C.; Jacques, P.; Speliotes, E.; Hoffmann, U.; Smith, C.; Saltzman, E.; McKeown, N. Sugar-sweetened beverage, diet soda, and fatty liver disease in the Framingham Heart Study cohorts. Journal of Hepatology 2015, 63, 462–469. [Google Scholar] [CrossRef]
- Centers for Disease, C.; Prevention (CDC). National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey (NHANES). Methods and Analytic Guidelines. 2023. Available online: https://www.cdc.gov/nchs/nhanes/irba98.htm (accessed on 5 Febuary 2023).
- Vuppalanchi, R.; Siddiqui, M.S.; Van Natta, M.L.; Hallinan, E.; Brandman, D.; Kowdley, K.; Neuschwander-Tetri, B.A.; Loomba, R.; Dasarathy, S.; Abdelmalek, M. , et al. Performance characteristics of vibration-controlled transient elastography for evaluation of nonalcoholic fatty liver disease. Hepatology 2018, 67, 134–144. [Google Scholar] [CrossRef]
- Centers for Disease, C.; Prevention (CDC). National Health and Nutrition Examination Survey (NHANES). NCHS Ethics Review Board (ERB) Approval. 2023. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 5 Febuary 2023).
- The American Heart Association (AHA) Added Sugars. 2018. Available online: https://www.heart.org/en/healthy-living/healthy-eating/eat-smart/sugar/added-sugars (accessed on 5 March 2023).
- Centers for Disease, C.; Prevention (CDC). Liver Ultrasound Transient Elastography. 2022. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2017-2018/P_LUX.htm (accessed on 18 Febuary 2023).
- Karlas, T.; Petroff, D.; Sasso, M.; Fan, J.a.-G.; Mi, Y.-Q.; de Ledinghen, V.; Kumar, M.; Lupsor-Platon, M.; Han, K.-H.; Cardoso, A. , et al. Individual patient data meta-analysis of controlled attenuation parameter (CAP) technology for assessing steatosis. Journal of hepatology 2017, 66, 1022–1030. [Google Scholar] [CrossRef]
- National Institute on Alcohol, A. ; Alcoholism. Alcohol's Effects on Health. 2023.
- The World Health Organization (WHO). Global Strategy on Diet, Physical Activity and Health. 2023. Available online: https://www.who.int/dietphysicalactivity/factsheet_adults/en/ (accessed on 18 Febuary 2023).
- Centers for Disease, C.; Prevention (CDC). Defining Adult Overweight and Obesity. 2018. Available online: https://www.cdc.gov/obesity/adult/defining.html. (accessed on 10 March 2023).
- Centers for Disease Control and Prevention (CDC). NHANES Survey. Standard Biochemistry Profile. Availabe online: . 2023. 2023; (accessed on 25 March 2023).
- National Kidney Foundation. CKD-EPI Creatinine Equation (2021). 2021. Available online: https://www.kidney.org/content/ckd-epi-creatinine-equation-2021 (accessed on 10 Febuary 2023).
- Avignon, A. Protecting the Liver: Should We Substitute Fruit Juices for SugarSweetened Beverages? Diabetes Care 2022, 45, 1032–1034. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.; Abdelmalek, M.; Sullivan, S.; Nadeau, K.; Green, M.; Roncal, C.; Nakagawa, T.; Kuwabara, M.; Sato, Y.; Kang, D.-H. , et al. Fructose and sugar: A major mediator of non-alcoholic fatty liver disease. Journal of hepatology 2018, 68, 1063–1075. [Google Scholar] [CrossRef]
- Park, W.Y.; Yiannakou, I.; Petersen, J.M.; Hoffmann, U.; Ma, J.; Long, M.T. Sugar-Sweetened Beverage, Diet Soda, and Nonalcoholic Fatty Liver Disease Over 6 Years: The Framingham Heart Study. Clinical Gastroenterology and Hepatology 2022, 20, 2524–2532. [Google Scholar] [CrossRef] [PubMed]
- Emamat, H.; Ghalandari, H.; Tangestani, H.; Abdollahi, A.; Hekmatdoost, A. Artificial sweeteners are related to non-alcoholic fatty liver disease: Microbiota dysbiosis as a novel potential mechanism. EXCLI Journal 2020, 19, 620–620. [Google Scholar] [CrossRef]
- Alves-Bezerra, M.; Cohen, D.E. Triglyceride Metabolism in the Liver. Comprehensive Physiology 2017, 8, epub–20171212. [Google Scholar] [CrossRef]
- Ipsen, D.; Lykkesfeldt, J.; Tveden-Nyborg, P. Molecular mechanisms of hepatic lipid accumulation in non-alcoholic fatty liver disease. Cell Molecular Life Science 2018, 75, 3313–3327. [Google Scholar] [CrossRef]
- Uebanso, T.; Ohnishi, A.; Kitayama, R.; Yoshimoto, A.; Nakahashi, M.; Shimohata, T.; Mawatari, K.; Takahashi, A. Effects of Low-Dose Non-Caloric Sweetener Consumption on Gut Microbiota in Mice. Nutrients 2017, 9, 560–560. [Google Scholar] [CrossRef]
- Aron-Wisnewsky, J.; Vigliotti, C.; Witjes, J.; Le, P.; Holleboom, A.; Verheij, J.; Nieuwdorp, M.; Clement, K. Gut microbiota and human NAFLD: disentangling microbial signatures from metabolic disorders. Nature Reviews Gastroenterology & Hepatology 2020, 17, 279–297. [Google Scholar] [CrossRef]
- Zani, F.; Blagih, J.; Gruber, T.; Buck, M.; Jones, N.; Hennequart, M.; Newell, C.; Pilley, S.; Soro-Barrio, P.; Kelly, G. , et al. The dietary sweetener sucralose is a negative modulator of T cell-mediated responses. Nature 2023, 615, 705–711. [Google Scholar] [CrossRef]
- Huby, T.; Gautier, E. Immune cell-mediated features of non-alcoholic steatohepatitis. Nature reviews 2022, 22, 429–443. [Google Scholar] [CrossRef]
- Kawano, Y.; Edwards, M.; Huang, Y.; Bilate, A.; Araujo, L.; Tanoue, T.; Atarashi, K.; Ladinsky, M.; Reiner, S.; Wang, H. , et al. Microbiota imbalance induced by dietary sugar disrupts immune-mediated protection from metabolic syndrome. Cell 2022, 185, 3501–3519. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.B.; Hu, E.D.; Xu, L.M.; Chen, L.; Wu, J.L.; Li, H.; Chen, D.Z.; Chen, Y.P. The relationship between obesity and the severity of non-alcoholic fatty liver disease: systematic review and meta-analysis. Expert review of gastroenterology & hepatology 2018, 12, 491–502. [Google Scholar] [CrossRef]
- Vilalta, A.; Gutiérrez, J.A.; Chaves, S.Z.; Hernández, M.; Urbina, S.; Hompesch, M. Adipose tissue measurement in clinical research for obesity, type 2 diabetes and NAFLD/NASH. Endocrinology, Diabetes & Metabolism 2022, 5, e00335–e00335. [Google Scholar] [CrossRef]
- Ventura, E.; Davis, J.; Goran, M. Sugar content of popular sweetened beverages based on objective laboratory analysis: focus on fructose content. Obesity (Silver Spring) 2011, 19, 868–874. [Google Scholar] [CrossRef]
- Walker, R.W.; Dumke, K.A.; Goran, M.I. Fructose content in popular beverages made with and without high-fructose corn syrup. Nutrition (Burbank, Los Angeles County, Calif.) 2014, 30, 928–935. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, X.; Cirillo, P.; Sautin, Y.; McCall, S.; Bruchette, J.; Diehl, A.M.; Johnson, R.; Abdelmalek, M. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. Journal of Hepatology 2008, 48, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, B.M.; Ahuja, S.P.; Marliss, E.B. Effects of intravenously administered fructose and glucose on splanchnic amino acid and carbohydrate metabolism in hypertriglyceridemic men. Journal of Clinical Investigation 1975, 56, 970–977. [Google Scholar] [CrossRef]
- Johnston, R.; Stephenson, M.; Crossland, H.; Cordon, S.; Palcidi, E.; Cox, E.; Taylor, M.; Aithal, G.; Macdonald, I. No difference between high-fructose and high-glucose diets on liver triacylglycerol or biochemistry in healthy overweight men. Gastroenterology 2013, 145, 1016–1025. [Google Scholar] [CrossRef]
- Naomi, N.; Ngo, J.; Brouwer-Brolsma, E.; Buso, M.; Soedamah-Muthu, S.; Perez-Rodrigo, C.; Harrold, J.; Halford, J.; Raben, A.; Geleijnse, J. , et al. Sugar-sweetened beverages, low/no-calorie beverages, fruit juice and non-alcoholic fatty liver disease defined by fatty liver index: the SWEET project. Nutrition & Diabetes 2023, 13, 6–6. [Google Scholar]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterology 2006, 6. [Google Scholar] [CrossRef]
- Varsamis, P.; Larsen, R.N.; Dunstan, D.W.; Jennings, G.L.; Owen, N.; Kingwell, B.A. The sugar content of soft drinks in Australia, Europe and the United States. The Medical Journal of Australia 2017, 206, 454–455. [Google Scholar] [CrossRef] [PubMed]
- Yuan, S.; Chen, J.; Li, X.; Fan, R.; Arsenault, B.; Gill, D.; Giovannucci, E.L.; Zheng, J.s.; Larsson, S.C. Lifestyle and metabolic factors for nonalcoholic fatty liver disease: Mendelian randomization study. European Journal of Epidemiology 2022, 37, 723–733. [Google Scholar] [CrossRef] [PubMed]
- Sewter, R.; Heaney, S.; Patterson, A. Coffee Consumption and the Progression of NAFLD: A Systematic Review. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Vlassara H, Cai W, Crandall J, et al. Inflammatory mediators are induced by dietary glycotoxins, a major risk factor for diabetic angiopathy [published correction appears in Proc Natl Acad Sci U S A. 2003 Jan 21; 100(2): 763.]. Proc Natl Acad Sci U S A. 2002, 99, 15596-15601. [Google Scholar] [CrossRef]
Figure 1.
The effect of sugar intake from SSB on risk of having NAFLD/NASH based on the multinominal logistical regression model. NAFLD was defined as simple steatosis without NASH. Model 1 was adjusted for age, gender, race, and PIR. Model 2 was adjusted for covariates in Model 1 and lifestyle pattern, including status of smoking, alcohol drinking, physical activity, and medical condition, daily dietary intake pattern, including total energy, total sugar, and total fat. Model 3 was adjusted for covariates in Model 2 and BMI status. No more than 36 g of added sugar for men and 25 g of added sugar for women was recommended by the American Heart Association (AHA) recommendation. For heavy SSB consumers, ≥72 and ≥50 g of sugar intake from SSB for men and women were used in this study, respectively.
Figure 1.
The effect of sugar intake from SSB on risk of having NAFLD/NASH based on the multinominal logistical regression model. NAFLD was defined as simple steatosis without NASH. Model 1 was adjusted for age, gender, race, and PIR. Model 2 was adjusted for covariates in Model 1 and lifestyle pattern, including status of smoking, alcohol drinking, physical activity, and medical condition, daily dietary intake pattern, including total energy, total sugar, and total fat. Model 3 was adjusted for covariates in Model 2 and BMI status. No more than 36 g of added sugar for men and 25 g of added sugar for women was recommended by the American Heart Association (AHA) recommendation. For heavy SSB consumers, ≥72 and ≥50 g of sugar intake from SSB for men and women were used in this study, respectively.
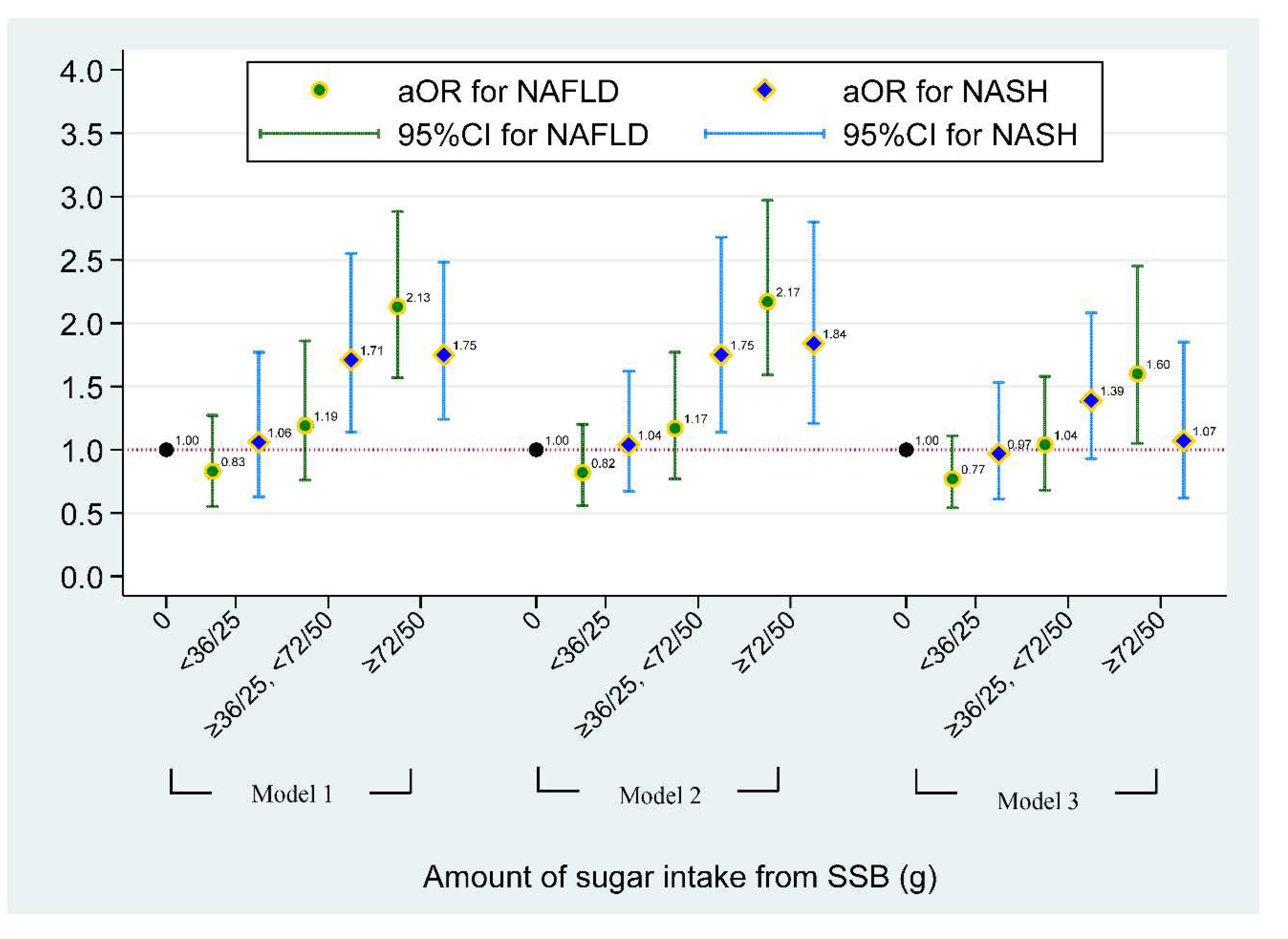
Figure 2.
The effect of type of SSB or ASB consumption on risk of having NAFLD/NASH based on the multinominal logistical regression model. NAFLD was defined as simple steatosis without NASH. Model 1 was adjusted for age, gender, race, and PIR. Model 2 was adjusted for covariates in Model 1 and lifestyle pattern, including status of smoking, alcohol drinking, physical activity, and medical condition, daily dietary intake pattern, including total energy, total sugar, and total fat. Model 3 was adjusted for covariates in Model 2 and BMI status. Non-soda intake was defined based on SSB consumer who did not intake ASB and regular soda. ASB only consumers were defined based on individuals who only consumed soda with no calories artificial sweetener. Individuals who consumed two or more types of SSB or ASB and with any types of SSB were defined as multiple SSB consumers.
Figure 2.
The effect of type of SSB or ASB consumption on risk of having NAFLD/NASH based on the multinominal logistical regression model. NAFLD was defined as simple steatosis without NASH. Model 1 was adjusted for age, gender, race, and PIR. Model 2 was adjusted for covariates in Model 1 and lifestyle pattern, including status of smoking, alcohol drinking, physical activity, and medical condition, daily dietary intake pattern, including total energy, total sugar, and total fat. Model 3 was adjusted for covariates in Model 2 and BMI status. Non-soda intake was defined based on SSB consumer who did not intake ASB and regular soda. ASB only consumers were defined based on individuals who only consumed soda with no calories artificial sweetener. Individuals who consumed two or more types of SSB or ASB and with any types of SSB were defined as multiple SSB consumers.
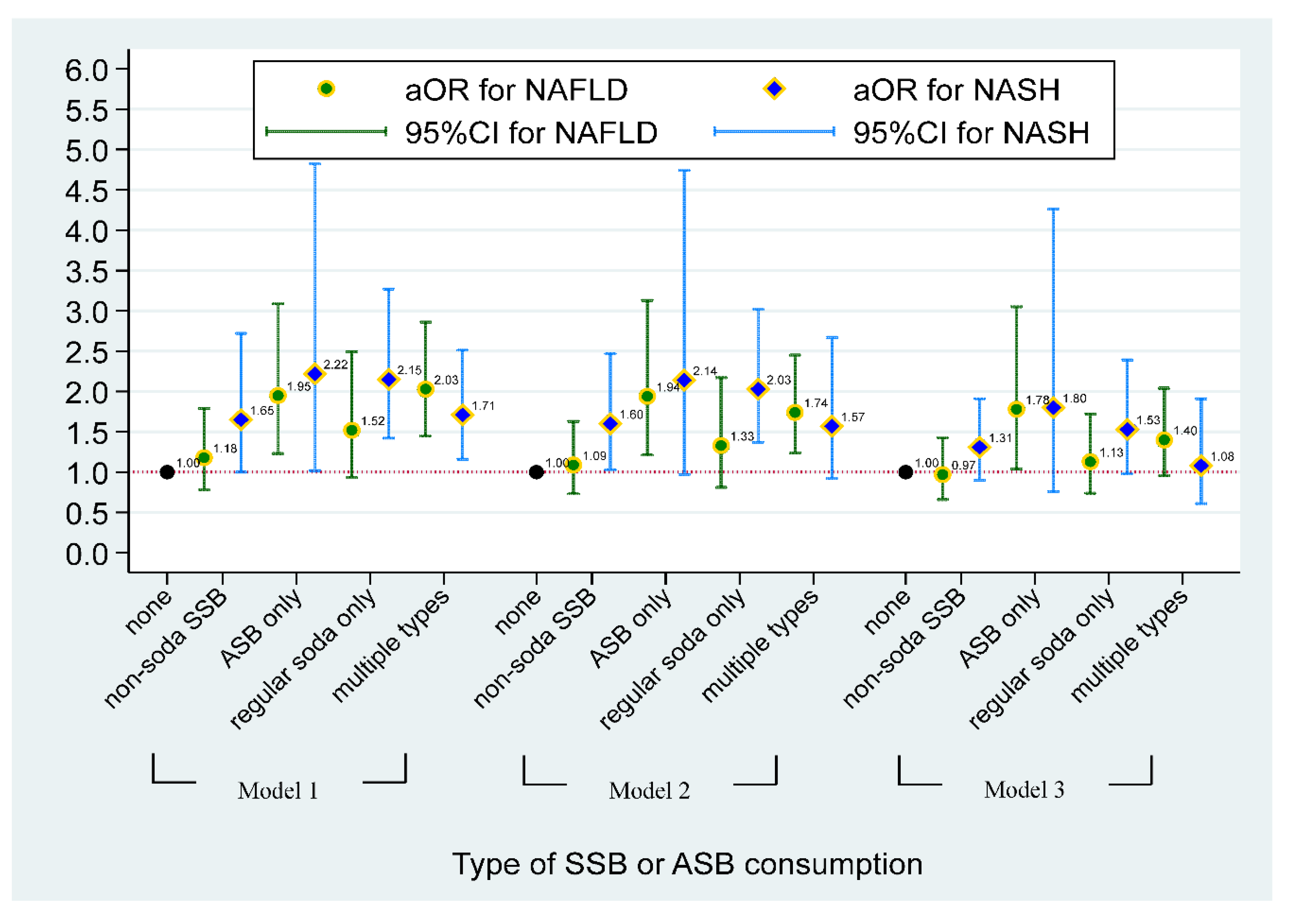

Table 1.
Distribution of demographic factors and NAFLD/NASH.
| Factors | Liver examination status | ||||
|---|---|---|---|---|---|
| Total | Normal | NAFLD 1 | NASH | P value | |
| Raw population 2 | N=3739 | N=1636 | N=1367 | N=736 | |
| Survey-weighted 3 | 100% | 46.8% | 32.7% | 20.5% | |
| Personal characteristics | |||||
| Age, years (mean±se) | 48.0±0.7 | 43.9±0.9 | 53.6±1.1 | 48.4±0.9 | <0.001 |
| Gender | |||||
| male | 45.7% | 41.4% | 28.7% | 30.0% | <0.001 |
| female | 54.3% | 51.4% | 36.0% | 12.6% | |
| Race | |||||
| non-Hispanic White | 63.3% | 47.1% | 32.6% | 20.3% | 0.002 |
| non-Hispanic Black | 11.5% | 56.2% | 33.1% | 10.7% | |
| Mexican American | 7.1% | 36.2% | 36.2% | 27.5% | |
| other Hispanic | 7.3% | 43.9% | 31.7% | 24.4% | |
| other Race | 10.8% | 43.7% | 30.8% | 25.5% | |
| PIR | |||||
| below poverty | 11.3% | 48.4% | 32.8% | 18.8% | 0.754 |
| 1 - 1.99 | 16.2% | 42.4% | 38.9% | 19.7% | |
| 2 - 2.99 | 15.6% | 46.3% | 31.1% | 22.7% | |
| 3 - 3.00 | 13.9% | 49.0% | 29.5% | 21.6% | |
| ≥ 4 | 43.1% | 47.6% | 32.3% | 20.1% | |
1 NAFLD was defined as simple steatosis without NASH. 2 Raw number of participants in this study without adjusted for sample survey design. 3 Results were obtained after adjusted for sample weights and complex study design. Abbreviation, PIR, Ratio of family income to poverty.
Table 2.
The sampling weights-adjusted distribution of Lifestyle, dietary patterns and SSB-related factors, and biomedical examination among NAFLD/NASH status.
Table 2.
The sampling weights-adjusted distribution of Lifestyle, dietary patterns and SSB-related factors, and biomedical examination among NAFLD/NASH status.
| Factors | Liver examination status | ||||
|---|---|---|---|---|---|
| Total | Normal | NAFLD 1 | NASH | P value | |
| Raw population 2 | N=3739 | N=1636 | N=1367 | N=736 | |
| Survey-weighted 3 | 100% | 46.8% | 32.7% | 20.5% | |
| Lifestyle patterns | |||||
| Cigarettes use | |||||
| none | 63.7% | 65.5% | 62.1% | 62.1% | 0.513 |
| former | 23.0% | 20.4% | 25.0% | 12.2% | |
| current | 13.3% | 14.1% | 12.9% | 25.7% | |
| Alcohol use | |||||
| none | 21.6% | 19.2% | 26.5% | 19.1% | 0.003 |
| light to moderate | 78.4% | 80.8% | 73.5% | 80.9% | |
| Physical activity (hr/week) | |||||
| low | 58.0% | 50.2% | 68.0% | 60.0% | <0.001 |
| adequate | 42.0% | 49.8% | 32.0% | 40.0% | |
| Medical conditions 4 | |||||
| no | 43.2% | 51.7% | 32.0% | 41.8% | <0.001 |
| yes | 56.8% | 48.3% | 68.0% | 58.2% | |
| Daily dietary pattern, mean±se | |||||
| Total caloric (kcal) | 2047±25 | 2002±31 | 2020±35 | 2191±43 | <0.001 |
| Total sugar (gm) | 102±1.6 | 99±1.7 | 103±2.5 | 109±4.5 | 0.019 |
| Total fat (gm) | 84.4±1.3 | 83.2±1.7 | 82.9±1.5 | 89.6±2.2 | 0.017 |
| Total caffeine (mg) | 162±5.4 | 151±6.1 | 176±10.1 | 167±8.9 | 0.037 |
| Total alcohol (gm) | 7.1±0.4 | 6.3±0.4 | 7.4±0.8 | 8.8±1.2 | 0.030 |
| SSB-related elements | |||||
| Sugar intake from total SSB (gm), mean±se | 38.1±1.4 | 35.4±1.3 | 40.3±2.9 | 40.7±2.9 | 0.023 |
| Sugar intake from each SSB, mean±se | |||||
| Soda (gm) | 20.7±1.2 | 19.1±1.3 | 21.3±1.6 | 23.4±2.5 | 0.067 |
| Fruit drinks (gm) | 5.1±0.4 | 5.0±0.6 | 5.4±0.6 | 4.9±0.7 | 0.990 |
| Sweetened tea/coffee | 9.8±0.9 | 8.6±0.7 | 11.7±1.8 | 9.4±1.6 | 0.350 |
| Sport/energy drinks | 2.5±0.3 | 2.7±0.3 | 2.0±0.5 | 3.0±0.7 | 0.914 |
| Type of SSB intake | |||||
| non-SSB intake | 26.9% | 29.9% | 25.9% | 21.9% | 0.065 |
| non-soda intake 5 | 21.7% | 22.7% | 19.1% | 23.5% | |
| ASB intake only 6 | 10.5% | 7.3% | 13.0% | 11.4% | |
| regular soda only | 19.8% | 18.6% | 18.9% | 24.1% | |
| multiple types | 21.1% | 20.5% | 23.2% | 19.1% | |
| Clinical Examination | |||||
| LSM (kPa), mean±se | 5.5±0.1 | 4.8±0.1 | 5.8±0.2 | 6.5±0.3 | <0.001 |
| ALT (U/L), mean±se | 21.7±0.4 | 18.3±0.6 | 15.8±0.2 | 38.5±0.9 | <0.001 |
| AST (U/L), mean±se | 21.1±0.3 | 20.4±0.6 | 17.2±0.1 | 29.0±0.6 | <0.001 |
| eGFR, mL/min/1.73m2, mean±se | 96.3±0.8 | 99.0±0.9 | 92.0±1.4 | 97.2±1.4 | 0.056 |
| BMI | |||||
| normal weight | 29.3% | 53.3% | 13.4% | 7.1% | <0.001 |
| overweight | 32.2% | 32.1% | 37.0% | 28.4% | |
| obese | 38.5% | 14.6% | 49.6% | 64.5% | |
1 NAFLD was defined as simple steatosis without NASH. 2 Raw number of participants in this study without adjusted for sample survey design. 3 Results were obtained after adjusted for sample weights and complex study design. 4 Medical condition includes asthma, diabetes, fatty liver, COPD, arthritis, hypertension, congestive heart failure, heart attack, weak/failing kidneys, angina, thyroid problem, and cancer/malignancy. 5 Individuals who consumed sweetened drinks other than ASB and regular soda were categorized into non-soda intake. 6 Individuals who only consumed soda with no calories artificial sweetener were defined as ASB only.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



