
Submitted:
09 August 2023
Posted:
10 August 2023
You are already at the latest version
Abstract
The problem of blood delivery has been a critical concern in past decades. However, the unsteady behavior of blood donors, along with the uncertainties associated with demands in a crisis imposes several challenges for resource management. In this research work, we analyze the blood delivery behavior in a crisis modeled by coupled queues of patients and blood sources. Using Markovian modeling and results associated with G-network, we derive two critical probabilities, namely lack of unit of blood (unit of donations) or not having any storage capacity left to accept new donors' blood. We propose a closed-form solution to calculate the optimal blood storage size, and also we suggest sufficient conditions that guarantee the feasibility of the model. Finally, we conduct a sensitivity analysis to investigate the impact of model parameters on storage size and the proportion of time that storage is full.
Keywords:
Blood supply chain
; queueing system
; disaster management
; Blood inventory management
1. Introduction
The role of the blood supply chain in healthcare systems proved to be critical due to the key role of blood in supplying oxygen and nutrition to body organs and serving as a lifeline for patients in need of blood transfusions and life-saving treatments [1,2]. However, several challenges shall be tackled to manage this complex supply chain efficiently [3]. These challenges include uncertainty in patients' and donors' arrival [4,5]. Such uncertainties, along with requirements for keeping blood units safe, lead to uncertainties in blood availability and a need to make decisions about appropriate storage size. The number of studies that addressed such a concern is limited. Two recent studies that take account of storage size and stochasticity nature of blood inventory level in their studies, used approximation and metaheuristic algorithms to address the problem [6,7].
Blood as a valuable living tissue within the human body, is of significant medical importance. For a successful human blood transfusion, it is crucial to evaluate the compatibility of two key antigen systems, namely: ABO and Rh resulting in the eight major blood types. It is worth noting that, some blood types are compatible with several other types, albeit with different priorities of substitution [8,9]. Given the perishability of blood and special storage requirements, deciding on the appropriate storage size is vital for reducing costs of investments, blood perishability, and rejecting donations because of the capacity [10,11].
Overall, the blood supply chain has several stages that include, but are not limited to, collecting donor’s blood and storing it, delivery of stored blood, and transfusing it to patients [12]. All of the aforementioned have uncertain natures in the form of stochasticity.
On the other hand, in natural disaster crises such as earthquakes, there is a need to supply blood to affected patients promptly [13,14]. Overall, a cut-point of 51 hours—less than 3 days—is suggested for the more than 2200 search and rescue processes studied [15]. This time is far less than a week shelf life suggested for the whole blood [16]. Therefore in this study, we only consider the storage capacity and ignore blood perishability.
In the literature, queueing models with Poisson arrivals and Exponential service times are used to model networks and inventory systems [7,17,18]. For instance, Gelenbe used the concept of “energy packets” a discretized interpretation of Energy arrival to model a node and an analytical routing of an energy-harvesting wireless sensor network [19,20]. Such networks were studied further considering intermittent connections in another study [21]. Recently level dependent perishable items are investigated using a Jackson network—an extension of queueing systems [22].
However, to the best of our knowledge, previous studies have not used an aggregated queueing model to investigate a blood supply chain with uncertainties in donors’ and patients’ arrival, along with a stochastic delivery system. In this study, we use an integrated queueing system to decide about the appropriate blood bank size designed to address crises due to an unusual blood demand caused by disasters. The study also investigates the stability conditions of the system such that human casualties are minimized. Finally, a sensitivity analysis is performed to identify the most crucial intervals for parameters to help managers know when to use means such as campaigns or investment in vehicles to improve system performance.
2. Materials and Methods
The blood delivery problem under study investigates a system with a random delivery of patients to the hospital wherein units of blood are stored. Throughout our modeling, we consider a storage constraint that decides the maximum capacity for storing units of blood safely. We wish to remind the readers that, in a crisis, the capacity for patient care spaces who need to be transferred for blood transfusion is considered unlimited (i.e., they are moved to safe areas and wait for ambulances to move them to a hospital). However, the quality of healthcare and safety concerns associated with the location of the crisis may impact the mortality rate of patients. What follows presents the notations used in this paper:
| The mortality rate of patients | |
| The rate of the local demand (i.e., not related to the crisis) | |
| The transportation rate per patient, including travel time | |
| The rate of finding victims in need of blood (patients) | |
| The blood donation rate | |
| The probability of having no blood stored in the storage | |
| The probability of having no storage capacity to accept donors | |
| The probability of having no patients in need of blood | |
| Utilization factor of blood storage | |
| Utilization factor of temporary patient care spaces | |
| Storage size decided based on the given parameter |
We wish to remind the readers that because the hospital and patients are not located in the same place, we need to transfer the patients or unit of blood; therefore, a transfusion is possible if and only if we have a patient, the unit of blood, and a vehicle ready to transfer either of them. Figure 1 illustrates the system’s behavior. In this figure, indicates the state of the system and means that there are patients in need of blood in the system and units of blood is stored. The red circles indicate states under which blood transfusion is impossible (i.e., either there is no blood or no patient). Using probabilities of having no patients in the system and no blood stored, we can decompose the system as shown in Figure 2.
Given the abovementioned, the interrelationship between blood storage, transportation, and the number of patients in need of blood can be modeled using a decomposition method (see Figure 2). As can be seen, the model is composed of two coupled queues for patients and blood storage, respectively. In this model, the patient queue follows an discipline and the blood queue (with limited storage) follows an discipline. Given the probabilities of blood stockout , absence of patients, and lack of space in storage , one may obtain the stationary states distribution as follows:
where , and . We now consider the case , that is:
The utilization factor of the blood queue is obtained as follows:
Substituting equations 1 and 4 in equations 2 and 3 yields:
As can be seen in Equations (6) and (7), we can obtain storage size (i.e., ) based on the probabilities of blood shortage or the proportion of time that we cannot accept any donations . For a simpler presentation, let us define , , we have:
By substituting and with and respectively, and using simple calculations, including rearranging equation (8) and taking logarithms of both sides, one obtains the following values for and :
Substituting and with their respective values we have:
It is worth noting that in Equation (12) if i.e. , there is a lower bound for . In other words, if there are always some blood donors that are declined, because the system does not have sufficient capacity. However, leads to a lower bound for that is more critical—it means some levels of blood shortage must be accepted.
Note that for small enough and , equations (6) and (7) turn into much simpler equations as follows:
Using a similar procedure as stated earlier, one obtains the following values for and :
In Equations (19) and (20), the second terms are obtained using L’Hopital’s rule.
Now that we have obtained the closed-form solutions to obtain the storage size, we are ready to analyze the stability conditions of the system. First, we investigate the lower bound for the system to be out of blood for patients (i.e., . The is defined by:
Therefore, one may calculate the following for different intervals of :
As can be seen in equation (22), when is less than 1 we face some shortages regardless of storage size. Given equation (5) and assuming that there are no patients in need of blood (i.e., to avoid constant blood shortage, we have:
That means the donation rate shall exceed the rate of local demand for blood to guarantee that there is no permanent shortage of blood units for local demand. Because we aim to avoid patients’ mortality for delays in blood transfusion, let us set to zero. By substituting equations (1) and (4) in equation (5), we have:
Given that is positive, we have . Now we investigate the transportation rate of patients. We wish to remark that, although the main goal of blood transportation is to reduce the number of patients in need of transfusion to zero (i.e., ), if we stay in , we do not need any storage and blood donors anymore. Now we are ready to investigate the lower bound of () as follow:
As can be seen in equation (25) to avoid a constant postponement of donations (i.e., having enough space to keep donations in the long run), we need be near zero, which is not achievable for greater than 1. Therefore, we have:
Given that in a crisis demands of on-site patients are much higher than the perishability plus demands from local patients (i.e. ) and by setting to zero, we have . Note that the relation is intuitive, given that campaigns to attract donors in a crisis are unhelpful when investments in transportation infrastructure did not take place in advance. So the stability conditions are as follows: (a) , (b) , (c), and (d) , note that relation (d) is inferred from relations (a) and (b). There is an additional condition that is stated earlier (after Equation (16)), (e) The following is a summarization of the aforementioned conditions, noting that conditions (a) and (c) are inferred from condition (e):
Finally, we wish to remind the readers that for calculating we need to use which itself is a function of Therefore, updating leads to a change in and , respectively. To overcome this issue, we will use a successive approximation algorithm, to update values of and , given the new value of (See Figure 3). This algorithm is applicable when we have a lower blood donation rate than patient discovery—i.e., inevitable shortage and accepting some mortality on patients’ part caused by delayed blood delivery—that is not addressed in this study.
3. Results
In this section, we evaluate the impact of changes in different parameters on parameters. First, we investigate the impact of changes in parameter values on . As can be seen in Equation (14), is a hypervolume in a six-dimensional space. Therefore, to visualize first, we rewrite Equation (14) as follows:
In our analysis, we always assess the impact of changes in coupled with changes in (Figure 4), (Figure 5), and (Figure 6).
Figure 4 investigates the impact of changes in the probability of tolerable blood unit shortage in percent— (x-axis, top), and the average blood donors per patient discovered— (y-axis, bottom) on the storage capacity— (z-axis, vertical). As can be seen in Figure 4, the combination of large values of and small values of increases drastically. Otehrwise, small values of can manage the our expectations. It is intuitive, having in mind that larger means more tollerations towards the unavailability of blood units and small values of leads to a lower storage space for blood units—there is a limited number of donors in comparison with patients which means most of the donated blood units are consumed in a short time.
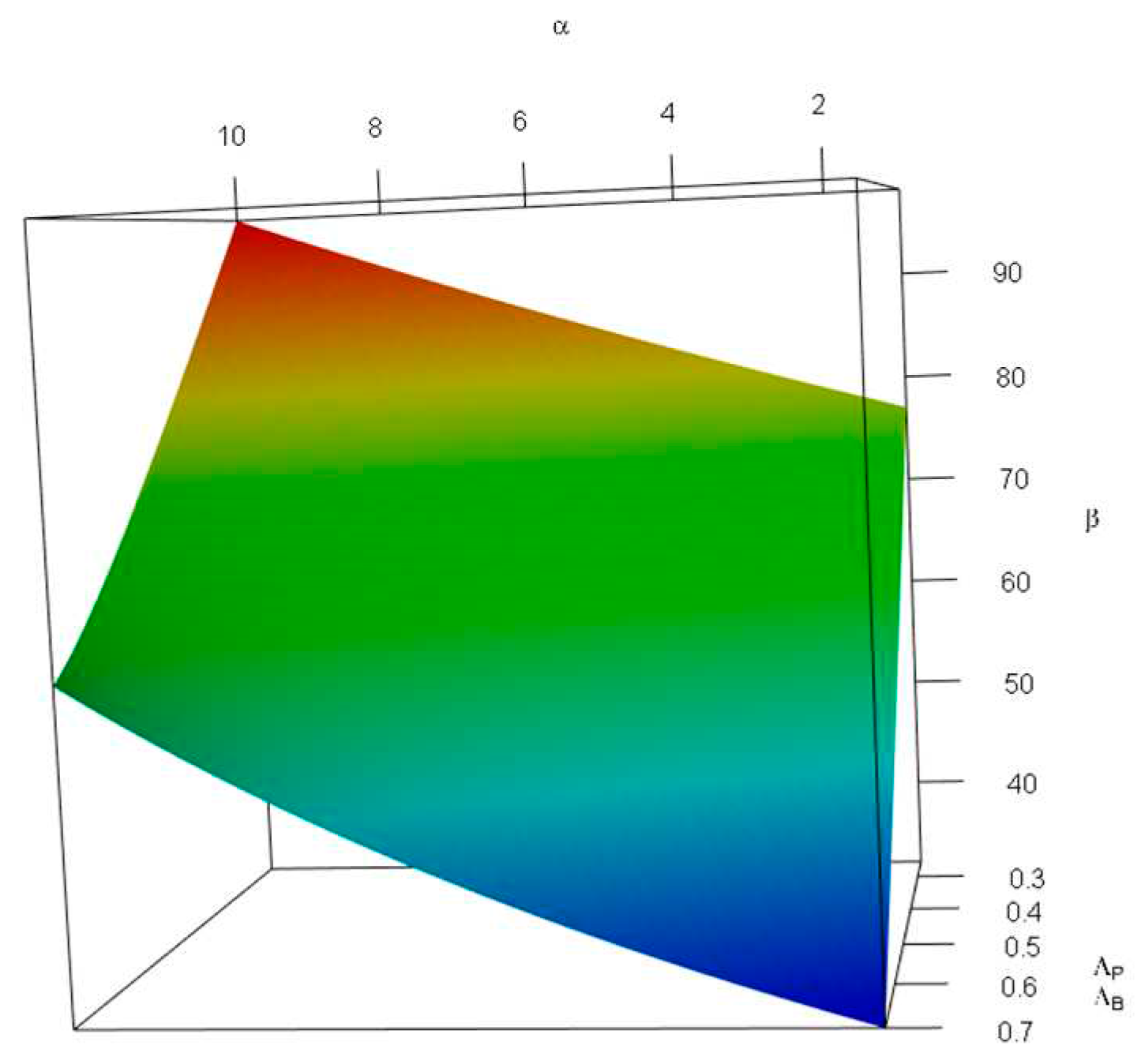
Figure 5 investigates the impact of changes in the probability of tolerable blood unit shortage in percent— (x-axis, top), and the average patient mortality per patient transfer per patient discovered— (y-axis, bottom) on the storage capacity— (z-axis, vertical). As can be seen in Figure 5, the combination of small values of and increases . We only discuss the impact of large values of . This means a high patient mortality per patient transfer in comparison with the patient discovery means less storage space requirement; however, this impact is more moderate than that of —in the latter almost a flat plane is observed.
Figure 5 investigates the impact of changes in the probability of tolerable blood unit shortage in percent— (x-axis, top), and the average local demand per patient discovered— (y-axis, bottom) on the storage capacity— (z-axis, vertical). As can be seen in Figure 6, the combination of large values of and small values of increases . We only discuss the impact of large values of . In other words, a lower local demand per patient discovery leads to a less storage space requirement; this impact is more severe than that of —in the latter a flatter plane was observed.
As stated earlier, obtaining is not easy for two reasons: (a) we need an iterative process to approximate its value (see Figure 3), and (b) has a lower bound that means is not attainable for some values. Here, we investigate the impact of , , and on . For simplicity we rewrite Equation (18) as follows:
We wish to remind the reader that and are dependent variables—i.e., we can obtain one using the other. Figure 7 demonstrates the impact of changes in the probability of tolerable blood unit shortage in percent— (x-axis, top), and the average patient discovered per donor— (y-axis, bottom) on the probability of not having any further capacity— (z-axis, vertical). For this figure, we limited values to the interval, and to —i.e., falls in intervals. We used such intervals to avoid obtaining invalid values of caused by inconsistency between shortage and rate of patient discovery—the combination of a high probability of shortage and low rates of patient discovery per donor is invalid. As can be seen in Figure 7, is an increasing function of , and a decreasing function of . This is because, on one hand, more tolerable shortage means less storage capacity; and on the other hand, less patient discovery in comparison with blood donors means a lower demand rate—i.e., the more time blood units need to be stored.
(in percent) for values of , and (in percent), given and .
As stated earlier, the values are applicable for cases wherein some levels of shortage in blood availability is inevitable; therefore, having the stability conditions means .
4. Discussion and Conclusion
In this study, we proposed a blood bank storage design policy to be used for disaster management—e.g., for designing a blood bank near an earthquake-prone area. We proposed a stochastic queueing model facing a coupled Poisson arrival process on both patient’s and donor’s queues. The probabilities of significance—i.e., the probability of having no blood stored in the bank or having no capacity to accept new donors, which then enable us to calculate a closed-form solution for optimal bank storage size given the aforementioned probabilities. We have also analyzed system stability conditions by obtaining acceptable donation and transportation rates, given patient discovery and local demand. These results are applicable in defining the number of allocated vehicles for disaster management purposes and running campaigns to encourage blood donations. Overall, blood collection campaigns are important and shall be designed based on the capacity to avoid donors’ dissatisfaction for reasons such as waiting for a long time or not accepting them because bank storage is full [12]. The results not only help us to decide about the optimum blood bank size, but they also declare the conditions under which the system stability is guaranteed.
With respect to the results and analysis conducted earlier, the blood bank size cannot be very small. Note that the combination of small values of probability of shortage and a low ratio of blood donors () to patients discovered means a high storage size. Furthermore, during disasters, there is often a significant increase in the demand for blood. Additionally, rejecting numerous donors can result in their dissatisfaction, and a high frequency of rejection reduces the likelihood of them returning to donate again. Therefore, instead of relying solely on designing campaigns that encourage a larger number of people to donate, we should focus on increasing storage capacity—see Figure 7 for donors’ rejection rate and Figure 4 for the relation among as well as [12]. On the other hand, if historical data suggests that the local demand for blood is high, we shall also consider such a demand in designing the blood bank (see Figure 6).
We wish to remind the readers that in emergencies unmatched Type O Rh-negative ( might be used for patients [23]. Such an approach persuades us to address the demand and supply for each blood type independently; therefore, although in this study we evaluated the storage capacity for blood donors and patients irrespective of the blood type, the model shall be employed for each blood type once to decide the capacity required. Given the uncertain nature of supply and demand in blood transfusion, it is better to avoid allocating unutilized storage of one blood type to another.
As a future direction of this research, blood perishability for longer periods can be taken into account. The researchers may also study batch delivery of patients or blood, and consider a network of blood banks and smaller storages to study a more realistic situation.
Author Contributions
Conceptualization A. P., A. H. A. S., and N. S.; methodology, A. P., A. H. A. S., and N. S.; software, A. P., A. H. A. S., and N. S.; formal analysis, A. P., A. H. A. S., and N. S.; writing—original draft preparation, A. P.; writing—review and editing, A. P., A. H. A. S., and N. S.; visualization, A. P.; supervision, A. H. A. S., and N. S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Fahimnia, B.; Jabbarzadeh, A.; Ghavamifar, A.; Bell, M. Supply chain design for efficient and effective blood supply in disasters. International Journal of Production Economics 2017, 183, 700–709. [Google Scholar] [CrossRef]
- Pirabán, A.; Guerrero, W.J.; Labadie, N. Survey on blood supply chain management: Models and methods. Computers & Operations Research 2019, 112, 104756. [Google Scholar] [CrossRef]
- Ageron, B.; Benzidia, S.; Bourlakis, M. Healthcare logistics and supply chain – issues and future challenges. Supply Chain Forum: An International Journal 2018, 19, 1–3. [Google Scholar] [CrossRef]
- Ramezanian, R.; Behboodi, Z. Blood supply chain network design under uncertainties in supply and demand considering social aspects. Transportation Research Part E: Logistics and Transportation Review 2017, 104, 69–82. [Google Scholar] [CrossRef]
- Torrado, A.; Barbosa-Póvoa, A. Towards an Optimized and Sustainable Blood Supply Chain Network under Uncertainty: A Literature Review. Cleaner Logistics and Supply Chain 2022, 3, 100028. [Google Scholar] [CrossRef]
- Meneses, M.; Santos, D.; Barbosa-Póvoa, A. Modelling the Blood Supply Chain. European Journal of Operational Research 2023, 307, 499–518. [Google Scholar] [CrossRef]
- Aghsami, A.; Samimi, Y.; Aghaie, A. A combined continuous-time Markov chain and queueing-inventory model for a blood transfusion network considering ABO/Rh substitution priority and unreliable screening laboratory. Expert Systems with Applications 2023, 215, 119360. [Google Scholar] [CrossRef]
- Duan, Q.; Liao, T.W. Optimization of blood supply chain with shortened shelf lives and ABO compatibility. International journal of production economics 2014, 153, 113–129. [Google Scholar] [CrossRef]
- Dillon, M.; Oliveira, F.; Abbasi, B. A two-stage stochastic programming model for inventory management in the blood supply chain. International Journal of Production Economics 2017, 187, 27–41. [Google Scholar] [CrossRef]
- Cetin, E.; Sarul, L.S. A blood bank location model: A multiobjective approach. European Journal of Pure and Applied Mathematics 2009, 2, 112–124. [Google Scholar]
- Kaya, O.; Ozkok, D. A blood bank network design problem with integrated facility location, inventory and routing decisions. Networks and Spatial Economics 2020, 20, 757–783. [Google Scholar] [CrossRef]
- Osorio, A.F.; Brailsford, S.C.; Smith, H.K. A structured review of quantitative models in the blood supply chain: a taxonomic framework for decision-making. International Journal of Production Research 2015, 53, 7191–7212. [Google Scholar] [CrossRef]
- Al-Mandhari, A. Earthquakes as triggers for public health disasters: WHO and health systems’ response. Eastern Mediterranean health journal 2023, 29, 165–167. [Google Scholar] [CrossRef] [PubMed]
- Ciaraglia, A.; Brigmon, E.; Braverman, M.; Kidd, E.; Winckler, C.J.; Epley, E.; Flores, J.; Barry, J.; DeLeon, D.; Waltman, E.; et al. Use of whole blood deployment programs for mass casualty incidents: South Texas experience in regional response and preparedness. J Trauma Acute Care Surg 2022, 93, e182–e184. [Google Scholar] [CrossRef] [PubMed]
- Adams, A.L.; Schmidt, T.A.; Newgard, C.D.; Federiuk, C.S.; Christie, M.; Scorvo, S.; DeFreest, M. Search is a time-critical event: when search and rescue missions may become futile. Wilderness Environ Med 2007, 18, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, L.; Hedner, U.; Nilsson, I.M.; Robertson, B. Shelf-life of bank blood and stored plasma with special reference to coagulation factors. Transfusion 1983, 23, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, B.; Hosseinifard, S.Z. On the issuing policies for perishable items such as red blood cells and platelets in blood service. Decision Sciences 2014, 45, 995–1020. [Google Scholar] [CrossRef]
- Ramírez, A.P.; Labadie, N.; Rueda, W.J.G. Vehicle Routing Problem for Blood Mobile Collection System with Stochastic Supply. In Proceedings of the proceedings of the international conference on industrial engineering and operations management; 2018. [Google Scholar]
- Gelenbe, E. Synchronising energy harvesting and data packets in a wireless sensor. Energies 2015, 8, 356–369. [Google Scholar] [CrossRef]
- Gelenbe, E.; Marin, A. Interconnected wireless sensors with energy harvesting. In Proceedings of the Analytical and Stochastic Modelling Techniques and Applications: 22nd International Conference, ASMTA 2015, Albena, Bulgaria, May 26-29, 2015. Proceedings 22, 2015, May 26-29; pp. 87–99.
- Zareei, S.; Afshar Sedigh, A.H.; Deng, J.D.; Purvis, M. Buffer management using integrated queueing models for mobile energy harvesting sensors. In Proceedings of the 2017 IEEE 28th Annual International Symposium on Personal, Indoor, and Mobile Radio Communications (PIMRC), 2017; pp. 1–5. [Google Scholar]
- Islam, M.A.; Islam, M.E.; Rashid, A. Stochastic optimization of level-dependent perishable inventory system by Jackson network. Ain Shams Engineering Journal 2023, 14, 101935. [Google Scholar] [CrossRef]
- Miraflor, E.; Yeung, L.; Strumwasser, A.; Liu, T.H.; Victorino, G.P. Emergency uncrossmatched transfusion effect on blood type alloantibodies. Journal of Trauma and Acute Care Surgery 2012, 72, 48–53. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A schema of the queueing system for blood transfusion. The red circles indicate states under which blood transfusion is impossible.
Figure 1.
A schema of the queueing system for blood transfusion. The red circles indicate states under which blood transfusion is impossible.
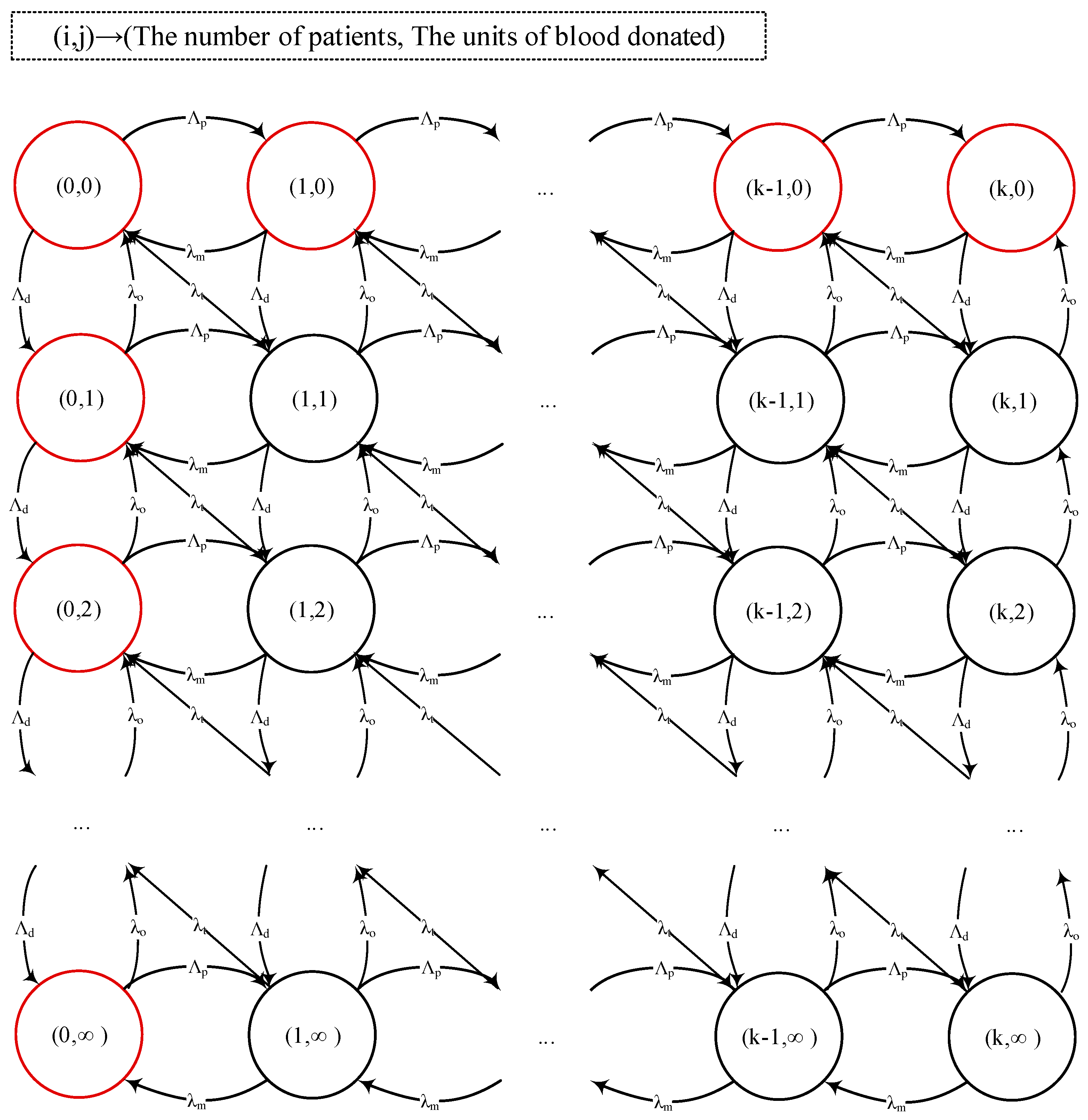
Figure 2.
The simplified queueing model of the blood delivery system: (I) Patient flow and (II) blood storage.
Figure 2.
The simplified queueing model of the blood delivery system: (I) Patient flow and (II) blood storage.
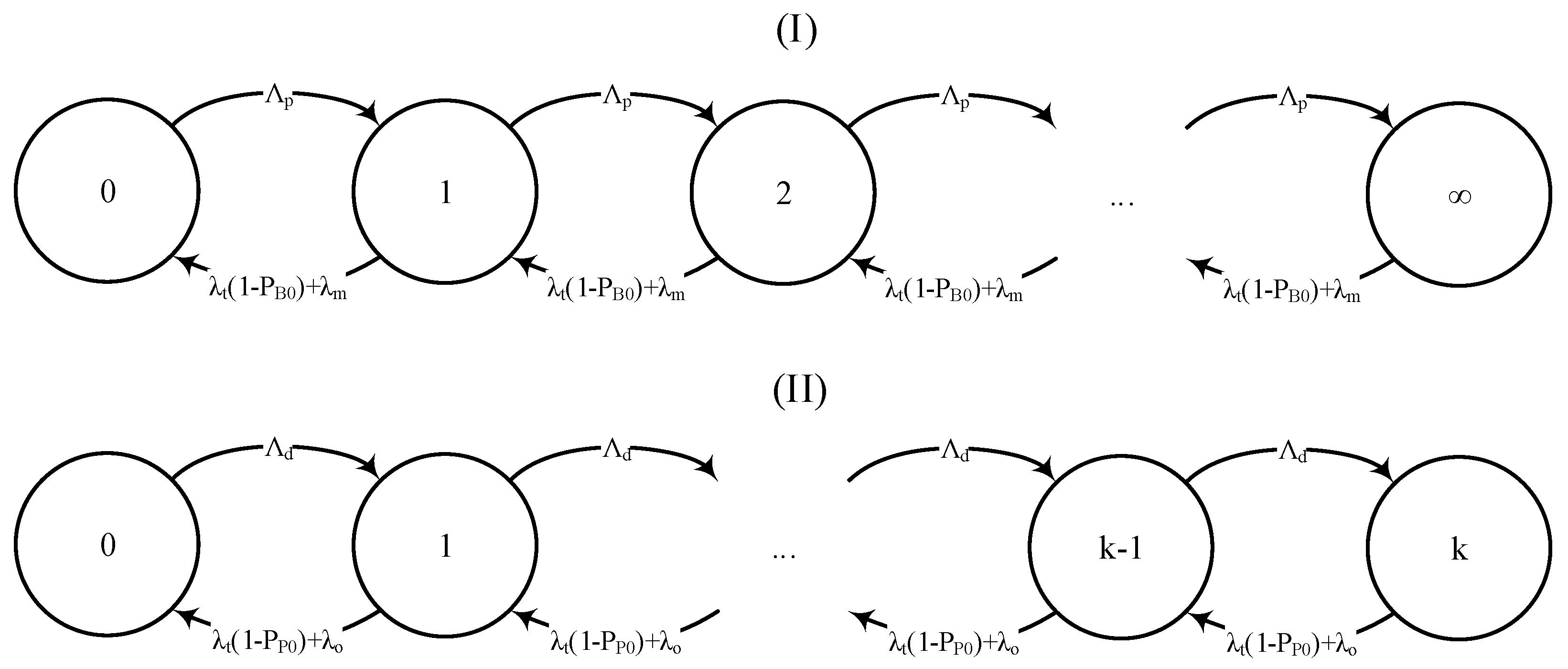
Figure 3.
Pseudo code of the algorithm used for successive approximation.
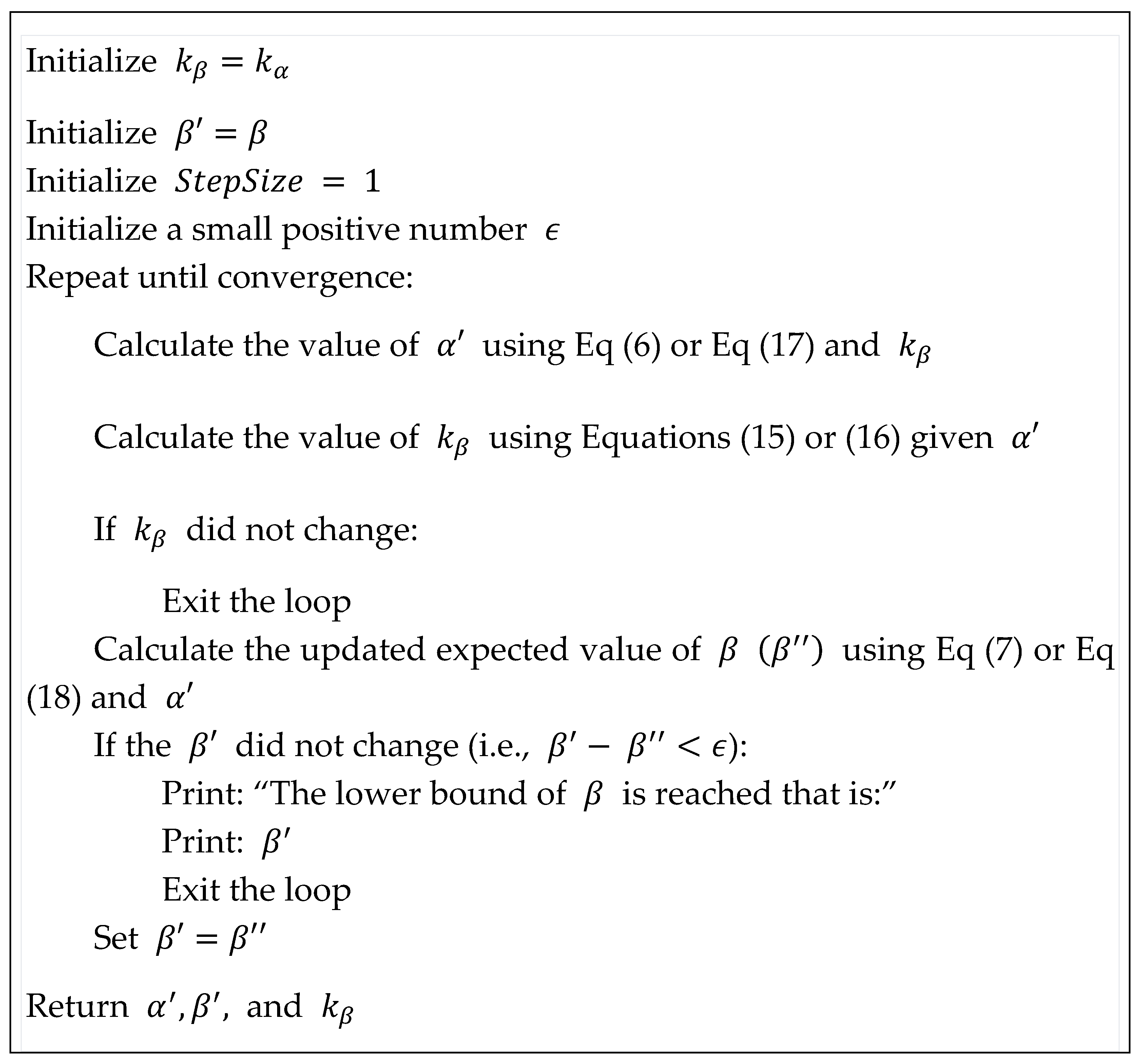
Figure 4.
Changes in with respect to the different values of and (in percent), given and —(a) front view, (b) back view.
Figure 4.
Changes in with respect to the different values of and (in percent), given and —(a) front view, (b) back view.
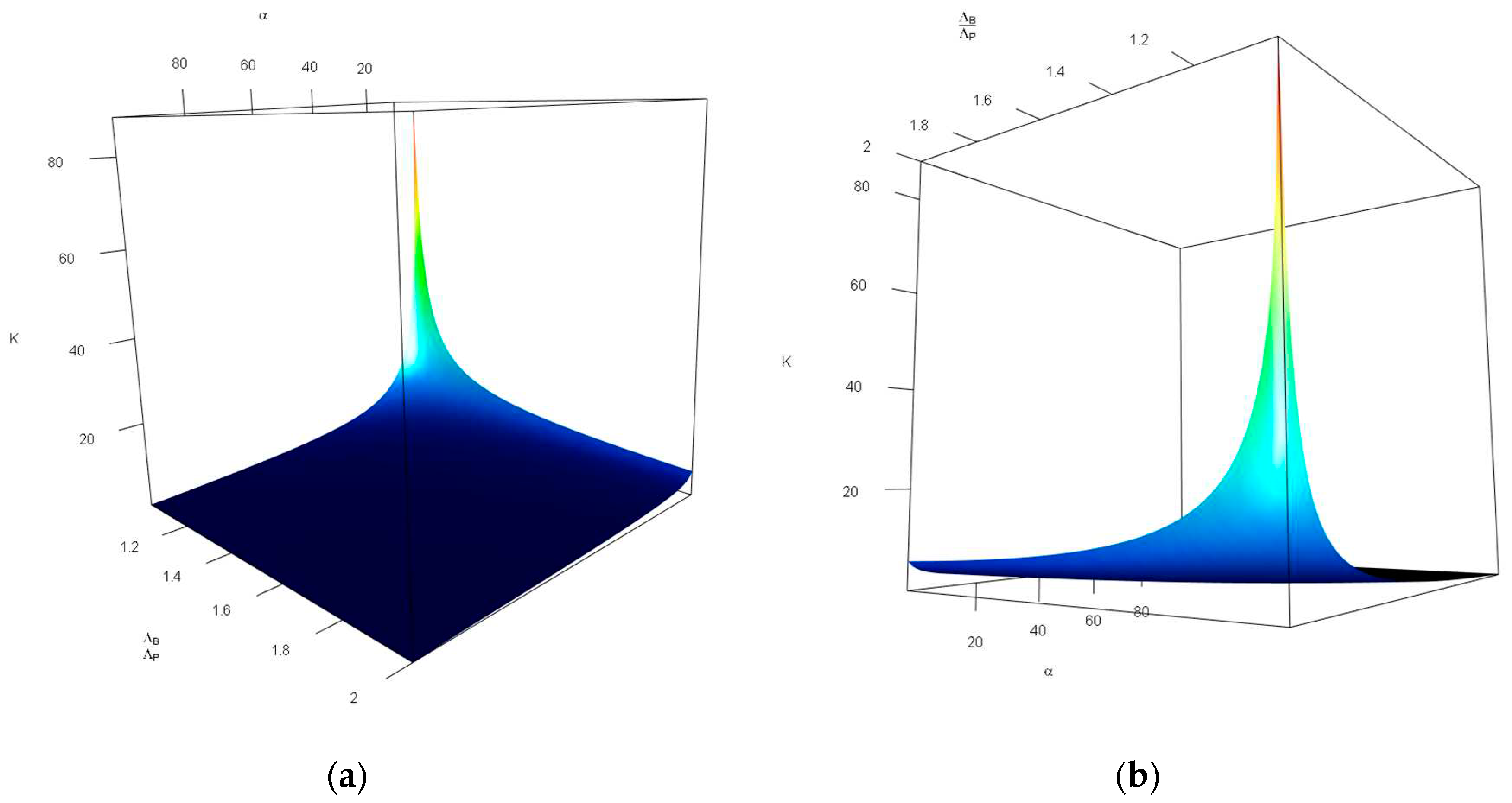
Figure 5.
Changes in with respect to the different values of and (in percent), given and —(a) side view, (b) front view.
Figure 5.
Changes in with respect to the different values of and (in percent), given and —(a) side view, (b) front view.
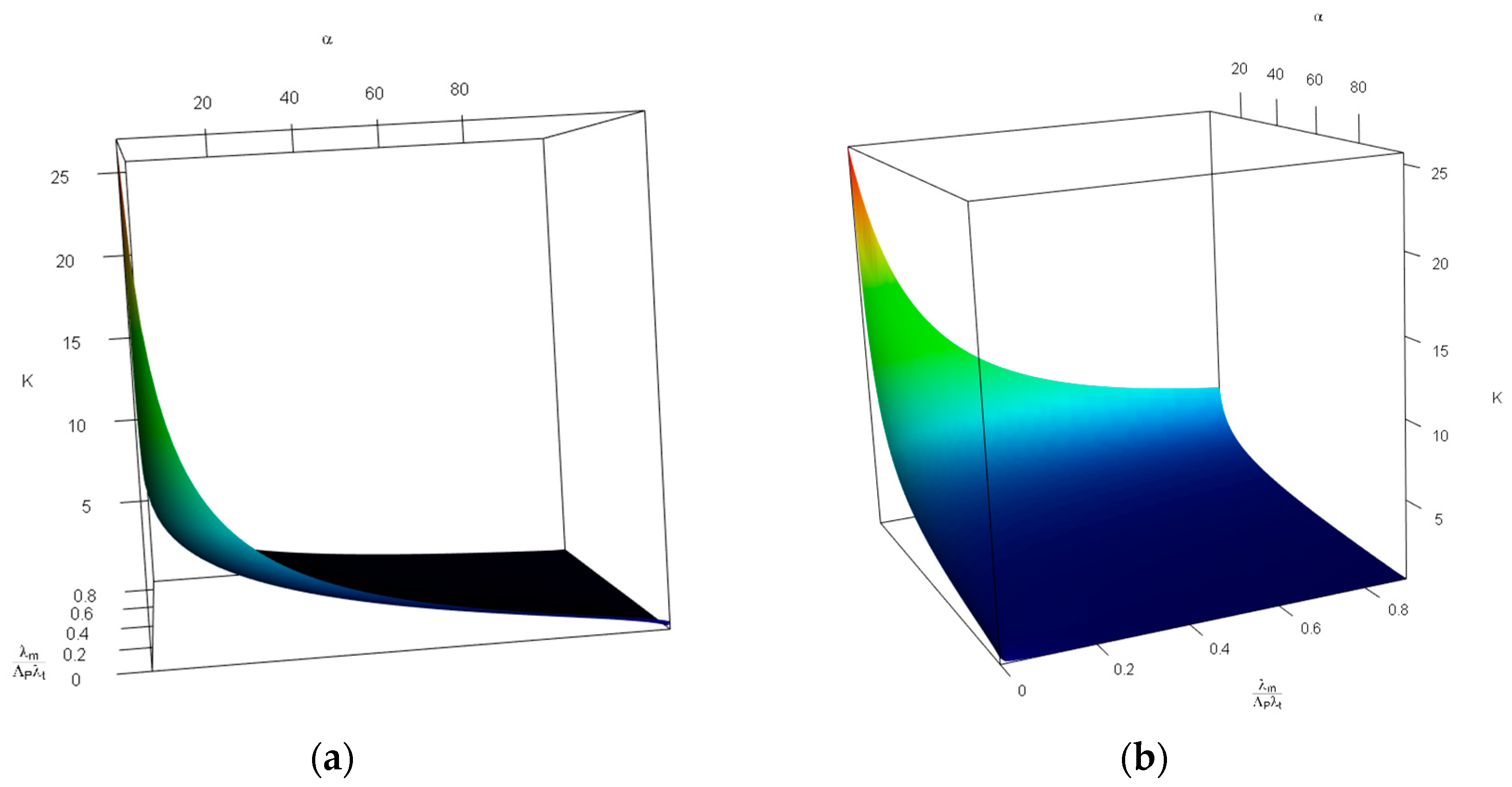
Figure 6.
Changes in with respect to the values of less than 0.25, and (in percent), given and —(a) front view, (b) back view.
Figure 6.
Changes in with respect to the values of less than 0.25, and (in percent), given and —(a) front view, (b) back view.
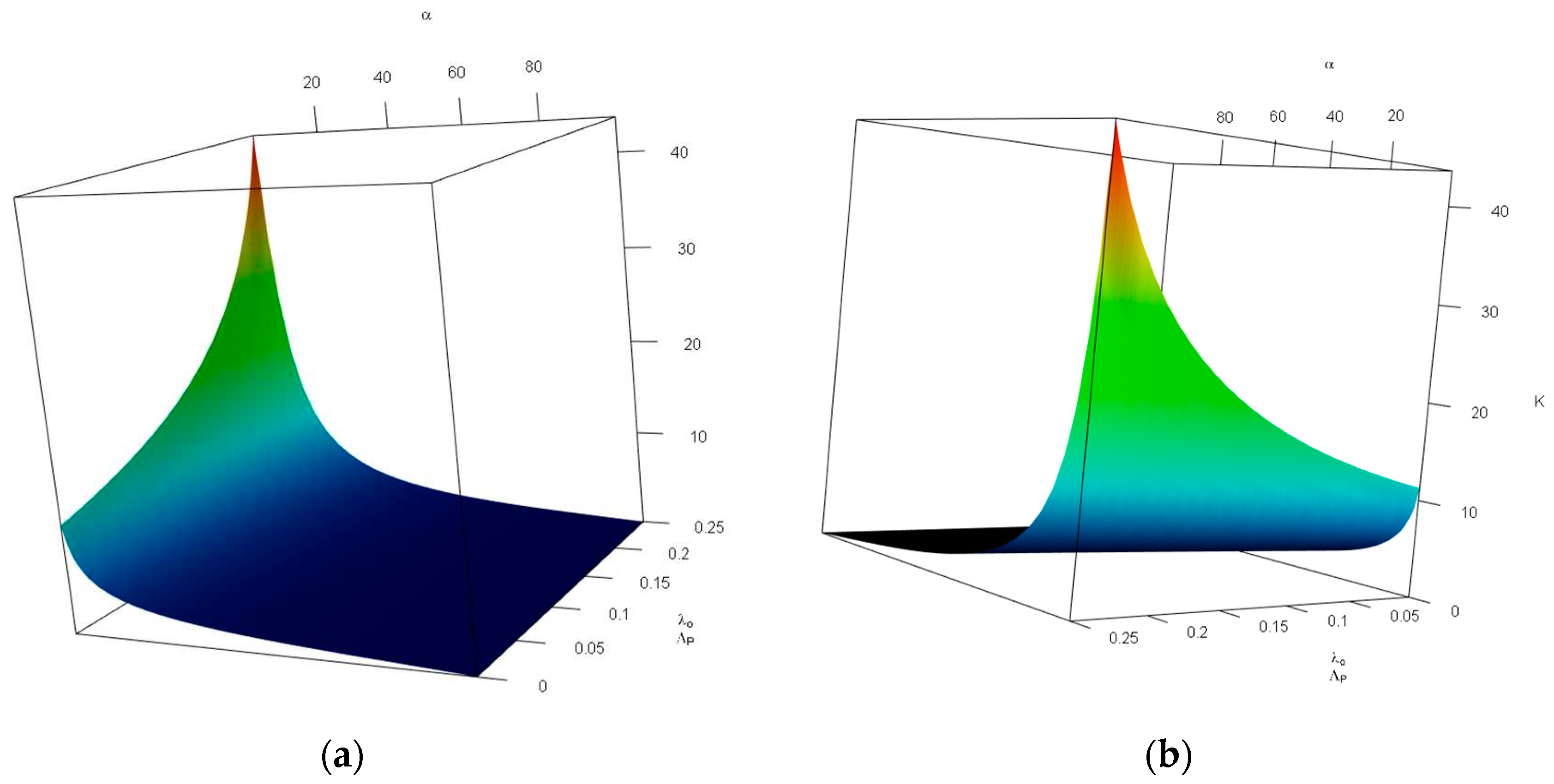
Figure 7.
Changes in
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



