
Submitted:
09 August 2023
Posted:
11 August 2023
You are already at the latest version
Abstract
Outdoor air pollution is a leading cause of death and premature death globally. Motorcycle-taxi drivers were most at risk associated with occupational exposure to ambient air pollution in urban areas. Therefore, a cross-sectional study was conducted to determine the influencing factors and prediction of lung function impairment in 308 motorcycle-taxi drivers living in Bangkok and adjacent provinces between February and June 2022. The study design included: data collection using questionnaires applied from the Thai version of ATS-DLD-78A: American Thoracic Society Division of Lung Diseases and Department of Disease Control, Ministry of Public Health, Thailand; a collection of respirable dust, and ambient air pollution parameters measured by per-sonal air sampling pump and real-time air quality index (AQI) station, and lung function determined by the spirometer. The results showed that 14 factors were significantly associated with lung function impairment (p<0.05). Apparently, seven influencing factors showing the most association were included: gender, the height of the subjects, history of allergies, exposure to respirable dust, mask types, helmet types, and family history of lung disease. The lung function impairment of motorcycle-taxi drivers was significantly predicted in 28.1% by regression analysis of these seven variables (R2=0.281). Therefore, this is the first report on influencing factors and prediction of lung function impairment among motorcycle-taxi drivers. These findings would be very useful for preventing and controlling measure ambient air pollution, setting policies and strategies to mitigate the risks for motorcycle-taxi drivers and the other ex-posed population.
Keywords:
respirable dust
; lung function impairment
; motorcycle taxi driver
1. Introduction
Ambient air pollution is a leading cause of death and premature death worldwide, with more than the estimated number of approximately 3 million premature deaths per year globally (Thurston et al., 2017). The World Health Organization estimates that more than 91% of the world’s population lives in areas where air quality exceeds the recommended values (World health organization, 2016). The significant air pollution that can affect health is particulate matter (PM). Particulate matter (PM) refers to inhalable particles, composed of carbon monoxide (CO), sulfur dioxide (SO2), nitrogen dioxide (NO2), polycyclic aromatic hydrocarbons (PAHs), mineral dust, or water. PM can be of different sizes and is generally defined by their aerodynamics. PM is separated into three main groupings: coarse particles (PM10), fine particles (PM2.5), and ultrafine particles (PM0.1), with PM2.5 and PM10 being the most common in the regulatory framework and relevant for health (Zaharia, 2014). PM10 and PM2.5 can enter the respiratory tract through blood flow and infiltrate the processes of various organs. The health effects related to PM exposure include acute upper and lower respiratory diseases, asthma, chronic obstructive pulmonary disease, pneumonia, bronchiolitis, lung cancer, stroke, dermatitis and allergy, neurodegenerative disease, hypertension in cardiovascular disease, premature birth, premature mortality, decreased birth weight, child height and body mass index (Chuang et al., 2020; Cordova et al., 2020; Jiang et al., 2020). The early detection of adverse respiratory exposure to air pollution has been determined by a lung function test, the principle of measuring the volume and flow rate of exhaled breath or breathing in the patient (American Thoracic Society, 2000; Summacheeva Foundation, 2018). Several studies reveal that lung function impairment was associated with exposure to PM10, PM2.5, PM1, PAHs, NO, and NO2 (Daleck et al., 2021; Yang et al., 2020).
In Thailand, the average concentration of PM10 and PM2.5 has tended to exceed the standard from 2010 to 2020, which averages high to a level that affects people’s health. Especially, Bangkok and adjacent urban provinces with terrible traffic had an average annual concentration of PM2.5 equal to 25 µg/m3 (range 6-40 µg/m3). Most of the yearly average exceeds Thailand’s and WHO standards (15 µg/m3 and 5 µg/m3) (Pollution Control Department, 2022). Motorcycle-taxi drivers are the groups of informal workers at high risk of exposure to ambient air pollution. Around 76.0% of them work in the central region of Thailand (Bureau of Highway Safety, 2021). They must drive to pick up or drop off passengers outside the building throughout their working hours, on average 10 hours per day, ranging from 4-19 hours per day (Pannipa Suebsuk et al., 2014). Therefore, there is a chance of exposure to ambient air pollution than in other occupations. In addition, a few previous studies have focused on health risk levels to benzene, toluene, ethylbenzene, and xylenes (BTEX) and carbonyl compounds (CCs) inhalation exposure of traffic policemen working in the inner city of Bangkok, commuters, exposure to BTEX in public transportation modes in Bangkok, assessing the risk and BTEX exposure among car park workers and occupational exposure of gasoline station workers to BTEX compounds in Bangkok (Kanjanasiranont et al., 2017; Loonsamrong et al., 2017; Ongwandee & Chavalparit, 2010; Tunsaringkarn et al., 2012).
Nowadays, the problems of the heavy traffic around Bangkok and adjacent provinces, motorcycle-taxi services are more popular used than cars or public buses for daily paratransit to provide more convenient, faster trips, and save time in areas, i.e., high traffic congestion, high density residential, and narrow dead-end street, etc. (Raphiphan et al., 2014). At present, the increasing number of registered motorcycles in Thailand amounted to approximately 21.7 million units (Traffic, 2022). However, up to date, motorcycle-taxi drivers exposed to respiratory dust or ambient air pollution causing lung function disorders have been rarely documented. It still requires more evidence to assess the effect of ambient PM on lung function among motorcycle-taxi drivers. Therefore, this study determined the assessment of the associations between exposure to respiratory dust in the working environment and lung function decline including predictions of lung function impairment among motorcycle-taxi drivers in Bangkok and adjacent provinces in Thailand. This finding provided the crucial information on the prediction of influencing factors associated with lung function impairment to assist in proper preventing actions and controlling strategies.
2. Materials and Methods
2.1. Study Area
The motorcycle taxi drivers were selected from the central region of Thailand. Those areas included Bangkok, Nonthaburi, Pathum Thani, Samut Prakan, Samut Sakhon, and Nakhon Pathom. Bangkok and adjacent provinces occupying 7,762 square kilometers (Department of Provincial Administration, 2020) with a population of 10,899,786 people and 5.6 million inhabitants (National Statistical Office, 2021). The data collection was grouped into six areas, as shown in Figure 1.
2.2. Study Design and Participants
A cross-sectional study was conducted among motorcycle taxi drivers who worked in ambient outdoor air between February and June 2022. The motorcycle taxi drivers aged over 20 years were randomly chosen. The total number of motorcycle taxi drivers were estimated 135,231 people in the studied areas (Department of Land Transport, 2021). A total of 308 studied subjects were determined using proportionate stratified sampling and distributed in each province by purposive sampling. Determining the sample size in cases where the questionnaire required a proportional conclusion and the sample size to have a confidence interval (1-α) was based on Equation (1). The calculated number of motorcycle taxi drivers in each province is shown in Table 1. The recruitment process was based on the inclusion and exclusion criteria. These inclusion and exclusion criteria for the study are shown in Table 2.
where; n= sample size, N = population, p = the portion of the population to have reasonable access (p = 0.5), e = tolerance interval or a specified proportion of the population for a given confidence level (e = 0.05, Z=1.96) (Yamane, 1973).
According to the number calculated to represent each motorcycle taxi driver group, all samples must have a negative result for COVID-19 with a screening antigen test kit prior to interview. The staff and the sample group strictly followed the procedures to prevent the spread of COVID-19 by the Ministry of Public Health (Ministry of Public Health, 2021; Simaporn Promsarn & Lertritwimarnman., 2020).
2.3. Data Collection
2.3.1. Data of Participants
All participants were face-to-face interviewed completely by questionnaires before examining their lung function test. Data collection in the questionnaires included: personal characteristics, respiratory symptoms (cough, phlegm, wheeze, and chest tightness), and work characteristics. The participant's identification was also measured their height and weight (checking obese participants, if the participant was unable to stand to have their height measured, arm span was used instead). Their age, sex, and race were also recorded. Subsequently, the participants who were recruited in this study did not become sick with the following symptoms or diseases: non-specific respiratory disease (NSRD): chronic respiratory symptoms (persistent cough, and phlegm: PCP), NSRD; chronic bronchitis, or bronchial asthma: (Uma Sawetskulanont, 1997), thoracic, abdominal or cerebral aneurysms, recent eye hemoptysis of unknown origin, pneumothorax, unstable cardiovascular status, recent myocardial infarction or pulmonary embolism surgery, acute disorders affecting test performance, such as nausea or vomiting, recent thoracic or abdominal surgical procedures. These symptoms were the exclusion criteria for recruiting the studied participants in this study.
2.3.2. Ambient Air Pollution Parameters
Data of ambient air pollution parameters were retrieved from the database of the Pollution Control Department. The questionnaires were applied from Thai version of ATS-DLD-78A: American Thoracic Society Division of Lung Diseases and Department of Disease Control, Ministry of Public Health, Thailand (Doungrutai Boudoung, 1999). Additionally, the exposure to respirable dust parameter of participants were measured using the personal air sampling pumps with an aluminum cyclone and PVC membrane filter of 5.0 µm pore size (UNIVERSAL PCXR8, SKC, Inc., USA). Personal air sampling pumps were calibrated and set up at 2.5 litre/minute; NIOSH Method 0600 using the technique of gravimetric (filter weight), gravimetric for analyzing the mass of respirable dust in the air (National Institute for Occupational Safety and Health, 1998).
Lung function test were measured using a calibrated portable spirometer (UNIVERSAL PCXR8, SKC, Inc., USA). Participants performed the lung function test in a standing position (Milanese et al., 2021; Redlich et al., 2014; Simaporn promsarn & lertritwimanman, 2020). The forced vital capacity (%FVC), % forced expiratory volume in 1 sec (%FEV1), forced expiratory volume in 1 sec/forced vital capacity (FEV1/FVC), and forced expiratory flow between 25% and 75% expired volumes (FEF25-75%) were measured. The predicted values were calculated in accordance with the National Health and Nutrition Survey III equations (Hankinson et al., 1999), adjusted for Asian ethnicity (Hankinson et al., 2010). %FEV1 and %FVC greater than 80% predicted and FEV1/FVC ratio greater than 70% predicted were used as the criteria for normal lung function.
2.4. Ethical Approval
Ethical approval to conduct this study was received from the Human Research Ethics Committee of Thammasat University, No.3. Ethical approval number 031/2565, and the approval date was 29 April 2022.
2.5. Data Analysis
The data were analyzed using Statistical Package for Social Sciences (SPSS version 23). Descriptive statistics such as frequency and percentage were used for analyzing the socio-demographic, work characteristics, respiratory symptoms of participants, exposure to respirable dust concentration, the 24-hour average concentration of PM2.5 and PM10, and lung function test. Pearson's correlation coefficient was used to determine the association between those variables and percentages for FVC. Furthermore, regression analysis was used to identify the factors significantly associated with predicted percentages for FVC and predict its possible occurrence. The regression analysis was also run to predict lung function impairment.
Before using regression analysis, several key assumptions were considered: the linear correlation was confirmed between percentages for FVC and the independent variables. The use of scatter plots showed whether there was a linear correlation. There were no multivariate normality and multicollinearity. Variance Inflation Factor (VIF) values and homoscedasticity were tested as assumption. A plot of standardized residuals versus predicted values showed whether points were equally distributed across all values of the independent variables. All key assumptions were passed for testing as shown in Figure 2.
3. Results
3.1. Demographic, Work Characteristics, and Respiratory Symptoms of Participants
Table 3 demonstrated the general profile, work characteristics, and respiratory symptoms of the sample population. There were 308 respondents, including 33 females and 275 males. The results showed that 89.3% of the male participants were between 40-59 years old, the education level was primary education (48.8%), most of them were married (62.7%), 45.1% of the participants have never smoked before, there was no the history of the COVID-19 patient (70.1%), most of the participants did not exercise (54.2%), which may result in the body mass index exceeding the Asia-Pacific guidelines: BMI>23.0 kg/m2 standard (64.9%). About 85.4% and 75.3% of the participants had no diabetes and hypertension, respectively. Most of the participants (42.6%) had more than 10 years of experience in this occupation and took 11 hours a day to perform tasks. Their resting places while waiting for passengers were near the road (85.4%). Types of equipment they wore while performing the task was a surgical mask (94.5%). Cotton and N95 respirator masks were rarely used. In addition, they wore an open-face helmets while working. However, while waiting for passengers in the resting place, they did not wear masks. Based on the data, the participants had only mild respiratory system symptoms.
3.2. The 24 Hours Average Concentration of PM2.5 and PM10 in Bangkok and Adjacent Provinces
The 24 hours average concentration of PM2.5 ranged from 5-33 µg/m3, with the highest PM2.5 concentration level at the Bangkok monitoring site and the lowest PM2.5 concentration at Nonthaburi and Samut Prakan province. These data from all real-time air quality index (AQI) stations were lower than Thailand’s standard. However, the maximum 24-hour average for all stations were higher than the air quality of WHO standard. The 24 hours average concentration of PM10 varied from 11-70 µg/m3. The highest PM10 concentration level was detected in Bangkok, while the lowest PM2.5 concentration level was at Samut Prakan province. The average PM10 concentration in all the locations were lower than Thailand’s standard. However, Bangkok and Pathum Thani province had PM10 concentrations level higher than the air quality of WHO standard (world Health Organization, 2021). All details can be considered in Table 5.
3.3. Exposure to Respirable Dust Concentration while Performing Tasks
Similar Exposure Groups (SEGs) were used to identify groups performing tasks experiencing the same general exposure to risks. The motorcycle taxi drivers from all six provinces were classified into six groups (SEG 1-6) depending on the level of PM10 and PM2.5 concentration level from real-time air quality index (AQI) stations. The information on respirable dust concentration from air personal sampling was presented in Table 6.
3.4. Lung Function Tests (LFTs)
Approximately 28.9% of the participants had a lung function impairment, with 24.7% of lung function impairment being restrictive lung disorder based on the criterion of the American Thoracic Society. All details can be considered in Table 7.
3.5. Association between Independent Variables and Lung Function Impairment
The association between the 14 independent variables and lung function impairment were analyzed using Pearson’s correlation coefficient, as shown in Table 8. The lung function impairment in this study was described in terms of predicted percentages for forced vital capacity (FVC).
The results showed that the correlation between the province, gender, family history of lung disease, height, hypertension, types of helmet, wearing a cotton mask, exposure to respirable dust concentration, wind direction and lung function impairment was low negative. On the other hand, there was a low positive correlation between distance from resting places while waiting for passengers with real-time air quality index (AQI) station, history of allergies, PM2.5, SO2, temperature and lung function impairment.
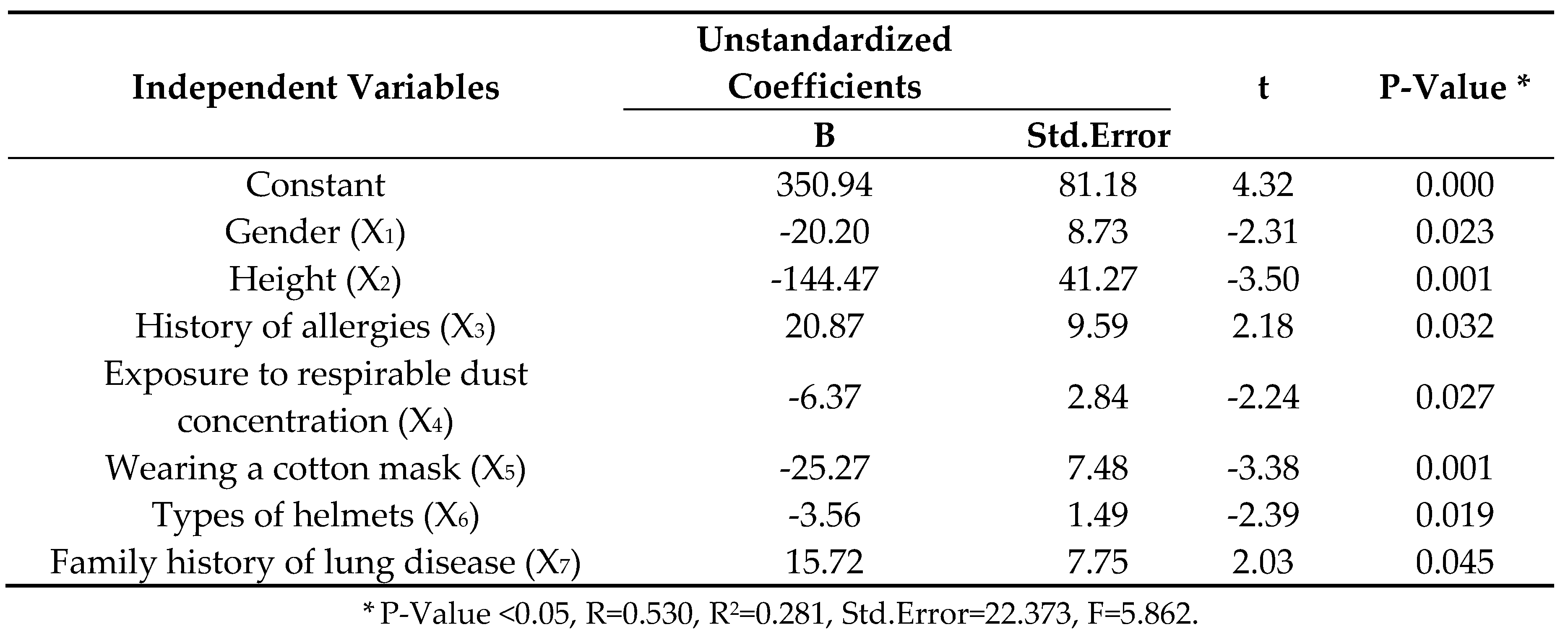
All significant variables were included in the model for their correlation with lung function impairment. Regression analysis covers fourteen affected variables from those analyses. Only seven influencing variables were tested using regression analysis as shown in Table 9. The regression analysis model formula was shown in Equation (2). A regression analysis model was run to predict the lung function impairment of motorcycle taxi drivers from seven influencing factors fairly total of 28.1% (R2=0.281), which was a moderate fit for the data.
where; Y= Lung function impairment was described in terms of predicted percentages for forced vital capacity (FVC), X1 = Gender (1 = Male, 2 = Female), X2 = Height (meter), X3 = History of allergies (1 = Yes, 2 = No), X4 = Exposure to respirable dust concentration (mg/m3), X5 = Wearing a cotton mask (1 = No, 2 = Yes), X6 = Types of helmet (1= Full, 2 = Open, 3 = Half), X7 = Family history of lung disease (1 = Yes, 2 = No).
Y= 350.939 – 20.204X1 – 144.465X2 + 20.867X3 – 6.370X4 – 25.269X5 – 3.563X6 + 15.721X7
4. Discussion
The motorcycle taxi drivers of Bangkok and adjacent provinces in Thailand have been heavily exposed to high concentrations of ambient air pollution and the impact of this on their lungs has been neither documented nor studied. The exposure to respirable dust concentration was negatively associated with %FVC (p<0.05) among motorcycle taxi drivers. These findings were consistent with the previous study (Aretz et al., 2021; Dauchet et al., 2018; Guo et al., 2019; Hou et al., 2020; Johannson et al., 2018; Ma et al., 2021; Syahira et al., 2020; Yang et al., 2021). Our study collected respirable dust exposure by air personal sampling. Those previous studies collected air pollution by using real-time air quality index (AQI) station. However, both of two methods sampling showed exactly correlation with lung function impairment. The advantage of air personal sampling showed the participants were actually exposed to respirable dust when compared to ambient air pollution sampling. Therefore, air personal sampling study had a more clearly relationship to the respiratory system among outdoor workers than an area sampling. It was evident from this study that demographic factors used to predict lung function impairments were gender(p=0.023) and height(p=0.001). Most participants were males (89.3%) with a mean height of 165.75+6.99 ranged from 149–185 centimeters because qualifications of this occupation require physical fitness and using driving skills (Ben Saad et al., 2014; China et al., 2020; Kan et al., 2007; Thanapon Lertchittasakul et al., 2019; Wang et al., 2020). In addition, The Global Lung Function Initiative has defined height as one of the other prediction equations for spirometry (Quanjer et al., 2012). Our study showed the positive correlation with lung function impairment as history of allergies(p=0.032), a family history of lung disease (p=0.045) that reversibility to inhaled bronchodilators is a marker of bronchial involvement in patients with allergic rhinitis, even in the absence of overt chest symptoms. Also reported that the duration of allergic rhinitis was related to the deterioration of nasal airflow limitation, indicating a close relation between nasal and bronchial airflow (Ciprandi & Cirillo, 2006). Furthermore, the genetic composition of an individual may be considered for monitoring and identifying people at risk of respiratory illnesses, as the results of studies in India and Canada (Okeleji et al., 2021; T.Warkentin et al., 2019; Thayyezhuth et al., 2021). There was a significant relationship between safety equipment and lung function impairment; wearing a cotton mask (p=0.001) and types of helmets (p=0.019)due to the theory that the self-protection against small particles entering the respiratory tract has to wear dust masks (Barry S. Levy et al., 2011), but in this study, we found that participants who wore a cotton mask during work of 7.1% had a negative relationship to the lung function impairment. Cotton masks were ineffective enough in filtering small particles that make their way into the respiratory tract; several studies found that personal masks were associated with respiratory diseases, especially must at least N95 to be effective against fine particulate matter enough (Chaaban et al., 2022; Paranthaman et al., 2022; Tanawat Rakkamon et al., 2015). Types of helmet help prevent traffic accidents, especially the head (Jenson & Unnikrishnan, 2015; Li et al., 2020). In addition, we also found association between a full face of helmets and lung function impairment because those devices had a face shield to protect against particulate matter while riding a motorcycle.
A regression analysis model was run to predict the lung function impairment of motorcycle taxi drivers from seven influencing factors fairly total of 28.1% (R2=0.281), which was a moderate fit for the data. Based on previous literature, there were demographics, health status, safety equipment, and air pollution exposure factors associated with lung function impairment which could predict lung function impairment by multiple logistic regression analysis. Nevertheless, those studies conducted in different occupations, ages, and the number of samples (Siriorn Sindhu et al., 2011; Tanawat Rakkamon et al., 2015; Ueyama et al., 2021).
5. Conclusions
Seven significantly influenced variables that could predict motorcycle taxi drivers' lung function impairment was 28.1%. The successful instrument used to understand individual impairment of lung function of motorcycle taxi drivers, including similar outdoor workers. The development of model in order to promote the preventive measures of respirable dust exposure of outdoor workers and ambient air pollution to be effective and lead to sustainable practices. The main limitation of this study was the lack of some data about personal air sampling in the working area due to budget constraints. Therefore, SEGs were used to represent the respirable dust concentration exposure of the sample group. Consequently, future research could improve the reliability of the data by collecting all personal air sampling and should be evaluated model to predict lung function impairment based on significant variables. Our findings may help policymakers develop effective policies and communication strategies to mitigate the hazards of respiratory systems among motorcycle taxi drivers.
Author Contributions
Conceptualization, Kimihito Ito and Orasa Suthienkul; Methodology, Arroon Ketsakorn; Software, Kamonwan Samana; Formal analysis, Kamonwan Samana; Investigation, Kamonwan Samana; Resources, Kamonwan Samana; Data curation, Kimihito Ito; Writing – original draft, Orasa Suthienkul; Writing – review & editing, Arroon Ketsakorn; Visualization, Kimihito Ito; Supervision, Orasa Suthienkul; Project administration, Arroon Ketsakorn; Funding acquisition, Arroon Ketsakorn.
Acknowledgments
This research project was supported by the National Research Council of Thailand (NRCT): NRCT5-RGJ63008-103.
Conflicts of Interest
The authors declare no conflict of interest.
References
- American Thoracic Society. What constitutes an adverse health effect of air pollution? American journal of respiratory and critical care medicine 2000, 161, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Aretz, B., Janssen, F., Vonk, J. M., Heneka, M. T., Boezen, H. M., & Doblhammer, G. (2021). Long-term exposure to fine particulate matter, lung function and cognitive performance: A prospective Dutch cohort study on the underlying routes. Environmental Research, 201, 111533. [CrossRef]
- Barry S. Levy, David H. Wegman, Sherry L. Baron, & Sokas, R. K. (2011). Occupational and environmental health: recognizing and preventing disease and injury (sixth ed.). Oxford university press.
- Ben Saad, H., Selmi, H., Hadj Mabrouk, K., Gargouri, I., Nouira, A., Said Latiri, H., Maatoug, C., Bouslah, H., Chatti, S., & Rouatbi, S. (2014). Spirometric “Lung Age” estimation for North African population. Egyptian Journal of Chest Diseases and Tuberculosis, 63(2), 491-503. [CrossRef]
- Bureau of Highway Safety, D. o. H. (2021). Traffic volume on highways in Bangkok Metropolitan Region. Available online: http://bhs.doh.go.th/download/traffic.
- Chaaban, O., Balanay, J. A. G., & Sousan, S. (2022). Assessment of best-selling respirators and masks: Do we have acceptable respiratory protection for the next pandemic? American Journal of Infection Control. [CrossRef]
- China, N., Vaz, D., Martins, C., Gomes, J., Ladeira, I., Lima, R., & Guimarães, M. (2020). Obtaining spirometric reference values when height is not available – comparison of alternative anthropometric measures. Pulmonology, 26(4), 198-203. [CrossRef]
- Chuang, K.-J.; Lin, L.-Y.; Ho, K.-F.; Su, C.-T. Traffic-related PM2.5 exposure and its cardiovascular effects among healthy commuters in Taipei, Taiwan. Atmospheric Environment: X 2020, 7, 100084. [Google Scholar] [CrossRef]
- Ciprandi, G., & Cirillo, I. (2006). The lower airway pathology of rhinitis. Journal of Allergy and Clinical Immunology, 118(5), 1105-1109. [CrossRef]
- Cordova, J. E. D.; Aguirre, V. T.; Apestegui, V. V.; Ibarguen, L. O.; V, B. N.; Steenland, K.; Rengifo, G. F. G. Association of PM2.5 concentration with health center outpatient visits for respiratory diseases of children under 5 years old in Lima, Peru. Environmental Health 2020, 19, 1–6. [Google Scholar]
- Daleck, A.; Wigmann, C.; Kress, S.; Altug, H.; Jirik, V. e.; Heinrich, J.; Abramson, M. J.; Schikowski, T. The mediating role of lung function on air pollution-induced cardiopulmonary mortality in elderly women: The SALIA cohort study with 22-year mortality follow-up. International Journal of Hygiene and Environmental Health 2021, 233, 113705. [Google Scholar] [CrossRef] [PubMed]
- Dauchet, L.; Hulo, S.; Cherot-Kornobis, N.; Matran, R.; Amouyel, P.; Edme, J.-L.; Giovannelli, J. Short-term exposure to air pollution: Associations with lung function and inflammatory markers in non-smoking, healthy adults. Environment International 2018, 121, 610–619. [Google Scholar] [CrossRef]
- Department of Land Transport, M. o. T. (2021). The Number of Driving Licences and Transport Personnel Licences Classified by Type. Available online: https://web.dlt.go.th/statistics/.
- Department of Provincial Administration, M. o. I. (2020). Area classified by region and province, year 2011 - 2020.
- Doungrutai Boudoung. (1999). Effect of Respirable Particulates on Lung Function among Traffic Policemen in Bangkok Chulalongkorn University].
- Guo, H., Sahu, S. K., Kota, S. H., & Zhang, H. (2019). Characterization and health risks of criteria air pollutants in Delhi, 2017. Chemosphere. [CrossRef]
- Hankinson, J. L., Kawut, S. M., Shahar, E., Smith, L. J., Stukovsky, K. H., & Barr, R. G. (2010). Performance of American Thoracic Society-recommended spirometry reference values in a multiethnic sample of adults: the multi-ethnic study of atherosclerosis (MESA) lung study. chest, 137(1), 138-145. [CrossRef]
- Hankinson, J. L., Odencrantz, J. R., & Fedan, K. B. (1999). Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med, 159(1), 179-187. [CrossRef]
- Hou, D., Ge, Y., Chen, C., Tan, Q., Chen, R., Yang, Y., Li, L., Wang, J., Ye, M., Li, C., Meng, X., Kan, H., Cai, J., & Song, Y. (2020). Associations of long-term exposure to ambient fine particulate matter and nitrogen dioxide with lung function: A cross-sectional study in China. Environment International, 144, 105977. [CrossRef]
- Jenson, D., & Unnikrishnan, V. U. (2015). Energy dissipation of nanocomposite based helmets for blast-induced traumatic brain injury mitigation. Composite Structures, 121, 211-216. [CrossRef]
- Jiang, Y., Chen, J., Wu, C., Lin, X., Zhou, Q., Ji, S., Yang, S., Zhang, X., & Liu, B. (2020). Temporal cross-correlations between air pollutants and outpatient visits for respiratory and circulatory system diseases in Fuzhou, China. BMC Public Health, 20:1131, 1-13. [CrossRef]
- ohannson, K. A.; Vittinghoff, E.; Morisset, J.; Wolters, P. J.; Noth, E. M.; Balmes, J. R.; Collard, H. R. Air Pollution Exposure Is Associated With Lower Lung Function, but Not Changes in Lung Function, in Patients With Idiopathic Pulmonary Fibrosis. Chest 2018, 154(1), 119–125. [Google Scholar] [CrossRef] [PubMed]
- Kan, H., Heiss, G., Rose, K. M., Whitsel, E., Lurmann, F., & London, S. J. (2007). Traffic exposure and lung function in adults: the Atherosclerosis Risk in Communities study. Thorax, 62, 873-879. [CrossRef]
- Kanjanasiranont, N., Prueksasit, T., & Morknoy, D. (2017). Inhalation exposure and health risk levels to BTEX and carbonyl compounds of traffic policeman working in the inner city of Bangkok, Thailand [Article]. Atmospheric Environment, 152, 111-120. [CrossRef]
- Li, J., Ma, T., Huang, C., Huang, X., Kang, Y., Long, Z., & Liu, M. (2020). Protective Mechanism of Helmet Under Far-field Shock Wave. International Journal of Impact Engineering, 143, 103617. [CrossRef]
- Loonsamrong, W., Taneepanichskul, N., Puangthongthub, S., & Tungsaringkarn, T. (2017). Health Risk Assessment and BTEX Exposure among Car Park Workers at a Parking Structure in Bangkok, Thailand [article in journal/newspaper]. Journal of Health Research; Vol 29 No 4: July - August 2015; 285-292 ; 2586-940X ; 0857-4421. Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,sso&db=edsbas&AN=edsbas.4A273663&authtype=sso&custid=s4775581&site=eds-live&scope=site&custid=s4775581.
- Ma, H., Liu, F., Yang, X., Liu, Q., Wang, X., Xing, X., Lin, Z., Cao, J., Li, J., Huang, K., Yan, W., Liu, T., Fan, M., Chen, S., Lu, X., Gu, D., & Huang, J. (2021). Association of short-term fine particulate matter exposure with pulmonary function in populations at intermediate to high-risk of cardiovascular disease: A panel study in three Chinese cities. Ecotoxicology and Environmental Safety, 220, 112397. [CrossRef]
- Milanese, M., Corsico, A. G., Bellofiore, S., Carrozzi, L., Di Marco, F., Iovene, B., Richeldi, L., Sanna, A., Santus, P., Schisano, M., Scichilone, N., Vancheri, C., & Cerveri, I. (2021). Suggestions for lung function testing in the context of COVID-19. Respiratory Medicine, 177, 106292. [CrossRef]
- Ministry of Public Health. (2021, November 30,2021). Public Health practices for preventing the spread of COVID-19 safety measures for organizations. Available online: https://stopcovid.anamai.moph.go.th/attach/w774/f20211201211017_iXg45j3zsx.pdf (accessed on 19 November 2022).
- National Institute for Occupational Safety and Health. (1998). Particulates not otherwise regulated, respirable 0600. In (3 ed., pp. 1-6).
- National Statistical Office, N. (2021). Number of employed people in formal and informal workers Classified by age group, sex, region and province, 2011 - 2020. Retrieved August 16. Available online: http://statbbi.nso.go.th/staticreport/page/sector/th/02.aspx.
- Okeleji, L. O., Ajayi, A. F., Adebayo-Gege, G., Aremu, V. O., Adebayo, O. I., & Adebayo, E. T. (2021). Epidemiologic evidence linking oxidative stress and pulmonary function in healthy populations. Chronic Diseases and Translational Medicine, 7(2), 88-99. [CrossRef]
- Ongwandee, M., & Chavalparit, O. (2010). Commuter exposure to BTEX in public transportation modes in Bangkok, Thailand [Article]. Journal of Environmental Sciences, 22(3), 397-404. [CrossRef]
- Pannipa, Suebsuk; Pongnumkul, Autchariya; Leartsudkanung, Darunee; Sareewiwatthana, Penchun. Predicting Factors of Lung Function Among Motorcycle Taxi Drivers in the Bangkok Metropolitan Area. Journal of Public Health 2014, 44(1), 79–92. [Google Scholar]
- Paranthaman, M. P., Peroutka-Bigus, N., Larsen, K. R., Phadke, K. S., Summers, T., Theodore, M., Hensley, D. K., Levine, A. M., Lee, R. J., & Bellaire, B. H. (2022). Effective antiviral coatings for deactivating SARS-CoV-2 virus on N95 respirator masks or filters. Materials Today Advances, 14, 100228. [CrossRef]
- Pollution Control Department. (2022). Overall air quality reporting. Available online: www.air4thai.pcd.go.th (accessed on 22 October 2022).
- Quanjer, P. H., Stanojevic, S., Cole, T. J., Baur, X., Hall, G. L., Culver, B. H., Enright, P. L., Hankinson, J. L., Ip, M. S. M., Zheng, J., & Stocks, J. (2012). Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. European Respiratory Journal, 40(6), 1324-1343. [CrossRef]
- Raphiphan, P., Zaslavsky, A., & Indrawan-Santiago, M. (2014). Building Knowledge from Social Networks on What is Important to Drivers in Constrained Road Infrastructure. Procedia Computer Science, 35, 720-729. [CrossRef]
- Redlich, C. A.; Tarlo, S. M.; Hankinson, J. L.; Townsend, M. C.; Eschenbacher, W. L.; Essen, S. G. V.; Sigsgaard, T.; Weissman, D. N. Official American Thoracic Society Technical Standards: Spirometry in the Occupational Setting. American journal of respiratory and critical care medicine 2014, 189, 984–994. [Google Scholar] [CrossRef] [PubMed]
- Simaporn, promsarn; lertritwimanman, P. New normal in spirometric procedures. Thai Journal of Tuberculosis Chest Disease and Critical Care 2020, 39(2), 76–81. [Google Scholar]
- Simaporn, Promsarn; Lertritwimarnman, P. New normal in Spirometric Procedures. Thai Journal of Tuberculosis Chest Disease and Critical Care 2020, 39, 76–81. [Google Scholar]
- Siriorn, Sindhu; Kamlungdee, Umaporn; Konggumnerd, R. Effect of smoke exposure on lung function among adults in communities. Thai Journal of Nursing Council 2011, 26(3), 93–106. [Google Scholar]
- Summacheeva Foundation. (2018). Guideline for Standardization and Interpretation of Pulmonary Function Test by Spirometry in Occupational Health Setting.
- Syahira, M. P. A., Karmegam, K., Diyana, M. Y. N. A., Irniza, R., Bahri, M. T. S., Vivien, H., Maizura, H. N., & Sivasankar, S. (2020). Impacts of PM2.5 on respiratory system among traffic policemen. 25-29. [CrossRef]
- Warkentin, T.M.; Lam, S.; Hung, R. J. Determinants of impaired lung function and lung cancer prediction among never-smokers in the UK Biobank cohort. EBioMedicine 2019, 47, 58–64. [Google Scholar] [CrossRef] [PubMed]
- Tanawat, Rakkamon; Na-songkhla, Thitima; Chuchuag, Varintip; Issara, O. Factors associated with pulmonary function among workers exposing ammonia from fresh natural latex purchasing process at rubber holder cooperative in Southern, Thailand. Disease Control Journal 2015, 41(4), 285–296. [Google Scholar]
- Thanapon Lertchittasakul, Arun Laoarun, & Boonsong, P. (2019, 26-28 June 2019). Quality of life of public motorcycle riders in Bangkok a case study in Thungkru, Rat Burana, Phasi Charoen, Bangkok Noi, Bang Khae district. The 4th National RMUTR Conference and The 1st International RMUTR Conference, Bangkok. 28 June.
- Thayyezhuth, D., Venkataram, R., Bhat, V. S., & Aroor, R. (2021). A study of Spirometric parameters in non asthmatic allergic rhinitis. Heliyon, 7(11), e08270. 11. [CrossRef]
- The National Environment Board. (2022, July 8, 2022). The standard for particulate matter less than 2.5 microns in the ambient air. Available online: http://www.ratchakitcha.soc.go.th/DATA/PDF/2565/E/163/T_0021.PDF (accessed on 13 November 2022).
- Thurston, G. D., Kipen, H., Annesi-Maesano, I., Balme, J., Brook, R. D., Cromar, K., Matteis, S. D., Forastiere, F., Forsberg, B., Frampton, M. W., Grigg, J., Heederik, D., Kelly, F. J., Kuenzli, N., Laumbach, R., Peters, A., Rajagopalan, S. T., Rich, D., Ritz, B., . . . Brunekreef, B. (2017). A joint ERS/ATS policy statement: what constitutes an adverse health effect of air pollution? An analytical framework. Eur Respir J, 49, 1-19. [CrossRef]
- Traffic, T. L. V. R. (2022). Number of registered motorcycles in Thailand from 2012 to the first eight months of 2021. Retrieved April13. Available online: https://www.statista.com/statistics/1179962/thailand-number-of-registered-motorcycles/.
- Tunsaringkarn, T., Siriwong, W., Rungsiyothin, A., & Nopparatbundit, S. (2012). Occupational Exposure of Gasoline Station Workers to BTEX Compounds in Bangkok, Thailand [article]. The International Journal of Occupational and Environmental Medicine, 3(3), 117-125. Available online: https://search.ebscohost.com/login.aspx?direct=true&AuthType=ip,sso&db=edsdoj&AN=edsdoj.3c553ee2a08748358625c2010fa3f3a6&authtype=sso&custid=s4775581&site=eds-live&scope=site&custid=s4775581.
- Ueyama, M., Hashimoto, S., Takeda, A., Maruguchi, N., Yamamoto, R., Matsumura, K., Nakamura, S., Terada, S., Inao, T., Kaji, Y., Yasuda, T., Hajiro, T., Tanaka, E., Taguchi, Y., & Noma, S. (2021). Prediction of forced vital capacity with dynamic chest radiography in interstitial lung disease. European Journal of Radiology, 142, 109866. [CrossRef]
- Uma Sawetskulanont. (1997). Effects of particulate matter on Tc-99m DTPA lung clearance in traffic policemen in Bangkok Metropolis Chulalongkorn University].
- Wang, Y.; Wang, T.; Xu, M.; Yu, H.; Ding, C.; Wang, Z.; Pan, X.; Li, Y.; Niu, Y.; Yan, R.; et al. Independent effect of main components in particulate matter on DNA methylation and DNA methyltransferase: A molecular epidemiology study. Environment International 2020, 134, 105296. [Google Scholar] [CrossRef] [PubMed]
- World health organization. (2016). Air pollution. Available online: https://www.who.int/health-topics/air-pollution#tab=tab_2.
- world Health Organization. (2021, 22 September 2021). Ambient (outdoor) air pollution. Available online: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 13 November 2022).
- Yamane, T. (1973). Statistics. An introductory analysis. Third edition. Harper & Row. Available online: https://books.google.co.th/books?id=sl75MgEACAAJ.
- Yang, M.; Guo, Y.-M.; Bloom, M. S.; Dharmagee, S. C.; Morawska, L.; Heinrich, J.; Jalaludin, B.; Markevychd, I.; Knibbsf, L. D.; Lin, S.; et al. Is PM1 similar to PM2.5? A new insight into the association of PM1 and PM2.5 with children’s lung function. Environment International 2020, 145, 106092. [Google Scholar] [CrossRef] [PubMed]
- Yang, T., Chen, R., Gu, X., Xu, J., Yang, L., Zhao, J., Zhang, X., Bai, C., Kang, J., Ran, P., Shen, H., Wen, F., Huang, K., Chen, Y., Sun, T., Shan, G., Lin, Y., Wu, S., Zhu, J., . . . Wang, C. (2021). Association of fine particulate matter air pollution and its constituents with lung function: The China Pulmonary Health study. Environment International, 156, 106707. [CrossRef]
- Zaharia, C. (2014). Particulate matter (settled particles, coarse PM10, fine PM2.5 or PM1, ultrafine particles) in urban atmosphere: characteristics, quality control and health effects. In (pp. 221-244).
Figure 1.
Six studied location of Bangkok and adjacent provinces in Thailand.
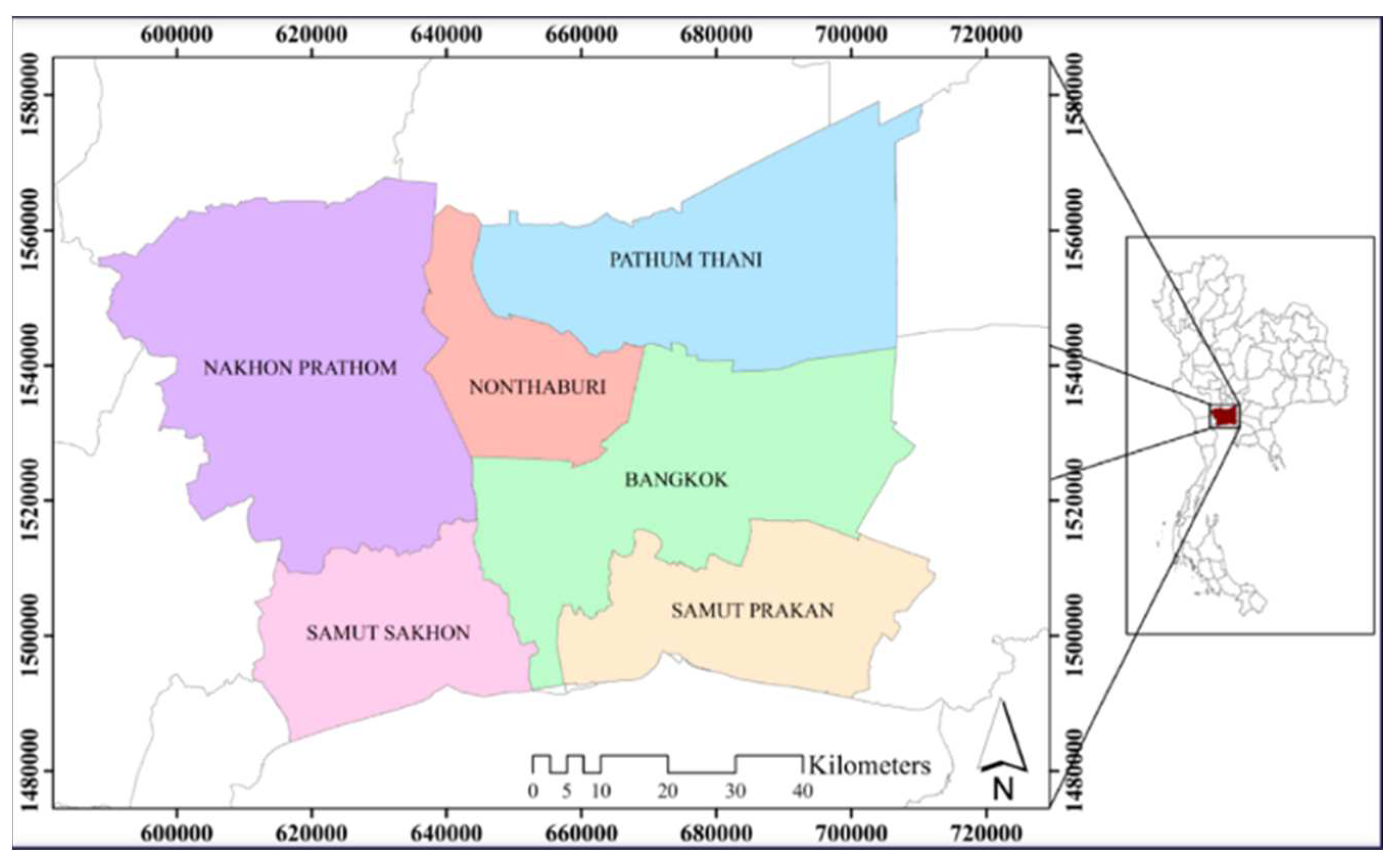
Figure 2.
(a) Normal P-P plot of regression standardized residual; (b) Scatterplot regression standardized residual and regression standardized predicted value.
Figure 2.
(a) Normal P-P plot of regression standardized residual; (b) Scatterplot regression standardized residual and regression standardized predicted value.
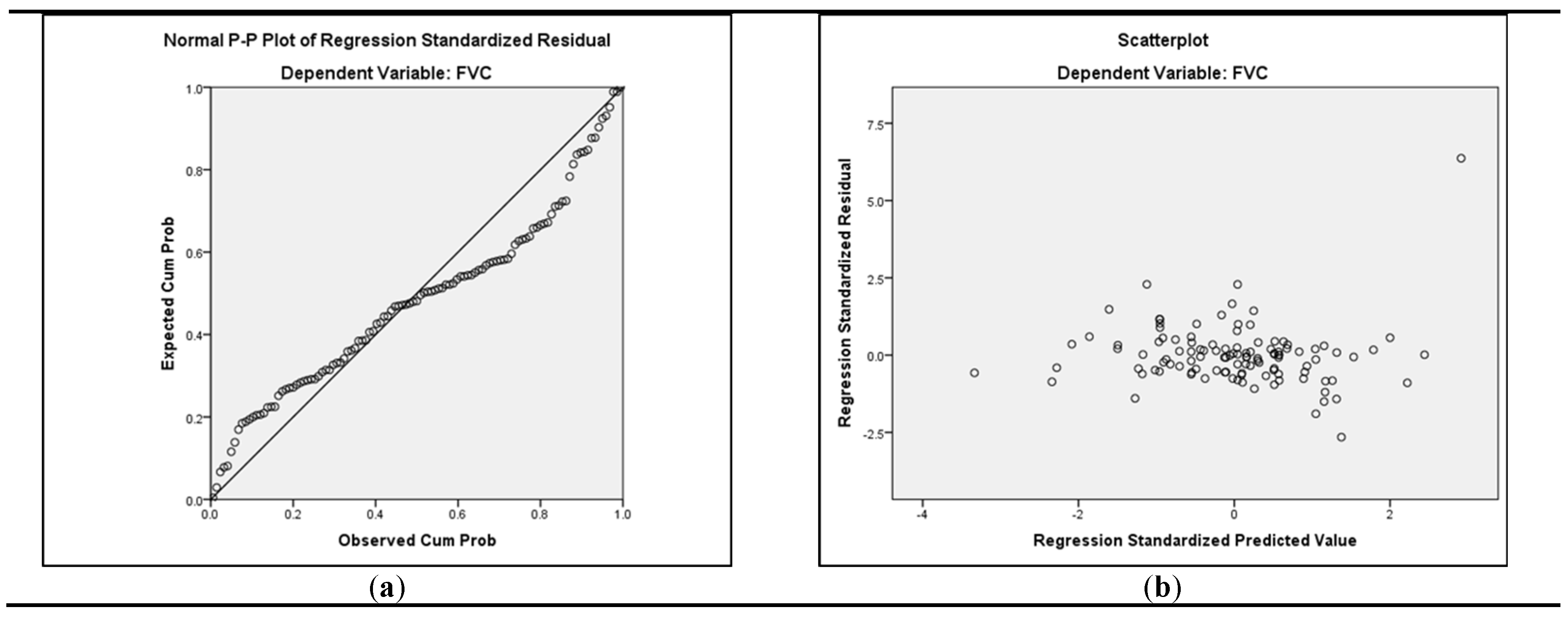

Table 1.
The studied number of motorcycle-taxi drivers in each province (n=308).
| Province | Number of Motorcycle Taxi Drivers 1 | Sample Size |
|---|---|---|
| Bangkok | 84,889 | 152 |
| Nonthaburi | 10,346 | 33 |
| Pathum Thani | 11,543 | 32 |
| Samut Prakan | 17,218 | 44 |
| Samut Sakhon | 4,949 | 35 |
| Nakhon Pathom | 6,286 | 12 |
| Total | 135,231 | 308 |
1 source: Department of Land Transport, Thailand (2020).
Table 2.
Inclusion and exclusion criteria for a cross-sectional study of motorcycle taxi drivers.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| - Over 20 years of age | - Diagnosis of chronic respiratory disease or any other chronic respiratory disease. |
| - Motorcycle taxi drivers who worked in ambient outdoor more than one year in Bangkok and adjacent provinces. | - Any acute or chronic condition that would limit the ability of the subject to participate in the study. |
| - Thai nationality and able to speak Thai language. | - Having an intermittent period working outdoor such as a stopping to work for other jobs outdoor and moving to indoor for doing work. |
| - Refusal to give informed consent. |
Table 3.
Lung function testing criteria.
| Activity | Length of Time to Stop before Lung Function Testing |
|---|---|
| Drinking alcohol | 4 hours |
| Eating a large meal | 2 hours |
| Vigorous exercise | 30 minutes |
| Smoking | >1 hour |
| For reversibility testing | |
| Taking short-acting bronchodilators | 6 hours |
| Taking long-acting bronchodilators (including combination inhalers) or twice-daily preparations | 24 hours |
| Taking tiotropium or once-daily preparations | 48 hours |
Table 4.
Demographic, work characteristics, and respiratory symptoms of participants (n=308).
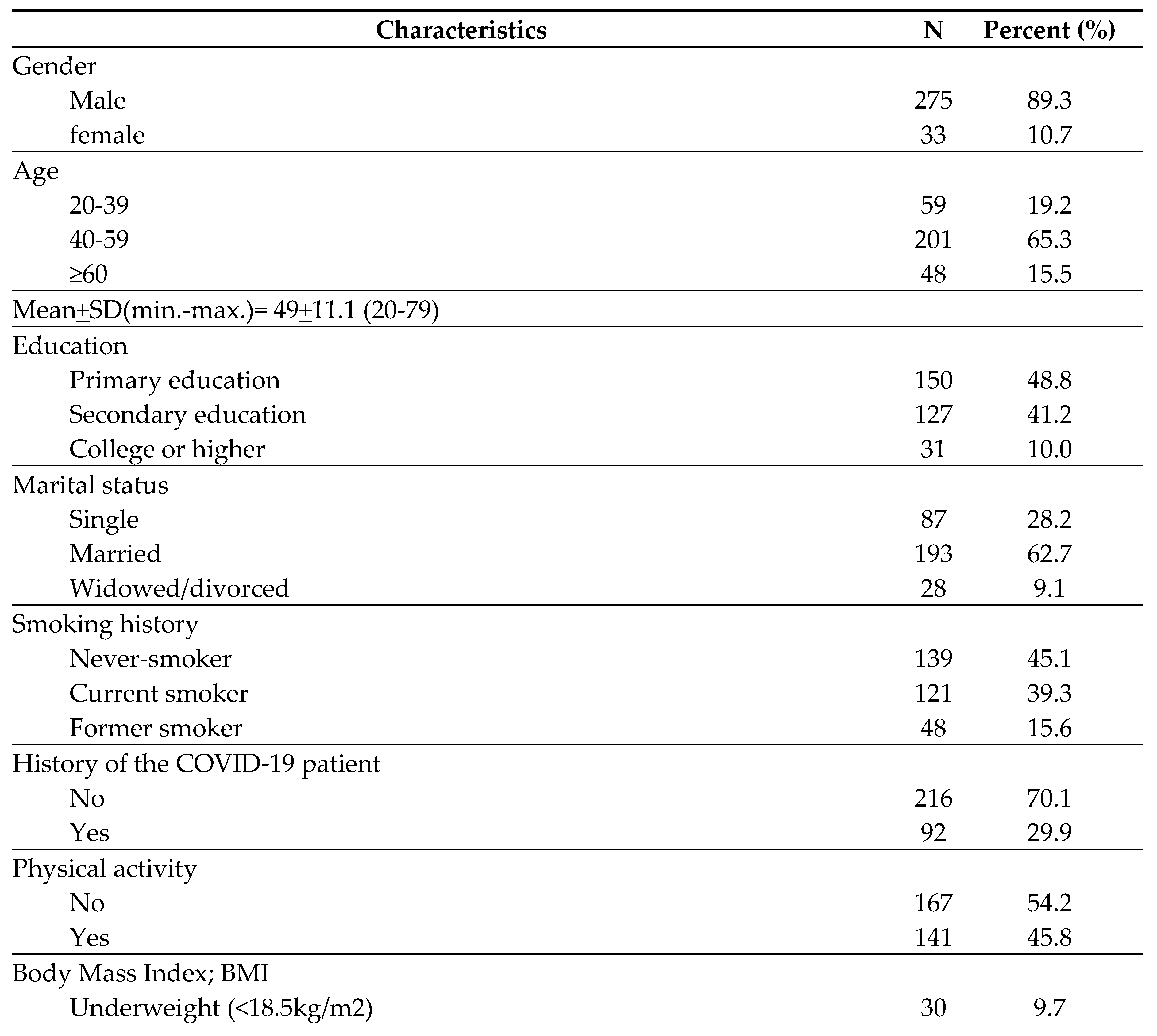
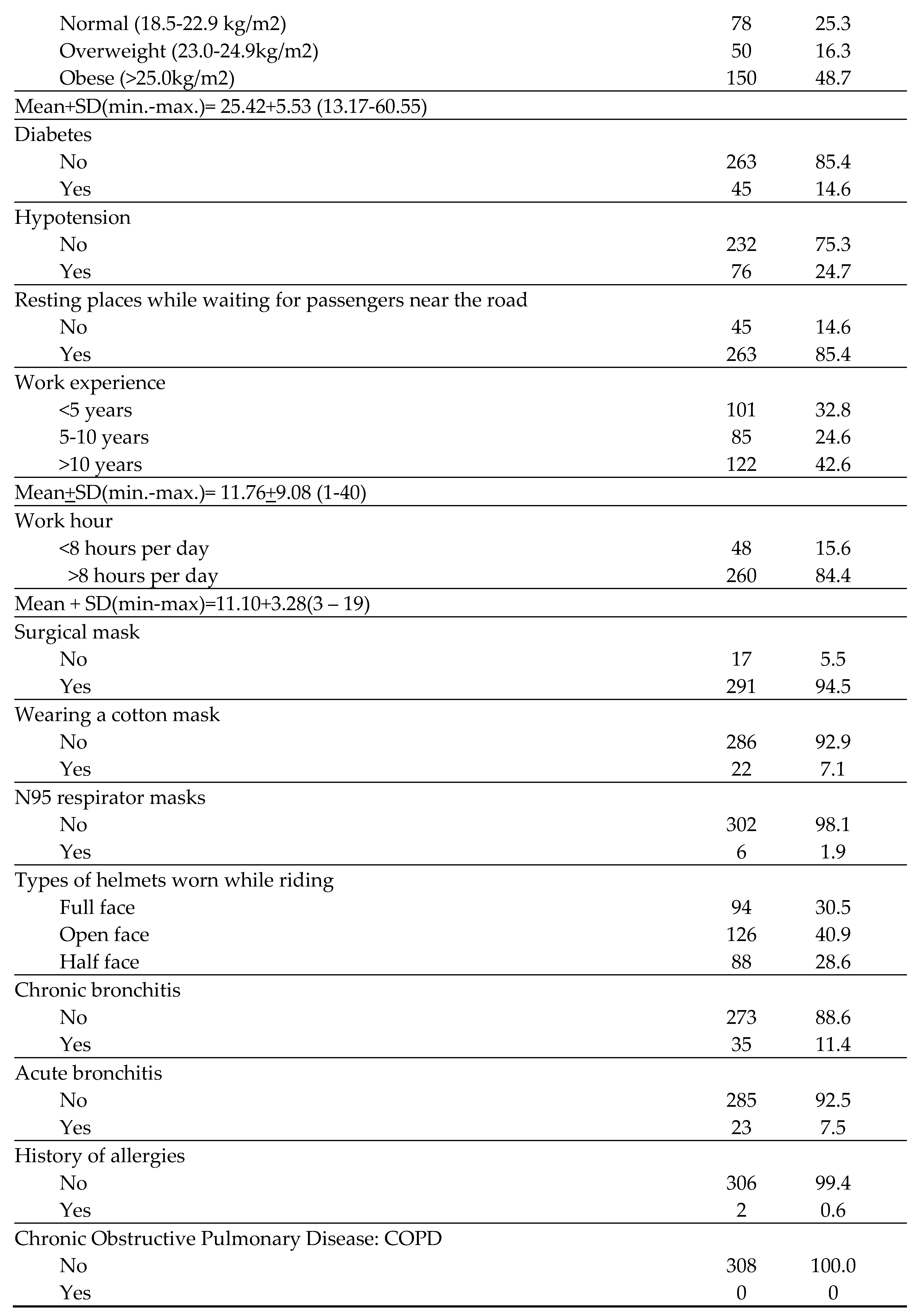
Table 5.
The 24 hours average concentration level of PM2.5 and PM10 in Bangkok and adjacent provinces.
Table 5.
The 24 hours average concentration level of PM2.5 and PM10 in Bangkok and adjacent provinces.
| Province | Station | PM2.5 (µg/m3) | PM10 (µg/m3) | ||||
|---|---|---|---|---|---|---|---|
| rangea | meanb | >stdc | rangea | meanb | >stdc | ||
| Bangkok | Din Daeng Community Housing | 17-33 | 23 | 0/30 | 38-70 | 51 | 0/30 |
| Pathum Thani | Bangkok University | 5-21 | 12 | 0/28 | 17-53 | 31 | 0/28 |
| Nonthaburi | Sukhothai Thammathirat Open University | 5-20 | 10 | 0/30 | - | - | - |
| Samut Prakan | Disabled and Handicapped Vocational Rehabilitation Center Station | 5-22 | 11 | 0/30 | 11-34 | 20 | 0/30 |
| Samut Sakhon | Samut Sakhon Highway District | 12-30 | 17 | 0/30 | - | - | - |
| Nakhon Prathom | Water supply reservoir | 6-21 | 10 | 0/30 | 13-40 | 21 | 0/30 |
The source of data was retrieved from the Pollution Control Department of Thailand. (Pollution Control Department, 2022). a minimum-maximum; b PM10 and PM2.5 concentration level average; c frequency of exceeding Thailand standard (The National Environment Board, 2022).
Table 6.
The concentration of respirable dust from air personal sampling each SEG (n=153).
| SEG | Work Performing Area | Number of Workers | Personal Air Samplings (Psoint) | Respirable Dust Concentration (mg/m3) | ||
|---|---|---|---|---|---|---|
| Max. | Min. | Mean | ||||
| SEG1 | Bangkok- Din Daeng District | 152 | 57 | 0.365 | Not detected | 0.029 |
| SEG2 | Pathum Thani- Khlong Nueng Subdistrict, Khlong Luang District | 32 | 21 | 0.094 | 0.003 | 0.024 |
| SEG3 | Nonthaburi- Sukhothai Thammathirat Open University | 33 | 15 | 0.018 | 0.002 | 0.006 |
| SEG4 | Samut Prakan- Song Khanong Subdistrict, Phra Pradaeng District | 44 | 34 | 0.025 | Not detected | 0.009 |
| SEG5 | Samut Sakhon- Om Noi Subdistrict, Krathum Baen District | 35 | 16 | 0.027 | 0.001 | 0.008 |
| SEG6 | Nakhon Prathom- Nakhon Pathom Subdistrict, Mueang District | 12 | 10 | 0.018 | Not detected | 0.008 |
Table 7.
Lung function test of the participants (n=308).
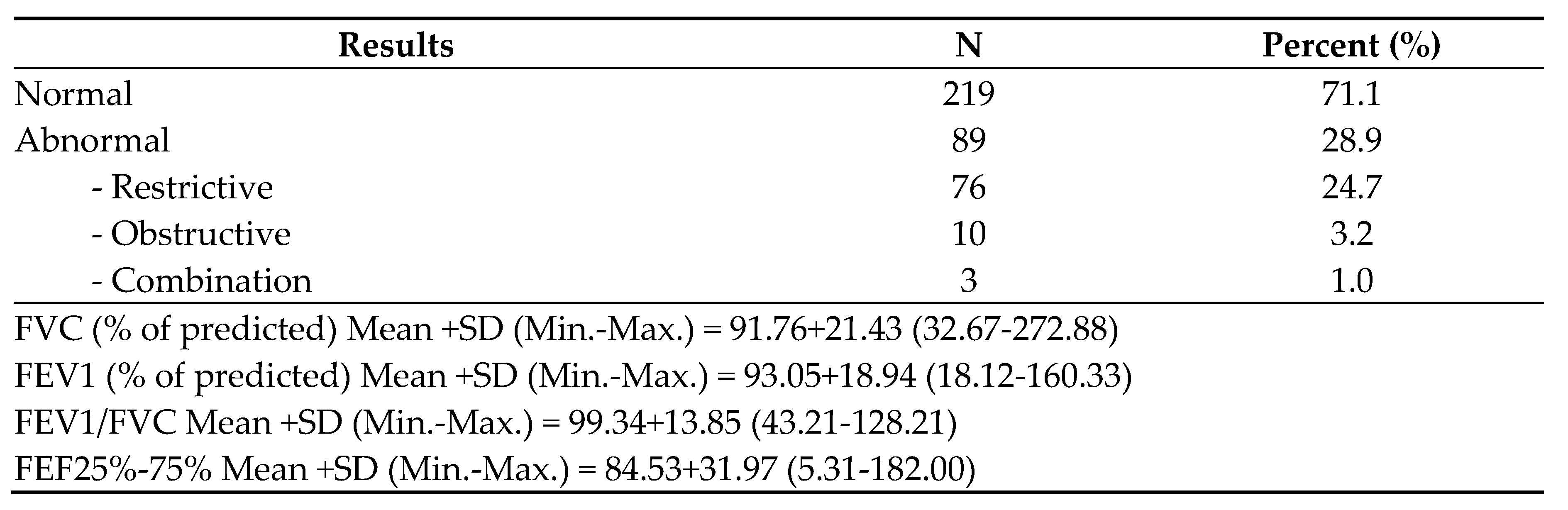
Table 8.
Association between independent variables and lung function impairment(n=308).
| Independent Variables | Pearson’s Correlation | P-Value * |
|---|---|---|
| Province | -0.18 | 0.002 |
| Gender | -0.13 | 0.028 |
| Distance from resting places while waiting for passengers with real-time air quality index (AQI) station | 0.20 | 0.001 |
| Family history of lung disease | -0.15 | 0.011 |
| Height | -0.13 | 0.028 |
| Hypertension | -0.13 | 0.021 |
| Types of helmet | -0.12 | 0.035 |
| Wearing a cotton mask | -0.15 | 0.009 |
| History of allergies | 0.15 | 0.007 |
| Exposure to respirable dust concentration | -0.11 | 0.047 |
| PM2.5 | 0.14 | 0.017 |
| SO2 | 0.17 | 0.003 |
| Wind direction | -0.14 | 0.015 |
| Temperature | 0.02 | <0.001 |
* p-value < 0.05.
Table 9.
Regression analysis model for predicting the lung function impairment (n=308).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



