
Submitted:
07 August 2023
Posted:
09 August 2023
You are already at the latest version
Abstract
Background and objectives: Huntington disease (HD) is characterized by motor, cognitive and psychiatric manifestations and is caused by an expansion of CAG repeats over 35 triplets on the huntingtin (HTT) gene. However, expansions in the range 27-35 repeats (intermediate allele) can be associated with pathological phenotypes. The onset of HD is conventionally defined by the onset of motor symptoms, but psychiatric disturbances can precede the motor phase by up to twenty years. The aims of the present study are to identify HD patients in the pre-motor phase of the disease among patients diagnosed with bipolar disorders and to evaluate any differences between bipolar patients carrying normal HTT allele and patients with expanded HTT gene. Methods: We assessed the HTT genotype in an Italian cohort of 69 patients affected by bipolar disorder type 1 and type 2. Results: No patient was found to be a carrier of the pathological HTT allele, but 10% of bipolar subjects carried an intermediate allele. Carriers of the intermediate allele were older at onset of psychiatric symptoms than non-carriers. Conclusion: The pathological HTT gene was not associated with bipolar disorder, while we found a higher frequency of the intermediate allele among the bipolar population with respect to healthy controls.
Keywords:
Huntington disease
; CAG
; HTT gene
; bipolar disorder
; intermediate allele
1. Introduction
Expansion of CAG triplets in the huntingtin gene (HTT) on chromosome 4 is responsible for Huntington disease (HD). The presence of 40 or more CAG triplets is invariably associated with manifest disease, while expansions in the range 36–39 repeats are considered to confer a reduced disease penetrance [1,2]. HD is characterized by motor, cognitive and psychiatric disorders [1]. Conventionally, HD onset is defined as the age of the onset of motor signs, however, often psychiatric disturbances, especially mood disturbances, can occur up to twenty years before the manifest motor phase [3,4]. HD is transmitted in an autosomal dominant manner, but new mutations can be generated in the offspring by the elongation of unstable alleles falling in the range 27–35 repeats, defined intermediate alleles (IA) [5]. The percentage of IA has been variably estimated between 0.45 to 8.7% [6,7] in the healthy population. The reported frequency of IA in European-based cohorts is about 6% [6]. Although the HTT gene with less than 36 CAG repeats is considered normal, a growing number of studies reported that subjects carrying IA are at higher risk of behavioral problems [8,9], or can even develop clinical phenotypes of HD [8,9,10,11]. In the present study we analyzed the HTT gene in a psychiatric-cohort of patients affected by bipolar disorder in order to identify pre-motor HD patients, to describe the frequency of IA and to detect clinic-demographic differences between patient with or without CAG expansions in the HTT gene.
2. Materials and Methods
2.1. Population
Blood samples of 69 unrelated patients affected by bipolar disorder type I and type II were genotyped for HTT gene. The diagnosis of bipolar disorder was made according to DSM IV criteria [12].
Demographic-clinical data included: age at the time of withdrawal, age at disease onset, gender, first symptom at onset, educational level, family history for psychiatric disorders. The genetic results were compared to a cohort of 104 healthy controls we recently described, 45 males (43.3%) and 59 females (56.7%) with a mean age of 64.4 (± 8.5) years [13].
2.2. Genetic analysis
Genomic DNA was isolated from peripheral blood sample using QIAamp DNA Blood Mini QIAcube kit (cat. No 51126 QIAGEN) and quality-checked with the QIAxpert spectrophotometer. DNA samples were stored at +4◦ until use. CAG repeat expansion of HTT gene was investigated with a polymerase chain reaction (PCR) amplification assay, using the primers 5′-[6-FAM] GACCCTGGAAAAGCTGATGA-3′ and 5′-GGCTGAGGAAGCTGAGGAG-3′. The forward primer was modified with the fluorescent dye 6-carboxyfluorescein (6-FAM) [14]. The size of the fragment was determined by capillary electrophoresis using the SeqStudio Genetic Analyzer (ThermoFisher) and analyzed with the GeneMapper software (v.4.0, Applied Biosystems). A set of known length HTT CAG alleles was used as size standard. A CAG trinucleotide expansion under 27 repetitions was considered as normal allele, IAs with repeats in the range 27–35, pathologic allele with expansion size >35 repeats.
2.3. Statistical analysis
The demographic-clinical features of bipolar patients were described by the mean and standard deviation in case of continuous variables, and by percentage in case of categorical variables. Due to the identification of IA, we performed a comparison between bipolar patients carrying IA (IA-carriers) and bipolar patients carrying the normal alleles (non-IA carriers). The comparison of the demographic-clinical features was made with nonparametric analysis: Fisher’s exact test for categorical variables and Mann-Whitney test for continuous variables. The study population was then compared to the healthy control group in terms of HTT CAG distribution and IA frequency. Mann-Whitney test and Fisher’s exact test were used as appropriate. Statistical analyses were performed using IBM SPSS Statistics 20.0 (IBM Corp., New York, NY).
3. Results
There were 69 bipolar patients with a mean age at disease onset of 34 years and female prevalence (60.9%) (Table 1). The onset of bipolar disorder was in the 49.2% of cases with depressive symptoms, in the 15.9% with maniacal symptoms and in the rest of the cases with a mix of both symptoms. More than 60% of patients had bipolar disorder type 1. Family history for psychiatric disorders was present in 43.5% of cases. The mean number of CAG repeats in HTT gene was 17.7 for the shorter allele and 21.03 for the longer one (Table 1). No patient was found to be a carrier of a pathological allele. We identified 7 bipolar patients carrying IA (IA-carriers). The mean length of IA was 28.6 (ranging 27–33). The comparison between bipolar patients IA-carriers and non- IA carriers is reported in Table 2. IA-carriers were older at disease onset than non-IA carriers (Table 2). The frequency of IA was statistically significant higher in bipolar patients, 10.14% (7 out of 69), than in the healthy control population, 5.8% (6 out of 104) (p < 0.001), while the range of normal CAG repeats was 13–26 in both groups. The distribution of the HTT CAG repeat length among the two cohorts is shown in Figure 1. The distribution of normal-range alleles differs in the two cohorts in a way that healthy subjects have higher number of triplets in both the alleles (Figure 1).
4. Discussion
The study of the HTT gene in a cohort of 69 patients with bipolar disorder did not identify any subjects in a pre-motor stage of HD, in fact no patient was a carrier of pathological allele. The IA was detected in 10.14% of cases. IA-carriers were older as compare with non- IA carriers at disease onset. Although psychiatric symptoms may often precede the motor phase of HD, there are few previous studies evaluating the frequency of the pathological expansion in the HTT gene in psychiatric patients: two studies in patients affected by major depression [15,16] and one in a Brazilian cohort affected by bipolar disorder [17]. Major depression was frequent as pre-motor phase of HD [15], while Ramos and colleagues [17], in line with our results, did not identify any association between the pathological HTT allele and bipolar disorder. The frequency of IA-carriers in our psychiatric cohort was almost the double than that detected in the local reference population. Data from the literature has already shown a higher risk of behavioral disturbances in subjects carrying IA [9,16], such as apathy, obsessive disorder, anxiety, depression, suicidal ideation. However, the mechanism by which the IA of HTT gene is associated with psychiatric manifestations remains unclear [9]: one hypothesis is through mechanisms unrelated to those leading to HD pathology [9], such as interaction with other genes [9]. In that case, the difference in the genetic structure between races could explained the lack of association between IA and bipolar disorder in the Brazilian population [17,18]. The analysis of the distribution of the HTT normal alleles revealed a statistically significant difference between bipolar patients and controls, with shorter normal alleles among patients. These data support the hypothesis of a non-linear association between the CAG repeat length and the risk of bipolar disorder, which means that both the normal alleles in the shorter range and the IA could increase the risk of developing bipolar disorder. This non-linear association has been already described between the HTT CAG length and the risk of developing major depression [16], and between the HTT size and the intelligence in the general population [19]. Therefore, it seems that the increasing size of non-pathological HTT gene confers an advantage until the values that determine pathology. In fact, the increasing number of HTT triplets is part of the evolutionary process [20] and the variation of the number of repeats across the normal range influences brain’s structure in healthy subjects [21]: longer non-pathological alleles have been found associated with an increasing volume of basal ganglia [21]. Studies on HD patients [22,23,24] demonstrated that the increasing size of normal allele could be protective by mitigating the effect of the pathological one and delaying disease onset. Interestingly, in the present cohort we found that bipolar patients carrying IA were older at disease onset as compare with non-IA carriers. Basal ganglia are involved in the pathophysiology of bipolar disorder [25,26], so, IA, via its effect on basal ganglia [21], could have a protective role and delay the onset of bipolar symptoms. Thus, the IA of HTT could act on the development of bipolar disorder with two different mechanisms: one that increases the risk of the disease and the other that postpones its onset. Another hypothesis could be that when the development of bipolar disorder is driven by the IA of HTT the age at onset is later than when it is caused by other genetic factors.
5. Conclusions
To our knowledge there is only another study evaluating the HTT genotype among bipolar patients [17] and like in our study bipolar disorder was not associated with the pathological HTT allele. In our cohort IA was associated with bipolar disorder but with a delayed age at onset. The results of the present study prompt further investigations into the role of the IA of HTT gene in the onset of bipolar disorder.
Author Contributions
Conceptualization, Camilla Ferrari; Formal analysis, Silvia Bagnoli and Assunta Ingannato; Investigation, Elena Capacci; Writing—original draft, Camilla Ferrari; Writing—review & editing, Sandro Sorbi and Benedetta Nacmias.
Funding
This research received no funding.
Institutional Review Board Statement
The study has been conducted in accordance with the ethical standards of the institutional research committee and with the Helsinki declaration and all the patients signed an informed consent.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- McColgan, P.; Tabrizi, S.J. Huntington’s disease: A clinical review. Eur J Neurol 2018, 25, 24–34. [Google Scholar] [CrossRef]
- Kay, C.; Hayden, M.R.; Leavitt, B.R. Epidemiology of Huntington disease. Handb Clin Neurol 2017, 144, 31–46. [Google Scholar] [PubMed]
- Ross, C.A.; Reilmann, R.; Cardoso, F.; McCusker, E.A.; Testa, C.M.; Stout, J.C.; et al. Movement Disorder Society Task Force Viewpoint: Huntington’s Disease Diagnostic Categories. Mov Disord Clin Pract 2019, 6, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Julien, C.L.; Thompson, J.C.; Wild, S.; Yardumian, P.; Snowden, J.S.; Turner, G.; et al. Psychiatric disorders in preclinical Huntington’s disease. J Neurol Neurosurg Psychiatry 2007, 78, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Hammer, M.B.; Singleton, A.B. Common Premutations in the General Population. JAMA Neurol 2019, 76, 639–640. [Google Scholar] [CrossRef] [PubMed]
- Apolinário, T.A.; Paiva, C.L.; Agostinho, L.A. REVIEW-ARTICLE Intermediate alleles of Huntington’s disease HTT gene in different populations worldwide: A systematic review. Genetics and molecular research 2017, 16. [Google Scholar] [CrossRef]
- Sundblom, J.; Niemelä, V.; Ghazarian, M.; Strand, A.S.; Bergdahl, I.A.; Jansson, J.H.; et al. High frequency of intermediary alleles in the HTT gene in Northern Sweden—The Swedish Huntingtin Alleles and Phenotype (SHAPE) study. Sci Rep 2020, 10, 9853. [Google Scholar] [CrossRef]
- Oosterloo, M.; Van Belzen, M.J.; Bijlsma, E.K.; Roos, R.A. Is There Convincing Evidence that Intermediate Repeats in the HTT Gene Cause Huntington’s Disease? J Huntingtons Dis 2015, 4, 141–148. [Google Scholar] [CrossRef]
- Killoran, A.; Biglan, K.M.; Jankovic, J.; Eberly, S.; Kayson, E.; Oakes, D.; et al. Characterization of the Huntington intermediate CAG repeat expansion phenotype in PHAROS. Neurology 2013, 80, 2022–2027. [Google Scholar] [CrossRef]
- Kenney, A.; Powell, S.; Jankovic, J. Autopsy-proven Huntington’s disease with 29 trinucleotide repeats. Mov Disord 2007, 22, 127–130. [Google Scholar] [CrossRef]
- Savitt, D.; Jankovic, J. Clinical phenotype in carriers of intermediate alleles in the huntingtin gene. J Neurol Sci 2019, 402, 57–61. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical manual of mental disorders, 4th ed.; 2000. [Google Scholar]
- Ingannato, A.; Bagnoli, S.; Bessi, V.; Ferrari, C.; Mazzeo, S.; Sorbi, S.; Nacmias, B. Intermediate alleles of HTT: A new pathway in longevity. J. Neurol. Sci. 2022, 438, 120274. [Google Scholar] [CrossRef] [PubMed]
- Jama, M.; Millson, A.; Miller, C.E.; Lyon, E. Triplet repeat primed PCR simplifies testing for Huntington disease. J. Mol. Diagn. 2013, 15, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Perlis, R.H.; Smoller, J.W.; Mysore, J.; Sun, M.; Gillis, T.; Purcell, S.; et al. Prevalence of incompletely penetrant Huntington’s disease alleles among individuals with major depressive disorder. Am J Psychiatry 2010, 167, 574–579. [Google Scholar] [CrossRef]
- Gardiner, S.L.; van Belzen, M.J.; Boogaard, M.W.; van Roon-Mom, W.M.C.; Rozing, M.P.; van Hemert, A.M.; et al. Huntingtin gene repeat size variations affect risk of lifetime depression. Transl Psychiatry 2017, 7, 1277. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.M.; Gillis, T.; Mysore, J.S.; Lee, J.M.; Alonso, I.; Gusella, J.F.; et al. Prevalence of Huntington’s disease gene CAG trinucleotide repeat alleles in patients with bipolar disorder. Bipolar Disord 2015, 17, 403–408. [Google Scholar] [CrossRef]
- Raskin, S.; Allan, N.; Teive, H.A.; Cardoso, F.; Haddad, M.S.; Levi, G.; et al. Huntington disease: DNA analysis in Brazilian population. Arq Neuropsiquiatr 2000, 58, 977–985. [Google Scholar] [CrossRef]
- Lee, J.K.; Conrad, A.; Epping, E.; Mathews, K.; Magnotta, V.; Dawson, J.D.; et al. Effect of Trinucleotide Repeats in the Huntington’s Gene on Intelligence. EBioMedicine 2018, 3, 47–53. [Google Scholar] [CrossRef]
- Hannan, A.J. Tandem Repeat Polymorphisms: Genetic Plasticity, Neural Diversity and Disease; Landes Bioscience and Springer Science: New York, 2012. [Google Scholar]
- Mühlau, M.; Winkelmann, J.; Rujescu, D.; Giegling, I.; Koutsouleris, N.; Gaser, C.; et al. Variation within the Huntington’s disease gene influences normal brain structure. PLoS ONE 2012, 7, e29809. [Google Scholar] [CrossRef]
- Aziz, N.A.; Jurgens, C.K.; Landwehrmeyer, G.B.; EHDN Registry Study Group; van Roon-Mom, W.M.; van Ommen, G.J.; et al. Normal and mutant HTT interact to affect clinical severity and progression in Huntington disease. Neurology 2009, 73, 1280–1285, Erratum in Neurology 2009, 73, 1608. Erratum in Neurology 2011, 76, 202. A. Ciarmielo [corrected to Ciarmiello, Andrea]. [Google Scholar] [CrossRef]
- Djoussé, L.; Knowlton, B.; Hayden, M.; Almqvist, E.W.; Brinkman, R.; Ross, C.; et al. Interaction of normal and expanded CAG repeat sizes influences age at onset of Huntington disease. Am J Med Genet. A 2003, 119A, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Volpi, E.; Terenzi, F.; Bagnoli, S.; Latorraca, S.; Nacmis, B.; Sorbi, S.; et al. Late-onset Huntington disease: An Italian cohort. J Clin Neurosci 2021, 86, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wang, Y.; Jia, Y.; Zhong, S.; Sun, Y.; Zhou, Z.; Zhang, Z.; Huang, L. Microstructural Abnormalities of Basal Ganglia and Thalamus in Bipolar and Unipolar Disorders: A Diffusion Kurtosis and Perfusion Imaging Study. Psychiatry Investig. 2017, 14, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Aylward, E.H.; Roberts-Twillie, J.V.; Barta, P.E.; Kumar, A.J.; Harris, G.J.; Geer, M.; Peyser, C.E.; Pearlson, G.D. Basal ganglia volumes and white matter hyperintensities in patients with bipolar disorder. Am. J. Psychiatry 1994, 151, 687–693. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Distribution of HTT gene length in bipolar patients (n = 62) and healthy controls (n = 98) with the exclusion of IA-carriers. (a) The distribution of CAG in the alleles 1 differs between healthy controls and bipolar patients (p < 0.001). (b) The distribution of CAG in the alleles 2 differs between healthy controls and bipolar patients (p 0.028).
Figure 1.
Distribution of HTT gene length in bipolar patients (n = 62) and healthy controls (n = 98) with the exclusion of IA-carriers. (a) The distribution of CAG in the alleles 1 differs between healthy controls and bipolar patients (p < 0.001). (b) The distribution of CAG in the alleles 2 differs between healthy controls and bipolar patients (p 0.028).
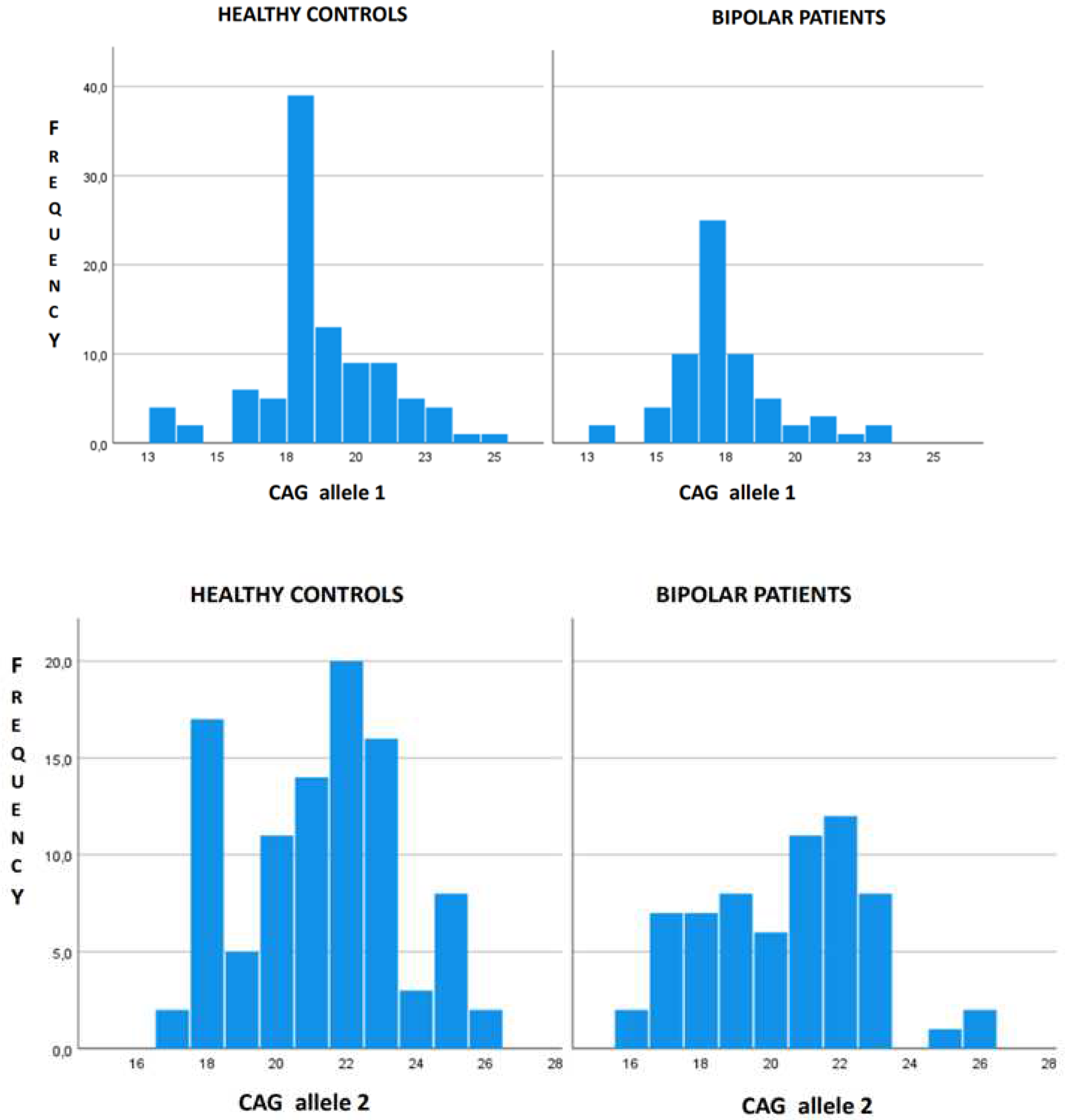

Table 1.
Clinical-demographic and genetic features of the studied patients.
| Patients (n = 69) | |
|---|---|
| Age (SD) | 53.91 (10.2) |
| Age at disease onset (SD) | 34.81 (13.4) |
|
Sex Male (%) Female (%) |
27 (39.1) 42 (60.9) |
| Education in years (SD) | 10.25 (3.1) |
|
Symptoms at onset Maniacal (%) Depression (%) Mix (%) |
11 (15.9) 34 (49.2) 24 (34.7) |
| Bipolar disorder Type 1 (%) | 44 (63.7) |
| Family history for psychiatric disorders (%) | 30 (43.5) |
HTT gene *
|
17.7 (2.1) 21.03 (3.3) - 0 7 (10.2) |
* Pathological allele > 35 CAG repeats; Intermediate allele 27–35 CAG repeats; normal allele <27 CAG repeats; Allele CAG 1 = shorter allele; Allele CAG 2 = longer allele.
Table 2.
Characteristics of bipolar patients by the genetic status of IA-carriers.
| No IA-carriers (n = 62) | IA-carriers (n = 7) | P | |
|---|---|---|---|
| Age at disease onset (SD) | 33.7 (13.5) | 43.3 (9.9) | 0.048 |
|
Sex Male (%) Female (%) |
23 (37.1%) 39 (62.9%) |
4 (57.3%) 3 (42.8) |
0.38 |
|
Symptoms at onset Maniacal (%) Depression (%) Mix (%) |
9 (14.5) 30 (48.4) 23 (37.1) |
2 (28.5) 4 (57.1) 1 (14.2) |
0.89 |
| Family history for psychiatric disorder (%) | 39 (45.1) | 2 (28.5) | 0.09 |
| CAG 1 (SD) | 17.37 (1.8) | 20.6 (2.3) | 0.09 |
| CAG 2 (SD) | 20.2 (2.08) | 28.6 (1.4) | < 0.001 |
* IA = intermediate allele.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



